November 2015 IMMUNE DESIGN - Jefferies · Phases 1 and 2 Underway ... Wayne Gombotz, PhD Chief...
28
IMMUNE DESIGN November 2015
Transcript of November 2015 IMMUNE DESIGN - Jefferies · Phases 1 and 2 Underway ... Wayne Gombotz, PhD Chief...

IMMUNE DESIGN
November 2015

2
Forward-looking Statements
This presentation contains forward-looking statements with respect to, among other things,
our business, financial condition, strategy and prospects, and has been prepared solely for
informational purposes. All statements, other than statements of historical fact, regarding
our strategy, potential future products, prospects, plans, opportunities and objectives
constitute “forward-looking statements.” These statements are not guarantees of future
performance and involve a number of unknown risks, assumptions, uncertainties and
factors that are beyond our control. Given these risks, assumptions and uncertainties, you
should not place undue reliance on these forward-looking statements.
Important factors that could cause actual results to differ materially from those indicated
by such forward-looking statements include, among others, our history of net losses and
expected net losses for the foreseeable future, that we have no product candidates
approved for commercialization and may never achieve profitability, that we will require
additional capital to finance our operations, that we may not be able to successfully
develop, obtain regulatory approval and commercialize our product candidates, all of
which are novel and in early clinical development, and those other risks that will be set
forth under the header “Risk Factors,” “Note Regarding Forward-Looking Statements” and
“Management’s Discussion and Analysis of Financial Condition and Results of Operations” in
our periodic reports filed with the Securities and Exchange Commission, including our
Quarterly Report for the period ended September 30, 2015. All statements contained in this
presentation are made only as of the date of this presentation and are subject to
uncertainty and changes. Except as required by law, we expressly disclaim any
responsibility to update such forward-looking statements, whether as a result of new
information, future events or otherwise.

3
Two types of CTL-
based Therapies
Two Main I-O
Categories
Adoptive T cell
transfer (CAR-T, TCR)
(personalized,
ex vivo)
Next-gen cancer
vaccination
(Off-the-shelf,
in vivo)
Remove the
Blockade
(checkpoint
inhibitors)
CD8 T cells
(CTLs)
tumor
killing
Immuno-Oncology The next pillar of
cancer treatment
Focused in Immuno-oncology to Induce T Cells in vivo
Two Product
Candidates
Clarifying the Landscape
Two Distinct
Approaches
Tumor
Blockade Killer T cells
CMB305
G100

4
CMB305: NY-ESO-1 first-in-class cancer vaccine
G100: intra-tumoral immune activation
Phase 2 and 1b
Initial PoC
readouts in 2016
Clinical validation
of MOAs in
Phase 1 trials
Validating
Partnerships
Onc: MRK, GNE
ID: Sanofi, Medi
Allergy: Sanofi
Finances enable
initial PoC
Tumor-induced
Immune
Blockade
Tumor
Killer T cells
Create the Army (IMDZ) + Remove the Defenses (CPIs)
Designed to make “cold tumors hot, and hot tumors hotter”
Re-arming Your Body with Next-gen Vaccination
Experienced Team
Platform beyond
current products

Innovative in vivo Product Candidates & Distinct MOAs
5
Four Partnered Non-oncology Programs
Two
Discovery
Platforms
Single or
Multi-MOA
Candidates
CMB305 LV305 “Prime” (vector+RNA Ag) & G305 “Boost” (TLR4+protein Ag)
G100 Potent TLR4 agonist
DC targeted to induce and expand Ag-
specific cytotoxic T cells
Activates DCs to present endogenous
Ags and expand pre-existing
cytotoxic T cells
Tumor Ag target = NYESO-1 Any antigen present in tumor
Intradermal and IM Injections Intratumoral Injection
ZVex
Platform (DC-tropic Lentivirus)
GLAAS
Platform (Synthetic TLR4 Ag)

