Normal anatomical variants
36
Normal Anatomical Variants Steve Corbett Guys and St Thomas’ NHS Foundation Trust
-
Upload
watanabeclub -
Category
Documents
-
view
744 -
download
0
Transcript of Normal anatomical variants

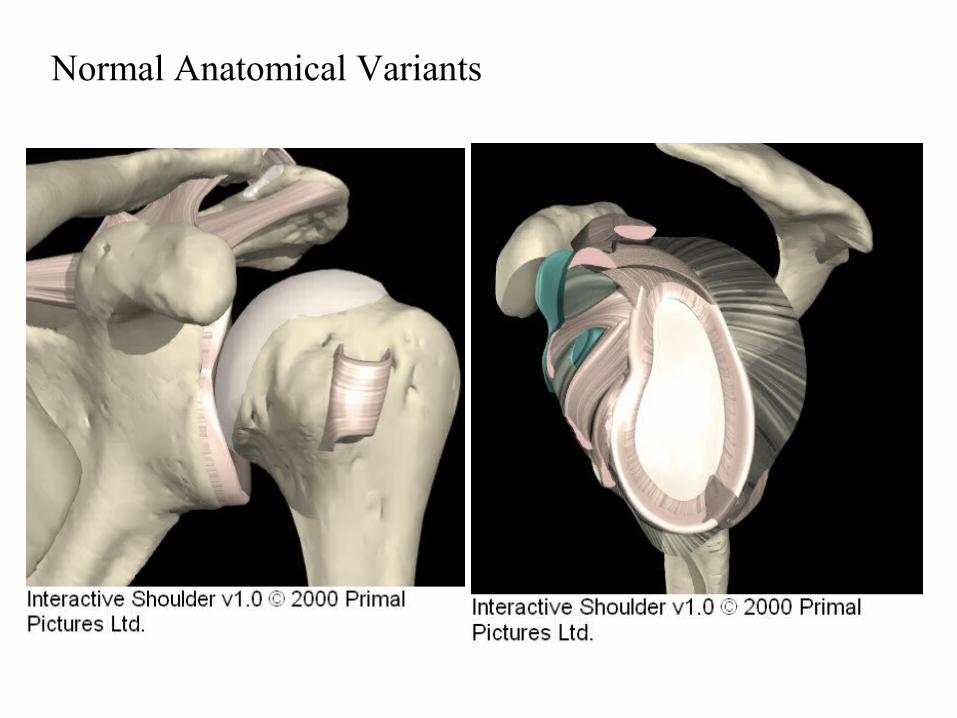
Normal Anatomical Variants
Steve CorbettGuys and St Thomas’ NHS Foundation Trust
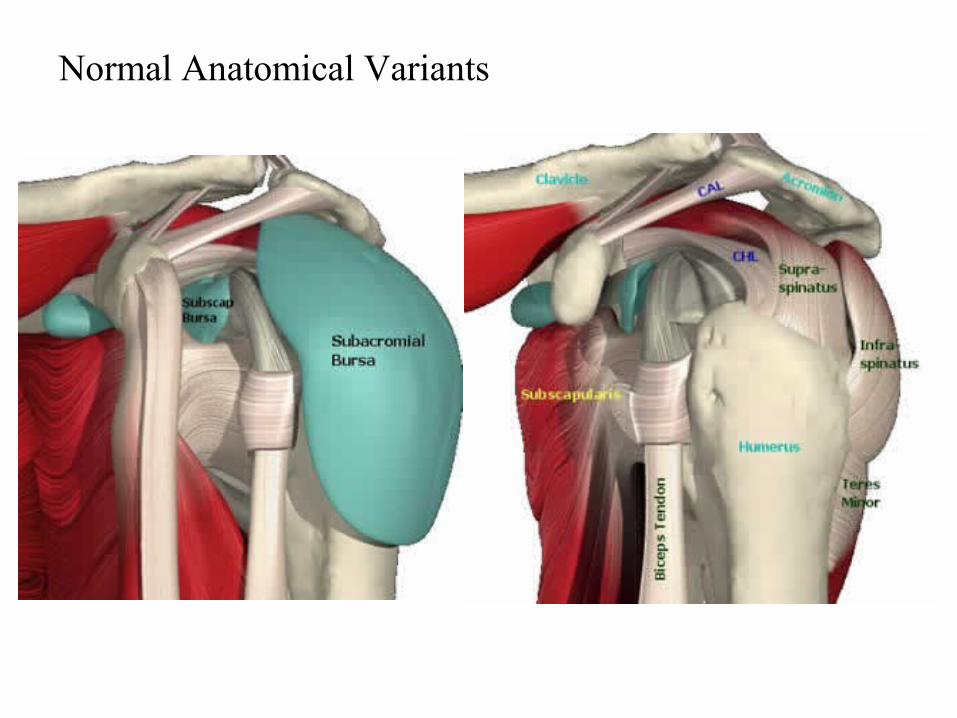
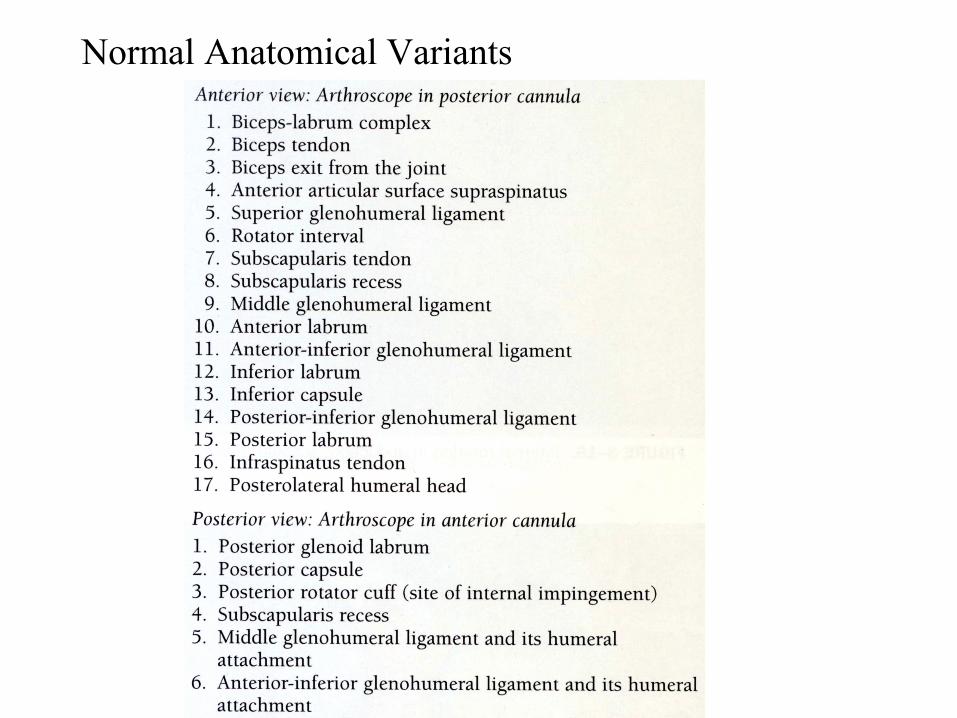
Normal Anatomical Variants
Normal Anatomical Variants
Normal Anatomical Variants

Normal Anatomical Variants
• Superior labrum / Biceps• Anterosuperior Quadrant• AI Quadrant• PI Quadrant
• PS Quadrant
• Biceps• AS head• Superior Cuff / Head• Posterior Cuff / Head
