Multi Vessel disease with STEMI – How to...
31
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr Thomas Alexander Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre and Hospital, Coimbatore, India
-
Upload
truongminh -
Category
Documents
-
view
216 -
download
0
Transcript of Multi Vessel disease with STEMI – How to...
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION
Dr Thomas Alexander
Dr. Thomas Alexander, M.D; D.M; F.A.C.C.Senior Consultant and Interventional Cardiologist
Kovai Medical Centre and Hospital, Coimbatore, India

Primary PCI is the standard interventional treatment in STEMI. In patients treated with primary PCI, multivessel disease is present in about
40-50% of hemodynamically stable patients and about 70-80 % of patients with cardiogenic shock.
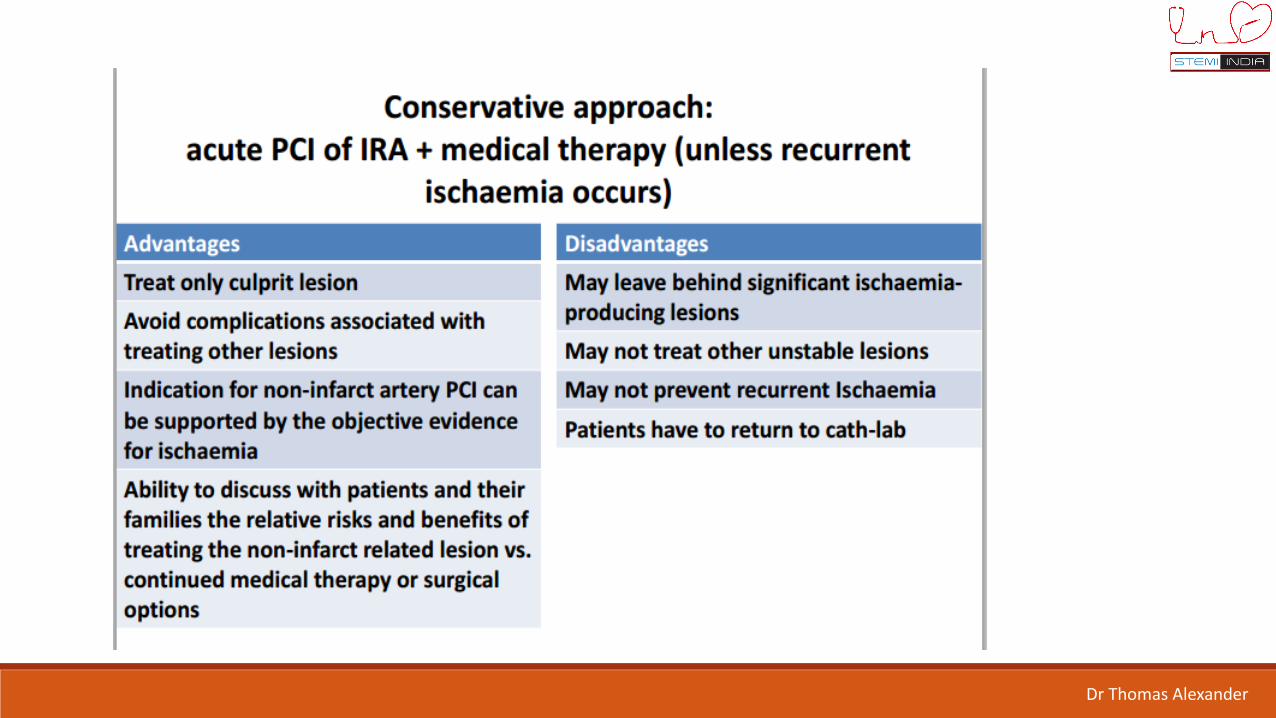
Two interventional strategies have been used for managing STEMI with MVD. Infarct-related or culprit vessel-only revascularization (CVR), no other diseased
vessels are targeted, regardless of their significance. The other strategy is multivessel revascularization (MVR), defined as an
intervention of more than one significant stenotic vessel, either adhoc or staged.
Multivessel intervention based on Angiography or based on FFR
Dr Thomas Alexander
Dr Thomas Alexander

Dr Thomas Alexander

Dr Thomas Alexander

NEJM 2013;369:1115
Culprit-only PCI (n=231) – no preventative PCIComplete revascularization (n=234) –
preventative PCIComplete revascularization performed during
index PCI
Dr Thomas Alexander

