Navigation Systems for Ablation
7
Navigation Systems for Ablation Bradford J. Wood, MD, Jochen Kruecker, PhD, Nadine Abi-Jaoudeh, MD, Julia K. Locklin, RN, MSc, Elliot Levy, MD, Sheng Xu, PhD, Luigi Solbiati, MD, Ankur Kapoor, PhD, Hayet Amalou, MD, and Aradhana M. Venkatesan, MD Navigation systems, devices, and intraprocedural software are changing the way interventional oncology is practiced. Before the development of precision navigation tools integrated with imaging systems, thermal ablation of hard-to- image lesions was highly dependent on operator experience, spatial skills, and estimation of positron emission tomography–avid or arterial-phase targets. Numerous navigation systems for ablation bring the opportunity for standardization and accuracy that extends the operator’s ability to use imaging feedback during procedures. In this report, existing systems and techniques are reviewed and specific clinical applications for ablation are discussed to better define how these novel technologies address specific clinical needs and fit into clinical practice. J Vasc Interv Radiol 2010; 21:S257–S263 Abbreviations: EM electromagnetic, PET positron emission tomography, RF radiofrequency, 3D three-dimensional, 2D two-dimensional IMAGE guidance and minimally inva- sive approaches have revolutionized the management of cancer. However, diagnosis and therapy remain dis- tinctly separate from each other in terms of time and space. For thermal ablation of cancer, this gap between diagnosis and therapy can be nar- rowed by the application of novel guidance technologies during the ab- lation procedure. “Medical global po- sitioning system” (or multimodality fusion-guided intervention) is enabled by electromagnetic (EM) tracking, and lets the physician navigate within a volume of imaging data (1–4). In this way, the precise spatial imaging infor- mation may be used when it is needed most, during the ablation procedure. Ablations may be facilitated by real- time updated information regarding the localization of needle, ultrasound (US) plane, and neoplastic target tis- sue margin during a composite abla- tion. Arterially enhancing hepatomas or tumors that are FDG-avid on positron emission tomography (PET) may be precisely localized and tar- geted during a multimodality ablation with “smart” needles and “smart” US that integrates arterial-phase com- puted tomography (CT), magnetic res- onance (MR) imaging, or PET data (5). A treatment plan can be implemented and adjusted during the procedure by using these accessory tools that aug- ment standard imaging (6 –11). During the same ablation session, tissue at risk for undertreatment can be identified, localized, targeted, and ablated, in- stead of waiting months for the resid- ual tumor to grow and be identified, at which time it might prove geometri- cally unfavorable for local therapy. Optimization of imaging-based navi- gation technologies will be key to es- tablishing the interventional radiology suite as the home for the operating room of the future and as the best location to deliver minimally invasive, image- guided local and regional oncologic therapies. The opportunity is ours to truly bring all the imaging information to the patient during ablation. BACKGROUND The skills of interventional radiolo- gists have recently been enhanced by navigation technologies with inter- faces similar to video games. Image- based navigation technology closes the natural gap between radiologic di- agnosis and therapy. Interventional oncology and interventional radiology outcomes are highly dependent on the accuracy of needles, catheters, and de- vices; navigation tools can help guide these devices with precision. Guid- ance technology for interventional radiology procedures is constantly evolving. Interventional radiologists rely on sophisticated manual skills (and on occasion, mental referencing of spatial information not available during procedures) to manipulate de- vices toward sometimes nebulous tar- gets. Navigation technology can en- From the Department of Radiology and Imaging Sciences (B.J.W., N.A.J., J.K.L., E.L., A.K., H.A., A.V.), Clinical Center, National Institutes of Health, 9000 Rockville Pike, Building 10, Room 1C341 MSC 1182, Bethesda, MD 20892; Philips Research North America (J.K., S.X.), Briarcliff Manor, New York; and Department of Diagnostic Imaging (L.S.), General Hospital of Busto Arsizio, Busto Arsizio, Italy. Re- ceived April 28, 2009; final revision received May 14, 2010; accepted May 17, 2010. Address correspon- dence to B.J.W.; E-mail: [email protected] This work was partially supported by the National Institutes of Health (NIH) Intramural Research Pro- gram and NIH Cooperative Research and Develop- ment Agreement 01864 with Philips Healthcare (Eindhoven, The Netherlands). B.J.W., J.K., S.X., and NIH have intellectual property in the field. B.J.W. is negotiating a Cooperative Research and Develop- ment Agreement with Biosound/Esaote (Indianap- olis, Indiana and Genoa, Italy). None of the other authors have identified a conflict of interest. © SIR, 2010 DOI: 10.1016/j.jvir.2010.05.003 S257
