
Nebraska Mortar & Pestle - n Pharm · 3 Daily News Dose - In Case You Missed It ... The Nebraska...
44
3 Daily News Dose - In Case You Missed It 6 2015 NPA Legislative Bill Summary 10 Creighton University School of Pharmacy & Health Professions News 12 Continuing Pharmacy Education Lesson #6 New Options for Disposal of Controlled Substances 21 Rx and e Law - Law vs. Ethics Inside This Issue Inside This Issue Inside This Issue Inside This Issue Nebraska Mortar & Pestle May/June 2015 Volume 78, Number 3 Official Publication of the Nebraska Pharmacists Association For NPA Members 24 Continuing Pharmacy Education Lesson #7 Biosimilars and the Future of Biologicsy 32 University of Nebraska Medical Center College of Pharmacy News 35 Continuing Pharmacy Education Lesson #8 Oral Anticoagulants and Reversal Strategies in Emergent Situationsy 40 Convention Recap & Photo Album Champions and Hosts
Transcript of Nebraska Mortar & Pestle - n Pharm · 3 Daily News Dose - In Case You Missed It ... The Nebraska...
3 Daily News Dose - In Case You Missed It
6 2015 NPA Legislative Bill Summary
10 Creighton University School of Pharmacy & Health Professions News
12 Continuing Pharmacy Education Lesson #6 New Options for Disposal of Controlled Substances
21 Rx and The Law - Law vs. Ethics
Inside This IssueInside This IssueInside This IssueInside This Issue
Nebraska Mortar & PestleMay/June 2015 Volume 78, Number 3Official Publication of the Nebraska Pharmacists Association
For NPA Members
24 Continuing Pharmacy Education Lesson #7 Biosimilars and the Future of Biologicsy
32 University of Nebraska Medical Center College of Pharmacy News
35 Continuing Pharmacy Education Lesson #8 Oral Anticoagulants and Reversal Strategies in Emergent Situationsy
40 Convention Recap & Photo Album
Champions and Hosts
2 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 3
Nebraska Pharmacists Association6221 S 58th St, Suite A, Lincoln, Nebraska 68516phone 402.420.1500 • fax 402.420.1406email m&[email protected] • website www.npharm.org
Board of DirectorsChairman, Firouzan ‘Fred’ Massoomi
President, Jennifer Tilleman
President-Elect, Lyndell White
Treasurer, Kimberlee Ross
Executive Vice President, Joni Cover
District Members Trevor Bertsch Connie Bolte Dana Griess Pam Miller Jeffrey Steffensmeier Nicole White
Pharmacy Technician Elina Pierce
Students Allisha Gabriel, CU Elizabeth Dudley, UNMC
Network Chairs Academia/Specialty Practice: Lori Murante Chain: Kimberlee Ross Hospital/Health-System: Jerome Wohleb Independent: Rick Clabaugh Industry: Stephanie Maciejewski Long-Term Care: Sheryl Havermann
StaffExecutive Vice President, Joni CoverNebraska DUR Director, Marcia MuetingFinance & Marketing Manager, Diane Webb
PublisherThe Nebraska Mortar & Pestle (M&P) (ISSN 0028-1891) is owned and published by the Nebraska Pharmacists Association to provide continuing pharmacy education, drug information, news, and trends in the profession of pharmacy. Opinions expressed by the contributors, whether signed or otherwise, do not necessarily reflect the attitudes of the publisher nor are they responsible for them.
The M&P is published six times a year in February, April, June, August, October and December. The subscription rate for non-members is $50 per year. The managing editor is Joni Cover ([email protected]). Office of publication is 6221 S 58th St, Suite A, Lincoln, NE 68516-3687. Second class postage paid at Lincoln, Nebraska, and at addition mailing offices. Postmaster: Send address changes to Nebraska Mortar & Pestle, 6221 S 58th St, Suite A, Lincoln, NE 68516-3687 or email m&[email protected].
We Hear That
1 Past NPA Board Member, Eric Stevens, RP, La Vista, passed away on April 27, 2015. Eric was a graduate of the University of Nebraska-Lincoln School of Pharmacy. He had retired from Shopko Pharmacy and had served several terms on the NPA Board of Directors. He was a Papillion Volunteer Firefighter, as well as an avid baseball fan and train enthusiast. Our condolences to the Stevens family!
BirthdaysAnniversariesWeddings
GraduationsWe Hear That
Annual ConventionThe 2016 NPA Annual Convention will be held on July 15th and 16th at the Cornhusker Hotel in Lincoln, Nebraska.
Cover Photo2015 Nebraska Mortar Bowl Champions - "The Top 10" team winners and UNMC PharmD Candidates - Brian Dahlke, Ashley Schenk, and Morgan Pusek; and Mortar Bowl Hostess, Jenny Tilleman, PharmD, and Host, Ed DeSimone, PharmD.

2 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 3
Top 10 Drug Disposal Pharmacy LocationsPharmacy Name Location Pounds Collected
Shopko Pharmacy Grand Island 94
Fulmer Pharmacy Holdrege 66
U-Save Pharmacy Northwest Grand Island 65
Kohll's/RxMPSS 5110 L St, Omaha 60
Walgreens Pharmacy 9512 S 71st Plz, Omaha 57
Kohll's Pharmacy and Home Care 2923 Leavenworth, Omaha 41
Hy-Vee Pharmacy 10808 Fort St, Omaha 35
Hy-Vee Pharmacy Papillion 33
Nebraska Medicine Pharmacy Bellevue 31
Hy-Vee Pharmacy 3410 N 156th St, Omaha 31
Daily News Dose
Your NPA member benefits include a daily email with important drug and health information, as well as answers to member questions. Below is a partial list of some of the most recent Daily News Dose items that you may have missed.
Daily News DoseIn Case You Missed It
Certificate of Licensure for Third Party ContractsA Certificate of Nebraska Licensure for facilities or for credentialed individuals can be generated from the Nebraska DHHS website at https://www.nebraska.gov/LISSearch/search.cgi Search for the license, then click on "Generate a certification of this license" at the bottom of the page.
Nebraska Pharmacy Technicians to be Certified by 2017With the passage of LB 37, pharmacy technicians need to be certified by a national or state certifying body by January 1, 2017. If you know of a pharmacy technician who is interested in becoming certified, let them know about the self-study materials that are available from the NPA. Training manuals and calculation workbooks offer an overview of pharmacy practice, human systems, pharmacy interventions, step-by-step math, and much more, to prepare technicians for certification testing.
Controlled Substances InventoryAs a reminder, each DEA registrant manufacturing, distributing or dispensing controlled substances is required to prepare an annual inventory of all stocks of controlled substances on hand within one year of the previous inventory. A copy of the annual inventory record is to be mailed to:
Nebraska Board of PharmacyNebraska Department of Health and Human ServicesDivision of Public Health, Licensure UnitPO Box 94986Lincoln, NE 68509-4986
OR a scanned copy of the annual inventory record can be sent by email to:[email protected]
Statewide Drug Disposal InitiativePharmacies across Nebraska continue to enroll in the statewide expansion of the drug disposal initiative. Pharmacies outside of Lancaster County have collected a total of 1,152 pounds of unwanted medications. Thanks and congratulations to the following pharmacies for collecting medications and being in the "Top 10" from January through April 2015. (See Table above.)
The following communities (with more than 1 pharmacy) have 100% participation of all pharmacies:
• Broken Bow: Holcomb Pharmacy, Shopko Pharmacy, and Varney Health Mart Pharmacy
• Central City: Corner Drug, Litzenberg Memorial County Hospital, and Norm's U-Save Pharmacy
• Falls City: Kex Rx Pharmacy & Home Care and Shopko Pharmacy
• Gothenburg: Gothenburg Discount Pharmacy and Shopko Pharmacy
• Loup City: Good Life Discount Pharmacy and Loup City Rx Shoppe
• Wayne: Shopko Pharmacy and U-Save Pharmacy
CD-10 Toolkit AvailableThe ICD-9 code sets that are currently used to report health care diagnoses and inpatient procedures must be replaced with ICD-10 code sets.
Mandated by law, this change will take place on October 1, 2015. Because ICD-10 will affect coding for everyone covered by the Health Insurance Portability and Accountability Act (HIPAA), it is important that pharmacy professionals are educated about the ICD-10 transition. A toolkit including ICD-10 resources and materials from the Centers for Medicare & Medicaid Services (CMS) has been developed to help the health care industry with the transition to ICD-10. http://www.mcrh.msu.edu/documents/rhc/icd10/resources/icd10regionalofficetoolkit-forexternalpartners20130913.pdf
To order an ICD-10 official code set, go to the NPA website at www.npharm.org for discounted pricing for NPA members.
4 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 5
Daily News Dose
Pictured from left: Back row - Abigail Anderson, MCRP, Program Specialist, Pharmacy Unit; and Jenny Minchow, PharmD, Pharmacy Consultant. Front row - Sharon Gruhn, Staff Assistant II; and Shelly Nickerson, PharmD, RP, Pharmacy Unit Administrator.
New Pharmacy Unit Administrator The NPA welcomes Shelly Nickerson, PharmD, to her new position as the Pharmacy Unit Administrator for the Department of Health and Human Services. Shelly graduated from Nebraska Wesleyan University with a BS in Biology. During her final year at Wesleyan, she worked as a pharmacy technician at a Walgreens pharmacy. She then moved to West Des Moines, Iowa continuing as a pharmacy technician for Walgreens, and in 2004, earned her Doctor of Pharmacy from Drake University.
A position with Walgreens took her to Arizona until family brought her back to Gothenburg in 2006. She worked for an independent pharmacy until she opened a pharmacy for Pamida in 2008. At the end of 2012, she moved to Hanover, New Hampshire to work at the Dartmouth-Hitchcock Medical Center. Her love for the "good life" soon resulted in their return to Nebraska where she worked part-time for the Northern Lights Hy-Vee before becoming the Director of Pharmacy for Gothenburg Memorial Hospital assisting with the implementation of EMR, CPOE, Omnicell, 340B, and epharmacy. Shelly lives in Gretna with her husband raising two children and is looking forward to the additional two she is expecting in August.
Nebraska MPJE ReviewThis is the time of year that new pharmacy graduates are studying for their MPJE. Could you pass the MPJE after all these years? Below are a few sample questions to test your knowledge. Be sure to select all the answers that apply.
1. According to Nebraska Pharmacy Law, which of the following practitioners may prescribe a narcotic Schedule II controlled substance in the course of their professional practices?
a. Physicians assistant b. Nurse Practitioner (APRN-NP) c. Veterinarian d. Optometrist e. Physical therapist
2. Faxing a written, signed, paper prescription for Schedule II controlled drugs may serve as the original prescription in which of the following situations:a. For a patient undergoing home infusion
of a narcotic that has been compounded for a direct parenteral administration
b. For administration to a patient living in a LTCF
c. For a patient in hospice care receiving a narcotic, bearing the words “hospice patient”
d. For a patient picking up medication at a community pharmacy
e. None of the above
3. After verbally consulting with a practitioner, according to the Nebraska Board of Pharmacy, what changes may a pharmacist make to a prescription written for a Schedule II drug?
a. The patient's address b. Directions for use c. The quantity prescribed d. The name of the controlled substance e. The issue date Answers:1. a, b, c and d; 2. a, b, and c; 3. a, b, c and eHow did you do? The recently updated Nebraksa MPJE Review is available for order. See the following page for an order form.
Reporting for the Parkinson Disease RegistgryAccording to Nebraska Revised Statute Section 81-6,103, "the pharmacist in charge of each
pharmacy located within the state or doing business in the state shall file a semiannual report with the department listing persons to whom the pharmacist has dispensed drugs on the list of drugs required to be reported under this section for Parkinson's disease.
The report shall include the name, address, and social security number of the person for whom the drugs were prescribed and the name and address of the prescribing physician. The department shall issue a list of drugs used for the treatment of Parkinson's disease to be reported under this section, shall review and revise the list annually, and shall distribute the list to each pharmacy located within the state or doing business in the state." Visit http://dhhs.ne.gov/publichealth/Pages/ced_parkinsons_forms.aspx for more information, including the reportable list of drugs.
Meeting with Governor RickettsLast month, members of the NPA Board of Directors, including (pictured from left) Connie Bolte, Pam Miller, Dana Griess, Nicole White, Jerome Wohleb, and Ally Strobel (not pictured Rick Clabaugh), along with Joni Cover, NPA Chief Executive Officer, and Marcia Mueting, Nebraska DUR Director, met with Governor Ricketts and members of his staff. The pharmacists role in health care, a prescription drug monitoring program, medical marijuana, health plans sending prescriptions out of Nebraska, and third party issues were some of the items discussed. The Governor was particularly interested to hear about our professions' challenges in rural Nebraska.

