
Transcatheter Aortic Valve Replacement -...
10
543 S ymptomatic aortic stenosis (AS) is a common valvu- lar heart disease that leads to a high rate of death if left untreated. 1,2 Transcatheter aortic valve implantation (TAVI) is a novel approach to treat patients with AS who are at high risk for or cannot tolerate surgical aortic valve replacement. 3,4 Several studies reported sex-specific incidence of complications and deaths after TAVI, but their results are inconsistent. Although some studies found no significant differences in 30-day mortality between men and women, 5,6 others, however, suggested a higher 30-day and 1-year mortality among the male population. 7,8 So, we performed a meta-analysis of published studies that reported sex-specific data on the incidence of post-TAVI com- plications and deaths, aiming at comprehensively and quan- titatively reviewing all the available studies and providing effect estimates. Methods Data Searches The Cochrane library and PubMed online databases (between January 1, 2002, and April 9, 2013) were searched. The following search strategy was used: (transcatheter or percutaneous or transcuta- neous or transarterial or transvascular or transfemoral or transapical or transaxillary or transaortic or transsubclavian) and (aortic valve) and (male or female or men or women or sex or gender). In addition, reference lists of pertinent articles were screened for potentially rel- evant citations missed by electronic searches. Study Selection Studies were initially screened at the level of title and abstract, and then full-length reports were retrieved for detailed evaluation. Two au- thors independently selected articles according to prespecified inclu- sion and exclusion criteria. Articles were included if they (1) reported Background—There were considerable discrepancies with regard to sex-related differences in complications and prognosis after transcatheter aortic valve implantation. Methods and Results—The Cochrane library and PubMed online databases were searched. Articles reporting sex-specific post–transcatheter aortic valve implantation complications and mortality were identified. Two authors selected studies and extracted data independently. Random- and fixed-effects models were used depending on between-study heterogeneity. There were 27 articles, a total of 9118 patients, enrolled in our systematic review and meta-analysis, including 4176 men and 4942 women. Pooled analyses suggested considerable sex-related differences in complications and early as well as midterm outcomes after transcatheter aortic valve implantation. The difference in the risk for heart block requiring permanent pacemaker implantation was noted to be significant only in the subgroup of the CoreValve-dominating studies (pooled risk ratio [RR, men versus women], 1.29; 95% confidence interval [CI], 1.13–1.47). Although men had significantly lower risks for major/life-threatening bleeding (pooled RR, 0.81; 95% CI, 0.68–0.96) and major vascular complications (pooled RR, 0.49; 95% CI, 0.37–0.66), they had poorer prognosis. In fact, male sex was associated with significantly higher risks for deaths at both 30 days (RR, 1.37; 95% CI, 1.07–1.76) and 1 year (RR, 1.30; 95% CI, 1.14–1.49). Conclusions—Although men had lower risks for major/life-threatening bleeding and major vascular complications after transcatheter aortic valve implantation, they had less favorable short-term and midterm survival. (Circ Cardiovasc Interv. 2013;6:543-551.) Key Words: aortic valve implantation ◼ aortic valve stenosis ◼ complication ◼ outcome ◼ sex characteristics ◼ transcatheter © 2013 American Heart Association, Inc. Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.113.000529 Received May 14, 2013; accepted August 23, 2013. From the Department of Cardiology, West China Hospital, Sichuan University, Chengdu, PR China. *Drs Zhao and Liao contributed equally to this work. Correspondence to Mao Chen, MD, PhD or Yuan Feng, MD, Department of Cardiology, West China Hospital, Sichuan University, 37 Guoxue St, Chengdu 610041, PR China. E-mail [email protected] or [email protected] Sex-Related Differences in Outcomes After Transcatheter Aortic Valve Implantation A Systematic Review and Meta-analysis Zhen-Gang Zhao, MD*; Yan-Biao Liao, MD*; Yong Peng, MD; Hua Chai, MD; Wei Liu, MD; Qiao Li, MD; Xin Ren, MD; Xue-Qin Wang, MS; Xiao-Lin Luo, MD; Chen Zhang, MD; Li-Hui Lu, MS; Qing-Tao Meng, MD; Chi Chen, MD; Mao Chen, MD, PhD; Yuan Feng, MD; De-Jia Huang, MD Transcatheter Aortic Valve Replacement e by guest on June 1, 2018 http://circinterventions.ahajournals.org/ Downloaded from
Transcript of Transcatheter Aortic Valve Replacement -...

543
Symptomatic aortic stenosis (AS) is a common valvu-lar heart disease that leads to a high rate of death if left
untreated.1,2 Transcatheter aortic valve implantation (TAVI) is a novel approach to treat patients with AS who are at high risk for or cannot tolerate surgical aortic valve replacement.3,4
Several studies reported sex-specific incidence of complications and deaths after TAVI, but their results are inconsistent. Although some studies found no significant differences in 30-day mortality between men and women,5,6 others, however, suggested a higher 30-day and 1-year mortality among the male population.7,8
So, we performed a meta-analysis of published studies that reported sex-specific data on the incidence of post-TAVI com-plications and deaths, aiming at comprehensively and quan-titatively reviewing all the available studies and providing effect estimates.
MethodsData SearchesThe Cochrane library and PubMed online databases (between January 1, 2002, and April 9, 2013) were searched. The following search strategy was used: (transcatheter or percutaneous or transcuta-neous or transarterial or transvascular or transfemoral or transapical or transaxillary or transaortic or transsubclavian) and (aortic valve) and (male or female or men or women or sex or gender). In addition, reference lists of pertinent articles were screened for potentially rel-evant citations missed by electronic searches.
Study SelectionStudies were initially screened at the level of title and abstract, and then full-length reports were retrieved for detailed evaluation. Two au-thors independently selected articles according to prespecified inclu-sion and exclusion criteria. Articles were included if they (1) reported
Background—There were considerable discrepancies with regard to sex-related differences in complications and prognosis after transcatheter aortic valve implantation.
