NERI Seminar - The Fiscal Implications of Demographic Change in the Health Sector
31
The Fiscal Implications of Demographic Change in the Health Sector Paul Goldrick-Kelly NERI (Nevin Economic Research Institute) Dublin [email protected] www.NERInstitute.net
-
Upload
nevininstitute -
Category
Healthcare
-
view
276 -
download
0
Transcript of NERI Seminar - The Fiscal Implications of Demographic Change in the Health Sector

The Fiscal Implications of Demographic Change in the Health
Sector
Paul Goldrick-KellyNERI (Nevin Economic Research Institute)[email protected]

Outline• Introduction• Data• Model Components
– Demographic Cost Drivers– Income and Residual Cost Drivers
• Projection Model• Assumptions• Results• Conclusions

Introduction• Context
– Substantial increases over two decades preceding crisis of 2008 from low base (Wren,2004).
– Fiscal retrenchment results in reduction in spending after crash. Expenditure plans of previous government imply restrained spending growth.
– Demographic change proceeds apace, population (still) expanding and ageing. This has associated costs.

Figure 1: Real Current Public Health Expenditure Per Capita 2000-2013 SHA(2011) (pg. 4)
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 20130
500
1000
1500
2000
2500
3000
3500
Rea
l Cur
rent
Pub
lic E
xpen
ditu
re P
er
capi
ta a
t Con
stan
t 201
3 €
Pric
es
Source: CSO (2015) Ireland’s System of Health Accounts, Annual Results 2013 (Preliminary)

Current Health Expenditure as a Percentage of GDP 2013SHA(2011)
(EU15 Members denoted by *)
Irelan
d GDP H
ybrid
*
Switzerl
and
Sweden
*
Netherl
ands
*
German
y*
France
*
Irelan
d*
Belgium
*
Portug
al*
Norway
Icelan
d
Hunga
ry
Croatia
Czech
Rep
ublic
Cyprus
Poland
Lithu
ania
Estonia
Roman
ia0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
Current Public Expenditure Other Current Expenditure
Cur
rent
Hea
lth E
xpen
ditu
re a
s a
% o
f GD
P
Source: Eurostat, CSO (2015) Ireland’s System of Health Accounts, Annual Results 2013 (Preliminary),Author’s Calculations

• This working paper aims to:– Quantify the costs associated with demographic change on
overall current public health expenditure using a simple model.
– Produce projections of public health spending to 2035.
– Briefly highlight likely compositional changes to health spending induced by an ageing and expanding population.

Data
• Data Sources include:– CSO (2013) Population Projections M1F1 and M2F2 with
attendant life expectancy and mortality rate projections by year cohort.
– EU-15 Average Age and Gender Specific costs (EU AWG, 2012). Irish data unavailable
– NERI (2015) and OECD (2013) estimates of GDP growth.
– SHA (2011) estimates of Current Public Health Expenditure (CSO, 2015).

Figure 2: Age and Gender Specific Average per Capita Current Public Expenditure EU-15
2013 Adjusted (pg.6)
Under
1 yea
r
4 yea
rs
8 yea
rs
12 ye
ars
16 ye
ars
20 ye
ars
24 ye
ars
28 ye
ars
32 ye
ars
36 ye
ars
40 ye
ars
44 ye
ars
48 ye
ars
52 ye
ars
56 ye
ars
60 ye
ars
64 ye
ars
68 ye
ars
72 ye
ars
76 ye
ars
80 ye
ars
84 ye
ars
88 ye
ars
92 ye
ars
96 ye
ars€0.00
€2,000.00
€4,000.00
€6,000.00
€8,000.00
€10,000.00
€12,000.00
Male Female
Source: EU Commission 2012 Ageing Report

Model Components• Demographic Component
– Age Composition - Literature indicates not very important (Zweifel et al.,1999; Anderson and Hussey, 2002).
– Death Related Costs – More significant predictor of health costs, proximity to death. High concentration of cost immediately preceding death. (Stooker et al.,2001; McGrail et al.,2000)
– Morbidity – Will increases in life expectancy result in a larger portion of life spent ill or healthy? (Expansion vs Compression)

Demographic Cost Drivers
• Age Composition– Most intuitive demographic driver of demand increases.
– Given high relative cost for certain cohorts (infants, women of child-bearing age, elderly) change in fertility and life expectancy will likely impact healthcare utilisation and cost.
– Common assumption that increases in the elderly population will result in higher average expenditures.

• Death related costs– Hypothesis states that relevant factor in cost incidence and care
demands is proximity to death rather than age per se (Gray, 2005).
– Majority of lifetime healthcare costs accumulate at the end of an individuals life.
– Death related costs higher for younger patients than old ones. Generally offset by lower mortality rates.

