Neurological assessment of head injuries using the … · Web view– Cranial and spinal nerves...
128
Cheshire and Mersey Critical Care Network Neuro Critical Care Work Book 1
Transcript of Neurological assessment of head injuries using the … · Web view– Cranial and spinal nerves...

Cheshire and Mersey Critical Care Network
Neuro Critical Care Work Book
Workbook Series
Number: xx1

Created by
Helen Jones RGN, MSC, Local Service Improvement Lead and Senior Sister, the Walton Centre for
Neurology & Neurosurgery NHS Trust.
Acknowledgement: Professor P Eldridge, Neurosurgical Consultant, the Walton Centre for
Neurology & Neurosurgery NHS Trust
Version 1 May 2012
Status Final
Changes H Jones
Review date 2014 May
Author Helen Jones
Owner Cheshire and Mersey Critical Care Network
CONTENTS Page
2

Introduction 4
Terminology 9
Anatomy and Physiology 10
Neurological conditions in critical care 33
Neurological assessment 43
Traumatic Brain Injury 60
Sedation scoring 80
Subarachnoid haemorrhage 89
Competencies and records of supervised practice
INTRODUCTION
3

This workbook has been produced to assist healthcare professionals in critical care in caring for
patients with intracranial injury and disease. Many of these patients require admission to critical
care and application of subsequent treatments to prevent secondary problems.
The book provides information regarding normal physiology, pathophysiology and neurological
assessment.
To determine your competence you are required to complete the following: -
Attendance at formal Trust/Unit training sessions.
Successful completion of the workbook.
Competency assessment
How to use this workbook
The workbook is divided into sections. There are questions and activities included which form an
important part of your learning and training. Please attach separate sheets if needed. It is your
evidence of learning.
You will need to obtain and read several documents to assist you in completing this workbook and you
will require access to books and other reference materials (see bibliography). When completed this
workbook will form part of your evidence of learning, professional development and competence. Please
keep this package in your portfolio as it could be used to gain further credits at university or college and
assist in meeting KSF and national competency requirements.
To help you with this work book, you need to revise the following:
Physiology of the brain and spinal cord, GCS
4

Learning Outcomes
Having completed this pack you will be able to: -
State the gross functions of the nervous system
Demonstrate a basic understanding of neurological conditions which may require critical care
Assess a patient using the Glasgow Coma Scale
Demonstrate an understanding of the pathophysiology of head injury
Demonstrate understanding of raised intracranial pressure and treatment options
Demonstrate an understanding of sedation use in critical care
Demonstrate an understanding of Subarachnoid haemorrhage and treatment
Expanded Scope of Practice (Nursing)
Nursing the head injured and neurologically compromised patient requires advanced
understanding of physiology and the mechanism of injury not covered in nurse training. Additional
training is therefore required to ensure competency in this area.
In line with the Scope of Professional Practice (NMC, 2008) the Cheshire and Mersey Critical Care
Network views practice from the following two perspectives: -
Clinical Practice
Clinical practice may be defined as an aspect of care, which may be undertaken by
Nurses/Midwives/Others who accept accountability for their actions and feel competent to
undertake a procedure. There is no formal assessment for these practices but there may be aspects
of care, which require a period of supervised, guided practice. This should form part of
preceptorship/mentorship or supervision programmes.
5

Expanded Practice
An expanded scope of practice may be defined as an aspect of care which may be undertaken by
Registered Nurses who have undergone the specified training and assessment, accept
accountability for their actions, feel competent to undertake the aspect of care, and have the
authority of the Trust to do so.
Professional implications
The publication of The Scope of Professional Practice by the NMC (2008) was an acknowledgement
that practice takes place in a context of continuing change and development. The principles on
which any development in the scope of practice must evolve are as follows:
1. The interests of the patient must predominate.
2. The practitioner must maintain their knowledge, skill, and competence.
3. The practitioner must also acknowledge the limits of their knowledge, skill, and
competence.
4. The practitioner must not jeopardise standards and must comply with the Code of Conduct.
5. The practitioner must recognise their direct and personal accountability.
6. The practitioner must avoid inappropriate delegation.
Nurses are first and foremost legally responsible for each and every nursing action undertaken or
omitted, and must practice in accordance with the standard of care of a reasonably prudent nurse
practicing under the same or similar circumstances.
The law relating to negligence principally seeks to identify conduct that does not reach an acceptable
professional standard. The registered nurse owes the patient in her care an individual and personal
duty of care. The duty of care encompasses the professional, moral, ethical, and sociological sphere
within which nursing operates. Deviation from this in any way is negligence. The individual holds
6

primary liability for his or her own actions. If the patient suffers harm from the nurse’s negligent
action or omissions, that nurse remains primarily liable, and could be sued directly.
ACTIVITY 1
Locate the following documents and familiarise yourself with their contents:
NMC - Code of Professional Conduct
NMC - The Scope of Professional Practice
For all procedures consult The Royal Marsden Manual (Dougherty et al, 2004)
Trust/Unit incident reporting policy
Medical Device/Equipment Guidelines
Trust frameworks, guidelines, protocols and documentation related to neuro critical care.
NB. To help you with this workbook, you also need to revise the physiology of the nervous system.
ACTIVITY 2
Describe why you are undertaking learning in neuro critical care
- To update / increase clinical skills and knowledge.
- Part of personal development.
7

- Function as effective member of the Critical Care team
- Participate in attempts to reduce related clinical incidents as an effective knowledgable practitioner.
ACTIVITY 3
How will you demonstrate your knowledge and competence following this training?
- Completion and assessment of the workbook
- Attend related training sessions, courses and conferences
- Self-assessment and review of personal practice
- Professional Development and peer reviews
- Incident free and safe clinical practice
TERMINOLOGY
TBI Traumatic Brain Injury
GCS Glasgow Coma Scale
EVD Extra Ventricular Drain
ICP Intracranial pressure
CPP Cerebral perfusion pressure
8

CSF cerebrospinal fluid
MAP mean arterial pressure
CNS central nervous system
PNS peripheral nervous system
SAH Subarachnoid haemorrhage
Normal A&P of the nervous system – a brief overview
It is essential to have background knowledge of anatomy and physiology in order to effectively
deliver care. This knowledge will enable you to recognise the abnormal and ensure timely
interventions are initiated. In the following section there will be an overview of this complex system.
Further reading is suggested to consolidate learning.
Section objectives:
9

1. Identify the structures within the nervous system
2. Understand how impulses are transmitted
3. Identify functions of the nervous system
Introduction:
The nervous system is the mechanism by which the body responds to environmental and
physiological changes, and creates the basis for all voluntary activity. The mechanism is principally
electrochemical and virtually all the energy consumption of the nervous system is devoted to
maintaining this system. A reflection of this is that the brain uses 20% of the oxygen consumed by
the body, 15% of the cardiac output although being less than 1% of the total mass of the individual.
It is increasingly being realised that the brain is also a highly plastic system; much more so than
previously appreciated. Put very simply, the nervous system gathers information, acts on it and has
the ability to store it. It is divided into parts:
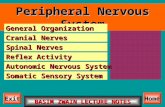
Peripheral – Cranial and spinal nerves that connect the body to the brain and spinal cord
Central – The brain and spinal cord
Autonomic – Part of the peripheral nervous system that controls automatic functions which have no conscious control, anatomically located within both the central and peripheral parts of the nervous system
fig 1 (mstrust.org.uk)
10

Nerve cells are called neurones and they are supported by neuroglia. Glial cells are located within
the central nervous system and provide a supportive medium, provide nutrients in particular for
synaptic function and have a role in repair after injury. They actually make up around 70% of brain
cells therefore it should come as no surprise that many brain tumours arise from glial cells. Glial cells
can be sub divided into types such as astrocytes and oligodendrocytes.
Myelinated cells conduct impulses more rapidly than others because they jump between junctional
stations called nodes of ranvier. Peripheral nerves and the 12 cranial nerves have this insulating
myelin sheath along the fibre, created by Schwann cells. For the central nervous system the myelin is
created by oligodendrocytes.
There are three types of neurones which ensure communication exists between the environment
and our body.
Motor neurone
Sensory neurone
Interneurone
Interaction between these neurones is critical for control.
The motor neurones act upon organs and muscles. Because they carry instructions from the brain
and they are efferent neurones. The impulse travels from the cell body, down the axon and
eventually to the organ or muscle it supplies.
The sensory neurone receives information from the environment such as heat, cold, pain, touch and
therefore is an afferent neurone.
Efferent = output Afferent = input
An example of this you can see literally with your own eyes is the consensual light reflex. If you
shine a pen torch in one pupil it will constrict. Look over to the other pupil and you will see that this
also has constricted at the same time. This is because the afferent message from the stimulated
retina has travelled to the brain and the efferent pathway via the oculomotor nerve III has sent a
message to the other pupil to respond in the same way. This is why it is important to look at both
eyes to compare responses when assessing reaction to light. Try it in the mirror! This is an example
of how the system of neurones modulates constantly according to stimulus.
11

Modulation can be described as ‘gating’. Another example is the gate theory relating to pain
perception. A nociceptor is a sensory receptor that sends signals that cause the perception of pain in
response to potentially damaging stimulus.
Fig 2
(http://faculty.washington.edu/chudler/pain.html)
The inhibitory neurone (I) will block or ‘gate keep’ and not allow signals to pass to the projection
neurone and on to the brain.
When the stimulus is simply non painful touch then the large fibres activate and the inhibitory neurone blocks the signal and there is no perception of pain.
When there is pain the signal is sent through the small nerve fibres to the projection neurone but this time the small nerve fibres block the inhibitory neurone and pain is perceived
Blocking pain or closing the pain gate is central to pain management. In chronic pain states this modulation may behave abnormally, sometimes becoming hypersensitive so that the pain persists long after the cause of the pain has been removed.
The interneurone transfers impulses, via synapses, between the sensory and motor neurones. At a simple level this creates reflex activity; when passed though the spinal cord to the brain via many “interneurons” it forms that basis of complex voluntary activity.
How is a nervous impulse transmitted?
12

Fig 3
Sodium and Potassium are charged ions. The inside of the cell is positively charged and the outside
of the cell is negatively charged. When sodium and potassium swap between the cell membrane and
the exterior of the cell this causes the electrical impulse to travel.
Once at the end of the cell the impulse must be carried across the gap (synapse) to the next cell.
Chemical transmitters are required to do this job. The electrical energy of the impulses releases the
transmitter into the narrow synaptic gap where the chemical binds to a specific receptor which
depolarises the nerve starting off a new electrical impulse in the next nerve. The same mechanism
activates muscles, where an efferent nerve fibre ends on a muscle – “the motor end plate”
Neurotransmitters include
Dopamine (low in Parkinson’s disease)
Serotonin
Acetylcholine (low in myasthenia gravis)
Adrenalin and nor-adrenaline
There are at least 50 neurotransmitters.
13

