Newborn Screening 50th Year Celebration: the Utah experience · PROP BKT. Newborn Screening in ......
33
Newborn Screening 50 th Year Celebration: the Utah experience Marzia Pasquali PhD FACMG Professor of Pathology and Pediatrics Medical Director, Biochemical Genetics and Newborn Screening University of Utah and ARUP Laboratories 17 October 2013
-
Upload
trinhkhanh -
Category
Documents
-
view
216 -
download
0
Transcript of Newborn Screening 50th Year Celebration: the Utah experience · PROP BKT. Newborn Screening in ......
Newborn Screening 50th Year Celebration: the Utah experience
Marzia Pasquali PhD FACMG
Professor of Pathology and Pediatrics Medical Director, Biochemical Genetics and Newborn Screening
University of Utah and ARUP Laboratories
17 October 2013
Newborn screening
Public health activity aimed at the early identification of
conditions for which timely intervention can lead to the
elimination or reduction of mortality, morbidity, and
disabilities associated with these conditions.

History of Newborn Screening
1961 Dr. Robert Guthrie (New York) • First to use dried blood spot sample (often referred to
as a Guthrie card)
• Developed Bacterial Inhibition Assay (BIA) to detect
elevated levels of phenylalanine in dried blood spots
• Blood spots are placed on agar media containing B.
subtilis spores and a chemical inhibitor
• Spores can not grow unless phenylalanine is present
• Measure diameter of bacterial growth around blood
spot and compare to growth around blood spots
enriched with known amounts of phenylalanine (semi-
quantitative)

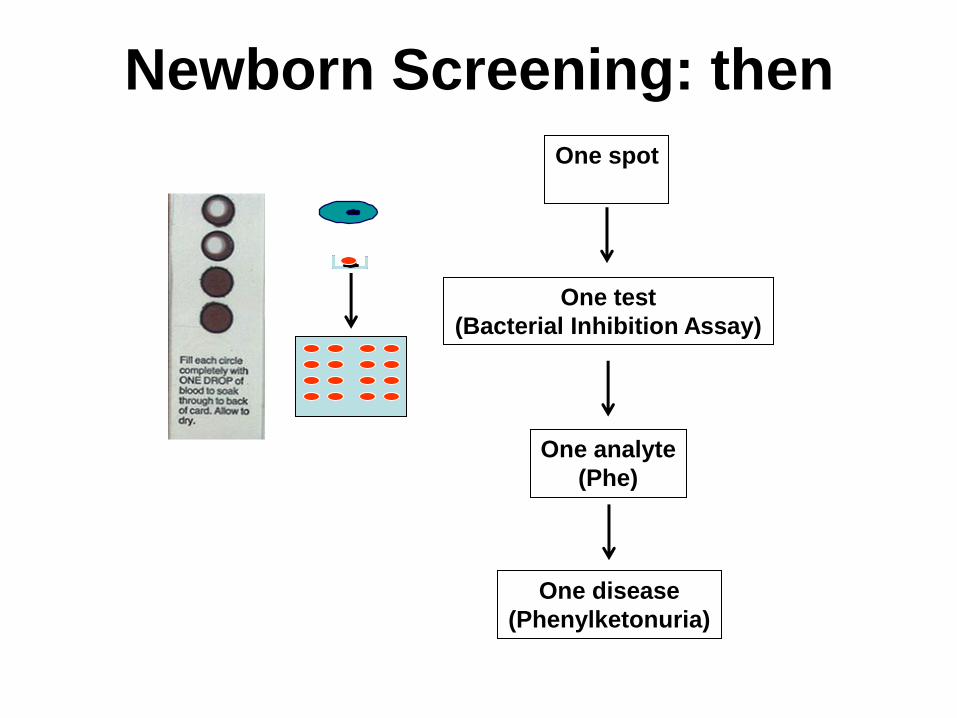
Newborn Screening: then
One analyte
(Phe)
One test
(Bacterial Inhibition Assay)
One disease
(Phenylketonuria)
One spot

Tandem Mass Spectrometry
• MS/MS can test
a number of
metabolites
simultaneously,
rather than one
analyte at a time
as in classic
screening
procedures.