-
Upload
aradhana-m -
Category
Documents
-
view
218 -
download
2
Transcript of Navigation Systems for Ablation

Navigation Systems for AblationBradford J. Wood, MD, Jochen Kruecker, PhD, Nadine Abi-Jaoudeh, MD, Julia K. Locklin, RN, MSc,
Elliot Levy, MD, Sheng Xu, PhD, Luigi Solbiati, MD, Ankur Kapoor, PhD, Hayet Amalou, MD, andAradhana M. Venkatesan, MD
Navigation systems, devices, and intraprocedural software are changing the way interventional oncology is practiced.Before the development of precision navigation tools integrated with imaging systems, thermal ablation of hard-to-image lesions was highly dependent on operator experience, spatial skills, and estimation of positron emissiontomography–avid or arterial-phase targets. Numerous navigation systems for ablation bring the opportunity forstandardization and accuracy that extends the operator’s ability to use imaging feedback during procedures. In thisreport, existing systems and techniques are reviewed and specific clinical applications for ablation are discussed tobetter define how these novel technologies address specific clinical needs and fit into clinical practice.
J Vasc Interv Radiol 2010; 21:S257–S263
Abbreviations: EM � electromagnetic, PET � positron emission tomography, RF � radiofrequency, 3D � three-dimensional, 2D � two-dimensional
IMAGE guidance and minimally inva-sive approaches have revolutionizedthe management of cancer. However,diagnosis and therapy remain dis-tinctly separate from each other interms of time and space. For thermalablation of cancer, this gap betweendiagnosis and therapy can be nar-rowed by the application of novelguidance technologies during the ab-lation procedure. “Medical global po-
From the Department of Radiology and ImagingSciences (B.J.W., N.A.J., J.K.L., E.L., A.K., H.A.,A.V.), Clinical Center, National Institutes of Health,9000 Rockville Pike, Building 10, Room 1C341 MSC1182, Bethesda, MD 20892; Philips Research NorthAmerica (J.K., S.X.), Briarcliff Manor, New York; andDepartment of Diagnostic Imaging (L.S.), GeneralHospital of Busto Arsizio, Busto Arsizio, Italy. Re-ceived April 28, 2009; final revision received May 14,2010; accepted May 17, 2010. Address correspon-dence to B.J.W.; E-mail: [email protected]
This work was partially supported by the NationalInstitutes of Health (NIH) Intramural Research Pro-gram and NIH Cooperative Research and Develop-ment Agreement 01864 with Philips Healthcare(Eindhoven, The Netherlands). B.J.W., J.K., S.X., andNIH have intellectual property in the field. B.J.W. isnegotiating a Cooperative Research and Develop-ment Agreement with Biosound/Esaote (Indianap-olis, Indiana and Genoa, Italy). None of the otherauthors have identified a conflict of interest.
© SIR, 2010
DOI: 10.1016/j.jvir.2010.05.003
sitioning system” (or multimodalityfusion-guided intervention) is enabledby electromagnetic (EM) tracking, andlets the physician navigate within avolume of imaging data (1–4). In thisway, the precise spatial imaging infor-mation may be used when it is neededmost, during the ablation procedure.Ablations may be facilitated by real-time updated information regardingthe localization of needle, ultrasound(US) plane, and neoplastic target tis-sue margin during a composite abla-tion. Arterially enhancing hepatomasor tumors that are FDG-avid onpositron emission tomography (PET)may be precisely localized and tar-geted during a multimodality ablationwith “smart” needles and “smart” USthat integrates arterial-phase com-puted tomography (CT), magnetic res-onance (MR) imaging, or PET data (5).A treatment plan can be implementedand adjusted during the procedure byusing these accessory tools that aug-ment standard imaging (6–11). Duringthe same ablation session, tissue at riskfor undertreatment can be identified,localized, targeted, and ablated, in-stead of waiting months for the resid-ual tumor to grow and be identified, atwhich time it might prove geometri-cally unfavorable for local therapy.
