Northern Voices Aug13
28
Mental Illness Fellowship NQ Inc Issue: AUGUST 2013 - Getting it right on rural mental health By Alison Fairleigh -Wed Jul 17, 2013 - ABC’s The DRUM You can't simply plonk mental health services into rural areas and hope that people will come. The best chance of making a difference is working from the ground up, writes Alison Fairleigh. This is one of a series of articles looking at issues relating to care in our communities in the lead up to the 2013 federal election. More coverage can be found at the ABC's election website Australia Votes. Recently, I popped down the street of my small rural town in north Queensland to pick up a couple of things at the shops. As I was jumping back in my car, I heard a loud "Oi" from across the street. I looked up to see the welcome and familiar face of a local male farm worker running across the road to say g'day. Max* is in his fifties, married with grown up kids, and has worked on farms his entire life. We took up the characteristic conversation pose for rural people of leaning on the bonnet of my car (I don't have a ute, otherwise it would have been on the tray-back) where we stayed talking for more than an hour. Max is a former colleague and we share a very special bond. You see, almost five years ago one of our male co-workers, John*, took his own life onsite and Max was one of two people to find him. Typical of rural areas, Max and John had gone to school together, grown up together, worked together and had more than their fair share of drinks together. It was a devastating blow to Max, and he explained to me over the bonnet of my car how, to this day, he is still deeply affected with flashbacks and the futility of John's decision. It is a scenario that plays out over and over again throughout our farming communities. Evidence indicates that the suicide rate among Queensland's agricultural workers - including farmers, farm managers, farm hands and shearers - is over twice the rate of those in other occupations. While suicide is devastating wherever it occurs, the impact is particularly harsh on rural communities where everyone knows someone who has been there. continues next page 159 Kings Road Pimlico QLD 4812 PO Box 979 Hyde Park QLD 4812 Tel: (07) 4725 3664 Fax: (07) 4725 3819 Email: [email protected] www.mifnq.org.au Editor: Deborah Wilson, Corporate Development Manager Tel: (07) 4725 3664 Fax: (07) 4725 3819 Email: [email protected] Compiled by: Margaret Sleeman, Receptionist © Mental Illness Fellowship of Nth Queensland Inc. PO Box 979 Hyde Park QLD 4812 All rights reserved. Printing & Design: Mental Illness Fellowship NQ Inc. MIFNQ reserves the right to edit articles for publication. The views expressed in this newsletter are not necessarily those of MIFNQ. Photo GPs are still the preferred health information
-
Upload
mental-illness-fellowship-nq-inc -
Category
Documents
-
view
227 -
download
8
description
MIFNQ's newsletter August 2013
Transcript of Northern Voices Aug13

Mental Illness Fellowship NQ Inc Issue: AUGUST 2013-Getting it right on rural mental health
By Alison Fairleigh -Wed Jul 17, 2013 - ABC’s The DRUM
You can't simply plonk mental health services into rural areas and hopethat people will come. The best chance of making a difference is workingfrom the ground up, writes Alison Fairleigh.This is one of a series of articles looking at issues relating to care in ourcommunities in the lead up to the 2013 federal election. More coveragecan be found at the ABC's election website Australia Votes.Recently, I poppeddown the street of mysmall rural town innorth Queensland topick up a couple ofthings at the shops. As Iwas jumping back inmy car, I heard a loud"Oi" from across thestreet.I looked up to see thewelcome and familiarface of a local malefarm worker runningacross the road to say g'day. Max* is in his fifties, married with grownup kids, and has worked on farms his entire life.We took up the characteristic conversation pose for rural people ofleaning on the bonnet of my car (I don't have a ute, otherwise it wouldhave been on the tray-back) where we stayed talking for more than anhour.Max is a former colleague and we share a very special bond. You see,almost five years ago one of our male co-workers, John*, took his ownlife onsite and Max was one of two people to find him.Typical of rural areas, Max and John had gone to school together, grownup together, worked together and had more than their fair share ofdrinks together. It was a devastating blow to Max, and he explained tome over the bonnet of my car how, to this day, he is still deeply affectedwith flashbacks and the futility of John's decision.It is a scenario that plays out over and over again throughout ourfarming communities. Evidence indicates that the suicide rate amongQueensland's agricultural workers - including farmers, farm managers,farm hands and shearers - is over twice the rate of those in otheroccupations.While suicide is devastating wherever it occurs, the impact isparticularly harsh on rural communities where everyone knowssomeone who has been there.
continues next page
159 Kings RoadPimlico QLD 4812PO Box 979Hyde Park QLD 4812Tel: (07) 4725 3664Fax: (07) 4725 3819Email: [email protected]
Editor: Deborah Wilson, CorporateDevelopment ManagerTel: (07) 4725 3664Fax: (07) 4725 3819Email: [email protected] by: Margaret Sleeman,Receptionist© Mental Illness Fellowship of NthQueensland Inc.PO Box 979Hyde Park QLD 4812All rights reserved.Printing & Design:Mental Illness Fellowship NQ Inc.MIFNQ reserves the right to editarticles for publication.The views expressed in thisnewsletter are not necessarily thoseof MIFNQ.
Photo GPs are still the preferred health information

Page 2 of 28
Contact UsEmail: [email protected]: Living Proof – PositiveStories of Mental IllnessTwitter: LivingProofQLDPhone: 1800 455 455TownsvillePhilippa Harris, QueenslandEducation & Training ManagerP: 07 4725 3664Street Address: 159 Kings Road,PIMLICO Q 4812Postal Address: PO Box 979, HYDEPARK Q 4812Regional QueenslandAlison Fairleigh, Rural CoordinatorP: 07 4725 3664E: [email protected] CoastJudy Kiellerup, RegionalCoordinator (SQ)P: 07 5442 1651Postal Address: PO Box 5080SUNSHINE COAST MC Q 4560
continued from previous pageMuch has been written about the complex factors influencing the highrate of suicide within rural communities, including, but not limited to,climate, declining profitability, bureaucracy and governmentregulations, isolation, stigma, lack of mental health education andservices, and masculinity.But we also have a considerable body of evidence telling us whichprograms and approaches do work in rural communities, and it is fromthis evidence that our policy makers under the new government musttake heed.Even where formal mental health services do exist inrural and remote communities, farmers and fishers in
particular are not likely to utilise these services.First and foremost, 'top-down' approaches do not work in ruralcommunities. 'Ground-up' is the most successful model of buildingcapacity in rural and remote communities to manage their health andmental health. This can be achieved by empowering individuals andgroups within local communities to work with existing models tostrengthen collaboration and leadership.Even where formal mental health services do exist in rural and remotecommunities, farmers and fishers in particular are not likely to utilisethese services. Nor do they tend to make use of telephone help lines,telehealth or online services.GPs are still the preferred health information source for farmers andfishers, who will travel considerable distances to ensure continuity ofcare through a trusted rural GP. It is therefore essential thatconsiderable investment is maintained in the delivery and support ofdoctors to rural and remote Australia who have sufficient mental healthtraining.However, farmers also respond well to receiving health and mentalhealth information through trusted sources such as recognisedcommunity groups (e.g. service clubs) or industry groups (e.g. statefarming organisations), and in group settings (e.g. industry forums).Therefore, the delivery of services to rural and remote communities canbe better achieved through a "community health developmentapproach", in which industry, government, health services andcommunity work together.Such an approach will utilise "soft entry points" - i.e. industry field daysand community events - to promote the effective use of availableservices, and will identify within communities credible individuals whocan act as "boundary crossers", having the trust of farmers, industryand health services alike.Agricultural production and services to farming form thesocioeconomic base for most rural communities. With the health andmental health of our farmers being one of the greatest challenges facingthe future of Australia's primary industries and rural communities,there is no room for delay.Get it right now, and we get it right for the future - ensuring healthy,sustainable and thriving rural communities. And with that, I hope, therewill be fewer people like Max, left struggling to cope with the loss of amate.*Names have been changed to protect privacy
Where to Go for HelpKids Helpline Chat OnlineFree, private and confidentialtelephone and online counsellingservice specifically for youngpeople aged between 5 and 25.Telephone Available 24/7 - 180055 1800Eheadspace Chat OnlineProvides online and telephonesupport and counselling to youngpeople aged between 12-25.Available 9AM-1AM AEST - 1800650 890Lifeline Chat Online24 hour crisis support 13 11 14Online counselling available 8AM-midnight

