
Myometrial Injection of Vasopressin
28
Verna Thomas, BSN, SRNA Myometrial Injection of Vasopressin
-
Upload
melvin-gray -
Category
Documents
-
view
33 -
download
0
description
Myometrial Injection of Vasopressin. Verna Thomas, BSN, SRNA. Objectives. Familiarize learner with myomectomy procedure and management options Describe anesthetic c onsiderations for myomectomy Identify purpose for use of vasopressin and mechanism of action - PowerPoint PPT Presentation
Transcript of Myometrial Injection of Vasopressin
Verna Thomas, BSN, SRNAVerna Thomas, BSN, SRNA
Myometrial Injection of Vasopressin
Myometrial Injection of Vasopressin
ObjectivesObjectives
• Familiarize learner with myomectomy procedure and management options
• Describe anesthetic considerations for myomectomy• Identify purpose for use of vasopressin and mechanism of
action• Recognize potential complications associated with use of
vasopressin • Engage the learner in a spirited discussion regarding a
case of myometrial vasopressin injection
• Familiarize learner with myomectomy procedure and management options
• Describe anesthetic considerations for myomectomy• Identify purpose for use of vasopressin and mechanism of
action• Recognize potential complications associated with use of
vasopressin • Engage the learner in a spirited discussion regarding a
case of myometrial vasopressin injection
3
Case of Interest• 29 y/o AA Female, • 67 kg• ASA 2, MP II• Employed RN• History of uterine fibroid, syncope at work,
received cardiac work-up, anemic• Robotic Assisted Laparoscopic
Myomectomy
4
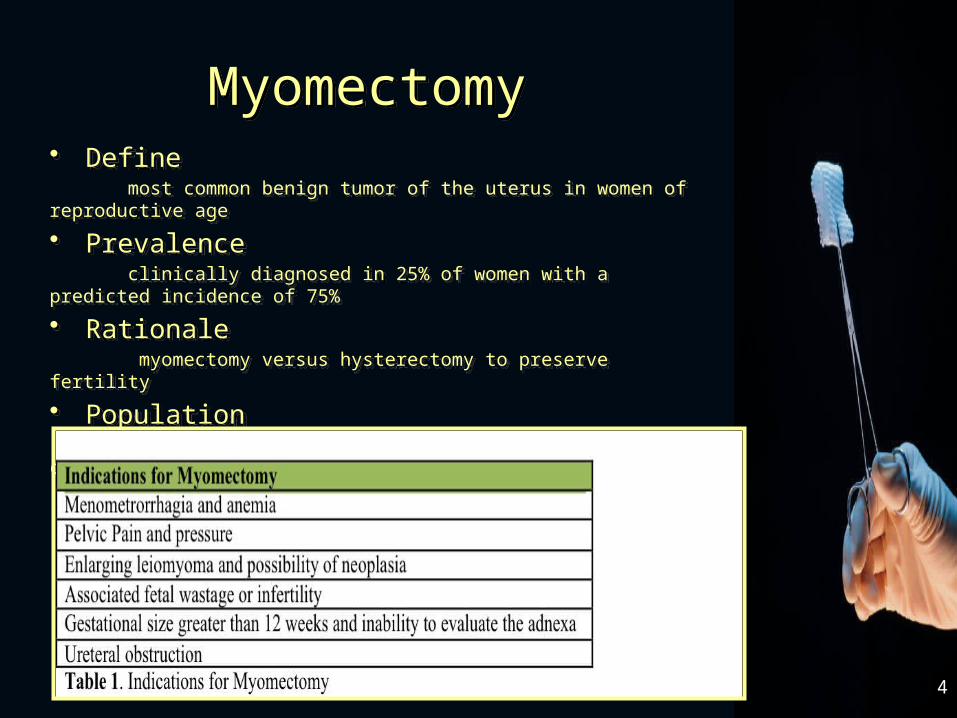
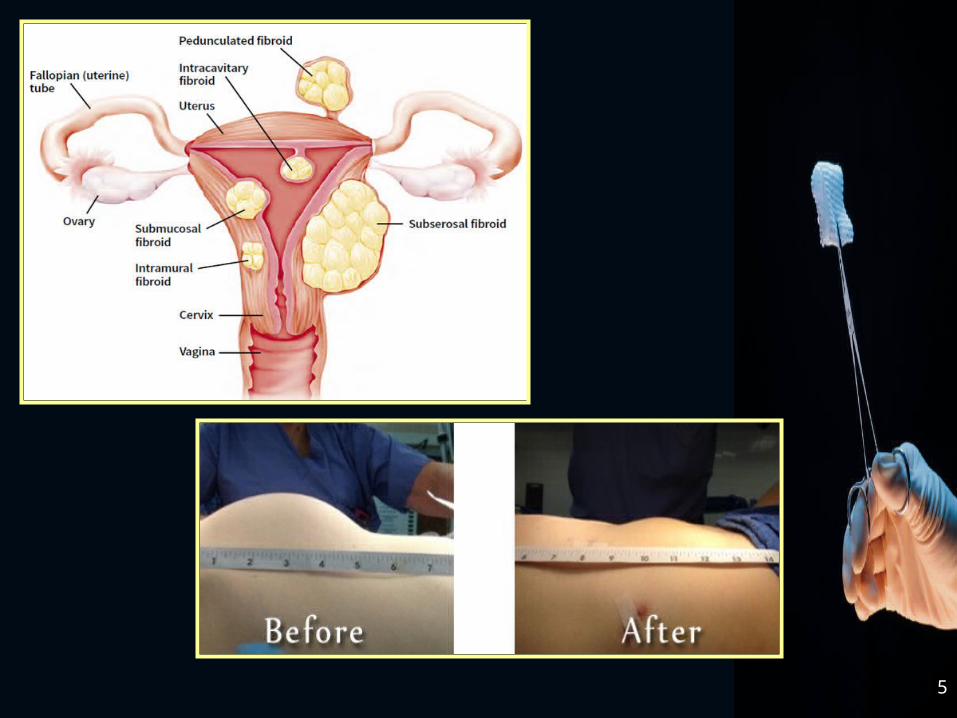
