Neonatal seizure2
27
NEONATAL NEONATAL SEIZURES SEIZURES Soumya Ranjan Parida Basic B.Sc. Nursing 4 th year Sum Nursing College
-
Upload
soumya-ranjan-parida -
Category
Healthcare
-
view
90 -
download
0
Transcript of Neonatal seizure2
NEONATAL NEONATAL SEIZURESSEIZURES
Soumya Ranjan ParidaBasic B.Sc. Nursing 4th year
Sum Nursing College

INTRODUCTIONINTRODUCTION
IT IS A MEDICAL EMERGENCY COMMONLY OBSERVED NEUROLOGICAL
PROBLEM IN NEW BORNS MAY AFFECT FUTURE NEUROLOGICAL &
MENTAL DEVELOPMENT INCIDENCE - TERM 0.2-0.8%
PRE TERM 15-20%

DEFINITIONDEFINITION
PAROXYSMAL ALTERATION OF NEUROLOGICAL FUNCTIONS
MOTOR BEHAVIOUR AUTONOMIC• DEFINITION INCLUDES EPILEPTIC SEIZURES – CLONIC NON-EPILEPTIC SEIZURES – SUBTLE,
GENERALISED TONIC EEG SEIZURES

CLASSIFICATIONCLASSIFICATION
SUBTLE [FRAGMENTARY] – 48%CLONIC – 32%MYOCLONIC –13%TONIC – 7%APNOEA* NON-EPILEPTIC MOVEMENTS –
JITTERINESS OR TREMORS, NORMAL MOVEMENTS SEEN IN PRETERM
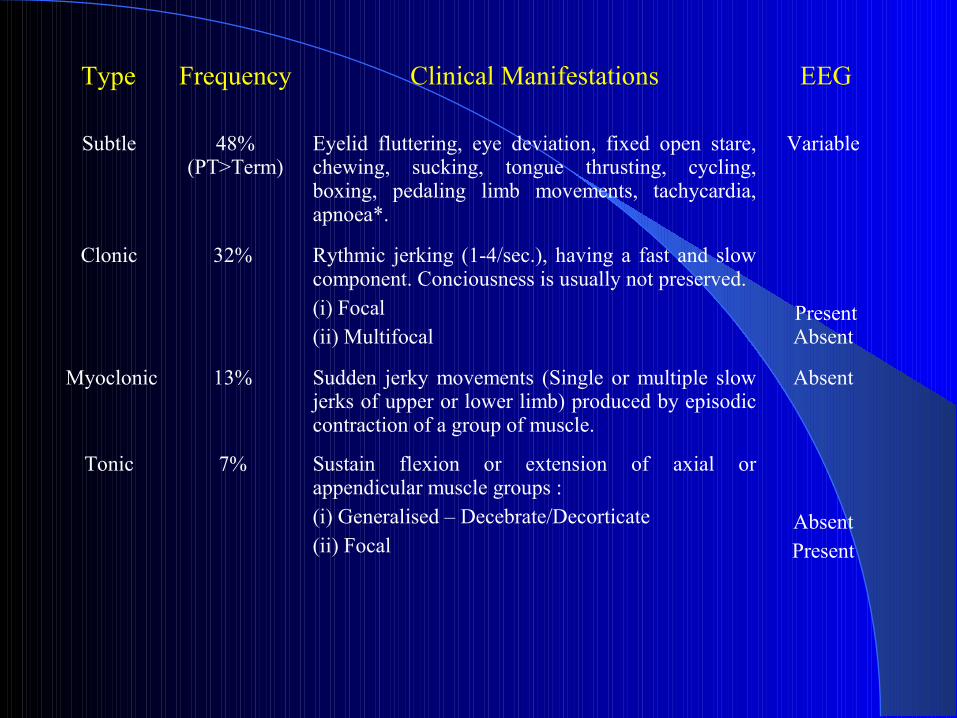
Type Frequency Clinical Manifestations EEG
Subtle 48% (PT>Term)
Eyelid fluttering, eye deviation, fixed open stare, chewing, sucking, tongue thrusting, cycling, boxing, pedaling limb movements, tachycardia, apnoea*.
Variable
Clonic 32% Rythmic jerking (1-4/sec.), having a fast and slow component. Conciousness is usually not preserved. (i) Focal (ii) Multifocal
Present Absent
Myoclonic 13% Sudden jerky movements (Single or multiple slow jerks of upper or lower limb) produced by episodic contraction of a group of muscle.
