
Nebraska Mortar & Pestle - Nebraska Pharmacists · PDF fileThe Nebraska Mortar & Pestle (M&P)...
44
3 Daily News Dose - In Case You Missed It 4 Continuing Pharmacy Education Lesson #9 Pediatric Toxicological Emergencies 12 Creighton University School of Pharmacy & Health Professions News 13 University of Nebraska Medical Center College of Pharmacy News 15 Continuing Pharmacy Education Lesson #10 USP37-NF32 Chapter <795> Pharmaceutical Compounding Nonsterile Preparations Inside This Issue Inside This Issue Inside This Issue Inside This Issue Nebraska Mortar & Pestle July/August 2014 Volume 77, Number 4 Official Publication of the Nebraska Pharmacists Association For NPA Members 25 Rx and e Law - Why is that Pharmacist Asking so Many Questions? 26 Continuing Pharmacy Education Lesson #11 Legal and Business Aspects of the Changing Medical Marijuana Landscape 35 Pharmacists as a Critical Member of the Integrated Care Team 37 Continuing Pharmacy Education Lesson #12 e Pharmacology of Medical Marijuana
Transcript of Nebraska Mortar & Pestle - Nebraska Pharmacists · PDF fileThe Nebraska Mortar & Pestle (M&P)...
3 Daily News Dose - In Case You Missed It
4 Continuing Pharmacy Education Lesson #9 Pediatric Toxicological Emergencies
12 Creighton University School of Pharmacy & Health Professions News
13 University of Nebraska Medical Center College of Pharmacy News
15 Continuing Pharmacy Education Lesson #10 USP37-NF32 Chapter <795> Pharmaceutical Compounding Nonsterile Preparations
Inside This IssueInside This IssueInside This IssueInside This Issue
Nebraska Mortar & PestleJuly/August 2014 Volume 77, Number 4Offi cial Publication of the Nebraska Pharmacists Association
For NPA Members
25 Rx and Th e Law - Why is that Pharmacist Asking so Many Questions?
26 Continuing Pharmacy Education Lesson #11 Legal and Business Aspects of the Changing Medical Marijuana Landscape
35 Pharmacists as a Critical Member of the Integrated Care Team
37 Continuing Pharmacy Education Lesson #12 Th e Pharmacology of Medical Marijuana
JulAug14WorkingCopy.indd 1 8/21/2014 6:16:59 PM

Nebraska Pharmacists Association6221 S 58th St, Suite A, Lincoln, Nebraska 68516phone 402.420.1500 fax 402.420.1406email m&[email protected] website www.npharm.org
Board of DirectorsChairwoman, Brenda Kiolbasa
President, Firouzan ‘Fred’ Massoomi
President-Elect, Jennifer Tilleman
Treasurer, Kimberlee Ross
Executive Vice President, Joni Cover
District MembersTrevor BertschConnie BolteDana GriessJeffrey SteffensmeierEric StevensNicole White
TechnicianKathleen Huxoll
StudentsAllisha Gabriel, CUMichaela Hruska, UNMC
Network ChairsAcademia/Specialty Practice, Lori MuranteChain, Kimberlee RossHospital/Health-System, Keith BergIndependent, Richard ClabaughIndustry, Stephanie MaciejewskiLong-Term Care, Sheryl Havermann
StaffExecutive Vice President, Joni CoverNebraska DUR Director, Marcia MuetingFinance & Marketing Manager, Diane Webb
PublisherThe Nebraska Mortar & Pestle (M&P) (ISSN 0028-1891) is owned and published by the Nebraska Pharmacists Association (NPA) to provide continuing pharmacy education, drug information, news and trends in the profession of pharmacy. Opinions expressed by the contributors, whether signed or otherwise, do not necessarily refl ect the attitudes of the publisher nor are they responsible for them.
The M&P is published six times a year at the end of the months of February, April, June, August, October and December. The subscription rate for non-members is $30.00 per year. The Managing Editor is Joni Cover, [email protected]. Offi ce of publication is 6221 S 58th Street, Suite A, Lincoln, NE 68516-3687. Second class postage paid at Lincoln, Nebraska, and at additional mailing offi ces. Postmaster: Send address changes to the Nebraska Mortar & Pestle, 6221 S 58th Street, Suite A, Lincoln, NE 68516-3687 or email m&[email protected].
Cover PhotoImage purchased from www.istockphoto.com
BirthdaysAnniversariesWeddings
GraduationsWe Hear Th at
� NPA Ambassador, Paul Athey, RP, participated in the Service Drug Howard McGinnis Memorial Golf Tournament on June 7th & 8th at the Cozad Country Club. Howard McGinnis passed away in June 2013. His son, Paul McGinnis, RP, owns the pharmacy. Pictured here:Michael Wickham, Paul Athey, Paul McGinnis, and Matt Wickham.
� Deines Pharmacy in Beatrice was one of this year's fi nalist for the 2014 Good Neighbor Pharmacy of the Year. For the past 23 years, owner Mitch Deines, RP, has applied a clinical approach to pharmacy with three nurses on staff and a robust durable medical equipment department with a mission of making everyday living easier. Harry Race Pharmacy, Sitka, Alaska, was named the winner. Visit https://www.youtube.com/watch?v=a7aEAfhBX9E to see the Deines Pharmacy nomination video.
JulAug14WorkingCopy.indd 2 8/21/2014 6:17:04 PM

Th e Nebraska Mortar & Pestle 3
Daily News Dose
Your NPA member benefi t includes a daily email with important drug and health information, as well as answers to member questions. Below is a partial list of some of the most recent Daily News Dose items that you may have missed.
Daily News DoseIn Case You Missed It
2015 Annual ConventionMark Your Calendar! Th e 2015 NPA Annual Convention will be held on April 24th and 25th at the Cornhusker Hotel in Lincoln, Nebraska.
Tramadol - Schedule IVOn August 18, 2014, Tramadol became a Schedule IV Controlled Substance. According to the Pharmacists Manual, “When a drug not previously listed as a controlled substance is scheduled or a drug is rescheduled, the drug must be inventoried as of the eff ective date of scheduling or change in scheduling.” All prescriptions must meet the requirements of a C-IV on August 18, 2014. Best practice would be to obtain a new prescription for existing orders.
Statewide Drug Disposal ProjectTh e NPA received a grant from the Nebraska Department of Environmental Quality to expand a Lancaster County pilot program for the collection of unwanted medications. As a partner in the Nebraska MEDS Coalition, the NPA will lead the eff ort to supply pharmacies across the state with containers to collect unwanted, non-controlled substance medications from patients. Pharmacies will be contacted in September or October with further information on how to join the eff ort.
USP Hazardous Drugs Chapter Th e NPA submitted comments to the United States Pharmacopeial Convention regarding the proposed General Chapter <800> Hazardous Drugs - Handling in Healthcare Settings, which the NPA does not support as written. Th e NPA stated that the proposal would be better suited for a best practices guideline. While the safety of pharmacists, patients, and other health care workers is important, the proposed regulations would be extremely diffi cult to meet, as well as create additional inconsistencies between regulatory agencies.
CPE Retention Records For Nebraska licensure, continuing pharmacy education (CPE) documentation should be kept for at least 2 years after license renewal. For example, the CPE credits earned from 01/02/2012 through 12/31/2013 were used to renew licenses on or by 01/01/2014 and should be kept at least until 01/01/2016. If you are licensed in another state, be sure to check with that state’s CPE retention requirements. ACPE CPE credits can be printed from NABP e-Profi les at any time.
Th ank You to Congressmen Terry and FortenberryTh e NPA thanks Congressman Lee Terry for cosponsoring HR 4190, a bill that would recognize pharmacists as providers under Medicare Part B. Th e NPA also thanks Congressman Jeff Fortenberry for cosponsoring HR 4577 and HR 4437. HR 4577 will allow any willing provider to participate in Part D preferred networks. HR 4437 will require PBMs to disclose reimbursement rates in contracts and update the rate once every 7 days to refl ect fl uctuation in the market. We appreciate our members of Congress who support the issues important to the pharmacy profession.
Member Contact InformationNPA Members can fi nd email addresses or phone numbers for other members by logging into the NPA website, then clicking on Member Directory Search. You can search by name, organization, or directory category. If you don’t want to share your contact information, make your changes by logging in and clicking on My Member Directory Options which allows you to choose whether or not you want to be included in the directory; what information you want other members to see; and in which categories you want to be included.
NPA President Visits IsraelNPA President, Fred Massoomi, had the unique opportunity to go to Israel and present at the Pharmaceutical Israeli Society. He spoke on the topic of proper hazardous drug handling. In his review of their processes, he found that the pharmacists are equally concerned about their safety and the safety of their patients. While in Israel, he took the opportunity to meet quite a few pharmacists in various practice sites. In this photo is a young pharmacist whom Fred met in Jerusalem. She was excited that he was a pharmacist from the United States and that he was interested in her practice site. Her practice site is Super-Pharm and is located literally meters from the holiest of holy sites in Jerusalem. He watched her compound a couple of prescriptions and counsel patients. Fred noted, “What I observed was the universal language of trust - the trust between a patient and a pharmacist. Although I could not understand the Hebrew consultation, I could easily see the compassion the pharmacist had for her patient and more importantly the sense of trust and gratitude the patient had for her pharmacist. As we continue to meander through the maze of healthcare reform, let’s hope we as a profession never lose that compassion and trust our patients need....globally.”
JulAug14WorkingCopy.indd 3 8/21/2014 6:17:04 PM

Pediatric Toxicological EmergenciesTh is CPE lesson was written by Kristin McNaughton, PharmD, and Jenna Preusker, PharmD, who have no fi nancial or confl ict of interest disclosures. Th is lesson does include a discussion of unlabeled or investigational use of a product(s) that has not yet been approved by the FDA for the use being presented.
ObjectivesAt the conclusion of this lesson, pharmacists should be able to:1. Identify commonly ingested and dangerous substances in pediatric patients.2. List strategies for prevention of pediatric poisoning in the community.3. Describe appropriate treatment strategies for selected toxic ingestions in the pediatric population.
IntroductionPreventing pediatric exposures to doses of potentially lethal drugs and toxins remains a challenge. Medication use is increasing in the United States in both adults and children. It is estimated that 82% of adults and 56% of children take at least one medication every week.1 Th e overall medication burden is on the rise as more Americans live longer with chronic conditions that necessitate the use of multiple medications such as diabetes, heart, lung, and kidney disease. Americans who took fi ve or more medications daily increased from 22% to 31% between 2000 and 2004.1 Increased medication use poses an increased risk of poisoning in children. One study demonstrated that more children are exposed and injured due to medications poisonings each year.2 Contact with more medications results in more episodes of prevention failure even with the best “poison proofi ng” strategies in place.
In younger children, unintentional exposures pose the greatest risk. Unintentional poisoning involves the unsupervised ingestion of medications, therapeutic errors, and exposure to environmental substances.3 As reported to the American Association of Poison Control Centers between 2001 and 2008, child self-exposure accounted for 95% of visits to a health care facility for evaluation of exposure to a pharmaceutical agent.2 As younger children age into adolescence, trends in exposures change from unintentional to intentional. Intentional poisonings involve suspected suicide attempts, abuse, and misuse. Teenagers have increased access to illicit drugs, alcohol, and over-the-counter (OTC) preparations as compared to younger children. Adolescents have greater access to the internet and infl uence of social media. In 2012, unintentional exposures outnumbered intentional exposures in all age groups except ages 13-19 years, and 51.2% of these patients required health care facility management.5
Th e evaluation of a child presumed to have been exposed to a toxic substance is a crucial step to ensure appropriate and eff ective treatment strategies are employed. Th e initial evaluation should include a precise history of the exposure, and a physical examination, within the context of known current ingestions and recreational practices. Contacting a poison control center is perhaps the most important initial
step when a toxic ingestion is suspected. A poison center can be reached by calling 1-800-222-1222 from anywhere in the United States. Poison centers and medical toxicologists can assist with the diagnosis of medicinal overdoses, as well as provide advice and treatment recommendations for stabilizing children who have been exposed to toxic compounds.4 One hallmark of poison center management is the use of follow-up calls to provide continued monitoring of case progress and medical outcome.5
Risk Factors for PoisoningsRisk factors for poisoning in small children are directly related to a child’s ability to access medications. Toddlers have an inherent curiosity and are able to grab more items that were previously out of reach and to open medications with simple caps. Normal curiosity and desire for oral stimulation cause children to place new objects directly into their mouth. Young toddlers, especially those under 3 years, are unable to distinguish safe products from unsafe products. Toxic amounts can be ingested before the child is deterred by the adverse taste of the product. Children are also well-known imitators who seek to mimic adult behaviors such as taking medications. School age children often believe they are helping by using toxic cleaning products or by attempting to
4 July/August 2014 www.npharm.org
Continuing Pharmacy Education Lesson #9
JulAug14WorkingCopy.indd 4 8/21/2014 6:17:05 PM

self-administer medications. Additionally, developmental issues can contribute to the increased risk of poisoning among adolescents. Teenagers desire independence and are increasingly exposed to peer pressure. Th is may cause them to take undue risks in experimenting with illicit drugs or prescription medications. Adolescents may take an overdose of medication as a suicide attempt or as a cry for help to gain needed attention.3
Environmental factors also contribute to the risk for poisoning. Kitchens, bathrooms, cars, and even garages may contain toxic pharmaceutical substances. Th ere is often a lack of appreciation for toxicity by parents due to their common use of their own medications.3 Issues may arise with storage that is easily accessible by children, especially in households where children may not routinely be present, such as a grandparent’s home. It is estimated that a grandparent’s medication is implicated in 10-20% of ingestions. In one study of exposures, grandparents’ medications were
stored in child-resistant containers only 45% of the time and medications were often left in accessible locations.10 Look-a-likes around the home also pose a problem for small children. Several medications look identical to candy, and liquid medications may look similar to juice. For teenagers, environmental risk factors are also related to the availability of medications, drugs, or other substances of abuse at school or home.3
Poison PreventionPoison prevention requires a multifactorial approach including legislation and education. Beginning in 1906, United States legislation and regulations have been implemented to protect children, adolescents, and adults from toxic exposures. Legislative measures have been more eff ective than educational strategies alone. Signifi cant reductions in poisonings and child deaths can largely be attributed to the regulations and legislation in Table 1.
Poison prevention also includes active interventions such as educational eff orts that target the avoidance of poisoning exposures. Th is starts in the provider’s offi ce. Clinicians should consider the risk of poisoning when prescribing medications and use less toxic therapies if appropriate. Pharmacists are important educators for parents and other caregivers about the risks associated with medications that are kept in a home with children and adolescents. Particular precautions should be taken with medications that are commonly involvedin fatal ingestions and those that are toxicin small doses such as the ones listed in Table 2. Other educational eff orts may involve community outreach projects, mass media campaigns, or education in a clinical setting. Emergency department visits for poisoning provide another important opportunity for education on how to prevent future exposures.
Table 1.United States Federal Legislation and Regulations for Protection from Toxic Exposures11
YearInstituted Legislation Signifi cant Implication
1906 Pure Food and Drug Act (Wiley Act) Created the Food, Drug, and Insecticide Administration which became the Food and Drug Administration (FDA) in 1930.
1927 Caustic Poison Act Required labels to warn parents of the dangers of lye and 10 other caustic substances.
1951 Durham-Humphrey Amendment Th e FDA explicitly defi ned two specifi c categories for medications: legend (prescription) and over-the-counter (OTC).
1961 Public Law 87-319 Designates the third week of March each year as National Poison Prevention Week for national recognition and entails widespread public education about poison prevention.
1966 Regulation of baby aspirin packaging Th e number of (81 mg) tablets in a single container was limited to 36 in response to the recognition that unintentional aspirin ingestion was a signifi cant cause of morbidity and mortality in young children. Between 1960 and 1980, deaths from aspirin ingestion dropped from 144 to 12.
1970 Poison Prevention Packaging Act (PPPA) Required child-resistant packaging for certain types of opiates and other dangerous drugs and other household products. Child-resistant containers impose a physical barrier to separate the child from the toxic product and are designed to delay the child’s ability to open the container long enough for an adult to discover the child before ingestion can occur.
2000 Public Law 106-174Poison Control Center Enhancement and Awareness Act
Ensured that all citizens had equal access to a poison control center. A single nationwide toll-free telephone number was established: 1-800-222-1222.9
2011 FDA Guidance for Industry: Dosage Delivery Devices for Orally Ingested OTC Liquid Drug Products
Th e FDA issued guidance to improve dosing instructions and clarity of marking on devices for oral liquid over-the-counter medications.
Th e Nebraska Mortar & Pestle 5
Continuing Pharmacy Education Lesson #9
JulAug14WorkingCopy.indd 5 8/21/2014 6:17:06 PM

Specifi c “safety rules” from the American Academy of Pediatrics that can readily be provided to parents and grandparents by pharmacists during counseling and include the following:12
• Medicine should always be called by its correct name.• Harmful products should be stored in a locked cabinet and out of the child’s sight and reach.• Safety caps should be replaced immediately after medication use.• Medication products should be stored in their original containers.• Medication labels should be read with care to ensure proper use.• Medications should not be taken in the view of small children, as children tend to imitate adult behavior. • Extra caution should be taken when a child is away from home, especially at a grandparent’s house due to increased risk of poisoning.• Old medications that are unused and substances used for outdated treatments, such as oil of wintergreen, boric acid, ammoniated mercury, oil of turpentine, and camphorated oil should be disposed of properly.• In the past, syrup of ipecac has been used to induce vomiting in a child that had swallowed a poison, but this practice is no
Table 2 .Substances Potentially Lethal to Small Children4,5,6,7,8
SubstanceEstimatedFatal Dose
CharcoalAdsorption Major Eff ects
Iron supplements 50 mg/kg No Severe vomiting, diarrhea, abdominal pain, lethargy
Tricyclics 15 mg/kg Yes Seizures, arrhythmias, hypotension
Beta-blockers Unclear Yes Seizures, hypoglycemia, bradycardia, and hypotension
Oil of Wintergreen (Methyl salicylate 98%)One teaspoonful contains 7,000 mg of salicylate = 90 tablets of baby (81 mg) aspirin
300 – 500 mg/kg Yes Phase 1: respiratory alkalosis – nausea, vomiting, diaphoresis, tinnitusPhase 2: progressive respiratory alkalosis – vertigo, hyperthermia, tachycardiaPhase 3: hypokalemia and metabolic acidosis – agitation, delirium, convulsions, stupor
Sulfonylureas < 1 mg/kg Yes Hypoglycemia
Calcium Channel Blockers < 40 mg/kg Yes Bradycardia, hypotension
Toxic Alcohols (i.e. methanol, ethylene glycol) 0.3 mL/kg No CNS depression
Clonidine Unclear Yes Bradycardia, hypotension, CNS depression
Opioids Unclear Yes Respiratory depression, sedation
longer recommended.4 It is not advised to intentionally cause vomiting through administration of syrup of ipecac, gagging the child, or giving salt water due to risk of aspiration.
Due to a large amount of healthcare spending following an exposure, poisoning represents a fi nancial burden to society. Most patients have minimal to no symptoms, but the ingestion often results in costly emergency room visits for guidance. With the direction of a poison control center, emergency room visits can be avoided and patients who truly require hospital intervention can be referred appropriately. A poison control center can help triage the situation and call the hospital while the patient is en route. Poison control center recommendations include lab tests, antidotes, other supportive treatment strategies, and guidance with length of stay. Th ese evidence based recommendations typically decrease the amount of inappropriate therapy and testing. A cost-benefi t analysis showed that for every $1.00 in poison control center funding, $7.67 was saved in direct medical costs.9 Th is cost underestimates the potential benefi ts of poison control centers, as it does not take into account decreased morbidity and mortality.
Ingested SubstancesTh e National Poison Data System reported that children younger than 6 years of age accounted for 48.4% of the 2.2 million exposures logged by poison centers in the United States in 2012.5 Th e top 5 exposures were cosmetics/personal care items (14%), analgesics (9.9%), household cleaning supplies (9.7%), foreign bodies (6.9%), and topical preparations (6.3%). Nine out of ten exposures occurred in a residence (at home or other) and 80% of incidents occurred when a child was not being directly supervised by an adult.5
Prescription and over-the-counter medications that are most toxic to small children include hypoglycemics, cardiovascular drugs, opioids, iron, and methysalicylates.4 Th e specifi c medications, doses, and clinical manifestations of toxicity are further outlined in Table 2. One study evaluating medication fatalities paralleled the substances required to have child-resistant closures by the Poison Prevention Packaging Act.6,11 Th is demonstrates the severe toxicity of several substances as well as the fact that child-resistant containers are not child-proof.
To appropriately focus eff orts, pharmacists and other health care providers need to be familiar with the medications
6 July/August 2014 www.npharm.org
Continuing Pharmacy Education Lesson #9
JulAug14WorkingCopy.indd 6 8/21/2014 6:17:06 PM

