
Mycobacterium lepra
67
Mycobacterium Leprae Dr.T.V.Rao MD Dr.T.V.Rao MD 1
-
Upload
tumalapalli-venkateswara-rao -
Category
Health & Medicine
-
view
5.073 -
download
1
Transcript of Mycobacterium lepra

Mycobacterium Leprae
Dr.T.V.Rao MD
Dr.T.V.Rao MD 1
Leprosy
• Vedas
• Bible
• Fear and Social outcasts
• Hansen 1868 - Identifies First microorganism
• Least understood and not cultured in artificial medium
Dr.T.V.Rao MD 2
What is Leprosy?
• It is a disease of Historical importamce
• World's oldest recorded disease
• Stigmatized disease• Gerhard Henrick Armauer
HansenDr.T.V.Rao MD 3

LEPROSY
It is a chronic infectious disease caused by M.leprae, an acid fast, rod shaped
bacillus. It mainly affects the skin, peripheral nerves, and mucosa of the
respiratory tract etc., It has left behind a terrifying image in history and human memory of mutilation, rejection and
exclusion from society.
Dr.T.V.Rao MD 4
Transmission
• Scientist are not quite sure how the disease is trasmitted but they believe that:
– It can be trassmitted from one person to another through
the air.

CarrierCarrier• Armadillo
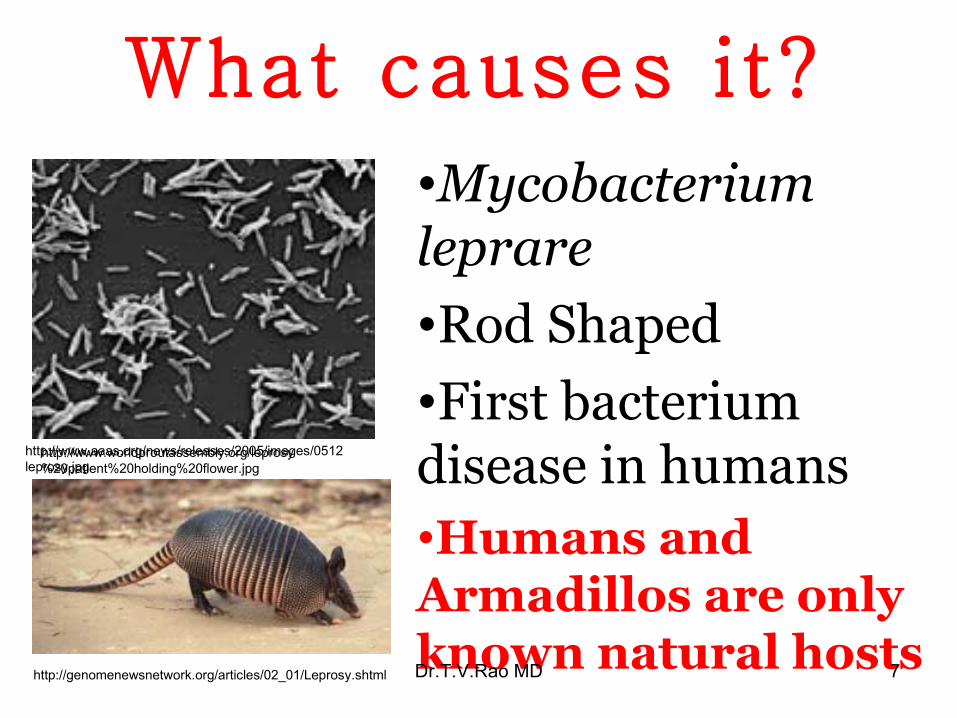
What causes it?
•Mycobacterium leprare•Rod Shaped•First bacterium disease in humans•Humans and Armadillos are only known natural hosts
http://www.aaas.org/news/releases/2005/images/0512leprosy.jpg
http://genomenewsnetwork.org/articles/02_01/Leprosy.shtml
http://www.worldproutassembly.org/leprosy%20patient%20holding%20flower.jpg
Dr.T.V.Rao MD 7

