
National Cancer Institute Workshop on Advanced Technologies in Radiation Oncology December 1, 2006.
80
National Cancer Institute Workshop on Advanced Technologies in Radiation Oncology December 1, 2006
-
Upload
tyler-gibbs -
Category
Documents
-
view
219 -
download
4
Transcript of National Cancer Institute Workshop on Advanced Technologies in Radiation Oncology December 1, 2006.

National Cancer Institute
Workshop on Advanced Technologies in Radiation Oncology
December 1, 2006

Edward C. Halperin, M.D., M.A.
Dean of the School of MedicineFord Foundation Professor of Medical Education
Professor of Radiation Oncology, Pediatrics, and History
University of Louisville

The Club of Radiation Oncology DeansSamuel HellmanAllen LichterEdward Halperin

Active Membership = 1


I have therefore concurred with myself and can assure you that the following views represent the unanimous opinion of the active membership.

Charge per Dr. Vikram’s email of 8/17/06
Compare, in reference to toxicity and survival, for childhood cancer, radiotherapy with conformal v. stereotactic v. IM/IGRT v. proton, neutron, carbon ions, pions et al. techniques

OutlineIs the question(s) moot?Is the answer(s) self-evident?What questions didn’t Dr. Vikram ask that
he should have?What do the data show in reference to
the charge I have been given?What shall we do?

Is the question(s) moot?

ACGME Requirements in Radiation Oncology for Residency Training
“The clinical core curriculum shall include experience in . . . pediatric [tumors]. . . . Residents must treat no fewer than 12 pediatric patients [in 4 years of residency] of whom a minimum of 9 have solid tumors.”

On 10/12/06 there were 79 accredited radiation oncology residencies in the U.S. with 569 residents on duty or ~ 142/year.

An estimate of the number of pediatric radiation oncology patients per year in the U.S. available for residency training and, potentially, for investigation of radiation treatment modality

Total Number ofChildhood Cancer cases/year
X
% of the cancer type
X
% of the cases
Requiring
Radiotherapy
=
Total teaching cases/year

Total Teaching
cases/ Year
÷
Residents on Duty =
Teaching cases/
Residents/Year

….big assumptions:
No cases go to private practice.
Cases are uniformly distributed (Wills, St. Jude, MSKCC, CHOP, etc)

Example: ALL (CNS prophylaxis, testicular relapse, TBI)
124 cases/year ÷ 569 trainees = 0.2 cases/year/trainee
8600 cases/
yearX 18% X 8% =
124
cases/
year

So, in a 4-year residency, casting aside the problem of the “big assumptions,” our trainee will see 0.8 cases of the most common malignancy of childhood.

Diagnosis
Teaching cases/
year
Teaching cases/year/ Resident
Cases
in 4 years
ALL 124 0.2 1
ANLL 28 0.05 <1
Lymphoma 481 0.8 3
Medulloblastoma 232 0.4 2
Asrocytoma, including brain stem
348 0.6 2
Ependymoma 77 0.1 <1
Neuroblastoma 86 0.2 1
Retinoblastoma 103 0.2 1

Diagnosis
Teaching Cases/
year
Teaching Cases/year/
ResidentCases
Wilms 34 0.06 <1
Ewing 103 0.2 1
Rhabdomyosarcoma 103 0.2 1
NRSTS 52 0.09 <1
Hepatic Tumors 17 0.03 <1
Germ cell and trophoblastic neoplasms
26 0.04 <1
Epithelial neoplasms 23 0.04 <1

“The only thing I really want to know about pediatric radiotherapy after finishing this residency program is your phone number.”

“… if you want to lead, you have to adjust to the environment in which you find yourself. You cannot wait for it to adjust to you.”
J.L. Gaddis, describing Dean Acheson. New Republic, 10/16/06, p.28

Many people assert that the Watergate scandal demonstrates that a free press is essential to democracy. All forms of print and electronic press are pleased to take credit for this achievement.

It can be argued, however, that it wasn’t the press at large who broke the Watergate story, it was two Washington Post reporters: Woodward and Bernstein.

Similarly, we have all seen dramatic images used to promote IMRT/IGRT and proton therapy in childhood tumors. It would be wrong to promote this technology on the basis of, from a public health standpoint, a tiny number of cases.

It is disingenuous to show your hospital administrator proton dosimetry for treating childhood craniopharyngioma as a technique for getting him/her to buy protons for treating bone metastases.