Fig 4
Activity:
What drugs do we use in critical care which affect chemical transmitters and in what situations? Write down as many as you can think of and read about how they act. Here is a starter:
1. Atracurium – a non-depolarising neuromuscular blocking drug used as a skeletal muscle
relaxant in rapid sequence induction for intubation. It blocks the effect of acetyl choline at
the motor endplate
2. ………………..
3. ………………..
4. ………………..
The peripheral nervous system.
14

This is divided into the autonomic nervous system which represents involuntary control of internal
organs such as blood vessels, cardiac muscles, smooth and visceral muscles; the ANS is further split
into the sympathetic and parasympathetic systems which work together to excite or inhibit
responses.
The somatic nervous system controls skeletal muscle, bones and joints.
Fig 5.
Organ Sympathetic System Parasympathetic System
Eye
Tear glands
Salivary glands
Lungs
Heart
Gut
Liver
Bladder
Dilates pupil
No effect
Inhibits saliva production
Dilates bronchi
Speeds up heart rate
Inhibits peristalsis
Stimulates glucose production
Inhibits urination
Constricts pupil
Stimulates tear secretion
Stimulates saliva production
Constricts bronchi
Slows down heart rate
Stimulates peristalsis
Stimulates bile production
Stimulates urination
Fig 6.
Somatic nervous system:
15

Reflex arc.
Fig 7. www.sciencegeek.net
The pain stimulus is transmitted up the afferent sensory neurone and then to the interneurone
within the spinal cord. The interneurone then relays the stimulus to the efferent motor neurone. The
muscle receives the stimulus and reacts. This reflex response can be elicited without the
involvement of the brain therefore does not reflect brain function and can be observed in a brain
dead patient. In order to increase reliability when testing a response to painful stimuli it is
recommended to locate a cranial nerve and exert pressure, this also increases reliability if there is a
high spinal injury.
16

Gross structures.
Fig 8
The brain and spinal cord are protected by bone (vertebrae and skull). Protection is further provided
by the meninges which exist in three membranous layers; the dural mater, arachnoid mater and pia
mater. In addition to these layers, the brain and spinal cord float in cerebrospinal fluid (CSF) which
circulates freely in the subarachnoid space. This fluid is produced at a rate of approximately 550ml
per day by the choroid plexus (about 70% of the total) and cells lining the ventricles. The fluid passes
out of the brain via the ventricles and there connecting channels, to pass over the surface of the
brain to be reabsorbed at the same rate into the venous sinuses. If there is a problem with
reabsorption such as blood from a subarachnoid haemorrhage clogging the system, then
hydrocephalus will develop (a build up of CSF). A lesion such as a tumour could also press down on
the communicating canals in the system and also cause hydrocephalus. A shunt can be inserted to
off load excess CSF. In the short term external ventricular drains can be used (EVD).
17

Fig 9 The CSF pathways.
The main network of arteries are found in the subarachnoid space. The four major arteries entering the skull are linked to form the Circle of Willis.
Fig 10. The Circle of Willis.
Cerebral aneurysms can form and if ruptured cause a subarachnoid haemorrhage.
The cerebrum.
The right and left cerebral hemispheres make up this structure. They are connected by the corpus
callosum. They receive afferent sensory information and send out efferent motor responses. The
cerebral cortex is a thin layer of cell nuclei (grey matter). White fibre tracts connect the nuclei to
synapse with other grey matter areas deeper in the brain.
18

http://www.bioon.com/book/biology/whole/image/1/1-6.tif.jpg Fig 11
Gyri are the worm like ridges which can be seen over the brain surface. Sulci are the grooves dividing
the gyri. Fissures are deeper divisions and there are fissures which are anatomically significant; the
Longitudinal fissure which divides the two hemispheres, the Transverse fissure which divides the
cerebellum from the cerebrum and the Sylvian fissure which divides the temporal lobe from the
frontal and parietal lobe.
The lobes of the brain.
Fig 12
19

Fig 13
Frontal Lobe
Primary motor cortex which controls motor movement of the opposite side of the body.
Fig 14
Representation of body of the motor strip of the frontal lobe. Not how the hands and feet and mouth have a larger representation.
20

Fig 15
Wernicke’s area (temporal lobe) – damage here would result in difficulty comprehending speech
(receptive dysphasia)
Broca’s area (frontal lobe) – Damage here would affect speech production although speech is
comprehended (expressive dysphasia)
The frontal lobe also controls emotions, regulates responses to social situations, controls executive decision making and goal directed problem solving.
The Parietal lobe.
Its major function is to integrate senses and provide spatial awareness. It processes tactile and
proprioceptive information, assists in visual cortex and motor communication, interprets taste
sensation. The body is represented in a sensory strip in a similar way to the motor strip:
21

Fig 16.
Note how the sensory parts of the body have a larger representation in the sensory strip of the
parietal lobe..
The occipital lobe.
This is the primary visual area. It interprets visual stimuli. The primary visual cortex processes size,
colour, light and motion.
The temporal lobe.
The main functions are; hearing, organisation and understanding language, memory formation and
retrieval.
All the lobes of the brain communicate with each other via feedback pathways. Further reading is
recommended to fully appreciate their functions.
The Diencephalon.
Within the brain are further structures with complex roles. The higher thought functions are to be
found nearer to the lobe surfaces and the more primitive and emotional functions can be found at
greater depths. Sometimes referred to as the ‘emotional brain’ this system is made up of grey
matter areas each with important roles. The Diencephalon is located above the brain stem.
22

Fig17
The AmygdalaStores emotional memories and has a role in producing and regulating hormone release for
emotional responses such as fight / flight .
The Hippocampus
Memory formation, classifying information, long-term memory storage, sense of space and location
are the main roles of this structure found deep in the temporal lobe.
The Hypothalamus
It is located deep within the brain and above the brain stem. It communicates closely with the
pituitary gland which controls many of the body’s functions via hormonal control. The Hypothalamus
has many roles:
Temperature regulation
Thirst and control of body water Appetite control
Endocrine control
Emotional reactions
Sleep and wakefulness
23

Stress response
The ThalamusThis is the relay station which receives afferent and efferent signals therefore the Thalamus the main
relay station in the brain. Most of the sensory signals; auditory, Visual, Somatosensory (from your
skin and internal organs), go through this region on their way to other parts of the brain for
processing. It also plays a function in motor control.
The basal ganglia.
Fig 18
Either side of the Thalamus are grey matter areas called the Basal Ganglia. The many areas have complex functions which include:
Control of the need to act upon an environmental stimuli such as hand washing when dirty, locking a door to keep safe.
Control of mood
Controlling automatic behaviours such as balancing when riding a bike
Control of movement
One of the main neuro transmitters used here is dopamine. It is degeneration in this area,
specifically the Substantia Nigra, which contributes to Parkinson’s disease.
24

The Brain Stem.
Fig 19
Mid brain
Pons
Medulla
Cranial Nerves III – XII have their nuclei in the brain stem.
Midbrain.
Is located above the pons and helps to regulate muscle tone, plays a role in auditory and visual
reflexes and co-ordination of movement.
Pons.
Main function is breathing regulation / respiratory drive.
Medulla Oblongata.
Merges into the spinal cord and includes important fiber tracts. It contains important control
centres:
Heart rate control
Blood pressure regulation
Breathing
Swallowing / gag
25

Cranial Nerves.
There are 12 pairs of cranial nerves. They do not cross over and so supply the same side of the body. III – XII originate in the brain stem.
Fig 20
Cranial Nerve: Major Functions:
I Olfactory smell
II Optic vision
III Oculomotor eyelid and eyeball movement, pupil constriction
IV Trochlear innervates superior obliqueturns eye downward and laterally
V Trigeminal chewing face & mouth touch & pain
VI Abducens turns eye laterally
VII Facial controls muscles of facial expression secretion of tears & salivataste
VIII Vestibulocochlear(auditory) hearing
26equilibrium, balance
IX Glossopharyngeal taste senses carotid blood pressure
X Vagus
senses aortic blood pressure slows heart rate stimulates digestive organstasteVocal cords
XI Spinal Accessory controls trapezius & sternocleidomastoidcontrols swallowing
XII Hypoglossal controls tongue movements
26

Key point: When brain stem death is suspected, the tests to diagnose brain death are focused upon examining the function of cranial nerves.
Activity:
Now log onto
www.aomrc.org. uk /.../42-a-code-of-practice-for-the-diagnosis-and-confirmation-of- death .
And read the document ‘A code of practice for the diagnosis and confirmation of death.’
Which cranial nerves are tested when confirming brain death?
……………………………………………………………………………………………………………..
…………………………………………………………………………………………………………….
…………………………………………………………………………………………………………….
…………………………………………………………………………………………………………….
Why is it important to monitor bloods and treat metabolic abnormalities such as a high sodium before carrying out brain stem tests?
……………………………………………………………………………………………………………….
……………………………………………………………………………………………………………….
What is the most important pre-condition for the diagnosis of brain death?
…………………………………………………………………………………………………..
Cerebellum
Fig 21
27

Is located in the posterior fossa of the skull. It is a vital part of the brain that communicates with the
higher brain and the peripheral nervous system by relays with the basal ganglia, being particularly
concerned with motor control, learned movements and balance. The final motor output from the
brain is from the motor cortex, through the thalamus (integrating the modulating inputs from the
cerebellum) to the upper motor neurones in the Pyramidal tract which cross in the front of the brain
stem (Pyramidal decussation) finally connecting via the corticospinal pathway to the lower motor
neurons in the anterior part of the spinal cord (lower brain stem for the cranial nerves).
The motor-cortico-spinal tracts cross over at the level of the medulla; the sensory pathways in the spinal cord. Many cerebellar functions are ipsilateral (control the same side of the body)
28

The main functions of this primitive part of the brain are:
Maintenance of Equilibrium
balance
posture
eye movement
Coordination of walking
Adjustment of Muscle Tone
Motor Leaning – Motor Skills
Cognitive Function
The posterior fossa structures lie beneath a tough shelf of dura around the level of the ear called the Tentorial Shelf. Above the shelf lie the four lobes. The area below the shelf is referred to as infratentorial or the posterior fossa. Because of the location of the cranial nerves in this area it is important to ensure the gag reflex and swallow are intact before allowing a patient to eat and drink if they have pathology or have had surgery in this location.
The Pituitary Gland
The master gland of the body sits in a central location in the brain and controls many body functions. It secretes hormones to maintain homeostasis including hormones that stimulate other endocrine glands in the body. Lesions on this gland can have devastating effects. Raised intracranial pressure can cause diabetes insipidus. This is not sugar diabetes; it is a disruption of water balance in the body. Antidiuretic hormone is no longer released and the body looses water at a rapid rate. Clinical features are:
Thirst
High urine output with a low specific gravity
Rising serum sodium
Rising blood osmolality
Low urine osmolality
The sodium in the body has not increased; it is simply the loss of water from the body that
causes sodium to be more concentrated. The treatment for diabetes insipidus is to administer
29

antidiuretic hormone, replace intravascular volume and also investigate and reverse the primary
cause which may be a tumour, infection or raised intracranial pressure.
The pituitary gland controls many hormones in the body and therefore disease of this gland can
manifest in many ways:
Thyroid dysfunction
Reproductive dysfunction
Growth dysfunction
Adrenal dysfunction
Fig 22
The Pineal Gland
A small structure in a central location in the brain. It is commonly calcified in adults. Briefly, the
role of this gland includes:
Melatonin production
Timing of sexual maturity
Circadian rhythm
30