Methods and Results—The Cochrane library and PubMed online databases were searched. Articles reporting sex-specific post–transcatheter aortic valve implantation complications and mortality were identified. Two authors selected studies and extracted data independently. Random- and fixed-effects models were used depending on between-study heterogeneity. There were 27 articles, a total of 9118 patients, enrolled in our systematic review and meta-analysis, including 4176 men and 4942 women. Pooled analyses suggested considerable sex-related differences in complications and early as well as midterm outcomes after transcatheter aortic valve implantation. The difference in the risk for heart block requiring permanent pacemaker implantation was noted to be significant only in the subgroup of the CoreValve-dominating studies (pooled risk ratio [RR, men versus women], 1.29; 95% confidence interval [CI], 1.13–1.47). Although men had significantly lower risks for major/life-threatening bleeding (pooled RR, 0.81; 95% CI, 0.68–0.96) and major vascular complications (pooled RR, 0.49; 95% CI, 0.37–0.66), they had poorer prognosis. In fact, male sex was associated with significantly higher risks for deaths at both 30 days (RR, 1.37; 95% CI, 1.07–1.76) and 1 year (RR, 1.30; 95% CI, 1.14–1.49).
Conclusions—Although men had lower risks for major/life-threatening bleeding and major vascular complications after transcatheter aortic valve implantation, they had less favorable short-term and midterm survival. (Circ Cardiovasc Interv. 2013;6:543-551.)
Key Words: aortic valve implantation ◼ aortic valve stenosis ◼ complication ◼ outcome ◼ sex characteristics ◼ transcatheter
© 2013 American Heart Association, Inc.
Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.113.000529
Received May 14, 2013; accepted August 23, 2013.From the Department of Cardiology, West China Hospital, Sichuan University, Chengdu, PR China.*Drs Zhao and Liao contributed equally to this work.Correspondence to Mao Chen, MD, PhD or Yuan Feng, MD, Department of Cardiology, West China Hospital, Sichuan University, 37 Guoxue St,
Chengdu 610041, PR China. E-mail [email protected] or [email protected]
Sex-Related Differences in Outcomes After Transcatheter Aortic Valve Implantation
A Systematic Review and Meta-analysis
Zhen-Gang Zhao, MD*; Yan-Biao Liao, MD*; Yong Peng, MD; Hua Chai, MD; Wei Liu, MD; Qiao Li, MD; Xin Ren, MD; Xue-Qin Wang, MS; Xiao-Lin Luo, MD; Chen Zhang, MD;
Li-Hui Lu, MS; Qing-Tao Meng, MD; Chi Chen, MD; Mao Chen, MD, PhD; Yuan Feng, MD; De-Jia Huang, MD
Transcatheter Aortic Valve Replacement
Original Article
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

544 Circ Cardiovasc Interv October 2013
the number or incidence of ≥1 complication and death for men and women separately; (2) used the standardized definition of complica-tions according to the Valve Academic Research Consortium criteria9; and (3) were human studies and published in English. Abstracts, let-ters, editorials, and reviews were excluded.
Data ExtractionTwo authors extracted data independently. A table was designed to record data of eligible studies on the year of publication, first au-thor, outcome definition, follow-up duration, number of men and women, prosthetic valve type, baseline characteristics, and number of complications and deaths. Baseline characteristics included age, body mass index, hypertension, diabetes mellitus, chronic obstruc-tive pulmonary disease, previous coronary artery disease, New York Heart Association class III or IV, previous myocardial infarction, previous percutaneous coronary intervention, previous peripheral vascular disease, previous cerebrovascular disease, atrial fibrillation, logistic European system for cardiac operative risk evaluation, mean aortic gradient, and vascular access. Complications included major/life-threatening bleeding, major vascular complications, permanent pacemaker implantation (PPMI), and stroke. Mortality included 30-day and 1-year death.
Data Synthesis and AnalysesThe risk ratio (RR) of men compared with women, with regard to post-TAVI complications and deaths at 30 days and 1 year, was calculated and synthesized using the Mantel–Haenszel method in the RevMan software version 5.10 (The Nordic Cochrane Centre, Copenhagen, Denmark). Heterogeneity was assessed by calculating the I2 statistic and its P value. A fixed-effects model was selected in the case of an I2 <50% and a corresponding P>0.1; otherwise, a random-effects model was used to obtain the combined effect estimates. Two-sided P<0.05 were considered statistically significant.
Sensitivity and Publication Bias AnalysesSensitivity analyses were performed by excluding 1 study at a time in case that ≥5 studies were included and by discarding smaller studies
(reporting no more than 100 successful TAVI procedures), where ap-plicable, using the STATA software version 12.0 (StataCorp, College Station, TX). Because the CoreValve (Medtronic Inc) is associated with a much higher risk for heart block requiring PPMI than the Edwards valve (Edwards Lifesciences LLC), an additional subgroup analysis was performed for this outcome according to the predomi-nant type of valve (CoreValve or Edwards valve) that was used in each study.
Publication bias was detected by Begg and Egger tests. Two-sided P<0.05 were considered statistically significant. In addition, funnel plots were constructed to inspect the symmetry visually.
Outcome Quality AssessmentGrading of Recommendations Assessment, Development, and Evaluation system evaluation was performed to grade the quality of evidence according to the Grading of Recommendations Assessment, Development, and Evaluation handbook. The GRADEpro software version 3.2 was used. We got the assessment by judging the design of study, risk of bias, inconsistency, and imprecision.
Present systematic review and meta-analysis were conducted and reported according to the recommendations of the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group.10
ResultsLiterature Search and Study SelectionThe process of study selection is illustrated in Figure 1. There were 1679 citations after removing duplicates. A total of 27 full-text articles were eligible for our systematic review and meta-analysis.5–8,11–33 These studies included 4176 men and 4942 women for the comparison of sex-related differences in complications and mortality after TAVI. Although the 2 stud-ies overlapped in patient population, they provided different outcomes. One reported 30-day mortality,22 and the other pro-vided 1-year mortality.33
Study and Patient CharacteristicsThe characteristics of the included studies are presented in Table 1. Of the 27 full-length reports, only 5 detailed the base-line data of men and women separately.5–8,26 The pooled sex-specific baseline characteristics based on these studies showed that men were more likely to experience diabetes mellitus, chronic obstructive pulmonary disease, coronary artery dis-ease, previous myocardial infarction, previous percutaneous
WhAT IS KNOWN
•Transcatheter aortic valve implantation has been shown to improve symptoms and survival effectively in surgically high-risk patients with severe aortic ste-nosis but is associated with specific complications.
