

Not just an MDT toolkit… What’s in the bag? · •Custom built MDM tool ... •How did the POC...
34
Not just an MDT toolkit… What’s in the bag? Shoni Colquist Queensland Cancer Control Analysis Team (QCCAT)
-
Upload
phungthien -
Category
Documents
-
view
215 -
download
3
Transcript of Not just an MDT toolkit… What’s in the bag? · •Custom built MDM tool ... •How did the POC...

Not just an MDT toolkit…What’s in the bag?
Shoni ColquistQueensland Cancer Control Analysis Team (QCCAT)

Cancer in QLD
• ~22,000 people diagnosed with cancer each year
• Cancer largest cause of premature death and disability in 2007, 18.6% of total burden
• Variation in outcomes across QLD eg.•Survival - Urban vs rural
•Treatment practices
• Cancer Stage important to understanding variation
Qld Cancer Control Safety and Quality Partnership
• Gazetted Quality Assurance Committee (QAC)
• Legislation – Health Services Act
• QCCAT - sub committee of partnership
Purpose of ‘The Partnership’• Facilitate participation of clinicians and administrators statewide
• Collection, coordination, analysis, reporting and feedback of cancer data
• Negotiate development and uptake of strategies to address safety and quality gaps
Governance

Employed multiple approaches
1. Utilise existing electronic sources of data
2. Responded to clinician need for improved data collection and coordination of Cancer data, especially Stage
3. Web application for collection of ‘missing’clinical data
4. Combined activities with ‘best practice’multidisciplinary care
5. Develop tools for analysis, reporting and feedback of cancer data

1. Utilise existing electronic sources of data
•Tools and technology•Enterprise Service Bus
•Patient matching and linking engine
•Data standardisation and normalisation
•Data integration
•Cancer specific data sets
•QLD Oncology Repository (QOR)

•Impacts and improvements•ESB - accesses 32 systems
•P, M&L engine – routinely match, link, de-duplicate 35 M records to produce Master list of
• 6.7 M distinct people
• 340,000 people with invasive cancer
•Data integration - timely updating of data, (source dependent) with clinically relevant details
•QOR 2000 - 2007 155,000 cases (public and private) linked to demographics, cancer diagnosis, treatment, death
1. Utilise existing electronic sources of data

32 sources
35 million rows
6.7 M distinct pts 155 k linked to clinical data
Data integrated
QOR
Data available to application suiteRoutine reporting
Accessible pt summary - secure Web access
Data standardisedTumour specific datasets