Mycobacterium leprae
• Appear as straight or curved rods• Size is 1 – 8 microns x 0.5 microns.• Polar bodies present as clubbed forms.• Lateral buds• Branching is observed.• Acid fast but less resistant only 5 % H2So4
• Live bacilli, solid uniform structure.• Dead appear as fragmented with
granules.Dr.T.V.Rao MD 8

Mycobacterium leprae• Acid fast bacilli• Strict human pathogens• Cannot be cultivated in-vitro• Armadillo’s used for obtaining M leprae• Transmission - ? Air borne• Low infectivity - prolonged contact required• Spectrum of clinical presentations
– dependent on host –parasite interactions
TuberculoidBorderline
TuberculoidBorderline
lepromatousLepromatous
Dr.T.V.Rao MD 9

Lepers are outcasts ?
Dr.T.V.Rao MD 10
Bell to ring byLeper.
Dr.T.V.Rao MD 11

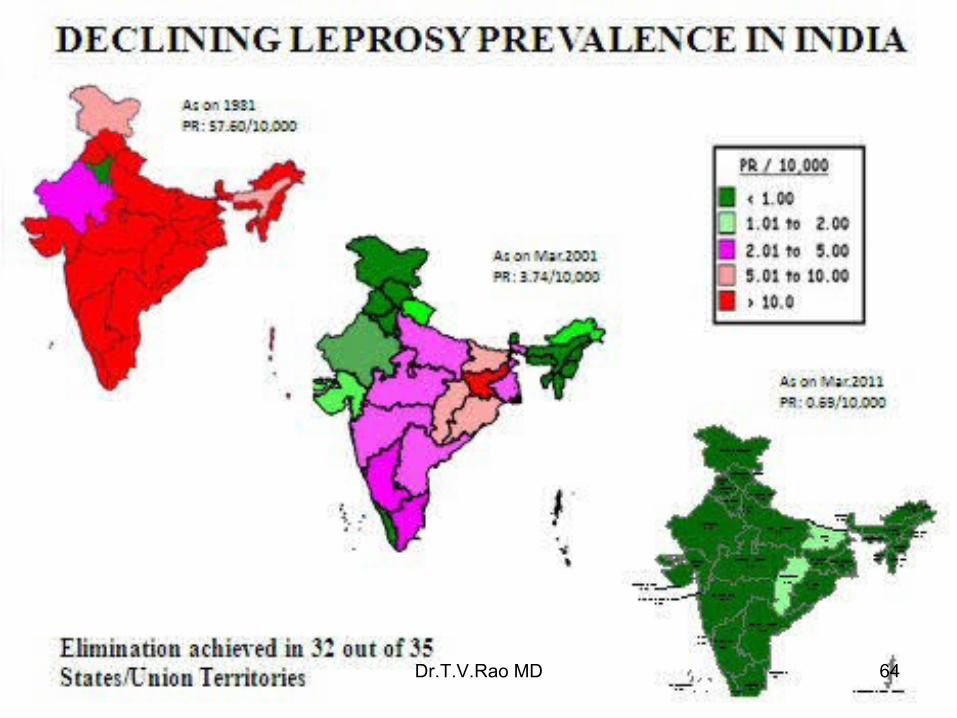
Leprosy in India
Dr.T.V.Rao MD 12

Bacterial Morphology
•Bacilli may present in singles, can be intracellular. Agglomerates.•Bacilli bound by lipid like substance ( Glia)•Masses are Globi•Appear cigar bundles.
Dr.T.V.Rao MD 13
Cultivation
• Not possible
• Can be propagated in Foot pads of Mice
• Granulomas develop at the site of inoculation.
• Nine banded armadillo highly susceptible.
• Chimpanzees
• Generation time 12 -13 days.• Average may be 8- 42 days.
Dr.T.V.Rao MD 14
Important Experimental Animal
Dr.T.V.Rao MD 15

Most Important experimentalAnimal
Dr.T.V.Rao MD 16

Resistance
• Viable for 9 -16 days, and in moist soil for 46 days
• Direct sunlight for two hours.
• Ultraviolet light for 30 minutes..
Dr.T.V.Rao MD 17