Is the answer(s) self-evident?

“There is never any reason to give any dose to uninvolved normal tissue. An increase in dose to the tumor will, to a point, improve local control. Achieving these objectives is self-evidently true and does not require randomized prospective trials.”

After all, we didn’t require randomized trials to prove the benefits of _____________.
SimulatorsLinAc v. Co60

Maybe we should have.

“Change is inevitable. Progress is optional.”
A. Stern, quoted in Penn. Gaz., 11/12/2006, p. 54

Set the bar of proof higher when the price is higher.


The Aspirin Analogy

Of ~56 African countries, 64% have no radiotherapy facilities.
Lancet Oncol, 2004;5:695

In Africa in 2002, the supply of Co60
and linear accelerators was 18% of the estimated need.
Lancet Oncol 2006;7:584

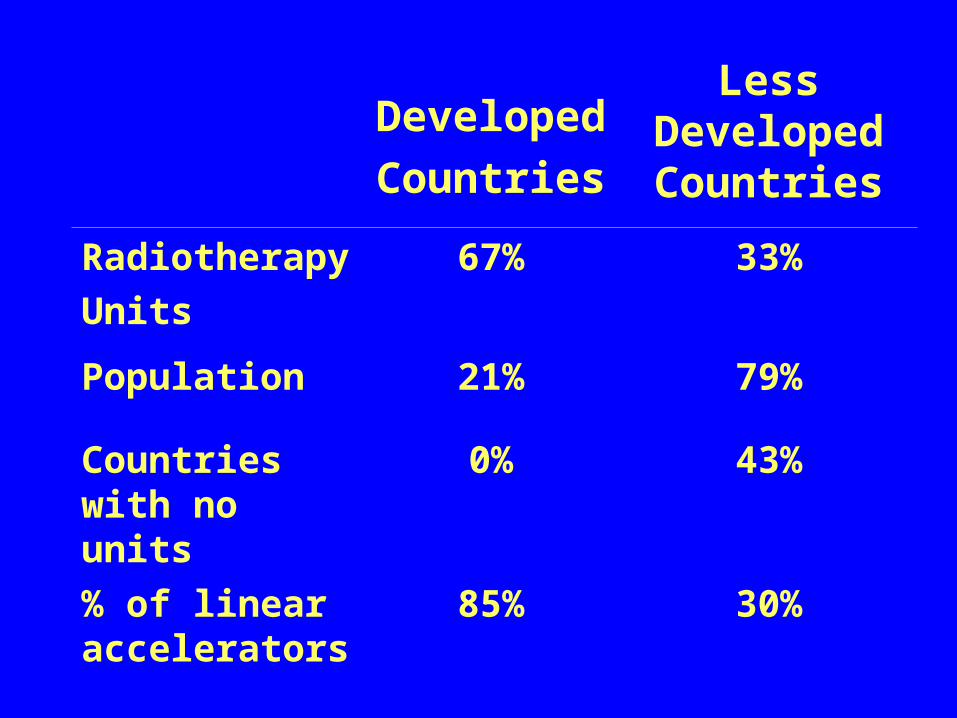
Developed
Countries
Less Developed Countries
Radiotherapy
Units
67% 33%
Population 21% 79%
Countries with no units
0% 43%
% of linear accelerators
85% 30%

Perhaps we should worry more about the provision of services to more of the world’s population, and less about inordinately expensive machines of unproven benefit for the wealthy?

“… in a world where more of the 100 largest economic entities are companies (52) than countries (48), a new set of rules will inevitably apply.”
Penn. Gaz., 11/12/2006, p. 54

Is the answer self-evident?

These are some sites/situations in which the target is such that it is nearly impossible to envision an improvement by new technology over standard techniques.
The target is the entire structure and, while IMRT/IGRT could be used to deal with tissue heterogeneity, that is likely to be “a long run for a short slide.” Also, with current technology IMRT may increase second malignant neoplasms.


TBIProphylactic cranial irradiationTesticular relapse radiotherapyWhole abdomen irradiation to 10 Gy

For some diseases the local control rate is dismal, few children live to suffer late effects, dose escalation has generally been fruitless, and high LET therapy has either been without benefit or made a bad situation worse.


Brain stem gliomaHigh grade supratentorial astrocytoma

For some diseases, the radiation dose is so low that it is hard to imagine a discernable benefitto technological innovation. (A better dose distribution does not equal a discernable benefit.)