•Previous reports were considerably discrepant in terms of the sex-related differences in complication profiles and prognosis after transcatheter aortic valve implantation.
WhAT ThE STuDy ADDS
•This study systematically reviewed and pooled the currently published sex-specific data on outcomes after transcatheter aortic valve implantation.
•The pooled analyses suggested significant sex- related differences in this regard.
•Men were less likely to experience major/life- threatening bleeding and major vascular complica-tions, but they had significantly higher risks for heart block requiring permanent pacemaker implantation and early as well as late deaths after transcatheter aortic valve implantation.
Potentially relevant citations identifiedusing predefined search strategy
(n=1679)
Citations left after removing duplicates(n=1644)
Studies excluded afterevaluating at the level of title
and abstract (n=1523)
Studies included in present meta-analysis(n=27)
Full-length articles retrieved for detailedeligibility assessment
(n=121)
Studies excluded after full review (n=94)
No full-length article (n=2)No sex-specific data (n=91)Sample size <10 (n=1)
Figure 1. Flow diagram of study selection.
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Zhao et al Sex-Specific Outcomes After TAVI 545
Table 1. Characteristics of Included Studies
First Author Year Country Follow-up Sex n
Valve Approach
EV/MCV (n/N) Ta/TA (n/N)
Buja et al5 2013 Italy 1 y Male 291 0/291 291/0
Female 368 0/368 368/0
Hayashida et al6 2012 France 1 y Male 129 102/27 85/44
Female 131 120/11 92/39
Buchanan et al7 2011 Italy 1 y Male 159 88/71 150/9
Female 146 97/49 133/13
Humphries et al8 2012 Canada 2 y Male 312 622/19 193/119
Female 329 158/171
Ye et al11 2009 Canada 1 y Male 13 13/0 0/13
Female 13 13/0 0/13
Rodes-Cabau et al12 2010 Canada 1 y Male 152 152/0 91/61
Female 187 187/0 71/116
Sinning et al13 2010 Germany 1 y Male 37 0/37 37/0
Female 40 0/40 40/0
Rodes-Cabau et al14 2011 Canada 1 y Male 43 43/0 21/22
Female 58 58/0 17/41
Tamburino et al15 2011 Italy 1 y Male 292 0/292 292/0
Female 371 0/371 371/0
Amabile et al16 2012 France 1 y Male 80 132/39 139/32
Female 91
Bagur et al17 2012 Canada NA Male 176 176/0 223/188
Female 235 235/0
Genereux et al18 2012 America 1 y Male 227 227/0 227/0
Female 192 192/0 192/0
Gotzmann et al19 2012 Germany 1 y Male 91 0/91 91/0
Female 107 0/107 107/0
Houthuizen et al20 2012 The Netherlands 1 y Male 360 292/387 473/206
Female 319
Lange et al21 2012 Germany 6 mo Male 155 127/293 290/130
Female 265
Lauten et al22 2012 Germany 30 d Male 544 249/1053 1179/123
Female 758
Munoz-Garcia et al23 (PPM*)
2012 Spain 30 d Male 65 0/65 65/0
Female 109 0/109 109/0
Munoz-Garcia et al24 2012 Spain 1 y Male 50 0/50 50/0
Female 83 0/83 83/0
Seiffert et al25 2012 Germany 1 y Male 145 116/29 68/77
Female 181 165/16 81/100
Stangl et al26 2012 Germany 3 mo Male 42 9/33 42/0
Female 58 8/50 58/0
Van Mieghem et al27 2012 The Netherlands, France
30 d Male 519 487/499 519/0
Female 467 467/0
Yong et al28 2012 The Netherlands 1 y Male 47 0/47 47/0
Female 72 0/72 72/0
Zhao et al29 2012 France 30 d Male 24 24/0 13/11
Female 24 24/0 15/9
Elhmidi et al30 2013 Germany 1 y Male 139 112/261 NA
Female 234(Continued)
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

546 Circ Cardiovasc Interv October 2013
coronary intervention, and peripheral vascular disease, although there were no significant differences in the mean logistic European system for cardiac operative risk evaluation between the 2 sexes (Table 2).
Sex Differences in Complications After TAVI
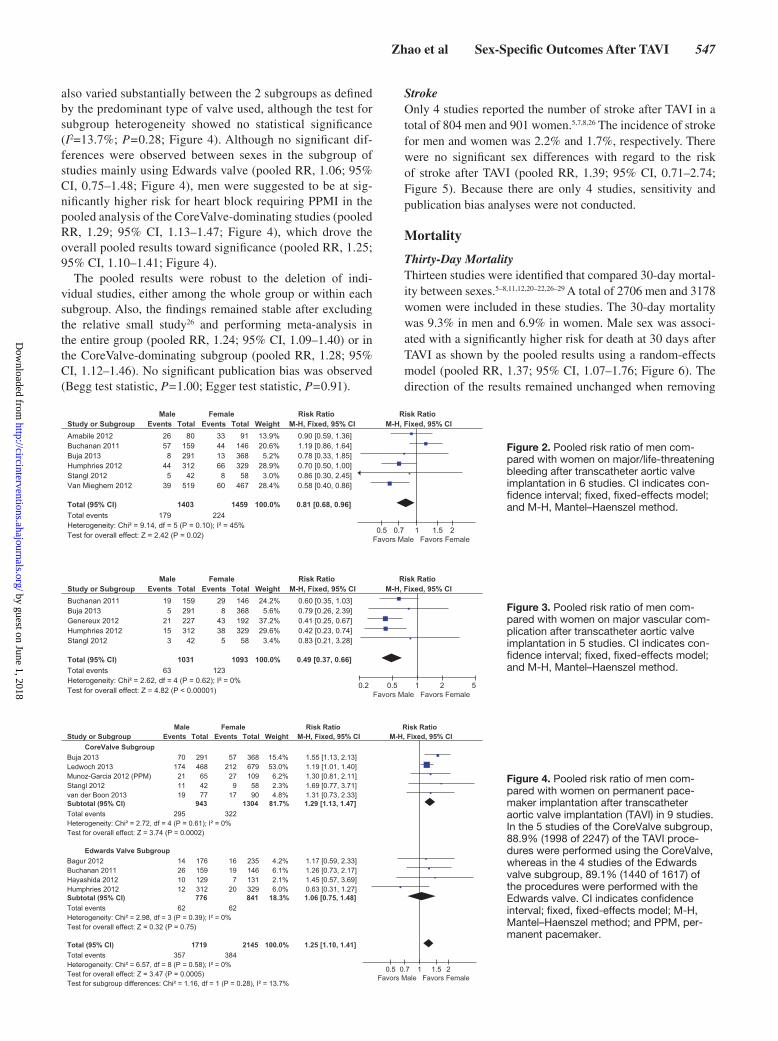
Major/Life-Threatening BleedingOnly 6 studies were eligible for the pooled analysis of sex dif-ferences in this outcome.5,7,8,16,26,27 These studies enrolled 1403 men and 1459 women, and the overall incidence of major/life-threatening bleeding was 12.8% and 15.3%, respectively. Men had a significantly lower risk for major/life-threatening bleeding (pooled RR, 0.81; 95% confidence interval [CI], 0.68–0.96; Figure 2). The pooled results remained stable after excluding the study, with no more than 100 successful TAVI procedures (pooled RR, 0.80; 95% CI, 0.67–0.96).26 However, pooled RR became insignificant on deletion of the studies by Humphries et al8 (pooled RR, 0.85; 95% CI, 0.69–1.04) and Van Mieghem et al27 (pooled RR, 0.89; 95% CI, 0.73–1.09). The Begg and Egger plot suggested no sig-nificant publication bias (Begg test statistic, P=1.00; Egger test statistic, P=0.81).