MyomectomyMyomectomy• Define most common benign tumor of the uterus in women of reproductive age
• Prevalence clinically diagnosed in 25% of women with a predicted incidence of 75%
• Rationale myomectomy versus hysterectomy to preserve fertility
• Population predominance amongst African American women of child-bearing age to ~
50y
• Define most common benign tumor of the uterus in women of reproductive age
• Prevalence clinically diagnosed in 25% of women with a predicted incidence of 75%
• Rationale myomectomy versus hysterectomy to preserve fertility
• Population predominance amongst African American women of child-bearing age to ~
50y
5
6
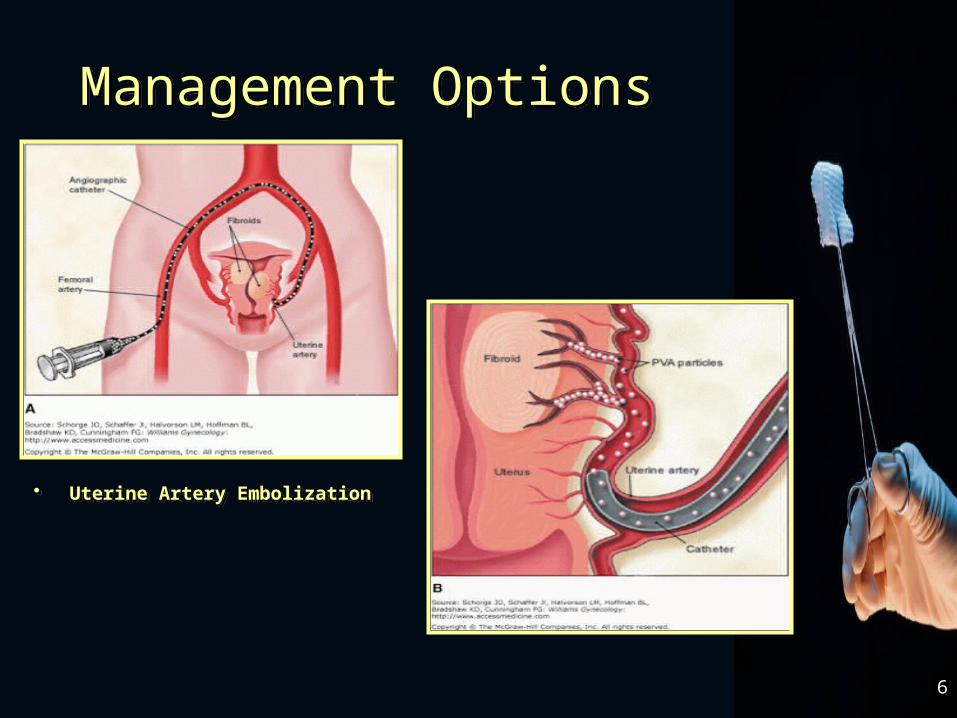
Management OptionsManagement Options
• Uterine Artery Embolization• Uterine Artery Embolization
7