CMB305 & G100 PRODUCT CANDIDATES
6

CMB305: Three Step Clinical Development Optimal Approach to Maximize Effectiveness of NY-ESO-1 Killer T cells
STEP 1
STEP 2
STEP 3
Combination
CPI
CMB305 Combined w/ CPI
LV305 G305
CMB305
LV305 G305
CMB305
+
Individual Building Blocks
G305 (GLAAS)
LV305 (ZVex)
Completed:
Data @ ASCO 2015
Ongoing:
Data H1’2016
Ongoing:
Initial Data H2’2016 Collaboration with Genentech
(atezolizumab)
✔
7
Tumor-induced
Immune
Blockade:
CPIs
Tumor
Killer T cells:
CMB305

G305 and LV305 Ph1 Data Support CMB305 Development
G305 LV305 CMB305 Im
munogenic
ity
Safe
ty
Clinic
al
Benefi
t
• Stable disease in 67% of
patients (med: 245d)
• CA125 response
• Stable disease in 67% of
patients (med: 208d)
• Progression cessation and
regression observed
• Favorable single agent
signal in sarcoma (PFR: 67%
(3mo)/42% (6mo))
G305: SD in 8/12pts at d70 (end TX); CA125 response (GCIG criteria) 600(D0)281(D70)207(D242)
LV305: SD in 8/12pts at d70 (end TX); 4/6 pts stopped tumor progression and tumor regression of 14% in one pt w/SD at
347+d; PFR=progression free rate (all LV305 patients had a form of sarcoma)
Ab: 9/12
CD4: 5/11
CD8: 2/10
n=12
CD4: 5/11 CD8: 6/11
n=12
3/11
CMB305
Phases 1
and 2
Underway
Predicted Immunogenicity with Both Agents
Safe (Grade 1-2 AEs only)
Signal of Individual Clinical Benefit
8

LV305 Ph1: NY-ESO-1 T-cell Responses Exceed Published Studies w/
Multiple Agents
9
0
10
20
30
40
50
60
70
80
LV305 2015 (n=12) Odunsi 2012(n=47)
Dhodapkar 2014(n=34)
Chen 2015(Arm A, n=18)
Percentage NY-ESO-1-specific T-cell responses in Patients*
All T cell responders CD4 CD8 CD4 & CD8
Odunsi, et al (2012) Efficacy of vaccination with vaccinia and fowlpox vectors expressing NY-ESO-1, PNAS 109:5797
Dhodapkar, et al (2014) Immunity with a Vaccine Targeting NY-ESO-1 to DEC-205, Sci Transl Med 6:232ra51
Chen, et al (2015) Immune responses with NY-ESO-1 in ISCOMATRIX and NY-ESO-1 fowlpox, Int J Cancer 136:E590 *CD4 and CD8, ELISPOT/ICS/Tetramer
ZVex Fowlpox DEC-205 mAb/NY-ESO-1/ NY-ESO-1 prot/IMX
+ Vaccinia Resiquimod/Poly-I:C + Fowlpox
49% 56%
44%
73%

0
10
20
30
40
50
60
70
80
2nd LineInactive
2nd LineActive
1st LineLow-High
range
IMDZ
PFR % at 3 months
10
0
10
20
30
40
50
60
2nd LineInactive
2nd LineActive
1st LineLow-High
range
IMDZ
PFR % at 6 months
* M. Van Glabbeke, et al. Progression-free rate as the principal end-point for phase II trials in soft-
tissue sarcomas. European Journal of Cancer 38 (2002) 543–549.
LV305 Ph 1:
Clinical Results Suggest Single Agent Activity in Sarcoma
21%
39%
67% 44-77%
8% 14%
>42%
30-56%
Active (low-high range)
Active (low-high range)
• Progression Free Rate (PFR) guides active vs. inactive therapies in Soft Tissue Sarcoma Trials*
• All LV305 patients had ≥ two prior treatments and <10cm in tumor size: 2nd line
• 4/6 patients had arrest of their sarcoma progression and tumor reduction (1/12) while on LV305