Major Vascular ComplicationOnly 5 studies evaluated the outcome of major vascular com-plications by sex.5,7,8,18,26 The occurrence rate of major vas-cular complication in men and women was 6.1% and 11.3% in the 5 eligible studies incorporating 1031 men and 1093 women. Pooled results suggested a significantly lower risk of major vascular complication in men (pooled RR, 0.49; 95% CI, 0.37–0.66; Figure 3). The results remained stable when omitting individual studies or the study with a relatively small sample size (pooled RR, 0.48; 95% CI, 0.36–0.65).26 No sig-nificant publication bias was observed (Begg test statistic, P=0.46; Egger test statistic, P=0.17).
Permanent Pacemaker ImplantationWe identified 9 studies that reported sex-specific incidence of PPMI.5–8,17,23,26,31,32 Data on 1719 men and 2145 women were available for analysis. In studies that predominantly used the CoreValve, heart block requiring PPMI was a com-mon complication after TAVI, with an incidence of 31.3% and 24.7% for men and women, respectively.5,23,26,31,32 How-ever, the rate of PPMI was much lower in studies mainly using Edwards valve, 8.0% in men and 7.4% in women.6–8,17 The pooled results of sex-related differences in this outcome
Table 2. Pooled Characteristics of Men and Women
Baseline Characteristics Men Women P Value
Age 80.6±1.6 (n=933) 82.1±1.2 (n=1032) <0.001
BMI 26±0.4 (n=333) 26.1±0.5 (n=335) 0.78
Hypertension, n/total (%) 564/774 (72.9) 711/886 (80.2) 0.31
Diabetes mellitus, n/total (%) 292/933 (31.3) 274/1032 (26.6) 0.03
COPD, n/total (%) 306/933 (38.6) 250/1032 (24.2) 0.006
NYHA class III or IV, n/total (%) 671/891 (75.3) 778/974 (79.9) 0.01
CAD, n/total (%) 588/774 (76.0) 459/886 (51.8) <0.001
Previous MI, n/total (%) 320/933 (34.3) 201/1032 (19.5) <0.001
Previous PCI, n/total (%) 411/933 (44.1) 282/1032 (27.3) <0.001
PVD, n/total (%) 257/774 (33.2) 189/886 (21.3) 0.02
Previous stroke, n/total (%) 140/933 (15.0) 120/1032 (11.6) 0.06
Atrial fibrillation, n/total (%) 172/645 (26.7) 183/755 (24.2) 0.50
Logistic EuroSCORE 24.0±1.3 (n=621) 22.7±1.4 (n=703) 0.06
Data are presented as number (percentage) or mean±SD. BMI indicates body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; EuroSCORE, European system for cardiac operative risk evaluation; MI, myocardial infarction; NYHA, New York Heart Association; PCI, percutaneous coronary intervention; and PVD, peripheral vascular disease.
Ledwoch et al31 2013 Germany 30 d Male 468 232/915 1034/113
Female 679
van der Boon et al32 2013 The Netherlands 1 y Male 77 0/77 167/0
Female 90 0/90
Zahn et al33 2013 Germany 1 y Male 547 244/1074 1203/115
Female 771
EV indicates Edwards valve; MCV, Medtronic CoreValve; NA, not available; PPM, permanent pacemaker; Ta, transarterial; and TA, transapical.*Included in the pooled analysis of the outcome of heart block requiring PPM.
Table 1. Continued
First Author Year Country Follow-up Sex n
Valve Approach
EV/MCV (n/N) Ta/TA (n/N)
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
Zhao et al Sex-Specific Outcomes After TAVI 547
also varied substantially between the 2 subgroups as defined by the predominant type of valve used, although the test for subgroup heterogeneity showed no statistical significance (I2=13.7%; P=0.28; Figure 4). Although no significant dif-ferences were observed between sexes in the subgroup of studies mainly using Edwards valve (pooled RR, 1.06; 95% CI, 0.75–1.48; Figure 4), men were suggested to be at sig-nificantly higher risk for heart block requiring PPMI in the pooled analysis of the CoreValve-dominating studies (pooled RR, 1.29; 95% CI, 1.13–1.47; Figure 4), which drove the overall pooled results toward significance (pooled RR, 1.25; 95% CI, 1.10–1.41; Figure 4).
The pooled results were robust to the deletion of indi-vidual studies, either among the whole group or within each subgroup. Also, the findings remained stable after excluding the relative small study26 and performing meta-analysis in the entire group (pooled RR, 1.24; 95% CI, 1.09–1.40) or in the CoreValve-dominating subgroup (pooled RR, 1.28; 95% CI, 1.12–1.46). No significant publication bias was observed (Begg test statistic, P=1.00; Egger test statistic, P=0.91).