2. Improved data collection and coordination of Cancer data,
especially Cancer stage•Tools and technology
•Custom built MDM tool - QLD Oncology On-Line
•QOOL does not behave like a traditional ‘silo’database - widely accessible by MDT members
•Relevant information integrated from numerous systems
•Capture stage at point of decision making with inbuilt stage calculations
•Make ‘sense’ of disparate sources of data
•Partnered with Aehrc - to extract cancer stage directly from text based pathology reports
•Impacts and improvements
• Tumour specific data able to be captured for all cancersModules in Lung, Breast, H&N, Gynae, Melanoma, CRC etc
• Relevant information available in real time for MDT discussion eg. Prior cancer history, pathology
•~ 50% pts have a documented complete stage – QOOL
•Cancer notification and staging system rapidly improving – extended to include many cancers
2. Improved data collection and coordination of Cancer data,
especially Cancer stage
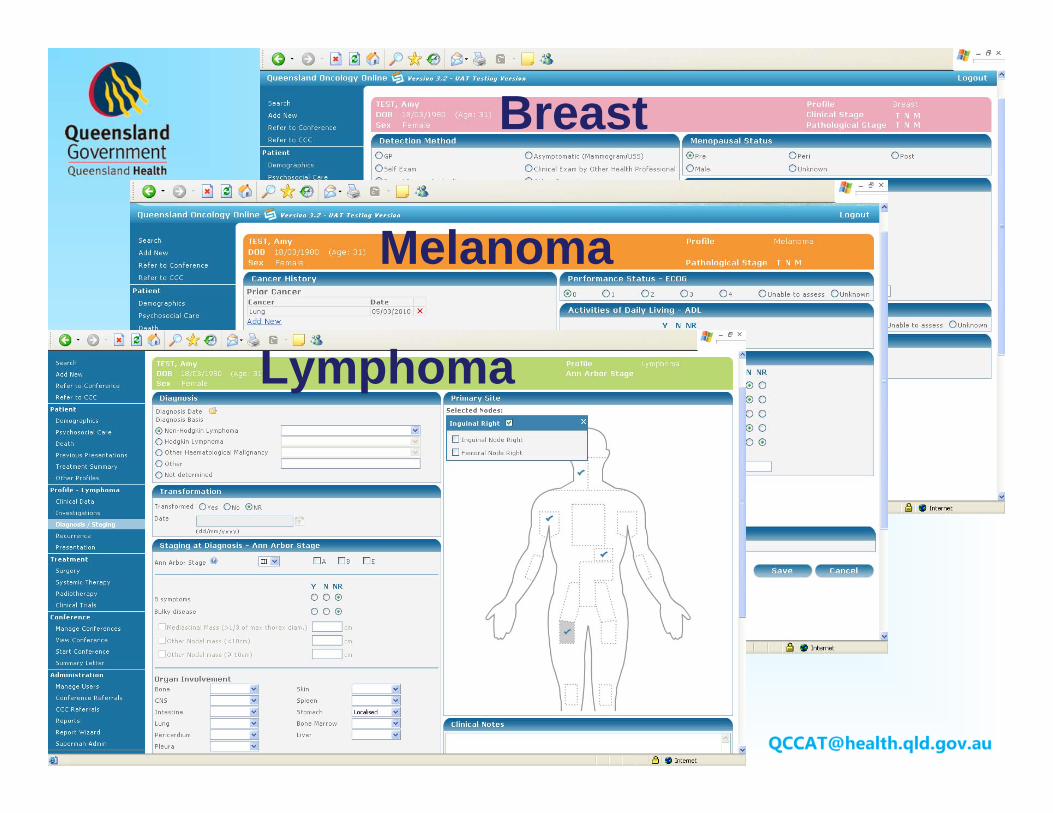
Breast
Melanoma
Lymphoma

Customised tumour specific MDM tool

Investigations

Real time pathology

3. Web application for collection of ‘missing’ clinical data
•Tools and technology•QLD Oncology On-Line – QOOL
•Web-based system
•Supports Multidisciplinary care
•Auto-population of demographic, diagnostic and treatment data
•Secure access to clinical summary, online scheduling, case conferencing

Routine Sources(prepopulate QOOL)
Cancer registryAdmitted patient dataSurgeryRadiotherapyPharmacyPathologyDeath
Routine Sources(prepopulate QOOL)
Cancer registryAdmitted patient dataSurgeryRadiotherapyPharmacyPathologyDeath
QOOL
Treatment planCancer StageECOG, Signs and SymptomsPrognostic FactorsClinical DataDates (referral, treatment)
QOOL
Treatment planCancer StageECOG, Signs and SymptomsPrognostic FactorsClinical DataDates (referral, treatment)

3. Web application for collection of ‘missing’ clinical data
•Impacts and improvements•Provides on-line clinical summary of patient journey regardless of patient, clinician, hospital location
•Facilitates communication between cancer care providers
• Over 50% patients have a documented treatment plan
•QOOL data collection fed back into QOR for analysis, contributing to population based cancer statistics

share MDM outcomes

4. Combined with ‘best practice’multidisciplinary care
• Tools and technology• Online scheduling for MDT case discussion
• Data is saved into a repository which can be viewed and updated by other QOOL users, and other QOOL data sources
• QOOL supports MDTs to capture clinically relevant details at point of decision making
• Strengthens partnership between public and private providers
• MDTs able to monitor activity

4. Combined with ‘best practice’multidisciplinary care
• Impacts and improvements• QOOL supports 40 MD teams state-wide
• ~ 800 (44%)new patients are receiving a multidisciplinary review each month
• 12 Multidisciplinary Meeting Coordinators (MDM-C) across Qld
• In last 3 months utilised by 350 staff across 24 facilities
• MDT participation in audit and peer review as part of routine clinical practice

