
NHSScotland Event 2015 LEADING INTEGRATION FOR QUALITY B:3 Finding Out What Matters When Time...
37
NHSScotland Event 2015 LEADING INTEGRATION FOR QUALITY B:3 Finding Out What Matters When Time Becomes Short
-
Upload
jonah-nicholson -
Category
Documents
-
view
213 -
download
0
Transcript of NHSScotland Event 2015 LEADING INTEGRATION FOR QUALITY B:3 Finding Out What Matters When Time...

NHSScotland Event 2015 LEADING INTEGRATION FOR QUALITY
B:3 Finding Out What Matters When Time Becomes Short
What can be done to identify people who may be in their last year of life in primary or secondary care?
• 1 = Clinical Judgement• 2 = SPICT• 3 = Patient and Family Request• 4 = Palliative Performance Scale• 5 = Surprise Question

Talking about ‘What Matters’

“Whatever the setting, care will be provided to the highest standards of quality and safety, with the person at the centre of all decisions.”
2020 Vision
Dr Kirsty BoydConsultant in Palliative Medicine, NHS Lothian
Honorary Clinical Senior LecturerThe University of Edinburgh
Dr Belinda HackingHead of Psychology Service for LD, Health,
Forensic, Neuropsychology and Older AdultsNHS Lothian
Talking about ‘What Matters’

Deteriorating Health
Deteriorating & ‘dying well’
Time
Best Supportive Care & Palliative Care
Living with progressive multimorbidity
Functional status
Talking about ‘What Matters’
‘Living well’ with long term conditions
Deteriorating Health
Deteriorating & ‘dying well’
Time
Best Supportive Care & Palliative Care
• All patients with advanced illnesses• All settings – home, hospital, care home• All around the world
• General indicators• Condition related indicators• Support for assessment and planning• Prompts talking about ‘What Matters’
• Online + Print + App
www.spict.org.uk
Supportive & Palliative Care Indicators Tool
Does an increased frequency of discussions about CPR improve the experiences of
patient, families & staff?
• 1 = Yes• 2 = No • 3 = Don’t know

• Hoping
• Coping
• Not ‘planning for dying’
Patient: “I’ve never broached the subject (of dying) cause I think like I’d rather be positive. I think “I’m not going to get worse.” (Female, 66: Liver failure, diabetes, IHD)
Carer: ‘We deal with everything just as it is happening, just day to day stuff and things. We just manage.’ (Carer for male, 87: renal failure, diverticular disease, mild dementia, prostate cancer,)
Patient: ‘I’m not afraid to die but I want to live’ (Female, 79: stage IV heart failure, renal failure)
Mason B et al. BMJ Supportive Palliative Care 2014;0:1–6. doi:10.1136/bmjspcare-2013-000639
Talking about ‘What Matters’ in advanced illness
‘It could be another year or two or a week or two, who knows…..but he’s obviously not terminal yet.’ GP

• Hoping
• Coping
• Planning
“I was worried I was going to be put on the dying pathway… I'm glad to be feeling better and I don’t want to think more about the future right now”
Patient
The doctor hedged around… it took a while til’ I saw what she was getting at and put her out of her misery.
Patient
Every time I'm asked, I have to go through and re-live it over again.. do they know how
that feels? Carer
‘What Matters’ in the last weeks to days of life
“These are not the kind of discussions for when you’re really not well” Patient
• Talking about ‘trying’ or ‘the chances’ if a treatment will not work , have a very poor outcome or not meet personal goals
directs people to ‘want everything done’.• Use of older terms, such as ‘futile’, ‘ treatment limitation’ or
’ceiling of treatment/care’risks making people think ‘nothing will be done for them’ or care will
be ‘rationed’.• Moving on to discussing treatment options and planning care
before understanding people’s goals and prioritiesmeans people cannot formulate meaningful goals due to lack of
a realistic understanding of their situation.
Talking about ‘What Matters’Getting the balance right

www.ec4h.org.uk


What do you know?
What are you expecting?
What’s happening?
What matters?
What would help?
Future Care PlanningAdvance care planning‘When and if’ plans
Anticipatory care planning‘What to do if’ plans
Final days of life planning‘What matters now’ plans
Plan the discussion• Urgency• Capacity• Key people• Understanding/ readiness (prognostic awareness)
Talking about ‘What Matters’
What we could do is..

