NDA 20-272/8-008 & 20-588/8-004 - Food and Drug ... FOR DRUG EV ALUA TION AND RESEARCH wroval...
106
CENTER FOR DRUG EV ALUA TION AND RESEARCH wroval Packa2e for: APPLICATION NUMBER: NDA 20-272/8-008 & 20-588/8-004 Trade Name: Risperdal Tablets 0.25, 0.5, 1, 2, 3 and 4 mg & Risperdal Oral Solution 1 mg/mL Generic Name: risperidone Sponsor: Janssen Pharmaceutica Approval Date: 03/03/2002 Indications: F or the treatment of schizophrenia.
Transcript of NDA 20-272/8-008 & 20-588/8-004 - Food and Drug ... FOR DRUG EV ALUA TION AND RESEARCH wroval...
CENTER FOR DRUG EV ALUA TION AND RESEARCH
wroval Packa2e for:
APPLICATION NUMBER:
NDA 20-272/8-008 & 20-588/8-004
Trade Name: Risperdal Tablets 0.25, 0.5, 1, 2, 3 and 4 mg &Risperdal Oral Solution 1 mg/mL
Generic Name: risperidone
Sponsor: Janssen Pharmaceutica
Approval Date: 03/03/2002
Indications: F or the treatment of schizophrenia.
CENTER FOR DRUG EVALUATION ANDRESEARCH
APPLICATION NUMBER:
NDA 20-272/8-008& 20-588/8-004
CONTENTS
Reviews / Information Included in this NDA Review.
xxx
x
x
x

CENTER FOR DRUG EVALUATION ANDRESEARCH
APPLICATION NUMBER:
NDA 20-272/8-008 & 20-588/8-004
APPROVAL LETTER

",s:\tK"k'h.,,l~)¡
(:. ~: DEPARTMENT OF HEALTH & HUMAN SERVICES~;:Public Health Service
Food and Drug AdministrationRockvile MD 20857
NDA 20-272/S-008NDA 20-588/S-004
Johnson & Johnson Pharmaceutical Research & Development, L.L.c.Attention: Edward G. Brann .Director, Regulatory Affairs1125 Trenton-Harbourton RoadTitusvile, NJ 08560
Dear Mr. Brann:
Please refer to your supplemental new drug applications dated March 12, 1997, received March 12,1997, submitted under section 505(b) ofthe Federal Food, Drug, and Cosmetic Act for Risperdal(risperidone) tablets and oral solution.
We acknowledge receipt of your submission dated January 28,2002, which constituted a completeresponse to our January 11,2002 action letter.
These supplemental new drug applications provide for the longer-term efficacy for risperidone in thetreatment of schizophrenia.
We have completed the review ofthese supplemental applications, as amended, and have concludedthat adequate information has been presented to demonstrate that the drug products are safe andeffective for use as recommended in the agreed upon enclosed labeling text. We note thatmodifications oflabeling text to more clearly state that this agent is indicated for the treatment ofschizophrenia (requested in our letter of September 25,2000) have been effected. Accordingly, thesesupplemental applications are approved effective on the date ofthis letter.
The final printed labeling (FPL) must be identical to the enclosed labeling (text for the package insert).
Please submit the copies offinal printed labeling (FPL) electronically to each application according to
the guidance for industry titled Providing Regulatory Submissions in Electronic Format - NDA
(January 1999). Alternatively, you may submit 20 paper copies of the FPL as soon as it is available butno more than 30 days after it is printed. Please individually mount ten ofthe copies on heavy-weightpaper or similar materiaL. For administrative purposes, these submissions should be designated "FPLfor approved supplement NDA 20-272/S-008, 20-588/S-004." Approval ofthese submissions by FDAis not required before the labeling is used.
Be advised that, as of April 1, 1999, all applications for new active ingredients, new dosage forms, newindications, new routes of administration, and new dosing regimens must contain an assessment of thesafety and effectiveness of the product in pediatric patients unless FDA waives or defers therequirement (63 FR 66632) (21 CFR 314.55). The Agency has not made a determination if a health

NDA 20-272/S-008NDA 20-588/S-004Page 2
benefit would be gained by studying risperidone in pediatric patients for its approved indication. FDAis deferring submission of the pediatric assessments of safety and effectiveness that may be requiredunder these regulations until February 1,2005.
If a letter communicating important information about this drug product (i.e., a "Dear Health CareProfessional" letter) is issued to physicians and others responsible for patient care, we request that yousubmit a copy ofthe letter to this NDA and a copy to the following address:
MEDWATCH, HF-2FDA5600 Fishers LaneRockvile, MD 20857
We remind you that you must comply with the requirements for an approved NDA set forth under21 CFR 314.80 and 314.81.
If you have any questions, call Steven D. Hardeman, R.Ph., Senior Regulatory Project Manager, at(301) 594-5525.
Sincerely,
(See appended electronic signature page)
Russell Katz, M.D.DirectorDivision of Neuropharmacological Drug ProductsOffice of Drug Evaluation ICenter for Drug Evaluation and Research
Enclosure

Description of revisions to Risperdal (risperidone) Labeling
Section of Labeling Description ofRevision(s)
DESCRIPTION Paragraph i, sentence i: changed from "an antipsychoticagent" to "a psychotropic agent"
CLINCAL PHACOLOGY: Paragraph i, sentence i: changed "antipsychotic drugs"Pharacodynamics to "drugs used to treat schizophrenia" and "antipsychotic
activity" to "therapeutic activity in schizophrenia"
CLINCAL PHACOLOGY: Before paragaph i, added subheading "Short-Term
Clinical Trials Efficacy" .
Paragraph i, changed "management of the manifestationsof psychotic disorders" to "treatment of schizophrenia"
Paragraph 2, sentence i: changed "effects of drugtreatment in psychosis" to "effects of drug treatment inschizophrenia"
CLINCAL PHACOLOGY: Added subheading "Long-Term Effcacy" and paragraphClinical Trials to describe RIS-USA-79 study design and results
INICATIONS AND USAGE Pargraph i: changed "management of the manfestationsof psychotic disorders" to "treatment of schizophrenia"
Paragrph 2, changed "antipsychotic effcacy ofRISPERDAL~" to "effcacy ofRISPERDAL~ inschizophrenia"
Paragraph 3: replaced first sentence with FDA statementon use ofRisperdal in long-term treatment; last sentence:changed "Therefore" to Neverteless"
DOSAGE AND ADMISTRATION: Paragaph i: added "short-term" twice as descriptor ofUsual Initial Dose clincal trals and sentence on titration schedule from
long-term study
Paragraph 2, sentence i: changed "Antipsychoticeffcacy" to Efficacy in schizophrenia" for consistencywith the intent of FDA 9/25/00 letter and added "short-term" as descriptor for clinical trials
DOSAGE AND ADMISTRTION: Repositioned subsection to follow "Usual Initial Dose"Maintenance Therapy subsection
Revised paragph to provide description and titrationschedule from long-term study and to incorporate FDA'schanges
Added the word "schizophrenic" to describe patients inthe first sentence.
DOSAGE AND ADMISTRATION: Added "schizophrenic" as a descriptor for "patients" inSwitching from Other Antipsychotics three places and changed "other patients" to "others"

This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.
/s/Russell Katz3/3/02 11:33:45 AM

CENTER FOR DRUG EVALUATION ANDRESEARCH
APPLICATION NUMBER:
NDA 20-272/8-008 & 20-588/8-004
APPRO V ABLE LETTER
('~~'È" ::.',Jtr't"l.ifl
DEPARTMENT OF HEALTH & HUAN SERVICES Public Health Service
Food and Drug AdministrationRockville MD 20857
NDA 20-272/S-008NDA 20-588/S-004
Janssen Research FoundationAttention: Edward G. BrannAssistant Director, Regulatory Affairsi 125 Trenton-Harbourton RoadP .O.Box 200Titusvile, NJ 08560-0200
Dear Mr. Brann:
Pleas refer to your supplemental new drug applications dated March 12, 1997, received March 12, 1997,submied under section 505(b) of the Federal Food, Drug, and Cosmetic Act for Risperdal (risperidone)tablets and oral solution.
Your submissions of July 25, 2001, constituted a complete response to our action letter of January 13,1998.
These supplemental new drug applications provide for the longer-term efficacy for risperidone in thetreatment of schizophrenia.
We have completed the review ofthese applications, as amended, and they are approvable. Before these
applications may be approved, however, it wil be necessary for you to submit revised draft labeling. Wehave made revisions to the four sections of labeling for which you have proposed changes. Specifically:
Under CLINCAL lRS, Long-Term Effcacy. We request that you replace your suggestedparagraph under this heading with the following:
"In a longer-term trial, 365 adult outpatients predominantly meetinglDSM-IV I criteria forschizophrenia and who had been cliically stable for at least 4 weeks on an antipsychoticmedication were randomized to Risperdal (2-8 mglday) or to an active comparator, for 1 to 2years of observtion for relapse. Patients receivig Risperdal experienced a signifcantly longertime to relapse over this time period compared to those receivig the active comparator."
In keeping with the current focus in Risperdal labeling on schizophrenia as an indication, and thepredominance of schizophrenia in the sample for study 79, we have included mention only ofschizophrenia, in order to avoid confusion among prescribers.
-c.~

NDA 20-272/S-008
"NA 20-588/S-004Page 2
c =lWe have C :i time to relapse, the one outcome designatedprospectively as the primary outcome for study 79.
We have also made othereditorial changes to bring the language into consistency with standardlanguage for the longer-term claim.)
· Under INICA nONS AN USAGE. The following paragraph should be inserted as the finalparagraph in this subsection:
"The effcacy ofRiperdal in delaying relapse was demonstrated in schizophrenic patients whohad been cliically stable for at least 4 weeks before initiation of treatment with Riperdal oran acti comparator and who were then observed for relapse during a period of 1 to 2 years
(see cliical Trials, under Cliical Pharmacology). Nevertheless, the physician who elects touse Riperdal for extended periods should periodically re-evaluate the long-term usefulnessof the drug for the individual patient (see Dosage and Administration)."
.
i
L JUnder DOSAGE AN ADMllRTION. The following paragraphs should be inserted to replacethe curent language under the subsections entitled Usual Initial Dose and Maintenance Therapy. Wehave not removed the language explaining the basis for weekly dose adjustments, and we have madeother editorial changes.
"Usual Initial Dose: RISPERDAL ~ (risperidone) can be administered on either a BID or a QDschedule. In early short-term clinical trials, RISPERDAL ~ was generally administered at 1 mg BIDiniall, wit incres in increments of 1 mg BID on the second and third day, as tolerated, to a target
dose of 3 mg BID by the third day. Subsequent short-term controlled trials have indicated that totaldaily risperidone doses of up to 8 mg on a QD regimen are also safe and effective. In a long-term
NDA 20-272/S-008NDA 20-588/S-004Page 3
controlled trial in stable patients, RISPERDAL was administered on a QD schedule at 1 mg QDinitially, with increases to 2 mg QD on the second day and to a target dose of 4 mg QD on the thirdday. However, Regardless of which regimen is employed, in some patients a slower titration may bemedically appropriate. Further dosage adjustments, if indicated, should generally occur at intervals of
not less than 1 week, since steady state for the active metabolite would not be achieved forapproximately 1 week in the typical patient. When dosage adjustments are necessary, small doseincrements/decrements of 1-2 mg are recommended.
Antipsychotic effcacy was demonstrated in a dose range of 4 to 16 mglday in short-term clinical trialssupporting effectiveness ofRISPERDAL cI, however, maximal effect was generally seen in a rangeof 4 to 8 mglday. Doses above 6 mglday for BID dosing Were not demonstrated to be more efficaciousthan lower doses, were associated with more extrapyramidal symptoms and other adverse effects, andare not generally recommended. In a single study supporting QD dosing, the efficacy results weregenerall stonger for 8 mg than for 4 mg. The safety of doses above 16 mgl day has not been evaluatedin clinical trials.
Maintenance Therapy: While there is no body of evidence available to answer the question of howlong the patient treated with RISPERDAL should remain on it, the effectiveness ofRISPERDAL 2mgdayto 8 mglday at delaying relapse was demonstrated in a controlled trial in patients who had beencliically stable for at least 4 weeks and were then followed for a period of 1 to 2 years. In this trial,RISPERDAL was administered on a QD schedule, at 1 mg QD initially, with increases to 2 mg QDon the second day and to a target dose of 4 mg QD on the third day (see Clinical Trials, under Clinical
Pharmacology). Nevertheless, patients should be periodically reassessed to determine the need formaintenance treatment with appropriate dose."
The labeling should be identical in content to the enclosed labeling (text for the package insert), and allprevious revisions as reflected in the most recently approved labeling must be included. Further, thelabelig changes as requested in our letter of September 25, 2000, must be effected in your response to thisaction letter. Specifically, modifications of labeling text to more clearly state that this agent is indicatedfor the treatment of schizophrenia should be made.
To facilitate review of your submission, please submit a highlighted or marked-up copy of labeling thatshows the changes that are being made.
If additional information relating to the safety or effectiveness of this drug becomes available, furtherrevision ofthe labeling may be required.
Within 10 days after the date ofthis letter, you are required to amend the supplemental applications, notifyus of your intent to fie amendments, or follow one of your other options under 21 CFR 314.110. In theabsence of any such action FDA may proceed to withdraw the applications. Any amendment shouldrespond to all the deficiencies listed. We wil not process a partial reply as a major amendment nor wilthe review clock be reactivated until all deficiencies have been addressed.

NDA 20-272/S-008NDA 20-588/S-004Page 4
If you have any questions, call Steven D. Hardeman, R.Ph., Senior Regulatory Project Manager, at (301)594-5525.
Sincerely,
(See appended electronic signature page)
Russell Katz, M.D.DirectorDivision of Neuropharmacological Drug ProductsOffce of Drug Evaluation ICenter for Drug Evaluation and Research

---------------------------------------------------------------------------------------------------------------------This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.---------------------------------------------------------------------------------------------------------------------/s/
Russell Katz1/11/02 08: 02: 17 AM

CENTER FOR DRUG EVALUATION ANDRESEARCH
APPLICATION NUMBER:
NDA 20-272/8-008 & 20-588/8-004
LABELING

NDA 20-272/20-588RISPERDAL ~ (risperidone) Tablets/Oral Solution
Part No. 7503220Physicians Insert
S c ~OOl¡ FA)"LQ-~,~ ~~c2 O?òOD
Laø:.s82~oog lEtl) 23-¿NONo. .~~ 2.,2. Bdtr" ,
.1.i-b'y~
ORIGiNAL
DESCRIPTION ,",RISPERDAL~ (nspendone) is a psychotropic agent belonging to a new chemical class, thebenzisoxazoledenvatives. The chemical designation is 3-(2-(4-(6-fiuoro' 1 ,2-benzisoxazol'3'yl)-1-pipendinYIJethYIJ-6,7,B,9-tetrahydro- 2-methyi-4H-pyndo(1 ,2-aJpynmidin-4-one. its molecuiar formula is C~HvFN.O, and its molecularweight is 41 OA9. The structurai formula is: ' .
a"yCH'"Y'CH.-CH,-()Ô
F
Risperidone is a white to slightly beige powder. It i5practically insol~b!e .in water, freely soluble in methylenechlonde, and soluble in meihanol and 0.1 !' HCI. '.RiSPERDAL~taiets are available in 0.25 mg (dark yellow), 0.5 mg (red-brown),Jmg (w~ite), 2 mg(orage),3 mg (yellow), and 4 mg (green) strengths. Inactive ingredients'are colloidal silcon (,lioxide, hydroxypropylmethylcellulose, lactose, magnesium stearate, microcrystallne cellu.lose, propyle".e glycol, sodium)aurylsulfate, and starch (corn). Tablets of 0.25, 0.5, 2, 3, and 4 mg also.contain talc and,ìilaniumdiox.icie. The0.25 mgtablets contain yellow iron oxide; the q.5 mg tablets contaiíi red iron oxide, th~:2 mg tablets:sOntainFP&C YellOW NO.6 Aluminum Lake; the.3 mg and 4 mg tablets contain D&Ç'Yellow N0,10; the 4 mg tabletscontain FD&C Blue No.2 Aluminum Lake. ,.' . ..'.",., " .RISPERDAL ~ is al~o available as.a 1 mgÍmL oral solution. The inactive ingredients .lor this solution aretartanc acid, benzoic acid, sodium hydroxideand purified water.
CLINICAL PHARMACOLOGYPharmacodynaniicsThe mechanism ofaction,ofHISPERDAL~(rispendone), as with other drugs Used to treat schizophrenia, isunknown, However, it has been proposed that this drug's therapeutic activity in schizophrenia is mediatedthrough... combination 01. dopamine type 2 (0,) and serotonin type 2 (5HT,) antagonism. Antagonismat receptors other than 0, and.5HT, may explain some of the other effects of RISPERDAL~.RiSPERDAL~ is a selective monoaminergic antagonist with highaffinity(Ki of O. t2 to 7:.3 nM)for theserotonin type 2 (5HT,), dopamine type 2 (0,), lX', and", adrenergic, and H, histaminergic receptors.RISPERDAL~antagonizes other receptors, but with lower potency. RISPERDAL~ has low to moderateaffinity (Ki of 47 to 253 nM)for the serotonin 5HT", 5HTm, and.5HT" receptors, weak affnity(Ki of 620 toBOO nM) for the dopamine 0, and haloperidol-sensitive sigma site,' and no.affinity .(when te~ted atconcentrations ::10'5 M) for c~olinergic muscarinic or ß1 and ß2 adra.r!ergic recepto~s: . ,,-PharmacokineticsRispendone is well absorbed; as illustrated by a mass balance study involving asingle.t mgoral dose of"C-risperidone 'as a solution in three healthy male volunteers, Total recovery of radloactivity..i.one weekwas B5%, including 70% in the unne and t S% in the feces. ....."Risperidone is extensively metabolized in the liver by cytochrôme P.~IID. to a 'major actiVe metabolite,9-hydroiinspendone,'which i5the predominant circulating specie, and appears approximately equi-effectivewith nspendone with respect to receptor binding activity and some effects in animals. (A second minor pathwayis Ndealkylation). Consequently, the c1inièal effect of the drug likely results from the combined concentrationsof rispendone plus 9-hydroxyrisperidone. Plasma concentrations of risperidone, 9-hydroxyrisperidone, andnspendone plus 9-hydroxyrispendone are dose proportional over the dosing range of 1 to 16 mg daily (0.5 toB mg BID). The relative oral bioavailabilty 01 rispendone lrom a tablet was 94% (CV~1 0%) when compared toa solution. Food does not affect either the rate or extent 01 absorption of risperidone. Thus; rispendone canbe'given with or without meals. The absolute oral bioavailabilty of risperidone was 70% (CV~25%).. Theehzynie catalyzing hYdroxYI.ation 01
risperidone' to 9-hydroxyrisperidohe, iscytochrome.p.~IID., also called deb'risoquinhydroxyiase, the 'enzyme responsible lormetaliolism 01 many neuroleptics, antidepres-sants, antiarrhythmics, and other drugs.Cytochro'me. P,';IID. is .subject: to. g'eneticpolymorphism (about 6'B% 01 Caucasians; and avery low percent of Asians have IiUle or no activitand are "poor metabolizers') and to inhibition bya vanety of substrates and some non-substrates;notably quinidin.e., Extensive metabolizers convertrisperidone rapidly. into g-hydroxyrispe(idone,while poor metabol.izers convert .it much moreslowly. Extensive. metabolizers, 'therelore, .havelower risperidone and higher 9-hydroxyrisperi-done concentrations than poor meiabolizers.Fôllowing oral administration of solution or tablet,mean peak plasma concentrations occurred atabout i hoW. PE,ak 9-hydroxyrisperidoneoccurred at about 3 hours i.nextensivemetabolizers, and 17 hours in poor rretabolizers.The apparent half-life of risperid~n.e Y¡as three.
JAN 1 4 200
- ~'i
~ -: '.
Clinical TrialsThe efficacy of RISPERDAL~ in the treatmentof,'schizophrenia was established. in lour short,term (4 to.B-week) .controlled trials of psychotic inpatients.whomet DSM-II-R critena. for schizpphrenia.Sev.eralinstruments were used lor assessing psychiatnc signs and Symptoms in these studies, among themthe Brief Psychiatnc Rating Scale (BPRS), a multi-item inventory of general psychopathology traditionallyused to evaluate the effects 01 drug treatment in,schizophrenia. The BPRSpsY~hosis cluster (conceptualdisorganization, hallucinatory behavior, suspiciousness,:-and unusual thought cbrient) is' considered aparticularly useful subset for assessing actively psychotic schizophrenic,pat.ients. A seQol1dJraditionalassessment, the Clinica Global Impression (CGI), reflects the impression of. a skiled observeI;,fullyAamilarwith the manifestations of schizophrenia, about the overalhclinicalstate.of the: patient. In addition, tWo morerecently develPPed,butless well evaluated ~ales,. were employed; th~se included the Positive ,and NegativeSyndrome Seale (PANSS) and the Scalè l?r,AssesingNegative. Symptoms (SANS):' .Theresulls oltlÌe tnals follow: ': ..... '.(1,) In a 9. ,ow. ee,k; Placebo-con,t. roo I,ied tnal (n~160) i,n, vO,lvin, g,t~ra, t, i,O,"', Of" R,IS,PERDAL ..In, doses up to 10,m. gJday(BID schedule), RISPERDAL. was generally superior tò' pJacebo on the BPRS .total score, on the BPRSpsychosis cluster, and marginally superior to placebo on the SANS.
(2) In'an B-week;plac~bo-controlled tnal (n~S13) invoiiìing 4 fixed doses of RISPERDAL. (2,6,10, and16 mgJday, on a BID schedule), all 4 RISPERDAL~ gr()ups weregeneraly supenor to placeDo on the BPRS totalsère,aPR§ psych?sis cluster, and CGI.seventy SCOre;Jl;~ 3, ~igheSt .RI§p.l~RDAL ~ dose groups,l'~re gen,erallysupenor to placebo on the PANSS negatlvesuoscae',ThemQ$t oonsl'Jentl posit)ie reSponsesanail meiureswere seen for the 6 mg dose group,. and there was no 'suggestion of .increased benefr.lrom larger doses. .
(3) In an,B-week, dose comparison tnal¡n~1356) involving'S fixed doses. of RISPÉRDAL~ (1.4.B, 12, and16 mgJday, on a BID schedule),'the fourhighest RISPERDAl~dose group~were geDerally'supenor tothe t mgRISPERDAL~ dose group on BPRS totalscore, BPRS psychosis cluster,and CGI. seventy scre: Nöne'of thedose groups were supenor to the 1 mg groû'p on the PANSS negatiye subscale. The'most conšísienilý'positiveresponses were seen for the 4 mg dose group. '. - '. ,.(4) In a 4-week; placebcntròlleddose'cómpanson tnal (n,,,246) ,inVOlVing 2 lixed:doses of RISPERD. AL ~(4 and B mg¡day on a QDschedule), both RISPERDAL~'doše:groups were generally.supenor to placebo' onseveral PANSSmeasures, including'a response:measurEf(,;20%'reduction in PANSS.total score), PANSStotal score, and the BPRS psychosis clusier (denved fromPANSS). The,results were generally stronger lorthe B mg than for the 4 mg dose group. " ,Long-Term EfficacyIna longer-term trial, 365 adult outpatients predomihantly meeting DSM-ii" eriterialorschizÒphrenia'àndwho had been clinically stable for at least 4weeks on an antipsychotic medication were randomized toRISPERDAL. (2-B mgJday) or to an' actve èomparätòr, lor 1 to 2 years 61 observation ior relapse: PatientsreCeiving RISPERDAL ~ expenenced a significantly longer time to relapse over this time penod compared tothose receiving the active comparator, . .INDICATlaNS AND USAGE .Ri'SPERDAL ~ (risperidóne) is indicated for the treatment of schizophrenia.The efficacy of RISPERDAL. in schizophrenià was estab.lished in short-term (6 to B-weeks) controlledtrials of schizophrenic inpatients (See CLINICAL PHARMACOLOGY).The effcacy of RISPERDAL~ in delaying relapse was demonstrated in schizophrenic patients who had beenclinically stable for at least 4 weeks before initiation,of treatment with RISPERDAL~ or an active comparatorand who were then observed for relapse dunng a p,eriod 011 to 2 years (See Clinical Tnals, under CLINICALPHARMACOLOGY). Nevertheless, the physician whO elec,ts to use RISPERDAL ~ for extended periodsshould penodically re-evaluate the long,term usefulness of the drug for the individual patient (See DOSAGEAND ADMINISTRATION).
CONTRAINDICATIONSRISPERDAL ~ (risperidone) is contraindicated'in patients with a known hypersensitivity to the product.
WARNINGS. . .NeurClleptit Malignant Syndrome (NMS). .' ' ,A potentially fatal symptom complex:sometimes relerred to.as NeùrolepticMalignant.Syndrome (NMS) hasbeen reported in association with antipsychotic drugs. Clinical manifestations of NMS are hyperpyrexia,muscle rigidity, altered mental status and evidence of autonomic instability (irregular pulse or bJood pres-sure, tachYcardia, diaphoresis and cardiac dysrhythmia). Additional sighs may include elevated creatinephosphokinase, myoglobinuria (rhabdomyolysis), and acute renal failure.The diagnostic evaluation of patients with this syndrome is complicated. In arriving at a diagnosis; it isimportant to identify cases where the clinical presentation includes both serious medical illness (e.g.,pneumonia, systemic infection, etc.) and untreated or inadequately treated extrapyramidal, signs andsymptoms (EPS), Other important considerations in the differential diagnosis include central anticholinergictoxicity, heat stroke, drug fever, and primary central nerVous system pathology. .The management ofNMS should include: 1)immediaíe discontinuation otantipsychotic drugs and: otherdrugs not essenlial to concurrent therapy; 2) intensive symptomatic treatment and medical monitonng; and3) treatment of any concomitant senous medical problems for which specific treatments are available. Thereis no general agreement about specific pharmacological treatment regimens for uncomplicated NMS.Ii a patient requires antipsychotic.drug treatmentafler recovery from NMS, the potential reintroduction ofdrug therapy should be carefully considered. The patient should be carefully monitored, since recurrences 01N~A~ h::VA_hp.An ri:mnrted.

