
NHHC chapter 22 ppt
54
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014 Nutrition and Renal Diseases Chapter 22
-
Upload
kellygcdet -
Category
Education
-
view
358 -
download
3
Transcript of NHHC chapter 22 ppt

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Nutrition andRenal Diseases
Chapter 22

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Introduction
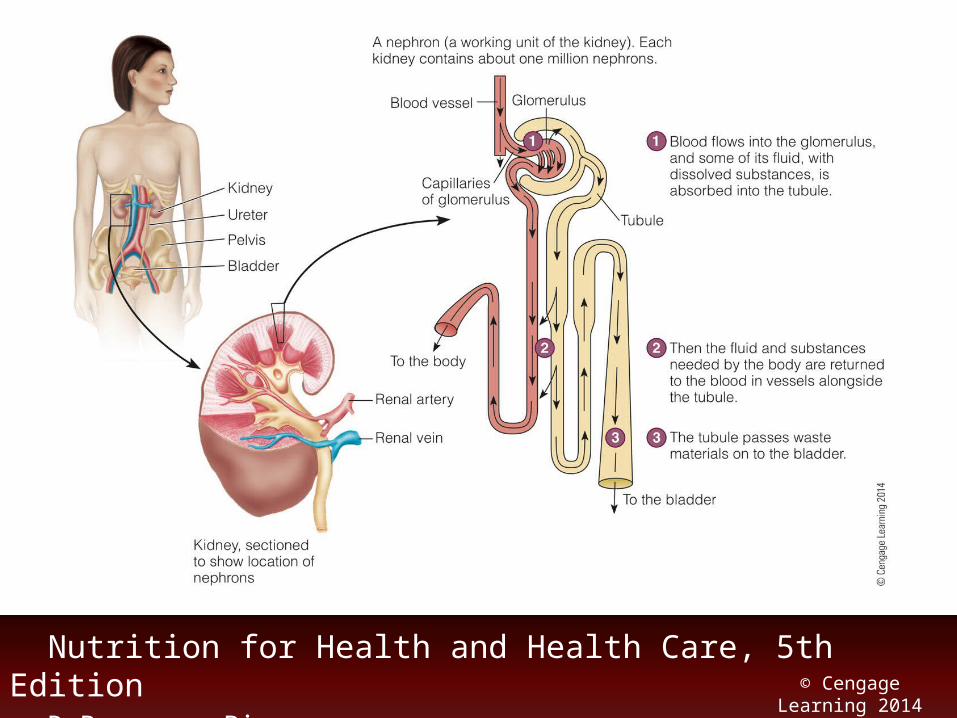
• Kidneys– Filter the blood and remove excess fluid and
wastes for elimination in urine– Nephron: working unit of the kidney
• Glomerulus: filters water and solutes from the blood
• Bowman’s capsule: surrounds the glomerulus; collects the filtrate that is passed to the tubules
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Introduction (cont’d.)
• Kidneys– Regulate the extracellular fluid volume
• Control osmolarity, electrolyte concentrations, and acid-base balance
– Excrete metabolic waste products• Urea and creatinine; various drugs and toxins
– Other roles• Secretes renin, produces erythropoietin, and
converts vitamin D to active form
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
The Nephrotic Syndrome
• Disorders causing severe glomerular damage: significant proteinuria– Damage to glomeruli
• Increases permeability to plasma proteins
• Causes– Glomerular disorders, diabetic nephropathy,
immunological and hereditary diseases, infections (kidneys or other), etc.

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
The Nephrotic Syndrome (cont’d.)
• Consequences of the nephrotic syndrome– Attempting to compensate: liver increases
synthesis of various plasma proteins • Some or the proteins produced in excess
– Edema• Hypoalbuminemia: contributes to a fluid shift
from blood plasma to the interstitial spaces • Impaired sodium excretion: sodium and water
retention

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
The Nephrotic Syndrome (cont’d.)
• Consequences of the nephrotic syndrome– Blood lipid abnormalities
• Elevated levels of LDL, VLDL, and lipoprotein(a)– Blood clotting abnormalities
• Increased risk of deep vein thrombosis– Other effects
• Susceptibility to infection; increased risk of rickets (children); PEM and muscle wasting

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
The Nephrotic Syndrome (cont’d.)
• Treatment of the nephrotic syndrome– Requires diagnosis and management of the
underlying disorder– Medications for complications
• Diuretics, ACE inhibitors, lipid-lowering drugs, anti-inflammatory drugs, and immunosuppressants
– Nutrition therapy• Helps to prevent PEM, correct lipid abnormalities,
and alleviate edema

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
The Nephrotic Syndrome (cont’d.)
• Nutrition therapy– Protein and energy
• Adequate to meet needs: helps minimize muscle tissue losses
• Why are high-protein diets not advised?– Lipids
• Dietary measures: usually inadequate for controlling blood lipids
• Lipid-lowering medications: usually prescribed