465 STEMI patients
1o endpoint: Cardiac death, non-fatal MI or refractory angina
2o endpoints: repeat PCI, non-cardiac death and individual components of 1o endpoint
Trial stopped early, mean follow-up 23 months (465 of the anticipated 600 patient enrollment)
Randomized following infarct-related artery (IRA)-PCI:
NEJM 2013;369:1115
Dr Thomas Alexander

PRAMI has a number of limitations.
The patients in the conservative group did not undergo a staged PCI or
even a test for ischemia.
PCI of all lesions > 50% without any proof of the hemodynamic
significance of the lesion.
Premature termination of the trial, which usually means that results
between the groups are frozen at the moment of the highest difference.
In addition, the differences between multi-vessel PCI and culprit PCI in
mortality are greater than between reperfusion and no reperfusion or
between primary PCI and fibrinolysis in large clinical trials, which is highly
unlikely.
NEJM 2013;369:1115
Dr Thomas Alexander
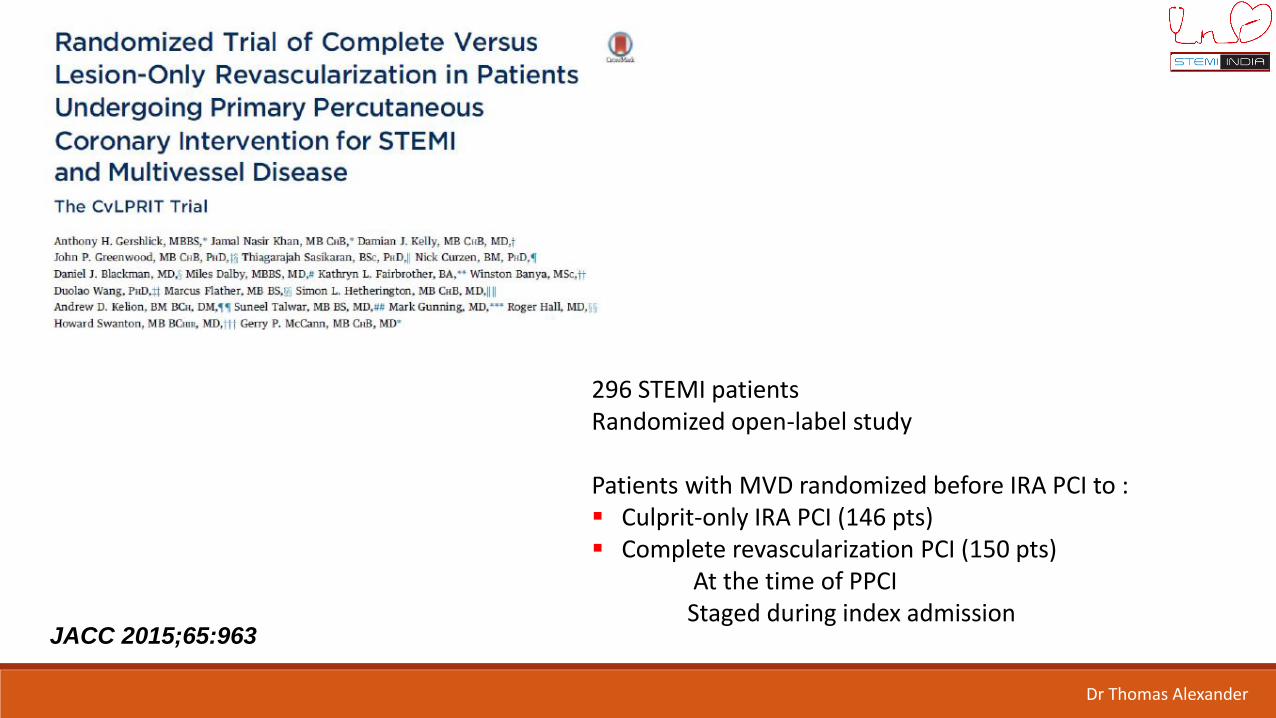
JACC 2015;65:963
296 STEMI patientsRandomized open-label study
Patients with MVD randomized before IRA PCI to : Culprit-only IRA PCI (146 pts) Complete revascularization PCI (150 pts)
At the time of PPCIStaged during index admission
Dr Thomas Alexander