-2óñ
oúrs
'TcY
~'õl
ì~~~
Tìíe
"ap
pare
nt h
alf-
I.ife
åf 9
-hyd
roxy
rispe
rldon
ewas
"about 2'1"'ho,urs'(CV=20%) in extensive
ïrie
t¡ib
oliz
ers
arid
30
hOIJ
rs'(C
V=
25%
) lu
poo
rm
etab
oliz
ers,
Ste
ady-
stat
e co
ncer
itrat
ions
'of
rispe
ridan
e ,a
re r
each
ediñ
1 :d
ay in
ext
ensi
vem
etab
oliz
ersa
nd w
ould
'be
expe
cted
to r
each
stea
dy s
tate
in a
bout
5 d
ays
in'p
oorm
etab
oliz
ers,
Ste
ady-
stat
e co
ncen
trat
ions
,of 9
-hyd
roxy
-ris
perid
one
are
reac
hed
in' 5
-6 d
ays'
(mea
sure
dir
iext
ensi
ve m
etab
oliz
ers)
,B
ecal
lse.
ris
peri
done
' and
9-h
ydro
xyri
sper
idon
ear
e ap
prox
imat
ely
eqlli
-affe
ctiV
e;'th
e sü
ni o
f the
irco
ncen
trat
ions
is p
ertin
ent T
he'p
harr
iaco
ki-
n.eJ
ics
ohth
e su
m o
f ris
perid
one
and
, 9-h
ydro
xyris
perid
one;
afte
r si
ngle
and
mul
tiple
- do
ses,
wer
e.sj
mila
rin
exte
nsiv
e an
d po
or, m
etab
oliz
ers:
",i.t
h an
ove
rallm
eari
eHni
inat
ion
"hai
f-iie
of,
abo
ut '2
0 h.
ours
. In
anal
yses
com
parin
g ~
àdve
'rs~
e re
actio
n r¡
:tes
in. ,
exte
nsiv
ean
d po
or m
etab
oliz
ers
in c
ontr
ollé
d''a
nd o
pen
stud
ies:
no
impo
rtan
t diff
eren
cesw
ere
seen
.R
ispe
rido
ne.c
ould
be
subj
ect f
o lv
iåki
rids
'of
drug
-dru
g in
te'rà
ctio
ns. F
irst,
inhi
bito
rs o
fcy
toch
rom
e P
",IID
, cou
ld' i
ntat
fere
with
conv
ersi
on o
f ris
perid
on'e
't09.
hydr
ox-
yris
perid
one.
Thi
s in
fact
occ
urs
with
qui
nidi
ne,
givi
ng e
ssen
tiaily
ail
reci
pien
ts a
:ris
peri
done
phar
mac
okin
etic
pro
fie ty
pica
l "of
poo
rm
etab
oliz
ers.
Tn,
e fa
vora
bie
and
adve
rse
effe
cts
of r
ispa
ridoh
e in
. pat
ient
s re
cei,V
in9,
quin
idin
eha
ve' n
ot b
een
eval
uate
d, b
ut o
bser
vatio
ns in
am
odes
t num
ber
(n=
70)
of p
oorm
etáb
oliz
ers
give
n ris
perid
one.
dono
t sug
gest
.im
port
ant
diff
eren
ces
betw
een
poor
and
ext
ensi
vem
etab
oliz
ers.
It w
ould
ais
o be
pos
sibl
e,lo
rri
sper
idpn
e to
inle
rfer
e ",
ith m
etab
olis
m o
f :o
ther
drug
s m
etab
oliz
edb1
\cyt
oc~
'orn
e_p"
,I.D
,.R
elat
ivel
y w
eak
bind
ingo
tris
peri
done
to. t
heen
zym
e su
gges
ts th
is is
unl
iKel
y (S
eeP
RE
CA
UT
ION
S a
nd D
RU
G IN
TE
RA
CT
ION
S).
The
pla
sma
prot
ein
bind
ing
of r
ispe
ridon
e w
as a
bout
90%
ove
r th
e in
vitr
o co
ncen
trat
ion
rang
e,
of 0
:5 to
200
ng/m
L an
d in
crea
sed
with
incr
easi
ng c
once
ntra
tions
of a
,-ac
id g
iyco
prot
ein.
Tne
pla
sma
bind
ing
of9-
hydr
oxyr
ispe
ridon
e w
as 7
7%. N
eith
er th
e pa
rent
nor
the
met
abol
ite d
ispl
aced
eac
h ot
her
from
the
plà~
ma
bind
ing,
site
s, H
igh
ther
apeu
tic c
once
ntra
tions
of s
ulfa
met
hazi
ne (
100
~g/
mL)
, war
farin
(10
~g/
mL)
and
carb
amaz
epin
eJ10
~g1
mL)
cau
sed
only
a s
light
incr
eas"
.in. t
he fr
ee .t
ract
ion
of r
ispe
ridon
e at
10
nglm
L an
d9-hydroxyrrspendone at 50 nglmL, changes of unknown climcal significance. ,,, '.'
Spe
cial
Pop
ulat
ions
Ren
al
Impa
irmen
t: In
pat
ient
s w
ith m
oder
ate
to s
ever
e re
nal d
isea
se, d
lear
aric
e of
the
sum
of r
ispe
ridon
ean
d its
act
ive
met
abol
ite d
ecre
ased
by
60%
com
pare
d to
you
ng h
ealth
y su
bjec
ts. R
ISP
ER
DA
L ~
dos
es s
houl
dbe
red
uced
in p
atie
nts
with
ren
al d
isea
se (
See
PR
EC
AU
TIO
NS
an
d D
OS
AG
EA
ND
,AD
MIN
IST
RA
TIO
N),
Hep
atic
Im
pair
men
t: W
hile
the
phar
mac
okin
etic
s of
ris
peri
done
in s
ubje
cts
wit
liver
-dis
ease
wer
e co
mpa
rabl
eto
thos
e in
you
ng h
ealth
y su
bjec
ts, t
he m
ean
free
frac
tion
of r
ispe
ridon
e in
pla
sma
was
incr
ease
db¥
abou
t35
% b
ecau
se o
f th
e di
min
ishe
d co
ncen
trat
ion
of b
oth
albu
min
and
a,a
cid
glyc
opro
tein
, RIS
PER
DA
L d
oses
shou
ld b
e re
d~ce
d in
pat
ient
s w
ith li
ver
dise
ase
(See
PR
EC
AU
TIO
NS
and
, D
OS
AG
E A
ND
AD
MIN
iST
RA
TIO
N),
Eld
erly
: In
h'ea
lthy
elde
rly s
ubje
cts
rena
l cle
aran
ce o
f bot
h ris
perid
one
and9
-hyd
roxy
rispe
ridon
e'w
asd.
ecre
ased
, and
-,el
imin
atio
n ha
lf-liv
es w
ere
prol
onge
d co
mpa
red
to y
oung
hea
lthy
subj
ects
. Oos
ings
houl
dbe
mod
ifed.
acco
rdin
gly
in th
e ei
derly
pat
ient
s (S
ee D
OS
AG
E A
ND
AD
MIN
IST
RA
TIO
N).
Rac
e an
d G
ende
r E
ffect
s: N
o sp
ecifi
c ph
arm
acok
inet
ic s
tudy
was
con
duct
ed to
inve
stig
ate
race
and
gend
er e
ffect
s, b
ut a
pop
ulat
ion
phar
mac
okin
etic
ana
lysi
s di
d no
t ide
ntiy
impo
rtan
t diff
eren
ces
in th
edi
spos
ition
of r
ispe
ridon
e du
e to
gen
der
(whe
ther
cor
rect
ed fo
r bo
dy w
eigh
t or
not)
or
race
.
~~~
::r-
vl-
ilUl
~:!"
§8 (T
, ~.~
::vi
vO p ;i'
3 r:
~
IIL
.~~ "
;7~2
Yg~ ~
~ (
f gr
¡;i~
,&i
~~ (f
:o~.
m Z75
0322
0
i'àic
fiye
Dys
kine
sìa
A s
yndr
ome
of p
oten
tially
irre
vers
ible
; inv
oiun
tary
, dys
kine
tic m
ovem
ents
may
dev
elop
in ,p
atie
nts
trea
ted
With
ant
ipsy
chot
ic d
rÙgs
., A
lthou
gh th
e pr
eval
ence
of
the
synd
rom
e ap
pear
s to
'be
high
est a
mon
g th
e el
derly
,es
peci
ally
eld
erly
wom
en, i
t is
impo
ssib
le to
rel
y up
on p
reva
lenc
e es
timat
es to
pre
dict
, at t
he in
cept
ion
ofan
tipsy
chot
ic tr
eatm
ent,
whi
chpa
tient
s.ar
e lik
ely,
to d
evei
op th
e"sy
n,dr
ome.
whe
ther
an
tipsy
chot
ic d
rug
prod
ucts
diff
er in
thei
r po
tent
ial t
o ca
use
tard
ive
dysk
ines
ia is
unk
now
n.T
he r
isk
Of d
evel
opin
g ta
rdiv
e dy
skin
esia
an
d th
e lik
elih
ood
that
it w
il be
com
e ir
reve
rsib
le a
re b
elie
ved
toin
crea
se a
s. th
e du
ratio
n oU
reat
men
t and
the
tota
l cum
ulat
ive
dose
,of
antip
sych
otic
dru
gs a
dmin
iste
red
toth
e pa
tient
incr
ease
. How
ever
, the
syn
drom
e ca
n de
velo
p, a
lthou
gh m
uch
less
com
mon
ly, a
fter
rela
tivel
ybr
ief t
reat
men
t per
iods
at/o
w d
oses
.T
here
is n
o kn
own
trea
tmen
t fo
r es
tabl
ishe
d ca
ses
of ta
rdiv
e dy
skin
esia
, alth
ough
the
synd
rom
e m
ay r
emit,
part
ially
or,
co
mpl
etel
y,
if a
ntip
sych
otic
trea
tmen
t is
with
draw
n. A
ntip
sych
otic
trea
tmen
t, its
elf;
how
ever
, may
supp
ress
(or
par
tially
sup
pres
s) th
e si
gnS
' and
sym
ptom
s of
the
synd
rom
e an
d th
ereb
y m
ay p
ossi
bly
mas
k th
eU
nder
lyin
g pr
oces
s. T
he e
ffect
that
sym
ptom
atic
su
ppre
ssio
n ha
s up
on th
e lo
ng-t
erm
cou
rse
of th
e,~
yndr
ome
is u
nkno
wn.
Giv
en th
ese
cons
ider
atio
,ns,
.i;l,
ISP
ER
DA
L ~
(ris
perid
one)
sho
uld
be p
resc
ribed
in a
man
ner
that
is m
ost,
likel
y to
min
imiz
e th
e oc
urre
nce
of. t
ardi
ve d
yski
ne,s
ia..
Chr
onic
ant
ipsy
chot
ic tr
eatm
ent s
houl
d ,g
ener
aliy
be
rese
rved
for
patie
nts
who
suf
fer
from
a q
iiron
ic il
ness
that
(1)
i",k
now
n to
res
pond
,to
ant
ipsy
chot
ic
drug
s, a
nd (
2) fo
r w
hom
alte
mat
ive,
equ
ally
ef
fect
e, b
ut p
oten
tially
less
ham
iful t
reat
men
ts a
re n
ot a
vaila
ble
or a
ppro
prja
te. I
n pa
tient
s w
hodo
req
uire
chr
onic
trea
tmen
t, th
ß sm
alle
st d
ose
and
the
shpr
test
dur
atio
n of
trea
tmen
tpro
duci
ng a
sati"
f¡ic
tory
clin
ical
res
pons
e sh
ould
be,
sou
ght T
he n
eed
for
cont
inue
d tr
eatm
ent s
haul
d be
'reas
sess
ed p
erio
dica
llIf
sign
s an
d sy
mpt
oms
of ta
rdiv
e dy
skin
esia
app
ear
in a
pat
ient
on
RIS
PE
RD
AL~
¡dru
g di
scon
iinua
tion
sl)o
uld
be c
onsi
dere
d, H
,ow
ever
, som
e, p
atie
nts
may
req
uire
trea
tmen
t with
RIS
P.E
RD
AL
~de
spite
the
pres
ence
of t
he s
yndr
ome.
Pote
ntia
l for
Pro
arrh
ythm
ic E
ffec
t~: R
ispe
rido
ne a
ndlo
r9,h
ydro
xyri
sper
idon
e ap
pear
s to
leng
tnen
the
OT
inte
rval
in s
ome
patie
nts,
alth
ough
ther
e i"
no a
vera
ge in
crea
se in
trea
ted
patie
nts,
eve
n at
12-
16 n
ig/d
ay,
wel
l abo
ve th
e re
com
men
ded
dose
. Oth
er d
rugs
that
pro
long
the
OT
inte
rva,
l hav
e be
en a
ssoc
iate
d w
it!)
the
occu
rren
ce o
f tor
sade
sde
poin
tes,
a li
fe-t
hrea
teni
ng, a
rrhy
thni
ia, B
rady
card
ia, e
lect
roly
te im
bala
nce,
conc
omita
nt' u
se w
ith o
ther
dru
gs' t
hat p
rolo
ng O
T, o
r th
e pr
esen
ce o
f con
geni
tal p
roio
ngat
ion
in O
T c
anin
crea
se th
e ri
sk f
or o
ccur
renc
e of
this
arr
hyth
mia
. 'PR
EèA
UT
ION
SG
ener
al ,
Orthostatic Hypotenslori:RISPERDAL ~ (risperidone) may induce
orth
osta
tic h
ypot
ensi
on ¡
¡¡¡s
ecia
ted,
with
dizz
ines
s, ta
chyc
ardi
a, a
nd in
som
e pa
tient
s, s
ynco
pe, e
spec
iallý
dur
ing
the
initi
al d
ose'
i¡tra
tion
perip
d,pr
obab
ly
refle
ctin
g its
alp
ha:a
dren
ergi
c an
tago
nist
ic
prop
ertie
s, S
ynco
p~w
as r
epor
ted
1n 0
.2%
'(6/2
607)
of
RIS
PE
RD
AL
~ tr
eate
d pa
tient
s in
' pha
se 2
'3 s
tudi
es:'T
he' r
isk
of o
rtho
stat
ic h
ypot
ensi
on a
nd s
ynco
pe m
ay b
em
inim
ized
by
limiti
ng th
e in
itial
dos
e to
2m
g to
tal (
eith
er'O
D o
r t m
gBID
) iri
'Orm
al a
dults
ana
O,5
'mg'
BID
in the elderly and patients with renal or hepatic impairment (See DOSAGE
AN
D A
DM
INIS
TR
AT
ION
),M
onito
ring
of o
rtho
stat
ic v
itai s
igns
sho
uld
be
cons
ider
ed in
pat
ient
s fo
r w
hom
mis
is o
f co
ncem
"A d
ose
redu
ctio
n sh
ould
be
cons
ider
ed. i
f hy
pote
nsio
n oc
curs
, RIS
P,E
RD
AL
~ s
l)oul
d be
,use
d w
ith p
artic
ular
'cau
tion
in p
atie
nts
with
kno
wn
card
iova
"cul
ar d
isea
se .(
hist
ory
of m
yoqa
rdia
i inf
arct
ion
9r is
cher
nia,
hea
rt/a
ilure
, or
cond
uctio
n ab
norn
ialit
ies)
; cer
ebro
vasc
ular
dis
ease
, and
con
ditio
ns w
hich
woO
ld p
redi
spos
e pa
tient
s to
hypo
tens
ion
e.g:
, deh
ydra
tion
and
hypo
vole
mia
. Clin
ical
ly s
igni
fican
t hyp
oten
sion
has
bee
n ob
serv
ed w
ithconcomitant use of RISPERDAL~arlantihypertensive medication, _
Sei
zuiis
: Dur
ing
prem
arke
ting
test
ing,
sei
zure
s oc
urre
d in
0.3
% (
9/26
07)
of R
ISP
ER
DA
L ~
trea
ted
patie
nts,
'tw
oin
ass
ocia
tion
with
hyp
onat
rem
ia. R
ISP
ER
DA
L~ s
houl
d be
use
d ca
utio
usly
in p
atie
nts
with
a,h
isto
ry o
f sei
zure
s.D
ysph
agia
: Eso
phag
eal d
ysm
otili
ty,a
ndas
pira
tion
have
bee
n as
soci
ated
with
ant
ipsy
chot
ic
drug
use
. Asp
iratio
npn
eum
onia
is a
com
mon
caus
e,of
.mor
bidi
ty a
nd m
orta
lity
in p
atie
nts
with
adv
ance
d A
lzhe
imet
s de
men
tia.
RIS
PE
RD
AL~
and
oth
er a
ntip
sych
otic
dru
gs
shou
ld b
e us
ed
caut
ious
ly in
pat
ient
s at
ris
k fo
r as
pira
tion
pneu
mon
ia.
, Hyp
erpr
olac
tinei
nia:
As
wiih
' btn
er d
rugs
that
ant
agen
iie d
opam
ineD
, rec
epto
rs, r
ispe
ridô
na e
leva
tes
prol
actin
,leve
ls a
nd th
e el
evat
ion
pers
ists
'dur
ing
chro
nic
adm
inis
trat
ion.
Tis
sue
cultu
re e
Xpe
rimen
ts in
dica
te'
that
appr
oxim
atel
y on
e-th
ird o
f hum
ari'b
reas
t can
cers
are
pro
lact
in d
epen
aent
in v
.itro
: 'a
fact
or e
fpot
entia
i im
port
ance
if th
e pr
escr
iptio
n of
the
se
drug
s is
con
teni
plat
ed in
a pa
tient
with
pre
viou
sly
dete
cted
bre
aste
aric
er, A
ltoug
h di
str-
banc
es s
uch
as g
alac
torr
ea; a
meh
orre
a, g
yecs
ta, a
nd im
pote
nce
have
bee
n re
port
ed w
ipro
lact
n-el
evat
ing
com
poun
ds, t
he c
linic
al s
igni
fican
ce o
f ele
vate
d se
rum
pro
lact
in le
vels
is u
nknO
Wn
for
mos
t pat
ient
s. A
s is
com
mon
with
com
poun
ds w
hich
. inc
reas
e pr
olac
tin r
elea
se, a
n in
crea
se
in p
itu"a
ry g
land
, m
amm
ary
glan
d, a
ndpa
ncr~
¡itic
isle
t cel
l hyp
erpl
asia
and
lor
neop
lasi
a w
as, o
bser
ved
in,.h
eris
perid
one
carc
inog
enic
ity,s
tudi
esconducted in mice,and rats,(See CARCINOI3ENESIS).However, neither clipical studies.
nor
epid
emio
logi
cst
udie
s co
nduc
ted
to d
ate
have
sho
wn
an a
ssoc
iatio
n be
twee
n ch
roni
c ad
min
istr
atio
n of
this
cla
ss o
f dru
gsan
d tu
mor
igen
esis
in h
uman
s; th
e av
aila
ble
evid
ence
is c
onsi
dere
d to
o lim
ited
to b
e co
nclu
sive
at t
his
time.
--

~IPotential for Cognitive and Motorlmpairment:Somnolence was a commonly re
port
ed a
dver
se e
vent
asso
ciat
ed w
ith R
ISP
ER
DA
L~ tr
eatm
erit,
espe
cial
lyw
hen
asce
rtai
ned
by
dire
ct q
uest
ioni
ng o
f pa
tient
s. T
his
adve
rse
even
t is
dose
rel
ated
, and
ina
stud
y ut
ilizi
ng a
che
cklis
t to
dete
ct a
dver
se e
vent
s, 4
1 %
of t
he h
igh
dose
patients (RISPERDAL~ 16 mg/day) reported somnolence compared
to 1
6% o
f pla
cebo
pa
tient
s. D
irect
ques
tioni
ng is
m
ore
sens
itive
for
dete
ctin
g ad
vers
e ev
ents
than
:spo
ntan
eous
rep
ortin
g, b
y w
hich
8%
of
RISPERDAL~ 16 m~day patients and 1% of placebo patients reported somnolence as an
adve
rse
even
t.Since,RISPERDAL has the potential to impair.judgment, thinking, or motor skills, patients
shou
ld b
eca
utio
ned
abou
t ope
ratin
g ha
zard
ous
mac
hine
ry, i
nciu
ding
aut
omob
iles,
. un
ti th
ey a
re
reas
onab
ly c
erta
inth
at R
iSP
E.R
DA
L~ th
erap
y do
es n
ot a
ffect
them
adv
erse
ly.
Pria
pism
: Rar
e ca
ses
of p
riapi
sm h
ave
been
rep
orte
d. W
hile
the
rela
tions
hip
of th
e ev
ents
to R
ISP
ER
DA
L ~
use
has
not b
een
esta
blis
hed,
oth
er d
rugs
with
alp
ha-a
dren
ergi
c bl
ocki
ng e
ffect
s ha
ve b
een
repo
rted
toin
duce
pria
pism
, and
it is
pos
sibl
e th
at R
ISP
ER
DA
L ~
may
sha
re th
is c
apac
ity. S
ever
e.
pria
pism
may
req
uire
surg
ical
inte
rven
tion.
Thr
ombo
tic T
hrom
bocy
tqpe
nic
Purp
ura
(TP)
: A s
ingl
e ca
se o
f T
IP w
a.s
repo
rted
in a
28
year
-oid
fem
ale
patie
nt r
ecei
ving
RIS
PE
RD
AL~
in a
larg
e,
open
pre
mar
ketin
g ex
perie
nce
(app
roxi
mat
ely
1300
.pat
ient
s). S
heex
peri
ence
d ja
undi
ce, f
ever
, and
bru
isin
g, b
ut e
vent
ually
rec
over
ed a
fter
rec
eivi
ng p
lasm
aphe
resi
s. T
here
latio
nshi
p to
RIS
PE
RD
AL
~ th
erap
y is
unk
now
n.A
ntie
met
ic e
ffec
t: R
ispe
rido
ne h
as a
n an
tiem
etic
eff
ect i
n an
imal
s; th
is e
ffec
t may
als
o oc
cur
in h
uman
s,an
d m
ay m
ask
sign
s an
d sy
mpt
oms
of o
verd
osag
e w
ith c
erta
in d
rugs
or
of c
ondi
tions
suc
h as
inte
stin
alob
stru
ctio
n, R
eye:
s sy
ndro
me,
and
bra
in tu
mor
.Body Temperatwe Regulation: Disruption of
body
tem
pera
ture
reg
ulat
ion
has
been
attr
ibut
ed
to a
ntip
sych
otic
agents.. Both hyperthermia and hypothermia haved,een reported
in a
ssoc
iatio
n w
ith R
ISP
ER
DA
L~: u
se.
Cau
tion
is a
dvis
ed w
hen
pres
crib
ing
for
patie
nts
who
will
be
expo
sed
to te
mpe
ratu
re e
xtre
mes
.S
uici
de:T
hepo
ssib
ility
of a
sui
cide
atte
mpt
is in
here
nt in
sc
hizo
phre
nia,
and
clo
se s
uper
Vis
ion
of h
igh
risk
patie
nts
shou
ld a
ccom
pany
diu
g th
erap
y, P
resc
riptio
ns fo
r'RIS
PE
RD
AL
~ s
houl
d be
writ
ten
for
the
smal
lest
quan
tity
of ta
blet
s co
nsis
tent
with
'goo
d pa
tient
man
agem
ent,
in o
rder
to r
educ
e th
e ris
k of
ove
rdos
e.U
se in
Pat
ient
s w
ith C
onco
mita
nt II
ness
: Clin
icai
exp
erie
nce
with
RIS
PE
RD
AL
~ in
pat
ient
s w
ith c
erta
inconcomitant systemic ilnesses
is li
mite
d. C
autio
n is
adv
isab
le.in
usi
ng R
ISP
ER
DA
L~ in
pat
ient
s W
ithdi
seas
es o
r co
nditi
ons
that
cou
ld
affe
ct m
etab
olis
m o
r he
mod
ynam
ic
resp
onse
s.RISPERDAL~ has
not b
een
evai
uate
d or
use
d to
any
app
reci
able
ext
ent i
n pa
tient
s w
ith. a
rec
ent h
isto
ry o
fm
yoca
rdia
l inf
arct
ion
or u
nsta
ble
hear
t dis
ease
. Pat
ient
s w
ith th
ese
diag
nose
s w
ere
excl
uded
from
clin
ical
stu
dies
durin
g th
e pr
oduc
t's p
rem
arke
t tes
ting.
The
ele
ctro
card
iogr
ams
of a
ppro
xim
atel
y 38
0'pa
tient
s w
hô r
ecei
ved
RIS
PE
RD
AL~
and
120
pat
ient
s w
ho r
ecei
ved
plac
ebo
in tw
o do
uble
-blin
d, p
lace
bo-c
ontr
olle
d tr
ials
wer
eev
alua
ted
and
the
data
rev
eale
d on
e fin
ding
of p
oten
tial c
once
m, i
.e,;
8 pa
tient
s'ta
king
RIS
PE
RD
AL
$ w
hose
baseline OTcinterval was iessthan 450
mse
c,
wer
e ob
serv
ed to
hav
e O
Tc
inte
rval
s gr
eate
r th
an 4
50 m
sec
duri
ng tr
eatm
ent;
no s
uch
prol
onga
tions
wer
e se
en in
the
smal
ler
plac
ebo
grou
p. T
here
wer
e 3
such
epi
sode
s in
the
appr
oxim
atel
y 12
5 pa
tient
s w
ho r
ecei
ved:
halo
perid
ol:B
ecau
se o
f the
'risk
s of
ort
host
atic
hyp
oten
sion
and
OT
pro
long
atio
n, c
autio
n sh
ould
be
obse
rved
In c
ardi
ac p
atie
nts
(See
WA
RN
ING
S a
nd P
RE
CA
UT
ION
S),
Incr
ease
d pl
asm
a'co
ncen
trat
ions
ofris
perid
one
and
9-hy
drox
yris
perid
one
occu
r in
pat
ient
s w
ith s
ever
ere
nal i
mpa
irmen
t (c
reat
ìnin
e cl
eara
nce
,,30
mU
min
/1.7
3 01
'), a
nd a
n in
crea
se in
the
free
frac
tion
of th
eris
perid
one
is s
een
in p
atie
nts
with
sev
ere
hepa
tic im
pairm
ent.
A lo
wer
sta
rtin
g do
se s
houl
d be
use
d in
suc
hpa
tient
s (S
ee D
OSA
GE
AN
D A
DM
iNIS
TR
AT
ION
). .
Information for Patients .
Phy
sici
ans
are
advi
sed
to d
iscu
ss th
e fo
llow
ing
issu
es w
ith p
atie
nts
for
who
m th
ey p
resc
ribe
RIS
PE
RD
AL~
,O
rtho
stat
ic H
ypot
ensi
on: P
atie
nts
shou
ld b
e ad
vise
d of
the
risk
of o
rtho
stat
ic h
ypot
ensi
on, e
spec
ially
dur
ing
the
perio
d of
initi
al d
ose
titra
tion,
Inte
rfer
ence
With
Cog
nitiv
e an
d..M
otor
Per
form
ance
: Sin
ce R
ISP
ER
DA
L $
has
the.
pot
entia
l to
impa
irju
dgm
ent,
th,in
king
, or
mot
or s
kils
, pat
ient
s sh
ould
be
caut
ione
d ab
out p
pera
ting
haza
rdou
s m
achi
nery
, inc
ludi
ngau
tom
obile
s, u
ntil
they
are
rea
sona
bly
cert
ain
that
RiS
PE
RD
AL~
ther
apy
does
not
affe
ct th
em a
dver
sely
.P
regn
ancy
: Pat
ient
s sh
ould
be
advi
sed
to n
otify
thei
r ph
ysic
ian
if th
ey b
ecom
e pr
egna
nt o
r in
tend
to b
ecom
epregnant during therapy, .'. '.' . .' .
Nur
sing
: Pat
ient
s sh
ould
. be
advi
sed
not t
Q b
reas
t fee
d an
infa
nt if
they
.are
taki
ng R
ISP
ER
DA
L~,
Con
c.om
itant
Med
icat
ion:
Pat
ient
s sh
ould
be
advi
sed
to in
fonn
thei
r ph
ysic
ians
if th
ey a
re ta
king
, or
plan
tota
ke, a
ny p
resc
riptio
n or
ove
r-th
e-co
unte
r dr
ugs,
sin
ce th
ere
is a
pot
entia
l for
inte
ract
ions
.A
lcoh
ol:
Pat
ient
s sh
ouid
be
advi
sed
to a
void
alc
ohol
whi
le ta
king
RiS
PE
RD
AL~
., L
abor
ator
y T
ests
No
spec
ific
labo
rato
ry te
sts
are
reC
Om
men
ded.
Dru
g In
tera
ctio
nsT
he in
tera
ctiO
ns o
f RiS
PE
RD
AL
~ a
nd o
ther
dru
gs h
ave
not b
een
syst
emat
ical
ly e
valu
ated
. Giv
en th
e pr
imar
yC
NS
effe
cts
olris
perid
one,
cau
tion
shou
ld b
e us
ed w
hen
RIS
PE
RD
AL~
is ta
ken
in c
ombi
natio
n w
ith o
ther
cent
rally
act
ing
drug
s an
d al
coho
L.
Bec
au"e
of i
ts p
oten
tial f
or in
duci
ng h
ypot
ensi
on, R
ISP
ER
DA
L ~
may
enh
ance
the
hypo
tens
ive
effe
cts
ofot
her
ther
apeu
tic a
gent
s' w
ith th
is p
Ote
ntia
L.R
ISP
ER
DA
L ~
may
ant
agon
ize
the
effe
cts
of le
vodo
pa a
nd d
opam
ine
agon
ists
.C
hron
ic a
dmin
istr
atio
n of
car
bam
azep
ine
with
ris
perid
one
may
incr
ease
the
clea
ranc
of r
ispe
ridon
e.C
hron
ic a
dmin
istr
atio
n of
clo
zapi
ne w
ith r
ispe
ridon
e m
ay d
ecre
ase
the
clea
ranc
e of
ris
perid
one.
Flu
oxet
ine
may
incr
ease
the
plas
ma
conc
entr
atio
n of
the
anti-
psyc
hotic
frac
tiOn
(ris
pedd
one
plus
9-h
ydro
xy-
risp
erid
one)
b¥.
r~is
in.~
.th.e
_ C
?n""
nt.r
~ti~
!,_
of. ~
s!?,
,!!~
?_n.
e:!l
lipu¥
!:n?
t,th"
_è'..
tiV!~
:t~~.
~I!!
~2;!
'J~;
.~~:
i~R
~~!~
o,n;
:.,

Dru
gslh
st in
~iE
ìfêY
ióc¡
¡õm
e'í;~
;iìòi
~iid
'()t~
èrFt
šòzY
;ñ¡l
š!A
ìšPë
RêJ
dnW
¡"~r
ñéft
föf~
xy"
~ri
sper
idon
e by
byt
ochr
omep
,,,II
D,,
an e
rizy
met
hat i
spol
ymor
ptiic
in th
e po
pula
tion
a,nd
that
can
be
inhi
bite
dby
a v
arie
ty o
f Psy
chpt
ropi
c 'a
nd
othe
r drugs (See CUNI,CALPHARMACOLOGY). Drug interactions' th
atre
duce
the
met
abol
ism
of r
isp~
ridon
e'to
9-h
ydro
xyris
perid
one
wou
ld in
crea
s,eJ
he p
lasm
a co
ncen
trat
ions
of
rispe
ridon
e an
d lo
wer
the'
con
cent
ratip
ns q
f"g-
hydr
oxyr
ispe
ridon
e. A
naly
sis
of c
linic
al s
tudi
es in
volv
ing
am
odes
t num
ber
of p
oor
met
abòl
ize'
rs'(n
=70
) do
es n
ot s
ugge
st th
at p
oor
and
exte
nsiv
e m
etab
oliz
ers
have
diffe
rent
rat
es o
f adv
erse
effe
cts.
No
com
paris
on
,at '
effe
ctiv
enes
s'
in th
e tw
o gr
oups
has
bee
n m
ade.
In v
itro
stud
ies
show
ed th
at d
rugs
met
abol
ized
bý
othe
r P
,,, is
ozým
es"in
clud
ing
1A1,
lA2,
IIC
9, M
P, a
ndIII
A4,
are
onl
y w
eak
inhi
bito
rs a
t ris
perid
onem
etab
olis
m.
Dru
gs M
etab
oliz
ed b
y C
yoch
rom
e P
",IID
,: in
vitr
o st
udie
s in
dica
te th
at r
ispe
ridon
e is
a r
eiat
ivel
ywea
k in
hibi
tor
of c
ytoc
hrom
e P
,,,IID
,. T
here
fore
, R.lS
PE
RD
AL.
is n
ot e
xpec
ted
to s
ubst
antia
liy In
hibi
t the
cle
aran
ce o
f dru
gs th
atar
e m
etab
oliz
ed b
y th
is e
nzym
atic
pat
hWay
. How
ever
, clin
icai
dat
a to
con
firm
this
exp
ecta
tion
are
not a
vaila
bie.
Car
cino
gene
sis,
Mut
agen
esis
, Im
pair
men
t of
Fert
ilty
Car
cino
gene
sis:
Car
cino
geni
city
stu
dies
wer
e co
nduc
ted
in S
wis
s al
bino
mic
e an
d W
ista
r ra
t~. F
ii~pe
ridon
ew
as a
dmin
iste
red
in th
e di
et a
t dos
espt
0.6
3,2.
5, a
nd 1
0 m
g/kg
for
18 m
onth
s to
mic
e an
d fo
r 25
mon
ths
tora
ts. T
hese
dos
es a
re e
quiv
alen
t to
'2:4
, 904
and
37.
5 tim
es th
e m
axim
um h
uman
dos
e (1
6 m
g/da
y) o
n a
mg/
kg b
asis
or
0.2,
0.75
and
3
times
the
max
imum
hum
an d
ose
(mic
e) o
rOA
, 1.5
, and
6
times
the-
max
imum
hum
an d
ose
(rat
s) o
n a
mg/
m2
basi
s, A
max
imum
tole
rate
d do
se w
as n
ot a
chie
ved
in m
ale
mic
e:J~
,her
e w
ere
stat
istic
aliy
sig
nific
ant i
ncre
ases
in p
ituita
ry g
land
ade
nom
as, e
ndoc
rine
panc
reas
ade
nom
as' a
nd
mam
mar
ygi
and
aden
ocar
cino
mas
. The
fol
low
ing
tabl
e su
mm
ariz
es th
e m
uitip
les
of th
e hu
man
dos
e, o
n a
mgi
m2
(mg/
kg)
basi
s at
whi
ch th
ese
tum
ors
occu
rred
MU
LTIP
LE O
F M
AX
IMU
M H
UM
AN
DO
SE
in m
gim
2 (m
gikg
)T
UM
OR
TY
PE
SPE
CIE
SSE
XL
OW
EST
HIG
HE
STE
FFE
CT
NO
EFF
EC
TL
EV
EL
LE
VE
LP
ituita
ry a
deno
mas
mou
sefe
mal
e0.
75 (
9.4)
0:2,
(2,4
)E
ndoc
rine
panc
reas
rat
mal
e1.
5 (9
.4)
0:4
(2.4
)ad
enom
asM
amm
ary
glan
dm
ouse
fem
ale
0.2
(2.4
)no
nead
enoc
arci
nom
asra
tte
mai
e00
4 (2
.4)
none
rat
mal
e6
(37.
5)1.
5 (9
.4)
Mam
mar
y gi
and
rat
mai
e1.
5 (9
.4)
0:4
(2.4
)ne
opla
sms,
Tot
al
Ant
ipsy
chot
ic d
rugs
hav
e be
en s
how
n to
chr
onic
ally
ele
vate
pro
lact
in ie
vels
in r
oden
ts. S
erum
pro
iact
inle
vels
wer
e no
t mea
sure
d du
ring
the
rispe
ridon
e ca
rcin
ogen
icity
stu
dies
; how
ever
, mèa
sure
men
ts d
urin
gsu
bchr
onic
toxi
city
stu
dies
sho
wed
that
ris
perid
one
elev
ated
ser
um p
rola
ctin
leve
ls 5
to 6
fold
'in m
ice
and
rats
at t
he s
ame
dose
s us
ed in
tlie
car
cino
geni
city
stu
dies
.-A
n in
crea
se in
mam
mar
y, p
itUita
ry, a
nden
docr
ine
panc
reas
neo
plas
ms
has
been
foun
d in
rod
ents
afte
r ch
roni
c ad
min
istr
atio
n of
oth
er
antip
sych
otic
drug
s an
d is
con
side
red
to b
e pr
olac
tin m
edia
ted.
The
rel
evan
ce fo
r hu
man
ris
k of
the
find
ings
of
prol
actin
-",
edia
ted
endo
crin
e tu
mor
s in
rod
ents
, is
unkn
own
(See
Hyp
rpro
lact
inem
ia u
nder
PR
EC
AU
TIO
NS
" G
EN
ER
AL)
.M
utag
enes
is: N
o ev
iden
ce a
t mut
agen
ic p
oten
tial f
ouis
perid
one
was
foun
d in
the
Am
es r
ever
se m
utat
ion
:est
, mou
se iy
mph
oma
assa
y, in
vitr
o ra
t hep
atoc
yte
DN
A-r
epai
r as
say,
in v
ivo
mic
ronu
cleu
s te
sUn
mic
e,:h
e se
x-lin
ked
rece
ssiv
e le
thai
test
in D
roso
phila
, or
thè
chro
mos
omal
abe
rrat
ion
test
in h
uman
lym
phoc
ytes
Jr Chinese hamster cells. ,
'mpa
irmen
t of F
ertil
ity: R
ispe
ridon
e (0
.16
to 5
mgi
g) w
as s
how
n to
impa
ir m
atin
g, b
ut n
ot fe
rtlit
y, in
Wis
tar
rats
n th
ree
repr
oduc
tive
stud
ies
(tw
o S
egm
ent I
and
a m
ultig
ener
atio
nal s
tudy
) at
dos
es 0
.1 to
3 ti
mes
the
max
imum
'eco
mm
ende
d hu
man
dos
e on
a m
g1m
2 ba
sis.
The
eff
ect a
ppea
red
to b
e in
fem
ales
sin
ce im
pair
ed m
atin
gie
havi
or w
as n
ot n
oted
in th
e S
egm
ent i
stu
dy in
whi
ch m
ales
onl
y w
ere
trea
ted.
In a
sub
chro
nic
stud
y in
Bea
gle
logs
in w
hich
ris
peri
done
was
adm
inis
tere
d at
dos
es o
f 0.
31 to
5 m
gig,
spe
rm m
otili
t and
con
cant
ratio
n w
ere
leer
ease
d at
dos
es 0
.6 to
10
times
the
hum
an d
ose
on a
mg/
m2
basi
s, D
ose-
rela
ted
deer
ease
s w
ere,
als
o, n
oted
1 se
rum
test
oste
rone
at t
he s
ame
dose
s. S
erum
test
oste
rone
and
spe
rm p
aram
eter
s pa
rtia
lly r
ecov
ered
but
emai
ned
decr
ease
d af
ter
trea
tmen
t was
dis
cont
inue
d. N
o no
-effe
ct d
oses
wer
e no
ted
in e
ither
ràt
or
dog.
'regn
ancy
''regnancyCategory C:The
tera
toge
nic
pote
ntia
l of
'risp
erid
onew
as
stud
ied
in th
ree
Seg
men
t II s
tudi
es in
.pra
gue-
Daw
ley
and
Wis
tar
rats
and
in o
ne S
egm
ent I
I stu
dy in
New
Zea
iand
rab
bits
. The
inci
denc
e of
ialfo
rmat
ions
was
not
incr
ease
d co
mpa
red
to c
ontr
oi in
offs
prin
g of
rat
s or
rab
bits
giv
en 0
04 to
6 ti
mes
the
J

Ihu
man
dos
e on
a m
g/m
' bas
is. I
n th
ree
repr
oduc
tive
stud
ies
in r
ats
(tw
o S
egm
ent I
I and
a m
ultig
ener
atio
nal
stud
y), t
here
was
an
incr
ease
in p
up d
eath
s du
ring
the
first
4 d
ays
oHac
tatio
n at
dos
es 0
.1 to
3 ti
mes
the
hum
ando
se o
n a
mg/
m' b
asis
. ltis
not
kno
wn
whe
ther
thes
e de
aths
wer
e,
due
to a
dir
ect'e
ffee
ton
the
fetu
ses
or p
ups
or to
effe
ets
on th
e da
ms.
The
rew
as n
o no
-effe
c do
se fo
r in
crea
sed
rat
pup
mor
talit
y. In
'oM
Seg
men
t II s
tudy
,th
ere
was
an
incr
ease
.in s
tiibo
m r
at p
ups
at a
do
se 1
.5 ti
mes
hig
hert
han
the
hum
an d
oseo
na m
g/m
' bas
is.
Pla
cent
al tr
ansf
er o
f ris
perid
one
occu
rs in
rat
pup
s. T
here
are
no
adeq
uate
and
w
ell-c
ontr
olle
d st
udie
s in
preg
nant
wom
en. H
owev
er, t
here
was
one
rep
ort o
f a c
ase
of a
gene
sis
of th
e co
rpus
cal
losu
m in
an
infa
ntex
pose
d to
ris
perid
one
in u
tero
. The
cau
sal r
elat
ions
hip
to R
ISP
ER
DA
L"'th
érap
y IS
'u
nkno
wn.
RiS
PE
RD
AL"
sho
uld
be u
sed
durin
g pr
egna
ncy
oniy
if th
e po
tent
ial'
beiie
fit ju
stifi
es th
e po
tent
ial r
isk
toth
e fe
tus.
Lábo
r an
d D
eliv
ery
The
eff
ect o
f R
ISPE
RD
ÀL
" on
labo
r an
d de
liver
y in
hum
ans
is u
nkno
wn.
Nursing Mothers " '
In a
nim
al s
tudi
es, r
ispe
ridon
e an
d 9-
hydr
oXys
perid
one
wer
e ex
cret
ed in
bre
asfr
iilk.
Ilha
s be
en d
emon
stra
ted
that
ris
perid
one
and
9-hy
drox
yris
perid
one
,are
als
o ex
cret
ed in
, hum
an b
reas
t milk
, The
refo
re, w
omen
rec
eivi
ngRISPERDAL" should not breast feed. '
Pedi
atri
c U
seS
afet
y an
d ef
fect
iven
ess
in c
hild
ren
have
not
bee
n es
tabl
ishe
d.G
eria
tric
Use
Clinical studies ?f RISPERDAL" did not include sufficient nùmbers of patients
aged
65
and
over
tode
term
irie
whe
ther
they
res
pond
dif
fere
ntly
fror
i you
nger
pat
ient
s: O
thêt
rep
orte
d cl
inic
al e
xper
ienc
e ha
sno
t ide
ntifi
ed d
iffer
ence
s in
res
pons
es b
etw
een
elde
riy a
nd y
oung
er p
atie
nts.
In g
ener
al, a
low
er s
tart
ing
dose
is r
ecom
m'e
nded
for
an e
lder
ly p
atie
nt, r
efle
ctin
g a
decr
ease
d ph
arm
acok
inet
iccl
eara
nce
in th
eel
derly
, as
wel
l as
a gr
eate
r fr
eque
ncy
of d
ecre
ased
hep
atic
, ren
al, o
r ca
rdia
c fu
nctio
n; a
nd
,of c
onco
mita
ntdi
seas
e or
oth
er
drug
ther
apy
(See
CliNICAL PHARMACOLOGY
and
DO
SA
GE
AN
D A
DM
INIS
TR
AT
ION
).W
hile
, el
derly
pat
ient
s ex
hibi
t a g
reat
er
tend
ency
to o
rtho
stat
ic h
ypot
ensi
on, i
ts r
isk
in th
e,el
deri
y m
ay, b
em
inim
ized
by
, lim
iting
the
initi
al d
ose
to,O
,5m
g8iD
fOllo
wed
by,c
aref
ul,ti
trat
ion
(See
PR
EC
AU
TIO
NS
).M
onito
ring
of
orth
osta
ticvi
tai s
igns
sho
uld
be c
onsi
dere
d .in
, pat
ient
s. f
or w
hom
this
is ,o
f co
ncer
n.T
his
drug
is k
now
n to
be
subs
tant
ially
exc
rete
d' b
y th
e ki
dney
, and
the
Jisk
of t
oxic
rea
ctio
ns to
this
dru
gmay be gr
eate
r in
pat
ient
s with impaired Jena
l fun
ctio
n. B
ecau
seei
derly
p¡iti
ents
are
mor
e lik
ely
to h
ave
decreased renal func
tion,
car
e sh
ould
,be
take
n in
,d
ose
sele
ctio
n, a
nd it
may
be
usef
ul to
mon
itor
rena
lfu
nctio
n (S
ee D
OS
AG
E A
ND
AD
MIN
IST
RA
TIO
N).
ADVERSE REACTfONS , .
Ass
ocia
ted
with
Dis
cont
inua
tion
of. T
reat
men
tApproximately,9% (244/2607Lof ,RISPERDAL" (risperidone)-treated patients in phase
2-3
stud
ies
disc
ontin
ued
trea
tmen
t due
to a
n ad
vers
e ev
ent,c
ompa
red
with
abo
ut 7
% o
n pl
aceb
o an
d 1.
0% o
n ac
tive
cont
roi d
rugs
. The
mor
e co
mm
on e
vent
s ("
0.3
%)
asso
ciat
ed w
ith d
isco
ntin
uatio
n an
d co
nsid
ered
to b
epo
ssib
iy o
r pr
obab
ly d
rug-
rela
ted
incl
uded
:
~~ RISPERDAL" ~
Ext
rapy
ram
idal
sym
ptom
s 2.
1 %
0%
Dizziness 0.7% 0%
Hyperkinesia 0.6% 0%
Somnolence 0.5% 0%
Nausea 0.3% 0%
Sui
cide
atte
mpt
was
ass
ocia
ted
with
dis
cont
inua
tion
in 1
.2%
of R
ISP
ER
DA
L"-t
reat
ed,p
atie
nts
com
pare
d to
0.6%
of p
lace
bo p
atie
nts,
but
; giv
en th
e al
mos
t 40-
fold
gre
ater
exp
osur
e, ti
me
in R
ISP
ER
DA
L" c
ompa
red
toplacebo patients, it is urilikelythat suicidealtempt is, a RISPERDAL"
rela
ted
adve
rse
even
t (Se
eP
RE
CA
UT
ION
S).
Dis
cont
inua
tion
for
extr
apyr
amid
al s
ympt
oms
was
0%
in p
lace
bo p
atie
nts
but 3
.8%
inactive-control patients in the phase 2-3 trials. .
inci
denc
e in
Con
trol
led
Tria
isC
omm
only
Obs
erve
d A
dver
se E
vent
s in
,Con
trol
led
CII
nica
l Tri
als:
In
two
6,10
8-w
eek
plac
ebo-
cont
rolle
dtr
ials
, spo
ntan
eous
ly-r
epor
ted,
trea
trie
nt-e
mer
gent
adve
rsè
even
ts w
ith
an' i
ncid
ence
of 5
% o
r gr
eate
r in
at
leas
t one
' of
the RISPERDAL" groups a
nd a
t lea
st
twic
e th
at
of p
iace
bo w
ere:
anx
iety
, som
nole
nce,
ext
ra-
pyra
mid
al s
ympt
oms,
diz
zine
ss, c
onst
ipat
ion,
nau
sèa,
dys
peps
ia, r
hini
tis, r
ash,
and
tach
ycar
dia.
Adv
erse
eve
nts
wer
e al
soel
ic~
ed in
one
of t
hese
two
tria
ls (
i.e"
In th
e fi
xed-
doSé
tria
l com
pari
ng R
ISPE
RD
AL
"at
dos
es o
f 2,6
,10,
and
16
mg/
dayw
ith p
lace
bo)
utili
zing
a
chec
klis
tfor
de
tect
ing
adve
rse
even
ts, a
met
hod
that
is m
ore
sens
itie
than
spo
ntan
eous
rep
ortin
g. B
y th
is m
etho
d, th
e fo
llow
ing:
addi
tiona
l com
mon
and
dru
g-re
iate
dad
vers
e ev
ents
wer
e pr
esen
t at a
t lea
st 5
% a
nd tw
ice
the
rate
of p
lace
bo: i
ncre
ased
dre
am a
ctiv
ity, i
ncre
ased
dura
tion
of s
leep
, acc
omm
oda~
on d
istu
rban
ces,
red
uces
aliv
atio
n,m
ictr
ition
dis
turb
ance
s,
diar
rhea
, wei
ght g
ain,
men
orra
gia,
dim
inis
hed
sex4
al d
esire
, ere
ctile
dys
fUnc
tion,
eja
cula
tory
dys
func
tiOn,
and
org
astic
dys
func
tion.
Adv
erse
Eve
nts
Occ
urrin
g at
an
Inci
denc
e of
1%
' or
Mor
e A
mon
g R
ISP
ER
DA
L"-T
reat
ed P
atie
nts:
The
tabl
etha
t fol
low
s en
umer
ates
adv
erse
eve
nts
that
occ
urre
d at
an
inci
denc
e of
1 %
or
mO
re, a
nd w
ere
at le
ast a
sfr
eque
nt a
mon
g R
ISP
ER
DA
L"-t
reat
ed p
atie
rits
trea
ted
at d
oses
ots
10
mg/
day'
than
am
ong
plac
ebo-
trea
ted
patie
nts
in th
e po
oled
res
ults
of t
wo
6 to
,8-w
eek
cont
rolle
d tr
ials
. Pat
ient
srec
eive
d R
ISP
ER
DA
L",d
oses
of 2
, 6,
10, o
r 16
mg/
day
in th
e do
se c
ompa
rison
trai
, or
Up
to a
max
imum
dos
e of
10
mg/
day
in th
e tit
ratio
n st
udy.
Thi
sta
ble
show
s th
e pe
rcen
tage
of
pat
ient
s in
ea
ch d
ose
grou
p (S
1o.
mg/
day
or 1
6 m
g/da
y) w
ho s
pont
aneo
usly
repo
rted
at i
east
Qne
epi
sode
of
an e
vent
at s
ome.
timed
urin
g th
eir
trea
tmen
t. Pa
tient
s gi
ven
dose
s of
2,6
, or
10 m
g di
d .n
ot d
iffer
mat
eria
lly in
thes
e ra
tes.
Rep
orte
d, a
dver
se e
vent
s w
ere
clas
sifie
d us
ing
the
Wor
id, J
jeal
ltQrq
apÎr
;itio
r:Ja
ffic
r.eq
taH
'is_:
wel
l. E
vent
s fo
r w
hich
the
RIS
PE
RD
AL
ø in
cide
nce
(in b
oth
dose
gro
ups)
was
equ
al to
or
less
than
plac
ebo
are
not l
iste
d in
the
tabl
e, b
ut in
clud
ed th
e fo
llow
ing:
ner
vous
ness
, inj
ury,
and
fung
al in
fect
ion.
, Inc
lude
s tr
emor
; dys
toni
a, h
ypok
ines
ia, h
yper
toni
a, h
yper
kine
sia:
ocu
logy
ric c
risis
, ata
xia,
abn
orm
al g
ait,
invo
lunt
ary
mus
cle
cont
ract
ions
, hyp
oref
lexi
a, a
kath
isia
, and
ext
rapy
ram
idal
dis
orde
rs. A
lthou
gh th
ein
cide
nce
of 'e
xtra
pyra
mid
al s
ympt
oms'
doe
s no
t app
ear
to d
iffer
for
the'
S 1
0 m
g/da
y' g
roup
and
pla
cebo
,th
e da
ta fo
r In
divi
dual
dos
e gr
oups
infix
ed d
ose
tria
ls d
o su
gges
t a d
ose/
resp
onse
rel
atio
nshi
p (S
eeD
OS
E D
EP
EN
DE
NC
Y
OF
AD
VE
RS
E E
VE
NT
S).
Dos
e D
epen
denc
y of
Adv
erse
Eve
nts:
Ext
rapy
ram
idal
sym
ptom
s: D
ata
from
two
fixe
d do
se tr
ials
pro
vide
d ev
iden
ce o
f do
se-r
eiat
edne
ss f
orex
trap
yram
idal
sym
ptom
s as
soci
ated
with
ris
perid
one
trea
tmen
t.T
wo
met
hods
wer
ë uS
,ed
tOni
easu
re e
xtra
pyra
mid
al s
ympt
oms
(EP
S)in
an
B,w
eek
tria
l com
parin
g fo
ur fi
xed
dose
s of
ris
perid
one
(2, 6
, 10,
and
16
mg/
day)
, inc
ludi
ng (
1) a
par
kins
onis
m s
core
(m
ean
chan
ge fr
om b
asel
ine)
from
the
Ext
rapy
ram
idal
Sym
ptom
Rat
ing
Sca
le a
nd (
2) in
cide
nce
of s
pont
aneo
us c
ompl
aint
s of
EP
S:
Dos
e G
roup
s'Pl
aceb
oR
is2
Rls
6R
is10
Ris
16
Park
inso
nism
1.2
d.g
1.8
2.4
2.6
EP
S In
cide
nce
"13
%13
%16
%20
%31
%S
imila
r m
ethò
ds w
e(e
used
to m
easu
re e
xtra
pyra
mid
al s
ympt
oms
(EP
S)
in a
n 8,
wee
k tr
ial c
ompa
ring
five
(ixed
dose
s of
ris
perid
one
(1, 4
, 8,1
2, a
nd 1
6.m
g/da
y): '
Ris
4R
is8
Ris
12
Ris
16
1.7
2.4
2.9
4.1
12%
18%
18%
21%
Oth
er A
dver
se E
vent
s: A
dver
se e
vent
dat
a el
icile
d by
a c
heck
list.f
or s
ide
effe
cts
from
a la
rge
stud
y co
mpa
ring
5 fix
ed d
oses
of R
iSP
ER
DA
L" (
r, 4
, 8, 1
2, a
nd 1
6 m
g/da
y) w
ere
expl
ored
for
dose
-rei
ated
ness
of a
dver
se e
vent
s.A
Coc
hran
-Arm
itage
Tes
t for
tren
d in
thes
e da
ta r
evea
led
a po
sitiv
e tr
end
(p~
0.05
) fo
r th
efol
iow
ing
adve
rse
even
ts: s
leep
ines
s; in
crea
sed
dura
tion
of s
leep
, 'ac
com
mod
atio
n di
stur
banc
es, o
rtho
stat
ic d
izzi
ness
, pal
pita
tions
,w
eigh
t gai
n, e
recl
ie d
ysfu
nctio
n, e
jacu
lato
ry d
ysfu
nctio
n, o
rgas
tic d
ysfu
nctio
n, a
sthe
nia/
assi
tude
fincr
ease
dfa
tigua
bilit
y, a
nd in
crea
sed
pigm
enta
tion.
Vita
l. S
ign
Clia
nges
: RIS
PE
RD
AL"
is a
ssoc
iate
d w
ith o
rtho
stat
ic h
ypot
ensi
on a
nd ta
chyc
ardi
a (S
eePRECAUTIONS). " ,
Wei
iiiit
Cha
nges
: The
pro
port
ions
of
RIS
PER
DA
L"
and
plac
ebo-
trea
ted
patie
nts
mee
ting
a w
eigh
t gai
ncr
iterio
n of
" 7%
of b
ody
wei
ght w
ere
com
pare
d in
a,p
ool o
f 6 to
8-w
eek
~Ia
cebo
-con
trol
ledt
riais
, rev
ealin
g a
stat
istic
ally
sig
nific
antly
gre
ater
inci
denc
e of
wei
ght g
ain
for
RIS
PE
RD
AL
(18%
) co
mpa
red
to p
lace
bo (
9%).
Labo
rato
ry C
hang
es: A
bet
wee
n gr
oup
com
paris
on fo
r 6
to 8
-wee
k pl
aceb
o-co
ntro
lled
tria
ls r
evea
led
nost
atis
tical
ly s
igni
fican
t RIS
PE
RD
AL
"/pl
aceb
o di
ffere
nces
in th
e pr
opor
tions
of p
atie
nts
expe
rienc
ing
pote
ntia
llyim
port
ant c
hang
es in
rou
tine
seru
m c
hem
istr
y, h
emat
olog
y, o
r ur
inal
ysis
par
amet
ers.
Sim
ilarly
, the
re w
ere
noRISPERDAL"/placebo differences in the
inci
denc
e of
dis
cont
inua
tions
for
chan
ges
in s
erum
che
mis
try,
hem
atol
ogy,
or
urin
alys
is. H
owev
er, R
ISP
ER
DA
L" a
dmin
istr
atio
n w
as a
ssoc
iate
d w
ith in
crea
ses
in s
erum
prol
actin
(Se
e PR
EC
AU
TIO
NS)
. ,E
CG
Cha
nges
: The
ele
ctro
card
iogr
ams
of a
ppro
xim
atel
y 38
0 pa
tient
s w
ho r
ecei
ved
RIS
PE
RD
AL"
and
120
patie
nts
who
rec
eive
dpla
cebO
.in tw
o do
uble
-blin
d, p
lace
boco
ntro
lled
tria
ls w
ere
eval
uate
d an
d re
veal
ed o
nefin
ding
of p
oten
tial c
once
m; i
.e.,
8 pa
tient
s ta
ngH
ISP
ER
DA
L" w
hose
bas
elin
e O
Tc
inte
rval
was
les
than
450
mse
cw
ere
obse
rved
to h
ave
OT
c in
terv
als
grea
ter
than
450
mse
e du
ring
trea
tmen
t (S
ee W
AR
NIN
GS
). C
hang
es o
fth
is ty
pe w
ere
not s
een
amon
g ab
out 1
20 p
lace
bo p
atie
nts,
but
wer
e se
en in
pat
ient
s re
ceiv
ing
halo
perid
ol (
3/12
6).
Oth
er E
vent
s O
bser
ved
Dur
ing
the
Pre
-Mar
ketin
g E
valu
atio
n of
RIS
PE
RD
AL"
Dur
ing
its p
rem
arke
ting
asse
ssm
ent,'
mul
tiple
dos
es o
f RIS
PE
RD
AL
" (r
ispe
ridon
e) w
ere
adm
inis
tere
d to
2607
pat
ient
s in
pha
se 2
and
3 s
tudi
es. T
he c
ondi
tions
and
dur
atio
n of
exp
osur
e to
RIS
PE
RD
AL"
var
ied.
grea
tly, a
nd in
clud
ed (
in o
verla
ppin
g ca
tego
ries)
ope
n an
d do
uble
-blin
d st
udie
s, u
ncon
trol
led-
arid
con
trol
led
ist
udie
s, in
patie
nt a
nd o
utpa
tient
stu
dies
, fix
ed-d
ose
and
titra
tion
stud
ies,
and
sho
rt-t
erm
or
long
er-t
erm
'ex
posu
re. I
n m
ost
stud
ies,
unt
owar
d ev
ents
ass
ocia
ted
with
this
exp
osur
e w
ere
obta
ined
by
spon
tane
ous:
repo
rt a
nd r
ecor
ded
by c
linic
al in
vest
igat
ors
usin
g te
rmin
olog
y of
thei
r ow
n ch
oosi
ng. C
onse
qu'e
ntly
, it i
s no
t jpo
ssib
ie to
pro
vide
a m
eani
ngfu
l est
imat
e. o
f th
e pr
opor
tion
of ,i
ndiv
idua
lsex
peri
enci
ng a
dver
se e
vent
s ¡
with
out f
irst g
'roup
irig
sim
ilar
type
s of
unt
owar
d ev
ents
into
a s
mal
ler
num
ber
of s
tand
ardi
zed
even
t ica
tego
ries.
In tw
o la
rge
stud
ies,
adv
erse
eve
nts
wer
e al
so e
licite
d ut
ilizi
ng th
e U
KU
(di
rect
que
stio
ning
) si
de ¡
effe
ct r
atin
g sc
ale,
and
thes
e ev
ents
wer
e no
t fur
ther
cat
egor
ized
usi
ng s
tand
ard
term
inol
ogy
(Not
e: T
hese
Ievents are marked with an asterisk in the listings that follow). ;
In th
e lis
tings
that
follo
w, s
pont
aneo
usly
rep
orte
d ad
vers
e ev
ents
wer
e cl
assi
fied
usin
g W
orld
Hea
lth:
Org
aniz
atio
n (W
HO
) pr
efer
red
term
s. T
he fr
eque
ncie
s pr
esen
ted,
ther
efor
e, r
epre
sent
the
prop
ortio
n of
the'
2607
pat
ient
s ex
pose
d to
mul
tiple
dos
es o
f RiS
PE
RD
AL"
who
exp
erie
nced
an
even
t of t
he
type
cite
d on
at
leas
t one
occ
asio
n w
hile
rec
eivi
ng R
ISP
ER
DA
L". A
ll re
port
ed e
vent
s ar
e in
clud
ed e
xcep
t tho
se a
lread
y I
liste
d in
Tab
le 1
, tho
se e
vent
s fo
r w
hich
a d
rug
caus
e w
as r
emot
e, a
nd th
ose
even
t ter
ms
whi
ch w
ere
so !
gene
ral a
s to
be
unin
form
ativ
e. It
is im
port
ant t
o em
phas
ize
that
, alth
ough
the
even
ts r
epor
ted
oCC
Urr
ed ¡
during treatment with RISPERDAL", they were not
necessarily caused by it. :
Eve
nts
are
furt
her
cate
goriz
ed b
y bo
dy s
yste
m a
nd li
sted
in o
rder
of d
ecre
asin
g fr
eque
ncy
acco
rdin
g to
the:
follo
win
g de
finiti
ons:
freq
uent
adv
erse
eve
nts
are
thos
e oc
curr
ing
in a
t lea
st 1
/ 00
patie
nts
(oni
y th
ose
not a
lread
y ¡
liste
d in
the
tabu
late
d re
su~t
s fr
o!"_
e~ac
eb.o
-con
trol
led
tri~
ls a
pe~¡
¡~~n
_~is
!~~.
~9U
~~~:
:\~_;
~t,a
,~~;
;;;~i
;~ls
J

