
Nessun titolo diapositiva - static.livemedia.gr · Pietro Invernizzi Division of Gastroenterology...
66
Pietro Invernizzi Division of Gastroenterology and Center for Autoimmune Liver Diseases University of Milan-Bicocca Monza, Italy Athens, 24 March 2018 Primary biliary cholangitis
Transcript of Nessun titolo diapositiva - static.livemedia.gr · Pietro Invernizzi Division of Gastroenterology...
Pietro Invernizzi
Division of Gastroenterology and
Center for Autoimmune Liver Diseases
University of Milan-Bicocca
Monza, Italy
Athens, 24 March 2018
Primary biliary cholangitis

Center for Autoimmune Liver Diseases
06/2016 Female (dob 1965) - PBC --> OLT on 03/201707/2016 Female (dob 1952) - PBC + sclerodermia --> on waiting list10/2016 Female (dob 1974) - PBC --> OLT on 09/2017 11/2016 Female (dob 1948) - PBC --> on waiting list05/2017 Female (dob 1962) - PBC + IBD --> on waiting list05/2017 Female (dob 1969) - PBC --> on waiting list06/2017 Male (dob 1943) - PBC + HCC --> OLT on 12/201708/2017 Female (dob 1959) - PBC death on waiting list12/2017 Female (dob 1952) - PBC --> on waiting list07/2017 Male (dob 1988) - PBC + AIH --> under evaluation12/2017 Female (dob 1982) - PBC + AIH --> under evaluation
Patients reffered to liver transplantation (2016-2017):

Primary biliary cholangitis (n=600)
Autoimmune hepatistis (n=250)
Primary sclerosing cholangitis (n=250)
(Cholangiocarcinoma)
BASIC
Genetics/Epigenetics
Immunology
Neuroendocrine
Carcinogenesis
New drugs
TRANSLATIONAL / CLINICAL
Biomarkers
Clinical trials
Epidemiology
Center for Autoimmune Liver Diseases
Pietro Invernizzi
University of Milan-
Bicocca
Italy

www.easl.e
u
MAY 23 – 24 / 2014. Milan,
Italy
PRIMARY BILIARY CIRRHOSIS
New name
September 2015 - Position paper
“Changing Nomenclature for PBC:
From ‘cirrhosis’ to ‘cholangitis’”
• Hepatology. 2015 Sep 15.
• Gut. 2015 Sep 14.
• Gastroenterology. 2015 Sep 15.
• J Hepatol. 2015 Sep 10.
• Clin Gastroenterol Hepatol. 2015 Sep 16.
• Am J Gastroenterol. 2015 Sep 29.
• Dig Liver Dis. 2015 Sep 23.
• Clin Res Hepatol Gastroenterol. 2015 Oct;39(5):e57-9.
PRIMARY BILIARY CHOLANGITIS

Outline
Genetics
Networks
Novel drugs
?

Outline
Genetics
Networks
Novel drugs
?

Pre GWAS 2008 GWAS
HLA story in PBC

HLA story in PBC
Pre GWAS 2008 GWAS
2003
Monocentric
study
Italy
PBC = 186
HC = 558
2008
Multicentric
Study
Italy
PBC = 664
HC = 1992

HLA polymorphisms in Italian PBC
Multicenter Study
HLA PBC Controls Pc Odds Ratio (95% C.I.)
(n=664) (n=1992)
(%) (%)
DRB1*08 7.2 2.3 0.000 3.3 2.4-4.5
DRB1*11 13.6 30.0 0.000 0.4 0.3-0.4
DRB1*13 8.6 11.2 0.000 0.7 0.3-0.9
Invernizzi et al. Hepatology 2008

HLA story in PBC
Pre GWAS 2008 GWAS
2003
Monocentric
study
Italy
PBC = 186
HC = 558
2008
Multicentric
Study
Italy
PBC = 664
HC = 1992
2010
GWAS
Italy
USA
Canada
PBC = 993
HC = 2483

Risk variants:
HLA
IL12A
IL12RB2
IRF5
IKZF3/ORMDL
3
SPIB
Genome-wide association study in PBC
Liu & Invernizzi Nature Genetics 2010