4 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 5
Name Date
Address
City State Zip
Phone Email
Are you Ready for the MPJE? Preparing for the Nebraska MPJE is easy with the Nebraska Pharmacists Association’s MPJE Review. Th is study guide addresses the objectives outlined by the National Association of Boards of Pharmacy (NABP). You can review the information at your own pace and assess your learning with the practice questions that are included.
Print $79plus tax
PDF File $49plus tax
To order call:
402.420.1500(Mon-Fri, 9am-4pm CST)
Or mail your order to: NPA6221 S 58th St, Ste ALincoln, NE 68516
What are the duties of a Pharmacist-In-Charge in Nebraska?
Which drugs can be dispensed pursuant to a delegated dispensing permit?
Who is subject to mandatory reporting?
What information can a pharmacist add or change on a CII prescription?
Nebraska MPJE Review
Order your Nebraska MPJE Review!
Check Number
Credit Card Number
Exp. Date / CSC# Signature
Printed CopyAllow 10 - 15 days for processing.
PDF FileLink will be sent to your email.
Allow 3 - 5 days for processing.
(Qty) ___ @ $________
= ____________
Tax + ____________
Total = ________________
Legislative Bill Summary
6 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 7
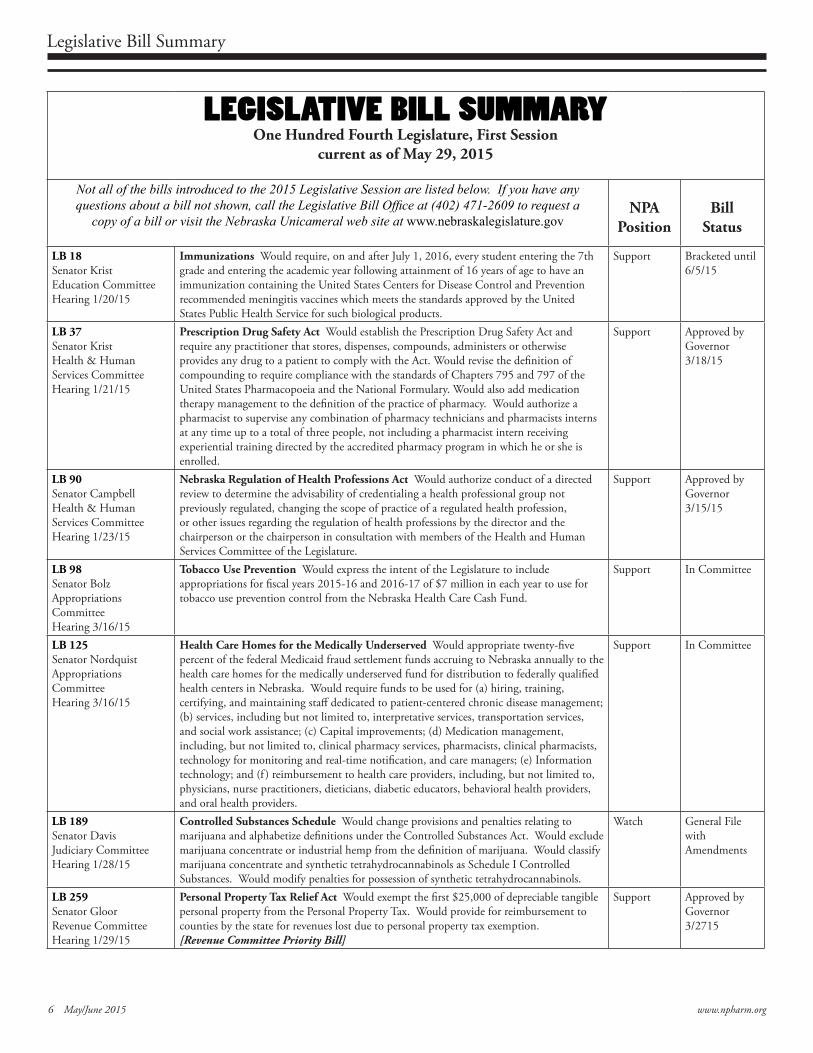
LEGISLATIVE BILL SUMMARYOne Hundred Fourth Legislature, First Session
current as of May 29, 2015
Not all of the bills introduced to the 2015 Legislative Session are listed below. If you have any questions about a bill not shown, call the Legislative Bill Office at (402) 471-2609 to request a
copy of a bill or visit the Nebraska Unicameral web site at www.nebraskalegislature.govNPA
PositionBill
Status
LB 18Senator KristEducation CommitteeHearing 1/20/15
Immunizations Would require, on and after July 1, 2016, every student entering the 7th grade and entering the academic year following attainment of 16 years of age to have an immunization containing the United States Centers for Disease Control and Prevention recommended meningitis vaccines which meets the standards approved by the United States Public Health Service for such biological products.
Support Bracketed until6/5/15
LB 37Senator KristHealth & Human Services CommitteeHearing 1/21/15
Prescription Drug Safety Act Would establish the Prescription Drug Safety Act and require any practitioner that stores, dispenses, compounds, administers or otherwise provides any drug to a patient to comply with the Act. Would revise the definition of compounding to require compliance with the standards of Chapters 795 and 797 of the United States Pharmacopoeia and the National Formulary. Would also add medication therapy management to the definition of the practice of pharmacy. Would authorize a pharmacist to supervise any combination of pharmacy technicians and pharmacists interns at any time up to a total of three people, not including a pharmacist intern receiving experiential training directed by the accredited pharmacy program in which he or she is enrolled.
Support Approved byGovernor3/18/15
LB 90Senator CampbellHealth & Human Services CommitteeHearing 1/23/15
Nebraska Regulation of Health Professions Act Would authorize conduct of a directed review to determine the advisability of credentialing a health professional group not previously regulated, changing the scope of practice of a regulated health profession, or other issues regarding the regulation of health professions by the director and the chairperson or the chairperson in consultation with members of the Health and Human Services Committee of the Legislature.
Support Approved byGovernor3/15/15
LB 98Senator BolzAppropriations CommitteeHearing 3/16/15
Tobacco Use Prevention Would express the intent of the Legislature to include appropriations for fiscal years 2015-16 and 2016-17 of $7 million in each year to use for tobacco use prevention control from the Nebraska Health Care Cash Fund.
Support In Committee
LB 125Senator NordquistAppropriations CommitteeHearing 3/16/15
Health Care Homes for the Medically Underserved Would appropriate twenty-five percent of the federal Medicaid fraud settlement funds accruing to Nebraska annually to the health care homes for the medically underserved fund for distribution to federally qualified health centers in Nebraska. Would require funds to be used for (a) hiring, training, certifying, and maintaining staff dedicated to patient-centered chronic disease management; (b) services, including but not limited to, interpretative services, transportation services, and social work assistance; (c) Capital improvements; (d) Medication management, including, but not limited to, clinical pharmacy services, pharmacists, clinical pharmacists, technology for monitoring and real-time notification, and care managers; (e) Information technology; and (f ) reimbursement to health care providers, including, but not limited to, physicians, nurse practitioners, dieticians, diabetic educators, behavioral health providers, and oral health providers.
Support In Committee
LB 189Senator DavisJudiciary CommitteeHearing 1/28/15
Controlled Substances Schedule Would change provisions and penalties relating to marijuana and alphabetize definitions under the Controlled Substances Act. Would exclude marijuana concentrate or industrial hemp from the definition of marijuana. Would classify marijuana concentrate and synthetic tetrahydrocannabinols as Schedule I Controlled Substances. Would modify penalties for possession of synthetic tetrahydrocannabinols.
Watch General FilewithAmendments
LB 259Senator GloorRevenue CommitteeHearing 1/29/15
Personal Property Tax Relief Act Would exempt the first $25,000 of depreciable tangible personal property from the Personal Property Tax. Would provide for reimbursement to counties by the state for revenues lost due to personal property tax exemption.[Revenue Committee Priority Bill]
Support Approved byGovernor3/2715
Legislative Bill Summary
6 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 7
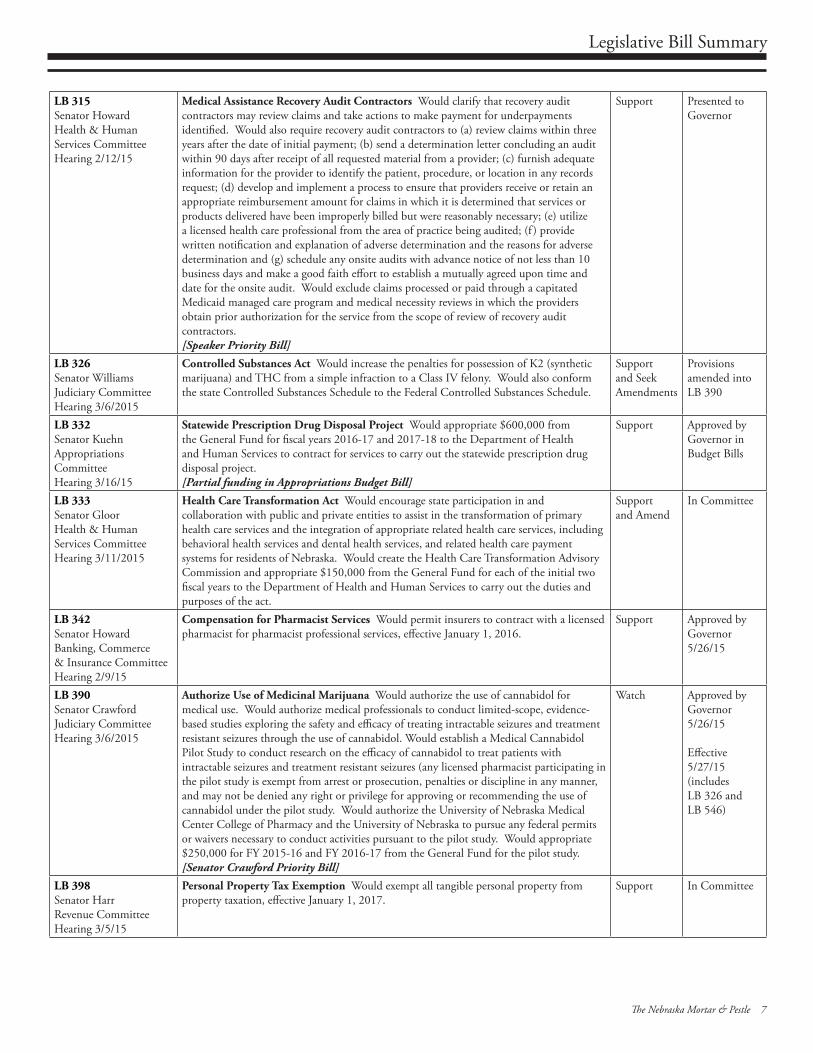
LB 315Senator HowardHealth & Human Services CommitteeHearing 2/12/15
Medical Assistance Recovery Audit Contractors Would clarify that recovery audit contractors may review claims and take actions to make payment for underpayments identified. Would also require recovery audit contractors to (a) review claims within three years after the date of initial payment; (b) send a determination letter concluding an audit within 90 days after receipt of all requested material from a provider; (c) furnish adequate information for the provider to identify the patient, procedure, or location in any records request; (d) develop and implement a process to ensure that providers receive or retain an appropriate reimbursement amount for claims in which it is determined that services or products delivered have been improperly billed but were reasonably necessary; (e) utilize a licensed health care professional from the area of practice being audited; (f ) provide written notification and explanation of adverse determination and the reasons for adverse determination and (g) schedule any onsite audits with advance notice of not less than 10 business days and make a good faith effort to establish a mutually agreed upon time and date for the onsite audit. Would exclude claims processed or paid through a capitated Medicaid managed care program and medical necessity reviews in which the providers obtain prior authorization for the service from the scope of review of recovery audit contractors. [Speaker Priority Bill]
Support Presented toGovernor
LB 326Senator WilliamsJudiciary CommitteeHearing 3/6/2015
Controlled Substances Act Would increase the penalties for possession of K2 (synthetic marijuana) and THC from a simple infraction to a Class IV felony. Would also conform the state Controlled Substances Schedule to the Federal Controlled Substances Schedule.
Supportand SeekAmendments
Provisionsamended intoLB 390
LB 332Senator KuehnAppropriations CommitteeHearing 3/16/15
Statewide Prescription Drug Disposal Project Would appropriate $600,000 from the General Fund for fiscal years 2016-17 and 2017-18 to the Department of Health and Human Services to contract for services to carry out the statewide prescription drug disposal project.[Partial funding in Appropriations Budget Bill]
Support Approved byGovernor inBudget Bills
LB 333Senator GloorHealth & Human Services CommitteeHearing 3/11/2015
Health Care Transformation Act Would encourage state participation in and collaboration with public and private entities to assist in the transformation of primary health care services and the integration of appropriate related health care services, including behavioral health services and dental health services, and related health care payment systems for residents of Nebraska. Would create the Health Care Transformation Advisory Commission and appropriate $150,000 from the General Fund for each of the initial two fiscal years to the Department of Health and Human Services to carry out the duties and purposes of the act.
Supportand Amend
In Committee
LB 342Senator HowardBanking, Commerce& Insurance CommitteeHearing 2/9/15
Compensation for Pharmacist Services Would permit insurers to contract with a licensed pharmacist for pharmacist professional services, effective January 1, 2016.
Support Approved byGovernor5/26/15
LB 390Senator CrawfordJudiciary CommitteeHearing 3/6/2015
Authorize Use of Medicinal Marijuana Would authorize the use of cannabidol for medical use. Would authorize medical professionals to conduct limited-scope, evidence-based studies exploring the safety and efficacy of treating intractable seizures and treatment resistant seizures through the use of cannabidol. Would establish a Medical Cannabidol Pilot Study to conduct research on the efficacy of cannabidol to treat patients with intractable seizures and treatment resistant seizures (any licensed pharmacist participating in the pilot study is exempt from arrest or prosecution, penalties or discipline in any manner, and may not be denied any right or privilege for approving or recommending the use of cannabidol under the pilot study. Would authorize the University of Nebraska Medical Center College of Pharmacy and the University of Nebraska to pursue any federal permits or waivers necessary to conduct activities pursuant to the pilot study. Would appropriate $250,000 for FY 2015-16 and FY 2016-17 from the General Fund for the pilot study.[Senator Crawford Priority Bill]
Watch Approved byGovernor5/26/15
Effective5/27/15(includesLB 326 andLB 546)
LB 398Senator HarrRevenue CommitteeHearing 3/5/15
Personal Property Tax Exemption Would exempt all tangible personal property from property taxation, effective January 1, 2017.
Support In Committee
Legislative Bill Summary
8 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 9
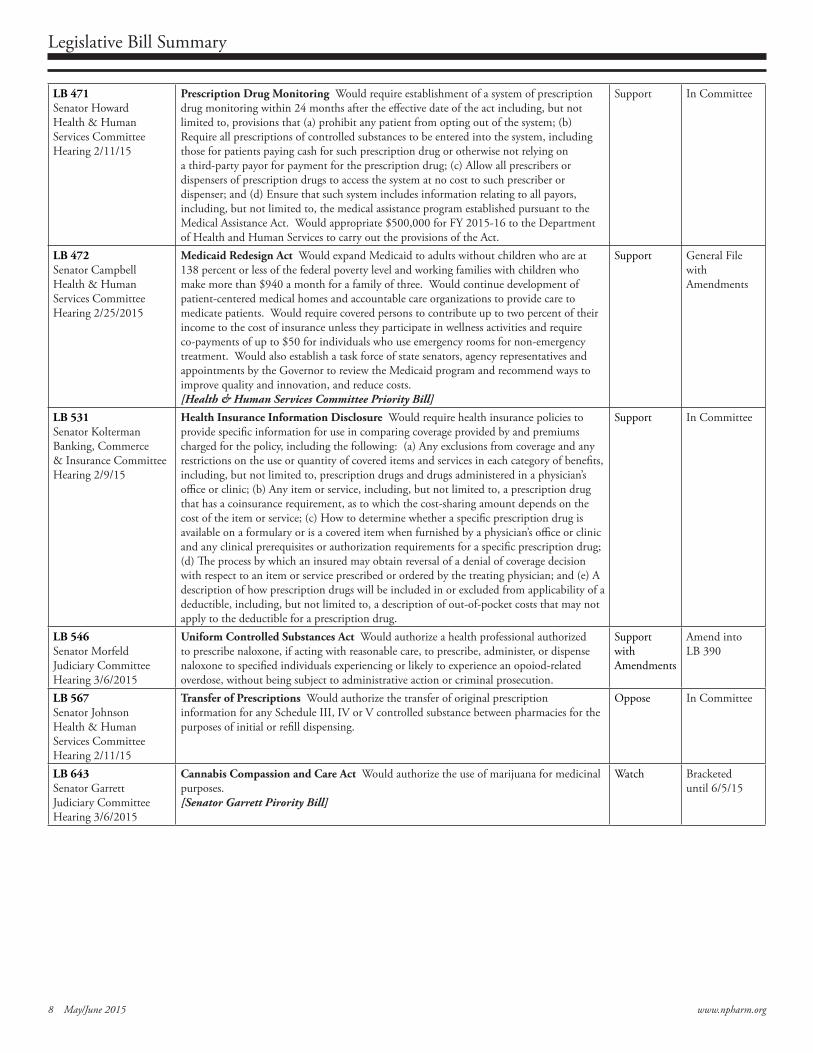
LB 471Senator HowardHealth & Human Services CommitteeHearing 2/11/15
Prescription Drug Monitoring Would require establishment of a system of prescription drug monitoring within 24 months after the effective date of the act including, but not limited to, provisions that (a) prohibit any patient from opting out of the system; (b) Require all prescriptions of controlled substances to be entered into the system, including those for patients paying cash for such prescription drug or otherwise not relying on a third-party payor for payment for the prescription drug; (c) Allow all prescribers or dispensers of prescription drugs to access the system at no cost to such prescriber or dispenser; and (d) Ensure that such system includes information relating to all payors, including, but not limited to, the medical assistance program established pursuant to the Medical Assistance Act. Would appropriate $500,000 for FY 2015-16 to the Department of Health and Human Services to carry out the provisions of the Act.
Support In Committee
LB 472Senator CampbellHealth & Human Services CommitteeHearing 2/25/2015
Medicaid Redesign Act Would expand Medicaid to adults without children who are at 138 percent or less of the federal poverty level and working families with children who make more than $940 a month for a family of three. Would continue development of patient-centered medical homes and accountable care organizations to provide care to medicate patients. Would require covered persons to contribute up to two percent of their income to the cost of insurance unless they participate in wellness activities and require co-payments of up to $50 for individuals who use emergency rooms for non-emergency treatment. Would also establish a task force of state senators, agency representatives and appointments by the Governor to review the Medicaid program and recommend ways to improve quality and innovation, and reduce costs.[Health & Human Services Committee Priority Bill]
Support General FilewithAmendments
LB 531Senator KoltermanBanking, Commerce& Insurance CommitteeHearing 2/9/15
Health Insurance Information Disclosure Would require health insurance policies to provide specific information for use in comparing coverage provided by and premiums charged for the policy, including the following: (a) Any exclusions from coverage and any restrictions on the use or quantity of covered items and services in each category of benefits, including, but not limited to, prescription drugs and drugs administered in a physician’s office or clinic; (b) Any item or service, including, but not limited to, a prescription drug that has a coinsurance requirement, as to which the cost-sharing amount depends on the cost of the item or service; (c) How to determine whether a specific prescription drug is available on a formulary or is a covered item when furnished by a physician’s office or clinic and any clinical prerequisites or authorization requirements for a specific prescription drug; (d) The process by which an insured may obtain reversal of a denial of coverage decision with respect to an item or service prescribed or ordered by the treating physician; and (e) A description of how prescription drugs will be included in or excluded from applicability of a deductible, including, but not limited to, a description of out-of-pocket costs that may not apply to the deductible for a prescription drug.
Support In Committee
LB 546Senator MorfeldJudiciary CommitteeHearing 3/6/2015
Uniform Controlled Substances Act Would authorize a health professional authorized to prescribe naloxone, if acting with reasonable care, to prescribe, administer, or dispense naloxone to specified individuals experiencing or likely to experience an opoiod-related overdose, without being subject to administrative action or criminal prosecution.
SupportwithAmendments
Amend intoLB 390
LB 567Senator JohnsonHealth & Human Services CommitteeHearing 2/11/15
Transfer of Prescriptions Would authorize the transfer of original prescription information for any Schedule III, IV or V controlled substance between pharmacies for the purposes of initial or refill dispensing.
Oppose In Committee
LB 643Senator GarrettJudiciary CommitteeHearing 3/6/2015
Cannabis Compassion and Care Act Would authorize the use of marijuana for medicinal purposes.[Senator Garrett Pirority Bill]
Watch Bracketed until 6/5/15
Pharmacy Quality Commitment® (PQC) provides a safety net for pharmacies to address continuous quality improvement (CQI) programs such as pharmacy network contracts, Medicare
Part D requirements under CMS Section 423.153 (c), and state mandates for CQI programs.
Do you have a safety net protecting you and your patients?
PQC is a risk management tool for pharmacists to use to address the growing emphasis on controlling medication errors. When implemented, pharmacies improve efficiency
and increase patient safety through an analysis of quality-related events.
Call toll free (866) 365-7472 or go to www.pqc.net for more information. PQC is sponsored by the Nebraska Pharmacists Association.
Do you have a safety net?
8 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 9
Notice to Amend the Bylaws of the Nebraska Pharmacists Association
10 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 11
www.spahp.creighton.edu
CREIGHTON DOCTOR OF PHARMACY CLASS OF 2015
The Creighton University School of Pharmacy and Health Professions graduated 174 students from the Doctor of Pharmacy class of May 2015. A Graduate Recogni�on & Hooding Ceremony was celebrated with their families Friday, May 15 on the Creighton campus. Saturday, May 16, graduates par�cipated in the Creighton morning commencement exercises at the CenturyLink Center Omaha. Of the gradua�ng class… 39% plan to pursue a career in community pharmacy
(nine in an independent se�ng), 21% will go on to residencies, 8% plan to prac�ce in a hospital se�ng, 3% ambulatory care, 4% chose other areas of prac�ce and 25% of the graduates were undecided.
De Hernanieva Abrasheva ‐ New Jersey* James Vincent Idong Agbayani ‐ Waipahu, Hawaii Oluyemi Adeola Aladejebi ‐ Greenwood, Indiana* John Todd Andersen ‐ Memphis, Tennessee Sarah Lorene Andrews ‐ Spokane, Washington* Taylor Chad Anglemyer ‐ Omaha, Nebraska Oluwatosin Arowomole ‐ Monee, Illinois* Lisa Marie Barnes ‐ Centerton, Arkansas* Trevor John Bauer ‐ Eau Claire, Wisconsin* Mark Andrew Benne� ‐ Roosevelt, Utah Andrew Jason Bergman ‐ Harlan, Indiana* Alicia Nicole Be�s ‐ Albia, Iowa Hibah Mumtaz Bhuiyan ‐ Chicago, Illinois* Sebas�an Biglione ‐ Buenos Aires, Argen�na* Andrew James Bracht ‐ West Point, Nebraska Kaitlin Marie Bresnahan ‐ Chicago, Illinois Emigene Ann Brown ‐ Allen, Texas* Rebecca Anne Buck ‐ Bradenton, Florida* Nhi Quynh Bui ‐ Lewisville, Texas Kevin Mar�n Burns ‐ Alabaster, Alabama* Jian Lei Cai ‐ Hardin, Montana Jocelyn Agnes Calado ‐ Watertown, Wisconsin Heather Annie Caton ‐ Aberdeen, South Dakota* Courtney Lynn Cerkas ‐ Greenville, Wisconsin* Kristyn Carol Chapman ‐ West Bend, Wisconsin Yan Dan Chen ‐ Brooklyn, New York Janet Aki Oguma Cheng ‐ Hun�ngton Beach, California* Shingairai B Chiwara ‐ Coolidge, Arizona Marc Thomas Choque�e ‐ Has�ngs, Nebraska Jared Michael Connell ‐ Kansas City, Missouri Rachel Theresa Coppinger ‐ Barnum, Iowa
Laura Marie Co�guala ‐ Orland Park, Illinois Kathleen Marie Cristofaro ‐ Elmira, New York* Ian Viloria Daguimol ‐ Kapolei, Hawaii Celeste Daniele Davis ‐ Russellville, Arkansas* Ali Jo Deneen ‐ South Saint Paul, Minnesota Megan Derba ‐ Springeld, Missouri Derek James Dickson ‐ Gilbert, Arizona Jeff Ray Digre ‐ St. Paul, Minnesota* Catherine Anne Dinkins ‐ Saint Louis, Missouri Tai Quoc Do ‐ Lincoln, Nebraska Charles Tri Doan ‐ San Jose, California Kris�ne Nicole Dodge ‐ Webster City, Iowa Patrick Allen Donat ‐ Sioux Falls, South Dakota Kathleen Breanne Drobnicki ‐ Redmond, Washington Elane Allyn Endeco� ‐ Maryville, Missouri Erica Rae Erixon ‐ Council Bluffs, Iowa Sean Michael Eubanks ‐ Grand Junc�on, Colorado* Kelley Ann Felt ‐ Evansville, Indiana* Amanda Lynn Fisher ‐ Lubbock, Texas* Charles John Flahave ‐ Saint Cloud, Minnesota Ashley Frances Fleming ‐ South Beloit, Illinois* Lisa Chee Ling Fong ‐ Honolulu, Hawaii Dabney Ann Fournier ‐ Parker, Colorado* Nathan Lynn Friend ‐ Salem, Missouri Danya Gammas ‐ Menlo Park, California* Kimberly Ann Garlena ‐ Hollsopple, Pennsylvania* Meredith Katherine George ‐ Libertyville, Illinois Katherine Elizabeth Grabau ‐ St. Louis, Missouri Peggy Lea Groeneveld ‐ Houghton, Michigan* Sun Han ‐ Tacoma, Washington Rhonda Kay Hanley ‐ Cha�anooga, Tennessee*
Pictured at right: New grad Andrew J. Bracht of West Point, Nebr. poses for a photo with Dr. Chris Bradberry while Julie Vollmuth, Pharm.D.’02, alumni advisory board president, and Curt Barr, BSPha’74, Pharm.D., look on during Friday night’s hooding ceremony.
Creighton University is a Jesuit, Catholic university bridging health, law, business & the arts and sciences for a more just world.