nl:'f
lLrî
"u~
9am
iafiï
í"fr
rëiõ
r.u1
iõtiT
í'';,-
::,'-:
':::::
''':':;
: :.,
,- ,0
'.--
:.:! '
0:'_
':"T
ha p
rasc
ribar
sho
uld
ba a
war
a th
at th
asa
figur
as c
anno
t~aJ
jsad
.to p
radi
ctth
a.in
ci~
anca
of s
ida
affa
cts
Inth
a.co
ursa
of
usua
l mad
ical
pra
ctic
a w
h~ra
pat
lant
char
acta
ri~.
tiCs.
~'ri
d ot
hè; f
acto
rsdi
ffar
Jrom
thos
a w
hich
prav
aila
d in
this
clin
ic~
1 tr
i~I,
Sim
ilariy
, tha
cita
d fm
quan
cies
can
notb
epom
pam
d w
ithfig
uras
obt
aina
d fr
omot
har
clin
icai
inva
stig
atio
ns in
volv
ingd
iffar
arit
trea
tnia
ntsi
usaS
ànd.
inva
stig
atbr
s, T
ha c
itad
figur
as,
how
avar
, 'do
prov
ida
tha
.pra
scrib
ing
phys
icia
n w
ith.s
oma,
basi
s fo
r as
tiri~
ting'
.tha
rala
tlva
cont
ribut
ion
ofdr
ug a
nd n
ondr
ugJa
ctor
sto
tha
sida
~ffa
ct in
cidø
nce
rata
ìn,th
èpdp
ulat
i6n,
sNdi
ad,
Tabla 1: Traaimant-Emargant'Advarsa Exparlance iricidanca
in 6
.to'B
-Wae
k C
ontr
olla
d,C
linic
al T
rial
s'
RIS
PER
DA
L'"
$10 mglday 16 mg(day
(N;324)' (N;77)
Psyc
hiat
ric
Dis
orda
rsIn
som
nia
Agi
tatio
nA
n~ia
tySo
mno
lanc
aA
ggra
ssiv
a ra
actio
nN
arvo
us S
ysta
mE
xtra
pyra
mid
al s
ympt
oms'
Haa
dach
aD
izzi
ness
Gas
troi
rites
tinal
Sys
tam
Con
stip
atio
nN
ausa
aD
yspa
psia
VO
miti
ngA
bdom
inal
pai
nS
aliv
a in
cmas
adT
oot
hach
a ,
Ras
pirä
tory
Sys
tam
Rhi
nitis
'C
ough
ing
Sinu
sitis
Phar
yngi
tisD
yspn
aaBodyasa Whola
Bac
k pa
inC
hast
pai
n,F
avar
Dar
mat
olog
ical
, Ras
hD
ry s
kin
Sabo
rrea
'In
fact
ioiis
Upp
ar r
aspi
rato
ryV
isua
lA
bnor
mal
vis
ion
Mus
culO
'Ska
lata
lA
rthr
algi
aC
ardi
ovas
cula
rTachycardia 3% 5% 0%
t Eva
nts
mpo
rtad
by
at la
ast 1
% o
f pat
iant
s tm
atad
with
RiS
PE
RD
AL'
" $
10 m
glda
y ar
a in
clud
ad, a
nd a
mro
unda
dto
tha
naar
ast %
, Com
para
tiva
rata
sfor
RIS
PE
RD
AL
'",16
mgl
day
and
plac
aboa
m p
rovi
dada
s
Bod
y S
ysta
ml
Pra
fart
ad T
arm
2'è%
22%
12%
3% 1% 17%
14%
4% 7% 6% 5% 5% 4% 2% 2% 10%
3% 2% 2% 1% 2% 2% 2% '2% 2% 1% 3% .2% 2%
'23% 26
%¿ö
% 8% 3%
:34% 12
%7% 13
%'
4% 10%
7% .,1%
0% 0% 8% 3% 1% 3% 0% 0% 3% 3% 5% 4% 0% 3% 1% 3%
Plac
abo
(N;1
42)
'19%
'20
%9% 1% 1% 16
%:
12%
1% 3% 3% 4% 4% 0% 1% 0% 4% 1% 1% 0% 0% 1% 1% 0% 1% 0% 0% 1%.
1% 0%
~~
~th
~~
~ ;;
c~-;
~;¡
;;gi;¡
;7ic
öl~
'iïi O
'óO
¡'-;li
entš
';rar
ë-ëv
arIiS
àra
'thos
e oc
curr
ing
Tnf
awar
ihan
1/1
000
patia
nt,
Psyc
hIat
ric
Dis
orde
rs: F
requ
ent:
incr
easa
d dr
eam
act
ivity
', di
min
isha
d sa
xual
das
ira',
narv
ousn
as'
Infr
aque
nt: i
mpa
ired
conæ
ntra
tlon,
dap
rass
ion,
apa
thy,
cat
aton
ic r
aact
ion,
aup
horia
, inc
raas
ad li
bide
amna
sia"
Rar
a: a
mot
iona
llabi
lity,
nig
htm
aras
, dal
iriu
m, w
ithdr
awal
syn
drom
a, y
awni
ng,
Cen
tral
and
Per
iphe
ral N
ervo
us S
yste
m D
isor
ders
: Fre
quen
t: in
craa
sad
slaa
p du
ratio
n', I
nfre
quen
dysa
rthr
ia, v
arig
o, s
tupo
r, p
araa
stha
sia,
con
fusi
on, R
are:
aph
asia
, cho
linar
gic
synd
rom
a, h
ypoa
stha
sia
tong
ue p
aral
ysis
,lag
cram
ps, t
ortic
olls
,' hy
poto
nia,
com
a, m
igra
ine,
hyp
arre
fiaxi
a, c
hom
oath
atos
is,
Gas
tro-
inte
stin
al D
isor
dars
: Fra
quen
t: an
orax
ia; r
aduc
ad s
aliv
atio
n', I
nfra
quan
t: fla
tula
nca,
dia
rrha
ain
craa
sad
appa
tita;
stom
atiti
s, m
alan
a, d
ysph
agia
, ham
orrh
oids
, gas
triti
s,' R
are:
faca
i 'in
cont
inan
cear
ucta
tion,
gas
troa
soph
agea
l raf
lux,
gas
troa
ntar
itis,
aso
phag
itis,
tong
ua d
isco
lorä
.tion
,cho
lalih
iaS
iS, t
ongu
iad
ama,
div
artic
uliti
s, g
ingi
vitis
" di
scol
omd
faca
s, G
I ham
orrh
aga,
ham
atem
asis
,B
ody
as a
Who
fe/G
ener
af D
isor
ders
: Fre
quen
t: fa
tigua
, Inf
requ
ent:
adam
a, r
igor
s, m
alai
sa, i
nflu
anza
-Iik
isy
mpt
oms,
Rar
e:,p
allo
r, a
nlar
gad
abdo
man
, alle
rgic
rea
ctio
n, a
scita
s, s
arco
idos
is, f
lush
ing,
Ras
pira
tory
Sys
tem
Dis
orde
rs: I
nfre
quan
t: hy
parv
antil
atio
n, b
ronc
hosp
asm
, pna
umon
ia, s
trid
or, R
arE
asth
ma,
incr
easa
d sp
utum
, asp
iratio
n,S
kfn
and
App
enda
ge D
isor
ders
:Fre
quen
t: in
crea
sed
pigm
anta
tion'
; pho
tose
nsili
vity
', In
freq
uent
: inc
reas
eisw
aatin
g, a
cna,
dac
mas
ad s
wea
ting,
alo
peci
a, h
ypar
kara
tosi
s, p
rurit
us, s
kin
axfo
liàtio
n, R
are:
bùl
louc
erup
tion,
ski
n ul
cara
tio'n
, agg
rava
tad
psor
iasi
s, fu
runc
ulos
is, v
erru
cà; d
arm
atiti
s lic
hano
id, h
ypar
tric
hoS
i,ga
nita
l pru
ritu
s, u
rtic
aria
, 'C
ardi
ovas
cula
r D
isor
ders
: Inf
requ
ent:
paip
itatio
n, h
ypar
tans
ion,
hyp
otan
sion
, AV
blo
ck, m
yoca
rdiE
infa
rctio
n,' R
are:
van
tric
ular
tach
ycar
dia,
ang
ina
pact
oris
, pm
mat
ura
atria
l con
trac
tions
, T w
ava
inva
rsio
n,va
ntric
ular
axtr
asys
tola
s, S
T d
apre
ssio
n, m
yoca
rditi
s,V
isio
n D
isor
ders
: Inf
requ
ent:
abno
rmal
acc
omm
odat
ion,
xar
opht
halm
ia, R
are:
dip
lopi
a, e
ya p
ain,
bla
phar
iti¡
phot
opsi
a, p
hoto
phob
ia, a
bnor
mai
lacr
imat
ion.
Met
abol
ic a
nd N
utri
tiona
fDis
orde
rs: I
nfre
quen
t: hy
pona
tram
ia, w
aigh
t inc
reas
e, c
mat
ina
phos
phok
inas
'in
crea
se, t
hirs
t, w
aigh
t dac
reas
e, d
iaba
tas
mal
litus
., R
are:
dac
raas
ad s
arum
iron
, cac
hexi
a, d
ahyd
ratio
rhy
poka
lem
ia, h
ypop
rota
inem
ia, h
yper
phos
phat
amia
, hyp
ertr
igly
carid
amia
, hyp
erur
icem
ia, h
ypog
lyca
mia
,U
rinar
y S
ystm
D
isor
ders
:Fre
iiant
:.pol
yuri
a/po
lydi
psia
', In
freu
ant:
urin
ary
inco
ntin
al1,
hem
atur
ia, d
ysur
iER
are:
uri
narY
rat
antio
n, c
ystti
s, ;a
nal i
nsuf
fcia
ncy,
Mus
cufo
-ske
teta
l Sys
tem
Dis
orde
r: I
nfru
ent:
mya
lgia
, Rar
e: a
rtro
sis,
syo
stos
is, b
ursi
ts, a
rtri
s, s
kale
tal p
air
Rep
rodu
ctiv
e D
isor
ders
, Fem
ale:
Fre
quan
t: m
anor
rhag
ia',
orga
stic
dys
func
tion'
, dry
vag
ina'
, tnf
requ
enno
npua
rpar
alla
ctat
ion,
am
anor
raa,
fam
ala
braa
st p
ain,
leuk
orrh
aa, m
astit
is, d
ysm
anor
rhaa
,. fa
mal
a pa
rina¡
pain
; int
arm
enst
rual
blea
ding
,yag
inal
hat
norr
haga
,L
ive'
rand
Bif
ialy
:Sys
tam
'Dis
orde
rs: i
nfre
quen
t: in
crea
sadS
GO
T, i
ncra
asad
SG
PT, R
are:
hap
atic
fai
lure
chól
asta
tic h
apat
itls,
chó
lacy
stiti
s"ch
olal
ithia
sis,
hap
atiti
s, h
apat
ocal
lula
r da
mag
i"Pl
atet
et, B
1ead
inga
nd C
lottl
ng'D
isor
ders
: Inf
requ
ant,'
api
stax
is, p
urpu
ra, R
are:
ham
orrh
age,
supa
rtic
i,ph
lebi
tis, t
hrom
boph
labi
tis, t
hrom
bocy
topa
nia,
Hea
ring
and
Ves
tibul
arD
isor
dars
:Rar
e:tin
nitu
s, h
ypar
acus
is, d
acea
sed
hear
ing,
Red
B
food
Cel
/Dis
orde
rs: I
nfre
quan
t: an
amia
, hyp
ochr
omic
ane
mia
, Rar
e: n
orm
ocyt
ic a
nem
ia,
Rep
rodu
ctiv
epfs
orde
rs¡
Mal
e: F
requ
ent:
arac
tia d
ySfu
hcjio
n', I
pfre
quan
t: ej
acul
atio
n fa
ilura
,W
hIte
Cel
/ iin
d R
esis
lanc
ii'D
isor
ders
: Rar
e: la
ukoc
osis
, iyp
hada
nopa
lhy,
lauc
opan
ia, p
alge
r-H
uat a
nom
ali
End
ocrin
e D
isor
ders
: Rar
e: g
ynac
omas
tia, m
ale
braa
st p
ain,
ant
idiu
mtic
hor
mon
a di
sord
ar,
Spe
claf
San
ses:
Rar
e: b
iltar
tast
a,. I
ncid
enca
bas
ad o
n el
icila
d,ra
port
s,P
ostln
trod
uctio
n R
epor
ts: A
dver
se'e
vant
s re
port
ad s
inca
mar
kat i
ntro
duct
ion
whi
ch
wer
e ta
mpo
rally
(bi
not n
aces
saril
y ca
usal
ly)
rala
tad
to R
ISP
ER
DA
L"!th
arap
y, in
clud
etha
follo
win
g: a
naph
ylac
tic r
aact
ior
angi
oade
ma.
apn
aa; a
tria
l fib
rilla
tion,
cam
brov
ascu
lar
diso
rdar
, inc
ludi
ng c
embr
ovas
cula
r ac
cida
nt, .
diE
bate
s m
alltu
s ag
grav
ated
, inc
ludi
ng d
iaba
tic k
etoa
cido
sis,
inta
stin
al,o
bstr
uctio
n, ja
undi
ca, m
ania
, pan
CrE
atiti
s, P
arki
nson
's d
lsea
sa a
ggra
vata
d,pu
lmon
ary.
ambo
lism
, Tha
m h
ave
bean
,r
are
rapo
rts
of s
Ud,
dan
deat
and/
or c
ardi
opul
mon
ary
arra
st in
pat
ient
s ra
caiv
ing
.RIS
PE
RD
AL
'", A
.cau
salra
latio
nshi
p w
ith R
ISP
ER
DA
lha
s no
t bae
n as
tabl
isha
d, It
is im
port
ant t
o no
te
that
sud
dan
and
unex
pact
ad d
eath
may
occ
ur in
psy
chot
ipa
tiant
s w
hath
erth
aym
rnai
n un
trêa
tad
or w
heth
ar th
eyar
a tr
aata
d w
ithot
har
antip
sych
otic
dru
gs,
DR
UG
AB
USE
AN
D D
EPE
ND
EN
CE
Con
trol
/ed
Sub
stan
ce C
lass
: RIS
PE
RD
AL
'"(ris
parid
ona)
is n
ot a
con
trol
led
subs
tanc
e,P
hysi
calå
ndP
sýèh
olôg
iè,D
epen
denc
e: R
ISP
ER
DA
L'"
has
not b
een
syst
amat
ical
ly s
tudi
ad in
ani
mai
s(hu
man
s fo
r its
' pot
entia
l for
abù
sa, t
olar
anca
or
phys
icai
dap
anda
nca,
Whi
lath
e cl
inic
al tr
ials
did
nbt
rev
e,
any
tend
ency
for
any
drug
,see
king
beh
avio
r, th
ese
obse
rvat
ions
wer
e no
t sys
tem
atic
and
it is
not
pos
sibl
e to
pred
ict o
n ,th
e ba
sis
of th
is lim
ited
expe
rienc
e th
e ex
tent
to w
hich
a C
NS
-act
ive
drug
wil
be m
isug
ed, d
iver
ted
and/or abused once marketed. Consequently, patients should be evaluated carefully
for
a hi
stor
y of
dru
gabuse"and such patients should be observed closely
for
sign
s of
RIS
PE
RD
AL"
mis
use
or a
buse
(e.
g.,
deve
lopm
ent o
f tol
eran
ce, i
ncre
ases
In d
ose,
dru
g-se
ekin
g be
havi
or).
OV
ER
DO
SAG
EH
uman
Exp
erie
nce:
Pre
mar
ketln
g ex
perie
nce
incl
uded
eig
ht r
epor
ts o
f acu
te R
ISP
ER
DA
L" (
rispe
ridon
e)ov
erdo
sage
with
est
imat
ed d
oses
ran
ging
from
20
to 3
00 m
g an
d no
fata
litie
s. In
gen
eral
, rep
orte
d si
gns
and
sym
ptom
s w
ere
thos
e re
sulti
ng fr
om a
n ex
agge
ratio
n of
the
drug
's k
now
n ph
arm
acol
ogic
al e
ffect
s, i.
e.,
drow
sine
ss a
nd s
edat
ion,
tach
ycar
dia
and
hypo
tens
ion,
and
ext
rapy
ram
idal
sym
ptom
s. O
ne c
ase,
invo
lvin
g an
estim
ated
ove
rdos
e of
240
mg,
was
ass
ocia
ted
with
hyp
onat
rem
ia, h
ypok
alem
ia, p
rolo
nged
OT
, and
wid
ened
OR
S. A
noth
er c
ase,
invo
lvng
an
estim
ated
ove
rdos
e of
36
mg,
was
ass
ocia
ted,
with
a s
eizu
re. p
ostm
arke
ting
expe
rienc
e in
clud
es r
epor
ts o
f acu
te R
ISP
ER
DA
L" o
vera
osag
e, w
ith e
stim
ated
dos
es o
f up
to 3
60 m
g. In
gene
ral,
the
mos
t fre
quen
tly r
epor
ted
sign
s an
d sy
mpt
oms
are
thos
e re
sulti
ng fr
om a
n ex
agge
ratio
nÖf t
hedr
ug's
kno
wn
phar
mac
oiog
ical
effe
cts,
i.e.
, dro
wsi
ness
, sed
atio
n, ta
chyc
ardi
a an
d hy
pten
sion
. Oth
er a
dver
seev
en,ts
, ',r
epor
ted"
si,n
c, e
rna
rket
intr
,od,
UC
,tiO
n w
hich
wer
e, te
mpo
rally
, (bu
t not
nec
essa
rily
caus
ally
) re
iat"
ed, t
oR
ISP
ER
DA
L"ov
erdo
se: i
nclu
de p
roio
nged
OT
inte
rval
,con
vuls
ions
, car
diop
ulm
onar
y ar
rest
, and
rar
e fa
talit
yas
s9ci
ated
with
mul
tiple
dru
g ov
erdo
se,.
Man
agem
ent o
f C
iver
cìi¡
sagè
:Jn
case
, of
acut
e ov
erdo
sage
, est
ablis
h an
d m
aìnt
ain
an a
irÝ
ay a
rid
ensu
read
equa
te o
xyge
natio
n an
d ve
ntila
tion.
Gas
tric
lava
ge (
afte
, r in
tuba
tion,
if p
atie
nt is
unc
onsc
ious
) 'a
ndad
min
istr
atio
n 9f
act
ivat
ed c
harc
oal,
toge
ther
with
a la
xativ
e sh
ould
be
cons
ider
ed. T
he p
ossi
bi(iW
of
obtu
ndat
ion,
sei
zure
s or
dys
toni
c re
actio
n of
the
head
and
nec
k fo
llow
ing
over
dose
may
cre
ate
a ris
k of
aspi
ratio
n w
ith in
duce
d em
esis
. Car
diov
ascU
larm
on~
orin
g sh
ould
com
men
ce im
med
iate
ly a
nd s
houl
d in
clud
eco
ntin
uous
ele
ctro
card
iogr
aphi
c m
onito
ring
to d
etec
t pos
sibl
e ar
rhyt
hmia
s. It
:ant
iarr
hyth
mic
ther
apy
isad
min
iste
red,
dis
opyr
amid
e, p
roca
inam
ide
and
quin
idin
e ca
rry
a th
eore
tical
haz
ard
of O
T-p
rolo
ngin
g ef
fect
sth
at m
ight
be
addi
tive
to th
ose
of r
lspe
rido
ne. S
imila
rly,
it is
rea
sona
ble
to'e
xpec
t tha
t ,th
e al
pha,
bloc
klng
prop
ertie
s of
bre
tyliu
ni m
ight
be
,add
itive
to th
ose,
of r
ispe
ridon
e, r
esul
ting
in p
robl
emat
ic h
ypot
ensi
on.
The
re I
s no
spe
cifc
ant
idot
eto
RiS
PER
DA
L".
The
refo
re a
ppro
pria
te s
uppo
rtiv
e m
easu
res
shou
ld b
e in
stitu
ted.
The
pos
sibi
lity
of m
ultip
le
drug
invo
lvem
ent s
houl
d be
con
side
red.
Hyp
oten
sion
and
circ
ulat
ory
colla
pse
shou
ldbe
trea
ted
w~
h ap
prop
riate
mea
sure
s su
ch
as in
trav
enou
s flu
ids
and/
or,
sym
path
omim
etic
age
nts
(epi
neph
rine
and
dopa
min
e sh
ould
not
be
used
, sin
ce b
eta
stim
ulat
ion
may
wor
sen
hypo
tens
ion
In th
e se
ttng
ofris
perid
one-
Indu
ced
alph
a bl
OC
kade
). In
cas
es
of s
ever
e ex
trap
yram
idal
sym
ptor
ns, a
ntic
holin
ergi
c m
edic
atio
nsh
ould
be
adm
inis
tere
d. C
lose
m
edic
al s
uper
visi
on a
nd m
onito
ring
shou
ld c
ontin
ue u
ntil
the
patie
nt r
ecov
ers,
DO
SA
GE
AN
D A
DM
INIS
TR
AT
ION
Usu
al
Initi
al D
ose:
,RIS
PER
DA
L"
(ris
peri
done
) ca
n be
adm
inis
tere
d on
eith
er a
BID
'or
a O
D s
ched
ule.
In
earl
ysh
ort-
term
clin
ical
tria
lS, R
ISP
ER
DA
L" w
as g
ener
ally
adm
inis
tere
d at
1 m
g B
ID in
itial
ly, w
ith in
crea
ses
inIn
crem
ents
ofl
mgB
ID o
nthe
;sec
ond
and
third
day
, as
tole
rate
d, to
a ta
rget
dos
e of
3 m
g B
ID b
y th
e th
ird
day.
Sub
sequ
ent s
hort
.term
con
trol
led
mal
s ha
ve In
dica
ted
that
tota
l dai
ly r
ispe
ridon
e do
ses
of u
p to
8 m
g on
a O
Dre
g, im
en, a
re a
lso,
s,af
e an
d ef
f"ec
tive.
In
a 10
, ng-
term
con
troi
ie,d
tria
l In
stab
le p
atie
nts;
-RIS
PER
DA
L"
was
adm
inis
tere
d ,O
n,a
OQ
sche
dule
at 1
mg
OD
initi
ally
, w~
h in
crea
ses
to 2
mgO
D o
n th
e se
cnd
day
and
to a
targ
etdo
se
of 4
mg
OD
on
the.
thil'
day
, How
ever
, reg
ardl
ess
of w
hich
reg
imen
is e
mpl
oyed
, in
som
e pa
tient
s a
slow
ertit
rati9
n m
ay b
e m
edic
ally
app
ropr
iate
. Fur
ther
dos
age
adju
stm
ents
, if i
ndic
ated
; sho
uld
gene
rally
occ
Ur
atin
terv
als
of n
ot le
ss th
an 1
wee
k, s
ince
ste
ady
stat
e fo
r th
e ac
tive
met
abol
ite w
ould
not
be
achi
eved
for
approximately liveek in the typical patient.When dosage adjustments are necessary,
smal
l dos
ein
crem
ents
/dec
rem
ents
of 1
-2 m
g ar
e re
com
men
ded.
Effi
cacy
'insc
hizo
phre
nia
was
demonstrated in a dose range of 4 to 16 mg/day in
shor
t-te
rm c
linic
al tr
ials
supp
ortin
g ef
fect
iven
ess,
of
RIS
PE
RD
AL"
, how
ever
, max
imal
.effe
ct w
as g
ener
ally
see
n in
a r
ange
of4
to 8
mglday. Doses above 6 mg/day forBID, dosing were not demonstrated to be
mor
e ef
ficac
ious
than
iow
erdo
ses,
wer
e as
soci
ated
with
mor
e ex
trap
yram
idal
sym
ptom
s an
d ot
her
adve
rse
effe
cts,
and
are
not
gene
rally
rec
omm
ende
d. In
a s
ingl
e st
Udy
sup
port
ing
OD
dos
ing,
the
effic
acy
resu
lts w
ere
gene
rally
str
onge
rfo
r 8
mgt
han
for
4 m
g. T
he.s
afet
y"of
dose
s ab
ove
16 m
glda
y ha
s no
t bee
n ev
alua
ted
in c
linic
al tr
ials
.M
aint
enan
ce T
hera
py:W
hile
:th'e
re is
no
body
of
evid
ence
ava
ilabl
e to
ans
wer
the
ques
tion
of h
ow lo
ng th
esc
hizo
phre
nic
patie
nt,tr
eate
d w
ithH
ISP
ER
DA
L" s
houl
d re
mai
n on
it, t
he e
ffect
iven
ess
of R
ISP
ER
DA
L"2
mg/
day:
to',8
m, g
lday
,atd
e,la
Yin
g re
laps
e w
as d
emon
stra
ted
in a
con
trol
led
tria
l~i ~
atle
nts
who
had
bee
ncl
iniC
all,y
sta
ble
lor
at le
ast
4.w
eeks
,a
nd,
we,
re
then
fO
Il0l
¡pr
a ~e
riqr
d on
i t .t
lear
s. I
n th
is tr
ial,
RIS
PER
DA
L"w
as a
dmin
iste
red
On
a O
D .s
ched
ule,
at 1
m' !
itial
lýÌ'w
~ in
cr, s
's to
2 m
g O
D o
n th
esecond day. and to'a target dose
of4
mg
OD
on
the
thi a
y (S
ee C
linic
al T
rials
, und
er C
LIN
ICA
LP
HA
RM
AC
OLO
GY
). N
ever
thel
ess,
pat
ient
s sh
ould
be
perio
dica
lly r
eass
esse
d to
det
erm
ine
the
need
for
mai
nten
ance
trea
tmen
t with
app
ropr
iate
. do
se.
Ped
iatr
ic U
se:
Saf
ety
and
effe
ctiv
enes
s'in
ped
iatr
ic p
atie
nts
have
not
bee
n es
tabl
ishe
d.D
osag
e in
Spe
cial
Pop
ulat
ions
:The
rec
onim
ende
d in
itial
dos
e is
0.5
mg
BID
in p
atie
nts
who
are
eld
erly
or
debi
liate
d, p
atie
nts
with
seve
r'l.I
enal
or
hepa
tic im
pair
men
t, an
d pa
tient
s ei
ther
pre
disp
osed
to h
ypot
ensi
onor
tor
who
m h
ypot
ensi
on w
ould
pos
e a
risk
. Dos
age
incr
ease
s in
thes
e pa
tient
s sh
ould
be
in in
crem
ents
of
no
mor
e th
an 0
.5 m
g B
ID.
Incr
ease
s to
dos
ages
abo
ve 1
.5 m
g B
ID s
houl
d ge
nera
lly o
ccur
at i
nter
vals
of a
tle
ast 1
wee
k. In
som
e pa
tient
s,
slow
er ti
trat
ion
may
be
med
ical
ly a
ppro
pria
te.
Eid
erly
or
pebi
ltate
d pa
i¡~nt
s" a
nd p
atie
nts
with
ren
al im
pairm
ent,
may
hav
e le
ss a
bilty
to e
limin
ate
RIS
PE
RD
AL"
,tha
n no
rmal
àdu
lts,.
Pat
ient
$ w
ith im
paire
d he
patic
func
tion
may
hav
e in
crea
ses
in th
e fr
eefr
actio
n of
.tber
ispe
ridon
e, p
ossi
bly
resu
lting
in a
n en
hanc
ed e
ffect
(S
ee C
liNIC
AL
PH
AR
MA
CO
LOG
Y).
Pat
ient
s w
ith a
pre
disp
ositi
on 1
0 hy
pote
nsiv
e re
actio
ns o
r fo
r w
hom
suc
h re
actio
ns w
ould
pos
e a
part
icul
arris
k Iik
ewi$
e ne
ed to
be.
tit
rate
d ca
utio
usiy
and
car
eful
ly m
onito
red
(See
PR
EC
AU
TIO
NS
). If
a o
nce-
a-da
ydo
sing
reg
imen
in th
e el
derly
or
debi
litat
ed p
atie
nt is
bei
ng c
onsi
dere
d, it
is r
ecom
men
ded
that
the
patie
nt b
e~
"''-
''''-~
-'';-
'''''ß
.~':~
_.."
"",=
-=,,,
..,,,,
,,,,-
!,,.,,
..r-.
~.'.
.."~
:,'::_
.":-
~ .~
~..~
.t~.~
.,=~
._~
~.!
_~'.!
Io!\"
'':..,
!!õ.':
~_
,l:,!~
~il.
~.h
.~$.
.to.~
. n!'c
;A~
::~d~
v_