1o outcome: MACE – total mortality/recurrent MI/heartfailure and ischemia- driven revascularization at 12months
JACC 2015;65:963
Dr Thomas Alexander

Small study – screened 850 patients over 48 months to enroll 296 Trial is underpowered to detect reduction in hard endpoints. The composite endpoint has many components, and none of the
components are significant. There are few events in the patients which adds to the
uncertainty of the results. The results are in sharp contrast to the results of the much larger
COURAGE trial, in which PCI of stable lesions despite proof a ischemia was not associated with an improved outcome compared to optimal medical therapy.
JACC 2015;65:963
CvLPRIT: has a number of limitations.
Dr Thomas Alexander
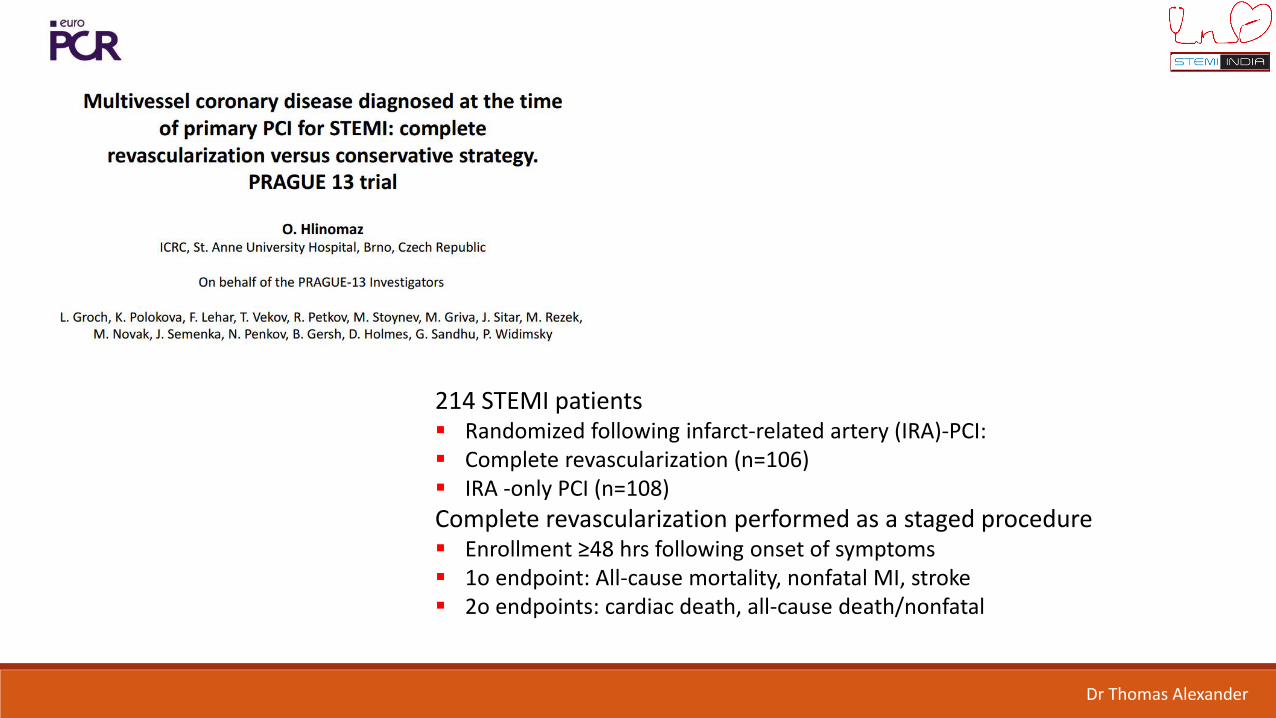
214 STEMI patients Randomized following infarct-related artery (IRA)-PCI: Complete revascularization (n=106) IRA -only PCI (n=108)
Complete revascularization performed as a staged procedure Enrollment ≥48 hrs following onset of symptoms 1o endpoint: All-cause mortality, nonfatal MI, stroke 2o endpoints: cardiac death, all-cause death/nonfatal
Dr Thomas Alexander