10 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 11
Ashley Ranae Hanson ‐ Sartell, Minnesota Terri Hasiak ‐ Papillion, Nebraska Taylor Doyle Hegarty ‐ Plymouth, Minnesota Chris�ne Kyeonga Heon ‐ Li�leton, Colorado* Raquel Donaire Her�g ‐ Chesapeake, Virginia* Michael Patrick Hinnenkamp ‐ Shoreview, Minnesota Kimberly Kam Lan Ho ‐ Honolulu, Hawaii April Michele Howell ‐ Texas* Brandon Lee Jacobi ‐ Omaha, Nebraska Michael Woo Jeon ‐ Hoffman Estates, Illinois Christopher James Johnson ‐ North Logan, Utah Sarah Elizabeth Kaufman ‐ Evansville, Indiana* Sojeet Kaur ‐ Macungie, Pennsylvania* Shannon Allison Kelly ‐ Kirkwood, Missouri Sun Kim ‐ Honolulu, Hawaii Jasmine Chiemi Kimura ‐ Honolulu, Hawaii Ryan Kinoshita ‐ Kailua, Hawaii Andrew Charles Klick ‐ Albert Lea, Minnesota Alex Labasan Kugler ‐ Colorado Springs, Colorado Sara Saori Kumasaka ‐ Honolulu, Hawaii Nancy Jackson Kuoe ‐ Kansas City, Missouri Emmanuel Steve Kuvetakis ‐ Omaha, Nebraska Lai Hung Lam ‐ Honolulu, Hawaii Micah Andrew Lansford ‐ Clovis, New Mexico Hong Ha Le ‐ Bao Loc ‐ Lam Dong, Vietnam Mark Anthony Lewandowski ‐ Raleigh, North Carolina* Marie LeVoir Ljosenvoor ‐ Aus�n, Minnesota* Allison Ann Luckenbill ‐ West Burlington, Iowa Taylor John MacKinnon ‐ Salem, Wisconsin Mardoqueo Joseph Mar�nez ‐ Albuquerque, New Mexico Casey Lynn Mashl ‐ Colorado Springs, Colorado* JonPaul Evans McCartney ‐ Pace, Florida* Meredith Ellen McElroy—Decatur, Alabama Keith Warren McLain ‐ Henderson, Nevada* Caitlyn Mary McMurtry ‐ Saint Charles, Missouri Michael James McQuade ‐ Port Orange, Florida* Meredith Ann Meyer ‐ Manning, Iowa Ammon Niels Landon Mitchell ‐ Mesquite, Nevada Briana Goodwin Moe ‐ Ewa Beach, Hawaii* Audrey Kris�ne Moehr ‐ Goose Lake, Iowa Brandon Joel Mooer ‐ Glendive, Montana* James Ma�hew Morran ‐ Omaha, Nebraska Amber O. Mortensen ‐ Glendale, Arizona* Rosemary Mu�ndi Mutunga ‐ Santa Rosa, California Jill Marie Mutziger ‐ Yankton, South Dakota* Michelle Chris�ne Myers ‐ Charleston, West Virginia* Kailani Blake Nakanishi ‐ Waipahu, Hawaii Terelle Ree Nash‐Keller ‐ Selby, South Dakota Timothy Ndugwa ‐ Kampala, Uganda Sara Lynn Nebbia ‐ Leawood, Kansas Chelsie Helene Neves ‐ Aiea, Hawaii Daniel Nguyen ‐ Roscoe, Illinois Megan Dena Nicklaus ‐ Webster Groves, Missouri Maddison C Nolfo ‐ O'Fallon, Missouri Linda Yen Nong ‐ Omaha, Nebraska Chelsea O'Brien ‐ Pennsylvania* John Andrew O'Regan ‐ Williams Bay, Wisconsin Hyung‐Joo Park ‐ Bellevue, Washington Parin Patel ‐ Hayward, California Rachele Ann Paul ‐ Hudson, Wisconsin* Taifa Peaks ‐ Raleigh, North Carolina* Mark William Pedginski ‐ S�llwater, Minnesota
Theresa H. Pelzel Poklemba ‐ Whitney Point, New York* Rebecca Lynn Pepper ‐ Lewes, Delaware* Debora Abrahao Pereira ‐ Gilbert, Arizona* Chau Quynh Pham ‐ Rockwall, Texa* John Manh Tinh Pham ‐ San Jose, California Bre� Allen Pie�g ‐ Carroll, Iowa Jamie Kay Ravenscra� ‐ Parkville, Missouri Aleah Marie Rodriguez ‐ Waukegan, Illinois Lauren Elizabeth Sacksteder ‐ Franklin Park, Illinois* Laila Ahmed Saleem ‐ Valencia, California* Angeline Elizibeth Salmons ‐ Warsaw, Missouri* Eric Allen Saul ‐ Casper, Wyoming* Jacqueline Ann Schabold ‐ Chicago, Illinois Cole Jeffrey Schafer ‐ Underwood, Iowa Ashley Marie Schilling ‐ Rapid City, South Dakota Jeffrey Sco� Schutzbach ‐ New Lenox, Illinois Saundra M Seep ‐ Getzville, New York* Keri Jean Seiser ‐ Webster City, Iowa Grant Mar�n Sha� ‐ Burnsville, Minnesota Elisa Sheil ‐ Kirbyville, Missouri* Shelby Malynn Shemanski ‐ Solon, Iowa Jay Daniel Sherer ‐ Columbus, Nebraska Hilary Jennifer Smith ‐ Centennial, Colorado Andrew Wayne Snyder ‐ Nixa, Missouri* Derek Dean Snyder ‐ Burwell, Nebraska Stephanie Ann Soler ‐ Casper, Wyoming* Sarah Rosalie Spencer ‐ Columbia, Maryland* Eric David Stemple ‐ Mount Vernon, Indiana* Thomas James Stetser ‐ Vacaville, California Jenna Elizabeth Sturm ‐ Wall Lake, Iowa Bri�any Aiko Suzuki ‐ Honolulu, Hawaii Kortnee Linn Tate ‐ East Peoria, Illinois* Pauline Tran ‐ Honolulu, Hawaii Victoria Lynn Travis ‐ Fairbanks, Alaska* Anne Mae Trivino ‐ Bartle�, Illinois Laurie Harumi Leilani Uehara ‐ Honolulu, Hawaii Dreana Rae Ihara Valenciano ‐ Lihue, Hawaii Kristen Nichole Wallinger‐Lange ‐ Stuart, Nebraska Michael Anthony Wankum ‐ St. Louis, Missouri Melissa K. K. Wauke –Honolulu, Hawaii* Michael Chris�an Wegner ‐ Omaha, Nebraska Kevin Michael Welch ‐ Topeka, Kansas Katelyn Ann Westrich ‐ Godfrey, Illinois Jason Jeremy White ‐ Kirkland, Washington* April Dawn Willoby ‐ Pekin, Illinois* Hyrum Todd Wilson ‐ Omaha, Nebraska Alexandra Jean Wohlgemuth ‐ Columbus, Nebraska* Yunuo (Enora) Wu ‐ Cedar Falls, Iowa Keith Yamamoto ‐ Honolulu, Hawaii Stanislav Viachaslavovich Yavid ‐ Minsk, Belarus
*Distance Pathway
Creighton University is a Jesuit, Catholic university bridging health, law, business & the arts and sciences for a more just world.
CREIGHTON UNIVERSITY DOCTOR OF PHARMACY CLASS OF 2015
SPOTLIGHT: Alexandra J. Wohlgemuth Pathway: Entry‐Level Distance Pharmacy Hometown: Columbus, Nebraska Daughter of: Jeff & Jeanne Bartels of Columbus, Nebraska Wife of: Nick Wohlgemuth of Bal�more, Maryland Sr. Award: Excellence in Non‐prescrip�on Medica�on Studies Post‐Graduate Plans: Alexandra is excited to begin the next chapter of her life, which includes star�ng her career as a community pharmacist in Bal�more and becoming a mother.
Continuing Pharmacy Education Lesson #6
12 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 13
New Options for Disposal ofControlled SubstancesThis CPE lesson was written by Anna Legreid Dopp, PharmD, Vice President of Public Affairs, Pharmacy Society of Wisconsin, and Sarah Sorum, PharmD, Vice President, Professional & Educational Affairs, Pharmacy Society of Wisconsin, who do not have any conflicts of interest, nor do they have any financial relationships with a commercial interest related to this lesson. Reprinted with permission from the Pharmacy Society of Wisconsin.
ObjectivesAt the conclusion of this lesson, pharmacists and pharmacy technicians should be able to:1. According to the DEA Final Rule for the disposal of controlled substances, define "collector" and "ultimate user";2. Outline the process for DEA registrants to modify their registration to include collection of controlled substances; 3. Describe the role of law enforcement, pharmacies, hospitals/clinics, and long-term care facilities in the collection of controlled substances for the purposes of disposal; 4. Outline requirements for the collection of controlled substances through take-back events, mail-back programs, and collection receptacles; 5. Discuss specific requirements for pharmacies, hospitals/clinics, and long-term care facilities in the management of collection receptacles; and 6. Describe opportunities and remaining challenges in the disposal of controlled substances.
On September 9, 2014, the DEA posted a final rule, effective October 9, 2014, in the Federal Register related to the disposal of controlled substances. This rule governs the secure disposal of controlled substances by DEA registrants, ultimate users (patients), and long-term care facilities (LTCFs). These regulations implement the Secure and Responsible Drug Disposal Act of 2010 by expanding options available to collect controlled substances from ultimate users for purposes of disposal to include: take-back events, mail-back programs, and collection receptacle locations. These regulations contain specific language allowing law enforcement to voluntarily continue to conduct take-back events, administer mail-back programs, and maintain collection receptacles. These regulations also allow
authorized manufacturers, distributors, reverse distributors, narcotic treatment programs, hospitals/clinics with an onsite pharmacy, and retail pharmacies to voluntarily administer mail-back programs and maintain collection receptacles. In addition, this rule expands the authority of authorized hospitals/clinics and retail pharmacies to voluntarily maintain collection receptacles at LTCFs and for long-term care facilities to use collection receptacles on behalf of current or previous residents.
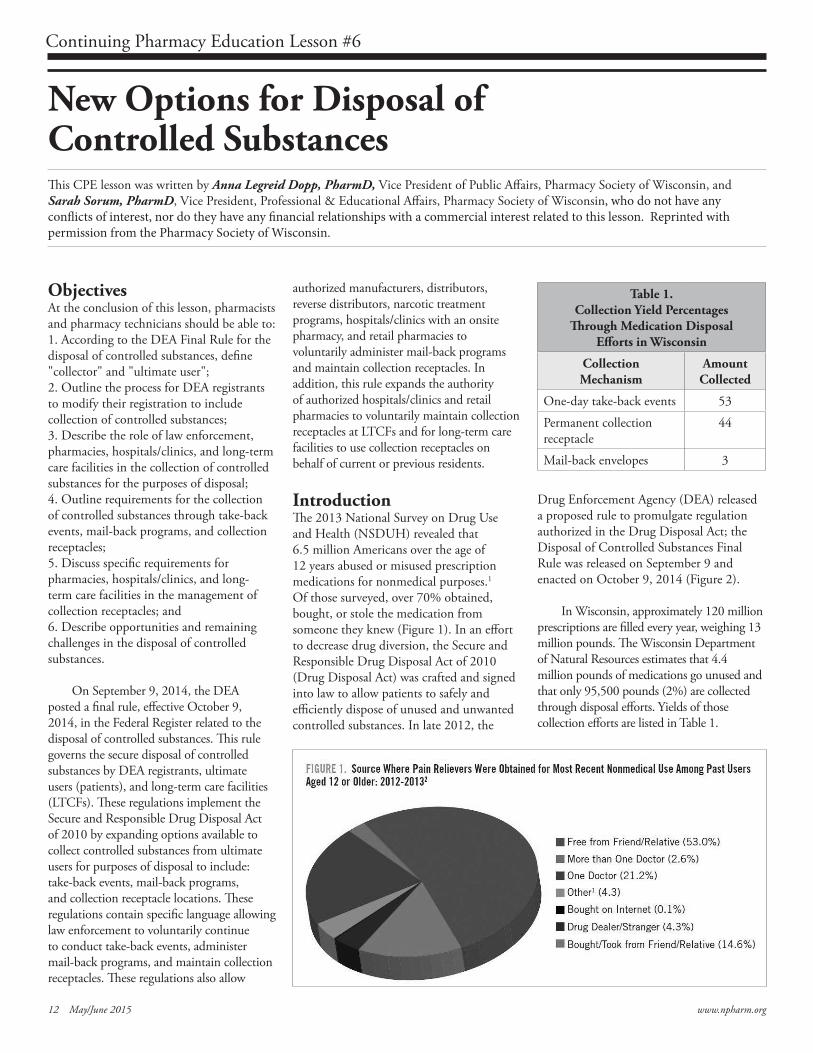
Introduction The 2013 National Survey on Drug Use and Health (NSDUH) revealed that 6.5 million Americans over the age of 12 years abused or misused prescription medications for nonmedical purposes.1 Of those surveyed, over 70% obtained, bought, or stole the medication from someone they knew (Figure 1). In an effort to decrease drug diversion, the Secure and Responsible Drug Disposal Act of 2010 (Drug Disposal Act) was crafted and signed into law to allow patients to safely and efficiently dispose of unused and unwanted controlled substances. In late 2012, the
Drug Enforcement Agency (DEA) released a proposed rule to promulgate regulation authorized in the Drug Disposal Act; the Disposal of Controlled Substances Final Rule was released on September 9 and enacted on October 9, 2014 (Figure 2).
In Wisconsin, approximately 120 million prescriptions are filled every year, weighing 13 million pounds. The Wisconsin Department of Natural Resources estimates that 4.4 million pounds of medications go unused and that only 95,500 pounds (2%) are collected through disposal efforts. Yields of those collection efforts are listed in Table 1.
Table 1. Collection Yield Percentages
Through Medication DisposalEfforts in Wisconsin
CollectionMechanism
Amount Collected
One-day take-back events 53
Permanent collection receptacle
44
Mail-back envelopes 3

Continuing Pharmacy Education Lesson #6
12 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 13
Prior to the passing of the Drug Disposal Act and the DEA’s Final Rule, efforts to collect unused medications were labor intensive, costly, and cumbersome given the lack of clarity, resources, and regulation surrounding medication disposal. The purpose of this lesson is to provide an overview of the Final Rule and the implications for pharmacists, pharmacy staff, and pharmacies. A list of commonly used and referenced drug disposal terms and their definitions is provided in Table 2.
Authorized Collectors of Controlled Substances for DestructionAccording to the Final Rule, the following groups may serve as “collectors” of controlled substances for the purpose of destruction:
• Manufacturers • Distributors • Reverse distributors • Narcotic treatment programs • Hospitals/Clinics with an onsite
pharmacy • Retail pharmacies
The DEA requires authorized collectors to register with the agency and specify which method of collection will be implemented. There is no fee to become an authorized collector. Collectors may receive controlled substances from: 1) ultimate users; 2) individuals lawfully entitled to dispose of deceased person’s controlled substances; and 3) LTCFs on behalf of residents who reside or resided at the LTCF with a receptacle.
Take-Back Programs On September 27, 2014, the DEA organized and hosted the ninth and last National Drug Take Back Day. Since its first event in 2010, the DEA collected more than 4.1 million pounds of prescription drugs in over 50 states, the District of Columbia, and several territories.2 The Final Rule contains specific language that continues to authorize law enforcement, either independently or in partnership with private entities or community groups, to voluntarily hold take-back events.
As in the past, only law enforcement can conduct take-back programs while other groups may assist. The Final Rule does not change existing law enforcement procedures regarding the handling, storage, transfer, or destruction of controlled substances, but it does outline procedures for take-back events themselves.
A law enforcement officer must be appointed to oversee the collection at the event. According to the regulation, no other person, such as a take-back event volunteer, can handle or touch the controlled substances prior to their transfer from the ultimate user to law enforcement. This restriction includes pharmacists; only law enforcement can accept substances from community members. However, nothing in the rule prohibits law enforcement from partnering with pharmacists, student pharmacists, or others to inventory or sort substances that have been collected by law enforcement provided that the collected substances remain under the control and custody of law enforcement. Law enforcement is responsible for maintaining adequate security to prevent diversion or theft.
Table 2. Terms and Definitions Referenced in the Disposal of Controlled Substances Final Rule
Ultimate user Person who has lawfully obtained, and who possesses, a controlled substance for his own use or for the use of a member of his household or for an animal owned by him or a member of his household.
Collection Receipt of a controlled substance for the purpose of destruction.
Non-retrievable Standard for destruction which alters a substance so that it cannot be transformed to a physical or chemical condition or state as a controlled substance or controlled substance analogue. Destruction renders the substance unavailable and unusable. Note: Flushing controlled substances or mixing controlled substances with coffee grounds or kitty litter are examples of existing methods of destruction that do not meet the non-retrievable standard.
Retail Pharmacy Includes any entity registered with DEA as a retail pharmacy vs. those registered as hospital/clinic. Closed door pharmacies, long-term care pharmacies, specialty pharmacies are likely registered with DEA as a “retail pharmacy.”
Onsite Located on or at the physical premises of the registrant’s registered location.
Reverse Distributor Person registered to acquire controlled substances from another registrant or law enforcement for the purpose of return or destruction.
Employee Criteria for designation of employee: • Persons who are directly paid by the registrant • Persons who are subject to direct oversight by the registrant • Persons who are required, as a condition of employment, to follow the registrant’s procedures and guidelines
pertaining to the handling of controlled substances • Persons who receive a performance rating or performance evaluation on a regular/routine basis from the registrant• Persons who are subject to disciplinary action by the registrant • Persons who render services at the registrant’s registered location

14 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 15
pharmacy’s ability to independently collect medications through mail-back programs due to the expense and difficulty of implementing and maintaining a destruction process at its facility.
An authorized collector that wishes to conduct a mail-back program needs to produce and provide specified packages (at no cost or for a fee) to patients. The authorized collector may provide this packaging in partnership with a third party. For example, a reverse distributor (authorized as a collector by DEA) could produce mail-back packages and allow a pharmacy, hospital, or other third party group to provide these packages to patients. In this case, the reverse distributor would be responsible for operating the mail-back program and would receive the mail-back packages directly at its registered location for onsite destruction. The authorized collector that is conducting the mail-back program is responsible for inventory management and record keeping requirements. In the above example, the reverse distributor is responsible for the record keeping requirements outlined by the DEA.
The Final Rule also lists the criteria for mail-back packages. Mail-back packages need to be: • Postage paid and pre-addressed to the
authorized mail-back location • Nondescript, tamper-evident, tear-
resistant, water- and spill-proof, and sealable
• Contain a unique identification number so that each package can be tracked
• Contain instructions for the user that indicate the process for mailing back that package, permitted substances that
can be sent, notice that packages may only be mailed from within the U.S., and notice that only packages provided by the authorized collector will be accepted for destruction
• Patients cannot be required to provide any personally identifiable information when mailing back controlled substances to an authorized collector
Mail-back packages received by the collector shall not be opened, x-rayed, or otherwise penetrated and the substances may not be individually handled, counted, inventoried, or otherwise discerned. The sealed mail-back packages must be destroyed onsite in a prompt manner. Pharmacies cannot receive sealed mail-back packages for disposal unless they will be destroying the sealed mail-back package onsite.
If a collector receives a mail-back package that they did not provide, the collector must notify the DEA Field Division Office in their area within three business days. This would apply to a pharmacy that receives a sealed mail-back package if they themselves are not the authorized mail-back collector even if they provided the mailer on behalf of a reverse distributor.
Bottom line: Pharmacies may facilitate participation in mail-back programs in partnership with a reverse distributor, for example, but would likely not conduct the mail-back program themselves as onsite destruction of received controlled substances is required.
Continuing Pharmacy Education Lesson #6
Bottom Line: Pharmacists, pharmacy technicians and student pharmacists can continue to participate in take-back events in partnership with law enforcement, but ultimate users may only transfer controlled substances directly to law enforcement.
Mail-Back Programs The DEA regulations state that mail-back programs may be conducted by registered manufacturers, distributors, reverse distributors, narcotic treatment programs, hospitals/clinics with an onsite pharmacy, or retail pharmacies that are (1) authorized as “collectors” and (2) have and utilize an “onsite” method of destruction at their registered location. In addition, they contain specific language allowing law enforcement to voluntarily continue to conduct mail-back programs.
The method of destruction is an important distinction to consider. The rules require that destruction must render the controlled substances “non-retrievable.” The most common form of destruction is through incineration. Flushing controlled substances or mixing controlled substances with coffee grounds or kitty litter are examples of existing methods of destruction that do not meet the non-retrievability standard. As listed earlier, the method of destruction must be completed onsite for mail-back programs. The DEA defines “onsite” as “located on or at the physical premises of the registrant’s registered location.” Specifically, a controlled substance is destroyed “onsite” when destruction occurs on the physical premises of the destroying registrant’s registered location. It is this requirement that will limit a