.-.,.
...._
_~.._
_.__
=t"
.,,_.
,_.~
,__.
.,_..,
."'''.
....,'
,._...
.''.''
'''''J
..""~
..,-.
.,"";
a""'
'll~;
t~~~
''~d;
ræ:i!
aÆir
i;~~.
i~,:,
',~:"
,-",
,,~,_
,",_
titra
ted
on a
twic
e-a-
day
regi
men
for
2-3
day
s at
the
targ
et d
ose.
Sub
sequ
ent s
witc
hes
to a
onc
e-a-
day
dosi
ng r
egim
en c
an b
e do
ne th
ere'
atté
r.R
eini
tatio
n of
Tre
atm
ent i
n pa
tient
s Pr
evio
usly
Dis
cont
inue
d: A
lthou
gh th
ere
are
no d
ata
to s
peci
fica
llyad
dres
s re
initi
atio
n of
trea
tmen
t, it,
is r
ecom
men
ded
that
whe
n re
star
ting
patie
nts
who
hav
e ha
d an
inte
rval
off R
ISP
ER
DA
L ~
,the
initi
al ti
trat
ion
sche
dule
sho
uld
be fo
llow
ed.
Switc
hing
fro
m o
iiier
Ant
ipsy
chot
ics:
The
re a
re n
o sy
stem
atic
ally
col
lect
ed d
ata
to s
peci
fica
lly a
ddre
sssw
itchi
ng s
Chi
zoph
reni
c pa
tient
s fr
om o
ther
ant
ipsy
chot
ics
to R
ISP
ER
DA
L~, o
r co
ncer
ning
con
com
itant
adm
inis
trat
ion
with
oth
er a
ntip
sych
otic
s, W
hile
imm
edia
te d
isco
ntin
uatio
n of
the
prev
ious
ant
ipsy
chot
ictr
eatm
ent m
ay b
e ac
cept
able
for
som
e sc
hizo
phre
nic
patie
nts,
mor
e 'g
radu
al d
isco
ntin
uatio
n m
ay b
e m
ost
appr
opria
te fo
r ot
hers
. In.
all c
ases
, the
:per
iod
of o
verla
ppin
g an
tipsy
chot
ic a
dmin
istr
atio
n sh
ould
be
min
imiz
ed, W
hen
switc
hing
sch
izop
hren
ic p
atie
nts
from
dep
ot a
ntip
sych
otic
s, if
med
ical
ly a
ppro
pria
te, i
nitia
teR
ISP
ER
DA
L ~
ther
apyi
n pl
ace
of th
e n.
ext s
ched
uled
inje
ctio
n. T
he n
eed
for
cont
inui
ng e
xist
ing
EP
Sm
edic
atio
n sh
ould
be
reev
alua
ted
perio
dica
lly.
HO
W S
UP
PLI
ED
RIS
PE
RD
AL~
.(ris
perid
one)
tabl
ets
are
impr
inte
d "J
AN
SS
EN
", a
nd é
ither
"R
is"
and
the
stre
ngth
"0,
25",
"0.5, or"R" and the
stre
ngth
"1"
, "2"
, "3"
, or
"4",
0.25
mg
dark
yel
low
tabl
et: b
~ttl
es o
f 60
ND
C 5
0458
-301
-04,
bot
tles
of 5
00 N
DC
5045
8,30
1-50
:0.
5mg
red-
brow
n ta
blet
: bot
tès
.of 6
0 N
DC
504
58-3
02-0
6, b
otte
s of
50Ò
ND
C 5
0458
-302
-50.
1 m
g w
hite
tabl
et: b
ottle
s of
60
ND
C 5
0458
-300
-06,
blis
ter
pack
of
1 O
ON
DC
504
58-3
00-0
1, b
ottle
s of
500
ND
C 5
0458
-300
-50,
2 m
g or
ange
tabl
et: b
ottle
s of
60N
DC
504
58-3
20-0
6, b
liste
r pa
ck o
f 100
ND
C 5
0458
-320
-01,
bot
tles
of 5
00N
DC
504
5.8-
320-
50,
3 m
g ye
llow
tabl
et: b
ottle
s of
60
ND
C 5
.045
8-33
0-06
, blis
ter
pack
of
100
ND
C 5
0458
-330
-01,
bot
tles
of 5
00N
DC
504
58-3
30-5
0.4
mg
gree
n ta
blet
: bot
tle.s
of 6
0 N
DC
.504
58-3
50-0
6, b
liste
r pa
ck o
f 100
ND
C 5
0458
-350
-01,
RIS
PE
RD
AL
~ (
rispe
ridon
e) 1
mg/
mL
oral
sol
utio
n (N
DC
504
58-3
05-0
3) is
sup
plie
d in
30
mL
botte
s w
ith a
calib
rate
d (I
n m
illgr
ams
and
mill
iiter
s) p
ipet
te. T
he m
inim
um c
alib
rate
d vo
lum
e is
0.2
5 m
L, w
hile
the
max
imum
calib
rate
d vo
ium
e is
3 m
L.T
ests
indi
cate
that
RIS
PE
RD
AL~
(ris
perid
one)
ora
l sol
utio
n is
com
patib
le in
the
follo
win
g be
vera
ges:
wat
er,
coff
ee,
oran
ge ju
ice,
and
iow
-fat
milk
; it i
s N
OT
com
patib
le w
ith e
ither
col
a or
tea,
how
ever
,S
tora
ge a
nd H
andl
ing
RISPERDAL~tablets should be stor
ed a
t con
trol
led
room
tem
pera
ture
15'
-25'
C (
59'-7
7'F
). P
rote
ct fr
om li
ght
and
moi
stur
e,K
eep
out o
f rea
ch o
f chi
ldre
n.R
ISP
ER
DA
L~'1
mgl
mL
oral
spl
utio
n sh
ould
be
stor
ed a
t con
trol
led
room
tem
pera
ture
15'
-25'
C (
59'-7
7'F
).P
rote
ct fr
om li
ght ?
ndfr
eezi
ng,
Kee
p ou
t ofr
each
of c
hild
ren.
7503
220
US
Patè
nt 4
,804
,663
Feb
ruar
y 20
02\l
Jans
sen
2000
RIS
PE
RD
AL~
tabl
ets
are
man
ufac
ture
d by
:JO
LLC
, Gur
abo,
Pue
rto
Ric
o or
Jans
sen-
Cila
g, S
pA, L
atin
a, It
aly
RIS
PE
RD
AL~
ora
l sol
utio
n is
man
ufac
ture
d.
by:
Jans
sen
Pha
rmac
eutic
a N
,V,
Bee
rse,
Bel
gium
RIS
PE
RD
AL~
tabl
ets
and
oral
sol
utio
n ar
e di
strib
uted
by:
.Ja
nsse
n P
harm
aceu
tica
Pro
duct
s, L
.P.
Titu
svile
, NJ
0856
0i
JAN
SSE
NPH
AR
MA
CE
UT
ICA
PR
OD
UC
TS
. L.P
.