Optimization of imaging-based navi-gation technologies will be key to es-tablishing the interventional radiologysuite as the home for the operating roomof the future and as the best location todeliver minimally invasive, image-guided local and regional oncologictherapies. The opportunity is ours totruly bring all the imaging informationto the patient during ablation.
BACKGROUND
The skills of interventional radiolo-gists have recently been enhanced bynavigation technologies with inter-faces similar to video games. Image-based navigation technology closesthe natural gap between radiologic di-agnosis and therapy. Interventionaloncology and interventional radiologyoutcomes are highly dependent on theaccuracy of needles, catheters, and de-vices; navigation tools can help guidethese devices with precision. Guid-ance technology for interventionalradiology procedures is constantlyevolving. Interventional radiologistsrely on sophisticated manual skills(and on occasion, mental referencingof spatial information not availableduring procedures) to manipulate de-vices toward sometimes nebulous tar-
gets. Navigation technology can en-S257

S258 • Review of Navigation Systems for Ablation August 2010 JVIR
hance conventional interventionalradiologic techniques by allowing pre-acquired images to be used duringprocedures, with real-time referencingof smart devices enabled by trackingof needles, guide wires, and US trans-ducers to guide the physician’s hand.Rapid image processing technologiesenable real-time display of multipla-nar, fused images, with the potentialto improve lesion targeting. Complexspatial relations that used to be doneby the imagination is now done by thecomputer and available for viewingduring an ablation procedure.
Navigation tools include needle-based, catheter-based, and imaging-based technologies. The developmentof EM tracking of needle tips and UStransducers to facilitate multimodalityimage-guided tumor ablation may al-ter the paradigm for what is consid-ered standard-of-care ablation. It isnow possible to “chisel” a compositeablation piece by piece, guided byreal-time feedback relative to PET,MR, or arterial-phase CT data. Know-ing exact locations of tumors and en-abling accurate delivery of needle-based therapies should translate intoimproved outcomes for therapies thatrely on accuracy, such as thermal ab-lation (whether RF ablation, laser,cryoablation, or microwave). Multi-modality fusion guidance combinesthe strengths of each modality. For ex-ample, the spatial resolution of CT canbe combined with the temporal reso-lution and real-time feedback of USimaging (ie, CT is the eye, US is thehand). Metabolic and functional de-tails can be coregistered to anatomicand morphologic data, resulting in asystem that provides multimodalityfusion guidance. Sculpting a compos-ite ablation can be facilitated by theknowledge of where the needle (andtreatment zone) has been and wherethe needle still needs to go. Identifica-tion of tumor tissue at risk for under-treatment is enabled by the spatialknowledge provided by tracking. In-terventional oncology and interven-tional radiologic outcomes are highlydependent on the accuracy of needle,catheter, and device position and loca-tion. Navigation systems help guidethese tools to where they need to be,based on real-time spatial feedback, in
relation to imaging data.IMAGE FUSION-GUIDEDPROCEDURES
Image coregistration is the joiningof two imaging datasets (rigid whereonly translation and rotation are per-formed or elastic where some local-ized stretching is performed for imagecorrespondence) (12), whereas imagefusion is the concurrent display ofthose datasets. Fusion may be accom-panied by an image overlay display,or by real-time updating of two ormore image data sets (or modalities)based on location of a device such as aneedle or a US transducer. Fusion dis-play techniques became widespreadfor diagnostic applications with PET/CT, but image fusion in interventionalradiology had remained only a theo-retical tool until recently. Fusion al-lows interactive multimodality target-ing by placing sensor coils on or insidebiopsy and ablation needles, US trans-ducers, guide wires, stent-grafts, cathe-ters, scalpels, steerable endoscopes, andon the patient’s skin. In the case of tu-mor ablation, the sensors are often lo-cated in a guiding needle or cannula, aswell as in or fixed to the US transduceritself. This enables the US transducer toact as a standard US, as well as a mul-tiplanar reconstruction plane selectiondevice, displaying the matching imag-ing plane of a previously obtained im-age data set (eg, on a different modalityor the same modality, but in a differentphase).