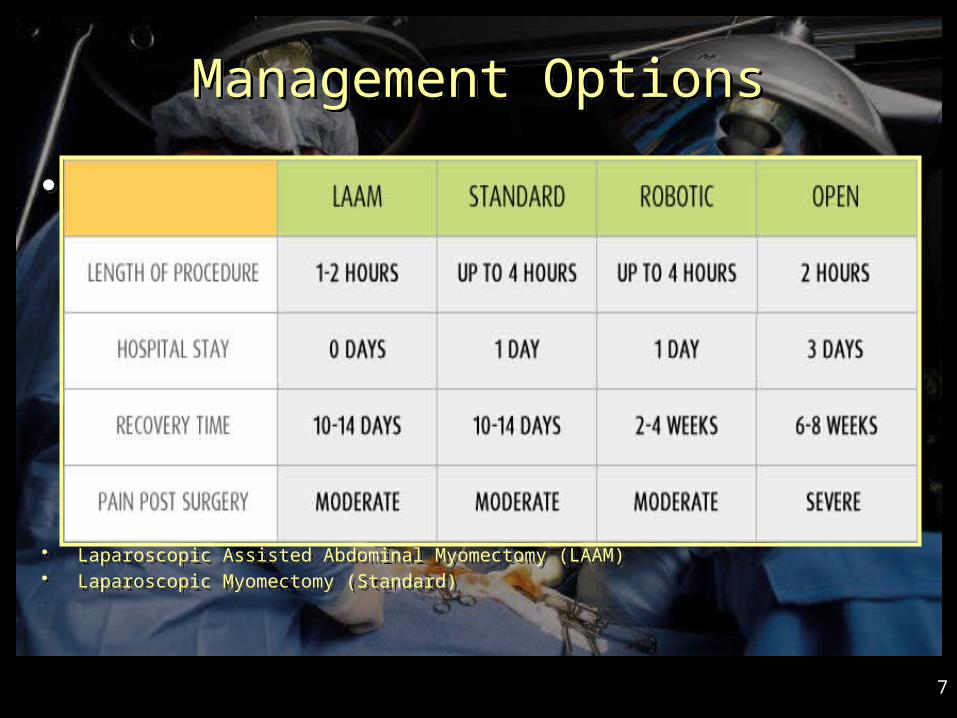
Management OptionsManagement Options
•
• Laparoscopic Assisted Abdominal Myomectomy (LAAM)• Laparoscopic Myomectomy (Standard)
•
• Laparoscopic Assisted Abdominal Myomectomy (LAAM)• Laparoscopic Myomectomy (Standard)
8
9
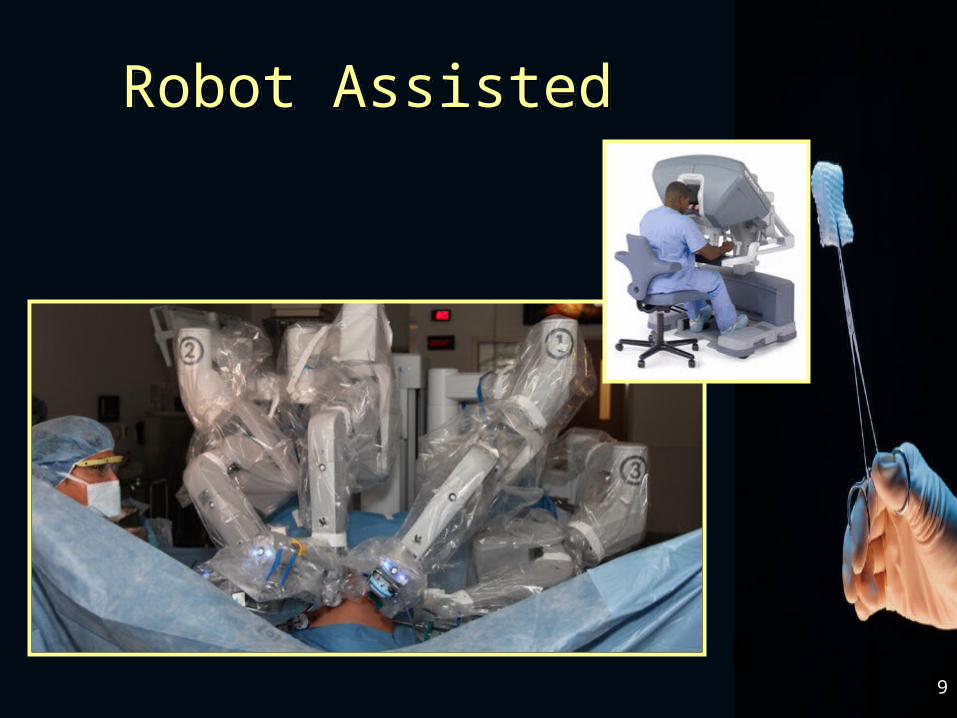
Robot AssistedRobot Assisted
10
Anesthesia ConsiderationsAnesthesia Considerations
• Bleeding• Hemodynamic Alteration• Respiratory Compromise• Positioning
• Bleeding• Hemodynamic Alteration• Respiratory Compromise• Positioning
11
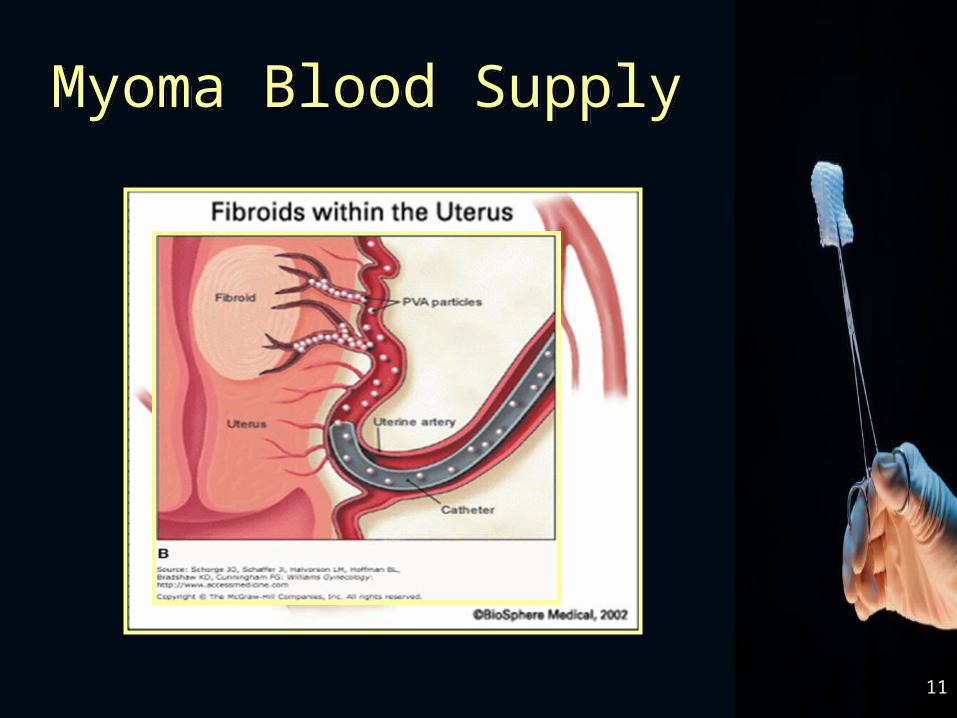
Myoma Blood SupplyMyoma Blood Supply
12
Case Update #1• Standard Induction• Trocars/Insufflation• Vasopressin Injection• Re-insufflation
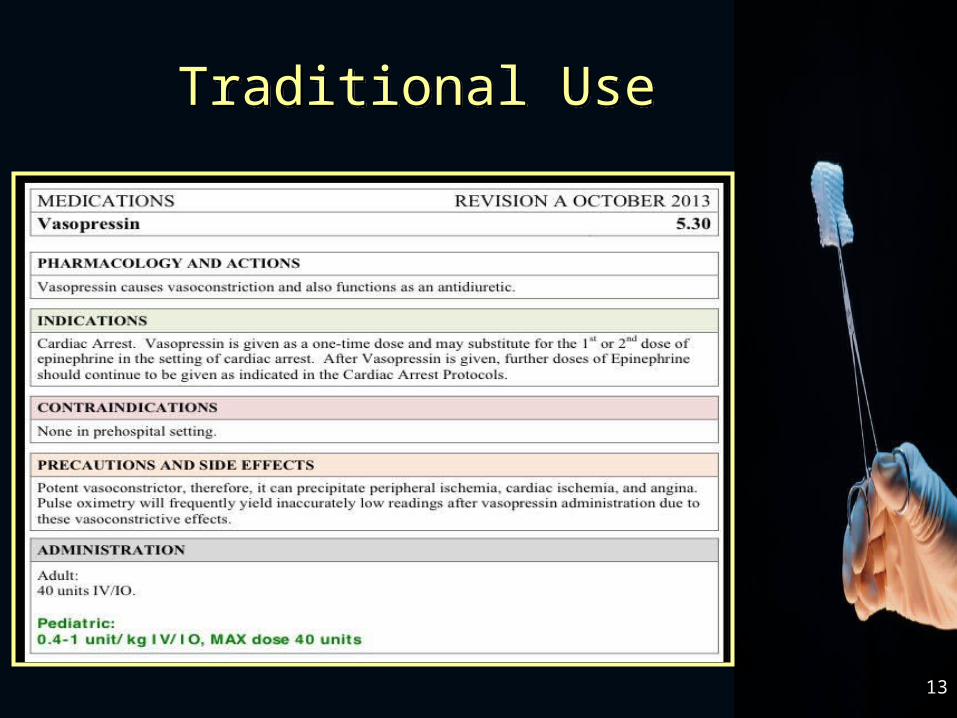
13
Traditional UseTraditional Use
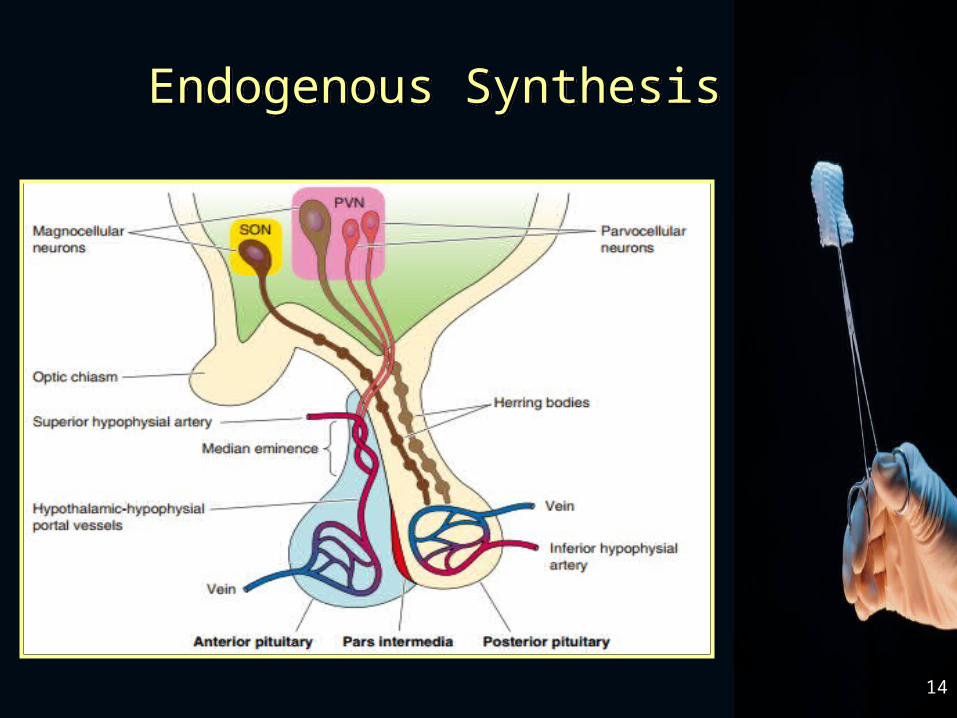
