New Techniques -...
11
1 R esistant hypertension has been linked to chronic exces- sive sympathetic drive, especially elevation of renal sym- pathetic activity in some groups of patients. 1,2 Against this background, renal artery ablation selectively denervating the kidneys emerges as an alternative treatment for such patients. Although initial trials 3,4 showed promising results with regard to large reductions in blood pressure (BP), disappointingly, the potential therapeutic role of renal denervation (RDN) in lowering BP is being challenged after the failure of recent SYMPLICITY HTN-3 trial 5 to show a benefit of RDN over the optimal medical therapy. The concept of RDN is supported by both experimental and early human evidence when surgical sympathectomy procedures were done and found to have huge effect on BP. 6–8 However, for the time being, the BP-lowering effect of cath- eter-based RDN is highly variable (the rates of nonresponse to RDN vary between 8% and 37%). 9 Kaiser et al 10 reported that repeated RDN could significantly decrease BP in non- responders to previous radiofrequency ablation procedure. These findings suggest that lack of BP reductions after RDN may be the results of incomplete denervation. Therefore, to minimize treatment failure of blind ablation, a method that could convert what is currently a purely anatomic procedure to one that involves quantifying the efficacy of RDN intrapro- cedurally and mapping the renal nerves to enable a targeted therapy is of great clinical significance. Background—Electric stimulation has been proved to be available to monitor the efficacy of renal denervation (RDN). This study was to evaluate the effectiveness of high-frequency stimulation (HFS)–guided proximal RDN. Methods and Results—A total of 13 Chinese Kunming dogs were included and allocated to proximal RDN group (n=8) and control group (n=5). HFS (20 Hz, 8 V, pulse width 2 ms) was performed from proximal to distal renal artery in all dogs. Radiofrequency ablations were delivered in proximal RDN group and only at the proximal positive sites where systolic blood pressure (BP) increased ≥10 mm Hg during HFS. Postablation HFS was performed over the previously stimulated sites. BP, heart rate, and plasma norepinephrine were analyzed. In 8 denervated dogs, preablation HFS caused significant BP increases of 6.0±5.0/3.4±5.5, 16.9±11.7/11.1±8.5, and 17.1±8.4/8.5±5.3 mm Hg during the first, second, and third 20 s of HFS at the proximal positive sites. After ablation, these sites showed a negative response to postablation HFS with increases of BP by 1.3±3.0/1.0±2.5, 0.8±3.9/1.5±3.4, and 1.5±4.5/0.7±3.8 mm Hg. Of note, no radiofrequency applications were delivered at the positive sites of middle renal artery, repeated HFS increased BP only by 3.3±5.3/2.8±4.2, 5.3±6.6/3.8±4.7, and 2.9±4.6/1.3±3.2 mm Hg, failed to reproduce the previous BP increases of 6.2±5.6/5.3±4.4, 15.0±9.3/10.2±6.2, and 14.9±7.7/8.4±4.7 mm Hg. At 3 months, BP and plasma norepinephrine substantially decreased in proximal RDN group. Whereas controls showed minimal BP decreases and had similar plasma norepinephrine concentrations as baseline. Conclusions—Renal afferent nerves can be mapped safely, and HFS-guided targeted proximal RDN can achieve apparent BP reduction and sympathetic inhibition. (Circ Cardiovasc Interv. 2015;8:e001847. DOI: 10.1161/CIRCINTERVENTIONS.115.001847.) Key Words: blood pressure ◼ catheter ablation ◼ heart rate ◼ hypertension ◼ renal artery © 2015 American Heart Association, Inc. Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.115.001847 Received May 29, 2014; accepted May 7, 2015. From the Department of Cardiology, the Second Affiliated Hospital of Chongqing Medical University, Chongqing Cardiac Arrhythmias Therapeutic Service Center, Chongqing, China (J.L., Z.W., T.Z., S.C., W.C., H.D., Z.T., H.Y., X.H., C.L., Z.L., Z.L., Y.Y.); Medizinische Klinik I, Krankenhaus Landshut/Achdorf, Landshut, Germany (B.Z.); and School of Life Sciences, the Chinese University of Hong Kong, Hong Kong, China (K.W.). *J. Lu and Dr Wang contributed equally to this work. Correspondence to Yuehui Yin, MD, Department of Cardiology, the Second Affiliated Hospital of Chongqing Medical University, Chongqing Cardiac Arrhythmias Therapeutic Service Center, No. 76, Linjiang Rd, Yuzhong District, Chongqing 400010, China. E-mail [email protected] Selective Proximal Renal Denervation Guided by Autonomic Responses Evoked via High-Frequency Stimulation in a Preclinical Canine Model Jiayi Lu, MM*; Zhenglong Wang, PhD*; Tingquan Zhou, PhD; Shaojie Chen, PhD; Weijie Chen, MM; Huaan Du, PhD; Zhen Tan, MM; Hanxuan Yang, MM; Xinyu Hu, MM; Chang Liu, MM; Zhiyu Ling, PhD; Zengzhang Liu, MD; Bernhard Zrenner, MD; Kamsang Woo, MD; Yuehui Yin, MD New Techniques by guest on July 20, 2018 http://circinterventions.ahajournals.org/ Downloaded from
Transcript of New Techniques -...

1
Resistant hypertension has been linked to chronic exces-sive sympathetic drive, especially elevation of renal sym-
pathetic activity in some groups of patients.1,2 Against this background, renal artery ablation selectively denervating the kidneys emerges as an alternative treatment for such patients. Although initial trials3,4 showed promising results with regard to large reductions in blood pressure (BP), disappointingly, the potential therapeutic role of renal denervation (RDN) in lowering BP is being challenged after the failure of recent SYMPLICITY HTN-3 trial5 to show a benefit of RDN over the optimal medical therapy.
The concept of RDN is supported by both experimental and early human evidence when surgical sympathectomy
procedures were done and found to have huge effect on BP.6–8 However, for the time being, the BP-lowering effect of cath-eter-based RDN is highly variable (the rates of nonresponse to RDN vary between 8% and 37%).9 Kaiser et al10 reported that repeated RDN could significantly decrease BP in non-responders to previous radiofrequency ablation procedure. These findings suggest that lack of BP reductions after RDN may be the results of incomplete denervation. Therefore, to minimize treatment failure of blind ablation, a method that could convert what is currently a purely anatomic procedure to one that involves quantifying the efficacy of RDN intrapro-cedurally and mapping the renal nerves to enable a targeted therapy is of great clinical significance.
Background—Electric stimulation has been proved to be available to monitor the efficacy of renal denervation (RDN). This study was to evaluate the effectiveness of high-frequency stimulation (HFS)–guided proximal RDN.
