
Mycobacterium leprae in bone marrow
2
BJHH 32 1–2 Please cite this article in press as: de Oliveira LR, Maltos AL. Mycobacterium leprae in bone marrow. Rev Bras Hematol Hemoter. 2014. http://dx.doi.org/10.1016/j.bjhh.2014.05.010 ARTICLE IN PRESS BJHH 32 1–2 rev bras hematol hemoter. 2 0 1 4; x x x(x x) :xxx–xxx Revista Brasileira de Hematologia e Hemoterapia Brazilian Journal of Hematology and Hemotherapy www.rbhh.org Images in Clinical Hematology Mycobacterium leprae in bone marrow Leonardo Rodrigues de Oliveira ∗ , André Luiz Maltos Q1 Universidade Federal do Triângulo Mineiro – UFTM, Uberaba, MG, Brazil a r t i c l e i n f o Article history: Received 4 March 2014 Accepted 17 March 2014 Available online xxx The case of a 54-year-old man, who was referred to eval- uate a consumptive syndrome with anemia and fever of unknown origin, is reported. A physical examination revealed madarosis, nodular lesions on the ears, nasal soft tissue collapse, subcutaneous nodules on arms and generalized lymphadenopathy. Laboratory tests showed anemia (Hb 8.8 g/dL, mean corpuscular volume 82.4 fL, mean corpuscular hemoglobin 24.5 pg), normal reticulocyte count (0.5%), throm- bocytosis (482 × 10 9 L –1 ), normal serum ferritin (268 ng/mL) and elevated C-reactive protein (124 mg/L). Serologies (viral hepatitis and human immunodeficiency virus) were non- reagent. Lepromatous leprosy was confirmed by staining for acid-fast bacilli using samples from the ear and subcutaneous nodules and bone marrow smears. Bone marrow was hyper- cellular with myeloid hyperplasia (myeloid–erythroid ratio 7:1) but without dysplasia. Mycobacterium leprae was detected lying free and in foamy histiocytes named Virchow cells (Figs. 1 and 2). 1,2 A multidrug therapeutic regimen (clofaz- imine, dapsone, rifampicin) was established with progressive improvement. ∗ Corresponding author at: Universidade Federal do Triângulo Mineiro – UFTM, Central de Quimioterapia, Rua Getúlio Guarita, s/n, 38080- 125 Uberaba, MG, Brazil. E-mail address: [email protected] (L.R. de Oliveira). Fig. 1 – Large cells (histiocytes) with their abundant cytoplasm filled with acid-fast bacilli (Mycobacterium leprae) in bone marrow (Ziehl-Neelsen stain) magnification 1000×. http://dx.doi.org/10.1016/j.bjhh.2014.05.010 1516-8484/© 2014 Associac ¸ão Brasileira de Hematologia, Hemoterapia e Terapia Celular. Published by Elsevier Editora Ltda. All rights reserved. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