Page 3 of 28Bushfire fallout tests kids' mental health
The AustralianAAP July 30, 2013EXPERTS have found around 10 per cent of children who experiencedTasmania's devastating bushfires are showing signs of mental healthproblems.A team co-ordinated by mental health organisation Beyond Blue hasscreened 212 children, finding 26 would benefit from more treatment.Post-traumatic stress disorder, anxiety and depression have beenidentified among the children, some who had to flee for their lives withtheir families or who saw animals being burned alive.Professor Brett McDermott, a co-founder of the program also usedsuccessfully after the Brisbane floods, said the smell of barbecue smokeor the sound of a siren could still be terrifying years later for a child.“They might have nightmares and flashbacks and feel like it'shappening all over again,” Professor Brett McDermott told AAP.“Or a reminder which might be real, like barbecue smoke, or symbolic,like an ambulance, can bring it all back to them.”As well as PTSD symptoms, parents, teachers and mental healthworkers are on the lookout for children who appear to show anemotional numbness or have developed phobias to things like fire orwind.Professor McDermott said theyounger the children, the lessable they were to process thecircumstances of the disaster.“Some of these kids have hadextremely frightening situationswhere they’ve been evacuatedthrough very dense smoke andthrough fire,” he said.“Some kids saw animals thatwere burning. These are really frightening kinds of things.”Children in every school affected by the fires have been through a two-stage screening process, while parents and teachers have receivedtraining as part of a $650,000 project also involving the Tasmaniangovernment and the Red Cross.Children needing treatment will receive a form of cognitive behaviouraltherapy, where they confront and train their thoughts about theirexperience.An important part of that was children being able to tell their story,professor McDermott said.“It was so frightening that they won’t tell anyone about it or it comesout in nightmares and dreams which isn’t helpful,” he said.“We get them to tell their story several times until it doesn’t have anypower over them any more.“The whole emotional burden of their story is diminished.”Professor McDermott said the figure of around 10 per cent wasconsistent with research from other bushfires.The flipside of the finding was that most parents were being reassuredtheir children were coping well, he said.
In This Edition
Getting it right on rural mentalhealth ...................................................... 1Bushfire fallout tests kids' mentalhealth ...................................................... 3CEO’s Update........................................ 4Committee Chatter ............................ 5MIFNQ 2013 AGM .............................. 7Imogen Rogers at Barefoot ............ 9Police to tackle mental health.....10Designing for mental health ........11Young men in crisis: mental healthstudy......................................................12Beyond madness: a modernapproach to hearing voices ..........13NRL enlists former Cowboys coachMurray Hurst as mental healthmanager of Queensland league ..15Game on ...............................................16Program Feedback...........................18That One Time I Went Nuts: WhyMental Health Care Matters ...........19New mental health service forTamworth............................................22Life expectancy for people withmental illness the same as 30 yearsago: report...........................................23Training & ProfessionalDevelopment......................................25

Page 4 of 28CEO’s UpdateI was at a meeting of carers recently in Cairns and their stories remind me once again of theneed for much more work to be done in the coordination of services, referral pathways,access, communication and relationships between clinical mental health services and thepeople who need them. There are many service gaps and people who should be receivingservices don't always get what they need in a timely way. This results in stress and angst forcarers as they try to navigate their way through the maze of services both private andgovernment funded, that is, where they exist at all! For people who are confronting mental illness for the firsttime this is a real challenge, who do you go to for advice and assistance? Who can you trust? Many start with theirGP but not all GPs have a sound knowledge of what is available for people in their local community, neither dosome of the formal clinical services. What is needed is one point of contact where people can be assured that theywill be listened to with empathy, offered information, advice and a warm assisted referral. The Mental IllnessFellowship of Australia (MIFA) has established such a point of contact where ever you are. It is Mi Networks, aphone number that puts the caller through to their nearest member of the Mental Illness Fellowship of Australia -1800 985 944.Of recent note is the publication of the report Obsessive Hope Disorder co-authored by John Mendoza. The reportprovides clear evidence that not much has improved for people with a mental illness over the last 30 yearsdespite successive state and federal governments' rhetoric and plans. With all good intentions state and federalplans have resulted in little real change on the ground. Services are still lacking coordination, there is littleinvolvement of people with a lived experience and carers in planning and implementation and there is certainly ashortfall in funding particularly in early intervention and prevention strategies. The report is available onlineand in hard copy from http://connetica.com.au/ohd-landing-page.This newsletter is the last prior to the Federal election and I would like to point out a number of key issues thatour politicians need to be aware of in order to keep mental illness on the national political agenda.Numbers of people with severe mental disordersApproximately 3 per cent of adult Australians suffer from severe mental disorders’. That is nearly 700,000people, each with their network of families, friends and colleagues. It has been estimated only 35 per cent ofAustralians with severe mental disorders access services for mental health. (ABS 2008: National Survey ofMental Health and Wellbeing 2007)Suicide and severe mental illnessThe information available about the rates of suicide of people with severe mental illness is alarming. Thelandmark report ‘People Living with Psychosis, 2010’ found that 49.5% of participants had attempted suicideat some point in their lifetime compared to 3.7% of the general population. The World Health Organisation hassuggested that ‘between 6 and 13% of all people with a diagnosis of schizophrenia will die by suicide’. This is adirect result of the extremely poor quality of life of people with severe mental illness, particularly psychoticdisorders. This group of people must be a priority in any suicide prevention strategy.EmploymentThere has been little advance on the 22% of people with severe mental illness reported in work or study in1997. Both in Australia and internationally there is ample evidence that employment rates could be dramaticallyhigher with the right strategies and supports—up to 65% of people with the most severe and persistent mentalillnesses can access either paid work or study with the right supports.Physical HealthPeople with severe and persistent mental illness have a life expectancy up to 25 years less than that of thegeneral population, and the gap is widening. For example, at least 25% or more of people with schizophreniahave diabetes—five times the community rate. While smoking rates in the general community have reduced toone of the lowest in the world, 42% of all cigarettes are now consumed by people with mental illness. Ourmember organisations conduct a successful tobacco free program around Australia because online and other quitmethods for the general population have proved to have little impact on people with severe and persistentmental illness.Housing and homelessnessOne third of people who were homeless in inner city areas have a severe mental illness. While there islimited provision of shared and ‘congregate’ housing models, surveys of people with mental illness consistentlyshow a preference for similar housing options to the general population, especially living alone or with one otherperson such as a partner. Carers have frequently listed housing security as one of their key concerns forpeople living with severe and persistent mental illness in the long term.
continues next page
Jeremy Audas, CEO

Page 5 of 28
MIFNQ Management Committee
President Bob JamesVice-President (vacant)Secretary Jenny ChapmanTreasurer Sandra HubertCommittee Members Alf MusumeciTanya ParkDonella PicklesSandi WinnerPromoting Recovery Through Services in the Community
conclusionCarer support and severe mental illnessPeople with severe and persistent mental illness are frequently supported by carers – family members, friendsand neighbours who choose to offer support to people with mental illness. Many do not identify as carers toavoid social stigma and discrimination. Mental health carers report that there continues to be a lack of respectfor their caring role from clinicians, mental health workers and others who still regularly exclude carers fromtreatment planning.Jeremy AudasChief Executive OfficerMental Illness Fellowship NQ Inc.
MIFNQ Office LocationsCAIRNS MACKAYSuite 7,129a Lake St, Cairns Q 4870 14-16 Wood St, Mackay Q 4740PO Box 816N Cairns Q 4870 PO Box 729 Mackay Q 4740P: (07) 4041 2543 P: (07) 4951 2955F: (07) 4041 2872 F: (07) 4953 0509E: [email protected] E: [email protected] (Head Office) SUNSHINE COAST - Living Proof159 Kings Rd, Pimlico Q 4812PO Box 979 Hyde Park Q 4812 PO Box 5080 Nambour Q 4560P: (07) 4725 3664 P: (07) 5442 1651F: (07) 4725 3819 F: (07) 5442 1651E: [email protected] E: [email protected] CALL: 1800 455 455

Page 6 of 28Committee ChatterThese are tumultuous times for organisations dependent on government funding to dotheir jobs. The ‘sea’ seems very rough indeed for ‘the good ship MIFNQ’. With a stillnewish State Government still finding its feet as it promotes its policies of austerity andefficiency and with a Federal election in just a few weeks [all in an era of promisedincreased of Mental Health funding] we are in uncertain times.What can we do? Well, we can hope – hope that governments [old and new] will stick totheir commitments and that they will understand that the reason they give us money toprovide the services we do is because there is no better way of getting the necessaryservices delivered. Nobody does it better, because we are closest to those needing theseservices. They seem to need continual reminding of that.Though we cannot just hope. And we haven’t been merely hoping. We have worked very hard at a local, stateand national level to make politicians of all parties understand the vital nature of the work we do and theresponsible, efficient and cost-effective way in which we do it.Jeremy, Adrianne, Allison and others [including me occasionally] have met with politicians and bureaucrats.Much effort has been aimed at focusing on just what more we might do to protect our people from any potentialloss of our services and to protect your Fellowship from being pushed aside by large corporations in the questby governments to reduce their bottom lines. We have gained some recognition of our importance to thedelivery of government-financed services, but we must continue to work to convince politicians of the truth ofour claims – both that these services are vital and that the best way of delivering them is through small locally-focused organisations with close community connections like your Fellowship.In the meantime, the best evidence of how vital we are is in the work that we do. We prove it every day, everytime we provide a service as nobody else can. While we do the very best that we can [and we know our best isTHE best that anyone can do] then we should feel secure. But we have to make sure that we continue toimprove AND that we make politicians and bureaucrats aware of this. We are so fortunate to have suchdedicated and skilled staff who just keep achieving more.An important part of my role at your Fellowship has been to try to build up our humble little organisation inthis environment where only the strong survive and where compliance and accountability get more demandingover the years. Having a strong Management Committee able to provide skills, knowledge and compassionateleadership is vital to us in this environment. Our Annual General Meeting is where we, as your board, areaccountable to you, and the place where new people are elected to your board to strengthen it. We look forwardto the opportunity to talk directly with you all then and to further build the strength of our board. We lookforward to people putting themselves forward to serve the Fellowship, perhaps by volunteering to join yourManagement Committee.Our Annual General Meeting is on Thursday 26 September at 5:00pm at 159 Kings Road, Pimlico.As time passes, people come and go. We grow old and we leave. We leave our jobs to retire or for any of amyriad of reasons. And we leave our voluntary positions. So it is with Tanya Park, who has served as actingPresident and Vice President and as an ordinary board member of your Management Committee for about 8years. Tanya leaves for Canada to take up a new position, leaving both JCU and the Fellowship after providingsignificant leadership and advice. We will miss Tanya and we wish her well in her new role – her new life on theother side of the world.Bob James
PresidentMental Illness Fellowship NQ Inc.
Bob James, President

