NEUROLOGICAL MECHANISMS UNDERLYING ROTATOR CUFF
215
NEUROLOGICAL MECHANISMS UNDERLYING ROTATOR CUFF SKELETAL MUSCLE PATHOPHYSIOLOGY AND IMPLICATIONS FOR THERAPY BY SANDEEP MANNAVA A Dissertation Submitted to the Graduate Faculty of WAKE FOREST UNIVERSITY GRADUATE SCHOOL OF ARTS AND SCIENCES in Partial Fulfillment of the Requirements for the Degree of DOCTOR OF PHILOSOPHY NEUROSCIENCE MAY 2012 Winston-Salem, North Carolina Approved By Thomas L. Smith, Ph.D., Advisor Mark E. Van Dyke, Ph.D., Chair Osvaldo Delbono, M.D., Ph.D. L. Andrew Koman, M.D. Zhongyu Li, M.D., Ph.D.
Transcript of NEUROLOGICAL MECHANISMS UNDERLYING ROTATOR CUFF

NEUROLOGICAL MECHANISMS UNDERLYING ROTATOR CUFF SKELETAL MUSCLE PATHOPHYSIOLOGY AND IMPLICATIONS FOR THERAPY
BY
SANDEEP MANNAVA
A Dissertation Submitted to the Graduate Faculty of
WAKE FOREST UNIVERSITY GRADUATE SCHOOL OF ARTS AND SCIENCES
in Partial Fulfillment of the Requirements
for the Degree of
DOCTOR OF PHILOSOPHY
NEUROSCIENCE
MAY 2012
Winston-Salem, North Carolina
Approved By
Thomas L. Smith, Ph.D., Advisor
Mark E. Van Dyke, Ph.D., Chair
Osvaldo Delbono, M.D., Ph.D.
L. Andrew Koman, M.D.
Zhongyu Li, M.D., Ph.D.

ii
DEDICATION
I dedicate this dissertation to: my parents, Venkata Rao Mannava, MD and Uma Mannava, MD;
to my wife, Kathleen A. Mannava, MD; and to my sister, Kavitha Mannava,
without your support, love, encouragement, and patience this would not be possible.
iii
ACKNOWLEDGEMENTS
I would like to sincerely thank my parents: Venkata Rao Mannava, MD and Uma
Mannava, MD. Without your love, support, and guidance, I would not be in the position
I am today. It is my hope that I have been able to take advantage of the many
opportunities that you have given me. I am truly blessed to be your son. I would also like
to thank my beautiful wife Kathleen A. Mannava, MD, who is the love of my life. Thank
you for allowing me to pursue my many interests; your unwavering support and love
keeps me grounded and strong. Finally, I would like to thank my sister Kavitha Mannava.
You have been a friend since you were born. You are the future and have inspired me to
do better…
I would like to thank my mentors Thomas L. Smith, PhD and L. Andrew Koman,
MD. Also, I would like to thank Riyaz H Jinnah, B. Chir, FRCS and Beth P. Smith, PhD.
Your support of my research ideas allowed me to pursue my sincere academic interests
during my time in the laboratory. You all took a chance in giving me this research and
clinical educational opportunity at Wake Forest University. I am grateful for the
opportunity to take part in your innovative program. I have learned a tremendous amount
from all of you, both professionally and personally. Thank you for letting me learn from
mistakes and experience the success of our collective research efforts.
I am grateful to my committee members Osvaldo Delbono, MD, PhD and
Zhongyu Li, MD, PhD. You have both been great role models during my pursuit of the
PhD degree after completing my medical school training. I truly appreciate your
invaluable insights, which have greatly improved the quality of my research endeavors. I
appreciate both of you giving me the most valuable gift of all, your time.
iv
I want to thank my committee chairman, Mark E. Van Dyke, PhD. Since I arrived
at Wake Forest University, we have met several times a month and I have learned a lot
from your very unique perspective. You have challenged me to improve my research,
have encouraged me after my many grant and manuscript rejections, and have
congratulated me after each success. Thank you for all you do for young orthopaedic
researchers at Wake Forest University and for all you do for our department.
All great research requires a capable and qualified team. Wake Forest University
School of Medicine’s Department of Orthopaedic Surgery has one of the best research
teams in the world. I would like to acknowledge and thank the great faculty for your
insights and help in completing these many projects: Michael F. Callahan, PhD;
Christopher J. Tuohy, MD; Gary G. Poehling, MD; and Walton W. Curl, MD. I would
also like to thank our wonderful orthopaedic residents for their support and help, both
professionally and personally: Thorsten M. Seyler, MD; Johannes F. Plate, MD; Jordan
M. Case, MD; Omar F. Nazir, MD; Maxwell K. Langfitt, MD; Patrick W. Whitlock, MD,
PhD; Jonathan C. Barnwell, MD; Austin V. Stone, MD; and Peter J. Apel, MD, PhD. I
have also been very fortunate to work with some very bright, motivated, and enthusiastic
medical students and graduate students, who I would like to thank: Walter F. Wiggins,
BS; Patrick Haubruck, BS; Simon M. Trach, BS; and Lauren A. Pace, BS. Finally, I
would like to acknowledge and thank the wonderful orthopaedic research staff: Eileen
Martin, Martha Holden, Janet Kelly, Casey Lively Northam, and Deanna Sizemore.
I would like to specifically mention and thank some of our collaborators from
other departments: Katherine R. Saul, PhD; Joel D. Stitzel, PhD; and Josh Tan, MS. I
would also like to thank my neuroscience collaborators and professors Carol Milligan,
v
PhD and Ronald W Oppenheim, PhD. I have learned from you both in the classroom and
from our collaborative research efforts. Thank you for making me a better basic scientist
and for supporting my research pursuits.
I am thankful for the research opportunities and mentorship I received earlier in
my educational career. Under the mentorship of Charles Antzelevitch, PhD (Masonic
Medical Research Laboratories, Utica, NY), Robert F Gilmour Jr., PhD (Cornell
University, Ithaca, NY), and Niels F. Otani, PhD (Cornell University, Ithaca, NY), I
developed my scientific curiosity and love of biomedical research. I appreciate the
amount of patience and support you provided me when I was younger, immature, and less
knowledgeable. Thank you for allowing me to learn in your laboratories and for inspiring
me to pursue biomedical research.
On a personal note, I would like to acknowledge the support of my good friends:
Matthew J. Carhart, JD; Robert F. Manfredo, JD; Vikram V. Bellapravalu, MBA;
Andrew Lombardo, MBA; and Philip Lombardo, PhD. We have known each other our
entire lives and have pushed each other to pursue greatness. I am proud of all you have
accomplished. Hopefully we are just getting started...

vi
TABLE OF CONTENTS
Table of Contents ..................................................................................................................... vi
List of Illustrations and Tables ........................................................................................... ix Chapter 2 Figures and Table .................................................................................................................... ix Chapter 3 Figures and Table .................................................................................................................... ix Chapter 4 Figures and Tables .................................................................................................................. ix Chapter 5 Figures and Table .................................................................................................................... ix Chapter 6 Figure ............................................................................................................................................. x
List Of Abbreviations ............................................................................................................. xi
Abstract .................................................................................................................................... xiv
Chapter 1 ..................................................................................................................................... 1
Introduction ............................................................................................................................... 1 Rotator Cuff Tears: A Description of the Clinical Problem .................................................. 2 Rationale for a Neuroscience Approach to Rotator Cuff Reconstruction Surgery ...... 2 Development and Characterization of a Small Animal Model for the Study of Rotator Cuff Function After Injury ............................................................................................... 5 Neuromodulation of In Vivo Soft-Tissue Biomechanical Properties Following Botulinum Neurotoxin A (BoNT-A) Injection: A Potential Therapeutic Strategy to Improve Operative Outcomes of Rotator Cuff Repair Surgery ........................................... 7 A Novel Paradigm for Rotator Cuff Research: Translating Basic Science Animal Model Studies to Clinical Recommendations Using Simulation Analysis ...................... 9 References .......................................................................................................................................... 10
Chapter 2 ................................................................................................................................... 17
Evaluation of In Vivo Rotator Cuff Muscle Function After Acute and Chronic Detachment of the Supraspinatus Tendon: An Experimental Study in an Animal Model ........................................................................................................................... 17
ADDENDUM ........................................................................................................................................ 17 Abstract ............................................................................................................................................... 18 Introduction ...................................................................................................................................... 20 Materials and Methods: ................................................................................................................. 21
Muscle Force Testing: ................................................................................................................................ 21 Muscle Force Data Standardization ..................................................................................................... 23 EMG Testing ................................................................................................................................................... 24 Histological analysis ................................................................................................................................... 24 Statistics .......................................................................................................................................................... 25 Source of Funding ....................................................................................................................................... 25
Results ................................................................................................................................................. 26 Discussion .......................................................................................................................................... 29 Acknowledgements......................................................................................................................... 34 References .......................................................................................................................................... 35
Chapter 3 ................................................................................................................................... 60
vii
Chemical Denervation with Botulinum Neurotoxin A Improves the Surgical Manipulation of the Muscle-Tendon Unit: An Experimental Study in an Animal Model .......................................................................................................................................... 60
Abstract ............................................................................................................................................... 61 Introduction ...................................................................................................................................... 63 Materials and Methods .................................................................................................................. 64
Botulinum Toxin Injection ....................................................................................................................... 65 Assessment of Active and Passive Muscle Properties .................................................................. 65 Statistical Analysis ...................................................................................................................................... 67
Results ................................................................................................................................................. 68 Discussion .......................................................................................................................................... 70 Acknowledgements......................................................................................................................... 74 Source of Funding ............................................................................................................................ 75 References .......................................................................................................................................... 76
Chapter 4 ................................................................................................................................... 93
Contributions of Neural Tone to In Vivo Passive Muscle-Tendon Unit Biomechanical Properties in a Rat Rotator Cuff Animal Model ............................. 93
Abstract ............................................................................................................................................... 94 Introduction ...................................................................................................................................... 95 Materials and Methods .................................................................................................................. 97
Botulinum Neurotoxin A and Saline Injection Procedure .......................................................... 97 Surgical Exposure and Experimental Apparatus ........................................................................... 98 Muscle Force Testing .............................................................................................................................. 100 Passive Load-Relaxation Testing ....................................................................................................... 100 Fung’s Quasilinear Viscoelastic Model (QLV) ............................................................................... 101 Statistics ....................................................................................................................................................... 103
Results ............................................................................................................................................... 104 Discussion ........................................................................................................................................ 105 Acknowledgements....................................................................................................................... 112 References ........................................................................................................................................ 113
Chapter 5 ................................................................................................................................ 132
The Science of Rotator Cuff Repairs: Translating Basic Science into Clinical Recommendations .............................................................................................................. 132
Abstract ............................................................................................................................................. 133 Introduction .................................................................................................................................... 135 Rotator Cuff Tears: A Clinical Problem .................................................................................. 135 The Rotator Cuff Muscle Undergoes Changes After Tendon Injury ............................. 137 In Vivo Biomechanics of Rotator Cuff Repair Surgery...................................................... 138 Evaluation of Muscle Function after Rotator Cuff Tears ................................................. 140 Computational Modeling of the Human Upper Extremity and Implications for Orthopaedic Surgery .................................................................................................................... 143 The Effect of Muscle-Tendon Unit Retraction on Passive and Active Tension: A Simulation Analysis of Rotator Cuff Tears ............................................................................ 145 Summary and Conclusions ......................................................................................................... 146 Source of Funding .......................................................................................................................... 147 Acknowledgements....................................................................................................................... 147 References ........................................................................................................................................ 149

viii
Chapter 6 ................................................................................................................................ 177
Clinical Relevance and Future Directions .................................................................. 177 Summary of Doctoral Thesis ..................................................................................................... 178 Clinical Relevance to Orthopaedic Surgery .......................................................................... 178 Future Direction for Rotator Cuff Surgery Research ........................................................ 179 The Study of Age –Related Changes and the Influence on Rotator Cuff Surgery..... 179 Future Directions of Botulinum Neurotoxin A (BoNT-A) Modulation of Soft-Tissue Biomechanics .................................................................................................................................. 182 A Bioengineering Approach to Rotator Cuff Surgery ........................................................ 184 References ........................................................................................................................................ 185
Curriculum Vitae ................................................................................................................. 191 Education .......................................................................................................................................... 191 Teaching............................................................................................................................................ 191 Professional Societies .................................................................................................................. 191 Research Support .......................................................................................................................... 192 Peer-Reviewed Manuscripts ...................................................................................................... 192 Book Chapters ................................................................................................................................. 194 Thesis Titles .................................................................................................................................... 194 United States Patent ..................................................................................................................... 194 Abstracts and Meeting Presentations .................................................................................... 194 Research Positions and Employment ..................................................................................... 199 Awards and Honors ...................................................................................................................... 200

ix
LIST OF ILLUSTRATIONS AND TABLES
Chapter 2 Figures and Table
Chapt 2, FIG 1 Pages 45-46 Chapt 2, FIG 2 Pages 47-48 Chapt 2, FIG 3 Pages 49-50 Chapt 2, FIG 4 Pages 51-52 Chapt 2, FIG 5 Pages 53-54 Chapt 2, FIG 6 Pages 55-56 Chapt 2, FIG 7 Pages 57-58 Chapter 2, Table 1 Page 59
Chapter 3 Figures and Table
Chapt 3, FIG 1 Pages 84-85 Chapt 3, FIG 2 Pages 86-87 Chapt 3, FIG 3 Pages 88-89 Chapt 3, FIG 4 Pages 90-91 Chapt 3, Table 1 Page 92
Chapter 4 Figures and Tables
Chapt 4, FIG 1 Pages 120-121 Chapt 4, FIG 2 Pages 122-123 Chapt 4, FIG 3 Pages 124-125 Chapt 4, FIG 4 Pages 126-127 Chapt 4, FIG 5 Pages 128-129 Chapt 4, Table 1 Page 130 Chapt 4, Table 2 Page 131
Chapter 5 Figures and Table
Chapt 5, FIG 1 Pages 160-161 Chapt 5, FIG 2 Pages 162-163 Chapt 5, FIG 3 Pages 164-165 Chapt 5, FIG 4 Pages 166-167 Chapt 5, FIG 5 Pages 168-169
x
Chapt 5, FIG 6 Pages 170-171 Chapt 5, FIG 7 Pages 172-173 Chapt 5, FIG 8 Pages 174-175 Chapt 5, Table 1 Page 176
Chapter 6 Figure
Chapt 6, FIG 1 Pages 189-190
xi
LIST OF ABBREVIATIONS
α Pennation Angle or Alpha (power analysis) μL Microliters ‘A’ Fung QLV Parameter (linear scaling elastic
component)
Ann of Biomed Eng Annals of Biomedical Engineering ant Anterior AUC Area Under the Curve (for Compound Motor
Action Potential)
‘B’ Fung QLV Parameter (nonlinear scaling elastic component)
BoNT-A Botulinum Neurotoxin A or Botulinum Toxin A ‘C’ Fung QLV Parameter (viscocity) CD1 Cluster-Designation 1 CE Contractile Element (representation of actin-
myosin interaction with a dashpot in the Hill Muscle Model)
CME Continuing Medical Education CMAP Compound Motor Action Potential CST Corticospinal Tract CT-Scan Computer-Tomography Scan ‘D’ Distal EMG Electromyography EPub Electronically Published FT Force Applied to Tendon g Grams
xii
Hz Hertz J Hand Surg Am Journal of Hand Surgery American Edition JBJS (Am.) The Journal of Bone and Joint Surgery American
Edition
KCl Potassium Chloride kg Kilogram ls
T Tendon Slack Length lo
M Resting Muscle Length lat Lateral ‘M’ Middle mA Milliampere mm Millimeter ms Millisecond N Newton(s) ‘P’ Proximal PCSA Physiological Cross-Sectional Area PMID PubMed Identification Number QLV Quasilinear Viscoelastic Model (described by Fung) R2 Coefficient of Determination RST Rubrospinal Tract s Second(s) Tau1 or τ1 Fung QLV Parameter (fast relaxation component
time constant)
Tau2 or τ2 Fung QLV Parameter (slow relaxation

xiii
component time constant) TST Tectospinal Tract U Units V Volt(s) VST Vestibulospinal Tract

xiv
ABSTRACT
Sandeep Mannava
Introduction: Rotator cuff tears are a common cause of upper-extremity disability. For
chronic, full-thickness, rotator cuff tears, repair surgery can be technically challenging
due to large gap distances and increased stiffness of the muscle-tendon unit. In contrast,
acute rotator cuff tears are associated with lower repair tensions, less fibro-fatty
infiltration of the muscle, and better functional outcomes. Animal models can be used to
understand rotator cuff muscle function and these results can be translated into clinical
recommendations using computational modeling.
Methods: In vivo muscle function, electromyography, and passive muscle-tendon unit
properties were studied before and after supraspinatus tenotomy in a rodent rotator cuff
injury model (acute vs chronic). Chemical denervation and Fung’s QLV model were used
to assess neural contributions to in vivo stress-relaxation biomechanical properties. Then,
a series of simulation experiments were conducted using a validated computational
human musculoskeletal shoulder model to assess both passive and active tension of
rotator cuff repairs based on surgical positioning.
Results: Muscle function was impaired at the tensions required to repair a chronically
torn rotator cuff (45% reduction from maximal twitch amplitude, p<0.05). Dysfunction in
the chronic tear setting was detectable via EMG (p<0.05). Although the chronically
injured muscle-tendon unit becomes more stiff; pharmacological modulation of the
nervous system with BoNT-A improves compliance by approximately 20% (p<0.05). At
adducted postures, computational data from simulated surgical repair of chronically torn
rotator cuff indicated that passive repair tension markedly exceeds the pullout strength of
xv
fixation techniques typically used in these surgeries and there was approximately a 50%
reduction in moment generating capacity after repair of chronically torn rotator cuff.
Discussion and Conclusion: Rotator cuff surgical outcomes may be improved by earlier
intervention, which results in lower surgical repair tensions and fewer electromyographic
neuromuscular changes. Our data suggest a direct experimental connection between high
repair tensions—chronic tear setting—and impaired contractile force. The
pharmacological modulation of increased muscle-tendon unit stiffness using BoNT-A has
the potential to facilitate the surgical manipulation of the muscle-tendon unit and protect
the repaired tendon. Simulation analysis stresses the importance of proper arm
positioning during intra-operative repair, post-operative healing, and rehabilitation.

1
CHAPTER 1
INTRODUCTION
Sandeep Mannava
2
ROTATOR CUFF TEARS: A DESCRIPTION OF THE CLINICAL PROBLEM
Rotator cuff tears are a common cause of upper extremity pain and disability.
The incidence of rotator cuff tears is approximately 4% in patients under the age of 40
years old, with the incidence increasing to 54% in patients over the age of 60 years old
[1]. About 300,000 rotator cuff surgeries are performed annually in the United States
with an economic burden of $3 billion [2, 3].
In healthy individuals, the four rotator cuff muscles act as dynamic stabilizers,
centering the humeral head on the glenoid in order to optimize upper-extremity function
during motion [4]. Once torn, rotator cuff tendons do not heal spontaneously, which can
lead to decreased range of shoulder motion, joint instability, chondral injury, and
decreased function [5]. Despite considerable surgical advances, these surgeries are still
associated with a high rate (20-90%) of recurrent tearing [5-10]. Factors contributing to
poor operative outcomes include advanced age [2], poor tendon quality [11], extensive
muscle atrophy and fibrofatty infiltration [12], increased time from injury [2, 3, 13], and
large tear size [2, 3, 14, 15]. Currently, there is no “gold-standard” surgical treatment that
successfully restores pre-injury shoulder strength, range of motion, and function [5-9]. A
research approach that utilizes neuroscience techniques may provide the insights needed
to improve functional outcomes after rotator cuff surgery.
RATIONALE FOR A NEUROSCIENCE APPROACH TO ROTATOR CUFF
RECONSTRUCTION SURGERY
Neuroscience is a broad field, encompassing the central nervous system (brain
and spinal cord), the peripheral nervous system, and skeletal muscle. In orthopaedics,
surgeons often deal with the more peripheral manifestations of pathological conditions
3
afflicting the central nervous system. For example, orthopaedic surgeons manage and
treat the muscle contractures and joint deformities that are associated with cerebral palsy
[16]. Additionally, orthopaedic surgeons directly operate and clinically manage spine
pathology. Further, the common orthopaedic conditions of carpal tunnel syndrome and
cubital tunnel syndrome are caused by nerve compression.
Insights can be gained from a neuroscience approach to the difficult problem of
fibrofatty degeneration of the rotator cuff muscles after chronic detachment of the tendon.
Many orthopaedic surgeons consider the structural changes that the muscle undergoes
irreversible [12, 17, 18], and little progress has been made since the first modern
description of the condition by E. Armory Codman. In his 1934 book The Shoulder:
Rupture of the Supraspinatus Tendon and Other Lesions in or about the Subacromial
Bursa, Dr Codman stated “the tendon was retracted to such a degree that I could not even
attempt a suture.” Orthopaedic research has focused on the tendon-to-bone interface (i.e.
how to re-attach the tendons to the humerus) [19-26]; however, the rotator cuff muscles
function as dynamic stabilizers and without adequate contractile strength of these
muscles, the repair of a torn tendon may be of little value to the patient. In fact, current
practice guidelines acknowledge the inadequacy of rotator cuff repair surgery in
reversing pathological changes in skeletal muscle structure and function [5-10]. Thus, a
more complete understanding of the pathophysiological mechanisms underlying rotator
cuff skeletal muscle dysfunction may improve clinical care.
The current understanding of rotator cuff muscle pathology is largely based upon
clinical studies, including physical examination and radiological imaging of the disease
state [17, 27, 28]. Some of the pathophysiological changes contributing to the muscle

4
dysfunction might be attributable to nerve compression or entrapment. Recently, an
association has been made between large rotator cuff tears and suprascapular neuropathy
in several clinical case series [29-31]. The suprascapular nerve takes a tortuous course
and has the potential to become entrapped or compressed by the atrophied and retracted
muscle-tendon unit in the suprascapular and spinoglenoid notches [32-34]. Unfortunately,
the literature is limited to clinical studies. Basic science data that has directly associated
suprascapular neuropathy to the chronicity of the torn rotator cuff tendon are not
currently available.
Basic science literature on rotator cuff pathology has been limited to structural
gene/protein expression [35, 36], histological examination [37-39], and biomechanical
studies [38, 40, 41]. Previous studies offer a limited physiological profile of rotator cuff
muscle function after injury to the rotator cuff tendon. Specifically, previous studies
examined isometric contractions at repair tensions below those required to surgically
reattach the muscle-tendon unit to the humeral head [42-45]. Many of the previous
studies have been performed in a classical physiology setting of ex vivo explanted whole
muscle or in vitro single muscle fiber studies [42-45]. The in vivo muscle function studies
of pathological rotator cuff muscles have been performed in the sheep model [45].
For advancement of the basic science understanding of how rotator cuff muscles
respond to surgical manipulation and tendinous injury, it is necessary to develop an in
vivo small animal rodent model to test rotator cuff muscle and suprascapular nerve
function. As Codman described in 1934, passive stiffness of the muscle-tendon unit is a
major determinant of surgical success and post-operative functional outcome [38, 40, 41].
Botulinum Neurotoxin A (BoNT-A) is a widely administered pharmacological agent that
5
has been utilized in neuroscience research and clinical management of spasticity [46, 47].
The novel orthopaedic use of this highly potent neurotoxin has the potential to
temporarily and reversibly cause chemical denervation and flaccid paralysis/paresis, thus
modifying passive stiffness and improving the surgical manipulation of otherwise stiff
skeletal muscle-tendon units. In summary, a systematic neuroscience-based approach and
understanding of rotator cuff pathology has the potential to improve orthopaedic clinical
practice for this common cause of upper-extremity pathology.
DEVELOPMENT AND CHARACTERIZATION OF A SMALL
ANIMAL MODEL FOR THE STUDY OF ROTATOR CUFF
FUNCTION AFTER INJURY
This doctoral thesis is divided into several chapters based upon the development
and characterization of a small animal model system for the study of rotator cuff
neuromuscular function after injury. To the best of our knowledge, there are no published
studies that evaluate in vivo rodent rotator cuff muscle function after rotator cuff tear. The
lack of these studies is probably due to the technical limitations of performing the
surgical dissection of the suprascapular nerve and isolation of the single rotator cuff
tendon in the rat model. Supraspinatus muscle atrophy following chronic rotator cuff
tears may place excessive traction on the suprascapular nerve, contributing to functional
decline. Electromyography (EMG) is an inexpensive, minimally invasive test for rapid
electrophysiological assessment of patients during normal and athletic upper extremity
motion [48-50]. After establishing an in vivo rat shoulder model, the utility of EMG in
diagnosing rotator cuff neuromuscular dysfunction was examined.
6
In Chapter 2, we describe the development of a functional rodent rotator cuff
animal model and studied the natural history of rotator cuff dysfunction after injury. The
rat shoulder is an established animal model for the study of human rotator cuff pathology
based on similarities in bony architecture of the shoulder region in these two species.
Unfortunately, most of the current rotator cuff literature has not addressed muscle and
nerve function after rotator cuff tears. The first goal of the doctoral thesis was to develop
a rat shoulder animal model to test in vivo muscle force and electromyography (EMG).
Muscle force testing was used to evaluate in vivo rat rotator cuff stimulation frequency-
dependent muscle recruitment, muscle-tendon unit displacement, single-twitch muscle
contraction, tetanic contraction, and fatigue in animals with acutely and chronically torn
rotator cuffs. Then EMG was performed in acute and chronic in vivo rat rotator cuff tear
model to study compound motor action potential (CMAP) amplitude and area under the
curve, as well as CMAP regional location heterogeneity. In Chapter 2, we were also able
to study passive changes to in vivo soft tissue biomechanical properties of the muscle-
tendon unit that occur after acute and chronic rotator cuff tears. We hypothesized that a
chronically torn rotator cuff tendon results in increased passive muscle-tendon unit
stiffness and reduced in vivo skeletal muscle contractile strength. Further, we
hypothesized that neuromuscular dysfunction can be detected by electromyography
(EMG) in the chronic tendon tear setting.
7
NEUROMODULATION OF IN VIVO SOFT-TISSUE BIOMECHANICAL
PROPERTIES FOLLOWING BOTULINUM NEUROTOXIN A (BONT-A)
INJECTION: A POTENTIAL THERAPEUTIC STRATEGY TO IMPROVE
OPERATIVE OUTCOMES OF ROTATOR CUFF REPAIR SURGERY
Based on the findings from Chapter 2, we identified excessive repair tension as a
major determinant of reduced muscle function following rotator cuff tears. Surgical repair
of a large chronic rotator cuff tear requires manipulation of a muscle-tendon unit that is
scarred, retracted, and stiffer than normal secondary to dis-use muscle atrophy [38, 40,
41]. Altering the passive properties of skeletal muscle by chemical denervation has the
potential to improve the surgical manipulation of the muscle-tendon unit by reducing
muscle stiffness and may ultimately improve surgical outcomes. Surgical and
rehabilitation experience with patients who have sustained neurological insults such as
cerebral palsy demonstrates significant influence of the nervous system over the passive
biomechanical properties of muscle. Passive visco-elastic properties of skeletal muscle-
tendon units are key determinants of surgical and post-operative functional success [38,
40, 41]. Most tendon repair studies have attempted to overcome increased muscle-tendon
unit stiffness and improve healing by focusing on the tendon-to-bone interface through
improvement of repair site strength by varying surgical techniques and suture materials
[19-26]. Injection of BoNT-A into the skeletal muscle shifts attention for repair to the
proximal portion of the muscle-tendon unit. Altering the passive properties of skeletal
muscle by chemical denervation has the potential to improve the surgical manipulation of
the muscle-tendon unit and ultimately improve surgical outcomes. Further, this strategy
has the added benefit of “bioprotecting” the tendon repair site. Presumably, by causing
8
temporary chemical paresis, the muscle will not be able to generate enough active force
to rupture the surgically repaired tendon [51, 52].
In Chapter 3, we first tested the hypothesis that Botulinum neurotoxin A (BoNT-
A) injection temporarily and reversibly changes active and passive skeletal muscle
properties. Specifically, the chemical denervation effected by the toxin alters the visco-
elastic properties of the muscle when compared to control, saline injected skeletal
muscle. Chapter 3 is our first published study demonstrating that the soft-tissue passive
properties of the muscle-tendon unit can be altered via chemical denervation in a mouse
gastrocnemius animal model. We postulated and then proved that BoNT-A injection can
improve the surgical manipulation of the muscle-tendon unit.
In Chapter 4, we utilized the rat rotator cuff animal model to study the influence
and contribution of neuronal tone on passive skeletal muscle-tendon unit visco-elastic
properties after chemical denervation using BoNT-A. Fung’s quasi-linear visco-elastic
mathematical model was used to study the effects of chemical denervation on passive
muscle properties. A standard muscle force testing experimental apparatus was used to
record and analyze the load-relaxation characteristics of skeletal muscle after chemical
denervation with BoNT-A. In Chapter 4, we report on our mathematical and experimental
determination of the relative contribution of the nervous system to soft-tissue
biomechanical properties.
9
A NOVEL PARADIGM FOR ROTATOR CUFF RESEARCH: TRANSLATING
BASIC SCIENCE ANIMAL MODEL STUDIES TO CLINICAL
RECOMMENDATIONS USING SIMULATION ANALYSIS
In conclusion, Chapter 5 summarizes our basic science animal data and discusses
the current literature on rotator cuff injuries and repairs. We further attempt to translate
our animal studies into clinical recommendations using a computational human upper-
extremity movement biomechanics model to perform a simulation analysis. In Chapter 5,
we present data that explores passive and active muscle properties in the context of acute
and chronic rotator cuff tears. For chronic, full-thickness, rotator cuff tears, repair surgery
can be technically challenging due to large gap distances and increased stiffness of the
muscle-tendon unit. In contrast, acute rotator cuff tears are associated with lower repair
tensions, less fibro-fatty infiltration of the muscle, and better functional outcomes.
Chapter 5 demonstrates how animal models can be used to understand rotator cuff muscle
function in the acute and chronic tear setting and how these results can be translated into
clinical recommendations using computational modeling. Chapter 6 briefly discusses the
clinical relevance of our basic science findings presented in this thesis and outlines future
experiments that we would like to pursue, related to rotator cuff dysfunction and repair
surgery.

10
REFERENCES
1. Sher, J.S., J.W. Uribe, A. Posada, B.J. Murphy, and M.B. Zlatkin, Abnormal
findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg
Am, 1995. 77(1): p. 10-5.
2. Oh, J.H., S.H. Kim, H.M. Ji, K.H. Jo, S.W. Bin, and H.S. Gong, Prognostic
factors affecting anatomic outcome of rotator cuff repair and correlation with functional
outcome. Arthroscopy, 2009. 25(1): p. 30-9.
3. Oh, L.S., B.R. Wolf, M.P. Hall, B.A. Levy, and R.G. Marx, Indications for
rotator cuff repair: a systematic review. Clin Orthop Relat Res, 2007. 455: p. 52-63.
4. Favard, L., G. Bacle, and J. Berhouet, Rotator cuff repair. Joint Bone Spine,
2007. 74(6): p. 551-7.
5. Aurora, A., J. McCarron, J.P. Iannotti, and K. Derwin, Commercially available
extracellular matrix materials for rotator cuff repairs: state of the art and future trends. J
Shoulder Elbow Surg, 2007. 16(5 Suppl): p. S171-8.
6. Bigliani, L.U., F.A. Cordasco, S.J. McIlveen, and E.S. Musso, Operative
treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am, 1992. 74(10): p.
1505-15.
7. Cordasco, F.A. and L.U. Bigliani, The rotator cuff. Large and massive tears.
Technique of open repair. Orthop Clin North Am, 1997. 28(2): p. 179-93.
8. Galatz, L.M., S. Griggs, B.D. Cameron, and J.P. Iannotti, Prospective
longitudinal analysis of postoperative shoulder function : a ten-year follow-up study of
full-thickness rotator cuff tears. J Bone Joint Surg Am, 2001. 83-A(7): p. 1052-6.
11
9. Murray, T.F., Jr., G. Lajtai, R.M. Mileski, and S.J. Snyder, Arthroscopic repair of
medium to large full-thickness rotator cuff tears: outcome at 2- to 6-year follow-up. J
Shoulder Elbow Surg, 2002. 11(1): p. 19-24.
10. Derwin, K.A., S.F. Badylak, S.P. Steinmann, and J.P. Iannotti, Extracellular
matrix scaffold devices for rotator cuff repair. J Shoulder Elbow Surg. 19(3): p. 467-76.
11. Riley, G.P., R.L. Harrall, C.R. Constant, M.D. Chard, T.E. Cawston, and B.L.
Hazleman, Tendon degeneration and chronic shoulder pain: changes in the collagen
composition of the human rotator cuff tendons in rotator cuff tendinitis. Ann Rheum Dis,
1994. 53(6): p. 359-66.
12. Goutallier, D., J.M. Postel, P. Gleyze, P. Leguilloux, and S. Van Driessche,
Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after
simple suture of full-thickness tears. J Shoulder Elbow Surg, 2003. 12(6): p. 550-4.
13. Bartolozzi, A., D. Andreychik, and S. Ahmad, Determinants of outcome in the
treatment of rotator cuff disease. Clin Orthop Relat Res, 1994(308): p. 90-7.
14. Cofield, R.H., J. Parvizi, P.J. Hoffmeyer, W.L. Lanzer, D.M. Ilstrup, and C.M.
Rowland, Surgical repair of chronic rotator cuff tears. A prospective long-term study. J
Bone Joint Surg Am, 2001. 83-A(1): p. 71-7.
15. Romeo, A.A., D.W. Hang, B.R. Bach, Jr., and S. Shott, Repair of full thickness
rotator cuff tears. Gender, age, and other factors affecting outcome. Clin Orthop Relat
Res, 1999(367): p. 243-55.
16. Koman, L.A., B.P. Smith, and J.S. Shilt, Cerebral palsy. Lancet, 2004.
363(9421): p. 1619-31.
12
17. Gladstone, J.N., J.Y. Bishop, I.K. Lo, and E.L. Flatow, Fatty infiltration and
atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with
poor functional outcome. Am J Sports Med, 2007. 35(5): p. 719-28.
18. Gerber, C., B. Fuchs, and J. Hodler, The results of repair of massive tears of the
rotator cuff. J Bone Joint Surg Am, 2000. 82(4): p. 505-15.
19. Dona, E., M.P. Gianoutsos, and W.R. Walsh, Optimizing biomechanical
performance of the 4-strand cruciate flexor tendon repair. J Hand Surg Am, 2004. 29(4):
p. 571-80.
20. Aslam, A. and A. Afoke, A new core suture technique for flexor tendon repair:
biomechanical analysis of tensile strength and gap formation. J Hand Surg Br, 2000.
25(4): p. 390-2.
21. Mortenson, R.A. and J.R. Urbaniak, Analysis of tensile strength of tendon
anastomosis. Surg Forum, 1972. 23(0): p. 470-1.
22. Dinopoulos, H.T., M.I. Boyer, M.E. Burns, R.H. Gelberman, and M.J. Silva, The
resistance of a four- and eight-strand suture technique to gap formation during tensile
testing: an experimental study of repaired canine flexor tendons after 10 days of in vivo
healing. J Hand Surg Am, 2000. 25(3): p. 489-98.
23. Aoki, M., P.R. Manske, D.L. Pruitt, H. Kubota, and B.J. Larson, Canine
cadaveric study of flexor tendon repair using tendon splint: tensile strength and the work
of flexion. Nippon Seikeigeka Gakkai Zasshi, 1995. 69(5): p. 332-41.
24. Barrie, K.A., S.W. Wolfe, C. Shean, D. Shenbagamurthi, J.F. Slade, 3rd, and
M.M. Panjabi, A biomechanical comparison of multistrand flexor tendon repairs using an
in situ testing model. J Hand Surg Am, 2000. 25(3): p. 499-506.
13
25. Greenwald, D.P., M.A. Randolph, H.Z. Hong, and J.W. May, Jr., Augmented
Becker versus modified Kessler tenorrhaphy in monkeys: dynamic mechanical analysis. J
Hand Surg Am, 1995. 20(2): p. 267-72.
26. McLarney, E., H. Hoffman, and S.W. Wolfe, Biomechanical analysis of the
cruciate four-strand flexor tendon repair. J Hand Surg Am, 1999. 24(2): p. 295-301.
27. Goutallier, D., J.M. Postel, L. Lavau, and J. Bernageau, [Impact of fatty
degeneration of the suparspinatus and infraspinatus msucles on the prognosis of surgical
repair of the rotator cuff]. Rev Chir Orthop Reparatrice Appar Mot, 1999. 85(7): p. 668-
76.
28. Goutallier, D., J.M. Postel, J. Bernageau, L. Lavau, and M.C. Voisin, Fatty
muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin
Orthop Relat Res, 1994(304): p. 78-83.
29. Gupta, R. and T.Q. Lee, Contributions of the different rabbit models to our
understanding of rotator cuff pathology. J Shoulder Elbow Surg, 2007. 16(5 Suppl): p.
S149-57.
30. Mallon, W.J., R.J. Wilson, and C.J. Basamania, The association of suprascapular
neuropathy with massive rotator cuff tears: a preliminary report. J Shoulder Elbow Surg,
2006. 15(4): p. 395-8.
31. Kelly, B.T., R.J. Williams, F.A. Cordasco, S.I. Backus, J.C. Otis, D.E. Weiland,
et al., Differential patterns of muscle activation in patients with symptomatic and
asymptomatic rotator cuff tears. J Shoulder Elbow Surg, 2005. 14(2): p. 165-71.
14
32. Greiner, A., K. Golser, M. Wambacher, F. Kralinger, and G. Sperner, The course
of the suprascapular nerve in the supraspinatus fossa and its vulnerability in muscle
advancement. J Shoulder Elbow Surg, 2003. 12(3): p. 256-9.
33. Warner, J.P., R.J. Krushell, A. Masquelet, and C. Gerber, Anatomy and
relationships of the suprascapular nerve: anatomical constraints to mobilization of the
supraspinatus and infraspinatus muscles in the management of massive rotator-cuff
tears. J Bone Joint Surg Am, 1992. 74(1): p. 36-45.
34. Piasecki, D.P., A.A. Romeo, B.R. Bach, Jr., and G.P. Nicholson, Suprascapular
neuropathy. J Am Acad Orthop Surg, 2009. 17(11): p. 665-76.
35. Jamali, A.A., P. Afshar, R.A. Abrams, and R.L. Lieber, Skeletal muscle response
to tenotomy. Muscle Nerve, 2000. 23(6): p. 851-62.
36. Baker, J.H. and E.C. Hall-Craggs, Changes in sarcomere length following
tenotomy in the rat. Muscle Nerve, 1980. 3(5): p. 413-6.
37. Meyer, D.C., H. Hoppeler, B. von Rechenberg, and C. Gerber, A
pathomechanical concept explains muscle loss and fatty muscular changes following
surgical tendon release. J Orthop Res, 2004. 22(5): p. 1004-7.
38. Safran, O., K.A. Derwin, K. Powell, and J.P. Iannotti, Changes in rotator cuff
muscle volume, fat content, and passive mechanics after chronic detachment in a canine
model. J Bone Joint Surg Am, 2005. 87(12): p. 2662-70.
39. Barton, E.R., J.A. Gimbel, G.R. Williams, and L.J. Soslowsky, Rat supraspinatus
muscle atrophy after tendon detachment. J Orthop Res, 2005. 23(2): p. 259-65.
15
40. Halder, A.M., S.W. O'Driscoll, G. Heers, N. Mura, M.E. Zobitz, K.N. An, et al.,
Biomechanical comparison of effects of supraspinatus tendon detachments, tendon
defects, and muscle retractions. J Bone Joint Surg Am, 2002. 84-A(5): p. 780-5.
41. Hansen, M.L., J.C. Otis, J.S. Johnson, F.A. Cordasco, E.V. Craig, and R.F.
Warren, Biomechanics of massive rotator cuff tears: implications for treatment. J Bone
Joint Surg Am, 2008. 90(2): p. 316-25.
42. Bjorkenheim, J.M., Structure and function of the rabbit's supraspinatus muscle
after resection of its tendon. Acta Orthop Scand, 1989. 60(4): p. 461-3.
43. Fabis, J., P. Kordek, A. Bogucki, and J. Mazanowska-Gajdowicz, Function of the
rabbit supraspinatus muscle after large detachment of its tendon: 6-week, 3-month, and
6-month observation. J Shoulder Elbow Surg, 2000. 9(3): p. 211-6.
44. Fabis, J., P. Kordek, A. Bogucki, M. Synder, and H. Kolczynska, Function of the
rabbit supraspinatus muscle after detachment of its tendon from the greater tubercle.
Observations up to 6 months. Acta Orthop Scand, 1998. 69(6): p. 570-4.
45. Coleman, S.H., S. Fealy, J.R. Ehteshami, J.D. MacGillivray, D.W. Altchek, R.F.
Warren, et al., Chronic rotator cuff injury and repair model in sheep. J Bone Joint Surg
Am, 2003. 85-A(12): p. 2391-402.
46. Seyler, T.M., B.P. Smith, D.R. Marker, J. Ma, J. Shen, T.L. Smith, et al.,
Botulinum neurotoxin as a therapeutic modality in orthopaedic surgery: more than
twenty years of experience. J Bone Joint Surg Am, 2008. 90 Suppl 4: p. 133-45.
47. Ramachandran, M. and D.M. Eastwood, Botulinum toxin and its orthopaedic
applications. J Bone Joint Surg Br, 2006. 88(8): p. 981-7.
16
48. Escamilla, R.F. and J.R. Andrews, Shoulder muscle recruitment patterns and
related biomechanics during upper extremity sports. Sports Med, 2009. 39(7): p. 569-90.
49. Reinold, M.M., L.C. Macrina, K.E. Wilk, G.S. Fleisig, S. Dun, S.W. Barrentine,
et al., Electromyographic analysis of the supraspinatus and deltoid muscles during 3
common rehabilitation exercises. J Athl Train, 2007. 42(4): p. 464-9.
50. Malanga, G.A., Y.N. Jenp, E.S. Growney, and K.N. An, EMG analysis of
shoulder positioning in testing and strengthening the supraspinatus. Med Sci Sports
Exerc, 1996. 28(6): p. 661-4.
51. Ma, J., J. Shen, B.P. Smith, A. Ritting, T.L. Smith, and L.A. Koman,
Bioprotection of tendon repair: adjunctive use of botulinum toxin A in Achilles tendon
repair in the rat. J Bone Joint Surg Am, 2007. 89(10): p. 2241-9.
52. De Aguiar, G., L.A. Chait, D. Schultz, S. Bleloch, A. Theron, C.N. Snijman, et
al., Chemoprotection of flexor tendon repairs using botulinum toxin. Plast Reconstr Surg,
2009. 124(1): p. 201-9.
17
CHAPTER 2
EVALUATION OF IN VIVO ROTATOR CUFF MUSCLE
FUNCTION AFTER ACUTE AND CHRONIC DETACHMENT OF
THE SUPRASPINATUS TENDON: AN EXPERIMENTAL STUDY IN
AN ANIMAL MODEL
Sandeep Mannava, Johannes F. Plate, Patrick W. Whitlock, Michael F. Callahan,
Thorsten M. Seyler, L. Andrew Koman, Thomas L. Smith, Christopher J. Tuohy
The following manuscript was published in JBJS (Am.). 2011 Sept 21. PMID: 21938374.
This chapter is reprinted with permission. Stylistic variations are due to the requirements
of the journal. Mannava performed the experiments, prepared the manuscript, and served
as corresponding author. T.L. Smith acted in an advisory and editorial capacity.
ADDENDUM: During committee review of the dissertation, it was determined that the
photomicrographs that comprise chapter 2, figure 2 may have been taken on two separate microscopes with
different focal lengths, resulting in images that have different magnification. The figure has been published
after peer-review. The study of muscle atrophy following tenotomy in the rat supraspinatus was extensively
studied by Barton et al (J Orthop Res. 2005 Mar; 23(2):259-65) who performed quantitative histological
analysis. Barton et al concluded that tendon detachment results in decreased muscle mass, decreased
muscle fiber size, and increased collagen content/fibrosis—these findings were significant when compared
to controls. For further information regarding histology of the rat rotator cuff after injury, please refer to the
manuscript Barton ER, Gimbel JA, Williams GR, Soslowsky LJ. Rat supraspinatus muscle atrophy after
tendon detachment. J Orthop Res. 2005 Mar; 23(2):259-65. PMID 15734235.
18
ABSTRACT
Background: Surgical repair of large chronic rotator cuff tears can be technically
demanding because it requires manipulation of a muscle-tendon unit that is scarred,
retracted, and stiffer than normal, which contribute to increased repair tensions. This
study characterizes in vivo rotator cuff muscle-tendon unit function after acute and
chronic injury at surgically relevant preload tensions.
Methods: Sixty-two Sprague-Dawley rats—healthy uninjured controls (n=22), acute
injury group (n=20), and chronic injury group (n=20)—underwent in vivo muscle force
testing and electromyography (EMG) of their supraspinatus muscle-tendon unit at various
preload tensions.
Results: Preload tension affected the maximal supraspinatus muscle contractile force in
all experimental groups (p<0.05). At the peak tension required to repair an acute tear,
there was between a 28%-30% reduction in maximal tetanic contraction amplitude in all
experimental groups (p<0.05). At the peak tension required to repair a chronic tear, there
was between a 40%-53% reduction in maximal tetanic contraction amplitude in all
experimental groups (p<0.05). The uninjured control group showed increased muscle
endurance (p<0.05) compared to the acute injury and chronic injury experimental groups
at all preload tensions. The chronically injured group showed reduced compound motor
action potential (CMAP) amplitude (p<0.05).
Conclusions: Both acute and chronic injury experimental groups demonstrated a
functional impairment related to increasing preload tensions, with the only difference
being the amount of tension required for surgical repair. The present study also associates

19
increased time from rotator cuff tendon injury to impaired in vivo rotator cuff muscle
EMG findings.
Clinical Relevance: The findings suggest that earlier surgical intervention, requiring
lower repair tension, may lead to improved functional outcomes.
20
INTRODUCTION
With the increasing age and activity level of the population, there has been an
increase in both prevalence and operative interventions for symptomatic rotator cuff tears
[2, 3]. Often, surgical intervention for rotator cuff tears is delayed until after conservative
treatment has failed [3, 45]. Surgical repair of a large chronic rotator cuff tear may
require the manipulation of a muscle-tendon unit that is scarred, retracted, and stiffer than
normal [38, 40, 41]. These physical changes contribute to the technical challenge of
rotator cuff surgery.
Changes in the structure of the muscle-tendon unit after rotator cuff injury
contribute to the increased tension required to attach the torn rotator cuff tendon back to
its anatomic humeral head footprint [38, 45, 53-55]. The increased repair tension may
impair healing at the tendon-bone interface, contributing to recurrent tearing after surgery
[53]. Additionally, the function of chronically torn rotator cuff muscle-tendon units is
also impaired after injury [42-45, 56]. With current repair techniques, reduced muscle
function is sometimes irreversible, even after a relatively short period of time from injury
[55].
The present study characterizes rotator cuff muscle-tendon unit function under
acute and chronic injury conditions at surgically relevant preload tensions. The surgically
relevant preload tensions were chosen to recreate the stress placed upon the muscle-
tendon unit during rotator cuff repair surgery. These preload tensions were determined
based on previously reported repair tensions in this animal model [53]. Our study used a
rat rotator cuff model to study in vivo muscle force and electromyography (EMG) of the
rotator cuff after acute and chronic detachment of the supraspinatus tendon. The study

21
hypothesized that observed muscle function would be impaired at tensions required to
perform rotator cuff repair surgery and that electrophysiological EMG assessment of the
muscle would be impaired in the chronic tendon tear setting.
MATERIALS AND METHODS:
Muscle function in 26 male Sprague-Dawley rats weighing 400-450 g (Charles
River, Wilmington, MA) were studied. Six un-injured rats served as healthy controls; the
remaining 20 rats had unilateral supraspinatus tendon detachment by methods previously
described [53]. These animals were divided into an acute injury group (n=10) with
muscle function tested four weeks after supraspinatus tenotomy and a chronic injury
group (n=10) with muscle function tested twelve weeks after supraspinatus tenotomy.
Additionally, EMG was studied in a total of 36 male Sprague-Dawely rats. Sixteen un-
injured rats served as healthy controls. The remaining 20 rats had their supraspinatus
tendon sharply detached and were divided into an acute injury group (n=10) and a
chronic injury group (n=10). Animals were sacrificed immediately after in vivo muscle
force and EMG testing. All experimentation was conducted after approval from the
Institutional Animal Care and Use Committee.
Muscle Force Testing:
The surgical exposure and in vivo physiological testing of the rat supraspinatus
muscle-tendon unit were conducted based upon previously described experimental
methods [57], using a physiological testing apparatus (Fig. 1) [57, 58]. The muscle-
tendon unit then was pretensioned to tensions ranging between 0.05N and 4N. Gimbel et
al. determined that these preload tensions are clinically relevant for this animal model
[53, 54], approximately 1.7N of peak repair tension was required at four weeks post-
22
tenotomy, and approximately 2.5N of peak repair tension was required at twelve weeks
post-tenotomy [53, 54]. A maximal preload tension of 4N was used to attain a full
preload tension versus maximum amplitude curve without causing gross injury.
Suprascapular nerve stimulation protocols were executed at these varying preload
tensions. The suprascapular nerve was supra-maximally stimulated with 1.5V during
muscle force recordings. To ensure that 1.5V was a supra-maximal stimulation, a range
of stimuli were tested between 0.6V to 2.0V, and in all cases, 1.5V produced maximal
single twitch muscle contraction.
To test frequency-dependent muscle fiber recruitment, the suprascapular nerve
was stimulated at frequencies of 1Hz, 60Hz, 80Hz, 100Hz, 150Hz, and 200Hz for one
second, and the maximal amplitude of the force of contraction was recorded. A recovery
time of 60 seconds was allowed between stimuli. This recovery time allowed for full
recovery of maximal contractile force. For the frequency-dependant recruitment protocol,
nerve stimulation was performed at a preload tension of 0.4N, the tension required to
repair the supraspinatus tendon immediately after tenotomy [53, 54].
The compliance and stiffness of the muscle was assessed by measuring the
displacement of the muscle-tendon unit (from the starting preload tension of 0.05N,
which was set as 0mm displacement) required to attain the various preload tensions. After
the muscle-tendon unit was immobilized to the linearly translating stage (Fig. 1A), the
stage was displaced away from the force transducer, to preload tensions ranging from
0.05N to 4N, and the amount of displacement required to attain these tension was
recorded. To test tension versus maximal single twitch and tetany force of contraction,
the muscle-tendon unit was ranged from 0.05N to 4N of preload tension, and the nerve
23
was stimulated at 1Hz and 150Hz for five seconds with a recovery time of 60 seconds
between stimuli.
For the fatigue protocol, the nerve was stimulated at 100Hz for 150 seconds at
preload tensions of 0.4N, 1.3N, and 2N with 300 seconds between stimuli to allow for
complete recovery. The amplitude of contraction was continually measured and recorded
throughout the entire 150 seconds of nerve stimulation. These data were expressed as
change from maximum standardized amplitude as a function of time at one second (max
amplitude), 30 seconds, 60 seconds, 90 seconds, 120 seconds, and 150 seconds.
Muscle Force Data Standardization
All muscle force measurements during testing were expressed as percentages of
the maximal contractile force generated by the tested muscle in order to normalize for
animal variability. Physiological testing in the in vivo setting results in data that is
variable due to experimental preparation and other environmental differences beyond the
control of the investigator. Increasing the number of animals studied could have reduced
the variability of the muscle force measurements; but in the present study this was not
feasible due to the large number of animals that would have been required. Therefore, in
order to compare the animals and groups, standardization was necessary. Previously
published reports used similar percentages in expressing their data [42-44], normalizing
against either the same muscle or the contralateral muscle in order to facilitate the
comparison of contractile amplitudes between animals and groups. After consultation
with a statistician, use of the contralateral muscle for standardization was determined to
be inappropriate because it was possible that muscle function of the contralateral
uninjured limb could be affected by injuring the opposite supraspinatus tendon.