-
Upload
andre-luiz -
Category
Documents
-
view
219 -
download
4
Transcript of Mycobacterium leprae in bone marrow
B
I
M
LQ1
U
a
A
R
A
A
Tuumcl8hbahranc7l(ii
1
h1r
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
ARTICLE IN PRESSJHH 32 1–2
rev bras hematol hemoter. 2 0 1 4;x x x(x x):xxx–xxx
Revista Brasileira de Hematologia e HemoterapiaBrazilian Journal of Hematology and Hemotherapy
www.rbhh.org
mages in Clinical Hematology
ycobacterium leprae in bone marrow
eonardo Rodrigues de Oliveira ∗, André Luiz Maltos
niversidade Federal do Triângulo Mineiro – UFTM, Uberaba, MG, Brazil
r t i c l e i n f o
rticle history:
eceived 4 March 2014
ccepted 17 March 2014
vailable online xxx
he case of a 54-year-old man, who was referred to eval-ate a consumptive syndrome with anemia and fever ofnknown origin, is reported. A physical examination revealedadarosis, nodular lesions on the ears, nasal soft tissue
ollapse, subcutaneous nodules on arms and generalizedymphadenopathy. Laboratory tests showed anemia (Hb.8 g/dL, mean corpuscular volume 82.4 fL, mean corpuscularemoglobin 24.5 pg), normal reticulocyte count (0.5%), throm-ocytosis (482 × 109 L–1), normal serum ferritin (268 ng/mL)nd elevated C-reactive protein (124 mg/L). Serologies (viralepatitis and human immunodeficiency virus) were non-eagent. Lepromatous leprosy was confirmed by staining forcid-fast bacilli using samples from the ear and subcutaneousodules and bone marrow smears. Bone marrow was hyper-ellular with myeloid hyperplasia (myeloid–erythroid ratio:1) but without dysplasia. Mycobacterium leprae was detected
Please cite this article in press as: de Oliveira LR, Maltos AL. Mycobahttp://dx.doi.org/10.1016/j.bjhh.2014.05.010
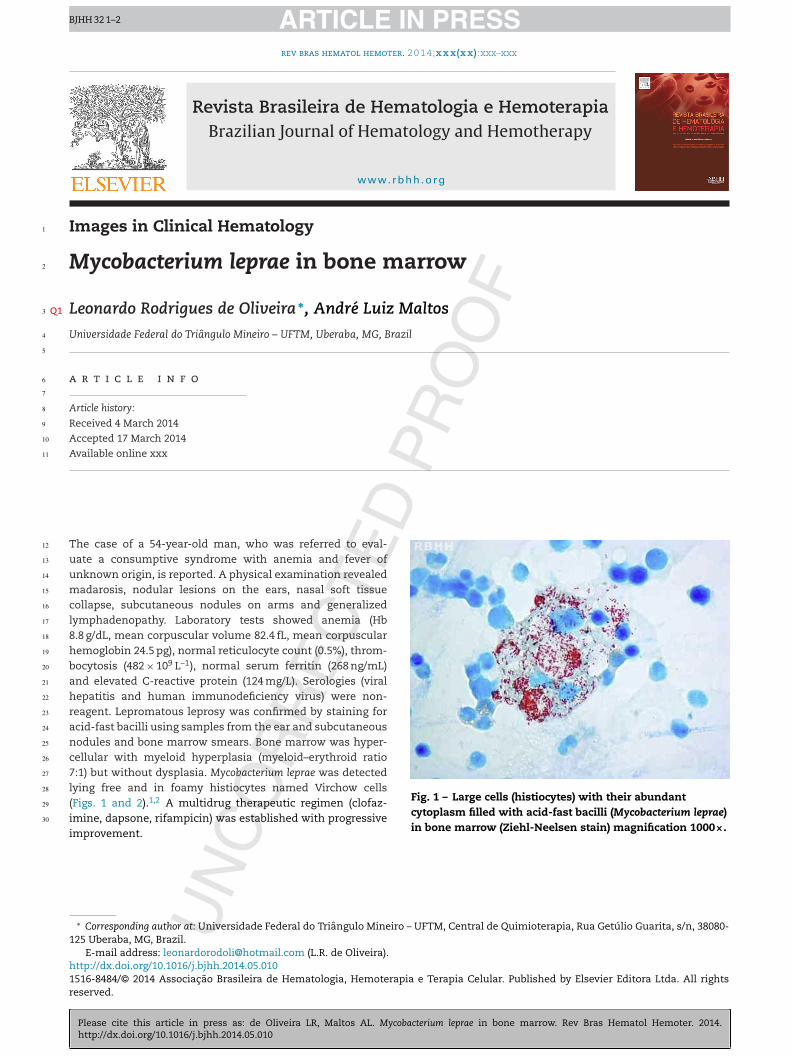
ying free and in foamy histiocytes named Virchow cellsFigs. 1 and 2).1,2 A multidrug therapeutic regimen (clofaz-mine, dapsone, rifampicin) was established with progressivemprovement.
∗ Corresponding author at: Universidade Federal do Triângulo Mineiro –25 Uberaba, MG, Brazil.
E-mail address: [email protected] (L.R. de Oliveira).
Fig. 1 – Large cells (histiocytes) with their abundantcytoplasm filled with acid-fast bacilli (Mycobacterium leprae)in bone marrow (Ziehl-Neelsen stain) magnification 1000×.
ttp://dx.doi.org/10.1016/j.bjhh.2014.05.010516-8484/© 2014 Associacão Brasileira de Hematologia, Hemoterapiaeserved.