HLA story in PBC
Pre GWAS 2008 GWAS
2003
Monocentric
study
Italy
PBC = 186
HC = 558
2008
Multicentric
Study
Italy
PBC = 664
HC = 1992
2010
GWAS
Italy
USA
Canada
PBC = 993
HC = 2483
2012
HLA-Dense array
Italy
PBC = 676
HC = 1440

HLA associations in PBC Dense array approach
676 Italian PBC
vs.
1440 controls
Results:
DRB1 (*08, *11)
DPB1
Invernizzi et al. Genes Immun 2012

HLA story in PBC
Pre GWAS 2008 GWAS
2003
Monocentric
study
Italy
PBC = 186
HC = 558
2008
Multicentric
Study
Italy
PBC = 664
HC = 1992
2010
GWAS
Italy
USA
Canada
PBC = 993
HC = 2483
2012
HLA-Dense array
Italy
PBC = 676
HC = 2483
Increasing study size
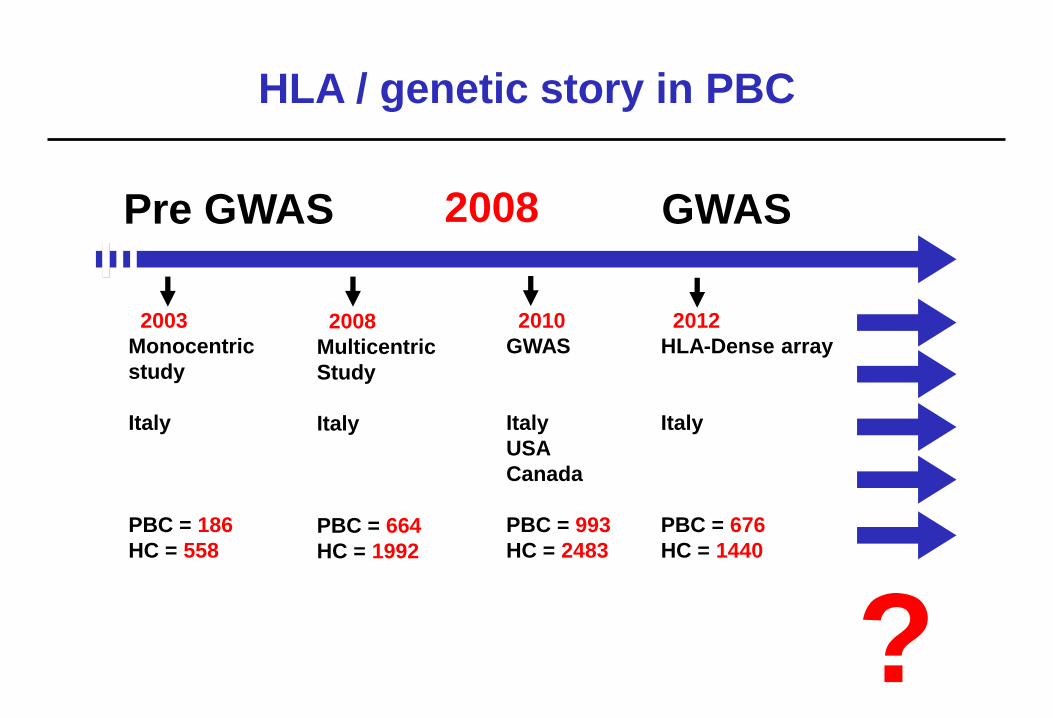
HLA / genetic story in PBC
Pre GWAS 2008 GWAS
2003
Monocentric
study
Italy
PBC = 186
HC = 558
2008
Multicentric
Study
Italy
PBC = 664
HC = 1992
2010
GWAS
Italy
USA
Canada
PBC = 993
HC = 2483
2012
HLA-Dense array
Italy
PBC = 676
HC = 1440
?