24
EMG Testing
EMG testing was performed using a Sierra Wave (Caldwell Laboratories,
Kennewick, WA) electrodiagnostic system. EMG testing consisted of supramaximal
stimulation of the suprascapular nerve for a duration of 0.1ms with a range of constant
currents (0.5mA to 2mA) to ensure that maximal compound motor action potential
amplitude was attained. Maximal compound motor action potential amplitude and area
under the curve (AUC) were recorded using a needle electrode placed at different
locations (proximal, middle, distal) on the supraspinatus muscle belly. The testing
protocol was repeated three times at each location, and the single result with the highest
amplitude and appropriate compound motor action potential waveform morphometry was
recorded.
Histological analysis
A total of 18 samples were collected from the uninjured control (n = 6), four
weeks post-tenotomy (n = 6), and twelve weeks post-tenotomy (n = 6) groups, after
muscle force testing. The mid-substance portion of the supraspinatus muscles were
processed for histology, embedded in paraffin, and sectioned with a microtome to obtain
5.0 μm thick cross-sections. The sections were mounted on slides and stained using
hemotoxylin and eosin (H & E, Sigma, St. Louis, MO), Masson’s Trichrome (Sigma, St.
Louis, MO), and 4,6-diamidino-2-phenylindole (DAPI, Vector, Burlingame, CA).
Representative light (H&E and Masson’s Trichrome) and fluorescence (DAPI)
micrographs were taken at 200x magnification. For DAPI stained sections, three high-
powered 200x, representative photomicrographs were taken per sample and then a
modified counting procedure [59] was used to quantify the fluorescence using ImageJ
25
(NIH, Bethesda, MD). Several of the samples were counted manually to verify the
accuracy of the automated quantification method. The quantified DAPI fluorescence was
averaged for the sample, and the average of the three images was used for further
statistical comparisons between groups. This method of analysis was employed to help
reduce sampling error.
Statistics
For a desired power of 0.8 and α = 0.05, a sample size of n = 5 for each group was
calculated. This calculation was consistent with historical physiological data in a rat
skeletal muscle model system [51, 57]. Muscle force measurements were converted to
percentages, and the data were expressed as averages ± standard error of measurement
(SEM) for each group. All other measurements were expressed as averages ± standard
error of the mean (SEM) for each group. For comparisons between and within groups, a
Two-Way Repeated Measures ANOVA followed by a Tukey post hoc test was
performed. An ANOVA followed by a Tukey post hoc test was used for comparisons of
DAPI quantification, maximal compound motor action potential amplitude, and
compound motor action potential area under the curve between groups. Significance was
defined as p<0.05. A linear regression was generated using the tension applied versus
displacement of the muscle-tendon unit data. Stiffness/compliance was calculated based
on regression analysis.
Source of Funding
All studies were completed with intra-departmental physician-scientist start-up funds. No
external funding source was utilized and no external funding source played a role in this
investigation.
26
RESULTS
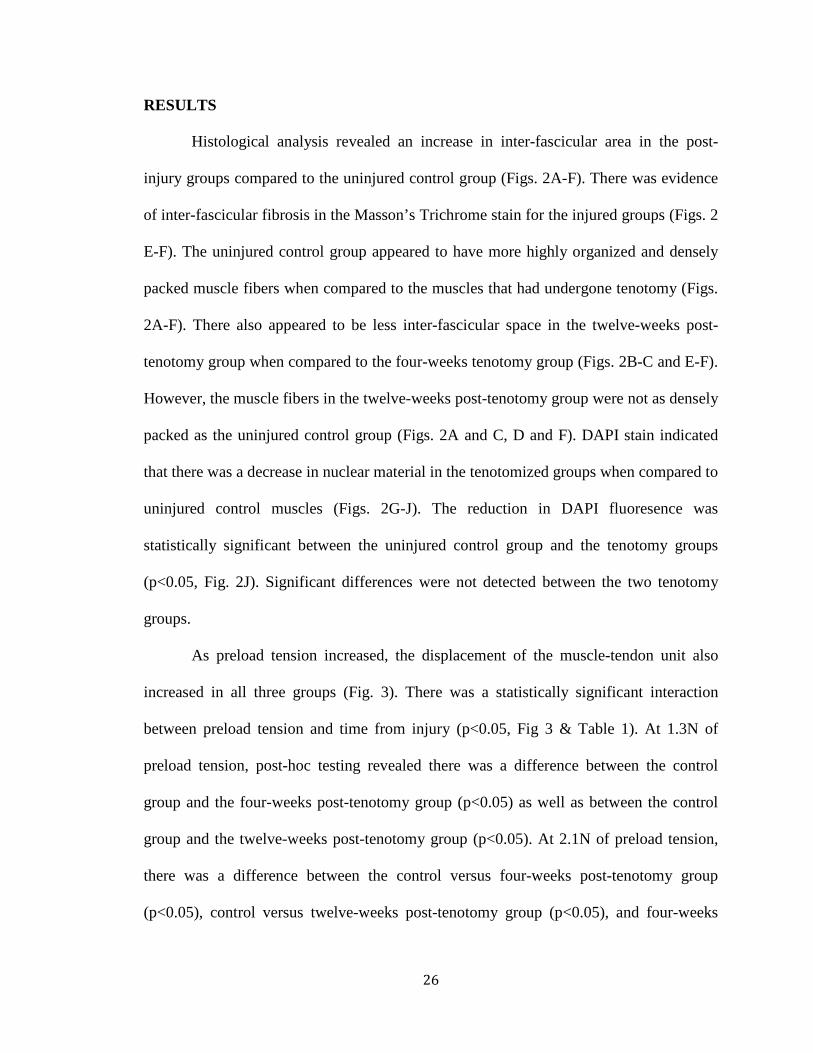
Histological analysis revealed an increase in inter-fascicular area in the post-
injury groups compared to the uninjured control group (Figs. 2A-F). There was evidence
of inter-fascicular fibrosis in the Masson’s Trichrome stain for the injured groups (Figs. 2
E-F). The uninjured control group appeared to have more highly organized and densely
packed muscle fibers when compared to the muscles that had undergone tenotomy (Figs.
2A-F). There also appeared to be less inter-fascicular space in the twelve-weeks post-
tenotomy group when compared to the four-weeks tenotomy group (Figs. 2B-C and E-F).
However, the muscle fibers in the twelve-weeks post-tenotomy group were not as densely
packed as the uninjured control group (Figs. 2A and C, D and F). DAPI stain indicated
that there was a decrease in nuclear material in the tenotomized groups when compared to
uninjured control muscles (Figs. 2G-J). The reduction in DAPI fluoresence was
statistically significant between the uninjured control group and the tenotomy groups
(p<0.05, Fig. 2J). Significant differences were not detected between the two tenotomy
groups.
As preload tension increased, the displacement of the muscle-tendon unit also
increased in all three groups (Fig. 3). There was a statistically significant interaction
between preload tension and time from injury (p<0.05, Fig 3 & Table 1). At 1.3N of
preload tension, post-hoc testing revealed there was a difference between the control
group and the four-weeks post-tenotomy group (p<0.05) as well as between the control
group and the twelve-weeks post-tenotomy group (p<0.05). At 2.1N of preload tension,
there was a difference between the control versus four-weeks post-tenotomy group
(p<0.05), control versus twelve-weeks post-tenotomy group (p<0.05), and four-weeks
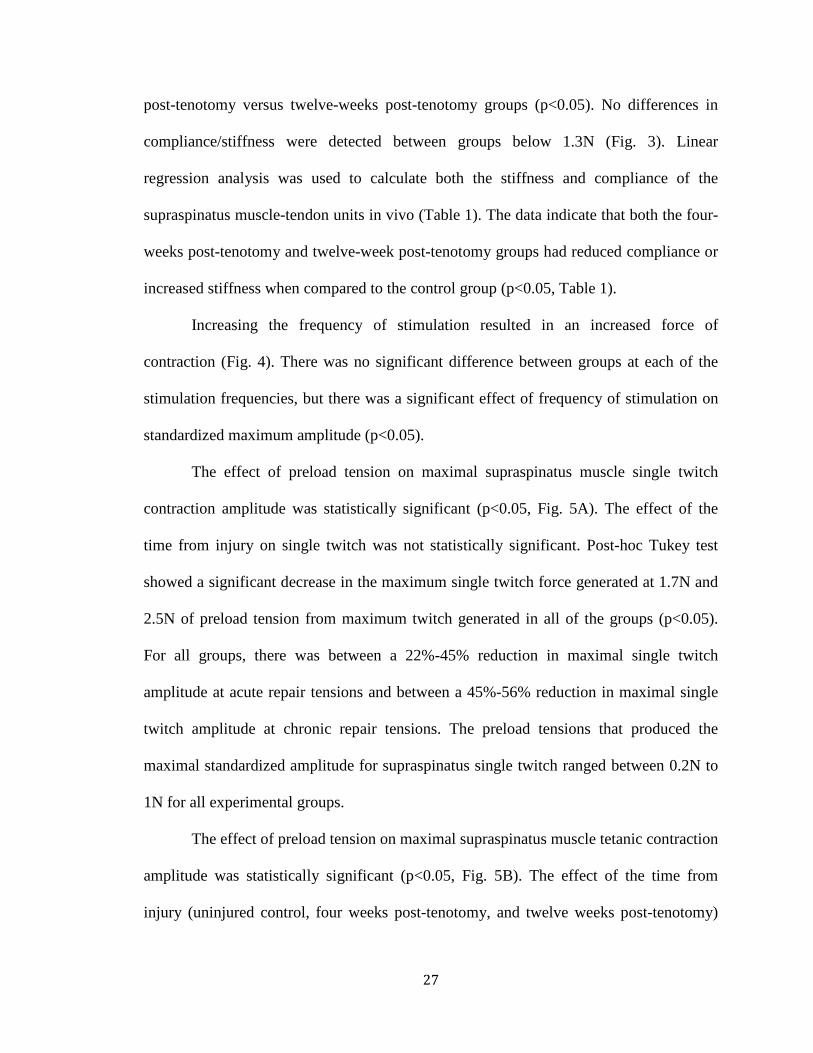
27
post-tenotomy versus twelve-weeks post-tenotomy groups (p<0.05). No differences in
compliance/stiffness were detected between groups below 1.3N (Fig. 3). Linear
regression analysis was used to calculate both the stiffness and compliance of the
supraspinatus muscle-tendon units in vivo (Table 1). The data indicate that both the four-
weeks post-tenotomy and twelve-week post-tenotomy groups had reduced compliance or
increased stiffness when compared to the control group (p<0.05, Table 1).
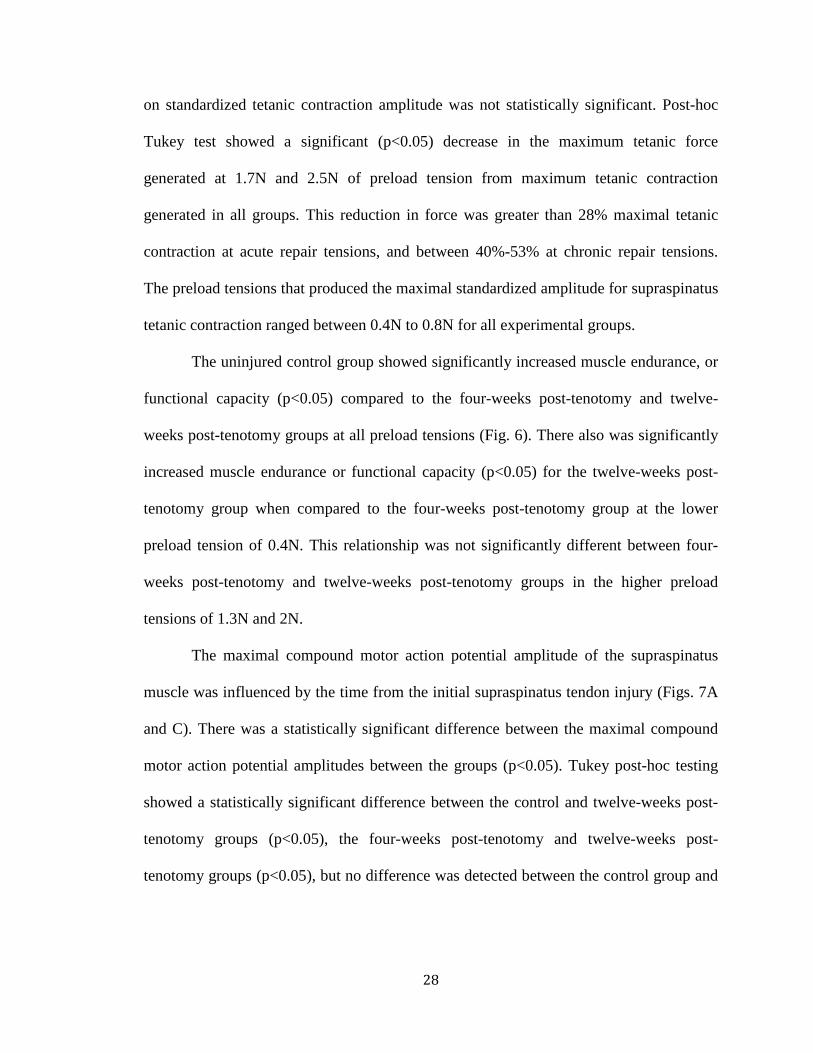
Increasing the frequency of stimulation resulted in an increased force of
contraction (Fig. 4). There was no significant difference between groups at each of the
stimulation frequencies, but there was a significant effect of frequency of stimulation on
standardized maximum amplitude (p<0.05).
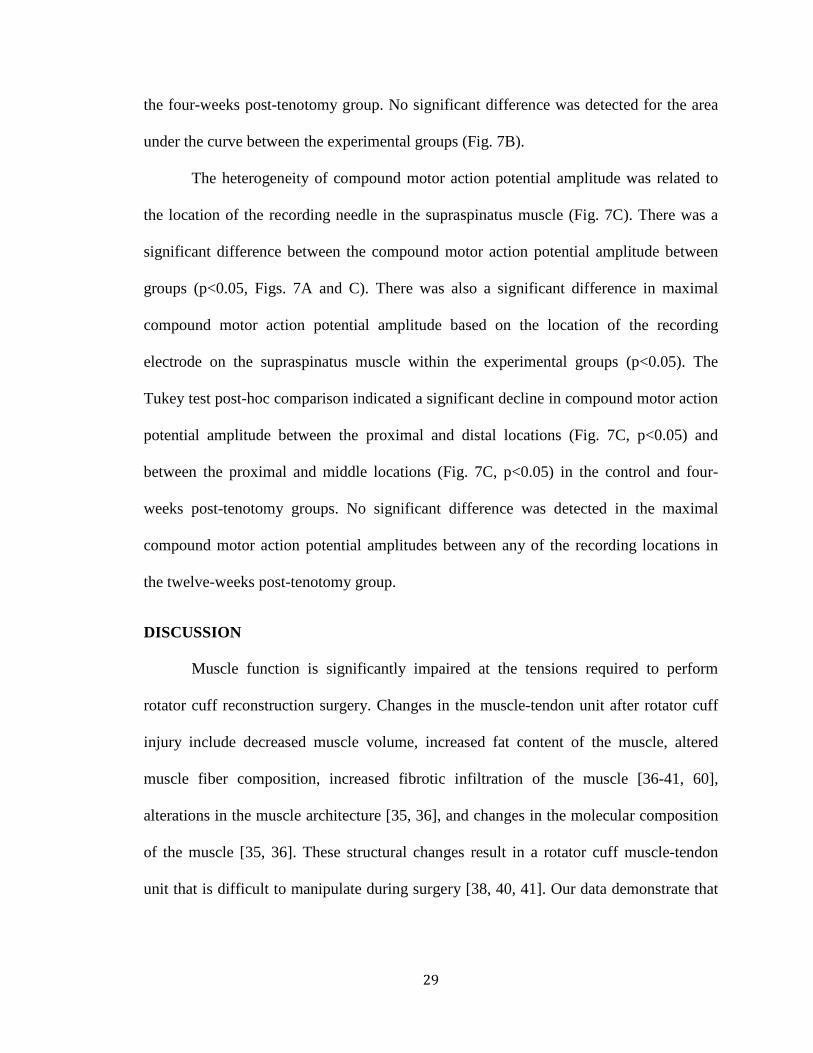
The effect of preload tension on maximal supraspinatus muscle single twitch
contraction amplitude was statistically significant (p<0.05, Fig. 5A). The effect of the
time from injury on single twitch was not statistically significant. Post-hoc Tukey test
showed a significant decrease in the maximum single twitch force generated at 1.7N and
2.5N of preload tension from maximum twitch generated in all of the groups (p<0.05).
For all groups, there was between a 22%-45% reduction in maximal single twitch
amplitude at acute repair tensions and between a 45%-56% reduction in maximal single
twitch amplitude at chronic repair tensions. The preload tensions that produced the
maximal standardized amplitude for supraspinatus single twitch ranged between 0.2N to
1N for all experimental groups.
The effect of preload tension on maximal supraspinatus muscle tetanic contraction
amplitude was statistically significant (p<0.05, Fig. 5B). The effect of the time from
injury (uninjured control, four weeks post-tenotomy, and twelve weeks post-tenotomy)
28
on standardized tetanic contraction amplitude was not statistically significant. Post-hoc
Tukey test showed a significant (p<0.05) decrease in the maximum tetanic force
generated at 1.7N and 2.5N of preload tension from maximum tetanic contraction
generated in all groups. This reduction in force was greater than 28% maximal tetanic
contraction at acute repair tensions, and between 40%-53% at chronic repair tensions.
The preload tensions that produced the maximal standardized amplitude for supraspinatus
tetanic contraction ranged between 0.4N to 0.8N for all experimental groups.
The uninjured control group showed significantly increased muscle endurance, or
functional capacity (p<0.05) compared to the four-weeks post-tenotomy and twelve-
weeks post-tenotomy groups at all preload tensions (Fig. 6). There also was significantly
increased muscle endurance or functional capacity (p<0.05) for the twelve-weeks post-
tenotomy group when compared to the four-weeks post-tenotomy group at the lower
preload tension of 0.4N. This relationship was not significantly different between four-
weeks post-tenotomy and twelve-weeks post-tenotomy groups in the higher preload
tensions of 1.3N and 2N.
The maximal compound motor action potential amplitude of the supraspinatus
muscle was influenced by the time from the initial supraspinatus tendon injury (Figs. 7A
and C). There was a statistically significant difference between the maximal compound
motor action potential amplitudes between the groups (p<0.05). Tukey post-hoc testing
showed a statistically significant difference between the control and twelve-weeks post-
tenotomy groups (p<0.05), the four-weeks post-tenotomy and twelve-weeks post-
tenotomy groups (p<0.05), but no difference was detected between the control group and
29
the four-weeks post-tenotomy group. No significant difference was detected for the area
under the curve between the experimental groups (Fig. 7B).
The heterogeneity of compound motor action potential amplitude was related to
the location of the recording needle in the supraspinatus muscle (Fig. 7C). There was a
significant difference between the compound motor action potential amplitude between
groups (p<0.05, Figs. 7A and C). There was also a significant difference in maximal
compound motor action potential amplitude based on the location of the recording
electrode on the supraspinatus muscle within the experimental groups (p<0.05). The
Tukey test post-hoc comparison indicated a significant decline in compound motor action
potential amplitude between the proximal and distal locations (Fig. 7C, p<0.05) and
between the proximal and middle locations (Fig. 7C, p<0.05) in the control and four-
weeks post-tenotomy groups. No significant difference was detected in the maximal
compound motor action potential amplitudes between any of the recording locations in
the twelve-weeks post-tenotomy group.
DISCUSSION
Muscle function is significantly impaired at the tensions required to perform
rotator cuff reconstruction surgery. Changes in the muscle-tendon unit after rotator cuff
injury include decreased muscle volume, increased fat content of the muscle, altered
muscle fiber composition, increased fibrotic infiltration of the muscle [36-41, 60],
alterations in the muscle architecture [35, 36], and changes in the molecular composition
of the muscle [35, 36]. These structural changes result in a rotator cuff muscle-tendon
unit that is difficult to manipulate during surgery [38, 40, 41]. Our data demonstrate that
30
the preload tensions applied to the acutely and chronically torn rotator cuff muscle-
tendon units during repair result in significantly decreased function.
The frequency dependent recruitment of supraspinatus muscle fibers was similar
regardless of injury group (Fig. 4). Even after tenotomy, the supraspinatus muscle is still
able to produce force when stimulated under certain supra-physiological conditions.
However, current single-stage repair methods using high repair tensions and
physiological nerve activation below the frequencies tested in this experiment may result
in decreased muscle function.
Similar to previous reports, muscle-tendon unit stiffness increased with time from
injury (Fig. 3, Table 1) [38, 40, 41]. There are several possible molecular mechanisms,
including change in sarcomere length and histological changes in muscle structure, which
might contribute to increased stiffness of the muscle-tendon unit after injury [35, 36].
Changes in muscle structure observed histologically (Fig. 2) might be partially
responsible for changes in passive biomechanical properties of the muscle-tendon unit
(Fig 3, Table 1).
Our study demonstrates, that the chronically injured group’s muscle-tendon unit
might gain some compliance (inversely related to stiffness, Table 1). An explanation for
this trend is that secondary attachment due to scarring of the detached tendon to
surrounding tissue results in the re-establishment of load during muscle contraction [42].
This attachment might result in partial reversal of the atrophic changes (Fig. 2) that occur
in the muscle after tendon injury, resulting in improved passive properties (Fig. 3, Table
1). The muscle does not recover fully after the repair of a chronic tear because the tendon
does not heal in a location where the muscle is ideally preloaded or stretched.
31
Muscle function testing demonstrated that there was a significant decline in the
force of muscle contraction at the peak tensions required to repair acutely injured and
chronically injured rotator cuff tears (Figs. 5A and B) [53, 54]. After internally
standardizing the amplitude of supraspinatus contraction, all of the groups responded to
increased preload tension similarly. This finding may indicate that an increased emphasis
needs to be placed on the tensions at which tendons are repaired, as muscle function was
significantly impaired at high repair tensions.
The exercise capacity of supraspinatus muscles associated with completely torn
tendons declines (Fig. 6). The difference between the chronically injured and acutely
injured group might be partially explained by the re-establishment of contraction after
secondary attachment of the torn tendon to surrounding tissue [42]. Our data showed that
as preload tension increases from 0.4N to 1.3N and 2N, the difference between the
acutely injured and chronically injured group was not significant. The greater strain
placed on these muscles associated with the injured tendons resulted in the impaired
ability of the muscle to sustain maximal contraction for an extended period of time. In the
setting of acute and chronic rotator cuff tears, the peak surgical repair tensions would be
sufficient to result in a significantly reduced ability for the muscle to sustain contraction.
This finding has implications for recommendations made for post-operative rehabilitation
protocols and exercise capacity [61-63].
Other investigators have demonstrated that rotator cuff muscles, associated with
torn rotator cuff tendons, fatigue faster and have a lower maximum force of contraction
after injury [42-45, 56, 64, 65]. Our study represents a more complete characterization of
muscle function at surgically relevant preload tensions that simulate the stress placed
32
upon the muscle-tendon unit during and following rotator cuff reconstruction surgery. It
is unclear how accounting for the increased tension will influence outcomes after repair
of torn rotator cuffs. Since a broad range for ideal repair tension was observed in our
study, future studies are needed to investigate, determine, and optimize the ideal repair
tension when repairs are performed.
Neuromuscular function of the supraspinatus muscle as detected by EMG is
significantly impaired after chronic injury to the supraspinatus tendon (Figs. 7 A and C).
Electrophysiological impairment of the supraspinatus muscle following tenotomy may
indicate that suprascapular nerve dysfunction contributes to decreased function following
rotator cuff tears (CME). However, it is possible that these observed compound motor
action potential changes are due to muscle architecture changes described previously in
the literature [36-41, 60] and observed in our histological analysis (Fig. 2). Alternatively,
the decreased compound motor action potential amplitude may result from a combination
of both nerve traction and muscle atrophy. Recently, nerve injury has been implicated as
possibly inciting some of the structural muscular changes that occur after rotator cuff
tendon detachment [29, 66].
Several case series have described an association between rotator cuff tears and
suprascapular neuropathy [30, 67]; however, the present study makes a direct connection
between impaired EMG findings and chronicity of the rotator cuff tear (CME). Future
studies are needed to characterize the mechanisms underlying the electrophysiological
changes observed in the present study, such as nerve tension after tenotomy or specific
histological markers for neuromuscular changes. Ideally nerve conduction velocity would
also be studied during experimentation. However, technical and anatomical limitations of

33
the in vivo model did not allow for consistent placement of the stimulator and the
recording electrode at a fixed distance to allow for measurement of the distance between
the stimulating electrode and the recording electrode.
Limitation of the physiological testing related to replication of joint-biomechanics
and the use of general anesthesia when using the rat rotator cuff animal model system are
previously noted in the literature [57]. The testing of more animals would have reduced
variability and increased the power of the study, perhaps revealing a significant
experimental group effect on preload tension versus maximal standardized muscle force
generated. Based upon the confidence intervals (Fig. 5), we conclude that a statistically
significant difference would probably not represent a physiological or clinically relevant
difference in this animal system. The experimental groups responded similarly to preload
tension, with increasing preload tensions reducing the force of muscle contraction
(p<0.05, Fig. 5).
The four-weeks and twelve-weeks post-tenotomy time-points were selected to
represent an acute and chronic rotator cuff tear, as the repair tension essentially plateaus
at twelve weeks post-tenotomy [53, 54]. In this rat rotator cuff model, spontaneous
healing and formation of a pseudo-tendon probably results in a reversal of atrophy, which
is not consistent with the human condition. Further, this animal model does not undergo
the robust fibro-fatty infiltration (Fig. 2) that is observed in chronic human rotator cuff
tears and large animal rotator cuff chronic injury models [37-39, 68, 69].
Based on the findings of our study, it is likely that impaired rotator cuff muscle
function at the peak repair tensions required to perform rotator cuff repair surgery will
disrupt the balance of gleno-humeral joint forces, thus affecting post-operative shoulder
34
biomechanics. Both acute and chronic injury experimental groups demonstrated a
functional impairment related to increasing preload tensions, with the only difference
being the amount of tension required at the time of surgical repair. Similarly, Davidson et
al demonstrated that excessive repair tension (in excess of eight pounds force) is
associated with worse clinical outcomes, when compared to patients whose rotator cuffs
required lower tension for repair (approximately two pounds force) [70]. Further,
impaired neuromuscular activity associated with the chronically torn rotator cuff may
contribute to impaired function following injury. Our study directly associates impaired
EMG findings to time from injury of the rotator cuff tendon. The findings suggest that
functional outcomes may be improved by earlier intervention at lower repair tensions;
however, future studies are needed to test this hypothesis.
ACKNOWLEDGEMENTS
We would like to thank Dr. Beth P. Smith, Dr. Riyaz H. Jinnah, Mrs. Eileen
Martin, and Mrs. Casey Northam for their support in the planning and execution of the
experiments, as well as useful suggestions in the preparation of this manuscript.
This project is taken in part from a dissertation submitted to the Neuroscience
Program, Wake Forest University Graduate School of Arts and Sciences, in partial
fulfillment of the requirements for the degree of Doctor of Philosophy.
35
REFERENCES
1. Sher, J.S., J.W. Uribe, A. Posada, B.J. Murphy, and M.B. Zlatkin, Abnormal
findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg
Am, 1995. 77(1): p. 10-5.
2. Oh, J.H., S.H. Kim, H.M. Ji, K.H. Jo, S.W. Bin, and H.S. Gong, Prognostic
factors affecting anatomic outcome of rotator cuff repair and correlation with functional
outcome. Arthroscopy, 2009. 25(1): p. 30-9.
3. Oh, L.S., B.R. Wolf, M.P. Hall, B.A. Levy, and R.G. Marx, Indications for
rotator cuff repair: a systematic review. Clin Orthop Relat Res, 2007. 455: p. 52-63.
4. Favard, L., G. Bacle, and J. Berhouet, Rotator cuff repair. Joint Bone Spine,
2007. 74(6): p. 551-7.
5. Aurora, A., J. McCarron, J.P. Iannotti, and K. Derwin, Commercially available
extracellular matrix materials for rotator cuff repairs: state of the art and future trends. J
Shoulder Elbow Surg, 2007. 16(5 Suppl): p. S171-8.
6. Bigliani, L.U., F.A. Cordasco, S.J. McIlveen, and E.S. Musso, Operative
treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am, 1992. 74(10): p.
1505-15.
7. Cordasco, F.A. and L.U. Bigliani, The rotator cuff. Large and massive tears.
Technique of open repair. Orthop Clin North Am, 1997. 28(2): p. 179-93.
8. Galatz, L.M., S. Griggs, B.D. Cameron, and J.P. Iannotti, Prospective
longitudinal analysis of postoperative shoulder function : a ten-year follow-up study of
full-thickness rotator cuff tears. J Bone Joint Surg Am, 2001. 83-A(7): p. 1052-6.
36
9. Murray, T.F., Jr., G. Lajtai, R.M. Mileski, and S.J. Snyder, Arthroscopic repair of
medium to large full-thickness rotator cuff tears: outcome at 2- to 6-year follow-up. J
Shoulder Elbow Surg, 2002. 11(1): p. 19-24.
10. Derwin, K.A., S.F. Badylak, S.P. Steinmann, and J.P. Iannotti, Extracellular
matrix scaffold devices for rotator cuff repair. J Shoulder Elbow Surg. 19(3): p. 467-76.
11. Riley, G.P., R.L. Harrall, C.R. Constant, M.D. Chard, T.E. Cawston, and B.L.
Hazleman, Tendon degeneration and chronic shoulder pain: changes in the collagen
composition of the human rotator cuff tendons in rotator cuff tendinitis. Ann Rheum Dis,
1994. 53(6): p. 359-66.
12. Goutallier, D., J.M. Postel, P. Gleyze, P. Leguilloux, and S. Van Driessche,
Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after
simple suture of full-thickness tears. J Shoulder Elbow Surg, 2003. 12(6): p. 550-4.
13. Bartolozzi, A., D. Andreychik, and S. Ahmad, Determinants of outcome in the
treatment of rotator cuff disease. Clin Orthop Relat Res, 1994(308): p. 90-7.
14. Cofield, R.H., J. Parvizi, P.J. Hoffmeyer, W.L. Lanzer, D.M. Ilstrup, and C.M.
Rowland, Surgical repair of chronic rotator cuff tears. A prospective long-term study. J
Bone Joint Surg Am, 2001. 83-A(1): p. 71-7.
15. Romeo, A.A., D.W. Hang, B.R. Bach, Jr., and S. Shott, Repair of full thickness
rotator cuff tears. Gender, age, and other factors affecting outcome. Clin Orthop Relat
Res, 1999(367): p. 243-55.
16. Koman, L.A., B.P. Smith, and J.S. Shilt, Cerebral palsy. Lancet, 2004.
363(9421): p. 1619-31.
37
17. Gladstone, J.N., J.Y. Bishop, I.K. Lo, and E.L. Flatow, Fatty infiltration and
atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with
poor functional outcome. Am J Sports Med, 2007. 35(5): p. 719-28.
18. Gerber, C., B. Fuchs, and J. Hodler, The results of repair of massive tears of the
rotator cuff. J Bone Joint Surg Am, 2000. 82(4): p. 505-15.
19. Dona, E., M.P. Gianoutsos, and W.R. Walsh, Optimizing biomechanical
performance of the 4-strand cruciate flexor tendon repair. J Hand Surg Am, 2004. 29(4):
p. 571-80.
20. Aslam, A. and A. Afoke, A new core suture technique for flexor tendon repair:
biomechanical analysis of tensile strength and gap formation. J Hand Surg Br, 2000.
25(4): p. 390-2.
21. Mortenson, R.A. and J.R. Urbaniak, Analysis of tensile strength of tendon
anastomosis. Surg Forum, 1972. 23(0): p. 470-1.
22. Dinopoulos, H.T., M.I. Boyer, M.E. Burns, R.H. Gelberman, and M.J. Silva, The
resistance of a four- and eight-strand suture technique to gap formation during tensile
testing: an experimental study of repaired canine flexor tendons after 10 days of in vivo
healing. J Hand Surg Am, 2000. 25(3): p. 489-98.
23. Aoki, M., P.R. Manske, D.L. Pruitt, H. Kubota, and B.J. Larson, Canine
cadaveric study of flexor tendon repair using tendon splint: tensile strength and the work
of flexion. Nippon Seikeigeka Gakkai Zasshi, 1995. 69(5): p. 332-41.
24. Barrie, K.A., S.W. Wolfe, C. Shean, D. Shenbagamurthi, J.F. Slade, 3rd, and
M.M. Panjabi, A biomechanical comparison of multistrand flexor tendon repairs using an
in situ testing model. J Hand Surg Am, 2000. 25(3): p. 499-506.

38
25. Greenwald, D.P., M.A. Randolph, H.Z. Hong, and J.W. May, Jr., Augmented
Becker versus modified Kessler tenorrhaphy in monkeys: dynamic mechanical analysis. J
Hand Surg Am, 1995. 20(2): p. 267-72.
26. McLarney, E., H. Hoffman, and S.W. Wolfe, Biomechanical analysis of the
cruciate four-strand flexor tendon repair. J Hand Surg Am, 1999. 24(2): p. 295-301.
27. Goutallier, D., J.M. Postel, L. Lavau, and J. Bernageau, [Impact of fatty
degeneration of the suparspinatus and infraspinatus msucles on the prognosis of surgical
repair of the rotator cuff]. Rev Chir Orthop Reparatrice Appar Mot, 1999. 85(7): p. 668-
76.
28. Goutallier, D., J.M. Postel, J. Bernageau, L. Lavau, and M.C. Voisin, Fatty
muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin
Orthop Relat Res, 1994(304): p. 78-83.
29. Gupta, R. and T.Q. Lee, Contributions of the different rabbit models to our
understanding of rotator cuff pathology. J Shoulder Elbow Surg, 2007. 16(5 Suppl): p.
S149-57.
30. Mallon, W.J., R.J. Wilson, and C.J. Basamania, The association of suprascapular
neuropathy with massive rotator cuff tears: a preliminary report. J Shoulder Elbow Surg,
2006. 15(4): p. 395-8.
31. Kelly, B.T., R.J. Williams, F.A. Cordasco, S.I. Backus, J.C. Otis, D.E. Weiland,
et al., Differential patterns of muscle activation in patients with symptomatic and
asymptomatic rotator cuff tears. J Shoulder Elbow Surg, 2005. 14(2): p. 165-71.
39
32. Greiner, A., K. Golser, M. Wambacher, F. Kralinger, and G. Sperner, The course
of the suprascapular nerve in the supraspinatus fossa and its vulnerability in muscle
advancement. J Shoulder Elbow Surg, 2003. 12(3): p. 256-9.
33. Warner, J.P., R.J. Krushell, A. Masquelet, and C. Gerber, Anatomy and
relationships of the suprascapular nerve: anatomical constraints to mobilization of the
supraspinatus and infraspinatus muscles in the management of massive rotator-cuff
tears. J Bone Joint Surg Am, 1992. 74(1): p. 36-45.
34. Piasecki, D.P., A.A. Romeo, B.R. Bach, Jr., and G.P. Nicholson, Suprascapular
neuropathy. J Am Acad Orthop Surg, 2009. 17(11): p. 665-76.
35. Jamali, A.A., P. Afshar, R.A. Abrams, and R.L. Lieber, Skeletal muscle response
to tenotomy. Muscle Nerve, 2000. 23(6): p. 851-62.
36. Baker, J.H. and E.C. Hall-Craggs, Changes in sarcomere length following
tenotomy in the rat. Muscle Nerve, 1980. 3(5): p. 413-6.
37. Meyer, D.C., H. Hoppeler, B. von Rechenberg, and C. Gerber, A
pathomechanical concept explains muscle loss and fatty muscular changes following
surgical tendon release. J Orthop Res, 2004. 22(5): p. 1004-7.
38. Safran, O., K.A. Derwin, K. Powell, and J.P. Iannotti, Changes in rotator cuff
muscle volume, fat content, and passive mechanics after chronic detachment in a canine
model. J Bone Joint Surg Am, 2005. 87(12): p. 2662-70.
39. Barton, E.R., J.A. Gimbel, G.R. Williams, and L.J. Soslowsky, Rat supraspinatus
muscle atrophy after tendon detachment. J Orthop Res, 2005. 23(2): p. 259-65.
40
40. Halder, A.M., S.W. O'Driscoll, G. Heers, N. Mura, M.E. Zobitz, K.N. An, et al.,
Biomechanical comparison of effects of supraspinatus tendon detachments, tendon
defects, and muscle retractions. J Bone Joint Surg Am, 2002. 84-A(5): p. 780-5.
41. Hansen, M.L., J.C. Otis, J.S. Johnson, F.A. Cordasco, E.V. Craig, and R.F.
Warren, Biomechanics of massive rotator cuff tears: implications for treatment. J Bone
Joint Surg Am, 2008. 90(2): p. 316-25.
42. Bjorkenheim, J.M., Structure and function of the rabbit's supraspinatus muscle
after resection of its tendon. Acta Orthop Scand, 1989. 60(4): p. 461-3.
43. Fabis, J., P. Kordek, A. Bogucki, and J. Mazanowska-Gajdowicz, Function of the
rabbit supraspinatus muscle after large detachment of its tendon: 6-week, 3-month, and
6-month observation. J Shoulder Elbow Surg, 2000. 9(3): p. 211-6.
44. Fabis, J., P. Kordek, A. Bogucki, M. Synder, and H. Kolczynska, Function of the
rabbit supraspinatus muscle after detachment of its tendon from the greater tubercle.
Observations up to 6 months. Acta Orthop Scand, 1998. 69(6): p. 570-4.
45. Coleman, S.H., S. Fealy, J.R. Ehteshami, J.D. MacGillivray, D.W. Altchek, R.F.
Warren, et al., Chronic rotator cuff injury and repair model in sheep. J Bone Joint Surg
Am, 2003. 85-A(12): p. 2391-402.
46. Seyler, T.M., B.P. Smith, D.R. Marker, J. Ma, J. Shen, T.L. Smith, et al.,
Botulinum neurotoxin as a therapeutic modality in orthopaedic surgery: more than
twenty years of experience. J Bone Joint Surg Am, 2008. 90 Suppl 4: p. 133-45.
47. Ramachandran, M. and D.M. Eastwood, Botulinum toxin and its orthopaedic
applications. J Bone Joint Surg Br, 2006. 88(8): p. 981-7.
41
48. Escamilla, R.F. and J.R. Andrews, Shoulder muscle recruitment patterns and
related biomechanics during upper extremity sports. Sports Med, 2009. 39(7): p. 569-90.
49. Reinold, M.M., L.C. Macrina, K.E. Wilk, G.S. Fleisig, S. Dun, S.W. Barrentine,
et al., Electromyographic analysis of the supraspinatus and deltoid muscles during 3
common rehabilitation exercises. J Athl Train, 2007. 42(4): p. 464-9.
50. Malanga, G.A., Y.N. Jenp, E.S. Growney, and K.N. An, EMG analysis of
shoulder positioning in testing and strengthening the supraspinatus. Med Sci Sports
Exerc, 1996. 28(6): p. 661-4.
51. Ma, J., J. Shen, B.P. Smith, A. Ritting, T.L. Smith, and L.A. Koman,
Bioprotection of tendon repair: adjunctive use of botulinum toxin A in Achilles tendon
repair in the rat. J Bone Joint Surg Am, 2007. 89(10): p. 2241-9.
52. De Aguiar, G., L.A. Chait, D. Schultz, S. Bleloch, A. Theron, C.N. Snijman, et
al., Chemoprotection of flexor tendon repairs using botulinum toxin. Plast Reconstr Surg,
2009. 124(1): p. 201-9.
53. Gimbel, J.A., S. Mehta, J.P. Van Kleunen, G.R. Williams, and L.J. Soslowsky,
The tension required at repair to reappose the supraspinatus tendon to bone rapidly
increases after injury. Clin Orthop Relat Res, 2004(426): p. 258-65.
54. Gimbel, J.A., J.P. Van Kleunen, S.P. Lake, G.R. Williams, and L.J. Soslowsky,
The role of repair tension on tendon to bone healing in an animal model of chronic
rotator cuff tears. J Biomech, 2007. 40(3): p. 561-8.
55. Gerber, C., D.C. Meyer, A.G. Schneeberger, H. Hoppeler, and B. von
Rechenberg, Effect of tendon release and delayed repair on the structure of the muscles
42
of the rotator cuff: an experimental study in sheep. J Bone Joint Surg Am, 2004. 86-A(9):
p. 1973-82.
56. Meyer, D.C., C. Gerber, B. Von Rechenberg, S.H. Wirth, and M. Farshad,
Amplitude and Strength of Muscle Contraction Are Reduced in Experimental Tears of the
Rotator Cuff. The American journal of sports medicine, 2011.
57. Mannava, S., W.F. Wiggins, K.R. Saul, J.D. Stitzel, B.P. Smith, L. Andrew
Koman, et al., Contributions of Neural Tone to In Vivo Passive Muscle-Tendon Unit
Biomechanical Properties in a Rat Rotator Cuff Animal Model. Annals of biomedical
engineering, 2011.
58. Mannava, S., M.F. Callahan, S.M. Trach, W.F. Wiggins, B.P. Smith, L.A.
Koman, et al., Chemical denervation with botulinum neurotoxin a improves the surgical
manipulation of the muscle-tendon unit: an experimental study in an animal model. J
Hand Surg Am, 2011. 36(2): p. 222-31.
59. Gupta, R. and O. Steward, Chronic nerve compression induces concurrent
apoptosis and proliferation of Schwann cells. J Comp Neurol, 2003. 461(2): p. 174-86.
60. Jozsa, L., P. Kannus, J. Thoring, A. Reffy, M. Jarvinen, and M. Kvist, The effect
of tenotomy and immobilisation on intramuscular connective tissue. A morphometric and
microscopic study in rat calf muscles. J Bone Joint Surg Br, 1990. 72(2): p. 293-7.
61. Peltz, C.D., J.J. Sarver, L.M. Dourte, C.C. Wurgler-Hauri, G.R. Williams, and
L.J. Soslowsky, Exercise following a short immobilization period is detrimental to tendon
properties and joint mechanics in a rat rotator cuff injury model. J Orthop Res, 2010.
28(7): p. 841-5.
43
62. Thomopoulos, S., G.R. Williams, and L.J. Soslowsky, Tendon to bone healing:
differences in biomechanical, structural, and compositional properties due to a range of
activity levels. J Biomech Eng, 2003. 125(1): p. 106-13.
63. Gimbel, J.A., J.P. Van Kleunen, G.R. Williams, S. Thomopoulos, and L.J.
Soslowsky, Long durations of immobilization in the rat result in enhanced mechanical
properties of the healing supraspinatus tendon insertion site. J Biomech Eng, 2007.
129(3): p. 400-4.
64. Safran, O., K.A. Derwin, K. Powell, and J.P. Iannotti, Changes in rotator cuff
muscle volume, fat content, and passive mechanics after chronic detachment in a canine
model. The Journal of bone and joint surgery. American volume, 2005. 87(12): p. 2662-
70.
65. Halder, A.M., S.W. O'Driscoll, G. Heers, N. Mura, M.E. Zobitz, K.N. An, et al.,
Biomechanical comparison of effects of supraspinatus tendon detachments, tendon
defects, and muscle retractions. The Journal of bone and joint surgery. American volume,
2002. 84-A(5): p. 780-5.
66. Rowshan, K., S. Hadley, K. Pham, V. Caiozzo, T.Q. Lee, and R. Gupta,
Development of fatty atrophy after neurologic and rotator cuff injuries in an animal
model of rotator cuff pathology. The Journal of bone and joint surgery. American
volume, 2010. 92(13): p. 2270-8.
67. Costouros, J.G., M. Porramatikul, D.T. Lie, and J.J. Warner, Reversal of
suprascapular neuropathy following arthroscopic repair of massive supraspinatus and
infraspinatus rotator cuff tears. Arthroscopy, 2007. 23(11): p. 1152-61.
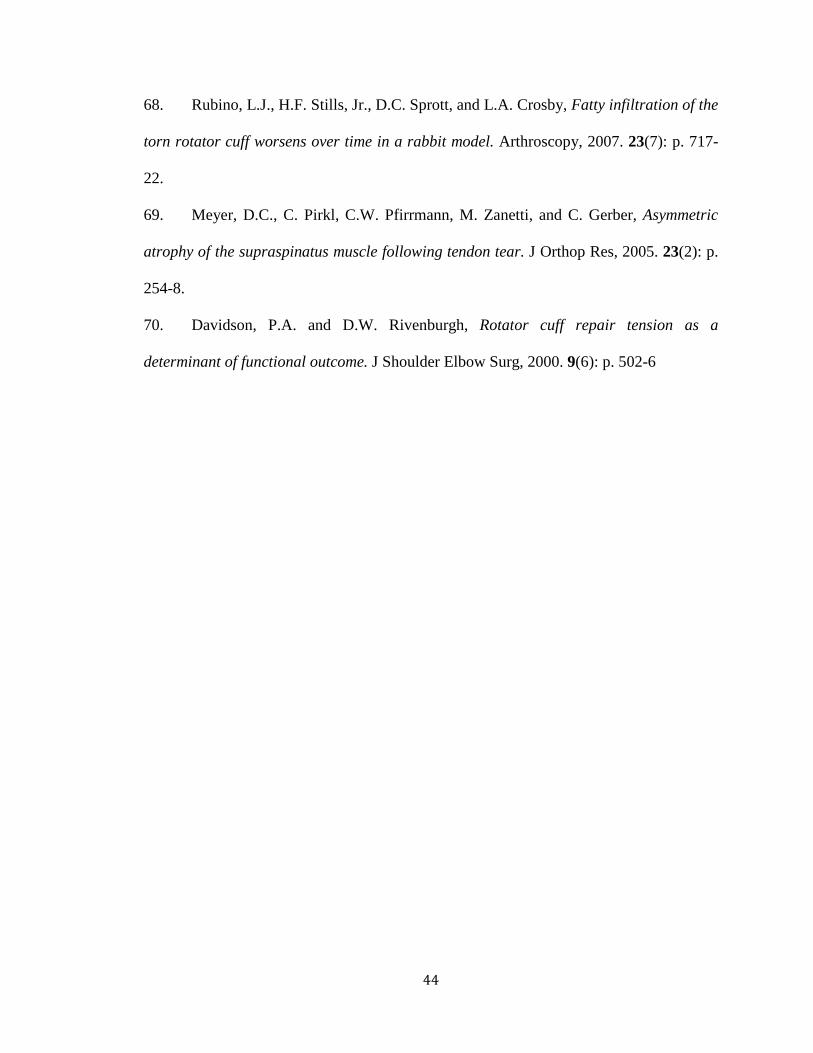
44
68. Rubino, L.J., H.F. Stills, Jr., D.C. Sprott, and L.A. Crosby, Fatty infiltration of the
torn rotator cuff worsens over time in a rabbit model. Arthroscopy, 2007. 23(7): p. 717-
22.
69. Meyer, D.C., C. Pirkl, C.W. Pfirrmann, M. Zanetti, and C. Gerber, Asymmetric
atrophy of the supraspinatus muscle following tendon tear. J Orthop Res, 2005. 23(2): p.
254-8.
70. Davidson, P.A. and D.W. Rivenburgh, Rotator cuff repair tension as a
determinant of functional outcome. J Shoulder Elbow Surg, 2000. 9(6): p. 502-6