Page 7 of 28MIFNQ 2013 AGM
Invites members and guests to attend the2013 Annual General Meeting
RSVP:Corporate Development ManagerP: (07) 4725 3664E: [email protected]
When: Thursday 26th September 2013
Time: Commencing at 5:00pm
Place: MIFNQ Townsville OfficeGround Floor, 159 Kings RoadPIMLICO Q 4812
RSVP: Friday 20th September 2013

Page 8 of 28
2013 ANNUAL GENERAL MEETINGAGENDA1. Minutes of previous AGM held on 2 October 20122. Business Arising from previous AGM3. Presentation of Annual Report4. President’s Report5. Treasurer’s Report6. Auditor’s Report7. Present Management Committee members to vacate office8. Election of Incoming Management Committee members9. Appointment of Auditor10. Appointment of Legal Representative11. President’s Acknowledgements12. Meeting Close
Nominations are now open for all Management Committee positions. Formsare available through the Townsville office or you can download them onour website at www.mifnq.org.au.
The Secretary should receive your Nomination by no later than 5:00pm onThursday 12th September 2013. A full list of Nominees will be displayedseven days prior to the AGM. Late nominations can be accepted from thefloor during the election process.
The SecretaryMental Illness Fellowship NQ Inc.P: 07 4725 3664F: 07 4725 3819E: [email protected] Kings Road Pimlico Q 4812PO Box 979 Hyde Park Q 4812

Page 9 of 28Imogen Rogers at Barefoot
Adapted from a Review by George HirstIt’s good to see a bit of unashamedly abstract painting for a change amid theoft-witnessed pleasing landscapes, seascapes and generally literal renderingsfound so regularly in North Queensland art exhibitions.Magnetic Island-based artist, Imogen Rogers, exhibited, To the Is-land, 36paintings recently at the Barefoot Gallery in Horseshoe Bay.To the Is-land reflects an interior world of predominantly female symbolismwith more than a little Earth Mother worship detectable. And while thesethemes are clearly significant to the artist theworks get more interesting for this reviewerwhen the fem-familiar prop is put aside and alittle discovery of what colour, shape, line andform can achieve without having to depict anyparticular thing. One work, Mountain (right),confidently plays off the confined structures of topography with a candy-colouredsky that wants to lift itself out of the picture and suggests many further adventuresin paint and pattern.Another piece, Janet Frame (left) is a loose and wild vermillion arrangement thatsmears close to the freedom and decisiveness found in the best of young children’sart. With the suggestions of a face amid chaoticfinger painting the play-off between straightlines and looped face shape suddenly gets serious and tormented withgashes of yellow teeth lines. Its brilliant red-headed namesake would nodoubt have been intrigued.Another piece, Adams Apple (right), again plays offforces of containment and release and while theeye has much to do travelling through thistruncated arrangement there is no retreat by theartist into patterned decoration and the work isthe stronger for it.While Rogers has attempted larger works such asPurple (right), the colour is confidently and cleanly applied but over forms which areless convincing and resolved within the canvas. As is so often the case, it is the smaller,less-stressed over works which hold the most possibilities.For this reviewer’s two bob’s worth, Imogen Rogers has excitement to share in hersmaller visual spaces when free of the universal symbols and the cultural baggage theyinevitably evoke.
To the Is-land was well worth a visit for a change from the usual suspect subject matterand the chance to see some engaging painting that isn’t trying to be a picture ofsomething.The Artist: Imogen RogersMy art work is all about inner expression. That you can take your thoughts thattrigger feelings and give them a voice.The process is a lived experience; also allowing the stillness which speaks onceyou have put a space around constant thoughts.If I can produce a painting when I am feeling down it gives me solace; if I canproduce a piece when I am feeling good then I want to share that with otherpeople.Contact Details:Email: [email protected]: www.imogenrogersartspace.comFacebook: www.facebook.com/ImogenRogersPeaceArt

Page 10 of 28
Police to tackle mental healthThe Sydney Morning Herald – 1 August 2013
By Emma Partridge, Crime ReporterEvery front-line police officer across NSW will receive specialised mentalhealth training, in a course to be introduced as early as next month,police say. The one-day course for all beat police comes after severalhigh-profile cases in recent years involving the fatal shooting of mentallyill people. One such case involvedSydney man AdamSalter, who died afterhe was shot in the backby police in hisLakemba family homein 2009.The mental healthintervention course, tobe run by NSW Policeand NSW Health, willbe the first of its kindin Australasia.A team of eight officersand nurses will travel to every police local area command in the state todeliver the training, which has been three years in the making.NSW Police spokesman for mental health Superintendent DavidDonohue said about 90 per cent of police had never had access to formalmental health education, despite interacting last year with 38,534people who suffered from mental illnesses. "Unfortunately there areincidents of police contact with mentally ill people with fatal outcomes,"Superintendent Donohue said.Police deal with about 100 mentally ill people every day, according tothe NSW Police Association. The interaction with those suffering from anillness has grown exponentially from 18,000 incidents in 2004 to 36,500in 2011."[The training] is making sure police have a degree of empathy for theperson they are dealing with,'' he said. ''Someone who is hostile to policeis not necessarily a danger to police but it's about making sure they aresafe. "The ethos of myself and the mental health team has always beenabout empathy and understanding because it's very difficult for police tomake assessments on people's mental health in a very short period oftime."The police mental health intervention team, headed by Inspector JoshMurchie, designed the course with the help of NSW Health.''Police are required to respond to a whole gamut of mental health-related incidents ranging from someone having a bad day and arguingwith their neighbour, right through to someone who is acutely psychoticand threatening to harm themselves or someone else up to the siege-type incidents,'' Inspector Murchie said.Superintendent Donohue said the course will teach officers aboutcommon mental illnesses and ways to identify certain conditions."Because sometimes we don't know if [a person] is drug-affected - or insome instances the person might be suffering from a brain injury," hesaid.continues next page
News in BriefReport shows restraints usedon mental health patientsdecline
ABC News, Friday 19 July 2013There has been a decline in theuse of force in Tasmania'smental health wards.The Australian Institute ofHealth and Welfare reportexamined the use of physical orchemical restraints.It has dropped from 15.6incidents for every 1,000 beddays in 2008-09 to about 13 lastfinancial year.The level is in line with rates inVictoria and Queensland.The most significant decreaseswere recorded in the ACT.Darren Carr of the MentalHealth Council says theTasmanian rate is still too high.Mr Carr says many of therecommendations made by theNational Seclusion and RestraintProject have not beenimplemented by the stategovernment."There's been a reduction in theuse of seclusion and restraint inacute mental health settings inpublic hospitals throughoutAustralia and we've seen areduction in Tasmania, but halfthe rate of reduction that we'veseen in other states," he said."We are disappointed that theresults are not better...becausewe know that we can actuallycut seclusion and restraintabout 10-fold further based onresults being achieved in theACT."
Killed in family home: Adam Salter , who was shot bypolice in 2009, and his sister Zarin
Darren Carr, Mental Health Council ofTasmania

Page 11 of 28
continued from previous pageCoronial findings from cases wherepolice have killed mentally illpatients would be discussed andofficers would have the chance toparticipate in mock scenarios. The"quick tool-kit" course would alsoinclude a refresher on mental healthlegislation and remind police of howto detain people who suffer from anillness."I have gone to jobs where theperson has wired up their entirehouse because they think someone was going to break in and that was avery real thing to them,'' Superintendent Donohue said. "The reality is, itis a real situation for that individual and we should be there to protectthem and look after them.''More than 1250 front-line police have undergone a four-day course inmental health intervention since 2007, and there are now 80 policeinspectors across the state who are trained as a mental health contactofficer.The NSW Police mental health intervention team became a permanentunit within the force in 2009.Designing for mental health
ABC Radio – RN Life Matters – 30 July 2013What’s your image of a psychiatric hospital? History has told us mentalhealth institutions are places of isolation, often places to be feared—sterile, barren wards or locked rooms. We know environment can havemarked effects on the psychological health of a person and it isenvironment, and particularly the garden, that has influenced the designof the mental health unit at the new Gold Coast University Hospital. Thedesign was recently awarded a high commendation at the 9th annualDesign and Health International Academy Awards, which were held inBrisbane this month. Megan Reading is a former nurse and PrincipalArchitect with Hassell, one of the architectural firms behind the design.
News in BriefMental health courseunderway in Cairns
ABC Radio Australia – 25 July 2013Nurses and community workersfrom six Pacific Island nationsare completing a much-neededmental health course at JamesCook University in Cairns.
The course, which runs for fourweeks, is supported by theAustralia Awards Fellowshipand answers a plea from PapuaNew Guinea nurses for furthertraining in the mental healthsector. The course will provide aboost to the shortage ofqualified mental health workersand the shortage of ongoingtraining opportunities in thePacific.This Online website is easy touse and may be useful for someof our readers.It has an anxiety and depressionquiz and based onanswers/results, you arereferred to appropriate servicesand supports.MindSpot is Government fundedand partnered by Macquarie Uniand Beyond Blue.MindSpot Clinic is a FREEtelephone and online service forAustralians with stress, worry,anxiety, low mood ordepression. It provides freemental health screeningassessments, therapist-guidedtreatment courses and referralsto help people recover and staywell. Go to MindSpothttp://www.mindspot.org.au/
Image: Gold Coast University Hospital Mental Health Unit (photo by ChristopherFrederick Jones)