Dr Thomas Alexander
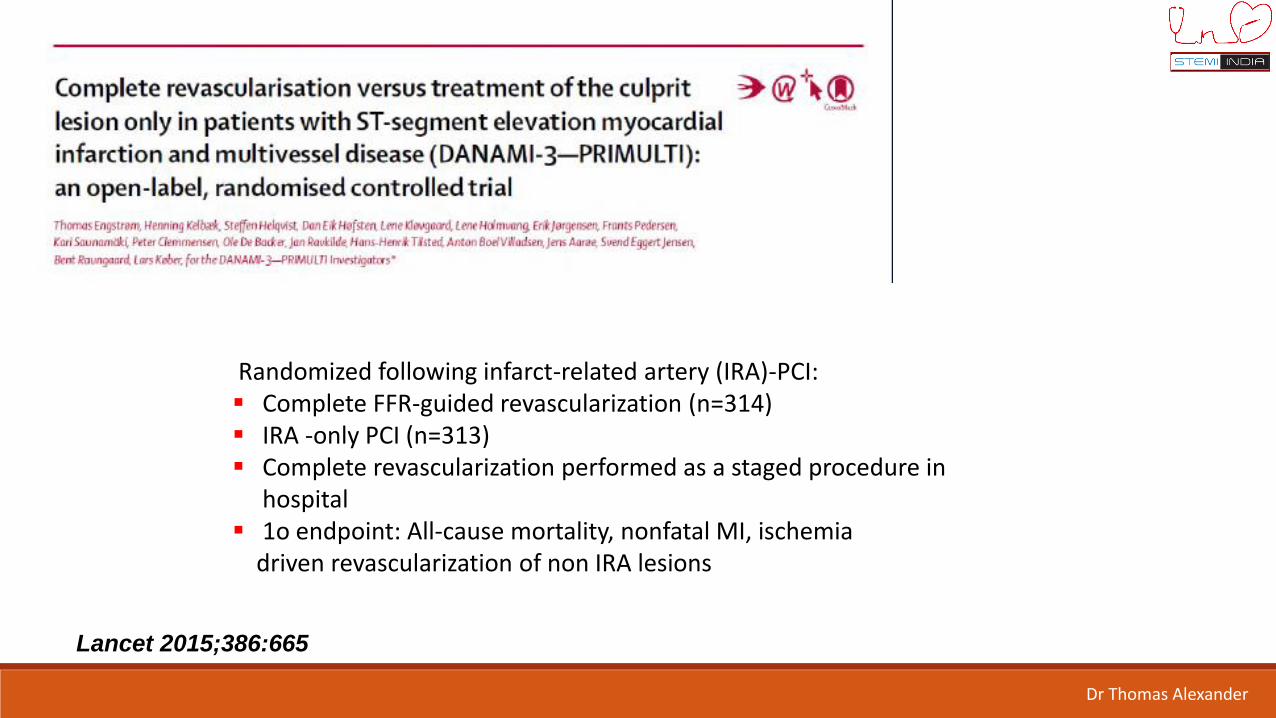
627 STEMI patients
Randomized following infarct-related artery (IRA)-PCI: Complete FFR-guided revascularization (n=314) IRA -only PCI (n=313) Complete revascularization performed as a staged procedure in
hospital 1o endpoint: All-cause mortality, nonfatal MI, ischemia
driven revascularization of non IRA lesions
Lancet 2015;386:665
Dr Thomas Alexander

Lancet 2015;386:665
10 Trials with 2285 patients 4 different revascularization strategies were studied
- Complete revascularization at Index procedure- Staged Complete – IRA at Index and Non culprit treated before discharge- Staged Complete – IRA at Index and Non culprit within few
weeks of discharge- Culprit only revascularization
Pairwise meta-analysis
Islam Y. Elgendy et al. JCIN 2017;10:315-324
Dr Thomas Alexander