StrokeOnly 4 studies reported the number of stroke after TAVI in a total of 804 men and 901 women.5,7,8,26 The incidence of stroke for men and women was 2.2% and 1.7%, respectively. There were no significant sex differences with regard to the risk of stroke after TAVI (pooled RR, 1.39; 95% CI, 0.71–2.74; Figure 5). Because there are only 4 studies, sensitivity and publication bias analyses were not conducted.
Mortality
Thirty-Day MortalityThirteen studies were identified that compared 30-day mortal-ity between sexes.5–8,11,12,20–22,26–29 A total of 2706 men and 3178 women were included in these studies. The 30-day mortality was 9.3% in men and 6.9% in women. Male sex was associ-ated with a significantly higher risk for death at 30 days after TAVI as shown by the pooled results using a random-effects model (pooled RR, 1.37; 95% CI, 1.07–1.76; Figure 6). The direction of the results remained unchanged when removing
Figure 2. Pooled risk ratio of men com-pared with women on major/life-threatening bleeding after transcatheter aortic valve implantation in 6 studies. CI indicates con-fidence interval; fixed, fixed-effects model; and M-H, Mantel–Haenszel method.
Figure 3. Pooled risk ratio of men com-pared with women on major vascular com-plication after transcatheter aortic valve implantation in 5 studies. CI indicates con-fidence interval; fixed, fixed-effects model; and M-H, Mantel–Haenszel method.
Figure 4. Pooled risk ratio of men com-pared with women on permanent pace-maker implantation after transcatheter aortic valve implantation (TAVI) in 9 studies. In the 5 studies of the CoreValve subgroup, 88.9% (1998 of 2247) of the TAVI proce-dures were performed using the CoreValve, whereas in the 4 studies of the Edwards valve subgroup, 89.1% (1440 of 1617) of the procedures were performed with the Edwards valve. CI indicates confidence interval; fixed, fixed-effects model; M-H, Mantel–Haenszel method; and PPM, per-manent pacemaker.
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

548 Circ Cardiovasc Interv October 2013
individual studies from the analysis or after discarding the 3 smaller studies (pooled RR, 1.35; 95% CI, 1.03–1.76).11,26,29 There was no evidence of significant publication bias (Begg test statistic, P=1.00; Egger test statistic, P=0.89).
One-Year MortalityA total of 16 studies enrolling 3013 men and 3649 women were eligible for meta-analysis.5–8,12–16,18–20,24,25,30,33 One-year mortality of men and women was 22.0% and 16.9%, respectively. Pooled analysis using a random-effects model showed that men had significantly higher 1-year mortality (pooled RR, 1.30; 95% CI, 1.14–1.49; Figure 7). The robustness of the results was con-firmed by the sensitivity analysis of deleting individual studies or omitting the 2 smaller studies (pooled RR, 1.29; 95% CI, 1.11–1.49).13,14 No significant publication bias was noted (Begg test statistic, P=0.56; Egger test statistic, P=0.98).
Grading of Recommendations Assessment, Development, and Evaluation System Evaluation Because all the 27 studies were observational studies, the evi-dence of quality of the complication and mortality outcomes
was moderate, except that the quality of major vascular com-plication after TAVI was high and quality of stroke was low (Table 3).
DiscussionThe major findings of present meta-analysis were that there were significant sex differences in terms of the risks for major/life-threatening bleeding, major vascular complication, 30-day mortality, and 1-year mortality after TAVI. Sex-related differences in the risk for heart block requiring PPMI were noted to be significant only in the subgroup of the CoreValve-dominating studies (pooled RR [men versus women], 1.29; 95% CI, 1.13–1.47). Although men were less susceptible to major/life-threatening bleeding (pooled RR, 0.81; 95% CI, 0.68–0.96) and major vascular complication (pooled RR, 0.49; 95% CI, 0.37–0.66), they had significantly higher risks for 30-day (pooled RR, 1.37; 95% CI, 1.07–1.76) and 1-year deaths (pooled RR, 1.30; 95% CI, 1.14–1.49).
Our findings were in line with those from the sex-specific analysis of the Placement of AoRTic TraNscathetER Valve
Figure 5. Pooled risk ratio of men com-pared with women on stroke after trans-catheter aortic valve implantation in 4 studies. CI indicates confidence interval; fixed, fixed-effects model; and M-H, Mantel–Haenszel method.
Figure 6. Pooled risk ratio of men com-pared with women on 30-day mortality after transcatheter aortic valve implantation in 13 studies. CI indicates confidence interval; M-H, Mantel–Haenszel method; and ran-dom, random-effects model.
Figure 7. Pooled risk ratio of men com-pared with women on 1-year mortality after transcatheter aortic valve implantation in 16 studies. CI indicates confidence interval; M-H, Mantel–Haenszel method; and ran-dom, random-effects model.
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Zhao et al Sex-Specific Outcomes After TAVI 549
Trial (PARTNER), which incorporated a total of 1334 men and 1231 women enrolled in either the randomized or non-randomized continued evaluation phase.34 In that study, male sex was also observed to be associated with a significantly higher incidence of comorbidities (coronary artery disease [87.6% versus 67.5%], prior coronary artery bypass graft [59.3% versus 24.4%], peripheral vascular disease [46.4% versus 39.4%], chronic kidney disease [20.6% versus 12.6%; P<0.001 for all]) and less favorable late outcomes (1-year mortality [24.3% versus 17.6%; P=0.0005], 2-year mortality [35.3% versus 29.6%; P=0.002]).
Given that female sex was a risk factor for major vascular complication and major/life-threatening bleeding, why did women have a better prognosis? This phenomenon could be explained from 3 aspects. (1) Although female sex was a risk factor of some complications (such as major vascular com-plication), these complications were not the major causes of deaths. Besides, another study found no significant differ-ences in prognosis between patients with and without major vascular complication.16 (2) The sex differences in the patho-physiological characteristics might serve as a possible under-lying mechanism. Several studies have demonstrated cardiac remodeling and fibrosis to be less prevalent and less severe in women with AS than those in men with AS, which might be related to the lower expression of collagen I, collagen III, metal matrix proteinase-2, and metal matrix proteinase-9 in women.35–37 Furthermore, AS has recently been demonstrated to share some common pathogenic bases with atherosclero-sis.38,39 As female sex is a protective factor for atherosclerosis, this may also affect AS. (3) The unbalanced baseline risk pro-files may be an important explanation. As shown in Table 2, diabetes mellitus, chronic obstructive pulmonary disease, and
atherosclerotic diseases were much more prevalent among the male patient population. The higher burden of these morbidi-ties in men may adversely affect their survival after TAVI.