Leprosy
• A chronic granulomatous
disease
• Involves
Skin, Peripheral nerves,
Nasal mucosa, Affecting tissues and organs.
Dr.T.V.Rao MD 18

Classification ( Madrid )
1 Lepromatous
2 Tuberculoid
3 Dimorphic
4 Intermediate.
Refers to immune status
Chemotherapy Host Immune Status
Dr.T.V.Rao MD 19

Symptoms
Tuberculoid Leprosy Symptoms • Severe pain • Muscle weakness• Skin stiffness and
dryness • Loss of fingers and toes • Eye problems• Blindeness• Enlarged nerves
Lepromatous Leprosy Symptom• Thickened skin on face • Nasal stuffiness • Bloody nose • Laryngitis • Collapsing of the nose • Swelling of the lymph nodes
in the groin and armpits • Scarring of the testes that
leads to infertility • Enlargement of male breasts
There is two ways leprosy is presented:
Types of LeprosyTypes of Leprosy
• Depending on clinical features, leprosy is classified as:
• Indeterminate Leprosy (IL)• Paucibacillary Leprosy (PB) • Borderline Tuberculoid Leprosy (BT)• Borderline borderline Leprosy (BB)• Borderline lepromatous Leprosy (BL)• Multibacillary Leprosy (MB)
Dr.T.V.Rao MD 21

Ridley and Jopling Classification
• Divided in to 5 types
1 Tuberculoid
2 Borderline Tuberculoid.
3 Borderline.
4.Boderline lepromatous
5 lepromatousDr.T.V.Rao MD 22

WHO classification• Two Groups
1 Paucibacillary 2 Multibacillary Paucibacillary (PB): the number of M. leprae in the body is small (less than 1 million) and a skin smear test is negative. The patient presents five or fewer skin lesions. Most cases of leprosy are PB.
Dr.T.V.Rao MD 23

WHO classification• 2 Multibacillary
• M. leprae can multiple in the body almost without any check and is thus present in high numbers. The bacillus has likely spread to almost all areas of skin and peripheral nerves. A skin smear test is positive and the patient presents more than five skin lesions.
Dr.T.V.Rao MD 24

Immunity• Innate Immunity• Humoral x Cellular immune response.• CMI destroys the bacilli.
• CMI determines the recovery.• Good CMI can manifest with Tuberculoid
leprosy.• Good response with DH Tuberculoid leprosy.• Lepromatous leprosy patient have large number
of CD 8 lymphocytes.
Dr.T.V.Rao MD 25
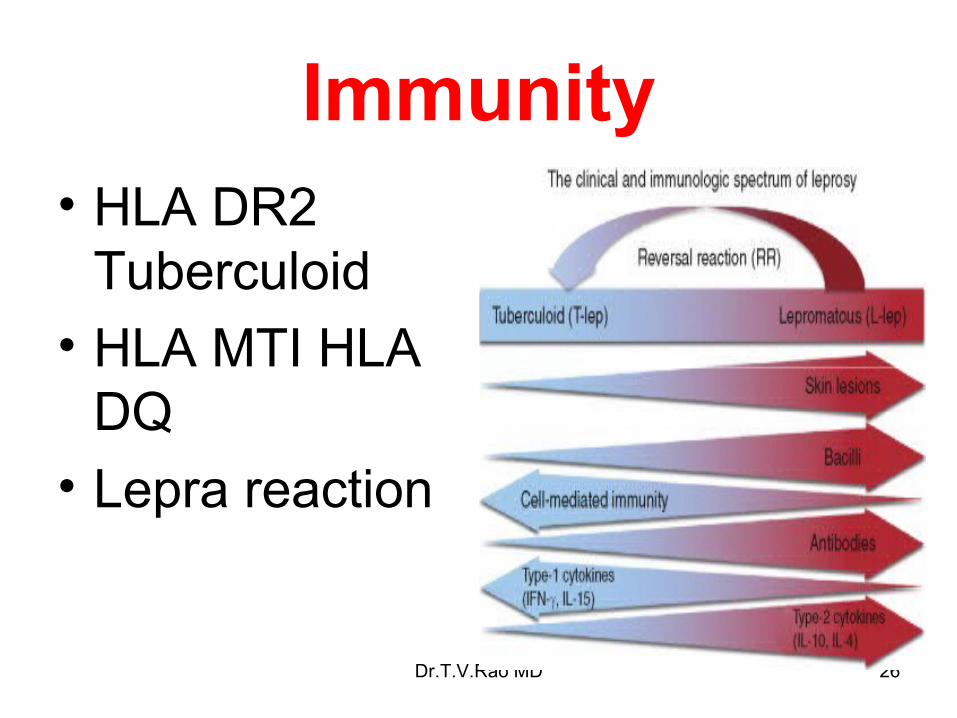
Immunity• HLA DR2
Tuberculoid• HLA MTI HLA
DQ• Lepra reaction
Dr.T.V.Rao MD 26
Pathology and Pathogenesis
• Bacilli seen as Globi inside lepra cells.• Can be seen extracellularly,• Multibacilllary disease.• Nodular lesions.• Granuloma.• Different pathways• Nodular lesions ulcerate• Invade mucosa of Nose, Mouth, URT• Involve RES, Eyes, Testis, Kidney. Bones
Dr.T.V.Rao MD 27