CENTER FOR DRUG EVALUATION ANDRESEARCH
APPLICATION NUMBER:
NDA 20-272/8-008 & 20-588/8-004
MEDICAL REVIEW(S)
CiÇLINICAL REVIEW/.... .
NDA 20-272/S-008Cross reference NDA 20-588/S-004
Clinical Review Cover Sheet
. Appears This WayOn Original

CLINICAL REVIEW,
Table of Contents
Tab I e of Co n tents ............ ... .... ...... ......... ........ .... ... ... ... ........... ... ....... ................. ....... 2
Ex ecutiv e Sum Mary . .... ... .... ... ... .... .... ...... ... ..... ......... ...... .............. ... ................. ....... 3
i. Reco m men dati 0 ns .............. ............................................................... ............ ........ 3
II. Summary of Clinical Findings ............................................................................. 3
C linI cal Revi ew .............................. .......................................................................... 5
i. Introduction and Background ............................................................................. 5
II. Clinically Relevant Findings From Chemistry, Animal Pharmacology and
Toxicology, Microbiology, Biopharmaceutics, Statistics and/or OtherCons ultan t Reviews.......... ................................... .................................... .............. 5
III. Description of Clinical Data and Sources ................................................. 6
v. Clinical Review Methods .ò.................................................................................... 7
VI. Integrated Review of Efficacy .............................................................................. 7
VI. Integrated Review of Safety ...............................................................................12
VIII. Dosing, Regimen, and Administration Issues ............................................18
IX. Conclusions and Recommendations ..................................................................19
XI. A P pen dix ................................................................................................ .............. 20
Page 2

,CLINICAL REVIEWExecutive Summary Section
Clinical Review forNDA 20-272/ 8-008
Executive Summarv
I. RecommendationsI recommend that the Division make an approvable action on supplement 008. I do not, however,agree,with some draft labeling proposals. C ..ì I( I1 , I
c: '". In place of this, I recommend that labeling state the
risperidone was superior to "rJactiveC J".
II. Summary of Clinical Findings
A. Brief Overview of Submission
This submission comprises a complete response to the Division's not-approved letter tosupplement 8 dated January 13, 1998. The sponsor proposes new labeling that describesrisperidone as being effective in the treatment of patients with schizophrenia L ..
C :Ifor up to ()-months.The sponsor submits one effcacy study RIS-USA-79 in support ofa claim of extended efficacy in the treatment of schizophreniai: J for upto (J-months. The sponsor also submits a pooled analysis of nine uncontrolled studies and apooled analysis ofRIS-USA-79 and RIS-INT-6.
B. EffcacyStudy USA-79 supports the claim that Risperdal is effective in maintaining a positive treatmentresponse for the symptoms of schizophrenia. D JC ~C .J It has been customary to allowclaims of extended efficacy based on the results of one positive, well designed, appropriately
red triaL. USA-79 meets this crteria; i:
J
J
Page 3

CLINICAL REVIEW..
Clinical Review Section
All diagnosesNumber (%) relapsed
Mean (SE) time to relapse
Relapse rate at 6 month a
Relapse rate at 1 year a
Relapse rate at end of trial a
SchizophreniaNumber relapsed
Relapse rate at 6 month a
Relapse rate at i year aRelapse rate at end oftrial a
RisperidoneN= 177
45 (25.4%)
452.2 (17.7)
19%
29%
34%
N= 14436 (25.0%)
19%
28%
34%
La: Kaplan-Meier estimates of relapse rate (probability of relapse).b: Stratified log-rank test controlling for investigator and sex.
i:
HaloperidolN= 188
75 (39.9%)
391. (21.8)
30%
45%
60%
N= 15662 (39.7%)
32%
47%
59%
p- value0.001 b
0.007 b
J:J
D. Effcacy ConclusionsStudy USA-79 supports the sponsor's claim that Risperdal is effective in maintaining treatmentresponse for schizophrenia. It has been customary to allow claims of extended efficacy based onthe results of one positive, well designed, appropriately controlled triaL. USA -79 meets thiscriteria; C J\ J~ JIn Study INT-6, a similarly designed study that was previously submitted, Risperdal wascompared to haloperidol and no treatment difference was observed. USA-79 had twice thenumber of patients in each group. This increase in statistical power is a possible explanation forthe difference between USA-79 being a positive study and INT-6 showing no difference.
VII. Integrated Review of Safety
Á. Brief Statement of Conclusions
These pooled long term controlled studies were not designed to establish long-term safety. Sinceboth INT -6 and USA-79 had haloperidol as an active control with no placebo comparator, long-term risperidone safety could only be compared to haloperidoL. Even then the studies were toosmall to detect differences of less than 1 %.
Page 12

CLINICAL REVIEW
Executive Summary Section
C. SafetyThis review focused on the long-term, controlled clinical trials. Risperdal has been on themarket in the US since 1993. The open label trials did not reveal uncommon, unexpected,unreported, serious adverse events that were likely to be drug related. Studies USA-79 and INT-6 were pooled for safety analysis. These studies were not designed to establish long-term safety.Since both INT-6 and USA-79 had haloperidol as an active control with no placebo comparator,long-term risperidone safety could only be compared to haloperidoL. Even then the pooledstudies were too small to detect differences of less than 1 %.
These two pooled studies detected only minimal differences between the two drugs' safetyprofies with the exception of the mean change in prolactin levels and weight gain. The meanprolactin level increased in the RIS group from 25.7 ng/ml at baseline to 40.2 ng/ml at end point,whereas it decreased in the HAL groups from 28.6 ng/ml to 22.6 ng/ml. Roughly twice thenumber of risperidone treated patients (58/241) gained? 7% of their baseline body weight whencompared to haloperidol treated patients (31/261).
,
I
1
D. DosingThe sponsor makes changes in the DOSAGE AND ADMINISTRA nON section of labeling thatreflect the dosing regimen in the long-term controlled trials USA-79 and INT-6. They areaccurate and acceptable from a clinical standpoint.
Appears This WayOn Original
Page 4

CLINICAL REVIEW
Clinical Review Section
Clinical Review
I. Introduction and Background
A. Drug Established and Proposed Trade Name, Drug Class, Sponsor's
Proposed Indication(s), Dose, Regimens, Age GroupsThis submission comprises a complete response to the Division's not-approved letter datedJanuary 13, 1998.
RISPERDAUID (risperidone) is an antipsychotic agent belonging to the benzisoxazolederivatives. Risperdal(í (risperidone) tablets and oral solutions are approved for the managementof the manifestations of psychotic disorders in adults.
The clinical trials in which the effectiveness of risperidone was established primarily studiedadult patients with schizophrenia for up to 8 weeks. The safety and effectiveness of risperidonehas not been established in any pediatric patient population. Risperidone may be given in QD orBID dose schedules. Clinical trials initiated dosing at I-mg PO BID but subsequent trialsestablished 8-mg QD dosing as effective. The safety of doses exceeding 16-mg/day has not beenestablished.
The sponsor proposes new labeling that describes risperidone as being effective in the treatmentof patients with schizophreniaC ) for up to(J-months.
B. State of Armamentarium for Indication(s)
Risperidone is one of four approved drugs that are considered "atypical Antipsychotics". Othermembers of this class include clozapine, olanzapine, and ziprasidone. Atypical antipsychoticagents are so named for their 5HT2 and D2 antagonist effects. "Typical" antipsychotics arebelieved to exert their primary clinical effect through D2 blockade alone though neither of thesetheories of effcacy are established as fact.
C. Important Milestones in Product Development
Risperidone was first registered in the UK in December 1992 and launched in May 1993 for thetreatment of schizophrenia and other psychotic conditions. Risperidone was marketed in 1994 inthe United States and has been used widely since then. It is now licensed world-wide in morethan 90 countries.
II. Clinically Relevant Findings From Chemistry, Animal Pharmacology
and Toxicology, Microbiology, Biopharmaceutics, Statistics and/or OtherConsultant ReviewsThere are no chemistry, animal pharmacology/toxicology, or biopharmaceutical issues in thissubmission.
Page 5

CLINICAL REVIEW
Clinical Review Section
HI. Description of Clinical Data and Sources
A. Overall DataThe sponsor submits one effcacy study RIS-USA-79 in support of a claim of extended efficacyin the treatment of schizophrenia C J' for up to Cl-months. The sponsoralso submits a pooled analysis of nine uncontrolled studies and a pooled analysis ofRIS-USA-79and RIS-INT-6 in support of safety information in draft labeling. Additionally one uncontrolledstudy (RIS-INT-23) of elderly patients is summarized in the ISS.
B T bl L. t th cr. IT. I. a es IS mg e mica ria s
Trials Included in the ISS for NDA 20-2521Supplement 008
Trial Design Number of Subjects Doseffuation(RISIHAL)
USA-79 DB, HAL controlled, PO 192/203 RIS: 2-8 mgldayexcluding Site 8 HAL: 5-20 mg/day
177/188 Up to 2-yearsINT -6 DB, HAL controlled, PO 91/99 RIS and HAL 5-20 mglday; 1 yearUSA-5 Open-label 7 RIS 1-16 mglday; I-yearUSA-6 Open-label 265 RIS 2-16 mglday; 1- year
USA-7 Open-label 105 RIS 2-16 mglday; 34-months
USA-9 Open-label 107 RIS 2-16 mglday; 1 year
INT -4 Open-label 386 RIS 2-16 mglday; 57-weeks
INT -8 Open-label 264 RIS 2-20 mglday; I-yearNED-2 3 studies pooledBEL-17INT-12 Open-label 483 RIS 2-16 mglday; 7-months
INT23 Open-label 180 RIS 0.5-8 mg/day; I-yearElderly
C. Postmarketing ExperienceRisperidone has been extensively used for a number of years. In April 2001, Janssen estimatesthe cumulative exposure at c. .J treatment months, corresponding to more than C. J
t: Jpatient years. There have been nine periodic safety update reports on risperidone. During
the time period from June 1, 1993 to May 31,2000,2065 verified reports became available atJRF from various sources.
D. Literature ReviewThe sponsor provides a literature review that summarizes clinical data on the efficacy and safetyof risperidone long-term use in subjects with schizophrenia r: :: asreported in 116 articles identified in literature searches ~overing the period up to 25 January2001. Safety results ofrisperidone were reported in 79 articles. Most of the articles were casereports. The sponsor discovered three double-blind, reference-controlled and 11 reference-controlled, open studies emerged from this search. There were 32 open, non-controlled studies.The number of subjects comprised in these articles who received risperidone amounted to a totalof 4,053 subjects. There were no unexpected adverse events.
Page 6

CLINICAL REVIEW
Clinical Review Section
V. Clinical Review Methods
A. How the Review was ConductedThis submission contained one effcacy study and a summary of multiple studies to review safetyparameters. Study USA-79 was the focus ofthe efficacy review. It has been customary in theDivision to allow claims of extended efficacy based on positive results in one well designed andadequately controlled study.
B. Overview of Materials Consulted in Review
Supplement 008 was an electronic submission. This submission represents a complete responseto a not approved action on supplement 008. No materials outside ofthe submission wereconsulted in this particular review;
C. Overview of Methods Used to Evaluate Data Quality and IntegrityRaw data was submitted to the Division of BiometrIcs via SAS transport files and analyzedaccording to the methods described in the sponsor's protocol. These results were compared tothe analyses in the submission. The submission was also examined for internal consistency.
D. Were Trials Conducted in Accordance with Accepted Ethical StandardsThe trial was performed in accordance with the declaration of Helsinki and its subsequentrevisions and the FDA Guideline 21 CFR Parts 50, 56, and 312.
E. Evaluation of Financial Disclosure
A financial disclosure and certification statement was included. This certified that JanssenResearch Foundation had not entered into any financial agreement with the clinical investigatorswhereby the value ofthe compensation would be effected by the outcome ofthe study.
VI. Integrated Review of Efficacy
A. Brief Statement of Conclusions
The data support the claim that Risperdal is effective in maintaining a positive treatmentresponse for the symptoms of schizophrenia. c: Ji: :: It has been customary to allow claims of extendedefficacy based on the results of one positive, well designed, appropriately controlled triaL. USA-79 meets this criteria; C :i
C JB. General Approach to Review of the Effcacy of the Drug
This submission contained one efficacy study and multiple studies to review safety parameters.Study USA-79 was the focus ofthe efficacy review. It has been customary to allow claims ofextended efficacy based on positive results in one well designed and adequately controlled study.
Page 7

Clinical Review Section
C. Detailed Review of Trialsc. JStudy RIS-USA-79: A comparison of risperidone and haloperidol for prevention of relapsein subjects with schizophrenia and schizoaffective disorders- is submitted to support theindication of"C :ischizophreniaC 'Jlong-termC r -C-l Investigators and SitesA listing of the investigators and sites may be found in Table C-L in the appendix,
C-2 ObjectivesThe primary objective of the study was to evaluate the efficacy ofrisperidone and haloperidol inthe prevention of relapse during maintenance treatment of stable outpatients with schizophreniaor schizoaffective disorder by treating them with risperidone or haloperidol for a minimum of 1year.
C-3 Study PopulationThis was a trial in outpatient men and women aged 18-65 years with chronic schizophrenia orschizoaffective disorder classified by Diagnostic and Statistical Manual, Fourth Edition (DSM-IV). Patients were clinically stable (as judged by the investigator) for 1 month prior to enrollmentinto the triaL. Stable was defined as receiving the same dosage of antipsychotic medication for 30days and living in the same residence for 30 days. Inclusion and exclusion criteria may be foundin Table C-2. In the appendix
C-4 DesignThis was a one-year double-blind, active (haloperidol), parallel group study of stable medicallytreated outpatients. Double blind treatment began after stratification by sex and randomization.Patients discontinued their current antipsychotic medications gradually over the first 7 days ofdouble blind treatment. The trial used a parallel-group design with 2 treatment arms: risperidoneand haloperidoL. Trial medication was escalated over the first 3 days of double-blind treatment toa dosage of 4 mg/day risperidone or 10 mg/day haloperidoL. For the first month of therapy,assessments were made at I-week intervals to allow adjustment of medication to within the rangeof2 mg to 8 mg/day for risperidone and 5 mg to 20 mg/day for haloperidoL. Thereafter, trialvisits were scheduled every 4 weeks. Additional visits were to be scheduled as needed. Patientswere to be followed until the last patient enrolled into the trial had completed 1 year of double-blind treatment. After the initial I-year double blind treatment period, patients could continue ondouble blind treatment up to 112-weeks.
Relapse did not require discontinuation oftrial medication. Double-blind conditions remained forpatients who relapsed and continued trial medication. A relapsed patient could receive otherwisedisallowed psychotropic medication (e.g. neuroleptics other than risperidone and haloperidol,thymoleptics, or antidepressants) and were to have all routine assessments. A relapsed patientwho had continued on trial medication and relapsed a second time was to be discontinued. Everypatient who received trial medication and withdrew from the trial was to have a final set oftrialassessments. Patients who were withdrawn because of trial medication-related events were to befollowed unti the event resolved or was no longer considered clinically significant.
Page 8

CLINICAL REVIEW
Clinical Review Section
C-5 AssessmentsThe primary efficacy parameter was the time to relapse. Relapse was defined as any 1 of thefollowing occurrences:
. psychiatric hospitalization,
. clinical judgment that an increase in level of care was necessary and increase in P ANSS
score of25% compared with Baseline, or an increase often points if the Baseline score was::40, (The increases in level of care and in P ANSS score had to occur within 2 weeks of eachother in order to qualify a patient's relapse.)
. deliberate self injury, in the investigator's opinion,
. emergence of clinically significant suicidal or homicidal ideation,
. violent behavior resulting in significant injury to another person or significant property
damage, in the investigator's opinion, or. significant clinical deterioration in the investigator's judgment (a CGI-C score of 6, "much
worse").. When the investigator rated the patient's CGI-C at 6, the patient was counted Analysis Plan
Secondary efficacy variables and safety assessments may be found in tables C-5.1 and C-5.2 inthe appendix.
C-6 Patient DispositionThe disposition of patients in study YSA-79 follows in table C-6.
Total number of patients discontinuedReason for discontinuation
Chose to discontinue 35 18.2 36 17,7Relapse 28 14.6 47 23.2Adverse event 24 12.5 30 14.8Lost to follow- up 10 5.2 10 4. 9Poor compliance 6 3. 1 15 7.4Administrative 6 3. 1 2 1. 0Other 3 1. 6 4 2. 0Inadequate response 2 1. 1 7 3, 4.Ineligible 0 0 3 1, 5Intercurrent ilness 0 0 2 1. 0Abnormal clinical laboratory result 0 0 1 0.5Upon visual inspection, one sees a disparity in the percentage of patients discontinuing due torelapse and poor compliance, but other reasons appear roughly equivalent. It is difficult toexplain the disparate numbers of patients who dropped out due to poor compliance since thedropout rate due to adverse events was only slightly higher in the haloperidol group. Poorantipsychotic medical compliance is linked to adverse treatment events. Since the primaryefficacy variable is time to relapse (a category of discontinuation) it appears that patients
Table C-6 Patient Disposition in Study USA-79RIS
N = 192
%59.4
nl14
HALN = 203n %
157 77.3
Page 9

¡CLINICAL REVIEW
Clinical Review Section
discontinuing for other reasons did not skew the results in favor ofRisperdal for inappropriatereasons.
C-7 Baseline Demographics/Severity of IlnessThe distribution of age, race, sex weight and height were similar between treatment groups.
Table C-7.1 Patient Demographics in Study USA-79RIS HAL
N = 192 N = 203n % n 0/0
Sex Female 57 29.7 66 32.5Male 135 70.3 137 67.5
Race White 91 47.4 97 47.8Black 72 37.5 72 35.5
Hispanic 24 12.5 29 l4.3Other 3 1. 5 2 1. 0
Oriental 2 1. 0 3 1. 5Mean SD Mean SD
Age years 40.8 10.72 40.1 10.43. Weight kg 82.0 19.62 83.6 19.87
Height cm 171.3 11.75 171.3 10.1 8
The distribution of diagnostic types were also reasonably similar.
DSM- ivdiagnosisDiagnosistype
Table C-7.2 Distribution of Diagnoses by treatment groups for Study USA79RIS HAL
N = 192 N = 203n %) n 0/0155 80.7 l69 83.337 19.3 34 l6.794 49.0 1 l4 56.255 28.6 45 22.219 9.9 21 LO.318 9.4 13 6.45 2, 6 7 3. 41 O. 5 3 1. 5
SchizophreniaSchizoaffective disorderParanoidUndifferentiatedDepressiveBipolarResidualDisorganized
C-8 Concomitant Medications.Anti-Parkinson drugs were taken by 48% ofrisperidone patients versus 60% haloperidolpatients. This difference was mainly in patients using cogentin (risperidone group 38% versushaloperidol group 49%) while other anti-Parkinson drugs were used equally between the twogroups (e.g. akineton, artane, benztropine, kemadrin).
C-9 Effcacy Results
Two analyses were performed. During the audit ofRIS-USA-79, it was determined that the datafrom 1 site did not meet the Jansen Pharmaceutia quality standard. Therefore, the analyses wereperformed with and without Site #8. Time to relapse was the primary efficacy variable.
Page 10

CLINICAL REVIEWClinical Review Section
Percentage of patients experiencing relapse (by criteria definition and treatment group) are listedin table C-9.1.
Criteria for relapse
Entire TrialPsychiatric hospitalization
Significant clinical deterioration (a CGI- C score of6)Increase in level of care was nec.essar and increase inPANSS score of25% compared with Baseline, or anincrease of 10 points if the Baseline score was 40
Emergence of clinically significant suicidal orhomicidal ideationTOTALS
Table C-9.i Percentage of Patients Experiencing Relapse in Study USA-79RIS HALN=l77 N=188n % n 0/020 44. 4 36 48. 016 35.6 22 29.38 17.8 l4 18.7
2.2 3 4.0
45 75
Figure 1 displays the Kaplan-Meier survival probability plot o.ftime to relapse in USA-79.
Figure 1: Kaplan-Meier survival probabilty plot of time to relapse
1.0
0.9
0.8
~ 0.7
:ëct 0.6.nEa. 0.5
~ 0.4.~:: 0.3(J
0.2
0.1
~~,~~...-""~.;~"
-!-':~~-Jt'-~~+"r- _ - - ~ -:Zi~,~~ _ _ _ _ -I.. å-'( ~fr-~~-h-£~M~e. ~ -// -M -&O:--£-l..
~~i~ :~~-I
iB;.,ie.~ i,~~- -.s --,(Æ¡ -E ,1._ ?_ ~~ _)_::._ ....~ E'
0.0
1 1 1 2 2 2 3 3 3 3 4 4 4 5 5 5 6 6 6 6 7 7 72 5 8 1 4 7 0 3 6 9 2 5 8 1 4 7 0 3 6 B 2 5 80 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Time (in days)
RIS~USA-79
., -:.-.~ HALOPERIDOL "'- ~ -~ RISPERIDONE-- -o 3 6
o 0
Patients in the risperidone treatment group had a longer mean time to relapse (452.2 days) thanthe patients in the haloperidol treatment group (391.3 days). Among the patients with diagnosisof schizophrenia, there was a statistically significant difference between the two treatments, infavor ofrisperidone, in the survival curves (p = 0.007). In the risperidone group, the Kaplan-Meier estimates of relapse rates, i.e. the probability of relapse, were 19%,29%, and 34%, at 6months, 1 year and at the end ofthe trial, respectively.
Table C-9.2 Time to Relapse in Study USA-79 by Diagnosis
Page 11

CLINICAL REVIEW'
Clinical Review Section
These two pooled studies detected only minimal differences between the two drugs safetyprofies with the exception of the mean change in prolactin levels and weight gain. The meanprolactin level increased in the RIS group from 25.7 ng/ml at baseline to 40.2 ng/ml at end point,whereas it decreased in the HAL groups from 28.6 ng/ml to 22.6 ng/ml. Roughly twice thenumber ofrisperidone treated patients (58/241) gained ;;7% oftheir baseline body weight whencompared to haloperidol treated patients (31/261).
I
L
B. . Description of Patient Exposure
This review of safety focuses on the long-term controlled trials-USA-79 and INT-6. Thefollowing table reflects drug exposure in the long-term controlled studies.
Table VII-B.t Estimated Risperidone Exposure in Lon~-term Controlled TrialsDuration oftreatment (days) RIS .:4 mg RIS4-6mg RIS ::6 mg Total RISTotal no. of subjects 29 156 98 2831- 90 days, n (%) 1 i (37.9) 46 (29.5) 27 (27.6) 84 (29.7)91- 180 days, n (%) 5 (17. 2) 14 (9. 0) 10(10.2) 29 (10.2)181- 270 days, n (%) 2 (6.9) 10 (6. 4) 6 (6. I) 18 (6. 4)271- 360 days, n (%) 1 (3.4) 10 (6. 4) 8 (8.2) 19 (6. 7)::360 days, n (%) 10 (34.5) 76 (48.7) 47 (48.0) 133 (47.0)Mean duration of treatment (days) 269 (50.7) 328 (20.5) 290 (21.2) 309 (14.5)
Total duration of exposure (patient- years) 21 140 78 239
C. Methods and Specific Findings of Safety ReviewThis review focuses on the long-term, controlled clinical trials. Risperdal has been on the marketin the US since 1994. Open label experience is valuable as a screen for very rare, unreported,serious adverse events. Further open label experience did not reveal this type of newinformation.
D. Adequacy of Safety Testing
These studies were not designed to establish long-term safety. Since both INT-6 and USA-79had haloperidol as an active control with no placebo comparator, longer-term exposure torisperidone could only be compared to haloperidoL. The studies were too small to detectdifferences in events that occur at a rate of less than 1 %.
Page 13

.
CLINICAL REVIEW
Clinical Review Section
There is a vast clinical experience with risperidone. The numbers of patients exposed in long-term controlled studies allowed for a reasonable estimate for an incidence rate for tardivedyskinesia of 1 % or greater. , r- :JL J
E. Summary of Critical Safety Findings and Limitations of Data
E-l Deaths in controlled trialsThere were two deaths in the risperidone treated patients and no deaths in the haloperidol treatedpatients. Neither risperidone treated patients' death was likely to be related to drug treatment.One patient completed suicide and the other died of multiple pulmonary emboli secondary todeep venous thrombosis of the both legs. Case summaries of these patients may be found in theappendix.
E-2 Serious Adverse EventsThere were no serious adverse events that were unexpected and considered likely to be drugrelated. The numbers and distribution of types of serious adverse events was roughly equalbetween the two treatment groups. Most of the serious adverse events were psychiatric in natureand likely to be related to the disease of schizophrenia as opposed to drug treatment. A table ofthe types of serious adverse events that occurred at least twice in one, or both treatment groups islisted in table E-2.1 in the appendix.
E-3 Discontinuations Due to Adverse EventsThe total number of discontinuations due to adverse events were greater in the haloperidoltreated patients versus risperidone treated patients. If one considers only adverse events that arelikely to be drug related as opposed to those that are likely to be incident to the disease, then thetwo treatment groups are less different. Nineteen versus 11 patients dropped out due to adverseevents that could be considered likely to be drug related. Hyperkinesia (potentially akathisia)occurred in 10 (3.3%) haloperidol treated patients versus 4 (1.4%) risperidone treated patients.The drop out rate for "extrapyramidal disorder" was slightly higher in the risperidone treatedpatients (5 (1.8%) risperidone versus 3(1.0% haloperidol)).
There are discrepancies between some tables of discontinuation data in the submission. There arediscrepancies in the total number of discontinuations due to adverse events between thesponsor's Table 4-3 and Table 4-9. The sponsor states that Table 4-3 is based on the trialtermination form and Table 4-9 is based on the adverse event form with action taken "permanentstop" regarding trial medication. In trial RIS-USA-79, a substantial number of subjects had"relapse" as reason for trial termination but also had an adverse event for which the treatmentwas permanently stopped. On the trial termination form, however, only "relapse" (which wasconverted into "insufficient response") was recorded. There are therefore more discontinuationsdue to adverse events than in the trial termination table. This coding difference does not appearto effect the rates at which patients dropped out due to adverse events.
Page 14

CLINICAL REVIEW
Clinical Review Section
Sponsor's Table 4-3 Reasons for trial discontinuation -controlled long-term trialsReason for discontinuation, n (%) RIS ..4 mg RIS 4 - 6 mg RIS ~ 6 mg Total RIS HALTotal number of subjects 29 156 98 283 302Completed 6 (20, 7) 71 (45.5) 45 (45.9) 122 (43.1) 83 (27.5)Discontinued 23 (79.3) 85 (54,5) 53 (54.1) 161 (56.9) 219 (72.5)Discontinuation reason:_ Insuffcient response 3 (10.3) 23 (14.7) 22 (22.4) 48(17.0) 83 (27.5)
Adverse event 8 (27, 6) 17(10.9) 11 (11.2) 36 (12.7) 47 (15.6)
- Withdrawal of consent 10 (34.5) 21 (13.5) 4 (4.1) 35 (12.4) 36 (11.9)_ Non compliance 0 7 (4.5) 11 (11.2) 18 (6. 4) 27 (8. 9)_ Lost to follow- up 0 13 (8. 3) 0 13 (4.6) 17 (5, 6)
- Other 2 (6.9) 4 (2.6) 5 (5.1) 11 (3.9) 6 (2.0)_ Ineligibility 0 0 0 0 3 ( 1. 0)
The types and numbers of adverse events leading to discontinuation are listed in the followingsponsor's table 4-9. To be listed in the table at least two patients in one of the treatment groupshad to discontinue for that reason.
Appears This Way. On Original
Page 15

CLINICAL REVIEWClinical Review Section
Sponsor's Table 4-9 Adverse events that led to treatment discontinuation in 0.5% of the totalRIS and HAL subjects - controlled long-term trials
WHO systeml organ class RIS .:4 mg RIS 4 - 6 RIS ;:6 mg Total RIS HALmg
WHO preferred tennTotal no. of subjects 29 156 98 283 302Total no. of discontinuations 9 (31. 0) 29 (18.6) 18 (18.4) 56 (19.8) 83 (27,5)due to AE , n (%) a)Psychiatric disorders 3 (10. 3) 21 (13.5) 14 (14.3) 38 (13.4) 56 (18.5)Psychosis 0 11 (7. 1) 3 (3.1) 14 (4. 9) 32 (10.6)Depression 1 (3.4) 4 (2.6) 4 (4.1) 9 (3.2) 4 (1.)Suicjde attempt 0 2 (1.) 4 (4.1) 6 (2.1) 2 (0.7)Hallucination 0 0 3 (3.1) 3 (1.) 1 (0.3)Agitation 0 0 0 0 4 (1. 3)Delusion 0 0 0 0 3 (1. 0)Somnolence 0 0 0 0 3 (1. 0)Anxiety 0 2 (1.) 0 2 (0.7) 3 (1.0)Schizophrenic reaction 0 1 (0.6) 1 (1.0) 2 (0.7) 2 (0.7)Nervousness 0 1 (0.6) 0 1 (0.4) 2 (0.7)Aggressive reaction 0 0 0 0 2 (0. 7)Central & peripheral 2 (6.9) 6 (3.8) 3 (3.1) 11 (3. 9) 19 (6. 3)nervous system disordersExtrapyramidal disorder 1 (3.4) 3 (1.9) 1 (1.0) 5 (1.8) 3 (1.0)Hyperkinesia 1 (3.4) 3 (1.9) 0 4 (1.4) 10 (3. 3)Dystonia 0 2 (1.) 0 2 (0.7) 1 (0.3)Tremor 0 0 2 (2.0) 2 (0.7) 2 (0.7)Oculogyric crisis 1 (3.4) 0 0 1 (0.4) 2 (0.7)Speech disorder 0 1 (0.6) 0 1 (0.4) 2 (0.7)Hypokinesia 0 0 0 0 2 (0. 7)Gastro- intestinal system 3 (10. 3) 0 0 3 (1.) 4 (1.3)disordersNausea 2 (6.9) 0 0 2 (0.7) 1 (0.3)Vomiting 2 (6.9) 0 0 2 (0.7) 1 (0.3)Body as a whole - general 0 1 (0.6) 0 1 (0.4) 9 (3.0)disordersAsthenia 0 0 0 0 2 (0. 7)Fatigue 0 0 0 0 2 (0. 7)Myo endo pericardial & 0 0 0 0 2 (0. 7)valve disordersMyocardial infarction 0 0 0 0 2 (0. 7)
Drop outs in the long-term studies reflected roughly the dropout rate from risperidone short termtrials in current labeling.
E-4 Adverse EventsCommon and drug related adverse events associated with long term use could not be elucidatedsince this was an active controlled triaL. In the ISS the sponsor suggests that the incidence rate ofcommon adverse events decreases with time. Whether this is actually representative of
Page 16

..
CLINICAL REVIEW.
Clinical Review Section
individual patients feeling fewer or decreased intensity of adverse events or a reflection ofpatients dropping out who poorly tolerate the drug is difficult to telL. r- JC JE-5 LaboratoryCentral TendencyThe sponsor reported that mean laboratory values did not change over time with the exception ofprolactin The mean prolactin level increased in the RIS group from 25.7 ng/ml at baseline to 40.2ng/ml at end point, whereas it decreased in the HAL groups from 28.6 ng/ml to 22.6 ng/mL.Visual inspection ofthe mean change tables confirmed this assertion.
Outlier AnalysisUpon visual inspection there were not differences in the incidence of outliers betweenhaloperidol and risperidoi1e patients with potentially clinically significantly high or low clinicallaboratory values. Table E-5.1 in the appendix displays this data.
E-6 ECGThere were no relevant changes in ECG parameters. QTc mean values using four correctionmethods were unremarkable. The incidence of patients with QTc values increases wascomparable between treatment groups as seen in table E-6.1 where Bazett's (B) and Fridericia(F) corrections are displayed.
Table E-6.1 Distribution of corrected QTc increases at end point relative to baseline - controlled long-term trials
Corrected QTc RIS RIS RIS Total RIS HALincreases ..4mg 4 - 6 mg _ 6mgQTcB n/ N assessed (%)
0- 30 ms 22/ 26 (84.6) 112/128 (87.5) 75/88 (85.2) 209/242 (86.4) 231/ 263 (87.8)31- 60 ms 3/ 26 (11.) 13/128 (10.2) 10/88 (11.4) 26/242 (10.7) 25/263 (9.5)~60 ms 1/26 (3.8) 3/128 (2.3) 3/88 (3. 4) 7/ 242 (2.9) 7/263 (2.7)
QTcF0- 30 ms 24/26 (92.3) 114/128 (89.1) 76/88 (86.4) 214/242 (88.4) 241/ 263 (91.6)31- 60 ms 2/26 (7.7) 12/ 128 (9.4) 10/88 (11.4) 24/242 (9.9) 19/263 (7.2)~60 ms 0/26 (0) 2/ 128 (1.6) 2/88 (2. 3) 4/242 (1.7) 3/263 (1.)
E-7 Weight and Vital SignsThere were more risperidone patients who gained ~7% of their baseline body weight thanhaloperidol treated patients. There was, however, no dose dependency for risperidone withrespect to weight gain.
% change frombaseline at end point
Table E-7.1 Incidence of Body Weight Increase ;:7% at end point- controlled long-term trials
RIS RIS":4mg 4-6mg
Increase ~ 7% 11/25 31/ i 28
RIS;: 6mg
ni N assessed16/ 88
Total RIS HAL
58/241 31/ 26 i
Page 17

CLINICAL REVIEW
Clinical Review Section
Mean weight change was significantly different from haloperidoL.Table E-7.2 Mean Weight Change in Controlled Clinical Trials
RIS HALn mean SE n mean SE p- value
Weight BL 166 82.48 182 84.20 0.590(kg) Year 1 99 2.49* 0.60 7l -0.20 0.89 0,016
Endpoint l66 2.36* 0.60 l82 -0.56 0,52 ~O.OOL
E-10 Special SearchesTardive Dyskinesia
The Extrapyramidal Symptom Rating Scale (ESRS) was used to determine the presence andseverity of tardive dyskinesia in Study USA-79. Emergence or worsening of dyskineticsymptoms were assessed using the following criteria: an increase from Baseline of~:3 points in 1item, or an increase of2 points in 2 or more items in the dyskinetic movement subscale on 2 ormore consecutive days. Patients were considered to have emergent or worsening dyskineticsymptoms ifthey met the criteria at any time during. the triaL. The existence of Baselinedyskinetic movement was also assessed with the following criteria: ~ 3 points in 1 item, or 2points in 2 items ofthe dyskinetic subscale for ESRS.
Eleven patients (3 RIS and 8 HAL) developed emergent or worsened tardive dyskinesia (TD)over the trial course. Ofthe patients with no symptoms at Baseline, 171 (98.3%) risperidonepatients and 177 (96.2%) haloperidol patients remained symptom-free throughout the triaL. Three
(1.7%) risperidone treatment group patients and 7 (3.8%) haloperidol treatment group patientsdeveloped emergent, persistent TD during the triaL. Of the 37 patients (18 RIS, 19 HAL), whohad dyskinetic symptoms at Baseline, 0 of the risperidone treatment group and 1 (5.3%) of thehaloperidol treatment group patients developed worsening symptoms by Endpoint.c ~c :i USA-79 produces an incidence of 1.7%(per year) ifone uses the mean duration of exposure (351 days) as the denominator.
The ISS reports that there were only 2 risperidone patients who developed tardive dyskinesia inthe controlled trial database. This number is manifestly smaller than the number reported for thesingle USA-79 triaL. C :iC -~VIII. Dosing, Regimen, and Administration IssuesThe sponsor makes changes in the DOSAGE AND ADMINISTRATION section oflabeling thatreflect the dosing regimen in the long-term controlled trials USA-79 and INT-6. They areaccurate and acceptable from a clinical standpoint.
Page 18