45
Chapter 2 Figures and Table
FIG 1: Experimental Apparatus. The experimental apparatus and key components are
labeled in these schematic diagrams. Panel A: A view of the entire physiological
apparatus is depicted. Panel B: The image focuses on the rat supraspinatus muscle-tendon
unit during force recording.
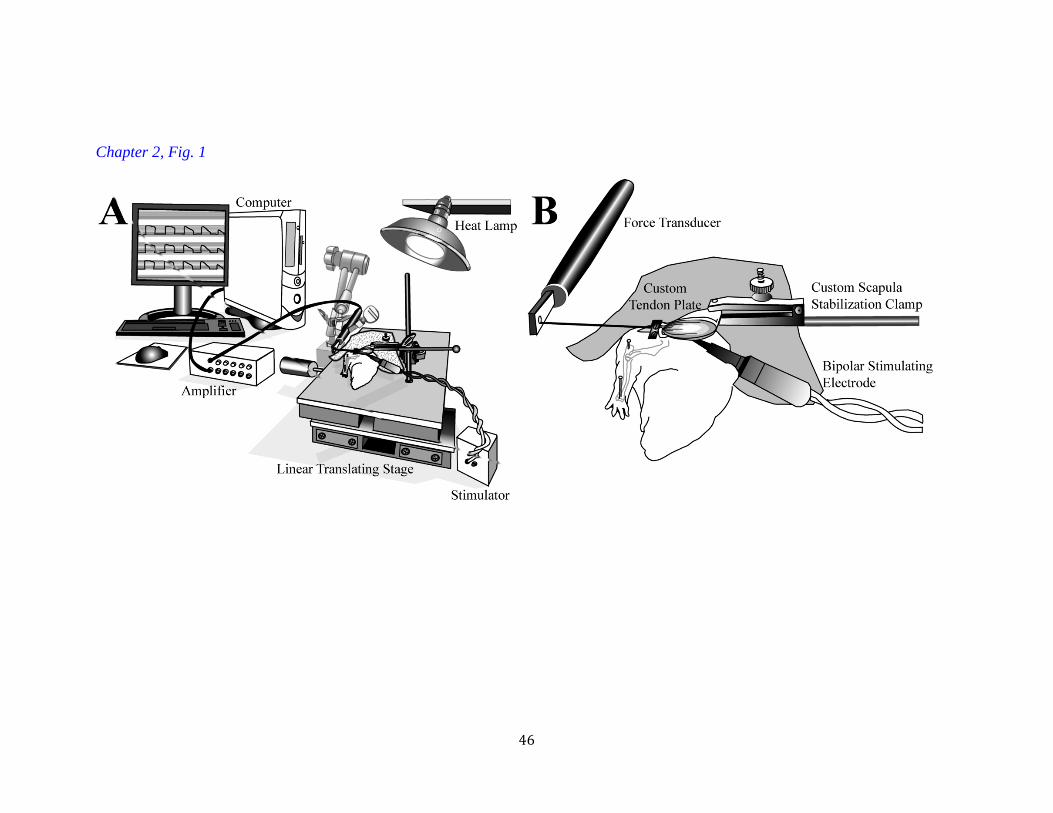
46
Chapter 2, Fig. 1
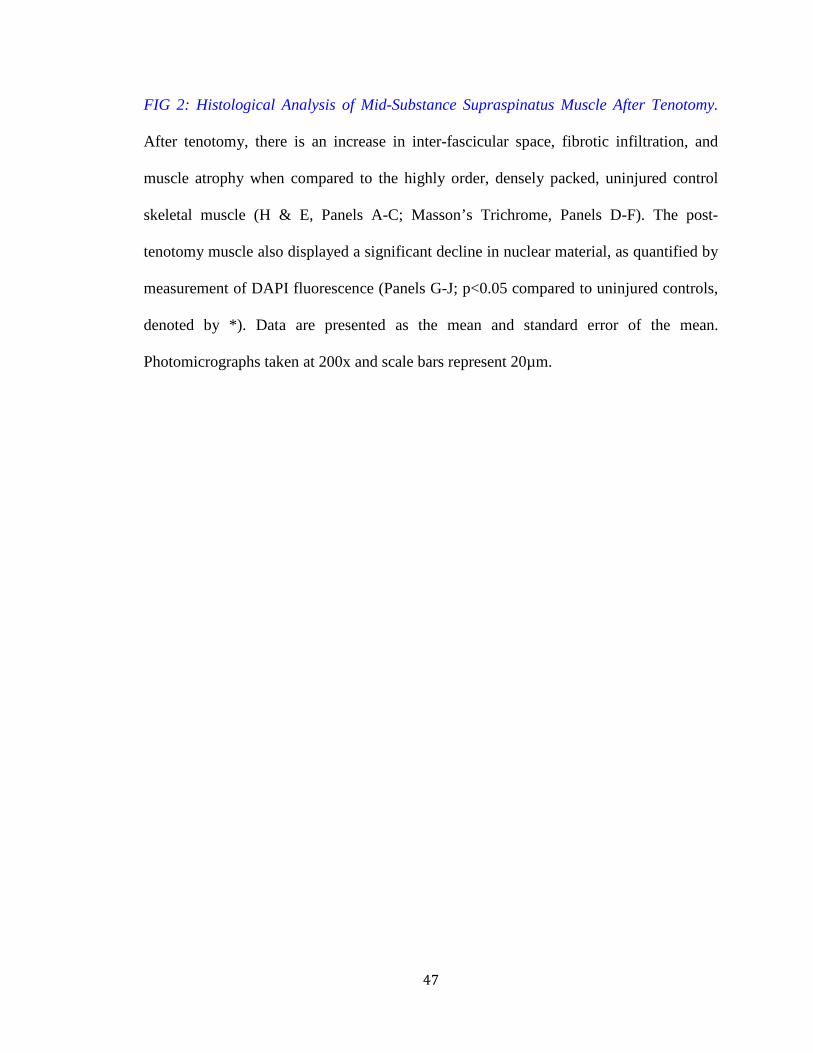
47
FIG 2: Histological Analysis of Mid-Substance Supraspinatus Muscle After Tenotomy.
After tenotomy, there is an increase in inter-fascicular space, fibrotic infiltration, and
muscle atrophy when compared to the highly order, densely packed, uninjured control
skeletal muscle (H & E, Panels A-C; Masson’s Trichrome, Panels D-F). The post-
tenotomy muscle also displayed a significant decline in nuclear material, as quantified by
measurement of DAPI fluorescence (Panels G-J; p<0.05 compared to uninjured controls,
denoted by *). Data are presented as the mean and standard error of the mean.
Photomicrographs taken at 200x and scale bars represent 20µm.

48
Chapter 2, Fig. 2
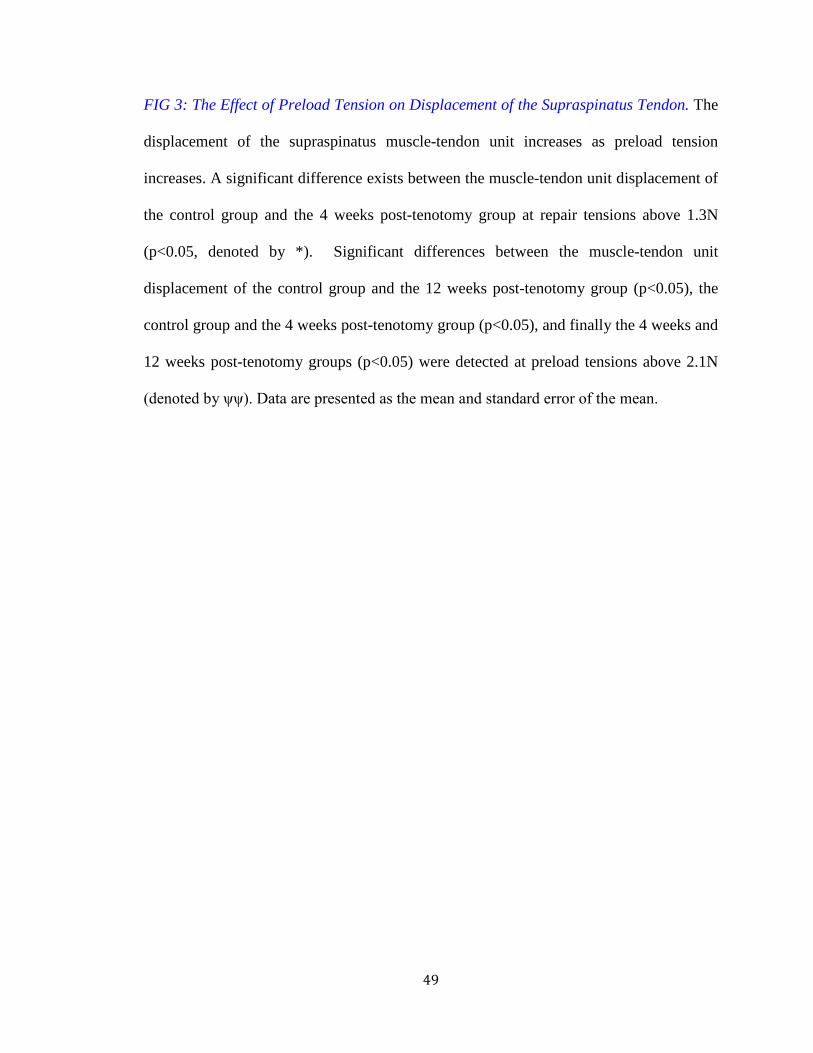
49
FIG 3: The Effect of Preload Tension on Displacement of the Supraspinatus Tendon. The
displacement of the supraspinatus muscle-tendon unit increases as preload tension
increases. A significant difference exists between the muscle-tendon unit displacement of
the control group and the 4 weeks post-tenotomy group at repair tensions above 1.3N
(p<0.05, denoted by *). Significant differences between the muscle-tendon unit
displacement of the control group and the 12 weeks post-tenotomy group (p<0.05), the
control group and the 4 weeks post-tenotomy group (p<0.05), and finally the 4 weeks and
12 weeks post-tenotomy groups (p<0.05) were detected at preload tensions above 2.1N
(denoted by ψψ). Data are presented as the mean and standard error of the mean.
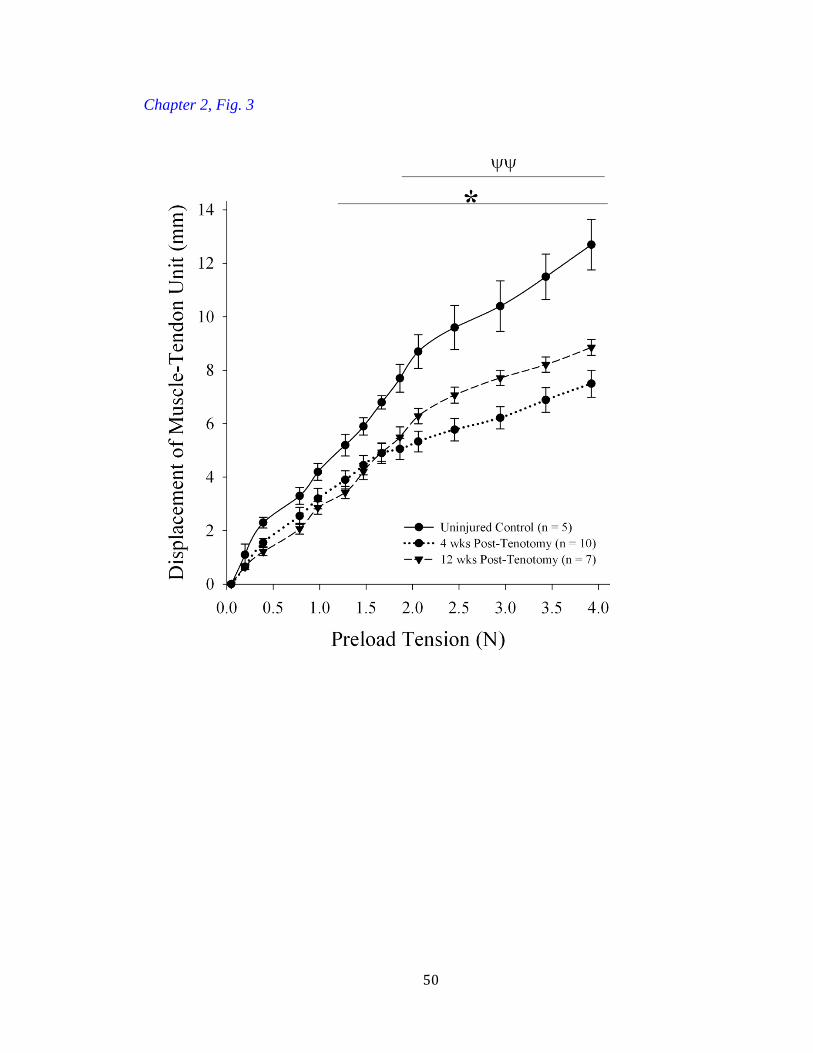
50
Chapter 2, Fig. 3
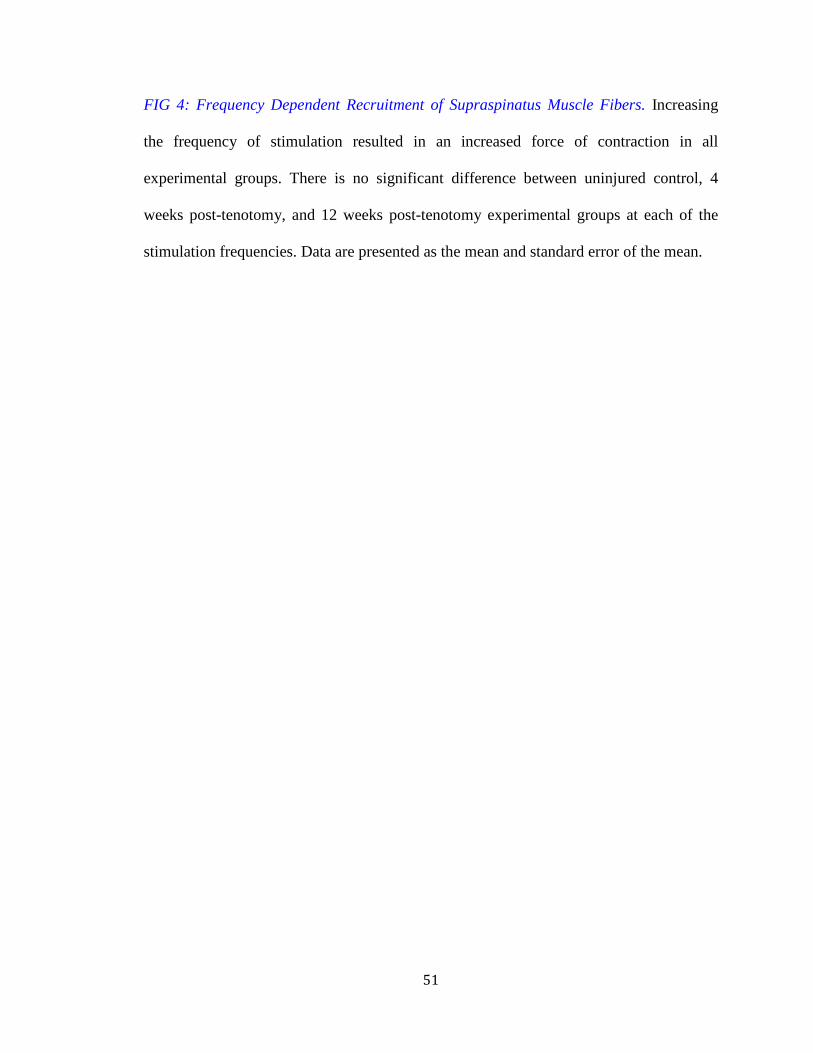
51
FIG 4: Frequency Dependent Recruitment of Supraspinatus Muscle Fibers. Increasing
the frequency of stimulation resulted in an increased force of contraction in all
experimental groups. There is no significant difference between uninjured control, 4
weeks post-tenotomy, and 12 weeks post-tenotomy experimental groups at each of the
stimulation frequencies. Data are presented as the mean and standard error of the mean.
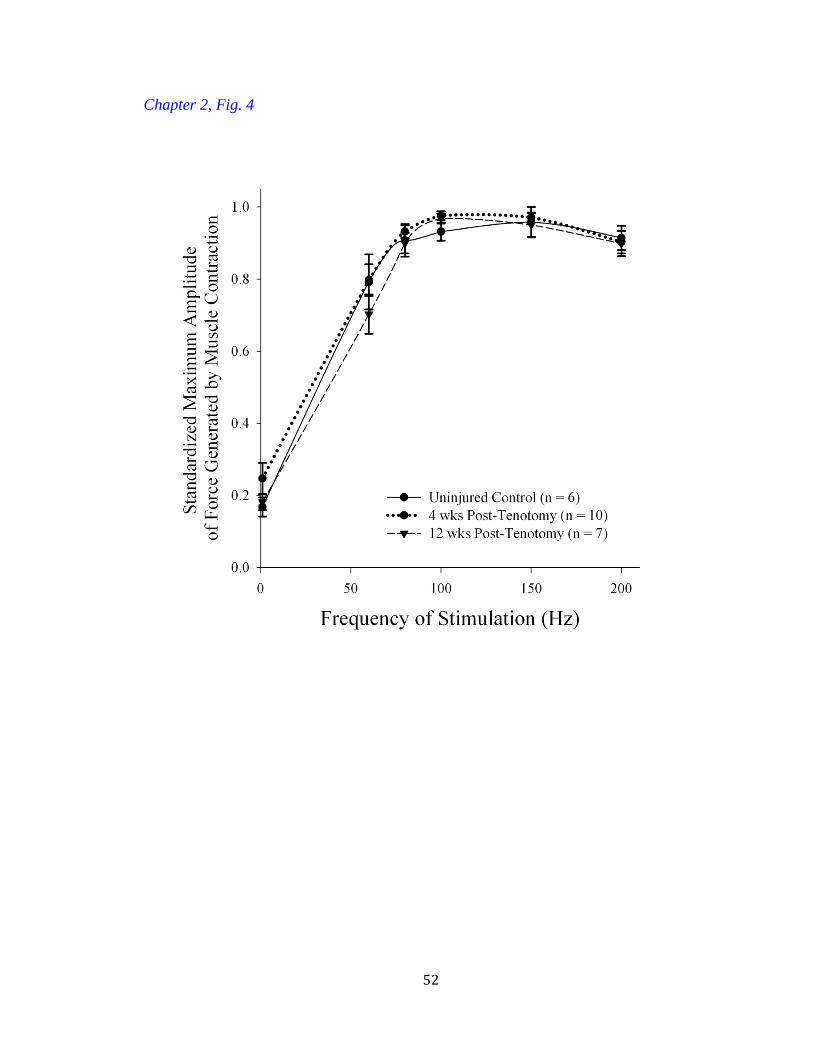
52
Chapter 2, Fig. 4
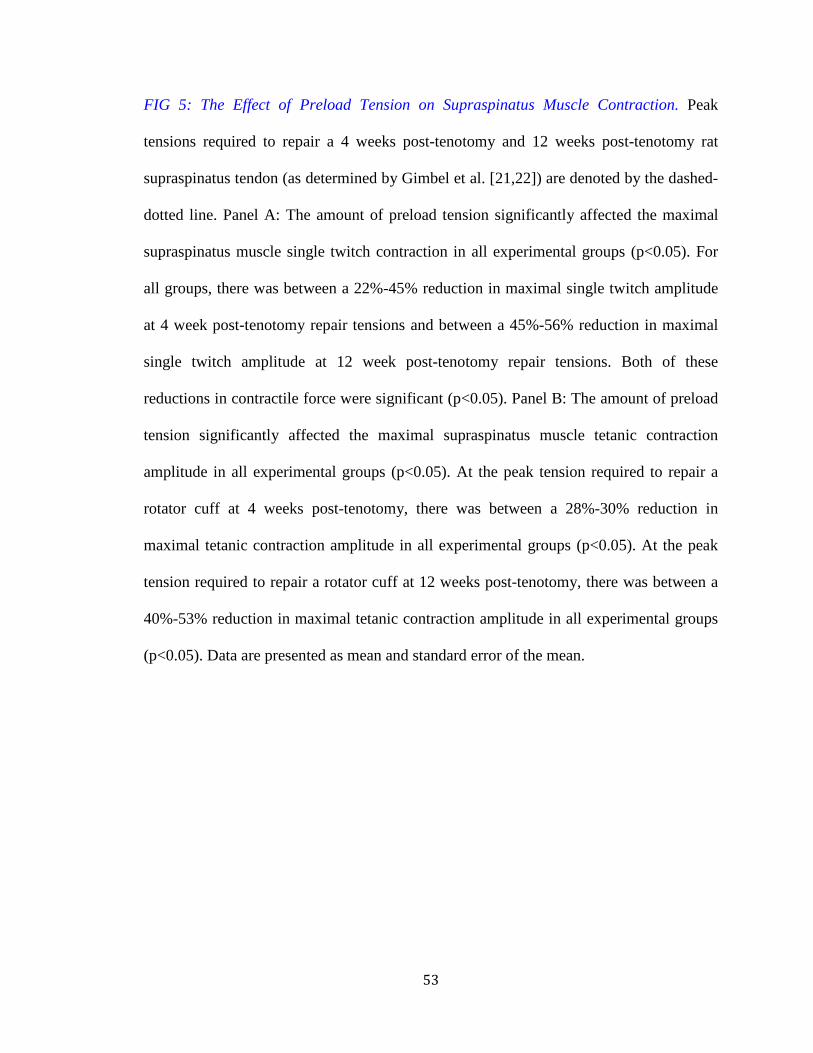
53
FIG 5: The Effect of Preload Tension on Supraspinatus Muscle Contraction. Peak
tensions required to repair a 4 weeks post-tenotomy and 12 weeks post-tenotomy rat
supraspinatus tendon (as determined by Gimbel et al. [21,22]) are denoted by the dashed-
dotted line. Panel A: The amount of preload tension significantly affected the maximal
supraspinatus muscle single twitch contraction in all experimental groups (p<0.05). For
all groups, there was between a 22%-45% reduction in maximal single twitch amplitude
at 4 week post-tenotomy repair tensions and between a 45%-56% reduction in maximal
single twitch amplitude at 12 week post-tenotomy repair tensions. Both of these
reductions in contractile force were significant (p<0.05). Panel B: The amount of preload
tension significantly affected the maximal supraspinatus muscle tetanic contraction
amplitude in all experimental groups (p<0.05). At the peak tension required to repair a
rotator cuff at 4 weeks post-tenotomy, there was between a 28%-30% reduction in
maximal tetanic contraction amplitude in all experimental groups (p<0.05). At the peak
tension required to repair a rotator cuff at 12 weeks post-tenotomy, there was between a
40%-53% reduction in maximal tetanic contraction amplitude in all experimental groups
(p<0.05). Data are presented as mean and standard error of the mean.
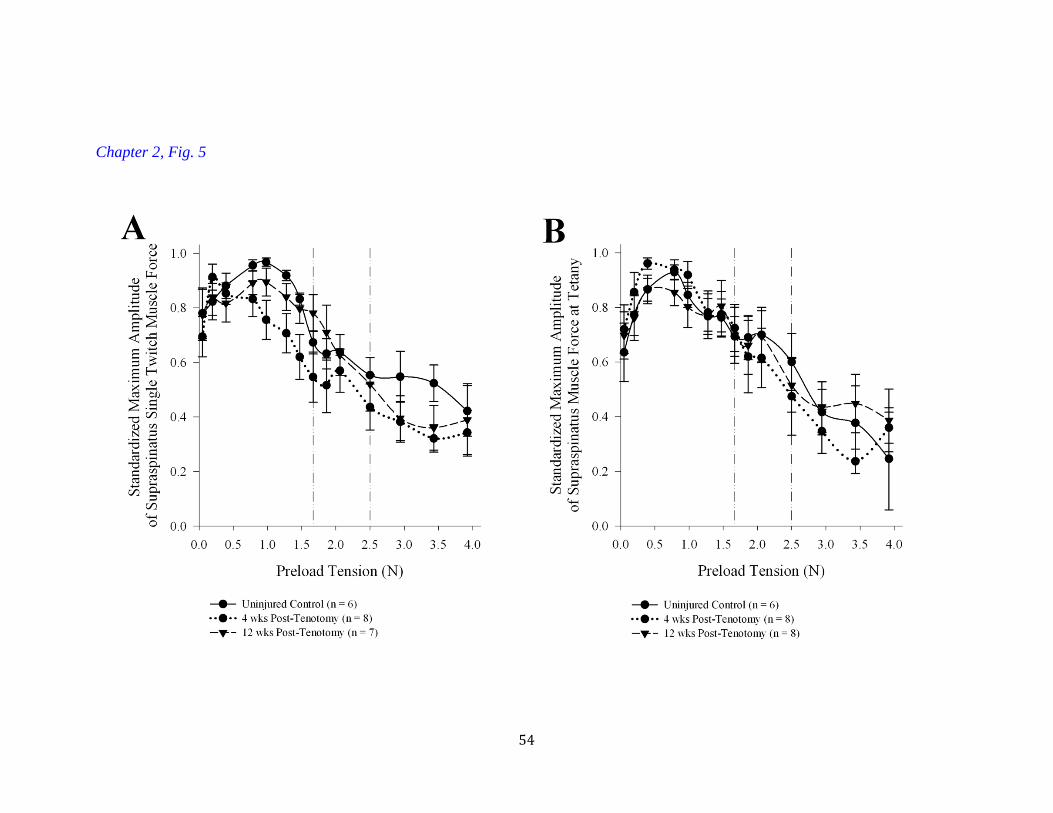
54
Chapter 2, Fig. 5

55
FIG 6: The Effect Of Time From Injury And Preload Tension On Supraspinatus Muscle
Endurance. The uninjured control group showed significantly greater muscle endurance
(p<0.05) compared to the 4 weeks post supraspinatus tenotomy and 12 weeks post
supraspinatus tenotomy experimental groups at all repair tensions. The 12 weeks post-
tenotomy group had significantly increased muscle endurance when compared to the 4
weeks post-tenotomy group at 0.4N repair tension (p<0.05), but this difference between
experimental groups was not significant at the higher preload tensions of 1.3N and 2.0N.
The data are expressed as change from maximal amplitude over time. The greater the
change from maximal amplitude indicates an inability to sustain maximal contraction.
Data are presented as mean and standard error of the mean.
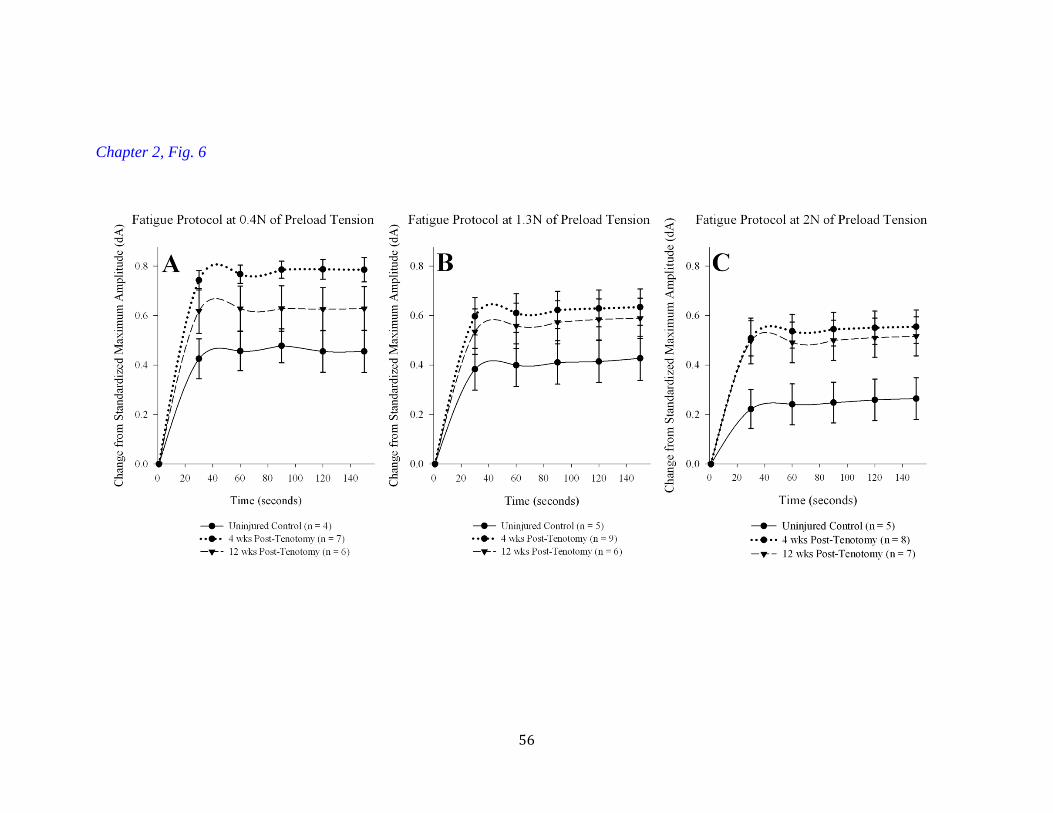
56
Chapter 2, Fig. 6
57
FIG 7: The Effect Of Time From Injury On Supraspinatus Electromyography (EMG)
With Suprascapular Nerve Stimulation. Panel A: The chronic injury group has
significantly lower maximal compound motor action potential (CMAP) amplitude when
compared to both the uninjured control (p<0.05, denoted by *) and acutely injured groups
(p<0.05, denoted by *). Panel B: No significant differences were detected between the
experimental groups when evaluating the area under the curve (AUC) of the compound
motor action potential. Panel C: The heterogeneity of compound motor action potential
amplitude was related to the location of the recording needle in the supraspinatus muscle.
The regional heterogeneity in compound motor action potential amplitude exists in the
control group between the proximal and distal (p<0.05, denoted by *) and proximal and
middle locations (p<0.05, denoted by *). Similarly, a significant difference existed in the
4 weeks post-tenotomy group between the proximal and distal locations (p<0.05, denoted
by ψ) and between the proximal and middle locations (p<0.05, denoted by ψ). This
decline in maximal compound motor action potential amplitude, detected in the control
and 4 weeks post-tenotomy groups, was not detected in the 12 weeks post-tenotomy
group. There was not a statistically significant difference in the maximal compound
motor action potential amplitudes between any of recording locations in the 12 weeks
post-tenotomy group. Panel D: The experimental apparatus and key components are
labeled in this schematic diagram. The image focuses on the rat supraspinatus muscle-
tendon unit during EMG recording. The recording ELECTRODE locations are labeled
‘D’ for distal, ‘M’ for middle, and ‘P’ for proximal. All data are presented as mean and
standard error of the mean.
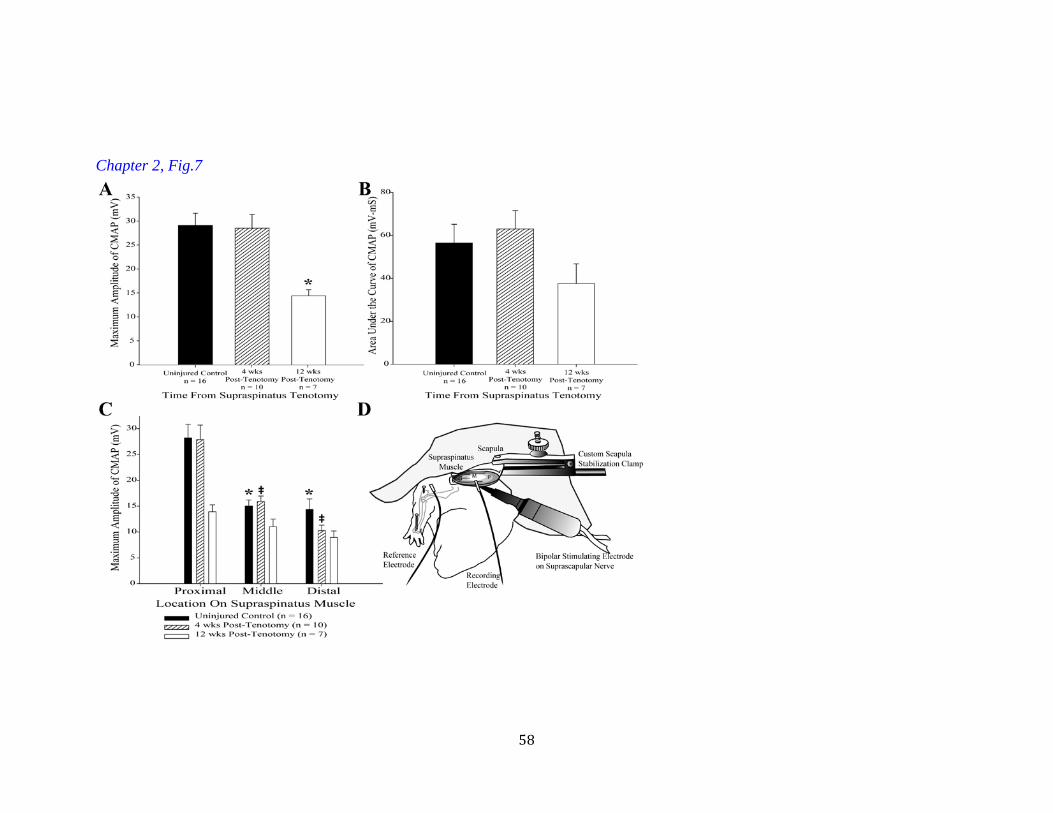
58
Chapter 2, Fig.7

59
Chapter 2, Table 1
Group
Slope Compliance
(mm/N) R2 P
Inverse of Slope Stiffness
(N/mm)
Control (n=5) 3.255 ± 0.214 0.974 <0.05 0.307 ± 0.021
Acute Injury (n=10) 1.7918 ± 0.094 * 0.929 <0.05 0.558 ± 0.029 *
Chronic Injury (n=7) 2.396 ± 0.092 *, ‡ 0.966 <0.05 0.417 ± 0.016 *
Table 1. Mean Linear Regression Analysis for Compliance/Stiffness Data * Signficant difference (p<0.05) when compared to the control group, Tukey post-hoc
‡ Signficant difference (p<0.05) when compared to the acute group, Tukey post-hoc
Average compliance and stiffness data expressed as MEAN ± SEM
60
CHAPTER 3
CHEMICAL DENERVATION WITH BOTULINUM NEUROTOXIN
A IMPROVES THE SURGICAL MANIPULATION OF THE
MUSCLE-TENDON UNIT: AN EXPERIMENTAL STUDY IN AN
ANIMAL MODEL
Sandeep Mannava, Michael F. Callahan, Simon M. Trach, Walter F. Wiggins, Beth P.
Smith, L. Andrew Koman, Thomas L. Smith, Christopher J. Tuohy
The following manuscript was published in the J Hand Surg Am. 2011
Feb;36(2):222-31. PMID: 21276885. This chapter is reprinted with permission.
Stylistic variations are due to the requirements of the journal. S. Mannava performed
the experiments, prepared the manuscript, and served as corresponding author. T.L.
Smith acted in an advisory and editorial capacity.

61
ABSTRACT
Purpose: The chemical denervation that results from botulinum neurotoxin A (BoNT-A)
causes a temporary reversible paresis that may result in easier surgical manipulation of
the muscle-tendon unit in the context of tendon rupture and repair. The purpose of the
study was to determine if BoNT-A injections can be utilized to temporarily and
reversibly modulate active and passive skeletal muscle properties.
Methods: Male CD1 mice weighing 40-50g were divided into a 1 week post-injection
group (n=13: n=5 saline and n=8 BoNT-A) and a 2 week post-injection group (n=17: n=7
saline and n=10 BoNT-A). The animals underwent in vivo muscle force testing and in
vivo biomechanical evaluation.
Results: There was a significant decline in the maximal single twitch amplitude (p<0.05)
and tetanic amplitude (p<0.05) at 1 week and at 2 weeks after BoNT-A injection, when
compared to saline injected controls. BoNT-A injection significantly reduced the peak
passive properties of the muscle-tendon unit as a function of displacement at 1 week
(p<0.05). Specifically, the stiffness of the BoNT-A injected muscle-tendon unit was
0.417 N/mm compared to the control saline injected group which was 0.634 N/mm, a
35% reduction in stiffness (p<0.05).
Conclusions: Pre-surgical treatment with BoNT-A may improve the surgical
manipulation of the muscle-tendon unit, thus improving operative outcomes. The results
implicate neural tone as a substantial contributor to the passive repair tension of the
muscle-tendon unit. The modulation of neural tone through temporary reversible paresis
is a novel approach that may improve intra-operative and post-operative passive muscle
properties, allowing for progressive rehabilitation while protecting the surgical repair site.