Our meta-analysis has several limitations. (1) Although great care was taken in selecting studies, the possibility of duplicated data synthesis as a result of their overlap in the patients enrolled cannot be completely ruled out. (2) The sex differences in long-term prognosis after TAVI could not be assessed because of the lack of studies. (3) The power of the Egger and Begg tests for funnel plot asymmetry is too low to distinguish chance from real asymmetry when there are no more than 10 studies eligible for the pooled analysis. Thus, the possibility of potential publication bias could not be ruled out, particularly from the meta-analyses of the bleeding, vascular complication, and pacemaker outcomes. (4) Because only 5 studies reported sex-specific baseline characteristics and the patient-level data were not available, the effects of potential mediators (comorbidities) could not be assessed. However, the unadjusted summary RRs presented in current meta-analyses can be interpreted as the total causal effects of sex, which might be more clinically relevant. (5) The sex-related differ-ences in post-TAVI outcomes, as observed in present meta-analyses, are not large enough to be used alone in treatment directing or patient counseling. Nevertheless, sex may be a useful part of the risk stratification model of TAVI, at least for major vascular complication and possibly for early as well as midterm mortality.
In conclusion, there were significant sex differences in complications and prognosis after TAVI. Although men had lower risks for major/life-threatening bleeding and major vas-cular complication after TAVI, they had less favorable short-term and midterm survival.
Table 3. Summary of GRADE Evidence Profile
Quality Assessment
Quality*No. of Studies Design Serious Risk of Bias Serious Inconsistency Serious Indirectness Serious Imprecision
Major/life-threatening bleeding after TAVI
6 Observational studies Possible† No No No Moderate
Major vascular complication after TAVI
5 Observational studies Unlikely‡ No No No High
New pacemaker implantation after TAVI
6 Observational studies Possible† No No No Moderate
Stroke after TAVI
4 Observational studies Possible† No No Yes§ Low
30-d mortality after TAVI
14 Observational studies Possible† No No No Moderate
1-y mortality after TAVI
17 Observational studies Possible† No No No Moderate
CI indicates confidence interval; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; RR, risk ratio; and TAVI, transcatheter aortic valve implantation.
*High quality indicates that further research is unlikely to change our confidence in the estimate of effect; moderate quality indicates that further research is likely to have an important effect on our confidence in the estimate of effect and may change the estimate; low quality indicates that further research is likely to have an important effect on our confidence in the estimate of effect and is likely to change the estimate.
†Although the unadjusted RRs represented the total causal effects of sex and thus cannot be confounded by the differences in comorbidity profiles, which were also driven by sex, the potential effects of exogenous factors that were independent of sex cannot be ruled out.
‡A value of RR <0.5 with statistical significance indicates that it is unlikely to be seriously biased.§The 95% CI for the pooled RR showed a wide variety.
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

550 Circ Cardiovasc Interv October 2013
DisclosuresNone.
References 1. Iung B, Baron G, Butchart EG, Delahaye F, Gohlke-Barwolf C, Levang
OW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24:1231–1243.
2. Varadarajan P, Kapoor N, Bansal RC, Pai RG. Clinical profile and natural history of 453 nonsurgically managed patients with severe aortic stenosis. Ann Thorac Surg. 2006;82:2111–2115.
3. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ; PARTNER Trial Investigators. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–2198.
4. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S; PARTNER Trial Investigators. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607.
5. Buja P, Napodano M, Tamburino C, Petronio AS, Ettori F, Santoro G, Ussia GP, Klugmann S, Bedogni F, Ramondo A, Maisano F, Marzocchi A, Poli A, Gasparetto V, Antoniucci D, Colombo A, Tarantini G; Italian Multicenter CoreValve Registry Investigators. Comparison of variables in men versus women undergoing transcatheter aortic valve implantation for severe aortic stenosis (from Italian Multicenter CoreValve registry). Am J Cardiol. 2013;111:88–93.
6. Hayashida K, Morice MC, Chevalier B, Hovasse T, Romano M, Garot P, Farge A, Donzeau-Gouge P, Bouvier E, Cormier B, Lefevre T. Sex-related differences in clinical presentation and outcome of transcatheter aortic valve implantation for severe aortic stenosis. J Am Coll Cardiol. 2012;59:566–571.
7. Buchanan GL, Chieffo A, Montorfano M, Maisano F, Latib A, Godino C, Cioni M, Gullace MA, Franco A, Gerli C, Alfieri O, Colombo A. The role of sex on VARC outcomes following transcatheter aortic valve implantation with both Edwards SAPIEN and Medtronic CoreValve ReValving System(R) devices: the Milan registry. EuroIntervention. 2011;7:556–563.
8. Humphries KH, Toggweiler S, Rodes-Cabau J, Nombela-Franco L, Dumont E, Wood DA, Willson AB, Binder RK, Freeman M, Lee MK, Gao M, Izadnegahdar M, Ye J, Cheung A, Webb JG. Sex differences in mortal-ity after transcatheter aortic valve replacement for severe aortic stenosis. J Am Coll Cardiol. 2012;60:882–886.
9. Leon MB, Piazza N, Nikolsky E, Blackstone EH, Cutlip DE, Kappetein AP, Krucoff MW, Mack M, Mehran R, Miller C, Morel MA, Petersen J, Popma JJ, Takkenberg JJ, Vahanian A, van Es GA, Vranckx P, Webb JG, Windecker S, Serruys PW. Standardized endpoint definitions for transcath-eter aortic valve implantation clinical trials: a consensus report from the Valve Academic Research Consortium. Eur Heart J. 2011;32:205–217.
10. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012.
11. Ye J, Cheung A, Lichtenstein SV, Altwegg LA, Wong DR, Carere RG, Thompson CR, Moss RR, Munt B, Pasupati S, Boone RH, Masson JB, Al Ali A, Webb JG. Transapical transcatheter aortic valve implan-tation: 1-year outcome in 26 patients. J Thorac Cardiovasc Surg. 2009;137:167–173.