Effective conversations about What Matters’
• Generalisation• Sometimes people choose a family member or a close friend to
make decisions for them if they get less well in the future. • Hypothetical questions
• If you were less well again like this in the future what do you think we should do?
• Hope linked with concern• We hope the (treatment) will help, but I am worried that at some
stage, maybe even soon, you will not get better…. What do you think?
• Accept uncertainty, change and diverse views• Can we talk about what is most important for you now,
and how we might cope with not knowing exactly what will happen and when?

What would help us most with having good discussions about deteriorating health, death and dying?A. Better public education and informationB. Cultural change in all care settings to give more
priority to quality of life not just mortality reduction
C. Staff support and training in shared-decision making and effective communication
D. Making conversations about patient goals and future care planning a part of routine care
E. More access to specialist palliative care services

Talking about ‘What Matters’
It is much more important to know what sort of patient has a disease than what sort of diseases a patient has.’
‘Medicine is a science of uncertainty and an art of probability.’
Sir William Osler

Finding out what matters when time is short… in Acute Medical and Surgical Units
Professor D. Robin TaylorConsultant Respiratory Physician,
NHS LanarkshireHonorary Fellow, Faculty of Medicine,
University of Edinburgh

Time
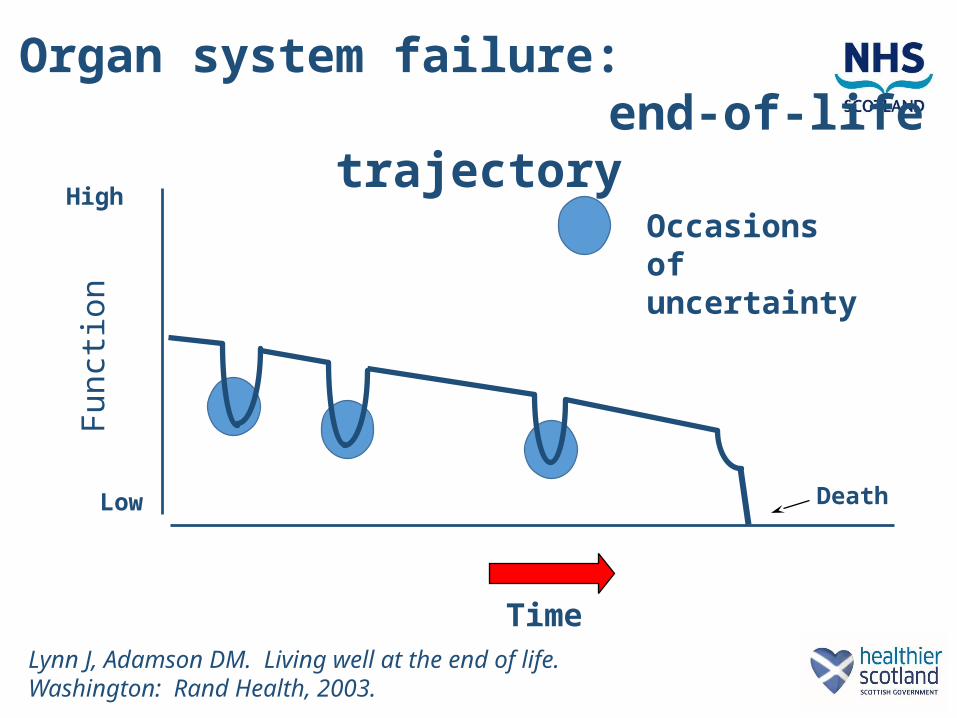
Organ system failure: end-of-life trajectory
Fun
ctio
n
High
Low Death
Acute on chronic deterioration
Lynn J, Adamson DM. Living well at the end of life. Washington: Rand Health, 2003.
Time