Salt and Water Balance.
The brain communicates with the vascular system and renal system to regulate water balance in
the body. It is no surprise that damage to the brain can result in syndromes that result in an
imbalance of salt and water. We have already looked at diabetes insipidus, however, there are
other manifestations of imbalances which can also be life threatening.
SIADH
Syndrome of inappropriate antidiuretic hormone release. The blood osmolality is low because
water is being retained. Antidiuretic hormone release reduces water loss via the kidneys. Sodium
in the blood will appear low and the blood is more dilute. Normally ADH is secreted when
osmoreceptors pick up a high serum osmolality which signals dehydration. The kidney retains
water. If there is an inappropriate secretion of ADH water is retained. Urine output will be low,
the patient may be confused, lethargic and have signs of water toxicity. Low serum sodium could
result in seizures, cerebral oedema and eventually death.
Serum osmolality will be less than 270, CVP may be high.
The treatment includes; fluid restriction, sodium replacement, diuretics, treat reversible causes.
Low sodium should be gradually increased over days as rapid correction can cause pontine
demyelination.
Cerebral Salt Wasting Syndrome.
CSW means that the body is excreting salt in the urine. Salt has a high osmotic action so carries
water with it. This results in a large diuresis in addition to a low serum sodium. The patient will
be dehydrated, confused, hypotensive and deteriorating. Treatment includes fluid replacement,
sodium replacement and treatment of reversible causes.
Neuro intensive care units will have a chart like this one to aid diagnosis. Sometimes the patient is
referred to an endocrinologist for an opinion because syndromes can be hard to diagnose and have
complex presentations.
31

Epilepsy and the Intensive care
There is a high risk of developing seizures in any patient who is neurologically compromised. A
seizure represents an uncontrolled electrical spasm of activity within the cerebral cortex, causing
a massive increase in cerebral metabolic demand so that damage due to hypoxia may occur. The
brain is very sensitive to change. Seizures may manifest because of the trauma, tumour, CNS
infection, sub-dural empyema, electrolyte, metabolic imbalance or pre-existing epilepsy.
Seizures must be controlled as a matter of urgency. When there has been a witnessed seizure
following trauma, a loading dose of anticonvulsant will be prescribed and then the drug
continued regularly at a maintenance dose. If the patient has known epilepsy then urgent re-
assessment of medication is required. Anticonvulsant levels should be assessed regularly and
reversible causes of the seizure should be sought out. If the seizure activity does not terminate
this could mean airway compromise and the patient should be admitted to intensive care for
airway protection and seizure control.
Status Epilepticus is manifested by unrelenting and resistant seizures. These are potentially
lethal and control must be gained. Cerebral metabolism therefore oxygen consumption will be
high and could cause irreversible damage such as ischaemia. Because of the increased muscle
32

activity and brain activity a rise in lactate levels will be seen and body temperature which can
mimic sepsis. Treatment, if not terminated by loading with anticonvulsant is deep barbiturate
coma. Thiopental Sodium is used to ‘rest’ the brain and terminate the seizure activity while the
cause is reversed. Since this will also arrest respiration it is always accompagnied by intubation
and artificial ventilation. Usually this will also mean observation of brain wave activity using a
cerebral function monitor. This is a simple form of EEG and allows the intensive care team to
measure efficacy of treatment. Too much barbiturate will over suppress activity, and depress
cardiac function (therefore bloodpressure) and too little will not be effective. Barbiturate can
also interfere with pupil size and reactivity and can confound this neurological observation. It
also takes a prolonged period to wear off once the drug has been stopped.
Anticonvulsants such as phenytoin have a narrow therapeutic index and are protein bound, this
means that there is a high risk of toxicity and that plasma levels must be adjusted to albumin
levels. Some of the toxic side effects – eg problems with balance - are irrelevant in ITU in a
ventilated patient, and the priority is to halt the status epilepticus.
Activity
Look up and write the equation used to adjust phenytoin level to albumen:
33

Neurological conditions which may require critical care admission:
Guillian Barre Syndrome is an example of a neurological illness which can result in an intensive care
admission. This is an autoimmune disease which results in the destruction of the myelin sheath
(demyelination). This disruption slows the impulse and could actually cause cell body death if severe
resulting in permanent disability. Breathing difficulties and autonomic dysfunction mean severe
cases of this disease require intensive therapy. Treatment includes steroids, immunoglobulins and
plasmapheresis plus respiratory support. Guillian Barre syndrome may be triggered by a minor
illness such as a respiratory infection.
Symptoms:
Bilateral muscle weakness commonly starting in the legs (ascending).
Numbness and parasthesia
Clumsiness
Reduced reflexes
Deterioration in lung function
Severe cases my result in total paralysis at the height of the disease process. The patient will be
aware and very frightened. Sedation for tolerance during this phase is essential. Treatment is aimed
at removing harmful auto antibodies in the plasma (plasmapheresis), steroids to reduce
inflammation and IV immunoglobulins to reduce the effects of the autoantibodies attacking the
nerve sheath. Total recovery is possible, however, severe forms of the disease may result in
34

permanent disability. As the nerves re-gain function the patient can experience severe pain and
critical care teams may require specialist advice on pain management.
Specific nursing considerations:
Monitoring of forced expiratory volumes regularly is essential to detecting respiratory deterioration
in non ventilated patients. Be aware of swallowing difficulties and the risk of aspiration. Be aware of
severe pain as function improves. This disease can result in severe autonomic dysfunction; swings in
blood pressure, tachy / bradycardia can pose a threat as they can be difficult to treat due to
unpredictability.
Activity:
Visit http://www.nhs.uk/conditions/Guillain-Barre-syndrome/Pages/Introduction.aspx
And read about this syndrome.
Myasthenia Gravis
Is a neuromuscular disorder which means the nerve / muscle interface is affected (neuromuscular
junction). This is also a form of autoimmune disease. Myasthenia Gravis causes poor transmission
across the synapse, the receptor sites for the neurotransmitter acetylcholine (neurotransmitter) are
attacked / blocked by auto antibodies. Treatment includes pyridostigmine and steroids. A severe
deterioration may result in requiring respiratory support whilst steroids and immunoglobulins and
in some cases plasmapheresis are administered and adjustment of medication is made.
35

Pyridostigmine is an anticholonesterase which helps to increase the duration of transmission by
enhancing the effect of acetylcholine. There is no cure for this disease therefore symptom control is
the focus of treatment. In some cases a tumour of the Thymus gland plays a role in the disease
(detected by CT of the chest). The Thymus gland has a role in normal immune function. It is thought
that developing immune cells may receive the ‘wrong’ instructions and attack the receptor sites at
the synapse.
Specific nursing care considerations:
Monitoring forced expiratory volumes in non ventilated patients is essential to detect the trend of
deterioration. Be aware of swallowing difficulties and the risk of aspiration. Be aware that muscle
weakness can improve with rest and worsen with activity. Diarrhoea can be a problem as a specific
side effect of pyridostigmine.
Activity:
Visit the National Institute for Neurological Disorders and Stroke (www.ninds.nh.gov) and read
about myasthenia gravis.
36

The Spine.
This section is brief as there is a separate work book on this subject.
Fig 23
There are 31 pairs of spinal nerves.
37

Fig 24
The anterior (front) horn is where the efferent motor pathways exit the spine on their way to the body. Anterior horn cell disease is effectively motor neurone disease. The posterior horn (back) is where the sensory neurones enter the central nervous system to carry the afferent messages to the brain.
Spinal injury can be devastating and not only result in motor weakness but also autonomic dysfunction. Injury can change the way the body responds to certain drugs and therapies. A separate package on the spine will complement this learning resource.
Activity
Look up the term ‘autonomic dysreflexia’ in relation to spinal injury. Write a brief account below on how this may impact on stability and nursing activities.
38

End of Section Activity.
Maybe the deep structures within your brain have retained the information; time to find out.
1. What are the two main divisions of the nervous system?
A.
b.
2. Name the three types of nerves found in the nervous system
a.b.c.
3. Name the neurones that make up the afferent pathways
4. Name the neurones that make up the efferent pathways
5. What is the difference between efferent and afferent?
6. Which section of the spinal cord holds efferent fibres?
a. Anterior horn
b. Posterior horn
7. Name the divisions of the peripheral nervous system:
8. Name the four lobes of the brain:
39

a.
b.
c.
d.
9. Name three functions for each of these lobes:
a.
b.
c.
d.
10. If the patient had a lesion in Wernicke’s area what might be observed?
11. If the patient had a lesion in Broca’s area what might be observed?
12. What is the name of the main ‘relay’ station deep within the brain?
13. Name at least three functions of the hypothalamus
14. How many pairs of cranial nerves are there?
15 Name six functions of the brain stem
40

a.
b.
c.
d.
e.
f.
16 Fill in the missing words:
The Cerebellum is located in the ..........................of the skull. It is a vital part of the brain that
communicates with the higher brain and the peripheral nervous system by relaying to
the................ ................, .................... and ..................... neurones via a pathway called
the .............. ...............
17 A patient with Guillian Barre syndrome may require intensive care. Why would this patient have muscle weakness?
a. The brain has been attacked by antibodies and cannot function
b. The myelin sheath made of protein has been attacked by auto antibodies and cannot transmit.
c. There are multiple lesions in the spinal cord
d. There is a lack of neurotransmitter
18 What is the name of the gap between the cells which must be traversed by the nerve impulse?
19 Name three neurotransmitters.
41

a.
b.
c.
20 A patient with Myasthenia Gravis may require intensive care because of muscle weakness. Why are the muscles weak?
a. The myelin sheath is being broken down by auto antibodies.
b. The receptor sites of the nerve receiving the message across synapse are not effective
c. A stroke in the motor strip of the frontal lobe
21 The Pituitary gland is the master gland of the body. It has many complex functions. Name four ways in which disruption of pituitary function can manifest
a.
b.
c.
d.
22. SIADH can be characterised by:
a. High urine output and low sodium
b. Low urine output and low sodium
c. High urine output and high sodium
23. A low sodium and high urine output could be:
a. SIADH
b. DI
c. CSW
42

