Neuropsychiatric Aspects of HIV University of Hawaii James Dilley, MD and Emily Leavitt, LCSW.
38
Neuropsychiatric Aspects of HIV University of Hawaii James Dilley, MD and Emily Leavitt, LCSW
-
Upload
agatha-george -
Category
Documents
-
view
216 -
download
0
Transcript of Neuropsychiatric Aspects of HIV University of Hawaii James Dilley, MD and Emily Leavitt, LCSW.

Neuropsychiatric Aspects of HIV
University of Hawaii
James Dilley, MD and Emily Leavitt, LCSW

Prevalence of MH Disorders among People with HIV/AIDS
n = 1489
0%
5%
10%
15%
20%
25%
30%
Any MDD PanicAny Mood
Any Anxiety
PTSD
Vitiello et al. AJPsych 2003, 160:547-54
from “HIV Cost and Services Utilization Study—1996”

Depression in HIV
• Most common dx in outpt settings
• Concern re: diagnosis in medically ill
• Emphasize cognitive/affective vs. neurovegatative signs/sxs
• Assoc with CD4, soc support and phys limitations and HIV sx
• Excellent pharmacologic response
• Give benefit of the doubt

INITIAL MAX
1. SSRI'sFluoxetine (Prozac) 10 mg 40 mg/DParoxetine (Paxil) 10 mg/D 40 mg/DSertraline (Zoloft) 50 mg 200 mg/D
2. OthersBupropion SR (Wellbutrin) 100 mg BID 200 BIDMirtazapine (Remeron) 15 mg 30 mg/ HSTrazodone (Desyrel) 50 mg 300 mg/HS
3. TCA'sDesipramine 100 mg 300 mg/ HS or AMNortriptyline 50 mg 150 mg/HS
Pharmacotherapy of Depression in HIV

Depression & Testosterone
• 50% of men with Sx HIV/AIDS have deficiency and sx of hypogonadism:
– Fatigue– Decreased libido– Decreased appetite– Decreased mood

Screening Tests
• Total Serum Testosterone: <300-400ng/dl
• Serum Free testosterone: <5-7 pcg/ml
• Tx: depot IM injections q ii wks (100-200mg IM; max 400 mg/wk)
• Patch (5-10mg; 1-2 times daily)
• Gel (25-100 mg to skin daily)
• Can see mood improvement

CNS: HIV’s Most Important Sanctuary Site
• HIV produces at diff rates in CNS vs. plsma
• Diff phen/genotypes: esp later in disease
• All ARV’s not = in treating CNS cx
• May result in peripheral success (pVL) but central failure

HIV Neuropathogenesis
Early and continuous seeding
Importance of Blood Brain Barrier

HAD: A Diagnosisof Exclusion
• HIV antibody positive
• No other treatable disorder known to be associated with mental status changes (e.g., no other CNS OI’s, trauma, metabolic disorders, etc.

Diagnosis Requires (continued):
• “Clinical findings of disabling cognitive and /or motor dysfunction interfering with occupation or activities of daily living”
• Neuropsychological testing often needed, especially in early cases--
• (1 SD below age/education adjusted norms on 2/8 tests) AND
• Either impairment in lower ext or fine motor skills or selfreported depression interfering with function

Pseudo-Dementia• Depression in “dementia’s clothing”
• Index of suspicion high if: – unremitting and detailed c/o memory pblms
– “I don’t know” responses to cog questions: communicates distress/emphasizes disability
– Behavior often incongruent w/level of complaint
– In early stages of HIV disease
– Frequently has past hx of psychiatric pblms

Cognitive Functions
A. MemoryShort-term vs. delayed
B. Concentration, Calculation and Constructional Ability
C. Personality Change: alteration or accentuation of pre-morbid traits
D. Language
E. Judgement“Reasonable plans”

Early Manifestations of HAD
• Cognitive
Memory Loss (names, historical details, etc.)
Impaired Concentration (difficulty reading, loses track of conversation)
Mental slowing (“not as quick,” less verbal)
Confusion (time, especially)

• BehavioralApathy, withdrawal, “depression”Agitation, hallucination
• MotorUnsteady gaitBilateral leg weaknessTremorLoss of fine motor coordination
Early Manifestations of HAD (continued)

Late Manifestations
• Cognitiveglobal dementia in all spheresconfusion and distractabilityslow verbal responsiveness
• Behavioralvacant staredisinhibition and restlessnessorganic psychosis
Late Manifestations (cont.)
• Motor
general slowing
truncal ataxia
weakness: legs > armspyramidal tract signs: spasticity, hyperreflexia