14
Endogenous SynthesisEndogenous Synthesis
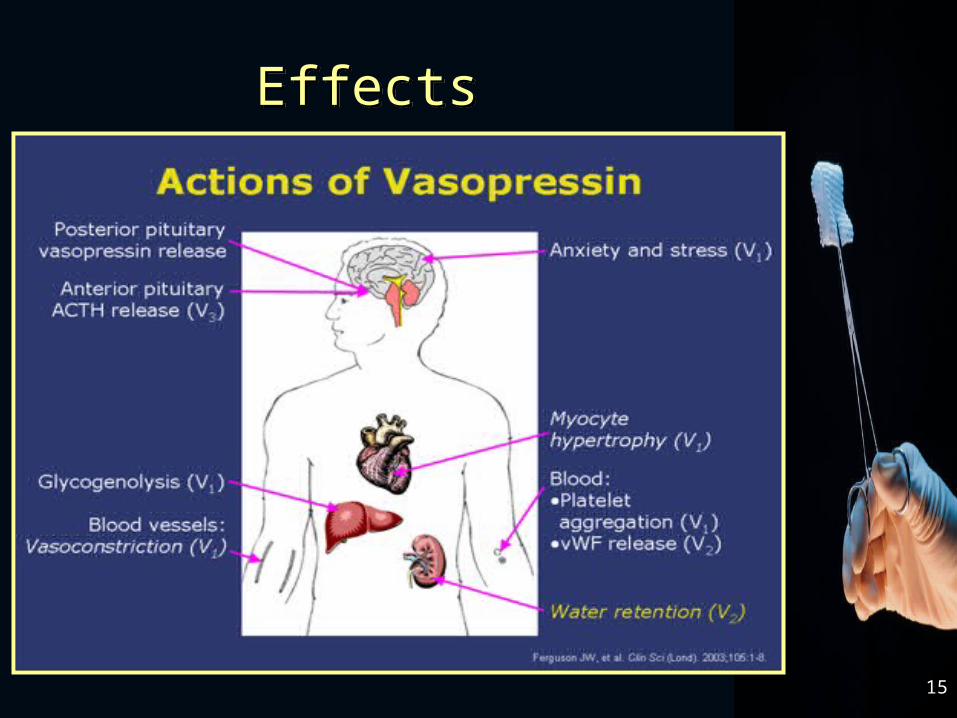
15
EffectsEffects
16
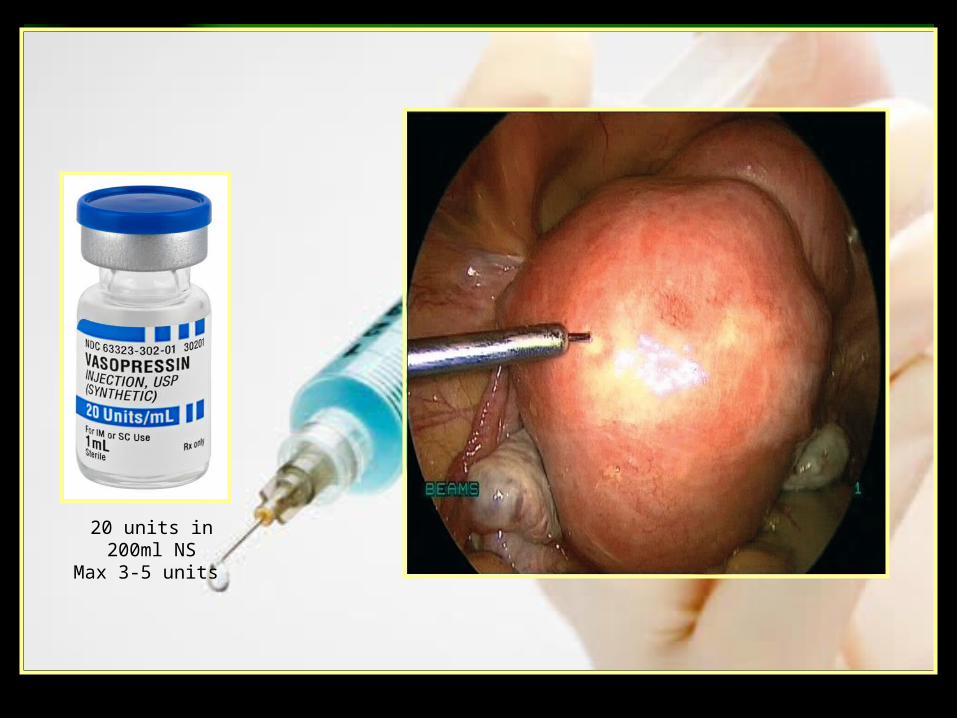
Synthetic Vasopressin in Myomectomy
Synthetic Vasopressin in Myomectomy
• Control bleeding• Potent vasoconstrictor• 20U/ml diluted in 100-200ml of NSS• Max injection 3-5U• Anesthesia should be notified before
injection• Aspirate before injection• 15-25 min half-life
• Control bleeding• Potent vasoconstrictor• 20U/ml diluted in 100-200ml of NSS• Max injection 3-5U• Anesthesia should be notified before
injection• Aspirate before injection• 15-25 min half-life
Medical Templates 2003Medical Templates 2003
Template 8Template 820 units in 200ml NS
Max 3-5 units
18
Case Update #2• Robotic Assisted Laparoscopic
Myomectomy• Approximately 45-60 min into the case• Incision through serosa• BP cuff cycling every 3 minutes
