NEPHROLOGY CONFERENCEkidneykidsja.com/wp-content/uploads/Genes-ethnicity-and... · 2016. 4. 21. ·...
46
1 st JAMAICAN PAEDIATRIC NEPHROLOGY CONFERENCE Jamaica Conference Centre Kingston Jamaica October 4 th 2014 in association with
Transcript of NEPHROLOGY CONFERENCEkidneykidsja.com/wp-content/uploads/Genes-ethnicity-and... · 2016. 4. 21. ·...

1st JAMAICAN PAEDIATRIC NEPHROLOGY CONFERENCE
Jamaica Conference Centre
Kingston Jamaica October 4th 2014
in association with

Genes, ethnicity and nephro1c syndrome
Rulan S. Parekh Professor of Pediatrics and Medicine
University of Toronto

Disclosures
• None

Learning Objec1ves
At the end of this session you will be able to:
1. Understand the impact of ethnicity on kidney disease outcomes
2. Understand geneDc risk leading to progression of kidney disease

Outline
• GeneDc causes of nephroDc syndrome and FSGS • Burden of FSGS/ESRD among African Americans • Discovery of chromosome 22 and progression of FSGS
• Clinical ImplicaDons

Gene1c risk
• SuscepDbility for nephroDc syndrome • Risk for progression to end stage renal disease

Genes Associated with Nephro1c Syndrome (Mendelian)
• Known modes of inheritance – Autosomal dominant/recessive/ X-‐linked
• EsDmated 25% of all steroid resistant focal segmental glomerulosclerosis have geneDc disorders – OveresDmated geneDc risk? – DefiniDon of steroid resistance varies – Clinical protocols also vary by center

Genes Associated with Nephro1c Syndrome (Mendelian)

TA Manolio et al. Nature 461, 747-‐753 (2009)
Odds RaDo
Feasibility of iden1fying gene1c variants by risk allele frequency and strength of gene1c effect

Architecture of kidney disease
FSGS
Genes
Environment
CKD
Genes
Environment
ESRD
Genes
Environment
Disease suscep1bility Disease Progression

Gene1c risk
• SuscepDbility for nephroDc syndrome • Risk for progression to end stage renal disease

On average, two humans are iden1cal in 99.1% of their DNA composi1on
• HapMap demonstrated that most variaDons are observed in the populaDons sampled but many do have difference in allele frequencies

Why do we think that genes contribute kidney disease?
• Clustering of kidney disease among families • Family history of kidney disease or ESRD increases risk significantly
– Family history of 2 members with kidney disease OR of ESRD 10.4 (95%CI 2.7-‐40)
• Familial clustering of specific phenotypes – FSGS – IgA nephropathy – DiabeDc nephropathy
• Heritability of kidney funcDon – 33-‐82%
• Ancestry – African Americans – Asians – Europeans

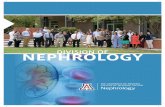
Appel, L. J. et al. Arch Intern Med 2008;168:832-‐839.
Cumula1ve incidence of composite outcome in the AASK trial and cohort

USRDS 2007
In 2006, rates of ESRD Whites 279 per million popula1on African Americans 1010 per million popula1on (~4.2 1mes greater than Whites) Na1ve Americans 489 per million popula1on (~1.9 1mes greater than Whites) Asians 388 per million popula1on (~1.3 1mes greater than Whites)
Incidence by race in the US New cases of ESRD

Incidence of reported ESRD by primary diagnosis in the US (2002-‐2006)
0
5
10
15
20
25
30
35
40
45
Diabetes Hypertension Glomerular Other
AllWhiteAfrican American
FSGS most common and African Americans > Whites


Approaches to iden1fying genes for ESRD • Linkage studies
– IdenDfy families with affected members
– Determine if suscepDbility gene (allele) is cosegregaDng with disease in the family
• AssociaDon studies – IdenDfy affected and unaffecteds – Compare differences in allele
frequencies • Candidate genes • Mapping by Admixture Linkage Disequilibrium (MALD)
• Genome wide associaDon study (GWAS)
AssociaDon No AssociaDon
Affected Unaffected Affected Unaffected

West Africans
Europeans
Admixture Mapping A approach to idenDfy disease genes in an admixed popula1on, such as African Americans, who derived from the mixing of the two geneDcally isolated populaDons (West Africans and Europeans)
African Americans

1 generaDon ago
2 generaDons ago
3 generaDons ago
4 generaDons ago
Admixture creates a mosaic
Two African chromosomes
Two European
chromosomes
One African, one European chromosome
Today

How does admixture mapping work?
African chromosome
European chromosome
Disease locus
These cases will be enriched in African ancestry at the disease locus compared to controls
Cases with disease (higher risk in African)

Nat Gen Oct. 2008 40(10): 1185-‐92
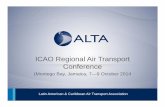
Admixture mapping can iden1fy novel suscep1bility locus for ESRD

Strong evidence of excess African ancestry on chromosome 22q12: 95% CI contained 22 genes

Nat Gen Oct. 2008 40(10)
Admixture mapping can iden1fy novel suscep1bility locus for FSGS

• Data recently available from the 1000 Genome Project • Region of interest highlighted by admixture mapping • APOL1 has potenDal “protecDve” effects from infecDous risk • APOL1, 2, 3, 4 are all important in selecDon • Frequency of the APOL1 variants (similar to MYH9) is high indicaDng gene or gene-‐ environment interacDon
• Mechanism of APOL1 leading to kidney disease is unclear


APOL1 associa1on with FSGS
Haplotype SNPs Pafern on Inheritance
FSGS Frequency
Control Frequency
G1-‐nonsynomous coding variants
rs73885319 rs60910145
Recessive 52% 18%
G2-‐ deleDon of 2 aminoacids
rs71785313 Recessive 23% 15%

Replica1on Studies of APOL1
• HIVAN-‐3-‐5 Dmes higher risk • Proteinuria-‐1-‐2 Dmes higher risk • ESRD-‐ 2 Dmes higher risk • FSGS-‐ 3-‐5 Dmes higher risk
• Always among African Americans • Risk alleles only present in those with west african ancestry

Associa1on but what about progression?