CLINICAL REVIEW
Clinical Review Section
IX. Conclusions and Recommendations
A. ConclusionsStudy USA-79 supports the sponsor's claim that Risperdal is effective in maintaining treatmentresponse for schizophrenia. It has been customary to allow claims of extended efficacy based onthe results of one positive, well designed, appropriately controlled triaL. USA-79 meets thiscriteria CC
:i
r'i.C
:i.J
:J
In Study INT -6, a similarly designed study that was previously sui,mitted, Risperdal wascompared to haloperidol and no treatment difference was observed. USA-79 had twice thenumber of patients in each group. This increase in statistical power might explain the differencebetween USA -79 being a positive study and INT -6 showing no difference.
These studies were not designed to establish long-term safety. Since both INT-6 and USA-79had haloperidol as an active control with no placebo comparator, long-term risperidone safetycould only be compared to haloperidoL. Even then the studies were too small to detect adverseevents that occurred at a rate of less than 1 %.
These two pooled studies detected only minimal differences between the two drugs safetyprofies' with the exception ofthe mean change in prolactin levels and weight gain. The meanprolactin level increased in the RIS group from 25.7 ng/ml at baseline to 40.2 ng/ml at end point,whereas it decreased in the HAL groups from 28.6 ng/ml to 22.6 ng/ml. Roughly twice thenumber ofrisperidone treated patients (58/241) gained ?7% of their l:mseline body weight whencompared to haloperidol treated patients (31/261).L ~r: J USA-79 produces an incidence of 1.7%(per year) if one uses the mean duration of exposure (351 days) as the denominator. The ISSreports that there were only 2 risperidone patients who developed tardive dyskinesia in thecontrolled trial database. This number is manifestly smaller than the number reported for thesingle USA-79 triaL. i: JC -J
B. RecommendationsI recommend that the Division make an approvable action on supplement 008. t: J
, Page 19

CLINICAL REVIEW
Clinical Review Section
c.the risperidone was superior to "rJactiveC- J".
.J i recommend that labeling state
Paul J. Andreason, MDClinical Reviewer, HFD-120
XI. AppendixTable C-l Listing of Investigators Sites for
USA-79Investigator Site
Site #02Ronald Brenner, M. D.St. John's EpiscopalHospital327 Beach 19th StreetFar Rockaway, NY i 1691
Site# 03David Brown, M. D.
441 1 Medical Parkway DriveAustin, TX 78756
Site #04Wayne K. Goodman, MD/Matthew Byerly, M, D,Department of PsychiatryUniversity of FloridaPSB 11- 4301600 SW Archer RoadGainesvile, FL 32610- 0256
Site #06James Chou, M. D.
Room 20N 1 1Department of PsychiatryBellevue Hospital Center550 First A venueNew York, NY 10016
Site #07Bar Cole, M. D./ Michael De
Priest, MDSouthern Nevada AdultMental Health Services6161 W. Charleston Blvd.Las Vegas, NY 89102
No. of Patients
Entered =33Randomized 30
Entered 15
Randomized= 15
Entered= 10
Randomized= 8
Entered= 24Randomized= 19
Entered= l7Randomized- l4
Page 20

CLINICAL REVIEWClinical Review Section
Table C-L Listing of Investigators Sites forUSA-79
Investigator Site
Site #08Cal Cohn, M. D.The Cohn Center,Psychiatr7777 SW FreewaySuite 1036Houston, TX 77074
Site #09John Csernansky, M, D.Washington University4940 Children's PlaceBox 8134
St. Louis, MO 63110
Site # 10John Davis, M, D.1601 West Taylor StreetChicago, IL 60612
Site # 11
Lawrence A. Dunn, M. D.Durham VA MedicalHospital508 Fulton
Durham, NC 27705
Site # 12Alan Green, M, D.David A. Klegon, MDCommonwealth ResearchCenterHarard Medical Center
74 Fenwood RoadBoston, MA 02 i 15
Site # 13
Alex Kopelowicz, M. D. (PI)15535 San FernandoMission Blvd.Mission Hils, CA 91345
No. of Patients
Entered= 35
Randomized= 30
Entered= 17
Randomized= 13
Entered= 0
Randomized= 0
Entered= 4
Randomized= 4
Entered= 9
Randomized= 9
Entered= 27
Randomized= 27
Page 21

CLINICAL REVIEW
Clinical Review Section
Table C-L Listing of Investigators Sites forUSA-79
Investigator Site
Site # 15Mark Hamer, M. D.VAMC - 116ADepartment of Psychiatr109 Bee StreetCharleston, SC 29401
Site # 16
Harold Harsch, M. D.General Hospital,Psychiatr - 175
8700 W. Wisconsin AveMilwaukee, WI 53226
Site # 17Federico Adan, M, DDominion Tower (D- 79)1400 NW 10 th AvenueSuite 307AMiami, FL 33136
Site #18George G. Jaskiw, M. D.Chief, Schizophrenia SectionPsychiatr Services 116- A (B)
Cleveland V AMC10,000 Brecksvile RoadBrecksvile, OH 44141
Site # 19Banole Johnon, M. D.The Mental Sciences Institute1300 MoursundHouston, TX 77030
Site # 20Ari Kiev, M. D.Social Psychiatry ResearchInstitute75 Booth AvenueEnglewood, NJ 07063
Site # 21
No. of PatientsEntered= 9
Randomized= 7
Entered= 8
Randomized= 7
Entered= 9
Randomized= 7
Entered= 8
Randomized= 6
Entered= 32Randomized= 30
Entered= 13
Randomized= 9
Entered= 1 8
Page 22

...CLINICAL REVIEW
Clinical Review Section
Table C-L Listing of Investigators Sites forUSA-79
Investigator Site
Mar Ann Knesevich, M. D.St. Paul Medical CenterSouthwestern Medical Center
5959 Har Hines Suite 924Dallas, TX 75235
Site # 22Douglas Levinson, M, D.Medical College of
Pennsylvania & HahnemannUniv. Hospital3200 Henr AvenueRoom 206APhiladelphia, P A 19129
Site 23H. E. Logue, M. D.Birmingham PsychiatryPharaceutical Studies, Inc.3490 Independence Drive
Birmingham, AL 35209
Site #24Robert M. Hamer Ph. D (PI)Matthew Menza, M. D.( CO- PI)RWJ Medical School675 Hoes LanePiscataway, NJ 08854
Site #26Raj Naka, M. D.16216 Baxter RoadChesterfield, MO 63017
Site # 28Charles Nemeroff, M. D.Emory University School ofMedicinel639 Pierce DriveSuite 4000Atlanta GA 30322
Site # 29
No. of PatientsRandomized= 10
Entered= 8
Randomized= 6
Entered= 32Randomized= 27
Entered= 5
Randomized= 5
Entered= 24Randomized= 21
Entered= 1
Randomized= 0
Entered= 2
Page 23

.,,:C,,_,_' -"" ",._'._'CLINICAL REVIEWiJ
Clinical Review Section
Table C-L Listing of Investigators Sites forUSA-79
Investigator Site
Vemon Neppe, M. D.NorthWest Outpatient Med, Ctr.l0330 Meridian Ave.Seattle, WA 98133Budgetl Contract:6808 44th Avenue, NESeattle, W A 98 i 15
Site # 30Sheldon Preskom, M. D,1 LOO N. St. Francis .
Suite 200Wichita, KS 672 1 4- 2878
Site #31Michael Plopper, M. D.Mesa Vista Hospital7850 Vista Hil AvenueSan Diego, CA 92 1 23
Site # 33George Simpson, M, D.Professor of PsychiatryUSC School of Medicine1937 Hospital Place
Grad HallLos Angeles, CA 90033
Site # 34Stephen Strakowski, M. D.Department of PsychiatryUniversity of CincinnatiML 559231 Bethesda AvenueCincinnati, OH 45267- 0559
Site # 35Marshall Thomas, M. D.University of Colorado4455 E. 12th AvenueDenver, CO 80220
Site # 36
No. of PatientsRandomized= 0
Entered= 16
RandoIDized= 13
Entered= 32Randomized= 27
Entered= 2
Randomized= 1
Entered= 7
Randomized= 5
Entered= 3
Randomized= 2
Entered= 16
Page 24

CLINICAL REVIEW
Clinical Review Section
Table C-L Listing of Investigators Sites forUSA-79
Investigator Site
Jose Yaryra- Tobias, M. D.
Institute for Bio- BehavioralTherapy and Research935 Northern Blvd.
Great Neck, NY 1 1021
Site # 39Scott A. West, M. D.Psychiatric Institute ofFlorida, P A77 W. Underwood Street3rd FloorOrlando, FL 32806
Site # 40Iring S. Kolin, M. D.
1065 Morse Blvd.Suite 202Winter Park, FL 32789
Site # 42Marin J. Miler, M. D. .Larue Carter Hospital2601 Cold Springs RoadIndianapolis, IN 46222
Site # 43George Pahl, M. D.13301 North Meridian
Suite 101
Oklahoma City, OK 73120
Site # 44Tai P. Yoo, MDMercy Hospital BehavioralMedicine Services5555 ConnerDetroit, MI 48213
No. of PatientsRandomized= 14
Entered= 1 1
Randomized= 9
Entered= 4
Randomized= 4
Entered= 1
Randomized= 1
Entered= 1 1
Randomiz;ed= 16
Entered= 5
Randomized= 5
Table C-2 Inclusion and Exclusion Criteria for Study USA-79INCLUSION CRITERIPatients who met the following criteria were eligible for this trial:
patient or legal guardian signed an approved informed consent
Page 25

CLINICAL REVIEW/Clinical Review Section
- male or female between 18 and 65 years of age- met DSM-IV criteria of schizophrenia or schizoaffective disorder- had a documented I-year history of schizophrenia or schizoaffective disorder since the firstpharmacological treatment for psychotic symptoms- within the past 24 months was discharged from an inpatient psychiatric unit, had a partialhospitalization, completed crisis management intervention, or stayed in a psychiatric hospitalemergency room holding area for at least 12 hours- received a stable dosage of antipsychotic medication for the 30 days prior to entering the trial(Stable was calculated by dividing the minimum dosage by the maximum dosage and defined asa ratio ~ 0.75,)- domiciled at the same address for at least 30 days preceding trial entry- was able to discontinue current antipsychotic medication, in the opinion ofthe investigator- was clinically stable, in the opinion ofthe investigator- had negative urine drug screens for cocaine, opiates, barbiturates, amphetamines,phencyclidine, lysergic diethylamide acid, and methadone- females had a negative pregnancy test
agreed to refrain from using ilicit drugs and abusing alcohol
EXCLUSION CRITERIPatients who met 1 or more ofthe following criteria were not eligible for this trial:- females who were pregnant or nursing- had another current DSM-IV Axis-I diagnosis (except caffeine or nicotine dependence) orAxis-II diagnosis of borderline personality disorder or antisocial personality disorder (A historyof substance dependence or substance abuse must be in remission for at least 3 months at thetime of Screening.)
- had clinically significant neurological disorder or other condition with neurologicalmanifestations, with the exception ofDSM-IV defined medication-induced movement disorders- had history or the presence of gastrointestinal, liver, or kidney diseases, or other conditions ofsufficient severity to interfere with the absorption, distribution, metabolism, or excretion of trialmedication- had clinically significant medical disease which would prohibit treatment with risperidone orhaloperidol- had unstable medical ilness, ie, unstable angina, labile hypertension, poorly controlled diabetes- received concomitant medication, other than OTC medications or antibiotics, for fewer than 14days at the time of Screening (Doses of concomitant medications should be stable for 14 days,that is, minor variations of up to 25% are permitted.)
had carcinoma during the previous 5 years (History of treated basal cell skin carcinoma isallowed.)was HIV -positive
- received current treatment with the antipsychotic clozapine or known 0 be refractory toantipsychotics- was acutely psychotic and showed no response or minimal response to risperidone at dosages:;8 mg/day or haloperidol at a dosage of:;20 g/day when given for 4 weeks minimum- was currently being treated with :;10 mg/day risperidone or :;25 mg/day haloperidol
Page 26

CLINICAL REVIEW
Clinical Review Section
- required treatment with antidepressants, lithium, carbamazepine, or valproic acid within the 30days preceding trial entry- had history of neuroleptic malignant syndrome- had known hypersensitivity to risperidone or haloperidol- had history of seizures requiring medication- received depot neur~leptic injections within 1 treatment cycle of Screening- received an investigational medication within 30 days before Screening- had history of attempted suicide in the previous 6 months or current suicidal ideation
was currently at risk for violent behavior against otherswas considered by the investigator as potentially noncompliant
Table C-5.1 Secondary Effcacy Variables in Study USA-79. relapse rates, I-year and Endpoint
. total and subscales ofPANSS,
. I-year relapse rate,
. clinical improvement measured by a 20% decline in total P ANSS score,
. CGI and CGI-C,
· QOLI,. Drug Attitude Inventory,
. cognitive function tests (Wechsler Memory Scale, California VerbalLearning Test,
Continuous Performance Task, Verbal Fluency, Digit Symbol, and Wisconsin Card Sort),and
. Health Care Resource Utilization
Table C-5.2 Safety Assessments in Study USA-79. adverse events
. clinical laboratory tests: blood chemistry profie: sodium, potassium, chloride, bicarbonate,
glucose, urea nitrogen, creatinine, calcium, phosphorus, uric acid, total bilirubin, alkalinephosphatase, serum glutamic oxalacetic transaminase, serum glutamic pyruvic transaminase,gamma glutamyl transpeptidase, lactic dehydrogenase, total serum protein, albumin, andprolactin complete blood count with differential and platelet count urinalysis by dip stick; ifabnormal, a microscopic examination urine drug screen serum pregnancy test (females ofchildbearing potential)
. ECG
. vital signs: pulse, respiration, temperature, blood pressure
. physical examination
. ESRS
Summaries of Deaths in Lone:-term Controlled Trials that were not Considered Drue:RelatedSubject 0152, a 41-year old Caucasian male in RIS-USA-79, was taking RIS 4 mg and wasadmitted to hospital on Day 97 ofthe trial for dyspnea and chest pain. The physician felt that thesymptoms were due to chest inflammation. One day later the subject was seen again by thephysician for the same symptoms and he recovered the same day. Eight days later the subject
Page 27

. .. .. ......CLINICAL REVIEW'.
Clinical Review Section
complained of difficulty breathing and pain in his left arm. He became pale, diaphoretic andcollapsed. He was pronounced dead when the emergency squad arrived. Autopsy revealed thecause of death as bilateral deep vein thrombosis with multiple pulmonary emboli. Theinvestigator considered this event unrelated to the trial medication.
Subject 435, a 39-year old Caucasian female who was taking RIS 12.5 mg in trial RIS-INT-6.Twenty-five days after the start of treatment, she committed suicide. There was no relation to thetrial medication according to the investigator. Listing AEA gives details about the events leadingto death.
Table E-2.1 Serious adverse events in:: 0.5% of the total RIS and HAL subjects-controlled long-term trials
WHO organ system class RIS RIS RIS Total RIS HALWHO preferred term ~4mg 4 - 6 mg ~ 6mgTotal no. of subjects 29 156 98 283 302No. of subjects with SAE, 4 (13.8) 38 (24. 4) 18(18.4) 60 (21. 2) 69 (22. 8)n(%)Psychiatric disorders 3 (10.3) 24 (15. 4) 13 (13. 3) 40 (14. 1) 52 (17. 2)Psychosis 0 1 8 (1 1. 5) 9 (9. 2) 27 (9.5) 38 (12. 6)Suicide attempt 0 3 (1. 9) 4(4.1) 7 (2. 5) 4 (1. 3)Depression 1 (3. 4) 2 (1. 3) 2 (2. 0) 5 (1. 8) 0Hallucination 1 (3,4) 0 2 (2. 0) 3 (1. 1) 1 (0. 3)Agitation 0 1 (0. 6) 1 (1. 0) 2 (0. 7) 5 (1. 7)Drug abuse 1 (3. 4) 1 (0. 6) 0 2 (0, 7) 1 (0. 3)Paranoid reaction 0 1 (0. 6) i (1. 0) 2 (0. 7) 0Schizophrenic reaction 0 1 (0. 6) 1 (1. 0) 2 (0. 7) 3 (1. 0)Aggressive reaction 0 0 0 0 2 (0. 7)Anxiety 0 0 0 0 3 (1. 0)Delusion 0 0 0 0 3 (1. 0)Body as a whole - general 0 6 (3. 8) 3 (3. 1) 9 (3. 2) 15 (5. 0)disordersInjury 0 2 (1. 3) 2 (2. 0) 4 (1. 4) 4 (1. 3)Chest pain 0 2 (1. 3) 1 (1. 0) 3 (1. l) 1 (0. 3)Syncope 0 1 (0. 6) 0 1 (0.4) 2 (0. 7)Therapeutic response 0 1 (0. 6) 0 1 (0. 4) 3 (1. 0)increasedCondition aggravated 0 0 0 0 2 (0. 7)Metabolic and nutritional 1 (3. 4) 2 (1. 3) 1 (1. 0) 4 (1. 4) 5 (1. 7)disordersDehydration 1 (3. 4) 0 1 (1. 0) 2 (0, 7) 0Diabetes melltus 0 2 (1. 3) 0 2 (0. 7) 1 (0. 3)Hyponatraemia 0 0 0 0 2 (0. 7)Central & peripheral 0 2 (1. 3) 1 (1. 0) 3 (1. 1) 4 (1. 3)nervous system disordersConvulsions 0 0 0 0 2 (0. 7)Myo endo pericardial & 0 0 0 0 2 (0. 7)valve disordersMyocardial infarction 0 0 0 0 2 (0. 7)
Page 28

......CLINICAL REVIEW).....
Clinical Review Section
Table E-5.1 Laboratory value changes beyond the predefined limits in :;2% ofthe total RIS and HAL subjectswith normal baseline values - controlled long-term trials
RIS RIS RIS Total RIS HALVariable -C4mg 4 - 6 mg :;6mgHematology ni N assessed (%)Hematocrit_ Abnormally low 0/22 (0) 31 1 l5 (2.6) 0/38 (0) 3/l75(1.7) 1/ 188 (0.5)_ Abnormally high 0/22 (0) 1/ 115 (0.9) 0/38 (0) 1/l75 (0.6) 4/188 (2.1)WBC_ Abnormally high 012 (0) 01 25 (0) .3/55 (5. 5) 3/82 (3. 7) 1/85 (1. 2)Blood chemistry ni N assessed (%)Chloride_ Abnormally low 01 25 (0) 21 iis (1.7) 2/38 (5. 3) 41 178 (2.2) 3/187 (1.6)_ Abnormally high 01 25 (0) 1/ 115 (0.9) 0/38 (0) 1/ 178 (0.6) 2/187 (1.)
GGT_ Abnormally high 1/26 (3. 8) 41 137 (2.9) 2/91 (2.2) 7/254 (2.8) 7/263 (2.7)Glucose_ Abnormally low 0/27 (0) II 141 (0,7) 01 92 (0) 1/260 (0.4) 01 272 (0)
_ Abnormally high 0/27 (0) 9/141 (6.4) 0192 (0) 9/260 (3,5) 81 272 (2.9)
SGPT (ALT)_ Abnormally high 1/26 (3. 8) 41 140 (2.9) 0192 (0) 5/258 (1.9) 61 270 (2.2)
Total protein_ Abnormally low 01 26 (0) 01 137 (0) 01 89 (0) 0/252 (0) 0/270 (0)_ Abnormally high 01 26 (0) 1/137 (0,7) 01 89 (0) 1/252 (0.4) 61 270 (2.2)
Appears This WayOn Original
Page 29

This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.
/s/Paul Andreason11/5/01 03: 16: 17 PMMEDICAL OFFICER
Thomas Laughren12/15/01 11: 55: 03 AMMEDICAL OFFICERI agree that this supplement is approvable i see memoto file for more detailed comments. - -TPL

MEMORANDUM DEPARTMENT OF HEALTH AND HUMAN SERVICESPUBLIC HEALTH SERVICE
FOOD AND DRUG ADMINISTRATIONCENTER FOR DRUG EVALUATION AND RESEARCH
DATE: December 15,2001
FROM: Thomas P. Laughren, M.D.Team Leader, Psychiatric Drug ProductsDivision of Neuropharmacological Drug ProductsHFD-120
SUBJECT: Recommendation for approvable action forRisperdal tablets and solution (risperidone) for the longer-term treatment of schizophrenia
TO: File NDA 20-272/S-008 & NDA 20-588/S-004
(Note: This overview should be fied with the 7-25-01
original submission.)
1.0 BACKGROUN
Risperdal is currently approved and marketed for the treatment of schizophrenia, in an immediate releasetablet (NA 20-272) and in an oral solution (NA 20-588). These supplements provide data in supportof a new claim for these same formulations in the longer-term treatment of schizophrenia, in a dose rage
of ( :i mg/day.
These supplements were originally submitted 3-12-97, and a nonapproval letter was issued 1-13-98. The3-12-97 submission included effcacy date from 4 trals, only 1 of which was a controlled tral (! -6), and
that study, a 1 year comparson of risperidone and haloperidol, demonstrated no difference between these2 active drugs in relapse, and thus, was considered uninterpretable. We also considered longer-term safetydata submitted in 3-12-97 to be uninterpretable. However, we did invite the sponsor to submit labelinglanguage to note the apparent lack of a 2D6 inhibitory effect for risperidone, as demonstrated in datasubmitted with these original supplements. We also, in the 1-13-98 letter, asked the sponsor to addlanguage in labeling to describe the results of a cross-fostering stdy that showed a direct toxic effect onthe fetus, and supported, in our view, the continuation of a Category C for pregnancy. Both of thesechanges were finally approved in a 7-19-01 letter.
1

Since the proposal is to use the currently approved Risperdal formulations for this expanded indication,there was no need for chemistr, pharacology, or biopharmaceutic reviews ofthis supplement. The focuswas on clinical data. The primary review ofthe efficacy and safety data was done by Paul Andreason,M.D., from the clinical group. Yeh-Fong Chen, Ph.D., from the Division of Biometrcs, also reviewed theefficacy data.
The study supporting this supplement was conducted under IN 31,931. The original supplements for thisexpanded indication (S-008 & S-004) were submitted 7-25-01.
We decided not to take these supplements to the Psychopharmacological Drugs Advisory Committee
(PDAC).
2.0 CHEMISTRY
As Risperdal tablets and solution are already marketed, there were no CMC issues requiring review forthis supplement.
3.0 PHARMCOLOGY
As Risperdal tablets and solution are already marketed, there were no phartox issues requiring reviewfor this supplement.
4.0 BIOPHARACEUTICS
As Risperdal tablets and solution are already marketed, there were no biopharmaceutics issues requiringreview for this supplement.
5.0 CLINICAL DATA
5.1 Effcacy Data
5.1.1 Overview of Study 79
Results from study 79 were submitted in support ofthis claim for the longer-term efficacy ofRisperdal inschizophrenia. This 35 center, US, outpatient, parallel group study enrolled patients with eitherschizophrenia or schizoaffective disorder (DSM-IV) who were judged to be stable by the investigator forat least 1 month prior to radomiztion. "Stable" was defied as receiving the same dosage of antipsychotic
2

medication and living in the same residence for 30 days. Patients meeting these criteria were radomized
(n=395) to either risperidone 4 mg/day (n= 192) or haloperidol 10 mg/day (n=203) for a minimum periodof i year, during which time they were observed for relapse. Medication was titrated up to these initialtarget doses over the first 3 days. During the first month of the trial, adjustments in medication could bemade weekly, within a range of2 to 8 mg/day for risperidone and 5 to 20 mg/day for haloperidoL.Thereafter, patients were seen monthly, some for periods of up to 2 years. The study ended when the lastrandomized patient reached the 1 year point.Relapse was defined as any 1 ofthe following:-psychiatric hospitalization-clinical judgement that an increase in level of care was necessary and an increase in P ANSS total scoreof25% compared to baseline, or an increase of i 0 if the baseline score was .: 40 (both had to occur withina 2 week period)-deliberate self injury-emergence of clinically significant suicidal or homicidal ideation-violent behavior resulting in significant injury to another person or significant property damage-CGI-C score of 6 or 7
The primary outcome was time to relapse. Secondary outcomes included relapse rate, and P ANSS totaland subscales, among others.
The primary analysis was the log-rank test for time to relapse,
Patients in study 79 were roughly 2/3 male, roughly Yz Caucasian and 1/3 Afrcan American, and the meanage was roughly 41 years. Roughly 82% of patients were schizophrenic.
Forty-one % ofrisperidone patients completed to 1 year, compared to 23% of haloperidol patients.Patients in the risperidone group had a longer mean time to relapse (452 days) than patients in thehaloperidol group (391 days), p=O.OO 1. Risperidone also was superior to haloperidol on this measure in
the subgroup with schizophrenia (p0.007), i: Jc. J However, the effect sizes were similar to those for the schizophrenic patientsL JC. .J The crude relapse risks at 1 year were23% for risperidone and 35% for haloperidol (p.009). The cumulative relapse rates at 1 year were 29%for risperidone and 45% for haloperidoL.
Dr. Chen did an analysis considering all censored patients as treatment failures, and this analysis alsofavored Risperdal over placebo (p=0.008).
Dr. Chen conducted subgroup analyses based on gender and race. This analysis showed a superiority ofrisperidone over haloperidol only for the male subgroup, however, the effect sizes were similar for bothsubgroups. Analyses based on race showed a superiority risperidone over haloperidol for both Caucasianand African American subgroups.
3

Comment: Both Drs. Andreason and Chen considered this a positive study supporting a claim oflonger-term effcacy for Risperdal in the treatment of schizophrenia, and I agree. I also agree with Dr. Andreaonthat labeling should J c: :ic: .. mention thatsuperiority was established over an active comparator in this triaL.5.1.2 Conclusions Regarding Effcacy Data
Study 79 demonstrated a benefit of risperidone over haloperidol for the maintenance of stability, or delayof relapse, in patients with schizophrenia who were stble at trial entr and were then observed for relapseduring a 1 to 2 year followup period.
5.2 Safety Data
Dr. Andreason's safety review of this supplement was based on 283 patients who received Risperdal ina pool of2 controlled long-term studies (Study 79 and INT -6). Dosing was according to the currentlyrecommended dose range for RisperdaL. There were no unexpected safety findings among these patients,and no basis for changes in the labeling for Risperdal from the standpoint of safety, C. :i
5.3 Clinical Sections of Labeling
We have modified the language in the 4 sections oflabeling in which the sponsor has proposed changes,i.e., Clinical Trials, Indications, Adverse Reactions, and Dosage and Administrtion. We have also addedlanguage changig the focus of the claim for this drg from "management of the manifesttions of psychosis"to "schizophrenia," as part of a class action for the antipsychotic drugs.
6.0 WORLD LITERATURE
4

Dr. Andreason reviewed the sponsor's report on a total of 116 published papers pertining to the longer-term use ofRisperdal in schizophrenia. He concluded that there were no unexpected adverse events
reported that would impact on Risperdal labeling.
7.0 FOREIGN REGULATORY ACTIONS
To my knowledge, Risperdal is not approved for the longer-term treatment of schizophrenia anywhere atthis time.
8.0 PSYCHOPHARMCOLOGICAL DRUGS ADVISORY COMMITTEE (pDAC)MEETING
As noted, we did not take this supplement to the Psychopharmacological Drugs Advisory Committee
(PDAC).
9.0 DSI INSPECTIONS
DSI did not, to my knowledge, inspect investigative sites for this supplement.
10.0 LABELING AN APPROV ABLE LETTER
10.1 Labeling Attached to Approvable Package
Our proposed labeling for this new claim is included in the approvable letter.
10.2 Foreign Labeling
To my knowledge, Risperdal is not approved for the longer-term treatment of shizophrenia anywhere atthis time.
10.3 Approvable Letter
The approvable letter includes our proposed labeling for this supplement.
11.0 CONCLUSIONS AN RECOMMENDATIONS
5

I believe that Janssen has submitted suffcient data to support the conclusion that Risperdal is effective andacceptably safe in the longer-term treatment of schizophrenia, I recommend that we issue the attched
approvable letter with our proposed labeling language for this expanded claim.
Appears This WayOn Original
cc:Orig NDAs 20-272/S-008 & NDA 20-588/S-004HFD-120HFD-120/TLaughren/Ratz/P Andreason/SHardeman
DOC: MMSCZLT.AEI
6

Appears This WayOn Original
7
---------------------------------------------------------------------------------------------------------------------This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.---------------------------------------------------------------------------------------------------------------------/s/
Thomas Laughren12/15/01 12: 11 :47 PMMEDICAL OFFICER

MEMORANDUM DEPARTMENT OF HEALTH AND HUMAN SERVICESPUBLIC HEALTH SERVICE
FOOD AND DRUG ADMINISTRATIONCENTER FOR DRUG EVALUATION AN RESEARCH
DATE: February 14,2001
FROM: Thomas P. Laughren, M.D.Team Leader, Psychiatric Drug ProductsDivision of Neuropharmacological Drug ProductsHFD-120
SUBJECT: Recommendation for approval action forRisperdal tablets and solution (risperidone) for the longer-term treatment of schizophrenia
TO: Pile NDA 20-272/S-008 & NDA 20-588/S-004
(Note: This overview should be fied with the 1-28-02 response to our 1-11-02
approvable letter.)
We issued an approvable letter for these supplements on 1-11-02, with proposed modifications to labeling.There were no issues other than labeling that needed resolution prior to tag a final approval action. The
sponsor has in fact accepted our proposed changes verbatim. They have also made changes throughoutlabeling to shift the focus ofthe claim from "psychosis" to "schizophrenia." as we had requested in a 9-25-00 letter.
There are only two issues that require further comment:
r-
-In the cover letter to their i -28-02 response, the sponsor has raised a question about a statementregardingi: :: we had included within a bracketed comment to them in our proposed
labeling. They express a concern about this sttement but they do not, in my view, ariculate any questionthat needs a response at this time. r. .:
1

CJ however, I thin they need to give us a more definitive question before we can provide a meaningfulresponse, Therefore, I recommend that we not respond to this vague inquiry at this time.
In summar, we have reached agreement with the sponsor on final labeling and I recommend that weapprove these supplements, with the agreed upon final labeling.
~lhlsWay0I Otigit
cc:Orig NDAs 20-272/S-008 & NDA 20-588/S-004HFD.:120HFD-120/TLaughren/Ratz/P Andreason/SHardeman
DOC: MEMSCZL T.API
2

This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.
/s/Thomas Laughren2/14/02 02: 07: 53 PMMEDICAL OFFICER

CENTER FOR DRUG EV ALUA TION ANDRESEARCH
APPLICATION NUMBER:
NDA 20-272/8-008 & 20-588/8-004
STATISTICAL REVIEW(S)

"
DEPARTMENT OF HEALTH AND HUMAN SERVICESPUBLIC HEALTH SERVICEFOOD AND DRUG ADMINISTRTIONCENTER FOR DRUG EV ALUA TION AND RESEARCH
STATISTICAL REVIEW AND EVALUATION
Medical Division: Division of Neuropharmacological Drug Products (HFD-120)Biometrics Division: Division of Biometrics I (HFD-710)
NDA NUMBER/SERIL NUMBER: 20-272/S-008 & 20-588/S-004
DATE RECEIVED BY CENTER: 7/25/01
DRUG NAME: RISPERDALiI (risperidone)
INICATION: Schizophrenia C- .:SPONSOR: Janssen Research Foundation
STATISTICAL REVIEWER: Yeh-Fong Chen, Ph.D.
STATISTICAL TEAM LEADER: Kun Jin, Ph.D.
BIOMETRICS DIVISION DIRCTOR: George Chi, Ph.D.
CLINICAL REVIEWER: Paul Andreason, M.D.
PROJECT MANAGER: Steve Hardeman, M.D.