Methods and Results—A total of 13 Chinese Kunming dogs were included and allocated to proximal RDN group (n=8) and control group (n=5). HFS (20 Hz, 8 V, pulse width 2 ms) was performed from proximal to distal renal artery in all dogs. Radiofrequency ablations were delivered in proximal RDN group and only at the proximal positive sites where systolic blood pressure (BP) increased ≥10 mm Hg during HFS. Postablation HFS was performed over the previously stimulated sites. BP, heart rate, and plasma norepinephrine were analyzed. In 8 denervated dogs, preablation HFS caused significant BP increases of 6.0±5.0/3.4±5.5, 16.9±11.7/11.1±8.5, and 17.1±8.4/8.5±5.3 mm Hg during the first, second, and third 20 s of HFS at the proximal positive sites. After ablation, these sites showed a negative response to postablation HFS with increases of BP by 1.3±3.0/1.0±2.5, 0.8±3.9/1.5±3.4, and 1.5±4.5/0.7±3.8 mm Hg. Of note, no radiofrequency applications were delivered at the positive sites of middle renal artery, repeated HFS increased BP only by 3.3±5.3/2.8±4.2, 5.3±6.6/3.8±4.7, and 2.9±4.6/1.3±3.2 mm Hg, failed to reproduce the previous BP increases of 6.2±5.6/5.3±4.4, 15.0±9.3/10.2±6.2, and 14.9±7.7/8.4±4.7 mm Hg. At 3 months, BP and plasma norepinephrine substantially decreased in proximal RDN group. Whereas controls showed minimal BP decreases and had similar plasma norepinephrine concentrations as baseline.
Conclusions—Renal afferent nerves can be mapped safely, and HFS-guided targeted proximal RDN can achieve apparent BP reduction and sympathetic inhibition. (Circ Cardiovasc Interv. 2015;8:e001847. DOI: 10.1161/CIRCINTERVENTIONS.115.001847.)
Key Words: blood pressure ◼ catheter ablation ◼ heart rate ◼ hypertension ◼ renal artery
© 2015 American Heart Association, Inc.
Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.115.001847
Received May 29, 2014; accepted May 7, 2015.From the Department of Cardiology, the Second Affiliated Hospital of Chongqing Medical University, Chongqing Cardiac Arrhythmias Therapeutic
Service Center, Chongqing, China (J.L., Z.W., T.Z., S.C., W.C., H.D., Z.T., H.Y., X.H., C.L., Z.L., Z.L., Y.Y.); Medizinische Klinik I, Krankenhaus Landshut/Achdorf, Landshut, Germany (B.Z.); and School of Life Sciences, the Chinese University of Hong Kong, Hong Kong, China (K.W.).
*J. Lu and Dr Wang contributed equally to this work.Correspondence to Yuehui Yin, MD, Department of Cardiology, the Second Affiliated Hospital of Chongqing Medical University, Chongqing Cardiac
Arrhythmias Therapeutic Service Center, No. 76, Linjiang Rd, Yuzhong District, Chongqing 400010, China. E-mail [email protected]
Selective Proximal Renal Denervation Guided by Autonomic Responses Evoked via High-Frequency
Stimulation in a Preclinical Canine ModelJiayi Lu, MM*; Zhenglong Wang, PhD*; Tingquan Zhou, PhD; Shaojie Chen, PhD;
Weijie Chen, MM; Huaan Du, PhD; Zhen Tan, MM; Hanxuan Yang, MM; Xinyu Hu, MM; Chang Liu, MM; Zhiyu Ling, PhD; Zengzhang Liu, MD; Bernhard Zrenner, MD;
Kamsang Woo, MD; Yuehui Yin, MD
New Techniques
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

2 Lu et al Proximal RDN With Electric Stimulation
A vagal response elicited by endocardial high-frequency stimulation (HFS) was used to reflect the contribution of abla-tion of epicardial autonomic ganglia in patients with atrial fibrillation.11 Chinushi et al12 successfully applied this con-cept to the field of RDN. In their study, HFS to renal artery before RDN could elicit an orthosympathetic response when stimulated renal afferent nerves activate central sympathetic nervous activity. In addition, the absence of BP-increasing response to postablation HFS was an indication to confirm the actual disruption of renal nerve fibers. The precise anatomic information in human from Sakakura et al13 indicated that the renal afferent nerves converge on the renal arteries closer to aorta. On the basis of these considerations, we applied HFS to map the renal afferent nerves and assessed the efficacy of HFS-guided proximal RDN.
Methods
AnimalsThe Chinese Kunming dog breed was originally developed from the local hybrid dogs by crossing local native dogs with working dogs.14 They have natural high BP,15 and are therefore ideal experimental ani-mals used for this study. Eligible dogs were older than 3 years and had a systolic BP (SBP) of ≥140 mm Hg (under anesthesia and via in-vasive BP monitoring). After selection, a total of 24 healthy Chinese Kunming dogs, weighing between 30 and 35 kg, were enrolled in the present study. Twelve animals were assigned to proximal RDN group, which underwent HFS and proximal renal artery ablation guided by the autonomic responses evoked via HFS (n=12). Another 12 animals were assigned to control group, which underwent HFS but no abla-tion on the proximal arteries was performed (n=12).
The experiment was approved by the animal experimentation eth-ics committee of the Chongqing Medical University, following the guidelines of the National Institutes of Health for the care and use of laboratory animals. Standard food and water feedings were given throughout the experimental period.
Animal Preparation and Renal AngiogramThe dogs were anesthetized with 3% sodium pentobarbital of 30 mg/kg by intraperitoneal injection, followed by a maintenance dose of 5 mg/kg per hour. Penicillin was given intramuscularly after the ablation for the prevention of infection. The surface ECG was continuously record-ed throughout the study by a multichannel recorder (Sichuan Jinjiang Electronic Science and Technology Company, China). Both sides of the femoral artery were punctured under sterile conditions, and an amount of 2000 IU unfractionated heparin was administered. The continuous invasive BP monitoring was recorded via the left femoral artery. A ded-icated 6F bipolar micropores irrigated ablation catheter (AquaSense, Synaptic Medical Limited, Beijing, China) was introduced via the right femoral artery and placed in the right or left renal artery for delivering HFS and radiofrequency energy. The bipolar AquaSense catheter con-sists of a 3.5-mm-long tip electrode, and the electrode spacing is 2 mm. There are 44 micropores located around the catheter tip that are open irrigated through a central lumen with heparinized saline to maintain lower tip-to-tissue temperature at the ablation site (Figure 1).
Bilateral renal angiography was performed using a 6F JR4 Judkins catheter (Cordis Corporation Miami, FL). If renal artery ab-normalities were found, diameters were below the minimum accept-able size (<4 mm, using inner diameter of 6F JR4 Judkins catheter as reference), or main renal artery length was shorter than 20 mm, the dog would be eliminated from the study.
HFS Protocol and Autonomic ResponsesHFS was applied from the proximal (5–10 mm from the ostium of renal artery) to the distal (5–10 mm from first distal main renal ar-tery bifurcation) segments of the left or right renal artery (Figure 2), via the bipolar electrodes of AquaSense catheter, as described earlier. The number of attempts of HFS on proximal, middle, and distal seg-ments of renal arteries depended on the ease of access of the target with the electrode. Rectangular electric stimuli were delivered at a frequency of 20 Hz, amplitude to 8 V, and pulse duration of 2 ms for 60 s using a Nerve and Muscle Stimulator (XinNuo B100; Sichuan Jinjiang Electronic Science and Technology Company). The positive autonomic response was defined as elevation of SBP by ≥10 mm Hg during HFS (study by Chinushi et al12 indicated that when electric stimulation activated the renal nerves, SBP would increase at least 10 mm Hg). After ablation, under fluoroscopic guidance, the catheter was repositioned over the previously stimulated sites and postabla-tion HFS was performed (using the same threshold as baseline). For analysis, each HFS of 60-s phases was subdivided into 20-s phases.