Islam Y. Elgendy et al. JCIN 2017;10:315-324
Dr Thomas Alexander
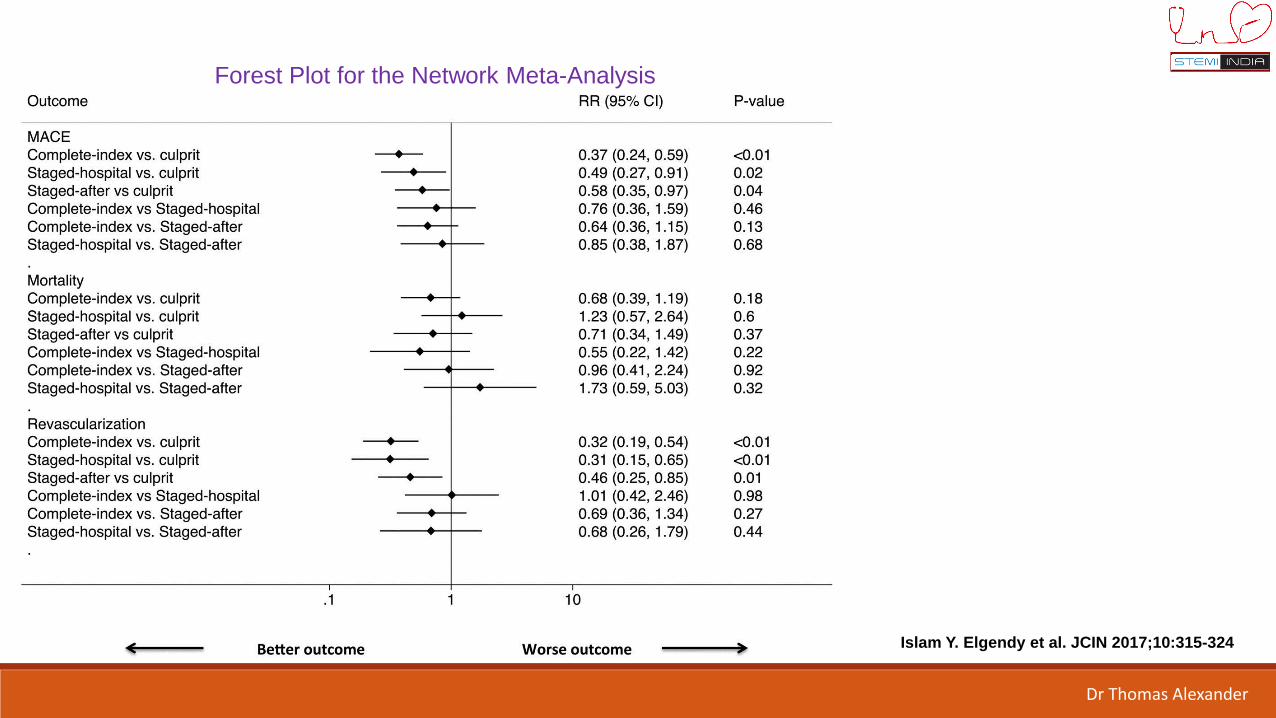
Forest Plot for the Network Meta-Analysis
Islam Y. Elgendy et al. JCIN 2017;10:315-324
Dr Thomas Alexander
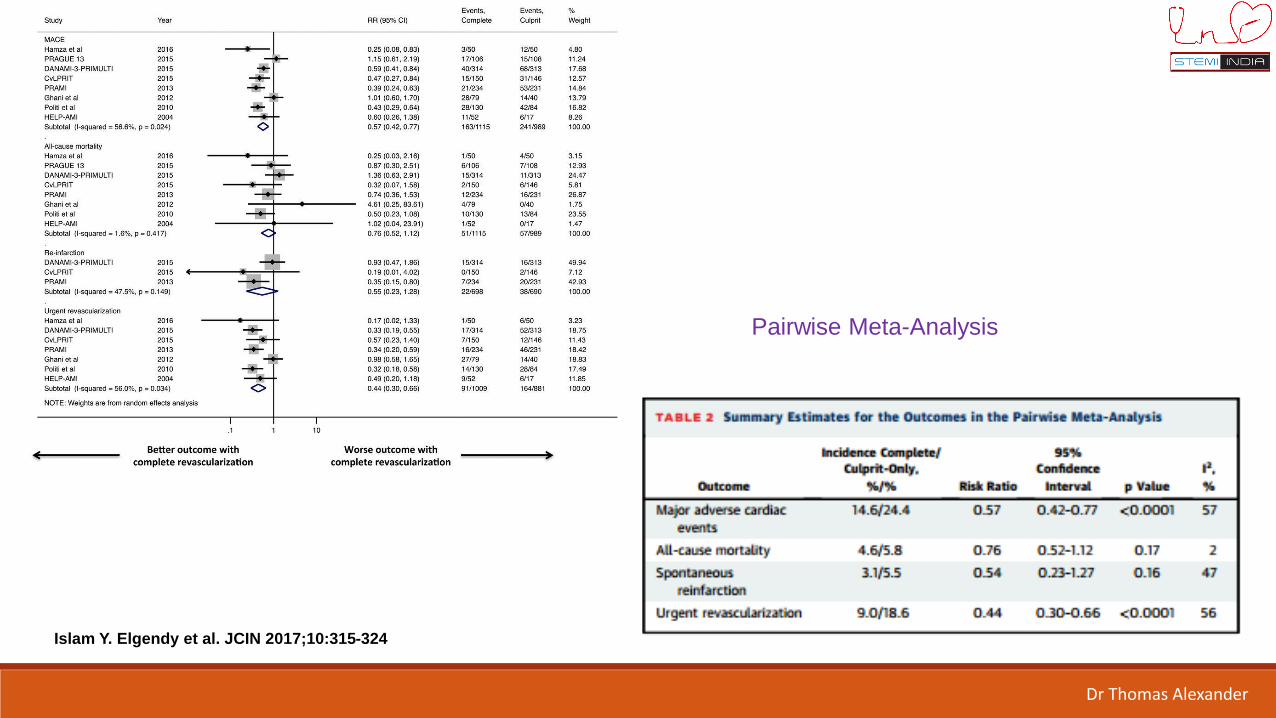
Pairwise Meta-Analysis
Islam Y. Elgendy et al. JCIN 2017;10:315-324
Dr Thomas Alexander
Current evidence from randomized trials suggests that the risk of all-cause mortality and spontaneous reinfarction is not different among the various revascularization strategies for multivessel disease.
Complete revascularization at the index procedure or as a staged procedure (either during the hospitalization or after discharge) was associated with a reduction of MACE due to reduction in urgent revascularization with no difference between these 3 strategies.
Islam Y. Elgendy et al. JCIN 2017;10:315-324
Conclusions: Randomised Trials
Dr Thomas Alexander
British Columbia Cardiac Registry - Largest registry to date –6503 STEMI patients with MVD
All cause mortality and repeat revascularization at 2 years Three strategies
- MV Intervention at Index procedure - MVI- Culprit Vessel Intervention only – CVI-O- Culprit vessel Intervention followed by staged Intervention – CVI-S
M. Bilal Iqbal et al. JCIN 2017;10:11-23
Dr Thomas Alexander