Organ system failure: end-of-life trajectory
Occasions of uncertainty
Fun
ctio
n
High
Low Death
Lynn J, Adamson DM. Living well at the end of life. Washington: Rand Health, 2003.
Time
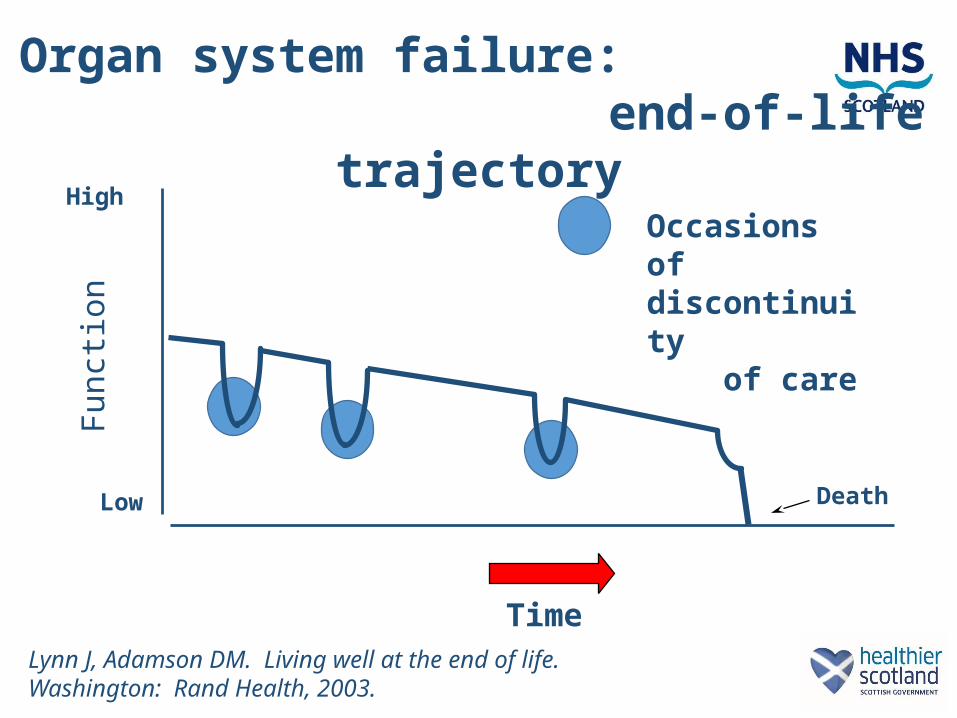
Organ system failure: end-of-life trajectory
Occasions of discontinuity of care
Fun
ctio
n
High
Low Death
Lynn J, Adamson DM. Living well at the end of life. Washington: Rand Health, 2003.

• Male, 78 years, end-stage COPD
• Several admissions for AECOPD over the previous year.
• Admitted with bronchopneumonia and Type 2 respiratory failure.
• End of life conversation with the patient and his family, at 4pm. Acknowledged to be terminally ill.
• Agreed that medical treatment would be limited to oxygen, fluids, haloperidol and morphine. This was documented.
• At 3 a.m. next morning, nursing staff noted the patient to be more breathless. In response, the on-call registrar commenced non-invasive ventilation (NIV) and aminophylline.
• Patient died on BiPAP 4 hours later. Family very angry.
Case study

Hiding behind uncertainty
We deal with the present and ignore the future
Limited treatment aims: to achieve a modified recovery from acute event
Relief for the clinician: prognostic truth-telling is avoided
Reprieve for the patient: perpetuation of illusions of recovery

Wrestling with discontinuity
of care
What is urgent is dealt with in isolation: the CONTEXT of an acute event is neglected
Risk versus benefit analysis is skewed: the risks of NOT intervening motivate inappropriate decision making and treatment
Default interventions are protocol-driven and indiscriminate

Scottish Public Service Ombudsman Report, 201400643 May 20, 2015
“Significantly, there was evidence of confusion between staff about whether Mr. X was being provided with active or end of life care”