Radiofrequency Catheter AblationIn proximal RDN group, after electric stimulation of renal arteries, ra-diofrequency ablation was performed over HFS-positive sites of proxi-mal renal artery where autonomic responses evoked by transcatheter HFS were obtained. Radiofrequency ablation used the AquaSense cath-eter, as described earlier, with saline irrigated manually to decrease the temperature of tissue–electrode interface. Radiofrequency energy deliv-ery and ablation time were always started at 8 W and 60 s, and increased to 15 W and 300 s if the autonomic response still occurred during pos-tablation HFS. The end point of ablation was defined as the failure to reproduce the positive BP-increasing response with repeated HFS.
Blood Sampling and Follow-UpBaseline blood sampling was obtained from the right femoral vein. Three milliliter of blood sampling to measure the plasma norepi-nephrine was obtained in EDTA. After high-speed centrifugation, the blood samples were stored at −80°C until assay. The plasma norepi-nephrine was assayed by high-performance liquid chromatography.
WHAT IS KNOWN
•A better understanding of the pathophysiological roles of the renal sympathetic nerves in resistant hypertension and a detailed knowledge of neuro-anatomy has allowed catheter-based renal denerva-tion to emerge as a promising alternative treatment for patients with resistant hypertension; however, the blood pressure–lowering effect of denervation pro-cedures performed by nonselective ablation of the renal artery wall is highly variable.
•Although electric stimulation has been shown to monitor the efficacy of renal denervation, there has been no report of transcatheter electric stimulation as a guide for renal denervation procedures.
WHAT THE STUDY ADDS
•Blood pressure and plasma norepinephrine were de-creased 3 months after high-frequency stimulation–guided targeted radiofrequency ablation compared with nondenervated controls.
•Specific high-frequency stimulation–guided abla-tions over the proximal electric stimulation respon-sive sites not only abolished the blood pressure response in the postablation period but also attenu-ated the blood pressure response to repeated high-frequency stimulation.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

3 Lu et al Proximal RDN With Electric Stimulation
During the follow-up period, the condition of all experimental dogs was observed daily. After the ablation or sham procedure of 3 months, follow-up assessments were conducted, which consisted of invasive BP measurements via the femoral artery, bilateral renal angi-ography, and plasma norepinephrine assay, as described above.
Statistical AnalysisAll continuous data were presented as mean±SD, and categorical variables were expressed as proportions. Differences of BP, heart rate (HR), ΔBP, and ΔHR during HFS were analyzed by 1-/2-way repeated measures ANOVA. Multiple pairwise comparisons were
Figure 1. Catheter used for high-fre-quency stimulation and radiofrequency ablation. A, The whole picture of Aqua-Sense catheter, (B) its curve, and (C) its tip. The 44 micropores located around the catheter tip were open irrigated with saline to maintain lower tip-to-tissue temperature during ablation. These micropores can also inject the contrast into renal artery visualizing the vessel. D–F, Contrast injection into the renal artery identifies the catheter position and its contact with the wall of vessel.
Figure 2. Catheter positioning during high-frequency stimulation. A and I, Renal artery before and after electric stimula-tion. During electric stimulation, the contrast was injected from AquaSense catheter to visualize the vessel. Under fluoroscopic guidance, catheter was serially positioned along the superior (B, D, F), and inferior (C, E, G, H) aspects of the renal artery to deliver high-frequency stimulation, from the proximal to the distal.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

4 Lu et al Proximal RDN With Electric Stimulation
performed with the Bonferroni test. Paired t tests were used to compare BPs and plasma norepinephrine concentrations before and 3 months after RDN, and these changes between proximal RDN group and controls were compared using Student t tests. Correlation between changes in systolic BP and plasma norepinephrine 3 months after RDN was assessed with Pearson test. A 2-tailed value of P<0.05 was regarded as statistically significant. All the statisti-cal analyses were performed with SPSS statistical software (version 17.0; Chicago, IL).
ResultsTwenty-four Chinese Kunming dogs in preparation for renal artery stimulation and ablation underwent bilateral renal angi-ography. Angiograms of all the renal arteries revealed that 2 dogs in proximal RDN group and 4 dogs in control group were excluded, and the remaining 18 dogs were anatomically eligible to perform HFS and RDN. No renal artery dissec-tion, stenosis, or other complications associated with electric stimulation and radiofrequency ablation procedure occurred in either group.
Autonomic Responses to HFS
Localization of Renal Afferent Nerves InnervationHFS to renal arteries caused significant increases in SBP (Figures 3 and 4). These changes often began during 20 to 40 s after the onset of HFS and returned to baseline within 2 to 5 minutes after its cessation. The number of attempts of HFS in each dog were 11±3 (range, 7–15). Autonomic responses evoked by HFS were elicited in 13 of 18 (72.2%) dogs with an average of 6±2 sites per dog, including 8 of 10 (80%) dogs in proximal RDN group and 5 of 8 (62.5%) in control group. The proximal and the middle segment of renal artery each required only a mean of 2±1 HFS attempts to determine a positive BP-increasing response. No BP eleva-tion was induced by HFS at the distal portion of renal artery.
Autonomic Responses in Proximal RDN Group Versus Control GroupWhen compared with the values before electric stimulation, HFS to renal arteries of 8 HFS responsive dogs in proximal
Figure 3. Blood pressure (BP) response at high-frequency stimulation (HFS) positive sites of proximal renal artery. A, HFS-positive site at proximal renal artery (red dot, also indicated by arrow). White dots represented HFS-negative sites, whereas red and yellow dots rep-resented HFS-positive sites. The radiofrequency (RF) energy was delivered only over red dot, the proximal responsive site. As shown, before ablation, HFS increased BP significantly (B1 and B2), whereas after ablation, repeated HFS was not associated with BP-increasing response (C1 and C2). RDN indicates renal denervation.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
5 Lu et al Proximal RDN With Electric Stimulation
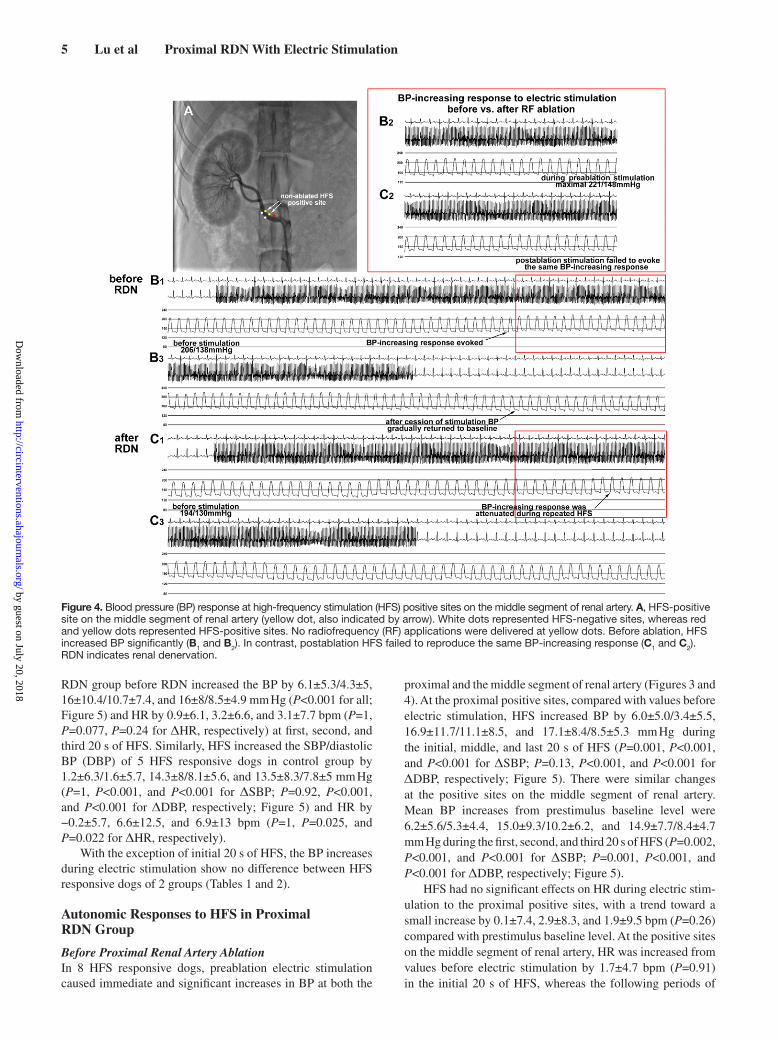
RDN group before RDN increased the BP by 6.1±5.3/4.3±5, 16±10.4/10.7±7.4, and 16±8/8.5±4.9 mm Hg (P<0.001 for all; Figure 5) and HR by 0.9±6.1, 3.2±6.6, and 3.1±7.7 bpm (P=1, P=0.077, P=0.24 for ΔHR, respectively) at first, second, and third 20 s of HFS. Similarly, HFS increased the SBP/diastolic BP (DBP) of 5 HFS responsive dogs in control group by 1.2±6.3/1.6±5.7, 14.3±8/8.1±5.6, and 13.5±8.3/7.8±5 mm Hg (P=1, P<0.001, and P<0.001 for ΔSBP; P=0.92, P<0.001, and P<0.001 for ΔDBP, respectively; Figure 5) and HR by −0.2±5.7, 6.6±12.5, and 6.9±13 bpm (P=1, P=0.025, and P=0.022 for ΔHR, respectively).