that are the most consequential – those that contribute the most emergency department visits, hospitalization, and harm. Th is section details ingestion of several substances that are of high concern and highlights management strategies in the event of ingestion.
OpioidsData indicate that frequent prescribing of opioid analgesics may contribute to overdose-related mortality among children who often ingest medications intended for an adult in the household.13,14 According to the 2010 United States mortality data opioids, alone or in combination, are the most commonly involved medications among pharmaceutical overdose deaths of all intents in all age groups.15
Th e classic presentation of opioid toxicity is miosis, decreased level of consciousness, and respiratory depression; however, these fi ndings are not consistently present. A respiratory rate of 12 breaths or less is strongly suggestive of opioid intoxication, especially if accompanied by stupor or miosis. Later in the clinical course of opioid toxicity, patients may fail to maintain oxygen saturations due to pulmonary edema. After the initial stabilization, the patient should be completely undressed to search for fentanyl patches and a thorough history should be obtained including questions regarding analgesic use and contact with anyone receiving treatment for chronic pain or opioid dependence. Because opioid analgesics are often co-formulated with acetaminophen, ingestion of acetaminophen should be evaluated as well.16
Fentanyl patches are especially dangerous as each patch contains a large reservoir of medicine to help maintain the diff usion gradient. For example, the 100 microgram per hour patch product contains a total of 10,000 micrograms of fentanyl per patch.18 Pediatric fatalities with fentanyl patches have been reported as a result of the patch an adult is wearing inadvertently being transferred to a child during sleep, by the child fi nding a patch and applying it unknowingly, or by the child ingesting used patches.17,18
Naloxone is a competitive mu-receptor opioid antagonist that reverses all signs of opioid toxicity. Th e onset of action of
naloxone given by the intravenous route is approximately two minutes and its duration is 20 to 90 minutes, which may be much shorter than the opioid it is reversing. It is also important to consider that the half-life of a given opioid can be dramatically longer in the overdose setting.18
Generally speaking, the dosing of naloxone is empiric and titratable. Th e initial naloxone dose for opioid intoxication in pediatric patients ≤5 years or ≤20 kg is 0.1 milligram (mg) per kilogram (kg) of body weight per dose with intravenous (IV) administration preferred. For patients >5 years or >20 kg, naloxone 2 mg IV per dose may be used.19 Naloxone may also be given by the intraosseous (IO), endotracheal (ET), intramuscular (IM), subcutaneous (SubQ), and intranasal routes. Children who ingest opioids often require larger doses of naloxone due to the higher dose of the opioid on a milligram per kilogram basis than adults. Th e dose of naloxone should be repeated every 2 to 3 minutes until the patient responds. It has been suggested that the maximum single dose used should be15 mg as respiratory depression is likely due to another cause if this dose is ineff ective.16
It is important to understand that the dose of naloxone required to restore respiration does not correspond with the severity of overdose, as the timing of respiratory depression does not associate with the peak serum concentration of the opioid, and that administration of naloxone does not prevent recurrence of respiratory depression.16 Th erefore, close patient monitoring should be provided, and if respiratory depression recurs, a continuous infusion of naloxone may be indicated.
Other management strategies include gastrointestinal decontamination with activated charcoal (which should be reserved for patients who present within one hour of ingestion), and whole-bowel irrigation with polyethylene glycol (which may be benefi cial in patch ingestion).16 Mechanical ventilatory support may also be employed.
Although opioids are highly eff ective in treating pain, it is important to ensure that patients receive adequate counseling regarding the dangers of inappropriate opioid use. Th e current recommendation for disposal of fentanyl patches is to fold the patch upon itself and fl ush down the toilet.20 Medication take back days provide
another opportunity to dispose of extra medications in a safe manner. It is critical that patients understand the need for appropriate storage and disposal of opioids, as these medications are potentially lethal.
AcetaminophenAcetaminophen is a commonly used analgesic and antipyretic in pediatric patients; however, repeated supratherapeutic dosing, accidental overdose, and intentional ingestion of acetaminophen can lead to acute liver failure or death.21 In the outpatient setting, correct acetaminophen dosing is complicated by the need to calculate a weight-based dose and then properly convert the dose into a volume based on the concentration available. Pharmacists can help promote safe acetaminophen use by pro actively providing information about this medication which may be perceived as harmless.25 Th e availability of multiple concentrations of liquid acetaminophen has been implicated in overdoses resulting in the voluntary withdrawal of more concentrated acetaminophen preparations by some manufacturers. Danger from the multiple formulations still exists as some patients may still have previously purchased concentrated product available in their medicine cabinet. 22
An acute ingestion of ≥150 mg/kg of APAP is potentially toxic. Th e current approach for evaluation involves obtaining a blood level 4 hours after the ingestion and plotting the value on the Rummack-Matthew nomogram to determine risk of hepatotoxicity. For chronic ingestions, an acetaminophen level, liver function, and coagulation studies should be obtained. Treatment is recommended if the acetaminophen level is >10 mcg/mL or AST or ALT are >50 IU/L.24
To limit systemic absorption, activated charcoal can be administered if a patient presents within one hour of ingestion; however, the antidote of choice for acetaminophen toxicity is N-acetylcysteine (NAC). If clinically appropriate, the two antidotes may be used together. When acetaminophen is given in therapeutic doses, it is primarily metabolized through glucoronidation and sulfation pathways and a small amount is metabolized through the cytochrome P450 2E1 enzyme
Th e Nebraska Mortar & Pestle 7
Continuing Pharmacy Education Lesson #9
JulAug14WorkingCopy.indd 7 8/21/2014 6:17:06 PM

(CYP 2E1). Metabolism through the CYP 2E1 pathway produces the metabolite N-acetyl-p-benzoquinone imine (NAPQI) which is toxic and reacts with cellular components resulting in hepatocyte death.21 NAPQI is then conjugated to glutathione to form the nontoxic mercapturic acid which is renally excreted. Acetylcysteine serves to replenish glutathione stores allowing for production of nontoxic metabolites.21 Infant CYP 2E1 metabolism is immature, but activity increases and reaches adult levels by one year of age.23
Acetylcysteine can be administered intravenously or orally and should be initiated ideally within 8 hours of an acute ingestion. Oral therapy is preferred unless contraindications exist. Th e usual recommended oral dose is a 140 mg/kg loading dose followed by 70 mg/kg every four hours for 72 hours or as tailored to patient clinical condition. If a patient is unable to tolerate oral therapy or has fulminant hepatic failure, intravenous NAC is recommended. Th e commonly used intravenous protocol is 150 mg/kg in200 mL over one hour, followed by 50 mg/kg in 500 mL over 4 hours, then 100 mg/kg in 1000 mL over 16 hours. Th e recommended volumes for dilution are modifi ed in patients <40 kg to prevent excessive hypotonic fl uid administration that can result in hyponatremia and seizures. For patients less than 12 years of age who weigh more than 20 kg, the volumes are halved. In patients who weigh less than 20 kg, the recommended total volumes for dilution are 3 mL/kg for the bolus, 7 mL/kg for the fi rst dose, and 14 mL/kg for the second dose.
Th e optimal duration of acetylcysteine therapy is unclear, but it has been suggested that acetylcysteine therapy be continued until acetaminophen blood levels are <10 mcg/mL and the patient is clinically well with normal liver function tests. Th erapy in cases of severe hepatotoxicity should be continued until serum liver transaminases fall below 1000 IU/L, bilirubin and coagulation studies are within normal limits, and the patient is clinically well, until the patient receives a liver transplant, or the patient expires.24
Common adverse eff ects associated with NAC administration include nausea and vomiting if given orally. To make NAC more palatable, it can be diluted in soda or
ingested through a straw. Intravenous use is associated with anaphylactoid reactions that often respond to decreased rate of infusion or administration of diphenhydramine.24
SulfonylureasSulfonylurea agents are commonly used in the treatment of Type 2 diabetes mellitus. In a child, ingestion of even a single sulfonylurea tablet can cause severe, life-threatening hypoglycemia. In 2012, the American Association of Poison Control Centers received 4,206 reports of exposures to sulfonylureas with 926 exposures in patients less than 19 years of age.5 Th e onset of hypoglycemia may be delayed in children, so caution should be taken when making initial assessments.
Sulfonylurea poisoning can produce sustained and profound hypoglycemia that is often refractory to intravenous dextrose, particularly in children.26 In infants and young children, the signs of hypoglycemia are frequently nonspecifi c and may include irritability, lethargy, or abnormal behavior.27 Severe hypoglycemia can progress to seizure and coma. Autonomic symptoms are less prominent in children than adults.7 Th e dose of sulfonylurea necessary to cause hypoglycemia in small children depends on a range of factors such as when the child last ate, whether the child is ill or malnourished, and the size of the child.
It is best to err on the side of caution and observe the child in the hospital if any doubt exists about the nature of the ingestion. Due to delayed hypoglycemia, in-hospital observation for 24 hours is recommended for any child with a sulfonylurea exposure, even if they are asymptomatic. Asymptomatic children should be allowed to eat, but intravenous (IV) dextrose should be avoided as it may mask hypoglycemia or stimulate further insulin release.7 If sulfonylurea overdose is diagnosed and treated quickly, patients generally recover without sequelae.27
Management strategies for symptomatic overdose of a sulfonylurea include activated charcoal, intravenous dextrose, subcutaneous octreotide (off -label), glucagon, and nutritional support. Table 3 further details these management strategies. Th e choice of treatment is determined by the timing of the ingestion and the severity of hypoglycemic symptoms.7 Once clinical euglycemia is established, the child should
be fed a calorie-rich meal. Intravenous dextrose contains only 3.4 kcal per gram and has a very short duration of action, while food provides a calorie-rich and longer lasting source of glucose.27
Serum glucose should be periodically monitored to identify recurrence of hypoglycemia. Serial neurologic examinations are also essential. Once the initial hypoglycemia is corrected, blood glucose should be measured twice more at 30 minute intervals. If the patient maintains euglycemia, serum glucose can be checked every 4-6 hours thereafter.27
Calcium Channel AntagonistsCalcium plays an important role in physiologic processes including muscle contraction and cardiac conduction. Calcium channel blockers (CCB) selectively inhibit calcium channels to produce physiologic eff ects. CCBs undergo signifi cant fi rst pass metabolism, so less drug will be metabolized quickly by the liver in an overdose situation. In overdose, enzymatic saturation can increase the bioavailability and half-life of the drug, as well as cause a loss in selectivity.28
Evidence of calcium channel blocker toxicity can be subtle initially. Th e clinical course can involve vasodilation resulting in refl ex tachycardia, then eventually bradycardia, refractory hypotension and/or hyperglycemia.29,30 Th e most commonly reported eff ects are lethargy and hypotension; however, prodromal events may not correspond to the level of toxicity.31 Signs of toxicity generally appear within 12 hours of ingestion, regardless of whether the ingestion is immediate or sustained release; however, case reports have documented slower decompensation resulting in death.29 Rapid onset of cardiovascular collapse can occur in symptomatic exposures. Th ere is no uniformly fatal dose that has been identifi ed, but fatalities have occurred after the ingestion of one or two CCB medications in toddlers.30,31 Nifedipine and verapamil have been most closely linked to toxicity, but fatalities have occurred with other CCBs as well.31
If there is a reasonable suspicion of CCB ingestion, administration of activated charcoal within 2 hours of ingestion may be considered.31 Patients should be placed on a cardiac monitor to evaluate potential conduction abnormalities28 and
8 July/August 2014 www.npharm.org
Continuing Pharmacy Education Lesson #9
JulAug14WorkingCopy.indd 8 8/21/2014 6:17:06 PM

observed for at least 6 hours for immediate-release preparations, and 12-24 hours for sustained-release preparations. Th ere is no defi nitive antidote, but rapid and aggressive therapy should be initiated in patients with clinical signs of deterioration.31 Treatment is supportive focusing on cardiovascular stability, and if needed, routine advanced cardiovascular life support measures should be employed. Potential treatment options include calcium, glucagon, insulin, and intravenous lipid emulsion.28,31
Attention Defi cit Hyperactivity Disorder MedicationsAttention defi cit hyperactivity disorder (ADHD) medication ingestions are becoming increasingly common. ADHD has traditionally been diagnosed in school-aged children aged 6 – 12 years. Th e latest recommendations by the American Academy of Pediatrics expanded the diagnostic criteria to include both preschool-aged children and adolescents. Th is expanded age criteria for the diagnosis
Table 3.Treatment strategies for sulfonylurea toxicity in pediatrics7,26,27
Strategy Dose CommentsActivated Charcoal Children: 1-2 g/kg/dose or 25-50 g/dose PO
Infants: 1 g/kg/dose PO• Activated charcoal should be given if patient presents within one
hour of the ingestion and patient will tolerate a dose (i.e. is not vomiting or unconscious).
• Unlikely to be eff ective if symptomatic, since hypoglycemia from sulfonylureas often occurs several hours after the ingestion.
Dextrose Children are treated with a 25 percent (D25W) or10 percent (D10W) dextrose solution, and neonates with a 10 percent dextrose solution.D5W: give 10-20 mL/kg if volume toleratedD10W: give 5-10 mL/kgD25W: give 2-4 mL/kgD50W: give 1-2 mL/kg (maximum recommended concentration 25%; can prepare by mixing 50% dextrose 1:1 with sterile water)Doses of dextrose may be repeated.
• Intravenous dextrose is administered for blood glucose readings below 60 mg/dL, and quickly increases glucose delivery to the brain.
• Intravenous dextrose should not be used as monotherapy for a sulfonylurea overdose. When given alone, IV dextrose can cause a transient hyperglycemia that triggers increased insulin release, leading to recurrent episodes of hypoglycemia.
Octreotide 1 – 2 mcg/kg (up to 150 mcg) every six hours. It may also be given as an IV bolus over several minutes or by continuous IV infusion. Octreotide should be administered for 24 hours.
• Symptomatic hypoglycemia is treated with both dextrose and octreotide, a synthetic peptide analog of somatostatin.
Glucagon Children weighing ≥ 44 lb (20 kg): 1 mg (1 IU) IM, IV, or SCChildren weighing < 44 lb (20 kg): 0.5 mg (0.5 IU) or, alternatively, 0.02—0.03 mg/kg (IU/kg) IM, IV, or SC. Dose should not exceed 1 mg.
• Th e effi cacy of glucagon is dependent upon hepatic glycogen stores, which may be depleted in the setting of prolonged hypoglycemia, and the short duration of glucagon also limits its eff ectiveness.
• Glucagon given intramuscularly raises serum glucose levels slightly and may be used as a temporizing measure while IV access is obtained, but is not a substitute for dextrose.
Nutritional Support Once clinical euglycemia is reached, children should be fed a calorie-rich meal.
• Food provides a more consistent and longer lasting source of glucose than intravenous dextrose, which in turn helps to prevent extreme fl uctuations in blood glucose.
of ADHD is resulting in more children receiving medications, and ultimately more risk for both unintentional and intentional exposures. Th e largest increase in any category of outpatient prescriptions was for ADHD medications to children, increasing 46% between 2002 and 2010. Th e number of children prescribed medications for ADHD has increased six-fold in several nations between 2000 and 2006 indicating that the trend is not unique to the United States.33
Emphasis is placed on the strong evidence behind the use of stimulant medications. Medications commonly utilized to treat ADHD include amphetamine/dextroamphetamine, atomoxetine, clonidine, guanfacine, lisdexamfetamine, and methylphenidate. Th e use of these medications has been linked with improved school performance and lower rates of adverse psychiatric disorders long term. Potential adverse eff ects are often related to the stimulating eff ects of these medications including agitation,
seizures, coma, ventricular dysrhythmias, and death.33
A recent study examined 63 incidents of unintentional ADHD medication overdoses in patients admitted to the hospital. Several patients were excluded who were not ill enough to be admitted and were only seen in the emergency department. Th e median length of hospital stay was 2 days. Th e study also highlighted the high rate of toxicity when the medication was not prescribed for the patient who overdosed. Th e ADHD drug was prescribed for the patient in only 22/63 (35%) of patients. In the rest of the cases, it was prescribed for the patient’s sibling, parent, grandparent, other family member, or friend.33
Treatment for ADHD medication overdose is based on symptom management and countering the stimulating pharmacodynamic eff ects. Among the patients who ingested stimulant medications in the study, benzodiazepines (74%) and antipsychotics (haloperidol 23%) were administered as treatments, and fi ve patients
Th e Nebraska Mortar & Pestle 9
Continuing Pharmacy Education Lesson #9
JulAug14WorkingCopy.indd 9 8/21/2014 6:17:06 PM

Continuing Pharmacy Education Lesson #9
(8%) required mechanical ventilation.33 In all but three cases, the child was able to be discharged to the care of the parents. In those three cases, the child was discharged to new foster care or to child protective services. Fortunately, no child died or exhibited permanent disability that was evident at the time of discharge. Th e cost of the hospitalizations ranged from $3,400 to $9,400, but several charges (i.e. ambulance costs, emergency department charges from referring facilities, etc.) were excluded, therefore, the cost to society is likely higher.33 Th is study revealed that the incidence and cost of hospital admissions due to toxicity of ADHD medications is currently on the rise. Th ese fi ndings represent a negative impact of increased prescribing patterns. Additionally, many children are poisoned by medications belonging to their siblings, reinforcing the importance of safe storage and handling principles.
ConclusionIn the event of a pediatric ingestion, pharmacists should be aware of general treatment principles and remember that local poison control centers represent an invaluable resource for the diagnosis and treatment of exposures. Th e centers also provide support 24 hours a day and can be reached by calling 1-800-222-1222. Knowledge of appropriate interventions allow pharmacists to prepare for ingestions and act quickly. Pharmacists can play a key role in poison prevention through counseling. Th ere is always a need for education regarding medication storage and reinforcement of these principles. Although medications are usually dispensed in child-resistant containers, no container is truly childproof and the potential for lethal exposure exists through weekly medication organizers, medications left next to a dinner plate, or through medications inadvertently dropped on the fl oor.
References1. Schillie S, Shehab N, Th omas K, et al. Medication overdoses leading to emergency department visits among children. Am J Prev Med. 2009; 37(3):181-187.2. Bond G, Woodward R, Ho M. Th e growing impact of pediatric pharmaceutical poisoning. J Pediatr. 2012; 160(2):265-270. 3. Committee on Injury and Poison Prevention, American Academy of Pediatrics. Injury prevention in and around the home. Injury Prevention and Control for Children and Youth, American Academy of Pediatrics: Elk Grove Village, IL 1997.
4. Barrueto F, Gattu R, Mazer-Amirshahi M. Updates in the general approach to the pediatric poisoned patient. Ped Clinics of North America. 2013; 60(5):1203-1220.5. Mowry J, Spyker D, Cantilena L Jr, et al. 2012 Annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 30th Annual Report. Clin Toxicol. 2013; 51(10):949-1229.6. Litovitz T, Manoguerra A. Comparison of pediatric poisoning hazards: an analysis of 3.8 million exposure incidents. A report from the American Association of Poison Control Centers. Pediatrics. 1992; 89(6):999.7. Michael J, Sztajnkrycer M. Deadly pediatric poisons: nine common agents that kill at low doses. Emerg Med Clin North Am. 2004; 22:1019-1050.8. Davis J. Are one or two dangerous? Methyl salicylate exposure in toddlers. Journ of Emerg Med. 2007; 32(1):63-69.9. Woolf A, Karnes D, Kirrane B. Preserving the United States’s poison control system. Clin Toxicol. 2011;49(4):284-286.10. McFee RB, Caraccio TR. “Hang up your pocketbook” – an easy intervention for the granny syndrome: grandparents as a risk factor in unintentional pediatric exposures to pharmaceuticals. J Am Osteo Assoc. 2006; 106(7): 405-11.11. Committee on Poison Prevention and Control, Board of Health Promotion and Disease Prevention, Institute of Medicine of the National Academies. Historical context of poison control. In: Forging a Poison Prevention and Control System, Th e National Academies Press, Washington D.C. 2004. p. 82. 12. American Academy of Pediatrics. Keep your home safe from poisons. Available at: http://www.healthychildren.org/English/safety-prevention/all-around/pages/Keep-Your-Home-Safe-From-Poisons.aspx (Accessed February 6, 2014).13. Bailey JE, Campagna E, and Dart RC. Th e underrecognized toll of prescription opioid abuse on young children. Ann Emerg Med. 2009; 53(4):419-424.14. Bond GR, Woodward RW, and Ho M. Th e growing impact of pediatric pharmaceutical poisoning. J Pediat. 2001; 10:265-270.15. Jones CM, Mack KA, and Paulozzi LJ. Pharmaceutical overdose deaths, United States, 2010. JAMA. 2013; 309(7):657-659.16. Boyer EW. Management of opioid analgesic overdose. NEJM. 2012; 367(2): 146-155.17. Institute for Safe Medication Practices. Fentanyl patch fatalities linked to “bystander apathy:” we all have a role in prevention. ISMP Medication Safety Alert! 2013. Available at: http://www.ismp.org/newsletters/acutecare/showarticle.asp?id=55. Accessed January 19, 2014.18. Prosser JM, Jones BE, and Nelson L. Complications of oral exposure to fentanyl transdermal delivery system patches. J Med Toxicol. 2010; 6:443-447.19. Kleinman ME, Chameides L, Schexnayder SM, et al. Part 14: Pediatric Advanced Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010; 122:876-908.20. National Alert Network. Proper disposal of fentanyl patches is critical to prevent accidental exposures. April 25, 2012. Accessed January 19, 2014.21. Ogilvie JD, Rieder MJ, Lim R. Acetaminophen overdose in children. CMAJ. 2012; 184(13):1492-1496.22. United States Food and Drug Administration. Know concentration before giving acetaminophen to infants. FDA Consumer Health Information. 2011.23. Hines RN. Th e ontogeny of drug metabolizing enzymes and implications for adverse drug events. Pharmacol Th er. 2008; 118:250-67.24. Algren DA. Review of N-acetylcysteine for the treatment of acetaminophen (paracetamol) toxicity in pediatrics. Second Meeting of the Subcommittee of the Expert Committee on the Selection and Use of Essential Medicines. 2008. Geneva, Switzerland. 25. Tzimenatos L, Bond GR. Pediatric Th erapeutic Error Study Group. Severe Injury or death in young children from therapeutic errors: a summary of 238 cases from the American Association of Poison Control Centers. Clin Toxicol. 2009; 47(4):348-354.26. Glatstein M, Scolnik D, Bentur Y. Octreotide for the treatment of sulfonylurea poisoning. Clin Toxicol. 2012; 50(9):795-804.27. Spiller HA, Sawyer TS. Toxicology of oral antidiabetic medications. Am J Health Syst Pharm. 2006; 63(10):929-938.28. Arroyo AM and Kao LW. Calcium channel blocker toxicity. Pediatr Emer Care. 2009; 25:532-541.29. Montiel V, Gougnard T, and Hantson P. Diltiazem poisoning treated with hyperinsulinemic euglycemia therapy and intravenous lipid emulsion. European Journal of Emergency Medicine. 2001; 18:121-123.30. Miller MA, Masneri DA, and Herold T. Delayed clinical decompensation and death after pediatric nifedipine overdose. Am J Emerg Med. 2007; 25(2);197-198.31. Spiller HA, Milliner BA, and Bosse GM. Amlodipine fatality in an infant with postmortem blood levels. J Med Toxicol. 2012; 8:179-182.32. Ranniger C and Roche C. Are one or two dangerous? Calcium channel blocker exposure in toddlers. Journ of Emerg Med. 2007; 33(2):145-154.33. Levine M, Froberg B, Ruha AM, et al. Assessing the toxicity and associated costs among pediatric patients admitted with unintentional poisonings of attention-defi cit/hyperactivity disorder drugs in the United States. Clin Toxicol 2013; 51(3):147-150.
10 July/August 2014 www.npharm.org
Policies for the Nebraska Mortar & Pestle (M&P) continuing pharmacy education lessons and quizzes:
1. M&P Quizzes are valid only for the membership year in which they are published. Quizzes for the 2014 Membership Year must be received by December 8, 2014. Quizzes cannot be carried over to another membership year.
2. If more than three questions are missed, the quiz will be returned. Th e quiz can be resubmitted.
3. CPE transcripts can be printed from NABP e-Profi les at www.nabp.net.
4. CPE credits are submitted to NABP by the 15th of each month. For example, M&P CPE quizzes completed in the month of August 2014, will be sent to NABP e-Profi les before September 15, 2014.
Th e Nebraska Council for Continuing Pharmacy Education (NCCPE) is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education (CPE).Th is CPE home study lesson has been accredited for 1.0 contact hour or 0.10 CEU. UAN #128-000-14-100-H01-P. Th is lesson is a knowledge-based CPE activity targeted to pharmacists.
Th e authors and the Nebraska Pharmacists Association disclaim any liability to you or your patients resulting from reliance solely upon the information contained herein.
Quiz Answers may be submitted:1. Online: www.npharm.org
2. Fax: 402-420-1406
3. Email: m&[email protected]
4. Mail: NPA Mortar & Pestle6221 S 58th St, Ste ALincoln, NE 68516
JulAug14WorkingCopy.indd 10 8/21/2014 6:17:06 PM