40+ MDTs, 600+ clinicians statewide
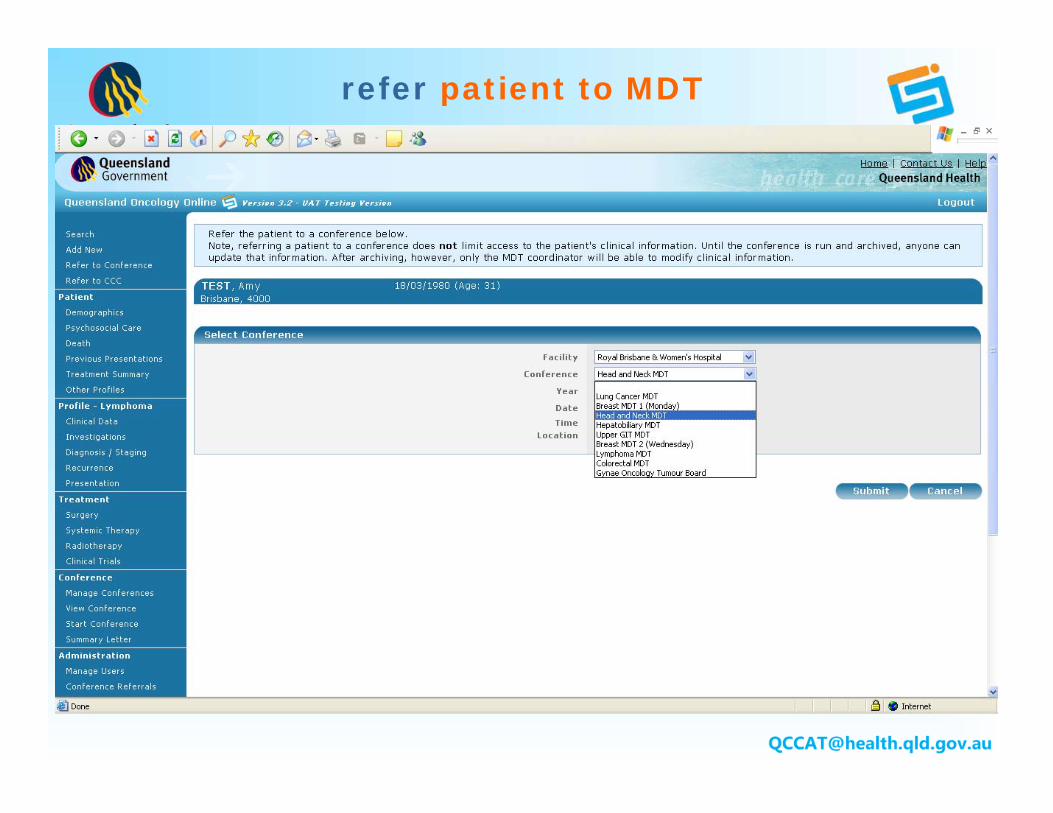
refer patient to MDT

monitor own activity

5. Develop tools for analysis, reporting and feedback
of cancer data
•Tools and technology•Oncology Analysis System – OASys
•Web based analytical tool
•Online clinical indicators
•Aggregate population data
•Comparative analysis
•Flexible querying

5. Develop tools for analysis, reporting and feedback of cancer data
•Impacts and improvements• Real Queensland data available 2000 - 2007 -
contains155,000 linked cases
•Set realistic targets
• Estimate cancer measures with better precision
•Look at small subgroups of unusual cases
•Find real tail of the curve: know where you stand
•Research, college audits

Oncology Analysis System

analyse casemix

examine treatment patterns …

… and outcome

audit your practice

plot cancer survival

Negotiate development and uptake of strategies to address
safety and quality gaps
•Approach has delivered systems and tools • to support implementation of IT solutions, quantify the issuesand identify the gaps in cancer services.
“… in my darker moments, I wonder whether all this work that I am doing will fall on deaf ears”.
(clinician involved in QAC activity)
• What impact has the data had in stimulating changes in delivery of cancer services? For eg.
•How did the POC report assist a regional EDMS to examine local practices? •What resulted from reporting that a MDT review appears to increase a patients chances of seeing a specialist within 14 days.

Negotiate development and uptake of strategies to address
safety and quality gaps

The future
•One size fits all approach will have limited impact
•Partnership maintains flexibility in approach to meet the complexity of ‘unknowns’
•Create space for new approaches
•Adopt the best approach for the specific circumstance


