With the exception of initial 20 s of HFS, the BP increases during electric stimulation show no difference between HFS responsive dogs of 2 groups (Tables 1 and 2).
Autonomic Responses to HFS in Proximal RDN Group
Before Proximal Renal Artery AblationIn 8 HFS responsive dogs, preablation electric stimulation caused immediate and significant increases in BP at both the
proximal and the middle segment of renal artery (Figures 3 and 4). At the proximal positive sites, compared with values before electric stimulation, HFS increased BP by 6.0±5.0/3.4±5.5, 16.9±11.7/11.1±8.5, and 17.1±8.4/8.5±5.3 mm Hg during the initial, middle, and last 20 s of HFS (P=0.001, P<0.001, and P<0.001 for ΔSBP; P=0.13, P<0.001, and P<0.001 for ΔDBP, respectively; Figure 5). There were similar changes at the positive sites on the middle segment of renal artery. Mean BP increases from prestimulus baseline level were 6.2±5.6/5.3±4.4, 15.0±9.3/10.2±6.2, and 14.9±7.7/8.4±4.7 mm Hg during the first, second, and third 20 s of HFS (P=0.002, P<0.001, and P<0.001 for ΔSBP; P=0.001, P<0.001, and P<0.001 for ΔDBP, respectively; Figure 5).
HFS had no significant effects on HR during electric stim-ulation to the proximal positive sites, with a trend toward a small increase by 0.1±7.4, 2.9±8.3, and 1.9±9.5 bpm (P=0.26) compared with prestimulus baseline level. At the positive sites on the middle segment of renal artery, HR was increased from values before electric stimulation by 1.7±4.7 bpm (P=0.91) in the initial 20 s of HFS, whereas the following periods of
Figure 4. Blood pressure (BP) response at high-frequency stimulation (HFS) positive sites on the middle segment of renal artery. A, HFS-positive site on the middle segment of renal artery (yellow dot, also indicated by arrow). White dots represented HFS-negative sites, whereas red and yellow dots represented HFS-positive sites. No radiofrequency (RF) applications were delivered at yellow dots. Before ablation, HFS increased BP significantly (B1 and B2). In contrast, postablation HFS failed to reproduce the same BP-increasing response (C1 and C2). RDN indicates renal denervation.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

6 Lu et al Proximal RDN With Electric Stimulation
HFS revealed significant changes in ΔHR, with increases of 3.5±4.6 bpm (P=0.035) and 4.4±5.5 bpm (P=0.027).
After Proximal Renal Artery AblationRadiofrequency ablation was performed over the proxi-mal positive sites of the 8 HFS responsive dogs. These sites showed a negative response to each phase of postablation HFS (Figure 3), with increases of BP by 1.3±3.0/1.0±2.5, 0.8±3.9/1.5±3.4, and 1.5±4.5/0.7±3.8 mm Hg (P=0.33 for ΔSBP; P=0.26 for ΔDBP; Figure 5) when compared with values before electric stimulation. Of note, no radiofrequency applications were delivered at the middle segment of renal artery, but the HFS-positive sites located in the middle region of renal artery still failed to reproduce the same BP-increasing response with repeated HFS after ablation (Figure 4). Only during the second 20 s of HFS, SBP and DBP were increased from prestimulus baseline level by 5.3±6.6 mm Hg (P=0.026) and 3.8±4.7 mm Hg (P=0.024), whereas during other phases, no significant changes were observed (Figure 5). During the initial and last 20 s of HFS, BP was increased from values before electric stimulation by 3.3±5.3/2.8±4.2 mm Hg (P=0.13 for ΔSBP, P=0.083 for ΔDBP), and 2.9±4.6/1.3±3.2 mm Hg (P=0.12 for ΔSBP and P=0.67 for ΔDBP), respectively.
After ablation, compared with values before electric stimulation, HR remained unchanged during all phases of repeated HFS at positive sites in both the proximal and the middle regions of renal artery. HFS to proximal positive sites increased HR by 0.8±2.6, 0.9±2.8, and 2.2±4.4 bpm (P=0.18)
and at the positive sites on middle segment of renal artery, HR was increased from prestimulus baseline values by 0.8±3.5, 0.5±3.0, and 0.4±3.6 bpm (P=0.83).
Autonomic Response Before Versus After Radiofrequency AblationIn 8 HFS responsive dogs, when compared with the auto-nomic response to HFS in the preablation state, a significant and substantial lower BP response was observed after RDN at positive sites on both proximal and middle segment of renal artery. When compared with the values before ablation, both mean and change of SBP and DBP during HFS after RDN were markedly attenuated (Tables 3 and 4).
Proximal Radiofrequency AblationRadiofrequency ablation was successfully obtained in 8 dogs responsive to HFS, obliterating the BP-increasing response to repeated HFS. A total of 3±1 radiofrequency applications were delivered in each dog, and average radiofrequency dura-tion for each lesion was 215±73 s (range, 60–300 s). The mean delivered radiofrequency energy was 11±2 W (range, 8–15 W), and maximum temperature of the catheter tip was 43±2°C (range, 40–45°C). Tissue impedance decreased from 214±47 before to 185±42 ohm after (P<0.001).