Langerhans cell histiocytosis (4-6 Gy)Post-transplant lymphoproliferative disorder (4-8 Gy)Transplantation Aplastic anemia Fanconi’s anemia Sickle cell anemia Intentional induction of chimerism

What questions didn’t Dr. Vikram ask that he should have?

The untoward detriments of technological change

In childhood cancer the push to use IMRT, IGRT, protons, etc. (all external beam techniques) inhibits the prudent use of superior alternatives.


Plaques for retinoblastoma (<entire anlage)
I125Ruthenium
Intra-operative radiotherapyIntra-oral coneP32 for Askin and DSRBCT

The dose has to go somewhere; or the case of the pancytopenic pineal patient


What do the data show in reference to the charge I have been given?



Hearing loss for cisDDP treated patients receiving posterior fossa irradiation (at the price of endocrinopathy?)
Neuroendocrine, salivary gland, and TMJ injury in juvenile nasopharngeal angiofibroma and of nasopharngeal carcinoma and rhabdomyosarcoma


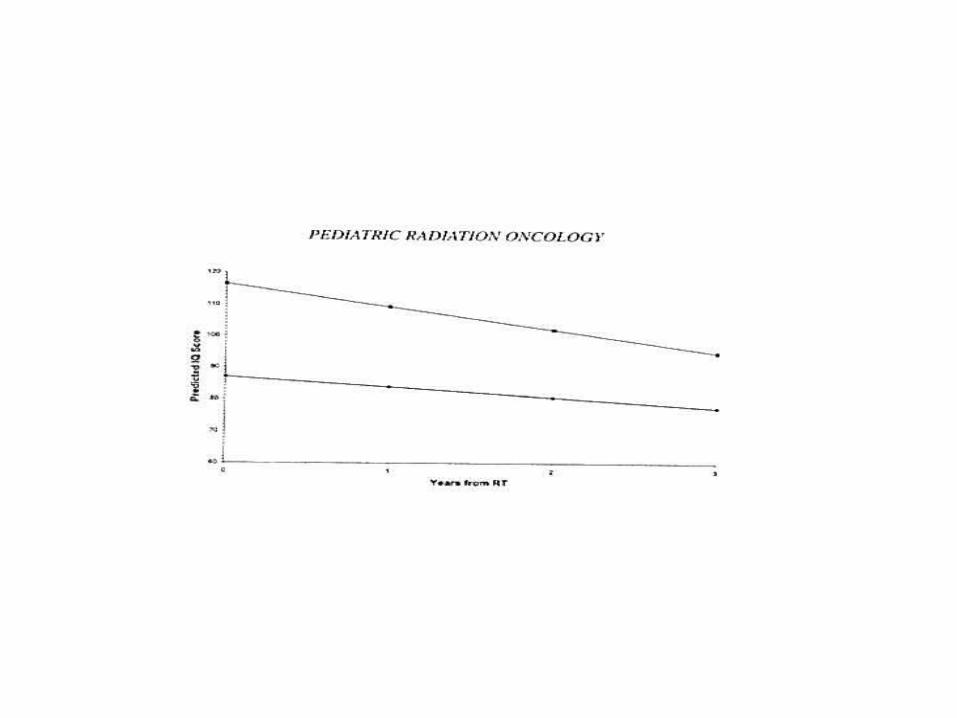
IQ loss in localized intracranial irradiation
Thyroid, cardiac, pulmonary, and GI injury in craniospinal irradiation
Sarcoma treatment








“[The] clinical benefits of technological advances [in radiotherapy] including image-guided radiotherapy, are challenging to describe. Randomised data for patients treated with and without image guidance is unlikely to ever exist.”
Dawson and Sharpe (PMH)
Lancet Oncol 2006;7:848

Adequate field placement is correlated with tumor control in pediatric
MedullablastomaEwing tumorHodgkin disease
IJROBP 1997;37:523

Halperin’s First Rule of Pediatric Radiotherapy:
“Most tumors are radioresistant if you miss them.”



To be tested…

Cardiac sparing WLIHepatic/renal parenchymal sparing WAI

What shall we do?
1. Re-engineering Linacs2. Forensic pathology3. Investing in late effects clinical research4. Dose escalation in ependymoma5. Invest in reasonably-priced radiotherapy
solutions in low-income countries6. Delete pediatrics from most radiotherapy
residency programs7. Establish late effects of childhood cancer fellowship training
Thank you.


