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
The Nephrotic Syndrome (cont’d.)
• Nutrition therapy– Sodium and potassium
• Low-sodium: helps control edema (Table 22-1)• Foods rich in potassium encouraged
– Vitamins and minerals• Supplements help patients avoid nutrient
deficiencies: particularly vitamin B6, vitamin B12, folate, iron, copper, and zinc

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
The Nephrotic Syndrome (cont’d.)
• Nutrition therapy– Vitamins and minerals
• Calcium and vitamin D supplements also advised

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury
• Kidney function deteriorates rapidly, over hours or days– Reduced urine output and build-up of
nitrogenous wastes in blood• Causes of acute kidney injury
– Consequence of severe illness, injury, or surgery

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Causes of acute kidney injury– Prerenal factors: cause a sudden reduction in
blood flow to the kidneys• Often involve a severe stressor such as heart
failure, shock, or blood loss– Intrarenal causes: factors that damage kidney
tissue• Infections, toxicants, drugs, or direct trauma

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Causes of acute kidney injury– Postrenal factors: prevent excretion of urine
due to urinary tract obstructions

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Consequences of acute kidney injury– Altered composition of blood and urine
• Kidneys unable to regulate levels of electrolytes, acid, and nitrogenous wastes in the blood
• Conditions of oliguria or anuria– Fluid and electrolyte imbalances
• Sodium retention: edema• Hyperkalemia: alters heart rhythm; heart failure• Hyperphosphatemia: leads to bone calcium losses
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Consequences of acute kidney injury– Uremia
• Nitrogen-containing compounds and various other waste products: may accumulate in the blood
– Uremic syndrome: cluster of disorders • Impairments in multiple body systems

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Treatment of acute kidney injury– Combination of drug therapy, dialysis, and
nutrition therapy • Restore fluid and electrolyte balances• Minimize blood concentrations of toxic waste
products

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Treatment of acute kidney injury– Drug treatment in acute kidney injury
• Why may it be necessary to lower doses of some usual medications, while others may need to be increased?
• Nephrotoxic drugs: must be avoided until kidney function improves

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Treatment of acute kidney injury– Drugs for acute kidney injury: depend on
cause of illness and complications• Immunosuppressants: inflammatory conditions• Diuretics: edema• Hyperalkalemia: potassium-exchange resins; may
require insulin• Other medications

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Treatment of acute kidney injury– Energy and protein
• Sufficient energy and protein: preserve muscle mass
• Protein recommendations : influenced by kidney function, degree of catabolism, and use of dialysis

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Treatment of acute kidney injury– Fluids
• Estimate needs: measure urine output and add 500 milliliters for water lost from skin, lungs, and perspiration
– Electrolytes• Serum electrolyte levels monitored closely:
determine appropriate electrolyte intakes

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Acute Kidney Injury (cont’d.)
• Treatment of acute kidney injury– Enteral and parenteral nutrition
• In cases requiring additional nutritional support, why is enteral support preferred over parenteral nutrition?
– Case Study – Woman with Acute Kidney Injury

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease
• Gradual, irreversible deterioration• Kidneys: large functional reserve
– Chronic disease typically progresses over many years without causing symptoms
• Most common causes– Diabetes mellitus and hypertension– What are other causes of chronic kidney
disease?

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Consequences of chronic kidney disease– Early stages
• Nephrons compensate by enlarging to handle the extra workload
– End-stage renal disease• Advanced stage of chronic kidney disease: dialysis
or a kidney transplant is needed to sustain life– Many symptoms: nonspecific
• Delays diagnosis of the condition

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Assessing kidney function– Glomerular filtration rate (GFR)
• Rate at which the kidneys form filtrate• Estimated using predictive equations: based on
serum creatinine levels, age, gender, race, and body size
• Categorized into stages (Table 22-4)– What other tests can assess kidney function?
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Altered electrolytes and hormones– As GFR falls:
• Remaining neurons increase activity to maintain electrolyte excretion
– Electrolyte disturbances• May not develop until third or fourth stage of
chronic kidney disease
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Altered electrolytes and hormones– Some hormonal adaptations to regulate
electrolyte levels create new complications• Increased aldosterone ► hypertension• Parathyroid hormone ► renal osteodystrophy
• Clinical effects of uremic syndrome– Hormonal imbalances
• Lead to anemia, bone disease, etc.