Electric current-induced BP elevation occurred not only during electric stimulation but also when radiofrequency energy was delivered. Preablation HFS increased BP of proxi-mal responsive sites from an average of 189.8±16/131.2±16.6
Table 1. Comparisons of Autonomic Response to HFS Between Proximal RDN Group and Control Group: Mean of BP
Proximal RDN Group Control Group P Value
Proximal RDN Group Control Group P Value
Proximal RDN Group Control Group P Value
SBP, mm Hg DBP, mm Hg HR, bpm
Before HFS 188.7±16.2 175.6±16.3 0.001 130.2±16.4 119.8±8.7 0.001 179±20.5 178.2±21.4 0.88
1st 20 s 194.8±16 176.8±17.7 <0.001 134.5±15.5 121.4±10.6 <0.001 179.9±18.5 178±20.8 0.69
2nd 20 s 204.6±14 189.8±17.2 <0.001 140.8±13.7 127.9±12 <0.001 182.2±20.8 184.8±22.3 0.61
3rd 20 s 204.7±14.7 189.1±14.4 <0.001 138.6±15.6 127.6±10.9 0.001 182.1±21.1 185.1±22.8 0.57
After HFS 189±18.1 176.5±17.6 0.004 129.1±18.8 119.8±12.4 0.015 176.9±20.5 180.5±22.4 0.48
Mean of BP and HR during HFS at positive sites of 13 HFS responsive dogs, including 8 in proximal RDN group and 5 in control group. Differences of BP, HR, ΔBP, and ΔHR between 2 groups during HFS were analyzed by 2-way repeated measures ANOVA. Multiple pairwise comparisons were performed with the Bonferroni test. DBP indicates diastolic blood pressure; HFS, high-frequency stimulation; HR, heart rate; P value, control group vs proximal RDN group; RDN, renal denervation; and SBP, systolic BP.
Figure 5. Blood pressure (BP) response to high-frequency stimulation (HFS). A, Systolic BP increases during electric stimulation in 8 HFS responsive denervated dogs before ablation and 5 HFS responsive nondenervated controls. B1 and B2, BP response to HFS before and after ablation of 8 HFS responsive dogs in proximal renal denervation group. B1, HFS-positive sites on proximal renal artery. B2, HFS-pos-itive sites on the middle segment of renal artery. Differences of systolic BP were analyzed by 1-way repeated measures ANOVA. When significance between groups was detected, the Bonferroni test was used to compute post hoc comparisons of significant values. *P<0.05 for before vs multiple time points during electric stimulation (1st 20 s, 2nd 20 s, and 3rd 20 s). RDN indicates renal denervation.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

7 Lu et al Proximal RDN With Electric Stimulation
to 203.1±13.1/138.8±14.7 mm Hg (P<0.001). Consistent with the change during HFS, an immediate and substan-tial BP-increasing response was also seen during abla-tion. Radiofrequency application increased BP from 186.8±19.4/128.4±19.6 to 207.2±17.2/141.5±16.8 mm Hg (P<0.001). BP showed no significant difference between HFS and radiofrequency ablation period (Figure 6).
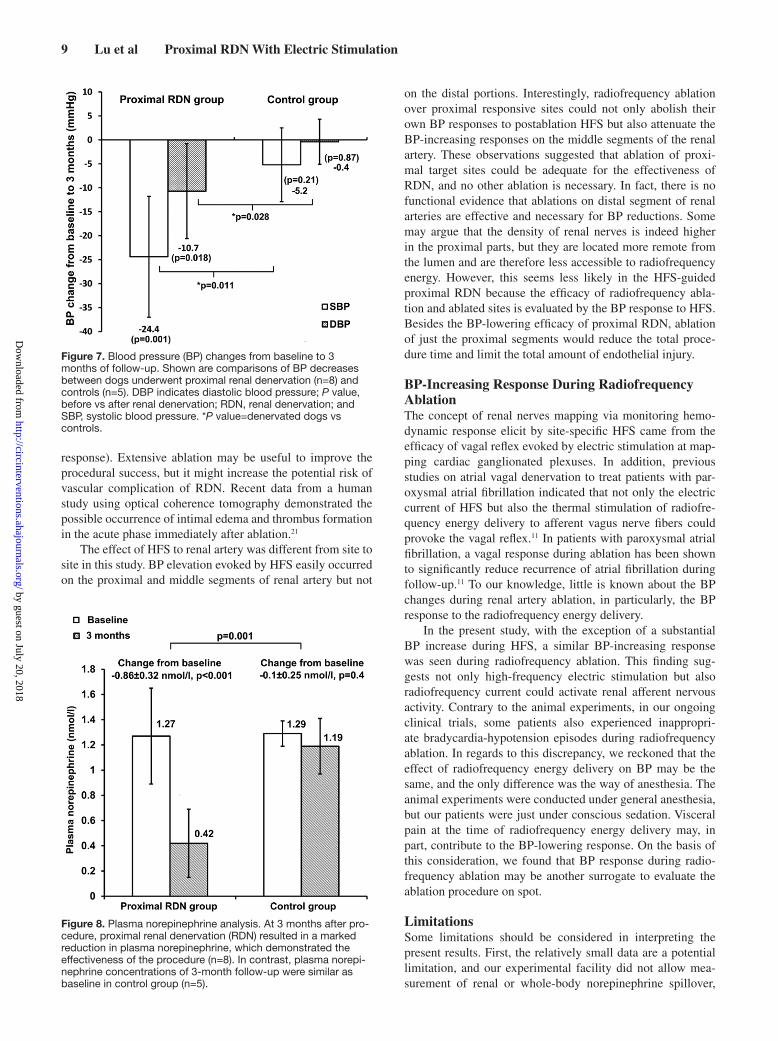
Plasma Norepinephrine and BP of Follow-UpThirteen dogs responsive to HFS underwent ablation or sham procedure and completed 3-month follow-up. The mean baseline BPs were 194±13.2/130.1±13.5 mm Hg in proxi-mal RDN group and 174.4±17.2/114.4±3.7 mm Hg in control group. After 3 months, significant BP decreases from base-line were observed in dogs underwent RDN, with reduc-tions of −24.4±12.6/−10.7±9.9 mm Hg (P=0.001 for ΔSBP and P=0.018 for ΔDBP, respectively; Figure 7). Whereas controls showed minimal BP decreases, with reductions of −5.5±7.7/−0.4±4.7 mm Hg (P=0.21 for ΔSBP and P=0.87 for ΔDBP, respectively; Figure 7).
The plasma norepinephrine concentrations at baseline were 1.27±0.38 nmol/L in proximal RDN group and 1.29±0.1 nmol/L in control group. Proximal RDN resulted in a marked reduction in plasma norepinephrine 3 months after radio-frequency ablation, with a decrease of −0.86±0.32 nmol/L (P<0.001; Figure 8). The decrease in plasma norepinephrine correlated with SBP reduction after 3 months, but the corre-lation was not statistically significant (r=0.632; P=0.18). In contrast, controls at 3 months of follow-up had similar con-centrations as baseline, with a reduction of 0.1±0.25 nmol/L (P=0.4; Figure 8).
DiscussionThe main findings of this study were as follows: (1) before RDN, HFS resulted in a positive autonomic response of an immediate increase in SBP>10 mm Hg in both proximal and middle regions of renal artery. No BP elevation was induced by HFS at the distal segment of renal artery; (2) radiofrequency applications were only performed over the proximal posi-tive sites, but after ablation repeated HFS failed to reproduce
Table 2. Comparisons of Autonomic Response to HFS Between Proximal RDN Group and Control Group: Change of BP
Proximal RDN Group Control Group P Value
Proximal RDN Group Control Group P Value
Proximal RDN Group Control Group P Value
ΔSBP, mm Hg ΔDBP, mm Hg ΔHR, bpm
1st 20 s 6.1±5.3 1.2±6.3 0.001 4.3±5 1.6±5.7 0.036 0.9±6.1 -0.2±5.7 0.42
2nd 20 s 16±10.4 14.3±7.9 0.43 10.7±7.4 8.1±5.6 0.1 3.2±6.6 6.6±12.5 0.16
3rd 20 s 16±8 13.5±8.3 0.19 8.5±4.9 7.8±5 0.55 3.1±7.7 6.9±13 0.14
Change of BP and HR during HFS at positive sites of 13 HFS responsive dogs, including 8 in proximal RDN group and 5 in control group. Differences of BP, HR, ΔBP, and ΔHR between 2 groups during HFS were analyzed by 2-way repeated measures ANOVA. Multiple pairwise comparisons were performed with the Bonferroni test. DBP indicates diastolic blood pressure; HFS, high-frequency stimulation; HR, heart rate; P value, control group vs proximal RDN group; RDN, renal denervation; and SBP, systolic BP.