BJHH 32 1–2cterium leprae in bone marrow. Rev Bras Hematol Hemoter. 2014.
UFTM, Central de Quimioterapia, Rua Getúlio Guarita, s/n, 38080-
e Terapia Celular. Published by Elsevier Editora Ltda. All rights
ARTICLE IN PRESSBJHH 32 1–2
2 rev bras hematol hemoter. 2
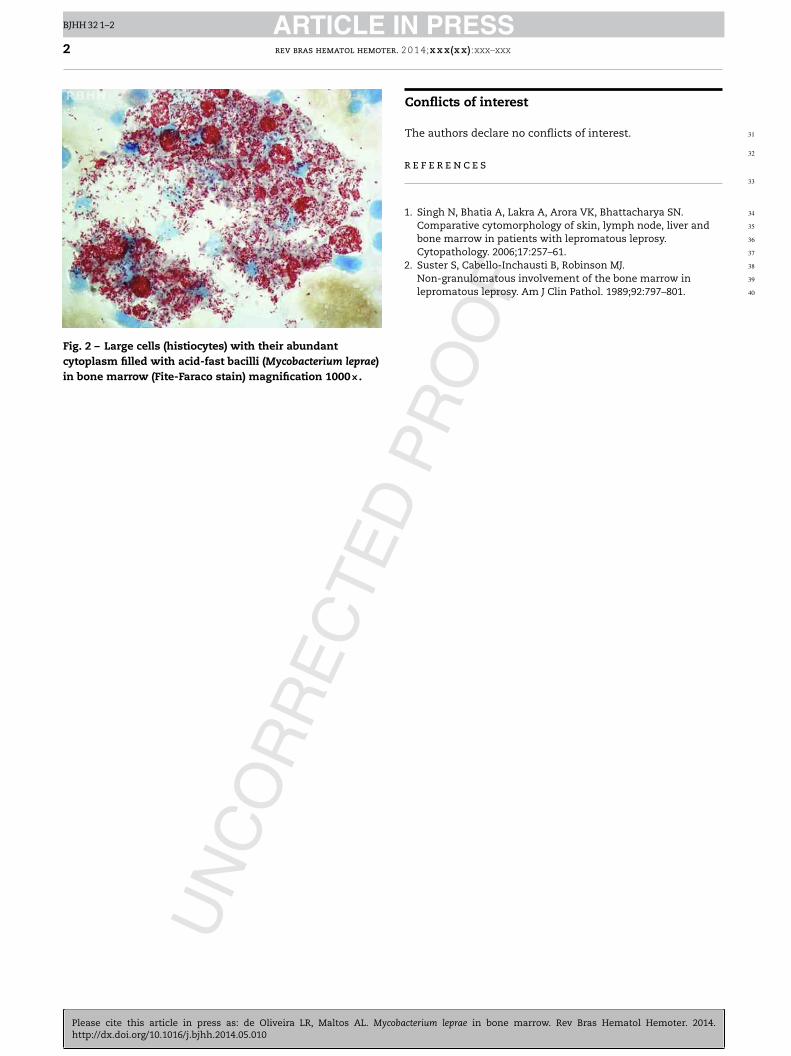
Fig. 2 – Large cells (histiocytes) with their abundantcytoplasm filled with acid-fast bacilli (Mycobacterium leprae)in bone marrow (Fite-Faraco stain) magnification 1000×.
r
1
Cytopathology. 2006;17:257–61.2. Suster S, Cabello-Inchausti B, Robinson MJ.
Non-granulomatous involvement of the bone marrow inlepromatous leprosy. Am J Clin Pathol. 1989;92:797–801.
31
32
33
34
35
36
37
38
39
40
Please cite this article in press as: de Oliveira LR, Maltos AL. Mycobahttp://dx.doi.org/10.1016/j.bjhh.2014.05.010
0 1 4;x x x(x x):xxx–xxx
Conflicts of interest
The authors declare no conflicts of interest.
e f e r e n c e s
. Singh N, Bhatia A, Lakra A, Arora VK, Bhattacharya SN.Comparative cytomorphology of skin, lymph node, liver andbone marrow in patients with lepromatous leprosy.
BJHH 32 1–2cterium leprae in bone marrow. Rev Bras Hematol Hemoter. 2014.


