• GHJ Surfaces• Bursa

Normal Anatomical Variants: Superior labrum/Biceps
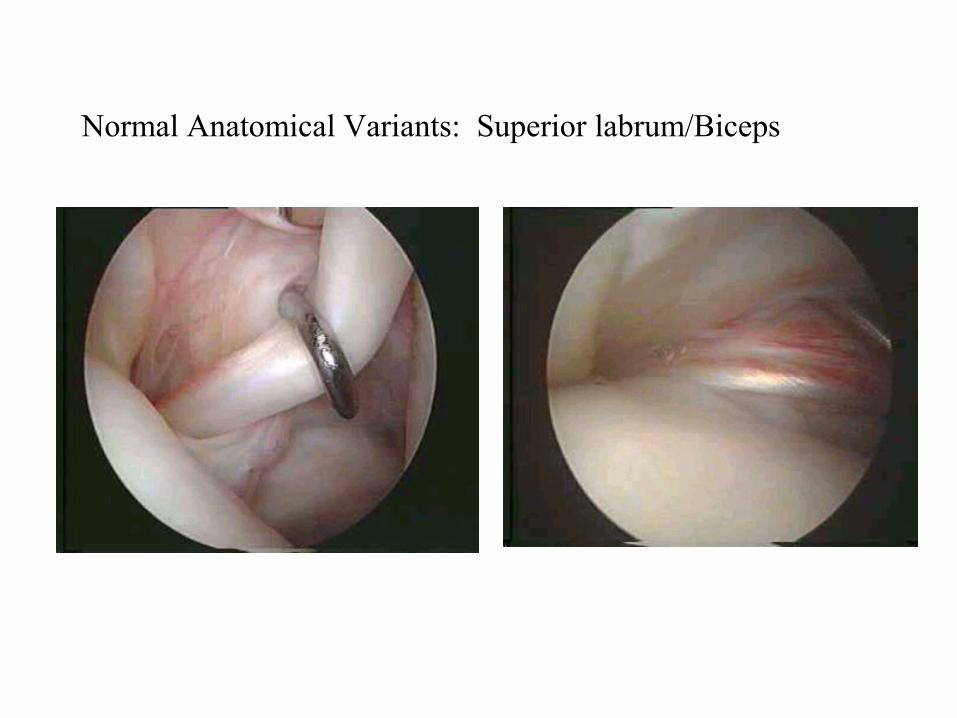
Normal Anatomical Variants: Superior labrum/Biceps
Normal Anatomical Variants: Superior labrum/Biceps
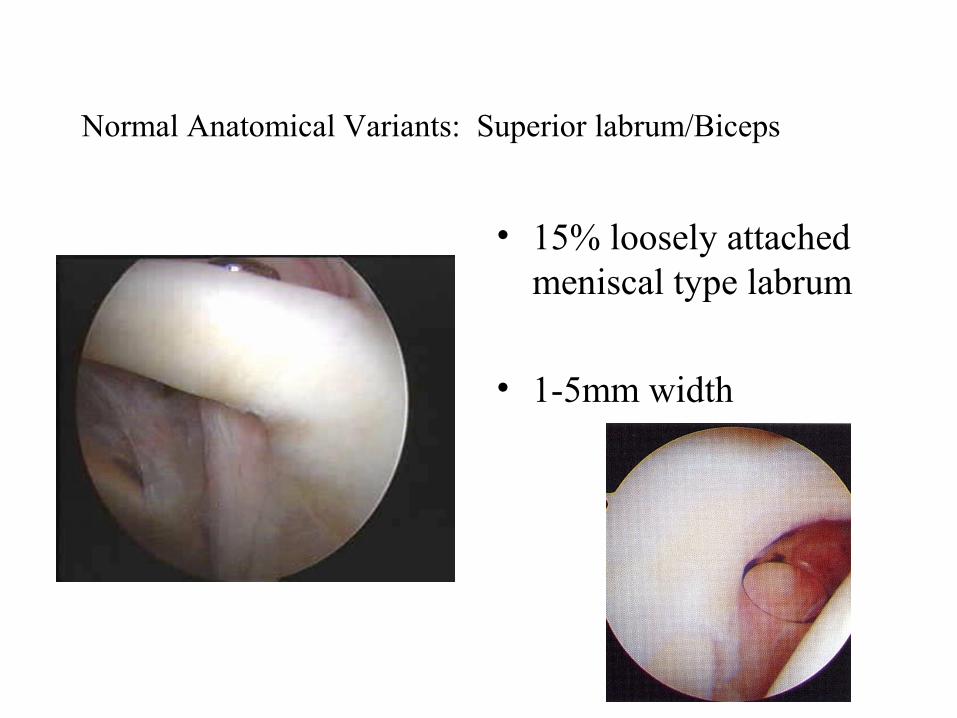
• 15% loosely attached meniscal type labrum
• 1-5mm width

Normal Anatomical Variants: Superior labrum/Biceps

Superior labrum/Biceps: SLAP
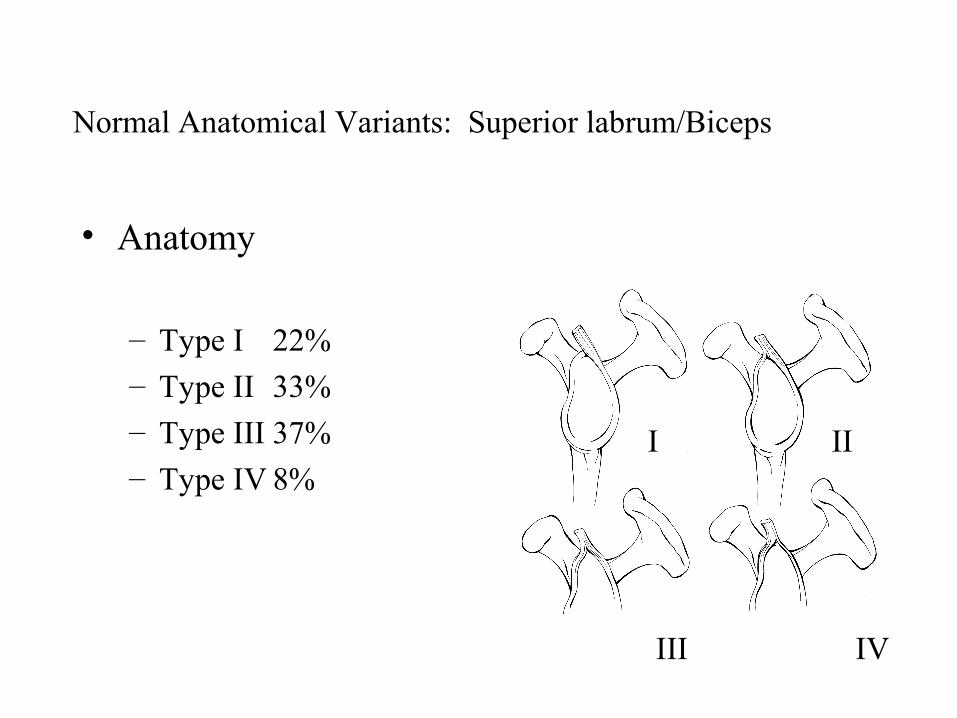
• Anatomy
– Type I 22%– Type II 33%– Type III 37%– Type IV 8%
I II
III IV
Normal Anatomical Variants: Superior labrum/Biceps
Normal Anatomical Variants: Superior labrum/Biceps
• Vincula Biceps
– Small strands of mesentry
– Pass from biceps to surrounding capsule