Page 12 of 28
Young men in crisis: mental health studyBy Clifford Fram, AAP National Medical Writer July 22, 2013YOUNG Australian men are in crisis, with half feeling stressed and nearlyone in 10 having thoughts about suicide, according to new research.Mental health experts are alarmed by the extent of the unhappiness, butthey are optimistic about finding an appropriate internet-based methodof helping the tech-savvy generation.
The research, which explores the impact of technology on mental healthand wellbeing, shows distressed 16-to-25-year-old men are likely to findhealth information on the internet as many listen to music and playgames online.The results suggest the current mental health system is failing youngmen, say the organisers. They believe improved mental health willreduce the number of suicides, vehicle accidents and fights, which arethe biggest killers of young men in Australia."For the last 20 years we have known our young men are not faringwell," says Young and Well Cooperative Research Centre CEO AssociateProfessor Jane Burns, whose organisation partnered with Movember andbeyondblue for the study."Technology presents our best prospect yet," she says. "We must partnerwith young men to create services that are more relevant to them." Theresearch shows distressed young men are likely to use the internet lateat night. "We must make sure we provide the right type of service at theright time, and that includes being available after 11 o'clock at night."There is a real sense of young men having to go through a rite of passageand they will eventually grow out of it. "But there is a group who end upbeing the drug, accident and suicide statistics that we are nervous andconcerned about."There are also those whose issues are never addressed, who end uphaving issues with drugs and alcohol in their 40s, and who end up beingsuicide stats in our older generation. "Let's work out what we need to doto ensure that when young men are in distress they know how to getsupport."That might not be going to speak to a professional. That may be gettingsupport in an online space they are comfortable with." Beyondblue CEOKate Carnell says the research provides invaluable insight into the onlinehabits of young men, particularly those who need support. "This willpave the way for better engagement with at-risk young men."* Readers seeking support and information about suicideprevention can contact Lifeline on 13 11 14.
News in BriefMental health services staffcut in central Queensland
Fraser Coast Chronicle – 17 July 2013SHOCK waves are runningthrough central Queensland'shealth sector as the impact ofstaff cuts to mental health anddrug and alcohol services takeeffect.Queensland Nurses Unionspokesman Dave Abraham said26 positions would be cut acrossthe region including five mentalhealth community supportworkers in Rockhampton, andGladstone's alcohol, tobacco andother drugs nurse unit manager."Mental health is crying out formore services, not less," MrAbraham said."Mental health is grosslyunderfunded, especially inyoung people where earlydiagnosis is a major area ofconcern…we need to put morein, not take it out."Mr Abraham said the union heldgrave concerns as responsibilityfor primary care was being putback on GPs and the non-government sector.But he said the government wasalso taking away support for theGPs and the non-governmentorganisations."It doesn't make sense…andwe're not sure this is the last ofthe cuts," he said.The cuts are the result of theintegration of mental health andalcohol, tobacco and other drugsservices.Mr Abraham said Gladstone hada lot of alcohol-related issueswith cashed-up workers."Having people in place to dealwith these sorts of issues isimportant," he said.A spokesman for MinisterLawrence Springborg onTuesday said the CQ healthboard had canvassed voluntaryredundancies and was re-structuring mental health anddrug and alcohol supportservices.
According to new research, nearly one in 10 young Australian men have hadthoughts about suicide. Source: AAP

Page 13 of 28
Beyond madness: a modern approach to hearingvoices
Authors: Adele de Jager and Paul Rhodes: – 10 July 2013Four years ago, a woman came to speak to my third year psychologyclass at the University of Auckland. Her story completely changed theway I thought about voice-hearing. Like most people, I associated“hearing things” with being very unwell psychologically; with madness.Yet here was an articulate, hilarious and confident woman – a mentalhealth educator – who was very much in touch with reality.The first voice she heard was asupportive, maternal voice whichdidn’t cause her any distress. Later,she heard a group of demonic-likevoices who threatened to harm her orthose she cared about. She wasdiagnosed with schizophrenia andinstitutionalised for many years.Her turning point came when sheasked her voices to show her some of their power by doing the dishes.When they didn’t, their hold over her started to loosen. Slowly, shelearnt how to deal with her voices, built relationships with others andfinally gained employment helping other voice-hearers. Hers is one ofthe stories of recovery recorded in Living with voices: 50 stories ofrecovery.What struck me most about her story was how easy it was to draw ananalogy between her voices and internal “self-talk”. Immediately, theexperience of voice-hearing seemed less foreign and incomprehensibleand more akin to what most people experience. This “inner-speech”theory is in fact the most well-known neuropsychological theory aboutwhat causes voices.Apart from making voice-hearing seem less foreign, her story challengedseveral assumptions I held. First, it seemed that she was able to live afunctional, productive and meaningful life while still hearing voices.Second, a diagnosis of schizophrenia is thought to carry with it a verypoor prognosis, with little hope of recovery.So, is her experience unique? It seems not. There is evidence of long-term recovery for around half of people distressed by their voices,enabling them to live meaningful lives and function to a degreeconsidered normal by most people.Indeed, it appears that hearing voices is not an abnormal humanexperience. General population studies show that 10% to 40% of thenon-psychiatric population hear voices at some point in their lives. It isalso not unusual for those who have lost a loved one to hear the voice ofthe deceased during the months following their death (although manyinitially deny this due to stigma surrounding voice-hearing). So it seemspossible to be a “healthy” voice-hearer.The other thing that really stood out from what she said was theprofound mismatch between her needs and the help she got. She neededto talk about her experiences and figure out how to deal with her voices.At that time, however, talking to voice-hearers about their voices wasdiscouraged as it was believed that this would worsen their symptoms.Instead, she was treated mainly with medication (in those days, largedoses of it). So, what treatments are available today? Medication remainsthe first-line treatment for distressed voice-hearers. Many findantipsychotic medications helpful, as they “dampen down” physical,mental and emotional responses.continues next page
About the Authors
Adèle de JagerRegistered ProvisionalPsychologist; Doctorate ofClinical Psychology / Master ofScience (Candidate) atUniversity of Sydney
Paul RhodesSenior Lecturer in ClinicalPsychology at the ClinicalPsychology Unit, University ofSydney. His research interestsinclude family therapy foranorexia nervosa, systemicapproaches to challengingbehaviour and developmentaldisabilities, reflective practice inclinical psychology, andqualitative methodologies. Paulis also Honorary Senior ClinicalPsychologist at The Children’sHospital, Westmead, where forthe past five years he has runthe Family Therapy Trainingand Research Clinic in theDepartment of PsychologicalMedicine. From 2008 to 2010 heserved as Contributing Editor ofthe Australian and New ZealandJournal of Family Therapy.