43

Neurological Observation in Critical Care
Well done. You have completed a whistle stop tour of the nervous system. Now it is time to look at the patient. How much do you know about the Glasgow Coma Scale. Are you confident to use it and interpret what you are seeing? Time to find out!
The following section is set out in a simple fashion so that the information can be read easily alongside rationale. Using your new knowledge of A&P You will now be able to make more sense of the observations you do.
Objectives for this section:
a. Understand the GCS observation tool and its limitations
b. Apply the tool and interpret results
c. Demonstrate an understanding of further clinical signs of raised intracranial pressure and how to detect them
The traumatic brain injury learning session follows the neurological observation session. It is following this section that you will be tested on your ability to tie the sections together and relate the information to patient care.
44

Neurological Assessment
‘ASSESSING AND RECORDING CONSCIOUS LEVEL FORMS A MAJOR PART OF NURSING ACTIVITIES…A RECORD OF NURSES’ OBSERVATIONS IS GREATLY SUPERIOR TO ANYTHING PRODUCED BY CONNECTING THE PATIENT TO A MACHINE.’ Teasdale 1975.
Developed by Teasdale and Jennett (1974), the Glasgow Coma Scale (GCS) is the tool used in most hospital and pre-hospital settings to assess level of consciousness (Dawes, et al 2007). The scale is not designed to be used in isolation but forms a major component of in-depth observation required for timely detection of neurological deterioration (NICE, 2007).
Frequent observation and recording of GCS concurrently with limb responses, pupil responses to light, blood pressure, pulse rate, oxygen saturation, respiratory rate, temperature and blood glucose monitoring complete this vital data set.
Differing techniques are often practised amongst nurses (Waterhouse, 2008), however, it is essential that assessment of the GCS is carried out using the same method to increase accuracy and control observer bias (Edwards, 2001).
The Glasgow Coma scale is comprised of evaluating three components each of which receive a score:
E = Eye opening (maximum = 4)
M = Motor response (best recorded) (maximum = 6)
V = Verbal response (maximum = 5)
MILD HEAD INJURY GCS 13 – 15
MODERATE HEAD INJURY GCS 9 – 12
SEVERE HEAD INJURY GCS 3 - 8
The highest point on the scale score is 15; the patient will be alert, orientated and have full limb power. The lowest point score is 3; there will be no response at all from each component. A base line GCS, pupil and vital sign assessment must be carried out at triage for all head injured patients. Regular monitoring thereafter will aid detection of deterioration which may be subtle over time. Prevention of secondary brain injury has primacy in the management of neurologically vulnerable patients; early detection and reporting of changes is a key role of the nurse (Hickey, 2009).
Limitations of the GCS:
If the patient is intubated / sedated
Tracheostomy – patient cannot speak
Local injury – eyes closed due to swelling
Focal neurological deficit – patient has expressive dysphasia
If the patient does not speak the same language as the assessor45

If the patient has taken analgesia/medication/alcohol
If the patient has learning difficulties (or a child)
Remember it is a scale and not a score – you should cite the result for each category, and although commonly, indeed routinely and mistakenly done it is not valid to add up the scores, or do any arithmetic on the values. Technically it is a non-parametric scale.
ACTION RATIONALE
Frequency of neurological observations
GCS assessment will be carried out by a
practitioner who has received training in the
techniques and has been passed as competent.
Observations should be performed and
recorded on a half-hourly basis until GCS equal
to 15 has been achieved.
Following assessment in A&E The minimum
frequency of observations for patients with GCS
equal to 15 should be as follows:
half-hourly for 2 hours
then 1-hourly for 4 hours
then 2-hourly thereafter.
If a patient with GCS equal to 15 deteriorates at
any time after the initial 2-hour period,
observations should revert to half-hourly and
follow the original frequency schedule (NICE,
2007).
This includes the full vital sign set: Bp, SA02,
pulse, resps, temp, GCS & pupil size and
reaction.
Inform medical staff of any deterioration without
delay.
It is recommended that nurses who are handing
Vigilance of the nursing team is vital for early
detection and treatment of deterioration thus
prevention of secondary brain injury and
improved prognosis.
The frequency of neurological observations is
determined by professional judgement
(Edwards, 2001). It is therefore essential that
decisions are made by a trained and competent
practitioner.
The condition of the patient, combined with
clinical judgement, should determine frequency.
The patient in A&E who has sustained a brain
injury must be observed frequently as early
intervention may prevent secondary injury.
Deterioration can be subtle in onset and the
patient requires detailed and frequent
observation.
If the patient is deteriorating there must be
assessment by an anaesthetist. Aspiration,
airway obstruction and subsequent lung
infiltration leads to hypoxia and secondary brain
injury therefore increased length of stay in
hospital and poor outcome.
46

over a patient perform the GCS together so a
‘shift change deterioration’ is not recorded.
In addition to a deteriorating GCS signs of raised
ICP include: headache, vomiting, seizure.
ACTION
A patient who is deteriorating and requires
transfer to CT / a specialist centre or has a GCS
less than 8 should be intubated.
RATIONALE
EYE OPENING –
Spontaneously 4 To speech 3 To pain 2 None 1 Eyes closed by swelling = C
Assess for eye opening by observing the patient
as you approach: eyes open spontaneously,
score 4.
If the patient’s eyes remain closed, say
something to elicit a response: eyes open,
score 3.
Speech, touch and finally pain is utilised.
If there is no response to speech, touch the
patient on hand, arm or shoulder and
shake, shout louder to elicit a response:
eyes open, score 3.
If there is no response, exert a peripheral painful
stimulus to the side of the finger nail.
eyes open, score 2.
If there is no eye opening following the
Assesses wakefulness, a function of structures
within the brainstem (Lindsay et al, 2004;
Waterhouse, 2005).
Spontaneous eye opening is an indication that
the arousal mechanisms within the brain are
Functioning (Teasdale, 1976).
If neuronal pathways are impaired due to
trauma or a rise in intracranial pressure, a
greater sensory stimulus is needed to evoke eye
opening (Edwards, 2001).
‘Central’ painful stimulus may result in the
patient grimacing and eye closure may persist
therefore pressure to the side of the nail of the
finger is used to determine ability to eye open.
(Waterhouse, 2005)
Peripheral pain may be applied to the side of the
finger not the nail bed to prevent damage
(Edwards, 2001).
47

application of painful stimulus, score 1.
ACTION
VERBAL RESPONSE
Orientated 5
Disorientated 4
Inappropriate words 3
Incomprehensible sounds 2
None 1
Endotracheal tube or tracheostomy = T
Ask questions to assess orientation to time, place
and person, e.g. ask the patient the month or
year, where they are and who they are.
Avoid questions that elicit a yes/no response.
Dysphasic patients cannot be assessed
accurately for orientation.
If correct answers are elicited to all 3 questions,
score 5.
If the patient cannot answer the above questions
correctly but is able to engage in conversation,
score 4.
If single word answers are given or if the patient
is unable to form a sentence; inappropriate
words,
score 3.
If only noises such as grunting sounds are made,
RATIONALE
Determines comprehension, cognition and
reflects the ability to process thoughts into
words. Be aware that confusion can be subtle
and only detected in conversation after a few
minutes. The patient may learn responses if
corrected following frequent observation
therefore variation of questions can be useful.
Core elements must be correct, the patient must
know who he/she is, where he/she is and the
date (Teasdale, 1976)
Focal lesions may cause speech difficulties such
as expressive/receptive dysphasia/aphasia and
may not indicate impaired consciousness
(Teasdale,1976):
Aphasia description:
Receptive aphasia: Inability to process written or spoken language
Expressive aphasia: Inability to express written or spoken language
Global aphasia: Inability to receive language or express using written or spoken language
Dysphasia description:
Receptive dysphasia: Inability or difficulty in
understanding the spoken word: due to damage
48

score 2.
If the patient makes no attempt to speak and no
sounds are made, score 1.
At this stage responses may not be elicited by
talking to the patient and a painful stimulus may
be required (Waterhouse, 2005).
If no verbal response is possible due to an
endotracheal tube or tracheostomy (without
a speaking valve) write ‘T’ against ‘none’.
to Wernicke’s area responsible for
comprehension of speech
Expressive dysphasia: Inability or difficulty in
putting thoughts into words: due to damage in
Broca’s area. The patient can understand what
has been said to them, but cannot find the right
words to reply.
Dysarthria: Slurred speech
(Lindsay et al, 2004).
Teasdale and Jennett (1974) recommended
descriptive narration beside the chart when
difficulties in categorising the patient are
experienced.
Motor response
Obey commands 6
Localise to pain 5
Flexion to pain 4
Flexion abnormal 3
Extension 2
None 1
Record the best arm response. Do not ask to
squeeze hands. Request a specific action, i.e;
‘raise your arms, wriggle your fingers, pull me
towards you, push me away.’ If the patient
cannot respond ask them to stick the tongue
out / move eyes to the left, right.
Assesses areas of the brain that identify sensory
input and ability to translate this into a motor
response (Lindsay, 2004).
The ability to follow a command indicates that
the patient can process instructions (Fischer
and Mathieson, 2001).
Grasping is a primitive reflex and may happen
spontaneously and not in response to command
(Teasdale, 1976)
Patients with a spinal lesion or neurological
condition may not be able to move limbs but
may be awake and able to move the tongue or
49

If no motor response to loud speech or touch is made: A painful stimulus should be used, pressure
applied over the supra-orbital nerve (except for
suspected facial fractures) or to the spinal
accessory nerve lying under the trapezius muscle
(except for high cervical fractures). Essentially
the painful stimulus should be located on or as
near to the head as possible and above the
clavicle.
Methods of applying central pain stimuli.
Trapezium squeeze (cervical spine C3-4): Use
thumb and two fingers as pincers. Feel for the
trapezium muscle and twist or squeeze.
Significant pressure is exerted for no longer than
20 seconds and any verbal and non verbal
responses noted.
Supraorbital pressure (trigeminal V): Under the
eyebrow edge feel for a notch. Press hard with
the thumb for a maximum of 30 seconds.
eyes to command.
Painful Stimuli
Painful stimuli can be central evoking a response
from the brain, or peripheral evoking primarily a
response from the spine (Edwards, 2001). There
may be contraindications for applying central
stimulus to the orbit (Lowry, 1998; Edwards,
2001; Waterhouse, 2005) therefore these
techniques should only be used by practitioners
trained and competent.
Orbit pressure should not be applied if facial
fractures are present or suspected.
‘Central’ painful stimuli is a more reliable
indicator of brain function because it stimulates
a cranial nerve and not a reflex arc.
Peripheral pain may evoke a spinal reflex action
and is therefore not as reliable (Lindsay et al,
2004; Edwards, 2001).
Localising to pain is a deliberate movement of
the arm across the midline of the body in an
attempt to push away from the source of the
painful stimuli (Fischer and Mathieson, 2001).
The patient may be spontaneously localising to
an irritant such as an oxygen mask. The patient
therefore demonstrates an awareness of
environment.
Flexion to pain is an indication of more severe
dysfunction (Lindsay et al, 2004; Fischer and
Mathieson, 2001). Abnormal flexion (arms
withdraw up and wrists rotate inwards) may be
50