Effect of HAART
• Significant changes in the epidemiology of CNS disorders since HAART
• In Sx illness– Studies are more consistent with subcortical
dementia
• In asx illness, NP findings are inconsistent– > Length of battery>NP deficits– Significance clinically is unclear
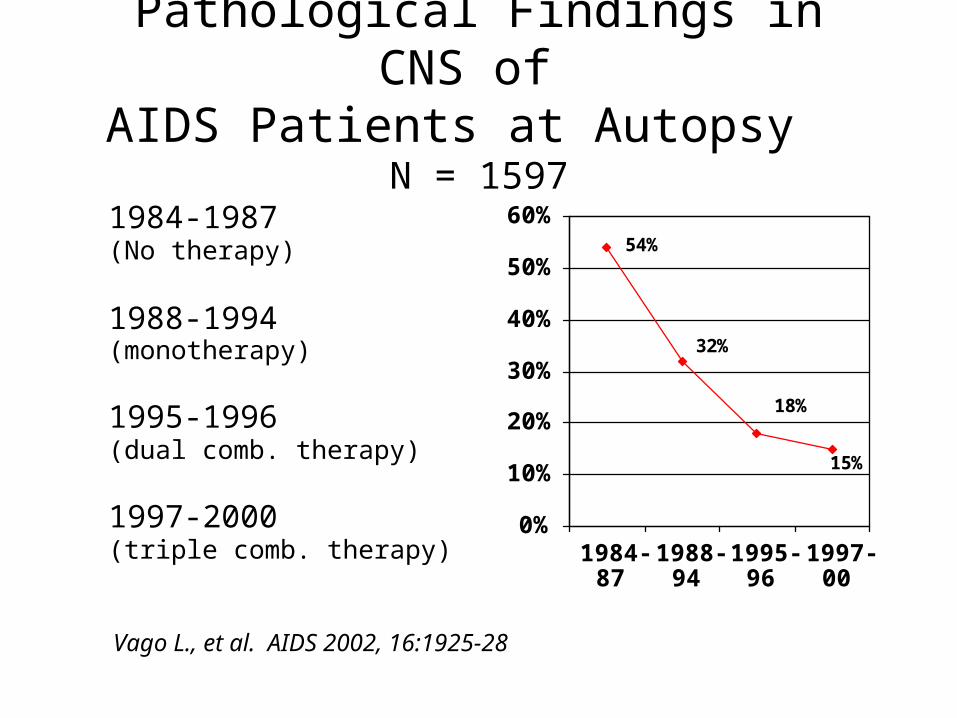
Pathological Findings in CNS of AIDS Patients at Autopsy N = 1597
1984-1987(No therapy)
1988-1994(monotherapy)
1995-1996(dual comb. therapy)
1997-2000(triple comb. therapy)
0%
10%
20%
30%
40%
50%
60%
1984-87
1988-94
1995-96
1997-00
54%
32%
18%
15%
Vago L., et al. AIDS 2002, 16:1925-28


Risk Factors for Cognitive Impairment in HIVCase Control: 90 HIV- ; 88 ASX; 94 SXCI = Scores of 2SD below the means of the control on 2 or more standard neuropsychological tests
RESULTS
OR Limits
Education <6 yrs cf. >6yrs 17.2 3.6 – 83.3
Antiviral Use Yes 0.1 0.0 – 0.3
CD4<200200-400
>500>500
8.66.9
1.0 – 71.01.0 – 48.4
De Ronchi D., et al. Arch. Neurology. 2002 May; 59(5):812-8

HAART Use & NP FunctionN = 130; Avg Age = 41; 42% NW; 82% AIDS
HAART
N 69
CD 4 254
UVL 42%
NPI 22%
Non-HAART
61
342
20% p<0.01
54% p<0.0001
Ferrando et al., AIDS, 1998, 12F 65-70
NOTE: IMP = 25D in the impaired direction of age-matched population-based norms
HAART= NRTI + Ritanavir, Indinavir or Nelfinavir

Median HIV RNA levels for brain (for all available brain regions) and peripheral tissues stratified by neurologic status:
non-demented, mild, and moderate/severe
0
1
2
3
4
5
6
7
8
9
10
Brain Only Peripheral Only
NoneMildModerate
p = 0.0128
p = 0.0002
McClernon D.R, et al. Neurology 2001, 57:1396-1401

Correlation of Plasma VL to CSF VLP CSF
< 200 >200
No No
No Yes*
No Yes
No Yes*
No No
CSF NP Status
< 200 >200
Yes No
Yes No
Yes No
Yes No
Yes No
Brew (Aus)
Ellis (US)
MacArthur (US)
Dore (US)
DiStephano (Italy)___________________________
* Correlation exists in ASX state

Favorable CNS Characteristics of ARVs
• % protein binding ( = better)
• lipid solubility ( = better)
• molecular weight ( = better)
• inhibitory concentration ( = better)

Medical Rx of HAD
1. Aggressive ARV: neuroprotective
2. Use combinations of 3, 4 or more
Should include:
• AZT, D4T, 3TC, Abac-NRTI
• Nevirapine, Efavirenz-NNRTI
• Indinavir - PI
(best BBB penetrance)