CountryDiscovery Discovery Validation Validation
Cases Controls Cases Controls
Canada 480 3,701 903 834
Italy 449 940 300 618
United Kingdom 1,816 5,161 1,792 2,515
United States of
America- - 721 294
Total 2,745 9,802 3,716 4,261
Cordell et al. Nat Commun 2015
International GWAS meta-analysis in PBCDiscovery and validation cohorts
PBC = 6461
Controls = 14.063Six novel risk loci:
2q12.1, 2q36.3, 4p16.3, 5q21.1
5q33.3, 6q23.3

Gene Loci Canada
USA
Italy-
Canada
USA
UK Japan
HLA Yes Yes Yes Yes Yes
IL12A - Yes Yes Yes -
IL12RB2 - Yes Yes Yes -
IRF5/TNPO3 - Yes Yes Yes -
ORMDL3/IK
ZF3
- Yes - Yes Yes
MMEL1 - Yes - Yes -
SPIB - Yes Yes Yes -
DENND1B - - Yes Yes -
CTLA-4 Yes - - -
STAT4 - Yes - Yes -
CD80 - - - Yes Yes
NFKB1 - - - Yes -
IL7R - - - Yes Yes
CXCR5 - - - Yes -
TNFRSF1A - - - Yes -
TNFSF1 - - - - Yes
POU2AF1 - - - - Yes
PBC “gene” list 2017
Increasing study size
Pre-GWAS 2009 2010 2011 2012

Sex chromosomes defects in PBC
Enhanced X monosomy (female)
Preferential X chromosome loss (female)
Increased Y chromosome loss (male)
Haploinsufficiency that unmasks PBC
susceptibility genes
Invernizzi et al. Lancet 2004
Invernizzi et al. J Immunol 2005
Miozzo et al. Hepatology 2007
Lleo et al. J Autoimmun 2013

Canadian & US
GWAS in PBC
US/Canadian
Chinese
Italian
XWAS in PBC
5,000 PBC vs. 10,000 controls
(USA, Canada, Italy, UK, Japan, China)
«XWAS: A Software Toolset for Genetic Data Analysis and
Association Studies of the X Chromosome»
J Hered 2015;106(5):666-71

And now?

Pathogenesis of PBC
Lleo & Invernizzi. J Hepatol 2012

Precision drugs (weapons)
PRECISION DRUGS
• FXR
• PPAR
• ASBT
• Anti-IL 12
• Anti-CXCL10
• Anti-CD20
• Anti-CD40L
• Anti-NOX 1 & 4

Anti-IL12 for PBC
Liu, Invernizzi, et al. Nature Genetics 2010
IL12
Genetic defect

Anti-IL12 for PBC
Liu, Invernizzi, et al. Nature Genetics 2010
IL12
Genetic defect
Anti-IL12
Clinical trial
Hirschfield, et al. Hepatology 2016

Outline
Genetics
Networks
Novel drugs
?

Networking story in PBC
2011

PI’s of the Global PBC Study Group (2012)
• Henk van Buuren, Rotterdam representing South of the Netherlands
• Gideon M. Hirschfield, Birmingham, UK
• Harry L.A. Janssen, Toronto, Canada
• Pietro Invernizzi, Milan, Italy
• Andrew L. Mason, Edmonton, Canada
• Cyriel Y. Ponsioen, Amsterdam representing North of the Netherlands
• Annarosa Floreani, Padova, Italy
• Christophe Corpechot, Paris, France
• Marlyn J. Mayo, Texas, USA
• Pier M. Battezzati, Milan, Italy
• Albert Parés, Barcelona, Spain
• Frederik Nevens, Leuven, Belgium
• Andrew K. Burroughs* & Douglas, London, UK
• Kris V. Kowdley, Seattle, USA
• Keith Lindor & Nicholas LaRusso, Rochester& Arizona, USA

Continuous growth
20111st prep meeting
20121st official meeting
n=3377 identified
Data collection
2014New presentations
n=4845 in database
20141st publication
Surrogate endpoint
Gastroenterology
20152nd publication
HCC
GUT
20156th investigator meeting
1 new submission
6 ongoing projects
3-9 new centers
20131st presentations
15 centers in 8 countries
2016n=6253 in database
20153rd publication
Globe score
Gastroenterology

Continuous growth
20111st prep meeting
20121st official meeting
n=3377 identified
Data collection
2014New presentations
n=4845 in database
20141st publication
Surrogate endpoint
Gastroenterology
20152nd publication
HCC
GUT
20156th investigator meeting
1 new submission
6 ongoing projects
3-9 new centers
20131st presentations
15 centers in 8 countries
2016n=6253 in database
20153rd publication
Globe score
Gastroenterology