Page 14 of 28
continued from previous pageBut they can have serious side-effects. These include changes inmetabolism that lead to weight gain and increased risk for stroke, heartdisease and diabetes. They may also make some people feel “foggy” or“zombie-like”. Medication is ineffective ineliminating voices in at least one-quarter of cases. This has lead totalking therapies gainingacceptance as a treatment fordistressing voices. Instead of tryingto get rid of voices, talkingtherapies aim to diminish thedistress they can cause.One way of doing this is throughconsidering the evidence for andagainst beliefs about voices that make the hearer feel more upset. If yourvoice says threatening things and you believe it is powerful and intendsto harm you, it makes sense to feel frightened. Testing out whether thevoice has the power to do things (like doing the dishes) in a carefullyplanned way (for example, it wouldn’t be helpful to ask for a messagethrough something ambiguous like a television program) can help thehearer feel more in control and less frightened.Other strategies that can help in day-to-day management of voice-hearing include decreasing overall stress, listening to certain music,reading and focusing one’s attention on other sounds. Unfortunately, noone formula works for everyone: a lot of trial and error is usuallyrequired to find out what works.The Maastricht approach – which is closely connected to the consumermovement, including the Hearing Voices Network – takes a more radicalperspective. It defines voices as representing an emotional problem,either literally or metaphorically. This opens up interpretivepossibilities, so even critical or threatening voices can be viewed ashelpful.One voice-hearer, for example, cameto interpret a voice saying “I’ll killyou” as a warning not to make aparticular decision in her life. Anotherperson who identifies that a criticalvoice appears or becomes louderwhen they are over-stressed or over-tired may come to respond by restingor giving excess work to a colleague.So the critical voice becomesprotective. Putting voices into thecontext of the hearer’s life historyhelps the hearer to make sense ofthem and identify what positive rolethey could have.Interestingly, voice-hearers’ style ofrelating to their voice is similar to how they relate to other people. Thosewho feel socially inferior to others, for instance, report feeling inferior totheir voices. They are also more likely to comply with instructions toharm themselves, while the opposite is true of those who feel superior inboth spheres.concludes next page
Mental Health First AidTraining The Mental HealthFirst Aid Programis run by MentalHealth First AidTM(MHFA) Australia,a national non-profit healthpromotion charityfocused on training andresearch. More informationabout MHFA Australia here:www.mhfa.com.auStandard Mental Health FirstAid covers the most commondisorders such as depression,anxiety, psychotic disorders andalcohol and drug problems.2013 Dates:8th & 9th Oct 20133rd & 4th Dec 2013Youth Mental HealthFirst Aid is for adultswho live or work with youngpeople. This course alsoaddresses self-harm and eatingdisorders. 2013 dates:5th & 6th Nov 2013Both courses cover thedevelopment of a 5-step actionplan for mental health first aid,managing suicide, panic attacks,psychotic behaviour and generalcommunication skills.Training Location: ArcadianSurf Lifesaving Club, The StrandRockpool, North Ward Q 4810Duration: 2 daysCost: $100 per personRegistration Forms availableonline at:http://www.mifa.org.au/mental-health-first-aidTo find out more contact ourQld Manager Education andTraining, Philippa Harris on4725 3664, or [email protected].
Some voice-hearers read a flare up ofvoices as a signal they’re stressed ortired.
One-quarter of people who heardisturbing voices
Page 15 of 28
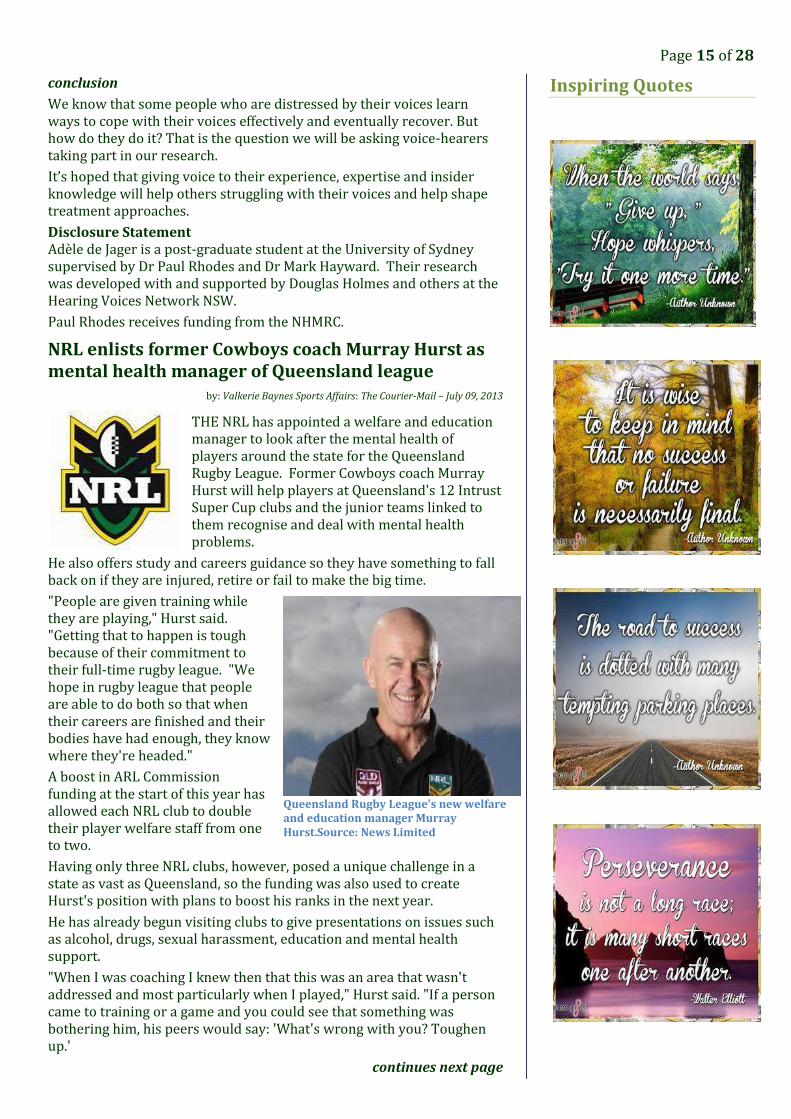
conclusionWe know that some people who are distressed by their voices learnways to cope with their voices effectively and eventually recover. Buthow do they do it? That is the question we will be asking voice-hearerstaking part in our research.It’s hoped that giving voice to their experience, expertise and insiderknowledge will help others struggling with their voices and help shapetreatment approaches.Disclosure StatementAdèle de Jager is a post-graduate student at the University of Sydneysupervised by Dr Paul Rhodes and Dr Mark Hayward. Their researchwas developed with and supported by Douglas Holmes and others at theHearing Voices Network NSW.Paul Rhodes receives funding from the NHMRC.NRL enlists former Cowboys coach Murray Hurst asmental health manager of Queensland leagueby: Valkerie Baynes Sports Affairs: The Courier-Mail – July 09, 2013THE NRL has appointed a welfare and educationmanager to look after the mental health ofplayers around the state for the QueenslandRugby League. Former Cowboys coach MurrayHurst will help players at Queensland's 12 IntrustSuper Cup clubs and the junior teams linked tothem recognise and deal with mental healthproblems.He also offers study and careers guidance so they have something to fallback on if they are injured, retire or fail to make the big time."People are given training whilethey are playing," Hurst said."Getting that to happen is toughbecause of their commitment totheir full-time rugby league. "Wehope in rugby league that peopleare able to do both so that whentheir careers are finished and theirbodies have had enough, they knowwhere they're headed."A boost in ARL Commissionfunding at the start of this year hasallowed each NRL club to doubletheir player welfare staff from oneto two.Having only three NRL clubs, however, posed a unique challenge in astate as vast as Queensland, so the funding was also used to createHurst's position with plans to boost his ranks in the next year.He has already begun visiting clubs to give presentations on issues suchas alcohol, drugs, sexual harassment, education and mental healthsupport."When I was coaching I knew then that this was an area that wasn'taddressed and most particularly when I played," Hurst said. "If a personcame to training or a game and you could see that something wasbothering him, his peers would say: 'What's wrong with you? Toughenup.'
continues next page
Inspiring Quotes
Queensland Rugby League's new welfareand education manager MurrayHurst.Source: News Limited

Page 16 of 28
continued from previous pageNow you understand that what the player might be worried about couldbe something that's very major. It could be mentally affecting him somuch that he could be thinking the worst scenario to alleviate that pain."Player welfare hit the spotlight thisyear with the tragic death ofCowboys squad member AlexElisala and another 20-year-old,Wests Tigers prop Mosese Fotuaika,while the Bulldogs' 2012 Dally Mwinner, Ben Barba, took time outfrom the game to deal withpersonal issues.The Bulldogs and the Knightsplayed for the beyondblue Cup onSunday in Mackay to boostawareness of mental health.NRL welfare and education manager Paul Heptonstall, who met withHurst on the Gold Coast last week to talk strategy, said it was vital to giveplayers education opportunities outside of football."We're trying to prepare them for something other than rugby leaguebecause the bottleneck is so thin with the people that play rugby leaguethat the majority of them aren't going to (make it)," Heptonstall said."If someone's at university or they're doing a trade, there's somethingelse within that person's life that is important."So when they do suffer an injury, or they might be dropped, or gothrough a form slump, or they might even be released, or they don't getthe call-up to progress to the next grade, it's not like the whole world istumbling in."Another key is encouraging players to speak up if they have a problem."It's not only destigmatising it from the players, it's destigmatising itfrom a coach's perspective as well because often players won't talkabout it because they're worried about being considered a liability,"Heptonstall said.
Leisure Accessible
For those that don't know us,Leisure Accessible providesrecreational opportunities forpeople with a disability andsenior citizens.The club operates "ROSIE", apurpose built 7.9m vessel with aflat deck and including anaccessible toilet. The side andfront ramps provide access forwheelchairs and passengers.
“ROSIE” is a smooth riding,stable boat that travels in a flatattitude, excellent for carriage ofpeople with a disability and thephysically impaired on fishingtrips and river cruising.If you are interested in findingout more, please get in touch viaemail –[email protected] or call Ken on 0407 674 652.
IMPORTANT DATES10 September World Suicide Prevention Day
12 September R U OK? Day
26 September MIFNQ Annual General Meeting
6-13 October Mental Health Week
10 October World Mental Health Day

Page 17 of 28
Game onExploring the impact of technologies on young men'smental health and wellbeing
Australian Policy Online: 22 July, 2013Jane M. Burns, and others | Young and Well Cooperative Research Centre (YAWCRC)New research finds that the Australian mental health system is failingyoung men and suggests modern technology offers the potential toimprove mental health and wellbeing.
Summary:The first Young and Well National Survey, a scientific study of youngmen from across Australia, uncovered alarming statistics that suggestour current mental health system is failing young men:Nearly one in five felt that life is hardly worth living.Nearly one in 10 thought about taking their own life.42 percent experience psychological distress.Unemployment and moderate to very high levels of psychologicaldistress trigger suicidal thoughts and behaviour.The research also identifies new methods of engagement with youngmen via technology that matches their current usage and behaviouronline, offering new hope for improving their mental health andwellbeing.Young men with moderate to very high levels of psychological distresswere more likely to:Talk about problems on the internet, with 66 percent finding ithelpful.Use the internet to find information for a mental health, alcohol orother substance abuse problem (48 percent).Be somewhat to very satisfied with the information they receivedonline (95 percent). Young men who reportedhigher levels of psychologicaldistress were more likely toaccess health information, listento (or download / upload)music and play games withothers on the internet.Young and Well Cooperative Research CentrePhone: 03 9937 1333Fax: 03 9416 4416Email: [email protected]: www.youngandwellcrc.org.auMailing and Street Address:Unit 17, 71 Victoria CrescentABBOTSFORD VIC 3067
A Life without StigmaBarbara Hocking |www.SANE.org
25 July, 2013
Stigma stops people asking forhelp and getting the treatmentand support they need. It makesit more difficult to findsomewhere decent to live, a job,a mortgage, or insurance. It canmake it more difficult to get helpto look after children, makefriends, feel good about yourself,or even to feel that life is worthliving. Stigma is a major barrierto recovery. If people withmental illness are to be includedas equal members of our society,then stigma and its associateddiscrimination must beeliminated.This report examines the impactstigma has on the lives of peopleaffected by mental illness,including an overview ofassociated issues from thegrowing body of research in thisarea. It describes some of themajor stigma-reductioninitiatives carried out inAustralia and overseas, looks atthe evidence base to identifywhat works, and makesrecommendations for futureaction in Australia to create alife without stigma.
To read the report, go towww.sane.org.