62
Type of Study: Basic Science
Key Words: Botulinum Neurotoxin Type A (BoNT-A); Chemical Denervation; Skeletal
Muscle; Tendon Repair Surgery;

63
INTRODUCTION
Tendon injuries commonly cause disability and place a high cost burden on the
United States economy [1]. Surgical repair of torn muscle-tendon units can be technically
demanding. In certain settings, these injuries have been associated with high rates of re-
tearing and continued diminished functional capacity after surgery [2-6]. In particular,
hand zone 2 flexor tendon repairs have been associated with re-rupture rates ranging from
0% to 16.6% [6-9]. Factors associated with poor post-operative outcomes following
muscle-tendon unit repair have been studied extensively in torn rotator cuff and include
advanced age [2], diminished tendon quality [10], muscle atrophy [11], and prolonged
time from injury [2, 12, 13].
After tendon rupture, the muscle undergoes many structural changes as it
atrophies including fibro-fatty infiltration of the muscle belly [14-18], decreased capillary
density [19], and reduced muscle volume [15, 16, 20]. These structural changes result in a
stiff and retracted muscle-tendon unit that is difficult to manipulate surgically [15, 21-
23]. After undergoing these changes, the repair tension required to re-attach the ruptured
muscle-tendon unit to its anatomical insertion progressively increases from the time of
injury. This increased repair tension results in impaired healing biomechanics [24, 25].
Historically, most tendon repair studies have attempted to overcome increased muscle-
tendon unit stiffness and improve healing by focusing on the tendon-to-tendon and the
tendon-to-bone interfaces. These studies documented improved repair site strength using
varying surgical techniques and suture materials [26-33]. More recently, there have been
attempts to completely eliminate repair tension through muscle paralysis by chemical
denervation using botulinum neurotoxin A (BoNT-A) and cast immobilization [34].
64
BoNT-A is a widely used pharmacological agent that, when injected
intramuscularly, can modulate skeletal muscle contractility by inhibiting presynaptic
release of acetylcholine [35, 36]. The chemical denervation that results from BoNT-A
causes a temporary reversible paresis that may result in easier surgical manipulation of
the muscle-tendon unit. These results have implications for potentially improving upper
extremity tendon repair surgery for ruptured zone II flexor tendons, biceps tendons,
triceps tendons, and rotator cuff. To date, most studies have focused on the active
isometric contractile properties of skeletal muscle after BoNT-A injection at repair
tensions below what is required to successfully repair the muscle-tendon unit to its
anatomical insertion [37-39]. The purpose of the present study was to characterize the
active contractile properties of the muscle-tendon unit over a wide range of surgically
relevant preload tensions after chemical denervation and recovery using a well-
characterized murine model. Further, the current study characterizes the neuronal
contribution to passive skeletal muscle tone. The study hypothesis was that BoNT-A
injections can be utilized to temporarily and reversibly alter active and passive skeletal
muscle properties at surgically relevant preload tensions and displacement distances.
MATERIALS AND METHODS
A total of 30 male CD1 mice weighing 40-50g (Charles River, Wilmington, PA)
were studied after approval from the Institutional Animal Care and Use Committee in
accordance with standards set forth by the National Institutes of Health and any national
law on the care and use of laboratory animals. While housed in the controlled
temperature vivarium with 12 hour light-dark cycles, chow and water were provided to
the mice ad libitum. The animals were divided into a 1 week post-injection group (n=13:
65
n=5 saline and n=8 BoNT-A) and a 2 week post-injection group (n=17: n=7 saline and
n=10 BoNT-A). All animals were immediately injected with a lethal dose of KCl under
general anesthesia after in vivo muscle function testing. All experimentation was triple-
blinded in that one scientist injected the animal, a second scientist performed all surgery,
and a separate third scientist performed the in vivo muscle function testing. The second
and third scientists were not aware of the injection status (saline versus BoNT-A) until
after experimentation and analysis was completed.
Botulinum Toxin Injection
Botulinum neurotoxin A (Allergan, Irvine, CA) was reconstituted as previously
described [37-39]. Briefly, a 100U vial of lyophylized BoNT-A was reconstituted with
normal saline. The toxin was injected into the gastrocnemius muscle at a dosage of 3
units/kg body weight in an injection volume of 10 µL with a Hamilton syringe (Fischer
Scientific, Pittsburgh, PA) equipped with a 30 gauge needle. For the control animals,
normal saline (0.9%) was injected in a similar manner. The dose and volume were chosen
based on previous experiments using this animal model with this dosing schedule, which
produced temporary reversible paresis in a relatively short period of time (i.e. 2 weeks)
[37]. All injections were performed percutaneously. Each head of the left gastrocnemius,
medial and lateral aspects, was injected with equal volumes (5 µL) and units of toxin
while the animals were anesthetized with isoflurane (Webster Veterinary, Patterson
Companies Inc., Sterling, MA).
Assessment of Active and Passive Muscle Properties
Control saline injected (n=12) and BoNT-A injected mice (n=18) were
anesthetized using isoflurane (1.0 – 1.5 vol % in oxygen) and remained under inhalation
66
anesthesia for the duration of the experiment. The surgical approach and isolation of the
gastrocnemius muscle and the sciatic nerve has been described previously [37-39]. After
the muscle and nerve were isolated with the aid of a dissection microscope, the mouse
was moved and strapped to a linearly translating stage. The lower limb of the animal was
pinned at the ankle joint and the femur with Kirschner wires to isolate gross movement.
In all cases, the strap and pins ensured that all contractile and passive force produced by
the gastrocnemius muscle-tendon unit translated perpendicular and “in line” with the
force transducer. After the mouse was sufficiently immobilized, the calcaneus was
disarticulated with the Achilles tendon still attached. The muscle-tendon-bone were then
attached to a force transducer (model FORT100; World Precision Instruments Inc.,
Sarasota, FL) with wire suture (Figure 1). The transducer was connected to an amplifier
(model 13-G4615-50; Gould, Cleveland, OH) through an interface controller (EMKA
Technologies Inc., Falls Church, VA) and an analog-to-digital converter card
(model:PCI-6023E, National Instruments, Austin, TX) connected to a personal computer.
The sciatic nerve then was stimulated using a bipolar hook electrode (FHC,
Bowdoinham, ME) and a pulse generator (model Tenma TGP110, BioSurplus Inc., San
Diego, CA). To electrically isolate the simulating hook electrode and sciatic nerve from
the surrounding tissue, a piece of Silastic® sheeting (Dow Corning Co., Midland, MI)
was wrapped around the exterior of the nerve and electrode. The stimulation protocol, the
force of muscle contraction, and the passive muscle-tendon unit properties were
controlled and recorded by IOX software, Slow Wave Analyzer (EMKA Technologies
Inc., Falls Church, VA). The body temperature of the mice was maintained during
experimentation with an external heat lamp.
67
Active muscle force testing consisted of supramaximal sciatic nerve stimulation to
produce a maximal single twitch contraction. A range of stimuli were tested between
0.6V and 2.0V, and maximal single twitch was recorded. In all cases, 1.5V was sufficient
to produce maximal single twitch contraction; thus, this voltage was used throughout
experimentation. The muscle-tendon unit then was pretensioned to preload tensions
ranging between 0.05N to 1N, the maximal preload tension of 1N corresponded to
approximately twice the average mouse body weight. The maximal preload tension of 1N
reduced the maximal amplitude of contraction without causing gross injury to the muscle-
tendon unit. To test preload tension versus maximal single twitch and tetany force of
contraction, the muscle-tendon unit was ranged from 0.05N to 1N of preload tension, and
the nerve was stimulated at 1Hz and 150Hz for 5 seconds with a recovery time of 60
seconds between stimuli. This rest period allowed for full recovery of maximal
contractile force.
Peak passive muscle-tendon unit properties were assessed after muscle force
testing was completed. The linear translating stage, to which the mouse was securely
attached, was displaced 1mm, 2mm, 3mm, 4mm, and 5mm. The peak passive force
produced by displacing the muscle-tendon unit from 0mm to each of the displacements
(1mm-5mm) was recorded by the force transducer. Between each of the displacement
experiments, the muscle-tendon unit was returned to 0mm displacement (set to 0.05N
preload tension) and was allowed to rest for 5 minutes.
Statistical Analysis
A power analysis was conducted prior to experimentation to determine the sample
size needed in each experimental group to detect statistically significant differences. For
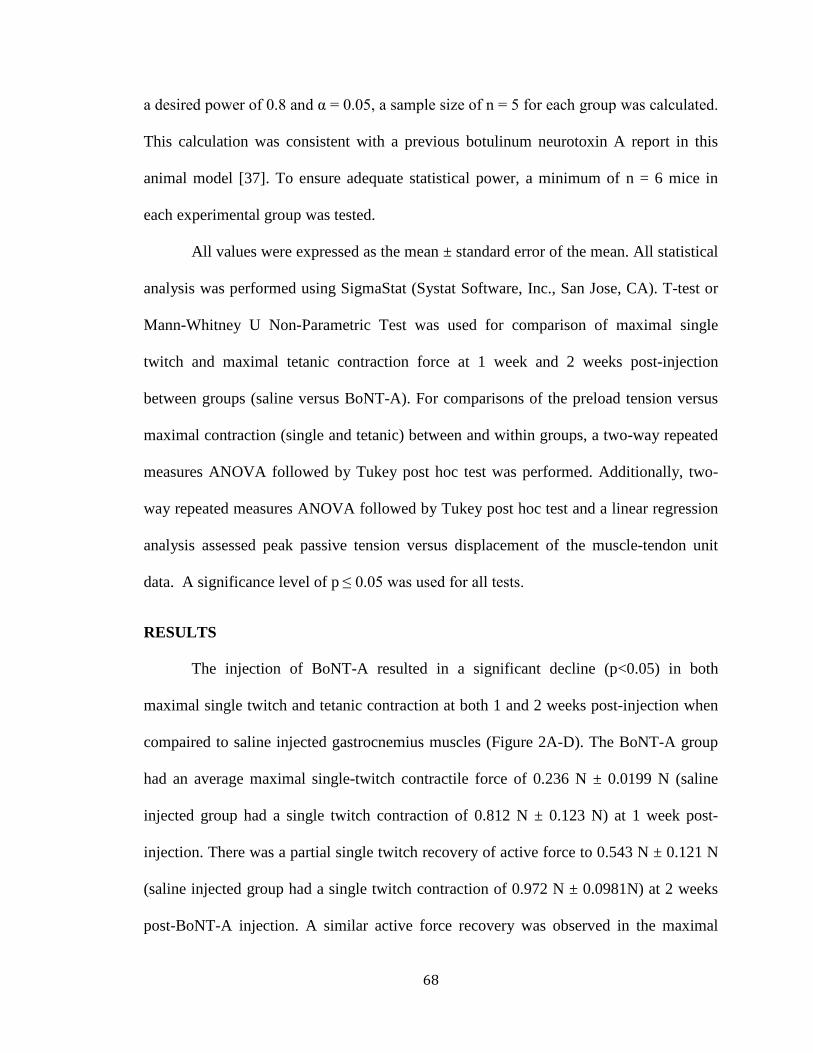
68
a desired power of 0.8 and α = 0.05, a sample size of n = 5 for each group was calculated.
This calculation was consistent with a previous botulinum neurotoxin A report in this
animal model [37]. To ensure adequate statistical power, a minimum of n = 6 mice in
each experimental group was tested.
All values were expressed as the mean ± standard error of the mean. All statistical
analysis was performed using SigmaStat (Systat Software, Inc., San Jose, CA). T-test or
Mann-Whitney U Non-Parametric Test was used for comparison of maximal single
twitch and maximal tetanic contraction force at 1 week and 2 weeks post-injection
between groups (saline versus BoNT-A). For comparisons of the preload tension versus
maximal contraction (single and tetanic) between and within groups, a two-way repeated
measures ANOVA followed by Tukey post hoc test was performed. Additionally, two-
way repeated measures ANOVA followed by Tukey post hoc test and a linear regression
analysis assessed peak passive tension versus displacement of the muscle-tendon unit
data. A significance level of p ≤ 0.05 was used for all tests.
RESULTS
The injection of BoNT-A resulted in a significant decline (p<0.05) in both
maximal single twitch and tetanic contraction at both 1 and 2 weeks post-injection when
compaired to saline injected gastrocnemius muscles (Figure 2A-D). The BoNT-A group
had an average maximal single-twitch contractile force of 0.236 N ± 0.0199 N (saline
injected group had a single twitch contraction of 0.812 N ± 0.123 N) at 1 week post-
injection. There was a partial single twitch recovery of active force to 0.543 N ± 0.121 N
(saline injected group had a single twitch contraction of 0.972 N ± 0.0981N) at 2 weeks
post-BoNT-A injection. A similar active force recovery was observed in the maximal

69
tetanic contraction, with the BoNT-A group having an average maximal tetanic
contraction of 0.85 N ± 0.13 N (saline injected group had a tetanic contraction of 3.33 N
± 0.04 N) at 1 week post-BoNT-A injection. There was a partial tetanic recovery of
active force to 1.57 N ± 0.28 N (saline injected group had a tetanic contraction of 2.92 N
± 0.12 N) at 2 weeks post-BoNT-A injection.
Preload tension significantly affected the maximal single twitch and tetanic
contraction amplitude in both saline and BoNT-A injected groups at 1 and 2 weeks post-
injection (p<0.05, Figure 3A-D). At 1 week after BoNT-A injection, there was a
significant difference between the preload tension versus maximal single twitch and
tetanic amplitude curves when compared to saline injected controls (p<0.05, Figure 3A
and B). Although the injection of BoNT-A decreased the amplitude of maximal single
twitch and tetanic contraction (Figure 2C and D), differences between BoNT-A and
saline injected preload tension versus maximal muscle force curves were not statistically
significant at 2 weeks post-injection (p=0.082 for Figure 3C single twitch and p=0.053
for Figure 3D tetanic contraction). The curve depicting the relationship between preload
tension and maximal contractile force appeared to flatten at 1 week post BoNT-A
injection, but the shape of the curve appeared to become more parabolic at 2 weeks after
injection (Figure 3A-D).
BoNT-A injection significantly reduced the peak passive properties of the
muscle-tendon unit as a function of displacement at 1 week (p<0.05, Table 1 and Figure
4A). Specifically, the stiffness of the BoNT-A injected muscle-tendon unit was 0.417
N/mm compared to the control saline injected group, which was 0.634 N/mm, a 35%
reduction in stiffness (p<0.05, Table 1). Post-hoc Tukey pairwise comparison testing
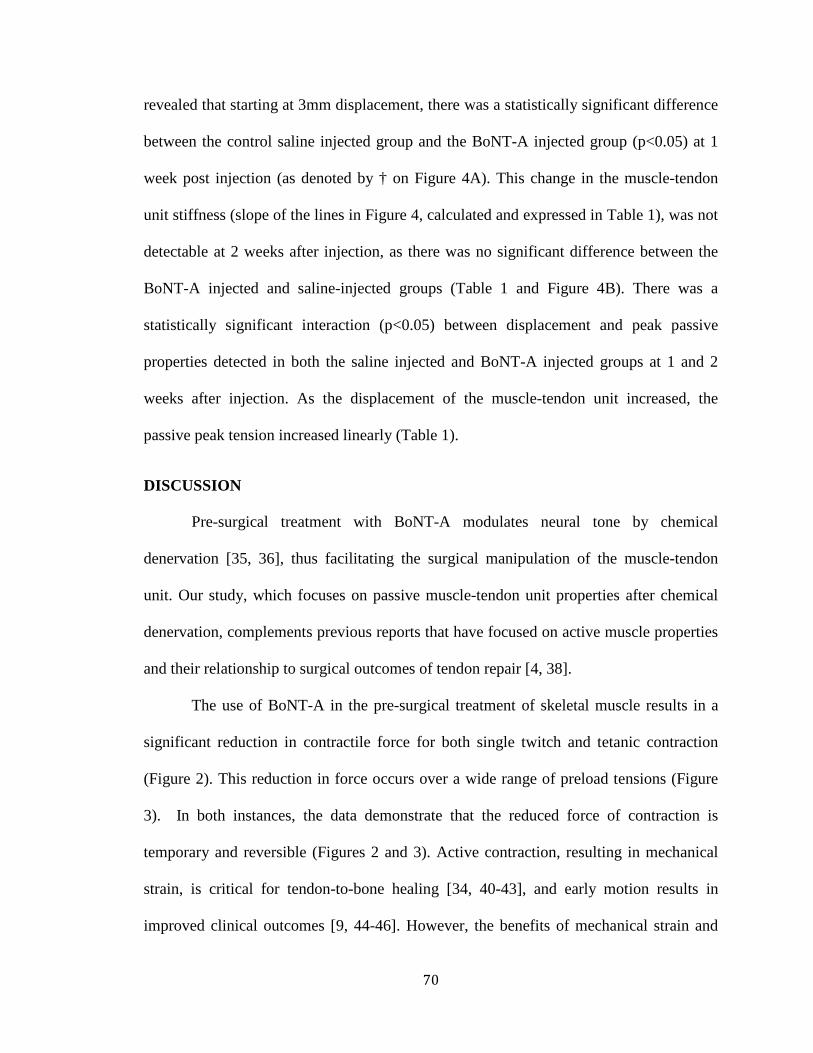
70
revealed that starting at 3mm displacement, there was a statistically significant difference
between the control saline injected group and the BoNT-A injected group (p<0.05) at 1
week post injection (as denoted by † on Figure 4A). This change in the muscle-tendon
unit stiffness (slope of the lines in Figure 4, calculated and expressed in Table 1), was not
detectable at 2 weeks after injection, as there was no significant difference between the
BoNT-A injected and saline-injected groups (Table 1 and Figure 4B). There was a
statistically significant interaction (p<0.05) between displacement and peak passive
properties detected in both the saline injected and BoNT-A injected groups at 1 and 2
weeks after injection. As the displacement of the muscle-tendon unit increased, the
passive peak tension increased linearly (Table 1).
DISCUSSION
Pre-surgical treatment with BoNT-A modulates neural tone by chemical
denervation [35, 36], thus facilitating the surgical manipulation of the muscle-tendon
unit. Our study, which focuses on passive muscle-tendon unit properties after chemical
denervation, complements previous reports that have focused on active muscle properties
and their relationship to surgical outcomes of tendon repair [4, 38].
The use of BoNT-A in the pre-surgical treatment of skeletal muscle results in a
significant reduction in contractile force for both single twitch and tetanic contraction
(Figure 2). This reduction in force occurs over a wide range of preload tensions (Figure
3). In both instances, the data demonstrate that the reduced force of contraction is
temporary and reversible (Figures 2 and 3). Active contraction, resulting in mechanical
strain, is critical for tendon-to-bone healing [34, 40-43], and early motion results in
improved clinical outcomes [9, 44-46]. However, the benefits of mechanical strain and
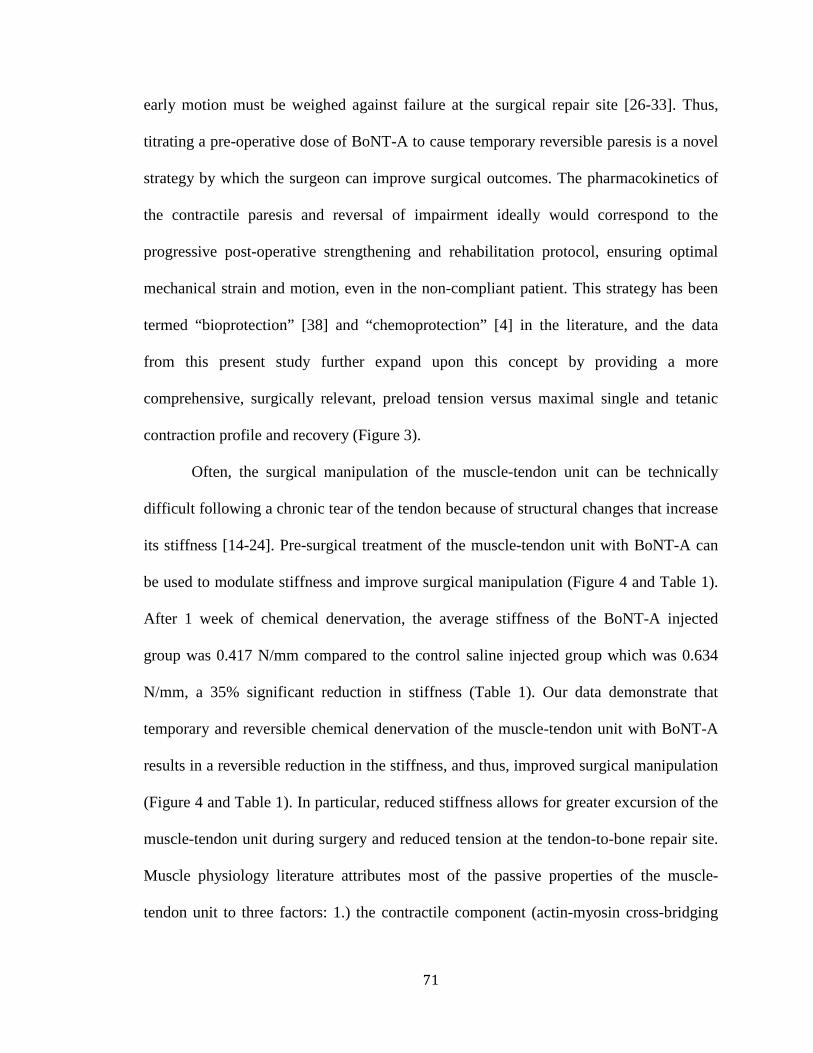
71
early motion must be weighed against failure at the surgical repair site [26-33]. Thus,
titrating a pre-operative dose of BoNT-A to cause temporary reversible paresis is a novel
strategy by which the surgeon can improve surgical outcomes. The pharmacokinetics of
the contractile paresis and reversal of impairment ideally would correspond to the
progressive post-operative strengthening and rehabilitation protocol, ensuring optimal
mechanical strain and motion, even in the non-compliant patient. This strategy has been
termed “bioprotection” [38] and “chemoprotection” [4] in the literature, and the data
from this present study further expand upon this concept by providing a more
comprehensive, surgically relevant, preload tension versus maximal single and tetanic
contraction profile and recovery (Figure 3).
Often, the surgical manipulation of the muscle-tendon unit can be technically
difficult following a chronic tear of the tendon because of structural changes that increase
its stiffness [14-24]. Pre-surgical treatment of the muscle-tendon unit with BoNT-A can
be used to modulate stiffness and improve surgical manipulation (Figure 4 and Table 1).
After 1 week of chemical denervation, the average stiffness of the BoNT-A injected
group was 0.417 N/mm compared to the control saline injected group which was 0.634
N/mm, a 35% significant reduction in stiffness (Table 1). Our data demonstrate that
temporary and reversible chemical denervation of the muscle-tendon unit with BoNT-A
results in a reversible reduction in the stiffness, and thus, improved surgical manipulation
(Figure 4 and Table 1). In particular, reduced stiffness allows for greater excursion of the
muscle-tendon unit during surgery and reduced tension at the tendon-to-bone repair site.
Muscle physiology literature attributes most of the passive properties of the muscle-
tendon unit to three factors: 1.) the contractile component (actin-myosin cross-bridging

72
interactions); 2.) the intra-myofibril series elastic component (titin and desmin); and 3.)
the parallel elastic components (connective tissue of the epimysium, perimysium, and the
endomysium) [47]. Often, the neural component of tone has been de-emphasized as a
significant contributor to passive biomechanical muscle-tendon unit properties [47]. By
chemically denervating the muscle with BoNT-A, our data demonstrate that neural tone
is an important contributor to muscle tone, and the flaccid paresis that follows pre-
operative BoNT-A injection may facilitate tendon repair surgery.
Although our study suggests that pre-surgical BoNT-A injection can improve
surgical manipulation of the muscle-tendon unit, future studies are needed to optimize the
presurgical dose of BoNT-A, and pharmacokinetic response studies are needed to
determine if outcomes will improve with bioprotection/chemoprotection. A limitation of
the present study is that longer period of time was not studied to ensure that the primary
end-point of muscle-tendon unit stiffness returned to “normal.” There are some recent
basic science reports and clinical reports that indicate that botulinum toxin A injection
may result in persistent structural changes in injected skeletal muscle [48], which can be
detected by needle EMG months after injection [49]. However, the majority of clinical
studies indicate that the orthopaedic applications of botulinum neurotoxin A injection are
both safe and effective, even after repeat injections, for treatment and management of
spasticity associated with cerebral palsy [35, 50, 51] and flexion contractures following
total knee arthroplasty [52]. Some initial studies in the literature suggest that BoNT-A
pretreatment will improve outcomes in both a rat animal model and a clinical hand zone 2
flexor tendon injury study [4, 38]. Accordingly, the notable findings presented in this
study warrant further investigation. The present study has the limitation of being
73
performed in a mouse gastrocnemius model. Despite the similarities that exist between
the muscle-tendon unit of a mouse and human, there are differences in size, volume, and
muscle fiber composition between the animal model and humans. Further, all
experimentation was performed in healthy muscle-tendon units that had not undergone
tenotomy or injury. Therefore, future studies are needed to study the effects of BoNT-A
in the post-tenotomy setting. All experimentation for this study was performed in vivo.
The tendon, attached to the calcaneus, was disarticulated and linearized with the force
transducer to ensure accurate force recordings from the muscle. Our in vivo
experimentation has the limitation that it does not replicate the exact biomechanics of
normal muscle-tendon-bone action. Further, it is possible that general anesthesia
influences muscle tone and function. However, muscle-tendon unit testing in both BoNT-
A and saline-injected groups were performed under general anesthesia in a similar
manner, with the same anesthetic agent and dose.
Focusing on the proximal muscle portion of the muscle-tendon unit has been
described as a “paradigm shift” [4] from historical attempts at tendon repair [4, 38]. In a
rat Achilles’ tendon animal model, temporary, chemical, partial paresis results in
“bioprotection” of the tendon repair, resulting in improved structural outcomes by
reducing the active muscle contractile force [38]. Similar favorable outcomes were
observed clinically in a study of hand zone 2 flexor tendon repairs [4]. However,
complete absence of tension has been demonstrated to impair the biomechanics of tendon
healing [34], as some mechanical strain provided by muscle contraction is required to
improve molecular remodeling and osteointegration [40-43]. Early motion is beneficial
because it reduces stiffness and increases range of motion, but overly strenuous early

74
rehabilitation may lead to gap formation at the repair site or tendon rupture [9, 44-46].
Clinically, the surgeon must balance post-operative rehabilitation and repair site integrity.
The study results suggest that pre-surgical treatment with BoNT-A will facilitate
the surgical manipulation of the muscle-tendon unit, thus potentially improving operative
outcomes. The results implicate neural tone as a considerable contributor to the passive
repair tension of the muscle-tendon unit. Our study suggests that modulation of neural
tone by causing temporary reversible paresis is a novel approach that may improve intra-
operative and post-operative passive muscle properties, allowing for progressive
rehabilitation while protecting the surgical repair site; however, future studies will be
necessary to confirm this hypothesis. The results of our study also have implications for
orthopaedic surgical repair of ruptured tendons, such as hand zone 2 flexor tendons,
biceps tendon, triceps tendon, rotator cuff, the Achilles tendon, and the quadriceps
tendon.
ACKNOWLEDGEMENTS
We would like to thank Dr Thorsten M. Seyler, Mrs Eileen Martin, and Mrs
Casey Northam for their support in the planning and execution of the experiments, as
well as useful suggestions in the preparation of this manuscript.
This project is taken in part from a dissertation submitted to the Neuroscience
Program, Wake Forest University Graduate School of Arts and Sciences, in partial
fulfillment of the requirements for the degree of Doctor of Philosophy.

75
SOURCE OF FUNDING
All studies were completed with intra-departmental physician-scientist start-up funds. No
external funding source was utilized and no external funding source played a role in this
investigation.
76
REFERENCES
1. Butler, D.L., N. Juncosa-Melvin, G.P. Boivin, M.T. Galloway, J.T. Shearn, C.
Gooch, et al., Functional tissue engineering for tendon repair: A multidisciplinary
strategy using mesenchymal stem cells, bioscaffolds, and mechanical stimulation.
J Orthop Res, 2008. 26(1): p. 1-9.
2. Oh, J.H., S.H. Kim, H.M. Ji, K.H. Jo, S.W. Bin, and H.S. Gong, Prognostic
factors affecting anatomic outcome of rotator cuff repair and correlation with
functional outcome. Arthroscopy, 2009. 25(1): p. 30-9.
3. Galatz, L.M., C.M. Ball, S.A. Teefey, W.D. Middleton, and K. Yamaguchi, The
outcome and repair integrity of completely arthroscopically repaired large and
massive rotator cuff tears. J Bone Joint Surg Am, 2004. 86-A(2): p. 219-24.
4. De Aguiar, G., L.A. Chait, D. Schultz, S. Bleloch, A. Theron, C.N. Snijman, et
al., Chemoprotection of flexor tendon repairs using botulinum toxin. Plast
Reconstr Surg, 2009. 124(1): p. 201-9.
5. Silfverskiold, K.L., E.J. May, and A.H. Tornvall, Gap formation during controlled
motion after flexor tendon repair in zone II: a prospective clinical study. J Hand
Surg Am, 1992. 17(3): p. 539-46.
6. Elliot, D., N.S. Moiemen, A.F. Flemming, S.B. Harris, and A.J. Foster, The
rupture rate of acute flexor tendon repairs mobilized by the controlled active
motion regimen. J Hand Surg Br, 1994. 19(5): p. 607-12.
7. Navali, A.M. and A. Rouhani, Zone 2 flexor tendon repair in young children: a
comparative study of four-strand versus two-strand repair. J Hand Surg Eur Vol,
2008. 33(4): p. 424-9.

77
8. Osada, D., S. Fujita, K. Tamai, T. Yamaguchi, A. Iwamoto, and K. Saotome,
Flexor tendon repair in zone II with 6-strand techniques and early active
mobilization. J Hand Surg Am, 2006. 31(6): p. 987-92.
9. Silfverskiold, K.L. and E.J. May, Flexor tendon repair in zone II with a new
suture technique and an early mobilization program combining passive and active
flexion. J Hand Surg Am, 1994. 19(1): p. 53-60.
10. Riley, G.P., R.L. Harrall, C.R. Constant, M.D. Chard, T.E. Cawston, and B.L.
Hazleman, Tendon degeneration and chronic shoulder pain: changes in the
collagen composition of the human rotator cuff tendons in rotator cuff tendinitis.
Ann Rheum Dis, 1994. 53(6): p. 359-66.
11. Goutallier, D., J.M. Postel, P. Gleyze, P. Leguilloux, and S. Van Driessche,
Influence of cuff muscle fatty degeneration on anatomic and functional outcomes
after simple suture of full-thickness tears. J Shoulder Elbow Surg, 2003. 12(6): p.
550-4.
12. Bartolozzi, A., D. Andreychik, and S. Ahmad, Determinants of outcome in the
treatment of rotator cuff disease. Clin Orthop Relat Res, 1994(308): p. 90-7.
13. Oh, L.S., B.R. Wolf, M.P. Hall, B.A. Levy, and R.G. Marx, Indications for rotator
cuff repair: a systematic review. Clin Orthop Relat Res, 2007. 455: p. 52-63.
14. Meyer, D.C., H. Hoppeler, B. von Rechenberg, and C. Gerber, A
pathomechanical concept explains muscle loss and fatty muscular changes
following surgical tendon release. J Orthop Res, 2004. 22(5): p. 1004-7.
78
15. Safran, O., K.A. Derwin, K. Powell, and J.P. Iannotti, Changes in rotator cuff
muscle volume, fat content, and passive mechanics after chronic detachment in a
canine model. J Bone Joint Surg Am, 2005. 87(12): p. 2662-70.
16. Barton, E.R., J.A. Gimbel, G.R. Williams, and L.J. Soslowsky, Rat supraspinatus
muscle atrophy after tendon detachment. J Orthop Res, 2005. 23(2): p. 259-65.
17. Joe, A.W., L. Yi, A. Natarajan, F. Le Grand, L. So, J. Wang, et al., Muscle injury
activates resident fibro/adipogenic progenitors that facilitate myogenesis. Nat Cell
Biol. 12(2): p. 153-63.
18. Uezumi, A., S. Fukada, N. Yamamoto, S. Takeda, and K. Tsuchida, Mesenchymal
progenitors distinct from satellite cells contribute to ectopic fat cell formation in
skeletal muscle. Nat Cell Biol. 12(2): p. 143-52.
19. Jozsa, L., P. Kannus, J. Thoring, A. Reffy, M. Jarvinen, and M. Kvist, The effect
of tenotomy and immobilisation on intramuscular connective tissue. A
morphometric and microscopic study in rat calf muscles. J Bone Joint Surg Br,
1990. 72(2): p. 293-7.
20. Fabis, J., M. Danilewicz, and A. Omulecka, Rabbit supraspinatus tendon
detachment: effects of size and time after tenotomy on morphometric changes in
the muscle. Acta Orthop Scand, 2001. 72(3): p. 282-6.
21. Halder, A.M., S.W. O'Driscoll, G. Heers, N. Mura, M.E. Zobitz, K.N. An, et al.,
Biomechanical comparison of effects of supraspinatus tendon detachments,
tendon defects, and muscle retractions. J Bone Joint Surg Am, 2002. 84-A(5): p.
780-5.
79
22. Hansen, M.L., J.C. Otis, J.S. Johnson, F.A. Cordasco, E.V. Craig, and R.F.
Warren, Biomechanics of massive rotator cuff tears: implications for treatment. J
Bone Joint Surg Am, 2008. 90(2): p. 316-25.
23. Gerber, C., D.C. Meyer, A.G. Schneeberger, H. Hoppeler, and B. von
Rechenberg, Effect of tendon release and delayed repair on the structure of the
muscles of the rotator cuff: an experimental study in sheep. J Bone Joint Surg
Am, 2004. 86-A(9): p. 1973-82.
24. Gimbel, J.A., S. Mehta, J.P. Van Kleunen, G.R. Williams, and L.J. Soslowsky,
The tension required at repair to reappose the supraspinatus tendon to bone
rapidly increases after injury. Clin Orthop Relat Res, 2004(426): p. 258-65.
25. Gimbel, J.A., J.P. Van Kleunen, S.P. Lake, G.R. Williams, and L.J. Soslowsky,
The role of repair tension on tendon to bone healing in an animal model of
chronic rotator cuff tears. J Biomech, 2007. 40(3): p. 561-8.
26. Dona, E., M.P. Gianoutsos, and W.R. Walsh, Optimizing biomechanical
performance of the 4-strand cruciate flexor tendon repair. J Hand Surg Am, 2004.
29(4): p. 571-80.
27. Aslam, A. and A. Afoke, A new core suture technique for flexor tendon repair:
biomechanical analysis of tensile strength and gap formation. J Hand Surg Br,
2000. 25(4): p. 390-2.
28. Mortenson, R.A. and J.R. Urbaniak, Analysis of tensile strength of tendon
anastomosis. Surg Forum, 1972. 23(0): p. 470-1.
29. Dinopoulos, H.T., M.I. Boyer, M.E. Burns, R.H. Gelberman, and M.J. Silva, The
resistance of a four- and eight-strand suture technique to gap formation during
80
tensile testing: an experimental study of repaired canine flexor tendons after 10
days of in vivo healing. J Hand Surg Am, 2000. 25(3): p. 489-98.
30. Aoki, M., P.R. Manske, D.L. Pruitt, H. Kubota, and B.J. Larson, Canine cadaveric
study of flexor tendon repair using tendon splint: tensile strength and the work of
flexion. Nippon Seikeigeka Gakkai Zasshi, 1995. 69(5): p. 332-41.
31. Barrie, K.A., S.W. Wolfe, C. Shean, D. Shenbagamurthi, J.F. Slade, 3rd, and
M.M. Panjabi, A biomechanical comparison of multistrand flexor tendon repairs
using an in situ testing model. J Hand Surg Am, 2000. 25(3): p. 499-506.
32. Greenwald, D.P., M.A. Randolph, H.Z. Hong, and J.W. May, Jr., Augmented
Becker versus modified Kessler tenorrhaphy in monkeys: dynamic mechanical
analysis. J Hand Surg Am, 1995. 20(2): p. 267-72.
33. McLarney, E., H. Hoffman, and S.W. Wolfe, Biomechanical analysis of the
cruciate four-strand flexor tendon repair. J Hand Surg Am, 1999. 24(2): p. 295-
301.
34. Galatz, L.M., N. Charlton, R. Das, H.M. Kim, N. Havlioglu, and S. Thomopoulos,
Complete removal of load is detrimental to rotator cuff healing. J Shoulder Elbow
Surg, 2009. 18(5): p. 669-75.
35. Seyler, T.M., B.P. Smith, D.R. Marker, J. Ma, J. Shen, T.L. Smith, et al.,
Botulinum neurotoxin as a therapeutic modality in orthopaedic surgery: more than
twenty years of experience. J Bone Joint Surg Am, 2008. 90 Suppl 4: p. 133-45.
36. Ramachandran, M. and D.M. Eastwood, Botulinum toxin and its orthopaedic
applications. J Bone Joint Surg Br, 2006. 88(8): p. 981-7.
81
37. Stone, A.V., J. Ma, P.W. Whitlock, L.A. Koman, T.L. Smith, B.P. Smith, et al.,
Effects of Botox and Neuronox on muscle force generation in mice. J Orthop Res,
2007. 25(12): p. 1658-64.
38. Ma, J., J. Shen, B.P. Smith, A. Ritting, T.L. Smith, and L.A. Koman,
Bioprotection of tendon repair: adjunctive use of botulinum toxin A in Achilles
tendon repair in the rat. J Bone Joint Surg Am, 2007. 89(10): p. 2241-9.
39. Shen, J., J. Ma, G.A. Elsaidi, C.A. Lee, T.L. Smith, K.H. Tan, et al., Gene
expression of myogenic regulatory factors following intramuscular injection of
botulinum A toxin in juvenile rats. Neurosci Lett, 2005. 381(3): p. 207-10.
40. Joshi, S.D. and K. Webb, Variation of cyclic strain parameters regulates
development of elastic modulus in fibroblast/substrate constructs. J Orthop Res,
2008. 26(8): p. 1105-13.
41. Nirmalanandhan, V.S., Shearn, J.T., Juncosa-Melvin, N., Rao, M., Jain, A.,
Gooch, C., et al., Optimizing the mechanical stimulus in culture to improve
construct biomechanics for tendon repair. molecular and cellular biomechanics,
2006. 3(4): p. 131-133.
42. Cousineau-Pelletier, P. and E. Langelier, Relative contributions of mechanical
degradation, enzymatic degradation, and repair of the extracellular matrix on the
response of tendons when subjected to under- and over- mechanical stimulations
in vitro. J Orthop Res, 2009.
43. Riboh, J., A.K.S. Chong, H. Pham, M. Longaker, C. Jacobs, and J. Chang,
Optimization of Flexor Tendon Tissue Engineering With a Cyclic Strain
Bioreactor. The Journal of Hand Surgery, 2008. 33(8): p. 1388-1396.

82
44. Aoki, M., H. Kubota, D.L. Pruitt, and P.R. Manske, Biomechanical and histologic
characteristics of canine flexor tendon repair using early postoperative
mobilization. J Hand Surg Am, 1997. 22(1): p. 107-14.
45. Chow, J.A., L.J. Thomes, S. Dovelle, J. Monsivais, W.H. Milnor, and J.P.
Jackson, Controlled motion rehabilitation after flexor tendon repair and grafting.
A multi-centre study. J Bone Joint Surg Br, 1988. 70(4): p. 591-5.
46. Gelberman, R.H., M.J. Botte, J.J. Spiegelman, and W.H. Akeson, The excursion
and deformation of repaired flexor tendons treated with protected early motion. J
Hand Surg Am, 1986. 11(1): p. 106-10.
47. Gajdosik, R.L., Passive extensibility of skeletal muscle: review of the literature
with clinical implications. Clin Biomech (Bristol, Avon), 2001. 16(2): p. 87-101.
48. Fortuna, R., M. Aurelio Vaz, A. Rehan Youssef, D. Longino, and W. Herzog,
Changes in contractile properties of muscles receiving repeat injections of
botulinum toxin (Botox). J Biomech.
49. Dunne, J.W., B.J. Singer, P.L. Silbert, and K.P. Singer, Prolonged vastus lateralis
denervation after botulinum toxin type A injection. Mov Disord. 25(3): p. 397-
401.
50. Lowe, K., I. Novak, and A. Cusick, Repeat injection of botulinum toxin A is safe
and effective for upper limb movement and function in children with cerebral
palsy. Dev Med Child Neurol, 2007. 49(11): p. 823-9.
51. Koman, L.A., J.F. Mooney, 3rd, B.P. Smith, F. Walker, and J.M. Leon,
Botulinum toxin type A neuromuscular blockade in the treatment of lower
83
extremity spasticity in cerebral palsy: a randomized, double-blind, placebo-
controlled trial. BOTOX Study Group. J Pediatr Orthop, 2000. 20(1): p. 108-15.
52. Seyler, T.M., R.H. Jinnah, L.A. Koman, D.R. Marker, M.A. Mont, S.D. Ulrich, et
al., Botulinum toxin type A injections for the management of flexion contractures
following total knee arthroplasty. J Surg Orthop Adv, 2008. 17(4): p. 231-8.
84
Chapter 3 Figures and Table
FIG 1: Experimental Apparatus. The experimental apparatus and key components are
labeled in this schematic diagram.
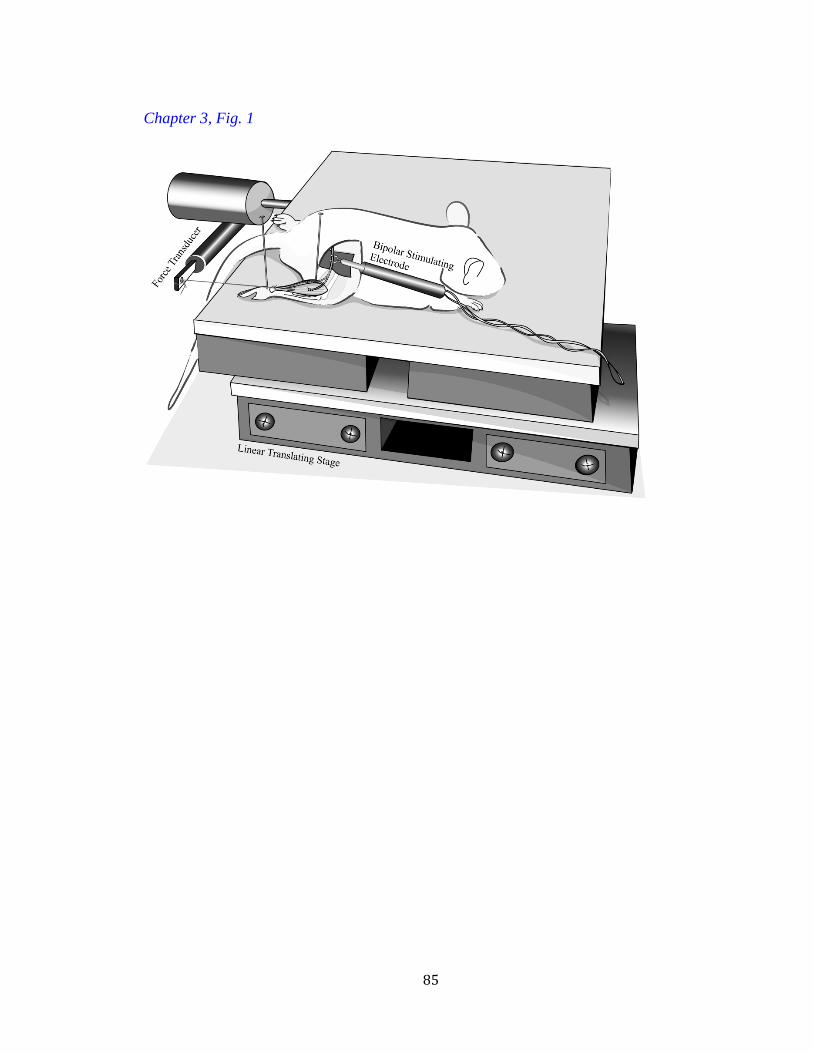
85
Chapter 3, Fig. 1
86
FIG 2: The Effect of BoNT-A on Gastrocnemius Muscle Contraction. There is a
significant reduction in both maximal single twitch and tetanic force of muscle
contraction at 1 week and 2 weeks after injection of BoNT-A when compared to saline
injected controls (p<0.05, denoted by *). Panels A-B represent maximal force of single
twitch and tetanic contraction one-week post-injection. Panels C-D represent maximal
force of single twitch and tetanic contraction two-weeks post injection. Data are
presented as the mean and standard error of the mean.