Lammers et al. Gastroenterology 2014

Networking story in PBC
2011 2012

Gender differences in the age-related likelihood
of achieving UDCA response criteria
Proportion of patients who did not meet the
criteria for response to UDCA after a minimum
of 2 years treatment because of the ALT/AST
criterion (2 ULN) related to their age at
diagnosis
Carbone M et al. Gastroenterology 2013
Predictors of response to UDCA
Sex & Age
n=2353

Networking story in PBC
2011 2012
Swiss PBC
Austro-German PBC
2016-17
ERN-RARE LIVER
European Reference
Network

PBC is an heterogeneous disease
Variant syndromes PBC – AIH overlap syndrome may be found in ~10% and thepremature ductopenic variant in ~5% of cases
Autoantibody profile Anti-centromere antibodies (ACA) are found in ~30%, anti-sp100antibodies in ~20-30% and anti-gp210 antibodies in ~10% ofcases
Symptom profile Pruritus is present in 40% and fatigue is present in 45% of cases
Modes of disease progression
Portal hypertensive-type versus hepatocellular failure-typeprogression
Rate of disease progression
Ranging from no overt progression at one end of the spectrum,to ESLD occurring within a few years of diagnosis, at the other
The biochemical response to UDCA Variable; it strongly predicts the long-term outcome.


Challenge

Outline
Genetics
Networks
Novel drugs
?

EASL PBC Guidelines: 2009-2017
2009
•Generalized to Management of
Cholestatic Liver Diseases
•ALP 3 x ULN Paris-I
Barcelona
•Budesonide and Fibrates
2017•First Guidelines Specific to PBC
•Patient-Centric Name Change: PBCirrhosis to PBCholangitis
Overall focus on patients, clinical care &
support
•Clear goal of prevention of complications
•Acknowledgement of FXR pathway
•ALP cut-off (<1.5) and bilirubin GLOBE
UK-PBC
•Forward thinking (non-invasive, risk scores
added as part of diagnosis)
•OCA firmly represented as second line
therapy, in line with SmPC/USPI
•Budesonide and Fibrates

Licensed treatments for PBC
First line: Bile acids
> Ursodeoxycholic acid (UDCA)
> Tauro-UDCA
EASL Clinical Practice Guidelines:
The diagnosis and management of patients with primary biliary cholangitis.
J Hepatol 2017 Jul;67(1):145-172. doi: 10.1016/j.jhep.2017.03.022. Epub 2017 Apr 18
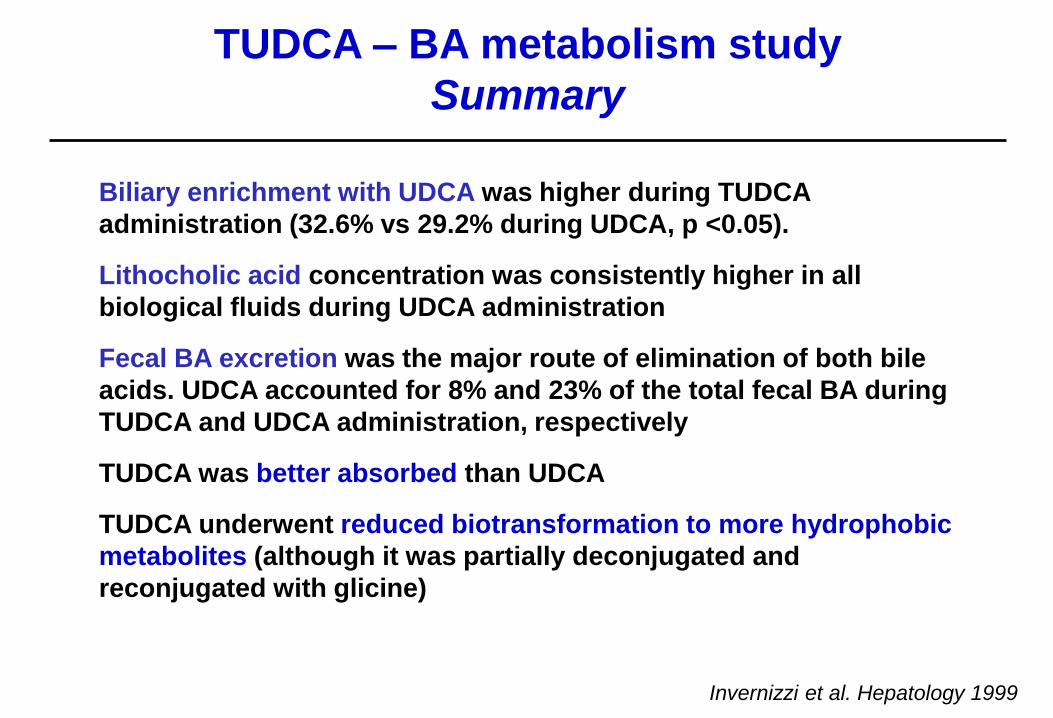
TUDCA – BA metabolism study
Summary
Biliary enrichment with UDCA was higher during TUDCA
administration (32.6% vs 29.2% during UDCA, p <0.05).
Lithocholic acid concentration was consistently higher in all
biological fluids during UDCA administration
Fecal BA excretion was the major route of elimination of both bile
acids. UDCA accounted for 8% and 23% of the total fecal BA during
TUDCA and UDCA administration, respectively
TUDCA was better absorbed than UDCA
TUDCA underwent reduced biotransformation to more hydrophobic
metabolites (although it was partially deconjugated and
reconjugated with glicine)
Invernizzi et al. Hepatology 1999