MEDICAL GLOBALPOSITIONING SYSTEMTECHNOLOGY: OPTICALVERSUS EM TRACKING
Optical tracking uses passive reflec-tors or active light emitters on deviceswithin view of a camera, instead ofsensor coils within differential mag-netic fields, as for EM tracking. Thesensor coils or reflectors are like theglobal positioning system device (orcar) and the EM field generator or in-frared camera is like the satellite. Thepresence of a coil in rapidly changingmagnetic fields elicits a weak electricalcurrent (by the Faraday law of electro-magnetic induction). Processing thiscurrent in the presence of the EM fieldgenerator can define a location withina Cartesian coordinate system (ie, XYZspace). The benefit of EM tracking (vs
optical) is that the device can resideout of sight and within the patient’sbody without erosion of signal. Thisrequirement for optical tracking istermed “line-of-sight,” and necessi-tates a clear and direct pathway for aphoton or infrared beam from camerato device (without intervening staff orbody parts). EM-enabled devices cantherefore reside deep within the bodyand still report their location. How-ever, EM tracking suffers in that theworking space is somewhat limited(approximately 40 � 40 cm to 70 �70cm), and there may be metallic artifactsfrom large metal objects such as tablesor x-ray sources or detectors, althoughmetal interactions have become lesserand lesser limitations in recent years as aresult of the evolution of tracking tech-nology. The EM field generator is typi-cally a flat plate under the patient or abrick-like device mounted near the pa-tient, and it must reside near the work-ing space of the patient for most EMapplications. Table 1 defines key termsfor tracking and navigation.
EM TRACKING HARDWAREAND SOFTWARE
Two major vendors manufacture theEM tracking equipment: Northern Digital(Waterloo, California) and AscensionTechnologies (Milton, Vermont). Multi-ple vendors have EM tracking solutionsfor percutaneous procedures with vary-ing degrees of complexity: PhilipsHealthcare (Eindhoven, The Nether-lands), Siemens (Erlangen, Germany),GE Healthcare (Milwaukee, Wisconsin),Veran Medical (St. Louis, Missouri), Es-aote (Indianapolis, Indiana), Civco (Ka-lona, Iowa), Hitachi (Twinsburg, Ohio),Sentinelle (Toronto, Ontario, Canada),and Ultrasonix (Richmond, British Co-lumbia, Canada), Traxtal (Toronto, Can-ada). Systems developed for surgicalprocedures can also be customized forpercutaneous ablation (Medtronic [Min-neapolis, Minnesota] and GE MedicalSystems).
The location of EM field generator,PC or cart, monitor, and skin patchsensors should be well planned outand rehearsed before initial use. TheEM tracking sensor hardware is oftenwithin a needle tip, within a guidewire tip, clipped to a US transducer, orwithin a soft foam adhesive skin patch(for semiautomatic detection and reg-istration). EM sensors are usually de-
scribed as having five or six degrees of
Wood et al • S259Volume 21 Number 8S
freedom, with the sixth degree (ifpresent) sensing rotation of the devicearound its main axis, primarily for USprobe tracking. The software enablesdisplay of the multimodality informa-tion. This is typically US plus CT orPET/CT for ablation or biopsy (or CTplus angiography for catheter-basedprocedures). Occasionally, data may
Table 1Glossary of Ablation Tracking Terms U
Term
Medical global positioning system Locfi
Multimodality fusion DisElectromagnetic tracking Me
wv
Target to registration error Difn
(Fiducial) registration error (orroot mean square)
Hon
Placement error A mDynamic reference Pat
wRegistration Ma
ered
Note.—2D � two-dimensional.