87
Chapter 3, Fig. 2

88
FIG 3: The Effect of Preload Tension on Gastrocnemius Muscle Contraction. Panels A-B
represent the relationship between preload tension and maximal single-twitch and tetanic
contraction 1 week post BoNT-A injection. Panels C-D represent the relationship
between preload tension and maximal single-twitch and tetanic contraction 2 weeks post-
BoNT-A injection. The amount of preload tension applied to the muscle tendon unit
significantly affected the maximal muscle single twitch and tetanic contractile force for
the saline injected controls (p<0.05, Panels A-D). Further, there was a significant
reduction in the muscle contractile force when the BoNT-A group was compared to the
saline injected controls at 1 week post-injection (Panels A-B). Data are presented as mean
and standard error of the mean.
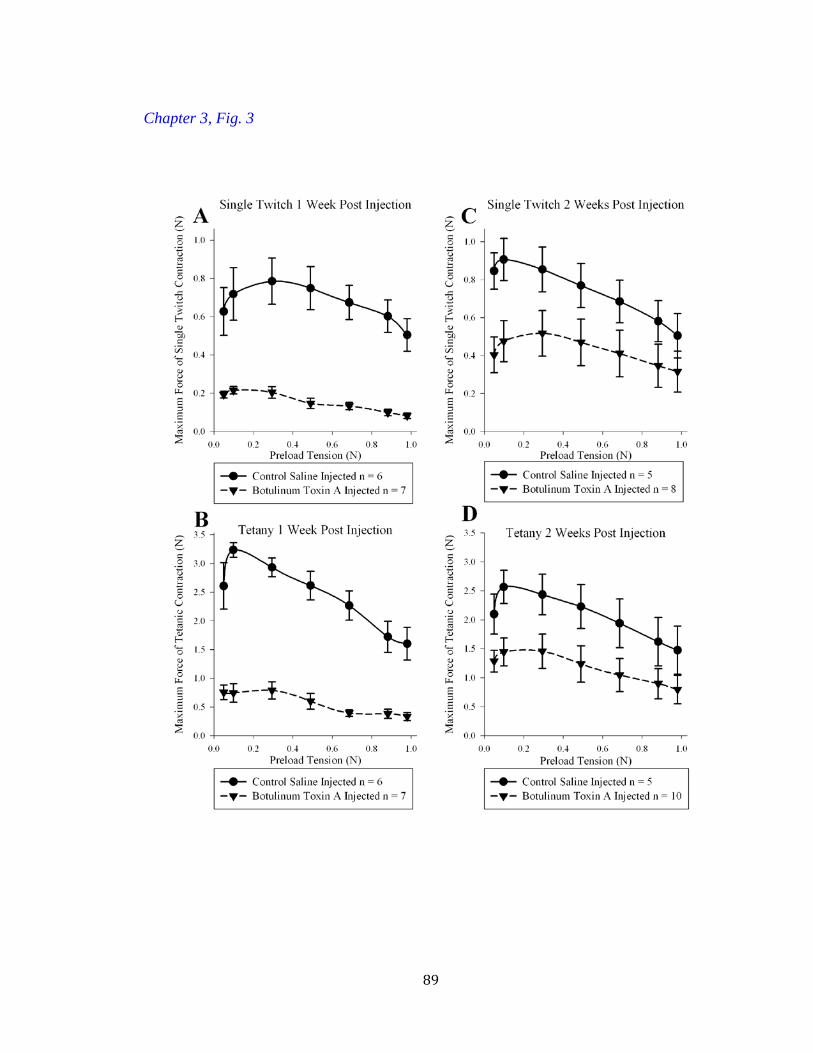
89
Chapter 3, Fig. 3

90
FIG 4: The Effect of Displacement of the Gastrocnemius-Muscle-Achilles-Tendon-Unit
on Passive Peak Tension. The passive peak tension of the muscle-tendon unit increases as
displacement increases. A significant difference exists between the muscle-tendon unit
peak passive tension BoNT-A injected experimental group compared to the saline
injected controls at 1 week post-injection starting above 3 mm displacement (p<0.05,
denoted by †, Panel A). Significant differences were not detected between the
experimental groups 2 weeks post-injection (Panel B). Data are presented as the mean
and standard error of the mean.
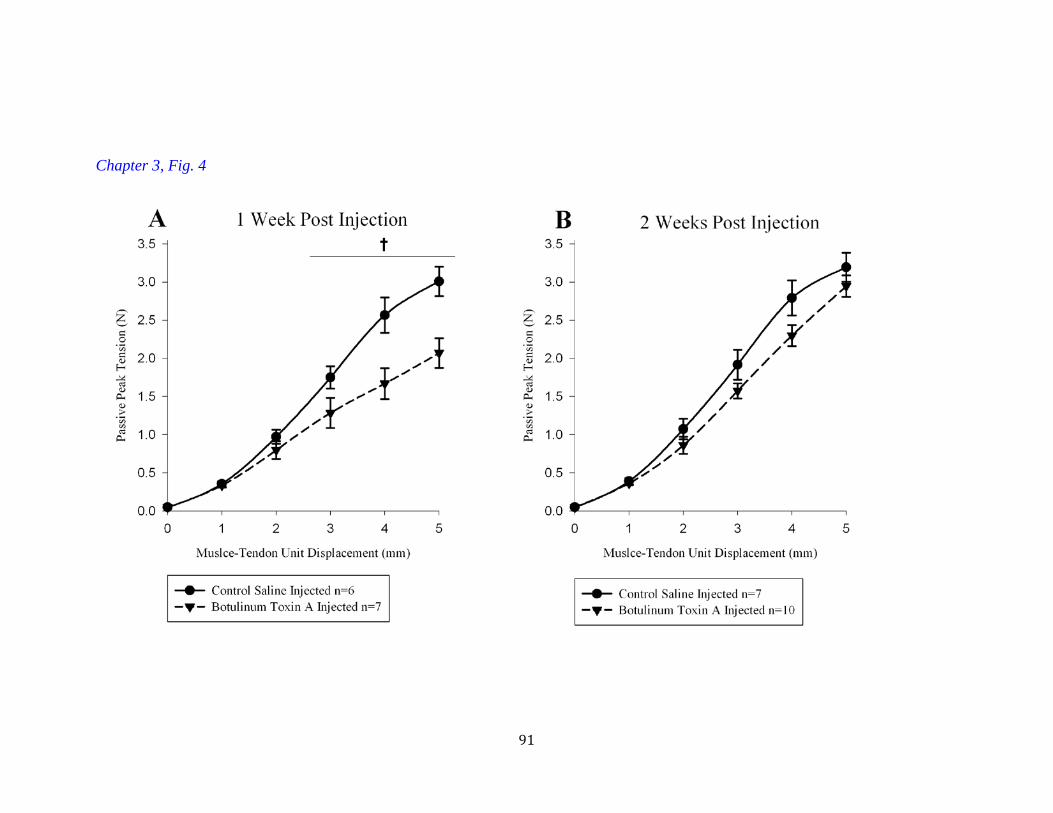
91
Chapter 3, Fig. 4
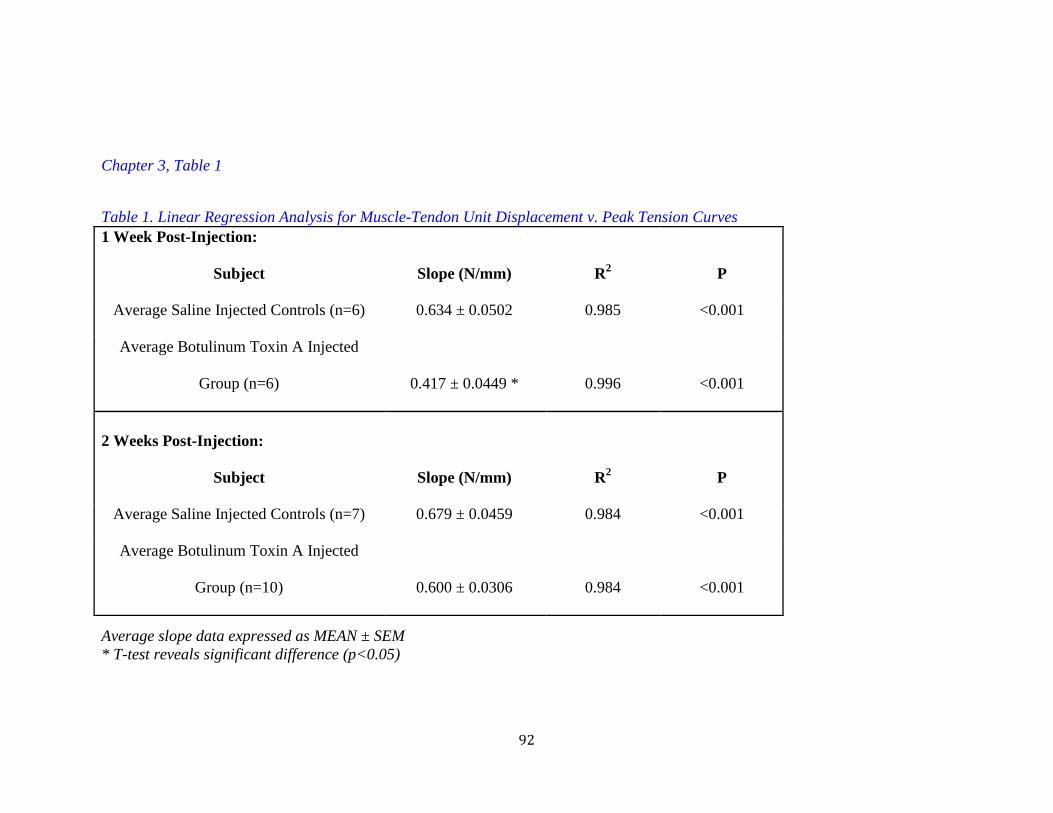
92
Chapter 3, Table 1
Table 1. Linear Regression Analysis for Muscle-Tendon Unit Displacement v. Peak Tension Curves 1 Week Post-Injection:
Subject Slope (N/mm) R2 P
Average Saline Injected Controls (n=6) 0.634 ± 0.0502 0.985 <0.001
Average Botulinum Toxin A Injected
Group (n=6) 0.417 ± 0.0449 * 0.996 <0.001
2 Weeks Post-Injection:
Subject Slope (N/mm) R2 P
Average Saline Injected Controls (n=7) 0.679 ± 0.0459 0.984 <0.001
Average Botulinum Toxin A Injected
Group (n=10) 0.600 ± 0.0306 0.984 <0.001
Average slope data expressed as MEAN ± SEM * T-test reveals significant difference (p<0.05)

93
CHAPTER 4
CONTRIBUTIONS OF NEURAL TONE TO IN VIVO PASSIVE
MUSCLE-TENDON UNIT BIOMECHANICAL PROPERTIES IN A
RAT ROTATOR CUFF ANIMAL MODEL
Sandeep Mannava, Walter F. Wiggins, Katherine R. Saul, Joel D. Stitzel, Beth P. Smith,
L. Andrew Koman, Thomas L. Smith, Christopher J. Tuohy
The following manuscript was published in the Ann of Biomed Eng. 2011 Mar 29. EPub.
PMID: 21445691. This chapter is reprinted with permission. Stylistic variations are due
to the requirements of the journal. S. Mannava performed the experiments, prepared the
manuscript, and served as corresponding author. T.L. Smith acted in an advisory and
editorial capacity.
94
ABSTRACT
Passive viscoelastic properties of muscle-tendon units are key determinants of
intra- and post-operative success. Atrophied, retracted, and stiff muscle-tendon units are
technically challenging to manipulate and perform poorly after surgical repair. This study
employs botulinum neurotoxin A (BoNT-A)-mediated inhibition of presynaptic
acetylcholine release to examine in vivo neural contributions to soft tissue biomechanical
properties. In vivo load-relaxation and active muscle contractile force testing protocols
were performed in the rat rotator cuff model. The passive properties were assessed using
linear regression analysis and Fung’s quasi-linear viscoelastic (QLV) model. BoNT-A
injected muscle-tendon units had a significant reduction in force of contraction
(p=0.001). When compared to saline-injected controls, the BoNT-A significantly
decreased parameter ‘A’ of the QLV model, which represents the linear elastic response
(p=0.032). The viscous properties in the BoNT-A treatment group were not significantly
different from saline-injected controls, as determined by comparison of QLV model
parameters ‘C,’ ‘τ1,’ and ‘τ2.’ In conclusion, neural tone contributes significantly to
muscle-tendon unit passive biomechanical properties. Pre-surgical treatment with BoNT-
A may improve the rehabilitation of muscle by altering its passive elastic properties.
Accordingly, pharmacological modulation of skeletal muscle stiffness with BoNT-A
increases flexibility, potentially improving function. Chemical denervation with BoNT-A
may also improve the manipulation of stiff and difficult to mobilize muscles during
surgical procedures.
95
INTRODUCTION
Approximately 300,000 rotator cuff repair surgeries are performed annually in the
United States, as rotator cuff tears are a common cause of upper-extremity pain and
disability [1]. Chronically torn rotator cuffs can pose an operative challenge because the
scarred and retracted muscle-tendon units are difficult to manipulate surgically [2-4].
Studies in rat [5, 6], sheep [7, 8], dog [2], and human rotator cuff [9] have demonstrated
that the muscle-tendon unit becomes retracted and stiffer after injury, which is attributed
to changes in the muscle’s structure [2, 5-8]. Specifically, as the muscle atrophies
following tendon injury, it undergoes sarcopenia [10], decreased muscle volume [2, 11,
12], fibrofatty infiltration [2, 11-13], decreased capillary density [2, 7, 8, 14], and muscle
fiber-type switching [12].
In some instances, full excursion of the injured muscle-tendon unit back to its
anatomical footprint on the humeral head is not possible during surgical repair of torn
rotator cuffs [6, 9]. Even when operative repair is possible, the repair tension might be
excessive, leading to early repair site failure or re-tears after surgery [6, 15, 16]. Other
investigators have demonstrated that repair tension, which is determined by the muscle-
tendon unit biomechanical properties, is an important factor that influences tendon-to-
bone healing in the rotator cuff [6]. In particular, excessive repair tension has been
associated with impaired tendon-to-bone healing [6] and worse patient-perceived
functional outcomes after rotator cuff repair surgery [9].
Passive skeletal muscle-tendon unit load-relaxation properties are key
determinants of operative success following tendon repair surgery [6, 17]. Most
biomechanical studies occur in the ex vivo or in vitro setting and focus on structural
96
components of the muscle, such as actin, myosin, titin, and desmin [17]. However, these
studies fail to evaluate the influence of the nervous system on skeletal muscle tone [17].
Surgical and rehabilitation experience with patients who have sustained neurological
insults, such as cerebral palsy or cerebrovascular accidents, demonstrates that the nervous
system influences the passive biomechanical properties of muscle [18-21].
The purpose of the current study is to use botulinum neurotoxin A (BoNT-A) to
examine and quantify in vivo neurological contributions to skeletal muscle tone, which
consists of elasticity and viscosity. BoNT-A is a potent, naturally occurring toxin that
results in a temporary and reversible muscle paresis through pre-synaptic neurological
blockade of acetylcholine release [18, 19, 22]. The present study employs Fung’s quasi-
linear visco-elastic (QLV) model to characterize the load-relaxation behavior of muscle-
tendon units in an in vivo animal model system. The use of QLV modeling to help
characterize a multi-component, muscle-tendon system in vivo was chosen because of the
clinical relevance for tendon repair surgery. Since the tendon of the supraspinatus is short
relative to the length of the muscle, in vivo biomechanical testing followed by QLV
analysis can be used to characterize neuronal influences on the muscle, as the tendon
contributions to passive biomechanical properties will likely be negligible in this
particular anatomic location [23]. The study hypothesis is that the nervous system
contributes to in vivo soft-tissue biomechanical properties; therefore, muscle-tendon unit
tone, specifically stiffness and elasticity, can be pharmacologically modulated with
BoNT-A.
97
MATERIALS AND METHODS
The rat shoulder model has been established in previous experiments as a suitable
model for the study of human rotator cuff pathology [24, 25]. A total of 12 male Sprague-
Dawley rats weighing 400-450g (Charles River, Wilmington, MA) were studied. While
housed in the controlled temperature vivarium with 12 hour light-dark cycles, chow and
water were provided to the rats ad libitum. The animals were divided into two
experimental groups based upon injection type. Six rats were injected with normal saline
and served as controls; the remaining six rats were injected with equal volumes of BoNT-
A. The injection protocol is described in greater detail below. At 1-week post-injection,
in vivo muscle function and biomechanical load-relaxation testing was performed. The
animals were sacrificed immediately after in vivo testing. Experimentation was blinded in
that one scientist injected the animal, and a second scientist performed all surgery and in
vivo testing. The second scientist was not made aware of the group designation of the
animals until after all data was collected and analyzed. All experimentation was
conducted after approval from the Institutional Animal Care and Use Committee.
Botulinum Neurotoxin A and Saline Injection Procedure
Botulinum neurotoxin A (Allergan, Irvine, CA) was reconstituted as previously
described.[26-28] Briefly, a 100U vial of lyophylized BoNT-A was reconstituted with
normal saline. The toxin was injected into the supraspinatus muscle at a dosage of 9
units/kg body weight in an injection volume of 10 µL with a Hamilton syringe (Fischer
Scientific, Pittsburg, PA) equipped with a 30 gauge needle. The dosage of BoNT-A was
determined based on previously published reports in this animal model system and

98
muscle [29, 30]. Control animals received an equal volume injection of normal saline
(0.9%) in a similar manner.
All injections were performed percutaneously. Animals were anesthetized with
isoflurane (Webster Veterinary, Patterson Companies Inc., Sterling, MA) and placed in
the prone position. The scapula and shoulder were shaved and prepped with alcohol. The
scapular spine was palpated, and the muscle was injected superior and caudal to that bony
landmark. The needle was advanced to the bone (suprascapular fossa) and then
withdrawn slightly. The injection volume was distributed over the volume of the muscle.
Surgical Exposure and Experimental Apparatus
Saline injected control animals (n=6) and BoNT-A animals (n=6) were
anesthetized with isoflurane 1-week post-injection. The time period of 1 week was
chosen because the period of time from injection was thought to be sufficient to cause
maximal skeletal muscle paresis, which is defined as a reduction in active contractile
force. Similarly, we hypothesized that passive biomechanical properties would also
change during this initial period of time following injection. Further, we felt that there
would be minimal changes in the muscle’s structure in the 1 week following BoNT-A
injection, making passive biomechanical comparisons of the load-displacement data
between experimental groups more likely to be attributable to the neural contributions
and less likely to be attributable to structural changes (i.e. atrophy). The injected upper-
limbs were shaved and prepped with the animal in the prone position. A skin incision was
made over the scapula, extending towards the humerus. The overlying musculature
(deltoid and trapezius) were reflected, and the acromioclavicular ligament was cut,
exposing the injected supraspinatus muscle-tendon unit. A custom titanium plate (6.5 mm
99
x 3 mm) with roughened contact surfaces was affixed to the freed supraspinatus tendon.
Clamp slippage was not observed during the experimental protocol. A rigidly affixed
custom clamp was then securely fastened to a linearly translating experimental table. This
custom clamp was attached to the inferior aspect of the scapula, below the scapular spine.
The clamp prevented the freely-gliding scapula from moving during experimentation.
The scapula was gently retracted from the thorax and a brachial plexus dissection was
performed to isolate the suprascapular nerve. A bipolar hook electrode was placed on the
suprascapular nerve. The nerve plexus and surrounding tissue was electrically isolated by
wrapping a piece of Silastic sheeting (Dow Corning Co, Midland, MI) around the exterior
of the suprascapular nerve and bipolar electrode. The rat’s upper extremity was
immobilized with straps and pins on a platform that translated linearly. A single body
strap and pins through the wrist and elbow were used to isolate other directional force
vectors, ensuring that contractile force and passive force produced by the supraspinatus
muscle-tendon unit translated perpendicular and ‘in line’ with the force transducer in all
experimental cases (Fig 1). If force was not directed perpendicular/‘in line’ with the force
transducer, it is possible that the recorded values of tension would be lower than what is
actually produced during active force of contraction and passive stretching protocols.
A steel wire was used to connect the custom titanium plate holding the
supraspinatus tendon to a force transducer (model FORT100; World Precision
Instruments Inc., Sarasota, FL). The transducer was connected to an amplifier (model 13-
G4615-50; Gould, Cleveland, OH) that was interfaced with a personal computer through
an interface controller (EMKA TECHNOLOGIES Inc., Falls Church, VA) and an
analog-to-digital converter card (model: PCI-6023E, National Instruments, Austin, TX).
100
A pulse generator (model Tenma TGP110, BioSurplus Inc., San Diego, CA) was used to
stimulate the suprascapular nerve. The stimulation protocol and the force recordings were
controlled and recorded by IOX software, Slow Wave Analyzer (EMKA Technologies
Inc., Falls Church, VA). During all experimental recordings, the body temperature of the
animals was monitored and maintained with an external heat lamp.
Muscle Force Testing
Supramaximal stimulation of the suprascapular nerve was produced with 1.5V. A
range of 0.6V to 2.0V was tested to ensure that maximal single twitch was attained at
1.5V of stimulation, and in all cases, this stimulation voltage produced maximal single
twitch contraction. The muscle-tendon unit was then pretensioned to 0.1N of preload
tension by moving the platform, based on previously published reports in this animal
model system [5, 6], and the suprascapular nerve was stimulated at a frequency of 100Hz,
150Hz, and 200Hz for 1 second, and maximal amplitude of the force of contraction was
recorded. A recovery time of 60 seconds was allowed between stimuli. This recovery
time allowed for full recovery of maximal contractile force. A total of three trials were
performed at each stimulation frequency, and the largest tetanic contractile amplitude was
recorded for each frequency. The stimulation protocol was performed to record the
maximal tetanic contractile force for saline injected controls and BoNT-A injected
animals 1-week after injection.
Passive Load-Relaxation Testing
A starting preload tension of 0.05N was set as 0mm displacement. Prior to the
passive load-relaxation testing, a preconditioning protocol of stretching the muscle-
tendon unit from 0mm to 1mm was executed and held for a duration of 10 seconds, then
101
relaxed to 0 mm for 30 seconds and this was repeated 10 times, based on a previously
published report of in vivo biomechanical testing in this rat rotator cuff model system [5].
The supraspinatus muscle-tendon unit remained connected to the experimental apparatus
after muscle force testing. The stage was then displaced away from the force transducer
to specific displacement increments (between 0 to 8 mm). The passive tension of the
muscle-tendon unit was assessed in vivo by measuring the passive tension produced by
the muscle-tendon unit while the muscle-tendon unit was displaced from 0mm to 8mm of
displacement in 2mm increments. Between load-relaxation cycles, the muscle-tendon unit
was returned to 0mm displacement and allowed to rest for 10 minutes. The passive
tension was continuously recorded for a duration of 210 seconds after displacement,
throughout the experimental protocol.
Fung’s Quasilinear Viscoelastic Model (QLV)
Fung’s quasilinear viscoelastic model (QLV) [31] has been used by others to
provide a mathematical description of the passive biomechanical behavior of the entire,
intact, in vivo muscle-tendon unit during loading and relaxation [5, 29]. Specifically, the
QLV model allows for the extraction of elastic and viscous parameters from the load-
relaxation experiments.
Fung [31] proposed that the uniaxial deformation, ε(t), of a viscoelastic tissue and
the resultant uniaxial stress, σ(t), exhibited the following relationship:
(1)
where G(t) is the reduced relaxation function proposed by Fung,
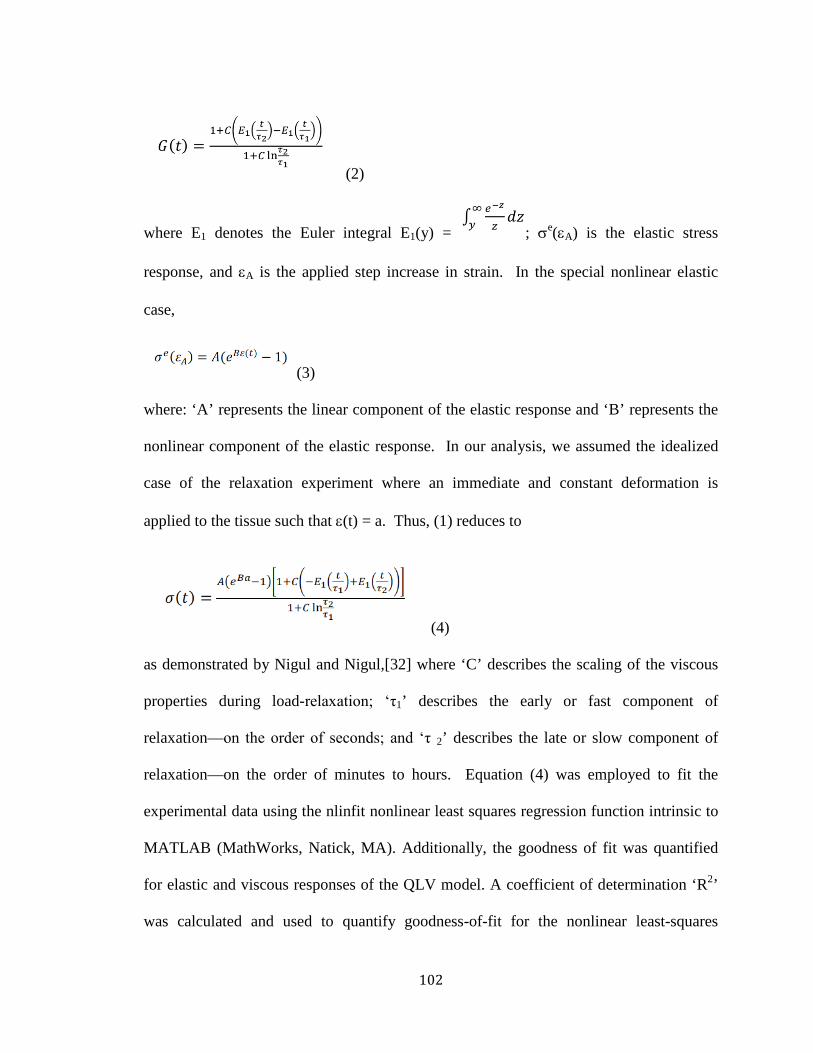
102
(2)
where E1 denotes the Euler integral E1(y) = ; σe(εA) is the elastic stress
response, and εA is the applied step increase in strain. In the special nonlinear elastic
case,
(3)
where: ‘A’ represents the linear component of the elastic response and ‘B’ represents the
nonlinear component of the elastic response. In our analysis, we assumed the idealized
case of the relaxation experiment where an immediate and constant deformation is
applied to the tissue such that ε(t) = a. Thus, (1) reduces to
(4)
as demonstrated by Nigul and Nigul,[32] where ‘C’ describes the scaling of the viscous
properties during load-relaxation; ‘τ1’ describes the early or fast component of
relaxation—on the order of seconds; and ‘τ 2’ describes the late or slow component of
relaxation—on the order of minutes to hours. Equation (4) was employed to fit the
experimental data using the nlinfit nonlinear least squares regression function intrinsic to
MATLAB (MathWorks, Natick, MA). Additionally, the goodness of fit was quantified
for elastic and viscous responses of the QLV model. A coefficient of determination ‘R2’
was calculated and used to quantify goodness-of-fit for the nonlinear least-squares
103
regression. Others have established this technique as an appropriate and validated method
in the rat rotator cuff animal model [5, 29].
When the QLV parameters A and B are varied, the passive tension versus time
curve undergoes a shift and there is a corresponding change in the peak and equilibrium
passive tensions (Fig 2A). Varying parameter ‘A’ results in a change in the passive
tension versus time graph which scales “linearly” (Fig 2A); whereas varying parameter
‘B’ results in a change in the passive tension versus time graph which scales nonlinearly
(Fig 2A). Varying the QLV parameters ‘C,’ ‘τ1,’ and ‘τ 2,’ affects the rate of load-
relaxation and may influence the equilibrium passive tension (Fig 2B). Examples of the
time histories for passive tension at varying displacements are shown (Fig 3). These
curves (Fig 3) are parameterized by the Fung’s QLV method described previously.
Statistics
All values were expressed as the mean ± standard error of the mean. Statistical
analysis was performed using SigmaStat (Systat Software Inc., San Jose, CA). A mixed
model ANOVA followed by a Tukey post hoc test was performed for between and within
group comparison of muscle force measurements stimulated at various frequencies (Fig.
4) and passive tension versus muscle-tendon unit displacement data (Fig 5). T-tests were
performed for comparison of peak stiffness, equilibrium stiffness, and QLV parameters
between BoNT-A experimental and saline-injected control groups. In vivo stiffness of the
muscle-tendon unit was determined based on the linear regression analysis (slope of the
line) for the tension (peak and equilibrium) versus displacement data (Fig 5). Linear
regression analysis was performed on the data recorded between 2 mm to 8 mm on the
passive tension versus displacement data (Fig 5). At 2mm of displacement, the preload

104
tension has been documented in the literature [5] to be on the linear portion of the load-
displacement curve. Therefore, regression analysis on this portion of the data would
presumably avoid the non-linear toe-region.
RESULTS
One week after the injection of BoNT-A, a significant decline (p=0.001) in
maximal tetanic contraction force was documented at all frequencies of stimulation when
compared to saline injected controls (Fig 4). At 1-week after the injection, the BoNT-A
injected group had an average maximal tetanic contractile force of 0.24 N ± 0.05 N, while
the saline injected group had an average maximal tetanic contractile force of 5.06 N ±
0.05 N.
Sample time histories for the control versus BoNT-A passive force development
at various displacements are shown (Fig. 3). Botulinum neurotoxin A significantly
reduced the peak passive tension of the muscle-tendon unit as a function of displacement
one week after injection (p=0.022, Fig 5 A). Post-hoc analysis revealed that there were
significant differences in peak passive tension between experimental groups at 6mm
displacement (p=0.002, Fig 5A) and at 8 mm displacement (p=0.012, Fig 5A). Similarly,
BoNT-A also reduced the equilibrium passive tension of the muscle-tendon unit as a
function of displacement one week after injection (p=0.043, Fig 5B). Post-hoc analysis
revealed that there were significant differences in equilibrium passive tension between
experimental groups at 6mm displacement (p=0.013, Fig 5B) and at 8 mm displacement
(p=0.006, Fig 5B).
As the displacement of the muscle-tendon unit increased, the passive tensions
(both peak and equilibrium) increased linearly (Fig 5 and Table 1). The slopes of the lines
105
representing in vivo stiffness of the muscle-tendon unit (Fig 5) were significantly
different between the BoNT-A group and the saline injected group for peak tension
(p=0.043, Table 1), as there was a 16.32% reduction in the in vivo stiffness of the
muscle-tendon unit for the BoNT-A injected group (Table 1). However, a significant
difference was not detected for the equilibrium tension (p=0.067, Table 1), as in vivo
stiffness was calculated from the displacement versus equilibrium tension data (Fig 5B),
which demonstrated a 22.7% reduction in the stiffness for the chemically denervated
experimental group.
QLV parameter A (representing linear scaling of the elastic response) was
significantly influenced by chemical denervation with BoNT-A one week post-injection
(Table 2). No significant differences in the elastic parameter B and the viscous
parameters C, τ1, and τ 2 were detected between experimental groups (Table 2). A
nonlinear least-squares regression (R2) was calculated to quantify the goodness-of-fit for
all of the time-history recordings to the QLV model: average Saline R2elastic = 0.9704
(Saline R2elastic range: 0.8769 – 0.9997); average Saline R2
viscous = 0.9968 (Saline R2viscous
range: 0.9888 – 0.9998); BoNT-A R2elastic = 0.9889 (BoNT-A R2
elastic range: 0.9757 –
0.9951); and BoNT-A R2viscous = 0.9990 (BoNT-A R2
viscous range: 0.9966 – 0.9997).
DISCUSSION
Neural tone significantly contributes to the passive, in vivo, soft-tissue, load-
relaxation biomechanical properties of the muscle-tendon unit. Chemical denervation
with BoNT-A influences both the active contractile force and passive viscoelastic
properties of the muscle-tendon unit. More specifically, the nervous system influences
the elastic component of the load-relaxation properties. These findings help to quantify
106
the neural contribution to in vivo muscle tone, which is experienced clinically during
physical therapy and rehabilitation of patients with insults to their nervous system (i.e.
when stretching a spastic muscle of a patient with cerebral palsy, the therapist often
experiences a stiff muscle that resists manipulation) [18-21]. Further, pre-operative
injection of BoNT-A facilitates the intra-operative surgical manipulation of the muscle-
tendon unit by decreasing stiffness (Table 1) and the elastic component ‘A ‘of Fung’s
QLV (Table 2). Pre-surgical chemical denervation is a novel approach to modulating the
in vivo soft-tissue biomechanics of the muscle-tendon unit and may facilitate the
mobilization of scarred, retracted, shortened, and atrophied muscle-tendon units during
surgery.
Resting muscle tone is attributed to a neural reflex loop, in which afferent sensory
nerves detect the contractile state of the muscle and then send a signal to efferent motor
neurons, via a synapse in the spinal cord. These efferent motor neurons provide
stimulation or inhibition of the muscle, resulting in appropriate contraction or relaxation.
In addition to the structural elements (i.e. actin, myosin, titin) of the musculoskeletal
system that contribute to passive muscle-tendon unit properties, this reflex arc helps to
maintain a basal level of contractile tone. The reflex loop is modulated by central nervous
system input via the corticospinal and reticulospinal tracts, both of which provide
inhibitory modulation of this reflex. BoNT-A blocks the transmission of the efferent
nerve input to the skeletal muscle, and thus disrupts the reflex loop [33]. It is likely that
the BoNT-A influences elasticity (or QLV parameter ‘A’) by disrupting this neural reflex
loop, blocking neural input to the skeletal muscle, and reducing stiffness.

107
Based upon our clinical experience, the effects of a one-time dose of BoNT-A on
inhibition of active contractile force are reversed by 4-6 months [18]. Yet in animal
studies, modulation of the passive stiffness of the muscle-tendon unit, by a one-time dose
of BoNT-A, seem to reverse two weeks after injection [34]. Our data demonstrate that
BoNT-A significantly reduces supramaximal contractile force (Fig 4). Recently, BoNT-A
chemical denervation was employed in the perioperative setting, in an animal model, to
protect a surgically repaired tendon injury. In this study, the chemically denervated
muscles could not generate enough strength to produce suture rupture [27]. Similar
favorable outcomes were demonstrated in a clinical tendon repair study [35]. In the non-
compliant patient, who attempts excessive activity before healing is allowed to occur
following surgery, pre-surgical BoNT-A injection provides “bio-protection” or “chemo-
protection” of the repair site because the chemically denervated muscle cannot generate
the necessary force to exceed the suture fixation techniques used to secure the torn
muscle-tendon unit to the bone [27, 35].
In addition to the proposed “chemo-protection” or “bio-protection” mechanisms,
it is likely that repair tension was also influenced by the use of BoNT-A. The healing of a
muscle-tendon unit to bone is based on many factors; however, the role of repair tension
has recently been appreciated. In the clinically relevant rat rotator cuff animal model,
repair tension increased with time after injury [5]. The higher tensioned repairs
demonstrated impaired healing at the tendon-bone interface as assessed by biomechanical
testing, histology, and molecular assays [6].
Another rat rotator cuff animal study employed BoNT-A in combination with
cast-immobilization of the rodent limb in order to reduce repair tension, with the goal of

108
chemically protecting the surgical repair. In this study by Galatz et al., the reduced repair
tension coupled with a complete absence of mechanical stimulation during healing led to
impaired histological and biomechanical tendon-to-bone healing [29]. Hettrich et al. also
reported mixed biomechanical and histological results of tendon healing after rotator cuff
injury and repair in the rat rotator cuff animal model [36]. However, these studies focused
on tendon-to-bone healing and did not quantify the passive biomechanical properties of
the muscle-tendon unit. Both studies conclude that further investigation is required at
earlier and later time points to determine the efficacy and influence of chemodenervation
on tendon-to-bone healing [29, 36].
Based upon previous reports in the literature regarding the relationship between
repair tension and tendon-to-bone healing, some investigators have attempted to optimize
the mechanical loading of the muscle-tendon unit after surgery. These investigators
repaired rotator cuff tendons in the rodent model and then studied various rehabilitation
protocols after surgery that employed treadmill running and continuous passive motion
[37, 38]. One study demonstrated that healing was not impaired with motion as assessed
biomechanically and histologically; however, the passive range of joint motion might be
adversely affected [37]. The other study demonstrated increased scar formation with
excessive early motion, which adversely affected tendon healing [38]. Biologically, some
motion or tension at the repair sight is necessary to improve healing; however, repair
tensions that are too high result in impaired healing [6, 29, 37-40]. Ideally, the BoNT-A
dose would be optimized for both pharmaco-kinetics and pharmaco-dynamics in the pre-
surgery setting to correspond with the patient’s rehabilitation protocol after tendon repair
surgery. In this way, pre-surgical injection of BoNT-A has the potential to allow for the
109
pharmacological control of repair site tension throughout the healing process, further
improving the mechano-biology of healing during rehabilitation following surgery [6, 29,
37-40].
Stress and strain is typically used for Fung’s QLV analysis of biological tissue,
such as tendon, ligament, or muscle. However, QLV parameters in the present study were
determined based upon loads and displacements because cross-sectional area and length
of the muscle-tendon unit are not known during in vivo experimentation. This method has
the limitation of being highly sensitive to differences in length and size of the samples
used. In the animal model system used, there was enough consistency between the
experimental subjects to detect significant differences. Additionally, other investigators
have successfully employed the method of parameterization of load-displacement data
using an in vivo rat rotator cuff animal model system [5]. It is possible that after 1 week
of BoNT-A injection, the muscles could have undergone an adaptive response, such as
atrophy, which might explain the differences in passive properties observed. A limitation
of this study is that muscle volume or physiological cross-sectional area (PCSA) was not
measured after experimentation to ensure that these structural changes did not occur.
Galatz et al. reported minimal structural changes at 14 days post-injection in the muscle’s
architecture, as determined by histological examination of rat supraspinatus injected with
9 units/kg of BoNT-A, the same dose used in our present study. However, Galatz et al.
did report some structural changes during their analysis [29]. Further, Hettrich et al.
reported a significant reduction in rat supraspinatus weight at 4 and 8 weeks after
injection [36]. Analysis of stress-strain data, as opposed to load-relaxation data, would
account for these potential differences in muscle structure after BoNT-A injection.
110
However, at 1 week after BoNT-A injection, we expect minimal atrophic changes to the
muscle’s structure.
A limitation of the present study is that only a single dose-volume combination of
BoNT-A was examined. Future studies are needed to elucidate the time-course of BoNT-
A’s modulation on the passive, in vivo, biomechanical properties of the muscle-tendon
unit. In addition, studying the effects of BoNT-A over a longer period of time would
determine if the stiffness and QLV parameters return to baseline. However, it is possible
that the passive properties might not return to the pre-injection state. A report in the
literature concluded that repeated BoNT-A injections may result in persistent structural
changes in skeletal muscle [41]. However, experience with orthopaedic surgical
applications has demonstrated that BoNT-A injections are both safe and reversible [18,
21, 42].
The present study also has the limitation of being performed in an animal model.
Despite the similarities between the rat and human shoulder, anatomical, structural (i.e.
muscle fiber composition, muscle size, muscle volume, etc.), and functional differences
(i.e. quadra-pedal versus bi-pedal) exist between the rodent model and humans. Despite
the advantages of in vivo testing in the rat model, the present experimental apparatus
does not allow for replication of the exact joint biomechanics of normal muscle-tendon-
bone action because the rotator cuff muscle-tendon unit was configured linearly with the
force-transducer to ensure accurate recording. A final limitation was that the in vivo
biomechanical testing was performed under general anesthesia, which may influence
resting muscle tone and function. However, identical muscle-tendon unit testing was
111
performed for both experimental groups, BoNT-A injected and saline injected, under the
same anesthetic conditions, with the same anesthetic agent and dose.
Recently, there has been an increased interest in understanding the nervous
system’s role during the pathogenesis and healing of rotator cuff tears [43-46]. Since the
shoulder is a dynamic joint with a complex range of motion, it requires the simultaneous
activation and coordination of many nerves, muscles, tendons, and bones to perform a
movement. Our data demonstrate that even at “rest,” the nervous system has a significant
role in passive skeletal muscle tone, which ultimately influences the motion and function
of the joint. The findings of the present study demonstrate that the nervous system
influences elasticity of the muscle-tendon unit, as QLV model parameter ‘A’ is
significantly changed after BoNT-A injection. These findings have implications for
mathematical modeling of the musculoskeletal system. Based on our QLV analysis, it is
likely that varying elasticity of the tissue in a model system would simulate neural
influences. More specifically, our data demonstrate that linear scaling of the elastic tissue
response would be most appropriate for investigation of neuronal influences using
computational techniques. However, these findings should be interpreted with caution, as
further investigation using computational analysis techniques and verification with in
vivo experimentation is necessary to validate this conclusion.
In conclusion, neural tone significantly contributes to muscle-tendon unit passive
biomechanical properties, and pre-surgical treatment with BoNT-A may improve the
rehabilitation of muscle by altering the passive elastic properties. Accordingly,
pharmacological modulation of skeletal muscle stiffness with BoNT-A increases
flexibility and may improve function. Chemical denervation with BoNT-A may also
112
improve the manipulation of stiff and difficult to mobilize muscles during surgical
procedures. Besides the rotator cuff, these findings have implications for the operative
repair and rehabilitation of many muscle-tendon units, such as biceps tendon, triceps
tendon, quadriceps tendon, Achilles tendon, and hand flexor tendons.
ACKNOWLEDGEMENTS
We would like to thank Mrs. Eileen Martin, Mr. Patrick Haubruck, and Dr.
Michael F. Callahan for their support in the planning and execution of the experiments.
No external financial support or potential conflicts were identified related to the subject
of this study. This project is taken in part from a dissertation submitted to the
Neuroscience Program, Wake Forest University Graduate School of Arts and Sciences, in
partial fulfillment of the requirements for the degree of Doctor of Philosophy.
113
REFERENCES
1. Aurora A, McCarron J, Iannotti JP, Derwin K. Commercially available
extracellular matrix materials for rotator cuff repairs: state of the art and future trends. J
Shoulder Elbow Surg. Sep-Oct 2007;16(5 Suppl):S171-178.
2. Safran O, Derwin KA, Powell K, Iannotti JP. Changes in rotator cuff muscle
volume, fat content, and passive mechanics after chronic detachment in a canine model. J
Bone Joint Surg Am. Dec 2005;87(12):2662-2670.
3. Halder AM, O'Driscoll SW, Heers G, Mura N, Zobitz ME, An KN, Kreusch-
Brinker R. Biomechanical comparison of effects of supraspinatus tendon detachments,
tendon defects, and muscle retractions. J Bone Joint Surg Am. May 2002;84-A(5):780-
785.
4. Hansen ML, Otis JC, Johnson JS, Cordasco FA, Craig EV, Warren RF.
Biomechanics of massive rotator cuff tears: implications for treatment. J Bone Joint Surg
Am. Feb 2008;90(2):316-325.
5. Gimbel JA, Mehta S, Van Kleunen JP, Williams GR, Soslowsky LJ. The tension
required at repair to reappose the supraspinatus tendon to bone rapidly increases after
injury. Clin Orthop Relat Res. Sep 2004(426):258-265.
6. Gimbel JA, Van Kleunen JP, Lake SP, Williams GR, Soslowsky LJ. The role of
repair tension on tendon to bone healing in an animal model of chronic rotator cuff tears.
J Biomech. 2007;40(3):561-568.
7. Gerber C, Meyer DC, Schneeberger AG, Hoppeler H, von Rechenberg B. Effect
of tendon release and delayed repair on the structure of the muscles of the rotator cuff: an
experimental study in sheep. J Bone Joint Surg Am. Sep 2004;86-A(9):1973-1982.

114
8. Coleman SH, Fealy S, Ehteshami JR, MacGillivray JD, Altchek DW, Warren RF,
Turner AS. Chronic rotator cuff injury and repair model in sheep. J Bone Joint Surg Am.
Dec 2003;85-A(12):2391-2402.
9. Davidson PA, Rivenburgh DW. Rotator cuff repair tension as a determinant of
functional outcome. J Shoulder Elbow Surg. Nov-Dec 2000;9(6):502-506.
10. Ward SR, Sarver JJ, Eng CM, Kwan A, Wurgler-Hauri CC, Perry SM, Williams
Jr GR, Soslowsky LJ, Lieber RL. Plasticity of Muscle Architecture After Supraspinatus
Tears. J Orthop Sports Phys Ther. Aug 6 2010.
11. Meyer DC, Hoppeler H, von Rechenberg B, Gerber C. A pathomechanical
concept explains muscle loss and fatty muscular changes following surgical tendon
release. J Orthop Res. Sep 2004;22(5):1004-1007.
12. Barton ER, Gimbel JA, Williams GR, Soslowsky LJ. Rat supraspinatus muscle
atrophy after tendon detachment. J Orthop Res. Mar 2005;23(2):259-265.
13. Meyer DC, Pirkl C, Pfirrmann CW, Zanetti M, Gerber C. Asymmetric atrophy of
the supraspinatus muscle following tendon tear. J Orthop Res. Mar 2005;23(2):254-258.
14. Jozsa L, Kannus P, Thoring J, Reffy A, Jarvinen M, Kvist M. The effect of
tenotomy and immobilisation on intramuscular connective tissue. A morphometric and
microscopic study in rat calf muscles. J Bone Joint Surg Br. Mar 1990;72(2):293-297.
15. Oh JH, Kim SH, Ji HM, Jo KH, Bin SW, Gong HS. Prognostic factors affecting
anatomic outcome of rotator cuff repair and correlation with functional outcome.
Arthroscopy. Jan 2009;25(1):30-39.
16. Oh LS, Wolf BR, Hall MP, Levy BA, Marx RG. Indications for rotator cuff
repair: a systematic review. Clin Orthop Relat Res. Feb 2007;455:52-63.
115
17. Gajdosik RL. Passive extensibility of skeletal muscle: review of the literature with
clinical implications. Clin Biomech (Bristol, Avon). Feb 2001;16(2):87-101.
18. Seyler TM, Smith BP, Marker DR, Ma J, Shen J, Smith TL, Mont MA, Kolaski
K, Koman LA. Botulinum neurotoxin as a therapeutic modality in orthopaedic surgery:
more than twenty years of experience. J Bone Joint Surg Am. Nov 2008;90 Suppl 4:133-
145.
19. Ramachandran M, Eastwood DM. Botulinum toxin and its orthopaedic
applications. J Bone Joint Surg Br. Aug 2006;88(8):981-987.
20. Brashear A, Gordon MF, Elovic E, Kassicieh VD, Marciniak C, Do M, Lee CH,
Jenkins S, Turkel C. Intramuscular injection of botulinum toxin for the treatment of wrist
and finger spasticity after a stroke. N Engl J Med. Aug 8 2002;347(6):395-400.
21. Koman LA, Mooney JF, 3rd, Smith BP, Walker F, Leon JM. Botulinum toxin
type A neuromuscular blockade in the treatment of lower extremity spasticity in cerebral
palsy: a randomized, double-blind, placebo-controlled trial. BOTOX Study Group. J
Pediatr Orthop. Jan-Feb 2000;20(1):108-115.
22. Longino D, Butterfield TA, Herzog W. Frequency and length-dependent effects
of Botulinum toxin-induced muscle weakness. J Biomech. Mar 2005;38(3):609-613.
23. Zajac FE. Muscle and tendon: properties, models, scaling, and application to
biomechanics and motor control. Crit Rev Biomed Eng. 1989;17(4):359-411.
24. Soslowsky LJ, Carpenter JE, DeBano CM, Banerji I, Moalli MR. Development
and use of an animal model for investigations on rotator cuff disease. J Shoulder Elbow
Surg. Sep-Oct 1996;5(5):383-392.
116
25. Soslowsky LJ, Thomopoulos S, Tun S, Flanagan CL, Keefer CC, Mostow J,
Carpenter JE. Neer award 1999 Overuse activity injures the supraspinatus tendon in an
animal model: A histologic and biomechanical study. Journal of Shoulder and Elbow
Surgery. 2000/4//;9(2):79-84.
26. Stone AV, Ma J, Whitlock PW, Koman LA, Smith TL, Smith BP, Callahan MF.
Effects of Botox and Neuronox on muscle force generation in mice. J Orthop Res. Dec
2007;25(12):1658-1664.
27. Ma J, Shen J, Smith BP, Ritting A, Smith TL, Koman LA. Bioprotection of
tendon repair: adjunctive use of botulinum toxin A in Achilles tendon repair in the rat. J
Bone Joint Surg Am. Oct 2007;89(10):2241-2249.
28. Shen J, Ma J, Elsaidi GA, Lee CA, Smith TL, Tan KH, Koman LA, Smith BP.
Gene expression of myogenic regulatory factors following intramuscular injection of
botulinum A toxin in juvenile rats. Neurosci Lett. Jun 24 2005;381(3):207-210.
29. Galatz LM, Charlton N, Das R, Kim HM, Havlioglu N, Thomopoulos S.
Complete removal of load is detrimental to rotator cuff healing. J Shoulder Elbow Surg.
Sep-Oct 2009;18(5):669-675.
30. Chen CM, Stott NS, Smith HK. Effects of botulinum toxin A injection and
exercise on the growth of juvenile rat gastrocnemius muscle. J Appl Physiol. Oct
2002;93(4):1437-1447.
31. Fung YC. Stress-strain-history relations of soft tissues in simple elongation. In:
Fung YC, Perrone N., Anliker M, ed. Biomechanics: Its Foundations and Objectives. San
Diego: Prentice-Hall; 1972:181-208.

117
32. Nigul I, Nigul U. On algorithms of evaluation of Fung's relaxation function
parameters. J Biomech. 1987;20(4):343-352.
33. Koman LA, Smith, B.P., and Goodman A. Botulinum Toxin Type A in the
Management of Cerebral Palsy. Winston-Salem, NC 27157: Wake Forest University
Press--Scientific Division; 2002.
34. Mannava S, Callahan MF, Trach SM, Wiggins WF, Smith BP, Koman LA, Smith
TL, Tuohy CJ. Chemical denervation with botulinum neurotoxin a improves the surgical
manipulation of the muscle-tendon unit: an experimental study in an animal model. J
Hand Surg Am. Feb 2011;36(2):222-231.
35. De Aguiar G, Chait LA, Schultz D, Bleloch S, Theron A, Snijman CN, Ching V.
Chemoprotection of flexor tendon repairs using botulinum toxin. Plast Reconstr Surg. Jul
2009;124(1):201-209.
36. Hettrich CM, Rodeo SA, Hannafin JA, Ehteshami J, Shubin Stein BE. The effect
of muscle paralysis using Botox on the healing of tendon to bone in a rat model. Journal
of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et al.]. Dec
29 2010.
37. Peltz CD, Dourte LM, Kuntz AF, Sarver JJ, Kim SY, Williams GR, Soslowsky
LJ. The effect of postoperative passive motion on rotator cuff healing in a rat model. J
Bone Joint Surg Am. Oct 2009;91(10):2421-2429.
38. Peltz CD, Sarver JJ, Dourte LM, Wurgler-Hauri CC, Williams GR, Soslowsky LJ.
Exercise following a short immobilization period is detrimental to tendon properties and
joint mechanics in a rat rotator cuff injury model. J Orthop Res. Jul 2010;28(7):841-845.

118
39. Bring DK, Reno C, Renstrom P, Salo P, Hart DA, Ackermann PW. Joint
immobilization reduces the expression of sensory neuropeptide receptors and impairs
healing after tendon rupture in a rat model. J Orthop Res. Feb 2009;27(2):274-280.
40. Rodeo SA, Delos D, Weber A, Ju X, Cunningham ME, Fortier L, Maher S.
What's new in orthopaedic research. J Bone Joint Surg Am. Oct 2010;92(14):2491-2501.
41. Fortuna R, Aurelio Vaz M, Rehan Youssef A, Longino D, Herzog W. Changes in
contractile properties of muscles receiving repeat injections of botulinum toxin (Botox). J
Biomech. Sep 7.
42. Lowe K, Novak I, Cusick A. Repeat injection of botulinum toxin A is safe and
effective for upper limb movement and function in children with cerebral palsy. Dev Med
Child Neurol. Nov 2007;49(11):823-829.
43. Gupta R, Lee TQ. Contributions of the different rabbit models to our
understanding of rotator cuff pathology. J Shoulder Elbow Surg. Sep-Oct 2007;16(5
Suppl):S149-157.
44. Mallon WJ, Wilson RJ, Basamania CJ. The association of suprascapular
neuropathy with massive rotator cuff tears: a preliminary report. J Shoulder Elbow Surg.
Jul-Aug 2006;15(4):395-398.
45. Kelly BT, Williams RJ, Cordasco FA, Backus SI, Otis JC, Weiland DE, Altchek
DW, Craig EV, Wickiewicz TL, Warren RF. Differential patterns of muscle activation in
patients with symptomatic and asymptomatic rotator cuff tears. J Shoulder Elbow Surg.
Mar-Apr 2005;14(2):165-171.