Newborn Screening: now
Multiple analytes
Many diseases
487.47 1485440
459.40 1444288
437.33 756800 288.29
745216 403.21 702080
375.34 479104 347.35
450416 313.37 426912
298.43 346880
319.24 403520
347.04 311184
347.48 392144
347.86 105628
400.44 170080
376.23 123656
426.23 209408 404.10
161568
437.58 666432
438.40 253632
454.42 134736
460.22 481056
482.55 268048
461.36 111876
488.41 552960
577.46 166384
489.48 165424
549.59 108612 513.07
90616 523.35 50356
One test
(MS/MS)
One spot

MS/MS analysis Two main classes of metabolites can be detected using
tandem mass spectrometry (MS/MS):
– Amino acids. The level of one
or more amino acids increases in disorders of amino acid metabolism (metabolic block close to the actual amino acid).
– Aminoacidopathies and Urea Cycle defects: • Phenylketonuria, Maple
Syrup Urine Disease, Homocystinuria, Citrullinemia, Argininosuccinic aciduria, Tyrosinemia Type I
– Acylcarnitines. In disorders of the intermediary metabolism of amino acids or of fatty acid oxidation the abnormal metabolites are conjugated with carnitine to facilitate their excretion and to balance the Coenzyme A pool.
– Organic acidemias and fatty acid oxidation defects: • Glutaric acidemia Type I,
Propionic acidemia, Methylmalonic acidemia
• MCADD, VLCADD, CUD, CPT-I and CPT-II deficiencies.

Secretary Advisory Committee on Heritable
Disorders and Genetic Diseases in Newborns and
Children TANDEM MASS SPECTROMETRY
(MS/MS)
Traditional methods
(EIA, HPLC,etc.)
OTHERS
Acylcarnitines Amino acids
FAO (5) OA (9) AA (6) Hematology (3) Others (5)
MCAD IVA PKU Hb SS CH SCID
VLCAD GA-1 MSUD Hb S/bThal BIOT HEAR
LCHAD HMG HCY Hb S/C CAH CCHD
Critical congenital
heart disease
TFP MCD TYR I GALT Pompe
CUD MUT ASA CF
Cbl A,B CIT
3MCC
PROP
BKT
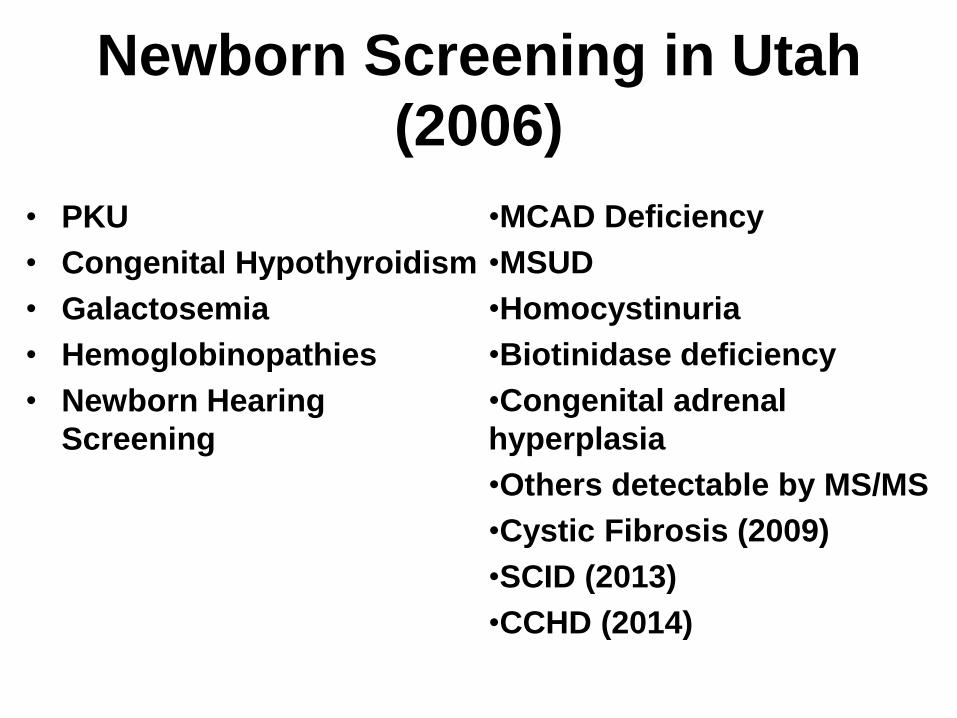
Newborn Screening in Utah
(2006)
• PKU
• Congenital Hypothyroidism
• Galactosemia
• Hemoglobinopathies
• Newborn Hearing
Screening
•MCAD Deficiency
•MSUD
•Homocystinuria
•Biotinidase deficiency
•Congenital adrenal
hyperplasia
•Others detectable by MS/MS
•Cystic Fibrosis (2009)
•SCID (2013)
•CCHD (2014)
Utah’s unique partnership
• A Pilot Project (2003-2005) was
established with the purpose of:
Evaluating the feasibility of expanding
newborn screening in Utah with a
private-public partnership involving the
Department of Health, ARUP
Biochemical Genetics laboratory, and
the Metabolic Center/Medical Genetics
at the University of Utah.