I. TABLE OF CONTENTS
1. Introduction and Background-------------------------------------------------------------------------------------- 22. Summary ofthe Sponsor's Results and Conclusions for Study RlS-USA-79 --------------------------------- 2
3. Description of the Sponsor's Studies and Statistical Methodologies-----------------~---------------------------- 3
3.1 Study RlS-USA -79----------------------------------------------------------------------------------------------------- 33.1.1 Trial Objectives--------------------------------------------------------------------------------------------------- 33.1.2 Trial Design------------------------------------------------------------------------------------------------------ 33 . 1 .3 E ffi cacy------------------------------------------------------------------------------------------------------------ 33.1.4 Statistical Methods and Analyses Planned----------------------------------------------------------------- 4
3.2 Study Rl S-!NT -6------------------------------------------------------------------------------------------------------- 63 .2. 1 Effi cacy Assessments---------------------------------------------------------------------------------------"----- 6
3 .2.2 Statisti cal Analyses----------------------------------------------------------------------------------------------- 7
4. Detailed Review of the Sponsor's Individual Study ResuIts-------------------------------------------------- 7
4. 1 Study Rl S- USA - 7 9----------------------------------------------------------------------------------------------------- 7
4.1,1 Subject Disposition----------------------------------------------------------------------------------------------- 74.1.2 Premature Discontinuations------------------------------------------------------------------------------------- 84.1.3 Demographics and Baseline Characteristics---------------------------------------------------------------- 84.1.4 Primar Efficacy Parameter-------------------------------------------------------------------------------- 94.1.5 Secondary Efficacy Parameters--------------------------------------------------------------------------- 11
4.1.6 Sponsor's Effcacy Conclusion---------------------------------------------------------------------------- 154.2 Study Rl S- INT -6-------------------------------------------------------------------------------------------------------- 16
4.2. 1 S ubj ect Dispositi on---------------------------------------------------------------------------------------------- 1 6
4.2.2 Premature Discontinuations------------------------------------------------------------------------------------- 164.2.3 Demographics and Baseline Characteristics---------------------------------------------------------------- 164.2.4 Primary Eff cacy Param eter------------------------------------------------------------------------------------ 164.2.5 Secondary Effcacy Parameters--------------------------------------------------------------------------- 164.2.6 Sponsor's E ffi cacy Concl usi on-------------------------------------~---------------------------------------- 1 8
5. Statistical Reviewer's Findings and Comments----------------------------------------------------------------------- 18
II. EXECUTIVE SUMMARY OF STATISTICAL REVIEWER'SFINDINGS
. This reviewer did not have any inconsistent findings on the values of the sponsor's statisticalanalysis results.
. C. J the sponsor had statistically significant test results shown on the primary and some
secondary effcacy endpoints for the whole study population on Study RIS-USA-79C. JC ~C ~. Except for two diagnosis groups, the sponsor did not perform any other subgroup analysis.
According to this reviewer's subgroup analysis results, the risperidone was shownsignificantly more effective than haloperidol for male patients but not for female patients. Forboth white and black patient groups, there existed statistically significant differences betweenthe risperidone and haloperidol treatments.
. After reversing the values for censoring variables in the early discontinued study patients, the
robustness ofthe test result for the primary endpoint was confirmed.

III. STATISTICAL REVIEW AND EVALUATION OF EVIDENCE
1. Introduction and Background
In response to the FDA's not approvable letter dated January 13, 1998, the sponsor submittedthis amendment to the supplement S-008 to provide for the long-term treatment of patients withschizophrenia C .:
According to the sponsor's submission, efficacy data supporting this amendment were derivedfrom clinical studies RIS-USA-79 and RIS-INT-6. The long-term efficacy ofrisperidone indelaying onset to relapse of schizophrenia c. :i was established by an indepth review of data from RIS-USA-79 in which an established agent, haloperidol was used as areference neuroleptic agent. Data from the earlier study, RIS-INT-6, comparing long-termtreatment with risperidone and haloperidol in the treatment of subjects with chronic schizopreniawere used to support the findings ofRIS-USA-79. Since Study RIS-INT-6 was reviewed before,this review wil be only focusing on the statistical evaluation for Study RIS-USA-79 but wilreport the sponsor's study outlnes and statistical results for both studies.
2. Summary of the Sponsor's Results and Conclusions for Study RIS-USA-79
The primary efficacy endpoint for Study RIS-USA-79 was time to relapse in stable outpatientswith chronic schizophrenia or schizoaffective disorder who received risperidone or haloperidolas maintenance treatment for at least I year. The secondary efficacy endpoints included relapserates at I-year and at endpoint, total and sub scales ofPANSS, CGI severity, CGI-relative tochange from the baseline assessment, cognitive function, quality of life, drug attitude inventoryand health care resource utilization. Table 1 shows a summary ofthe sponsor's efficacy resultsfor the primary and some important secondary endpoints.
Table 1. Summary of Efficacy ResultsEffcacy Risperidone Haloperidol p-value
Primary Variable N=I77 N=188. Time to Relapse (days) 452.23 (SE 17.68) 391.3 (SE 21.83) 0.001Secondary Variables. Number of patients with Psychotic Relapse
---- at 1 year 41 (23.2%) 65 (34.6%) 0.009_n_ at Endpoint 45 (25.4%) 75 (39,9%) 0.002
. P ANSS, change from Baseline to Endpoint BL mean change BL mean change---- Total PANSS score 65.06 -3.15 67.38 1.79 pO:O.OOl
---- Positive symptoms 18,58 -1.6 19.15 -0,24 0.005---- Negative symptoms 16.98 -0.53 17.80 0.77 0,004---- Disorganized thoughts 14,97 -0.79 15.38 0.17 0.014m_ Uncontrolled hostility/excitement 1.04 0.29 6.26 0.73 0.076---- Anxiety/depression factor 1.45 -0.52 8.76 0.24 0.005
. CGI-C, change from Baseline to Endpoint---- Very much improvement 12 (6.9%) 8 (4.3%) 0:0.001
---- Much improvement 41 (23.7%) 25 (13.4%)
---- Minimum improvement 50 (28,9%) 35 (18.7%)
---- Unchanged 35 (20.2%) 59 (31.6%)
2

According to the sponsor's test results shown on Table 1, they concluded that risperidOrie wasstatistically significantly more effective than haloperidol in maintaining clinical efficacy over a1- to 2- year period in stable subjects with schizophrenia or schizoaffective disorder. Log-termtreatment with risperidone was associated with superior symptom improvement includingstatistically significantly superior efficacy against haloperidol on positive, negative and affectivesymptoms.
3. Description of the Sponsor's Studies and Statistical Methodologies
3.1 Study RIS-USA-79
3.1.1 Trial Objectives
The primary objective of this double-blind study is to compare the time to relapse in stableoutpatient schizophrenics and subjects with schizoaffective disorder receiving risperidone orhaloperidol for at least 1 year.
Secondary objectives include comparing the effects of these two drugs on the incidence ofrelapse, symptom measures (P ANSS, CGI), extrapyramidal side effects (ESRS), compliance,cognitive function (6 item test battery), subject satisfaction, quality of life and resource use.
3,1.2 Trial Design
This was a double-blind trial in outpatients with chronic schizophrenia or schizoaffectivedisorder classified by Diagnostic and Statistical Manual, Fourth Edition (DSM-N). Patientswere judged by the investigator to be clinically stable for 1 month prior to enrollment into thetrial, discontinued their current antipsychotic medications, and were assigned to treatment usinga randomization scheme that 'Yas stratified by sex. Stable was defined as receiving the samedosage of antipsychotic medication for 30 days and living in the same residence for 30 days.
The trial used a parallel-group design with 2 treatment arms: risperidone and haloperidoL. Trialmedication was escalated over the first 3 days of double-blind treatment to a dosage for 4 mg/dayrisperidone or 10 mg/day haloperidoL. For the first month oftherapy, assessments were made atI-week intervals to allow adjustment of medication to within the range of2 mg to 8 mg/day forrisperidone and 5 mg to 20 mg/day for haloperidoL. Thereafter, trial visits were scheduled every4 weeks. Additional visits were to be scheduled as needed. Patients were to be followed until thelast patient enrolled into the trial had completed 1 year of double-blind treatment. Patients whorelapsed a second time were to be discontinued from the triaL.
3.1.3 Effcacy
Several parameters were used to evaluate the efficacy of risperidone for maintenance treatmentof patients with stable schizophrenia or schizoaffective disorder.
3
3. I .3.1 Primary Efficacy Parameter
The primary efficacy parameter was the time to relapse. Relapse was defined as anyone of thefollowing occurrences:
· psychiatric hospitalization,· clinical judgment that an increase in level of care was necessary and increase in P ANSS
score of25% compared with Baseline, or an increase often points if the baseline score was::40, (The increases in level of care and in P ANSS score had to occur within 2 weeks of eachother in order to qualifY a patient's relapse.)
· deliberate self injury, in the investigator's opinion,· emergence of clinically significant suicidal or homicidal ideation,· violent behavior resulting in significant injury to another person or significant propert
damage, in the investigator's opinion, or· significant clinical deterioration in the investigator's judgment (a CGI-C score of6, "much
worse").
When the investigator rated the patient's CGI-C at 6, the patient was counted as relapsed even ifthe investigator did not indicate relapse.
3.1.3.2 Secondary Efficacy Parameters
The secondary efficacy parameters were:· Relapse rates at I-year and at Endpoint· Total PANSS
· P ANSS subscale scores· Clinical improvement measured by a 20% decline in total P ANSS score· CGI and CGI-C
· Quality oflife (the Delight-Terrible (D-T) scales in the brief Quality of Life Interview)· Cognitive function tests· Drug Attitude Inventory and,· Health Care Resource Utilization
3.1.4 Statistical Methods and Analyses Planned
Assume that a projected relapse rate over a I-year period of25% in the risperidone group and40% in the haloperidol group, 165 patients per treatment, or a total of 330 patients were reqiredto achieve the power of 0.8. To adjust for patient discontinuations resulting from reasons otherthan disease relapse, the protocol specified the randomization of 414 patients from 40 sites. Allstatistical tests were interpreted at the 5% 2-tailed significance level, unless otherwise noted.
Trial sites were sorted by the number of patients enrolled. Iftoo few patients were entered at asite, the site was grouped with another site accordingly by size. Sites with the fewest patientswere pooled with the next smallest site; If the number of patients was not ¿ 12 after pooling, the
4

next smallest site was included in the pool. The process was repeated until all-sites had aminimum of 12 patients.
Two populations of patients were defined for purposes of analyses:1. All randomized patients who received trial medication were counted in the population for
safety analyses;2. All randomized patients who received trial medication and who had at least 1 post-Baseline
assessment were counted in the intent-to-treat population for the analyses of changes fromBaseline.
There were 4 weekly visits numbered 3 through 6 (Week 1 to Week 4) starting the double-blindtreatment. Visits could continue through 27 months oftreatment and were numbered 7 through33 (Week 8 through Week 112). Visits 3 through 6 were to be performed on specified days plusor minus 1 day (i.e., Visit 3 could be made on trial days 7,8 or 9). Visit 7 through 33 were to bemade on the specified day plus or minus 4 days from the previous visit (i.e., Visit 7 could bemade on trial days 53 through 61). Any deviation from this schedule was considered a violationof the protocol.
3.1.4.1 For Baseline Demographic Characteristics
Demographic information was summarized statistically for age, with mean values, standarddeviations, standard errors, median values, and minimum and maximum values provided. Forpatient sex and race, frequency counts were provided by treatment group. Inter-group differenceswere evaluated with a 2-way ANOV A model with treatment and investigator as factors. Forcategorical data, the Cochran-Mantel-Haenszel (CMH) test, adjusting for investigator, was used.
3.1.4.2 For Primary Parameter- Time to Relapse
Kaplan-Meier survival curves were generated for each treatment group. Between treatmentdifferences were assessed using a stratified log-rank test controlling for investigator and sex.
Relapse rate at 6 month, 1 year, and at end ofthe trial, were estimated by using Kaplan-Meiermethod.
Secondary analyses were performed on the subsets of patients who had diagnosis ofschizophrenia or schizoaffective in order to assess the consistency in treatment effects acrossthese subgroups. Whereas a similar statistical method, a stratified log-rank test controllng forinvestigator and sex, was applied in the analysis of the schizophrenia subgroup. For the
schizoaffective subgroup, a non-stratified log-rank was used due to the small sample size.
3.1.4.3 For the Secondary Parameters
3.1.4.3.1 Relapse Rate
One-year relapse rate frequency tables were generated and CMH tests were applied controllngfor investigator and sex. A similar analysis was performed for the endpoint data.
5

The differences in relapse rates between the two treatment groups were assessed for the subsetsof patients who had diagnosis of schizophrenia or schizoaffective at baseline. Similar to theanalysis on the time to relapse data, due to the small sample size, the between treatmentcomparison for the schizoaffective subgroup was based on the chi-square test without controllngfor the investigator and sex effects.
3.1.4.3.2 Positive and Negative Symdrome Scale (P ANSS)
The changes from baseline in total P ANSS score and sub scale scores were calculated at eachassessment time point. Within-group differences were calculated using the paired t-test and inter-group comparisons were performed using an ANCOV A model with investigator, treatment, andsex as factors, and the baseline value as a covariate.
3.1.4.3.3 Cognitive Assessments
Treatment differences in each ofthe cognitive assessment tests were analyzed using ANCOV Awith investigator, sex, and treatment as factors, and the baseline value as a covariate.
3.1.4.3.4 Drug Attitude Inventory (DAI)
Between treatment differences were evaluated with the CMH test controllng for investigator andsex. For total DAI, the sum of all items was calculated, and inter-treatment differences in thechanges from baseline were analyzed using the ANOV A model with factors of treatment, sex,
and investigator.
3.1.4.3.5 Quality of Life Interview (QOLI)
Descriptive statistics for the observed changes from baseline were provided for the Delight-Terrible (D- T) scales, which were added together, with total calculated scores. Treatmentdifferences in D- T scales were examined using ANCOV A with factors for treatment, sex andinvestigator as factors, and baseline scores as covariates.
3.2 Study RIS-INT-6
RIS-INT-6 was the first long-term study with risperidone to be conducted under double-blindconditions. The trial was of a multicenter, multinational, double-blind, randomized designcomparing the efficacy of risperidone and haloperidol over 1 year in patients with an acuteexacerbation of chronic shcizophrenia at selection.
3.2.1 Effcacy Assessments
3.2.1.1 Primary Efficacy Parameter
The primary efficacy parameter was the time to discontinuation as a result of adverse events orclinical relapse. Relapse was defined as a deterioration in the subject's clinical condition thatcould not be managed satisfactorily after adjustment of dosage within protocol limits
6

3.2.1.2 Secondary Efficacy Parameters
The secondary efficacy parameters were:. Total PANSS
· PANSS subscale scores (positive, negative, and psychopathology scales)· CGI. Quality of life
. Patient compliance
3.2.2 Planned Statistical Analyses
Sample size determination was based on a projected I-year relapse rate of 25% in the risperidonegroup and of 55% in the haloperidol group. It was estimated that 80 subjects per treatment group,or a total of 160 subjects were would provide 90% power to detect statistically significantdifference in the relapse rates at a two-tailed significance level of 0.05. To account for patientdiscontinuations for reasons other than disease relapse, a total of 180 subjects across 40 centerswere randomized.
The primary efficacy parameter (the time to discontinuation because of adverse events orpsychotic relapse) was estimated by the Kaplan-Meier product-limit method and comparedbetween treatment groups by means of the Gehan' s generalized Wilcoxon test, stratified forcountr.
Changes from baseline to endpoint in P ANSS total and subscale scores were subjected to a two-way analysis of covariance (ANCOY A) model with factors for baseline score, treatment, andcountry. A clinical response was defined as a 50% or greater reduction in P ANSS score. Thenumber of responders and the CGI scores in each treatment group was compared using theCochran-Mantel-Haenszel tests for general association. The compliance rating scale scores ineach group were compared using the Yan Eletern test.
4. Detailed Review of the Sponsor's Individual Study Results
4.1 Study RIS-USA-79
4.1.1 Subject Disposition
In total, 397 subjects were enrolled into RIS-USA-79 from 32 sites in the USA: 395 subjectreceived trial medication (192 risperidone and 203 haloperidol). At the time of stopping the trial,78 subjects were stil being treated with risperidone and 46 were stil receiving haloperidoL.
During the audit ofRIS-USA-79, the sponsor determined that the data from Site #8 did not meetthe Janssen Pharmaceutical quality standards, so the analyses were performed with and withoutSite #8. Since the sponsor mentioned that the results from the analyses with or without this sitewere found generally consistent. In the sponsor's study report for efficacy analyses, the efficacydata without Site #8 were presented but with brief summaries of the all site population analyses.
7

After excluding data from Site #8, there were total 365 subjects in the efficacy analyses. Thegroups of risperidone and haloperidol had 177 subjects and 188 subjects, respectively.
4.1.2 Premature Discontinuations
As shown in Table 2, more subjects discontinued treatment with haloperidol (77.3%) than wasthe case for risperidone (59.4%). This was principally due to a higher rate of relapse in thehaloperidol group (23.2%) than in the risperidone group (14.6%).
Table 2. Summary of Reasons for Premature DiscontinuationReasons for Discontinuation Risperidone Haloperidol
N=192 N=203
n % n %Chose to discontinue 35 18.2 36 17.7Relapse 28 14.6 47 23.2Adverse event 24 12.5 30 14.8Lost to follow-up 10 5.2 10 4.9Poor compliance 6 3.1 is 7.4Administrative 6 3.1 2 1.0Other 3 1.6 4 2.0Inadequate response 2 1.0 7 3.4Ineligible 0 0 3 1.Intercurrent ilness 0 0 2 1.0Abnormal c1inicallaboratorv result 0 0 1 0.5Total Number ofSubiects Discontinued 114 59.4 157 77.3
4.1.3 Demographics and Baseline Characteristics
The demographic characteristics were well balanced between the treatment groups. Overall31.1 % of the patients were female; 47.6% were white and 36.5% were black. Their meanage:!SD was 40.5:!1 0.56 years old (median age 39 years and range 20 years to 65 years old).Their mean weight:SD was 82.8:!19.74 kg and their mean height:SD was 171.3:!lO.96 cm.Table 3 provides a by treatment summary of the demographic and Baseline characteristics for the395 patients who were randomized and received trial medication.
Table 3. Baseline Dèmographic Characteristics including data from Site #8Demographic Data Risperidone Haloperidol
N=192 N=203
n % N %Sex Female 57 29.7 66 32.5
Male 135 70.3 137 67.5Race White 91 47.4 97 47.8
Black 72 37.5 72 35.5Hispanic 24 12.5 29 14.3Other 3 1.5 2 1.0Oriental 2 1.0 3 1.5
8

Mean SD Mean SDAge (years) 40.8 10.72 40.1 10.43Weight (kg) 82.0 19.62 83.6 19.87Height (cm) 171.3 11.75 171.3 10.18
The without Site #8 baseline demographic characteristics by treatment groups were shown inTable 3.1. Overall 30.1% of the patients were female; 47.7% were white and 35.6% were black.The mean age:SD was 40.2::10.51 years old. Their mean weight:SD was 82.8::19.11 kg andmean height:SD was 171.3::11.01 cm and.
Table 3.1. Baseline Demographic Characteristics without data from Site #8Demographic Data Risperidone Haloperidol
N=I77 N=188
n % N %Sex Female 50 28.2 60 31.9
Male 127 71.8 128 68.1Race White 81 45.8 93 49.5
Black 67 37.9 63 33.5Hispanic 24 13.6 27 14.4Other 3 1.7 2 1.0Oriental 2 1.1 3 1.6
Mean SD Mean SDAge (years) 40.3 10.62 40.1 10.43Weight (kg) 82.8 19.21 82.8 19.06Height (em) 171.5 11.87 171.2 10.16
4.1.4 Primary Efficacy Parameter
Since the sponsor determined that the data from Site #8 did not meet the Janssen Pharmaceuticalquality standards, they only presented the data analyses for the primary and secondary efficacyvariable excluding data provided by this site in their study report.
According to the sponsor's study report, subjects in the risperidone treatment group had a longermean time to relapse (452.2::17.7 days) than the subjects in the haloperidol treatment group
(391.3::21.8 days). However, as the last observations for both treatment groups were censored,the mean time to relapse may be underestimated.
The 25th percentile for time to relapse was 292 days for the risperidone treatment group and 113days for the haloperidol treatment group. Median time to relapse was 406 days for subjects onhaloperidol, but there were too few relapsing subjects in the risperidone group to determine amedian time to relapse. There were insufficient numbers of relapse subjects in either treatmentgroup to calculate the 75th percentile relapse rates.
9

Using the stratified logrank test, there was a statistically significant difference, in favor ofrisperidone, between the survival distribution ofthe 2 treatment groups (p=O.OOI). The Kaplan-Meier survival probability plot of time to relapse is shown in Figure 1.
Figure 1. Kaplan-Meier Survival Probabilty plot of time to relapse
(Note: The upper curve is for Risperidone group and the lower curveis for Haloperidol group)
q
lXQ) ci~
1LQ)inD-II to
16 ci0:Olc:
ëii!D
Õ ''
~ ci
:eII.J0è: N
ci
0ci
0 200 400 600 800
Time (days)
The one year relapse rate (probabilty of relapse), based on the Kaplan-Meier estimates, were29% and 45% for the risperidone and haloperidol groups, respectively. The Kaplan-Meierestimates for the relapse rates were consistently lower in the risperidone group than in thehaloperidol group at 6 month (19% versus 30%), 1 year (29% versus 45%), and at the end of thetrial timepoints (34% versus 60%).
In order to verify the results for subjects with C :J for those withschizophrenia, the analyses were repeated in each diagnosis of the population. These results areshown in Table 4.
Among the patients with diagnosis of schizophrenia (n=200), there was a statistically significantdifference between the two treatments, in favor ofrisperidone, in the survival curves (p=0.007).In the risperidone group, the Kaplan-Meier estimates of relapse rates, i.e., the probability ofrelapse, was 19%,28% and 34%, at 6 months, 1 year and at the end of the trial, respectively.These rates were consistently lower than those in the haloperidol group (32%, 47% and 59%respectively)
c .=i
10

~ JC. J Nonetheless, th~-Kaplan-M~ier estimates of
relapse ratesat 6 months, 1 year and at the end ofthe trial were 19%,34%, and 34%, in the risperidone group,which were consisetntly lower than the corresponding rates in the haloperidol group (21 %, 37%and 62%, respectively).
Table 4. Analysis of Time to Relapse in Patients with Schizophrenia and SchizoaffectiveDisorders
Risperidone Haloperidol P-valueAll diaenoses N=I77 N=188 0.001 b
Number (%) relapsed 45 (25.4%) 75 (39.9%)Mean (SE) time to relapse* 452.2 (17.7) 391.3 (21.8)Relapse rate at 6 montha 19% 30%Relapse rate at 1 yeara 29% 45%Relapse rate at end of triaia 34% 60%25% Quartile (days) 292.0 113.050% Quartile (days) ---- 406Schizophrenia N=144 N=156 0.007°Number relapsed 36 (25.0%) 62 (39.7%)Relapse rate at 6 montha 19% 32%Relapse rate at 1 yeara 28% 47%Relapse rate at end of triaia 34% 59%25% Quartile (days) 293.0 109.050% Quartile (days) ---- 385
L ~- -
*The estimated means were biased, since the last observations were censored."Kaplan-Meier estimates of relapse rate (probabilty of relapse).bStratified log-rank test controllng for investigator and sex.C ~4,1.5 Secondary Effcacy Parameters
4.1.5.1 Relapse Rates (The Crude Rates)
Of365 patients in the trial, 41 patients (23.2%) in the risperidone treatment group and 65patients (34.6%) in the haloperidol treatment group relapsed by the end ofthe first year(p=0.009). At Endpoint, 45 patients (25.4%) on risperidone treatment and 75 patients (39.9%) onhaloperidol had relapsed (p=0.002).
Similar significant differences (p=O.OII) were apparent in subgroup analyses of patients withschizophrenia. C. .J11

c =lTable 5. Relapse Rates in Subjects with Schizophrenia and Schizoaffective Disorders
Relapse Rates Risperidone Haloperidol P-value
n I % N I %All diagnoses N=I77 N=1881 Year 41
I
23.2 65
I34.6 0,009
Endpoint 45 25.4 75 39.9 0.002
Schizophrenia N=144 N=1561 Year 32
I
22.2 56
I
35.9 0.016Endpoint 36 25.0 62 39.7 0.011
C ,~
As it was shown in Table 6, most ofthe patient relapses were due to the psychiatrichospitalization and clinical deterioration.
Table 6. Summary of the Number of Subjects Discontinuing due to Relapse by Criteria ofR ie apse
Criteria for Relapse Risperidone HaloperidolEntire Trial N=I77 N=188
n % n %Psychiatric hospitalization 20 44.4 36 48.0Significant clinical deterioration (a CGI-C score of 6) 16 35.6 22 29.3Increase in level of care was necessar and increase in P ANSS 8 17.8 14 18.7score of 25% compared with Baseline, or an increase of 10points if the Baseline score was 0(40
Emergence of clinically significant suicidal or homicidal 1 2.2 3 4.0ideationTotals 45 75
4.1.5.2 Positive and Negative Symptom Scale (PANSS)
There was no significant difference in baseline measures of positive, negative or affectivesymptoms on the PANSS (see Table 7).
The mean shift from baseline on the P ANSS total score at endpoint was better in the risperidonetreatment group (-3.15), compared to + 1.79 in the haloperidol treatment group. At endpoint,there was a significant difference in favor of risperidone over haloperidol for the total P ANSSscore (p..O.OOl) and for both the positive (p=0.005) and negative (p=0.004) subscales. A similaradvantage for risperidone was also seen on the anxiety/depression (p=0.005) and disorganizedthoughts (p=0.014) subscales ofthe PANSS. The between treatment difference for uncontrolledhostility/excitement was on the borderline of significance (p=0.076).
12
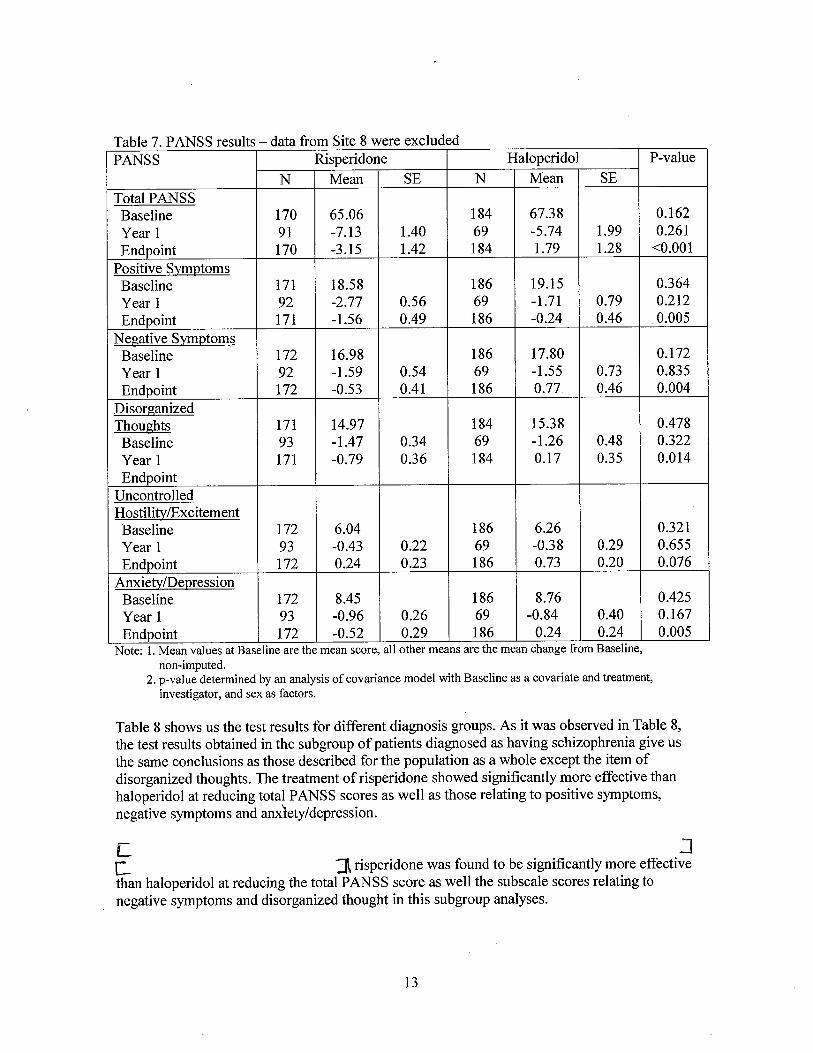
Table 7. PANSS results - data from Site 8 were excludedP ANSS Risperidone Haloperidol P-value
N Mean SE N Mean SE
Total PANSSBaseline 170 65.06 184 67.38 0.162Year 1 91 -7.13 1.40 69 -5.74 1.99 0.261
Endpoint 170 -3.15 1.42 184 1.79 1.28 .-0.001
Positive SymptomsBaseline 171 18.58 186 19.15 0.364Year 1 92 -2.77 0.56 69 -1.71 0.79 0.212Endpoint 171 -1.56 0.49 186 -0.24 0.46 0.005
Negative SymPtomsBaseline 172 16.98 186 17,80 0.172Year 1 92 - 1.59 0.54 69 -1.55 0.73 0.835Endpoint 172 -0.53 0.41 186 0.77 0.46 0.004
DisorganizedThoughts 171 14.97 184 15.38 0.478
Baseline 93 -1.47 0.34 69 -1.26 0.48 0.322Year 1 171 -0.79 0.36 184 0.17 0.35 0.014Endpoint
UncontrolledHostilitvÆxcitementBaseline 172 6.04 186 6.26 0.321
Year 1 93 -0.43 0.22 69 -0.38 0.29 0.655Endpoint 172 0.24 0.23 186 0.73 0.20 0.076
Anxietv/DepressionBaseline 172 8.45 186 8.76 0.425Year 1 93 -0.96 0.26 69 -0.84 0.40 0.167Endpoint 172 -0.52 0.29 186 0.24 0.24 0.005
Note: 1. Mean values at Baseline are the mean score, all other means are the mean change from Baseline,non-imputed.
2. p-value determined by an analysis of covariance model with Baseline as a covariate and treatment,investigator, and sex as factors.
Table 8 shows us the test results for different diagnosis groups. As it was observed in Table 8,the test results obtained in the subgroup of patients diagnosed as having schizophrenia give usthe same conclusions as those described for the population as a whole except the item ofdisorganized thoughts. The treatment of risperidone showed significantly more effective thanhaloperidol at reducing total PANSS scores as well as those relating to positive symptoms,negative symptoms and anxlety/depression.L ~c :i risperidone was found to be significantly more effectivethan haloperidol at reducing the total P ANSS score as well the subscale scores relating tonegative symptoms and disorganized thought in this subgroup analyses.
13