12. Rodes-Cabau J, Webb JG, Cheung A, Ye J, Dumont E, Feindel CM, Osten M, Natarajan MK, Velianou JL, Martucci G, DeVarennes B, Chisholm R, Peterson MD, Lichtenstein SV, Nietlispach F, Doyle D, DeLarochelliere R, Teoh K, Chu V, Dancea A, Lachapelle K, Cheema A, Latter D, Horlick E. Transcatheter aortic valve implantation for the treatment of severe symptomatic aortic stenosis in patients at very high or prohibitive surgi-cal risk: acute and late outcomes of the multicenter Canadian experience. J Am Coll Cardiol. 2010;55:1080–1090.
13. Sinning JM, Ghanem A, Steinhauser H, Adenauer V, Hammerstingl C, Nickenig G, Werner N. Renal function as predictor of mortality in pa-tients after percutaneous transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2010;3:1141–1149.
14. Rodes-Cabau J, Gutierrez M, Bagur R, De Larochelliere R, Doyle D, Cote M, Villeneuve J, Bertrand OF, Larose E, Manazzoni J, Pibarot P, Dumont E. Incidence, predictive factors, and prognostic value of myocardial injury following uncomplicated transcatheter aortic valve implantation. J Am Coll Cardiol. 2011;57:1988–1999.
15. Tamburino C, Capodanno D, Ramondo A, Petronio AS, Ettori F, Santoro G, Klugmann S, Bedogni F, Maisano F, Marzocchi A, Poli A, Antoniucci D, Napodano M, De Carlo M, Fiorina C, Ussia GP. Incidence and pre-dictors of early and late mortality after transcatheter aortic valve im-plantation in 663 patients with severe aortic stenosis. Circulation. 2011;123:299–308.
16. Amabile N, Azmoun A, Ghostine S, Ramadan R, Haddouche Y, Raoux F, To NT, Troussier X, Nottin R, Caussin C. Incidence, predictors and prog-nostic value of serious hemorrhagic complications following transcatheter aortic valve implantation. Int J Cardiol. 2013;168:151–156.
17. Bagur R, Rodes-Cabau J, Gurvitch R, Dumont E, Velianou JL, Manazzoni J, Toggweiler S, Cheung A, Ye J, Natarajan MK, Bainey KR, DeLarochelliere R, Doyle D, Pibarot P, Voisine P, Cote M, Philippon F, Webb JG. Need for permanent pacemaker as a complication of transcath-eter aortic valve implantation and surgical aortic valve replacement in elderly patients with severe aortic stenosis and similar baseline electrocar-diographic findings. JACC Cardiovasc Interv. 2012;5:540–551.
18. Genereux P, Webb JG, Svensson LG, Kodali SK, Satler LF, Fearon WF, Davidson CJ, Eisenhauer AC, Makkar RR, Bergman GW, Babaliaros V, Bavaria JE, Velazquez OC, Williams MR, Hueter I, Xu K, Leon MB. Vascular complications after transcatheter aortic valve replacement: in-sights from the PARTNER (Placement of AoRTic TraNscathetER Valve) trial. J Am Coll Cardiol. 2012;60:1043–1052.
19. Gotzmann M, Korten M, Bojara W, Lindstaedt M, Rahlmann P, Mugge A, Ewers A. Long-term outcome of patients with moderate and severe pros-thetic aortic valve regurgitation after transcatheter aortic valve implanta-tion. Am J Cardiol. 2012;110:1500–1506.
20. Houthuizen P, Van Garsse LA, Poels TT, de Jaegere P, van der Boon RM, Swinkels BM, Ten Berg JM, van der Kley F, Schalij MJ, Baan J Jr, Cocchieri R, Brueren GR, van Straten AH, den Heijer P, Bentala M, van Ommen V, Kluin J, Stella PR, Prins MH, Maessen JG, Prinzen FW. Left bundle-branch block induced by transcatheter aortic valve implantation increases risk of death. Circulation. 2012;126:720–728.
21. Lange R, Bleiziffer S, Mazzitelli D, Elhmidi Y, Opitz A, Krane M, Deutsch MA, Ruge H, Brockmann G, Voss B, Schreiber C, Tassani P, Piazza N. Improvements in transcatheter aortic valve implantation outcomes in lower surgical risk patients: a glimpse into the future. J Am Coll Cardiol. 2012;59:280–287.
22. Lauten A, Zahn R, Horack M, Sievert H, Linke A, Ferrari M, Harnath A, Grube E, Gerckens U, Kuck KH, Sack S, Senges J, Figulla HR; German Transcatheter Aortic Valve Interventions Registry Investigators. Transcatheter aortic valve implantation in patients with low-flow, low-gradient aortic stenosis. JACC Cardiovasc Interv. 2012;5:552–559.
23. Munoz-Garcia AJ, Hernandez-Garcia JM, Jimenez-Navarro MF, Alonso-Briales JH, Dominguez-Franco AJ, Fernandez-Pastor J, Pena Hernandez J, Barrera Cordero A, Alzueta Rodriguez J, de Teresa-Galvan E. Factors predicting and having an impact on the need for a permanent pacemaker after CoreValve prosthesis implantation using the new Accutrak delivery catheter system. JACC Cardiovasc Interv. 2012;5:533–539.
24. Munoz-Garcia AJ, Hernandez-Garcia JM, Jimenez-Navarro MF, Alonso-Briales JH, Dominguez-Franco AJ, Rodriguez-Bailon I, Molina-Mora MJ, Hernandez-Rodriguez P, Such-Martinez M, de Teresa-Galvan E. Survival and predictive factors of mortality after 30 days in patients treated with percutaneous implantation of the CoreValve aortic prosthesis. Am Heart J. 2012;163:288–294.
25. Seiffert M, Schnabel R, Conradi L, Diemert P, Schirmer J, Koschyk D, Linder M, Kersten JF, Grosser A, Wilde S, Blankenberg S, Reichenspurner H, Baldus S, Treede H. Predictors and outcomes after transcatheter aor-tic valve implantation using different approaches according to the Valve Academic Research Consortium definitions. Catheter Cardiovasc Interv. November 21, 2012. doi: 10.1002/ccd.24751.: http://onlinelibrary.wiley.com/doi/10.1002/ccd.24751/full. Accessed April 15, 2013.