14 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 15
Table 3. Collection Receptacle Requirements
Receptacle Location • Must be securely placed and maintained inside the collector’s registered location• Must be located within the immediate proximity of a designated area where controlled substances are stored and
at which an employee is present (e.g., can be seen from the pharmacy counter)
Receptacle Security • Must be securely fastened to a permanent structure so that it cannot be removed • Must be a securely locked, substantially constructed container with a permanent outer container and removable
inner liner • The opening must be capable of being locked at times when an employee is not present (e.g., when the pharmacy
department is closed) or not being regularly monitored by an long-term care facility employee
Receptacle Labeling • Must prominently display a sign indicting that only non-controlled drugs and Schedule II, III, IV or V controlled substances are acceptable for collection
Continuing Pharmacy Education Lesson #6
Collection Receptacles The regulation continues to allow, using specific language, Federal, State, tribal, and local law enforcement to voluntarily maintain collection receptacles at the law enforcement’s physical location. The DEA authorizes manufacturers, distributors, reverse distributors, narcotic treatment programs, hospitals/clinics with an onsite pharmacy, and retail pharmacies to be “collectors” with authorization to maintain collection receptacles at their registered location. With the exception of LTCFs, collection receptacles are not allowed at other locations like community centers, schools, churches, etc. The placement and maintenance of a collection receptacle will likely be the most commonly employed mechanism of disposal that a pharmacy will choose to provide as a service to patients.
Only ultimate users and persons lawfully entitled to dispose of an ultimate user decedent’s property may deposit controlled substances in a collection receptacle. An individual may not gather controlled substances from friends, or neighbors for bringing into the pharmacy, for example. Once a substance has been deposited into a collection receptacle, the substance shall not be counted, sorted, inventoried, or otherwise individually handled.
It is important to note that DEA registrants, such as hospitals, cannot use the collection receptacles to dispose of unused controlled substances in their inventory or stock. As a reminder, a controlled substance dispensed for immediate administration
pursuant to an order for medication in an institutional setting remains under the custody and control of that registered institution even if the substance is not fully exhausted (e.g., some of the substance remains in a vial, tube, transdermal patch, or syringe after administration but cannot or may not be further utilized, commonly referred to as "drug wastage" and "pharmaceutical wastage"). Such remaining substance must be properly recorded, stored, and destroyed in accordance with DEA regulations (21 CFR 1317.90 and 1317.95), and all applicable Federal, State, tribal, and local laws and regulations, although the destruction need not be recorded on a DEA Form 41.
There are specific requirements for placing and hosting a collection receptacle. They are provided in Table 3.
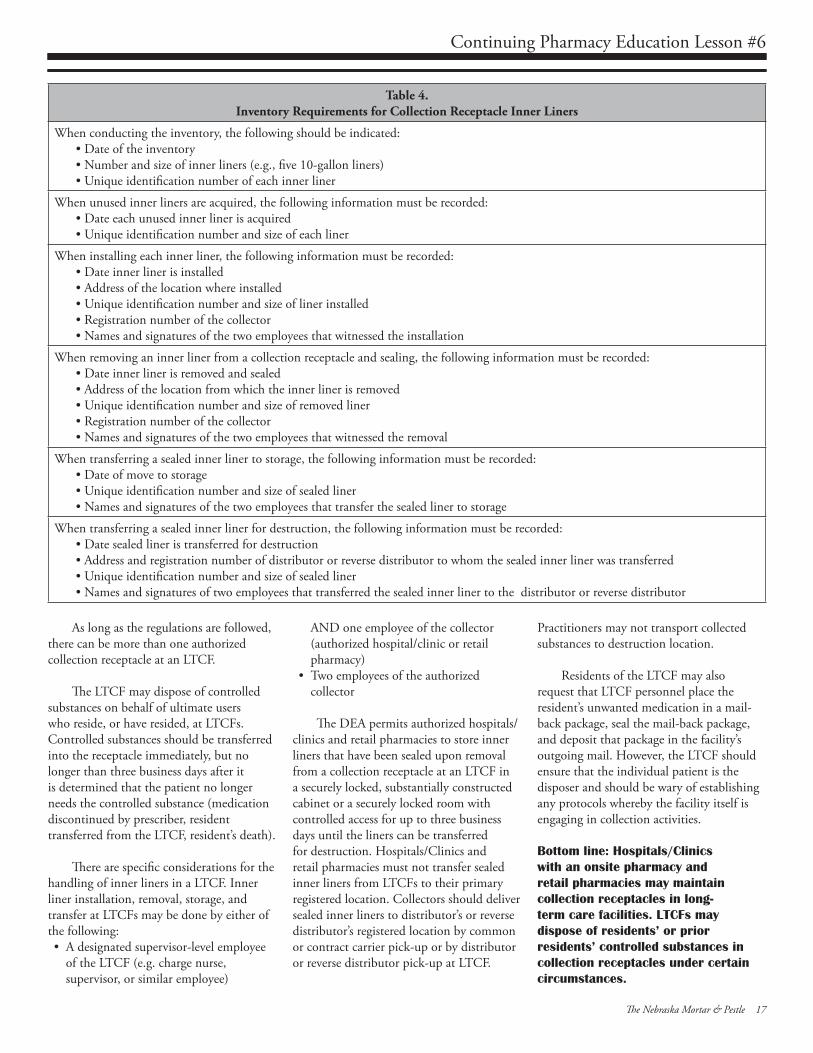
Inner liners may be used in a collection receptacle. The Final Rule outlines specific requirements for the handling of inner liners. Inner liner requirements are outlined in Figure 3.
Upon removal of the inner liner, a hospital/clinic with an onsite pharmacy or a retail pharmacy must do one of the following: • Promptly destroy the inner liner and its
contents “onsite”, rendering it “non-retrievable”
• Promptly deliver the inner liner and its contents to a distributor’s or reverse distributor’s registered location by common or contract carrier pick-up or by distributor or reverse distributor pick-
up at the registrant’s registered location • Request assistance from the Special
Agent in Charge of the Administration in the area in which the authorized hospital/clinic or pharmacy is located
• Securely store the sealed inner liner and its contents at the collector’s registered location in either a securely locked, substantially constructed cabinet or a securely locked room with controlled access until prompt destruction can occur
Collectors maintaining collection receptacles need to keep inventory of unused inner liners on hand and sealed inner liners on hand awaiting destruction. These inventory requirements are outlined in Table 4.
Bottom line: Use of a collection receptacle is the most likely method pharmacies would provide to their patients for disposal of controlled substances. Pharmacies utilizing inner liners must have a complete, accurate record of each inner liner.
Considerations for Hospitals and Clinics with an Onsite Pharmacy The Final Rule allows hospitals and clinics with an onsite pharmacy to modify their registration with the DEA to become authorized collectors. It states that a hospital/clinic has an “onsite pharmacy” when it has a pharmacy located on the physical premises of the registrant’s

Continuing Pharmacy Education Lesson #6
16 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 17
Considerations for Collection Receptacles in Long-term Care Facilities The Final Rule authorizes that hospitals/ clinics with an onsite pharmacy and retail pharmacies may maintain collection receptacles at LTCFs. In the DEA Final Rule, a “long-term care facility” is defined as “a nursing home, retirement care, mental care, or other facility or institution, which provides extended health care to resident patients.” This definition is different from how a LTCF is defined in Nebraska resulting in some confusion about whether the new rule applies to assisted living facilities. Nebraska Revised Statute 38-2826.01 - Long-term care facility, defined.Long-term care facility means an intermediate care facility, an intermediate care facility for persons with developmental disabilities, a long-term care hospital, a mental health center, a nursing facility, or a skilled nursing facility, as such terms are defined in the Health Care Facility Licensure Act.
Although the collection receptacle is located in a LTCF, the authorized hospital/clinic with an onsite pharmacy or authorized retail pharmacy is responsible for:• Installation, management, and
maintenance of the collection receptacle • Removal and sealing of inner liners or
supervision of this activity
• Transferring and storage of sealed inner liners or supervision of this activity
Registrants that wish to maintain collection receptacles at LTCFs must include the name and physical location of each LTCF at which they intend to operate a collection receptacle in their application for a modified registration with the DEA. This means that if a pharmacy wants to add additional facilities to their list of LTCFs where they maintain a collection receptacle, they will have to further modify their registration with the DEA. If a LTCF changes ownership and changes its name, the authorized collector must modify its registration with DEA. Records related to collection receptacles at LTCFs must be maintained at the authorized collector’s registered location and not at the LTCF.
Pharmacies that provide collection receptacles at LTCFs do not need to provide medications for the LTCF or have any other relationship with them. In addition to meeting the requirements for all collection receptacles (above), a receptacle in an LTCF needs to be located in a secured area monitored by LTCF employees. The authorized collector (e.g., pharmacy) is responsible for ensuring the regular monitoring of LTCF personnel and ensuring the appropriate security procedures are in place at LTCFs in the event of suspected tampering or diversion.
registered location. Hospitals/clinics that volunteer and register to be collectors must place collection receptacles in locations that are regularly monitored by employees, but not in proximity of any area where emergency or urgent care is provided.
Controlled substances dispensed pursuant to a medication order by a practitioner in a hospital or clinic for immediate administration at the practitioner’s registered location remain under the custody and control of the DEA registrant. Therefore, if that substance is not fully used (e.g., some of the substance remains in a vial, tube, transdermal patch, or syringe after administration but cannot or may not be further utilized, commonly referred to as "drug wastage" and "pharmaceutical wastage"), the DEA registrant must destroy the remaining, unusable controlled substance. A collection receptacle may not be used.
Bottom line: Hospital/clinics with onsite pharmacies may maintain collection receptacles in non-urgent/ emergency care areas that are regularly monitored by employees.
)
16 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 17
Continuing Pharmacy Education Lesson #6
Table 4. Inventory Requirements for Collection Receptacle Inner Liners
When conducting the inventory, the following should be indicated: • Date of the inventory• Number and size of inner liners (e.g., five 10-gallon liners)• Unique identification number of each inner liner
When unused inner liners are acquired, the following information must be recorded: • Date each unused inner liner is acquired • Unique identification number and size of each liner
When installing each inner liner, the following information must be recorded:• Date inner liner is installed • Address of the location where installed • Unique identification number and size of liner installed • Registration number of the collector • Names and signatures of the two employees that witnessed the installation
When removing an inner liner from a collection receptacle and sealing, the following information must be recorded: • Date inner liner is removed and sealed • Address of the location from which the inner liner is removed • Unique identification number and size of removed liner • Registration number of the collector • Names and signatures of the two employees that witnessed the removal
When transferring a sealed inner liner to storage, the following information must be recorded: • Date of move to storage • Unique identification number and size of sealed liner • Names and signatures of the two employees that transfer the sealed liner to storage
When transferring a sealed inner liner for destruction, the following information must be recorded:• Date sealed liner is transferred for destruction • Address and registration number of distributor or reverse distributor to whom the sealed inner liner was transferred • Unique identification number and size of sealed liner • Names and signatures of two employees that transferred the sealed inner liner to the distributor or reverse distributor
As long as the regulations are followed, there can be more than one authorized collection receptacle at an LTCF.
The LTCF may dispose of controlled substances on behalf of ultimate users who reside, or have resided, at LTCFs. Controlled substances should be transferred into the receptacle immediately, but no longer than three business days after it is determined that the patient no longer needs the controlled substance (medication discontinued by prescriber, resident transferred from the LTCF, resident’s death).
There are specific considerations for the
handling of inner liners in a LTCF. Inner liner installation, removal, storage, and transfer at LTCFs may be done by either of the following: • A designated supervisor-level employee
of the LTCF (e.g. charge nurse, supervisor, or similar employee)
AND one employee of the collector (authorized hospital/clinic or retail pharmacy)
• Two employees of the authorized collector
The DEA permits authorized hospitals/ clinics and retail pharmacies to store inner liners that have been sealed upon removal from a collection receptacle at an LTCF in a securely locked, substantially constructed cabinet or a securely locked room with controlled access for up to three business days until the liners can be transferred for destruction. Hospitals/Clinics and retail pharmacies must not transfer sealed inner liners from LTCFs to their primary registered location. Collectors should deliver sealed inner liners to distributor’s or reverse distributor’s registered location by common or contract carrier pick-up or by distributor or reverse distributor pick-up at LTCF.
Practitioners may not transport collected substances to destruction location.
Residents of the LTCF may also request that LTCF personnel place the resident’s unwanted medication in a mail-back package, seal the mail-back package, and deposit that package in the facility’s outgoing mail. However, the LTCF should ensure that the individual patient is the disposer and should be wary of establishing any protocols whereby the facility itself is engaging in collection activities.
Bottom line: Hospitals/Clinics with an onsite pharmacy and retail pharmacies may maintain collection receptacles in long-term care facilities. LTCFs may dispose of residents’ or prior residents’ controlled substances in collection receptacles under certain circumstances.
Continuing Pharmacy Education Lesson #6
18 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 19
Policies for the Nebraska Mortar & Pestle (M&P) continuing pharmacy education lessons and quizzes:
1. M&P Quizzes are valid only for the membership year in which they are published. Quizzes for the 2015 Membership Year must be received by December 7, 2015. Quizzes cannot be carried over to another membership year.
2. If more than three questions are missed, the quiz will be returned. The quiz can be resubmitted.
3. CPE transcripts can be printed from NABP e-Profiles at www.nabp.net.
4. CPE credits are submitted to NABP by the 15th of each month. For example, M&P CPE quizzes completed in the month of August 2015, will be sent to NABP e-Profiles before September 15, 2015.
The Nebraska Council for Continuing Pharmacy Education (NCCPE) is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education (CPE).This CPE home study lesson has been accredited for 1.0 contact hour or 0.10 CEU. UAN #0128-0000-15-295-H03-P for pharmacists and #0128-0000-15-295-H03-T for pharmacy technicians. This lesson is a knowledge-based CPE activity targeted to pharmacists and pharmacy technicians.
The Nebraska Pharmacists Association disclaim any liability to you or your patients resulting from reliance solely upon the information contained herein.
Quiz Answers may be submitted:1. Online: www.npharm.org
2. Fax: 402-420-1406
3. Email: m&[email protected]
4. Mail: NPA Mortar & Pestle 6221 S 58th St, Ste A Lincoln, NE 68516
Considerations for Hospice Patients Home hospice and homecare personnel are often challenged by disposal of controlled substances after a patient dies. In the Final Rule, the DEA clarifies that home hospice and homecare personnel may not dispose of the deceased patients’ controlled substances.
Options for disposal of controlled substances when a patient dies at home include: • A person “lawfully entitled to dispose of
the decedent’s property” OR a member of the deceased patient’s household may deliver the controlled substance(s) to an authorized collector (take-back event, mail-back program, collection receptacle)
• The hospice or homecare organization can partner with an authorized collector to provide mail-back packages for the person “lawfully entitled to dispose of the decedent’s property” OR a member of the deceased patient’s household
• A person “lawfully entitled to dispose of the decedent’s property” OR a member of the deceased patient’s household may flush the substance(s) or mix with kitty litter or coffee grounds and throw the substance(s) away
Bottom line: Home hospice and homecare personnel cannot collect controlled substances from patients or their families for the purpose of disposal.
Conclusion The Disposal of Controlled Substances Final Rule outlines specific methods for ultimate users to dispose of unwanted controlled substances through collection receptacles, take-back events, and mail-back programs. Pharmacists and pharmacy technicians should be prepared to answer questions from patients about these options, as well as be aware of how the regulations impact pharmacy and institutional practice.
References 1. Substance Abuse and Mental Health
Services Administration. 2013 National Survey on Drug Use and Health. Available at: http://www.samhsa. gov/data/NSDUH/2013SummNatFindDetTables/ NationalFindings/NSDUHresults2013.pdf. Accessed: October 10, 2014.
2. DEA’s Ninth and Final Prescription Drug Take Back Event Press Release. Available at: http://www.justice.gov/dea/divisions/hq/2014/ hq092314.shtml. Accessed: October 13, 2014.
Publisher's Note:This analysis of the DEA Final Rule regarding the Disposal of Controlled Substances was completed as a member service by the PSW staff and reprinted by the NPA, and should not be considered a legal analysis of the final rule. Pharmacists should review the final rule in its entirety prior to planning for a disposal program.
Reprinted with permission from the Pharmacy Society of Wisconsin. This article was originally published in the November/December 2014 issue of the Journal of the Pharmacy Society of Wisconsin and CPE credit was offered. Learners should not seek duplicate credit.