• Bifid Biceps
– 1 part attached to cable
– 2nd part attached to tubercle
• Complete absence
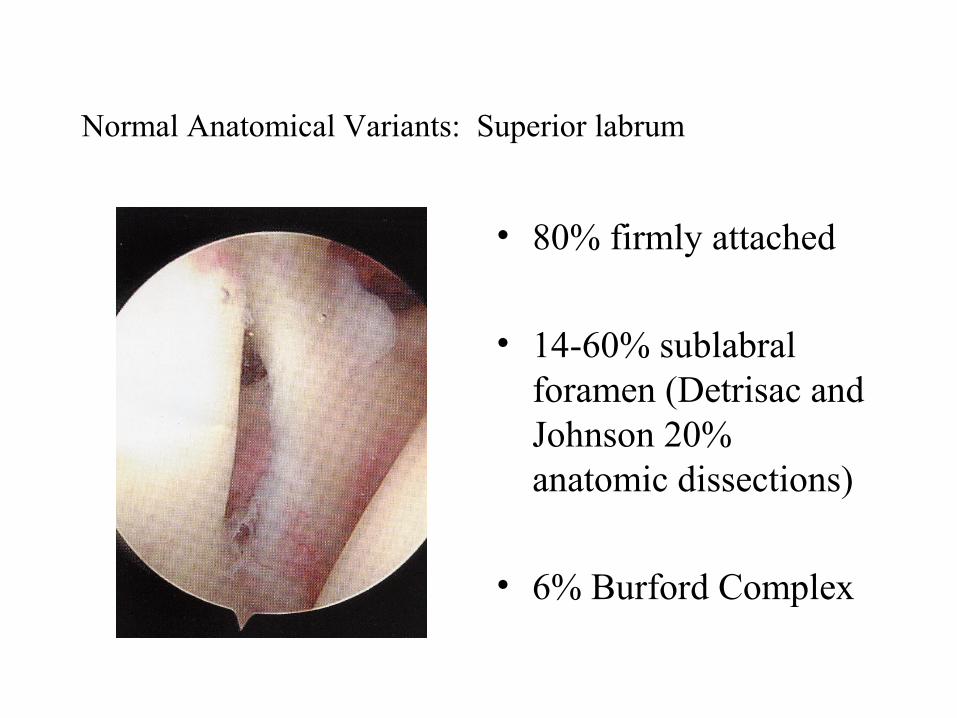
Normal Anatomical Variants: Superior labrum
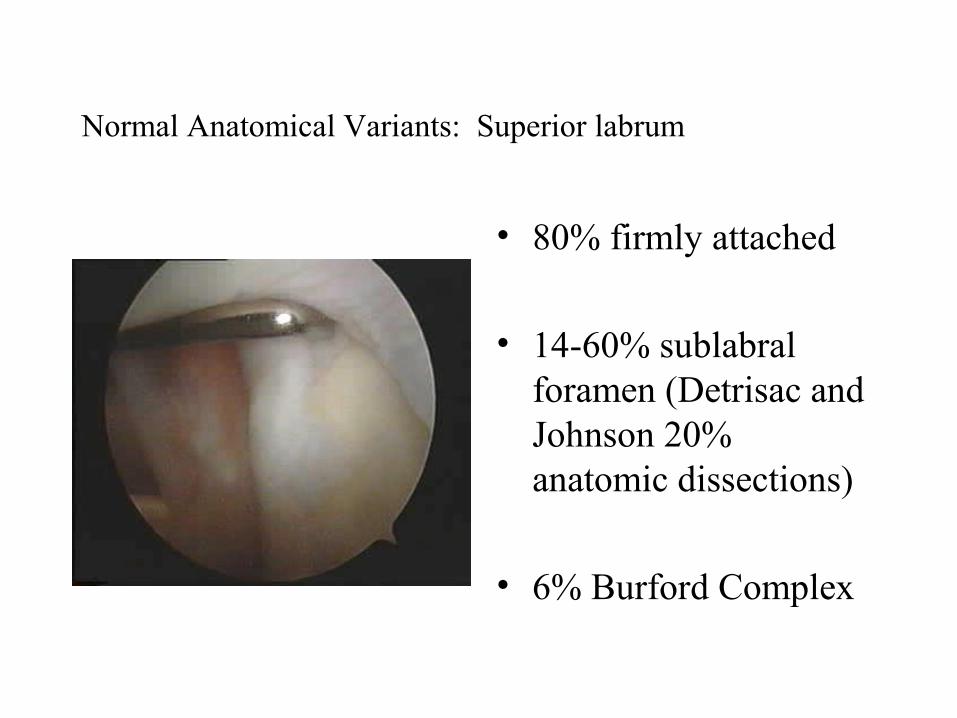
• 80% firmly attached
• 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections)
• 6% Burford Complex

Normal Anatomical Variants: Superior labrum
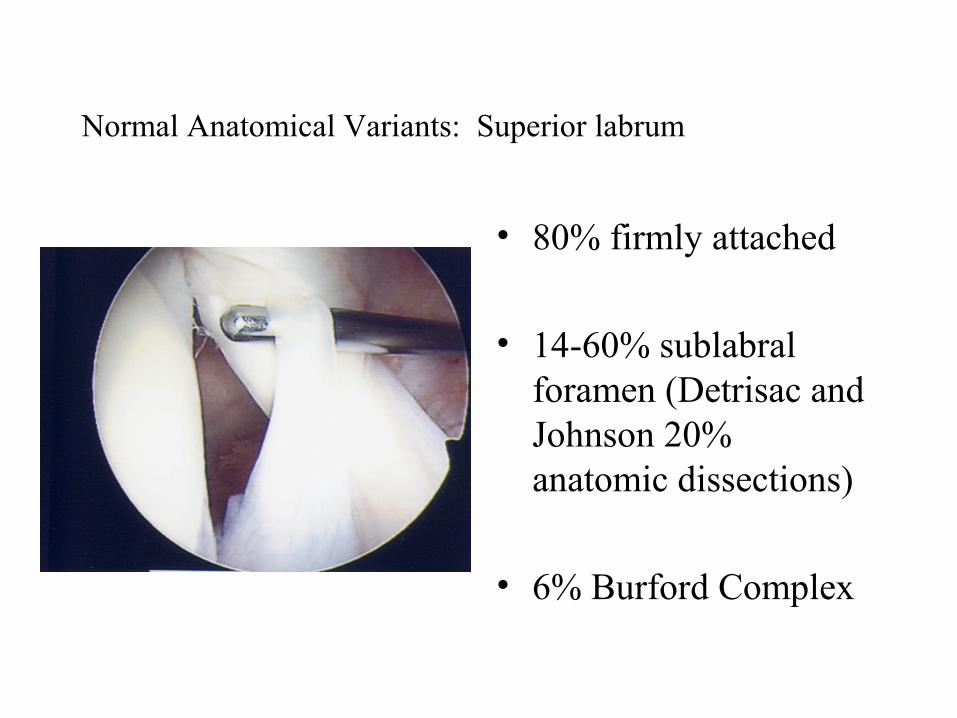
• 80% firmly attached
• 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections)
• 6% Burford Complex
Normal Anatomical Variants: Superior labrum
• 80% firmly attached
• 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections)
• 6% Burford Complex
Normal Anatomical Variants: Superior labrum