Absent
Tonic 7% Sustain flexion or extension of axial or appendicular muscle groups : (i) Generalised – Decebrate/Decorticate(ii) Focal
Absent Present
JITTERINESS OR TREMORSJITTERINESS OR TREMORS Fast Movement (4 – 6 per second) Absence of fast and slow components. Stimulus sensitive. Frequency is more. Symmetrical tremors of limbs/extremities. Abolish by sucking or flexion of limb. Not associated with chewing movements, Tongue
thrusting and eye movements. Not associated with physiological (HR, RR,
SaO2)/Autonomic changes and EEG correlates.
NORMAL MOVEMENTS NORMAL MOVEMENTS COMMONLY SEEN IN PRETERMSCOMMONLY SEEN IN PRETERMS
Benign neonatal sleep myoclonus in REM sleep in preterm with normal EEG.
Fragmentary myoclonic jerks. Eye movements – Roving or dysconjugate
eye movements with occasional non- sustained nystagmoid jerks.
CAUSESCAUSES
AGE
FIRST DAY
BETWEEN 1-3 DAYS
BETWEEN 4-14 DAYS
BETWEEN 2-8 WEEKS
CAUSES
HIE, HYPOCALCEMIA, PYRIDOXINE DEPENDENCY
ICH, HYPOGLYCEMIA, INBORN ERRORS OF METABOLISM
INFECTION, METABOLIC, KERNICTERUS, TETANY
INFECTION, HEAD INJURY, IBM, BENIGN
COMMON CAUSES OF COMMON CAUSES OF NEONATAL SEIZURESNEONATAL SEIZURES
HIE Commonest cause of seizures in neonates. Secondary to Perinatal asphyxia. Constituting 50-65% of all neonatal seizures. Seizures of HIE starts within 12 hours. Onset within 24-48 hrs. Subtle seizures are commonest.
ICH Seizures due to SAH, intra parenchymal hemorrhage or SDH
occur more often in term babies. Intraventricular hemorrhage more common in preterm babies. Mostly occur within 2-7 days.
Continue.....
COMMON CAUSES OF COMMON CAUSES OF NEONATAL SEIZURESNEONATAL SEIZURES
Hypoglycemia – Screening is indicated in VLBW (<1500 gm) Preterm (<35 weeks) IUGR (SGA) Infants of diabetic mother Large for gestational age Infants with Rh haemolytic disease Infants born to mothers receiving therapy (terbutaline/
propanolol/oral hypoglycaemic agents) Neonates with perinatal birth asphyxia/ polycythemia/
sepsis/shock/RDS/hypothermia Neonates on IV fluid and TPN
Continue.....
COMMON CAUSES OF COMMON CAUSES OF NEONATAL SEIZURESNEONATAL SEIZURES
Hypocalcemia – Screening is indicated in :
1. Early onset (within first 3 days) Prematurity Infants of diabetic mother Birth asphyxia
2. Late onset (presents at end of first week) Hypomagnesemia Increased phosphate load (cow’s milk) Hypoparathyroidism Vitamin D deficiency

MANAGEMENTMANAGEMENT
INCLUDES DIAGNOSIS AND TREATMENT
DIAGNOSIS
- HISTORY TAKING
- GENERAL PHYSICAL EXAMINATION
- SYSTEMIC EXAMINATION

INVESTIGATIONSINVESTIGATIONS
FIRST LINE INVESTIGATIONS - CBC, ELECTROLYTES [Ca+2, PO4, Na+1, Mg+2],
BLOOD SUGAR, BILIRUBIN, VENOUS pH AND BASE EXCESS
- CSF & BLOOD CULTURE - EEG & CRANIAL USG SECOND LINE INVESTIGATIONS - CT SCAN / MRI - TORCH / VDRL - AMMONIA / ABG / LACTATE / PYRUVATE LEVELS - BABY’S METABOLIC SCREENING
EEG (Electroencephalography)EEG (Electroencephalography)
Both Diagnostic and Prognostic. Ictal EEG is useful for Diagnosis of suspected
seizures and in neonates receiving muscle relaxant therapy.
Interictal EEG is useful for long term prognosis. Abnormal EEG indicates high risk for
neurological sequalae. Persistently abnormal EEG increases the risk of
seizure recurrence.