CMB305: Targeting NY-ESO-1 in Multiple Solid Tumors
CMB305 Dose Esc.
(LV305 & G305)
Q1’16 Q2’16 Q4’15
CMB305 Phase 1 dose escalation (DE) completed
CMB305 Phase 1 dose expansion in sarcoma, ovarian and lung at optimal
dose (n=32) – started Q3’15/ongoing
CMB305 randomized Phase 2 study with atezolizumab in soft tissue sarcoma
- initiated November ’15
11
CMB305 rPh 2 in Soft Tissue Sarcoma - ONGOING
atezolizumab vs. atezolizumab & CMB305
CMB305 Ph1 Expansion – ONGOING Four tumors - signal seeking for additional indications
Potential: CMB305 Phase 2
Randomized in 2nd Indication
Q3’16

G100: Using a Tumor to Expand the Immune Response
STEP 2
Combination Opportunities with Check-point inhibitors (CPIs)
CPI
+
STEP 1
Single Agent + RadRx
G100
Initial Data
Presented at ASCO 2015
✔ + G100 +
CPI G100 +
Three Features of Intratumoral (i.t) Immune Activation:
1. Tumor lysis (e.g., tumor radiation) releases endogenous tumor antigens
2. i.t. G100 activates the pre-existing immune response and primes a new one to released
tumor antigens
3. i.t. G100 and tumor lysis may eliminate both the treated and distal (non-treated) tumors
(“abscopal effect”).
12
Collaboration with Merck
(KEYTRUDA®)

13
• Cohort A: 2/2 pts with locoregional disease completed G100 followed by surgery plus RT
and are free of recurrence (336+ & 467+ days).
− Pt 002 had a pathologic CR following the G100 injections alone.
• Cohort B: 2/6 patients with metastatic disease have an ongoing PR after 2 cycles of therapy
and are in follow-up.
- Pt 006 had 28% regression in the injected tumor following G100 alone; this regressed
completely after the second cycle consisted of RT plus G100.
0 50 100 150 200 250 300 350 400
001-002
001-004
001-001
001-003
001-005
001-006
001-007
001-008
001-110
DAYS SINCE 1ST DOSE
G100 CLINICAL RESPONSE
Rx: d0,7 (LR) & d21 (Met, each cycle)
Radiation + 6 weekly doses cycles 2-4
NED (incl. surgery and/or XRT)
PR (incl. surgery and/or XRT)
Progressive Disease
Radiation Therapy
Surgery
Locoregional
Metastatic
G100: MCC Phase 1 Combined Treatment ORR of 50%

G100 +/- RadRx: MCC Ph1 –
Orphan; n=10
G100+RadRx +/- KEYTRUDA: f-NHL Ph1/2 Randomized
Orphan; n=30
✔
14
G100: Potential in Wide Range of Accessible Tumors
Q1’16 Q2’16 Q4’15 Q3’16
G100 Ph1 in Merkel cell carcinoma
data presented at ASCO 2015 (n-8/10) – 50% ORR per protocol
Full enrolled – data expected H2’16
Safe (Grade 1/2)
• Ph1/2 G100 + Rad Rx in NHL with/without KEYTRUDA planned for H2’15

Immuno-Oncology (ZVex & GLAAS)
Infection & Allergy (GLAAS)
Phase 2 Phase 1
First-in-class Immunotherapy Pipeline
G103 HSV Vaccine
Food Allergy Vaccine
RSV Vaccine
Exclusive License
Exclusive License
Joint Program
G100 (Merkel cell carcinoma)
G100 + KEYTRUDA® Randomized (f-NHL)
G305
LV305 DE & Expansion (sarcoma, ovarian, lung)
LV305 + KEYTRUDA® Expansion (melanoma)
CMB305 DE & Expansion (sarcoma, ovarian, lung)
CMB305 + atezolizumab vs. atezolizumab Randomized (Soft Tissue Sarcoma)
15