1.92 (1.19, 3.10) p=0.008
ESRD-‐free survival by APOL1 risk alleles among prevalent CKD (n=179)

Does blood pressure modify risk?


AASK Exposure, Outcome and Analysis • Exposure: SNPs on chromosome 22
3 SNPs in APOL1 4 SNPs in MYH9
• Outcome: Composite of ESRD or doubling of serum creatinine (halving of GFR in intervention-based analysis)
• Analysis: Time to event analysis using Cox proportional hazard models- and effect of BP
rs16996616
rs71785313
rs73885319
rs60910145
rs4821481
rs3752462
rs2032487
rs4821480
MYH9
APOL1
E1 Haplotype
G1 Haplotype
6bp deletion

0.00
0.25
0.50
0.75
1.00
Prop
ortio
n Su
rvivi
ng
0 2 4 6 8 10Follow-up (years)
0 copy of APOL1 risk variants
1 copy of APOL1 risk variants
2 copies of APOL1 risk variants
HR 1.9 (P<0.001) comparing 2 copies to all others
Two copies of the APOL1 risk variants associated with faster CKD progression in 693 AAs in AASK

0.00
0.25
0.50
0.75
1.00
Prop
ortio
n Su
rviv
ing
0 2 4 6 8 10Follow-up (years)
APOL1 non-‐risk
APOL1 risk
APOL1 non-‐risk
APOL1 risk
No Proteinuria
Proteinuria
Pinterac1on= 0.16
APOL1 risk variants did not modify effects of proteinuria on CKD progression in AASK

0.00
0.25
0.50
0.75
1.00
Prop
ortio
n Su
rviv
ing
0 1 2 3 4Follow-up (years)
APOL1 non-‐risk Intensive
APOL1 risk Standard
APOL1 risk Intensive
APOL1 non-‐risk Standard
Pinterac1on= 0.72
APOL1 risk variants did not modify effects of BP goals (intensive vs standard) on CKD progression
in AASK

0.00
0.25
0.50
0.75
1.00
Prop
ortio
n Su
rviv
ing
0 1 2 3 4Follow-up (years)
APOL1 risk Other
APOL1 non-‐risk ACE-‐I APOL1 non-‐risk
Other
APOL1 risk ACE-‐I
Pinterac1on= 0.72
APOL1 risk variants did not modify effects of drug therapies (ACE-I vs Other) on CKD progression in
AASK

EA
AA APOL1 Non-‐Risk
AA APOL1 Risk
APOL1-Non Risk AA vs. all EA HR 1.6 (1.1, 2.2)
APOL1-Risk AA vs. all EA HR 2.7 (1.8, 4.1)
AA with APOL1 Risk Variants Have Faster CKD Progression than EA and AA without APOL1 Risk:
CKD Patients without Diabetes

EA
AA APOL1 Non-‐Risk
AA APOL1 Risk
APOL1-Risk AA vs. all EA HR 2.0 (1.4, 2.7)
APOL1-Non Risk AA vs. all EA HR 1.4 (1.1, 1.8)
AA with APOL1 Risk Variants Have Faster CKD Progression than EA and AA without APOL1 Risk:
CKD Patients with Diabetes

Differences in eGFR Slope Comparing AA Risk Groups vs all EAs, Stratified by Diabetes Status
Difference in eGFR Slope
With Diabetes Without Diabetes EsDmate ml/min/yr P value EsDmate ml/
min/yr P value
AA APOL1 risk vs. All EA* -‐1.3 <0.001 -‐1.05 <0.001
AA APOL1 non-‐risk vs. All EA* -‐0.4 0.09 0.08 0.65
AA APOL1 risk vs. AA APOL1 non-‐risk -‐1.1 0.005 -‐1.2 <0.001
*Adjusted for age, gender, clinical site and baseline eGFR, educaDon, nephrologist use and ACE/ARB use, systolic blood pressure, body mass index, HBA1c and smoking

Challenges with APOL1 • Allele frequency is high ~11% APOL1 carriers of risk allele
• Need a second hit to develop disease – Gene x gene or gene x environment interacDon
• SelecDon panern is uncertain • Biological mechanism unclear • Is it a marker or is it causal?

Gene1cs just got personal

When in Doubt, Spit It Out “Spit Party”
New York Times, Lifestyles Sec1on, 2008

Clinical u1lity and validity in gene1c screening
• Need to ask: – Will you change therapy? – How will you counsel the family given that variable inheritance panerns and penetrance
– Which genes ? Only those with known funcDonal exons variants? What do we do with discovery of new variants and polymorphisms during tesDng
– Not yet for APOL1

Individualized medicine in nephro1c syndrome
• Ethnicity does impact incidence and outcomes in nephroDc syndrome
• Individualizing medical care: – Ancestry (ethnicity) – Family and personal medical history – Personal circumstances (stress, access to care, etc) – Exposures, medicines and supplements, etc
• GeneDc informaDon when appropriate and available

Ques1ons?