119
46. Rowshan K, Hadley S, Pham K, Caiozzo V, Lee TQ, Gupta R. Development of
fatty atrophy after neurologic and rotator cuff injuries in an animal model of rotator cuff
pathology. J Bone Joint Surg Am. Oct 6 2010;92(13):2270-2278.
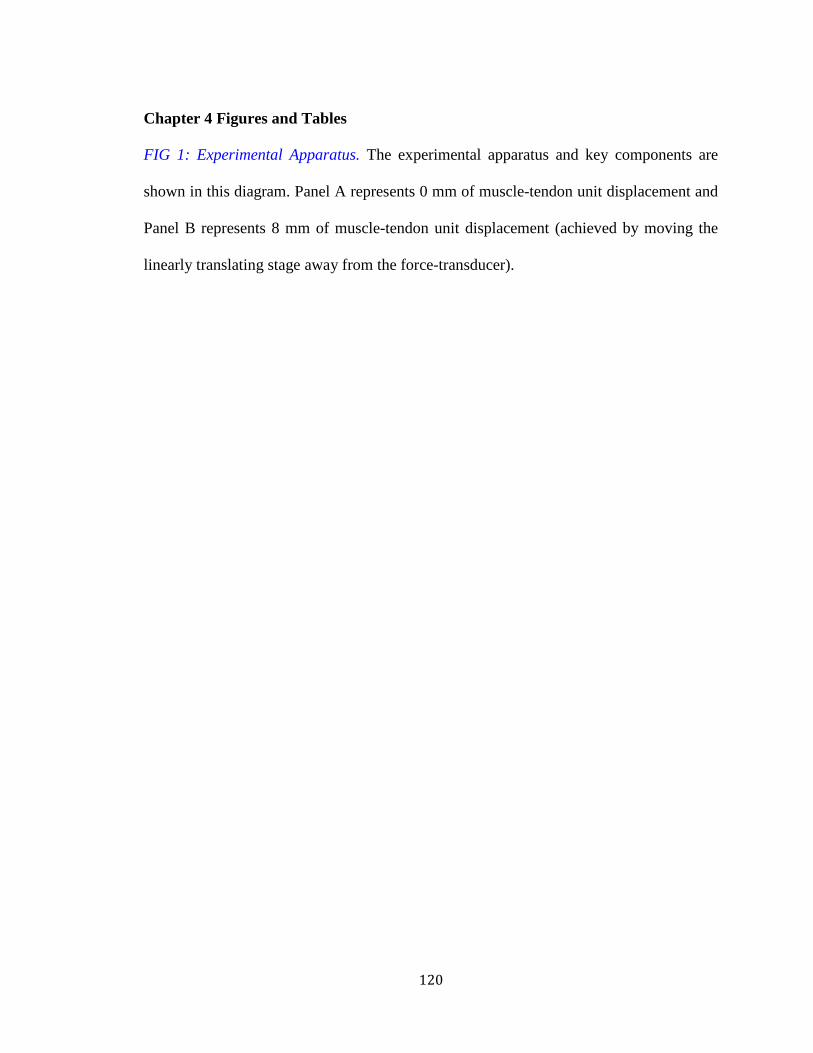
120
Chapter 4 Figures and Tables
FIG 1: Experimental Apparatus. The experimental apparatus and key components are
shown in this diagram. Panel A represents 0 mm of muscle-tendon unit displacement and
Panel B represents 8 mm of muscle-tendon unit displacement (achieved by moving the
linearly translating stage away from the force-transducer).

121
Chapter 4, Fig. 1

122
FIG 2: The Effect of Varying QLV Model Parameters on a Sample Time History of Data
for a 4mm Displacement of the Rat Supraspintus Muscle-Tendon Unit. Panel A
demonstrates how doubling parameters ‘A’ and ‘B’ influence the passive tension versus
time sample data. Panel B demonstrates how doubling parameters ‘C,’ ‘τ1,’ and ‘τ 2,’
influence the passive tension versus time sample data.
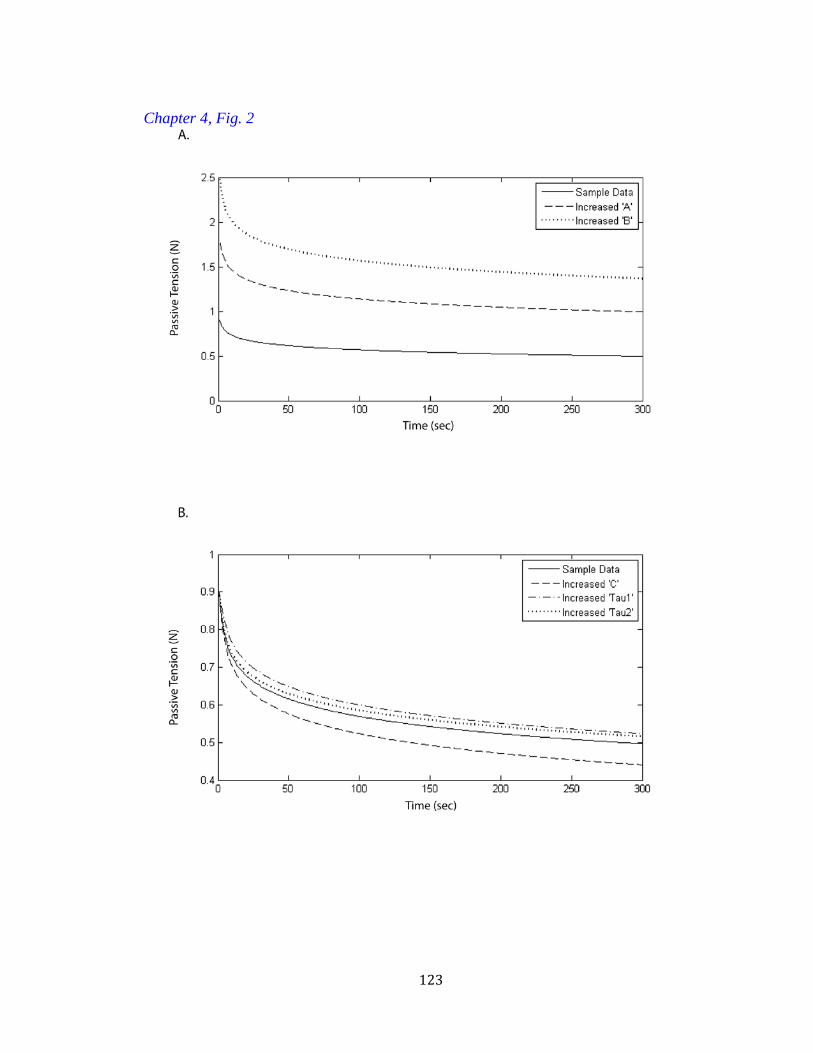
123
Chapter 4, Fig. 2

124
FIG 3: Sample Time Histories of BoNT-A versus Saline Injected Supraspinatus Muscle-
Tendon Units after Various Displacements. The BoNT-A demonstrated lower passive
tension when compared to saline-injected controls throughout the time history.
Goodness-of-fit of the time-histories to the QLV model were assessed by nonlinear least-
squares regression and reported in the results.
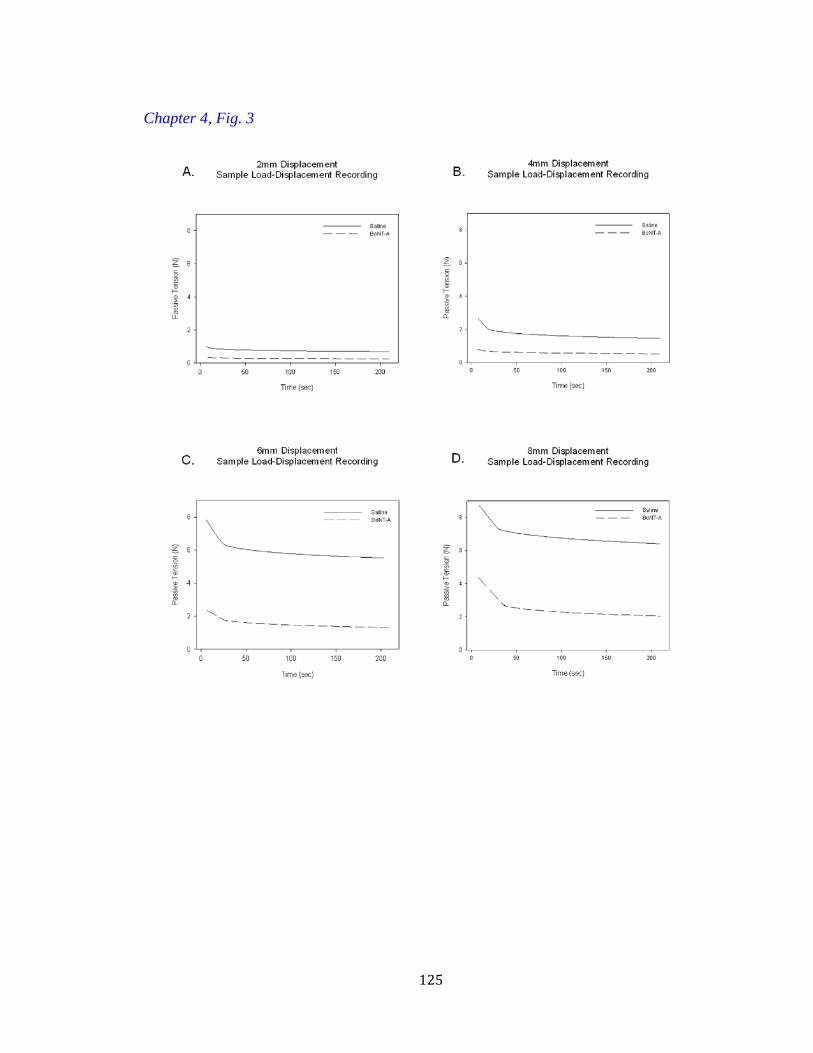
125
Chapter 4, Fig. 3

126
FIG 4: The Effect of BoNT-A on Rat Supraspinatus Muscle Contraction. There is a
significant reduction in the maximal tetanic muscle contractile force at all frequencies of
stimulation studied at one week after injection of BoNT-A when compared to saline
injected controls (p=0.001). Data are presented as the mean ± standard error of the mean.
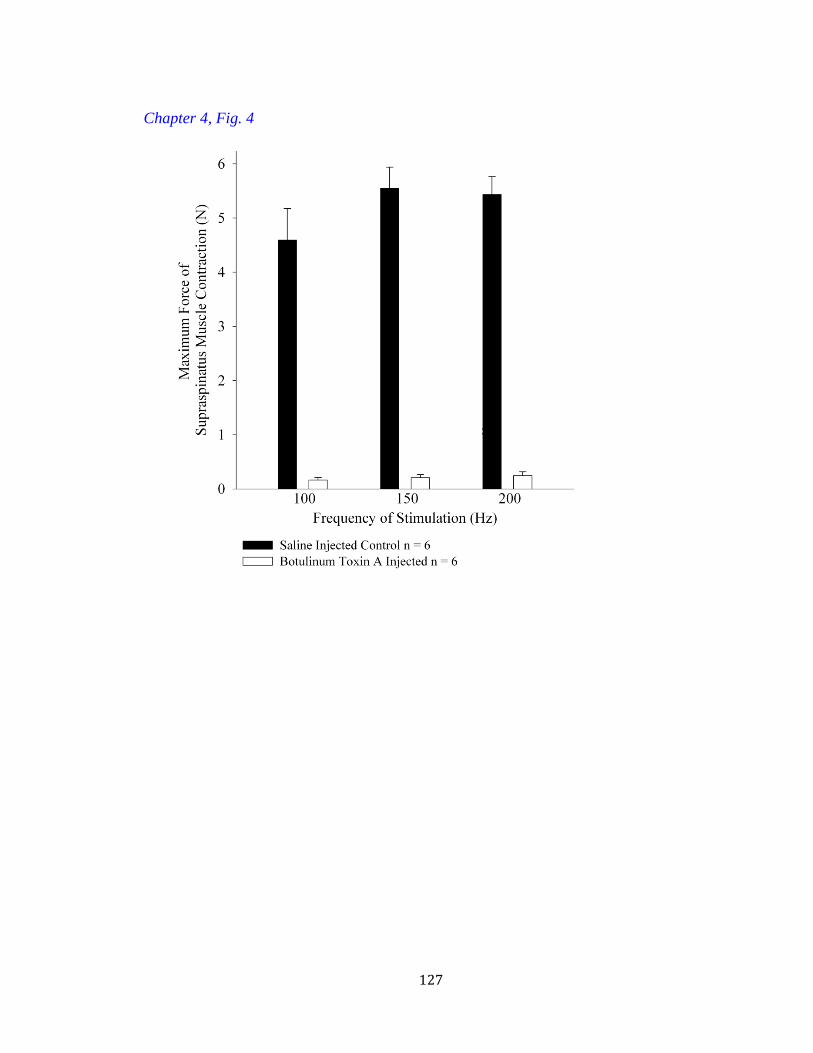
127
Chapter 4, Fig. 4
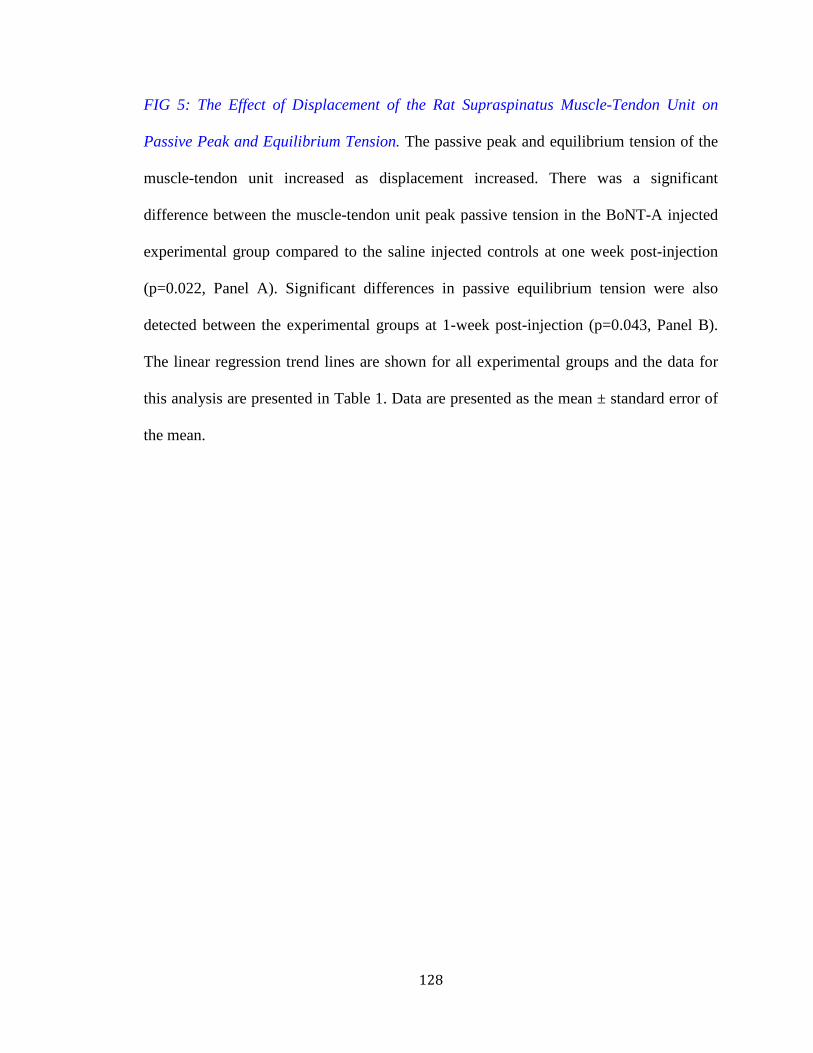
128
FIG 5: The Effect of Displacement of the Rat Supraspinatus Muscle-Tendon Unit on
Passive Peak and Equilibrium Tension. The passive peak and equilibrium tension of the
muscle-tendon unit increased as displacement increased. There was a significant
difference between the muscle-tendon unit peak passive tension in the BoNT-A injected
experimental group compared to the saline injected controls at one week post-injection
(p=0.022, Panel A). Significant differences in passive equilibrium tension were also
detected between the experimental groups at 1-week post-injection (p=0.043, Panel B).
The linear regression trend lines are shown for all experimental groups and the data for
this analysis are presented in Table 1. Data are presented as the mean ± standard error of
the mean.
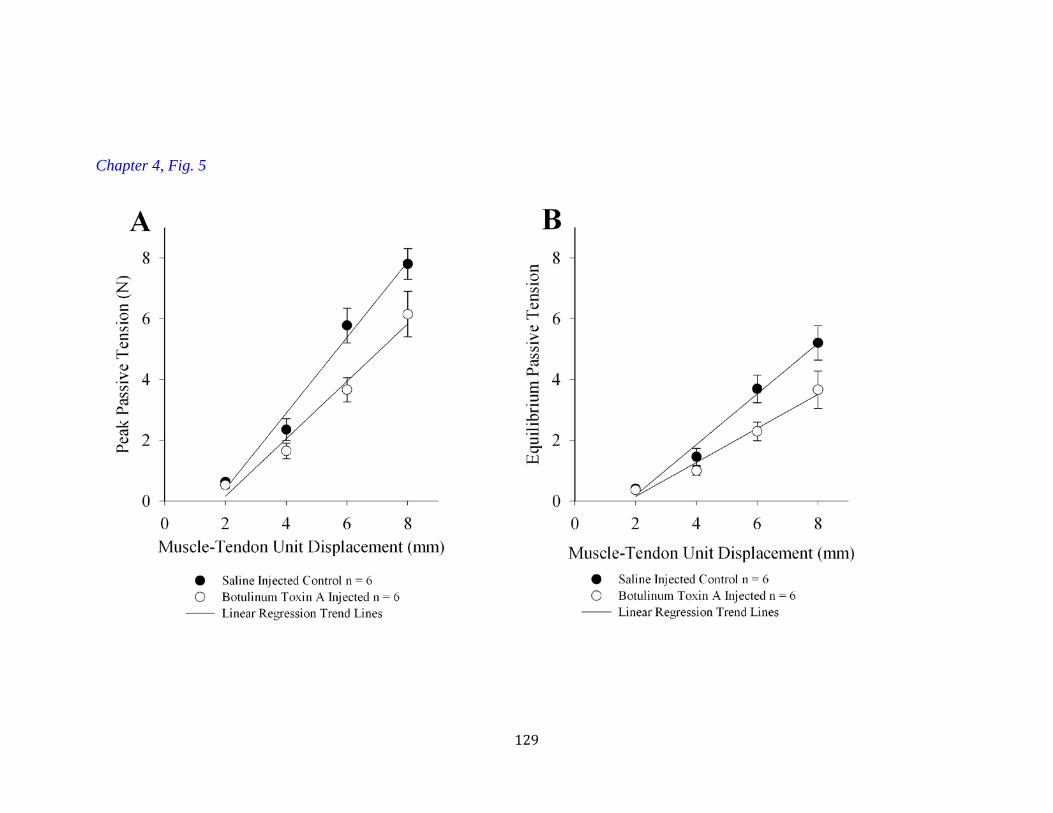
129
Chapter 4, Fig. 5

130
Chapter 4, Table 1
Table 1. Linear Regression Analysis for rat supraspinatus muscle tendon unit before and after botulinum neurotoxin A injection Displacement versus Peak Tension (Figure 2A)
Subject n
Slope Stiffness (N/mm) R2 P
Average Control 6 0.98 ± 0.074 0.952 0.005
Average
Botulinum Toxin A
6 0.82 ± 0.146 * 0.934 0.007
Displacement versus Equilibrium Tension (Figure 2B)
Subject
Slope Stiffness (N/mm) R2 P
Average Control 6 0.651 ±
0.0779 0.947 0.005
Average
Botulinum Toxin A
6 0.503 ± 0.0751 0.94 0.006
Average slope data expressed as MEAN ± SEM * T-test reveals significant difference (p=0.040)
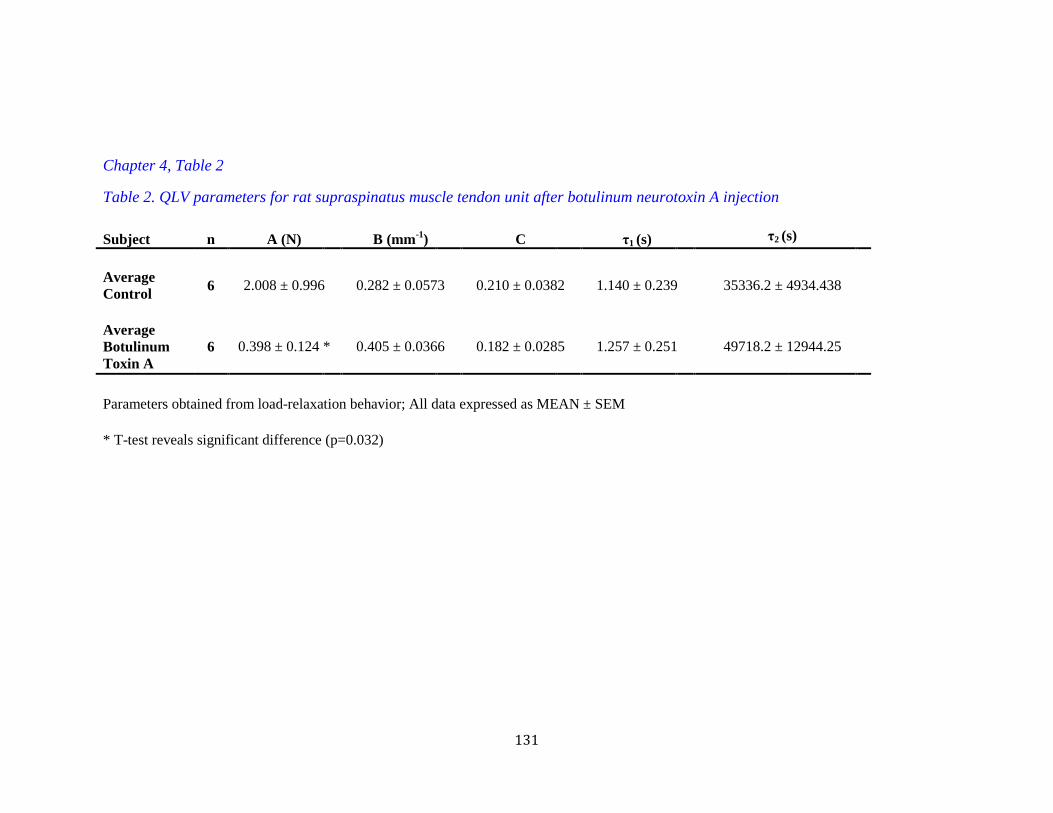
131
Chapter 4, Table 2
Table 2. QLV parameters for rat supraspinatus muscle tendon unit after botulinum neurotoxin A injection
Subject n A (N) B (mm-1) C τ1 (s) τ2 (s) Average Control 6 2.008 ± 0.996 0.282 ± 0.0573 0.210 ± 0.0382 1.140 ± 0.239 35336.2 ± 4934.438
Average Botulinum Toxin A
6 0.398 ± 0.124 * 0.405 ± 0.0366 0.182 ± 0.0285 1.257 ± 0.251 49718.2 ± 12944.25
Parameters obtained from load-relaxation behavior; All data expressed as MEAN ± SEM * T-test reveals significant difference (p=0.032)
132
CHAPTER 5
THE SCIENCE OF ROTATOR CUFF REPAIRS: TRANSLATING
BASIC SCIENCE INTO CLINICAL RECOMMENDATIONS
Sandeep Mannava, Christopher J. Tuohy, Thorsten M. Seyler, Johannes F. Plate,
L. Andrew Koman, Patrick W. Whitlock, Thomas L. Smith, Katherine R. Saul
S. Mannava performed the experiments, prepared the manuscript that was presented at
the 2011 AAOS Annual Meeting in San Diego, CA, and served as corresponding author.
T.L. Smith acted in an advisory and editorial capacity. K.R. Saul served in an advisory
role and helped complete the simulation analysis.
133
ABSTRACT
Introduction: For chronic, full-thickness, rotator cuff tears, repair surgery can be
technically challenging due to large gap distances and increased stiffness of the muscle-
tendon unit. In contrast, acute rotator cuff tears are associated with lower repair tensions,
less fibro-fatty infiltration of the muscle, and better functional outcomes. This study
demonstrates how animal models can be used to understand rotator cuff muscle function
in the acute and chronic tear setting and how these results can be translated into clinical
recommendations using computational modeling.
Methods: In vivo muscle function, electromyography (EMG), and passive muscle-tendon
unit properties were studied before and after supraspinatus tenotomy in a rodent rotator
cuff injury model (acute vs chronic). Then, a series of simulation experiments were
conducted using a validated computational human musculoskeletal shoulder model to
assess both passive and active tension of rotator cuff repairs based on surgical
positioning.
Results: In vivo muscle function was impaired at the tensions required to repair a
chronically torn rotator cuff (approximately a 50% reduction from maximal twitch
amplitude, p<0.05). Dysfunction in the chronic tear setting was detectable via EMG
(p<0.05). At adducted postures, computational data from simulated surgical repair of
chronically torn rotator cuff indicated that passive repair tension markedly exceeds the
pullout strength of suture and anchor techniques typically used in these surgeries. Further,
simulation analysis indicated there was approximately a 50% reduction in moment
generating capacity after repair of chronically torn rotator cuff.

134
Conclusions: The rat data suggest a direct experimental connection between high repair
tensions—chronic tear setting—and impaired contractile force. Simulation analysis
confirmed that functional outcomes are compromised when excessively retracted rotator
cuff muscle-tendon units are repaired in a single-stage procedure.
Clinical Relevance: Functional outcomes following surgical repair of rotator cuffs may
be improved by earlier intervention because the acute tear setting requires lower surgical
repair tension and is associated with fewer neuromuscular changes.
135
INTRODUCTION
Rotator cuff tears are a common cause of upper-extremity disability, particularly
in elderly patients over 60 years of age [55, 71, 72]. For chronic, full-thickness, rotator
cuff tears, repair surgery can be technically challenging due to large gap distances and
increased stiffness of the muscle-tendon unit. In contrast, acute rotator cuff tears are
associated with lower repair tensions, less fibro-fatty infiltration of the muscle, and better
functional outcomes. This study demonstrates how animal models can be used to
understand rotator cuff muscle function in the acute and chronic tear setting and how
these results can be translated into clinical recommendations using computational
modeling.
ROTATOR CUFF TEARS: A CLINICAL PROBLEM
Rotator cuff tears are a common cause of upper extremity pain and disability that
results in nearly 4.5 million physician visits [55] and more than 75,000 operative repairs
annually [68], in the United States. Approximately 20% of all adults have a torn rotator
cuff [72] and the distribution of tears is skewed towards the older patient population [55,
71, 72]. In one study of shoulder magnetic resonance imaging, approximately 4% of
patient’s under the age of 40 were diagnosed with a rotator cuff tear; this number rose to
approximately 54% of patients over the age of 60 [62].
Disability from rotator cuff pathology affects approximately 20% of older adults,
who struggle to maintain their independence because of reduced upper-limb function
secondary to pain and weakness [1, 56]. As the average age of the United States’
population increases and older patients live a more active lifestyle, the number of rotator
cuff repair surgeries performed annually continues to rise [54, 55]. Despite many

136
technological advances, recent studies have reported variable clinical operative results,
with some studies reporting a high rotator cuff repair failure rate [21, 24] and others
reporting more favorable outcomes [52].
The rotator cuff functions as a dynamic stabilizer, acting to optimize the position
of the humeral head on the articular surface of glenoid during motion and to provide
initiation of arm forward flexion and abduction. Rotator cuff failure can lead to abnormal
and unbalanced gleno-humeral joint forces, which can ultimately lead to pain during
movement of the affected limb [19, 37, 48, 69]. Current treatment recommendations for
rotator cuff pathology often delay surgical intervention until conservative management
options are exhausted [7, 55]. Delayed surgical repair may result in disease progression
and changes to the muscle-tendon unit [2, 16, 30, 31, 39, 51, 60], which some consider
irreversible with current single-staged repair surgery [7, 49, 59, 67].
Since the rotator cuff muscles require complex neuro-physiological coordination
to perform their function, many research efforts have focused on studying rotator cuff
pathology using animal models. These studies have employed rat [28, 29], rabbit [49, 58,
59, 67], dog [15], sheep [7, 26], and non-human primates [63] to study the natural history
of the disease process and test innovative operative solutions. However, findings in
animal models can be difficult to interpret and translate into clinical practice for patient
benefit. The present study will demonstrate how animal studies are used to gain insights
regarding rotator cuff pathologies. In particular, we will present data related to muscle
function after acute and chronic rotator cuff tears in a rat rotator cuff animal model. We
then performed a simulation analysis using a computational model of human upper-
extremity motion in order to “scale” the small animal findings to the human condition.

137
This research paradigm of using advanced computational modeling to help interpret
animal studies will improve the pace of basic-science innovation. Further, this process
may help facilitate the translation of research findings into clinical solutions that improve
the care of patients, resulting in an expedited return to work or recreation following
rotator cuff surgery.
THE ROTATOR CUFF MUSCLE UNDERGOES CHANGES AFTER TENDON
INJURY
Numerous animal studies have examined the changes that occur in the skeletal
muscle associated with the torn rotator cuff tendon. Previous experimental investigations
have established the rat shoulder model as suitable for the study of human rotator cuff
pathology because of upper-extremity anatomy similarities between the two species (Fig.
1) [64, 66]. Barton et. al reported that the rat supraspinatus undergoes a rapid dis-use
atrophy, with muscle fiber type switching to fast-muscle fibers, decreased muscle mass,
and increased inter-fasicular fibrosis [2]. Findings from our laboratory in the rat model
demonstrate similar changes (Fig. 2) [45]. Interestingly, after isolated rotator cuff
tenotomy, the rat supraspinatus muscle does not undergo the anticipated fibro-fatty
infiltration of the muscle-belly, which has been observed in some instances of clinical
rotator cuff tears [22, 32, 40].
Studies that utilize the rabbit animal model to study muscle structure after
tenotomy have demonstrated similar atrophic changes described in the rat literature, with
the added benefit of recapitulating the fatty degeneration seen clinically [49, 58, 59, 67].
Utilizing the rabbit rotator cuff model, various authors suggested that rotator cuff tendon
tears have neuromuscular implications [38, 57]. In particular, the fatty infiltration that is
138
seen after rotator cuff tears may result from a nerve-injury component [33, 57] or a more
complex neuromuscular connectivity dysfunction [38]. These basic science studies are
consistent with recent case series that demonstrated electromyographic (EMG)
dysfunction after rotator cuff tears, which were reversible upon rotator cuff repair. These
studies concluded that “reducing” the atrophied and retracted rotator cuffs during repair
surgery resulted in decreased tension placed upon the suprascapular nerve as it coursed
through the suprascapular or spinoglenoid notch [9, 43]. Similarly, our group recently
reported EMG changes in compound motor action potential amplitude in chronically
injured rat rotator cuffs, directly relating electrophysiological rotator cuff dysfunction to
time from tendon injury (Fig. 3) [45]. These studies are among the first published reports
that relate rotator cuff tendon tears to a complex neuromuscular system, requiring
activation and coordination of many nerves and muscles in concert in order to produce
purposeful upper-extremity movement.
Skeletal muscle changes following rotator cuff tears have also been described in
larger animal model systems, such as sheep [7, 26] and dog [60]. These studies confirmed
that the muscle-tendon unit changes after rotator cuff tears. In particular, the rotator cuff
muscle atrophies, resulting in less mass and higher fat content [7, 26, 60].
IN VIVO BIOMECHANICS OF ROTATOR CUFF REPAIR SURGERY
Numerous animal studies have studied the natural history of rotator cuff injuries.
In particular, these studies quantified the passive tension required to “reduce” the injured
tendon back to its humeral insertion [26, 28, 29, 60]. The muscle-tendon unit structural
changes described previously [2, 7, 26, 38, 57, 60] result in a stiff an retracted rotator cuff
that is difficult to manipulate during surgery. In the rat rotator cuff animal model, Gimbel
139
et al. reported that the repair tension required to re-appose the supraspinatus tendon to the
humeral head rose rapidly and progressively from the time of injury [28]. Further, they
demonstrated that higher repair tensions were associated with a reduced quality of
tendon-to-bone healing, as demonstrated biomechanically [29]. Similar changes to the
passive biomechanics of the muscle-tendon unit were demonstrated in the canine model
[60] and sheep model [2, 26]. These studies reported that passive stiffness of the rotator
cuff was increased in the chronically torn setting, presumably because of the progressive
changes in the skeletal muscle and rotator cuff tendon structure [7, 26, 60]. A cadaveric
study performed by Halder et al. supports the animal studies and predicts that retraction
following rotator cuff tears contributes to decreased shoulder function, particularly
decreased torque and strength [34]. A clinical study by Davidson and Rivenburgh
measured intraoperative rotator cuff repair tensions in 67 consecutive patients and
correlated these tensions to clinical outcomes, as determined by strength measurements
and validated clinical metrics (Constant Score, American Shoulder and Elbow Surgeons’
functional criteria, and visual analog scale score). The study concluded that high repair
tensions were correlated with worse subjective and objective outcome measures [10].
Recently, our group published two reports which explored a novel mechanism by
which surgeons can chemically denervate a muscle-tendon unit pre-operatively in order
to improve the manipulation of the muscle-tendon unit during surgery [44, 46]. Our
initial animal study was performed in a mouse gastrocnemius model and demonstrated
that the stiffness of the muscle-tendon unit can be reduced by approximately 30% one-
week following an intramuscular botulinum neurotoxin A injection [44]. In a follow-up
report using the rat rotator cuff model, we demonstrated that injection of botulinum
140
neurotoxin A could pharmacologically modulate and reduce the elasticity of the in vivo
viscoelastic muscle-tendon unit. Based upon our animal data, the nervous system
contributes to the in vivo passive biomechanical properties of repair tension experienced
during rotator cuff repair [46]. Treatment of the rotator cuff with botulinum neurotoxin A
prior to surgery, may improve the surgical manipulation of the stiff and retracted tendon
[44, 46], with the additional benefit of “bioprotecting” the tendon-to-bone repair. By
temporarily and reversibly weakening the muscle, the active contractile force cannot
generate enough force to cause rupture of the repair site [42]. Recent reports in the rat
rotator cuff model, in which “bioprotection” of the repair site was employed,
demonstrated either equivocal or reduced healing biomechanics at the tendon-to-bone
junction [25, 35]. However, further studies are needed to investigate the clinical benefit
of botulinum neurotoxin A modulation of biomechanical stiffness and the potential for
“bioprotection” of the repair site. Our department is currently conducting a prospective,
randomized, double-blinded study exploring the benefit of adjunct botulinum neurotoxin
A injection for rotator cuff repair.
EVALUATION OF MUSCLE FUNCTION AFTER ROTATOR CUFF TEARS
The shoulder has an extensive range of motion that requires the simultaneous
neuromuscular coordination of numerous muscle-tendon units to produce purposeful
movement. Rotator cuff investigators have largely focused their basic science efforts on
tendon-to-bone fixation, where surgical interventions occur during operative repair [3-5,
23, 47]. The structural changes in the muscle-tendon unit that result in increased repair
tension have also been the subject of many investigations [7, 26, 28, 60]. Since the rotator
cuff acts as a dynamic stabilizer during upper extremity motion, the consequences of
141
structural muscle changes (i.e. atrophy, fibro-fatty infiltration, fiber-type switching, etc)
on contractile force possibly influences post-operative functional outcomes.
Unfortunately, limited literature exists on the function of the rotator cuff muscles after
tendon tears [6, 8, 10, 17, 18, 27, 45, 50].
Several studies have examined exercise capacity in the rabbit shoulder model,
correlating reduced muscle force with histological and radiographic changes that occur
with dis-use atrophy following rotator cuff tendon tears [6, 17, 18]. Similarly, Meyer et
al. demonstrated that chronic tendon tears in the sheep model were associated with
atrophy, retraction, and fatty infiltration, which resulted in reduced amplitude of muscle
contractile force in this chronically injured experimental group. The authors concluded
that computer tomography of the rotator cuff and the associated radiographic changes
could only indirectly and approximately predict the reduced function [50]. Coleman et al.
demonstrated that muscle function was likely to improve in the sheep model when repair
was conducted in the acute tear setting. The authors suggested that when repair is
undertaken in the chronic tear setting, the muscle might not recover full function.
Essentially, as conservative management is pursued and surgery is delayed, their data
suggest that a “point of no return” exists where full function will not be achieved with
current single-stage rotator cuff repair [7].
In a study conducted by Gerber et al., thirteen patients were evaluated by
magnetic resonance imaging, and fibrofatty infiltration of their rotator cuff muscles was
assessed using Goutallier staging [27]. Intraoperative muscle contractile amplitude was
assessed after electrical nerve stimulation and was correlated to the anatomic cross-
sectional area and the amount of fibrofatty infiltration. The authors concluded that higher

142
Goutallier staging resulted in impaired muscle function [27]. Davidson and Rivenburgh
demonstrated reduced isokinetic strength in their patients, when the rotator cuff was
repaired under excessive tension (i.e. repair tension exceeding 8 lbs-force) [10].
Recently, we published a report that examined the functional consequences of
rotator cuff tears in a rat model. There were three experimental groups: 1.) uninjured
controls; 2.) acute injury (muscular function was tested 4-weeks after supraspinatus
tenotomy); and 3.) chronic injury (muscular function was tested 12-weeks after
supraspinatus tenotomy). Histological changes (Fig. 2) in the muscle architecture were
identified that were consistent with increased in vivo stiffness of the muscle-tendon unit
in the acute and chronic tear setting [45]. Our findings were similar to previous published
reports in this animal model [2, 28, 29]. Then in vivo muscle-function testing of the
supraspinatus muscle-tendon unit was performed for a wide range of repair tensions,
creating a comprehensive contractile amplitude versus preload/repair tension profile of
rotator cuff function after injury (Fig. 4). Our data demonstrates that regardless of
experimental group, muscle function is exquisitely sensitive to preload tension [45].
Specifically, we demonstrated that there was a 50% reduction in maximal contractile
amplitude (Fig. 4, p<0.05) [45] at preload tensions equivalent to the chronic repair
tension required to reappose the stiff, retracted supraspinatus muscle-tendon unit to the
humeral head in this rat model [28, 29]. The findings indicate that there is a broad range
of repair tensions in which the supraspinatus muscle is able to generate maximal force;
however, current single-stage repair techniques, which occasionally require excessive
repair tensions, reduce functional capacity significantly. These data provide evidence that
link histological changes after rotator cuff tears to increased stiffness of the muscle
143
tendon unit to reduced muscle contractile amplitude. In conclusion, the study suggests
that improved functional outcomes would be achieved by earlier surgical interventions
for rotator cuff repair [45], thereby avoiding what some investigators consider
irreversible structural and biomechanical changes to the muscle-tendon unit.
COMPUTATIONAL MODELING OF THE HUMAN UPPER EXTREMITY AND
IMPLICATIONS FOR ORTHOPAEDIC SURGERY
In the chronic rotator cuff tear setting, retraction and excessive repair tension
were identified as key contributors to reduced functional capacity in a rat rotator cuff
model. Despite anatomical similarities between rat and human shoulders (Fig. 1), the
mass of the rotator cuff muscles between the two differs by orders of magnitude. Many
surgeons are hesitant to change their management of patients based upon animal data. To
aid in the interpretation of the functional rat data, retraction of chronically torn rotator
cuff muscle-tendon units was examined in a computational human upper-extremity
model.
Computational musculoskeletal models are libraries of data derived from
anatomical (i.e. muscle architecture, anatomical paths) and functional experiments (i.e.
joint moments, muscle force) compiled into an accessible and predictive mathematical
framework (Fig. 5). The force that a muscle-tendon unit generates in these model systems
is dependent on several factors, such as the architecture of the muscle-tendon unit (fiber
length, muscle cross-sectional area, pennation, tendon length) and the stretch in the
muscle and tendon. Hill-type muscle models are mathematical representations of the
mechanical properties of muscle that use non-linear springs (length-dependent elements)
and dashpots (velocity-dependent elements) to capture the force-generating behavior of
144
muscle (Fig. 6) [73]. Graphical representations of mathematical models are useful
clinically because they permit surgeons to interact intuitively with the models. These
graphical models facilitate research because parameters can be easily altered to examine
different clinical conditions (Fig. 6).
We have developed a musculoskeletal model of the upper limb representing the
anthropometry and muscle parameters of a 50th percentile male (Fig. 6) [36]. The
shoulder portion of the musculoskeletal model has three degrees of freedom represented
with definitions recommended by the International Society of Biomechanics [70].
Scapular and clavicular movements representing a normal shoulder rhythm are
incorporated into the model [11]. The upper-extremity musculoskeletal model was
implemented in OpenSim, an open-source software platform [12]. The model
incorporates:
• Skeletal representations of the torso, clavicle, scapula, humerus, radius,
ulna, wrist, and hand
• 15 degrees of freedom including glenohumeral joint, elbow, forearm,
wrist, index finger, and thumb
• 50 Hill-type muscle-tendon actuators representing the muscles and muscle
compartments crossing the shoulder, elbow, forearm, and wrist based on
architectural parameters measured from cadaveric experiments
• Moment arm and maximum isometric joint moment profiles consistent
with experimental values.
The upper limb model used in our study has been used previously to examine
multiple clinically relevant scenarios, including the consequences of Steindler
145
flexorplasty [61], brachioradialis to flexor pollicis longus transfer after spinal cord injury
[53], and latissimus dorsi transfer [20]. Computational models permit us to alter
parameters to represent clinical conditions or interventions in order to understand the
consequences in a way that would be impractical or impossible to explore in vivo (Table
1). Through computational modeling, researchers and surgeons can work together to
identify approaches to improve upper limb function.
THE EFFECT OF MUSCLE-TENDON UNIT RETRACTION ON PASSIVE AND
ACTIVE TENSION: A SIMULATION ANALYSIS OF ROTATOR CUFF TEARS
Numerous animal studies and our own data suggest that the tension required to
repair torn rotator cuff tendons to the humeral head influences surgical outcomes and
may be influenced by gap length and posture. A more detailed understanding of the
forces produced in the human shoulder throughout a full range shoulder postures for a
variety of clinically relevant gap distances may allow surgeons to predict surgical
outcomes, determine surgical candidacy, and to make evidence-based recommendations
for post-operative immobilization and rehabilitation that protect the repair site. The
purpose of our simulation analysis was to characterize the dependence of passive force
and active moment-generating capacity on shoulder posture and tear size in the
supraspinatus following surgical repair of uninjured, acute, and chronic retracted gap
tendon lengths. To represent a surgically repaired supraspinatus muscle-tendon unit, the
tendon slack length was shortened by a gap distance, while the anatomical path of the
muscle was maintained. Tendon slack length was shortened by 1.5cm to represent the
acute tear setting and 3cm to represent the chronic tear setting. Passive forces were
compared to previously reported values for suture pull out strength and anchoring

146
techniques typically used in these repairs (191-287N) [13, 41]. The calculated outcome
measures included passive muscle-tendon force throughout various ranges of motion
(thoracohumeral angle, plane of elevation, and axial rotation) and active moment-
generating capacity throughout abduction (Fig. 7).
Larger gap distances, simulating a chronically torn rotator cuff tendon, and
smaller thoracohumeral angles are associated with increased passive forces (Fig. 7). In
certain postures, the passive tension of chronically torn supraspinatus muscle-tendon
units exceeds anchor fixation methods. Further, larger gap distances are associated with
reduced peak isometric moment-generating capacity, with reductions up to 53% for
simulated chronic rotator cuff tears (Fig. 8). This study elucidates the biomechanical
consequences of repairs of large gap lengths in the rotator cuff and provides insight as to
why repairs in the chronic tear setting are associated with poorer clinical outcomes.
Increased abduction of the arm used to reduce the supraspinatus tendon intraoperatively
for the repair of larger gaps may ultimately lead to increased failure postoperatively
during shoulder adduction. For larger tendon defects, the loss of strength in the
supraspinatus may be substantial following repair, even if retearing is prevented.
Methods for reducing gap lengths, such as tendon grafts or graft substitutes, may limit the
negative biomechanical consequences of the surgical repair of excessively retracted
rotator cuff muscle-tendon units.
SUMMARY AND CONCLUSIONS
Chronically torn rotator cuff muscle-tendon units may be characterized by
increased fibro-fatty infiltration, resulting in a reduced ability to tolerate high repair
tensions. Outcomes of rotator cuff repair may be improved by earlier surgical

147
intervention, which results in lower surgical repair tensions and fewer electromyographic
neuromuscular changes. Our data suggest a direct experimental connection between high
repair tensions in the chronic tear setting and impaired contractile force. There is a
similar reduction of muscle contractile force by approximately 50% in the chronic tear
setting based on our research using both rat (Fig. 4) and simulation analysis (Fig. 8).
Therefore, we are confident our clinical recommendations are translatable from animals
to humans. Simulation analysis stresses the importance of proper arm positioning during
intra-operative repair, post-operative healing, and rehabilitation. Modifications in patient
instructions regarding post-operative arm positioning and range of motion guidelines will
reduce repair site tension. Current research efforts in our laboratory are focused on
reducing repair tension by using tissue-engineered constructs to bridge the large gap
distances that are common after chronic tears in order to improve patient outcomes.
SOURCE OF FUNDING
All studies were completed with intra-departmental physician-scientist start-up funds. No
external funding source was utilized and no external funding source played a role in this
investigation.
ACKNOWLEDGEMENTS
The three-dimensional CT-scans shown in Figure 1 were produced in
collaboration with the Center for Biomolecular Imaging of Wake Forest School of
Medicine. Part of this study was performed in collaboration with the Wake Forest
University Graduate School of Arts and Sciences Summer Research Opportunities
Program. We would like to thank Dr. Beth P. Smith, Dr. Riyaz H. Jinnah, Mrs. Eileen
148
Martin, and Mr Anthony Santago for their support in the planning and execution of the
experiments, as well as useful suggestions in the preparation of this manuscript.
This project is taken in part from a dissertation submitted to the Neuroscience
Program, Wake Forest University Graduate School of Arts and Sciences, in partial
fulfillment of the requirements for the degree of Doctor of Philosophy.
149
REFERENCES
1. Trends in Aging-- United States and Worldwide. pp. 101-106. Edited, 101-106,
Centers for Disease Control and Prevention, 2003.
2. Barton, E. R.; Gimbel, J. A.; Williams, G. R.; and Soslowsky, L. J.: Rat
supraspinatus muscle atrophy after tendon detachment. J Orthop Res, 23(2): 259-65,
2005.
3. Bedi, A.; Fox, A. J.; Harris, P. E.; Deng, X. H.; Ying, L.; Warren, R. F.; and
Rodeo, S. A.: Diabetes mellitus impairs tendon-bone healing after rotator cuff repair.
Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et
al.], 19(7): 978-88, 2010.
4. Bedi, A.; Fox, A. J.; Kovacevic, D.; Deng, X. H.; Warren, R. F.; and Rodeo, S.
A.: Doxycycline-mediated inhibition of matrix metalloproteinases improves healing after
rotator cuff repair. The American journal of sports medicine, 38(2): 308-17, 2010.
5. Bedi, A.; Kovacevic, D.; Hettrich, C.; Gulotta, L. V.; Ehteshami, J. R.; Warren, R.
F.; and Rodeo, S. A.: The effect of matrix metalloproteinase inhibition on tendon-to-bone
healing in a rotator cuff repair model. Journal of shoulder and elbow surgery / American
Shoulder and Elbow Surgeons ... [et al.], 19(3): 384-91, 2010.
6. Bjorkenheim, J. M.: Structure and function of the rabbit's supraspinatus muscle
after resection of its tendon. Acta orthopaedica Scandinavica, 60(4): 461-3, 1989.
7. Coleman, S. H.; Fealy, S.; Ehteshami, J. R.; MacGillivray, J. D.; Altchek, D. W.;
Warren, R. F.; and Turner, A. S.: Chronic rotator cuff injury and repair model in sheep. J
Bone Joint Surg Am, 85-A(12): 2391-402, 2003.
150
8. Coleman, S. H.; Fealy, S.; Ehteshami, J. R.; MacGillivray, J. D.; Altchek, D. W.;
Warren, R. F.; and Turner, A. S.: Chronic rotator cuff injury and repair model in sheep.
The Journal of bone and joint surgery. American volume, 85-A(12): 2391-402, 2003.
9. Costouros, J. G.; Porramatikul, M.; Lie, D. T.; and Warner, J. J.: Reversal of
suprascapular neuropathy following arthroscopic repair of massive supraspinatus and
infraspinatus rotator cuff tears. Arthroscopy, 23(11): 1152-61, 2007.
10. Davidson, P. A., and Rivenburgh, D. W.: Rotator cuff repair tension as a
determinant of functional outcome. J Shoulder Elbow Surg, 9(6): 502-6, 2000.
11. de Groot, J. H., and Brand, R.: A three-dimensional regression model of the
shoulder rhythm. Clinical biomechanics, 16(9): 735-43, 2001.
12. Delp, S. L.; Anderson, F. C.; Arnold, A. S.; Loan, P.; Habib, A.; John, C. T.;
Guendelman, E.; and Thelen, D. G.: OpenSim: open-source software to create and
analyze dynamic simulations of movement. IEEE transactions on bio-medical
engineering, 54(11): 1940-50, 2007.
13. Demirhan, M.; Atalar, A. C.; and Kilicoglu, O.: Primary fixation strength of
rotator cuff repair techniques: a comparative study. Arthroscopy : the journal of
arthroscopic & related surgery : official publication of the Arthroscopy Association of
North America and the International Arthroscopy Association, 19(6): 572-6, 2003.
14. Demirhan, M.; Atalar, A. C.; and Kilicoglu, O.: Primary fixation strength of
rotator cuff repair techniques: a comparative study. Arthroscopy, 19(6): 572-6, 2003.
15. Derwin, K. A.; Baker, A. R.; Codsi, M. J.; and Iannotti, J. P.: Assessment of the
canine model of rotator cuff injury and repair. Journal of shoulder and elbow surgery /
American Shoulder and Elbow Surgeons ... [et al.], 16(5 Suppl): S140-8, 2007.