26. Stangl V, Baldenhofer G, Knebel F, Zhang K, Sanad W, Spethmann S, Grubitzsch H, Sander M, Wernecke KD, Baumann G, Stangl K, Laule M. Impact of gender on three-month outcome and left ventricular remodeling after transfemoral transcatheter aortic valve implantation. Am J Cardiol. 2012;110:884–890.
27. Van Mieghem NM, Tchetche D, Chieffo A, Dumonteil N, Messika-Zeitoun D, van der Boon RM, Vahdat O, Buchanan GL, Marcheix B, Himbert D, Serruys PW, Fajadet J, Colombo A, Carrie D, Vahanian A,
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from

Zhao et al Sex-Specific Outcomes After TAVI 551
de Jaegere PP. Incidence, predictors, and implications of access site com-plications with transfemoral transcatheter aortic valve implantation. Am J Cardiol. 2012;110:1361–1367.
28. Yong ZY, Wiegerinck EM, Boerlage-van Dijk K, Koch KT, Vis MM, Bouma BJ, Henriques JP, Cocchieri R, Piek JJ, de Mol BA, Baan J Jr. Predictors and prognostic value of myocardial injury during transcatheter aortic valve implantation. Circ Cardiovasc Interv. 2012;5:415–423.
29. Zhao QM, Lognone T, Ivascau C, Sabatier R, Roule V, Dahdouh Z, Massetti M, Grollier G. Procedural results and 30-day clinical events analysis fol-lowing Edwards transcatheter aortic valve implantation in 48 consecutive patients: initial experience. Chin Med J (Engl). 2012;125:2807–2810.
30. Elhmidi Y, Bleiziffer S, Piazza N, Ruge H, Krane M, Deutsch MA, Hettich I, Voss B, Mazzitelli D, Lange R. The evolution and prognostic value of N-terminal brain natriuretic peptide in predicting 1-year mortal-ity in patients following transcatheter aortic valve implantation. J Invasive Cardiol. 2013;25:38–44.
31. Ledwoch J, Franke J, Gerckens U, Kuck KH, Linke A, Nickenig G, Krulls-Munch J, Vohringer M, Hambrecht R, Erbel R, Richardt G, Horack M, Zahn R, Senges J, Sievert H. Incidence and predictors of permanent pace-maker implantation following transcatheter aortic valve implantation: analysis from the German transcatheter aortic valve interventions regis-try. Catheter Cardiovasc Interv. March 8, 2013. doi: 10.1002/ccd.24915.: http://onlinelibrary.wiley.com/doi/10.1002/ccd.24915/full. Accessed April 15, 2013.
32. van der Boon RM, Van Mieghem NM, Theuns DA, Nuis RJ, Nauta ST, Serruys PW, Jordaens L, van Domburg RT, de Jaegere PP. Pacemaker dependency after transcatheter aortic valve implanta-tion with the self-expanding Medtronic CoreValve System. Int J Cardiol. January 4, 2013. doi: 10.1016/j.ijcard.2012.11.115.:
http://www.internationaljournalofcardiology.com/article/S0167-5273%2812%2901628-2. Accessed April 15, 2013.
33. Zahn R, Gerckens U, Linke A, Sievert H, Kahlert P, Hambrecht R, Sack S, Abdel-Wahab M, Hoffmann E, Schiele R, Schneider S, Senges J; German Transcatheter Aortic Valve Interventions-Registry Investigators. Predictors of one-year mortality after transcatheter aortic valve implantation for se-vere symptomatic aortic stenosis. Am J Cardiol. 2013;112:272–279.
34. Kodali SK, Williams M, Humphries K, Cohen D, Nkomo V, Weissman N, Thourani V, Svensson L, Tuzcu EM, McAndrew TC, Leon MB, Miller DC, Kirtane A. Sex-specific differences in late mortality after transcath-eter aortic valve replacement in the PARTNER trial. J Am Coll Cardiol. 2013;61(suppl 10):E1864.
35. Fielitz J, Leuschner M, Zurbrugg HR, Hannack B, Pregla R, Hetzer R, Regitz-Zagrosek V. Regulation of matrix metalloproteinases and their in-hibitors in the left ventricular myocardium of patients with aortic stenosis. J Mol Med (Berl). 2004;82:809–820.
36. Petrov G, Regitz-Zagrosek V, Lehmkuhl E, Krabatsch T, Dunkel A, Dandel M, Dworatzek E, Mahmoodzadeh S, Schubert C, Becher E, Hampl H, Hetzer R. Regression of myocardial hypertrophy after aortic valve re-placement: faster in women? Circulation. 2010;122(11 suppl):S23–S28.
37. Villari B, Campbell SE, Schneider J, Vassalli G, Chiariello M, Hess OM. Sex-dependent differences in left ventricular function and structure in chronic pressure overload. Eur Heart J. 1995;16:1410–1419.
38. Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: patho-genesis, disease progression, and treatment strategies. Circulation. 2005;111:3316–3326.
39. O’Brien KD. Pathogenesis of calcific aortic valve disease: a disease pro-cess comes of age (and a good deal more). Arterioscler Thromb Vasc Biol. 2006;26:1721–1728.
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from
Feng and De-Jia HuangWang, Xiao-Lin Luo, Chen Zhang, Li-Hui Lu, Qing-Tao Meng, Chi Chen, Mao Chen, Yuan
Zhen-Gang Zhao, Yan-Biao Liao, Yong Peng, Hua Chai, Wei Liu, Qiao Li, Xin Ren, Xue-QinSystematic Review and Meta-analysis
Sex-Related Differences in Outcomes After Transcatheter Aortic Valve Implantation: A
Print ISSN: 1941-7640. Online ISSN: 1941-7632 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Cardiovascular Interventions
doi: 10.1161/CIRCINTERVENTIONS.113.0005292013;6:543-551; originally published online September 24, 2013;Circ Cardiovasc Interv.
http://circinterventions.ahajournals.org/content/6/5/543World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circinterventions.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Interventions Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Cardiovascular Interventionsin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 1, 2018http://circinterventions.ahajournals.org/
Dow
nloaded from


