TREATMENTTREATMENT
VENTILATION, CIRCULATION & CEREBRAL METABOLISM (TABC)
SPECIFIC THERAPY TARGETED FOR UNDERLYING ETIOLOGY
ANTIEPILEPTIC DRUGS [AED]

ALGORITHM FOR MANAGEMENT ALGORITHM FOR MANAGEMENT OF NEONATAL SEIZURESOF NEONATAL SEIZURES
ABNORMAL MOVEMENTS
SEIZURES JITTERINESS
CLINICAL EVALUATION
PRIMARY MANAGEMENT DRAW BLOOD FOR
[TABC] INVESTIGATIONS
RBS [RANDOM BLOOD SUGAR]
CONTD....
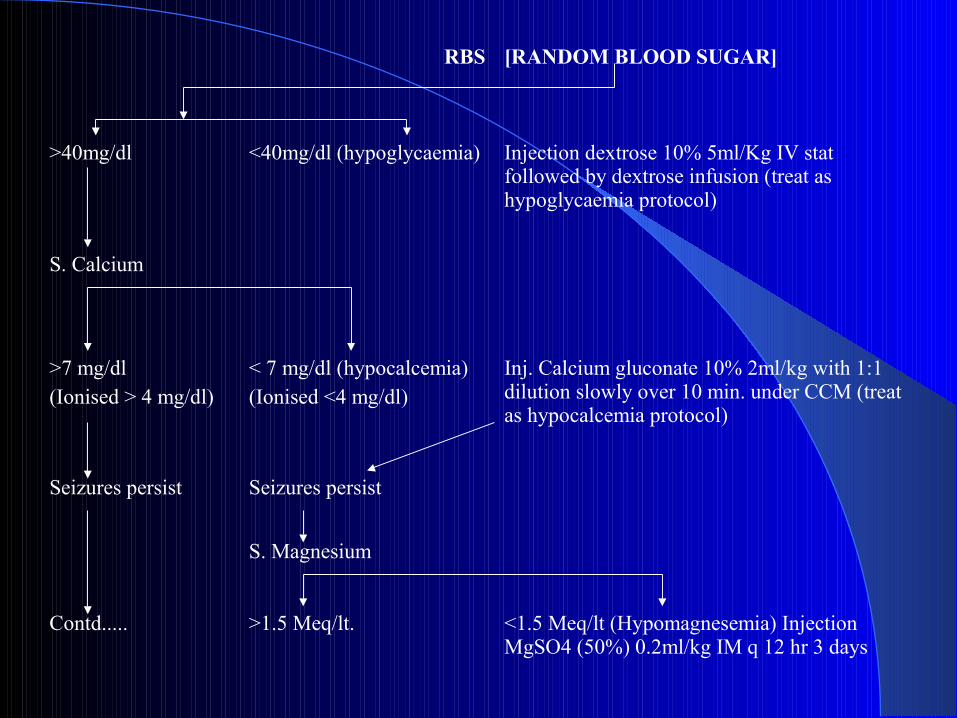
RBS [RANDOM BLOOD SUGAR]
>40mg/dl <40mg/dl (hypoglycaemia) Injection dextrose 10% 5ml/Kg IV stat followed by dextrose infusion (treat as hypoglycaemia protocol)
S. Calcium
>7 mg/dl(Ionised > 4 mg/dl)
< 7 mg/dl (hypocalcemia) (Ionised <4 mg/dl)
Inj. Calcium gluconate 10% 2ml/kg with 1:1 dilution slowly over 10 min. under CCM (treat as hypocalcemia protocol)
Seizures persist Seizures persist
S. Magnesium
Contd..... >1.5 Meq/lt. <1.5 Meq/lt (Hypomagnesemia) Injection MgSO4 (50%) 0.2ml/kg IM q 12 hr 3 days
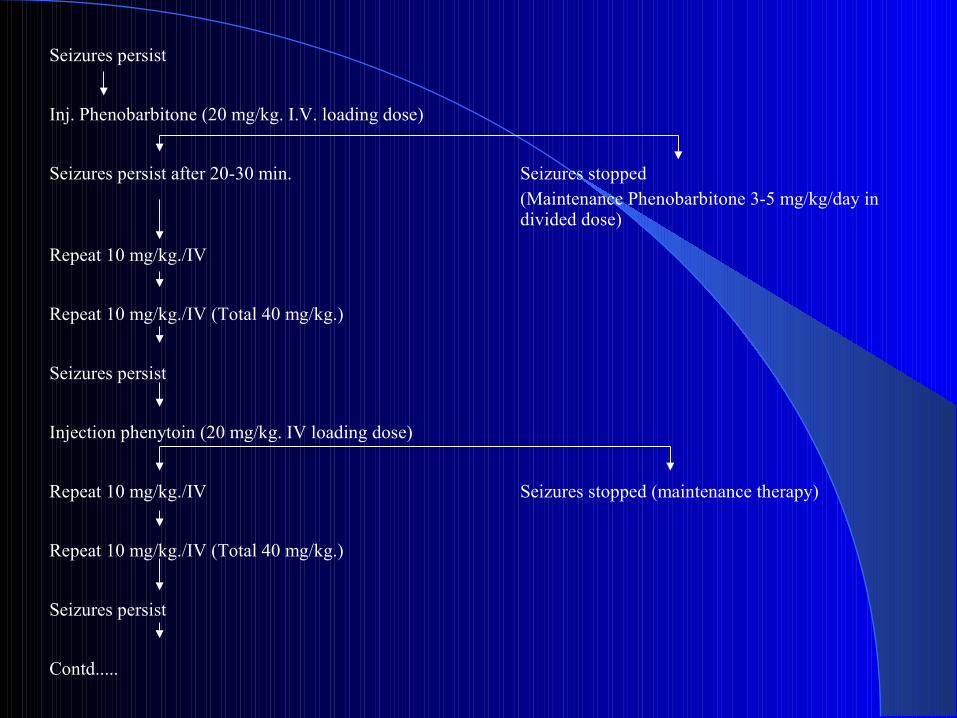
Seizures persist
Inj. Phenobarbitone (20 mg/kg. I.V. loading dose)