Factors Influencing Efficacy of ARV Rx:
• Stage of HIV disease
• Degree of CNS replication/resistance
• Integrity of BBB
• Specific treatment strategy/ARV choice

Some Neuroprotective Disappointments
Nimodipene interaction with CAH
Peptide T block gp-120
*Memantine NMDA antagonist/showing efficacy for ADV
*Deprenyl Anti-oxidant/anti-poptotic
Lexipafant PAF antagonist
*some benefits

Case History - “JC”
ID: 42 y/o GWM architect admitted for agitation,irritability, decreased sleep, and grandiose delusions. Brought in by lover of 7 yrs.
HPI Two mos intermittent confusion/ hypomania (rapid speech, disorganized thinking over last 3 days; focus on spiritual issues. Felt friends were trying to harm him, stated he had been cured of AIDS; claimed he was a millionaire.
PMH HIV infected x 10 years; current CD4 count = 70.
No OI’s. No previous psych hx.

Case History - “JC” (cont.)MS: Alert, mildly agitated, unable to sit still.
Speech: mildly pressured, loud, but interruptable.Thought process: overly inclusive, loose assns.Content: grandiose, “richest family in California,”had “cured himself of AIDS.” Some paranoia.Cognitive: 0 x 2. Memory: Imm = 4/4; 2/4 @ 5 mins. 3/4 with prompts.Attention: Serial 7’s = mult. Errors;
WORLD backwards, “d-l-o-w.”Abstraction: Some concreteness.Construction: OKInsight: noneJudgement: impaired

Case History - “JC” (cont.)
Diff Dx:
Axis 1: Delirium due to HIV disease (293.0).Dementia due to HIV disease (294.1)R/O BADR/O Toxic Psychosis
Axis II: Deferred
Axis III: AIDS

Hospital Course
LAB: MRI: Extensive cortical atrophy.LP: unremarkable
Rx: Trilafon 2mg p.o. BID and 4 mg @ HSValproic acid 250mg p.o. BID and 500 mg @ HSAtivan 0.5 mg p.o. BID and prn agitation

Psychotropic Medication Use
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Any Anti-Anx StimulantsAnti-D Anti-Psych
NOTE: Use among Af-Am was significantly lower than White or Hispanic.
Vitiello et al. AJPsych 2003, 160:547-54
from “HIV Cost and Services Utilization Study—1996”

Psychopharmacology in HIV Disease
Consider geriatric dosing - “start low and go slow”
Look for low-anticholinergic meds
ConsiderPay special attention to Ritonavir (NORVIR - strong CYP3A4 inhibitor)
Overall, anti-HIV meds are not problematic
Pharmacotherapy of Anxiety Disorders
1. “Reactive” Anxiety - Lorazepam 0.5 mg B/TIDMax: 4 mg q 4 hrs
2. Panic Disorders with or without Agoraphobia Paroxetine (Paxil) 10-40 mg/D Lorazepam for breakthrough
3. GAD - Paroxetine; Buspirone (Buspar) 5-10 mg BID - 20 mg TID
Note: Buspirone is the “does not” drug: cause tolerance, physical dependence or a withdrawal syndrome, have abuse potential (hypnotic, muscle relaxant activity), work right away

Ritonavir (Norvir)(Potent inhibitor of CP450, esp. 2D6 and 3A4)
1. Adjust Anti-depressants SSRI’s - initially by 1/2 TCA’s - initially by 1/2 to 1/3Nefazodone and St. John’s Wort
2. Avoid Benzodiazepines Anti-psychoticsClonazepam (Klonopin) ClozapineAlprazolam (Xanax) PimozideDiazepam (Valium)Flurazepam (Dalmane)Triazolam (Halcion)Zolpidem (Ambien)
2. AllowTemazepam (Restoril)Oxazepam (Serax)Lorazepam (Ativan)Bupropion (Wellbutrin)

Methadone
• Ritonavir and Nevirapine (and likely Efavirenz) has been shown to lead to significant withdrawal symptoms in stable methadone users
• Should follow serum meth levels before & after initiation; may need to increase by 25-30%

Other Pharm Issues
• Sildenafil levels may be significantly raised by Ritonavir, Saquinavir and Indinavir--potentially serious CV effects (DNE 25mg)
• Fatal case reports have been filed suggesting Ritonavir in combination with methamphetamine and Ecstasy (MDMA) was the cause of death
• St. John’s Wort: may decrease PI’s

ARV Classes
Fusin
Inhibitor
Reverse Integrase Protease
Fuseon Transcriptase Inhibitors
NRTI NNRTI
AZT Nevirapine*DDI DelavardineDDC DMP-266D4T Efavirenz*3TC
IndinavirRitonavirSaquinavirNelfinavir
*Induce CP450 3A4 and 2D6