Not to be used if facial fractures are suspected or
confirmed. Use if a high cervical insult or injury
suspected.
If there is no localising response then peripheral
pain to the finger may be used. Assess each limb
separately and record the best response.
an indication of a lesion in the cerebral
hemisphere or internal capsule (Fischer and
Mathieson, 2001).
Extension (arms push down) indicates severe
cerebral damage below the level of the red
nucleus
(Lindsay et al, 2004).
No response may indicate a spinal cord lesion or
late stage raised intracranial pressure.
ACTION RATIONALE
PUPIL REACTIONS
(See appendix p 16 – 17)
Determine patient history that may affect pupil
reactions e.g. cataracts, iridectomy or recent
drug therapy that may dilate or constrict the
pupil.
Note the size, shape, equality and position of the
pupils (both eyes simultaneously).
Using a pen torch, shine the light moving from
Abnormal reactions can indicate raised
intracranial pressure and/or damage to the
oculomotor nerve (see A&P). Both pupils should
react at the same time if light is directed at one
eye. This is called a consensual response.
Progressive dilatation and loss of pupil reaction
on one side can be due to pressure on the
oculomotor nerve on the same side. Damage can
be caused by a variety of lesions, however, if
pressure continues, the nerve on the other side
can also be compressed resulting in bilaterally
unreactive, dilated pupils; a sign of severe
51

the outer towards the inner aspect of the eye.
Observe the size shape and reaction of the pupil
and record brisk reactions as + and sluggish
reactions as ‘S’.
Wait a few seconds before repeating the
procedure in the other eye.
TESTING LIMB POWER
damage and brain herniation (Lindsay et al,
2004).
Both pupils should be assessed at the same time
to observe and compare reaction.
IDENTIFICATION OF FOCAL DEFICIT
ACTION RATIONALE
LIMB POWER
(recorded on limb section of chart)
Each limb will be assessed
Arm strength.
Ask the patient to close their eyes and hold their
arms out in front of them, palms facing up. If the
patient can maintain this position, record the
power as normal.
The power of each limb should be recorded
separately on the lower section of the
assessment chart.
The best response is charted on the GCS graph at
the top of the chart using one dot.
If an arm drifts downwards record that limb as
mildly weak. The mildest response is that the
palm rotates to a downward position known as
pronator drift.
Limb responses may give clues to the origin of
the neurological dysfunction (Lindsay et al,
2004); eg, a weak limb on the right side will
indicate damage to the left motor strip, or
ipsilateral spinal cord
The GCS is the total score of the best responses;
however, it is essential to reveal any weakness
and difference in power. Clinical examination of
the limbs may be carried out to aid clarity. Each
limb may be scored out of 5:
5 normal
4 move against some resistance
3 move against gravity only
2 Can move with gravity eliminated
1 Flicker
0 nothing
Assessment of strength is then transcribed onto
the limb assessment section of the observation
52

If the patient is unable or has extreme difficulty
in lifting their arms off the bed but can make
some movement (eg move fingers) record as
severely weak.
If the patient is unable to move their arms, apply
pain and record the response
(see figure on posturing)
Leg strength.
Ask the patient to raise their legs off the bed or
place hand on the sole of the foot and ask the
patient to push, then place hand on top of the
patients foot and ask them to pull their foot
upwards. Place hands on both knees and ask the
patient to push the knees up hard. Record
whether the power of each leg is normal or
mildly weak if the patient can comply.
If the patient cannot lift their legs easily but can
make some movement, record as severely weak.
If the patient cannot move the legs the response
to painful stimulus will be documented as
described.
chart
normal strength - full movement against both gravity and resistance.
mild weakness - limb moves against gravity but not against resistance (no push/pull).
severe weakness – limb is able to move but unable to lift against gravity.
Lower limb response to peripheral painful stimuli
is not reliable due to involvement of spinal
reflexes therefore the best limb response
charted on the GCS will be from the arms
(Hickey, 2009;Lindsay et al,2004).
ACTION
VITAL SIGNS
Will be monitored and recorded concurrently
with neurological assessment:
RATIONALE
GCS is one component of assessment. Vital signs
complete the full complement of data on which
treatment and intervention can be based.
53

Temperature
Investigate and treat cause of temperature.
Septic screen
liaise with microbiology team
Fluid from ear / nose which tests positive for
glucose may be cerebrospinal fluid
Pulse –
Blood Pressure
Beat to beat real time invasive monitoring will
be used for all patients requiring intubation and
for patients who are deteriorating:
ECG
Invasive Bp
Blood gas analysis
On going ABCDE assessment
Base of skull fracture and CSF
rhinorrhoea/otorrhoea (CSF drip from nose/ear)
increase risk of infection.
A patient who has sustained a severe head
injury may have localised damage to the
temperature regulating centre in the
hypothalamus. As the patient’s temperature
rises vasodilation of the cerebral blood vessels
takes up more room in the closed box of the
skull (Waterhouse, 2005; Lindsay et al, 2004). A
raised temperature will also increase metabolic
demands on the brain.
Bradycardia – the heart rate may drop as low as
35-50 beats per minute in the later stages of
raised intracranial pressure (Lindsay et al,2004).
Tachycardia – can occur where there is damage
to the hypothalamus and in the terminal stages
of raised ICP (Lindsay et al, 2004).
Tachycardia also indicates a need for fluid
resuscitation and further investigation of the
cause and subsequent treatment must be
initiated without delay.
Hypertension – a rising systolic blood pressure
combined with a widening pulse
pressure is a late sign of increasing ICP (Lindsay
et al, 2004). Treatment of hypertension must be
discussed with a senior medical colleague as
sudden lowering of blood pressure may result in
secondary injury (infarct) because the CPP has
been reduced when the ICP has been high.
Hypotension – if autoregulation is impaired by a
54

Pupil assessment
Cerebral perfusion = mean arterial pressure
(MAP) – intracranial pressure (ICP)
HYPOXIA & HYPOTENSION PREVENTION – ABCDE
MAP > 80 PO2 > 13 PCO2 4.5 – 5
SAO2 > 97 TIMELY INTUBATION
Respirations
cerebral event hypotension results in decreased
blood flow and therefore oxygen supply to the
brain.
Cerebral perfusion (CPP) must be maintained to
prevent secondary injury.
Hypotension may also be caused by
hypovolaemia, sepsis, sedative drugs etc. Causes
of hypotension must be treated immediately.
The target cerebral perfusion pressure is 60 – 70
mmHg. CPP below 60 carries a risk of secondary
brain injury through infarction and cerebral
oedema.
ICP is not electronically monitored in A&E. In
order that perfusion of the brain is protected it is
recommended that an MAP of > 80 should be
achieved (see Walton Centre guidelines). It is
vital that blood pressure below this level is
treated urgently.
Respiration assessment is a vital early warning
sign of reducing consciousness. Respiratory
depression and loss of airway protection will
occur as the GCS score falls.
If the patient is deteriorating there must be
assessment by an anaesthetist
if GCS falls to 13 or less.
Intubation is essential at GCS 8 or less.
Aspiration and subsequent lung
infiltration leads to hypoxia and
secondary brain injury and increased
length of stay in critical care & poor
55

prognosis.
Follow local care plan, guidelines and care bundles for care of the unconscious patient & artificially ventilated patient.
ACTION
Urine output will be monitored hourly.
Insert a urinary catheter if GCS is 12 or less.
If urine output exceeds 3oo ml per hour for two consecutive hours perform urine specific gravity, paired urine and serum osmolality. Report results to medical colleagues.
RATIONALE
Diabetes insipidus (DI) indicated by excessive urine output, low urine osmolality and rising serum osmolality and serum sodium.
Normally the pituitary gland secretes antidiuretic hormone (ADH) when blood osmolality rises. This function is disrupted due to rising ICP. Large volumes of water are passed and the sodium concentration in the blood is raised. This is not to be confused with therapeutic diuresis which follows the administration of mannitol used to treat high ICP. It is essential to have the diagnosis made by a senior medical colleague. Treatment is the administration of antidiuretic hormone (DDAVP).(Hickey, 2009)
ACTION
Avoid neck flexion
keep the body in alignment.Nurse head up by 20 - 30 degrees.
If spinal injury is suspected – tilt the bed end down to achieve position whilst maintaining alignment.
RATIONALE
Cerebral venous drainage will be impeded by neck flexion and poor body positioning. This will cause a rise in ICP. Intra-abdominal pressure may also cause a rise in ICP therefore hips should not be bent at an acute angle (Hickey, 2009).Risk of aspiration into the lungs is increased in intubated patients if nursed at an angle less than 30 degrees (ventilator care bundle).
ACTION
Observe for seizure activity
When the patient is sedated and artificially ventilated seizure activity is difficult to detect but may be manifested by tachycardia, pupil changes and cardiovascular instability.
RATIONALE
A,B,C,D,E protocol. Seizure control immediately. Seizures increase cerebral metabolism and increase ICP therefore risk of secondary brain injury.
ACTION
Specific fluid balance:A detailed hourly fluid balance account will be maintained.Aim for a neutral balance.
RATIONALE
Blood volume must be maintained to prevent hypotension and maintain cerebral blood flow.Water balance between the intravascular space and brain tissue depends upon an osmotic
56

Avoid use of hypOtonic solutions and 5% glucose.Monitor serum sodium determine cause if low.
Mannitol will be administered by expert request to manage high ICP
Hypertonic saline administration may be requested (refer to Walton Centre guidelines)
gradient. Glucose contained within crystalloid infusion will be metabolised and the remaining water will infiltrate the brain tissue & contribute to cerebral oedema.Traumatic brain injury can cause disorders of sodium balance (see above section).Mannitol is an osmotic diuretic and will cause excess diuresis. Intravascular volume must be maintained using colloid.
Hypertonic saline reduces brain water and increases intravascular volume. Serum sodium will rise and serum osmolality will rise. This is the therapeutic nature of hypertonic saline (Refer to Walton Centre ICP management guidelines).
ACTION
Blood gases – specific value ranges
Maintain PO2 > 13 kpaMaintain CO2 4.5 – 5 kpaPre-oxygenation with 100% O2 for 60 seconds prior to suctioning ET tube.
(refer to Walton Centre ICP management protocol)
RATIONALE
Maintain oxygenation of the damaged brain.
CO2 can cause vasodilatation of cerebral vessels which will then take up more room in the confines of the skull (see appendix). ICP will rise.
Sedation of the artificially ventilated patient specifics
In acute stages of head injury management sedation must be adequate to prevent coughing and bucking on the endotracheal tube spontaneously and when suction is applied.Sedation holds (ventilator care bundle) should not be performed in acute ICP management.
RATIONALE
Coughing and straining will increase ICP.
Ventilator mode:
Ventilator modes which give predictable tidal volumes are recommended
RATIONALE
Sudden rises in CO2 due to poor compliance with pressure limited modes may occur.
Abnormal posturing.
57

Afferent = impulse in from environment
Efferent = impulse from the brain
REFERENCES
58
Responses to external stimulus cannot be modified by the control centres in the brain as the connections are damaged. Extension instead of flexion in the muscle is seen.