Pediatric Toxicological EmergenciesQuiz #9, July/August 2014, UAN #128-000-14-100-H01-P
2014 Quiz #9 - NPA CPE Home Study Answer FormPediatric Toxicological Emergencies
UAN #128-000-14-100-H01-P 1.0 Contact Hour - Knowledge Based CPE Activity
Name ________________________________________________________
Mailing Address _______________________________________________
City/State/Zip _________________________________________________
*NABP e-Profi le # ______________ *Date of Birth (MMDD) _________*Required for ACPE credit.
Circle one (1) Answer:1. a b c d 6. a b c d2. a b c d 7. a b c d3. a b c d 8. a b c d4. a b c d 9. a b c d5. a b c d 10. a b c d
CPE Home Study Evaluation 1. Rate this lesson: (Excellent) 5 4 3 2 1 (Poor)
2. Did this lesson meet each of its objectives? ___ Yes ___ No3. Was the content without commercial bias? ___ Yes ___ No 4. Did the lesson meet your educational/practice needs? ___ Yes ___ No5. Comments/future topics are welcome. ________________________
The deadline for this quiz is December 8, 2014
Keep the TOP portion for your records. Return the BOTTOM portion to the NPA offi ce.Or, take this quiz online at www.npharm.org
Continuing Pharmacy Education Quiz #9
1. What nationwide phone number can be used to reach a Poison Control Center?
a. 1-800-555-1212b. 1-800-222-1222c. 1-800-POISONS (1-800-764-7667)d. 1-800-HELP NOW (1-800-435-7669)
2. Children under six years of age accounted for what percent of exposures logged by poison control centers in 2012?
a. 15.3%b. 30.9%c. 48.4%d. 67.3%
3. According to a cost-benefi t analysis, every $1.00 spent in poison control center funding resulted in savings of:
a. $1.07b. $3.45c. $5.90d. $7.67
4. As children become adolescents, which type of exposure becomes more common?
a. Accidentalb. Developmentalc. Intentionald. Th erapeutic error
5. Which strategy is appropriate for parents to prevent ingestion by children in the home?
a. Keep medications in unlabeled containersb. Refer to medications as candyc. Store medications out of the reach of childrend. Take medications in front of children
6. What class of medications is most commonly involved in pharmaceutical overdose deaths?
a. Attention Defi cit Hyperactivity Disorder Medicationsb. Calcium Channel Blockersc. Opioidsd. Sulfonylureas
7. Th e antidote of choice for acetaminophen toxicity is:a. Acetylcysteineb. Epinephrinec. Flumazenild. Naloxone
8. How long should a child be observed if a sulfonylurea ingestion is suspected?
a. 12 hours, at homeb. 12 hours, in the hospitalc. 24 hours, at homed. 24 hours, in the hospital
9. Although there is no uniformly fatal dose for calcium-channel blockers, fatalities have been reported with pediatric ingestions as small as:
a. 1-2 tablets/capsulesb. 5-6 tablets/capsulesc. 10-12 tablets/capsulesd. 18-20 tablets/capsules
10. Which symptom is suspicious for toxicity associated with an ADHD medication ingestion?
a. Bradycardiab. Hypotensionc. Seizured. Somnolence
Th e Nebraska Mortar & Pestle 11
JulAug14WorkingCopy.indd 11 8/21/2014 6:17:07 PM

12 July/August 2014 www.npharm.org
Michele Faulkner, Pharm.D.’94 – Professor of Pharmacy Practice (primary) and Professor of Neurology (secondary)
Th omas Lenz, Pharm.D.’99 – Professor of Pharmacy Practice
Mikayla Spangler, Pharm.D., BCPS – Associate Professor of Pharmacy Practice (primary) and Associate Professor of Family Medicine
(secondary)
www.spahp.creighton.eduwwwwwww.w.w.spspspahahhp.p.p.crccreieie ghghghtototon.n.n.edededuuu
www.spahp.creighton.eduWHITE SELECTED AS NACDS FACULTY SCHOLAR
YOUNG ALUMNI APPRECIATION AWARD 2014
Nicole White, Pharm.D.’10, assistant professor of pharmacy practice, was selected a 2014-15 Faculty Scholar by the National Association of Chain Drug Stores (NACDS) Foundation. She is one of only eight pharmacy faculty nationwide to be awarded the distinction this year. Th e program is designed to educate junior faculty at U.S. pharmacy schools about eff ective and meaningful community pharmacy-based patient care research. White will partake in this year-long program under the guidance and leadership
of Dr. Melissa Somma McGivney and Dr. Kim Coley. White will receive a research
grant to launch a patient-focused research project conducted in a community pharmacy setting and will be able to identify a research mentor and small working group at Creighton to aid with her project development. Using various teaching methods, NACDS will provide each faculty scholar with opportunities for expert advice and peer-to-peer review throughout the year. Th e class will have their fi rst in-person meeting in August at the 2014 NACDS Total Store Expo in Boston, Massachusetts.
Glenda Rodriguez Millard, Pharm.D.’10, of Wichita, Kansas was selected as the 2014 recipient of the Young Alumni Appreciation Award for Pharmacy. Aft er beginning her work at Walgreens in 2010, Dr. Millard developed a personal interest in the treatment of HIV patients. She became credentialed as an HIV pharmacist, and she initiated the use of a cellphone at her facility. Currently she is working with Walgreens to set up a dedicated location for a HIV clinic. Th rough all her achievements, she has increased the revenue at her location by $55,000 per month. Dr. Millard is an impressive example of the potential impact graduates can have on community pharmacy.
Christopher Destache, Pharm.D.’84, professor of pharmacy practice, was awarded a grant from Cerexa, Inc. to evaluate the use of ceft aroline (Tefl aro) in the treatment of patients with complicated skin and skin structure infection or
community-acquired bacterial pneumonia. Th e Creighton School of Pharmacy and Health Professions is one of 100 clinical sites in the nation that enrolls patients that have received ceft aroline for a wide variety of Gram-positive infections, many of which have acute bacterial skin and skin structure infection or community-acquired bacterial pneumonia. Th ose granted the Cerexa Award will collect
data and conduct a retrospective study on the role ceft aroline plays within the community. As principle investigator, Dr. Destache will utilize this grant to collect data amongst patients who have received a minimum of 4 doses of ceft aroline and have a positive culture for an organism that is susceptible to this drug.
DESTACHE AWARDED CEREXA GRANT
J. Chris Bradberry, Pharm.D., Dean, (left ) Glenda Millard, Pharm.D.’10 Marty Feltner, Pharm.D.’99,
PHARMACY FACULTY PROMOTIONS EFFECTIVE JULY 1, 2014
JulAug14WorkingCopy.indd 12 8/21/2014 6:17:07 PM

Th e Nebraska Mortar & Pestle 13
To steal a boxing term, the UNMC College of Pharmacy is one of the best pound-for-pound fighters in the nation.
UNMC ranks No. 19, up from No. 25 a year ago, in the latest American Association of Colleges of Pharmacy (AACP) Faculty Research Grant Institutional Rankings for the fiscal year 2013. The College of Pharmacy brought in $5.5 million in National Institutes of Health (NIH) research grants. But, when adjusted for the number of full-time equivalency (FTE) faculty, UNMC's ranking surges to No. 8 in the country, its sixth year in a row in the total-dollars-per-faculty top 10.
UNMC is the smallest pharmacy school in the top 30. Yet, at $168,411 in funding per faculty, it is comparable to the University of North Carolina at Chapel Hill UNC Eshelman School of Pharmacy and the University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, which finished Nos. 2 and 5 in the overall rankings.
"Our faculty's ability to sustain a high standard of excellence and productivity in research, and an equally high standard in education, is a reflection of their commitment to our vision, and of the effort, creativity and passion each of our people brings to his or her job," said Courtney Fletcher, Pharm.D., dean of the College of Pharmacy.
"We have developed a cohort of faculty who take seriously why they are here. And we obviously support them and create an environment that allows them to do the things that they do best."
The single-biggest award in the College of Pharmacy's funding portfolio is an $11.2 million (over multiple years) National Institutes of Health COBRE (Centers of Biomedical Research Excellence) grant, with Tatiana Bronich, Ph.D., as principal investigator. But, Dr. Fletcher also highlighted a handful of other successes:
Yuri Lyubchenko, Ph.D., uses nanoimaging to investigate neurodegenerative disorders like Alzheimer's, Huntington's and Parkinson's diseases.
Jonathan Vennerstrom, Ph.D., studies new drugs to treat emerging infectious diseases.
Serguei Vinogradov, Ph.D., works to better deliver drugs to treat cancers, HIV and hepatitis.
Dong Wang, Ph.D., investigates novel drug delivery strategies to treat musculoskeletal diseases and to improve health for those with orthopedic implants.
The College of Pharmacy is operating at full capacity, Dr. Fletcher said, but will have ample opportunity to expand its research enterprise in the new Lozier Center for Pharmacy Sciences and Education and Center for Drug Discovery, which is expected to open in 2015.
Drs. Roche, Krobot step down, stay busy The College of Pharmacy said goodbye June 30 to two longtime faculty members -- but they aren't going anywhere. Ted Roche, Ph.D., retired after a 48-year career during which he earned numerous accolades, including pharmacy's Distinguished Teaching Award and UNMC's Outstanding Teacher Award. He was held in such esteem he was named an honorary alumnus by the UNMC Alumni Association in 2010.
Dr. Roche is expected to revel in his emeritus status and remain a familiar face on campus, including serving as a member of the college's curriculum committee. "We'll still see him around," said
Michelle Parks of the College of Pharmacy dean's office.
Charles Krobot, Pharm.D., a College of Pharmacy distinguished teacher and distinguished alum, worked for decades at Clarkson and University hospitals before joining the UNMC faculty 13 years ago. He stepped down June 30 as pharmacy's associate dean for student affairs. But he, too, will stick around. Dr. Krobot continues to work part-time, coordinating courses on aseptic
technique and legal and ethical principles and assisting with other courses as needed.
Christopher Shaffer, Pharm.D., assistant professor of pharmacy practice, is the new associate dean for student affairs.
College of Pharmacy stands tall among peers
Dean Fletcher
Drs. Roche and Krobot (left to right)
JulAug14WorkingCopy.indd 13 8/21/2014 6:17:07 PM

A BUYING GROUP FOR INDEPENDENT RETAIL PHARMACIES
...owned by 19 State Pharmacy Organizations...a leader negotiating on behalf of independents
...saving pharmacies money for more than 25 years...financially supports the State Pharmacy Organizations
...serving pharmacies nationwide
1-888-200-0998 | www.pacealliance.com
JulAug14WorkingCopy.indd 14 8/21/2014 6:17:07 PM

United States Pharmacopeiaand the National FormularyUSP37-NF32 Chapter <795>Pharmaceutical Compounding Nonsterile Preparations
Th is CPE lesson was written by Samuel Augustine, BS Pharm, PharmD, Professor, Pharmacy Practice Department, Creighton University School of Pharmacy & Health Professions, who has no fi nancial or confl ict of interest disclosures.
Continuing Pharmacy Education Lesson #10
What is USP37-NF32 General Chapter: <795> Pharmaceutical Compounding – NonSterile Preparations (Chapter <795>)? How does it impact pharmacy compounding? Th e USP is under continual revision and the current Chapter <795> contains all of the information that is in its newest revision which became offi cial May 1, 2014. In his article, What Does USP <795> Mean to You?, Michael Gaunt of the Institute for Safe Medication Practices begins with this statement, “If you are like most pharmacists, you probably would respond by saying, "I don't know very much about USP <795>." USP Chapter <795> addresses the extemporaneous compounding of pharmaceuticals and defi nes what constitutes good compounding practices.”1
Th e purpose of Chapter <795> is to provide guidance on good compounding practices for the preparation of nonsterile compounded formulations. Th e recent update of Section 503A of the Food Drug and Cosmetic Act now requires pharmacists that compound to “comply with the standards of an applicable United States Pharmacopoeia or National Formulary monograph, if a monograph exists, and the United States Pharmacopoeia chapters on pharmacy compounding.2 It is more relevant to the practice of pharmacy today than ever before.
ObjectivesAt the conclusion of this lesson, pharmacists and certifi ed pharmacy technicians should be able to:1. Provide a brief history of the USP chapter on Nonsterile Compounding,2. Explain the diff erences in the USP’s defi nition of Nonsterile Compounding and compare it with other defi nitions of compounding and the diff erences between the terms preparations and products as they are applied,3. Review selected sections of USP37-NF32 General Chapter: <795> Pharmaceutical Compounding – NonSterile Preparations, 4. State the Categories of Compounding and the Responsibilities of the Compounder,5. Review the Compounding Process for Nonsterile Preparations,6. Describe the General Guidelines for Assigning Beyond-Use Dating (BUD) for compounded preparations and explain the diff erence between BUDs and expiration dates, and 7. Review documentation and compounding controls required by Chapter <795>.
Chapter’s HistoryAn Expert Advisory Panel and a Review Panel on Pharmacy Compounding Practices were formed by the United States
Pharmacopeia (USP) Convention in 1993. In 1996, it published General Chapter Pharmacy Compounding Practices <1161> to guide all compounding professionals in regard to proper compounding practices and techniques. With the enactment of FDA’s Modernization Act of 1997, Chapter <1161> was renumbered to an enforceable Chapter <795> and renamed to Pharmaceutical Compounding – NonSterile Preparations. It became offi cial in 2000 and has undergone several revisions to its current form in USP37-NF32. Th e Compounding Quality Act of 2013 now references USP’s compounding chapters specifi cally. Assurance of patient safety continues to be the reason for these chapters. Th ey also protect compounders by setting standards of practice that are to be followed when processing compounded preparations. Note that in each section of the compounding chapters, the use of “shall” connotes a mandatory activity while the use of “should” indicates a recommended activity.
Organization of Chapter <795> Th is review focuses on various areas of USP Chapter <795>. Its introduction maintains that compounding is “an integral part of pharmacy practice and is essential for provision of health care”3 and emphasizes that extemporaneously compounded
Th e Nebraska Mortar & Pestle 15
JulAug14WorkingCopy.indd 15 8/21/2014 6:17:07 PM

preparations must have “acceptable strength, quality and purity”.3 Its general headings cover the entire gamut of non-sterile compounding including: categories of compounding, responsibilities of the compounder, the compounding process, compounding facilities, compounding equipment, component selection, handling and storage, stability criteria and beyond-use dating, packaging and drug preparation containers, compounding documentation, quality control, patient counseling, training and compounding for animal patients.
Defi nitionsChapter <795> defi nes several terms specifi c to pharmaceutical compounding. A compounder is defi ned as “a professional authorized by the appropriate jurisdiction to perform compounding pursuant to a prescription or medication order by a licensed prescriber.”3 A particular jurisdiction may authorize an individual other than a pharmacist to compound based on the practice act of that profession. Compounding is an integral part of pharmacy practice, but the use of “compounder” in the defi nition of compounding means that Chapter <795> applies to all individuals that are responsible for compounding nonsterile preparations, not pharmacists only.
Th is section defi nes compounding as: “Th e preparation, mixing, assembling, altering, packaging, and labeling of a drug, drug-delivery device, or device in accordance with a licensed practitioner’s prescription, medication order, or initiative based on the practitioner/patient/pharmacist/compounder relationship in the course of professional practice. Compounding includes the following:
• Preparation of drug dosage forms for both human and animal patients • Preparation of drugs or devices in anticipation of prescription drug orders based on routine, regularly observed prescribing patterns • Reconstitution or manipulation of commercial products that may require the addition of one or more ingredients • Preparation of drugs or devices for the purposes of, or as an incident to, research (clinical or academic), teaching, or chemical analysis
• Preparation of drugs and devices for prescriber’s offi ce use where permitted by federal and state law”3
Chapter <795>’s defi nition diff ers from the FDCA’s Section 503A defi nition which states: “--the term ‘compounding’ does not include mixing, reconstituting, or other such acts that are performed in accordance with directions contained in approved labeling provided by the product's manufacturer and other manufacturer directions consistent with that labeling.”4 When manufactured products are prepared, any deviations that are not consistent with manufacturer’s directions or product labeling must be considered compounding. For example, something as simple as adding a fl avoring agent to a commercial antibiotic suspension otherwise prepared according to the manufacturer’s labeling (package insert) makes the manufactured product a compounded preparation. Th e “compounder” in this example must determine if the addition has any adverse eff ect on the strength, quality or purity of the preparation.
Manufacturing is defi ned in the USP General Chapter as: “Th e production, propagation, conversion, or processing of a drug or device, either directly or indirectly, by extraction of the drug from substances of natural origin or by means of chemical or biological synthesis. Manufacturing may also include any packaging or repackaging of the substance(s) or labeling or relabeling of containers for resale by pharmacies, practitioners, or other persons.”3 Chapter <795> diff erentiates a compounded material from a manufactured one using the term preparation. “Preparation-For the purposes of this chapter, is a compounded drug dosage form or dietary supplement or a device to which a compounder has introduced a drug. Th is term will be used to describe compounded formulations; the term product will be used to describe manufactured pharmaceutical dosage forms.”3
Th e National Association of Boards of Pharmacy’s (NABP) also provides defi nitions for compounding and manufacturing in its Model State Pharmacy Act and Model Rules document:
“"Compounding" means the preparation of Components into a Drug product (1) as the result of a Practitioner’s Prescription Drug Order or initiative based on the Practitioner/patient/Pharmacist relationship in the course of professional practice, or (2) for the purpose of, or as an incident to, research, teaching, or chemical analysis and not for sale or Dispensing. Compounding includes the preparation of Drugs or Devices in anticipation of receiving Prescription Drug Orders based on routine, regularly observed prescribing patterns. And "Manufacturing" means the production, preparation, propagation, conversion, or processing of a Drug or Device, either directly or indirectly, by extraction from substances of natural origin or independently by means of chemical or biological synthesis. Manufacturing includes the packaging or repackaging of a Drug or Device or the Labeling or relabeling of the container of a Drug or Device for resale by pharmacies, Practitioners, or other Persons.”5 Nebraska’s statutes relating to the Pharmacy Practice Act uses NABP’s defi nition for compounding.
Categories of CompoundingChapter <795> provides three categories of nonsterile compounding: simple, moderate and complex based on these criteria:• degree of diffi culty or complexity of the
compounding process• stability information and warnings• packaging and storage requirements• dosage forms• complexity of calculations• local versus systemic biological disposition• level of risk to the compounder• potential for risk of harm to the patient
Each of the categories is further defi ned. Simple preparations: “making a preparation that has a … USP compounding monograph or that appears in a peer-reviewed journal article that contains specifi c quantities of all components, compounding procedure and equipment, and stability data for that formulation with appropriate BUDs; or reconstituting or manipulating commercial products that may require the addition of one or more ingredients as directed by the manufacturer. Examples include Captopril Oral Solution, Indomethacin Topical Gel, and Potassium Bromide Oral Solution, Veterinary.”3
Continuing Pharmacy Education Lesson #10
16 July/August 2014 www.npharm.org
JulAug14WorkingCopy.indd 16 8/21/2014 6:17:08 PM

