
Nucleic acid metabolism lecture nam03
24
Dr. Aga Syed Sameer CSIR Lecturer (Demonstrator) Department of Biochemistry, Medical College, Sher-I-Kashmir Institute of Medical Sciences, Bemina, Srinagar, Kashmir, 190010. India. Nucleic Acid Metabolism Purine Catabolism Errors of NAM
-
Upload
aga-syed-sameer -
Category
Science
-
view
90 -
download
5
Transcript of Nucleic acid metabolism lecture nam03

Dr. Aga Syed SameerCSIR Lecturer (Demonstrator)
Department of Biochemistry,
Medical College,
Sher-I-Kashmir Institute of Medical Sciences,
Bemina, Srinagar, Kashmir, 190010. India.
Nucleic Acid MetabolismPurine CatabolismErrors of NAM

Nucleic Acid Digestion
• Ingested nucleic acids are degraded to nucleotides
• by pancreatic nucleases, and
• intestinal phosphodiesterases in the intestine
• Group-specific nucleotidases and non-specific phosphatases degrade nucleotides into nucleosides

Nucleic Acid Digestion• Direct absorption of nucleosides
• Further degradation Nucleoside + H2O → Base + Ribose
(nucleosidase)
Nucleoside + Pi → Base + R-1-phosphate
(n. phosphorylase)
MOST INGESTED NUCLEIC ACIDS ARE DEGRADED AND EXCRETED

Purine Degradation• All purine degradation leads to uric acid (but it might not
stop there)
• Nucleotides broken into nucleosides by action of 5’-nucleotidase (hydrolysis reactions)
• Xanthine is the point of convergence for the metabolism of the purine bases
• Xanthine is then converted into Uric acid by the action of Xanthine oxidase
• Purine ribonucleotide degradation pathway is same for purine deoxyribonucleotides

Xanthine Oxidase• A homodimeric protein
• Contains electron transfer proteins
• FAD
• Mo-pterin complex in +4 or +6 state
• Two 2Fe-2S clusters
• Transfers electrons to O2 H2O2
• H2O2 is toxic
• Disproportionated to H2O and O2 by Catalase

Purine Degradation• Adenosine is deaminated to Inosine by ADA
• Purine nucleoside phosphorylase (PNP) then catalyses the conversions as:
• Inosine Hypoxanthine
• Xanthosine Xanthine
• Guanosine Guanine
• Ribose-1-Phosphate then splits offCan be isomerized to ribose-5-phosphate

Purine Degradation

Purine Degradation
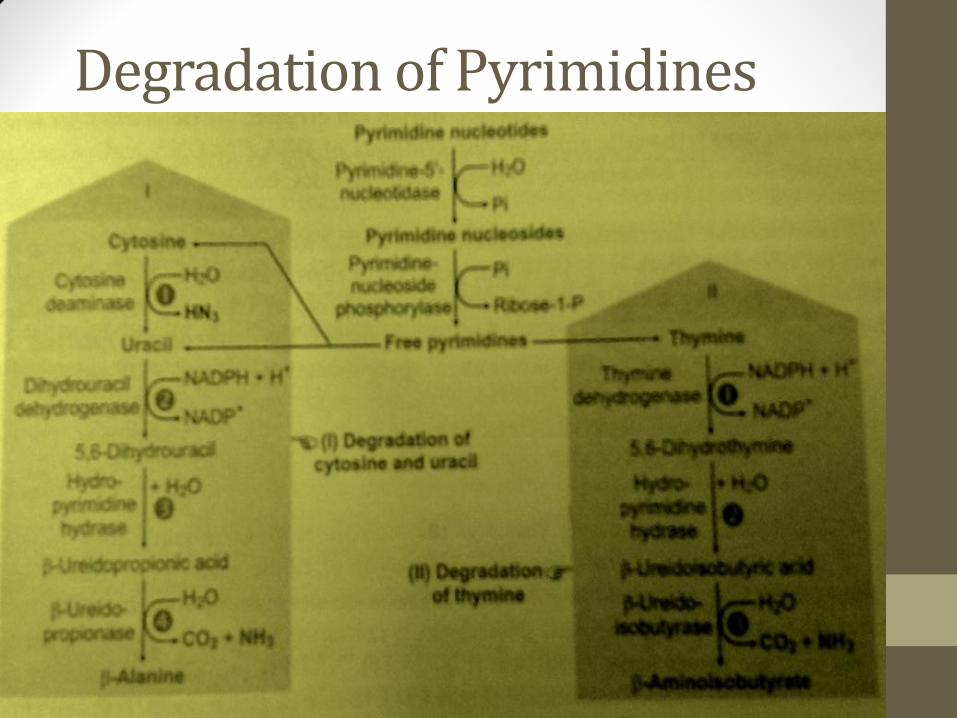
Degradation of Pyrimidines