be displayed as preprocedural CT plus
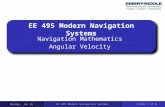
intraprocedural CT, as in the case ofan arterial-phase–enhancing hepato-cellular carcinoma that is conspicuousonly briefly during the arterial phaseof enhancement. In this case, the arte-rial-phase CT image outlines the loca-tion of the tumor, and this informationis superimposed on the unenhancedprocedural CT (Fig 1). Real-time US
in the Present Review
Definiti
ation of a device or image in relation to pgenerator is the satellite and the needle ti
y of multiple modalities; useful during pronism, based on electromagnetic field genein a 3D volume of imaging data (CT, MR,mence between the real and virtual needle ple position is displayed.ell the images or points match up (a meaguarantee for accuracy (ideally � 2 mm)
sure of the proximity of the needle to theor sensor placed on patient that corrects foout this, patient must remain in exact posiing colocalized images to images or image
(root mean square); rigid registration matration (elastic, warping) matches with flermation between different images or differ
(when tracked) can also select the
plane of the enhanced CT for display(ie, multiplanar reconstruction alongthe needle path).
STEPS AND WORKFLOW
The sequence of steps and eventswill be dictated by which modalityshows the tumor margin the best, as
Figure 1. Arterial-phase CT (a) show-ing earlier nonenhancing RF ablationtreatments and solitary enhancing hepa-tocellular carcinoma (arrow). Targetinginterface for placement of virtual needle(colored line intersection in b–d). Virtualneedle in target corresponds with actualneedle on CT scan (e).
rocedural imaging; “the electromagneticthe car”uresr, to locate a needle (or US plane)T) or locate a 2D US plane within 3D
ions. A measure of how exact the
e of registration quality); necessary, but
nt targetatient or generator motion or breathing;nace to “magnetic space”; registrationes uses fixed images versus deformablele images, accounting for organ shift or
times
sed
on
aliz repeld p ispla cedcha ratoith PE
olufere ositeedw w surot aea poi
ch r pith tio
tch sprror tchgis xib
efo ent
well as operator preferences and pat-

played, as well as a view down the needle shaft (lower left).
* Optional steps.
S260 • Review of Navigation Systems for Ablation August 2010 JVIR
terns of CT and US use for biopsy andablation. Table 2 shows one of themore common workflows for CT andUS guidance. The steps may differ ifone is registering with automatic skinpatches, or if one is using manual reg-istration with anatomic points (ie,landmarks) or scan-plane matching(umbilicus or nipples). The umbilicusor nipple level provides rough align-ment and the matched anatomicpoints provide fine tuning. Specificpoint matching in the liver often in-volves selecting anatomic registrationpoints along the porta hepatis oridentifiable shapes from vesselbranching points. Automated regis-tration methods further simplify theprocess. The role for verification CTor US is also procedure-dependent.Navigation tools are usually for aug-mentation, and often supplement, in-stead of replace, standard imagingguidance techniques. If using a dy-namic reference sensor or patch, onecan move the field generator box andthe patient without altering the reg-istration. If not using this specialsensor on the skin, one must main-tain the patient and field generatorimmobile during the procedure andreposition the CT table to the sameworking spot (and record the Z-axistable number). Staff should be
ct)
on less mobile ribs or sternum)ting towards needle entry and target
skin patch � grid –
s then fine tune by matching anatomicdiaphragm)
level of breathing with image or gatingfeedback
dle insertion or repositioning
Figure 2. Patient with recurrent tumor and multiple recent nondiagnostic CT-guidedbiopsies. Graphical user interface showing metabolic activity (blue dots) on PET scantargeted with navigation to sample viable part of tumor. PET data was registered toprocedural multiplanar reconstructed CT and procedural US for real-time feedback.Virtual needle represented by blue line. Multiplanar/multimodality navigation is dis-
Table 2Steps and Workflow for CT- and US-guided Ablation and/or Biopsy
Step Procedure
1 Confirm software and hardware set up and data transfer path (via PACS or dire2 Plan and identify target and margin3 Choose combination of modalities for image guidance4 Position patient, screening US for region of access � skin entry point5 Wide sterile prep of skin6* (� sterile CT opaque grid)/(� place registration patches near target, preferably7 Drape electromagnetic field generator box and position near working space poin8* � Procedural CT of region with breath hold at same level as during procedure �9 Send or retrieve and load CT images in navigation system
10 Semiautomatic registration with patches versus rough registration with umbilicupoints or landmarks on US and CT (correlate specific vein shapes or porta or
11 Secure cables and cords12 Confirm adequacy of registration at skin (verify left–right and cranial–caudal)13* Select skin entry point14 Mark target(s) and margin(s) on navigation system15 Reproduce breathing level and choose needle angle to target16* Verify target with ultrasound or CT during insertion (as needed); can also verify17 Insert tracked needle, adjusting angle along way to target based upon navigation18 If composite ablation, redefine target (as undertreated tissue) for subsequent nee
Note.—PACS � picture archiving and communication system.