Licensed treatments for PBC
First line: Bile acids
> Ursodeoxycholic acid (UDCA)
> Tauro-UDCA
Italy
China
EASL Clinical Practice Guidelines:
The diagnosis and management of patients with primary biliary cholangitis.
J Hepatol 2017 Jul;67(1):145-172. doi: 10.1016/j.jhep.2017.03.022. Epub 2017 Apr 18
Licensed treatments for PBC
First line: Bile acids
> Ursodeoxycholic acid (UDCA)
> Tauro-UDCA
Italy
China
Second line:Obeticolic Acid (OCA)
EASL Clinical Practice Guidelines:
The diagnosis and management of patients with primary biliary cholangitis.
J Hepatol 2017 Jul;67(1):145-172. doi: 10.1016/j.jhep.2017.03.022. Epub 2017 Apr 18

Fib
rosis
/ d
ucto
pen
ia
Time
Immune-mediated cholangitis
Cholestasis
Immune-
modulatory
drugs
Anti-
cholestatic
drugs&
Cirrhosis
Anti-fibrotic drugs
Immuno-pathogenesis of PBC / ideal therapies

• FXR agonists
(OBETICOLIC ACID)
• PPAR agonists
• FGF19
• BIOLOGICS

FXR agonists
(OBETICOLIC ACID)

Obeticholic acid
Bile Acid
Metabolism
Lipid
Metabolism
Carbohydrate
Metabolism
Controls bile acid
biosynthesis, disposal
and transport
Downregulates hepatic
fatty acid biosynthesis and
VLDL formation
Insulin signaling & sensitivity
and hepatic gluconeogenesis
HO OH
CO2H
INT-747
RXRFXR
Inflammation &
Fibrosis
Anti-inflammatory & anti-
fibrotic effects in the liver,
intestine and kidney

Confidential Draft – Do Not Distribute
Re
sp
on
de
rs
(%
)
0 .5 3 6 9 1 2 O L E
3
O L E
6
O L E
9
O L E
1 2
O L E
1 5
O L E
1 8
O L E
2 1
O L E
2 4
0
2 0
4 0
6 0
8 0
P la c e b o U D C A n =
O C A 5 -1 0 m g U D C A n =
O C A 1 0 m g U D C A n =
M o n th s
D o u b le -B lin d P h a s e
R a n d o m iz e d T r e a tm e n t
O p e n -L a b e l E x te n s io n
A ll R e c e iv e O C A
5 m g T it r a t io n
***
***
***
***
***
***
***
***
*** ***
D B T r e a tm e n t G r o u p
P la c e b o p a t ie n ts s ta r t e d O C A d u r in g th e O L E n = 6 4 6 0 5 9 5 9 5 5 5 5 5 4 5 2
7 3 7 3 7 3 7 3 7 3 /6 6
7 0 7 0 7 0 7 0 7 0 /6 3 6 3 6 2 6 2 6 0 5 7 5 7 5 8 5 7
7 3 7 3 7 3 7 3 7 3 /6 4 6 4 5 9 6 1 5 9 5 8 5 9 5 8 5 7
Significant Increase in OCA-Treated Patients Meeting Primary
Endpoint During the Double-Blind Phase and the OLE
†Number of patients who continued treatment in the OLE after completing the double-blind phase of the study.***p<0.0001; p-values for comparing treatments in the DB phase are obtained using CMH General Association test stratified by randomization strata factor; OLE study ongoing. During the DB patients with missing values were considered non-responders (the n values represent the initial number of patients per treatment group). During the OLE patients with missing values and patients who had discontinued were excluded from the analysis at that timepoint. During the DB phase, 3 patients discontinued from placebo, 7 patients from OCA 5-10 mg, and 9 patients from 10 mg OCA.
†
†
†