Dawes, E. Lloyd, H. Durham, L (2007) ‘Monitoring and recording patient’s neurological observations.’ Nursing Standard. 22 (10) pp 40 – 45
Dougherty, L and Lister, S (Eds) (2004) The Royal Marsden Hospital Manual of Clinical NursingProcedures 6th Ed London: Blackwell
Edwards, S L (2001) Using the Glasgow Coma scale: analysis and limitations British Journal ofNursing Vol. 10 No. 2 pp. 93-101
Fischer,J and Mathieson, C (2001) The history of the Glasgow Coma Scale: implications for practice.Critical Care Nursing Quarterly. Vol 23 No 4 pp. 52-57
Hickey, J V (2009) The Clinical Practice of Neurological and Neurological and Nursing. Philadelphia:Lippincott-Raven
Lindsay, K, W. Bone, Callander (2004) Neurology and Neurosurgery Illustrated. 4th Ed. London. Churchill Livingstone.
Lowry, M (1999) The Glasgow Coma Scale in clinical practice: a critique. Nursing Times Vol. 95 No.22 pp. 40-42
National Institute for Clinical Excellence (2007) ‘Head Injury: Triage, Assessment and Early Management of Head Injury in Children, Infants and Adults.’ www.nice.org.uk/CG056 (accessed June 2010)
Shah, S (1999) Neurological Assessment. Nursing Standard Vol. 13 No. 22 pp. 49-56
Stewart, N (1996) Neurological Observations. Professional Nurse Vol. 11 No. 6 pp 377-378
Teasdale, G. (1976) ‘Assessment of Head Injuries.’ British Journal of Anaesthesia. Vol 48. Pp 761 - 766
Teasdale, G. Jennett, B. (1974) ‘Assessment of coma and impaired consciousness: a practical scale.’ The Lancet. 2, 7282, pp 81 - 84
Waterhouse, C (2005) The Glasgow Come Scale and other neurological observations. (learningzone: neurological assessment) Nursing Standard Vol. 19 No. 33 pp. 56
Waterhouse, C. (2008) ‘An audit of nurses’ conduct and recording of observations using the Glasgow Coma Scale.’ British Journal of Neuroscience Nursing. Vol 4 No 10. Pp 492 - 499
59

FURTHER READING
Dootson, S (1990) Critical Care: Sensory Imbalance and Sleep Loss Nursing Times Vol. 86 No. 35pp. 26-29.
Ellis, A and Cavanagh, SJ (1992) Aspects of Neurological Assessment using the Glasgow ComaScale. Intensive Critical Care Nursing Vol. 8 No.2 pp 94 - 99
Hickey, J V (2009) The Clinical Practice of Neurological and Neurological and Nursing. Philadelphia:Lippincott-Raven
Hudak, C, Gallo, B, Morton, P (1998) Critical Care Nursing. Philadelphia: Lippincott
Lindsay, K, W. Bone, Callander (2004) Neurology and Neurosurgery Illustrated. 4th Ed. London. Churchill Livingstone.
Mooney, G and Comerford, DM (2003) Neurological Observations. Nursing Times Vol. 99 No. 17 pp.24-25
Price, T (2002) Painful stimuli and the Glasgow Coma Scale. Nursing in Critical Care Vol. 7 No. 1pp. 19-23
Teasdale, G M and Murray, L (2000) Revisiting the Coma Scale and Coma Score. Intensive CareMedicine Vol. 26 No. 2 pp 153-154
Woodward S (1997) Practical Procedures for Nurses. Neurological Observations Nursing Times Vol. 93 Nos. 45-48 parts 5.1 – 5.4
Pictures sourced from:
www.mstrust.org.uk
www.faculty.washington.net
www.bioon.com
www.sciencegeek.net
www.medicalook.com
www.biologymad.com
TRAUMATIC BRAIN INJURY
60

Each year, an estimated 1 million people in the UK go to hospital as a result of a head injury.
Males are more likely to have a head injury than females and the age group most at risk is
between 15 and 29 years of age.
GOALS FOR THIS SECTION:
1. Understand that traumatic brain injury is a process, not an event
2. Understand the pathophysiological mechanisms involved in traumatic brain injury
Definition: Severe Head trauma associated with a Glasgow Coma Score of ≤ 8 after resuscitation
EYE OPENING VERBAL RESPONSE MOTOR RESPONSE
(please refer to GCS section)
TBI is a process, not one event
Primary injury is that directly caused by the trauma; secondary by the effects afterwards, such as brain swelling. Secondary injury can be more damaging than primary injury. The main mechanisms of brain injury are:
◦ Extracranial injuries causing hypoxia, hyoptension
◦ Brain Contusion
◦ Increased intracranial pressure ( ICP) due to brain swelling or itracranial blood clots
◦ Diffuse Axonal Injury (DAI)
CT reveals a left sided subdural haematoma and frontal haemorrhagic contusions. There is mid line shift. On examination his right pupil is 5mm in size and fails to constrict to light.
Bp = 95 / 60
MAP = 77
ICP = 25 and is set to rise as a heamatoma expands and contusions swell.
61

MAP 77 – ICP 25 = CPP 52
Cerebral perfusion is not being met and infarction occurs. Urgent surgical action is required!
Autoregulation.
Cerebral auto regulation is the mechanism for maintaining a constant cerebral blood flow in the face
of changes in systemic blood pressure. The control of this process is quite complex, as is the control
of systemic blood pressure, and relies on both neural and metabolic (chemical) mechanisms
controlling the diameter of peripheral blood vessels, both venous and arterial and arterioles, and the
force, volume and rate of cardiac contractions. Baroreceptors detecting blood volume are located
in the atria, great veins, pulmonary vessels, aortic arch and carotid sinus. The carotid body via the
glossopharyngeal nerve detects the influence of systemic oxygenation – the chemosensitve parts of
the brain stem detect changes due to acidosis – such as rising carbon dioxide levels, or lactic acidosis
from ischaemia producing efferent responses from the brain stem via the parasympathetic (primarily
vagus nerve) and sympathetic systems. These systems – via sympathetic innervation of brain blood
vessels , together with the local microchemical environment influence the diameter of these vessels
resulting in autoregulation – a constant cerebral blood, though set to the metabolic needs of the
brain – thus blood flow is higher when the patient is awake, and locally when a particular part of the
brain is active - such as Broca’s area when the patient is talking. It is this local effect that is
measured by functional MRI scans. This system, in particular the level of acidosis in the respiratory
centre in the brain stem also plays a major role in the control respiratory function, though in
ventilated patients on ITU these responses will not be apparent.
Autoregulation may fail in disease states particularly head injury and sub-arachnoid haemorrhage. In
this circumstance falls in perfusion pressure will then produce a fall in blood flow and ischaemic
damage results. It is therefore critical to maintain adequate CPP in these circumstances.
The blood brain barrier.
62

Endothelial cells within the capillary bed make up the blood brain barrier (BBB). Together with other
cells such as astrocytes, they provide an interface between the blood and brain tissue via tight
junctions between the cells. Transport of gases and nutrients, protection from toxic substances and
protection from changes in oncotic pressure are functions of the BBB thus homeostasis is maintained
(Tortora, Grabowski, 2000). However, the BBB will not be intact after TBI. Disruption of the blood
brain barrier will lead to transcapillary leakage and cerebral oedema, and loss of cerebral
autoregulation (Nordström 2003).
These are the reasons why it is vital to maintain the CPP. In the absence of ICP monitoring the MAP
must be maintained at 80mmHg while a specialist neuro intensive care bed is secured.
63
CEREBRAL PERFUSION PRESSURE
INTRACRANIAL PRESSURE

This graph demonstrates a loss of autoregulation following TBI. CPP is reduced by increases in ICP.
64
The oculomotor III nerve is compressed and the pupil fixes and dilates
The brain stem is compressed producing the Cushing response – BP up, HR down

Herniation schematic from Robbins and Cotran. Pathologic Basis of Disease. 7th ed. Philadelphia: Elselvier; 2005.
The key concept of the non compressible box of the skull is a vital point to appreciate as secondary injury results in this evolving scenario. The brain stem is compressed as the cerebellar tonsils herniate through the foramen magnum. Brain death is imminent.
THINK AHEAD
Triage History Imaging Neurosurgical referral Keep communicating
A SSESSMENT & TIMELY ACCESS TO NEUROSURGICAL ADVICE
TRIAGE REFERAL ON GOING GCS & pupil assessment EWS & 2 WAY COMMUNICATION
HYPOXIA & HYPOTENSION PREVENTION – ABCDE
MAP > 80 PO2 > 13 PCO2 4.5 – 5 SAO2 > 97 TIMELY INTUBATION
EARLY IMAGING & REPORTING < 1 HOUR WHEN GCS 13 OR LESS
Consider trauma series CT head, C0 – T5, chest, image pelvis & abdomen
AMBULANCE TRANSFER TO NEUROSURGICAL CENTRE < 4 HOURS FROM TRIAGE
65

Pre-warn ambulance service of impending emergency transfer
DECISION MAKING BY SENIOR DOCTOR IN BOTH HOSPITALS
Consultant involvement to support timely decisions
It is imperative that the patient with an expanding lesion is identified early and is transported to expert help without delay.
Treatment Options:
Surgical Management:
Evacuation of space occupying lesion (haematoma, abscess, tumour)
Evacuation of contusions and removal of bone flap = decomrpessive craniectomy
Insertion of an extraventricular drain (EVD) to off load CSF and decrease ICP (Lumbar puncture contraindicated with expanding Space Occupying Lesion!)
Medical Management:
Protection of airway
Control of CO2 & PO2
MAP > 80mmhg
ICP less than 20, CPP between 60 – 70
Euvolaemia
Body alignment
Sedation
Control of seizures
Consider prophylactic anticonvulsant
Antibiotics / antivirals for CNS infections
Steroids for tumour
66

Normothermia
Glucose control
Haemostasis
Homeostasis
Therapeutic hypothermia
Barbiturate coma
REFERENCES:
The Brain Trauma Foundation. (2007), Guidelines for the management of traumatic
brain injury, Journal of Neuro Trauma, vol 24, Supplement 1, Pp S- 59 S
- 64. p 17-23. p 47-74.
Nordström CH. (2003), Assessment of critical thresholds for cerebral perfusion pressure by bedside
monitoring of regional energy metabolism. Neurosurg Focus;15:5.
Tortora G J, Grabowski S R, (2000) Principles of anatomy and physiology. John Wiley & sons, inc. New
York. 9th ed. p 447 – 448. ISBN 0-471-36692-7
67