• 80% firmly attached
• 14-60% sublabral foramen (Detrisac and Johnson 20% anatomic dissections)
• 6% Burford Complex
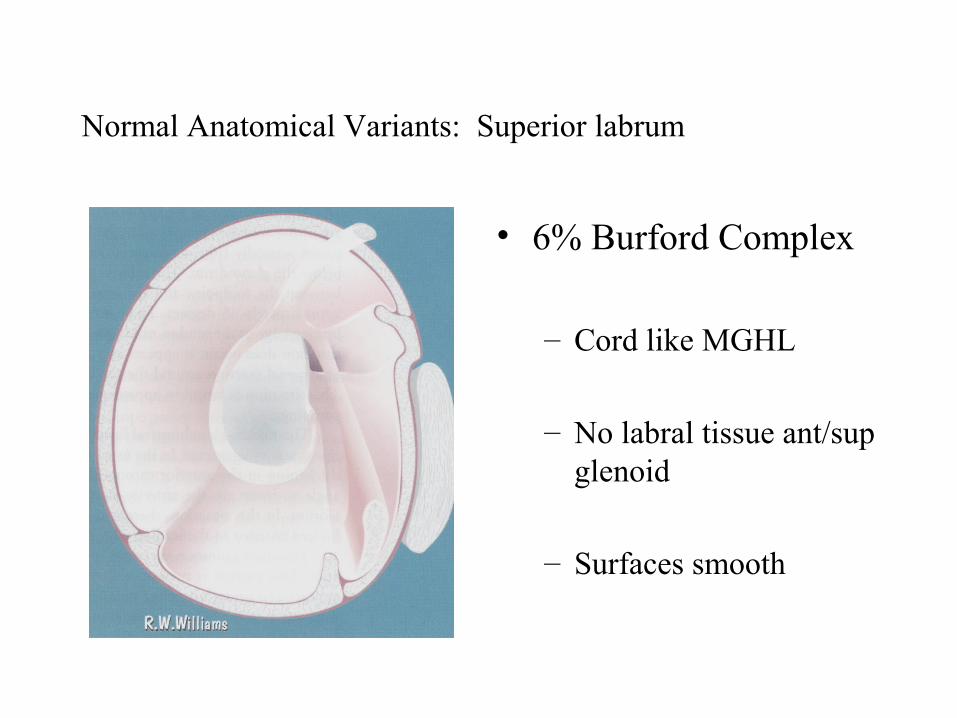
Normal Anatomical Variants: Superior labrum
• 6% Burford Complex
– Cord like MGHL
– No labral tissue ant/sup glenoid
– Surfaces smooth

Normal Anatomical Variants: Superior labrum
• 6% Burford Complex
– Cord like MGHL
– No labral tissue ant/sup glenoid
– Surfaces smooth
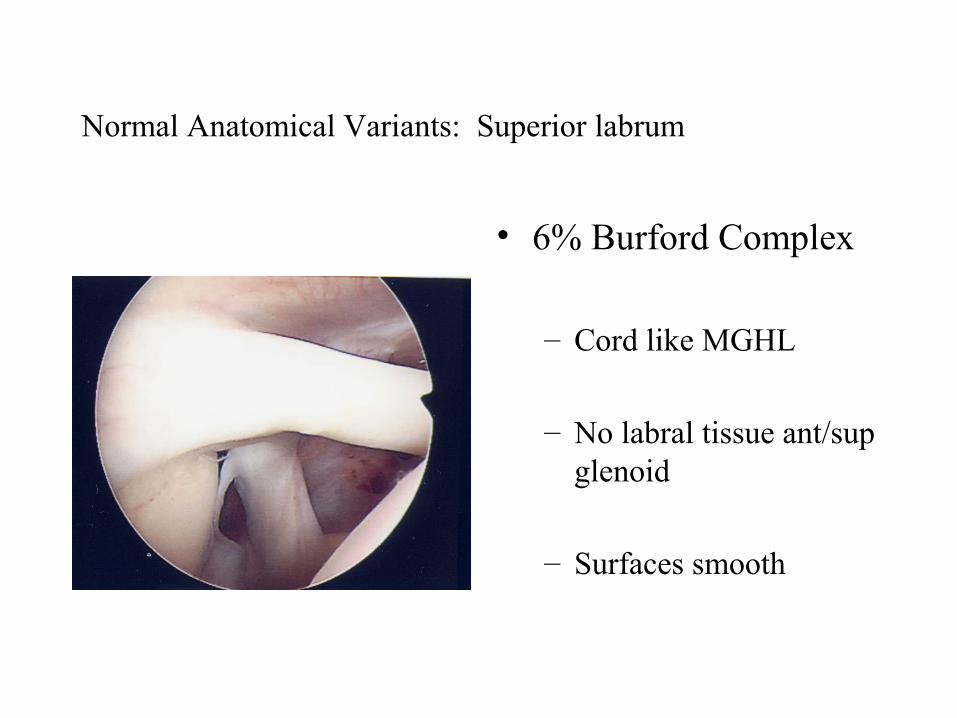
Normal Anatomical Variants: Superior labrum
• 6% Burford Complex
– Cord like MGHL
– No labral tissue ant/sup glenoid
– Surfaces smooth

Normal Anatomical Variants: Superior labrum
• Divides sup. 2/5 and inf. 3/5.