Page 18 of 28
A supportive program for tobacco smokers with a mental Illness (carers alsowelcome).Are you or someone you know thinking about quitting or cutting down theirtobacco use?If so, join the Tobacco and Mental Illness teams FREE peer supported 5 weektobacco program and get information about what options there are for peoplewho want to make changes.
Program FeedbackFrom participants of the National Tobacco Mental IllnessProgramQuotes from participants at the end of the July program:What changes did you notice whilst participating in theprogram?“Finance and emotional wellbeing. Feel like the happiest man in theworld”I don’t cough as badlyLost 3kgs and my health feels better for itHave become more motivated since I quitI have enough money to buy new clothesI have more breathe, the cravings are now gone and I can feel myappetite coming backFeeling happy to be able to breathe when completing mountainclimbs... was never able to do that before!Was feeling excellent as a non-smoker.. a lot of energy!My clothes smell a little betterWhat was the most important/beneficial part of the course: Talking to a group facilitator who has been through the samequitting process as us in the group. I also found her (terrible)drawing and no nonsense deliver of what was actually in a cigarettevery important Talking thorough all the triggers and making plans. It was nice tohave a facilitator that understood where we were coming from andwho had walked in our shoes Talking through the problems Seeing some people's success Positive outlook on myself and future as non smoker Carbon monoxide readings, shock factor Being applauded every week when I had made it through without acigarette and having Nicole check in on me weekly.Any other comments:Very well presentedI really liked the group, it really made me make the decision to giveupWonderful, special people, sharing, compassionate, extremelyhelpful.
Helping peoplewith mental
illness to beGroup Support
ProgramNEXT COURSEDate: 15 August 2013Time:10am – 12pm weeklyLocation:Uniting Care CommunityTraining Room, 276-280Ross River Rd Aitkenvale.
Info and Bookings:Rebecca WoodNTMI Project OfficerM: 0434 742 322E: [email protected] just turn up on the day.

Page 19 of 28
DISCLAIMERThe information in this articleis provided for generalinformation only. It is notintended as medical advice,and should not be relied uponas a substitute forconsultations with qualifiedhealth professionals who candetermine your individualmedical needs.We hope this information is ofhelp to you in thinking aboutfurther questions that youmight want to ask yourdoctors and qualified healthprofessionals.
Mental Illness Fellowship NQ Inc
That One Time I Went Nuts: Why Mental Health CareMatters
By Josephine Ganner – 23 July 2013 - www.greatist.com.Foul LanguageI don’t like the word “crazy”. It leaves a bitter taste in my mouth, and it'sa term I have run from in my life. I don’t want to be crazy. I don’t want tofeel helpless and out of control.But as the song goes, you can’t always get what you want. Over the pastseveral years I’ve had ample experience with “crazy” — personally,professionally, and in my family. I’ve made it through to the other sidewhile others have not, and the experiences have only strengthened mybelief in the importance of changing the way this country approachesmental health care. It is my hope that in sharing these experiences, I canhelp jumpstart a conversation about mental health in this country that islong overdue.Working to be “Not Crazy”As a teenager, I wasdesperate to bedifferent than “crazy”. Istruggled withanorexia and thepressure to be aperfect distancerunner. My anxietiesthreatened to consumeme with the fear that I,too, would end upbeing saved some day— as my father hadsaved my mother,pulling her from her depression. I would cry, drink alone in my room,and write angry poetry about the complexities of my mind, about beingleft to grow up on my own as my mother traveled the globe on a questfor corporate domination. I have grown from my years of teen angst,but my anxieties surrounding “crazy” have not altered.I’m not the only member of my family to feel these anxieties. Two yearsago, my then-nineteen-year-old little brother and I sat parked in ourdriveway. I can picture it so clearly: He gazes at me, tears falling downhis beet red face. “Jo,” He pleads. He grips the steering wheel as his handsshake. “Jo. I am not crazy.” I nod. “I know crazy Jo, and I am not crazy.Mama is crazy.” I nod in agreement. My brother is upset.Misunderstood. Growing up. Still processing his angst.
DiagnosisThis past year, my brother (pictured left)was diagnosed with Bipolar Disorder uponbeing admitted to a hospital’s psych wardfor 10 days.The scary, manic, psychosis-experiencing,hearing voices, “let’s practice flying off theroof” kind of bipolar.The kind that turns a star athlete and life-of-the-party Golden Boy into a recluse whofears the world and won’t leave his roomfor months. The kind that forces a twenty-one-year-old kid at thebeginning of his life into hospitals and electroconvulsive therapy.continues next page
Josephine Ganner
Josephine Ganner is anactress, mental healthactivist, and co-founder of 26Percent Productions, a filmproduction companydedicated to giving a voice tothose who suffer from MentalIllness. She is the creator ofthe blog OkNo and can befound lending her comedicchops to the stages of LosAngeles and New York. Theopinions expressed hereinare hers. To learn more aboutJo, check out her website(www.josephineganner.com)or find her on Twitter orFacebook.

Page 20 of 28
continued from previous pageMy brother’s illness terrifies me. In the months leading up to him gettinghelp in Colorado, I would sit outside his bedroom and listen to himscreaming out of desperation at voices inside his head. He would tellthem to leave him alone. He would verbally attack himself, tellinghimself that nobody loved him or liked him. That nobody wanted himthere. That he was worthless. That he deserved to die.My little brother suffered for months with the terrorizing voices in hishead, trying to hide his illness. He didn’t want to go back to the hospitalwith the catatonic masses. He would suppress his reactions in public, butwithin the privacy of his room he was tortured by instructions to killhimself and hurt his family.A Deathly DrugI knew that my brother was on a medication that could make his skin falloff. “How terrible,” I remember thinking. “Who would put somebody onsuch a drug?”My brother was in Colorado being treated for Bipolar Disorder, about tobegin electroconvulsive therapy, and I knew that afterward he would beforever changed. I want to help him and others like him — to see, tounderstand, and to remember what the illness was like before treatment.To give the world a glimpse into the lives and struggles of those whosuffer from mental illness.I am an actor, and what I know how to do is tell stories. So I created afilm production company, 26 Percent Productions, to tell my brother’sstory and the stories of the millions of people who are affected by MentalIllness. Twenty six percent of Americans suffer from a diagnosablemental illness, and it only seems right the work that my companyproduces gives a voice to those who suffer.I also knew that come hell or high water I would get my own depressionunder control. So I enlisted the help of my psychiatrist, whononchalantly prescribed me a drug called Lamictal.Ten days later, I was filming a documentary about mental illness withmy brother in Colorado, only to find myself, unexpectedly, in a hospital.This time, I was the patient. A rash had spread all over my body andmucus membranes. My mouth and throat were exploding in painfullumps and a white paste resembling a yeast infection. My lungs werebubbling inside of me. My eyes burned. To go to the bathroom felt like anancient form of fire torture.I had developed Stevens Johnsons Syndrome, a rare immune reaction tomy prescription of Lamictal — the same drug that my brother had beenprescribed with intense caution. The same drug for which he got bloodtests and for which the dosage was slowly increased every two weeks.My prescription did not include such precautions. As a result, inresponse to the drug my body decided to burn itself from the inside out,making my skin fall off.Dreams, Screams, and PsychosisI do not remember anything past the first day. I was transferred to theUniversity of Colorado Hospital’s ICU burn unit, where I remained forthe month of March in a drug-induced coma, on the brink of death. Mybody burned. My rash turned into bubbling blisters that sloughed offinternally and externally. In order to save my sight and my life, I enduredtwo amniotic membrane surgeries and was put on life support.While I was sick, I experienced an intense psychosis that was so real andso terrifying I honestly believed I was being sexually abused and that Iwould never see my family again.
continues next page
LAMICTALLamictal is approved by the FDAfor the maintenance treatmentof adults with bipolar disorder.It has been found to help delaybouts of depression, mania,hypomania (a milder form ofmania), and mixed episodes inthose being treated withstandard therapy. It is especiallyeffective in the prevention ofbipolar depression. It is the firstFDA-approved therapy sincelithium for maintenance inbipolar disorder. Lamictal isconsidered a mood-stabilizinganticonvulsant and is mostcommonly prescribed toprevent or control seizures inthe treatment of epilepsy.Recent studies have shown itmay possess antidepressanteffects in bipolar disorder.Lamictal Side EffectsLamictal comes in several typesof tablets, such as chewable ororally disintegrating. It adds tothe effects of other centralnervous system suppressantssuch as alcohol -- and to thosefound in many antihistamines,cold medications, painmedications, and musclerelaxants. Check with yourdoctor before taking any ofthese. Three out of every 1,000people taking Lamictal willdevelop a rash. Sometimes therash can prove serious or evenfatal. If a rash develops, thisdrug should be stoppedimmediately. Common sideeffects of Lamictal include: Headache Dizziness Diarrhea Dream abnormalities Itching Vision difficultiesMedication errors haveoccurred in filling Lamictalprescriptions because otherdrugs have similar names, likeLamisil, lamivudine, Ludiomil,labetalol, and Lomotil. To avoidconfusion, make sure the drugname is clearly written on yourprescription.