alerted to avoid dislodging the field

Wood et al • S261Volume 21 Number 8S
generator and to exercise cautionwith regard to sterility.
For PET or MR guidance, select theappropriate MR sequence or attenua-tion-corrected PET. For PET guidance,manually register earlier CT (fromPET/CT) to intraprocedural planningCT with the use of anatomic points (ie,bones and landmarks) and then blendin PET data and fade the display be-tween PET (or MR), US, and CT asneeded (Fig 2). Keep in mind positionand breathing differences, as PET im-ages are usually acquired during shal-low respiration. There is a wide vari-ety of practice patterns that canaccommodate tracking (Table 3).
ROTATIONALANGIOGRAPHY-BASEDTOOLS
Cone-beam CT is the creation of a“CT-like” image with a 23- or 46-cmfield of view from an angiography ma-chine after rotation of the C-armaround the patient. Dyna-CT (SiemensMedical Solutions, Erlangen Ger-many), Innova-CT (GE Healthcare),
Table 3Methods for Tracking during Ablation
Procedure
1 Needle tracking: track ablatioshaft or hub
2 US tracking: sensor attached3 Ablation needle can be placed
coaxially after removing a tplaced before the actual ab
4 Registration is manual or semlandmarks, umbilicus, nipp
Table 4When to Use Tracking during Ablation
Lesions seen only on arterial phaseLesion margins seen best on MR imagingLesions best identified with PET/CTLocalizing specific part of tumor for biopLesions not seen at all on USComposite ablations requiring multiple n
difficult treatment planLocalization of tumor tissue at risk for in
treatmentIdentification of safest pathway, given coDome lesionsLesions under ribsDuring “gas out” from tissue cooking
and Xper-CT (Philips Healthcare) are
three such commercially available sys-tems. This method then enables cone-beam CT guidance, whereby targetsand needle pathways are plannedwith this CT-like volumetric informa-tion (X-per guide [Philips Healthcare],I-guide and I-Guide Cappa [Siemens],or Innova CT [GE Medical Systems]).Dynamic three-dimensional (3D) road-mapping can provide reference toprevious image volumes such as CTangiography or rotational angiogra-phy/CT. The next generation of inter-ventional radiology suites also inte-grate methods for 3D navigationwith tracking systems referencingmultiple modalities or by enablingspatial information with what wasonce only a two-dimensional (2D)modality (ie, x-ray or US). Althoughthe systems each have different soft-ware and display formats, the con-cept remains the same: providing 3Dimaging capabilities and informationin the interventional radiology suitein the hopes of improving or facili-tating needle, catheter, wire, or de-vice placement.