Table 3. Autonomic Response to HFS Before vs After Radiofrequency Ablation in Proximal Renal Denervation Group: Mean of BP
Before Ablation After Ablation P Value Before Ablation After Ablation P Value Before Ablation After Ablation P Value
SBP, mm Hg DBP, mm Hg HR, bpm
Before HFS
Ablated HFS-positive sites 189.8±16.0 186.7±18.1 0.6 131.2±16.6 130.3±17.7 0.88 186.4±22.5 185.3±20.8 0.88
Nonablated HFS-positive sites 187.6±16.9 183.1±18.0 0.46 129.2±16.6 126.9±17.5 0.7 171.6±15.5 175.1±14.6 0.5
1st 20 s
Ablated HFS-positive sites 195.8±14.0 188.0±18.8 0.18 134.5±15.3 131.3±17.9 0.58 186.5±19.7 186.1±20.15 0.95
Nonablated HFS-positive sites 193.8±18.1 186.4±18.4 0.24 134.5±16.3 129.7±17.7 0.42 173.3±14.9 175.9±13.1 0.59
2nd 20 s
Ablated HFS-positive sites 206.7±13.5 187.5±18.4 0.001 142.3±14.3 131.8±17.6 0.065 189.3±22.5 186.2±22.3 0.69
Nonablated HFS-positive sites 202.6±14.6 188.4±18.3 0.018 139.4±13.4 130.7±17.3 0.11 175.1±16.8 175.6±14.4 0.92
3rd 20 s
Ablated HFS-positive sites 206.9±14.0 188.2±18.6 0.002 139.7±15.9 131.0±18.0 0.14 188.3±23.6 187.5±23.9 0.92
Nonablated HFS-positive sites 202.5±15.5 186.0±18.5 0.008 137.6±15.6 128.2±18.0 0.11 176.0±16.8 175.6±15.6 0.94
After HFS
Ablated HFS-positive sites 190.4±17.8 184.8±18.1 0.37 130.4±19.8 128.2±17.7 0.73 182.3±23.78 186.8±21.8 0.57
Nonablated HFS-positive sites 187.6±18.8 182.4±19.1 0.42 127.8±18.2 125.7±18.6 0.74 171.4±15.4 174.2±15.3 0.6
Eight dogs responsive to HFS in proximal renal denervation group underwent RF ablation. Mean of BP and HR during HFS at HFS-positive sites of the 8 dogs before and after RF ablation. RF ablation was performed over proximal HFS-positive sites, and no RF applications were delivered at HFS-positive sites on the middle segment of renal artery. Differences of BP, HR, ΔBP, and ΔHR before and after RF ablation during HFS were analyzed by 2-way repeated measures ANOVA. Multiple pairwise comparisons were performed with the Bonferroni test. DBP indicates diastolic blood pressure; HFS, high-frequency stimulation; HR, heart rate; P value, before vs after RF ablation; RF, radiofrequency; and SBP, systolic blood pressure.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

8 Lu et al Proximal RDN With Electric Stimulation
the same BP-increasing response at the positive sites of both proximal and middle segment of renal artery; (3) BP and plasma norepinephrine substantially decreased 3 months after HFS-guided proximal RDN. However, nondenervated con-trols showed minimal BP and plasma norepinephrine changes; (4) consistent with the change during HFS, an immediate and substantial BP-increasing response was seen during ablation.
HFS-Guided RDNBoth renal afferent nerves and efferent sympathetic fibers are distributed in close proximity to the lumen–intima interface of the renal artery and should thus be accessible via catheter ablation, but the interventionalists still have to accept a black box during the procedure. Previous studies12,16,17 indicated that stimulation of renal afferent nerves could activate central car-diovascular nuclei and subsequently increase systemic sym-pathetic nervous activity and BP. To date, there has been no report of transcatheter HFS-guided RDN, only several recent studies investigating whether the transcatheter HFS could be
available to confirm the degree of denervation of renal nerves immediately after catheter-based RDN. In our study, besides real-time evaluation of denervation, we applied HFS to detect the location of renal afferent nerves. BP-increasing responses elicit by HFS occurred on the proximal and not on the distal segments of renal artery. These findings corroborate anatomic study by Sakakura et al13 showing sensory fibers converge on the proximal parts of renal arteries.
Renal nerves regulate systemic BP by 2 pathways. Efferent sympathetic fibers supply every aspect of the kidney, includ-ing the vasculature, juxtaglomerular apparatus, and renal tubu-lar cells, and control vascular resistance, renin release, and sodium retention.18 Renal afferent reflex could activate ros-tral ventrolateral medulla neurons in the brain, alter systemic sympathetic nervous activity, and contribute to the develop-ment of hypertension.19 Accordingly, it was hypothesized that destroying either efferent or afferent renal nerves could result in hypotensive effect of RDN. In the present study, radiofre-quency energy application was guided by previous evoked BP rises with HFS within the lumen of the renal arteries. At 3 months after the targeted ablation, the dogs showed apparent BP decreases and systemic sympathetic inhibition. In contrast, nondenervated controls showed minimal BP and plasma nor-epinephrine changes. Our findings suggested that HFS might be used to select appropriate sites for RDN. Although the reduced renal blood flow evoked by electric stimulation was defined as the efferent response,20 because of facility limita-tions, we cannot comment on the sympathetic efferent nerves had also been ablated by the HFS-guided RDN.
Proximal RDNFrom anatomic study, distal renal arteries have abundant sym-pathetic nerves, whereas renal afferent fibers converge on proximal segments.13 In daily clinical practice, radiofrequency ablations are applied discretely form the first distal main renal artery bifurcation all the way back to the ostium (although the number of ablation points is not a strictly fixed variable, 6 is recommended as routine procedure to provoke a BP-lowering
Figure 6. Blood pressure (BP) during high-frequency stimulation (HFS) and radiofrequency (RF) ablation. Eight HFS responsive dogs in proximal renal denervation group underwent RF ablation. Shown are BP values of ablation sites during HFS and RF energy delivery. DBP, diastolic blood pressure; and SBP, systolic blood pressure.