Pilot Project: Study Design (1)
• This study was approved by the Institutional
Review Board of the University of Utah (IRB_00011072, Supplemental Newborn Screening for the Early Diagnosis of Inborn Errors of Metabolism in Utah).
• Facility: University of Utah hospital (3,000-4,000 births per year)
• Subjects: Infants born at the U of U hospital (neonatal intensive care unit babies were excluded). Mothers had to sign a consent form.

Filter paper
Pilot Project: Study Design (2)
MS/MS
DoH

Nu
mb
er
of
ba
bie
s
0
1000
2000
3000
Total births
Pilot project
Oct 03-Dec 03 Jan 04-Sep 04 Oct 03-Sep'04
30%
68%
91%
Pilot Project: Participation
Oct 03-Dec 03 Jan 04-Sept 04 Oct 05-Sept 05
• 4,827 first screen and 690 second
screen samples were analyzed
– 1.7% first screen and 0.6% second screen
needed follow-up
– 0.1% needed confirmatory testing
– 1 infant with Glutaric acidemia type I was
identified and treated
Pilot Project: Results
Pilot Project: Conclusions
• Integration of private and public resources allows the prompt identification and treatment of children with metabolic disorders.
• Bidirectional data exchange between the State and the testing laboratory is necessary for good turnaround time.
• Education of health care professional and of the community is of paramount importance for a successful implementation of a new program.

UTAH Newborn Screening Program
The efficiency and effectiveness of a newborn screening program is dependent upon the smooth integration of sample collection, laboratory testing, follow-up, diagnosis, timely
treatment, and tracking of outcomes.
Follow-up
Clinical care Education
Evaluation
Medical Home
MS/MS screening in Utah: 2006-2013
• Total screens: 416,557
– Total metabolic disorders: 188 1:2,216
– Total maternal cases: 24
• PKU/Hyperphe/Biopt
• MCAD deficiency
• 3-Methylcrotonylglycinuria
• VLCAD deficiency
• Glutaric acidemia type I
• Primary carnitine deficiency (CUD)
• LCHAD deficiency

Thank You
• ARUP
– Newborn Screening and Biochemical Genetics Laboratories
– Dr. N. Kusukawa
– Dr. C. Kjeldsberg
• Utah Department of Health
– Kim Hart, Dr. H. Randall, Dr. R. Atkinson, N. Brown
– Fay Keune, Dr. F. Tait
• University of Utah Metabolic Clinic
– Dr. N. Longo, Dr. L. Botto, Dr. A. Warnock, S. Ernst, Krista
Viau
SCID Newborn Screening in Utah
Patricia Slev, PhD, D(ABCC)
Medical Director, Serologic Hepatitis and Retrovirus Laboratory
Co-Director, Immunogenetics Laboratory
Assistant Professor of Pathology,
University of Utah, School of Medicine