For cone-beam CT guidance, con-
escription
eedle itself internally (“tip tracking”) on
r embedded in transducerndem to tracked guide needle orked stylet or tracked outer cannula,on needletomated: matching skin points, imaging
, or test simple image overlay
Biopsy
quence
(only part of tumor “hot” on PET)
le insertions, complex geometries or
ficient heating near the end of a
lex angle of insertion
ventional orthogonal 2D fluoroscopy
images are referenced to the rotationalangiography or cone-beam CT frame-work to provide guidance for needle-based procedures such as ablation, bi-opsy, or vertebroplasty. A skin entryand target define a pathway chosen onthe CT-like image from the cone-beamCT. The needle advancement is moni-tored incrementally in the view 90°orthogonal to the needle or axial to theneedle (ie, down the needle shaft or“bird’s eye” view). Each orthogonalviewpoint has the selected pathwaysuperimposed on the fluoroscopic im-age, so needle adjustments can bemade by comparing actual the needleto the superimposed planned path-way.
MECHANICAL LASERPOINTERS AND NEEDLESTABILIZATION DEVICES
Various commercial devices existfor needle stabilization and angle se-lection including disposable bubblelevelers with protractor-like needleguides (InRad, Kentwood, Michigan),disposable adhesive arcs that stabilizethe needle (Neo-Rad, Oslo, Norway;and AprioMed [Uppsala, Sweden, andLondonderry, New Hampshire]) andautomated laser pointers that integratewith the CT table (Neo-Rad) or inte-grate directly with the CT software(National Institutes of Health, Be-thesda, Maryland; and Philips Health-care). Many of these solutions are low-cost devices to facilitate needleplacement accuracy, which can be acritical determinant of outcome afterablation. Needle stabilization can alsobe important when heavy ablation de-vices are subjected to gravity, floppingdown during a CT in a lateral ap-proach.
CLINICALOUTCOMES/PATIENTIMPACT
The accuracy, clinical utility, andimpact on patient outcomes is becom-ing better defined for EM tracking andmultimodality image fusion for guid-ance of biopsy and thermal ablationprocedures. Many procedures are en-abled by the technology, such that tar-gets would not have been definedwithout the ability to use arterial-phase CT or PET or MR information
D
n n
to ota
raclatiiaules
or
se
sy
eed
suf
mp
during the procedure. Specifically, for

S262 • Review of Navigation Systems for Ablation August 2010 JVIR
biopsy and ablation, tracking can im-prove accuracy in terms of angle selec-tion toward a predetermined pointtarget (6), and there may be advan-tages in terms of delivering a pre-scribed treatment plan or adding to-gether multiple individual ablations tofully envelop a tumor with a compos-ite ablation (ie, multiple overlappingablation volumes).
CLINICAL USE OF EMTRACKING FOR BIOPSY ANDABLATION
It is important to keep in mind thatsome systems will track the needle tipwhereas others will track the shaft orhub. Tracking the needle tip could the-oretically better account for tip deflec-tion or bending, organ deformation, ororgan motion.
US can be tracked with or without atracked needle. If US is used alonewithout a tracked needle, one mustlook for needle images on US to refer-ence the actual needle to the targetlocation or previous imaging modal-
Figure 3. Enhanced CT scans before (a)Treatment planning sequence (c–f) with stumor location (red), which was manuallya margin of normal tissue (f).
ity. Tracking the US and needle is
most useful for the concurrent displayof other modalities. There is a broadvariety of potential clinical indicationsfor the use of tracking during biopsyand ablation (Table 4).
FUTURE DIRECTIONS
Navigation techniques have ini-tially been applied to facilitate needleplacement toward a predefined target.Future work will refine integrated abla-tion treatment plans in a fashion similarto radiation therapy dose maps (Figs 2, 3).Such standardization should de-crease the variability of practice pat-terns, and even enable less experiencedoperators to deliver precise ablations.The registration process will becomefully automated with integrated elasticwarping, tissue deformation, andbreathing and motion compensation.The navigation systems will become in-creasingly integrated with the imagingsystems themselves (ie, embedded inthe US transducer, console, and angiog-raphy tables). This will in turn lead tobroader ease of use and streamlined
after (b) RF ablation with navigation shential overlapping of planned treatmentmented at the beginning of the procedure.
workflow. EM tracking treatment plans
will identify tissue at risk for undertreat-ment and incorporate imaging such asUS contrast, elastography, MR spectros-copy, and diffusion maps. PET-guidedablation will become a standard tool fordefining treatment margins, and theEM-tracked biopsy will become a toolfor drug discovery and personalizedmedicine, selecting and verifying molec-ular-targeted therapies. Trainees in in-terventional radiology will learn needleplacement skills on EM tracking simu-lators instead of patients.