151
16. Fabis, J.; Danilewicz, M.; and Omulecka, A.: Rabbit supraspinatus tendon
detachment: effects of size and time after tenotomy on morphometric changes in the
muscle. Acta Orthop Scand, 72(3): 282-6, 2001.
17. Fabis, J.; Kordek, P.; Bogucki, A.; and Mazanowska-Gajdowicz, J.: Function of
the rabbit supraspinatus muscle after large detachment of its tendon: 6-week, 3-month,
and 6-month observation. Journal of shoulder and elbow surgery / American Shoulder
and Elbow Surgeons ... [et al.], 9(3): 211-6, 2000.
18. Fabis, J.; Kordek, P.; Bogucki, A.; Synder, M.; and Kolczynska, H.: Function of
the rabbit supraspinatus muscle after detachment of its tendon from the greater tubercle.
Observations up to 6 months. Acta orthopaedica Scandinavica, 69(6): 570-4, 1998.
19. Favard, L.; Bacle, G.; and Berhouet, J.: Rotator cuff repair. Joint, bone, spine :
revue du rhumatisme, 74(6): 551-7, 2007.
20. Favre, P.; Loeb, M. D.; Helmy, N.; and Gerber, C.: Latissimus dorsi transfer to
restore external rotation with reverse shoulder arthroplasty: a biomechanical study.
Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et
al.], 17(4): 650-8, 2008.
21. Fealy, S.; Adler, R. S.; Drakos, M. C.; Kelly, A. M.; Allen, A. A.; Cordasco, F.
A.; Warren, R. F.; and O'Brien, S. J.: Patterns of vascular and anatomical response after
rotator cuff repair. Am J Sports Med, 34(1): 120-7, 2006.
22. Fuchs, B.; Weishaupt, D.; Zanetti, M.; Hodler, J.; and Gerber, C.: Fatty
degeneration of the muscles of the rotator cuff: assessment by computed tomography
versus magnetic resonance imaging. Journal of shoulder and elbow surgery / American
Shoulder and Elbow Surgeons ... [et al.], 8(6): 599-605, 1999.
152
23. Galatz, L.; Rothermich, S.; VanderPloeg, K.; Petersen, B.; Sandell, L.; and
Thomopoulos, S.: Development of the supraspinatus tendon-to-bone insertion: localized
expression of extracellular matrix and growth factor genes. Journal of orthopaedic
research : official publication of the Orthopaedic Research Society, 25(12): 1621-8, 2007.
24. Galatz, L. M.; Ball, C. M.; Teefey, S. A.; Middleton, W. D.; and Yamaguchi, K.:
The outcome and repair integrity of completely arthroscopically repaired large and
massive rotator cuff tears. J Bone Joint Surg Am, 86-A(2): 219-24, 2004.
25. Galatz, L. M.; Charlton, N.; Das, R.; Kim, H. M.; Havlioglu, N.; and
Thomopoulos, S.: Complete removal of load is detrimental to rotator cuff healing. J
Shoulder Elbow Surg, 18(5): 669-75, 2009.
26. Gerber, C.; Meyer, D. C.; Schneeberger, A. G.; Hoppeler, H.; and von
Rechenberg, B.: Effect of tendon release and delayed repair on the structure of the
muscles of the rotator cuff: an experimental study in sheep. J Bone Joint Surg Am, 86-
A(9): 1973-82, 2004.
27. Gerber, C.; Schneeberger, A. G.; Hoppeler, H.; and Meyer, D. C.: Correlation of
atrophy and fatty infiltration on strength and integrity of rotator cuff repairs: a study in
thirteen patients. Journal of shoulder and elbow surgery / American Shoulder and Elbow
Surgeons ... [et al.], 16(6): 691-6, 2007.
28. Gimbel, J. A.; Mehta, S.; Van Kleunen, J. P.; Williams, G. R.; and Soslowsky, L.
J.: The tension required at repair to reappose the supraspinatus tendon to bone rapidly
increases after injury. Clin Orthop Relat Res, (426): 258-65, 2004.
153
29. Gimbel, J. A.; Van Kleunen, J. P.; Lake, S. P.; Williams, G. R.; and Soslowsky,
L. J.: The role of repair tension on tendon to bone healing in an animal model of chronic
rotator cuff tears. J Biomech, 40(3): 561-8, 2007.
30. Gladstone, J. N.; Bishop, J. Y.; Lo, I. K.; and Flatow, E. L.: Fatty infiltration and
atrophy of the rotator cuff do not improve after rotator cuff repair and correlate with poor
functional outcome. The American journal of sports medicine, 35(5): 719-28, 2007.
31. Goutallier, D.; Postel, J. M.; Bernageau, J.; Lavau, L.; and Voisin, M. C.: Fatty
muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan.
Clinical orthopaedics and related research, (304): 78-83, 1994.
32. Goutallier, D.; Postel, J. M.; Gleyze, P.; Leguilloux, P.; and Van Driessche, S.:
Influence of cuff muscle fatty degeneration on anatomic and functional outcomes after
simple suture of full-thickness tears. Journal of shoulder and elbow surgery / American
Shoulder and Elbow Surgeons ... [et al.], 12(6): 550-4, 2003.
33. Gupta, R., and Lee, T. Q.: Contributions of the different rabbit models to our
understanding of rotator cuff pathology. J Shoulder Elbow Surg, 16(5 Suppl): S149-57,
2007.
34. Halder, A. M.; O'Driscoll, S. W.; Heers, G.; Mura, N.; Zobitz, M. E.; An, K. N.;
and Kreusch-Brinker, R.: Biomechanical comparison of effects of supraspinatus tendon
detachments, tendon defects, and muscle retractions. The Journal of bone and joint
surgery. American volume, 84-A(5): 780-5, 2002.
35. Hettrich, C. M.; Rodeo, S. A.; Hannafin, J. A.; Ehteshami, J.; and Shubin Stein,
B. E.: The effect of muscle paralysis using Botox on the healing of tendon to bone in a rat
154
model. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons
... [et al.], 2010.
36. Holzbaur, K. R.; Murray, W. M.; and Delp, S. L.: A model of the upper extremity
for simulating musculoskeletal surgery and analyzing neuromuscular control. Annals of
biomedical engineering, 33(6): 829-40, 2005.
37. Hsu, J. E.; Reuther, K. E.; Sarver, J. J.; Lee, C. S.; Thomas, S. J.; Glaser, D. L.;
and Soslowsky, L. J.: Restoration of anterior-posterior rotator cuff force balance
improves shoulder function in a rat model of chronic massive tears. Journal of
orthopaedic research : official publication of the Orthopaedic Research Society, 2011.
38. Jamali, A. A.; Afshar, P.; Abrams, R. A.; and Lieber, R. L.: Differential
expression of neural cell adhesion molecule (NCAM) after tenotomy in rabbit skeletal
muscle. Journal of orthopaedic research : official publication of the Orthopaedic Research
Society, 20(2): 364-9, 2002.
39. Jozsa, L.; Kannus, P.; Thoring, J.; Reffy, A.; Jarvinen, M.; and Kvist, M.: The
effect of tenotomy and immobilisation on intramuscular connective tissue. A
morphometric and microscopic study in rat calf muscles. J Bone Joint Surg Br, 72(2):
293-7, 1990.
40. Kim, H. M.; Dahiya, N.; Teefey, S. A.; Keener, J. D.; Galatz, L. M.; and
Yamaguchi, K.: Relationship of tear size and location to fatty degeneration of the rotator
cuff. The Journal of bone and joint surgery. American volume, 92(4): 829-39, 2010.
41. Ma, C. B.; Comerford, L.; Wilson, J.; and Puttlitz, C. M.: Biomechanical
evaluation of arthroscopic rotator cuff repairs: double-row compared with single-row
fixation. The Journal of bone and joint surgery. American volume, 88(2): 403-10, 2006.
155
42. Ma, J.; Shen, J.; Smith, B. P.; Ritting, A.; Smith, T. L.; and Koman, L. A.:
Bioprotection of tendon repair: adjunctive use of botulinum toxin A in Achilles tendon
repair in the rat. J Bone Joint Surg Am, 89(10): 2241-9, 2007.
43. Mallon, W. J.; Wilson, R. J.; and Basamania, C. J.: The association of
suprascapular neuropathy with massive rotator cuff tears: a preliminary report. J Shoulder
Elbow Surg, 15(4): 395-8, 2006.
44. Mannava, S.; Callahan, M. F.; Trach, S. M.; Wiggins, W. F.; Smith, B. P.;
Koman, L. A.; Smith, T. L.; and Tuohy, C. J.: Chemical denervation with botulinum
neurotoxin a improves the surgical manipulation of the muscle-tendon unit: an
experimental study in an animal model. J Hand Surg Am, 36(2): 222-31, 2011.
45. Mannava, S.; Plate, J. F.; Seyler, T. M.; Whitlock, P. W.; Callahan, M. F.;
Koman, L. A.; Smith, T. L.; and Tuohy, C. J.: Evaluation of in vivo rotator cuff muscle
function after acute and chronic detachment of the supraspinatus tendon: an experimental
study in an animal model. . JBJS [Am.], ACCEPTED for publication 2011.
46. Mannava, S.; Wiggins, W. F.; Saul, K. R.; Stitzel, J. D.; Smith, B. P.; Andrew
Koman, L.; Smith, T. L.; and Tuohy, C. J.: Contributions of Neural Tone to In Vivo
Passive Muscle-Tendon Unit Biomechanical Properties in a Rat Rotator Cuff Animal
Model. Annals of biomedical engineering, 2011.
47. Manning, C. N.; Kim, H. M.; Sakiyama-Elbert, S.; Galatz, L. M.; Havlioglu, N.;
and Thomopoulos, S.: Sustained delivery of transforming growth factor beta three
enhances tendon-to-bone healing in a rat model. Journal of orthopaedic research : official
publication of the Orthopaedic Research Society, 2011.
156
48. Matsen, F. A., 3rd: Clinical practice. Rotator-cuff failure. The New England
journal of medicine, 358(20): 2138-47, 2008.
49. Matsumoto, F.; Uhthoff, H. K.; Trudel, G.; and Loehr, J. F.: Delayed tendon
reattachment does not reverse atrophy and fat accumulation of the supraspinatus--an
experimental study in rabbits. Journal of orthopaedic research : official publication of the
Orthopaedic Research Society, 20(2): 357-63, 2002.
50. Meyer, D. C.; Gerber, C.; Von Rechenberg, B.; Wirth, S. H.; and Farshad, M.:
Amplitude and Strength of Muscle Contraction Are Reduced in Experimental Tears of
the Rotator Cuff. The American journal of sports medicine, 2011.
51. Meyer, D. C.; Hoppeler, H.; von Rechenberg, B.; and Gerber, C.: A
pathomechanical concept explains muscle loss and fatty muscular changes following
surgical tendon release. J Orthop Res, 22(5): 1004-7, 2004.
52. Millett, P. J.; Horan, M. P.; Maland, K. E.; and Hawkins, R. J.: Long-term
survivorship and outcomes after surgical repair of full-thickness rotator cuff tears. Journal
of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et al.], 2011.
53. Mogk, J. P.; Johanson, M. E.; Hentz, V. R.; Saul, K. R.; and Murray, W. M.: A
simulation analysis of the combined effects of muscle strength and surgical tensioning on
lateral pinch force following brachioradialis to flexor pollicis longus transfer. Journal of
biomechanics, 44(4): 669-75, 2011.
54. Oh, J. H.; Kim, S. H.; Ji, H. M.; Jo, K. H.; Bin, S. W.; and Gong, H. S.:
Prognostic factors affecting anatomic outcome of rotator cuff repair and correlation with
functional outcome. Arthroscopy, 25(1): 30-9, 2009.
157
55. Oh, L. S.; Wolf, B. R.; Hall, M. P.; Levy, B. A.; and Marx, R. G.: Indications for
rotator cuff repair: a systematic review. Clin Orthop Relat Res, 455: 52-63, 2007.
56. Rejeski, W. J.; Ip, E. H.; Marsh, A. P.; Miller, M. E.; and Farmer, D. F.:
Measuring disability in older adults: the International Classification System of
Functioning, Disability and Health (ICF) framework. Geriatr Gerontol Int, 8(1): 48-54,
2008.
57. Rowshan, K.; Hadley, S.; Pham, K.; Caiozzo, V.; Lee, T. Q.; and Gupta, R.:
Development of fatty atrophy after neurologic and rotator cuff injuries in an animal
model of rotator cuff pathology. The Journal of bone and joint surgery. American
volume, 92(13): 2270-8, 2010.
58. Rowshan, K.; Hadley, S.; Pham, K.; Caiozzo, V.; Lee, T. Q.; and Gupta, R.:
Development of fatty atrophy after neurologic and rotator cuff injuries in an animal
model of rotator cuff pathology. J Bone Joint Surg Am, 92(13): 2270-8, 2010.
59. Rubino, L. J.; Sprott, D. C.; Stills, H. F., Jr.; and Crosby, L. A.: Fatty infiltration
does not progress after rotator cuff repair in a rabbit model. Arthroscopy : the journal of
arthroscopic & related surgery : official publication of the Arthroscopy Association of
North America and the International Arthroscopy Association, 24(8): 936-40, 2008.
60. Safran, O.; Derwin, K. A.; Powell, K.; and Iannotti, J. P.: Changes in rotator cuff
muscle volume, fat content, and passive mechanics after chronic detachment in a canine
model. J Bone Joint Surg Am, 87(12): 2662-70, 2005.
61. Saul, K. R.; Murray, W. M.; Hentz, V. R.; and Delp, S. L.: Biomechanics of the
Steindler flexorplasty surgery: a computer simulation study. The Journal of hand surgery,
28(6): 979-86, 2003.
158
62. Sher, J. S.; Uribe, J. W.; Posada, A.; Murphy, B. J.; and Zlatkin, M. B.: Abnormal
findings on magnetic resonance images of asymptomatic shoulders. The Journal of bone
and joint surgery. American volume, 77(1): 10-5, 1995.
63. Sonnabend, D. H.; Howlett, C. R.; and Young, A. A.: Histological evaluation of
repair of the rotator cuff in a primate model. The Journal of bone and joint surgery.
British volume, 92(4): 586-94, 2010.
64. Soslowsky, L. J.; Carpenter, J. E.; DeBano, C. M.; Banerji, I.; and Moalli, M. R.:
Development and use of an animal model for investigations on rotator cuff disease. J
Shoulder Elbow Surg, 5(5): 383-92, 1996.
65. Soslowsky, L. J.; Carpenter, J. E.; DeBano, C. M.; Banerji, I.; and Moalli, M. R.:
Development and use of an animal model for investigations on rotator cuff disease.
Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et
al.], 5(5): 383-92, 1996.
66. Soslowsky, L. J.; Thomopoulos, S.; Tun, S.; Flanagan, C. L.; Keefer, C. C.;
Mostow, J.; and Carpenter, J. E.: Neer award 1999 Overuse activity injures the
supraspinatus tendon in an animal model: A histologic and biomechanical study. Journal
of Shoulder and Elbow Surgery, 9(2): 79-84.
67. Uhthoff, H. K.; Matsumoto, F.; Trudel, G.; and Himori, K.: Early reattachment
does not reverse atrophy and fat accumulation of the supraspinatus--an experimental
study in rabbits. Journal of orthopaedic research : official publication of the Orthopaedic
Research Society, 21(3): 386-92, 2003.
68. Vitale, M. A.; Vitale, M. G.; Zivin, J. G.; Braman, J. P.; Bigliani, L. U.; and
Flatow, E. L.: Rotator cuff repair: an analysis of utility scores and cost-effectiveness.
159
Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons ... [et
al.], 16(2): 181-7, 2007.
69. Williams, G. R., Jr.; Rockwood, C. A., Jr.; Bigliani, L. U.; Iannotti, J. P.; and
Stanwood, W.: Rotator cuff tears: why do we repair them? The Journal of bone and joint
surgery. American volume, 86-A(12): 2764-76, 2004.
70. Wu, G. et al.: ISB recommendation on definitions of joint coordinate systems of
various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and
hand. Journal of biomechanics, 38(5): 981-992, 2005.
71. Yamaguchi, K.; Ditsios, K.; Middleton, W. D.; Hildebolt, C. F.; Galatz, L. M.;
and Teefey, S. A.: The demographic and morphological features of rotator cuff disease. A
comparison of asymptomatic and symptomatic shoulders. The Journal of bone and joint
surgery. American volume, 88(8): 1699-704, 2006.
72. Yamamoto, A.; Takagishi, K.; Osawa, T.; Yanagawa, T.; Nakajima, D.; Shitara,
H.; and Kobayashi, T.: Prevalence and risk factors of a rotator cuff tear in the general
population. J Shoulder Elbow Surg, 19(1): 116-20, 2010.
73. Zajac, F. E.: Muscle and tendon: properties, models, scaling, and application to
biomechanics and motor control. Critical reviews in biomedical engineering, 17(4): 359-
411, 1989
160
Chapter 5 Figures and Table
FIG 1: Anatomical Similarities Between the Rat and Human Shoulder. Three-
dimensional reconstructions of computer-tomography radiographic studies for rat
shoulder (Panel A) and for human shoulder (Panel B) are depicted. The supraspinatus
tendon in both species pass beneath an enclosed arch, as described by Soslowsky et al.
[65].
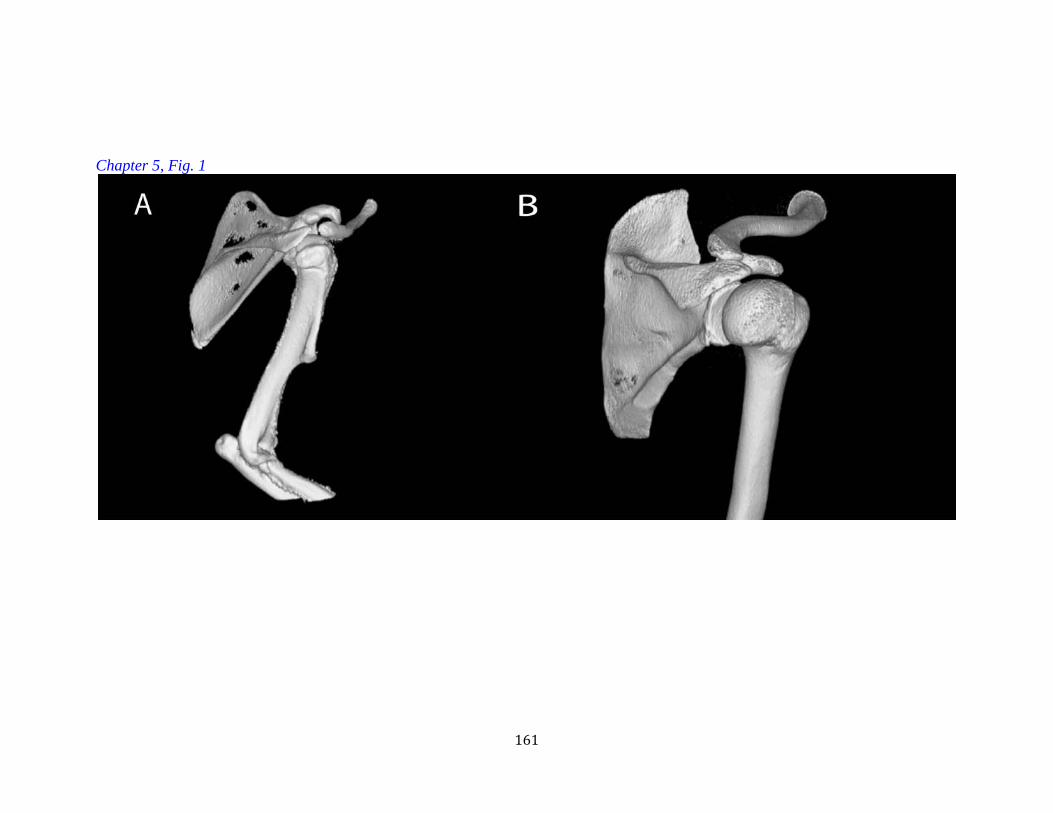
161
Chapter 5, Fig. 1
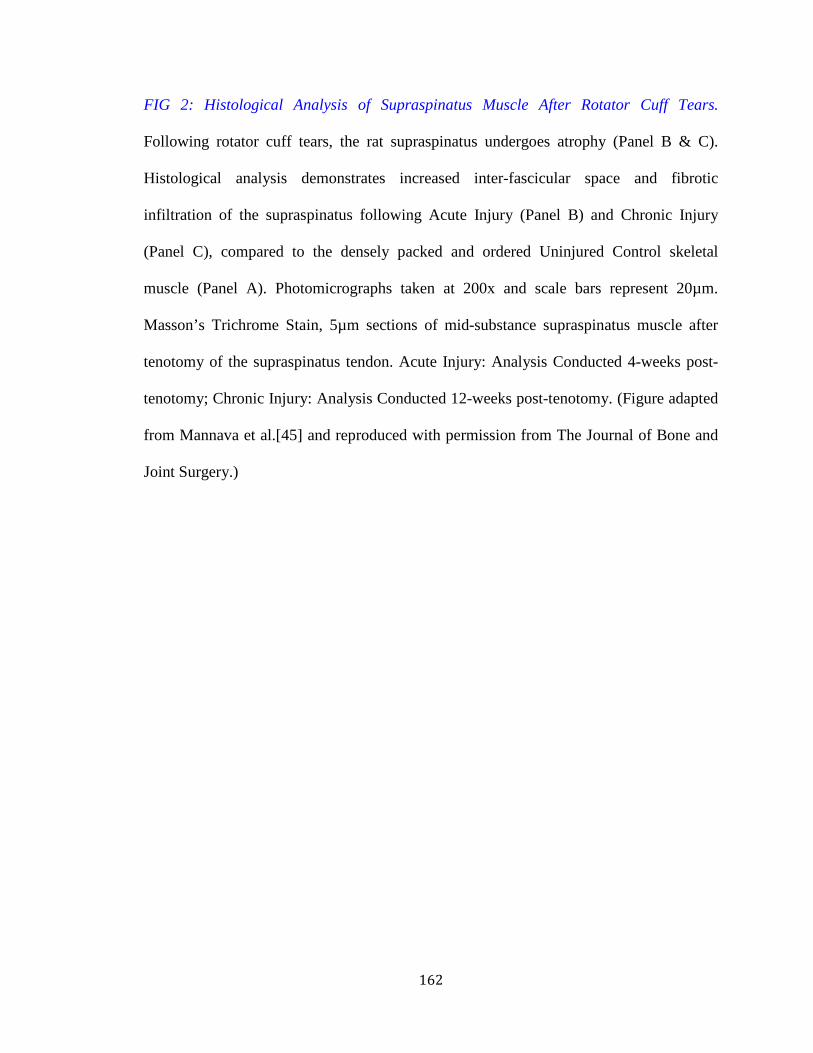
162
FIG 2: Histological Analysis of Supraspinatus Muscle After Rotator Cuff Tears.
Following rotator cuff tears, the rat supraspinatus undergoes atrophy (Panel B & C).
Histological analysis demonstrates increased inter-fascicular space and fibrotic
infiltration of the supraspinatus following Acute Injury (Panel B) and Chronic Injury
(Panel C), compared to the densely packed and ordered Uninjured Control skeletal
muscle (Panel A). Photomicrographs taken at 200x and scale bars represent 20µm.
Masson’s Trichrome Stain, 5µm sections of mid-substance supraspinatus muscle after
tenotomy of the supraspinatus tendon. Acute Injury: Analysis Conducted 4-weeks post-
tenotomy; Chronic Injury: Analysis Conducted 12-weeks post-tenotomy. (Figure adapted
from Mannava et al.[45] and reproduced with permission from The Journal of Bone and
Joint Surgery.)

163
Chapter 5, Fig. 2

164
FIG 3: Chronicity of Rotator Cuff Injury Influences Supraspinatus Electromyography
(EMG). Compound motor action potential (CMAP) and area under the curve (AUC) were
recorded by electromyography (EMG) from the supraspinatus muscle, following
suprascapular nerve stimulation. Panel A: After the rat rotator cuff was chronically
injured, there was lower maximal compound motor action potential (CMAP) amplitude
when compared to both the uninjured control (p<0.05, denoted by *) and acutely injured
groups (p<0.05, denoted by *). Panel B: Significant differences in AUC of the CMAP
were not detected between the experimental groups. All data are presented as mean and
standard error of the mean. Acute Injury: EMG Tested 4-weeks post-tenotomy; Chronic
Injury: EMG Tested 12-weeks post-tenotomy. (Figure adapted from Mannava et al.[45]
and reproduced with permission from The Journal of Bone and Joint Surgery.)
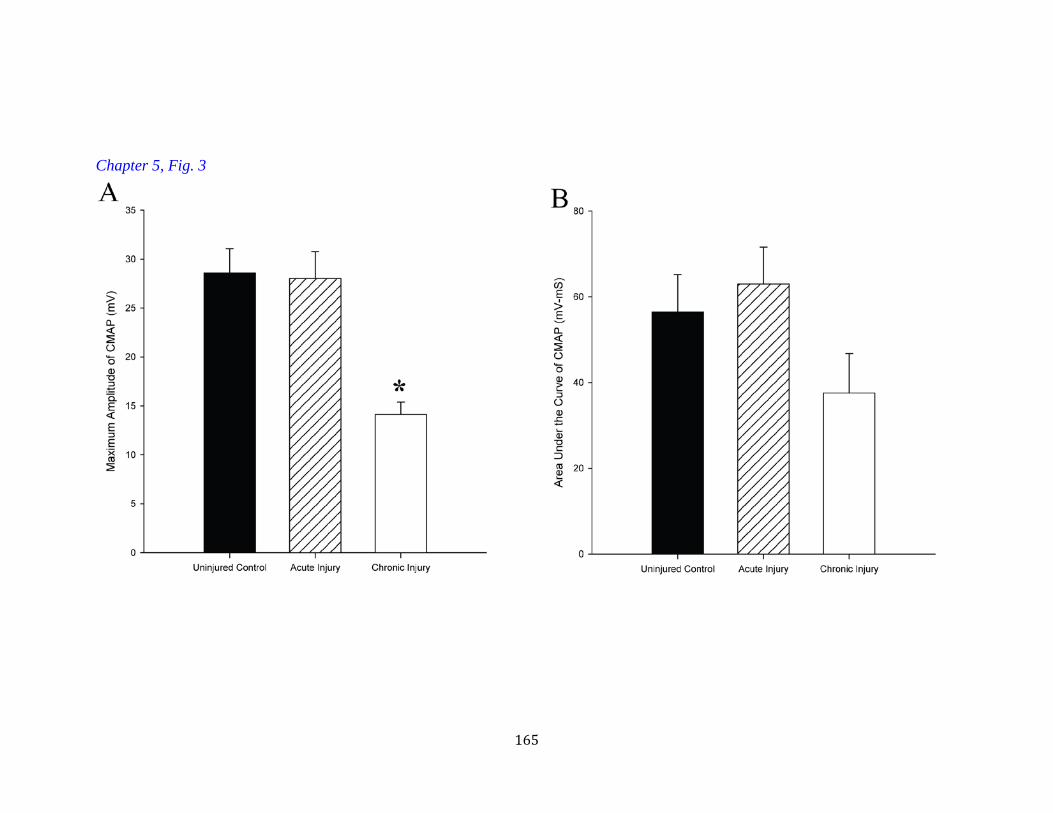
165
Chapter 5, Fig. 3
166
FIG 4: Repair Tension Influences Supraspinatus Muscle Function. The peak tension
required to repair an acutely torn rat rotator cuff is approximately 1.7N of preload
tension.[28, 29] The peak tension required to repair a chronically torn rat rotator cuff is
approximately 2.5N.[28, 29] Preload or repair tension affected the maximal supraspinatus
muscle single twitch contraction in all experimental groups (p<0.05). For all groups,
there was between a 22%-45% reduction in maximal single twitch amplitude at acute
repair tensions and between a 45%-56% reduction in maximal single twitch amplitude at
chronic repair tensions. Both of these reductions in contractile force were significant
(p<0.05). Data are presented as mean and standard error of the mean. (Figure adapted
from Mannava et al. [45] and reproduced with permission from The Journal of Bone and
Joint Surgery.)
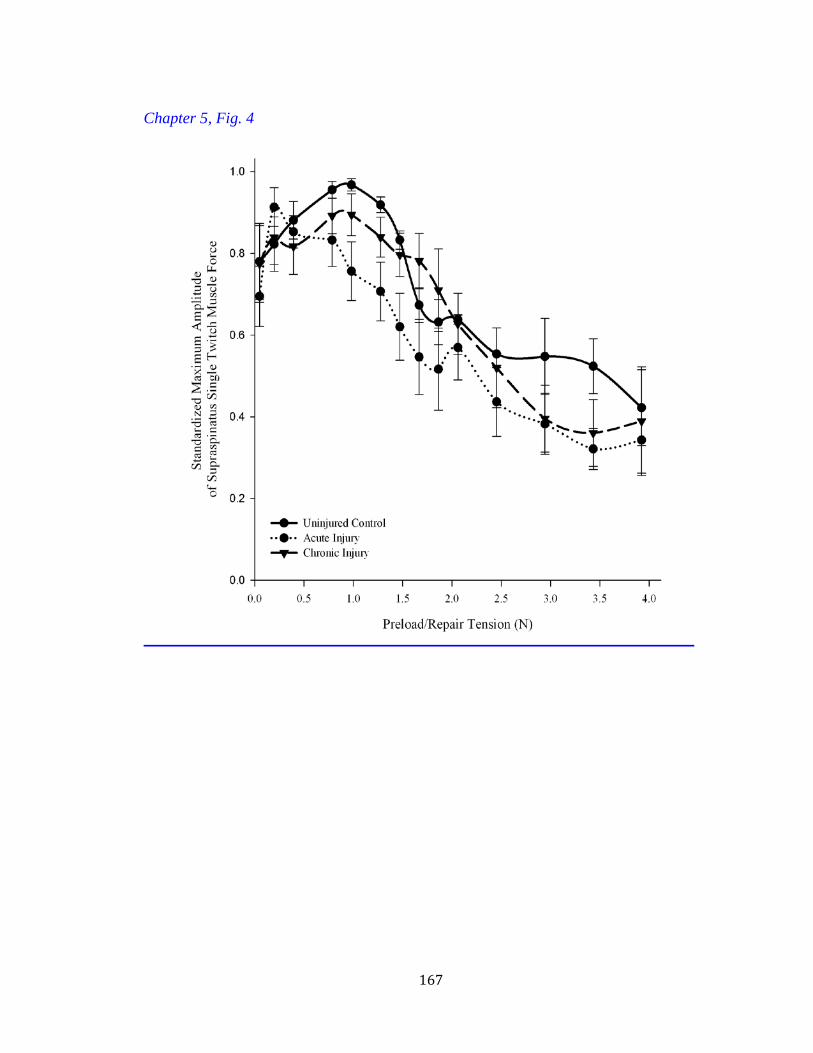
167
Chapter 5, Fig. 4

168
FIG 5. Schematic diagram depicting the elements required to create an orthopaedic movement biomechanics model.
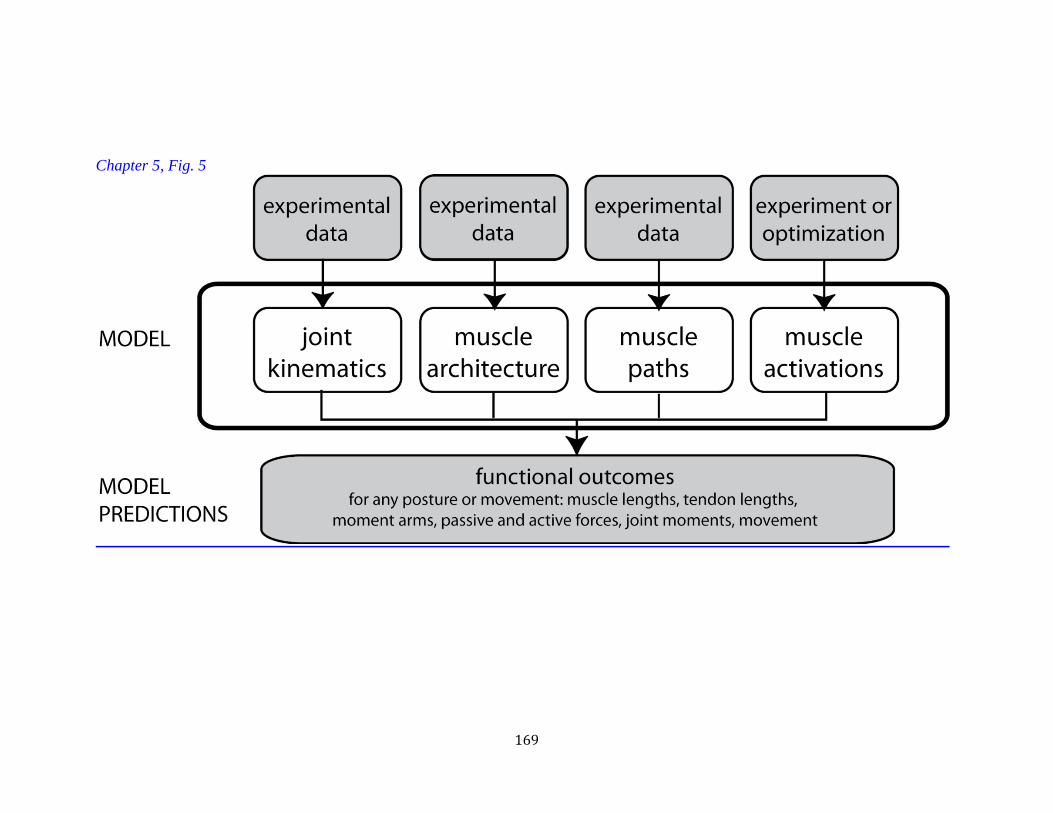
169
Chapter 5, Fig. 5
170
FIG 6. The Shoulder Portion of the Musculoskeletal Model. A musculoskeletal model
was developed for of the upper limb representing the anthropometry and muscle
parameters of a 50th percentile male [36]. Some of the parameters used for the
development of this model are shown in schematic form.
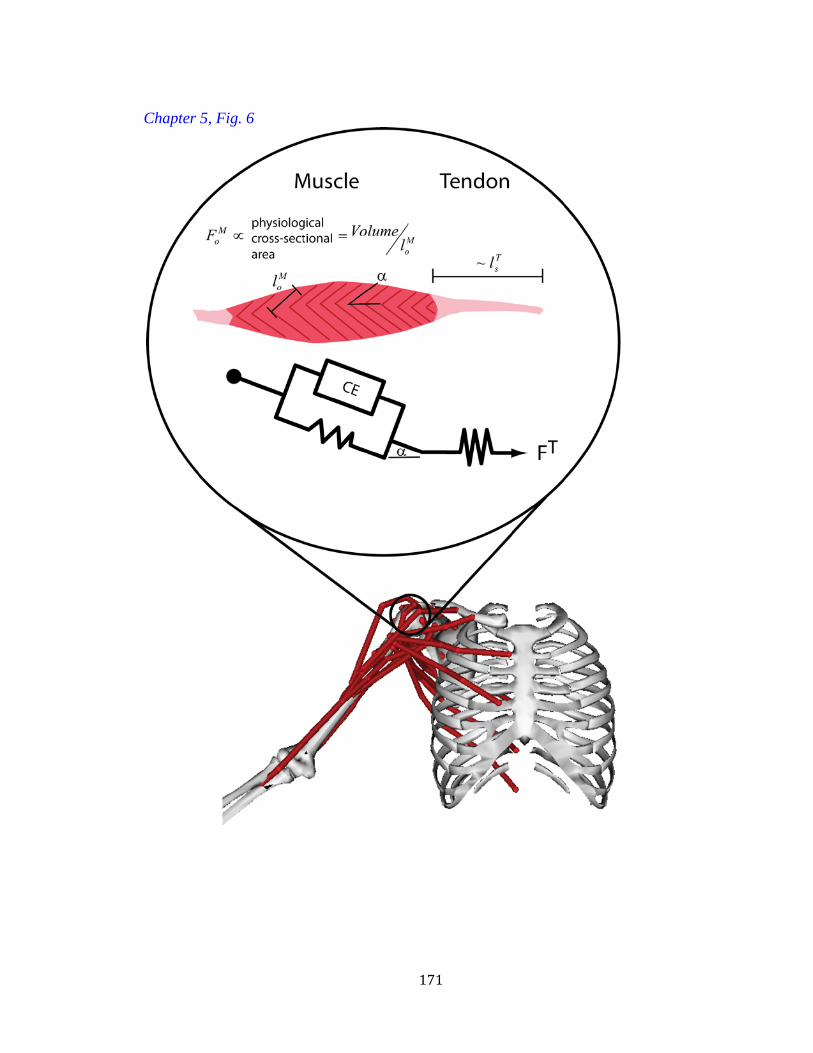
171
Chapter 5, Fig. 6
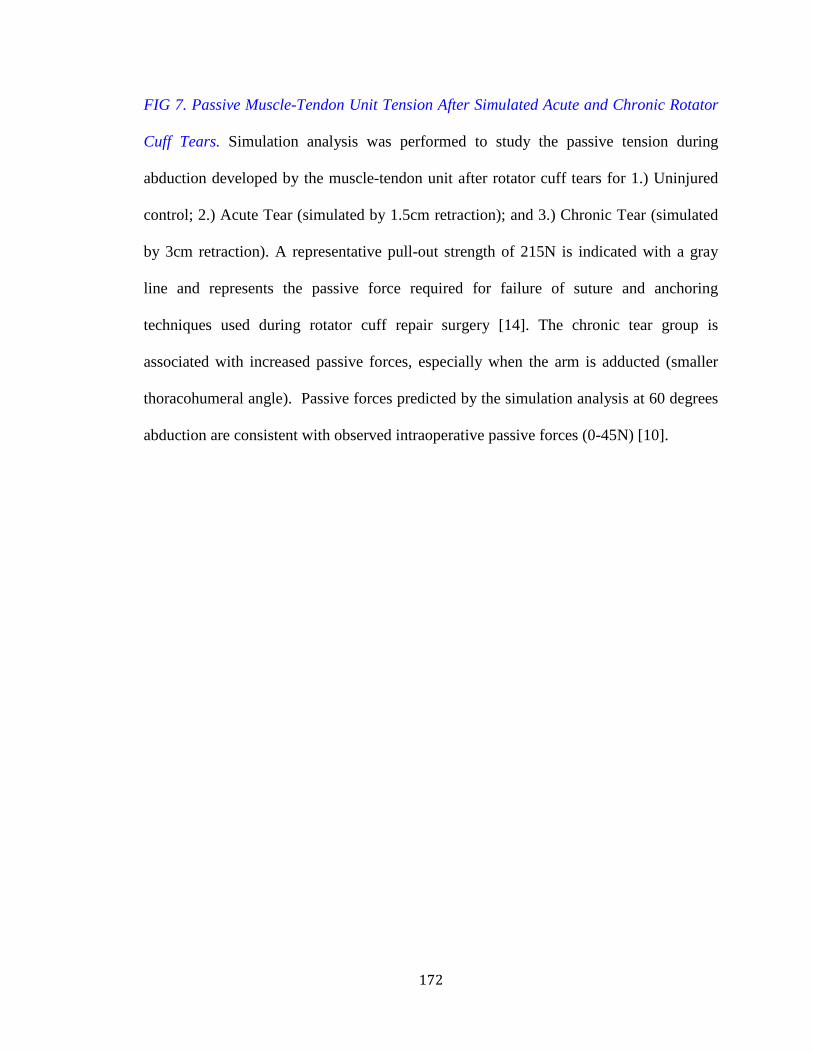
172
FIG 7. Passive Muscle-Tendon Unit Tension After Simulated Acute and Chronic Rotator
Cuff Tears. Simulation analysis was performed to study the passive tension during
abduction developed by the muscle-tendon unit after rotator cuff tears for 1.) Uninjured
control; 2.) Acute Tear (simulated by 1.5cm retraction); and 3.) Chronic Tear (simulated
by 3cm retraction). A representative pull-out strength of 215N is indicated with a gray
line and represents the passive force required for failure of suture and anchoring
techniques used during rotator cuff repair surgery [14]. The chronic tear group is
associated with increased passive forces, especially when the arm is adducted (smaller
thoracohumeral angle). Passive forces predicted by the simulation analysis at 60 degrees
abduction are consistent with observed intraoperative passive forces (0-45N) [10].
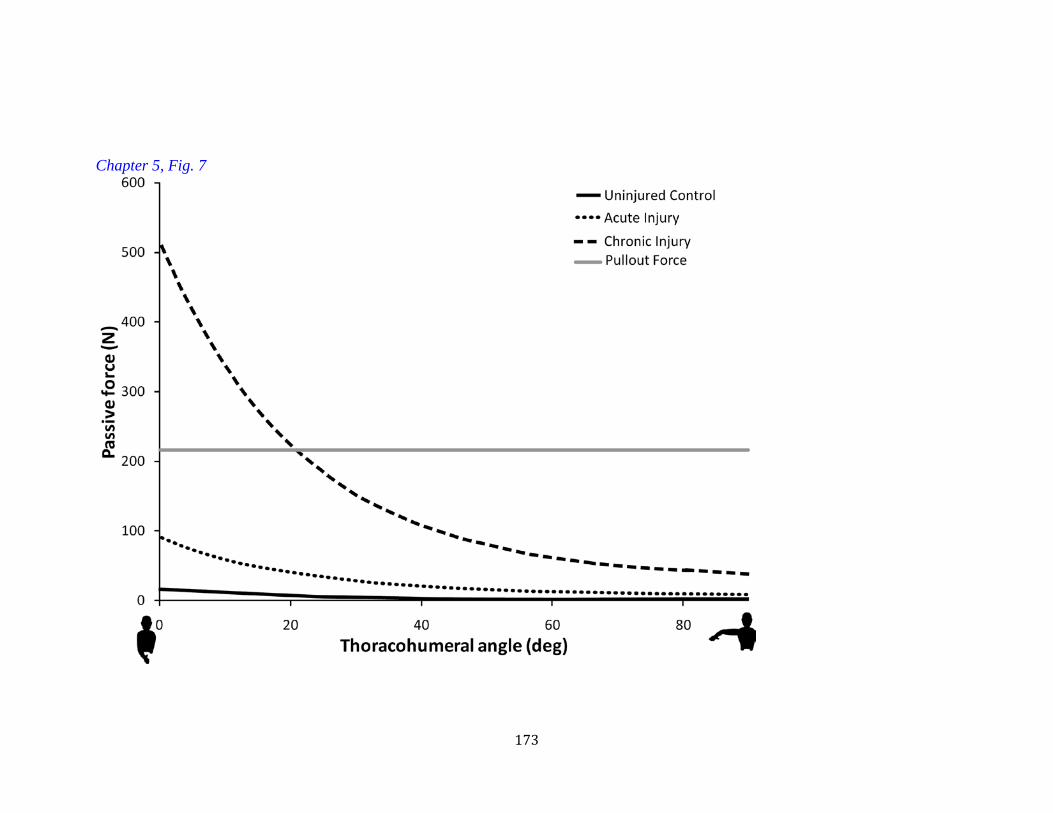
173
Chapter 5, Fig. 7
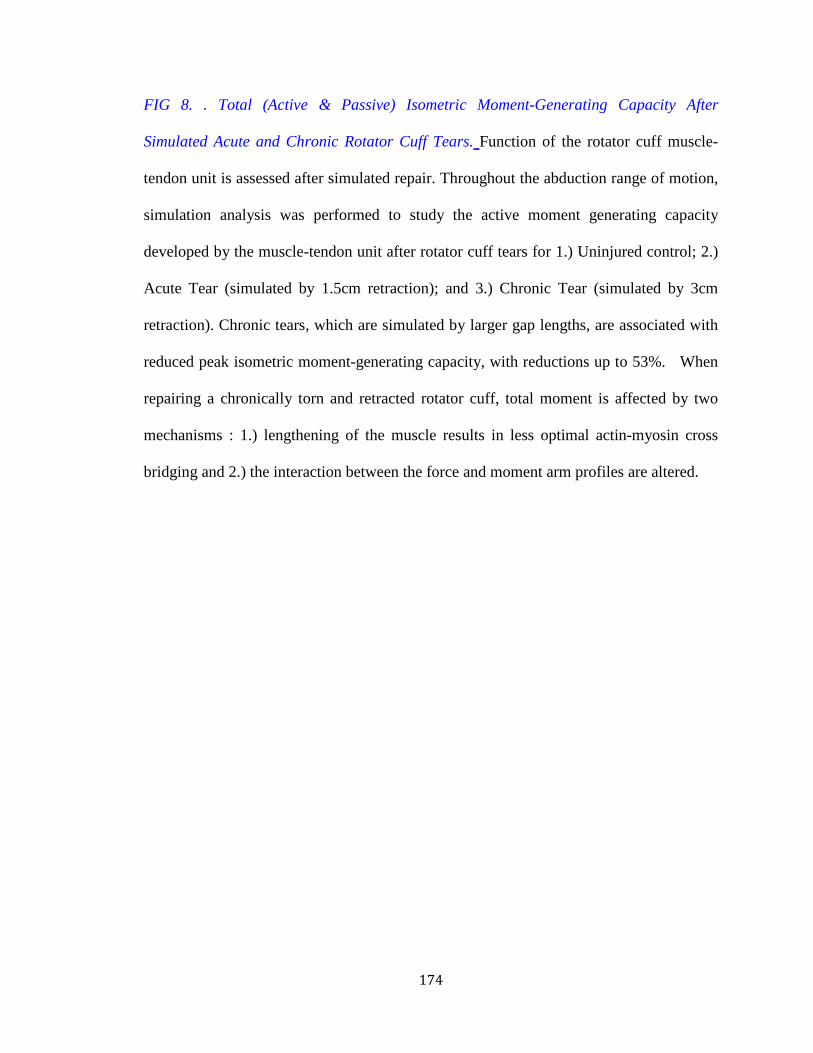
174
FIG 8. . Total (Active & Passive) Isometric Moment-Generating Capacity After
Simulated Acute and Chronic Rotator Cuff Tears. Function of the rotator cuff muscle-
tendon unit is assessed after simulated repair. Throughout the abduction range of motion,
simulation analysis was performed to study the active moment generating capacity
developed by the muscle-tendon unit after rotator cuff tears for 1.) Uninjured control; 2.)
Acute Tear (simulated by 1.5cm retraction); and 3.) Chronic Tear (simulated by 3cm
retraction). Chronic tears, which are simulated by larger gap lengths, are associated with
reduced peak isometric moment-generating capacity, with reductions up to 53%. When
repairing a chronically torn and retracted rotator cuff, total moment is affected by two
mechanisms : 1.) lengthening of the muscle results in less optimal actin-myosin cross
bridging and 2.) the interaction between the force and moment arm profiles are altered.
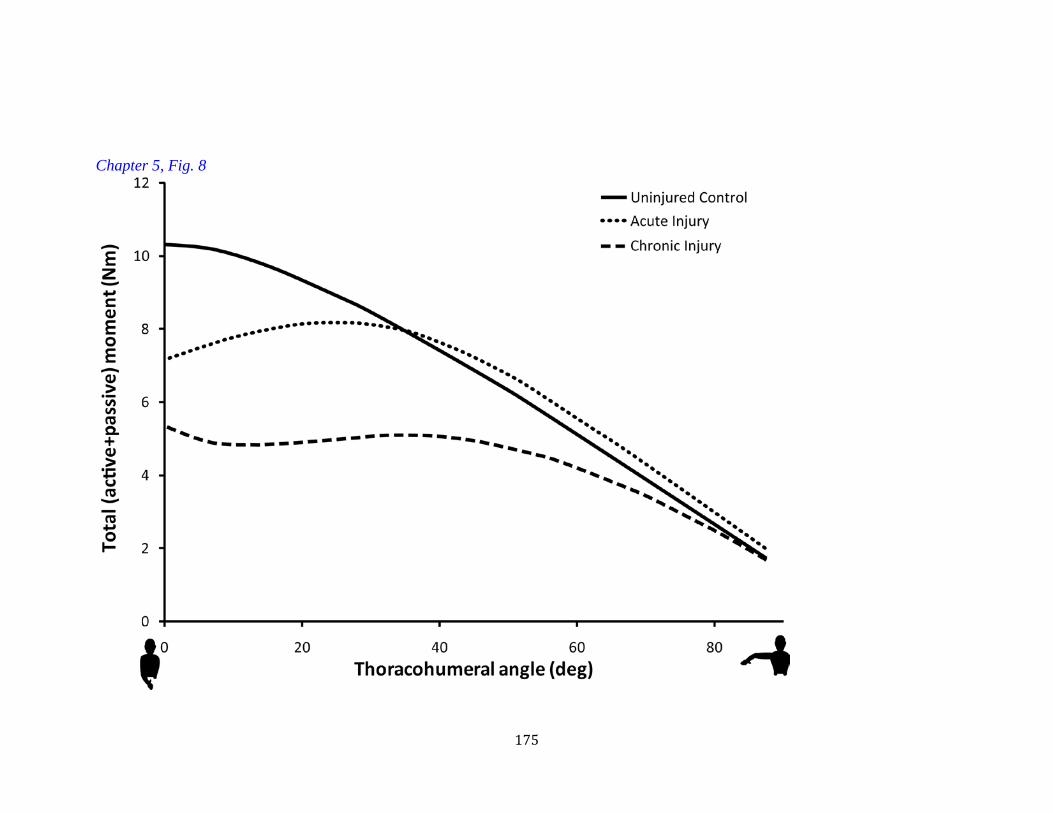
175
Chapter 5, Fig. 8
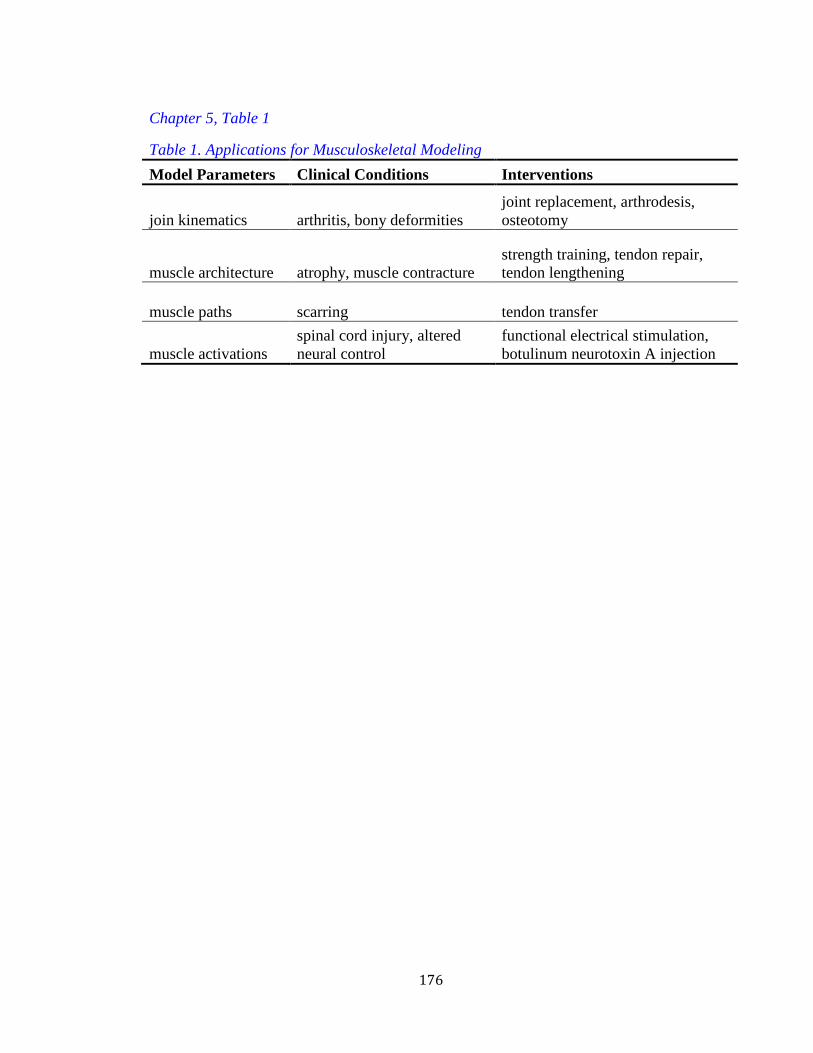
176
Chapter 5, Table 1
Table 1. Applications for Musculoskeletal Modeling Model Parameters Clinical Conditions Interventions
join kinematics arthritis, bony deformities joint replacement, arthrodesis, osteotomy
muscle architecture atrophy, muscle contracture strength training, tendon repair, tendon lengthening
muscle paths scarring tendon transfer
muscle activations spinal cord injury, altered neural control
functional electrical stimulation, botulinum neurotoxin A injection