• Variable in depth

Normal Anatomical Variants: Subscapularis / SGHL
• Leading edge may be split or bifid
• 3%
• SGHL present in nearly 100%, Occassionally frayed

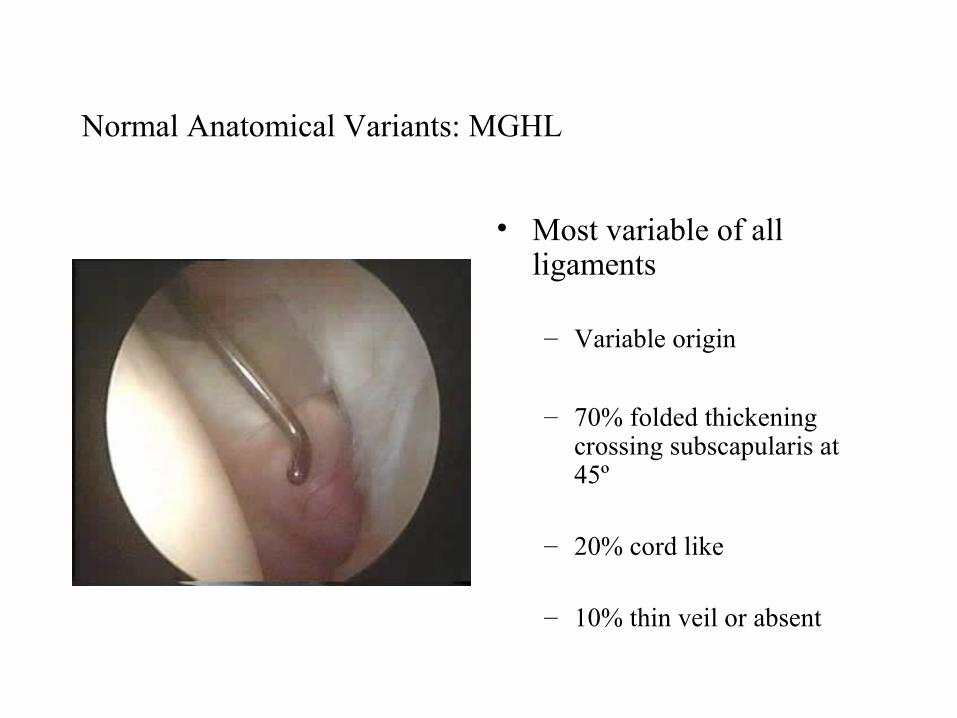
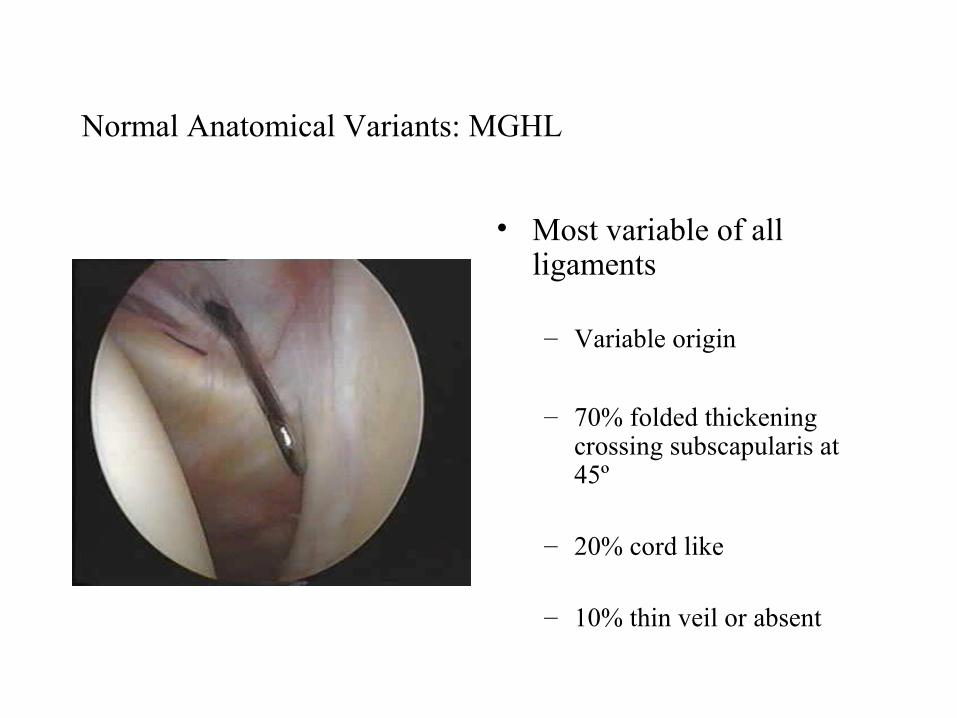
Normal Anatomical Variants: MGHL
• Most variable of all ligaments
– Variable origin
– 70% folded thickening crossing subscapularis at 45º
– 20% cord like
– 10% thin veil or absent
Normal Anatomical Variants: MGHL
• Most variable of all ligaments
– Variable origin
– 70% folded thickening crossing subscapularis at 45º
– 20% cord like
– 10% thin veil or absent