• Morbidity Compression or Expansion– Debate as to whether healthcare improvements characterised by
expansions or contractions with respect morbidity.
– Morbidity expansion implies that increases in life expectancy translate into more years spent in ill-health. Chronic illness and disability drives increases.
– Morbidity compression proponents suggest that number of years spent in good health will increase as life expectancy increases. The relative portion of life spent in ill-health shrinks.
– Some evidence for morbidity compression outpacing life expectancy gains within “treatment groups”-Hubert and Frees (1994), Chakravarty et al. (2008).

Income and Residual Cost Drivers• Income
– Response of health demanded to income changes. Measured via and income elasticity of health demand. For every 1% change in income, what is the percentage change in health demanded?
• Residual– Expenditure growth left unexplained by demographic or income related factors.
– Thought to include factors such as:I. TechnologyII. Relative PricesIII. Institutional Arrangements and Policies
– Difficult to forecast these factors. Relative Prices, “Baumol Effect” may be relevant for particular sectors, but can’t be assumed for health service as a whole.

Current Public Health ExpenditureDemographicFactors
Age Composition of Population
Death Related Costs
Morbidity
Income
ResidualTechnology
Relative Prices
Institutional Arrangements
Determinants of Current Public Health Expenditure Growth

Projection Model
Per capita current public spending cost growth is a function of demographic cost pressure, the response of health demand to changes in income (Real GDP per Capita) and residual growth factors (OECD, 2015).

• Demographic cost growth:– Death Costs → Multiply age/gender specific per capita death costs
by decedent population by cohort. Mortality rates from CSO.
– Survivor Costs → Subtract cohort specific death costs from total health costs for that cohort and divide by the surviving population.
– Under morbidity expansion, survivor and death per capita costs remain constant. Under compression, per capita survivor costs adjusted according to LE gains. Constant ratio between per capita survivor and death related costs used to calculate adjusted death costs in accordance with survivor adjustments.

Assumptions• Demographic Component
– Central Scenario uses M1F1 projections. Sensitivity analyses uses M2F2.
– Death related costs= 4 times cost of oldest cohort (100+) for all below 60. Thereafter coefficient allowed decline linearly to unity for oldest cohort. (OECD 2015)
– Morbidity Compression= constant cost profile across forecast period.
– Morbidity expansion= gains in life expectancy translate into healthy years 1 for 1 over 65. Coefficient declines to zero at 44, i.e.LE gains don’t result in adjusted costs for individuals under 45 (Caley and Sidhu, 2010).

• Income Component– Central scenario sets ε at 0.8. Sensitivity performed for
elasticities of 0.6 and 1.
– M1F1 growth equals QEO projections to 2017, 3% annually thereafter (OECD).
– M2F2 growth same to 2017. Rest of forecast growth=Employment Growth + Productivity Growth (1.5%).

• Residual Component– Residual set at 1.5% annually. Country specific residual from
growth accounting not included because period analysed potentially atypical and would result in explosive cost growth.
– 2 scenarios are presented. First has residual constant for entirety of forecast period. Second sees residual decline linearly to zero by 2035. Second scenario models an implicit policy response to curb cost growth.

Scenario Gains in Life Expectancy= Gains in healthy life years
Cost Profile Remains Constant
Residual stays a constant 1.5%
Residual declines from 1.5% in 2013 to 0 in 2035
Scenario 1 Morbidity Expansion
Scenario 1 Morbidity Compression
Scenario 2 Morbidity Expansion
Scenario 2 Morbidity Compression
Table of Nomenclature for Results

Results
Years (Inclusive)
Million € Spending Pressure(at 2013 prices)
% Overall Annual Expenditure Growth due to demographics
Morbidity Expansion
Morbidity Compression
Morbidity Expansion
Morbidity Compression
Population Projection
M1F1 M2F2 M1F1 M2F2 M1F1 M2F2 M1F1 M2F2
2013-2015 €152.37 €142.42 €121.35 €111.40 1.16% 1.08% 0.92% 0.85%2016-2018 €195.91 €167.46 €162.53 €134.16 1.44% 1.24% 1.21% 1.00%2019-2021 €237.49 €189.23 €202.03 €154.01 1.67% 1.35% 1.44% 1.11%2022-2024 €265.95 €202.07 €228.21 €164.80 1.78% 1.38% 1.56% 1.15%2025-2027 €281.94 €210.23 €243.00 €171.96 1.79% 1.38% 1.58% 1.16%2028-2030 €295.92 €220.25 €256.14 €181.40 1.78% 1.39% 1.59% 1.18%2031-2033 €303.43 €223.18 €264.15 €185.17 1.73% 1.35% 1.57% 1.16%2034-2035 €306.85 €222.16 €267.87 €184.82 1.68% 1.30% 1.53% 1.13%
Table 1: Average Annual Direct Demographic Cost Pressure (pg. 14)