Continuing Pharmacy Education Lesson #10
Moderate preparations are those that require “special calculations or procedures (such as calibration of dosage unit mold cavities) to determine quantities of components per preparation or per individualized dosage units; or making a preparation for which stability data for that specifi c formulation are not available. Examples include Morphine Sulfate Suppositories, diphenhydramine hydrochloride troches, and mixing two or more manufactured cream products when the stability of the mixture is not known.”3
Complex preparations “require special training, environment, facilities, equipment, and procedures to ensure appropriate therapeutic outcomes. Examples of possible complex preparation types include transdermal dosage forms, modifi ed-release preparations, and some inserts and suppositories for systemic eff ects.”3
Responsibilities of the CompounderIn order to keep compounded preparations of acceptable strength, quality, and purity, compounders are must be knowledgeable of all the contents of Chapter <795>. Table 1 is a list that individuals should be familiar with that relate to compounding. Compounders must also be familiar with all applicable compounding laws, guidelines, and standards.
General Principles of CompoundingGeneral Principles of Compounding covers areas that include a variety of conditions required to ensure the quality of preparations. Th ese include:1. Personnel are appropriately trained
and are capable of performing and qualifi ed to perform their assigned duties. Such training should be documented.
2. Compounding ingredients of the appropriate identity, purity, and quality are purchased from reliable sources and are properly stored according to manufacturer specifi cations or USP standards.
3. Bulk component containers are labeled with appropriate Occupational Safety and Health Administration
Table 1.USP Chapters for Compounders
Pharmaceutical Compounding – NonSterile Preparations <795>
Pharmaceutical Compounding – Sterile Preparations <797>
Pharmaceutical Dosage Forms <1151>
Pharmaceutical Calculations in Prescription Compounding <1160>
Quality Assurance in Pharmaceutical Compounding <1163>
Prescription Balances and Volumetric Apparatus <1176>
Stability Considerations in a Dispensing Practice <1191>
Written Prescription Drug Information – Guidelines <1265>
(OSHA) hazard communication labels, and Material Safety Data Sheets (MSDSs) are available to compounding personnel for all drugs and chemicals used in compounding.
4. All equipment used in compounding is clean, properly maintained, and used appropriately.
5. Th e compounding environment is suitable for its intended purpose; and procedures are implemented to prevent cross-contamination, especially when compounding with drugs (e.g., hazardous drugs and known allergens like penicillin) that require special precautions.
6. Only authorized personnel are allowed in the immediate vicinity of the drug compounding operations.
7. Th ere is assurance that processes are always carried out as intended or specifi ed and are reproducible.
8. Compounding conditions and procedures are adequate for preventing errors.
9. All aspects of compounding are appropriately documented.
10. Adequate procedures and records exist for investigating and correcting failures or problems in compounding, testing, or the preparation itself.3
Compounding ProcessCriteria for the compounding process are set to ensure that the preparation will meet the intended needs of the patient for the therapeutic outcome. Th ese range from ensuring chemical and physical properties of the components in the preparation to establishing a Beyond-Use Date (Table 2).
Compounding Facilitiesand EquipmentTh e focus of the facilities section is on the requirements for space and design for the safe and orderly processing of compounded preparations to prevent mix-ups and adventitious cross contamination. It addresses general requirements for plumbing, heating, ventilations, air conditioning and potable water supply/use. General storage conditions are defi ned in the USP’s General Notices and Requirements and Packaging and Storage Requirements<659> and referenced in Chapter <795> along with the requirement to follow manufacturer’s labeled storage conditions. Th e environment must be controlled to prevent decomposition and contamination of chemicals. Monitoring processes and equipment are also recommended in this section as well as the handling of hazardous drugs. (Note: USP is proposing a separate General Chapter for handling hazardous drugs in health care settings.)
Requirements for equipment and utensils used in compounding drug preparations provide that these must have appropriate design, capacity and be of suitable composition in order to protect the purity of the compounded preparations. Cleaning, storage, and calibration activities along with the potential for use of disposable equipment are all recommended in this section.
Component Selection, Handling and StorageGuidelines that are required for selecting, handling, and storing components for
Th e Nebraska Mortar & Pestle 17
JulAug14WorkingCopy.indd 17 8/21/2014 6:17:08 PM

compounded preparations are provided in this section. Th ese include the certifi cation, quality, storage, and expiration dating of the ingredients used in processes. Th ere is a requirement that components be manufactured in an FDA-registered facility. If this is not possible, the compounder must use their professional judgment to select a reliable source. Compounders are also required to establish the purity and safety of the components by reasonable means which are described as a Certifi cate of Analysis and the manufacturer’s reliability and reputation.
Stability Criteria and Beyond-Use DatingA manufacturer’s expiration date is determined using scientifi c techniques and statistical analysis. Because each drug product has unique chemical and physical properties, good manufacturing practices will not provide a single set of rules that would cover all situations. Th e
Table 2.Criteria – Compounding Each Drug Preparation3
Dose, safety, and intended use of preparations or devices have been evaluated for suitability.Master Formulation Records should be created before initial compounding a preparation time - records shall be followed each time that preparations are made. Compounding Records should be completed each time preparations are compounded.Ingredients used in formulations have expected identity, quality, and purity… Certifi cates of Analysis, when applicable, and MSDSs have been consulted for all ingredients used.Compounding is done in an appropriately clean and sanitized area dedicated to this activity.Only one preparation is compounded at one time in a specifi c workspace.Appropriate compounding equipment has been selected and inspected for cleanliness and correct functioning and is properly used.Reliable BUDs are established to ensure that fi nished preparations have accepted potency, purity, quality, and characteristics, at least until labeled BUD.Personnel…maintain good hand hygiene and wear clean clothing appropriate to type of compounding performed (e.g., hair bonnets, coats, gowns, gloves, facemasks, shoes, aprons, or other items) as needed for protection of personnel from chemical exposures and prevention of drug contamination.Preparations are made in accordance with Chapter <795>, other offi cial standards referenced in chapter, and relevant scientifi c data and information. Critical processes (including but not limited to weighing, measuring, and mixing) are verifi ed by compounder to ensure procedures… will consistently result in expected qualities in fi nished preparation.Final preparations are assessed using factors such as weight, adequacy of mixing, clarity, odor, color, consistency, pH, and analytical testing as appropriate. Th is information is recorded on Compounding Records.Preparations are packaged as recommended in Packaging & Drug Preparation Containers of Chapter <795>’s section. Preparation containers are labeled according to applicable state and federal laws. Labeling shall include BUD and storage and handling information Labeling should indicate that “this is a compounded preparation”. Master Formulation Records & Compounding Records have been reviewed by compounder to ensure that errors have not occurred in compounding process and preparations are suitable for use. Preparations are delivered to patients or caregivers with appropriate consultation.
Beyond-Use Date (BUD) diff ers from an expiration date since it is often based on conservative but reasonable estimates. BUD is defi ned in USP <795> as “the date after which a compounded preparation shall not be used.”3 Th e determination of that date takes into account when the preparation was compounded and the intent for its immediate use. Criteria used to assign the BUD are diff erent from those applied to a manufactured product. Conservative considerations for setting a BUD should be applied and drug-specifi c stability documentation and scientifi c literature should be used if available. See Table 3 for a list of considerations to be used in BUD determinations.
When establishing a BUD using a manufactured product as the source of an active pharmaceutical ingredient the compounder may not use the manufacturer’s product expiration date alone. Th e compounder is required to “refer
to the manufacturer for stability information and to the literature for applicable information on stability, compatibility, and degradation of ingredients”.3 Other sections of the USP are also to be referred to. Table 4 provides the guidance for establishing BUD by type of formulation.
Packaging and Drug Preparation ContainersContainer and container components must protect the quality, strength and integrity of the preparation. Th e compounder is required to ensure that container and container components meet USP standards described in several of its enforceable chapters. Performance of the tests in those chapters is not a requirement, but an understanding of standards within each is required. If a USP monograph for the compounded preparation is available, the compounder must use the container it specifi es.
Continuing Pharmacy Education Lesson #10
18 July/August 2014 www.npharm.org
JulAug14WorkingCopy.indd 18 8/21/2014 6:17:08 PM

Continuing Pharmacy Education Lesson #10
Table 4.BUD by Type of Formulationa
For Nonaqueous Formulations—Th e BUD is not later than the time remaining until the earliest expiration date of any API or 6 months, whichever is earlier
For Water-Containing Oral Formulations—Th e BUD is not later than 14 days when stored at controlled cold temperatures
For Water-Containing Topical/Dermal and Mucosal Liquid and Semisolid Formulations—Th e BUD is not later than 30 daysa Th ese maximum BUDs are recommended for nonsterile compounded drug preparations in the absence of stability information that is applicable to a specifi c drug or preparation. Th e BUD shall not be later than the expiration date on the container of any component.
Table 3.Considerations for Applying a BUD3
nature of the drug and its degradation mechanismdosage form and its componentspotential for microbial proliferation in the preparationcontainer in which it is packagedexpected storage conditionsintended duration of therapy
Compounding DocumentationTh is section requires compounders who dispense prescriptions to comply with pharmacy record-keeping requirements of their state. If the manufacturer’s labeling instructions for the mixing of the preparation are followed, further documentation is not required. All other compounding requires documentation as set forth by this section. Examples of documents that provide the required sections of a Master Formulation Record and a Compounding Record are presented in Appendix 1 and 2, respectively.
Written standard operating procedures (SOPs), step-by-step instructions, are recommended. Th e suggested list of SOPs respective to nonsterile compounded preparations includes these sections: facilities, equipment, personnel, preparation, packaging, and storage of preparations. Th eir implementation provides for consistency of procedures and also works as references for training of personnel.
Another requirement is for compounding personnel to have ready access to Material Safety Data Sheets (MSDSs) for bulk chemicals and drug
substances located in the compounding facility. Th ese may be in electronic or hard copy format.
Quality ControlTh e quality control of compounded preparations ensures their safety and performance. Chapter <795> requires the compounder to use prudent pharmaceutical judgment in their review of calculations, accuracy, and precision of measurements of the correct ingredients and the compounding process. Th e fi nished preparation must be observed for expected appearances. An investigation of any discrepancies along with actions to correct problems must be performed before the preparation can be dispensed.
Compounding controls in this section necessitate the proper execution of the compounding process as established by the Master Formulation Records, the Compounding Records and any other of the pharmacy’s written procedures. It requires the documentation of any deviations from the compounding process. Verifi cation of each procedure and each stage of the compounding process must be performed as well as monitoring of the function of any compounding
equipment. Verifi cations of critical steps in the process by a trained second person are recommended. It is important to diff erentiate between the terms verify and verifi cation and validate and validation. In the case of compounded preparations, the terms verify and verifi cations are used to ensure that all processes are checked for appropriateness and accuracy. Validate and validations are used to describe controlled testing of manufactured products in the manufacturing process. A validation process is more involved and time consuming when it is compared to a verifi cation activity. Th e General Information Chapter, Quality Assurance in Pharmaceutical Compounding <1163> is recommended as a source for further guidance in developing and applying compounding quality control procedures.
Patient CounselingTh is requires the dispensing pharmacist to counsel the patient or the patient’s agent about the “proper use, storage, handling and disposal of the compounded preparation.”3 According to this section, counseling on compounded preparations must include instruction for the patient or patient’s agent to report any adverse events and/or any changes to the physical characteristics of the preparation to the compounder. Th e pharmacist is directed to General Information Chapter <1191>, under its heading of Responsibility of Pharmacists, which provides among other things physical signs of deterioration of dosage forms. Th is section requires the compounder to document any reported problems and to follow up with appropriate corrective actions.
TrainingTh e implementation of an on-going training program for all compounding personnel in the facility is to be ensured by the compounder. Th is section recommends an annual evaluation of compounding personnel. Requirements and recommendations for training procedures are listed in Table 5.
Th e Nebraska Mortar & Pestle 19
JulAug14WorkingCopy.indd 19 8/21/2014 6:17:08 PM

SummaryChapter <795> was developed to provide standards of practice for all compounders of nonsterile pharmaceuticals in order to improve and maintain patient safety. Th e Chapter is under continuous review and revision to provide contemporary compounding practices that are safe and eff ective. Pharmacists involved in compounding have the responsibility to understand and apply standards issued by the USP in order to ensure that extemporaneously compounded, nonsterile preparations have acceptable, strength, quality and purity.
References1. What Does USP <795> Mean to You. Pharmacy Times April 18, 2013 http://www.pharmacytimes.com/publications/is-sue/2013/April2013/What-Does-USP-795-Mean-to-You accessed January 8, 2014.2. Section 503A of the Federal Food, Drug and Cosmetic Act http://www.fda.gov/Drugs/GuidanceComplianceRegulatory-Information/PharmacyCompounding/ucm376733.htm accessed January 8, 2014.3. US Pharmacopeial Convention, Inc. United States Pharmacopeia 37 National Formulary 32 Rockville, MD:US Pharma-copeial Convention, Inc; 2014.4. Th e Drug Quality and Security Act. HR 3204 (PL 113-54). November 27, 2013. http://beta.congress.gov/113/plaws/publ54/PLAW-113publ54.pdf Accessed February 28, 2014. 5. Th e Model State Pharmacy Act and Model Rules of the National Association of Boards of Pharmacy (Model Act) http://www.nabp.net/publications/model-act/ Accessed February 28, 2014
Continuing Pharmacy Education Lesson #10
20 July/August 2014 www.npharm.org
Policies for the Nebraska Mortar & Pestle (M&P) continuing pharmacy education lessons and quizzes:
1. M&P Quizzes are valid only for the membership year in which they are published. Quizzes for the 2014 Membership Year must be received by December 8, 2014. Quizzes cannot be carried over to another membership year.
2. If more than three questions are missed, the quiz will be returned. Th e quiz can be resubmitted.
3. CPE transcripts can be printed from NABP e-Profi les at www.nabp.net.
4. CPE credits are submitted to NABP by the 15th of each month. For example, M&P CPE quizzes completed in the month of August 2014, will be sent to NABP e-Profi les before September 15, 2014.
Th e Nebraska Council for Continuing Pharmacy Education (NCCPE) is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education (CPE).Th is CPE home study lesson has been accredited for 2.0 contact hours or 0.20 CEUs. UAN #128-000-14-101-H03-P/T. Th is lesson is a knowledge-based CPE activity targeted to pharmacists and pharmacy technicians.
Th e authors and the Nebraska Pharmacists Association disclaim any liability to you or your patients resulting from reliance solely upon the information contained herein.
Quiz Answers may be submitted:1. Online: www.npharm.org
2. Fax: 402-420-1406
3. Email: m&[email protected]
4. Mail: NPA Mortar & Pestle6221 S 58th St, Ste ALincoln, NE 68516
Table 5.Training Procedures3
All employees involved in pharmaceutical compounding shall read and become familiar with chapter <795>. Th ey should be familiar with the contents of USP Pharmacists’ Pharmacopeia and other relevant publications, including how to read and interpret MSDSs
All employees shall read and become familiar with each of the procedures related to compounding, including those involving the facility, equipment, personnel, actual compounding, evaluation, packaging, storage, and dispensing
All personnel who compound hazardous drugs shall be fully trained in the storage, handling, and disposal of these drugs. Th is training shall occur before preparing or handling hazardous drugs.
All training activities shall be documented. Th is includes meetings between compounder and employees to review work activities and provide feedback.
Compounders shall demonstrate procedures for employees and shall observe and guide employees throughout the training process. Employees will then repeat procedures without any assistance from, but under direct supervision of, compounders.
When employees have demonstrated to compounders their verbal and functional knowledge of procedures, then and only then, will employees be permitted to perform procedures without direct supervision. Th e compounder should be physically present and shall approve all ingredients, quantities, and fi nal preparations.
When compounders are satisfi ed with employees’ knowledge and profi ciency, compounders will sign documentation records to show that employees were appropriately trained.
Compounders shall continually monitor work of employees and ensure that employees’ calculations and work are accurate and adequately performed.
Compounders are solely responsible for fi nished preparations.
JulAug14WorkingCopy.indd 20 8/21/2014 6:17:08 PM
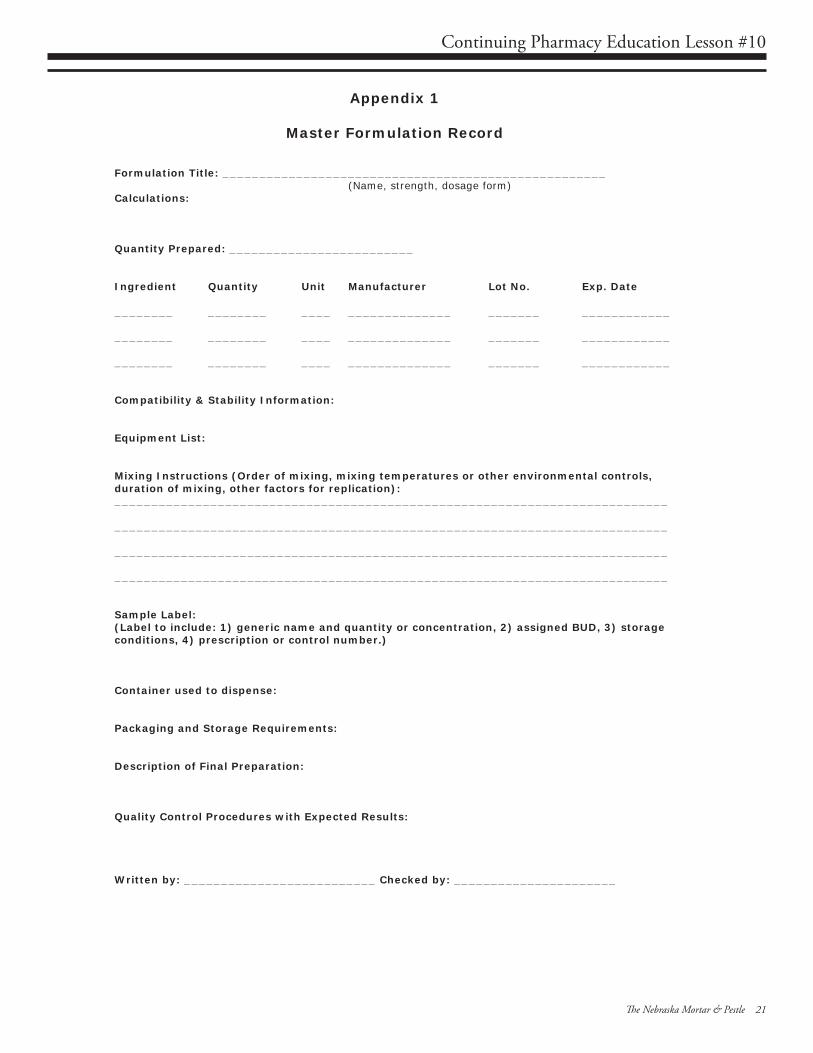
Continuing Pharmacy Education Lesson #10
Th e Nebraska Mortar & Pestle 21
Appendix 1
Master Formulation Record
Formulation Title: ____________________________________________________ (Name, strength, dosage form)
Calculations:
Quantity Prepared: _________________________
Ingredient Quantity Unit Manufacturer Lot No. Exp. Date
________ ________ ____ ______________ _______ ____________
________ ________ ____ ______________ _______ ____________
________ ________ ____ ______________ _______ ____________
Compatibility & Stability Information:
Equipment List:
Mixing Instructions (Order of mixing, mixing temperatures or other environmental controls, duration of mixing, other factors for replication): ___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
Sample Label: (Label to include: 1) generic name and quantity or concentration, 2) assigned BUD, 3) storage conditions, 4) prescription or control number.)
Container used to dispense:
Packaging and Storage Requirements:
Description of Final Preparation:
Quality Control Procedures with Expected Results:
Written by: __________________________ Checked by: ______________________
JulAug14WorkingCopy.indd 21 8/21/2014 6:17:08 PM

Continuing Pharmacy Education Lesson #10
22 July/August 2014 www.npharm.org
Appendix 2
Compounding Record
Preparation Name: ____________________________________________________ (Name, strength, dosage form)
Master Formula Record: _________________________
Ingredient Quantity Unit Manufacturer Lot No. Exp. Date
________ ________ ____ ______________ _______ ____________
________ ________ ____ ______________ _______ ____________
________ ________ ____ ______________ _______ ____________
Quantity Prepared: _____________________________
Prepared By: __________________________ Approved By: __________________________
QC Performed By: ____________________________
Date Prepared: ___________________ Control or Prescription Number: ______________
Beyond-Use Date: _________________
Attach Duplicate Label:
Quality Control Testing:
Test: Results:
____________________________ ____________________________________
____________________________ ____________________________________
____________________________ ____________________________________
Released by: __________________________ Date: _______________________
Comments: (Document Quality Control issues, adverse reactions and/or preparation problems.)
JulAug14WorkingCopy.indd 22 8/21/2014 6:17:08 PM