Degradation of Pyrimidines• CMP and UMP degraded to bases similarly to purines
• Dephosphorylation
• Deamination
• Glycosidic bond cleavage
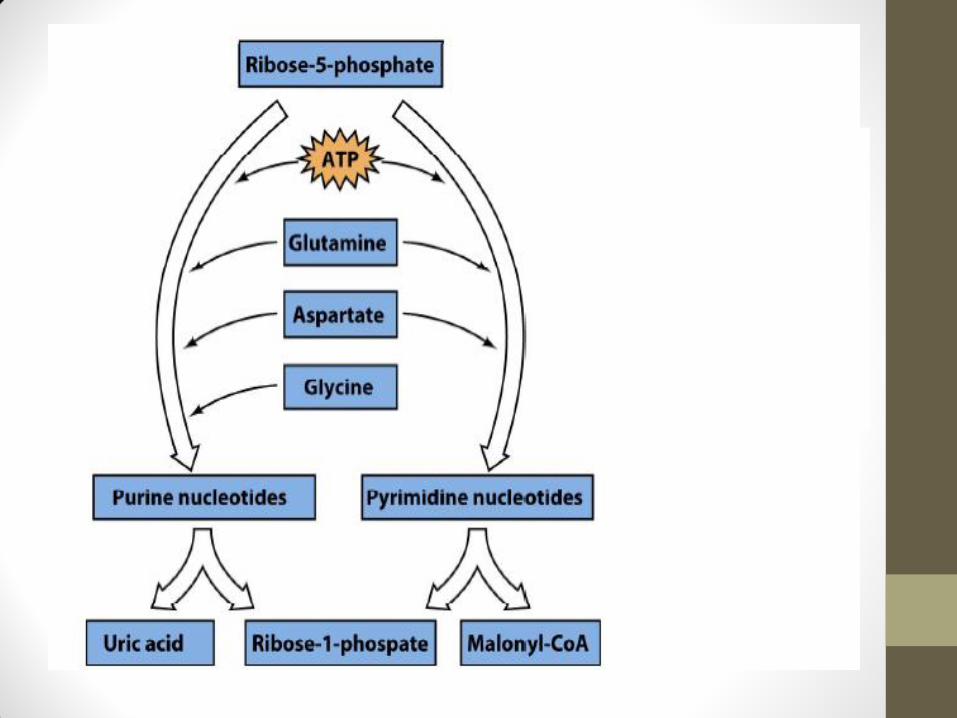
• Uracil reduced in liver, forming β-Alanine
• Is then converted to malonyl-CoA used in fatty acid synthesis for energy metabolism
• dTMP is degraded to β-Amino Isobutyrate
• Is then converted to methyl malonyl-CoA used in fatty acid synthesis for energy metabolism
Inborn Metabolic Errors

Gout• Group of disorders - Impaired excretion or
overproduction of uric acid
• Uric acid crystals as Sodium Urate precipitate into joints (Gouty Arthritis), kidneys, ureters (stones)
• Lead also impairs uric acid excretion – lead poisoning from pewter drinking goblets
• Deposits of Sodium Urate form Tophi in the joints and lead to inflammation; causes chemotaxis of Granulocytes which in turn phogocytize Urate Crytals
• Phagocytosis leads to production of ROS’s leading to tissue damage

Gout• Due to change in environment, lactate production in
synovial joints increases leading to decrease in pH which fosters further deposition of sodium urate crystals
• Gout may be Primary & Secondary
• Primary is due to cumulative defect in the purinemetabolism and regulation leading to increased synthesis of Purines
• Secondary results from cancer, polycythemia, renal insufficiency etc

Gout

Gout

• Xanthine oxidase inhibitors
inhibit production of uric acid, modality for treating gout symptoms
• Allopurinol treatment
hypoxanthine analog that binds to Xanthine Oxidase to decrease uric acid production
• Cholchicine treatment
is used to decrease the movement of granulocytes into the affected area
Management

Management by Allopurinol• Allopurinol is purine base analog
• Three mechanisms• Allopurinol is oxidized to alloxanthine by xanthine oxidase
• Then Allopurinol and alloxanthine are inhibitors of xanthine oxidase
• This inhibition decreases urate formation
• Then concentrations of Allopurinol and alloxanthineincrease but do not precipitate as urate does.
• Hypoxanthine and Xanthine concentration also increases but it is relatively more soluble than uric acid
• Allopurinol and alloxanthine are excreted into the urine

Mechanism of Action

Lesch-Nyhan Syndrome• A defect in production or activity of HGPRT
• X linked defect more manifested in Males
• Causes increased level of Hypoxanthine and Guanine (↑in degradation to uric acid)
• Also, PRPP accumulates stimulates production of purine nucleotides (and thereby increases their degradation)
• Causes gout-like symptoms, but also neurological symptoms of spasticity, aggressiveness, self-mutilation
• First neuropsychiatric abnormality that was attributed to a single enzyme

Adenosine Deaminase Deficiency
• Results in SCID “Severe Combined Immunodeficiency”
• It selectively kills lymphocytes, as ADA has highest activityin cytosol of lymphocytes• Results in adenosine accumulation which in turn is converted to
dATP. ↑dATP causes inhibition of Ribonuleotide Reductase
• Both B- & T-Cells are lacking from the immune system of the affected patient
• Both of these are otherwise known to mediate much of the immune response
• Death usually occurs within two years of birth

Purine Autism• 25% of autistic patients may overproduce purines
• To diagnose, must test urine over 24 hours
• Biochemical findings from this test disappear in adolescence
• Must obtain urine specimen in infancy, but it’s difficult to do!
• Pink urine due to uric acid crystals may be seen in diapers

Others Errors
• Orotic Aciduria: Type I and II• Defective Orotate Phosphoribosyl Transferase and OMP
Decarboxylase
• Growth Retardation and Megaloblastic Anaemia
• Reye’s Syndrome:• Secondary Orotic Aciduria
• Defective/Deficiency of Mitochondrial OrnithineTranscarbamoylase (of urea cycle)
• Carbamoyl Phosphate of Mitochondria fails to get efficiently converted to Citrulline; enters cytosol, leading to overproduction of pyrimidines – especially Orotic Acid


















![8. nucleic acid metabolism [compatibility mode]](https://static.fdocuments.in/doc/165x107/5875b2721a28ab8b618b6631/8-nucleic-acid-metabolism-compatibility-mode.jpg)