Seizures persist after 20-30 min. Seizures stopped(Maintenance Phenobarbitone 3-5 mg/kg/day in divided dose)
Repeat 10 mg/kg./IV
Repeat 10 mg/kg./IV (Total 40 mg/kg.)
Seizures persist
Injection phenytoin (20 mg/kg. IV loading dose)
Repeat 10 mg/kg./IV Seizures stopped (maintenance therapy)
Repeat 10 mg/kg./IV (Total 40 mg/kg.)
Seizures persist
Contd.....
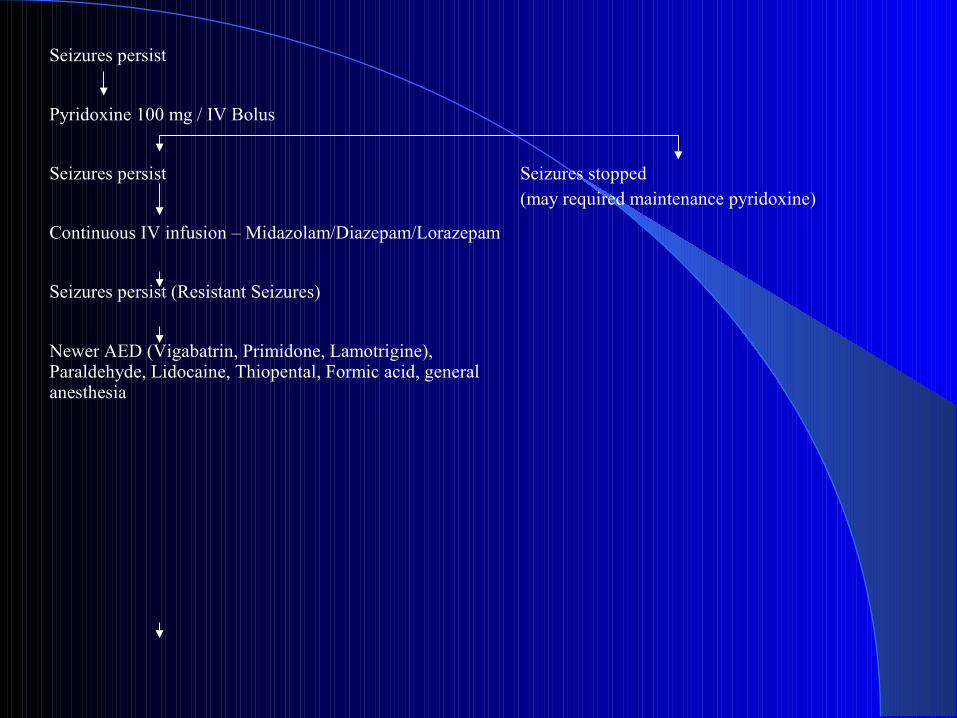
Seizures persist
Pyridoxine 100 mg / IV Bolus
Seizures persist Seizures stopped(may required maintenance pyridoxine)
Continuous IV infusion – Midazolam/Diazepam/Lorazepam
Seizures persist (Resistant Seizures)
Newer AED (Vigabatrin, Primidone, Lamotrigine), Paraldehyde, Lidocaine, Thiopental, Formic acid, general anesthesia
ANTIEPILEPTIC THERAPY ANTIEPILEPTIC THERAPY [AED][AED]
PHENOBARBITONE
DOSE – 20 mg/kg. IV Bolus Stat
40 mg/kg. IV Maximum Cumulative PHENYTOIN
DOSE – 20 mg/kg. IV Bolus Stat
40 mg/kg. IV Maximum Cumulative FOSPHENYTOIN
BENZODIAZEPINESBENZODIAZEPINES
DIAZEPAM Dose : 0.1 – 0.3 mg./kg. IV Slowly stat &