TEAM, FINANCE AND STRATEGIC OUTLOOK
16

Carlos Paya, MD, PhD Chief Executive Officer
President
Vice President
Stephen R. Brady, JD, LLM Executive Vice President, Strategy & Finance
VP, Corporate
Development
Wayne Gombotz, PhD Chief Development Officer
Vice President
Senior Director
Richard T. Kenney, MD, FACP Chief Medical Officer
Chief Medical Officer
Jan H. ter Meulen, MD, DTM&H Chief Scientific Officer
Executive Director
Frank J. Hsu, MD Vice President, Head of Oncology
Chief Medical Officer
Senior Medical Director
Christopher Whitmore, CPA Vice President, Finance & Administration
Sr. Director Finance
Corporate Controller
17
Team: Experienced and Proven Executive Leadership
Prior Experience

18
Board of Directors
Ed Penhoet, PhD,° Alta (Chair)
David Baltimore, PhD,* §°Independent
Franklin M. Berger, Independent
Carlos Paya, MD, PhD, IMDZ
Scientific Advisors (SAB)
Rafi Ahmed PhD,§ Emory (Chair)
David Baltimore, PhD,* §° Caltech
Larry Corey, MD,° FHCRC
Phil Greenberg, MD, FHCRC
Clinical Advisors (CAB)
Mario Sznol, MD, Yale (Chair)
Jedd Wolchok, MD, PhD, MSKCC
Jeff Weber, MD, PhD, Moffitt
F. Stephen Hodi, MD, Dana Farber
Robert Maki, MD, PhD, Mt. Sinai
William R. Ringo, Independent
Peter Svennilson, TCG
Brian Atwood, Versant
Lewis W. Coleman, Independent
Carl June, MD,° U of Penn
Ron Levy, MD,§° Stanford
Steven Reed, PhD, IDRI
Inder Verma, PhD,§° Salk Institute
Patrick Hwu, MD, MD Anderson
Nina Bhardwaj, MD, PhD,° Mt. Sinai
Kristen Hege, MD, Celgene
David Parkinson, MD,° NEA
Lawrence Baker, DO, U Michigan
*Nobel Laureate, §National Academy of Sciences, °Institute of Medicine of the National Academies
Team: Exceptional Board and Advisors

Financial Highlights & Upcoming 2015-16 Newsflow
• Cash as of September 30, 2015 $120.5 million
• Expected 2015 net operating cash burn $36-40 million
• Expected YE-2015 cash balance ~$110 million
• Total shares outstanding ~20 million
19
Data** Timing*
• Phase 1 data on CMB305 dose escalation
• Initial Phase 1 data on CMB305 signal-seeking expansion arm (sarcoma)
• Phase 1 data for all patients in G100 in Merkel Cell Carcinoma
• Initial Phase 1 data on LV305 expansion study
Q1’16
• Phase 2 randomized study – initial data on CMB305 + atezolizumab in sarcoma
• Phase 1b randomized study – initial data on G100+KEYTRUDA® in NHL H2’16
Trial starts Timing*
• Initiate Phase 1 study of G100 + KEYTRUDA® in NHL
• Initiate Phase 1 LV305 expansion + KEYTRUDA® in melanoma NRs to α-PD1
Initiate Phase 2 randomized study of CMB305 + atezolizumab in sarcoma
Q4’15
Q4’15
Q4’15
*Timing is estimated. Although data may be available, we may elect to submit it for presentation at an appropriate medical meeting.

20
IMMUNE DESIGN
ZVex
Platform
GLAAS
Platform
Single
Agent
CPIs
Radiation
CAR-T/TCR
Oncolytic Virus
Other
✓
✓
✓
Poised for a Central Role in the I-O Landscape