Pathogenesis• Leprosy target cell Schwanncell
• Causes Anesthesia Muscle paralysis.
• Repeated injuries to Anesthetic areas leads to gradual destruction.
• Infiltration of skin, subcutaneous lesions leads to formation of visible lesions.
• First lesions Non specific indeterminate skin lesions
Dr.T.V.Rao MD 28

Hyper reactive -TuberculoidLeprosy
• Tuberculoid leprosy with small number of localized skin lesions, contain so few bacilli.
• Granulomatous response that often damages major nerve trunks.
Dr.T.V.Rao MD 29

Anergic – Lepromatous leprosy
• Skin lesions are numerous or confluent
• Contain high number of bacilli
• Cluster of globi within monocytes
Dr.T.V.Rao MD 30

Other Intermediate Form
• Classified as
1 Borderline Tuberculoid
2 Mid borderline
3 Borderline lepromatous
Dr.T.V.Rao MD 31
Who is at risk?
• Mainly affects:– Skin– Eyes – The peripheral nerves– Mucosa of the upper respiratory tract
• It can affect all ages and both sexes
• 95% of people who are exposed do not develop
Dr.T.V.Rao MD 32

Who is at risk?Who is at risk?
http://microbes.historique.net/images/lep3.jpg
http://www.leprosymission.org/web/pages/leprosy/images/girlwithleprosypatch.jpg
http://www.leprosymission.org/web/pages/leprosy/leprosy.html
bp2.blogger.com/.../s320/lepromatous_leprosy.jpg
Dr.T.V.Rao MD 33

Other consequences
• Destruction of Nasal bones.
• Collapse of Nose
• Eye is damaged - lead to blindness. Dr.T.V.Rao MD 34

Pathology and PathogenesisTuberculoid Leprosy
,Tuberculoid High degree of Immunity.Tuberculoid -- Few skin lesions, Sharply demarcatedMaculo anesthetic patches • Neural Involvement.• Involves Hands and Feet.• Bacilli – few bacilli are seen• A paucibacillary diseases • CMI Adequate.Lepromin test positve• Good Prognosis
Dr.T.V.Rao MD 35

Borderline Leprosy
• Contains characters of both Tuberculoid and Lepromatous leprosy
Dr.T.V.Rao MD 36

How to diagnose leprosy
Examine skin
Check for patches
Test for sensation
Count the number of patches
Look for damage to nervesDr.T.V.Rao MD 37

Diagnosis of Leprosy
• Diagnosis must therefore be made by doing a biopsy, in which a small piece of skin is taken to analyse for the leprosy bacterium. Early diagnosis is very important because it can prevent permanent deformities and disability.
Dr.T.V.Rao MD 38