Confidential Draft – Do Not Distribute
OCA Treatment Showed Sustained Improvement in ALP
Over Time
***p<0.0001; †p-value for comparing active treatments to placebo is obtained using an ANCOVA model with baseline value as a covariate and fixed effects for treatment and randomization strata factor, p-value based on LS mean difference values; ‡p-value for the within treatment comparisons are obtained using a paired t-test.
Mean (SD) Change from BL (U/L)
Placebo± UDCA
OCA 5-10 mg ± UDCA
OCA 10 mg ± UDCA
∆ 12 Months† -7.7 (88.0) -103.5 (87.0)*** -117.7 (73.3)***
∆ OLE 24 Months‡ -101.0 (87.2)*** -120.9 (96.6)*** -102.5 (79.4)***
0 3 6 9 1 2
0
1 0 0
2 0 0
3 0 0
4 0 0
5 0 0
M o n t h s
Me
an
(
SD
) A
LP
(
U/L
)
A L P 1 . 6 7 x U L N
O L E
3
O L E
6
O L E
1 2
U L N
5 m g T i t r a t i o n
D o u b l e - B l i n d P h a s e
R a n d o m i z e d T r e a t m e n t
O p e n - L a b e l E x t e n s i o n
A l l R e c e i v e O C A
O L E
9
O L E
1 5
O L E
1 8
O L E
2 1
O L E
2 4
O C A 5 - 1 0 m g U D C AP l a c e b o U D C A O C A 1 0 m g U D C A P l a c e b o p a t i e n t s r e c e i v i n g O C A d u r i n g O L E U D C A

© UEG. 2017
OCA adverse effects and caveats
Pruritus
• Common, dose related
Nevens et al NEJM 2016; 375: 631-643
Cholesterol changes
• Decrease in HDL cholesterol
Potential risk of chronic increase
in FGF19
• Increase risk of HCC in mouse
models
Warning in decompensated
cirrhosis*
38
56
68
01
10
*FDA Post-Marketing Letter reporting 19 deaths, 8 with reported causes (7 cases of Child B or C cirrhosis and receiving 5 mg daily;
8 additional cases reported serious liver injury without death (3 cases with Child B or C cirrhosis and receiving 5 mg daily