Continuing Pharmacy Education Quiz #6
18 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 19
New Options for Disposal of Controlled SubstancesQuiz #6, May/June 2015, ACPE #0128-0000-15-295-H03-P/T
2015 Quiz #6 - NPA CPE Home Study Answer FormNew Options for Disposal of Controlled Substances
UAN #0128-0000-15-295-H03-P for pharmacistsUAN #0128-0000-15-295-H03-T for technicians
1.0 Contact Hour - Knowledge Based CPE Activity
Name ________________________________________________________
Mailing Address _______________________________________________
City/State/Zip _________________________________________________
*NABP e-Profile # ______________ *Date of Birth (MMDD) _________*Required for ACPE credit.
Circle one (1) Answer:1. a b c d 5. a b c d2. a b 6. a b c d3. a b 7. a b c d 8. a b c 4. a b c d 9. a b c d
CPE Home Study Evaluation 1. Rate this lesson: (Excellent) 5 4 3 2 1 (Poor)
2. Did this lesson meet each of its objectives? ___ Yes ___ No3. Was the content without commercial bias? ___ Yes ___ No 4. Did the lesson meet your educational/practice needs? ___ Yes ___ No5. Comments/future topics are welcome. ________________________
The deadline for this quiz is December 7, 2015
Keep the TOP portion for your records. Return the BOTTOM portion to the NPA office.Or, take this quiz online at www.npharm.org
1. An authorized “collector” of controlled substances may include:
a. Hospital/Clinic with an onsite pharmacy b. Retail pharmacy c. Reverse distributor d. All of the above
2. True or False. Due to their registration status with the DEA, community pharmacies are automatically considered authorized collectors of controlled substances for the purposes of disposal. No additional registration with DEA is required to install a collection receptacle.
a. True b. False
3. True or False. “Ultimate user” is defined by DEA to mean a “person who has lawfully obtained, and who possesses, a controlled substance for his own use or for the use of a member of his household or for an animal owned by him or by a member of his household.”
a. True b. False
4. All of the following statements about take-back events are true EXCEPT: a. Law enforcement must appoint an officer to oversee the
collection event.b. Pharmacists, pharmacy technicians, and student
pharmacists can continue to participate in take-back events.
c. Specific recommendations for collection bins are provided in the Final Rule.
d. Student pharmacists may collect substances from patients at their car windows and deposit them in collection barrels for analysis.
5. Mail-back packages must: a. Be addressed so they are mailed to the pharmacy b. Be nondescript, tamper-evident, tear-resistant, water-
and spill-proof, and sealable c. Contain a unique identification number d. Both B and C are true
6. Collection receptacle inner liners must: a. Be opened and an inventory of controlled substances
must be conducted monthly and reported to DEA b. Be waterproof, tamper-evident, and tear-resistant c. Once removed from a collection receptacle at a
pharmacy and sealed, be securely stored at the pharmacy in either a securely locked, substantially constructed cabinet or a securely locked room with controlled access until prompt destruction can occur
d. Both B and C are true
7. When removing an inner liner from a collection receptacle at a long-term care facility (LTCF): a. A designated charge nurse and the pharmacy delivery
driver can record the date inner liner is removed and sealed, the address of the LTCF, the ID number and size of removed liner, the pharmacy DEA number, and their signatures.
b. The Director of Nursing for the facility may review disposed substances in the inner liner to determine how to minimize waste.
c. The hospital maintaining the collection receptacle may transport the sealed inner liner from the LTCF to the hospital for collection by their reverse distributor
d. The sealed inner liners may be stored at the LTCF in a securely locked, substantially constructed cabinet or securely locked room with controlled access for up to a week.
20 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 21
*Compensated endorsement.Not licensed to sell all products in all states.
Learn more about Pharmacists Mutual’s solutions for you – contact your local field representative or call 800.247.5930:
www.phmic.com
Our commitment to quality means you can rest easy.
50511
Endorsed* by:
Melissa McKean, CISR, CIC
800.247.5930 ext. 7127308.870.2873
20 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 21
Rx and The Law
AND THE LAWBy Don R. McGuire, Jr., RPh, JD
This series, Pharmacy and the Law, is presented by Pharmacists Mutual Insurance Company and the Nebraska Pharmacists Association through Pharmacy Marketing Group, Inc., a company dedicated to providing quality products and services to the pharmacy community.
Law Vs. Ethics
I recently attended a conference which had some very thought-provoking sessions. While the conference was
billed as a pharmacy law conference, ethical issues kept percolating to the surface. What is the difference between law and ethics? Why should I care? What impact can ethics have on pharmacy practice?
We should care because law and ethics work together to maintain our society. Law is a rule of conduct that is formally recognized by a society as binding and is enforced by that society. Ethics on the other hand is less structured and less formal. As a professional, pharmacists must use their professional skills for the benefit of their patients. Ethics involves the decision-making process required to treat patients. Many times the choices faced are not dealt with directly by laws.
Some commentators view laws as the baseline for professional conduct. This must mean that there is some advanced mode of practice that exceeds the requirements of the law. For example, if a pharmacist is required to undergo an annual skills assessment, there would be nothing to prevent the assessment being done every six months if it was thought that it provided better care for the patient. It still complies with the requirement set by law. The cost/benefit analysis and the decision-making process that ensues to decide if every six months is warranted is where ethics comes into play.
Some pharmacists don’t believe that ethical questions will affect them. They follow the law every day and that will suffice. However, there is a limitation on the effectiveness of the law. Law tends to be
reactionary, not proactive. Law deals with yesterday’s problems, not tomorrow’s. Also, law is limited. There are not laws to address every single issue that comes up in today’s society. If there were, our code books would be enormous. This is why lawyers are always talking about the “reasonable person”. What would a reasonably prudent pharmacist have done in your situation? This is the measuring stick for situations where black and white laws don’t exist, which is most of the time. These situations make pharmacists nervous because there may not be one “right” answer. Most likely there will be a best answer. Many people wish that more laws were simple right or wrong choices, but the reality is that our society is too complicated for such laws. Changing one little factor in a scenario may drastically change your conclusion.
Look at this list of issues if you think that pharmacists aren’t faced with ethical decisions;
• Should pharmacists be involved in the dispensing of Medical Marijuana?
• Should pharmacies sell alcohol or tobacco products?
• Should pharmacists take part in executions by lethal injection?
• Should pharmacists have the right to refuse to dispense drugs based on their personal morals?
• Should pharmacists dispense drugs for assisted suicide?
Depending on your state, most of these activities are legal. If following the law is your only criteria, then there is little
to debate here. But, ethical questions can arise because of a number of different reasons. It could be a conflict between the pharmacist’s moral values and the law. It could be competing laws that don’t coincide leaving the individual to try to reconcile the two different laws. They might also arise when there is no applicable law at all. Ethical questions might also arise when a patient’s needs cannot be met within the legal guidelines.
Chances are that we are all going to be faced with these types of choices at some point in our professional lives. Take time to prepare before you are faced with an urgent decision. There are plenty of references available that explain the principles of ethics and the decision-making process. When you are better prepared, the challenges are easier to handle. The ostrich approach is not going to prepare you well. Pharmacists are required to study the applicable laws. They should also study ethics because law and ethics work hand in hand. Neither alone is sufficient for pharmacists’ practices in the 21st Century.
1 American Society for Pharmacy Law’s Developments in Pharmacy Law XXV. Thanks to Ken Baker and Bruce White for planting the seeds of this article.
©Don R. McGuire, Jr., RPh, JD, is General Counsel, Senior Vice President, Risk Management & Compliance, at Pharmacists Mutual Insurance Company. This article discusses general principles of law and risk management. It is not intended as legal advice. Pharmacists should consult their own attorneys and insurance companies for specific advice. Pharmacists should be familiar with policies and procedures of their employers and insurance companies, and act accordingly.
PHARMACY TECHNICIAN CERTIFICATION BOARD
2215 Constitution Avenue, NW • Suite 101 • Washington, DC 20037(800) 363-8012 • Fax: (202) 888-1699
CERTIFICATIONASHP/ACPE-Accredited Pharmacy Technician Education ProgramBeginning in 2020, PTCB will require initial candidates for certification to complete a pharmacy technician education program accredited by the American Society of Health-System Pharmacists (ASHP)/Accreditation Council for Pharmacy Education (ACPE).
Leaders in the profession have demonstrated a desire for pharmacy technicians to follow the same credentialing model as pharmacists by becoming certified and registered with the state. Pharmacists are required to graduate from an accredited pharmacy school before they sit for the NAPLEX board exam and become licensed by their state Board of Pharmacy.
The number of ASHP/ACPE-accredited pharmacy technician education programs is growing. ASHP/ACPE-accredited programs include practical experience in addition to didactic course work, thereby providing well-rounded training for technicians. Many large employers have also begun developing their own training programs and are seeking ASHP accreditation.
In a March 2012 survey, 78% of respondents agreed that 2020 is a reasonable year by which to implement required accredited education.
This requirement will affect new individuals applying for national certification following the implementation date. It will not affect already certified pharmacy technicians applying for PTCB recertification.
RECERTIFICATIONPatient Safety CEAs part of the 20 hours of CE currently required for PTCB recertification, CPhTs now must complete one CE hour of patient safety, in addition to the one hour of law CE currently required. This requirement took effect in 2014.
Pharmacy technicians assist pharmacists with duties that impact patient care and safety. It is important that technicians continue to be educated on how their routine responsibilities shape the medication distribution system. By learning to identify potential errors in the system and how to report these, pharmacy technicians can affect the medication safety culture within pharmacies.
PTCB:
• Encourages pharmacy associations and other national CE providers to create patient safety CE programs specifically for pharmacy technicians.
• Highlights new patient safety CE programs on ptcb.org.
Certification and Recertification Requirements What is changing?
®www.ptcb.org
22 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 23
Name Date
Address
City State Zip
Phone Email
Pharmacy Technician Training Materials
Order your training manuals today!
Check Number
Credit Card Number Exp. Date /
CVC # Signature
Pharmacy Certifi ed Technician Training Manual and Calculations Workbook PackageThis package includes the Pharmacy Certifi ed Technician Training Manual and CD-ROM with master drug table, glossary, and answer key, as well as the Pharmacy Certifi ed Technician Calculations Workbook and accompanying CD-ROM that includes step-by-step math and problem answers. • $67.95 plus tax and $13.95 shipping and handling
Pharmacy Certifi ed Technician Calculations Workbookand CD-ROMThe calculations workbook includes a wide variety of math examples, review questions and real-life applications. The CD-ROM includes all of the problem answers with the step-by-step math to arrive at the solutions• $22.95 plus tax and $4.95 shipping and handling
Pharmacy Certifi ed Technician Training Manual and CD-ROMThe training manual covers concepts included on the Pharmacy Technician Certifi cation Exam administered by the Pharmacy Technician Certifi cation Board (PTCB). This manual features review questions, as well as real-life stories from technicians around the nation. The accompanying CD-ROM includes a master drug table, glossary, and answer key. Calculations are not included.• $49.95 plus tax and $7.95 shipping and handling
Refund PolicyTh e NPA has a no-return, no-refund policy on any manual or book purchased.
Calculations Workbook
(Qty) ___ @ $22.95 = $________
Training Manual
(Qty) ___ @ $49.95 = $________
Package - Manual and Workbook
(Qty) ___ @ $67.95 = $________
Subtotal +Tax (7%) +Shipping Total $____________
$____________
$____________$____________
To order:Call402-420-1500(Mon-Fri, 9am-4pm CST)
MailNebraska Pharmacists Association (NPA)6221 S 58th St, Ste ALincoln, NE 68516
Fax402-420-1406
Please allow 7 - 10 daysfor processing and mailing.
From home or work, at your own pace, use these self-study materials to prepare for the Pharmacy Technician Certifi cation Exam. Learn more about the exam at www.ptcb.org.
22 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 23
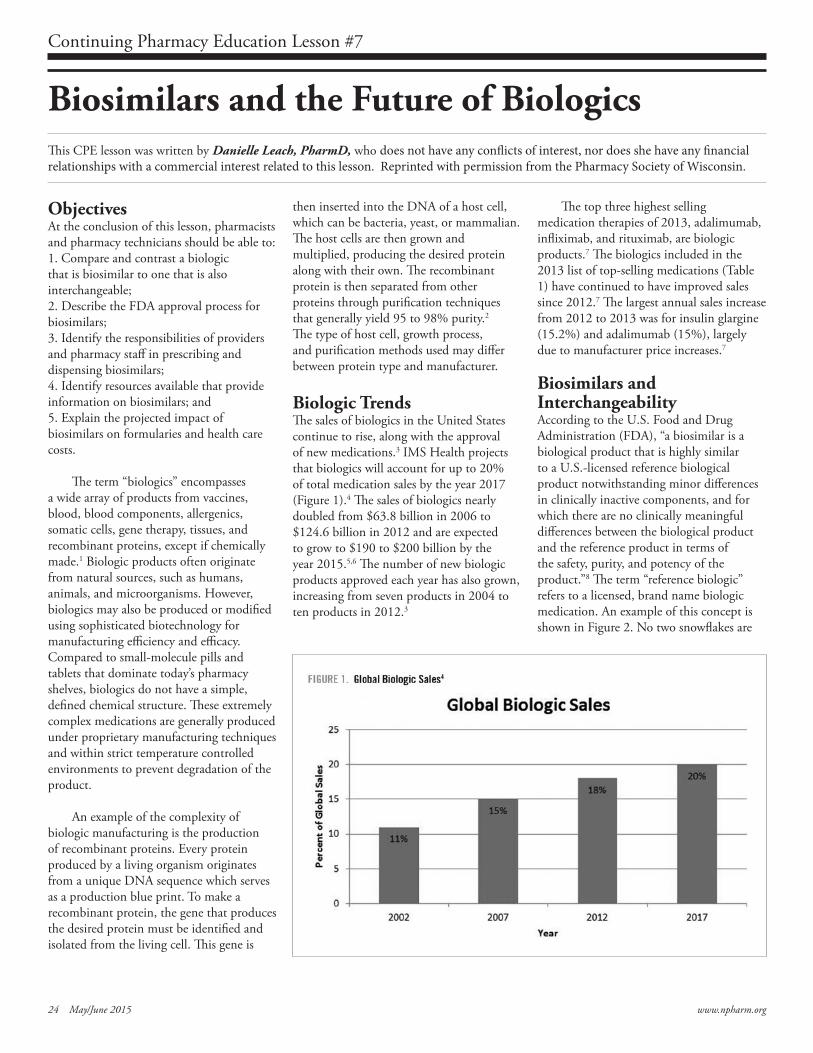
Biosimilars and the Future of BiologicsThis CPE lesson was written by Danielle Leach, PharmD, who does not have any conflicts of interest, nor does she have any financial relationships with a commercial interest related to this lesson. Reprinted with permission from the Pharmacy Society of Wisconsin.
ObjectivesAt the conclusion of this lesson, pharmacists and pharmacy technicians should be able to:1. Compare and contrast a biologic that is biosimilar to one that is also interchangeable;2. Describe the FDA approval process for biosimilars;3. Identify the responsibilities of providers and pharmacy staff in prescribing and dispensing biosimilars;4. Identify resources available that provide information on biosimilars; and5. Explain the projected impact of biosimilars on formularies and health care costs.
The term “biologics” encompasses a wide array of products from vaccines, blood, blood components, allergenics, somatic cells, gene therapy, tissues, and recombinant proteins, except if chemically made.1 Biologic products often originate from natural sources, such as humans, animals, and microorganisms. However, biologics may also be produced or modified using sophisticated biotechnology for manufacturing efficiency and efficacy. Compared to small-molecule pills and tablets that dominate today’s pharmacy shelves, biologics do not have a simple, defined chemical structure. These extremely complex medications are generally produced under proprietary manufacturing techniques and within strict temperature controlled environments to prevent degradation of the product.
An example of the complexity of biologic manufacturing is the production of recombinant proteins. Every protein produced by a living organism originates from a unique DNA sequence which serves as a production blue print. To make a recombinant protein, the gene that produces the desired protein must be identified and isolated from the living cell. This gene is
then inserted into the DNA of a host cell, which can be bacteria, yeast, or mammalian. The host cells are then grown and multiplied, producing the desired protein along with their own. The recombinant protein is then separated from other proteins through purification techniques that generally yield 95 to 98% purity.2 The type of host cell, growth process, and purification methods used may differ between protein type and manufacturer.
Biologic TrendsThe sales of biologics in the United States continue to rise, along with the approval of new medications.3 IMS Health projects that biologics will account for up to 20% of total medication sales by the year 2017 (Figure 1).4 The sales of biologics nearly doubled from $63.8 billion in 2006 to $124.6 billion in 2012 and are expected to grow to $190 to $200 billion by the year 2015.5,6 The number of new biologic products approved each year has also grown, increasing from seven products in 2004 to ten products in 2012.3
The top three highest selling medication therapies of 2013, adalimumab, infliximab, and rituximab, are biologic products.7 The biologics included in the 2013 list of top-selling medications (Table 1) have continued to have improved sales since 2012.7 The largest annual sales increase from 2012 to 2013 was for insulin glargine (15.2%) and adalimumab (15%), largely due to manufacturer price increases.7
Biosimilars and InterchangeabilityAccording to the U.S. Food and Drug Administration (FDA), “a biosimilar is a biological product that is highly similar to a U.S.-licensed reference biological product notwithstanding minor differences in clinically inactive components, and for which there are no clinically meaningful differences between the biological product and the reference product in terms of the safety, purity, and potency of the product.”8 The term “reference biologic” refers to a licensed, brand name biologic medication. An example of this concept is shown in Figure 2. No two snowflakes are
Continuing Pharmacy Education Lesson #7
24 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 25
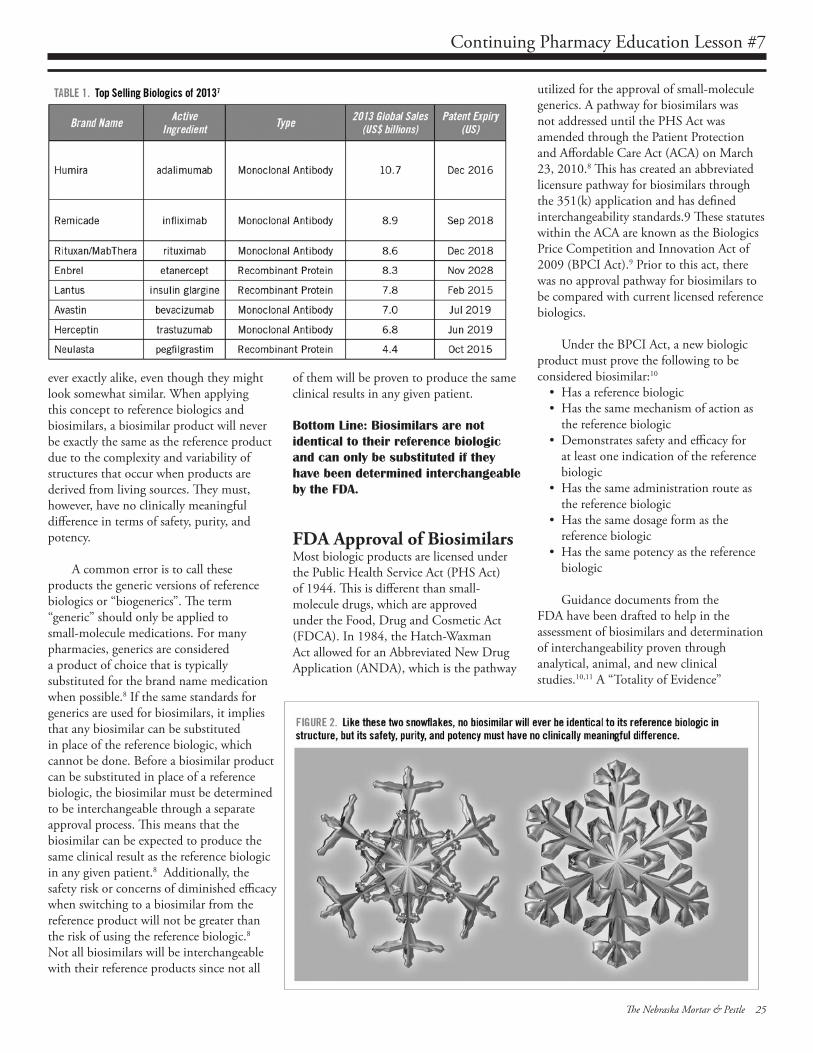
Continuing Pharmacy Education Lesson #7
ever exactly alike, even though they might look somewhat similar. When applying this concept to reference biologics and biosimilars, a biosimilar product will never be exactly the same as the reference product due to the complexity and variability of structures that occur when products are derived from living sources. They must, however, have no clinically meaningful difference in terms of safety, purity, and potency.
A common error is to call these products the generic versions of reference biologics or “biogenerics”. The term “generic” should only be applied to small-molecule medications. For many pharmacies, generics are considered a product of choice that is typically substituted for the brand name medication when possible.8 If the same standards for generics are used for biosimilars, it implies that any biosimilar can be substituted in place of the reference biologic, which cannot be done. Before a biosimilar product can be substituted in place of a reference biologic, the biosimilar must be determined to be interchangeable through a separate approval process. This means that the biosimilar can be expected to produce the same clinical result as the reference biologic in any given patient.8 Additionally, the safety risk or concerns of diminished efficacy when switching to a biosimilar from the reference product will not be greater than the risk of using the reference biologic.8 Not all biosimilars will be interchangeable with their reference products since not all
of them will be proven to produce the same clinical results in any given patient.
Bottom Line: Biosimilars are not identical to their reference biologic and can only be substituted if they have been determined interchangeable by the FDA.
FDA Approval of BiosimilarsMost biologic products are licensed under the Public Health Service Act (PHS Act) of 1944. This is different than small-molecule drugs, which are approved under the Food, Drug and Cosmetic Act (FDCA). In 1984, the Hatch-Waxman Act allowed for an Abbreviated New Drug Application (ANDA), which is the pathway
utilized for the approval of small-molecule generics. A pathway for biosimilars was not addressed until the PHS Act was amended through the Patient Protection and Affordable Care Act (ACA) on March 23, 2010.8 This has created an abbreviated licensure pathway for biosimilars through the 351(k) application and has defined interchangeability standards.9 These statutes within the ACA are known as the Biologics Price Competition and Innovation Act of 2009 (BPCI Act).9 Prior to this act, there was no approval pathway for biosimilars to be compared with current licensed reference biologics.
Under the BPCI Act, a new biologic product must prove the following to be considered biosimilar:10
• Has a reference biologic • Has the same mechanism of action as
the reference biologic• Demonstrates safety and efficacy for
at least one indication of the reference biologic
• Has the same administration route as the reference biologic
• Has the same dosage form as the reference biologic
• Has the same potency as the reference biologic
Guidance documents from the FDA have been drafted to help in the assessment of biosimilars and determination of interchangeability proven through analytical, animal, and new clinical studies.10,11 A “Totality of Evidence”
24 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 25
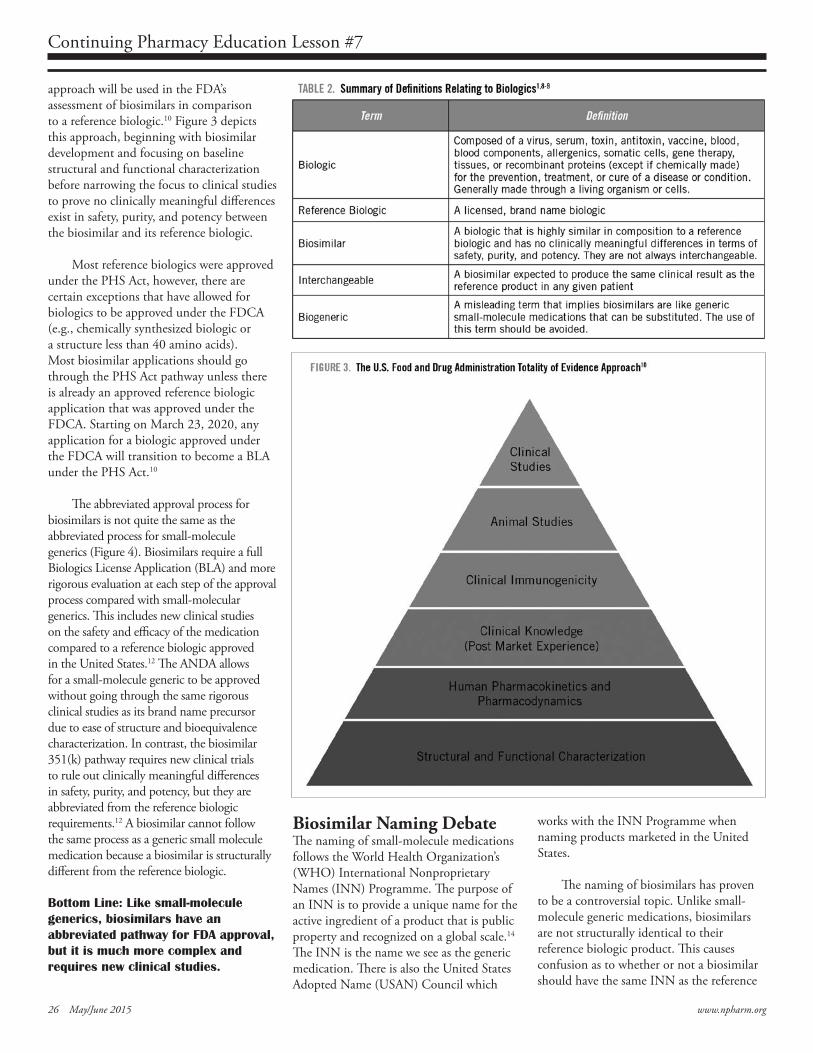
Continuing Pharmacy Education Lesson #7
approach will be used in the FDA’s assessment of biosimilars in comparison to a reference biologic.10 Figure 3 depicts this approach, beginning with biosimilar development and focusing on baseline structural and functional characterization before narrowing the focus to clinical studies to prove no clinically meaningful differences exist in safety, purity, and potency between the biosimilar and its reference biologic.
Most reference biologics were approved under the PHS Act, however, there are certain exceptions that have allowed for biologics to be approved under the FDCA (e.g., chemically synthesized biologic or a structure less than 40 amino acids). Most biosimilar applications should go through the PHS Act pathway unless there is already an approved reference biologic application that was approved under the FDCA. Starting on March 23, 2020, any application for a biologic approved under the FDCA will transition to become a BLA under the PHS Act.10
The abbreviated approval process for biosimilars is not quite the same as the abbreviated process for small-molecule generics (Figure 4). Biosimilars require a full Biologics License Application (BLA) and more rigorous evaluation at each step of the approval process compared with small-molecular generics. This includes new clinical studies on the safety and efficacy of the medication compared to a reference biologic approved in the United States.12 The ANDA allows for a small-molecule generic to be approved without going through the same rigorous clinical studies as its brand name precursor due to ease of structure and bioequivalence characterization. In contrast, the biosimilar 351(k) pathway requires new clinical trials to rule out clinically meaningful differences in safety, purity, and potency, but they are abbreviated from the reference biologic requirements.12 A biosimilar cannot follow the same process as a generic small molecule medication because a biosimilar is structurally different from the reference biologic.
Bottom Line: Like small-molecule generics, biosimilars have an abbreviated pathway for FDA approval, but it is much more complex and requires new clinical studies.
Biosimilar Naming DebateThe naming of small-molecule medications follows the World Health Organization’s (WHO) International Nonproprietary Names (INN) Programme. The purpose of an INN is to provide a unique name for the active ingredient of a product that is public property and recognized on a global scale.14 The INN is the name we see as the generic medication. There is also the United States Adopted Name (USAN) Council which
works with the INN Programme when naming products marketed in the United States.
The naming of biosimilars has proven to be a controversial topic. Unlike small-molecule generic medications, biosimilars are not structurally identical to their reference biologic product. This causes confusion as to whether or not a biosimilar should have the same INN as the reference
26 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 27
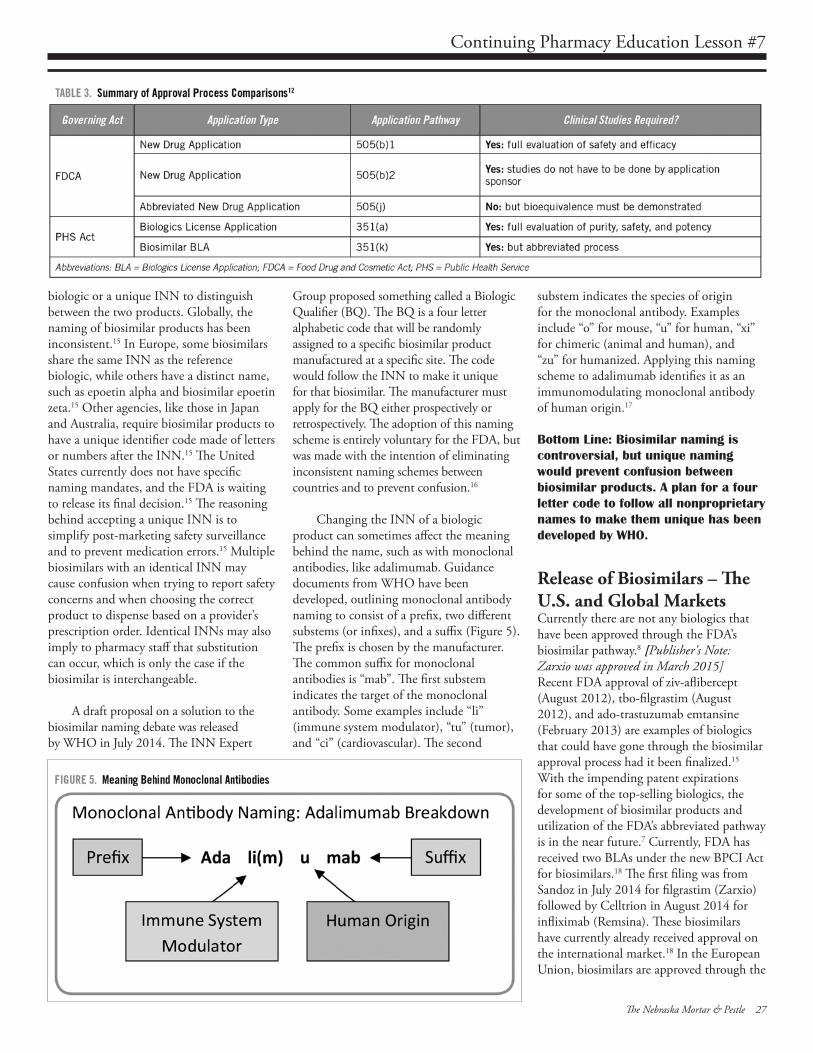
Continuing Pharmacy Education Lesson #7
biologic or a unique INN to distinguish between the two products. Globally, the naming of biosimilar products has been inconsistent.15 In Europe, some biosimilars share the same INN as the reference biologic, while others have a distinct name, such as epoetin alpha and biosimilar epoetin zeta.15 Other agencies, like those in Japan and Australia, require biosimilar products to have a unique identifier code made of letters or numbers after the INN.15 The United States currently does not have specific naming mandates, and the FDA is waiting to release its final decision.15 The reasoning behind accepting a unique INN is to simplify post-marketing safety surveillance and to prevent medication errors.15 Multiple biosimilars with an identical INN may cause confusion when trying to report safety concerns and when choosing the correct product to dispense based on a provider’s prescription order. Identical INNs may also imply to pharmacy staff that substitution can occur, which is only the case if the biosimilar is interchangeable.
A draft proposal on a solution to the biosimilar naming debate was released by WHO in July 2014. The INN Expert
Group proposed something called a Biologic Qualifier (BQ). The BQ is a four letter alphabetic code that will be randomly assigned to a specific biosimilar product manufactured at a specific site. The code would follow the INN to make it unique for that biosimilar. The manufacturer must apply for the BQ either prospectively or retrospectively. The adoption of this naming scheme is entirely voluntary for the FDA, but was made with the intention of eliminating inconsistent naming schemes between countries and to prevent confusion.16
Changing the INN of a biologic product can sometimes affect the meaning behind the name, such as with monoclonal antibodies, like adalimumab. Guidance documents from WHO have been developed, outlining monoclonal antibody naming to consist of a prefix, two different substems (or infixes), and a suffix (Figure 5). The prefix is chosen by the manufacturer. The common suffix for monoclonal antibodies is “mab”. The first substem indicates the target of the monoclonal antibody. Some examples include “li” (immune system modulator), “tu” (tumor), and “ci” (cardiovascular). The second
substem indicates the species of origin for the monoclonal antibody. Examples include “o” for mouse, “u” for human, “xi” for chimeric (animal and human), and “zu” for humanized. Applying this naming scheme to adalimumab identifies it as an immunomodulating monoclonal antibody of human origin.17
Bottom Line: Biosimilar naming is controversial, but unique naming would prevent confusion between biosimilar products. A plan for a four letter code to follow all nonproprietary names to make them unique has been developed by WHO.
Release of Biosimilars – The U.S. and Global MarketsCurrently there are not any biologics that have been approved through the FDA’s biosimilar pathway.8 [Publisher's Note: Zarxio was approved in March 2015] Recent FDA approval of ziv-aflibercept (August 2012), tbo-filgrastim (August 2012), and ado-trastuzumab emtansine (February 2013) are examples of biologics that could have gone through the biosimilar approval process had it been finalized.15 With the impending patent expirations for some of the top-selling biologics, the development of biosimilar products and utilization of the FDA’s abbreviated pathway is in the near future.7 Currently, FDA has received two BLAs under the new BPCI Act for biosimilars.18 The first filing was from Sandoz in July 2014 for filgrastim (Zarxio) followed by Celltrion in August 2014 for infliximab (Remsina). These biosimilars have currently already received approval on the international market.18 In the European Union, biosimilars are approved through the
26 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 27
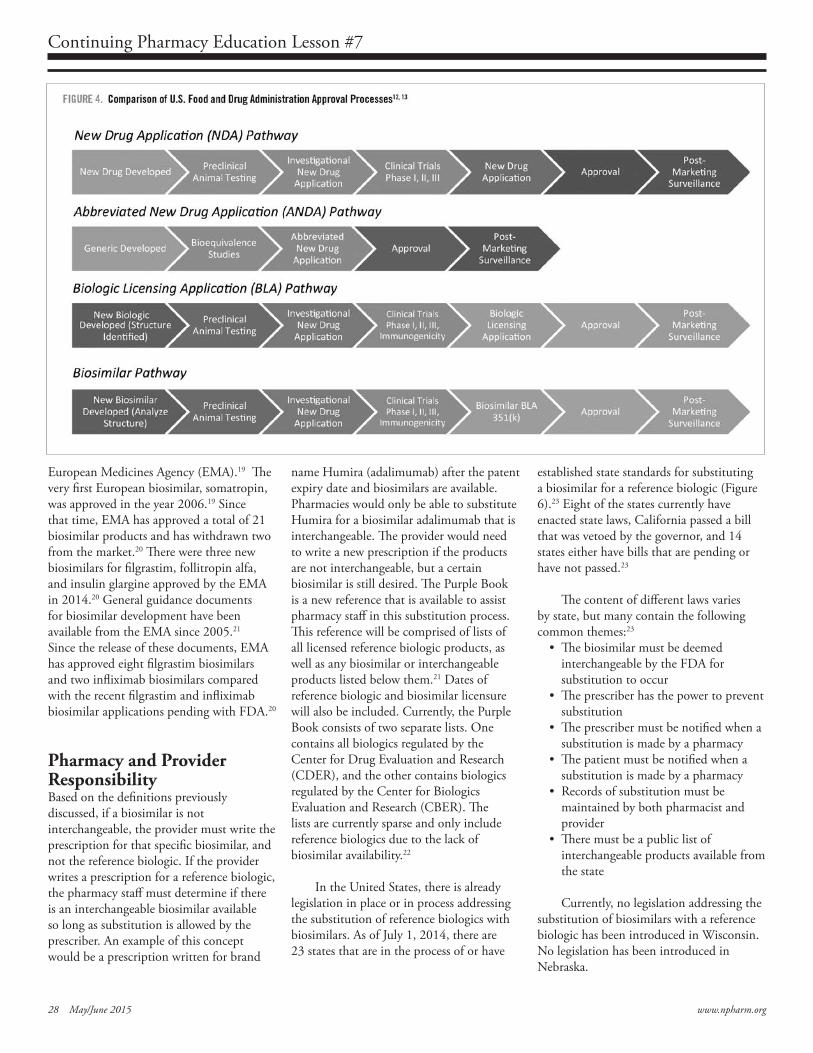
Continuing Pharmacy Education Lesson #7
European Medicines Agency (EMA).19 The very first European biosimilar, somatropin, was approved in the year 2006.19 Since that time, EMA has approved a total of 21 biosimilar products and has withdrawn two from the market.20 There were three new biosimilars for filgrastim, follitropin alfa, and insulin glargine approved by the EMA in 2014.20 General guidance documents for biosimilar development have been available from the EMA since 2005.21 Since the release of these documents, EMA has approved eight filgrastim biosimilars and two infliximab biosimilars compared with the recent filgrastim and infliximab biosimilar applications pending with FDA.20
Pharmacy and Provider ResponsibilityBased on the definitions previously discussed, if a biosimilar is not interchangeable, the provider must write the prescription for that specific biosimilar, and not the reference biologic. If the provider writes a prescription for a reference biologic, the pharmacy staff must determine if there is an interchangeable biosimilar available so long as substitution is allowed by the prescriber. An example of this concept would be a prescription written for brand
name Humira (adalimumab) after the patent expiry date and biosimilars are available. Pharmacies would only be able to substitute Humira for a biosimilar adalimumab that is interchangeable. The provider would need to write a new prescription if the products are not interchangeable, but a certain biosimilar is still desired. The Purple Book is a new reference that is available to assist pharmacy staff in this substitution process. This reference will be comprised of lists of all licensed reference biologic products, as well as any biosimilar or interchangeable products listed below them.21 Dates of reference biologic and biosimilar licensure will also be included. Currently, the Purple Book consists of two separate lists. One contains all biologics regulated by the Center for Drug Evaluation and Research (CDER), and the other contains biologics regulated by the Center for Biologics Evaluation and Research (CBER). The lists are currently sparse and only include reference biologics due to the lack of biosimilar availability.22
In the United States, there is already legislation in place or in process addressing the substitution of reference biologics with biosimilars. As of July 1, 2014, there are 23 states that are in the process of or have
established state standards for substituting a biosimilar for a reference biologic (Figure 6).23 Eight of the states currently have enacted state laws, California passed a bill that was vetoed by the governor, and 14 states either have bills that are pending or have not passed.23
The content of different laws varies by state, but many contain the following common themes:23
• The biosimilar must be deemed interchangeable by the FDA for substitution to occur
• The prescriber has the power to prevent substitution
• The prescriber must be notified when a substitution is made by a pharmacy
• The patient must be notified when a substitution is made by a pharmacy
• Records of substitution must be maintained by both pharmacist and provider
• There must be a public list of interchangeable products available from the state
Currently, no legislation addressing the substitution of biosimilars with a reference biologic has been introduced in Wisconsin. No legislation has been introduced in Nebraska.
28 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 29
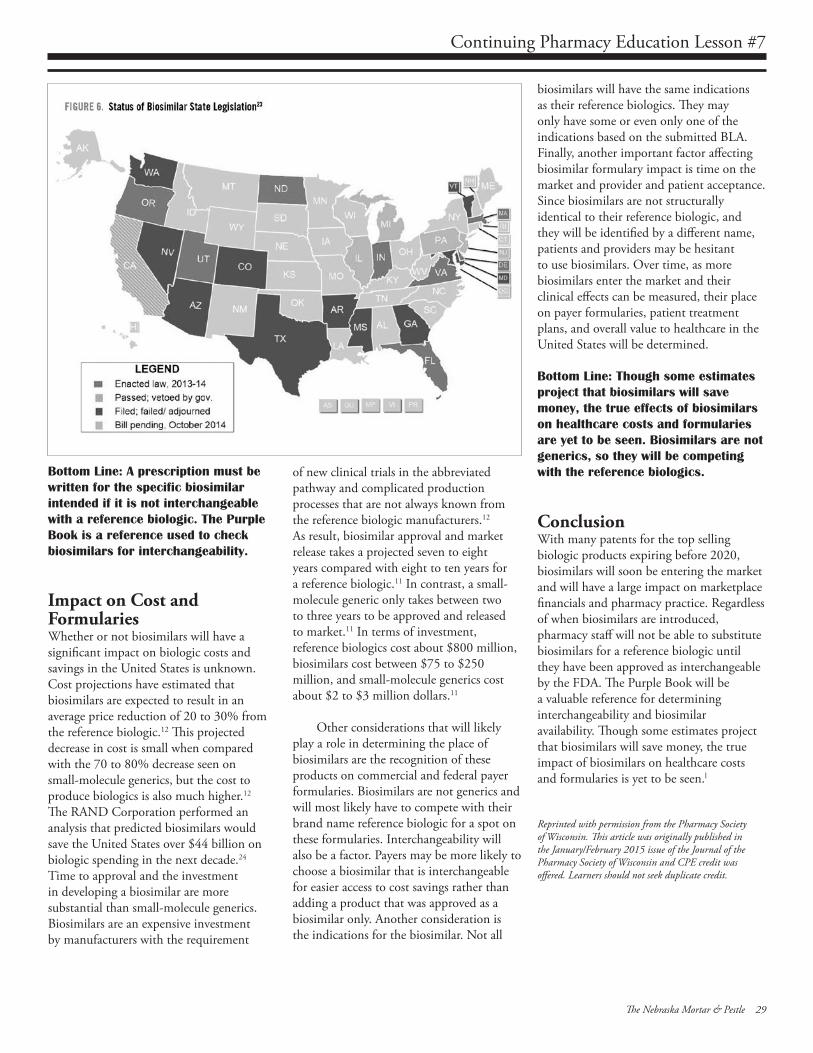
Continuing Pharmacy Education Lesson #7
Bottom Line: A prescription must be written for the specific biosimilar intended if it is not interchangeable with a reference biologic. The Purple Book is a reference used to check biosimilars for interchangeability.
Impact on Cost and FormulariesWhether or not biosimilars will have a significant impact on biologic costs and savings in the United States is unknown. Cost projections have estimated that biosimilars are expected to result in an average price reduction of 20 to 30% from the reference biologic.12 This projected decrease in cost is small when compared with the 70 to 80% decrease seen on small-molecule generics, but the cost to produce biologics is also much higher.12 The RAND Corporation performed an analysis that predicted biosimilars would save the United States over $44 billion on biologic spending in the next decade.24 Time to approval and the investment in developing a biosimilar are more substantial than small-molecule generics. Biosimilars are an expensive investment by manufacturers with the requirement
of new clinical trials in the abbreviated pathway and complicated production processes that are not always known from the reference biologic manufacturers.12 As result, biosimilar approval and market release takes a projected seven to eight years compared with eight to ten years for a reference biologic.11 In contrast, a small-molecule generic only takes between two to three years to be approved and released to market.11 In terms of investment, reference biologics cost about $800 million, biosimilars cost between $75 to $250 million, and small-molecule generics cost about $2 to $3 million dollars.11
Other considerations that will likely play a role in determining the place of biosimilars are the recognition of these products on commercial and federal payer formularies. Biosimilars are not generics and will most likely have to compete with their brand name reference biologic for a spot on these formularies. Interchangeability will also be a factor. Payers may be more likely to choose a biosimilar that is interchangeable for easier access to cost savings rather than adding a product that was approved as a biosimilar only. Another consideration is the indications for the biosimilar. Not all
biosimilars will have the same indications as their reference biologics. They may only have some or even only one of the indications based on the submitted BLA. Finally, another important factor affecting biosimilar formulary impact is time on the market and provider and patient acceptance. Since biosimilars are not structurally identical to their reference biologic, and they will be identified by a different name, patients and providers may be hesitant to use biosimilars. Over time, as more biosimilars enter the market and their clinical effects can be measured, their place on payer formularies, patient treatment plans, and overall value to healthcare in the United States will be determined.
Bottom Line: Though some estimates project that biosimilars will save money, the true effects of biosimilars on healthcare costs and formularies are yet to be seen. Biosimilars are not generics, so they will be competing with the reference biologics.
ConclusionWith many patents for the top selling biologic products expiring before 2020, biosimilars will soon be entering the market and will have a large impact on marketplace financials and pharmacy practice. Regardless of when biosimilars are introduced, pharmacy staff will not be able to substitute biosimilars for a reference biologic until they have been approved as interchangeable by the FDA. The Purple Book will be a valuable reference for determining interchangeability and biosimilar availability. Though some estimates project that biosimilars will save money, the true impact of biosimilars on healthcare costs and formularies is yet to be seen.l
Reprinted with permission from the Pharmacy Society of Wisconsin. This article was originally published in the January/February 2015 issue of the Journal of the Pharmacy Society of Wisconsin and CPE credit was offered. Learners should not seek duplicate credit.
28 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 29
Continuing Pharmacy Education Lesson #7
References1. The U.S. Food and Drug Administration.
What Are “Biologics” Questions and Answers. Updated April 14, 2009. http://www.fda.gov/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacco/CBER/ucm133077.htm. Accessed October 22, 2014.
2. Generic Pharmaceuticals Association. Manufacture and Characterization of Biologics and Biosimilars. Updated 2013. http://www.gphaonline.org/gpha-media/gpha-resources/manufacture-and-characterization-of-biologics-and-biosimilars. Accessed October 29, 2014.
3. Dalzell M. In 5 years, >50% of top-selling drugs will be biologics. Managed Care. Posted October 2013. http://www.managedcaremag.com/archives/2013/10/5-years-50-top-selling-drugs-will-be-biologics. Accessed October 22, 2014.
4. IMS Health. The Global Use of Medicines Outlook through 2017. September 2013. http://www.imshealth.com/deployedfiles/imshealth/Global/Content/Corporate/IMS%20Health%20Institute/Reports/Global_Use_of_Meds_Outlook_2017/Biologics_Market.pdf. Accessed October 22, 2014.
5. GaBi Online. Biologicals sales have almost doubled since 2006. Posted July 6, 2013. http://www.gabionline.net/Biosimilars/General/Biologicals-sales-have-almost-doubled-since-2006. Accessed October 22, 2014.
6. Amgen. Trends in Biologic Medicine Report. Thousand Oaks, CA: Amgen Inc.; 2013.
7. GaBi Online. Top 8 blockbuster biologicals 2013. Posted June 6, 2014. http://www.gabionline.net/Biosimilars/General/Top-8-blockbuster-biologicals-2013. Accessed October 22, 2014.
8. The U.S. Food and Drug Administration. Information for Consumers (Biosimilars). Updated September 9, 2014. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/ucm241718.htm. Accessed October 22, 2014.
9. The U.S. Food and Drug Administration. Information for Healthcare Professionals (Biosimilars). Updated September 9, 2014. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/ucm241719.htm. Accessed October 22, 2014.
10. Sherman RE. Biosimilar Biologic Products: Biosimilar Guidance Webinar. U.S. Food and Drug Administration. February 15, 2012. http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/UCM292463.pdf. Accessed October 22, 2014.
11. U.S. Food and Drug Administration. Guidance for Industry: Quality Considerations in Demonstrating Biosimilarity to a Reference Protein Product. February 2012. http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm291134.pdf. Accessed October 22, 2014.
12. Lucio SD, Stevenson JG, Hoffman JM. Biosimilars: implications for health-system pharmacists. Am J Health-Syst Pharm. 2013;70(22):2004-2017.
13. U.S. Food and Drug Administration. Drug Approval Process. http://www.fda.gov/downloads/Drugs/ResourcesForYou/Consumers/UCM284393.pdf. Accessed October 22, 2014.
14. World Health Organization. International Nonproprietary Names. http://www.who.int/medicines/services/inn/en/. Accessed November 12, 2014.
15. Alexander EA. The biosimilar name debate: what’s at stake for public health. GaBI Journal. 2014;3(1):10-12.
16. World Health Organization. Biologic qualifier: an INN proposal. Revised July 2014. http://www.who.int/medicines/services/inn/bq_innproposal201407.pdf?ua=1. Accessed November 12, 2014.
17. World Health Organization. International Nonproprietary Names (INN) for Biological and Biotechnological Substances: A Review. Update 2011. http://www.who.int/medicines/services/inn/BioRev2011.pdf. Accessed November 12, 2014.
18. Gaffney A. FDA Receives First-Ever Biosimilar Application for Monoclonal Antibody. Regulatory Affairs Professionals Society. Posted August 11, 2014. http://www.raps.org/Regulatory-Focus/News/2014/08/11/20001/FDA-Receives-First-Ever-Biosimilar-Application-for-Monoclonal-Antibody/. Accessed November 12, 2014.
19. GaBi Online. Biosimilars Approved in Europe. Updated 10/17/2014. http://www.gabionline.net/Biosimilars/General/Biosimilars-approved-in-Europe. Accessed November 12, 2014.
20. European Medicines Agency. European Public Assessment Reports. Updated September 2014. http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/landing/epar_search.jsp&mid=WC0b01ac058001d125. Accessed November 12, 2014.
21. European Medicines Agency. Overarching Biosimilar Guidelines. Updated September 2014. http://www.ema.europa.eu/ema/index.jsp?curl=pages/regulation/general/general_content_000408.jsp#Overarchingbiosimilarguidelines. Accessed November 22, 2014.
22. The U.S. Food and Drug Administration. Purple Book: Lists of Licensed Biological Products with Reference Product Exclusivity and Biosimilarity or Interchangeability Evaluations. Updated October 1, 2014. http://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeuticbiologicapplications/biosimilars/ucm411418.htm. Accessed October 22, 2014.
23. National Conference of State Legislatures. State Laws and Legislation Related to Biologic Medications and Substitution of Biosimilars. Posted July 1, 2014. http://www.ncsl.org/documents/health/Biologics_BiosimilarsNCSLReport_July_2014.pdf. Accessed October 22, 2014.
24. Mulcahy AW. Biosimilar Medications Could Create Billions in Health Care Savings. RAND Corporation. Posted November 3, 2014. http://www.rand.org/news/press/2014/11/03.html. Accessed November 13, 2014.
30 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 31
Policies for the Nebraska Mortar & Pestle (M&P) continuing pharmacy education lessons and quizzes:
1. M&P Quizzes are valid only for the membership year in which they are published. Quizzes for the 2015 Membership Year must be received by December 7, 2015. Quizzes cannot be carried over to another membership year.
2. If more than three questions are missed, the quiz will be returned. The quiz can be resubmitted.
3. CPE transcripts can be printed from NABP e-Profiles at www.nabp.net.
4. CPE credits are submitted to NABP by the 15th of each month. For example, M&P CPE quizzes completed in the month of August 2015, will be sent to NABP e-Profiles before September 15, 2015.
The Nebraska Council for Continuing Pharmacy Education (NCCPE) is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education (CPE).This CPE home study lesson has been accredited for 1.0 contact hour or 0.10 CEU. UAN #0128-0000-15-296-H03-P for pharmacists and #0128-0000-15-296-H03-T for pharmacy technicians. This lesson is a knowledge-based CPE activity targeted to pharmacists and pharmacy technicians.
The authors and the Nebraska Pharmacists Association disclaim any liability to you or your patients resulting from reliance solely upon the information contained herein.
Quiz Answers may be submitted:1. Online: www.npharm.org
2. Fax: 402-420-1406
3. Email: m&[email protected]
4. Mail: NPA Mortar & Pestle 6221 S 58th St, Ste A Lincoln, NE 68516