Dying without dignity Parliamentary and Health Ombudsman Report (England), May 20, 2015
Not recognising that people are dying and not responding to their needs
Poor symptom controlPoor communicationInadequate services out of hours Poor care planningDelays in diagnosis and referrals for
treatment

End of life care
Palliative treatments
Anticipatory Care Plan
Treatment Escalation / Limitatione.g. Ceiling of Treatment

Hospital Anticipatory Care Plan:“Ceiling of Treatment”
These things matter (1)• To minimise harm by avoiding both
over-treatment and under-treatment
• To minimise harm caused by discontinuity of care

Hospital Anticipatory Care Plan:“Ceiling of Treatment”
These things matter (2)To prompt and encourage review of
treatments which may be potentially futile, burdensome and contrary to the patient’s wishes
To prompt and encourage good communication with patients about the levels of treatment that are appropriate

Hospital Anticipatory Care Plan:“Ceiling of Treatment”
These things matter (3)In the event of deterioration occurring in an
alreadyill patient …to provide guidance as to when and/or how
to escalate treatment or limit further medical interventions
to provide for improved communication between medical and nursing staff so that they may respond appropriately and consistently.

Ceiling of Treatment: ethics
Futile orBurdensome and/orContrary to the patient’s wishes

Ceiling of Treatment: ethics
Futile orBurdensome and/orContrary to the patient’s wishes
UNETHICAL

HACP / C of T: pro forma 3
ROUTINE BLOODS YES / NO OPERATION YES / NOIV FLUIDS YES / NO ANTIBIOTICS YES / NO BLOOD TRANSFUSION YES / NO TRANSFER TO HDU / ITU / CCU YES / NO INVASIVE PROCEDURES: CPR IN THE EVENT OF ARREST YES*/ NOInterventional radiology YES / NO Endoscopy YES / NOCentral line YES / NO OTHER (state) ……………………… YES / NO Arterial line YES / NOArterial puncture YES / NO *A standard DNACPR form should still be completed. This form is not a replacement even although
reference to CPR is made.

HACP / CofT: pro forma 4
The specific details of this plan should ideally be discussed with the patient (see Note 3 below), or when this is not possible, with the patient’s family /designated other support person. This discussion should be clearly documented separately in the patient’s hospital record. Has been discussed with the patient: YES NOT POSSIBLE Name of family member / designated other whom this has been communicated with: ……………………………………………………………………………Person completing this document ……………………………… (Signature) ……………… (Print Capitals) ……………………………… (Position) ………… (Date)………… (Time) Authorised by (consultant responsible) ……………………………..……… (Sign and date) ………………
• • • • • • • • • •

Hospital Anticipatory Care Plan:“Ceiling of Treatment”
These things matter (4):
Common sense Compassion Communication

Hospital Anticipatory Care Plan:“Ceiling of Treatment”
8 versions: Advanced Malignancy, Cardiology, Frailty in Gen. Med., Liver Disease, Orthopaedics, Renal, Respiratory, Surgery.
In WGH: all versions now available in medical, surgical and orthopaedic wards, ECU and HDU.
In Hairmyres: A and E, Surgery, Respiratory
In Monklands: C of E, Respiratory, ID, Renal. Training for nursing staff (n=80) and FY1s (n=20),
continuing MCN Pall. Care Focus Group input (Univ. of Stirling)C of T included in DNACPR training for FY1 and FY2Aim to include C of T in all introductory and induction
courses for FY1s and nurses.

I have had a personal experience of attending / caring for an elderly relative with a chronic progressive condition e.g. heart failure, COPD, and the prognosis was thought about and discussed during the last 12 months of life. • 1 = I have not had that experience• 2 = I have had that experience and prognosis WAS
NOT meaningfully discussed at any time• 3 = I have had that experience and prognosis WAS
meaningfully discussed but only during the terminal phase
• 4 = I have had that experience and prognosis WAS meaningfully discussed at an appropriate time

In either a professional OR a personal capacity, I have experienced a situation in which the absence of a treatment escalation / limitation plan has contributed adversely to patient care. • 1 = no, never • 2 = yes, once only or once in a while • 3 = yes, quite frequently


