Timeline
• 2010 Uniform Panel Recommendation
• 2011 Utah SCID Subcommittee
Parent Advocate, March of Dimes, Pediatric Immunology, Pediatric
Bone Marrow Transplant Division
• 2012 Utah Genetics Advisory Committee and Newborn Screening
Subcommittee recommend screening for SCID
• 2013 Governor approves kit fee increase
• 2013 Pilot
• 2013 Implementation (July)
Why Screen ?
• Fatal without treatment
• Asymptomatic at birth
• Effective Treatment
hematopoietic stem cell transplant (HSCT)
enzyme replacement
gene therapy
• Early intervention is key
<3 months = 95% survival
>3 months = 65% survival
March of Dimes
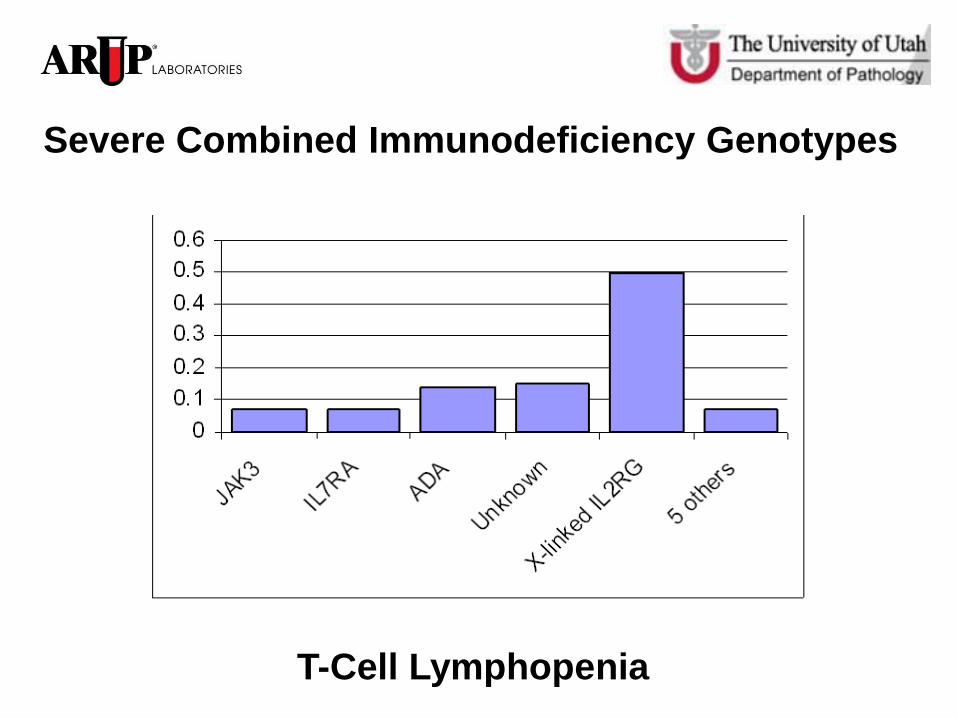
Severe Combined Immunodeficiency Genotypes
T-Cell Lymphopenia
• Marker/Target – T-cell Receptor Excision Circle (TREC)
Circular, episomal, DNA fragment formed as a byproduct of successful
T-cell receptor rearrangement, during maturation in the thymus
TREC do not replicate with mitosis and therefore are diluted with
cell division
Peripheral concentrations correlate with T-cell production in the
thymus
Marker for T- cell lymphopenia not SCID
• Assay
Real-time PCR
Reported cut-offs and concentrations vary by laboratory due to
differences in reagents, calibrators and instrumentation
TREC Assay for SCID