USP37-NF32 Chapter <795> Pharmaceutical Compounding - Nonsterile PreparationsQuiz #10, July/August 2014, ACPE UAN #128-000-14-101-H03-P/T
2014 Quiz #10 - NPA CPE Home Study Answer FormUSP37-NF32 Chapter <795>
Pharmaceutical Compounding - Nonsterile PreparationsUAN #128-000-14-101-H03-P for pharmacists
UAN #128-000-14-101-H03-T for pharmacy technicians2.0 Contact Hours - Knowledge Based CPE Activity
Name ________________________________________________________
Mailing Address _______________________________________________
City/State/Zip _________________________________________________
*NABP e-Profi le # ______________ *Date of Birth (MMDD) _________*Required for ACPE credit.
Circle one (1) Answer:1. a b c d 6. a b c d2. a b c d 7. a b c d3. a b c d 8. a b c d4. a b c d 9. a b c d5. a b c d 10. a b c d
CPE Home Study Evaluation 1. Rate this lesson: (Excellent) 5 4 3 2 1 (Poor)
2. Did this lesson meet each of its objectives? ___ Yes ___ No3. Was the content without commercial bias? ___ Yes ___ No 4. Did the lesson meet your educational/practice needs? ___ Yes ___ No5. Comments/future topics are welcome. ________________________
The deadline for this quiz is December 8, 2014
Keep the TOP portion for your records. Return the BOTTOM portion to the NPA offi ce.Or, take this quiz online at www.npharm.org
1. In what year did Chapter <795> became an offi cial enforceable USP General Chapter?
a. 1993 c. 1997b. 1996 d. 2000
2. Unlike Chapter <795>, according to the FDCA section503A, compounding does not include:
a. formulating preparations which require special training and environmentb. making preparations for which stability data for that specifi c formulation are not availablec. preparing devices for the purposes of, or as an incident to, research d. reconstituting a commercial product without deviating from package insert directions
3. According to Chapter <795>, this preparation would be considered as an example of the moderate category of compounding:
a. Indomethacin Topical Gel, USPb. Morphine Sulfate Trochec. Potassium Bromide Oral Solution, Veterinaryd. Triiodothyronine Sustained Release Capsule
4. Pharmacists that compound nonsterile preparations are requiredto be knowledgeable on which Chapter?
a. <795> c. <1160>b. <797> d. <1265>
5. Which is not a criterion used in the determination of the BUD of a compounded preparation?
a. assignment of the BUD to be the same as the manufacturer’s expiration dateb. consideration of the potential for microbial proliferation in the preparationc. intended duration of therapy of the compounded preparationd. use of degradation characteristics and mechanisms the of a drug entity
6. Which water-containing formulation would be expected to have the shortest BUD?
a. dermal liquid c. oral liquidb. mucosal liquid d. semisolid
7. According to the compounding documentation section of Chapter <795>, all compounding personnel must have ready access to:
a. Facility’s SOPs c. Master Formulation Recordsb. Compounding Records d. Material Safety Data Sheets
8. Chapter <795>’s quality control section does not require the compounder to provide which of the following?
a. fi nished preparation to be observed for expected appearancesb. investigations of any discrepancies in compounding of the preparationc. review of the accuracy and precision of measurements of the correct ingredientsd. validation of critical steps in the process by a trained second person
9. Th e dispensing pharmacist is required to counsel the patient or the patient’s agent to report any changes to the physical characteristics of the preparation to the pharmacy. Th ese physical signs of deterioration of dosage forms can be found in USP General Information Chapter:
a. <1151> c. <1191>b. <1163> d. <1265>
10. Which of the following training procedures for personnel involved in compounding nonsterile preparations are required?
a. mandatory annual training for all compounding personnel in the facilityb. compounders to sign documents that state that they are satisfi ed with the employees’ knowledge and profi ciency to show they have been appropriately trainedc. personnel compounding preparations are to be solely responsible for fi nished preparationsd. any trained employees must verify other employees’ calculations and work as accurate
Continuing Pharmacy Education Quiz #10
Th e Nebraska Mortar & Pestle 23
JulAug14WorkingCopy.indd 23 8/21/2014 6:17:08 PM

www.phmic.com
your single sourcefor insurance protection
Not licensed to sell all product in all states.
we will be there, standing beside you
from one generation to the nextAt Pharmacists Mutual, we are committed to building lasting relationships with our customers, always promising to focus on our members’ best interests. We are proud to be the leading provider of specialty commercial and personal insurance products and risk management services for the pharmacy profession. Give us a call, we look forward to partnering with you.
Find us on Social Media:
Melissa McKean, CISR, CIC
800.247.5930 ext. 7127308.870.2873
JulAug14WorkingCopy.indd 24 8/21/2014 6:17:08 PM

Rx and Th e Law
Th e Nebraska Mortar & Pestle 25
AND THE LAWBy Don R. McGuire, Jr., RPh, JD
Th is series, Pharmacy and the Law, is presented by Pharmacists Mutual Insurance Company and the Nebraska Pharmacists Association through Pharmacy Marketing Group, Inc., a company dedicated to providing quality products and services to the pharmacy community.
WHY IS THAT PHARMACIST ASKING SO MANY QUESTIONS?
©Don R. McGuire, Jr., RPh, JD, is General Counsel, Senior Vice President, Risk Management & Compliance, at Pharmacists Mutual Insurance Company. Th is article discusses general principles of law and risk management. It is not intended as legal advice. Pharmacists should consult their own attorneys and insurance companies for specifi c advice. Pharmacists should be familiar with policies and procedures of their employers and insurance companies, and act accordingly.
One of the duties required of pharma-cists under OBRA ’90 is that a Drug
Utilization Review (DUR) be performed. In the years since, the profession has de-veloped specialized areas of DUR, such as medication reconciliation in the hospital setting. In the end, a healthcare professional should make sure that the patient is on the correct drugs for their condition(s), that they are taking them at the correct dosages, and that all the medications work together. Th e professional best suited to provide this service, whatever you call it, is a pharmacist.
What does the pharmacist need in order to provide this service eff ectively? Up to date patient information and an up to date medication list are key. Reasonable eff orts to obtain this information should be made by the pharmacist or their staff . Patients are sometimes reluctant to pro-vide this information. It may be a privacy concern, embarrassment, or it may be that they don’t understand why it is needed by the pharmacist. Patient education may be helpful in the latter case. In the hospital setting, an accurate list upon admission may diffi cult to obtain initially, but with the help of the physician’s offi ce, and many times the patient’s community pharmacist, the blanks can easily be completed. Medication reconciliation is also important at discharge. Discontinued or changed dosages are communicated to the patient. Th e patient
should give this new information to their community pharmacist and pharmacists should be looking for it if they are aware of any hospital admissions or procedures. Continued focus on continuum of care will allow all pharmacists to better serve their patients through increased access to current information.
In the end, the pharmacist must proceed with the information at hand. Th e patient should understand that the quality of the DUR depends on the information that the pharmacist has to use. We cannot force patients to provide the necessary in-formation. However, the pharmacist should document their attempt to gather it if they cannot obtain it.
Once the review is fi nished, the key to a successful DUR encounter is to take action with any fi ndings that are out of the ordi-nary. Th is may mean having a discussion with the patient about their condition and/or their therapy. Many times these conver-sations can clear up any misinterpretations or other mistakes. A well-informed patient can be a good ally to make sure that their therapy is appropriate.
But at other times, a call to the pre-scriber about one or more drugs that are causing concern, or have the potential to cause a problem, is required. Again, docu-mentation is key. Make good notes about the conversations or phone calls. Record the
date, time, participants, and the content of the discussions. If changes to therapy need to be made, make sure that the changes are well-documented also. Don’t assume that someone else has discussed your concerns with the patient or has interacted with the prescriber. Many times the pharmacist is the last line of protection for the patient. Th is doesn’t excuse those professionals who have acted before you, but in most situa-tions, there is no one to take action after you. Th ere are also situations where pre-scribers will not change the ordered therapy. Th e pharmacist must then act to protect the patient within their professional boundar-ies. A previous article in this series discussed refusing to fi ll prescriptions.
Th e patients’ health and well-being depend on all healthcare professionals do-ing their respective jobs to the best of their abilities. For pharmacists, one aspect of this means doing your best to gather patient information, performing a thorough DUR, and carrying through with any needed recommendations. Your patients may not realize that this is going on behind the scene, so educate them about what you are doing to protect them. Th ey should value your service even more.
JulAug14WorkingCopy.indd 25 8/21/2014 6:17:09 PM

Legal and Business Aspects of the Changing Medical Marijuana LandscapeTh is CPE lesson was written by Hyrum Wilson, PharmD Candidate, Creighton University School of Pharmacy & Health Professions, who has no fi nancial or confl ict of interest disclosures. Th is lesson does include a discussion of unlabeled or investigational use of a product(s) that has not yet been approved by the FDA for the use being presented. Note: Th e laws as discussed here were current as of July 2014.
ObjectivesAt the conclusion of this lesson, pharmacists and certifi ed pharmacy technicians should be able to:1. Describe the process to qualify for use of medical marijuana. 2. Identify the regulatory and business aspects of the medical marijuana industry. 3. Explain the concerns regarding the legalization of medical marijuana.
IntroductionTrends in medical marijuana useTh e fi rst state to allow the medical use of marijuana was California, when it passed Proposition 215 in 1996. During the decade following, nearly one state per year passed legislation legalizing medical marijuana. Since 2012, this rate has accelerated. Nine states have adopted medical marijuana laws, bringing the total to twenty-three states which allow the use of marijuana for the treatment of specifi c medical conditions.1 (See Table 1).
In addition to the use of marijuana for medical diagnoses, there has been wide-spread adoption of marijuana for recreational use. Eighteen states have
decriminalized the use of marijuana for recreational purposes. In these states, possession is a civil instead of a criminal matter.2 And two states, Colorado and Washington, legalized the use of recreational marijuana for persons over the age of eighteen. Nebraska decriminalized the possession of up to one ounce of marijuana in 1979, but does not have a medical marijuana law. In July 2014, the New York Times ran a week-long series of editorials calling for an end to federal government’s prohibition stance towards marijuana. Th e editorial series covered everything from federal obstruction of marijuana research to the economic and social impacts of the ‘war on drugs’.
Despite the current permissiveness toward marijuana use and popular sentiment (a May 2013 Fox News Poll found 85% of respondents in favor of medical marijuana), the Drug Enforcement Agency (DEA) has kept marijuana on the list of Schedule I drugs, stating there is no established, safe medical use for marijuana. Th e DEA has relied on state and local authorities to address marijuana activity through their own laws. As states have taken steps to legalize and/or decriminalize
cannabis containing products, Eric Holder, the Attorney General of the United States, released guidelines stating federal resources should not be used to prosecute individuals who use medical marijuana in compliance with state laws.3 In 2013, Deputy Attorney General James Cole informed the governors of Colorado and Washington that their offi ce would not pursue legal actions regarding marijuana use in these states as long as the states provided a strict regulatory system and adequate enforcement.4
Legal Aspects Surrounding the Use of MarijuanaHow do patients qualify for medical marijuana?In states with medical marijuana laws, a patient can obtain cannabis for medical purposes by being seen by a physician, advanced practice registered nurse, homeopathic or naturopathic physician, and in some cases, a physician assistant. Because marijuana remains a Schedule I drug, prescribers cannot write a prescription for it, nor can pharmacists dispense it if presented with a prescription. Instead, states allow prescribers to write a recommendation for a patient to use marijuana, which can
Continuing Pharmacy Education Lesson #11
26 July/August 2014 www.npharm.org
JulAug14WorkingCopy.indd 26 8/21/2014 6:17:09 PM

Continuing Pharmacy Education Lesson #11
Table 1.States with Medical Marijuana Laws
State Marijuana Limits Home Cultivation DispensariesAlaska 1 ounce 6 plants, no more than 3 mature Not allowed
Arizona 2.5 ounces 12 plants if the patient is greater than 25 miles from a dispensary
Yes, a maximum of 126 dispensaries, about 1 per 10 pharmacies
California Not defi ned in state law Home cultivation is not allowed No, state law only allows for co-operatives and collectives
Colorado 1 ounce 6 plants, no more than 3 mature Yes, a total of 470 “medical marijuana centers”
Connecticut 2.5 ounces Home cultivation is not allowed Yes, dispensaries must be run by a licensed pharmacist
Delaware 6 ounces Home cultivation is not allowed Yes, a maximum of 3 “compassion centers”
District of Columbia 2 ounces Home cultivation is not allowed Yes, a maximum of 8 dispensaries
Hawaii 4 ounces 7 plants Not allowed
Illinois 2.5 ounces Home cultivation is not allowed Yes, a maximum of 60 dispensaries
Maine 2.5 ounces 6 plants Yes, a maximum of 8 dispensaries
Massachusetts 10 ounces No, although a special “hardship cultivation registration” can be applied for
Yes, a maximum of 35 dispensaries
Maryland To be determined Home cultivation is not allowed Yes
Michigan 2.5 ounces 12 plants Not allowed
Minnesota 30 days supply, excludes smoking
Home cultivation is not allowed Yes, a maximum of 2 dispensaries
Montana 1 ounce 4 mature plants, 12 seedlings Not allowed
Nevada 2.5 ounces every 14 days 3 mature plants, 4 seedlings Yes, a maximum of 66 dispensaries
New Hampshire 2 ounces Home cultivation is not allowed Yes, a maximum of 4 “alternative treatment centers”
New Jersey 2 ounces every 30 days Home cultivation is not allowed Yes, a maximum of 6 “alternative treatment centers”
New Mexico 6 ounces 4 mature plants, 12 seedlings Yes
New York 30 days supply Home cultivation is not allowed Yes
Oregon 24 ounces 6 mature plants, 18 seedlings Yes
Rhode Island 2.5 ounces 12 plants Yes, a maximum of 3 “compassion centers”
Vermont 2 ounces 2 mature plants, 7 seedlings Yes, a maximum of 4 dispensaries
Washington 24 ounces 15 plants Medical marijuana dispensaries are not allowed, 334 retail marijuana stores are approved
Th e Nebraska Mortar & Pestle 27
JulAug14WorkingCopy.indd 27 8/21/2014 6:17:09 PM

Continuing Pharmacy Education Lesson #11
then be used to either purchase cannabis products or cultivate a set number of marijuana plants at home.5 Th e federal government tried to disallow the practice of recommending marijuana for medical use, but lost in federal court when the Ninth Circuit Court of Appeals ruled physicians cannot be sanctioned for providing accurate information to patients if it is based on sincere medical judgment.6
Only Maryland requires a prescriber to undergo special training or clinical certifi cation in order to recommend marijuana. One organization, the American Academy of Cannabinoid Medicine, off ers board certifi cation for interested physicians. Some states require a practitioner to register with the state prior to recommending cannabis to a patient.
One notable exception to marijuana recommendation authority is for physicians working in Veterans Administration facilities. Since federal facilities must abide by federal laws, the recommendation of marijuana for medical treatment is prohibited.7 Th is can be problematic for many veterans, as marijuana has been shown to have effi cacy for the treatment of post-traumatic stress syndrome.
Not every condition is covered in every state that allows medical marijuana. (See Table 2) Every state with a comprehensive medical marijuana law specifi cally mentions diseases such as cancer, multiple sclerosis, and HIV/AIDS.8 Other conditions such as glaucoma, chronic pain, and seizure disorders are not mentioned in every law, but medical marijuana programs have a process for allowing conditions not specifi cally covered under state law.
Who is allowed to purchase and possess marijuana?Patients who wish to use marijuana to treat their disease have a few rules they must follow to qualify. With the exception of Washington, patients are required to obtain an ID card in order to purchase, possess, and legally use marijuana.8 Th ese cards are typically valid for one year and must be renewed upon expiration. In the event the patient is cured of their qualifying disease or condition, the cards must be surrendered to the state. Out of the twenty-three states which allow medical marijuana, fi fteen have prescription drug monitoring programs
(PDMP).9 Only Arizona and New York include medical marijuana on their PDMP, but there is legislation in Massachusetts (H 1917) proposing tracking marijuana through their state’s PDMP.
Due to fi nancial or medical hardships, some patients are unable to purchase marijuana for themselves. In
Table 2.Medical Marijuana Covered Conditions
State
Diseases Conditions
Can
cer
HIV
/AID
S
Gla
ucom
a
Mus
cle
Spas
tici
ty D
isor
ders
Ano
rexi
a or
Was
ting
Seiz
ure
Dis
orde
r
Chr
onic
Pai
n
Chr
onic
Nau
sea
Alaska x x x x x x x x
Arizona x x x x x x x x
California x x x x x x x x
Colorado x x x x x x x x
Connecticut x x x x x x
Delaware x x x x x x x
District of Columbia x x x x
Hawaii x x x x x x x x
Illinois x x x x x
Maine x x x x x x x x
Maryland x x x x x x x x
Massachusetts x x x
Michigan x x x x x x x x
Minnesota x x x x x x x x
Montana x x x x x x x x
Nevada x x x x x x x x
New Hampshire x x x x x x x x
New Jersey x x x x x
New Mexico x x x x x x x x
New York x x x x x x x
Oregon x x x x x x x x
Rhode Island x x x x x x x x
Vermont x x x x x x
Washington x x x x x x x x
these instances, a patient can designate a caregiver to assist them in obtaining medical marijuana.8 Eight states limit the number of patients a caregiver can help to one, and six more states allow a single caregiver to assist up to fi ve patients. Montana has no limit on the number of patients a single caregiver can help. Th is led to the unintended
28 July/August 2014 www.npharm.org
JulAug14WorkingCopy.indd 28 8/21/2014 6:17:10 PM

Continuing Pharmacy Education Lesson #11
consequence of some caregivers opening a retail location (Montana only allows home cultivation) by acting as a ‘caregiver’ to every patient who walked through their door. Montana is revising its law to limit the number of patients to three.5
Caregivers in most states undergo the same registration process as patients. Th ey apply for an ID card which allows them to purchase and transport a limited quantity of marijuana for a specifi c patient. Th ey cannot be compensated for their time or labor, but they can be compensated for direct costs such as the actual cost of marijuana or mileage for travel.
Where patients are allowed to obtain marijuana is very state-dependent. Alaska is one of fi ve states which allows only home cultivation of marijuana for medical use. Other states do not allow home cultivation and all cannabinoid products must be purchased from a registered dispensary. Eight states allow for a combination of methods for marijuana procurement. Massachusetts, for example, requires all marijuana to be purchased through a licensed treatment center, but patients who can demonstrate hardship can get a waiver for home cultivation. Th e majority of states with marijuana dispensaries divide the state along county or law enforcement districts. Each district is allowed a certain number or proportion of dispensaries to ensure there are no underserved populations.
For states that allow marijuana dispensaries, there was concern about patients purchasing the maximum amount of marijuana from several diff erent dispensaries. In response, medical marijuana patients are required to designate the dispensary from which they purchase their cannabis, which is included on the patient’s ID cards. Dispensaries must check the ID to ensure they are the designated source for that person’s medical marijuana.10 Th e notable exception is Washington which has no registry and does not require ID cards. Any person in this state can possess up to twenty-four ounces (one and one-half pounds) of marijuana for either medical or recreational use.
Seventeen of the twenty-three states with medical marijuana laws limit the amount of marijuana a patient can possess to under six ounces. Massachusetts allows up to ten ounces, which the Massachusetts
Department of Public Health has determined to be suffi cient for sixty days. Twelve states allow for home cultivation of marijuana. Th ey typically limit the number of marijuana plants to six or less, but there are variances between state laws.
Where can a patient use medical marijuana?All states prohibit the use of marijuana in specifi c places. Th e most common places where marijuana is banned include prisons, hospitals, schools, school buses, and in public. Most states ban smoking marijuana in bars and restaurants. Th ere are also provisions which allow employers to ban the use of marijuana at a place of employment. Additionally, landlords may prohibit the smoking of marijuana on their premises, although they cannot refuse to rent to a person for being a medical marijuana patient.
With all the restrictions on where patients can or cannot smoke marijuana, there is a burgeoning industry dedicated to providing alternatives. One company off ers “pot tours,” which makes special accommodations for people to use marijuana outside of their home. Since many hotels do not allow the smoking of marijuana in their rooms, these tours provide vaporizable cannabis products which comply with both state regulations and hotel policy.
Another newly formed industry providing an alternative location to consume marijuana products are smoking clubs. Similar to how an organization like Elks Lodge or American Legion is able to circumvent local tobacco regulations, a smoking club is a private organization only open to members and not the general public.11 Since all states ban on-site consumption at licensed cannabis shops, these clubs do not have cannabis products for sale, but they do provide a safe environment for its members. Public consumption bans only prohibit the smoking of marijuana. Both vaporizing and consuming cannabis infused goods in public are still legal.
Since marijuana is a Schedule I drug on the national level, this causes diffi culties for patients who wish to travel to another state for work or vacation. Many states do not allow the importation or exportation of
marijuana, even for personal medical use. Depending on the patient’s destination, it may not be possible to travel without entering states that do not allow marijuana use of any kind. A few states, such as Arizona and New Hampshire, recognize marijuana ID cards from other states, but they are not valid for purchasing marijuana in those states. Patients must bring their own supply from their home state.
Iowa recently passed a bill allowing the use of cannabidiol extract for the treatment of intractable epilepsy. However, the law does not make any provisions for the extract to be produced in the state. Th e patient or caregiver must travel to a diff erent state to obtain the extract. Very few states allow non-residents to qualify for medical marijuana. Recreational states, such as Colorado, are an option, but there is no route from Iowa to Colorado that passes through a state where marijuana possession is legal. A Colorado man was sentenced to twelve to eighteen months in prison by a Nebraska judge for possession of marijuana. He had legally purchased the marijuana from a dispensary in Colorado, but was in violation of the law when he crossed into Nebraska.12 It is also illegal to bring marijuana onto an airplane, and it cannot be sent to a patient via mail.
What other laws are there regarding marijuana?With the increase in the number of states with legal medical and recreational marijuana use, a major concern is the safety of residents. People using marijuana are more likely to have a traffi c accident.13 In response, many states have enacted laws regarding driving while under the infl uence of drugs (DUID). Th ere are two schools of thought when it comes to DUID laws, per se and measurable.
Eighteen states have per se DUID laws.14 Th is means any driver testing positive for tetrahydrocannabinol (THC) is automatically charged with impaired driving. THC is one of the main components of marijuana and is responsible for many of its psychoactive eff ects, but THC levels alone do not tell the whole story. Th ere is a lack of studies showing how THC levels and level of impairment defi nitively correlate with each other. Th e United States Department of Justice has
Th e Nebraska Mortar & Pestle 29
JulAug14WorkingCopy.indd 29 8/21/2014 6:17:10 PM