Biosimilars and the Future of BiologicsQuiz #7, May/June 2015, ACPE #0128-0000-15-296-H03-P/T
2015 Quiz #7 - NPA CPE Home Study Answer FormBiosimilars and the Future of Biologics
UAN #0128-0000-15-296-H03-P for pharmacistsUAN #0128-0000-15-296-H03-T for technicians
1.0 Contact Hour - Knowledge Based CPE Activity
Name ________________________________________________________
Mailing Address _______________________________________________
City/State/Zip _________________________________________________
*NABP e-Profile # ______________ *Date of Birth (MMDD) _________*Required for ACPE credit.
Circle one (1) Answer:1. a b c d 5. a b c d2. a b c d 6. a b 3. a b 7. a b c d4. a b c d 8. a b
CPE Home Study Evaluation 1. Rate this lesson: (Excellent) 5 4 3 2 1 (Poor)
2. Did this lesson meet each of its objectives? ___ Yes ___ No3. Was the content without commercial bias? ___ Yes ___ No 4. Did the lesson meet your educational/practice needs? ___ Yes ___ No5. Comments/future topics are welcome. ________________________
The deadline for this quiz is December 7, 2015
Keep the TOP portion for your records. Return the BOTTOM portion to the NPA office.Or, take this quiz online at www.npharm.org
1. Which term matches the definition: “A biosimilar expected to produce the same clinical results as the reference product in ANY given patient.”
a. Biogeneric b. Biosimilar c. Interchangeable d. Reference Biologic
2. Which term matches the definition: “A biologic highly similar to a reference biologic with no clinically meaningful differences in terms of safety, purity, and potency, but is not proven to have the same clinical results in every patient.”
a. Biogeneric b. Biosimilar c. Interchangeable d. Reference Biologic
3. True or False. The new abbreviated biosimilar BLA pathway is just as fast as the ANDA pathway for small-molecule generics because clinical trials are not necessary for approval.
a. True b. False
4. Biosimilars must demonstrate what characteristic(s) for approval with a BLA?
a. Different dosage form than the reference biologic b. Same administration route as the reference biologic c. Same efficacy for at least one indication of the
reference biologic d. Both B and C
Continuing Pharmacy Education Quiz #7
5. In terms of interchangeability, which of the following are acceptable?
a. A provider writes a prescription for a reference biologic, assuming that any biosimilar will be substituted
b. An interchangeable biosimilar is substituted for a prescription written for its reference biologic
c. One biosimilar is substituted for a prescription written for a different biosimilar
d. None of the above
6. True or False. If a provider writes a prescription for a brand name biologic, any biosimilar can be substituted because it has the exact same active ingredient.
a. True b. False
7. Which of the following are available biosimilar resources?
a. Biotechnology Industry Organization b. The FDA website c. The Purple Book d. All of the above
8. True or False. Though projections have been made, the true effects of biosimilars on formularies and healthcare costs remains to be seen.
a. True b. False
30 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 31
32 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 33
The Holland Performing Arts Center was the venue for the 2015 Scholastic Honors Convocation on May 8. Fifty-six seniors were vested with their doctoral hoods and took the Pharmacistʼs Oath. Senior recognition awards and the 2015 Preceptor and Site of the Year Awards were also presented at the Convocation. Spring Commencement was held at the Ralston Arena May 9. The 2015 graduates and senior award recipients are presented below and on the following page.
Spring 2015 Honors Convocation and Commencement
2015 Doctor of Pharmacy Degree Recipients
Ashley Austin, OmahaDaniel Bailey, Boulder, COTara Bergland, Treynor, IAJoshua Blood, BeatriceElizabeth Brabec, WayneBrice Buryanek, Hawarden, IADavid Cawthorn, ElkhornCarolyn Corn, Omaha
with distinctionSylvia Dang, Rosemead, CAZhan Ge, Sheffield, IANolan Hannan, WahooSloane Hartzell, HallamDeeko Hassan, Rochester, MNChet Hellbusch, ColumbusKayla Hoelting, LawrenceYimei Huang, Chengdu, ChinaMegan Irlmeier, Exira, IACaroline Jamison, Arlington
with distinctionKatrina Keebler, SterlingJessica Kehm, Grand Island
Michael Keiser, GothenburgJustin Lane, Auburn
with high distinctionHien Le, LincolnAndrew Lemke, St. PaulCody Lobeda, AuroraMichelle Mahr, SidneyRichard Marlatt, GordonAmy Mayer, ElkhornMarissa McMahon, PalmyraKhalid Mohamed, Ethiopia Ban Mohammed, LincolnDaralyn Morgenson, Louisville
with high distinction Kelsey Morris, LincolnJoseph Nekola, RalstonOlivia Nguyen, LincolnSarah Paasch, Elkhorn
with distinctionCassandra Pauley, Panama, IACharleen Phan, LincolnEmily Prinz, West Point
with distinction
Amanda Reinhardt, CambridgeAndrea Scheiblhofer, LincolnAshley Schenk, Prague
with high distinction Caci Schulte, Blair
with distinction Jenalee Schwab, Hampton, IA Drew Smith, MilburnHannah Snyder, Yutan Cory Sueper, Humphrey Amanda Summers, AuburnVan Tran, Lincoln Philip Van De Velde, Papillion
with distinction Amanda Voigt, Topeka, KS Jenna Waters, Lincoln Stephanie Wetovick, Kearney
with distinction Lance Wilson, GrantJenna Woods, Omaha Li Yin, Rowland Heights, CA