Activity 7. END OF SECTION TEST:
Now you have read and absorbed the contents of this section using the structures in your brain, it is
time to see if you have retained the information and can relate this to how you care for a patient
who requires intensive care because they are neurologically compromised. Good luck.
1. CPP STANDS FOR: .............................................................
2. Complete the equation:
CPP = ...........................................................................
Your patient has a BP of 100/60 and an ICP of 26 what is the cerebral perfusion pressure?
68

3. Name four mechanisms of brain injury:
4. What range is a normal ICP?
5. What MAP would be an ideal target for a patient without an intracranial pressure monitor?
6. How would you apply painful stimuli to assess limb reponses of the patient cannot obey
commands?
7. How can you differentiate between flexion and extension of a limb?
8. What is the name for this posture? The patient pushes the arms down.
69

9. What is the name for this posture?
10. Describe a normal pupil response to light.
70

11. What is consensual response to light?
12. If there is a dilated pupil which does not respond to light, what could be the clinical
significance?
13. Once the patient is intubated is it necessary to continue to assess the pupils?
a. Yes
b. No
14. How can a carbon dioxide above 5kpa affect intracranial pressure?
a. Causes vasoconstriction
b. Causes vasodilatation and a raised ICP
c. Causes a higher urine output
15. What is the difference between afferent and efferent?
71

16. What could happen to the serum sodium if the patient has diabetes insipidus?
a. It would be rising
b. It would be reducing
c. There would be no change
17. What would happen to the urine output if the patient had diabetes insipidus?
a. It would be low
b. It would be high
c. There would be no change
18. What would happen to the serum osmolality if the patient had diabetes insipidus?
a. It would rise
b. It would fall
c. It would not change
72

19. What is the treatment for diabetes insipidus?
20. Why is it important to avoid neck flexion in a head injured patient?
You have a growing body of knowledge. Why not put yourself to the test with a virtual patient?
Activity.
The THINK AHEAD e-learning package Online.edgehill.ac.uk
73

The ‘Think Ahead’ learning package has been developed to support and educate medical and nursing staff involved in the delivery of care to head injured patients in the acute setting, including emergency departments, surgical and medical assessment centres and observation wards.
Think Ahead is an interactive and intuitive package which offers a multi-media learning experience and more information is available at: online.edgehill.ac.uk.
An insight into the use of sedation in Neuro critical care
Helen Jones
Therapeutic sedation is administered in the critical care setting for a wide range of reasons. It is used
to contribute to the control of intracranial pressure, agitation, stress, delirium and to keep the
patient from self harm (Bion,1999). In the general intensive care setting, sedation with analgesia is
used to achieve compliance and comfort during therapeutic mechanical ventilation. A ‘tube tolerant’
state is achieved utilising a sedation scoring tool such as the Ramsay Scale or Richmond Agitation
Sedation Scale, in combination with a sedation protocol.
74

There has been a critical re-evaluation of sedation techniques in the last ten years and the goal of
heavily sedated and comatose patients on mechanical controlled modes of ventilation has been
replaced by the concept of the awake yet compliant, comfortable patient who can interact with the
environment and exercise the muscles of respiration. This, together with the practice of sedation
holds (Kress and Pohlman et al, 2000) has led to reduced length of stay and better outcome
following critical illness (Jackson and Proudfoot et al, 2010). Important in this process is the ability to
assess the level of sedation the patient requires and administer appropriate agents to achieve
therapeutic effect by following an evidence based pathway.
A survey of 192 critical care units in the UK revealed that 88% utilised a sedation scoring tool, 66.4%
of which used the Ramsay Sedation Score. 80% used an evidence based sedation protocol for
guidance. Propofol was the preferred agent for sedation in the first 24 hours and for weaning from
mechanical ventilation..
The pharmacological properties of propofol allow for rapid weaning from ventilation and its use in
critical care has been correlated with reduced length of stay and increased critical care capacity
(Krishnan et al, 2004). Propofol has been used widely in neuro-intensive care because it allows rapid
assessment of neurology after the infusion has been stopped; this has obvious benefits as the critical
care team can assess the patient’s neurological function in a timely fashion. It has also been reported
to have neuro-protective properties and has been shown to reduce intracranial pressure (ICP) in
several studies (Hutchens et al, 2006). However, the potentially lethal but rare propofol-related
infusion syndrome (PRIS) has been highlighted in an increasing volume of case reports and a large
prospective study (Roberts et al, 2009), administration through the guidance of protocol is therefore
essential. The study by Roberts et al (2009) revealed that the syndrome can manifest soon after the
infusion has started and at low doses. Critically ill adults were recruited from 11 critical care units in
the US. Of the 1017 patients 35% were neurosurgical. All patients were administered propofol
beyond 24 hours and monitored for manifestation of PRIS associated symptoms. A patient was
deemed to have PRIS if they developed metabolic acidosis and cardiac dysfunction together with
one or more significant symptoms; rhabdomyolysis, elevated triglyceride levels or renal failure. 1.1%
of the 1017 developed PRIS as defined by the study. None of the 1.1% developed rhabdomyolysis or
Brugada ecg patterns. Of the 11 patients who were diagnosed with PRIS two developed symptoms
within the first day of administration of propofol and 10 developed symptoms within 3 days. There
were two deaths and these were also the only patients who received a propofol dose exceeding 83
ug/kg/min. Due to the early onset of PRIS symptoms in their cohort of patients the authors advised
that clinical signs of PRIS should be monitored from the commencement of the agent.
75

This was the first large trial which debated this complex and poorly defined syndrome although
many case studies have been published. The authors stated that among 71 previously published case
studies 86% received a dose exceeding 83 ug/kg/min. Despite increasing reports of the syndrome
there remains a lack of international consensus on definition.
PRIS results in impairment of fatty acid chain oxidation and inhibits oxidative phosphorylation in the
mitochondria (vernooy and Delhaas et al, 2006).
PRIS symptoms:
Acidosis
Lactic acid build up
Raised CK
Raised triglyceride levels
Urine myoglobin
Dark urine
Bradyarrhythmias
Pyrexia
Raised potassium
Most of these elements are monitored routinely in critical care. Indeed, these clinical signs can
reflect the state of critical illness, organ failure and sepsis. However, triglyceride levels could be
added to routine screening for patients receiving propofol infusion to aid detection of PRIS. In
addition, attention must be drawn to ecg changes such as Brugada ecg patterns:
electrocardiographic changes which herald sudden death due to PRIS are typically ST-segment
elevation in leads V1 – V3 (Vernooy and Delhaas et al, 2006).
Administration of sedation for intracranial pressure (ICP) control is essential. Full compliance with
artificial ventilation must be achieved to facilitate manipulation of carbon dioxide levels and to
prevent coughing which will increase the ICP. Under this condition, higher doses of sedation will be
used to achieve maximal therapeutic effect. In addition sedation suppresses the cerebral metabolism
which reduces blood flow ; therefore blood volume and consequently also ICP. Once cerebral
76

metabolism is maximally suppressed there is no further advantage in increasing the dose of
sedation, though in practice this level is rarely reached except in total barbiturate coma. EEG control
maybe used to assess the suppression, or its simpler derivatives such as the Cerebral Function
Monitor, or BIS. Conversion from propofol infusion to midazolam infusion would seem desirable if
ICP continues to be monitored and weaning from ventilation is not clinically advised. A sedation
scoring system would not be practical in this situation; however, it is necessary to know how much
sedation is required in order to limit the negative effects of sedation: hypotension, accumulation,
increased dependence on vasopressors, organ dysfunction and increased length of stay in critical
care.
Response to sedation can depend upon: body mass index, age, alcohol and drug use, hepatic and
renal function. The amount of sedation required to achieve therapeutic effect can therefore vary
greatly. It is essential to have knowledge of all these factors when considering the use of sedation.
In control of intracranial pressure:
Assess body mass index
Use a protocol to guide choice of agent – propofol not to exceed 24 hours if weaning is not
clinically advised – assess triglyceride levels daily and monitor for symptoms of PRIS.
BIS monitoring
Concomitant use of analgesia
Exempt from sedation hold element of ventilator care bundle
In achieving tube tolerance and control of agitation where ICP is not actively managed:
Assess body mass index
Use of sedation score tool
Concomitant use of analgesia
Pain relief scoring tool
Consider remifentanil as alternative to propofol
The use of sedation protocols can reduce weaning time from ventilation and therefore reduce length
of stay in critical care (Chanques et al, 2006; Quenot et al, 2007). It is therefore appropriate to
develop and introduce such protocols.
77

Manufacturers of sedative agents continue to develop products for the acute setting. Propofol has
been used widely in all critical care settings because of its short duration of action and ease of use
for weaning from mechanical ventilation. Remifentanil is also a short acting agent which has been
used in weaning with good results (Di Nardo et al, 2005) and may be used to achieve a tube tolerant
state.
Considering the diversity of symptoms for PRIS and the heterogeneity of the critically ill patient it is
clearly difficult to diagnose with a significant degree of confidence. The reported cases may be the
‘tip of an iceberg’ or may not have been PRIS because symptoms cross over with many critical care
conditions such as sepsis. In order to increase patient safety it seems appropriate to limit the use of
propofol by the following methods:
Introduction of sedation pathway which can be nurse led
Introduction of sedation scoring tool used concurrently with pain scoring
THE RAMSAY SEDATION SCALE
Level 1: Patient anxious and agitated, restless or both.
Level 2: Patient cooperative, orientated and tranquil.
Level 3: Patient responds to commands only
Level 4: Patient exhibits a response to a light glabellar tap or a loud auditory stimulus.
Level 5: Patient exhibits a sluggish response to a light glabellar tap or loud auditory
stimulus.
Level 6: No response to a light glabellar tap or loud auditory stimulus.
The Ramsay Sedation Score has two clearly defined categories. 1-3 assess wakefulness, 4-6
assess degrees of sleep. This does not replace the use of the Glasgow Coma Scale assessment of
patients. A Ramsay sedation score of 2 would be the target for patients sedated to maintain
‘tube tollerance’ and a reduction in agitation. However, the ‘orientated’ descriptor may not be
78

applicable for patients who are neurologically compromised. This element is also difficult to
assess when the trachea is intubated. The scale has been validated for clinical use and is utilised
in a significant percentage of UK critical care units.
The Richmond Agitation Scale (RASS)
A scale with a range from +4 to -5. A score of 0 is the desired level of sedation. The RASS is linked to
the CAM ICU work sheet for the diagnosis of delirium and is therefore a commonly used scale in
critical care units. It could be argued that the RASS, because of it’s detailed and abundant
descriptors, is more sensitive when applied to patients with complex neurology would also link
more effectively with risk assessments.
Score Term Description
+4 Combative Overtly combative or violent, immediate
danger to staff
+3 Very agitated Pulls on or removes tubes or catheters or has
aggressive behavior toward staff
+2 Agitated Frequent nonpurposeful movement or patient
ventilator dyssynchrony
+1 Restless Anxious or apprehensive but movements not
aggressive or vigorous
0 Alert and calm
-1 Drowsy Not fully alert, but has sustained (more than 10
seconds) awakening, with eye contact/eye
opening to voice
-2 Light sedation Briefly (less than 10 seconds) awakens with
eye contact to voice
-3 Moderate sedation Any movement (but no eye contact) to voice
79