even noted that a positive drug test cannot determine the degree of impairment.15
Marijuana used for research studies is produced at only one federally controlled facility at the University of Mississippi. Th e process to obtain marijuana from this site is lengthy; therefore, very few researchers undergo this type of study. THC is rapidly metabolized to a number of metabolites, the major one is carboxy-THC. THC and its metabolites are lipid-soluble leading to a very long elimination half-life. While the impairing eff ects of THC may last a few hours, THC metabolites can be measured in a person’s urine for up to fourteen days.16 A heavy marijuana user can test positive for THC metabolites for up to ten months after ceasing marijuana use.
In order to address the issues brought up by the per se laws, some states have adopted measurable DUID laws. Th ese laws set a specifi c level of allowable THC in the blood before assuming impairment. Th e accepted level for THC impairment is 5 ng/ml. In Colorado, a person who fails a roadside drug test can take a fi eld sobriety test to show a lack of impairment. In Washington, the allowable level of THC is only valid for persons over the age of twenty-one. Minors in the state can have their driver’s license revoked for having any level of measurable THC in their blood.17
Many law enforcement agencies test blood for THC. Th is is invasive for the driver, inconvenient for the offi cer, and a potential route for transmission of blood-borne pathogens. One company has developed a product to test saliva for the presence of THC. It does not produce an actual level, just a positive or negative depending on if salivary THC levels exceed 25 ng/ml. Th e saliva test can tell if a person has recently smoked marijuana, but cannot determine the frequency of use or level of impairment.18 It also cannot provide an accurate result for non-smoked cannabis products.
It is important to note that many non-THC products can produce a false-positive on a drug test. Some proton-pump inhibitors, like rabeprazole and pantoprazole, can cause a positive result for THC.19 Some NSAIDs like ibuprofen, naproxen, and ketoprofen, can lead to false-positives. Vitamin B2, or ribofl avin,
can cause a false-positive test. Not all false-positives come from oral medications. Some soaps and shampoos have ingredients that can also cause false-positive tests.20
Business Aspects of Medical MarijuanaFollowing state regulationsStates have varied regulations for marijuana dispensaries. Applications to open a dispensary are lengthy and the cost for fees and legal work are expensive.21 A full overview of the legal obligations is beyond the scope of this lesson, but a brief snapshot of the law is important to understand the challenges that states are facing.
Fifteen of the twenty-three states with medical marijuana laws allow for dispensaries or other physical locations outside the home where marijuana can be grown and/or purchased. Half of these states allow dispensaries to be for-profi t, while the other half require dispensaries to be not-for-profi t organizations. New Jersey requires the fi rst six dispensaries in the state to be not-for-profi t, but after that owners may decide to be either for profi t or not-for-profi t. California does not allow retail dispensaries, but does allow collectives. A collective is a facility that cultivates and processes marijuana and is owned and operated by a group of medical marijuana patients. Th e marijuana produced is only available to members of that collective and cannot be sold to the public.22 Washington is unique in that there are regulations in place for the management of recreational marijuana facilities, but dispensaries are not addressed in the medical marijuana laws.
Several states that have more recently legalized medical marijuana have taken additional steps to legitimize the medical aspect of the laws by requiring medical professionals to take part in the dispensaries. Arizona requires all dispensaries to appoint a medical director. Although this physician is not part of the day-to-day operations of the dispensary, they provide training and information to the employees and patients of Arizona dispensaries. Connecticut, which approved its medical marijuana bill in 2012, requires a pharmacist to be the owner of the licensed dispensary.23
Dispensaries are also required to
maintain an extensive security system in the facility. Th is includes video surveillance, physical security such as safes, and security personnel. Owners and employees of dispensaries must also be over twenty-one, have no felony convictions, and undergo fi ngerprinting and a background check.
Banking and professional considerationsSince California passed the fi rst medical marijuana law in 1996, dispensaries have operated as a cash only business. Due to federal banking laws, money from drug sales could be construed as money laundering and could result in civil and criminal actions being taken against the bank and its employees. Also, dispensaries do not qualify for a merchant account to accept credit cards. In 2014, the Department of Justice and Department of Treasury issued a set of guidelines telling banks they would not be prosecuted by providing services to establishments which sell legalized marijuana.24 However, both Departments fell short of off ering immunity for banks who do so. In July 2014, the House of Representatives voted to allow banks to provide traditional banking services to marijuana businesses that are legal under state law (H.R. 5016).
It is important for healthcare professionals to understand that their current malpractice insurance may not cover cases where medical marijuana was recommended or dispensed. Some policies cover the policyholder when the treatment has been approved by the FDA, while others specifi cally exempt cases which involve marijuana. It is necessary for both physicians and pharmacists involved in medical marijuana to ensure that their policy addresses these issues.
Economic considerationsOne of the major selling points for states to legalize marijuana has been the additional revenue from the taxation of the production and sale of marijuana products. Many states have had modest increases to their revenues. New Mexico collected a little over $650,000 from sales tax on medical marijuana in 2012, while Maine’s medical marijuana program produced a $400,000 surplus for the state. Other states have seen a greater impact from legalizing medical marijuana.
Continuing Pharmacy Education Lesson #11
30 July/August 2014 www.npharm.org
JulAug14WorkingCopy.indd 30 8/21/2014 6:17:10 PM

Arizona, whose medical marijuana program was passed in 2010, generated over $5.5 million before a single retail establishment opened.25 Arizona is expecting to generate over $140 million in revenue from the medical marijuana industry, with 6.6% of that passing along to the state in the form of sales tax.
Th e economic impact in the states with legalized recreational use are even greater. Before legalizing cannabis use for adults over the age of twenty-one, Colorado was generating approximately $6 million in sales tax and $35 million annually in licensing fees. Since legalizing recreational marijuana, Colorado generated nearly $12 million in sales tax and close to $30 million overall in the fi rst quarter of 2014.26
Washington has predicted an even greater fi nancial windfall from its marijuana policies. Washington charges a 25% excise tax on all marijuana produced, processed, and sold at retail stores in addition to local and state sales taxes. Th is is estimated to bring in over $400 million for the state of Washington.27
In addition to extra revenue from licensing and taxes, states benefi t from job creation from these industries. Th ere are an estimated ten thousand people directly involved in marijuana businesses in Colorado alone, although it is not clear how many are associated with the medical or recreational side of the business. In Arizona, which only allows medical marijuana, an estimated fi fteen hundred jobs will be created.
Potential Drawbacks Surrounding the Use of MarijuanaImpact on crime ratesIn 2007, the Offi ce for the National Drug Control Policy (ONDCP) released a report which noted that although marijuana use among teens is down 25% over the previous fi ve years, teens who use marijuana are fi ve times more likely to steal than teens who abstain from marijuana.28 Th is information was based on a questionnaire undertaken by the Substance Abuse and Mental Health Services Administration (SAMHSA) in 1992. Th e SAMHSA report went on to state the results do not establish a causal
link between illicit drug use and criminal behaviors.
Th e Community of Anti-Drug Coalitions of America (CADCA) off ered a similar report. During the 2005-2006 school year, high school students who carried weapons onto school property, were injured by weapons at school, or involved in a serious fi ght at school, had high percentages of concomitant marijuana use.29 Th ey also stopped short of claiming causality, but did show a strong correlation between violence at school and drug use in teens.
Th ere are, however, confl icting reports regarding this correlation between marijuana use and crime rates. Researchers at the University of Texas – Dallas tracked crime data from the FBI Uniform Crime Report and socioeconomic data from the Bureau of Labor Statistics, Bureau of Economic Analysis, and the Census Bureau from the time medical marijuana was fi rst approved in 1996 through 2006. Th ey were unable to show that legalization of medical marijuana had any eff ect on homicide, rape, robbery, assault, burglary, larceny, or auto theft. In fact, two types of violent crime, homicide and assault, decreased at rates greater than would be expected.30
Colorado, which approved the legal consumption of marijuana for recreational purposes, reported a decrease of 14.6% in property crimes and a decrease in violent crimes by 2.4% over the same period in 2013. Th is result more closely aligns with current medical thinking, which notes cannabis reduces the likelihood of violence during intoxication due to THC, which can cause a decrease in aggressive and violent behaviors.
One type of delinquent activity that has increased since the legalization of marijuana for medical and recreational purposes is driving while under the infl uence of drugs. In 1999, a cannabinoid was present in the blood of 57.9 out of every 1,000 traffi c fatalities. By 2010, 116.9 out of every 1,000 traffi c fatalities tested positive for marijuana.31
Another area of concern was the potential for robberies at marijuana dispensaries due to having large quantities of both marijuana and cash on their premises. In 2009, the Los Angeles Police Department
reported a total of forty-seven robberies reported out of the 800 area dispensaries. Th e area’s 350 banks were robbed a total of seventy-one times over the same period, a rate of nearly twice that of dispensaries.32 Multiple reports from Denver, Colorado Springs, and Sacramento had the same results. Area dispensaries were victims of crime at a lower rate than banks and liquor stores.
Other potential drawbacks to medical marijuanaOne potential area for concern regarding legalized marijuana is the increased number of home fi res caused by the manufacturing of hash oil. Th e process, which involves using butane to extract THC from dried marijuana clippings, has resulted in ten cases of severe burns in the fi rst three months and a dozen home fi res. Th e state of Colorado has only had twelve cases of serious hash oil related burns in the past two years.
A fi nal area of potential confl ict involves the children of parents who use medical or recreational marijuana in states where it is legal. A handful of cases have emerged where Child Protective Services (CPS) has taken custody of children from parents who use medical marijuana in states where it is legal. Some states, such as Illinois and New Hampshire, have specifi cally addressed this matter, putting addendums into law stating the usage of medical marijuana should not be used against a parent in cases of child custody. Th ese provisions are not uniformly applied as some CPS agents are either unaware of the law or decide the danger to the child posed by the presence of marijuana outweighs the legal protections under the law.33
ConclusionAs more states continue to legalize marijuana for medical and recreational purposes, health care professionals should understand the myriad of legal and practical issues surrounding the implementation of these laws. Lacking federal approval of cannabis as a medicinal agent, each state has developed their own unique set of laws regarding the production, dispensing, and use of marijuana and marijuana-containing
Continuing Pharmacy Education Lesson #11
Th e Nebraska Mortar & Pestle 31
JulAug14WorkingCopy.indd 31 8/21/2014 6:17:10 PM

Continuing Pharmacy Education Lesson #11
products. It is important for health care providers to familiarize themselves with the laws in their state so they can provide accurate and timely information for their patients who may have questions. For health care providers in states without medical marijuana laws, it is equally important to understand both the fi nancial and sociological impacts medical marijuana laws have had in other states in order to make an informed decision when legislation is introduced in those states. With the number of states passing medical marijuana laws increasing, it is only a matter of time before pharmacists come face-to-face with these issues.
References1. New York to be next state to allow medical marijuana. Cable News Network. www.cnn.com/2014/06/20/health/new-york-medical-marijuana. Published June 21 2014. Accessed July 01, 2014.2. Marijuana Decriminalization in U.S. Capital Passes Council. Bloomberg. www.bloomberg.com/news/2014-03-04/marijuana-decriminalization-in-u-s-capital-passed-by-city-1-.html. Published March 04 2014. Accessed July 01, 2014.3. U.S. Department of Justice (DOJ). Attorney General Announces Formal Medical Marijuana Guidelines. www.justice.gov/opa/pr/2009/October/09-ag-1119.html. October 19, 2009. Accessed July 01, 2014.4. DOJ. Justice Department Announces Update to Marijuana Enforcement Policy. www.justice.gov/opa/pr/2013/August/13-opa-974.html. August 29, 2013. Accessed July 01, 2014.5. Hanson, K. State Medical Marijuana Laws. National Conference of State Legislatures. www.ncsl.org/research/health/state-medical-marijuana-laws.aspx. June 27, 2014. Accessed July 01, 2014.6. Conant v. Walters. 309 F.3d 629 (9th Cir October 29, 2002).7. Ferner, M. Veterans Still Can't Discuss Medical Marijuana With Th eir VA Doctors. Th e Huffi ngton Post. www.huffi ngtonpost.com/2014/05/01/veterans-medical-marijuana_n_5244565.html. May 01, 2014. Accessed July 01, 2014.8. Marijuana Policy Project (MPP). State-by-state medical marijuana laws 2013. www.mpp.org/assets/pdfs/library/State-by-State-Laws-Report-2013.pdf. Accessed July 01, 2014.9. U.S. Drug Enforcement Administration. Questions & Answers - State Prescription Drug Monitoring Programs. www.deadiversion.usdoj.gov/faq/rx_monitor.htm. October 2011. Accessed July 01, 2014.10. N.H. Rev. Stat. Ann. § HB573-FN: 126W (2013). Use of Cannabis For Th erapeutic Purposes. 11. Sullum, J. Colorado Couple To Open First Offi cially Approved Cannabis Café. Forbes. www.forbes.com/sites/jacobsullum/2014/03/11/colorado-couple-to-open-fi rst-offi cially-approved-cannabis-club. March 11, 2014. Accessed July 01, 2014.12. Coloradoan gets time for medical marijuana in his trunk. Lincoln Journal-Star. journalstar.com/news/local/911/coloradoan-gets-time-for-medical-marijuana-in-his-trunk/article_e79c814b-cd48-589f-9f24-ca519b15746c.html. Published July 01, 2014. Accessed July 01, 2014. 13. Ramaekers J, Berghaus G, Laar M, Drummer O. Dose Related Risk of Motor Vehicle Crashes after Cannabis Use. Drug and Alcohol Dependence 73.2 (2004): 109-19.
14. Governors Highway Safety Association. State Drug Impaired Driving Laws. www.ghsa.org/html/stateinfo/laws/dre_perse_laws.html. July 01, 2014. Accessed July 01, 2014.15. DOJ. Fact Sheet: Drug Testing in the Criminal Justice System. www.ncjrs.gov/pdffi les/dtest.pdf. March 1992. Accessed 01 July 2014.16. Gustafson R, Levine B, Stout P, et al. Urinary Cannabinoid Detection Times after Controlled Oral Administration of Δ9-Tetrahydrocannabinol to Humans. Clinical Chemistry 49.7 (2003): 1114-124.17. Wash. Rev. Code § 46.20.3101 (2012). Implied consent — License sanctions, length of.18. THC Saliva Test (marijuana only). NarcoCheck. www.narcocheck.com/en/saliva-drug-tests/thc-marijuana-saliva-test.html. Accessed July 01, 2014. 19. Protonix [package insert]. Philadelphia, PA: Wyeth Pharmaceuticals Inc. 2012.20. Derewicz M. Researchers Uncover Reason for False-positive Marijuana Tests in Babies. Th e University of North Carolina at Chapel Hill Gazette. gazette.unc.edu/2012/08/07/researchers-uncover-reason-for-false-positive-marijuana-tests-in-babies. August 07, 2012. Accessed July 01, 2014. 21. Annear S. Massachusetts Grants First 20 Medical Marijuana Dispensary Licenses. Boston Magazine. www.bostonmagazine.com/news/blog/2014/01/31/massachusetts-medical-marijuana-20-licenses-issued. January 31, 2014. Accessed July 01, 2014. 22. State of California Department of Justice. Guidelines for the Security and Non-Diversion of Marijuana Grown for Medical Use August 2008. www.ag.ca.gov/cms_attachments/press/pdfs/n1601_medicalmarijuanaguidelines.pdf. Accessed July 01, 2014. 23. Conn. Gen. Stat. § 21a-408h (2012). Dispensaries. Licensure. Regulations. Fees.24. Kovaleski S. U.S. Issues Marijuana Guidelines for Banks. Th e New York Times. www.nytimes.com/2014/02/15/us/us-issues-marijuana-guidelines-for-banks.html. February 02, 2014. Accessed July 01, 2014. 25. MPP. State Medical Marijuana Programs’ Financial Information. www.mpp.org/assets/pdfs/library/State-Medical-Marijuana-Programs-Financial-Information.pdf. October 18, 2013. Accessed July 01, 2014. 26. State of Colorado Department of Revenue. Marijuana Taxes, Licenses, and Fees Transfers and Distribution April 2014 Sales Reported in May. www.colorado.gov/cs/Satellite/Revenue-Main/XRM/1251633259746. June 2014. Accessed July 01, 2014. 27. Zamarra L. Modeling Cannabis Businesses and Costs of Legal Compliance Draft. BOTEC Analysis Corporation. lcb.wa.gov/publications/Marijuana/I-502/small_business_impact_statement/botec_white_paper_1.pdf. June 18, 2013. Accessed July 01, 2014.28. National Criminal Justice Reference Service. National Drug Control Strategy. www.ncjrs.gov/pdffi les1/ondcp/216431.pdf. February 2007. Accessed July 01, 2014. 29. Community Anti-Drug Coalitions of America. Th e Relationship Between Alcohol, Drug Use and Violence Among Students. www.cadca.org/fi les/Th e_Inextricable_Link_0.pdf. Accessed July 01, 2014. 30. Morris RG, TenEyck M, Barnes JC, Kovandzic TV (2014) Th e Eff ect of Medical Marijuana Laws on Crime: Evidence from State Panel Data, 1990-2006. PLoS ONE 9(3): e92816. doi: 10.1371/journal.pone.009281631. Rudisill TM, Zhao S, Abate MA, Coben J, Zhu M. Trends in drug use among drivers killed in U.S. traffi c crashes, 1999–2010. Accident Analysis and Prevention. 2014. 70: 178-187. 32. Castro T. LAPD chief: Pot clinics not plagued by crime. Los Angeles Daily News. January 16, 2010. www.dailynews.com/20100117/lapd-chief-pot-clinics-not-plagued-by-crime. Accessed July 01, 2014. 33. Cannabis and custody. Omaha World-Herald. June 16, 2014:4A.
32 July/August 2014 www.npharm.org
Policies for the Nebraska Mortar & Pestle (M&P) continuing pharmacy education lessons and quizzes:
1. M&P Quizzes are valid only for the membership year in which they are published. Quizzes for the 2014 Membership Year must be received by December 8, 2014. Quizzes cannot be carried over to another membership year.
2. If more than three questions are missed, the quiz will be returned. Th e quiz can be resubmitted.
3. CPE transcripts can be printed from NABP e-Profi les at www.nabp.net.
4. CPE credits are submitted to NABP by the 15th of each month. For example, M&P CPE quizzes completed in the month of August 2014, will be sent to NABP e-Profi les before September 15, 2014.
Th e Nebraska Council for Continuing Pharmacy Education (NCCPE) is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education (CPE).Th is CPE home study lesson has been accredited for 1.0 contact hour or 0.10 CEU. UAN #128-000-14-102-H04-P/T. Th is lesson is a knowledge-based CPE activity targeted to pharmacists and pharmacy technicians.
Th e authors and the Nebraska Pharmacists Association disclaim any liability to you or your patients resulting from reliance solely upon the information contained herein.
Quiz Answers may be submitted:1. Online: www.npharm.org
2. Fax: 402-420-1406
3. Email: m&[email protected]
4. Mail: NPA Mortar & Pestle6221 S 58th St, Ste ALincoln, NE 68516
JulAug14WorkingCopy.indd 32 8/21/2014 6:17:10 PM

Continuing Pharmacy Education Quiz #11
Legal and Business Aspects of the Changing Medical Marijuana LandscapeQuiz #11, July/August 2014, ACPE UAN #128-000-14-102-H04-P/T
2014 Quiz #11 - NPA CPE Home Study Answer FormLegal and Business Aspects of the Changing
Medical Marijuana LandscapeUAN #128-000-14-102-H04-P for pharmacists
UAN #128-000-14-102-H04-T for pharmacy technicians1.0 Contact Hour - Knowledge Based CPE Activity
Name ________________________________________________________
Mailing Address _______________________________________________
City/State/Zip _________________________________________________
*NABP e-Profi le # ______________ *Date of Birth (MMDD) _________*Required for ACPE credit.
Circle one (1) Answer:1. a b c d 6. a b c d2. a b c d 7. a b c d3. a b c d 8. a b c d4. a b c d 9. a b c d5. a b c d 10. a b c d
CPE Home Study Evaluation 1. Rate this lesson: (Excellent) 5 4 3 2 1 (Poor)
2. Did this lesson meet each of its objectives? ___ Yes ___ No3. Was the content without commercial bias? ___ Yes ___ No 4. Did the lesson meet your educational/practice needs? ___ Yes ___ No5. Comments/future topics are welcome. ________________________
The deadline for this quiz is December 8, 2014
Keep the TOP portion for your records. Return the BOTTOM portion to the NPA offi ce.Or, take this quiz online at www.npharm.org
1. When was the fi rst state medical marijuana law passed?a. 1979b. 1988c. 1996d. 2001
2. How many states allow the use of marijuana for the treatmentof specifi c medical conditions?
a. 9b. 18c. 23d. 32
3. In some states, which of the following health care providerscan provide a recommendation for medical marijuana?
a. Chiropractorb. Homeopathic physicianc. Optometristd. Pharmacist
4. In most states, which of the following is a valid disease or condition for a medical marijuana recommendation?
a. Arthritisb. Depressionc. Macular Degenerationd. Multiple Sclerosis
5. Which of the following states allow both medical marijuana dispensaries and home cultivation of marijuana?
a. Connecticutb. Hawaiic. New Jerseyd. Rhode Island
6. Which of the following scenarios is an illegal use of marijuana?a. Consuming a cannabis-infused product in publicb. Smoking marijuana at a dispensaryc. Smoking marijuana inside a private, members-only clubd. Vaporizing marijuana in public
7. What is the level of THC in the blood a person over the age of twenty-one can have in the state of Washington before being considered impaired?
a. 3 ng/mlb. 5 ng/mlc. 8 ng/mld. 10 ng/ml
8. Which of the following medications can lead to a false-positive reading for THC?
a. Lisinoprilb. Metforminc. Pantoprazoled. Simvastatin
9. Which state requires a pharmacist to own a dispensary?a. Connecticutb. Delawarec. Massachusettsd. Oregon
10. Which of the following crimes increased in frequency after legalizing medical marijuana?
a. Assaultb. Driving under the infl uence of drugsc. Homicided. Property crimes
Th e Nebraska Mortar & Pestle 33
JulAug14WorkingCopy.indd 33 8/21/2014 6:17:10 PM

WE ARE.We are the Alliance for Patient Medication Safety (APMS), a federally listed Patient Safety Organization. Our Pharmacy Quality Commitment (PQC) program helps you implement and maintain a continuous quality improvement program that offers strong federal protection for your patient safety data and your quality improvement work. PQC also helps you comply with quality assurance requirements found in network contracts, Medicare Part D, and state regulations. We offer flexible and powerful tools, ongoing training and support to keep your pharmacy running efficiently, and most importantly, to keep your patients safe.
PQC IS BROUGHT TO YOU BY YOUR STATE PHARMACY ASSOCIATION
LEARN MORE:Call toll free (866) 365-7472 or visit www.pqc.net
“I’M ALWAYS WATCHING OUT FOR MY PATIENTS, BUT WHO’S WATCHING OUT FOR ME?”
JulAug14WorkingCopy.indd 34 8/21/2014 6:17:10 PM