19
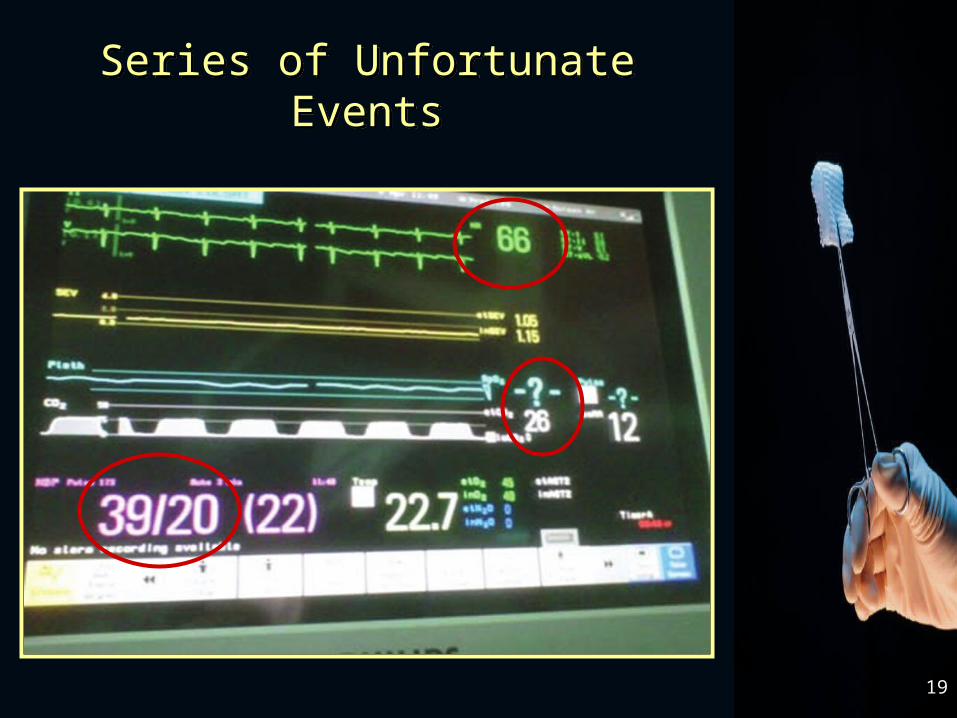
Series of Unfortunate EventsSeries of Unfortunate Events
20
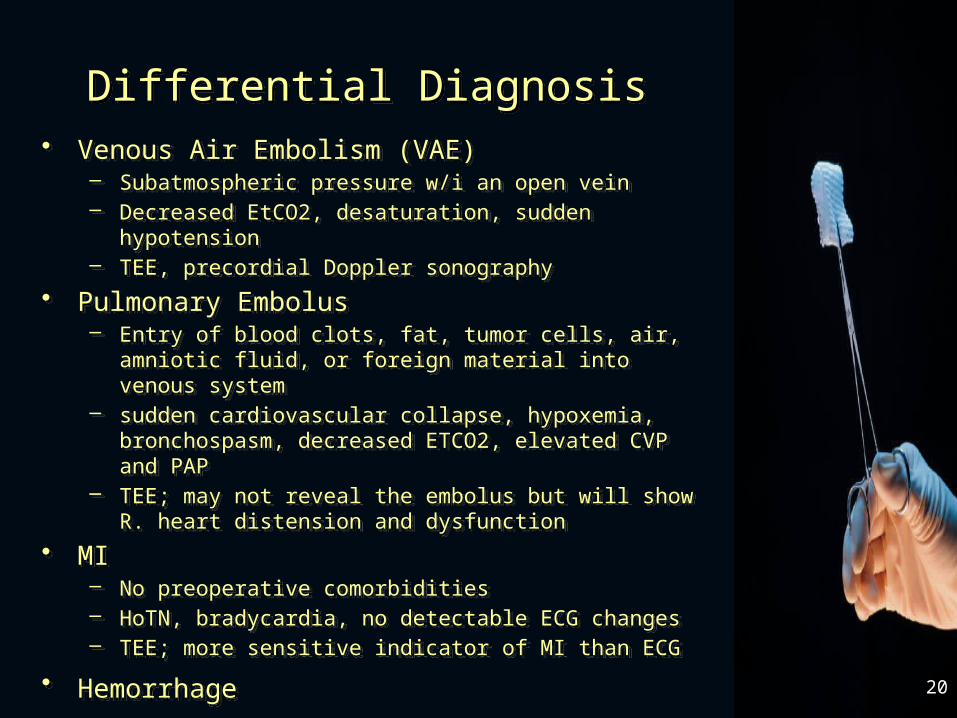
Differential DiagnosisDifferential Diagnosis• Venous Air Embolism (VAE)
– Subatmospheric pressure w/i an open vein– Decreased EtCO2, desaturation, sudden hypotension– TEE, precordial Doppler sonography
• Pulmonary Embolus– Entry of blood clots, fat, tumor cells, air, amniotic fluid, or
foreign material into venous system– sudden cardiovascular collapse, hypoxemia, bronchospasm,
decreased ETCO2, elevated CVP and PAP – TEE; may not reveal the embolus but will show R. heart
distension and dysfunction
• MI– No preoperative comorbidities– HoTN, bradycardia, no detectable ECG changes– TEE; more sensitive indicator of MI than ECG