32 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 33
2015 Senior Award Recipients Rho Chi Achievement Award
Philip Van De Velde
Phi Lambda Sigma Award Kelsey Morris
Merck Pharmaceutics Award Ashley Schenk
Merck Medicinal Chemistry Award Justin Lane
Cunningham Memorial Award in Pharmacodynamics
Emily Prinz
Mylan Pharmaceuticals Award Justin Lane
Barbara Osborne Manchester Award Jenalee Schwab
Eli Lilly Achievement Award Michael Keiser
Teva Pharmaceuticals Outstanding Student Award Nolan Hannan
Facts and Comparisons Award of Excellence in Clinical Communication
Carolyn Corn
Joseph B. Burt Memorial Award Caroline Jamison
Phyllis Rhodes Award Daralyn Morgenson
Academy of Students of Pharmacy Certificate of Recognition Award
Kelsey Morris
Varro and Virginia Tyler Award Ashley Schenk
Stephen A. Scholtz Memorial Award Tara Bergland
Bradley G. Wulf Memorial Award Caci Schulte
Pharmacist Mutual Insurance Company Award Sarah Paasch
Excellence in Advanced Practice Experience Recognition
Caroline Jamison Michelle Mahr
Patient Care Champion Award Yimei Huang Emily Prinz
2015 Preceptors of the Year
UNMC College of Pharmacy annually recognizes a preceptor for their outstanding contributions toward the professional development of future pharmacists. This year it is with great honor that we recognize Joy Beranek and Staci Hubert for their contributions and commitment to excellence.
Drs. Beranek, ʼ07 and Hubert, ʼ94, both graduates from the College of Pharmacy, work at Ashland Pharmacy, and have continued to promote and advance the pharmacy profession by giving back and mentoring student pharmacists at their site.
The P4 class takes nominations and votes on the Preceptor of the Year.The following comments are just a few reasons why Drs. Beranek and Hubert were selected for this award. They provided free lunch. Thatʼs
enough to make pharmacy students love you.
They allowed students to jump right in to the practice as a licensed professional. They were open to students learning the system their pharmacy uses, providing cognitive services and providing services such as blood pressure readings.
Students were able to spend time in both retail and compounding pharmacy for a very unique pharmacy experience.
Both pharmacists have such a positive attitude and are not easily frustrated when a student makes a mistake.
They provide amazing continuity of care to their patients and put all of the concerns of their patients first. Their patients seem to enjoy coming into the pharmacy and are comfortable asking questions about their medications.
Congratulations Drs. Beranek and Hubert!
The Site of the Year was also presented at the ceremony. This award, established by the class of 2015, was created to help promote the interdisciplinary approach to health care outside the Nebraska Medicine system. With site experiences such as multidisciplinary rounds, shadowing and daily interaction with other health care professionals, interactions are not just limited to preceptors alone. They include a team of professionals, and this award recognizes the team. This yearʼs recipient was awarded to the Grand Island Veterans Affairs Ambulatory Care rotation, lead by Drs. Lourdes Heuermann, Lisa Bilslend,
Brent Bollwitt, and Paula Carlson. One of the P4 students said in their nomination, “It wasnʼt just one preceptor that made this rotation great. It was all of the preceptors in combination with meeting the great veterans there.”
Congratulations Grand Island Veterans Affairs clerkship!
Dr. Fletcher (left) and P4 Class President, Carolyn Jamison (right), pictured with Preceptors of the Year (top) and Site of the Year recipients

34 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 35
A Buying group for independent retAil phArmAcies
...owned by 19 state pharmacy organizations...a leader negotiating on behalf of independents
...saving pharmacies money for more than 25 years...financially supports the state pharmacy organizations
...serving pharmacies nationwide
1-888-200-0998 | www.pacealliance.com
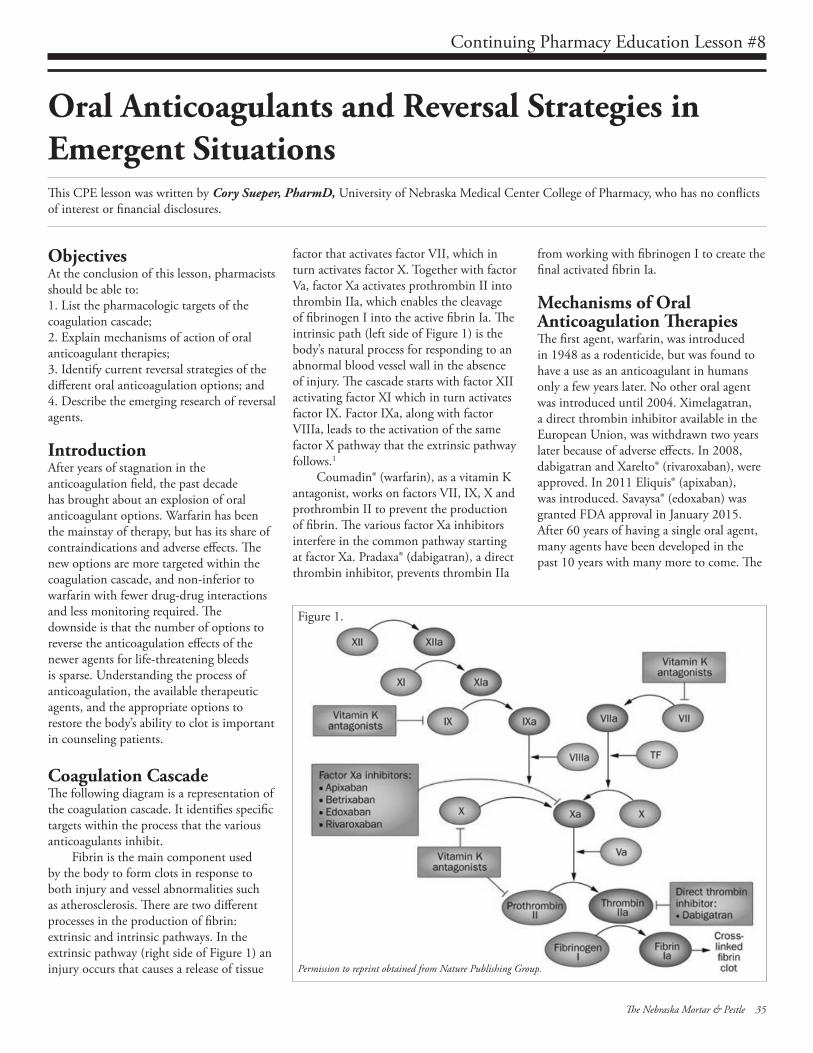
ObjectivesAt the conclusion of this lesson, pharmacists should be able to:1. List the pharmacologic targets of the coagulation cascade;2. Explain mechanisms of action of oral anticoagulant therapies;3. Identify current reversal strategies of the different oral anticoagulation options; and 4. Describe the emerging research of reversal agents.
IntroductionAfter years of stagnation in the anticoagulation field, the past decade has brought about an explosion of oral anticoagulant options. Warfarin has been the mainstay of therapy, but has its share of contraindications and adverse effects. The new options are more targeted within the coagulation cascade, and non-inferior to warfarin with fewer drug-drug interactions and less monitoring required. The downside is that the number of options to reverse the anticoagulation effects of the newer agents for life-threatening bleeds is sparse. Understanding the process of anticoagulation, the available therapeutic agents, and the appropriate options to restore the body’s ability to clot is important in counseling patients.
Coagulation CascadeThe following diagram is a representation of the coagulation cascade. It identifies specific targets within the process that the various anticoagulants inhibit.
Fibrin is the main component used by the body to form clots in response to both injury and vessel abnormalities such as atherosclerosis. There are two different processes in the production of fibrin: extrinsic and intrinsic pathways. In the extrinsic pathway (right side of Figure 1) an injury occurs that causes a release of tissue
Oral Anticoagulants and Reversal Strategies in Emergent Situations
factor that activates factor VII, which in turn activates factor X. Together with factor Va, factor Xa activates prothrombin II into thrombin IIa, which enables the cleavage of fibrinogen I into the active fibrin Ia. The intrinsic path (left side of Figure 1) is the body’s natural process for responding to an abnormal blood vessel wall in the absence of injury. The cascade starts with factor XII activating factor XI which in turn activates factor IX. Factor IXa, along with factor VIIIa, leads to the activation of the same factor X pathway that the extrinsic pathway follows.1
Coumadin® (warfarin), as a vitamin K antagonist, works on factors VII, IX, X and prothrombin II to prevent the production of fibrin. The various factor Xa inhibitors interfere in the common pathway starting at factor Xa. Pradaxa® (dabigatran), a direct thrombin inhibitor, prevents thrombin IIa
from working with fibrinogen I to create the final activated fibrin Ia.
Mechanisms of Oral Anticoagulation TherapiesThe first agent, warfarin, was introduced in 1948 as a rodenticide, but was found to have a use as an anticoagulant in humans only a few years later. No other oral agent was introduced until 2004. Ximelagatran, a direct thrombin inhibitor available in the European Union, was withdrawn two years later because of adverse effects. In 2008, dabigatran and Xarelto® (rivaroxaban), were approved. In 2011 Eliquis® (apixaban), was introduced. Savaysa® (edoxaban) was granted FDA approval in January 2015. After 60 years of having a single oral agent, many agents have been developed in the past 10 years with many more to come. The
This CPE lesson was written by Cory Sueper, PharmD, University of Nebraska Medical Center College of Pharmacy, who has no conflicts of interest or financial disclosures.
Permission to reprint obtained from Nature Publishing Group.
Figure 1.
34 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 35
Continuing Pharmacy Education Lesson #8

introduction of novel anticoagulants, with their targeted action, has brought about the need for more focused and specific reversal agents.
WarfarinWarfarin, a coumarin, is a vitamin K antagonist that interferes with the cyclic inter-conversion of vitamin K for its coagulant effect. Vitamin K is a cofactor in the coagulation cascade of factors II, VII, IX, and X, and is required for their biological activity. Without vitamin K, the coagulant factors produced by the liver have reduced procoagulant activity. Warfarin also can have potential procoagulant effects because of its inhibitory effects on proteins C and S, which are natural anticoagulants. Warfarin’s approved indications include prophylaxis in patients undergoing surgery, prevention of systemic embolism in patients with heart valve replacement, valvular heart disease, atrial fibrillation and acute myocardial infarction, and treatment of venous thromboembolism and pulmonary embolism.2
In patients on anticoagulant therapy with warfarin who require immediate surgery or in cases of life threatening blood loss, the following strategies are recommended to reverse warfarin activity:
• Based on clinical trial data, it is recommended to give vitamin K doses of 5 to 10 mg by slow IV infusion and repeat the dose after 12 hours if needed.
• The drug, Kcentra®, is the recommended agent for reversal of vitamin K antagonists in emergent situations, and may be administered on an INR- dependent basis. If a patient’s INR is greater than 6, a dose of 50 units per kg with a max of 5000 units as a one-time dose is recommended. An INR range of 4 to 6 warrants a dose of 35 units per kg with a max of 3500 units and a dose of 25 units per kg with a max of 2500 units is indicated with an INR of 2 to 4. If Kcentra is contraindicated, consider a frozen plasma dose of 1 to 2 units, depending on urgency, up to 20 ml per kg and repeat every 6-12 hours as needed.
• In the case of a patient who objects to receiving blood products, consider the drug Novoseven, which contains no blood products, at 20 mcg per kg as a one-time dose.3
DabigatranDabigatran is a direct inhibitor of both free and clot-bound thrombin. Inhibition of thrombin prevents the conversion of fibrinogen to fibrin; the final product of the coagulation cascade that forms the thrombus at the site of injury. Because this drug is more targeted, it provides a more predictable anticoagulation response and does not require routine monitoring or dose adjustment for anticoagulation. Dabigatran has approved indications for the prevention of stroke and systemic embolism in non-valvular atrial fibrillation, and treatment (after 5-10 days of parenteral anticoagulation) and prevention of distal venous thromboembolism and pulmonary embolism.4
In patients on dabigatran who require immediate surgery or in cases of life-threatening blood loss, the following strategies are recommended to reverse the drug’s activity:
• If ingested within the past two hours, administer activated charcoal to prevent new drug from entering systemic circulation.
• Although considered off-label and not FDA approved, the drug factor VIII inhibitor bypassing activity (FEIBA) can be considered as a reversal agent. When treating patients with intracranial hemorrhage, the recommended dose is 50 units per kg with a max of 5000 units as a one-time dose. A non-intracranial hemorrhage dose is 25 units per kg with a max of 2500 units as a one-time dose.
• If the situation is not time sensitive and patient is hemodynamically stable, hemodialysis can be considered and will achieve about 60 percent removal from the body.3
RivaroxabanRivaroxaban is a selective inhibitor of factor Xa blocking the major step in the coagulation cascade in the production of fibrin. As a targeted drug that provides a predictable and specific anticoagulation response, rivaroxaban does not need routine monitoring, but does require a dose adjustment for decreased renal function when used for stroke prophylaxis in nonvalvular atrial fibrillation. It is FDA approved for the reduction of stroke and systemic emboli risk in
nonvalvular atrial fibrillation, treatment and prevention of recurrence of distal venous thromboembolism and pulmonary embolism, and venous thromboembolism prophylaxis after lower joint replacement surgery.5
In patients who require immediate surgery or in cases of life threatening blood loss, the following strategies are recommended to reverse rivaroxaban activity:
• If ingested within the past two hours, administer activated charcoal to prevent new drug from entering systemic circulation.
• The drug Kcentra, a non-activated four factor prothrombin complex concentrate, may be considered as a reversal agent. In cases of intracranial hemorrhage, the recommended dose is 50 units per kg with a max of 5000 units as a one-time dose. A non-intracranial hemorrhage dose is 25 units per kg with a max of 2500 units as a one-time dose.6
ApixabanSimilar to rivaroxaban, apixaban is a selective inhibitor of factor Xa and prevents the downstream production of fibrin, the final product of the coagulation cascade. The benefits and indications of this drug are similar to those of rivaroxaban.7
In patients who require immediate surgery or in cases of life threatening blood loss, the following strategies are recommended to reverse apixaban activity:
• If ingested within the past two hours, administer activated charcoal to prevent new drug from entering systemic circulation.
• The drug Kcentra, a non-activated four factor prothrombin complex concentrate, may be considered as a reversal agent and dosing is the same as that suggested for reversal of rivaroxaban.6
EdoxabanEdoxaban, another selective inhibitor of factor Xa, is in the same class as rivaroxaban and apixaban, and was recently approved by the FDA. It has approved indications for the prevention of stroke and systemic emboli in nonvalvular atrial fibrillation and for treatment of deep vein thrombosis, or
36 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 37
Continuing Pharmacy Education Lesson #8