The future of quality patient care relies on learning from the success stories and best practices of today
in order to shape the health care system of tomorrow. Six Medicare plans were recently acknowledged by the Pharmacy Quality Alliance (PQA) for excellence in medication safety, based on the Centers for Medicare & Medicaid Services’ (CMS) Star Ratings. Th e Chinese Community Health Plan of California, Humana’s Medicare plan in Illinois, and four Kaiser Permanente regions (California, Colorado, Hawaii and the Mid-Atlantic region) were recognized for their achievement of a 5-star rating on the PQA measures of medication safety and appropriate use that are included in the CMS Star Rating Program for Medicare plans, as well as achievement of at least a 4.5-star summary plan rating. Th e six awardees spoke to the best practices that contribute to their outstanding medication management, and ultimately ensure optimal medication outcomes.
With the advent of new quality incentive structures put in place through federal government programs, health plans and PBMs are becoming increasingly focused on medication use quality. Pharmacists can contribute meaningfully to the quality goals of these organizations as a member of a virtual integrated care team. Of the fi fteen quality measures used by CMS to evaluate Medicare Part D plans in 2014, fi ve relate to medication safety and adherence. Th ese measures account for nearly 50% of a given Part D sponsor’s star rating, and represent a potential impact area for pharmacist intervention. In fact, in a systematic review of interventions to improve adherence to medications for cardiovascular disease and diabetes, Cutrona et al. found that interventions in
a pharmacy conducted by a pharmacist improved medication adherence more than any other professional in any other setting.
Th is represents a tremendous opportunity for pharmacies. But to take advantage of this opportunity, pharmacists must transition their approach from a mindset of quality measurement resistance, to quality measurement engagement. To facilitate this transition to becoming an engaged partner, many community pharmacies are using EQuIPP, the Electronic Quality Improvement Platform for Plans & Pharmacies. EQuIPP is a performance information management platform that provides unbiased, benchmarked data on the quality of medication use to both health plans and community pharmacies. It allows pharmacists at an individual store or corporate level, to see exactly how individual pharmacies are performing on the medication use quality measures that matter to payors.
Th e unique position of pharmacists in the community setting grants enhanced patient access and excellent opportunities for medication management. Pharmacists are increasingly viewed as a key collaborative partner. Managing the quality of medication use is now a recognized component of ensuring optimal care. Collaboration on shared quality targets and goals connects pharmacies to other partners along the care continuum.
Pharmacies are not exempt from quality measurement. Health plans and PBMs are already moving forward with incentive and penalty programs for pharmacies based on quality performance. Pharmacists are an integral part of the solutions to meet payors’ quality needs. Being proactive in this new quality environment is a must.
Moving forward, pharmacists should look to initiate dialogue, establish and nurture relationships, and seek opportunities to deliver point-of-care interventions that drive quality. Payors are not the only health care organizations with quality goals. Other health care organizations have performance measures that they are accountable for that can be directly infl uenced by pharmacists. In addition to making contributions to health plan quality goals, pharmacists can reach out to local Accountable Care Organizations (ACOs), and Patient Centered Medical Homes (PCMHs) to look for collaboration points. Examples of areas that pharmacists can impact include ACO measures of medication reconciliation and infl uenza immunization, or helping them reach quality measure goals related to cholesterol, A1Cs, and blood pressure through appropriate medication management. Of the 33 quality measures a federal Medicare Shared Savings Program ACO has to meet, at least 11 of them can be infl uenced by community pharmacists. Focus should be centralized on interventions that drive specifi c goals; communicating ways in which pharmacists infl uence the safe and eff ective use of medications and reach these goals will lay the foundation for the pharmacist’s role in integrated care teams.
References1. Pharmacy Quality Alliance. PQA Recognizes Six Medicare Plans for Excellence in Medication Use and Safety Based on CMS’ Star Ratings [Press release]. http://pqaalliance.org/im-ages/uploads/fi les/Press%20Release%202014_QualityAward.pdf. Accessed June 30, 2014.2. Cutrona S, Choudhry N, Shrank W, et al. Modes of delivery for interventions to improve cardiovascular medication adher-ence. Th e American Journal Of Managed Care [serial online]. 2010;16(12):929-942. Available from: MEDLINE, Ipswich, MA. Accessed June 30, 2014.3. Center for Medicare and Medicaid Services. ACO Quality Measures. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Downloads/ACO-Shared-Savings-Program-Quality-Measures.pdf. Accessed June 30, 2014.
Critical Member of the Integrated Care Team
Pharmacists as a Critical Memberof the Integrated Care Team
By Samuel Stolpe, PharmD, PQA Director, Quality Strategies; and Maria Scarlatos, PharmD, PQA Executive Fellow
Th e Nebraska Mortar & Pestle 35
JulAug14WorkingCopy.indd 35 8/21/2014 6:17:11 PM

Advance Your CareerIt’s fast easy and free! Register today and explore the opportunities that will take your career to the next level.
Post your Resume AnonymouslySimply post your resume or create an anonymous career profile and employers will contact you directly with new opportunities.
Search Through Premier Job PostingsSearch the many jobs that cater to your field and are not widely available on other career sites.
Receive Job AlertsCreate job alerts based on various criteria and new opportunities will be sent directly to you via email.
Hire qualified job seekersReach qualified candidates that have the experience and expertise to fill your positions.
Save time and moneyAbility to single out candidates that specialize in your field and advertise positions to them at a fraction of what it costs on other job boards.
Post multiple positionsFrom one posting package to unlimited access, there are many options available to assist you in your recruitment.
Receive resume alerts Create resume alerts based on various criteria and qualified candidates will be sent directly to you via email.
job seeker employer
CAREER CENTERSearching for a job or looking to fill a position?
Visit theCareer Center today!
With easy to use search tools the Nebraska Pharmacists
Association Career Center is a #1 source for job seekers
to find opportunities to help them advance their careers.
Employers will also find that the
Career Center provides the
resources needed to
make their recruitment
more efficient and
successful.
www.npharm.org
For more information, visit us online at www.npharm.org
JulAug14WorkingCopy.indd 36 8/21/2014 6:17:11 PM

Th is CPE lesson was written by Justin Lane, PharmD Candidate, University of Nebraska Medical Center College of Pharmacy, who has no fi nancial or confl ict of interest disclosures. Th is lesson does include a discussion of unlabeled or investigational use of a product(s) that has not yet been approved by the FDA for the use being presented.
Continuing Pharmacy Education Lesson #12
Th e Pharmacology of Medical Marijuana
ObjectivesAt the conclusion of this lesson, pharmacists should be able to:1. Explain the mechanism of action of marijuana and relate it to conditions it may treat.2. Identify general dosing guidelines and the diff erent formulations of marijuana.3. Defi ne the possible indications (FDA approved and non-FDA approved) for the uses of medical marijuana.4. Examine potential side eff ects from marijuana treatment.5. Identify what key facts pharmacists should relay to patients in the traditional pharmacist-patient relationship.
IntroductionIn the last several years the legalization of medical marijuana has been hotly debated. As of July 2014, twenty-three states and the District of Columbia have introduced medical marijuana laws, and over half of these have enacted laws within the last fi ve years.1 As a pharmacist, it is important to be knowledgeable about this medicinal agent in order to educate patients in the best way possible. Pharmacists may become responsible for the safe dispensing of marijuana should it ever become legal in Nebraska, and patients should feel comfortable discussing marijuana with health care providers.
Mechanism of ActionHow marijuana eff ects the body is not completely understood. Although the eff ects are complex, several components
have been identifi ed that have pharmacological activity. Th ere are over 400 diff erent compounds in the Cannabis sativa plant, the plant from which marijuana is derived. Most drugs have one chemical entity contributing to its eff ect; however, marijuana has multiple chemical entities contributing to its eff ect. Th e group of compounds in marijuana thought to contribute to its mechanism of action are called cannabinoids. It is possible that approximately 60 to 70 cannabinoids are present in marijuana. Cannabinoids are extremely lipophilic and produce a variety of pharmacological eff ects. Th e lipophilic property of cannabinoids allows them to cross the blood brain barrier and exert their eff ects on the central nervous system (CNS). Th e three most abundant cannabinoids in marijuana are delta-9-tetrahydrocannabinol (THC), cannabidiol (CBD), and cannabiol. Th e concentration of THC is highest in the fl owers and leaves of the plant, and lowest in the roots, stems, and seeds.2 THC has been proven to be one of the constituents responsible for the psychoactive properties of marijuana.3
CBD has been shown to be non-psychoactive and may reduce the psychotropic side eff ects of THC.4 CBD has anticonvulsant properties in animal models, but data in human models is sparse. CBD has shown both neuro-protective and anti-infl ammatory properties. Th ere have been many case reports claiming that mixtures containing both CBD and THC are eff ective in treating epilepsy, but randomized, double-blinded, controlled
trials are lacking. Spasticity related to multiple sclerosis and cancer pain are two other indications pharmaceutical companies are interested in utilizing mixtures of CBD and THC.5
Like many other agents in medicine, cannabinoids act through activation of receptors in both the central and peripheral nervous system. Th ese receptors are named CB1 and CB2. CB1 receptors are more prevalent in the CNS, while CB2 receptors are more prevalent in the periphery. THC is a partial CB1 agonist with limited CB2 activity. Th e resulting pharmacological action these receptors create depends on where they are located in the brain and how tightly the cannabinoids bind to the receptor. Synthetic cannabinoids including “K2” or “spice” can bind to CB1 receptors more tightly than THC causing intense psychoactive eff ects. CB1 receptors in the basal ganglia of the brain are extremely dense and contribute to dyskinesia, while CB1 receptors in other locations of the brain can induce dopamine release. Th e release of dopamine is responsible for triggering the reward pathway in the human brain and may possibly contribute to marijuana addiction.3
According to the DSM-IV guidelines, 9% of those who use marijuana will become addicted. Th is number increases to 1 in 6 (16%) among those who begin smoking marijuana as teenagers and further increases to 25-50% in people who use marijuana daily.6 Th ere is evidence of withdrawal syndrome in people who quit
Th e Nebraska Mortar & Pestle 37
JulAug14WorkingCopy.indd 37 8/21/2014 6:17:12 PM

using marijuana. Symptoms of marijuana withdrawal include irritability, sleeping diffi culties, dysphoria, craving, and anxiety.3 Th ese withdrawal symptoms likely contribute to the addiction potential of marijuana.
Th ere are various other mechanisms through which THC may exert eff ects on the human body. THC can interact with cell wall lipids and eff ect prostaglandin biosynthesis, decreasing infl ammation. Reducing the production of prostaglandins may decrease pain in patients who use marijuana. Marijuana can also stimulate opiate receptors in the forebrain. Th ese receptors may explain its eff ect on reducing chemotherapy-induced nausea and vomiting as stimulation of opiate receptors leads to direct inhibition of the emetic center in the brain.2
Potential IndicationsBecause marijuana is a Schedule I controlled substance, research on marijuana in the United States is challenging. Th ere are various studies cited in the next few paragraphs; however, it should be noted that this lesson is not a complete review of all studies conducted on marijuana. Th e studies cited here were selected because their conclusions represent the majority of studies performed. With all of these indications, there are studies that both support and disprove the effi cacy of marijuana. Most indications do not have large, high-quality studies supporting marijuana’s safety and effi cacy.
Cancer-induced nausea and vomitingDronabinol, which contains synthetic THC, is currently FDA approved for the treatment of chemotherapy-induced nausea and vomiting (CINV) refractory to other agents. Th e American Society of Clinical Oncologists recommends that cannabinoids should be reserved for patients who are intolerant or refractory to fi rst-line therapy.3 First-line therapy currently includes 5-HT3 serotonin receptor antagonists, NK1 inhibitors including aprepitant or fosaprepitant, and dexamethasone.7
A study published in 2001 concluded that dronabinol was more eff ective than conventional anti-emetics which included prochlorperazine, and metoclopramide at controlling acute CINV.8 In another study, dronabinol was found not to be superior to ondansetron in controlling chronic CINV following highly emetogenic chemotherapy. Nausea intensity and vomiting/retching were actually lower in patients treated with dronabinol, but there was not a large enough diff erence for statistical signifi cance.9 Th e study only included a small sample size of 61 patients making it underpowered to fi nd any diff erence between the two treatments. Some evidence also suggests dronabinol may be more eff ective in treating nausea and vomiting in certain age populations including children.5
Th e inhaled form of marijuana has not been studied as in depth as the oral form for CINV. One open-label study from 1988 suggested inhaled cannabis was eff ective in 78% of 56 patients whose CINV could not be controlled by conventional measures.10 Th is study was conducted prior to the introduction of 5-HT3 antagonists in the last decade. Overall, the majority of evidence shows dronabinol is eff ective for treating nausea and vomiting associated with chemotherapy. Th e oral route is the formulation most studied and is a legitimate indication for the use of medical marijuana.
HIV/AIDS and cancer cachexiaDronabinol is also FDA approved for cachexia associated with HIV/AIDS or cancer. Most of the positive data for this indication have been obtained from patient surveys. Increases in appetite are self-reported and have not been demonstrated in many clinical trials. One of the major clinical trials was done in 2006 by the Cannabis-In-Cachexia-Study-Group. Th is trial compared the eff ects of cannabis extract (2.5 mg of THC, 1 mg of cannabidiol), 2.5 mg of THC, and placebo on appetite and quality of life in patients demonstrating cachexia related to cancer. 243 patients were randomly assigned to the three arms and no statistically signifi cant diff erences
in patients’ appetite or quality of life were found between any of the arms. It is worth noting that there was a signifi cant placebo eff ect that occurred during this study. 69% of patients reported an increase in appetite with placebo alone. Th is compared with 73% and 58% of patients reporting an increase in appetite with cannabis extract and THC, respectively.11
Th ere are a few clinical studies showing dronabinol is eff ective for cachexia. Beal et al performed a randomized clinical trial in 139 patients comparing dronabinol 2.5 mg twice daily vs. placebo. Dronabinol was associated with an increased appetite over baseline vs. placebo (38% vs. 8% P=0.015) and increased weight gain vs. placebo (22% vs. 10.5% gained > 2 kg). Th is study concluded that dronabinol was safe and eff ective for anorexia associated with weight loss in patients with AIDS.12
Th e clinical trial data for weight loss in patients with AIDS are confl icting, but there seems to be a connection between cannabinoid receptors and appetite stimulation. A CB1 antagonist, rimonabant, was available in Europe for the treatment of obesity and type 2 diabetes mellitus in 2006. Several studies confi rmed the effi cacy of rimonabant for both of these indications. Even though the agent appeared to have effi cacy, the use of this agent was suspended in 2008 due to signifi cant psychiatric side eff ects. Th e fact that clinical studies supported that the CB1 antagonist rimonabant was effi cacious for weight loss may suggest cannabinoid agonists are of value for appetite stimulation. Other CB1 antagonists have been tested in trials recently, but side eff ects limit their use. More CB1 antagonists are expected to be investigated in the upcoming years.5
Chronic painClinical trial data regarding the treatment of pain with medical marijuana are confl icting. Since pain can be the result of several diff erent disorders, it is diffi cult for studies to prove which kind of pain marijuana may be eff ective in treating. Patients can have pain due to multiple reasons, which
Continuing Pharmacy Education Lesson #12
38 July/August 2014 www.npharm.org
JulAug14WorkingCopy.indd 38 8/21/2014 6:17:13 PM

Continuing Pharmacy Education Lesson #12
adds complexity to this issue. For example, neuropathic pain, postoperative pain, chronic pain, and cancer pain are just a few diff erent types of pain. It is estimated that 10 mg of THC is roughly equivalent to 60 mg of codeine with respect to analgesic eff ect.5
A study performed in 2003 reviewed THC use in postoperative pain. It was a double-blind, randomized, placebo-controlled study that investigated 40 women undergoing an elective abdominal hysterectomy. Patients were given either 5 mg of THC or placebo two days after surgery when patient-controlled analgesia was discontinued. Th e primary outcome was a summed pain intensity diff erence calculated by a visual analog scale six hours after the study medication was given. Th e study concluded that there was no diff erence in the primary outcome between THC and placebo.13 Other studies have shown a dose-dependent analgesic eff ect in postoperative pain, suggesting the evidence is mixed.
Studies have also been conducted evaluating cannabis use for chronic pain. Ware et al concluded in 2010 that a single inhalation of 25 mg of 9.4% THC three times daily for fi ve days reduced the intensity of pain, improved sleep, and was well tolerated. It should be noted that the study only included 24 patients indicating that the statistical signifi cance is fairly weak.14
One study looked at the use of marijuana in conjunction with opioids for chronic pain. A study in 2011 concluded that vaporized cannabis might augment the analgesic eff ects of opioids. Th is combination is thought to allow lower dosing and decrease side eff ects associated with both agents.15 Cannabinoids have proven to have an analgesic eff ect, but both when and how to use them best has yet to be determined.
Spasticity – multiple sclerosisHigh-quality studies looking at cannabis use to treat spasticity in multiple sclerosis have been performed over the years. With the
evidence being somewhat mixed, the FDA has not approved THC and/or CBD for this use. Th is lesson will review two of the bigger studies examining cannabinoids in treating spasticity due to multiple sclerosis conducted over the last decade.
Th e largest study conducted to evaluate marijuana in treating spasticity is the Cannabinoids in Multiple Sclerosis (CAMS) study. Th is study examined 630 patients from 33 diff erent centers in the United Kingdom. Th ey were randomized to receive THC, oral cannabis extract, or placebo. Th e primary outcome measured was the change in the Ashworth spasticity scale that looked at overall spasticity scores. Th e study concluded that there was no statistically signifi cant diff erence in the primary outcome of spasticity. Although there was no diff erence in the primary outcome, patients tended to feel better. Patients stated an objective diff erence in mobility and improvement in their pain in the treatment groups. Some of the side eff ects associated with the treatment groups included dizziness, light-headedness, dry mouth, diarrhea, constipation, and increased appetite.16
Another large study examining cannabinoid use in multiple sclerosis was performed in 2012. After 2 patients withdrew from the study, 277 patients with stable multiple sclerosis were randomized to oral cannabis extract or placebo. Twenty-two diff erent centers in the United Kingdom were utilized during this study. Th e study was a double-blind, phase III study which included a two week titration phase from 5 mg of THC to a maximum 25 mg of THC daily, followed by a 10-week maintenance phase. Th e majority of patients could tolerate 10 mg to 15 mg of THC daily, with only 24.5% of patients reaching and maintaining the maximum 25 mg dose. Th e study looked at four outcomes with the primary outcome measure being a category rating scale. Th is scale measured patient reported change in muscle stiff ness. Th e other three outcomes were category rating scales that assessed spasms, sleep quality, and body pain.
Th e results from this study were rather encouraging. Relief from muscle stiff ness occurred in twice as many patients taking the cannabis extract compared to placebo (29.4% vs. 15.7% P=0.004). Th e other outcomes studied showed similar effi cacy for cannabis. Like the CAMS study, the drawback to using cannabis for multiple sclerosis is the side eff ects associated with its use. 30 patients (21%) withdrew from the cannabis arm due to adverse eff ects, compared to nine patients (6.7%) in the placebo arm. Th e more common side eff ects seen in the cannabis extract group compared to placebo were dizziness, disturbance in attention, somnolence, dry mouth, GI eff ects, urinary tract infections, and falls. From the data, it appears that cannabis can be effi cacious for spasticity in multiple sclerosis, but the side eff ects can be dose-limiting in some patients.17
GM Pharmaceuticals produces a formulation named Sativex® - a mucosal spray that contains an equal ratio of THC and CBD. Th e product has launched in 11 countries including Spain, Italy, Germany, and the United Kingdom, and approved in another 13 countries. Sativex® is derived from the marijuana plant and is not synthetically created like dronabinol. Sativex® is currently conducting phase III studies in the United States for use with chronic cancer pain; is set to begin studies for use with multiple sclerosis, and has phase I and II studies underway for other indications. Th e metered dose spray allows patients to titrate to desired eff ects and could decrease the consequences associated with smoking marijuana.18 Th ere is some concern regarding abuse with this formulation leading the FDA to include a dose counter to reduce abuse potential.
GlaucomaMost people are aware of marijuana use in treating glaucoma, but surprisingly, there are few studies demonstrating the effi cacy of such treatment. Most of these studies are extremely small in sample size. One of the studies done was uncontrolled, unmasked, nonrandomized, and only included nine patients. Participants were given oral THC
Th e Nebraska Mortar & Pestle 39
JulAug14WorkingCopy.indd 39 8/21/2014 6:17:13 PM