Normal Anatomical Variants: MGHL
• Most variable of all ligaments
– Variable origin
– 70% folded thickening crossing subscapularis at 45º
– 20% cord like
– 10% thin veil or absent

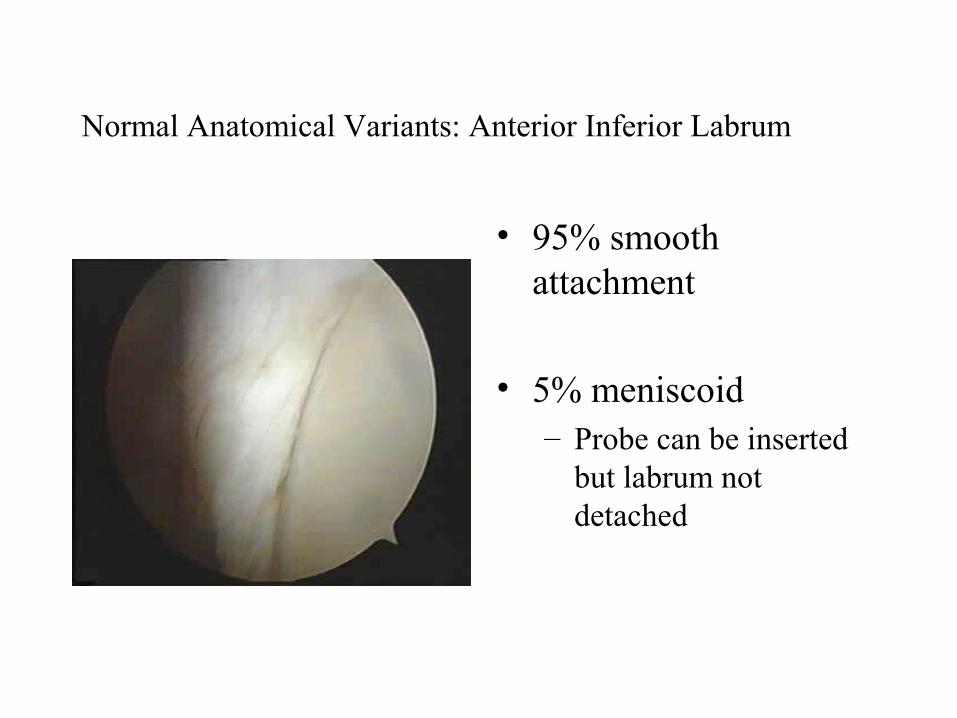
Normal Anatomical Variants: Anterior Inferior Labrum
• 95% smooth attachment
• 5% meniscoid– Probe can be inserted
but labrum not detached

Normal Anatomical Variants: Anterior Inferior Labrum
• 95% smooth attachment
• 5% meniscoid– Probe can be inserted
but labrum not detached
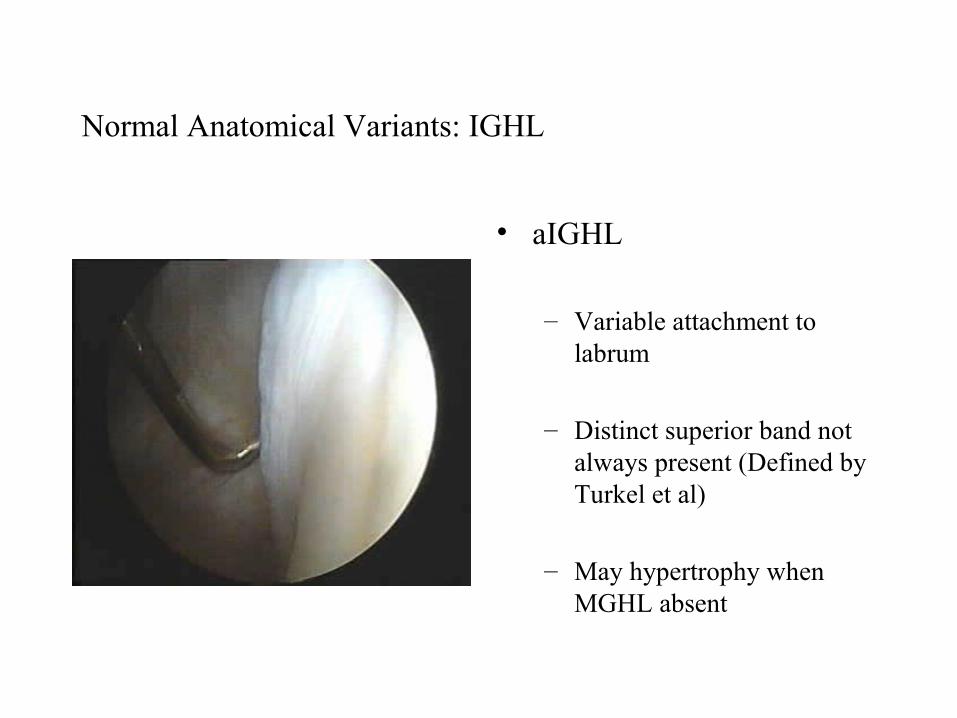
Normal Anatomical Variants: IGHL
• aIGHL