BACKGROUND INFORMATION
21

An Immune Response is Key for Checkpoint Inhibitors
22
1. and Image. Tumeh, Paul C., et. al. “PD-1 blockade induces responses by inhibiting adaptive immune resistance.” Nature, 515: 568-571 (27 November 2014).
2. Taube, JM, et al. “Colocalization of inflammatory response with B7-h1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune
escape,” Science of Translational Medicine 2012 March 28; 4(127). Available at: http://www.ncbi.nlm.nih.gov/pubmed/22461641. Accessed August 2015 and Sznol, M. and L.
Chen “Antagonist antibodies to PD-1 and B7-H1 (PD-L1) in the treatment of advanced human cancer,” Clinical Cancer Research 2013 March 1; 19(5): 1021-1034. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/23460533. Accessed August 2015
3. J Clin Oncol 33, 2015 (suppl; abstr 9005)
Large Potential Opportunity:
• IMDZ’s agents are designed to create T anti-tumor T cells that should synergize with CPIs for tumor killing
• 34% ORR in metastatic melanoma patients treated with pembro + ipi (KEYNOTE-001) 3 –
• Potential market entry in remaining ~66% of patients exhibiting an inadequate response to treatment w/ CPIs
Tumor regression after treatment
with αPD-1 requires T Cells1
TIL (-) PD-L1 (-)
TIL (-) PD-L1 (+)
TIL (+) PD-L1 (+)
TIL (+) PD-L1 (-)
41% 1% 38% 20%
Significant % of melanoma
patients do not have pre-existing
T Cells2 N=110
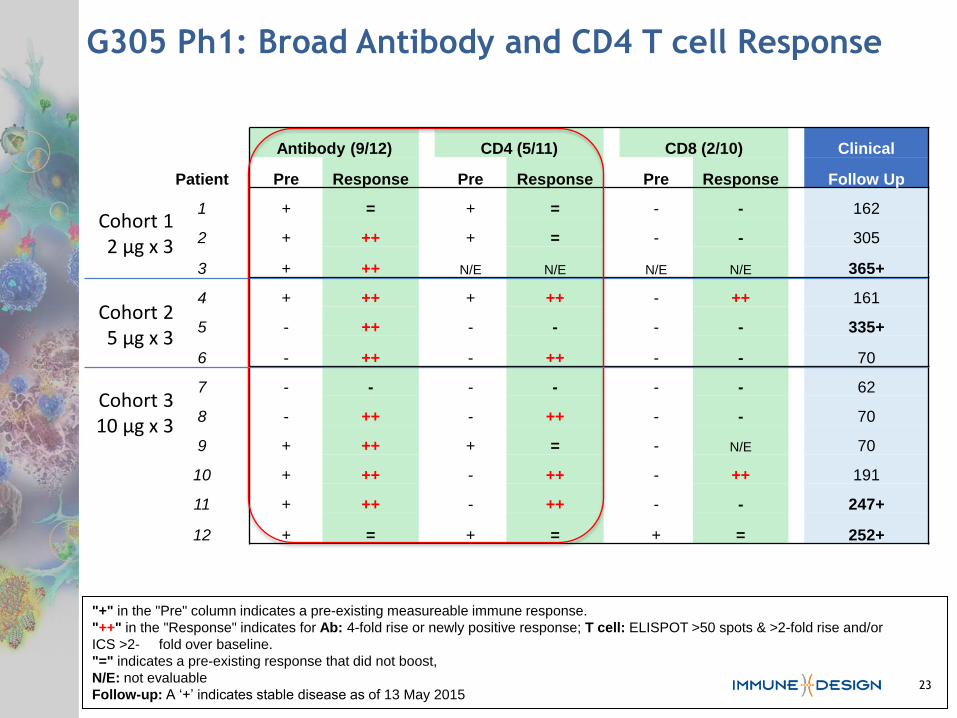
G305 Ph1: Broad Antibody and CD4 T cell Response
Antibody (9/12) CD4 (5/11) CD8 (2/10) Clinical
Patient Pre Response Pre Response Pre Response Follow Up
1 + = + = - - 162
2 + ++ + = - - 305
3 + ++ N/E N/E N/E N/E 365+
4 + ++ + ++ - ++ 161
5 - ++ - - - - 335+
6 - ++ - ++ - - 70
7 - - - - - - 62
8 - ++ - ++ - - 70
9 + ++ + = - N/E 70
10 + ++ - ++ - ++ 191
11 + ++ - ++ - - 247+
12 + = + = + = 252+
Cohort 1 2 µg x 3
Cohort 2 5 µg x 3
Cohort 3 10 µg x 3
"+" in the "Pre" column indicates a pre-existing measureable immune response.
"++" in the "Response" indicates for Ab: 4-fold rise or newly positive response; T cell: ELISPOT >50 spots & >2-fold rise and/or
ICS >2- fold over baseline.
"=" indicates a pre-existing response that did not boost,
N/E: not evaluable
Follow-up: A ‘+’ indicates stable disease as of 13 May 2015 23