capsules for 1 to 9 months in addition to their previous glaucoma regimen. A decrease in intraocular pressure occurred in all nine patients at the onset of treatment, but by the end of treatment, the response was lost. Patients seemed to develop tolerance and all subjects experienced toxic side eff ects to the treatment. Defi nite conclusions cannot be made from a study of this type, and more studies will be needed to conclude the benefi t of treating glaucoma with marijuana.19
Dravet syndromeDravet syndrome is a severe myoclonic form of epilepsy that begins in infancy and is resistant to current treatment. Children diagnosed with this disorder have a poor prognosis, as they are at increased risk for sudden unexplained death in epilepsy and status epilepticus events. Unfortunately, children do not outgrow this condition, making management of this condition vital.20
CBD has shown to produce anticonvulsant eff ects, and there have been case reports of CBD being eff ective for Dravet syndrome. Unfortunately, no high-quality studies evaluating pure CBD in epilepsy have been completed.21 Th ere are randomized, double-blinded studies planned to assess CBD in treating Dravet syndrome. Th e FDA has recently granted Epidiolex© for fast track designation, which contains only CBD. Th is designation facilitates the drug approval process for drugs that can have an impact on rare, serious disorders with few or no available treatments. Th e company that produces Epidiolex©, GW Pharmaceuticals, is also interested in conducting a clinical development program for Lennox-Gastaut syndrome, another form of severe epilepsy.20
DosingDue to the multiple compounds contributing to marijuana’s pharmacological eff ect, dosing can be challenging. A pharmacist should feel comfortable dispensing medical marijuana only when they are certain the dose of marijuana is accurate and consistent every time. For example, pharmacists would not feel
comfortable dispensing 80 mg of lisinopril when the ordered amount is 10 mg. Large overdoses would lead to signifi cant adverse events. Conversely, giving a patient 5 mg of oxycodone when they are prescribed 20 mg would be unethical and might not treat the patient’s pain adequately.
Th ere is a silver lining with dosing medical marijuana. A few studies have concluded that the chance of overdosing on marijuana leading to death is extremely unlikely. A cohort of over 65,000 marijuana users was examined and there was no increase in mortality associated with cannabis use on an average 10-year follow-up. Th is does not mean that marijuana intoxication cannot lead to death by driving under the infl uence or other mechanisms secondary to intoxication, but it is thought to be nearly impossible to die from a marijuana overdose.22
To further complicate the dosing of marijuana, there are multiple ways for administration. Marijuana can be smoked, vaporized, eaten in various foods, applied topically or taken orally through oils and tinctures. Dosing can vary depending on the strain of marijuana used and the route of administration. Th ere have been attempts to standardize the dose of THC in diff erent strains of marijuana. Low doses are considered below 7 mg, medium doses between 7 mg and 18 mg, and high doses over 18 mg. To get the same amount of drug absorbed orally as through an inhalation formulation, a patient may need to ingest three to fi ve times more THC to receive the desired eff ects. Th is type of classifi cation (low, medium, and high) may work well for dosing THC, but sometimes THC is not the main ingredient in a specifi c strain of marijuana or may not be present at all.23
Dosing of marijuana derivativesSince there is signifi cant inter-patient variability with response to cannabinoids, titration of dosing is critical for optimum response to marijuana. For chemotherapy-induced nausea/vomiting, the dose should begin at 5 mg/m2 by mouth 1-3 hours before administration of chemotherapy,
then every 2-4 hours afterwards for a total of 4-6 doses per day. If the initial dose is not eff ective and side eff ects are not evident, the dose can be increased by increments of 2.5 mg/m2, up to a maximum of 15 mg/m2 not to exceed 6 doses per day. Side eff ects are more common at higher dosages.3
As an appetite stimulant, dronabinol should be dosed at 2.5 mg by mouth before lunch and dinner. Similar to CINV, the dose can be increased if more response is desired and side eff ects are absent. Th e dose can be titrated up to a maximum of 20 mg per day in divided doses for CINV.3
Side Eff ectsShort-term eff ectsOverall, marijuana is fairly well tolerated and has a positive side eff ect profi le if administered in low doses. Finding the right dose with minimum side eff ects will be important if marijuana is to be used medically. In many scenarios, side eff ects might not allow patients to titrate up to suffi cient dosages to make marijuana a useful agent. Mild side eff ects associated with marijuana include headache, dry eyes, dry mouth, dizziness, light-headedness, numbness, and cough.5 Th e psychoactive eff ects associated with THC may include anxiety, depression, drowsiness, fatigue, dysphoria, and reduced motor function. Marijuana has an impact on the cardiovascular system as well. Within ten minutes of smoking a marijuana cigarette, heart rate and cardiac output will increase and may last for two to three hours.3
Smoking marijuana can have adverse eff ects on the lungs. Symptoms of chronic bronchitis are common with smoking marijuana including cough, wheezing, increased bronchial secretion, exertional dyspnea, nocturnal awakening, and chest tightness. It has been shown that smoking marijuana can decrease the FEV1/FVC ratio in patients. Some studies suggest that while it may decrease the FEV1/FVC ratio, it does not impact the ratio as severely as tobacco does. Marijuana smoke has several known carcinogens and it is theorized that smoking marijuana can cause secondary
Continuing Pharmacy Education Lesson #12
40 July/August 2014 www.npharm.org
JulAug14WorkingCopy.indd 40 8/21/2014 6:17:13 PM

Continuing Pharmacy Education Lesson #12
malignancies. More evidence is needed as no studies have proven that smoking marijuana causes cancer.3
Long-term eff ectsTh e long-term eff ects that marijuana can have on an individual are not as well documented as the short-term eff ects. Repeated use of THC can lead to tolerance in individuals. Tolerance can happen due to down-regulation or decreased sensitization of the CB1 receptor. Patients can also have withdrawal symptoms from marijuana if discontinued suddenly; however, due to marijuana’s fairly long half-life, withdrawal symptoms are usually not intense and do not require medical intervention.3
Along with tolerance and withdrawal, there is evidence that early and prolonged exposure to cannabinoids is associated with psychotic diseases including schizophrenia. Using marijuana during the adolescent stage increases the risk of inducing psychotic like eff ects in this population. Th ere is a hypothesis stating that the brain is in a crucial time period during adolescence, since it is actively developing and maturing. Th is process may persist into one’s early 20’s. Cannabis may have the ability to disrupt these important development processes and cause signifi cant harm during these years.24
Drug-Herb InteractionsAs with other herbal medications, there are drug interactions with marijuana. THC is metabolized through CYP-450 enzymes, particularly the CYP2C9 and CYP3A4 pathways. Medications with narrow therapeutic windows that are metabolized through these pathways should be monitored closely for adverse events. Examples of these types of medication include anti-retrovirals including NRTIs, NNRTIs, and protease inhibitors. Th e metabolism of these agents may be decreased. Th is interaction may lead to increased side eff ects due to increased levels of drug with concurrent use of marijuana, however, the effi cacy of these compounds will not change. A pharmacist should be mindful of an increased incidence of side eff ects when these agents are used together.3
Another class of agents with signifi cant drug interactions with smoked marijuana includes anti-psychotics. Like smoking cigarettes, there are components within the smoke of marijuana that can induce CYP1A2 enzymes. Th is pathway primarily metabolizes olanzapine and clozapine. Th ere will be a decrease in effi cacy if a patient is on a combination of these agents. Marijuana may also interfere with anti-psychotics from a pharmacodynamic standpoint. Combining marijuana with benzodiazepines, alcohol, or other CNS depressants could lead to synergistic CNS depression, leading to respiratory depression. THC has known psychoactive pharmacologic properties, which may complicate anti-psychotic therapy and control of various psychological conditions.3 Do not initiate medical marijuana in a patient with known psychological conditions, especially anxiety, depression, bipolar disorder, and schizophrenia. Marijuana has shown to exacerbate the symptoms associated with these conditions and there is a poor risk to benefi t ratio in these patients.25
INR should be closely monitored if a patient is taking warfarin and using medical marijuana. Th ere is no experimental evidence examining the interaction between warfarin and marijuana. Th e perceived interaction is mostly theoretical and should not cause great concern. A pharmacist should be aware of the possibility of this interaction and monitor INR accordingly. 26
Patient CounselingExplaining to patients how to titrate marijuana to their desired eff ects is extremely important. When marijuana is inhaled, it takes 2 - 30 minutes to take eff ect. Th is diff ers substantially from when marijuana is administered orally. Marijuana that is ingested orally usually takes 2 - 3 hours to take eff ect. An uninformed marijuana user may eat one brownie or cookie with marijuana in it and not feel any immediate eff ect. Th is could lead the user to ingest multiple doses in a row, leading to unnecessary adverse eff ects if they are not aware of the delayed absorption properties with the oral formulation.23
Pharmacists should also be aware of the euphoric eff ects marijuana can cause. A patient in chronic pain may actually prefer to be in a euphoric state to alleviate pain, but a pharmacist must counsel on the safe use of such a drug. Detecting marijuana in drivers in car accidents is increasing at an alarming rate. Patients should never drive or operate heavy machinery while using any formulation of marijuana. From 2005 to 2009, almost a third of drivers killed in accidents tested positive for non-alcoholic drugs. Th e number one non-alcoholic drug in their system was cannabinol, a metabolite of THC. From 1999 to 2010, the prevalence of cannabinol in drivers killed in car accidents increased from 4.2% to 12.2%.27
Since marijuana has psychoactive properties, patients with schizophrenia or bipolar disorder should never use marijuana. Even if a patient is in relapse, marijuana is unsafe and may have negative consequences on the course of the illness.24 Th is is a situation where pharmacists could be the last barrier between a patient receiving medical marijuana and exacerbating a serious mental condition.
Pharmacists should be aware that for most indications, marijuana may not be as effi cacious as drugs already on the market. Th is is not saying that marijuana has no place in the medical fi eld, but patients should be informed that there is not suffi cient evidence to indicate its eff ectiveness over other available agents. Marijuana may work well in some patients, but may cause signifi cant side eff ects in others. Regulations have been tight in the United States regarding research on marijuana, thereby limiting data. Recently, regulations for researching marijuana seem to be loosening, which will likely allow more studies to be performed in the future. Pharmacists need to stay informed with the current literature regarding the safety and effi cacy of medical marijuana. Th is will allow pharmacists to continue to provide accurate and important information to their patients.
Th e Nebraska Mortar & Pestle 41
JulAug14WorkingCopy.indd 41 8/21/2014 6:17:13 PM

Continuing Pharmacy Education Lesson #12
References1. National Conference of State Legislature. (2014). State medical marijuana laws. Retrieved June 16, 2014, from http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx2. Natural Database Marijuana (2014). Stockton, California: Natural Medicines Comprehensives Database. Retrieved fromhttp://naturaldatabase.therapeuticresearch.com/nd/PrintVersion.aspx?id=947&&AspxAutoDetectCookieSupport=13. Gold Standard, Inc. Medical Marijuana. Clinical Pharmacology [database online]. Available at: http://www.clinicalpharmacology.com. Accessed: July 2, 2014.4. Wade, D. T., Makela, P., Robson, P., House, H., & Bateman, C. (2004). Do cannabis-based medicinal extracts have general or specifi c eff ects on symptoms in multiple sclerosis? A double-blind, randomized, placebo-controlled study on 160 patients. Multiple Sclerosis (Houndmills, Basingstoke, England), 10(4), 434-441. 5. Marijuana, Natural Products Database. Lexicomp. Wolters Kluwer Health, Inc. Hudson, OH. Available at: http://online.lexi.com. Accessed July 2, 2014.6. Volkow, N. D., Baler, R. D., Compton, W. M., & Weiss, S. R. (2014). Adverse health eff ects of marijuana use. Th e New England Journal of Medicine, 370(23), 2219-2227. 7. American Society of Clinical Oncology, Kris, M. G., Hesketh, P. J., Somerfi eld, M. R., Feyer, P., Clark-Snow, R., et al. (2006). American society of clinical oncology guideline for antiemetics in oncology: Update 2006. Journal of Clinical Oncology : Offi cial Journal of the American Society of Clinical Oncology, 24(18), 2932-2947. 8. Tramer, M. R., Carroll, D., Campbell, F. A., Reynolds, D. J., Moore, R. A., & McQuay, H. J. (2001). Cannabinoids for control of chemotherapy induced nausea and vomiting: Quantitative systematic review. BMJ (Clinical Research Ed.), 323(7303), 16-21. 9. Meiri, E., Jhangiani, H., Vredenburgh, J. J., Barbato, L. M., Carter, F. J., Yang, H. M., et al. (2007). Effi cacy of dronabinol alone and in combination with ondansetron versus ondansetron alone for delayed chemotherapy-induced nausea and vomiting. Current Medical Research and Opinion, 23(3), 533-543. 10. Vinciguerra, V., Moore, T., & Brennan, E. (1988). Inhalation marijuana as an antiemetic for cancer chemotherapy. New York State Journal of Medicine, 88(10), 525-527.11. Cannabis-In-Cachexia-Study-Group, Strasser, F., Luftner, D., Possinger, K., Ernst, G., Ruhstaller, T., et al. (2006). Comparison of orally administered cannabis extract and delta-9-tetrahydrocannabinol in treating patients with cancer-related anorexia-cachexia syndrome: A multicenter, phase III, randomized, double-blind, placebo-controlled clinical trial from the cannabis-in-cachexia-study-group. Journal of Clinical Oncology : Offi cial Journal of the American Society of Clinical Oncology, 24(21), 3394-3400. 12. Beal, J. E., Olson, R., Laubenstein, L., Morales, J. O., Bellman, P., Yangco, B., et al. (1995). Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. Journal of Pain and Symptom Management, 10(2), 89-97. 13. Buggy, D. J., Toogood, L., Maric, S., Sharpe, P., Lambert, D. G., & Rowbotham, D. J. (2003). Lack of
analgesic effi cacy of oral delta-9-tetrahydrocannabinol in postoperative pain. Pain, 106(1-2), 169-172. 14. Ware, M. A., Wang, T., Shapiro, S., Robinson, A., Ducruet, T., Huynh, T., et al. (2010). Smoked cannabis for chronic neuropathic pain: A randomized controlled trial. CMAJ : Canadian Medical Association Journal = Journal De l’Association Medicale Canadienne, 182(14), E694-701. 15. Abrams, D. I., Couey, P., Shade, S. B., Kelly, M. E., & Benowitz, N. L. (2011). Cannabinoid-opioid interaction in chronic pain. Clinical Pharmacology and Th erapeutics, 90(6), 844-851. 16. Zajicek, J., Fox, P., Sanders, H., Wright, D., Vickery, J., Nunn, A., et al. (2003). Cannabinoids for treatment of spasticity and other symptoms related to multiple sclerosis (CAMS study): Multicentre randomised placebo-controlled trial. Lancet, 362(9395), 1517-1526. 17. Zajicek, J. P., Hobart, J. C., Slade, A., Barnes, D., Mattison, P. G., & MUSEC Research Group. (2012). Multiple sclerosis and extract of cannabis: Results of the MUSEC trial. Journal of Neurology, Neurosurgery, and Psychiatry, 83(11), 1125-1132. 18. GWPharma. GW Pharmaceuticals. June 2014. Available at http://www.gwpharm.com/default.aspx. Accessed July 2, 201419. Flach, A. J. (2002). Delta-9-tetrahydrocannabinol (THC) in the treatment of end-stage open-angle glaucoma. Transactions of the American Ophthalmological Society, 100, 215-22; discussion 222-4. 20. GWPharma. GW Pharmaceuticals Announces Epidiolex Receives Fast Track Designation From FDA for the Treatment of Dravet Syndrome. June 6, 2014. Available at http://www.gwpharm.com/GW%20Pharmaceuticals%20Announces%20Epidiolex%20Receives%20Fast%20Track%20Designation%20from%20FDA%20for%20the%20Treatment%20of%20Dravet%20Syndrome.aspx. Accessed July 2, 201421. Devinsky, O., Cilio, M. R., Cross, H., Fernandez-Ruiz, J., French, J., Hill, C., et al. (2014). Cannabidiol: Pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders.Epilepsia, 55(6), 791-802.22. Sidney, S. (2003). Comparing cannabis with tobacco--again. BMJ (Clinical Research Ed.), 327(7416), 635-636.23. Sonya, C. (2014). How pharmacists can counsel patients on medical marijuana. Retrieved June 16, 2014, from http://www.pharmacist.com/how-pharmacists-can-counsel-patients-medical-marijuana 24. Radhakrishnan, R., Wilkinson, S. T., & D’Souza, D. C. (2014). Gone to pot - A review of the association between cannabis and psychosis. Frontiers in Psychiatry, 5, 54. 25. Duckworth, K., & Freedman, J. (2013). Marijuana and mental illness. Retrieved June 16, 2014, from http://www.nami.org/Content/NavigationMenu/Hearts_and_Minds/Smoking_Cessation/Marijuana_and_Mental_Illness.htm 26. Ge, B., Zhang, Z., & Zuo, Z. (2014). Updates on the clinical evidenced herb-warfarin interactions. Evidence-Based Complementary and Alternative Medicine: ECAM, 2014, 957362. 27. Brady, J. E., & Li, G. (2014). Trends in alcohol and other drugs detected in fatally injured drivers in the United States, 1999-2010. American Journal of Epidemiology, 179(6), 692-699.
42 July/August 2014 www.npharm.org
Policies for the Nebraska Mortar & Pestle (M&P) continuing pharmacy education lessons and quizzes:
1. M&P Quizzes are valid only for the membership year in which they are published. Quizzes for the 2014 Membership Year must be received by December 8, 2014. Quizzes cannot be carried over to another membership year.
2. If more than three questions are missed, the quiz will be returned. Th e quiz can be resubmitted.
3. CPE transcripts can be printed from NABP e-Profi les at www.nabp.net.
4. CPE credits are submitted to NABP by the 15th of each month. For example, M&P CPE quizzes completed in the month of August 2014, will be sent to NABP e-Profi les before September 15, 2014.
Th e Nebraska Council for Continuing Pharmacy Education (NCCPE) is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education (CPE).Th is CPE home study lesson has been accredited for 1.0 contact hour or 0.10 CEU. UAN #128-000-14-103-H01-P. Th is lesson is a knowledge-based CPE activity targeted to pharmacists.
Th e authors and the Nebraska Pharmacists Association disclaim any liability to you or your patients resulting from reliance solely upon the information contained herein.
Quiz Answers may be submitted:1. Online: www.npharm.org
2. Fax: 402-420-1406
3. Email: m&[email protected]
4. Mail: NPA Mortar & Pestle6221 S 58th St, Ste ALincoln, NE 68516
JulAug14WorkingCopy.indd 42 8/21/2014 6:17:13 PM

Continuing Pharmacy Education Quiz #12
Th e Pharmacology of Medical MarijuanaQuiz #12, July/August 2014, ACPE UAN #128-000-14-103-H01-P
2014 Quiz #12 - NPA CPE Home Study Answer FormTh e Pharmacology of Medical Marijuana
UAN #128-000-14-103-H01-P1.0 Contact Hour - Knowledge Based CPE Activity
Name ________________________________________________________
Mailing Address _______________________________________________
City/State/Zip _________________________________________________
*NABP e-Profi le # ______________ *Date of Birth (MMDD) _________*Required for ACPE credit.
Circle one (1) Answer:1. a b c d 6. a b c d2. a b c d 7. a b c d3. a b c d 8. a b c d4. a b c d 9. a b c d5. a b c d 10. a b c d
CPE Home Study Evaluation 1. Rate this lesson: (Excellent) 5 4 3 2 1 (Poor)
2. Did this lesson meet each of its objectives? ___ Yes ___ No3. Was the content without commercial bias? ___ Yes ___ No 4. Did the lesson meet your educational/practice needs? ___ Yes ___ No5. Comments/future topics are welcome. ________________________
The deadline for this quiz is December 8, 2014
Keep the TOP portion for your records. Return the BOTTOM portion to the NPA offi ce.Or, take this quiz online at www.npharm.org
1. Which cannabinoid is responsible for the psychoactive eff ectsof marijuana?
a. cannabidiolb. cannabiolc. THCd. all of the above
2. What is the proposed mechanism of action for cannabinoids?a. cannabinoid receptor agonist b. cannabinoid receptor antagonistc. serotonin receptor agonistd. serotonin receptor antagonist
3. Which of these would be considered a withdrawal symptomto marijuana?
a. anxietyb. insomniac. irritabilityd. all of the above
4. Which of the following indications is/are FDA approved?a. THC for cachexia associated with HIV/AIDS or cancerb. THC for cancer induced nausea and vomitingc. THC for spasticity associated with multiple sclerosisd. a and b
5. What is the maximum dose of dronabinol when used for CINV?a. 10 mg/m2
b. 15 mg/m2
c. 20 mg/m2
d. 25 mg/m2
6. Which of these conditions can marijuana exacerbate symptoms of?a. CHFb. chronic kidney diseasec. hypotensiond. schizophrenia
7. When used concurrently with marijuana, which drug or class of medications may lead to increased side eff ects due to increased levels of drug?
a. antipsychotics (olanzapine/clozapine)b. barbituratesc. benzodiazepinesd. NNRTI’s
8. Smoking marijuana can induce which CYP enzyme?a. CYP1A2b. CYP2C9c. CYP2C19d. CYP3A4
9. Which antipsychotic may have reduced concentrations when used with marijuana?
a. aripiprazoleb. haloperidolc. olanzapine d. risperidone
10. On average, how long does it take orally ingested marijuana to take eff ect on the body?
a. 30 minutesb. 1 hourc. 2 hoursd. 5 hours
Th e Nebraska Mortar & Pestle 43
JulAug14WorkingCopy.indd 43 8/21/2014 6:17:13 PM
Consider These Important Issues...
• Reality-based valuation is critical to making a sale.• Exposure to the largest pool of buyers increases ability
to get best price.• Chains are not your only option, there are many private
buyers in the market today.• Confidentiality is critical to maintaining value.• There is financing available for qualified buyers of
profitable businesses, including employees and children.• Transaction structure is the key to minimizing taxes
upon sale.• Doing this alone is NOT a good idea.
Don’t leave money on thetable when you transition the ownership of your business.
“Our 14 year track record of successfully completing more than 400independent pharmacy sales speaks for itself.”
1-(877)-360-0095
www.buy-sellapharmacy.com
Completely
confidential!
Your Local Specialist
Larry [email protected]: 1-(847)-949-2477
Return Service Requested
Nebraska Mortar & Pestle6221 S 58th Street, Suite A, Lincoln, Nebraska 68516www.npharm.org ~ 402-420-1500 ~ m&[email protected]
Deliver to NPA Member:
PRSRT STDUS POSTAGE
PAIDPERMIT #586LINCOLN NE
Connect With the NPA
Like us on Facebook at www.facebook.com/NebraskaPharmFollow us on Twitter at www.twitter.com/NebraskaPharmConnect with us on LinkedIn at www.linkedin.com
JulAug14WorkingCopy.indd 44 8/21/2014 6:17:13 PM







![Mortar-Pestle and Microwave Assisted Regioselective ...file.scirp.org/pdf/IJOC20120300015_46985024.pdf · ducting micro wave assisted nitration reactions [35-43]. Microwaves are a](https://static.fdocuments.in/doc/165x107/5b932ade09d3f23a718d4e23/mortar-pestle-and-microwave-assisted-regioselective-filescirporgpdfijoc20120300015.jpg)