Page 21 of 28
continued from previous pageThis psychosis lasted for days in the ICU. At one point, I tried to run awayfrom the hospital on all fours and found myself, soon after, in astraitjacket with each wrist bound to the bed. Any human under theinfluence of such high doses of pain medications and sedatives mightinterpret their physical state and inability to move as torture.The experience of coming off my pain medication in the hospital andrealizing what was real and what was not real was disconcerting. I haddaily therapy sessions. I should probably get a PTSD counselor. But mypsychosis has ended. I experienced truly “crazy” — and let me tellyou: It is a scary, scary, slope to slip down.The Path to RecoveryI lived.I lost my looks. I lost my body. Ilost my muscle mass and energyand a month of my life. But Ilived. That is my firstaccomplishment. I can sit hereand be thankful today that Ihave a voice. That I have mysight.That I lost only 60 percent of my skin. I can be thankful that slowly butsurely my eyelashes will grow back and the red baby skin rash coveringmy body will fade over the next few years. My wounds will heal. I willmove on. I will move back to New York and use my new perspective forgood. I will get back on that stage and into those auditions and I willcreate documentaries that change the world.I’m all good.Well, I will be all good.The Ones Left BehindMy brother, meanwhile, is still in Colorado. He is still on Lamictal. He isstill undergoing electroconvulsive therapy and every day is a struggle. Ido not know what rests in his future. I hope for the best. But as one of mybrother’s doctors put it, “Mental health is the bad stepchild ofhealthcare.” It doesn’t get the support it needs and nobody wants totalk about it.Instead, we rely on quick fixes. In modern (Western) culture, the swingsof highs and lows that we as humans feel are being plastered with falsepromises in prescription bottles and overpriced therapy. A quick fix forour every emotion. We have found solace in bottles. Pills. Booze. Wefeel better knowing that our money is being spent on “fixing us,” even ifour shrink just prescribes us pills.But maybe we were never really broken. Some of us have it rougher thanothers, but I guarantee that if we took a step back we would witnesswhat the literary canon was writing about all those years ago: the humancondition. Pain and desperation have been around for a lot longer thanwe give them credit for. It’s just that our perception of them has shifted.Maybe all I needed during the dark times in my life — all most of us need— was a friend.Somebody to hold my hand and tell me that these feelings, dear human,are part of growing up — part of life. Today, I can advocate for myself. Ihave a voice. But it is those like my brother who do not. The silentsufferers of mental illness, the men and women who sit alone, afraid toleave the house. To be a casualty of the drug companies is one thing; tobe a casualty of your mind and a failing system is quite another.
concludes next page
News in BriefMental health groupurges continued reforms
ABC News - Mon Aug 12, 2013A Toowoomba mental healthgroup has urged the next federalgovernment to keep crucialreforms to the sector.
The Toowoomba Clubhousehelps people with mental illnessget jobs, homes and integrateback into society.Executive director Luke Terrysays there has been a change inthe Federal Government'sapproach to mental health inrecent years with more moneyand resources provided to helpthe marginalised.He says the reforms are notcompleted and he is worriedthey are at risk because ofbudget constraints. "We need tomake sure the next government,whoever it is, increases thatfunding, as well there needs tobe a continued commitment tomental health," he said.Mr Terry says the major partiesneed to consider ending thepractice of institutionalisationand move to community-basedcare but he says that requiresadvertising campaigns to breakdown stigmas about people withmental illness. "It's been provenall over the world, especially inthe UK they made thecommitment to get rid ofinstitutions," he said. "Peopleliving in institutions can livevery happily in the community."Mr Terry wants more federalinitiatives to change the widercommunity's perceptions aboutpeople with mental illness.
Photo: 26 Percent Productions
Luke Terry, Executive Director

Page 22 of 28
conclusionHow to HelpWhat can be done? We must advocate for them. We can give them a voiceby spreading awareness of mental illness and of Stevens JohnsonsSyndrome. By ending social stigma and shifting people’s perspective inregards to the “scary crazy people”.The truth is that my brother is afraid of you, dear reader. Probablymore so than you are of him. He is kind and gentle and likes to draw anddo physics problems. He is soft-spoken and has a sheepish smile, boyishgood looks, and a quick wit.But he is tortured by a sickness that cannot be fixed with an antibioticand a bandage. It doesn’t have a clear-cut beginning and end. But thatdoes not mean, under any circumstances, that he should be left by thewayside.We must allow it to be okay for people struggling with mental illness toask for help. We must hold our judgment and support the evolution ofmental health care toward a system that supports the full road to — asystem that doesn’t pick and choose who it will heal based on theirmonetary value or their insurance.It is not enough to lock somebody away and throw away the key. Wemust be brave enough to admit that 26 percent of us struggle withmental health issues. Brave enough to admit that we as individualsmay belong to the 26 percent, and that that's okay. It is okay to feelafraid, to question reality, to feel "off", to feel excruciatingly low.Heck, it’s even okay to run around naked on the roof every so oftenbecause a voice told you to. What is important is to know that those whodo are not alone and that there are people in this world who care. Whowant to help.Even if you are not part of the 26 percent, you know someone whosuffers. It is now the time to be brave. To muster the strength to ask forhelp or lend a helping hand.To change the way you think and talk about mental illness and itstreatment, which in turn has the power to change the way otherpeople think about these issues. It is time to listen. To embrace the 26percent and the stories they have to tell.My wounds will heal. What I cannot tolerate is a system that tells mylittle brother his cannot.New mental health service for Tamworth
Catherine Clifford – ABC News – 17 June 2013A 24-hour, 20-bed facility to help people with mental illness re-integrateinto the community is to be established in Tamworth. The Minister forMental Health, Kevin Humphries, announced the multi-million dollarinitiative on Monday.It's the first of its kind in the state to be operated by a non-governmentorganisation.
continues next page
There are many ways that youcan support us and the work wedo at MIFNQ. If you haven’tdone so already, why notbecome a member.Membership is free and anapplication form is on the backpage or you can join online atour website.Volunteering is another wayyou can make a valuablecontribution. We always havelots of opportunities forvolunteers to make a differenceto our services and programs.You may like to volunteer withadministration tasks, assist withour extensive library, are ahandyman or assist with ourprogram courses which canrange from reading, music,cooking, arts and crafts and awhole lot more. Many of ourvolunteers find they can receiveas much themselves as theygenerously give.Partnerships/SponsorsYou might also considerbecoming a business partner orsponsor of the Fellowship. Ourdedicated staff put in manyhours of unpaid work to enableus to provide the best servicewe can in the community.Business partnerships allow uskeep the corporate servicesdepartment running effectivelyand efficiently while allowing usto plan for future growth andthe ever increasing demand forservices. And donating toMIFNQ online is easy.Online Donations - Secureonline donations can be made athttp://www.givenow.com.au/mifnq.

Page 23 of 28
The 2013|2014 Far NorthQueensland Book can beordered from your localMIFNQ office or online at
https://www.entertainmentbook.com.au/orderbooks/2
700u79
continued from previous pageServices Manager in charge of the program, Jim Booth, says the programis specifically designed to support people who've recently left prison orhospital."It means that we will have staff on duty 24 hours a day and that meansif anyone feels any symptoms, any depression or anxiety, any fear thenthey can access staff immediately," he said."Staff can provide emergency medication 24 hours a day and it meansthat if there are any disturbances than, obviously, staff can go andintervene."Jim Booth says beds will be shared between Tamworth and Newcastle,with the majority of the beds set aside in Tamworth."This is for people who are moving out of hospitalisation, out of mentalhealth institutions and, in some cases out of Corrective Services, makingtheir way back to the community but still needing 24-hour care," he said."They will be referred by one of the health organisations because this isthe only one in regional NSW at this stage."Life expectancy for people with mental illness thesame as 30 years ago: report
By Eliza Harvey | The World Today | Aug 7, 2013
A damning report has found the life expectancy for peoplesuffering from a mental illness has not improved in 30 years.The finding is in stark contrast to the advances made for Australianssuffering from illnesses like heart disease and cancer.Mental health expert Professor John Mendoza co-authored the report,which looks at mental illness in Australia over the past three decades.He says Australia hasmade no progress inclosing the gap in lifeexpectancy for peoplewho experiencesignificant mental healthdisorders."So we're talkingdifferent psychosis,schizophrenia, bipolarand major depression,"Professor Mendoza said."If you experience thatillness, this year inAustralia your life expectancy is no better than when David Richmondcompleted his report on closing down institutional care in 1983."Now I can think of no other area of health care where we've gotcommon conditions where that's the case." The research also foundmental illness is now the biggest contributor to disability in the country.People are 'falling through the cracks'Professor Mendoza blames the grim state of mental health care onfailures to invest in research and intervention. "What we've really failedto do is what we've done so well in areas like breast cancer, where weinvested very sensibly in research and we've built our capacity and ourknowledge to intervene much earlier," he said.
continues next page
Entertainment Book
The Entertainment™ Book isa local restaurant and activityguide, which provideshundreds of up to 50% offand 2-for-1 offers from thefinest restaurants, cafés,attractions, theatres andaccommodation.Entertainment™ Books havebeen distributed by fund-raising organisationsthroughout Australia andNew Zealand for the past 18years.MIFNQ will again be sellingthese books as a way to raisefunds to aide in our efforts toassist those living withmental illness whilesupporting their carers andfamilies.Photo: Research has found mental illness is nowthe biggest contributor to disability in the country.(stock.xchng/Nihan Aydi)
$55
$55
$55