– Variable attachment to labrum
– Distinct superior band not always present (Defined by Turkel et al)
– May hypertrophy when MGHL absent
Normal Anatomical Variants: Inferior capsular recess
• Normally smooth
• Delicate synovial covering
• Small fenestrations
• Post. Sup. Band pIGHL not always well visualised (Schwartz et al)
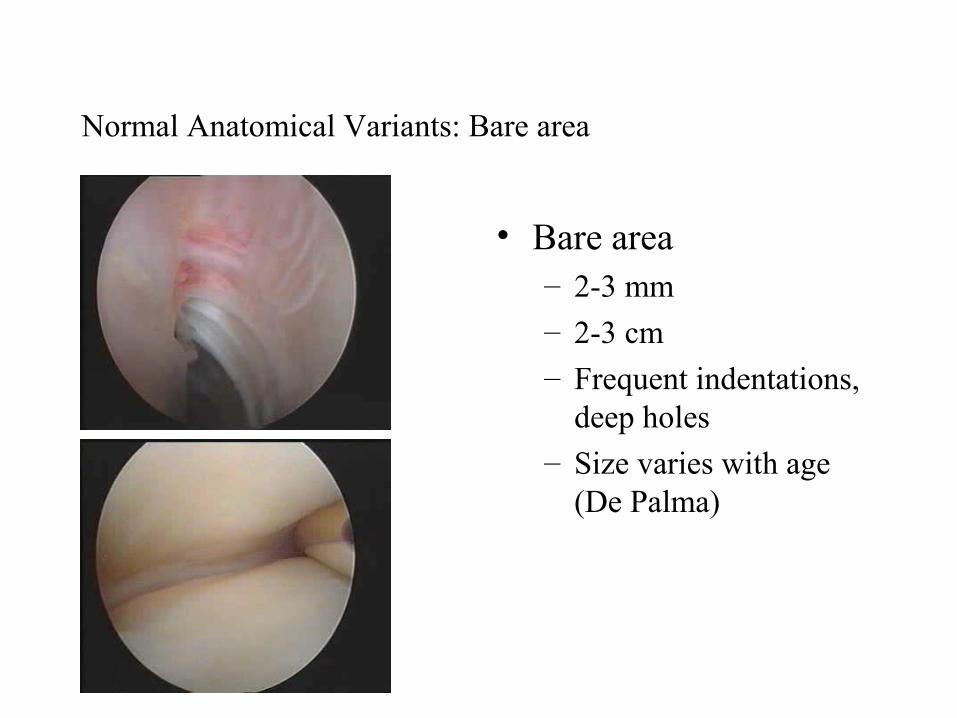
Normal Anatomical Variants: Bare area
• Bare area– 2-3 mm– 2-3 cm– Frequent indentations,
deep holes
– Size varies with age (De Palma)
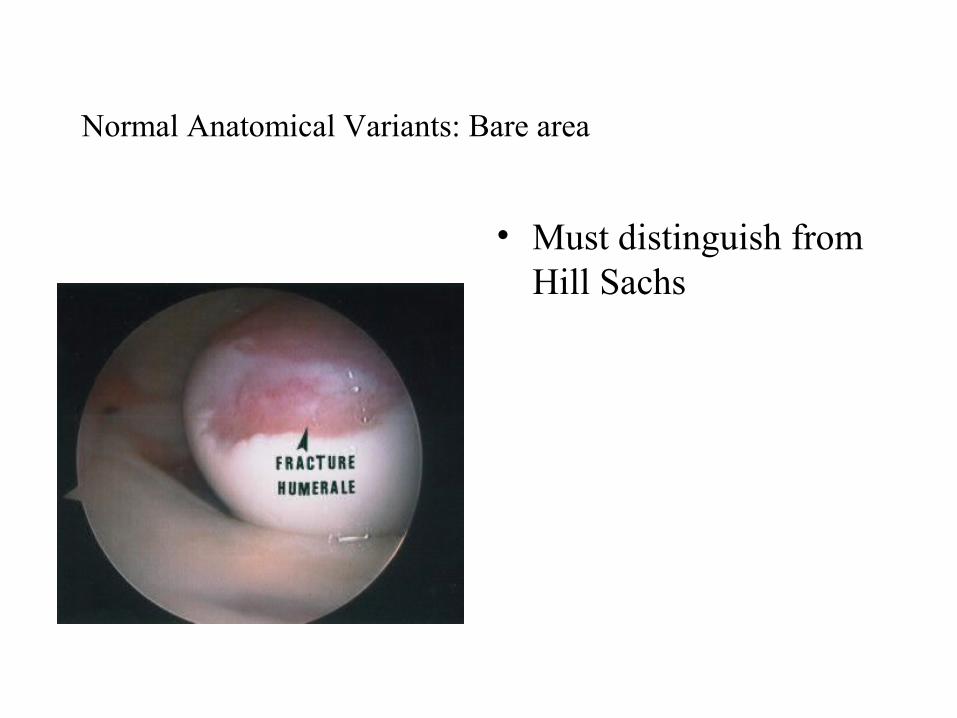
Normal Anatomical Variants: Bare area
• Must distinguish from Hill Sachs