Infusion of 0.3 mg./kg./hr. MIDAZOLAM Dose : 0.15 mg/kg. IV stat followed by 0.1
mg/kg./hr. by infusion LORAZEPAM Dose : 0.10 mg/kg. over 2-5 minutes IV

OTHER THERAPIES OTHER THERAPIES PYRIDOXINE Dependency should be suspected in refractory
seizures, positive family history & if there is history of in utero fluttering
EEG typically shows generalized burst of spikes of 1-4 Hz.
Pyridoxine dependency requires a dose of 50 mg. per day & deficiency 5 mg./day
EXCHANGE TRANSFUSION Indicated in life threatening metabolic disorders,
accidental injection of LA, Transplacental transfer of maternal drugs & kernicterus
MAINTENANCE & DURATION OF AEDMAINTENANCE & DURATION OF AED
MAINTENANCE – Monotherapy is preferred. Wean the baby to only phenobarbitone.
DURATION – determined by the cause, neurological examination & EEG.
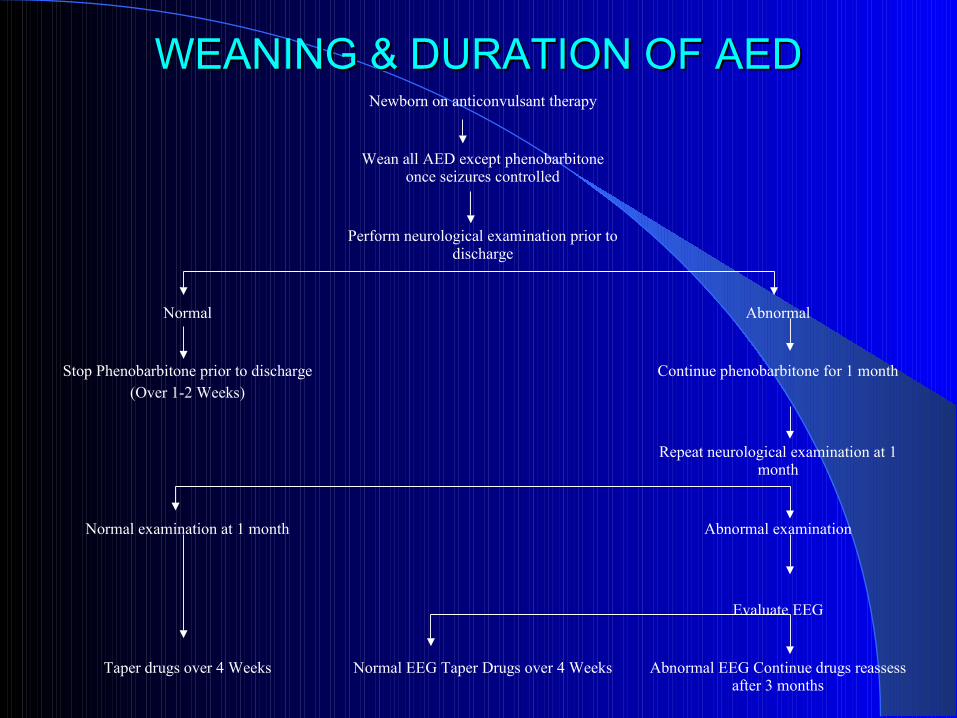
Newborn on anticonvulsant therapy
Wean all AED except phenobarbitone once seizures controlled
Perform neurological examination prior to discharge
Normal Abnormal
Stop Phenobarbitone prior to discharge(Over 1-2 Weeks)