Table 4. Autonomic Response to HFS Before vs After Radiofrequency Ablation in Proximal Renal Denervation Group: Change of BP
Before Ablation After Ablation P Value Before Ablation
After Ablation P Value Before Ablation After Ablation P Value
ΔSBP, mm Hg ΔDBP, mm Hg ΔHR, bpm
1st 20 s
Ablated HFS-positive sites 6.0±5.0 1.3±3.0 0.002 3.4±5.5 1.0±2.5 0.12 0.1±7.4 0.8±2.6 0.72
Nonablated HFS-positive sites 6.2±5.6 3.3±5.3 0.13 5.3±4.4 2.8±4.2 0.095 1.7±4.7 0.8±3.5 0.51
2nd 20 s
Ablated HFS-positive sites 16.9±11.7 0.8±3.9 <0.001 11.1±8.5 1.5±3.4 <0.001 2.9±8.3 0.9±2.8 0.36
Nonablated HFS-positive sites 15.0±9.3 5.3±6.6 0.001 10.2±6.2 3.8±4.7 0.002 3.5±4.6 0.5±3.0 0.028
3rd 20 s
Ablated HFS-positive sites 17.1±8.4 1.5±4.5 <0.001 8.5±5.3 0.7±3.8 <0.001 1.9±9.5 2.2±4.4 0.91
Nonablated HFS-positive sites 14.9±7.7 2.9±4.6 <0.001 8.4±4.7 1.3±3.2 <0.001 4.4±5.5 0.4±3.6 0.018
Eight dogs responsive to HFS in proximal renal denervation group underwent RF ablation. Change of BP and HR during HFS at HFS-positive sites of the 8 dogs before and after RF ablation. RF ablation was performed over proximal HFS-positive sites, and no RF applications were delivered at HFS-positive sites on the middle segment of renal artery. Differences of BP, HR, ΔBP, and ΔHR before and after RF ablation during HFS were analyzed by 2-way repeated measures ANOVA. Multiple pairwise comparisons were performed with the Bonferroni test. DBP indicates diastolic blood pressure; HFS, high-frequency stimulation; HR, heart rate; P value, before vs after RF ablation; RF, radiofrequency; and SBP, systolic blood pressure.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
9 Lu et al Proximal RDN With Electric Stimulation
response). Extensive ablation may be useful to improve the procedural success, but it might increase the potential risk of vascular complication of RDN. Recent data from a human study using optical coherence tomography demonstrated the possible occurrence of intimal edema and thrombus formation in the acute phase immediately after ablation.21
The effect of HFS to renal artery was different from site to site in this study. BP elevation evoked by HFS easily occurred on the proximal and middle segments of renal artery but not
on the distal portions. Interestingly, radiofrequency ablation over proximal responsive sites could not only abolish their own BP responses to postablation HFS but also attenuate the BP-increasing responses on the middle segments of the renal artery. These observations suggested that ablation of proxi-mal target sites could be adequate for the effectiveness of RDN, and no other ablation is necessary. In fact, there is no functional evidence that ablations on distal segment of renal arteries are effective and necessary for BP reductions. Some may argue that the density of renal nerves is indeed higher in the proximal parts, but they are located more remote from the lumen and are therefore less accessible to radiofrequency energy. However, this seems less likely in the HFS-guided proximal RDN because the efficacy of radiofrequency abla-tion and ablated sites is evaluated by the BP response to HFS. Besides the BP-lowering efficacy of proximal RDN, ablation of just the proximal segments would reduce the total proce-dure time and limit the total amount of endothelial injury.
BP-Increasing Response During Radiofrequency AblationThe concept of renal nerves mapping via monitoring hemo-dynamic response elicit by site-specific HFS came from the efficacy of vagal reflex evoked by electric stimulation at map-ping cardiac ganglionated plexuses. In addition, previous studies on atrial vagal denervation to treat patients with par-oxysmal atrial fibrillation indicated that not only the electric current of HFS but also the thermal stimulation of radiofre-quency energy delivery to afferent vagus nerve fibers could provoke the vagal reflex.11 In patients with paroxysmal atrial fibrillation, a vagal response during ablation has been shown to significantly reduce recurrence of atrial fibrillation during follow-up.11 To our knowledge, little is known about the BP changes during renal artery ablation, in particularly, the BP response to the radiofrequency energy delivery.
In the present study, with the exception of a substantial BP increase during HFS, a similar BP-increasing response was seen during radiofrequency ablation. This finding sug-gests not only high-frequency electric stimulation but also radiofrequency current could activate renal afferent nervous activity. Contrary to the animal experiments, in our ongoing clinical trials, some patients also experienced inappropri-ate bradycardia-hypotension episodes during radiofrequency ablation. In regards to this discrepancy, we reckoned that the effect of radiofrequency energy delivery on BP may be the same, and the only difference was the way of anesthesia. The animal experiments were conducted under general anesthesia, but our patients were just under conscious sedation. Visceral pain at the time of radiofrequency energy delivery may, in part, contribute to the BP-lowering response. On the basis of this consideration, we found that BP response during radio-frequency ablation may be another surrogate to evaluate the ablation procedure on spot.
LimitationsSome limitations should be considered in interpreting the present results. First, the relatively small data are a potential limitation, and our experimental facility did not allow mea-surement of renal or whole-body norepinephrine spillover,
Figure 7. Blood pressure (BP) changes from baseline to 3 months of follow-up. Shown are comparisons of BP decreases between dogs underwent proximal renal denervation (n=8) and controls (n=5). DBP indicates diastolic blood pressure; P value, before vs after renal denervation; RDN, renal denervation; and SBP, systolic blood pressure. *P value=denervated dogs vs controls.
Figure 8. Plasma norepinephrine analysis. At 3 months after pro-cedure, proximal renal denervation (RDN) resulted in a marked reduction in plasma norepinephrine, which demonstrated the effectiveness of the procedure (n=8). In contrast, plasma norepi-nephrine concentrations of 3-month follow-up were similar as baseline in control group (n=5).
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

10 Lu et al Proximal RDN With Electric Stimulation
which is the gold standard to estimate the sympathetic nervous activity. Second, in our study, HFS in 5 dogs produced either no effect on BP or a slight decrease in BP. The electric stimuli in the current study were the maximum stimulation settings of the stimulator (20 Hz, 8 V, and pulse width 2 ms). Therefore, we did not have sufficient data to explain this observation by whether different stimulation thresholds would be applied or whether these sites lack renal afferent nerves. However, con-sidering that no BP-increasing response to HFS occurred at any site of the renal artery in these 5 dogs and HFS (20 Hz, 15 V, and pulse width 10 ms) caused a consistent BP increase in humans,17 we suggested that the HFS (20 Hz, 8 V, and pulse width 2 ms) unable to activate the renal afferent sensory nerves in these HFS nonresponsive dogs might contribute to this phenomenon. Finally, the present study was conducted in healthy and young animals. Atherosclerosis and calcification predominantly occur at the ostial sites of renal arteries. Limit-ing ablation at the proximal part of renal artery may have a higher risk for restenosis after ablation. Therefore, whether our findings in HFS-guided proximal RDN can be directly applied into the human situation remains unclear. However, our previous clinical study did not suggest such an outcome. It indicated that proximal RDN has a similar safety and efficacy profile compared with full-length RDN (unpublished data).
ConclusionsRenal afferent nerves predominantly reside in proximal renal arteries and can be mapped using HFS safely. HFS-guided tar-geted proximal RDN can achieve apparent BP reduction and central sympathetic inhibition.
Sources of FundingThis study was supported, in part, by research grants from the Science and Technology Committee of Yuzhong District, Chongqing, China (20110301), the Foundation for Key Research of Chongqing Municipal Health Bureau, China (2011-1-045), the Chongqing Science and Technology Commission, China (cstc2013jcyjA10066), and the Innovative Research Team of Chongqing KuanRen Hospital.
DisclosuresNone.
References 1. DiBona GF. Sympathetic nervous system and hypertension. Hypertension.