PPAR agonists

FIBRATES
MDR3PPARa
O-oxidation
enzymes
LTB4
ApoAII
ICAM-I
VCAM1
Anti-
inflammation
Biliary phospholipid
secretion
Inactivation of hydrophobic
bile acids
Protection of BECs
NF-kB
IL-1, IL-6
COX2
PGE E2
Th2
Ig production
AutoimmunityDohmen et al. (modified) WJG 2004
Use of PPAR agonists (fibrates ) in PBC
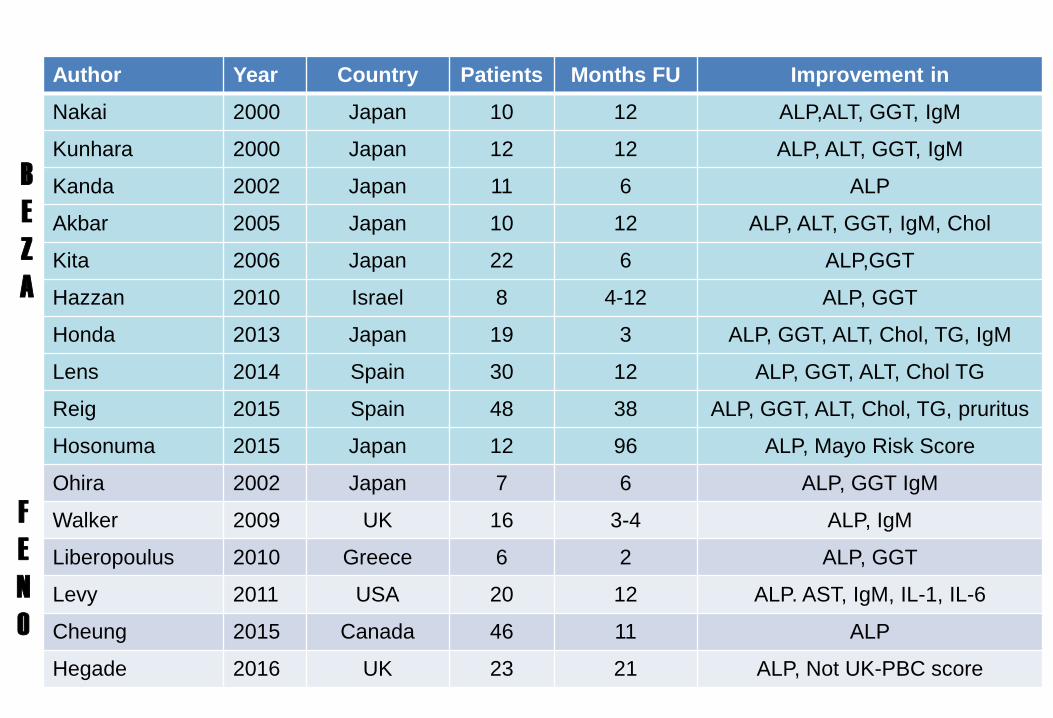
Author Year Country Patients Months FU Improvement in
Nakai 2000 Japan 10 12 ALP,ALT, GGT, IgM
Kunhara 2000 Japan 12 12 ALP, ALT, GGT, IgM
Kanda 2002 Japan 11 6 ALP
Akbar 2005 Japan 10 12 ALP, ALT, GGT, IgM, Chol
Kita 2006 Japan 22 6 ALP,GGT
Hazzan 2010 Israel 8 4-12 ALP, GGT
Honda 2013 Japan 19 3 ALP, GGT, ALT, Chol, TG, IgM
Lens 2014 Spain 30 12 ALP, GGT, ALT, Chol TG
Reig 2015 Spain 48 38 ALP, GGT, ALT, Chol, TG, pruritus
Hosonuma 2015 Japan 12 96 ALP, Mayo Risk Score
Ohira 2002 Japan 7 6 ALP, GGT IgM
Walker 2009 UK 16 3-4 ALP, IgM
Liberopoulus 2010 Greece 6 2 ALP, GGT
Levy 2011 USA 20 12 ALP. AST, IgM, IL-1, IL-6
Cheung 2015 Canada 46 11 ALP
Hegade 2016 UK 23 21 ALP, Not UK-PBC score
B
E
Z
A
F
E
N
O

2-year multicenter, double-blind, randomized, placebo-
controlled trial of bezafibrate (400 mg/d) + UDCA
Corpechot et al EASL 2017
Inadequate
biochemical
response to
UDCA
(Paris-2 criteria)
Randomization
N=100
Premature termination
N=4
Bezafibrate
400 mg/dl
N=50
Placebo
N=46
Placebo
N=44
Bezafibrate
400 mg/dl
N=50
Bezafibrate
400 mg/dl
N=48
Placebo
N=50
Premature termination
N=2
Premature termination
N=2
Recruiting centers: 21
Recruiting period: 22/10/2012 – 22/10/2014
UDCA 13-15 mg/Kg/d
M0 M3 M6 M9 M12 M15 M18 M21 M24

M24 complete biochemical responsePrimary endpoint
Corpechot et al EASL 2017
30%

M24 normal alkaline phosphatase levelSecondary endpoint
Corpechot et al EASL 2017
67%
M2
4 n
orm
alA
LP

Biologics

Immune-related precision drugs (weapons)
PRECISION DRUGS
• Anti-IL 12
• Anti-CXCL10
• Anti-CD20
• Anti-CD40L
• Anti-NOX 1 & 4

Anti-IL12 for PBC
Liu, Invernizzi, et al. Nature Genetics 2010
IL12
Genetic defect
Anti-IL12
Clinical trial
Hirschfield, et al. Hepatology 2015