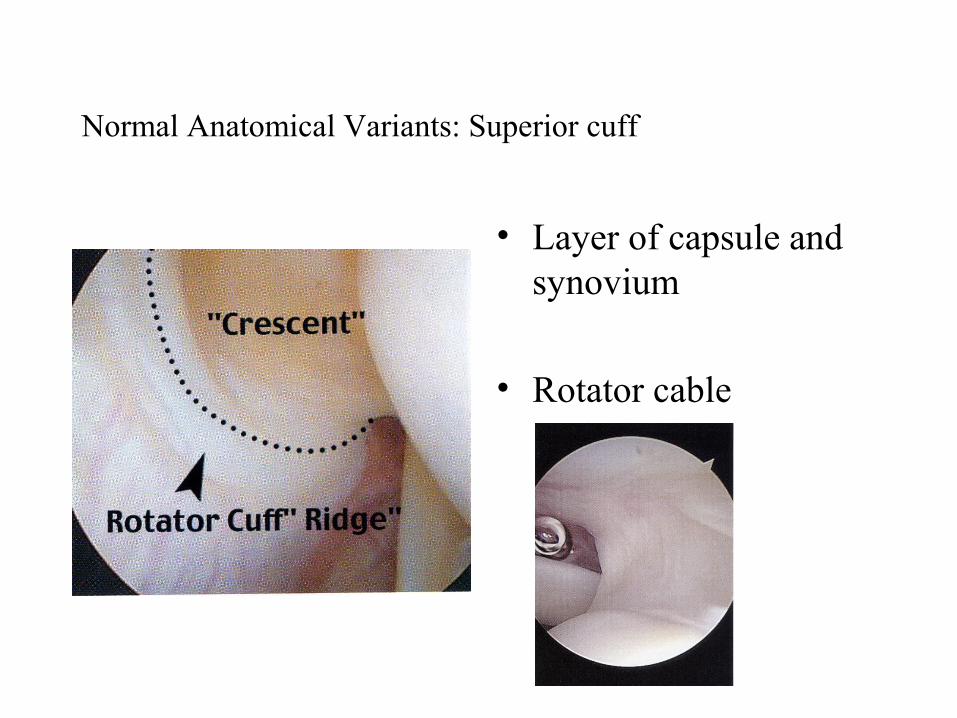
Normal Anatomical Variants: Superior cuff
• Layer of capsule and synovium
• Rotator cable
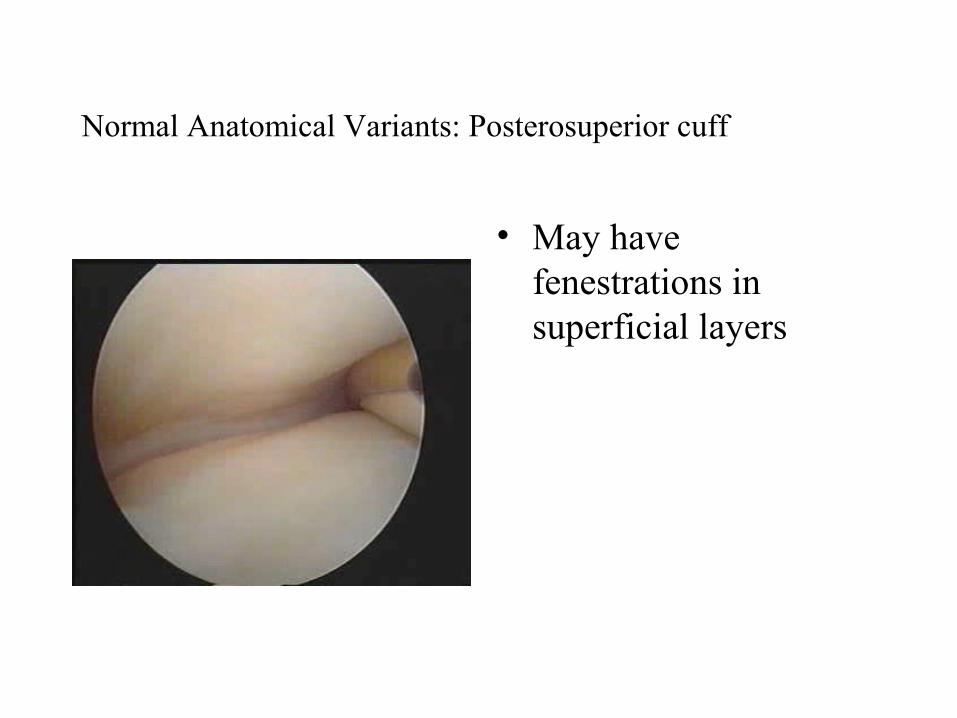
Normal Anatomical Variants: Posterosuperior cuff
• May have fenestrations in superficial layers
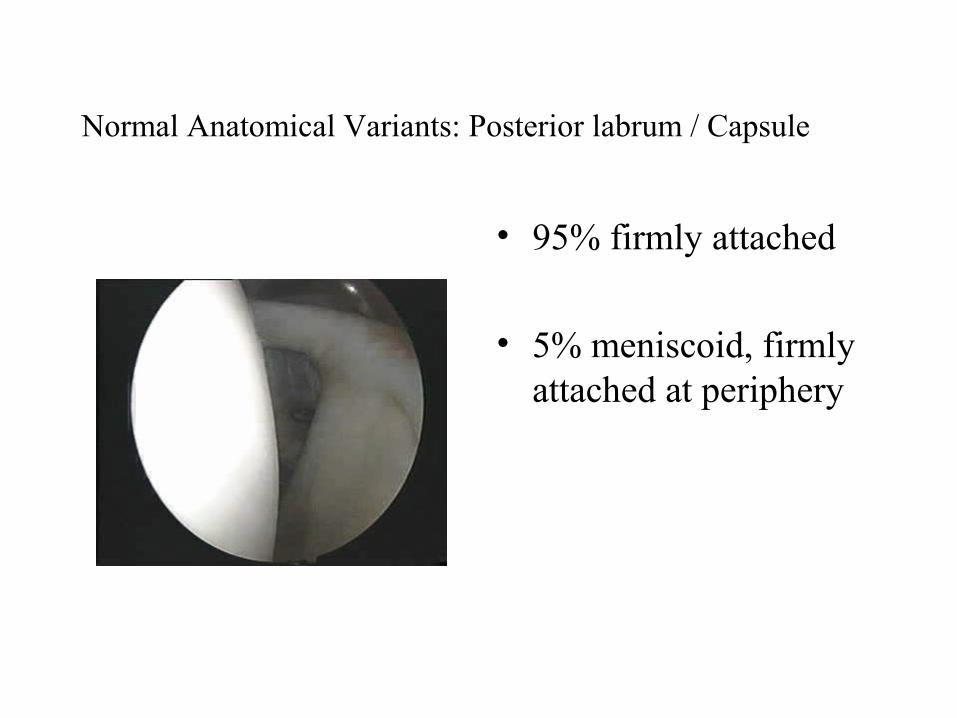
Normal Anatomical Variants: Posterior labrum / Capsule
• 95% firmly attached
• 5% meniscoid, firmly attached at periphery
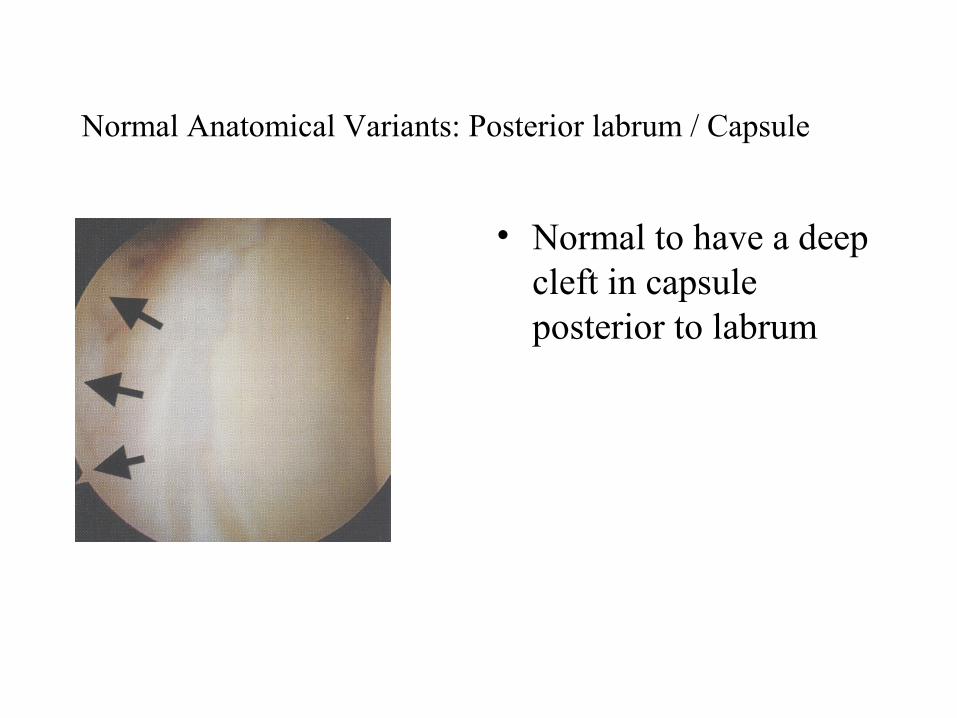
Normal Anatomical Variants: Posterior labrum / Capsule
• Normal to have a deep cleft in capsule posterior to labrum

Thank you