Page 24 of 28
continued from previous page"Now if you go into mental health, it's astark contrast - you do not have thatinfrastructure. You do not have thatinvestment in research and you do nothave the workforce to actually respondto the level of need that's in ourcommunity. "Your chances of gettingcoordinated care, effective care, aredependent on where you live, yourcapacity to pay and your determination -or those of your loved ones - to actuallyget that care."This leads to people "falling through the cracks", Professor Mendozasaid. Health and welfare lecturer Ingrid Ozols says she is an example ofsomeone who benefited from a good treatment program."I have bipolar disorder, I have tried to take my life on several occasions,but I've been really lucky," she said. "I've had great mental health careand I know I'm in the minority. And [that care is] what's helped me tobecome someone who can contribute to society."Doctors say targeting mental illness atwork is crucial in reducing the numberof people becoming acutely unwell andneeding hospital treatment."I have a colleague who once said it's OKto be nosy. We're such a good society atbeing disconnected, we need to be moreconnected than ever," Ms Ozols said."We don't have the extended familieslike we used to so we need to reach outto our neighbours, reach out to astranger and say 'look, how are thingsfaring?' "And then we need to learn theskills - how do you have a braveconversation?" A greater focus on selfcare and programs that teach sufferers how to keep mentally well arethe main way to improve the system, Ms Ozols said.Obsessive Hope DisorderReportObsessive Hope Disorder of broken intothree reports: Summary, Technical andPerspectives. Each report may bepurchased separately or as a full suiteof all three reports. Reports areavailable in Printed format or E-version.For a detailed description of eachreport and to place your order, go to:http://connetica.com.au/ohd-landing-pageFREE: Synopsis of ReportApology: Publication Error. TheObsessive Hope Disorder Summary Reportincludes an error indicating that screenviewing or free download options areavailable for this report. This is incorrect. Copies of the Summary report, in E-Version or as a printed copy, are available for purchase only. Should you wishto proceed, select from the options provided above. We apologise for anyconfusion or concern.
Book Review
Authors:Prof Marius Romme, Dr SandraEscher, Jacqui Dillon, Dr DirkCorstens and Prof MervynMorrisSynopsis:Marius Romme and SandraEscher's new analysis of thehearing voices experienceoutside of the illness model, hasresulted in accepting andmaking sense of voices. Thisstudy of 50 stories forms theevidence for this successful newapproach to working with voicehearers.Quote:"This is essential reading formental health workers of allprofessions, which challengesconventional thinking, empowersmental health service users andlooks forward to a more humaneapproach to psychiatric care."Richard Bentall, Professor of ClinicalPsychology, Bangor University, WalesAvailable From:Richmond Fellowship ofWestern AustraliaPO Box 682 Bentley WA 6982Online Store: $35.00 + postagehttp://www.rfwa.org.au/shop.htmlAngus & Robertson Book StoresPrice: $54.99
Prof. John Mendoza
Ingrid Ozols

Page 25 of 28
Hard at work in Cairns
Training & Professional DevelopmentGlenda Blackwell – MIFNQ - Townsville
Assisting Families ProgramIn July a group of stafffrom our 3 centres,Mackay, Cairns andTownsville and 2 womenfrom Mental IllnessFellowship NT (Darwinand Alice Springs)went toCairns to be trained asfacilitators in a newprogram - AssistingFamilies.It is modular programdesigned for carers andfamilies looking aftersomeone with a mental illness. It is interactive, informative and flexibleand will be a wonderful addition to our suite of programs at MIFNQ.David and Mary from Schizophrenia Fellowship of NSW and RemindTraining were wonderful trainers over the 2 days. Launch dates will beannounced and for more information call MIFNQ on 47253664.Counselling TrainingTacked on to these 2 days of trainingwas a day of upskilling for ourMIFNQ counsellors.This is essential to have an effectiveservice that offers the best for ourclients.Thank you Barbara Anderson for aninformative day.
Mental Health First AidIn July we were invited todeliver MHFA to a group ofJCU students from thePsychology Club. We wereable to work with Camillafrom JCU in presenting. Itwas a great 2 days oflearning and sharingstories and I feel we all gota lot from the course.Here at MIFNQ we offerthe Standard and YouthMHFA courses. They aredesigned to aid people tobe like first –aiders, maybefirst on the scene when someone is having a panic attack or a colleaguedoesn’t seem to be doing well at work, till professional help can beprovided.Ideal for reception staff, teachers, really for anyone around people. Youcan contact MIFNQ on 47253664 for more information.continues next page
Barbara Anderson, Counselling &Support Manager, MIFNQ
Everybody passed!

Page 26 of 28
ProfessionalDevelopmentProfessional developmentis important for our staffto grow skills and learnnew ones that are able tobe utilised in our workwith clients.This is vital in MIFNQoffering a service that isup to date, evidence basedand useful.Glenda (left) and Pip (right), MIFNQ counsellors recently travelled toSydney for the 11th World Association for Contextual Behavioural
Science (“ACBS”) conference held at the University of NSW.
The Importance of RolePlayingRuss Harris is the author of “TheHappiness Trap”, “The RealityTrap” and many other books .Joe Ciarocchi is a prolificresearcher and author of“Emotional Intelligence forEveryday Life”, “Get Out of YourMind and Into Your Life forTeens”The Lesson...
Books by Kelly Wilson
Acceptance and CommitmentAcceptance and CommitmentTherapy (“ACT”) guru, KellyWilson from Mississippi sharinghis expertise and wisdom.Kelly is the author of “Mindfulnessfor Two” and “The Wisdom toKnow the Difference”.
Russ (left) and Joe (right) role playing

Page 27 of 28
Living Proof – Positive Stories of Mental IllnessMental Illness Fellowship NQ IncMIFNQ-Cairns Mental Health Carers’ Support HubMIFNQ-Day To Day Living
MIFNQInc
@CairnsCarersHub@MIFNQ@LivingProof@Roads2Recovery
MIFNQInc
www.mifnq.org.au
Townsville has an extensive collection of books, DVD’s, CDs, VHS andcassettes for members to borrow. Feel free to come in and browse around.Library Hours: Monday – Friday 9:00am to 4:00pm
Mi Networks AUSTRALIAMi Networks is our promise that we can help connect you to information and services youneed. From the moment you walk in the door or pick up the phone, we will welcome you.We will listen and discuss your needs. Many of our staff and volunteers have someunderstanding of what you are experiencing, in part because they’ve experienced mentalillness or have cared for someone living with mental illness.Our PromiseA place you are welcome -- We promise to treat you like a person, not a number. We will always have time tolisten, question and discuss. We want to know how you are, what you need and how we can help.Peer Support -- Many of our staff and volunteers have lived experience: either living with mental illness or as thecarers of someone with mental illness. We are people with similar experiences and we will have someunderstanding of what you are going through.Relevant Information -- We offer tailored and up-to-date information to assist you, your family members, friendsand carers. If we don’t have the information you require, we will help you find it.Community Networks--We are linked into our local networks and have established strong and supportiveworking relationships with other services. We are connected to a broad range of programs, supports andinformation.A National Network --We offer a range of one-on-one and group support programs for you, your family members,friends and carers across Australia. If we can’t assist you on-site at one of our locations, we will connect you withsomeone who can.Personalised Referral -- We will refer you to the services and supports that best meet your needs. This may be aprogram we offer or it may be provided by someone else. We will support you to find the best fit for you.For further information go to the MiNetworks website http://www.minetworks.org.au/ or call 1800 985 944

Page 28 of 28OFFICIAL USE ONLYReceived: ___________________Membership No: ___________Entered: ____________________Initials: _____________________
MEMBERSHIP APPLICATION FORMI would like to become a member of Mental Illness Fellowship NQ Inc. Membership is free.
Individual Family Organization
Please select the category/categories which relate to you:
Family Member Friend Someone who experiences mental illness
Health Professional Student Other _____________________________
What Program/s are you currently enrolled in (if any):
Day to Day Living Early Psychosis MH First Aid
Mental Illness Education Respite Well Ways
DONATIONS AND REQUESTSI wish to support the work of MIFNQ, I have enclosed a donation of:
$100 $50 $25 Other ____________________________________
Please contact me about a regular contribution
I wish to donate in other ways…. __________________________________________________
Please contact me with information about helping the Fellowship through my Will
YOUR DETAILS
Name: .......................................................................................................................................................................
Address: ...................................................................................................................................................................
..................................................................................................................................................................................
Phone Home: ................................................. Work: .....................................................................................
Fax: ................................................................. Mobile: ...................................................................................
Email: .......................................................................................................................................................................
Email Consent (please sign) ........................................................................................................................................(This consent allows MIFNQ to contact you via electronic media)
Image Consent (please sign) .......................................................................................................................................(This consent allows MIFNQ to use your image on print and/or electronic media)On completion return to:Email:[email protected] Fax:(07) 4725 3819 Post:REPLY PAID 979Membership AdministrationMental Illness Fellowship NQ IncPO Box 979HYDE PARK QLD 4812