Reduction in ALP
✓ 90 mg s.c. weeks 0,4, and 8 to 20 wks
✓ Median ALP 12% at 6 months
Hirschfield GH et al, Hepatology 2015
Anti-IL 12 for PBC
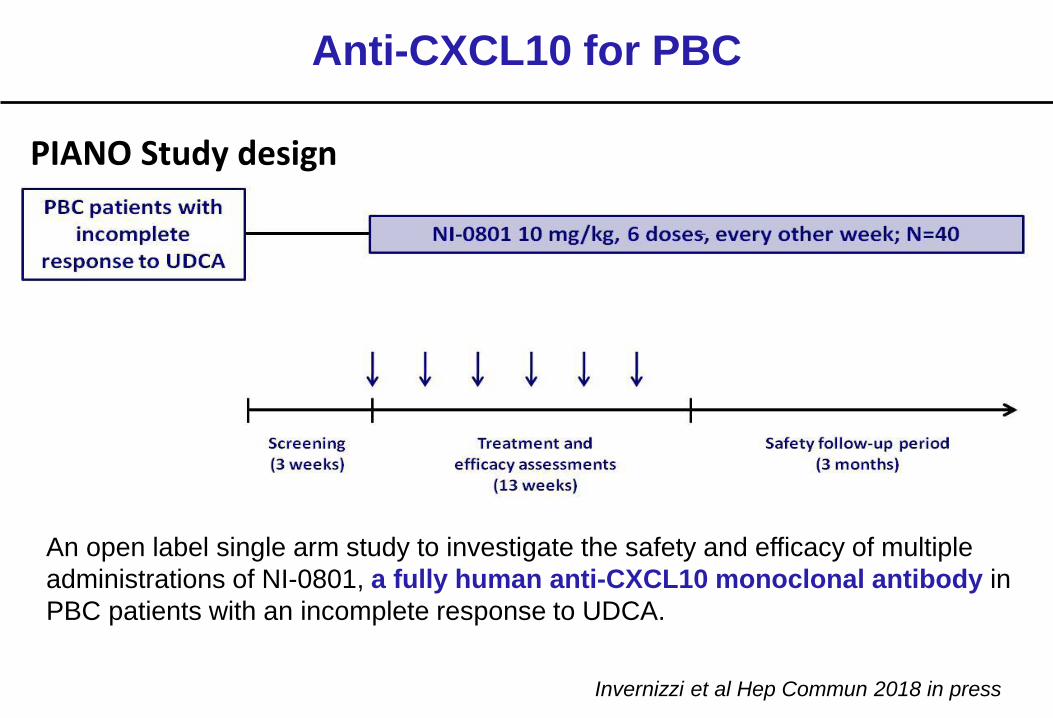
PIANO Study design
Anti-CXCL10 for PBC
An open label single arm study to investigate the safety and efficacy of multiple
administrations of NI-0801, a fully human anti-CXCL10 monoclonal antibody in
PBC patients with an incomplete response to UDCA.
Invernizzi et al Hep Commun 2018 in press

Tsuda M, et al. Hepatology. 2012
Anti-CD20 (Rituximab) for PBC
CONCLUSIONS:
• depletion of B cells influences
the induction, maintenance
and activation of both B and T
cells
• potential mechanism for
treatment of patients with
PBC with an incomplete
response to UDCA.

Meyer, et al. Am J Gastroenterol. 2013
Anti-CD20 (Rituximab) for PBC
CONCLUSIONS:
• safe and associated with a
significant decrease in
autoantibody production
• had limited biochemical
efficacy

NADPH oxidases (NOX): 7 ROS producing enzymes
NOX enzymes are the only specialized ROS-producing systems
NOX2NOX1 NOX3 NOX4 NOX5 DUOX1/2
NOX1 NOX2 NOX3 NOX4 NOX5 DUOX1/2
O2- O2
- O2- O2
- O2- O2
-
p22phoxp22phox p22phox p22phox

THANKS
DIVISION OF GASTROENTEROLOGY and CENTER FOR AUTOIMMUNE LIVER DISEASESPietro INVERNIZZIMarco CARBONEFrancesca BERNUZZIFederica MALINVERNOMarta GEMMAVincenzo RONCAAlessio GERUSSILaura CRISTOFERIGiulia BONATOVasiliki LIGOURA


