Continue phenobarbitone for 1 month
Repeat neurological examination at 1 month
Normal examination at 1 month Abnormal examination
Evaluate EEG
Taper drugs over 4 Weeks Normal EEG Taper Drugs over 4 Weeks Abnormal EEG Continue drugs reassess after 3 months
WEANING & DURATION OF AEDWEANING & DURATION OF AED
PROGNOSISPROGNOSIS
NORMAL OUTCOME – 50-60%NEUROLOGICAL SEQUALAE – 30-40%
(C.P., M.R., SEIZURES) MORTALITY – 15-20% PROGNOSIS DEPENDS UPON
ETIOLOGY, SEIZURE PATTERN & EEG BACKGROUND
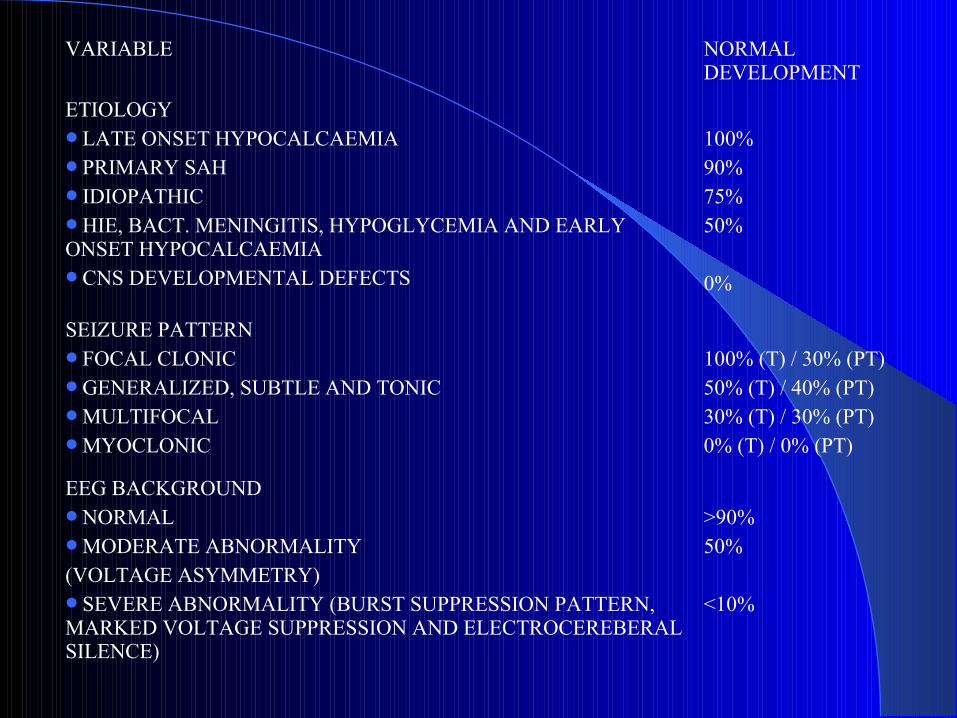
VARIABLE NORMAL DEVELOPMENT
ETIOLOGYLATE ONSET HYPOCALCAEMIAPRIMARY SAHIDIOPATHICHIE, BACT. MENINGITIS, HYPOGLYCEMIA AND EARLY ONSET HYPOCALCAEMIACNS DEVELOPMENTAL DEFECTS
100%90%75%50%
0%
SEIZURE PATTERNFOCAL CLONICGENERALIZED, SUBTLE AND TONICMULTIFOCAL MYOCLONIC
100% (T) / 30% (PT)50% (T) / 40% (PT)30% (T) / 30% (PT)0% (T) / 0% (PT)
EEG BACKGROUNDNORMALMODERATE ABNORMALITY(VOLTAGE ASYMMETRY)SEVERE ABNORMALITY (BURST SUPPRESSION PATTERN, MARKED VOLTAGE SUPPRESSION AND ELECTROCEREBERAL SILENCE)
>90%50%
<10%

THANKS