Table 8, P ANSS results in subjects with schizophrenia 1: JPANSS Mean change at endpoint versus baseline
Schizophrenia ,
Risperidone Haloperidol p-valueN=144 N=156
Total PANSS -3.01 2.22 0.004(n=139) (n=152)
Positive -1.56 0.05 0.008Symptoms (n=140) (n=154)
Negative -0.51 0.73 0.026Symptoms (n=141) (n=154)
Disorganized -0.61 0.17 0.146Thoughts (n=140) (n=152) /UncontrolledHostilty/ 0.41 0.77 0.251Excitement (n=141) (n=154)
Anxiety/ -0.75 0.36 ~0.001Depression (n=141) (n=154) -Note: 1. N denotes the total number of patients in the group but n denotes the number of patients used to compute
the mean change from Baseline to the endpoint.2. p-values were from the analysis of covariance test of no difference between treatment groups with baseline
score as covariate.
4.1.5.3 Clinical Global Impression (CGI/CGI-C)
The CGI ratings at Baseline were comparable in both groups, however, during double-bltndtreatment, symptoms decreased more with risperidone treatment than with haloperidol treatment.Table 9 shows that the overall CGI ratings at endpoint were significantly better with risperidonethan with halopericdol (p~O.OOI), with 59.5% ofrisperidone-treated subjects compared with36.4% of the haloperidol group being minimum improved, much improved or very muchimproved.
T bl 9 CGI C fr B l Y 1 dEd .a e - om ase me to ear an n lpomtRisperidone Haloperidol p-valuen % n %
Year 1 N=93 N=70Very much improvement 7 7.5 4 5.7 0.006Much improvement 28 30.1 14 20.0Minimum improvement 27 29.0 19 27.1Unchanged 28 30.1 27 38.6 ,
Endpoint N=173 N=187Very much improvement 12 6.9 8 4.3 ~0.001Much improvement 41 23.7 25 13.4Minimum improvement 50 28.9 35 18.7Unchanged 35 20.2 59 31.6
14
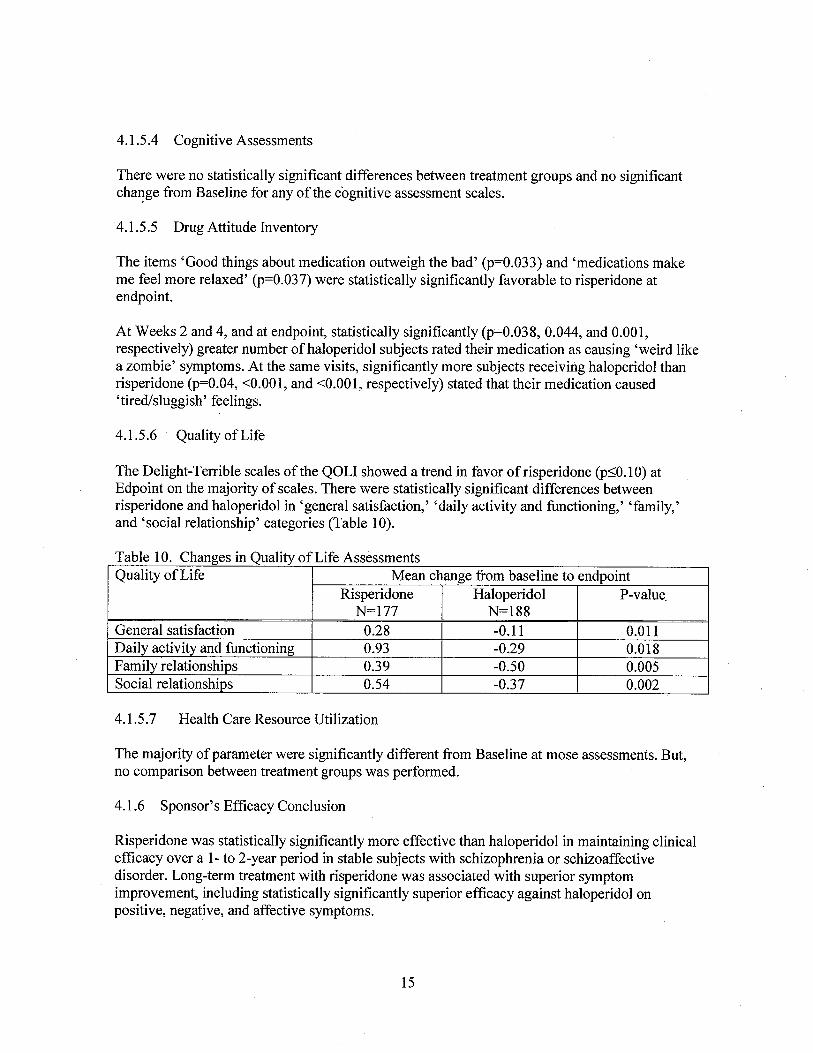
4.1.5.4 Cognitive Assessments
There were no statistically significant differences between treatment groups and no significantcha~ge from Baseline for any of the cognitive assessment scales.
4.1.5.5 Drug Attitude Inventory
The items 'Good things about medication outweigh the bad' (p=0.033) and 'medications makeme feel more relaxed' (p=0.037) were statistically significantly favorable to risperidone atendpoint.
At Weeks 2 and 4, and at endpoint, statistically significantly (p=0.038, 0.044, and 0.001,respectively) greater number of haloperidol subjects rated their medication as causing 'weird likea zombie' symptoms. At the same visits, significantly more subjects receiving haloperidol thanrisperidone (p=0.04, -:0.001, and -:0.001, respectively) stated that their medication caused'tired/sluggish' feelings:
4.1.5.6 Quality of Life
The Delight-Terrible scales of the QOLI showed a trend in favor ofrisperidone (p:S0.10) atEdpoint on the majority of scales. There were statistically significant differences betweenrisperidone and haloperidol in 'general satisfaction,' 'daily activity and functioning,' 'family,'and 'social relationship' categories (Table 10).
Table 10. Changes in Quality of Life AssessmentsQuality of Life Mean change from baseline to endpoint
Risperidone Haloperidol P-value.N=I77 N=188
General satisfaction 0.28 -0.11 0.011Daily activity and functioning 0.93 -0.29 0.018Family relationships 0.39 -0.50 0.005Social relationships 0.54 -0.37 0.002
4.1.5.7 Health Care Resource Utilization
The majority of parameter were significantly different from Baseline at mose assessments. But,no comparison between treatment groups was performed.
4.1.6 Sponsor's Efficacy Conclusion
Risperidone was statistically significantly more effective than haloperidol in maintaining clinicaleffcacy over a 1- to 2-year period in stable subjects with schizophrenia or schizoaffectivedisorder. Long-term treatment with risperidone was associated with superior symptomimprovement, including statistically significantly superior efficacy against haloperidol onpositive, negative, and affective symptoms.
15
The finding that risperidone is superior to haloperidol, which has itself been shown to beeffective in preventing relapses, indicates that risperidone has an important role to play in thelong-term treatment of schizophrenia.
4.2 Study RIS-INT-6
4.2.1 Subject Disposition
A total of 190 subjects were recruited into the study from 48 centers in seven countries: 91
subjects were assigned to treatment with risperidone and 99 received haloperidoL.
4.2.2 Premature Discontinuations
A significantly greater proportion of subjects discontinued treatment with haloperidol (62subjects; 63%) than was the case with risperidone (47 subjects; 52%; p=0.04 CMH test).
The primary reason for discontinuing therapy was insufficient efficacy (including psychoticrelapse) which accounted for 20 subjects (22%) in the risperidone group and 32 subjects (32%)in the haloperidol group.
4.2.3 Demographics and Baseline Characteristics
The subjects in the risperidone group comprised 57 male and 34 female patients with a medianage of33 year (range: 18 to 65 years). The haloperidol group included 58 male and 41 femalepatients with a median age of34 years (range: 18 to 65 years).
4.2.4 Primary Efficacy Parameter: Withdrawal for Adverse Events and/or Psychotic Relapse
In total 25 subjects (27%) withdrew from risperidone and 26 (26%) withdrew from haloperidolbecause of adverse events and/or psychotic relapse. Regarding the time to discontinuation, 25%of the subjects in the risperidone group dropped out by Day 141 (lower 95% CI: Day 78)whereas 25% of the subjects in the haloperidol group had done so by Day 100 (lower 95% CI;Day 36). The difference between the groups was not statistically significant (p=0.457, Gehan'sgeneralized Wilcoxon test stratified for country).
4.2,5 Secondary Efficacy Parameters
4.2.5.1 PANSS Scores
Baseline P ANSS scores were found to be comparable in the two groups of subjects. However,subjects treated with risperidone tended to have a significantly greater change in total PANSSscore at end point (-24.6) than those receiving haloperidol (-18.9; p=0.059 ANOV A). Thecorresponding changes in the total P ANSS-derived BPRS scores were -14.0 for risperidone and-10.8 for haloperidol (p=0.061).
16

As shown in Table i 1, the mean changes in total P ANSS scores were progressive throughout the52 week evaluation period in both groups of subjects,
Table 11. P ANSS resultsPANSS Risperidone Haloperidol p-value
N Mean SE N Mean SETotal P ANSS
Baseline 91 95.8 1.91 99 96.8 1.91 0.059Year 1 45 -39.0 3.90 36 -38.3 4.26Endpoint 91 -24.6 3.08 99 -18.9 2.89
Positive SubscaleBaseline 91 22.8 0.67 99 23.5 0.72 0.082Year 1 45 -11.7 1.21 36 -11.9 1.37Endpoint 91 -7.9 0.92 99 -6.6 0.94
Negative Subscale
Baseline 91 26.0 0.76 99 26.5 0.76 0.103Year 1 45 -8.7 1.19 36 -8.1 1.43Endpoint 91 -5.9 0.87 99 -4.6 0.77
Thoughts DisturbancesBaseline 91 13.4 0.43 99 14.2 0.42 0.1 05Year 1 45 -6.7 0.71 36 -6.9 0.75Endpoint 91 -4.6 0.54 99 -4.2 0.52
HostilityBaseline 91 8.5 0.32 99 8.7 0.33 0.410Year 1 45 -3.9 0.47 36 -3.8 0.71Endpoint 91 -2.2 0.43 99 -1.7 0.47
Anxiety/DepressionBaseline 91 11.6 0.34 99 11.1 0.39 0.291Year 1 45 -4.7 0.60 36 -4.5 0.54Endpoint 91 -2.5 0.47 99 -1.6 i 0.45
Note: Mean values at Baseline are the mean score, all other means are the mean change from Baseline.
4.2.5.1 Clinical Global Improvement (CGI)
The mean baseline values ofthe CGI were 5.0 for risperidone and 5.1 for haloperidoL. Thecorresponding mean scores at end point, were 3.8 and 4.1, respectively (p=0.103, CMH test).
The mean overall CGI change score versus baseline were also comparable in the two treatmentgroups at endpoint (3.1 for risperidone and 3.2 for haloperidol, p=0.357).
4.2.5.2 Quality of Life
The mean total Quality of Life score at baseline was 47.0 for risperidone and 45.4 withhaloperidoL. There was a significantly greater improvement in the risperidone group for the
17

cluster 'instrumental role functioning' (+2.3) than was apparent in the haloperidol group (+ 1.0;p=0.037). The changes from baseline to end point on the other subscales were similar in the twotreatment groups.
4.2.5.3 Compliance Rating Scale
The majority of patients in both groups (77%) had 'good' or 'very good' scores on thecompliance rating scale at endpoint. There was no significant between-group difference at anytime point during the study.
4.2.6 Sponsor's Efficacy Conclusions
Because of the choice of comparator, as well as other design considerations, the conclusions thatcan be drawn from the results ofRIS-INT-6 are somewhat limited. Nonetheless, the findings arenot inconsistent with those of RIS- USA -79, and support the conclusion that risperidone is aneffective antipsychotic for the long-term treatment of schizophr~nia.
5. Statistical Reviewer's Findings and Comments
1. When the sponsor's study RIS-USA-79 was evaluated, this reviewer did not find anyinconsistent test results with the sponsor's. For the primary endpoint and the secondaryendpoints, this reviewer was able to exactly duplicate the sponsor's results.
2. £. :i the sponsor had statistically significant test results shown on the primary and some
secondary efficacy endpoints in the whole study population (i.e, patients with eitherschizophrenia or schizoaffective disorder) for Study RIS-USA-79C- JC _ JC :J. Table 12 shows thesummary of p-values for all study patients, only schizophrenia patients r: JC .:
Table 12. Summary ofp-values for the Whole Study Population and Sub-populationsEffcacy variables All Diagnoses Schizophrenia 'r- --
(N=365) (N=300) , =Primary Variable. Time to Relapse (days) 0.001 0.007 -Secondary Variables. NuIIber of patients with Psychotic Relapse
---- at 1 year 0,009 0.016---- at Endpoint 0.002 0.011
. P ANSS, change from Baseline to Endpoint---- Total PANSS score ~0.001 0.004---- Positive symptoms 0.005 0.008--- Negative symptoms 0,004 0.026---- Disorganized thoughts 0.014 0.146---- Uncontrolled hostility/excitement 0.076 0.251---- Anxiety/depression factor 0,005 ~0.001 '- -
18

3. Except for two diagnosis groups, the sponsor did not perform any other subgroup analysis.
They did mention in the protocol that" Ifthe size ofthe study permits, relevant demographicor baseline value-defined subgroups wil be examined for unusually large or small responses,e.g., comparison of effects by age, sex, and race." However, it is not clear what they mean'permits' .
Since there are reasonable number of patients in both female and male groups as well aswhite and black race groups, it would be interested to know the analysis results among thesesubgroups. This reviewer performed subgroup analyses similar to what were shown inTable 4 and summarized results in Tables 13 and 14.
As we can observe in Table 13, the risperidone was shown statistically significantly moreeffective than haloperidol for male patients but not for female patients. Since the risperidonetreatment group did have smaller relapse rates than the haloperidol treatment group forfemale patients, the lack of ability to detect differences between these two groups may be dueto the insufficient sample size.
According to Table 14, there existed statistically significant difference between therisperidone and haloperidol treatment groups on both white and black patient groups.
Table 13. Subgroup Analyses for GenderRisperidone Haloperidol P-value*
Female Patients N=50 N=60 0.1280Number relapsed 12 (24%) 22 (36.7%)Relapse rate at 6 montha 11% 24%Relapse rate at 1 yeara 32% 38%Relapse rate at end of triaia 32% 58%25% Quartile (days) 292 20050% Quartile (days) ---- 590Male Patients N=127 N=128 0.0012Number relapsed 33 (26%) 53 (41.4%)Relapse rate at 6 montha 22% 33%Relapse rate at 1 yeara 28% 49%Relapse rate at end of triaia 34% 61%25% Quartile (days) 282 10750% Quartile (days) ---- 375* p-values were obtained from the log-rank test without any stratification,
19

Table 14. Subgroup Analyses for Race of White and BlackRisperidone Haloperidol P-value*
White Patients N=81 N=93 0.0133Number relapsed 25 (30.9%) 39 (41.9%)Relapse rate at 6 montha 27% 39%Relapse rate at 1 yeara 35% 59%Relapse rate at end of triaia 41% 70%25% Quartile (days) 154 7950% Quartile (days) ---- 278Black Patients N=67 N=63 0.0333Number relapsed 13 (19.4%) 23 (36.5%)Relapse rate at 6 montha 12% 17%Relapse rate at 1 yeara 26% 35%Relapse rate at end of trial
a 26% 55%25% Quartile (days) 348 22550% Quartile (days) ---- 582*p-values were obtained from the log-rank test without any stratification,
4. To check ifthe early discontinued patients influence the test results for the primary endpoint,time to relapse, this reviewer treated them as failures by reversing their censoring variablesand reran the analyses. The p-value shows .0008. So, it assures us the robustness ofthe testresult for the primary endpoint. The Kaplan-Meier Survival curves for this case is shown inthe following figure.
Figure 2. Kaplan-Meier Survival Probability plot of time to relapse after reversing censoringvariables for the early discontinued patients. (Note: The upper curve is forRisperidone group and the lower curve is for Haloperidol group)
C!
coQ) cii!u.Q).,0.m lD~ c:Clcë¡¡mÕ ."~ ci:em.con. N
ci
oci
a 200 400
Time (days)
600 800
20

Yeh-Fong Chen, Ph.D.Mathematical Statistician
Concurrence:
Dr. Jin Dr. Chi
cc: NDA 20-272 (S-008)HFD-120/Dr. KatzHFD-120/Dr. Laughren
HFD-120/Dr. Andreason
HFD-120/Mr. Hardeman
HFD-700/Dr. AnelloHFD-710/Dr. Chi
HFD-710/Dr. JinHFD-710/Dr. Chen
This review consists of21 pages. MS Word: C:/yfchen/nda20272_s008/review,doc
21
This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.
/s/Yeh- Fang Chen12/20/01 10: 03: 07 AMBIOMETRICS
Kun Jin12/20/01 11:21:05 AMBIOMETRICS
George Chi12/21/01 11:44:39 AMBIOMETRICS

CENTER FOR DRUG EVALUATION ANDRESEARCH
APPLICATION NUMBER:
NDA 20-272/8-008 & 20-588/8-004
ADMINISTRATIVE and CORRESPONDENCEDOCUMENTS

EXCLUSIVITY SUMRY for NDA # 20-272 SE8-008 & 20-588 SE8-004Trade Name Risperdal Generic Name risperidoneApplicant Name: Johnson & Johnson Pharmaceutical Research &DevelopmentHFD- 120Approval Date 3/3/02PART I: IS AN EXCLUSIVITY DETERMINATION NEEDED?
1. An exclusivity determination will be made for all originalapplications, but only for certain supplements. CompleteParts II and III of this Exclusivity Summary only if youanswer "YES" to one or more of the following questions aboutthe submission.
a) Is it an original NDA? YES/ / NO /i/
b) Is it an effectiveness supplement? YES / ~/ NO / /
If yes, what type (SEl, SE2, etc.)? SE8
c) Did it require the review of clinical data other than tosupport a safety claim or change in labeling related tosafety? (If it required review only of bioavailabilityor bioequivalence data, answer "NO.")
YES / ~/ NO / /If your answer is "no" because you believe the study is abioavailability study and, therefore, not eligible forexclusivity, EXPLAIN why it is a bioavailability study,including your reasons for disagreeing with any argumentsmade by the applicant that the study was not simply abioavailability study.
If it is a supplement requiring the review of clinicaldata but it is not an effectiveness supplement, describethe change or claim that is supported by the clinicaldata:
Page 1
d) Did the applicant request exclusivity?
YES / / NO /~/
If the answer to (d) is "yes," how many years ofexclusi vi ty did the applicant request?
e) Has pediatric exclusivity been granted for this ActiveMoiety?
YES / / NO /~/
IF YOU HAVE ANSWERED "NO" TO ALL OF THE ABOVE QUESTIONS, GODIRECTLY TO THE SIGNATURE BLOCKS ON Page 9.
2. Has a product with the same active ingredient (s), dosage form,strength, route of administration, and dosing schedulepreviously been approved by FDA for the same use? (Rx to OTe)Switches should be answered No - Please indicate as such).
YES / / NO /~/
If yes, NDA # Drug Name
IF THE ANSWER TO QUESTION 2 IS "YES," GO DIRECTLY TO THESIGNATURE BLOCKS ON Page 9.
3. Is this drug product or indication a DESI upgrade?
YES / / NO /--/
IF THE ANSWER TO QUESTION 3 IS "YES," GO DIRECTLY TO THESIGNATURE BLOCKS ON Page 9 (even if a study was required for theupgrade) .
Page 2

PART II: FIVE-YEAR EXCLUSIVITY FOR NEW CHEMICAL ENTITIES(Answer either #1 or #2, as appropriate)
1. Single active ingredient product.
Has FDA previously approved under section 505 of the Act anydrug product containing the same active moiety as the drugunder consideration? Answer "yes" if the active moiety(including other esterified forms, salts, complexes, chelatesor clathrates) has been previously approved, but thisparticular form of the active moiety, e.g., this particularester or salt (including salts with hydrogen or coordinationbonding) or other non-covalent derivative (such as a complex,chelate, or clathrate) has not been approved. Answer "no" ifthe compound requires metabolic conversion (other thandeesterification of an esterified form of the drug) to producean already approved active moiety.
YES / ~/ NO / /
If "yes," identify the approved drug product (s) containing theactive moiety, and, if known, the NDA # (s) .
NDA # 20-272 Risperdal tablets
NDA # Risperdal oral soln20-588
NDA #
2. Combination product.
If the product contains more than one active moiety (asdefined in Part II, #1), has FDA previously approved anapplication under section 505 containing anyone of the activemoieties in the drug product? If, for example, thecombination contains one never-before-approved active moietyand one previously approved active moiety, answer "yes." (Anactive moiety that is marketed under an OTC monograph, butthat was never approved under an NDA, is considered notpreviously approved.)
YES / / NO / /
Page 3

If "yes/" identify the approved drug product (s) containing theactive moietyi andi if known i the NDA # (s) .
NDA #
NDA #
NDA #
IF THE ANSWER TO QUESTION i OR 2 UNER PART II is II NO i II GODIRECTLY TO THE SIGNATURE BLOCKS ON Page 9. IF "YES1 II GO TO PARTIII.
PART III: THREE-YEAR EXCLUSIVITY FOR NDA i S AN SUPPLEMENTS
To qualify for three years of exclusivity i an application orsupplement must contain "reports of new clinical investigations(other than bioavailability studies) essential to the approval ofthe application and conducted or sponsored by the applicant."This section should be completed only if the answer to PART II iQuestion i. or 2 i was "yes."
i. Does the application contain reports of clinicalinvestigations? (The Agency interprets "clinicalinvestigations" to mean investigations conducted on humansother than bioavailability studies.) If the applicationcontains clinical investigations only by virtue of a right ofreference to clinical investigations in another applicationianswer "yes i" then skip to question 3 (a). If the answer to3 (a) is "yes" for any investigation referred to in anotherapplication, do not complete remainder of summary for thatinvestigation.
YES I ~I NO I_I
IF II NO i II GO DIRECTLY TO THE SIGNATURE BLOCKS ON Page 9.
2. A clinical investigation is "essential to the approval" if theAgency could not have approved the application or supplementwi thout relying on that investigation. Thus, theinvestigation is not essential to the approval if i) noclinical investigation is necessary to support the supplementor application in light of previously approved applications(i.e., information other than clinical trials, such asbioavailability data, would be sufficient to provide a basis
Page 4

for approval as an ANDA or 505 (b) (2) application because ofwhat is already known about a previously approved product), or2) there are published reports of studies (other than thoseconducted or sponsored by the applicant) or other publiclyavailable data that independently would have .been sufficientto support approval of the application, without reference tothe clinical investigation submitted in the application.
For the purposes of this section, studies comparing twoproducts with the same ingredient (s) are considered to bebioavailability studies.
(a) In light of previously approved appiications, is aclinical investigation (either conducted by theapplicant or available from some other source,including the published literature) necessary tosupport approval of the application or supplement?
YES / ~/ NO /__/
If "no," state the basis for your conclusion that aclinical trial is not necessary for approval AN GODIRECTLY TO SIGNATURE BLOCK ON Page 9:
(b) Did the applicant submit a list of published studiesrelevant to the safety and effectiveness of this drugproduct and a statement that the publicly availabledata would not independently support approval of theapplication?
YES / ~/ NO / /(1) If the answer to 2 (b) is "yes," do you personally
know of any reason to disagree with the applicant'sconclusion? If not applicable, answer NO.
YES / / NO /~/
If yes, explain:
Page 5

(2) If the answer to 2 (b) is "no," are you aware ofpublished studies not conducted or sponsored by theapplicant or other publicly available data that couldindependently demonstrate the safety and effectivenessof this drug product?
YES I I NO ILl.
If yes, explain:
(c) If the answers to (b) (1) and (b) (2) were both "no,"identify the clinical investigations submitted in theapplication that are essential to the approval:
Investigation #1, Study # RIS-USA-79
Investigation #2, Study #
Investigation #3, Study #
3. In addition to being essential, investigations must be "new"to support exclusivity. The agency interprets "new clinicalinvestiga.tion" to mean an investigation that 1) has not beenrelied on by the agency to demonstrate the effectiveness of apreviously approved drug for any indication and 2) does notduplicate the results of another investigation that was reliedon by the agency to demonstrate the effectiveness of apreviously approved drug product, i. e., does not redemonstratesomething the agency considers to have been demonstrated in analready approved application.
(a) For each investigation identified as "essential to theapproval," has the investigation been relied on by theagency to demonstrate the effectiveness of a previouslyapproved drug product? (If the investigation was reliedon only to support the safety of a previously approveddrug, answer "no.")
Investigation #1 YES I
YES I
I
I
I
NO I
NO I
I
I
NO ILI
Investigation #2
Investigation #3 YES I
If you have answered lIyes" for one or moreinvestigations, identify each such investigation and theNDA in which each was relied upon:
Page 6

NDA #NDA #NDA #
Study #Study #Study #
(b) For each investigation identified as "essential to theapproval," does the investigation duplicate the resultsof another investigation that was relied on by the agencyto support the effectiveness of a previously approveddrug product?
Investigation #1 YES /
YES /
/
/
/
NO / /
/
NO /~/
Investigation #2
Investigation #3 YES / NO /
If you have answered "yes" for one or moreinvestigations, identify the NDA in which a similarinvestigation was relied on:
NDA # Study #
NDA # Study #
NDA # Study #
(c) If the answers to 3 (a) and 3 (b) are no, identify each"new" investigation in the application or supplement thatis essential to the approval (i. e., the investigationslisted in #2 (c), less any that are not "new") :
Investigation #-l, Study # RIS-USA-79
Investigation # , Study #
Investigation # , Study #
4. To be eligible for exclusi vi ty, a new investigation that isessential to approval must also have been conducted orsponsored by the applicant. An investigation was "conductedor sponsored by" the applicant if, before or during theconduct of the investigation, 1) the applicant was the sponsorof the IND named in the form FDA 1571 filed with the Agency,or 2) the appl icant (or its predecessor in interest) providedsubstantial support for the study. Ordinarily, substantialsupport will mean providing 50 percent or more of the cost ofthe study.
Page 7
(a) For each investigation identified in response toquestion 3 (c): if the investigation was carried outunder an IND, was the applicant identified on the FDA1571 as the sponsor?
Investigation #1
IND # 31-931 YES / ~/ NO / / Explain:
Investigation #2
IND # YES / / NO / / Explain:
(b) For each investigation not carried out under an IND orfor which the applicant was .not identified as thesponsor, did the applicant certify that it or theapplicant i s predecessor in interest providedsubstantial support for the study?
Investigation #1
YES / __I Explain NO / __I Explain
Investigation #2
YES / / Explain NO / / Explain
Page 8

(c) Notwithstanding an answer of "yes" to (a) or (b), are. there other reasons to believe that the applicantshould not be credited with having "conducted orsponsored" the study? (Purchased studies may not beused as the basis for exclusivity. However, if allrights to the drug are purchased (not just studies onthe drug), the applicant may be considered to havesponsored or conducted the studies sponsored orconducted by its predecessor in interest.)
YES /__/ NO /~/
If yes, explain:
Steven D. Hardeman, R. Ph. 3-21-02
Signature of PreparerTitle: Senior Regulatory Proj ect Manager
Date
Page 9

---------------------------------------------------------------------------------------------------------------------This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.---------------------------------------------------------------------------------------------------------------------/s/
Steve Hardeman3/21/02 11:45:06 AMSigned for Dr. Katz
...,è'~ ".V1:.
( -l~~~,::~t-DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Serviæ
Food and Drug AdministrationRockvile, MD 20857
NDA 20-272\S-008NDA 20-588\S-004
Johnson & Johnson Pharmaceutical Research & Development L.L.CAttention: Susan J. MerchantManager, Regulatory Affairs1125 Trenton-Harbourton RoadTitusvile, New Jersey 08560-0200
Dear Ms. Merchant:
We acknowledge receipt of your April 22, 2002 submission containing final printed labeling inresponse to our March 3, 2002 letter approving your supplemental new drug applications forRisperdal(I (risperidone) Tablets and Oral Solution.
We have reviewed the labeling that you submitted in accordance with our March 3, 2002 letterand we find it acceptable.
However, we note that under CLINICAL TRILS section, "short-term efficacy" subheading ismissing and it needs to be added at the next printing.
If you have any questions, call Ms. Melaine Shin R.Ph., Regulatory Management Officer, at 301-594-5793.
Sincerely,
(See appended electronic signature page)
Russell Katz, M.D.DirectorDivision of Neuropharmacological Drug ProductsOffice of Drug Evaluation ODE ICenter for Drug Evaluation and Research

This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.
/s/Russell Katz1/14/03 08: 50: 41 AM

Division of Neuropharmacological Drug Products
REGULATORY PROJECT MANAGER REVIEW
Application Number: NDA 20-272/SE8-008NDA 20-588/SE8-004
Name of Drug: RisperdalCI (risperidone) Tablets and Oral Solution
Applicant: Johnson & Johnson Pharmaceutical Research & Development L.L.C.
Material Reviewed:
· NDA 20-272/SE8-008 (FA): April 22, 2002· NDA 20-588/SE8-004 (FA): April 22, 2002· AP letter based on submitted labeling text: March 3,2002
Baclmround and Summary:
NDA 20-272/S-008 and NDA 20-588/S-004 were approved on March 3, 2002 whichincorporated the addition of safety and efficacy information in the long-term treatment ofschizophrenia. The sponsor submitted the FPL on April 22, 2002.
Review:
1. Under CLINICAL TRILS section, subsection heading "short-term effcacy" is missing.
2. Under STORAGE AND HANDLING section, the following were added:
7503220Ds Patent 4,804,663February 2002~J anssen 2000
RISPERDALCI tablets are manufactured by:JOLLC, Gurabo, Puerto Rico orJanssen-Cilag, SpA, Latina, Italy
RISPERDALCI oral solution is manufactured by:Janssen Pharmaceutica N.V,Beerse, Belgium

NDA 20-272/S-008 & NDA 20-588/S-004 page 2
RISPERDALQD tablets and oral solution are distributed by:Janssen Pharmaceutica Products, L.P.Titusvile, NJ 08560
Conclusions:
Upon discussion with the Clinical Team Leader, Dr. Thomas Laughren, I recommend that weissue an Acknowledge & Retain letter and ask the sponsor to provide the corrected version(addition of "short-term efficacy" subheading) ofFPL at the next printing.
Melaine Shin, RPh.Regulatory Management Officer
Robbin Nighswander, R.Ph.Supervisory Regulatory Health Project Manager

This is a representation of an electronic record that was signed electronically andthis page is the manifestation of the electronic signature.-------------------------------------------------------------------------------------------------------~-------------/s/
Melaine Shin12/19/02 11:26:52 AMCSO
Robbin Nighswander1/2/03 10: 22: 56 AMCSO

/'''-~~ .øl,:::ir- DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
Food and Drug AdministrationRockville, MD 20857
NDA 20-272
Janssen Research FoundationAttention: EDWARD G. BRANN1125 TRNTON-HARBOURTON ROADP.O.Box 200
TITUSVILLE, NJ 08560
Dear MR. BRANN:
We refer to your new drug application (NDA) submitted under section 505(b) of theFederal Food, Drug, and Cosmetic Act for RiSPERDAL (RISPERIDONE) TABLETS. .
We have received your submission of May 11, 2000, reporting on your postmarketingstudy commitment to assess the long-term safety and efficacy of risperidone.
We conclude that study RIS-USA-79, entitled "A Comparison of Risperidone andHaloperidol for Prevention of Relapse in Subjects with Schizophrenia and
Schizoaffective Disorders" fulfills the above postmarketing study commitment.
This completes all of your postmarketing study commitments acknowledged in our letterof December 29, 1993.
We encourage you to propose labeling changes based on the results of study RIS- USA -79in a prior approval NDA supplement.
If you have any questions, call Steven D. Hardeman, RPh., Senior Regulatory ProjectManager, at (301) 594-5525.
Sincerely,
RUSSELL KATZ, M.D.
DIRECTOR
DIVISON OF NEUROPHARMACOLOGICAL
DRUG PRODUCTS
OFFICE OF DRUG Ev ALUA nON I
CENTER FOR DRUG Ev ALUA nON AND RESEARCH
/s/Russell Katz3/28/01 03: 25: 34 PM