Retrospective Utah Pilot Study
• 4,999 dried blood samples (DBS)
4,665 non- NICU
344 NICU
• TREC Singleplex Assay
TREC concentrations
b -actin concentrations
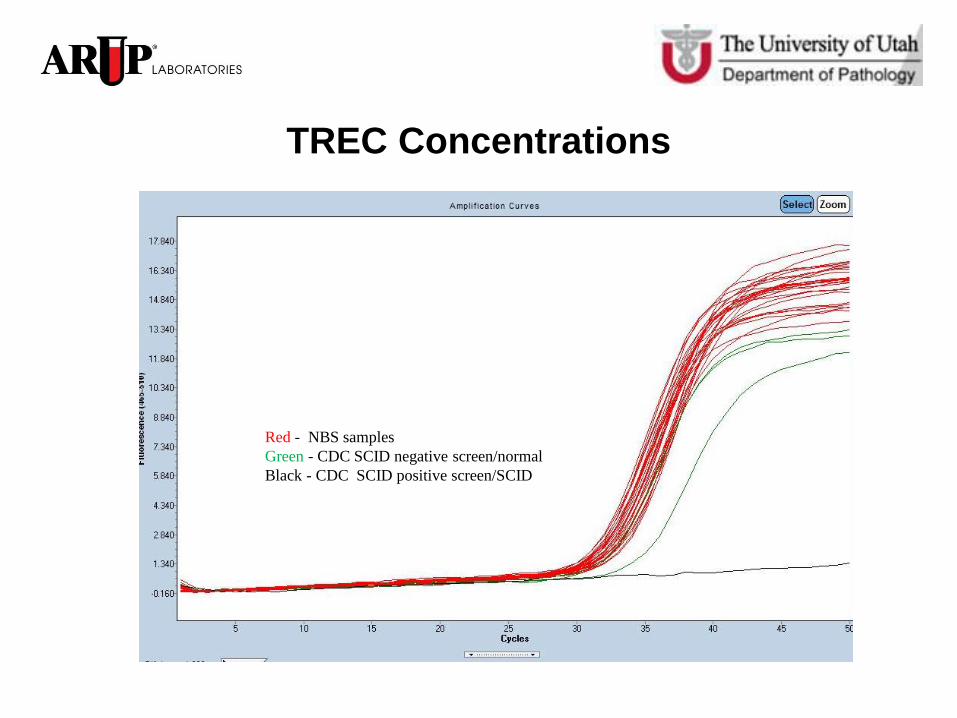
TREC Concentrations
Red - NBS samples
Green - CDC SCID negative screen/normal
Black - CDC SCID positive screen/SCID

Reference Gene Concentrations
(b -actin)
Red - NBS samples
Green - CDC SCID negative screen/normal
Black - CDC SCID positive screen/SCID