G305 Ph1: Stable Disease Across Different Tumors
Efficacy:
• Stable disease: 8/12 patients (67%) achieved a best response of SD
— Median duration of SD of 245+ days (range: 161 to 365+ days).
• One patient (#3) had a CA125 response on d70 (based on GCIG Criteria)
24

LV305 Ph1: CD8 and Broad T-cell Responses
25
Cohort 1
108 vg x 3
Cohort 2
109 vg x 4
Cohort 3
1010 vg x 4
Cohort 1A
108 vg x 4
Antibody: 0/12 CD4: 5/11 CD8: 6/11
Pre Response Pre Response Pre Response
1 + = + ++ + ++
2 + = - ++ - ++
3 - - - - - -
4 + = - ++ - -
5 + = + ++ - -
6 - - - - - -
7 - - - - - ++
8 + = - - - ++
9 + = N/E N/E N/E N/E
10 - - - ++ - ++
11 + = - - - -
12 - - - - - ++
"+" in the "Pre" column indicates a pre-existing measureable immune response.
"++" in the "Response" indicates for Ab: 4-fold rise or newly positive response; T cell: ELISPOT >50 spots & >2-fold rise and/or ICS >2-
fold over baseline.
"=" indicates a pre-existing response that did not boost,
N/E: not evaluable
Follow-up: A ‘+’ indicates stable disease as of 13 May 2015

LV305 Ph1: Stable Disease & Progression Arrest in STS
26 26
• Stable Disease (SD):
— 8/12 (67%) at the end of treatment; median duration 208 d (139-347 +)
— PFR (Progression free rate): 67% (3 months) and >42% (6 months)
• 4/6 pts with evidence of prior tumor growth stabilized and stopped progression
— Tumor regression of up to 14% observed in one pt w/ SD at 347+ days
Rx: d0,21,42 (Cohort 1) & d63 (Cohorts 1A-3); Staging CT: d0, d63 (Cohort 1) or d84 (Cohorts 1A-
3), then every 8 wks; 1 pt did not complete all planned doses due to PD; "+" indicates pts with
documented pre-LV305 tumor growth: "+" indicates those pts who stabilized following LV305
0 50 100 150 200 250 300
151006
150014
151016
151020
150035
150051
151039
150050
151026
151119
151057
151070
DAYS SINCE 1ST DOSE
PA
TIEN
T N
UM
BER
L
347+
326+ Cohort 1
108 vg x 3
Cohort 2
109 vg x 4
Cohort 3
1010 vg x 4
Cohort 1a
108 vg x 4
Stable Disease
Progressive Disease
Staging CT
Eval. Tumor growth per irRC
Tumor growth
before LV305
+
-
+
+
-
+/-
+
-
+
-
-
+
# Prior Tx
5
1
3
2
3
4
Surg/rad
Surg/rad
2
3
Rad
3

Sindbis envelope
provides selective in
vivo DC targeting
Integration-deficient
and replication-
incompetent for safety
Lack of prior immunity
allows for multiple
dosing
ZVex: First in vivo DC Targeting Gene Delivery Vector
Designed to generate CD8s in vivo
Sindbis
Lenti
27
*Immune Design data.
Capacity for substantial genetic payload = new potential products

Activates innate
immunity (G100)
(TH1 cytokines,
chemokines and NK cells)
Activates adaptive
immunity (GLAAS + Ag)
(De novo induction of Ag-
specific CD4 T and B cells)
Expanding favorable
safety and efficacy
database
(>1,200 subjects)
Potential in oncology,
and infectious and
allergic diseases
GLAAS: Potent TLR4 Agonist - Broad Clinical Exposure
28
*Immune Design and IDRI data; Lambert et al., PLoS One, 2012
Designed to induce CD4s, ABs & NK cells in vivo