CONCLUSIONS
The use of navigation technologyand multimodality image fusion rep-resents a novel and important meansby which to optimize image-guidedinterventions. Although speculative,improved imaging and navigationtools could potentially reduce proce-dure time, radiation dose, and compli-cations while enhancing standardi-zation. Interventional radiology as adiscipline is continuously finding newways to use its foundation in imaging
complete treatment of enhancing tumor.umes (green) superimposed on estimatede treatment volume covers the tumor plus
and owequ volseg Th
to improve what minimally invasive

Wood et al • S263Volume 21 Number 8S
physicians do. Navigation tools at thefingertips of the physician have thepotential to improve delivery of mini-mally invasive image-guided local andregional cancer therapies.
References1. Banovac F, Cheng P, Campos-Nanez E,
et al. Radiofrequency ablation of lungtumors in swine assisted by a naviga-tion device with preprocedural volu-metric planning. J Vasc Interv Radiol2010; 21:122–129.
2. Wood BJ, Locklin JK, Viswanathan A,et al. Technologies for guidance of ra-diofrequency ablation in the multimo-dality interventional suite of the future.J Vasc Interv Radiol 2007; 18:9–24.
3. Wood BJ, Zhang H, Durrani A, et al.Navigation with electromagnetic track-ing for interventional radiology proce-dures: a feasibility study. J Vasc Interv
Radiol 2005; 16:493–505.4. Yaniv Z, Wilson E, Lindisch D, ClearyK. Electromagnetic tracking in theclinical environment. Med Phys 2009;36:876–892.
5. Krucker J, Xu S, Glossop N, et al.Electromagnetic tracking for thermalablation and biopsy guidance: clinicalevaluation of spatial accuracy. J VascInterv Radiol 2007; 18:1141–1150.
6. Baegert C, Villard C, Schreck P, Soler L,Gangi A. Trajectory optimization forthe planning of percutaneous radiofre-quency ablation of hepatic tumors.Comput Aided Surg 2007; 12:82–90.
7. Banovac F, Abeledo H, Campos-NanezE, et al. An image-guided system foroptimized volumetric treatment plan-ning and execution for radiofrequencyablation of liver tumors. Int J ComputAssist Radiol Surg 2007; 2(Suppl 1):S146–S151.
8. Chen CR, Miga MI, Galloway RL.
Optimizing needle placement in treat-ment planning of radiofrequencyablation. Proc SPIE 2006; 6141.
9. Trovato K, Dalal S, Kruecker J, Ven-katesan A, Wood BJ. Automated RFAplanning for complete coverage oflarge tumors. Proc SPIE 2009; 7261.
10. Villard C, Soler L, Papier N, et al.RF-Sim: a treatment planning tool forradiogrequency ablation of hepatic tu-mors. In: Program and Abstracts fromthe Seventh International Conferenceon Information Visualization, 2003; pp.561–566.
11. Villard C, Soler L, Gangi A.Radiofrequency ablation of hepatic tu-mors: simulation, planning, and contri-bution of virtual reality and haptics.Comput Methods Biomech BiomedEng 2005; 8:215–227.
12. Crum WR, Hartkens T, Hill DL.Non-rigid image registration: theoryand practice. Br J Radiol 2004; 77
(Suppl):S140–S153.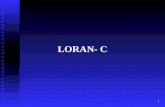










![Inertial Navigation Systems - Indico [Home]indico.ictp.it/event/a12180/session/23/contribution/14/material/0/... · Inertial Navigation Systems. Inertial Navigation Systems ... •](https://static.fdocuments.in/doc/165x107/5a94bdc87f8b9a451b8c1652/inertial-navigation-systems-indico-home-navigation-systems-inertial-navigation.jpg)