Pilot Study Results
0
100
200
300
400
500
600
Sa
mp
le n
um
bers
TREC concentration (copies/µl whole blood)
TREC concentration distribution in healthy and NICU babies
Healthy babies frequency
NICU babies frequency
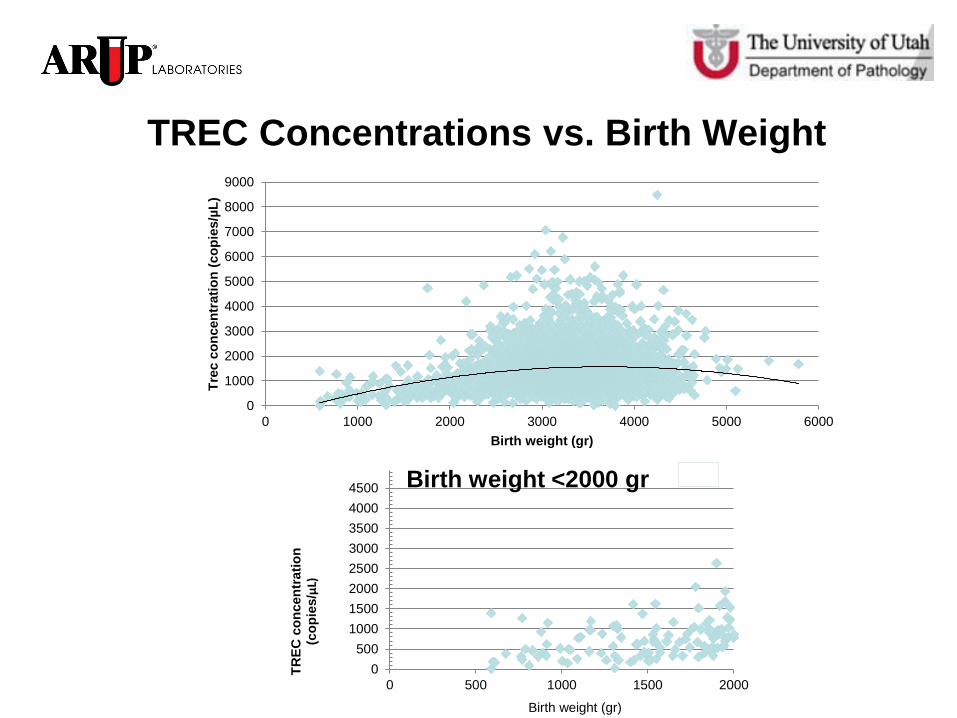
TREC Concentrations vs. Birth Weight
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
0 1000 2000 3000 4000 5000 6000
Tre
c c
on
cen
trati
on
(co
pie
s/µ
L)
Birth weight (gr)
0
500
1000
1500
2000
2500
3000
3500
4000
4500
0 500 1000 1500 2000
TR
EC
co
ncen
trati
on
(c
op
ies/μL)
Birth weight <2000 gr
Birth weight (gr)
Detecting SCID
• Established Cutoff
• Detected CDC SCID positive DBS
• Detected SCID DBS
Reticular Dysgenesis
Adenosine Deaminase Deficiency
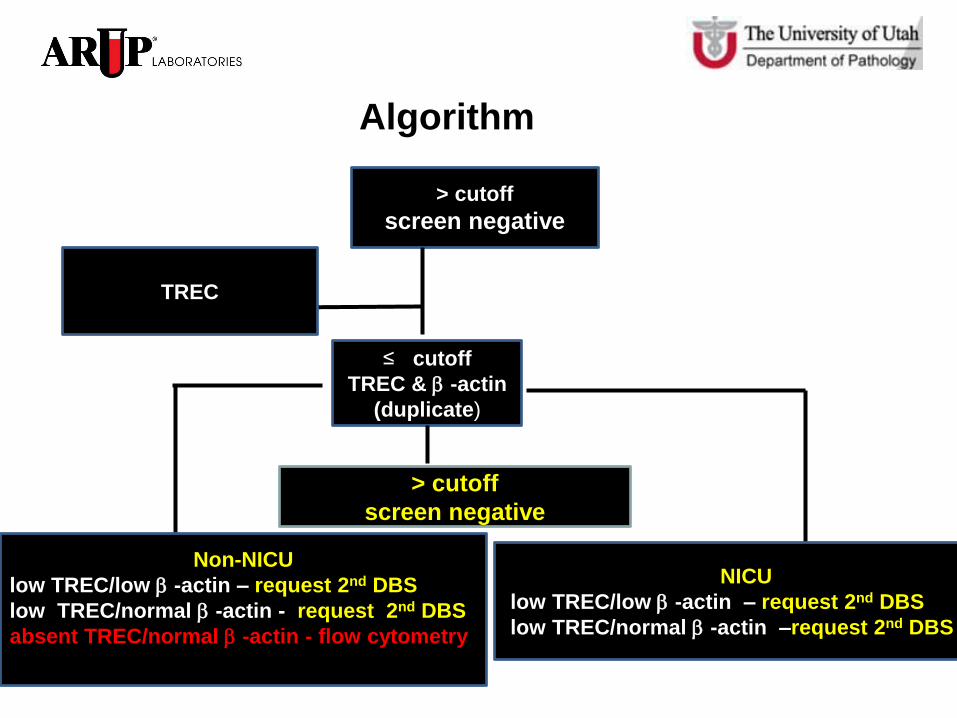
Algorithm
≤ cutoff
TREC & b -actin
(duplicate)
Non-NICU
low TREC/low b -actin – request 2nd DBS
low TREC/normal b -actin - request 2nd DBS
absent TREC/normal b -actin - flow cytometry
NICU
low TREC/low b -actin – request 2nd DBS
low TREC/normal b -actin –request 2nd DBS
TREC
> cutoff
screen negative
> cutoff
screen negative
The First Quarter
• Screened 13,200 babies
• NICU population accounts for the
majority of repeat DBS testing
• Confirmatory Testing – 3 babies
1 mild lymphopenia
2 profound lymphopenia
Acknowledgements
• Utah Department of Health
Dr. Harper Randall, Kim Hart , Dr. Robin Atkinson, Norm Brown
• Dr. Mei Baker
• ARUP/University of Utah
– Dr. Marzia Pasquali, Dr. Noriko Kusukawa, Dr. Harry Hill, Dr. Carl Wittwer
– New Technology Group, Newborn Screening Lab, Molecular Genetics Lab
– Wei Xiong, Jorja Warren, Dr. Orly Ardon, Dr. Jeff Stevenson
• Primary Children’s Medical Center, Immunology Division
Dr. Karin Chen
• SCID Subcommittee
Dr.Rich Harward (UDOH), Julie Drake (March of Dimes), Michael Pulsipher (Bone Marrow Transplant) Nan Streeter (UDOH), Jill Heaps (Parent Advocate)