Figure 5: Cumulative Demographic Cost Pressure at 2013 Prices (pg.15)
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
2030
2031
2032
2033
2034
2035
0
1
2
3
4
5
6
M1F1 Morbidity Expansion M1F1 Morbidity Compression M2F2 Morbidity Expansion M2F2 Morbidity Compression
Cum
ulat
ive
Dem
ogra
phic
Cos
t Pre
ssur
e 20
13
Pric
es (€
Bill
ions
)

Figure 6: Decomposition of Real Average per Capita Current Health Expenditure growth 2013-2035 (pg.18)
Expan
ded M
orbidi
ty Sce
nario
1
Compre
ssion
of M
orbidi
ty Sce
nario
1
Expan
ded M
orbidi
ty Sce
nario
2
Compre
ssion
of M
orbidi
ty Sce
nario
2
Averag
e Rea
l GDP G
rowth
Per Cap
ita0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
4.00%
Demographic Component Income Component Residual Component
Ann
ual A
vera
ge P
er C
apita
Cos
t Gro
wth

Figure 7: M1F1 Projections 2035 Sensitivity Analysis according in Income
Elasticity (pg.19)
Mobidity Expansion Scenario 1
Mobidity Compression Scenario 1
Mobidity Expansion Scenario 2
Mobidity Compression Scenario 2
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
7.29% 7.29% 7.29% 7.29%
2.91% 2.48%1.34% 0.97%
Current Public Spending as % GDP 2013 Relative Current Public Spending Increase % GDP 2035
Pu
bli
c H
ealt
h S
pen
din
g as
a %
of G
DP

Figure 8: M2F2 Projections 2035 Sensitivity Analysis according in
Income Elasticity (pg.21)
Mobidity Expansion Scenario 1 Mobidity Compression Scenario 1
Mobidity Expansion Scenario 2 Mobidity Compression Scenario 2
-2.00%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
7.29% 7.29% 7.29% 7.29%
2.91% 2.48%1.34% 0.97%
0.21%0.18%
0.18%0.16%
Current Public Spending as a % GDP 2013 Relative Increase in Spending as % GDP M1F1Relative Deviation from M1F1 Estimates as % GDP
Cur
rent
Pub
lic H
ealth
Spe
ndin
g as
a %
of G
DP

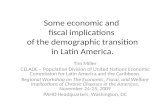
Figure 9: Age Decomposition of Current Health Expenditure Cost Growth (pg.22)
2013
2035
M1F
1 Morb
idity
Expan
sion
2035
M1F
1 Morb
idity
Compre
ssion
2035
M2F
2 Morb
idity
Expan
sion
2035
M2F
2 Morb
idity
Compre
ssion
0%10%20%30%40%50%60%70%80%90%
100%
70.00%58.68% 59.63% 56.16% 57.06%
30.00%41.32% 40.37% 43.84% 42.94%
Under 65 Over 65

Conclusions• Significant demographic cost pressures exist in the
forecast model.– Annual cost pressure exceeds €100 million in all cases.
– Doesn’t attain €200 for MC M2F2. In all other cases, exceeds €200 million from 2019. Reaches €300 million in 2034 in ME M1F1.
– Cost growth ≈ 1% annually
– Cumulative demographic costs exceed €1 billion between 2019 and 2021. Range from €3.57 billion to €5.66 billion in 2035.

• Current Public Health Spending will increase to 2035. – Range of central estimates between 8.3 and 10.2% of forecast
GDP in 2035, Though this is higher under the most pessimistic assumption set (maximum ≈ 11.6%).
• Changes in composition of public health spending.– Over 65s go from 30% to over 40% of spend 2013 to 2035.

• Complicating factors to consider include:– Possible inefficiency within the current system upwardly biasing forecast
estimates.
– Absence of Irish Specific cost profiles.
– Residual cost growth accuracy given its lack of explanatory power.
– European and domestic rules restraining expenditure growth.
– Likely endogeneity between components.
– Political Choices.

Policy Questions• What are appropriate investment levels?
• Are there efficiencies that can mitigate residual cost growth?
• What is the vision for the health service?
• What is a reasonable time frame for such a vision’s realisation?

www.NERInstitute.net