Laboratory Diagnosis• Lepromatous – easy to diagnose.• Tuberculoid difficult• Histological examination 0n skin Biopsy• Detection for Acid Fast Bacilli.• Nasal discharges,• Slit skin smears.• Ear lobes• Take specimens from unaffected areas too• Stain with Z N method with 5% H2So4
Dr.T.V.Rao MD 39

Dr.T.V.Rao MD 40

Z N Staining and description of bacilli
• Stain weakly, irregularly dead
• Count the bacilli in high power field called as Bacterial index
• Clinically active disease With No bacilli – Pauci bacillary disease
• With bacilli - Multibacillary diseases
Dr.T.V.Rao MD 41

Smear Examination• 1 + 1 -10 bacilli / 100 fields• 2 + 1-10 bacilli / 10 fields.• 3 + 1 – 10 bacilli / one field.• 4 + 10 – 100 bacilli / one field• 5 + 100 - 1000 bacilli /field• 6 + > 1000 bacilli /field Number of Bacilli seen in each field is
recorded as Bacillary index
Dr.T.V.Rao MD 42

The bacteriological index (BI)
• This is an expression of the extent of bacterial loads. It is calculated by counting six to eight stained smears under the 100 x oil immersion lens. in a smear made by nicking the skin with a sharp scalpel and scraping it;
Dr.T.V.Rao MD 43

Quantifying the bacillus as per WHO
• 1+ At least 1 bacillus in every 100 fields.
• 2+ At least 1 bacillus in every 10 fields.• 3+ At least 1 bacillus in every field.
• 4+ At least 10 bacilli in every field.
• 5+ At least 100 bacilli in every field.
• 6+ At least 1000 bacilli in every field.•Number of Bacilli seen in each field is recorded as Bacillary indexDr.T.V.Rao MD 44
Bacteriological Index• Indicates the Prognosis of the Disease
• Total score in all smears
------------------------------------
Number of smears
Eg 16/8 =2
So the index is 2
-Dr.T.V.Rao MD 45

The Morphological index (MI)
• This is calculated by counting the numbers of solid-staining acid-fast rods. Only the solid-staining bacilli are viable. It is not unusual for solid-staining M. leprae to reappear for short periods in patients being successfully treated with drugs. It is important to recognize that measurement of MI is liable for observer variations and therefore not always reliable.
Dr.T.V.Rao MD 46

Morphological index (MI)
• The fluid and tissue obtained are spread fairly thickly on a slide and stained by the Ziehl-Neelsen method and decolorized (but not completely) which 1% acid alcohol. The results are expressed on a logarithmic scale.
Dr.T.V.Rao MD 47

Lepromin Test• Mitsuda in 1919 – skin test – delayed
hypersensitivity.• Lepromin is boiled emulsified lepromatous tissue –
rich in lepra bacilli.• Lepromins, made from boiled bacilli from
lepromatous lesions.• Leprosins ultisonicates of tissue free bacilli• Human source ,Leprosins –H ,Armadillo – Leprosins - A
• Events in the reaction Biphasic reaction• Fernandez Reaction .> 24 – 48 hours, remains for 3 –
5 days, like tuberculin reaction, little significant.
Dr.T.V.Rao MD 48

Lepromin test• Mitsuda in 1919.• Human source of bacilli Lepromin H• Armadillos source of bacilli Lepromin A• Bacillary Lepromin - Dharmendra antigen• Inject 0.1 ml of LeprominRead for two types of reactions 1 Early Farnedez reaction 2 Late Mitsuda reaction
Dr.T.V.Rao MD 49
Lepromin Test• Mitsuda reaction occurs after 1 – 2 weeks.
prominent after 4 weeks• Infiltration with Lymphocytes ,Epitheloid
cells,and giant cells,• Indicates CMI• Differentiates those mount immune
response and those cannot• Now antigens are derived from Armadillo
derived lepra bacilliDr.T.V.Rao MD 50
Lepromin Test (Cont)
• Test is not employed for Diagnosis of leprosy,
• Effectiveness of CMI
• Helps to asses the prognosis
• Positive test good response /recovery
• Negative Bad prognosisDr.T.V.Rao MD 51