• Hemorrhage
• Venous Air Embolism (VAE)– Subatmospheric pressure w/i an open vein– Decreased EtCO2, desaturation, sudden hypotension– TEE, precordial Doppler sonography
• Pulmonary Embolus– Entry of blood clots, fat, tumor cells, air, amniotic fluid, or
foreign material into venous system– sudden cardiovascular collapse, hypoxemia, bronchospasm,
decreased ETCO2, elevated CVP and PAP – TEE; may not reveal the embolus but will show R. heart
distension and dysfunction
• MI– No preoperative comorbidities– HoTN, bradycardia, no detectable ECG changes– TEE; more sensitive indicator of MI than ECG
• Hemorrhage
*
21
Transesophageal Echocardiogram
Akinesis
Transesophageal Echocardiogram
Akinesis
*
22
Transesophageal Echocardiogram
Normal
Transesophageal Echocardiogram
Normal
23
Case Update #3• Weak/thready carotid pulse• Absent radial pulses• PEA w/ACLS• Central line placement• Swan ganz placement• Milrinone and Epinepherine infusion• Pulmonary Edema• Lasix • Refractory hypoxemia
25
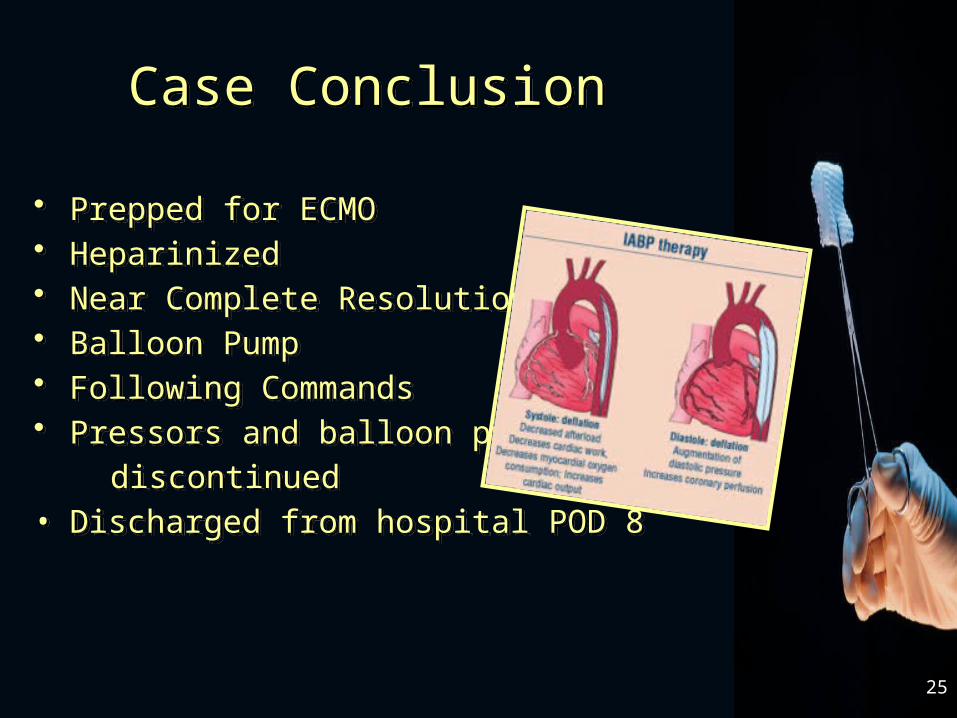
Case ConclusionCase Conclusion
• Prepped for ECMO• Heparinized• Near Complete Resolution• Balloon Pump• Following Commands• Pressors and balloon pump
discontinued• Discharged from hospital POD 8
• Prepped for ECMO• Heparinized• Near Complete Resolution• Balloon Pump• Following Commands• Pressors and balloon pump
discontinued• Discharged from hospital POD 8
What Did We Learn
Vigilance• Never deviate from standard of care• Treated the BP• Notified the surgeon and called for help• Rapid assessment and
treatment/supportive care
27
28
Questions/CommentsQuestions/Comments


