-4 Deep sedation No response to voice, but any movement to
physical stimulation
-5 Unarousable No response to voice or physical stimulation
Key Learning Points:
Sedation scoring reduces anxiety therefore can reduce the incidence of delirium and post
traumatic stress which impact upon recovery / morbidity.
Sedation scoring enables the patient to continue to interact and move limbs and muscles of
breathing therefore reducing length of stay in critical care.
Improved psychotropic medication use will reduce side effects of sedation
References:
Bion, J. (1999) Intensive Care Medicine: Fundamentals of anaesthesia and acute medicine. BMJ
publishing. London.
Chanques G, Jaber S, Barbotte E. et al (2006). ‘Impact of systematic evaluation of pain and agitation
in an intensive care unit.’ Crit Care Med. 34:1691-1699.
Di Nardo, M. Paperini, A. Mosca, C et al (2005) ‘Weaning from mechanical ventilation using
remifentanil versus midazolam-morphine analgo sedation: our experience.’ Critical Care. 9 (supp 1). P
135. Available at: www.http://ccforum.com/content/9/s1/p135
80

Hutchens, M, P. Memtsoudis, S. Sadovinkoff, N. (2006) ‘Propofol for sedation in neuro-intensive
care.’ Neurocritical Care. 4 (1). Pp 54-62.
Jackson, D, L. Proudfoot, C. Cann, K. Et al. (2010) ‘A systematic review of sedation practice in the ICU
on resource use, costs and patient safety.’ Critical Care. 14. R59
Available at: www.http://ccforum.com/content/14/2/R59
Kress J,P. Pohlman A,S. O'Connor M,F, et al. (2000) ‘ Daily interruption of sedative infusions in
critically ill patients undergoing mechanical ventilation’. N Engl J Med.342:1471–1477. doi:
10.1056/NEJM200005183422002.
Krishnan, J, A. Moore, D. Robeson, C. Et al. (2004) ‘A prospective, controlled trial of a protocol based
strategy to discontinue mechanical ventilation.’ American Journal of Respiratory and Critical care
Medicine. 169. 673-678.
Quenot J,P. Ladoire S. Devoucoux, F et al (2007) ‘Effect of a nurse-implemented sedation protocol on
the incidence of ventilator-associated pneumonia’ Crit Care Med .35:2031-2036.
Reschreiter, H. Maiden, M. Kapilla, A. (2008). ‘Sedation practice in the intensive care unit: a UK
national survey.’ Critical Care. 12. Available at:
www.http://ccforum.com/content/12/6/R152
Roberts, R, J. Barletta, J, F. Fong, J. Et al. (2009) ‘Incidence of propofol-related infusion syndrome in
critically ill adults: a prospective, multicenter study.’ Critical Care. 13. Available at:
www.http://ccforum.com/content/13/5/R169
81

Vernooy, K. Delhaas, T. Cremer, O. et al (2006) ‘Electrocardiographic changes predicting sudden
death in propofol-related infusion syndrome.’ Heart Rhythm. 3 (2). Pp 131-137.
Subarachnoid Haemorrhage.
Prior to reading this section it is essential to revise the anatomy and physiology section of this work
book, specifically the subarachnoid space, CSF pathways and Circle of Willis. Please use
supplementary reading material to enhance your learning as you work through the section. Useful
websites include:
www.nhs.uk/conditions/ Subarachnoid - haemorrhage
www.brainandspine.org.uk/.../ subarachnoid _ haemorrhage /
www.avmsupport.org.uk
82

A haemorrhage into the space where the cerebrospinal fluid circulates is called a Subarachnoid
Haemorrhage (SAH). This is commonly caused by the rupture of a cerebral aneurysm located in the
main Circle of Willis or one of the branches or an arteriovenous malformation.
SAH is graded in severity using the WFNS scale – the poorer the grade the worse the prognosis and
the higher the treatment risk:
World Federation of Neurosurgery grading system (Teasdale et al)
Grade GCS Focal neurological defict
I 15 None
II 13/14 - None
III 13/14 Present
IV 7-12 Present or absent
V 6 or less Present or absent
An older scale, called the Hunt and Hess scale was used in the past – it differs from the WFNS scale
in taking into consideration meningism which is due to irritation of the meninges by the blood, and
believed to correlate with cerebral vasospasm, in which circumstance treatment of the aneurysm is
thought to have a higher risk of post-procedural ischaemic deficit.
Hunt and Hess scale:
83

It is difficult to classify those ventilated as they cannot be assessed, and it may be undesirable to
reverse the ventilation in order to assess the patient as this may produce its own secondary insult..
The initial rupture of an aneurysm can result in a sudden loss of consciousness as the cerebral
circulation is disrupted. The level of consciousness may improve subsequently. Emergency care
must be focused upon protecting the airway and addressing immediate threats to life. Diagnosis is
determined by a CT scan in the first instance and then a lumbar puncture. Once the diagnosis has
been made referral to a neurosurgical expert will follow. Depending upon the severity of the bleed
the patient will either be transferred to a ward at the local neurosurgical centre or critical care.
Further imaging to aid detection of the culprit vessel will be completed once the patient is stable.
These include:
CT angiogram
Digital subtraction angiography (DSA)
84

The vessels of the brain are highlighted by dye and the bleeding point and type of abnormality is
detected.
Appropriate treatment can then be planned. Options include:
Image guided insertion of coils into the aneurysm to seal it.
Clipping of the aneurysm (only usually performed if the surgeon is evacuating an associated
intracerebral clot – often this is secondary to a middle cerebral artery aneurysm).
Surgical removal of an arteriovenous malformation, or treatment with stereotactic
radiosurgery either alone or sometimes combined with embolisation. This is usually
performed electively after recovery from the effects of the haemorrhage.
Unfortunately these measures to prevent re-bleeding do not prevent other side effects of bleeding
into the subarachnoid space. Hydrocephalus may develop as blood blocks the re-absorption system
in the CSF circulation (see A&P section). The treatment is the insertion of an extraventricular drain
(EVD). This drain is inserted into a ventricle and acts as an escape for the CSF that will build up. It is a
gravity drain and the amount drained can be controlled by adjusting the height of the chamber in
relation to the external auditory meatus or bridge of the nose (the anatomical zero point at which
CSF exits the ventricles through the foramen of monro and circulates). The blood will eventually
break down and the CSF system will return to function and the drain may be removed. If there are
on-going problems with hydrocephalus an internal shunt may be required.
85

Prevention of secondary injury is paramount. Spasm of cerebral vessels in response to the free blood
can cause devastating problems relating to cerebral perfusion. Spasm is most likely to develop
between day 3 and day 12 following the bleed. Risks of spasm gradually reduce until 21 days post
bleed when the risk is negligible. The treatment to ameliorate or prevent vessel spasm is a calcium
channel blocker called Nimodipine. 60 mg 4 hrly must be continued for the 21 day period. If the
patient cannot absorb the tablet form the IV is available in a 0.02% solution, both have the same
efficacy.
Prior to and following the securing of the aneurysm it is essential to maintain cerebral perfusion.
Before the aneurysm is secured the MAP must be maintained for perfusion (see head injury
management) as hypotension will cause reduced cerebral blood flow, however, hypertension may
be associated with a greater risk of re-bleed. Once the aneurysm is secured hypertensive therapy
86

may be required to maintain perfusion. This therapy must be guided by a neurosurgeon / neuro-
vascular intervention specialist.
Adequate circulating volume is also essential to cerebral perfusion therefore strict observation of
fluid balance and avoidance of dehydration is vital.
Patients who have had a SAH may suffer from disorders of sodium balance (see previous notes on
this subject). Any change in serum sodium, urine output must be investigated.
Subarachnoid haemorrhage – Activity 9.
Label the layers of the brain in this diagram
87

The Circle of Willis is ……….……………………….. found in the ………………………….
Space
Label the Ventricles:
88

Name at least two causes of SAH:
Label the main arteries in the Circle of Willis: 1, 2, 6, 9, 12, 17
89

6. Describe common symptoms of a SAH
90

7. A SAH is graded in severity using the ……………………………………scale
Briefly describe the 1 – 5 scale and conscious level / deficits expected in each
8. Name at least two diagnostic tests used to detect a SAH
91

9. List 4 complications of SAH
10. Nimodipine can reduce complications, which one?
a. Stroke
b. Re-bleed
c. Low sodium
d. High sodium
11.Side effects of Nimodipine include:
92

12.A drop in GCS could be caused by:
14. EVD stands for E V D
15. An EVD is the treatment for a complication of SAH, which one?
16.Why would we monitor sodium levels closely in this patient group?
17.What treatment is there available? Name three.
93

a/
b/
c/
18.What does HHH stand for?
COMPETENCIES & RECORDS OF SUPERVISED PRACTICE
94

- There are a number of clinical competencies that can be achieved associated with this
area of practice. Please refer to the national competency folder and documentation.
STANDARDS FOR ASSESSMENT
95

COMPETENCY ASSESSMENT CRITERIA
Stage 0 Not applicable
Stage 1 Foundation
Can demonstrate basic skills that contribute to the activity under direct supervision of a competent practitioner
Applies to a practitioner gaining experience and developing skills and knowledge Developing knowledge of relevant policies, procedures and guidelines
Stage 2 Intermediate
Can demonstrate acceptable performance in the activity, but requires some supervision and guidance
Relies on some instruction Demonstrates knowledge and understanding of relevant policies, procedures and
guidelines
Stage 3 Proficient
Can demonstrate competent performance in the activity to specific criteria without direct supervision
Can supervise and instruct others in a range of activities related to roles and responsibilities
Consistently applies knowledge and understanding of any relevant policies, procedures and guidelines to the activity
Stage 4 Advanced
Can demonstrate skilled activity with advanced theoretical knowledge and understanding based on current research/best practice, relevant policies, procedures and guidelines
96

Can problem solve through critical analysis and evaluate in more complex situations
Stage 5 Expert
Can demonstrate skilled performance based on intuition, expert knowledge and established practice
Can solve problems through critical analysis and evaluation in more complex situations
Can identify new areas for research and change, and leads in the development of practice/service delivery
Ref. Adapted from
Storey L., Howard J., Gilles A. (2002)
Radcliffe Medical
RECORD OF SUPERVISED PRACTICE
Supervised practice of undertaking care of a head injured patient
The minimum standard to be achieved is stage 3 ‘Proficient’ and level 1 of the national competencies relating to neuro critical care
97

Procedure Comments Standard Achieved
Date
98

Learner Signature:……………… Preceptor/Assessor Signature:……………………
RECORD OF SUPERVISED PRACTICE
Procedure Comments Standard Date
99

Achieved
100

Learner Signature:……………… Preceptor/Assessor Signature:……………………
101

102