177
CHAPTER 6
CLINICAL RELEVANCE AND FUTURE DIRECTIONS
Sandeep Mannava

178
SUMMARY OF DOCTORAL THESIS
In summary, the data presented in this thesis suggest that rotator cuff surgical
outcomes may be improved by earlier intervention, which results in lower surgical repair
tensions and fewer electromyographic neuromuscular changes. Our data suggest a direct
experimental connection between high repair tensions—chronic tear setting—and
impaired contractile force. The pharmacological modulation of increased muscle-tendon
unit stiffness using BoNT-A has the potential to reduce the requirement for high-repair
tensions, facilitating the surgical manipulation of the muscle-tendon unit and protecting
the repaired tendon. Simulation analysis stresses the importance of proper arm
positioning during intra-operative repair, post-operative healing, and rehabilitation. Thus,
changing patient instructions on post-operative arm positioning and ranges of motion will
reduce repair site tension.
CLINICAL RELEVANCE TO ORTHOPAEDIC SURGERY
The universal goals of rotator cuff surgery are to restore normal joint motion,
return the patient to full upper-extremity function, and to prevent further degenerative
disease. Despite many recent surgical advances, favorable outcomes after rotator cuff
repair surgery remain a challenge for the orthopedic surgeon. Thus, surgeons must
continue to unravel the biology that underlies rotator cuff pathophysiology in an attempt
to improve surgical intervention. By unraveling the biological mechanisms underlying
rotator cuff pathology in this clinically-relevant animal model system, the results of this
thesis may have the potential to improve the understanding of neuromuscular function
after rotator cuff tears, which may eventually lead to patient-specific interventions and
management for rotator cuff tears. Ultimately, an improved biological understanding of

179
rotator cuff pathophysiology allows for evidence-based guidelines in the treatment and
management of rotator cuff dysfunction. Improved surgical techniques will eventually
lead to an expedited return to independent living and recreational activities for patients
who have undergone rotator cuff surgery.
FUTURE DIRECTION FOR ROTATOR CUFF SURGERY RESEARCH
Our research efforts are centered on addressing clinical problems, and ultimately,
to improve patient care by translating this basic-science knowledge into clinical practice.
The experiments in this thesis allowed us to test the feasibility of utilizing an established
and well-characterized animal model system in order to improve our understanding of
rotator cuff neuromuscular function after injury in a small animal model. This proposal
represents a critical step in building a portfolio of functional rotator cuff data. However,
future studies will need to study the cellular and molecular basis of the
pathophysiological phenomena observed after rotator cuff injury in a small animal model,
large animal models [1-3] and, ultimately, clinical rotator cuff reconstruction studies.
Further, future molecular studies of in vivo osteointegration, tendon remodeling, and
muscle healing are needed to better elucidate the molecular mechanisms, cell signaling
pathways, and growth factor expression underlying rotator cuff healing. These future
studies will improve our molecular understanding of rotator cuff healing, which may
ultimately lead to improved surgical outcomes following tendon repair surgery.
THE STUDY OF AGE –RELATED CHANGES AND THE INFLUENCE ON
ROTATOR CUFF SURGERY
With increasing age and activity level of the population, there has been a similar
increase in both the prevalence and the number of operative interventions for
180
symptomatic rotator cuff tears [4-6]. Rotator cuff tears are a common cause of upper
extremity pain and disability in older adults. It is estimated that 20% of adults experience
a rotator cuff tear, with prevalence increasing to near 50% in adults over the age of 70
[7]. Chronic disability from rotator cuff tendinopathy affects approximately 20% of older
adults who struggle to maintain independence while faced with reduced mobility and
subsequent difficulty performing activities of daily living (ADLs) [8]. Difficulty
performing upper limb tasks such as lifting is one of the first indicators of disability [9].
Advanced age has been associated with decreased muscle function [10-14] and
healing potential after injury [13, 14], possibly due to molecular and structural changes in
the muscle occurring throughout the normal aging process [10, 11]. Some of the
detrimental changes associated with aging include loss of muscle mass [15, 16], a decline
in growth factor or trophic support of the muscle tissue (i.e. decreased IGF-1) [17, 18],
excitation-contraction uncoupling, impaired intracellular calcium handling [19, 20], age-
related denervation [21], and altered molecular expression of proteins essential for force
production [19, 20]. Myogenic regulatory factors, such as MyoD and Myf5, play an
important role during skeletal muscle development and its response to injury following
rotator cuff tears [22].
Despite the clinical knowledge that advanced patient age is a risk factor for sub-
optimal rotator cuff repair outcomes [13, 14, 23-25], there is limited understanding of
why senescent patients perform poorly following surgery. The rat rotator cuff is an
established animal model suitable for the study of human rotator cuff pathology [26, 27].
However, many basic science rodent studies have not addressed the influence of age on

181
rotator cuff pathology because the National Institutes of Health has limited access to the
Aged Rodent Colony to National Institutes of Aging funded researchers.
We are amongst the first in orthopaedic surgery to utilize the National Institutes
of Aging in vivo Aged Rodent Colony animal model to study the effects of age on
supraspinatus muscle dysfunction. We are actively funded through the Orthopaedic
Research and Education Foundation to characterize how the normal aging process
influences rotator cuff muscle-tendon unit structure and function. Due to the high
prevalence of rotator cuff tears in the elderly patient population and the heterogeneity of
patient activity level, it is difficult to study how tendon injury and age-related changes
influence rotator cuff function in the clinical setting. The N.I.A. animal model utilized in
this study allows us to explore the natural history of age-related rotator cuff changes in
isolation from rotator cuff injury. We hypothesized that aged muscle undergoes structural
and molecular changes that reduce its functional capacity. We are also actively funded to
study the influence of age on tendon-to-bone healing, through the use of biomechanical
and histological techniques.
Additionally, we have recently begun a pilot project studying the natural history
of aging on rotator cuff muscle-tendon unit properties in a characterized aged vervet
monkey model. Current research efforts are focused on studying age related histological
changes to the skeletal muscle structure, biomechanical characterization of the upper
extremity musculature (using laser diffraction, advanced radiological imaging, and
careful dissection), and tendon-to-bone biomechanical properties. We are hoping to use
these studies as pilot data to obtain funding to study the natural history of rotator cuff

182
changes after tendon tear and attempt experimental interventions in this large animal
model.
FUTURE DIRECTIONS OF BOTULINUM NEUROTOXIN A (BONT-A)
MODULATION OF SOFT-TISSUE BIOMECHANICS
We are currently conducting a series of murine studies with BoNT-A to better
understand the mechanism by which chemical denervation improves the surgical
manipulation of the muscle-tendon unit. In particular, we have designed a series of
experiments to study the myotatic reflex (FIG. 1), whose component parts of the reflex
loop consist of the Golgi tendon organ, the intrafusal muscle fibers, afferent / efferent
neural connections to the α- and γ-motoneurons, as well as inter-neurons. In this series of
experiments, we explore the role of BoNT-A on inhibiting the normal recovery of the
resting tone after stretching. We propose and will study the three possible mechanisms by
which the BoNT-A might influence passive properties:
1. Muscle response to passive stretch is partially controlled by the efferent arm
of the γ-motoneuron pathway. The γ-activation of the intrafusal muscle fibers
utilizes the neurotransmitter (acetylcholine); therefore, γ-motoneurons are
susceptible to the inhibiting effect of BoNT-A [28]. Pharmacological
inhibition with BoNT-A may prevent the intrafusal muscle fibers from
adapting to length changes; therefore, the length sensor for the muscle might
become dysfunctional. This proposed mechanism prevents the whole muscle
from contracting to its normal length after stretching, thus, maintenance of
resting tone may be impaired after BoNT-A injection.
183
2. Stretching of the muscle-tendon unit is sensed by the Golgi tendon organs,
which excite the α-motoneurons to activate muscle contraction. This reflex
loop protects the muscle from damage due to excessive strain. The efferent
arm of the α-motorneurons is inhibited by the injection of the BoNT-A.
Therefore, a percentage of tension initially produced at resting length is
decreased in chemically denervated muscle due to pharmacological, pre-
synaptic, neuromuscular, blockade of transmission that ultimately results in
decreased muscle contractility.
3. Titin has the ability to adapt its stiffness based upon the concentration of
intramuscular calcium [29]. One study reported that calcium induced titin
confirmation changes resulted in a 25% increase in total muscle stiffness [30].
BoNT-A injection may modulate passive in vivo muscle-tendon unit
properties through its indirect interaction with the titin protein [31]. After
BoNT-A injection, the denervated muscle contracts less frequently and each
contraction produces less force. The concentration of intracellular calcium in
BoNT-A denervated muscle is reduced, presumably resulting in a less stiff
titin configuration, contributing to decreased passive tension.
We are also conducting a series of experiments in the mouse gastrocnemius muscle-
tendon unit model that studies structural changes in the skeletal muscle after BoNT-A
injection. Specifically, we will attempt to calculate an in vivo modulus for the muscle-
tendon unit, before and after chemical denervation. This series of experiments will allow
us to characterize the contributions of structural alterations to improved muscle
manipulation versus the neural contributions to improved muscle manipulation.

184
Ultimately, we would like to study the effect of pre-surgical BoNT-A injection on
clinical outcomes following rotator cuff repair surgery. Our department is currently
conducting a double-blinded, placebo-controlled, clinical study testing the role of BoNT-
A on improved operative rotator cuff outcomes. Based on this initial study, we might
propose expanding the use of BoNT-A in future rotator cuff studies.
A BIOENGINEERING APPROACH TO ROTATOR CUFF SURGERY
We are also actively collaborating with our colleagues in biomedical engineering
using our basic-science mathematical findings to drive movement biomechanical
computational analysis of upper extremity motion. This collaboration represents another
source of translational research funding and support. Through this collaborative effort,
we are attempting to develop a laser-diffraction device for the intra-operative evaluation
of z-band distance. With powerful mathematical techniques, we can “scale” our murine
and rodent findings to a human. Further, upper-extremity movement biomechanics
analysis and radiographic imaging in human subjects allows us to test our hypotheses in
our patient populations.
185
REFERENCES
1. Coleman, S.H., et al., Chronic rotator cuff injury and repair model in sheep. J
Bone Joint Surg Am, 2003. 85-A(12): p. 2391-402.
2. Gerber, C., et al., Neer Award 2007: Reversion of structural muscle changes
caused by chronic rotator cuff tears using continuous musculotendinous traction. An
experimental study in sheep. J Shoulder Elbow Surg, 2009. 18(2): p. 163-71.
3. Gerber, C., et al., Effect of tendon release and delayed repair on the structure of
the muscles of the rotator cuff: an experimental study in sheep. J Bone Joint Surg Am,
2004. 86-A(9): p. 1973-82.
4. Oh, J.H., et al., Prognostic factors affecting anatomic outcome of rotator cuff
repair and correlation with functional outcome. Arthroscopy, 2009. 25(1): p. 30-9.
5. Oh, L.S., et al., Indications for rotator cuff repair: a systematic review. Clin
Orthop Relat Res, 2007. 455: p. 52-63.
6. Derwin, K.A., et al., Extracellular matrix scaffold devices for rotator cuff repair. J
Shoulder Elbow Surg. 19(3): p. 467-76.
7. Yamamoto, A., et al., Prevalence and risk factors of a rotator cuff tear in the
general population. J Shoulder Elbow Surg, 2010. 19(1): p. 116-20.
8. Trends in Aging-- United States and Worldwide, 2003, Centers for Disease
Control and Prevention. p. 101-106.
9. Rejeski, W.J., et al., Measuring disability in older adults: the International
Classification System of Functioning, Disability and Health (ICF) framework. Geriatr
Gerontol Int, 2008. 8(1): p. 48-54.
186
10. Delbono, O., Molecular mechanisms and therapeutics of the deficit in specific
force in ageing skeletal muscle. Biogerontology, 2002. 3(5): p. 265-70.
11. Larsson, L., et al., Aging-related changes in skeletal muscle. Mechanisms and
interventions. Drugs & aging, 2000. 17(4): p. 303-16.
12. Raj, I.S., et al., Aging and the force-velocity relationship of muscles.
Experimental gerontology, 2010. 45(2): p. 81-90.
13. Oh, J.H., et al., Effect of age on functional and structural outcome after rotator
cuff repair. The American journal of sports medicine, 2010. 38(4): p. 672-8.
14. Oh, J.H., et al., Prognostic factors affecting anatomic outcome of rotator cuff
repair and correlation with functional outcome. Arthroscopy : the journal of arthroscopic
& related surgery : official publication of the Arthroscopy Association of North America
and the International Arthroscopy Association, 2009. 25(1): p. 30-9.
15. Larsson, L., et al., Effects of ageing on the motor unit. Progress in neurobiology,
1995. 45(5): p. 397-458.
16. Hunter, G.R., et al., Effects of resistance training on older adults. Sports medicine,
2004. 34(5): p. 329-48.
17. Renganathan, M., et al., L-type Ca2+ channel-insulin-like growth factor-1
receptor signaling impairment in aging rat skeletal muscle. Biochemical and biophysical
research communications, 1997. 235(3): p. 784-9.
18. Owino, V., et al., Age-related loss of skeletal muscle function and the inability to
express the autocrine form of insulin-like growth factor-1 (MGF) in response to
mechanical overload. FEBS letters, 2001. 505(2): p. 259-63.
187
19. Payne, A.M., et al., Neurogenesis of excitation-contraction uncoupling in aging
skeletal muscle. Exercise and sport sciences reviews, 2004. 32(1): p. 36-40.
20. Delbono, O., Neural control of aging skeletal muscle. Aging cell, 2003. 2(1): p.
21-9.
21. Frey, D., et al., Early and selective loss of neuromuscular synapse subtypes with
low sprouting competence in motoneuron diseases. The Journal of neuroscience : the
official journal of the Society for Neuroscience, 2000. 20(7): p. 2534-42.
22. Frey, E., et al., Adipogenic and myogenic gene expression in rotator cuff muscle
of the sheep after tendon tear. Journal of orthopaedic research : official publication of the
Orthopaedic Research Society, 2009. 27(4): p. 504-9.
23. Verma, N.N., et al., Outcomes of arthroscopic rotator cuff repair in patients aged
70 years or older. Arthroscopy : the journal of arthroscopic & related surgery : official
publication of the Arthroscopy Association of North America and the International
Arthroscopy Association, 2010. 26(10): p. 1273-80.
24. Romeo, A.A., et al., Repair of full thickness rotator cuff tears. Gender, age, and
other factors affecting outcome. Clinical orthopaedics and related research, 1999(367): p.
243-55.
25. Yamaguchi, K., et al., The demographic and morphological features of rotator
cuff disease. A comparison of asymptomatic and symptomatic shoulders. The Journal of
bone and joint surgery. American volume, 2006. 88(8): p. 1699-704.
26. Soslowsky, L.J., et al., Development and use of an animal model for
investigations on rotator cuff disease. J Shoulder Elbow Surg, 1996. 5(5): p. 383-92.

188
27. Soslowsky, L.J., et al., Neer award 1999 Overuse activity injures the
supraspinatus tendon in an animal model: A histologic and biomechanical study. Journal
of Shoulder and Elbow Surgery. 9(2): p. 79-84.
28. Stampacchia, G., et al., Change of stretch reflex threshold in spasticity: effect of
botulinum toxin injections. Arch Ital Biol, 2004. 142(3): p. 265-73.
29. Labeit, D., et al., Calcium-dependent molecular spring elements in the giant
protein titin. Proc Natl Acad Sci U S A, 2003. 100(23): p. 13716-21.
30. Joumaa, V., et al., The origin of passive force enhancement in skeletal muscle.
Am J Physiol Cell Physiol, 2008. 294(1): p. C74-8.
31. Lieber, R.L., Skeletal muscle structure, function & plasticity : the physiological
basis of rehabilitation. 2nd ed2002, Philadelphia: Lippincott Williams & Wilkins. xii, 369
p.
189
Chapter 6 Figure
Figure 1: Schematic diagram depicting the myotatic reflex arc. The myotatic or stretch
reflex functions as a regulatory sensor for changes in muscle length and contributes to the
resting tone of skeletal muscle. This reflex loop is modulated by the central nervous
system through long-tract pathways:
Voluntary: corticospinal tract (CST): anterior (ant) and lateral (lat)
Postural: Vestibulaspinal Tract (VST), Tectospinal Tract (TST). Rubrospinal Tract (RST)
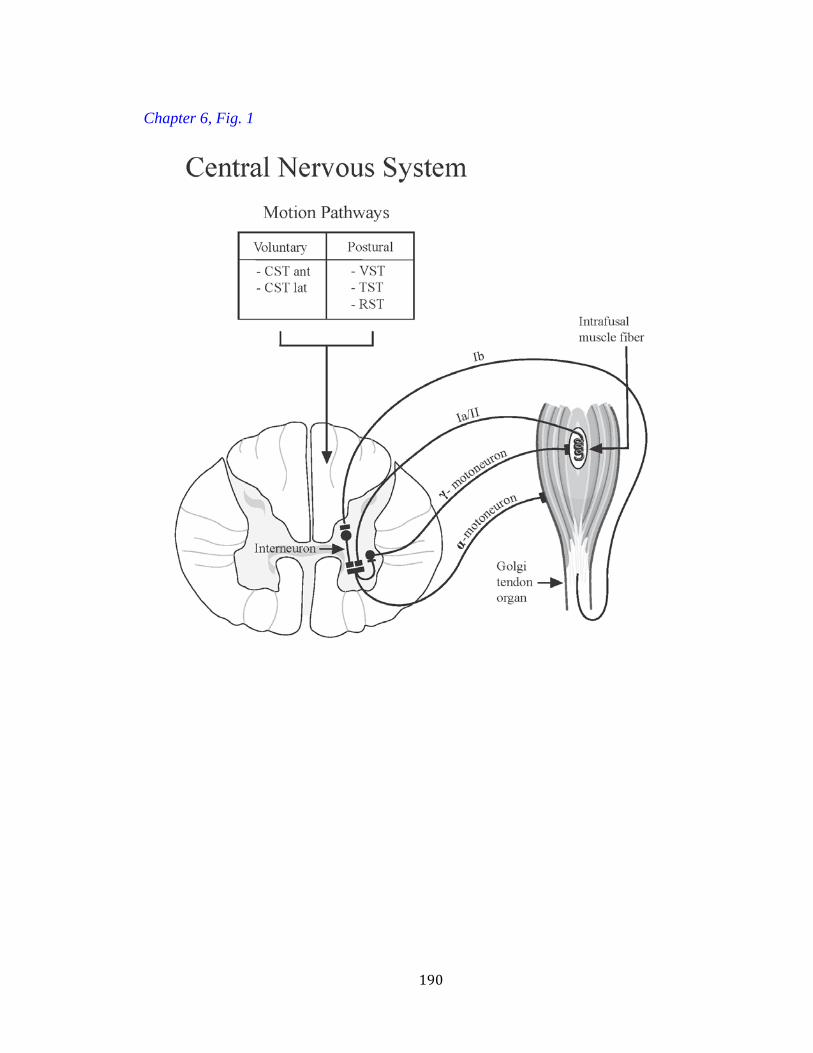
190
Chapter 6, Fig. 1
191
CURRICULUM VITAE
SANDEEP MANNAVA, MD Resident, Physician Scientist Training Program
Department of Orthopaedic Surgery Wake Forest University School of Medicine
EDUCATION
WAKE FOREST UNIVERSITY GRADUATE SCHOOL OF ARTS AND SCIENCES Doctor of Philosophy (Ph.D.), The Neuroscience Program Winston-Salem, North Carolina May 2012 STATE UNIVERSITY OF NEW YORK AT SYRACUSE—UPSTATE MEDICAL UNIVERSITY Doctor of Medicine (M.D.) Syracuse, New York May 2009 CORNELL UNIVERSITY Bachelor of Science (B.S), Biological Sciences (concentration: Animal Physiology) Cum Laude, High Honors in Biology, Distinction in Research Ithaca, New York May 2005
TEACHING
Clinical Volunteer Faculty Facilitator at the Wake Forest University School of Medicine: • Case Centered Learning Course (1st year medical student curriculum 2009-2010) • Standardized Patient Assessment (2nd year medical student curriculum 2011) • Standardized Patient Assessment (1st year medical student curriculum 2011-2012)
PROFESSIONAL SOCIETIES
Orthopaedic Research Society—Associate Member American Academy of Orthopaedic Surgery—Resident Member Society for Neuroscience (SfN)—Student Member Biomedical Engineering Society (BMES)—Student Member

192
RESEARCH SUPPORT
Principal Investigator: Orthopaedic Research and Education Foundation Resident Clinician Scientist Training Grant ($20,000) Title: The Effect of Age on Tendon-to-Bone Healing: A Biomechanical and Histological Assessment of Surgically Repaired Rotator Cuffs PI: Sandeep Mannava Co-I: Thomas L. Smith (mentor/sponsor), Joel D Stitzel, Christopher J Tuohy Co-Investigator: Wake Forest University Intramural Research Grant Re-Submission ($20,000) Title: Optimization of bioreactor preconditioning protocols for the maturation of seeded, naturally-derived scaffolds PI: Christopher J Tuohy Co-I: Sandeep Mannava, Thorsten M Seyler, Thomas L Smith, Patrick W Whitlock
PEER-REVIEWED MANUSCRIPTS
1. Plate JF, Haubruck P, Walters J, Mannava S, Smith BP, Smith TL, Tuohy CJ. Rotator Cuff Injuries in Professional and Recreational Athletes. Accepted for publication in J Surg Orthop Adv, March 6, 2012. IN PRESS
2. Lang JE, Mannava S, Floyd AJ, Goddard MS, Smith BP, Modifi A, Jinnah RH. Robotic Systems in Orthopaedic Surgery. JBJS (Br.). 2011 Oct;93(10):1296-9.
3. Mannava S, Plate JF, Stone AV, Smith TL, Smith BP, Koman LA, Tuohy CJ. Recent advances for the management of Raynaud phenomenon using botulinum neurotoxin A. J Hand Surg (Am.). 2011 Oct;36(10):1708-10. PMID 21903346.
4. Mannava S. Plate, JF, Seyler, TM, Whitlock, PW, Callahan, MF, Koman, LA, Smith, TL, Tuohy, CJ. Evaluation of in vivo rotator cuff muscle function after acute and chronic detachment of the supraspinatus tendon: an experimental study in an animal model. JBJS (Am.). 2011 Sept 21;93(18):1702-11. PMID: 21938374
5. Saul KR, Hayon S, Smith TL, Tuohy CJ, Mannava S. Postural dependence of
passive tension in the supraspinatus following rotator cuff repair: a simulation analysis. J Clin Biomech. 2011 Oct;26(8):804-10. PMID: 21596463
193
6. Mannava S, Wiggins WF, Saul KS, Stitzel JD, Smith BP, Koman LA, Smith TL, Tuohy CJ. Contributions of Neural Tone to In Vivo Passive Muscle-Tendon Unit Biomechanical Properties in a Rat Rotator Cuff Animal Model. Ann of Biomed Eng. 2011 Mar 29. PMID: 21445691
7. Mannava S, Callahan MF, Trach SM, Wiggins WF, Smith BP, Koman LA,
Smith TL, Tuohy CJ. Chemical Denervation with Botulinum Neurotoxin A Improves the Surgical Manipulation of the Muscle-Tendon Unit: An Experimental Study in an Animal Model. J Hand Surg Am. 2011 Feb;36(2):222-31. PMID: 21276885
8. Otani NF, Mo A, Mannava S, Fenton FH, Cherry EM, Luther S, Gilmour RF Jr.
Characterization of multiple spiral wave dynamics as a stochastic predator-prey system. Phys Rev E Stat Nonlin Soft Matter Phys. 2008 Aug; 78(2 Pt 1):021913. PMID: 18850871
9. Burashnikov A, Mannava S, Antzelevitch C. Transmembrane action potential
heterogeneity in the canine isolated arterially perfused right atrium: effect of IKr and IKur/Ito block. Am J Physiol Heart Circ Physiol. 2004 Jun;286(6):H2393-400. PMID: 15148061

194
BOOK CHAPTERS
1. Brown PJ, Plate JF, Mannava S, Stitzel JD. Injury Mechanisms of Five Common Sports Related Orthopaedic Injuries. Orthopaedic Biomechanics. Beth Winklestein, editor. Submitted July 8, 2011 to CRC/Taylor and Francis Publishing Company. IN PRESS.
2. Whitlock PW, Seyler TM, Mannava S, Poehling GG. A tissue-engineered approach to ligament and tendon reconstruction. Sports Injuries: Prevention, Diagnosis, Treatment, Rehabilitation. Editors: Mahmut Doral et al. Springer. 1st Edition., 2011, XII, 1020 p. 706 illus., 481 in color., Hardcover SBN: 978-3-642-15629-8. DOI: 10.1007/978-3-642-15630-4_157, © Springer-Verlag Berlin Heidelberg 2011
THESIS TITLES
1. Mannava S. (2012). The Neurological Mechanisms Underlying Rotator Cuff Skeletal Muscle Pathophysiology and Implications for Therapy. Wake Forest University Graduate School of Arts and Sciences. Doctoral Thesis (The Neuroscience Program)
2. Mannava S, Otani NF, Gilmour RF. (2005). The Predator-Prey Relationship in
2D Spiral Wave Simulations. Cornell University Undergraduate Honors Thesis.
UNITED STATES PATENT
Mannava S, Tanaka MF, Tuohy CJ. Tissue tensioning devices and related methods. Utility Patent Application No. 12/942,311 filed November 9, 2010 in United States Patent and Trademark Office MULTIMEDIA/VIDEO: • Case JM, Mannava S, Cheetham S, Long BJ, Stubbs AJ. Physical Examination of the
Shoulder. [MULTIMEDIA/VIDEO]. AAOS 2012 Annual Meeting. San Francisco, CA. February 7, 2012. Selected as a FEATURED PRESENTATION
ABSTRACTS AND MEETING PRESENTATIONS
1. Mannava S, Plate JF, Seyler TM, Whitlock PW, Callahan MF, Smith TL, Tuohy CJ. Muscle function after rotator cuff injuries in an animal model. [ABSTRACT].
195
Surgical Sciences Research Day. Wake Forest University School of Medicine. Winston-Salem, NC. November 19, 2009.
2. Mannava S, Plate JF, Seyler TM, Tuohy CJ, Callahan MF, Koman LA, Smith
TL. Evaluation of Rotator Cuff Muscle Dysfunction. [ABSTRACT]. 10th Annual Graduate Student Research Day, Spring 2010. Wake Forest University Graduate School of Arts and Sciences. Winston-Salem, NC.
3. Mannava S, Plate JF, Seyler TM, Whitlock PW, Callahan MF, Smith TL, Tuohy
CJ. The pathophysiology of rotator cuff dysfunction and implications for therapy: A series of related in vivo animal studies. [ABSTRACT]. Resident Research Day. Wake Forest University School of Medicine. Winston-Salem, NC. April 16, 2010.
4. Mannava S, Plate JF, Seyler TM, Callahan MF, Smith TL, Koman LA, Tuohy
CJ. Novel Use of Electromyography (EMG) to Evaluate In Vivo Rotator Cuff Muscle Function After Acute and Chronic Detachment of the Supraspinatus Tendon: An Experimental Study in an Animal Model. [ABSTRACT]. Poster Presentation at the Southern Orthopaedic Association 2010 Annual Meeting, Fajardo, Puerto Rico.
5. Mannava S, Plate, JF, Seyler, TM, Callahan MF, Smith TL, Koman LA, Tuohy
CJ. Evaluation of In Vivo Rotator Cuff Muscle Function After Acute and Chronic Detachment of the Supraspinatus Tendon: An Experimental Study in an Animal Model. [ABSTRACT]. Podium Presentation at the Southern Orthopaedic Association 2010 Annual Meeting, Fajardo, Puerto Rico.
6. Mannava S, Wiggins WF, Callahan MF, Smith TL, Koman LA, Tuohy CJ.
Innovations in the management of complex and chronic tendon injuries. [ABSTRACT] Podium Presentation at the North Carolina Orthopaedic Association 2010 Annual Meeting. Asheville, NC.
7. Tuohy CJ, Plate JF, Callahan MF, Koman LA, Smith TL, Mannava S.
Pathophysiologic Mechanisms of Rotator Cuff Dysfunction and Implications for Therapy. [ABSTRACT] Podium Presentation at the North Carolina Orthopaedic Association 2010 Annual Meeting. Asheville, NC.
196
8. Mannava S, Plate JF, Callahan MF, Smith TL, Tuohy CJ, Koman LA. Evaluation of In Vivo Muscle Function After Rotator Cuff Tears Using Electromyography in an Animal Model. [ABSTRACT] Podium Presentation at the Eastern Orthopaedic Association 2010 Annual Meeting. Naples, FL. TRAVEL AWARD WINNING PAPER.
9. Mannava S, Wiggins WF, Stitzel J, Callahan MF, Koman, LA, Smith TL, Tuohy
CJ. Contributions of neural tone to muscle-tendon unit stress-relaxation biomechanical properties. [ABSTRACT] Podium Presentation at the Biomedical Engineering Society (BMES) 2010 Annual Meeting. Austin, TX. TRAVEL AWARD WINNING PAPER.
10. Holzbaur KS, Hayon S, Smith T, Tuohy C, Mannava S. Passive tension in
supraspinatus following rotator cuff repair: a simulation analysis. [ABSTRACT] Podium Presentation at the Biomedical Engineering Society (BMES) 2010 Annual Meeting. Austin, TX. TRAVEL AWARD WINNING PAPER.
11. Mannava S, Wiggins WF, Callahan MF, Stitzel J, Koman, LA, Tuohy CJ, Smith
TL. Neurological influences and modulation of skeletal muscle tone. [ABSTRACT] Poster Presentation at the Society for Neuroscience (SfN) 2010 Annual Meeting. San Diego, CA.
12. Mannava S, Tuohy CJ, Seyler TM, Stitzel J, Hayon S, Whitlock PW, Smith TL,
Saul KR. The Science of Rotator Cuff Repairs: Translating Basic Science into Clinical Recommendations. [Scientific Exhibit ABSTRACT] Presentation at the AAOS 2011 Annual Meeting. San Diego, CA. SELECTED AS A TOP 20 EXHIBIT.
13. Mannava S, Seyler TM, Pace LA, Whitlock PW, Smith BP, Koman LA, Smith
TL, Tuohy CJ. Age-Related Changes Affect Supraspinatus Muscle Function: An Experimental Study in an Animal Model. [ABSTRACT] Presentation at the ORS 2011 Annual Meeting. San Diego, CA.
14. Sikes CV, Brown PJ, Danelson KA, Seyler TM, Mannava S, Jinnah RH, Stitzel
JD, Lang JE. Biomechanical Analysis of Hip Core Decompression Techniques and Fracture Risk. [ABSTRACT] Presentation at the ORS 2011 Annual Meeting. San Diego, CA.
197
15. Mannava S, Saul KR, Seyler TM, Koman LA, Smith TL, Tuohy CJ. Rotator Cuff
Dysfunction After Acute and Chronic Tears: Translating Animal Studies to Clinical Recommendations Using Simulation Analysis. [ABSTRACT] Presentation at the 2010 OREF / ORS Atlantic Coast Resident Research Symposium—Duke University. Durham, NC.
16. Mannava S, Saul KR, Plate JF, Seyler TM, Koman LA, Tuohy CJ, Smith TL.
Rotator Cuff Dysfunction After Acute and Chronic Tears: Translating Animal Studies to Clinical Recommendations Using Simulation Analysis. [ABSTRACT] Surgical Sciences Research Day. Wake Forest University School of Medicine. Winston-Salem, NC. November 11, 2010. GOLD MEDAL WINNER OF BASIC SCIENCE AWARD
17. Mannava S, Wiggins WF, Saul KR, Stitzel J, Koman, LA, Tuohy CJ, Smith TL.
Chemical Denervation with Botulinum Neurotoxin A Modulates Skeletal Muscle Tone: Assessment of Neural Contributions to In Vivo Soft-Tissue Biomechanics. [ABSTRACT] Poster Presentation at the Western North Carolina Society for Neuroscience (SfN).Wake Forest University School of Medicine. Winston-Salem, NC. November 11, 2010.
18. Pace LA, Hill P, Garrett J, Ma J, Apel P, Mannava S, Barnwell J, Smith B, Li Z,
Koman LA, Smith T, Van Dyke M. Clinical Translation of a Keratin Biomaterial Hydrogel for Nerve Repair. [ABSTRACT] Podium Presentation at NCTERM 2010.
19. Pace LA and Mannava S. Clinical Translation of a Keratin Biomaterial Hydrogel
for Nerve Repair: From Mice to Men. [Invited Lecture]. Wake Forest University School of Medicine, Regenerative Medicine Interest Group. Winston-Salem, NC. January 21, 2011.
20. Mannava S, Koman LA, Seyler TM, Plate JF, Tuohy CJ, Saul KR, Smith TL.
Translating Animal Studies to Clinical Recommendations with Computational Analysis for the Study of Rotator Cuff Dysfunction After Acute and Chronic Tears. [ABSTRACT] 11th Annual WFU Post-Doctoral Research Day. March 2011. Winston-Salem, NC. AWARD WINNER (runner-up): INTEGRATIVE SCIENCES CATEGORY.
198
21. Mannava S, Plate JF, Seyler TM, Whitlock PW, Saul KR, Smith TL, Tuohy CJ.
The Science of Rotator Cuff Repairs: Translating Basic Science into Clinical Recommendations. [ABSTRACT]. Resident Research Day. Wake Forest University School of Medicine. Winston-Salem, NC. April 1, 2011.
22. Schweppe ML, Goddard MS, Mannava S, Plate JF, Seyler TM, Lang JA.
Accuracy of Component Positioning and the Associated Learning Curve of the Direct Anterior Approach in Total Hip Arthroplasty. [ABSTRACT]. Resident Research Day. Wake Forest University School of Medicine. Winston-Salem, NC. April 1, 2011.
23. Tuohy CJ, Plate JF, Pace LA, Saul KR, Koman LA, Smith TL, Mannava S. Age-
related changes affect rotator cuff muscle function. [ABSTRACT]. Eastern Orthopaedic Association Annual Meeting. Williamsburg, VA. October 19, 2011.
24. Koman LA, Plate JF, Mannava S, Stone AV, Jinnah RH, Smith TL. Plate JF,
Pace LA, Saul KR, Addressing The Shortage of Academic Orthopaedic Surgeons: Evaluation of an Innovative Seven-Year Physician Scientist Residency Training Program. [ABSTRACT]. Eastern Orthopaedic Association Annual Meeting. Williamsburg, VA. October 19, 2011.
25. Smith TL, Haubruck P, Saul KR, Wiggins WF, Stitzel JD, Smith BP, Tuohy CJ, Mannava S. In vivo biomechanics of neural mechanisms influencing stretching of the muscle-tendon unit. [ABSTRACT]. Biomedical Engineering Society Annual Meeting. Hartford, CT. October 12, 2011.
26. Plate JF, Mannava S, Seyler TM, Saul KR, Pace LA, Smith TL, Tuohy CJ. Age Influences Healing and Function of Rotator Cuff Muscles. [ABSTRACT]. North Carolina Orthopaedic Association. Kiawah Island, SC. October 7, 2011.
27. Haubruck P, Mannava S, Schmidmaier G, Smith BP, Saul KR, Koman LA, Tuohy CJ, Smith TL. Bioprotection of the muscle-tendon unit improves surgical manipulation in an animal model. [ABSTRACT]. European Orthopaedic Research Society 2011 Annual Meeting. Vienna, Austria.
199
RESEARCH POSITIONS AND EMPLOYMENT
2009-present Physician Scientist/Resident, Department of Orthopaedic Surgery Wake Forest University School of Medicine Post-Doctoral Research Fellow Wake Forest University Institute For Regenerative Medicine (Mentors: Thomas L. Smith, PhD and L. Andrew Koman, MD)
2006-2007 Graduate Research Assistant, State University of New York at Syracuse -
Upstate Medical University, Department of Pharmacology, Patch Clamp Analysis of Ion Channel Dynamics in Heart Failure and Fibrillation (Ik1 and Gap Junctions) (Mentor: Justus MB Anumonwo, PhD)
2004-2005 Research Assistant, Cornell University
Department of Biomedical Sciences Mathematical Modeling Of Ventricular Fibrillation Using Small-World Network Theory, Scale Free Network Theory, and The Predator-Prey Differential Equation Model (Mentor: Robert F. Gilmour Jr, PhD)
2003 Urban Semester Student, Weill Cornell Medical School
Department of Physiology and Biophysics Three Dimensional Characterizations of Ventricular Fibrillation and Real Time Fibrillation Control (Mentor: David J Christini, PhD)
2002-2003 Summer Research Fellow, Masonic Medical Research Laboratory,
Department of Experimental Cardiology Studied Electrical Conduction Heterogeneity During Atrial Fibrillation (Mentor: Charles Antzelevitch, PhD)

200
AWARDS AND HONORS
• Wake Forest University 11th Annual Graduate Student and Post-Doc Research Day, March 22, 2011. Integrative Sciences Category (RUNNER-UP Paper)
• Wake Forest University School of Medicine Surgical Science Basic Science Award, First Place (2010)
• Wake Forest University Graduate School of Arts and Sciences, Alumni Student Award (2010)
• Eastern Orthopaedic Association Travel Award (2010)
• Howard Hughes Research Scholarship (2004)
• American Heart Association Award (2004)
• Masonic Medical Research Laboratory Summer Fellowship (2002 and 2003)