Problems of over diagnosis• Wrong diagnosis in 0% to 28.6% (9.4%)
Govt. of India, WHO, NIHFW 2004• Causes:
1. lack of knowledge by HCP to exclude dermatological and neurological conditions mimicking leprosy, therefore many doubtful cases included
Causes of under diagnosisCauses of under diagnosis
• Thicken peripheral nerve with sensory deficit highly subjective
• Tools used for sensation testing in the field is of low to moderate scientific validity
• Lesions on the face, difficult to elicit sensory impairment
• Difficult to diagnose clinically the early LL cases without slit smear examination and\or skin biopsy

Treatment of Leprosy• Multidrug regime Rifampicin 600 mg / once month Dapsone 100/day Clofazimine 50 mg/daily. Continue for 6 monthsOther Drugs for Leprosy 1.Ethionamide 2.Prothionamide.
Dr.T.V.Rao MD 54
About DapsoneAbout Dapsone• It was discovered by
German chemists Fromm and Wittmann in 1908
• Was not utilized as a treatment until decades later
• Available in 25mg & 100 mg tablets
• Rated a pregnancy risk category C by the American Food and Drug Administration

About RifampicinAbout Rifampicin• In the U.S. Rifampicin is marketed as:
– Rifadin (Aventis)– Rifater ( in combination with isoniazid and
pyrazinamide) (Aventis)– Rimactane (Novartis)
• Do not wear contact lenses while taking Rifampicin
• Rated a pregnancy risk category C by the American Food and Drug Administration

Pharmaceutical Treatment
• Multiple Drug Treatment (MDT)
• There are several effective chemotherapeutic agents:
Dapsone (diaphenylsulfone, DDS), Rifampicin (RFP), Clofazimine (CLF), Ofloxacin (OFLX), and Minocycline (MINO) constitute the backbone of the multidrug therapy (MDT) regimen.
Dr.T.V.Rao MD 57

Side Effects• Occasional cutaneous
eruptions
• A slight reddish coloration of urine, sweat, and tears
• Brownish Black discoloration and dryness of skin
• Dapsone (DDS)
• Rifampicin (RFP)
• Clofazimine (CLF)

Dosage Cont’d......
Multidrug Therapy for Paucibacillary (PB) Leprosy
RFP Dapsone
Adult
50-70kg
600mg/m* 100mg/d
Child10-14 years
450mg/m* 50mg/d
Less than 10 years
300mg/m* 25mg/d
PB patients treated with MDT are cured within six months
*RFP monthly doses are given under supervision Dr.T.V.Rao MD 59

Cost of MDT- Cost of MDT- FundingFunding
• Since 1995, WHO has supplied MDT FREE of cost to all leprosy patients in the world.
• Initially drug funds were provided by Nippon Foundation
• Since 2000, donations are provided by Novartis and the Novartis Foundation for Sustainable Development
FREE

Prophylaxis
• Long term chemotherapy
• BCG vaccine useful
Dr.T.V.Rao MD 61
Epidemiology• Nasal secretions – rich source of
infection,
• Skin contact get infected.
• Incubation 2 – 5 years.
• May take 30 years to manifest.
• I/3 world Leprosy patients are Indians.
• Orissa and Bihar highest.Dr.T.V.Rao MD 62

Prevention Of Leprosy• Early Diagnosis and treatment.• BCG vaccination ?• Health awareness and active surveillance high
endemic areas• Field trails with different vaccines BCG + killed lepra bacilli ( ICRC ) bacillus have not given conclusive results.
Dr.T.V.Rao MD 63
Dr.T.V.Rao MD 64
What is LeprosyToday
• No at all a feared disease.
• Only 5 % spouse infective rate
• Leprosy is uncommon in most countries today, but it causes massive suffering in the areas where it is still found. These areas are largely confined to tropical and subtropical regions of Africa, Asia, and Central and South America.
• .Dr.T.V.Rao MD 65

Dr.T.V.Rao MD 66

Programmed Created by Dr.T.V.Rao MD for Medical and Paramedical Students in
the Developing World
Dr.T.V.Rao MD 67


