2013;61:556–560. doi: 10.1161/HYPERTENSIONAHA.111.00633. 2. Esler M. The sympathetic nervous system through the ages: from Thomas
Willis to resistant hypertension. Exp Physiol. 2011;96:611–622. doi: 10.1113/expphysiol.2010.052332.
3. Krum H, Schlaich M, Whitbourn R, Sobotka PA, Sadowski J, Bartus K, Kapelak B, Walton A, Sievert H, Thambar S, Abraham WT, Esler M. Catheter-based renal sympathetic denervation for resistant hyperten-sion: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373:1275–1281. doi: 10.1016/S0140-6736(09)60566-3.
4. Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, Bohm M. Renal sympathetic denervation in patients with treatment-resistant hy-pertension (The Symplicity HTN-2 Trial): a randomised controlled trial. Lancet. 2010; 376: 1903–1909.
5. Bhatt DL, Kandzari DE, O’Neill WW, D’Agostino R, Flack JM, Katzen BT, Leon MB, Liu M, Mauri L, Negoita M, Cohen SA, Oparil S, Rocha-Singh
K, Townsend RR, Bakris GL; SYMPLICITY HTN-3 Investigators. A con-trolled trial of renal denervation for resistant hypertension. N Engl J Med. 2014;370:1393–1401. doi: 10.1056/NEJMoa1402670.
6. Huang WC, Fang TC, Cheng JT. Renal denervation prevents and re-verses hyperinsulinemia-induced hypertension in rats. Hypertension. 1998;32:249–254.
7. Foss JD, Fink GD, Osborn JW. Reversal of genetic salt-sensitive hyperten-sion by targeted sympathetic ablation. Hypertension. 2013;61:806–811. doi: 10.1161/HYPERTENSIONAHA.111.00474.
8. MORRISSEY DM, BROOKES VS, COOKE WT. Sympathectomy in the treatment of hypertension; review of 122 cases. Lancet. 1953;1:403–408.
9. Ukena C, Cremers B, Ewen S, Böhm M, Mahfoud F. Response and non-re-sponse to renal denervation: who is the ideal candidate? EuroIntervention. 2013;9(Suppl R):R54–R57. doi: 10.4244/EIJV9SRA10.
10. Kaiser L, Beister T, Wiese A, von Wedel J, Meincke F, Kreidel F, Busjahn A, Kuck KH, Bergmann MW. Results of the ALSTER BP real-world registry on renal denervation employing the Symplicity system. EuroIntervention. 2014;10:157–165. doi: 10.4244/EIJV10I1A24.
11. Pappone C, Santinelli V, Manguso F, Vicedomini G, Gugliotta F, Augello G, Mazzone P, Tortoriello V, Landoni G, Zangrillo A, Lang C, Tomita T, Mesas C, Mastella E, Alfieri O. Pulmonary vein denervation enhances long-term benefit after circumferential ablation for paroxys-mal atrial fibrillation. Circulation. 2004;109:327–334. doi: 10.1161/01.CIR.0000112641.16340.C7.
12. Chinushi M, Izumi D, Iijima K, Suzuki K, Furushima H, Saitoh O, Furuta Y, Aizawa Y, Iwafuchi M. Blood pressure and autonomic responses to electrical stimulation of the renal arterial nerves before and after abla-tion of the renal artery. Hypertension. 2013;61:450–456. doi: 10.1161/HYPERTENSIONAHA.111.00095.
13. Sakakura K, Ladich E, Cheng Q, Otsuka F, Yahagi K, Fowler DR, Kolodgie FD, Virmani R, Joner M. Anatomic assessment of sympathetic peri-arterial renal nerves in man. J Am Coll Cardiol. 2014;64:635–643. doi: 10.1016/j.jacc.2014.03.059.
14. Wang GD, Cheng LG, Fan RX, Irwin DM, Tang SS, Peng JG, Zhang YP. Signature of balancing selection at the MC1R gene in Kunming dog popu-lations. PLoS One. 2013;8:e55469. doi: 10.1371/journal.pone.0055469.
15. Lu J, Ling Z, Chen W, Du H, Xu Y, Fan J, Long Y, Chen S, Xiao P, Liu Z, Zrenner B, Yin Y. Effects of renal sympathetic denervation using saline-irrigated radiofrequency ablation catheter on the activity of the renin-an-giotensin system and endothelin-1. J Renin Angiotensin Aldosterone Syst. 2014;15:532–539. doi: 10.1177/1470320313506480.
16. Gal P, de Jong MR, Smit JJ, Adiyaman A, Staessen JA, Elvan A. Blood pressure response to renal nerve stimulation in patients undergoing renal denervation: a feasibility study. J Hum Hypertens. 2015;29:292–295. doi: 10.1038/jhh.2014.91.
17. Pokushalov E, Romanov A, Corbucci G, Artyomenko S, Baranova V, Turov A, Shirokova N, Karaskov A, Mittal S, Steinberg JS. A randomized comparison of pulmonary vein isolation with versus without concomitant renal artery denervation in patients with refractory symptomatic atrial fi-brillation and resistant hypertension. J Am Coll Cardiol. 2012;60:1163–1170. doi: 10.1016/j.jacc.2012.05.036.
18. DiBona GF, Kopp UC. Neural control of renal function. Physiol Rev. 1997;77:75–197.
19. Kumagai H, Oshima N, Matsuura T, Iigaya K, Imai M, Onimaru H, Sakata K, Osaka M, Onami T, Takimoto C, Kamayachi T, Itoh H, Saruta T. Importance of rostral ventrolateral medulla neurons in determining efferent sympathetic nerve activity and blood pressure. Hypertens Res. 2012;35:132–141. doi: 10.1038/hr.2011.208.
20. Booth LC, Nishi EE, Yao ST, Ramchandra R, Lambert GW, Schlaich MP, May CN. Reinnervation of renal afferent and efferent nerves at 5.5 and 11 months after catheter-based radiofrequency renal de-nervation in sheep. Hypertension. 2015;65:393–400. doi: 10.1161/HYPERTENSIONAHA.114.04176.
21. Templin C, Jaguszewski M, Ghadri JR, Sudano I, Gaehwiler R, Hellermann JP, Schoenenberger-Berzins R, Landmesser U, Erne P, Noll G, Lüscher TF. Vascular lesions induced by renal nerve ablation as assessed by op-tical coherence tomography: pre- and post-procedural comparison with the Simplicity catheter system and the EnligHTN multi-electrode renal denervation catheter. Eur Heart J. 2013;34:2141–8, 2148b. doi: 10.1093/eurheartj/eht141.
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Kamsang Woo and Yuehui YinHanxuan Yang, Xinyu Hu, Chang Liu, Zhiyu Ling, Zengzhang Liu, Bernhard Zrenner,
Jiayi Lu, Zhenglong Wang, Tingquan Zhou, Shaojie Chen, Weijie Chen, Huaan Du, Zhen Tan,High-Frequency Stimulation in a Preclinical Canine Model
Selective Proximal Renal Denervation Guided by Autonomic Responses Evoked via
Print ISSN: 1941-7640. Online ISSN: 1941-7632 Copyright © 2015 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Cardiovascular Interventions
doi: 10.1161/CIRCINTERVENTIONS.115.0018472015;8:Circ Cardiovasc Interv.
http://circinterventions.ahajournals.org/content/8/6/e001847World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circinterventions.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Interventions Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Cardiovascular Interventionsin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 20, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from