pulmonary embolism after 5-10 days of parenteral anticoagulation therapy. Because it is so new, there are currently no guidelines for reversal.8
Agents Used in Reversal StrategiesNovosevenNovoseven®, a Recombinant Coagulation Factor VIIa, is a reversal agent for patients on warfarin who object to blood products and cannot receive first line agents. Novoseven is also used for treatment of bleeding and prevention of bleeding for surgeries and procedures in adults and children with hemophilia A or B with inhibitors, congenital Factor VII (FVII) deficiency, and people with Glanzmann’s thrombasthenia who have a decreased response to platelet transfusions.9
Caution is advised for Novoseven use in patients who have an increased risk for blood clots, such as with disseminated intravascular coagulation (DIC), atherosclerosis, crush injury, septicemia, uncontrolled bleeding after giving birth, history of heart disease, liver disease, or in patients receiving prothrombin complex concentrate. Because of their mechanism of action, the most common and serious side effect of all anticoagulation reversal agents is thrombosis. Novoseven is a powder that must be reconstituted before administration.9
FEIBAFEIBA®, an Anti-Inhibitor Coagulant Complex, is the current choice for treating over -anticoagulation with dabigatran. FEIBA is also indicated for the control of spontaneous bleeding episodes or to prepare for surgical interventions in hemophilia A and hemophilia B patients with inhibitors.9
The use of FEIBA is contraindicated in the following:
1. Patients who have known anaphylactic or severe hypersensitivity reactions to the product.
2. Patients who are known to have a normal coagulation mechanism.
3. For the treatment of bleeding episodes resulting from coagulation factor deficiencies in the absence of inhibitors to coagulation factor VIII or coagulation factor IX.
4. Patients with significant signs of DIC.5. Patients with acute thrombosis or
embolism (including myocardial infarction).
When treating a patient with FEIBA for an indicated therapy, the infusion should not exceed a single dosage of 100 U/kg and daily doses of 200 U/kg of body weight. If larger doses are warranted and patients are receiving more than 100 U/kg of FEIBA, they must be monitored for the development of DIC and/or symptoms of acute coronary ischemia. High doses of FEIBA should be given only as long as absolutely necessary to stop bleeding. The adverse reactions reported in clinical studies with FEIBA were anamnestic (immune) response, somnolence, dizziness, dysgeusia, dyspnea, hypoesthesia, nausea, chills, pyrexia, chest pain and discomfort.9
KcentraKcentra®, a non-activated 4-factor prothrombin complex concentrate, is used as an antidote for warfarin, rivaroxaban, and apixaban. Kcentra is a blood coagulation factor replacement product indicated for the urgent reversal of acquired coagulation factor deficiency induced by vitamin K antagonist therapy in adult patients with acute major bleeding, the need for urgent surgery or other invasive procedure. Studies have also shown that Kcentra has some efficacy in partially reversing anti-Xa therapies. Coadministration of Kcentra with vitamin K is recommended to maintain vitamin K-dependent clotting factor levels once the effects of Kcentra have diminished.10
Reversal therapy with this drug is contraindicated in patients with known anaphylactic or severe systemic reactions to Kcentra or any of its components (including heparin, factors II, VII, IX, X, proteins C and S, antithrombin III and human albumin). Use in patients with heparin-induced thrombocytopenia (HIT) is contraindicated, as the product contains small amounts of heparin, and in patients with DIC. In clinical trials, the most frequent adverse reactions observed in subjects receiving Kcentra were headache, nausea/vomiting, hypotension, and anemia. The most serious adverse reactions were thromboembolic events including
stroke, pulmonary embolism, and deep vein thrombosis. Kcentra is stored as a powder and must be reconstituted before administration.10
Emerging Reversal Therapy IdarucizumabIdarucizumab is a new fully humanized antibody fragment (Fab). Pre-clinical studies indicate idarucizumab binds specifically to dabigatran and is currently going through a phase III clinical trial (RE-VERSE AD) scheduled to be completed in 2016. The FDA granted Idarucizumab breakthrough therapy designation in June 2014, which puts it on the fast track for approval once phase trials are complete. Limited data are available, but the data released from RCT Phase I trials are encouraging.11
The first phase I trial provided proof of concept in a study of swine and the ability of idarucizumab to greatly reduce blood loss in those test subjects on dabigatran that suffered trauma.12
In another phase I trial, a two part random control trial of 145 healthy males was completed. The subjects received single, progressively increasing IV doses of up to 8 g of idarucizumab to test for potential adverse effects with or without having dabigatran in their system. They also were evaluated for potential reversal of dabigatran anticoagulation on doses of 220 mg twice a day for three days. On the fourth day, the patients were given five minute IV infusions of 1 g, 2 g, and 4 g doses of idarucizumab. The action of the antidote was detected immediately after the five minute infusion using an assay of thrombin time. The reversal was complete and sustained in seven of the nine subjects in the 2 g dose and in all eight of the patients in the 4 g dose arms. The 1 g dose demonstrated complete reversal, but after 30 minutes, some of the anticoagulation effects returned. The adverse events were of mild intensity in both parts of the study. In part one: 5 of 110 had six adverse events, three of which were noted after administration of the idarucizumab and included headache, erythema, and migraine. In part two: 5 of 35 patients developed six adverse events, two of which were noted after administration of the idarucizumab and included feeling hot and erythema.11
36 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 37
Continuing Pharmacy Education Lesson #8

The final phase I data was from a random control two-way cross-over trial of 46 volunteers from 45 to 80 years of age. The patients were given a variable dose of dabigatran based on their creatinine clearance; 220 mg twice a day for four days if creatinine clearance was greater than 60 ml/min or 150 mg twice a day for four days if creatinine clearance was between 30 ml/min and 60 ml/min. Two hours following the last dabigatran dose, the subjects were given randomized idarucizumab doses of 1 g, 2.5 g, 5 g, or two doses of 2.5 g one hour apart. Analysis of efficacy was measured using unbound dabigatran, thrombin time, ecarin clotting time, and activated partial thromboplastin time.13
The reversal of dabigatran’s action was determined to be immediate after infusion, based on the unbound dabigatran levels and the consistent prolonged clotting times. The reversal of the dabigatran was sustained in the doses of 2.5 g, 5 g, and the two doses of 2.5 g one hour apart. The 1 g dose allowed a partial return of activity after a period of between 2 to 4 hours. Two months after the administration of idarucizumab, the subjects received a second, identical course of dabigatran and idarucizumab with the same results. The study also looked at the ability to return the body to a state of anticoagulation, and based on pharmacodynamics and pharmacokinetic measurements versus placebo, dabigatran had efficacy 24 hours after administration of idarucizumab. The doses given were safe and well tolerated and the only adverse effect reported was a transient dose-related increase in urinary protein levels.13
PER977PER977 (Perosphere), is a small, synthetic, water-soluble, cationic molecule that binds to factor Xa inhibitors, edoxaban, rivaroxaban, and apixaban, and the oral thrombin inhibitor, dabigatran. Phase II studies have shown to reverse anticoagulation in these oral agents. In patients who received 60 mg of edoxaban, clotting time decreased to within 10 percent of baseline within 10 minutes of administering a single dose of PER977 and was sustained for 24 hours. Additional phase II clinical studies are ongoing.14
ConclusionWhen choosing an anticoagulant, there are several options for health care professionals and patients. No longer should unfamiliarity or bleeding risk be a barrier for deciding the best medication for a patient. There are multitudes of options that are specific and safe with the advent of targeted reversal strategies, the risks of bleeding may be minimized. The field of anticoagulation has just started to address the different possibilities and avenues of study.
References1. DiPiro J. Pharmacotherapy: A Pathophysiologic
Approach. 8 ed: McGraw-Hill; 20122. Hirsh, J., Dalen, J., Anderson, D.,Poller, L., Bussey,
H., Ansell, J., Deykin, D.; Oral Anticoagulants: Mechanism of Action, Clinical Effectiveness, and Optimal Therapeutic Range; Chest. 2001; 119: 8s-21s.
3. Pabinger I, Brenner B, Kalina U, et al; Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. Journal of Thrombosis and Haemostasis 2008; 6: 622-631.
4. Stangier J. et al. Pharmacokinetic Profile of the Oral Direct Thrombin Inhibitor Dabigatran Etexilate in Healthy Volunteers and Patients Undergoing Total Hip Replacement. J Clin Pharmacol. 2005; 45:555–63.
5. Xarelto [package insert]. Leverkusen, Germany: Janssen; 2011
6. Fawole A, Daw HA, Crowther MA. Practical management of bleeding due to the anticoagulants dabigatran, rivaroxaban, and apixaban. Cleve Clin J Med. 2013 Jul;80(7):443-51.
7. Eliquis [package insert]. New York, NY: Bristol-Myers Squibb; 2011
8. Giugliano, R., et al; Edoxaban versus Warfarin in Patients with Atrial Fibrillation; N Engl J Med. 2013; 369: 2093-104.
9. Kalus, J.; Pharmacologic interventions for reversing the effects of oral anticoagulants; Am J Health-Syst Pharm. 2013; 70: Suppl 1.
10. Bechtel et al. Treatments for reversing warfarin anticoagulation in patients with acute intracranial hemorrhage: a structured literature review; International Journal of Emergency Medicine 2011, 4:40.
11. Data from First Phase I Study of Antidote for Pradaxa (dabigatran etexilate mesylate) Presented at American Heart Association Scientific Sessions; 2013
12. Honickel, M., Grottke, O., Van Ryn, J., Ten Cate, H., Rossaint, R., Spronk, H.; Use of a specific antidote to dabigatran (idarucizumab) reduces blood loss and mortality in dabigatran-induced and trauma-induced bleeding in pigs; Crit Care. 2014; 18: pp 99.
13. Glund, S., Stangier, J., Schmol, M., Moschetti, V., Haazen, W., De Smet, M., Gansser, D., Norris, S., Lang, B., Reilly, P.; Idarucizumab, a Specific Antidote for Dabigatran: Immediate, Complete and Sustained Reversal of Dabigatran Induced Anticoagulation in Elderly and Renally Impaired Subjects; Antithrombotic Therapy: Anticoagulant Therapy, Moscone Center. 2014; Session 332.
14. Ansell, J., et al.; Use of PER977 to Reverse the Anticoagulant Effect of Edoxaban; N Engl J Med. 2014; 371:2141-2142. PER977
15. Reprinted by permission from Macmillan Publishers Ltd: [Nature Reviews: Cardiology], 2013.
Policies for the Nebraska Mortar & Pestle (M&P) continuing pharmacy education lessons and quizzes:
1. M&P Quizzes are valid only for the membership year in which they are published. Quizzes for the 2015 Membership Year must be received by December 7, 2015. Quizzes cannot be carried over to another membership year.
2. If more than three questions are missed, the quiz will be returned. The quiz can be resubmitted.
3. CPE transcripts can be printed from NABP e-Profiles at www.nabp.net.
4. CPE credits are submitted to NABP by the 15th of each month. For example, M&P CPE quizzes completed in the month of August 2015, will be sent to NABP e-Profiles before September 15, 2015.
The Nebraska Council for Continuing Pharmacy Education (NCCPE) is accredited by the Accreditation Council for Pharmacy
Education (ACPE) as a provider of continuing pharmacy education (CPE).This CPE home study lesson has been accredited for 1.0 contact hours or 0.10 CEU. UAN #0128-0000-15-297-H01-P. This lesson is a knowledge-based CPE activity targeted to pharmacists.
The authors and the Nebraska Pharmacists Association disclaim any liability to you or your patients resulting from reliance solely upon the information contained herein.
Quiz Answers may be submitted:1. Online: www.npharm.org
2. Fax: 402-420-1406
3. Email: m&[email protected]
4. Mail: NPA Mortar & Pestle 6221 S 58th St, Ste A Lincoln, NE 68516
Beginning January 2015, pharmacy technician CE hours earned must be in a pharmacy-technician specific subject matter. This ACPE accredited activity is NOT pharmacy technician-specific and ACPE credit may not be earned for pharmacy technicians. Contact the NPA office for free ACPE accredited pharmacy technician-specific CE activities for NPA members from the 2015 Pharmacy TEAM Series.
38 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 39
Continuing Pharmacy Education Lesson #8

Oral Anticoagulants and Reversal Strategies in Emergent SituationsQuiz #8, May/June 2015, ACPE #0128-0000-15-297-H01-P
2015 Quiz #8 - NPA CPE Home Study Answer FormOral Anticoagulants and Reversal Strategies in Emergent Situations
UAN #0128-0000-15-297-H01-P for pharmacists1.0 Contact Hours - Knowledge Based CPE Activity
Name ________________________________________________________
Mailing Address _______________________________________________
City/State/Zip _________________________________________________
*NABP e-Profile # ______________ *Date of Birth (MMDD) _________*Required for ACPE credit.
Circle one (1) Answer:1. a b c d 6. a b c d2. a b c d 7. a b c d3. a b c d 8. a b c d4. a b c d 9. a b c d5. a b c d 10. a b c d
CPE Home Study Evaluation 1. Rate this lesson: (Excellent) 5 4 3 2 1 (Poor)
2. Did this lesson meet each of its objectives? ___ Yes ___ No3. Was the content without commercial bias? ___ Yes ___ No 4. Did the lesson meet your educational/practice needs? ___ Yes ___ No5. Comments/future topics are welcome. ________________________
The deadline for this quiz is December 7, 2015
Keep the TOP portion for your records. Return the BOTTOM portion to the NPA office.Or, take this quiz online at www.npharm.org
Continuing Pharmacy Education Quiz #8
1. The cofactor activated by factors IX and VII that is the target of some novel oral anticoagulants developed in the last decade is: a. Factor II b. Factor VIIa c. Factor Xa d. Thrombin
2. The drug that targets factors VII, IX, and X as well as prothrombin II is: a. Edoxaban b. Dabigatran c. Idarucizumab d. Warfarin
3. The final product of the coagulation cascade that is responsible for clotting at the sites of injury is: a. Fibrin Ia b. Fibrinogen I c. Prothrombin II d. Thrombin IIa
4. Warfarin was first developed and marketed as a product to: a. Fertilize plants b. Grow hair c. Kill rodents d. Treat acne
5. The recommended agent for reversal of vitamin K antagonists in emergent situations is: a. FEIBA b. Idarucizumab c. Kcentra d. Vitamin E
6. In cases where the patient objects to receiving blood products and the preferred reversal agent for warfarin can’t be used, the alternative recommendation is: a. FEIBA b. Kcentra c. Novoseven d. PER977
7. The most serious adverse effect of all anticoagulation reversal agents is: a. Blood clots b. Dizziness c. Headache d. Nausea
8. The current strategy for counteracting dabigatran is to use the drug: a. FEIBA b. Idarucizumab c. Kcentra d. Warfarin
9. The more targeted pharmaceutical drug that is currently undergoing phase III trials for reversal of dabigatran is: a. Idarucizumab b. Kcentra c. Novoseven d. PER977
10. The small molecule that is currently undergoing phase II studies for its potential to reverse all anti-Xa inhibitors is: a. FEIBA b. Idarucizumab c. Novoseven d. PER977
38 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 39
Thank you to our convention donors, exhibitors, and sponsors.
Exhibitors• AbbVie• Actavis• AstraZeneca• Baxter Healthcare Corporation• Boehringer-Ingelheim Pharmaceuticals• Cardinal Health• Creighton University School of Pharmacy & Health Professions• Dakota Drug• Eli Lilly & Company• Great Plains Quality Innovation Network & CIMRO of Nebraska• HealthCare Solutions• Janssen Pharmaceuticals• Liberty Software• McKesson• Merck & Company Vaccines• Nebraska Pharmacy Foundation• Nebraska MEDS
Sponsors• AmerisourceBergen• Blue Cross and Blue Shield of Nebraska• Creighton University School of Pharmacy & Health Profession• McKesson• National Association of Chain Drug Stores (NACDS)• Nebraska Pharmacists Corporation• Pharmacists Mutual Companies• Winter Wolf Consulting
Donors• Pharmacists Mutual Companies• Rx Systems
• Novo Nordisk• Otsuka Pharmaceuticals• Pharmacists Mutual Companies• Pharmacy Technician Certification Board• QS/1 Data Systems• RxPlus Pharmacies• Sanofi Pharmaceuticals• Smart-Fill• Southeast Community College• Teva Pharmaceuticals• University of Nebraska Foundation• Vertex Pharmaceuticals• Walgreens• Winter Wolf Consulting
ConventionNPANebraska Pharmacists Association
40 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 41
• Novo Nordisk• Otsuka Pharmaceuticals• Pharmacists Mutual Companies• Pharmacy Technician Certification Board• QS/1 Data Systems• RxPlus Pharmacies• Sanofi Pharmaceuticals• Smart-Fill• Southeast Community College• Teva Pharmaceuticals• University of Nebraska Foundation• Vertex Pharmaceuticals• Walgreens• Winter Wolf Consulting
Photo AlbumConventionNPANebraska Pharmacists Association
40 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 41

Photo AlbumConventionNPANebraska Pharmacists Association
42 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 43
Photo AlbumConventionNPANebraska Pharmacists Association
42 May/June 2015 www.npharm.org The Nebraska Mortar & Pestle 43
Do you know the three most commonmistakes that pharmacy owners make whencontemplating the sale of their pharmacy?
To learn what they are, and to learn much more about theservices we provide for independent pharmacy ownersthinking about ownership transition and/or retirement, visitour web site, www.buy-sellapharmacy.com. Click on thebutton on the home page that says “Pharmacy Owner’sQuestions” or call your local Buy-Sell Associate directly atany time. By doing so, you will have the opportunity toearn a $100.00 GIFT of valuable marketing materials foruse in your pharmacy.
Don’t leave money on thetable when you transition the ownership of your business.
“Our 15 year track record of successfully completing more than 400independent pharmacy sales speaks for itself.”
1-(877)-360-0095www.buy-sellapharmacy.com
Completelyconfidential!
Your Local SpecialistLarry [email protected]: 1-(847)-949-2477
BuySell_ads15_Layout 1 12/2/14 4:54 PM Page 5
Return Service Requested
Nebraska Mortar & Pestle6221 S 58th Street, Suite A, Lincoln, Nebraska 68516www.npharm.org ~ 402-420-1500 ~ m&[email protected]
Deliver to NPA Member:
PRSRT STDUS POSTAGE
PAIDPERMIT #586LINCOLN NE
Connect With the NPA
Like us on Facebook at www.facebook.com/NebraskaPharmFollow us on Twitter at www.twitter.com/NebraskaPharmConnect with us on LinkedIn at www.linkedin.com






![Indonesian Food - MYTEACUP.COMmyteacup.com/cookbooks/Indonesian-Food.pdf[INDONESIA]: Used as an ... the chilis, chop finely, then crush with salt using a pestle and mortar. ... From](https://static.fdocuments.in/doc/165x107/5b0ca1097f8b9a2f788c831e/indonesian-food-indonesia-used-as-an-the-chilis-chop-finely-then-crush.jpg)