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Clinical effects of uremic syndrome– Altered heart function/increased heart disease
risk– Neuromuscular disturbances
• Malaise, irritability, sensory deficits, seizures, etc.– Other effects
• Defects in platelet function and clotting factors; increased skin pigmentation and severe pruritus; suppressed immune responses

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Protein-energy malnutrition– Anorexia: contributes to the poor food intake
• Due to hormonal disturbances, nausea and vomiting, restrictive diets, uremia, and medications
– Nutrient losses• Consequence of vomiting, diarrhea,
gastrointestinal bleeding, and dialysis– Catabolic state
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Treatment of chronic kidney disease– Treatment goals
• Slow disease progression• Prevent or alleviate symptoms
– Drug therapy for chronic kidney disease• Antihypertensive drugs• Erythropoietin (epoetin): anemia• Others: phosphate binders, sodium bicarbonate,
and active vitamin D

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Treatment of chronic kidney disease– Dialysis: removes excess fluid and wastes
from the blood• Hemodialysis: blood is circulated through a
dialyzer– Nutrition therapy for chronic kidney disease
(Table 22-5)
Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy for chronic kidney disease– Energy: adequate intake to maintain a healthy
weight and prevent wasting– “How To” Increase kCalories and Protein in
Meals (Chapter 23)– Protein: enough protein to meet needs and
prevent wasting• Between 0.6 and 0.8 g/kg of body weight per day in
later stages

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy for chronic kidney disease– Lipids: restrict intakes of saturated fat, trans
fat, and cholesterol• Why are persons with chronic kidney disease often
encouraged to consume high-fat foods?– Sodium and fluids
• Mild sodium restriction may be beneficial• Fluids: not restricted until urine output decreases• What water intake restrictions apply during dialysis?

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy for chronic kidney disease– Potassium
• Early stages: normal potassium intake levels• Hyperkalemia conditions: potassium restrictions• Potassium-diuretics: potassium supplementation• Dialysis patients: control potassium intake (Table
22-6)

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy for chronic kidney disease– Phosphorus, calcium, and vitamin D
• Serum phosphorus and calcium levels: monitored in kidney disease patients
• Elevated phosphorus levels: restrict intake• What accounts for the risk of hypercalcemia?• Vitamin D supplements

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy for chronic kidney disease– Vitamins and minerals
• Multivitamin supplements: typically recommended for all patients with chronic kidney disease
• Limit vitamin C: 100 milligrams per day• Vitamin A supplements: not recommended• Hemodialysis patients: intravenous iron along with
erythropoietin therapy

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy for chronic kidney disease– Enteral and parenteral nutrition
• Formulas: more kcalorically dense and lower protein and electrolyte concentrations than standard formulas
• What is intradialytic parenteral nutrition?

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy for chronic kidney disease– Diet compliance: difficult aspect of treatment
(Table 22-8)– Case Study – Man with Chronic Kidney
Disease

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Kidney transplants– Benefits
• Restores kidney function, allows a more liberal diet, and frees the patient from routine dialysis
– What are barriers to kidney transplants?– Immunosuppressive drug therapy
• Prevent tissue rejection following transplant surgery
• Be aware of diet-drug interactions (listed in text)

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Chronic Kidney Disease (cont’d.)
• Nutrition therapy after kidney transplant– Most nutrients
• Consume at levels recommended for the general population
– Primary reason for dietary adjustments• Side effects of drugs

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones
• Crystalline mass– Forms within the urinary tract
• Formation of kidney stones– Stone constituents become concentrated in
urine• Allowing crystals to form and grow
– Most common constituent• Calcium oxalate

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Factors predisposing an individual to stone formation– Dehydration or low urine volume– Obstruction– Urine acidity– Metabolic factors– Renal disease

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Types of kidney stones– Calcium oxalate stones
• Hypercalciuria: common abnormality in people with calcium oxalate stones
– Uric acid stones• Urine: abnormally acidic; contains excessive uric
acid, or both• Frequently associated with gout

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Types of kidney stones– Cystine and struvite stones
• Cystine stones: people with inherited disorder cystinuria
• Struvite stones: composed primarily of magnesium ammonium phosphate; form in alkaline urine

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Consequences of kidney stones– Renal colic
• Severe, stabbing pain when stone passes through the ureter
• Hematuria: blood in urine– Urinary tract complications
• Urination urgency, frequent urination, or inability to urinate
• Urinary tract obstruction, and possibly infection

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Prevention and treatment of kidney stones– Drink 12 to 16 cups of fluids daily
• Maintain urine volumes of at least 2½ liters per day– Calcium oxalate stones
• Reduce urinary calcium and oxalate levels• Adjust calcium, oxalate, protein, and sodium
intakes• Medications: diuretics; drugs to inhibit crystal
formation; and drugs to reduce uric acid production

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Prevention and treatment of kidney stones– Uric acid stones
• Diets restricted in purines: may help to control urinary uric acid levels
• Drug treatments: allopurinol to reduce uric acid levels and potassium citrate to reduce urine acidity

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Prevention and treatment of kidney stones– Cystine and struvite stones
• High fluid intakes• Medications may be needed• What is a central strategy in preventing struvite
stones?

Nutrition for Health and Health Care, 5th Edition DeBruyne ■ Pinna © Cengage Learning 2014
Kidney Stones (cont’d.)
• Medical treatment for kidney stones– Medications
• Relax ureter• Increase urine flow
– Extracorporeal shock wave lithotripsy• High-amplitude sound waves to degrade the stone
– Surgical methods• Higher success rate• More invasive


