M. Bilal Iqbal et al. JCIN 2017;10:11-23
Dr Thomas Alexander
In patients with STEMI undergoing primary percutaneous coronary intervention, a strategy of CVI-S seems to be associated with lower mortality and repeat revascularization rates.
However, MVI may be considered in selected patients and in the setting of non-culprit left anterior descending artery disease
M. Bilal Iqbal et al. JCIN 2017;10:11-23
Conclusions: Registry Data

Potential Factors that could Influence the decision to do
multi-vessel intervention at the Index procedure
Number of diseased Vessels
Focal or diffuse disease
Severity and location of stenosis – 50%, CTO
Size of Index infarction – LV Function
Hemodynamic and Electrical Stability
Technical complexity
Co-morbid conditions – Renal function, Diabetes
Need for FFR
Cost considerations – CABG
Time of the Day
Dr Thomas Alexander

< 30% residual stenosis
Excellent IRA PCI Result TIMI – III Epicardial flow
TIMI III myocardial blush grade
Persistent Ischemic pain
Unstable hemodynamics
Remote ST-T changes
Low contrast volume and short procedure
Severity of lesion – critical
Low anticipated technical difficulty
High anticipated success rate and
Low rate of anticipated complication
MVI at Index Procedure
Dr Thomas Alexander

Dr Thomas Alexander

Conclusions
Recent evidence suggests that early treatment of significant non-culpritartery lesions in patients with STEMI, would reduce global ischemic burdenand protect against short and medium-term recurrent ischemic events.
Though, randomised trials show that MVI at Index procedure or stagedyield similar benefits, these enrol relatively low risk patients.
The largest registry data to date shows that the staged MVI has the lowestmortality and repeat revascularisation rate.
Dr Thomas Alexander
Conclusions
Benefit of FFR to non culprit vessel intervention, needs to be clarified
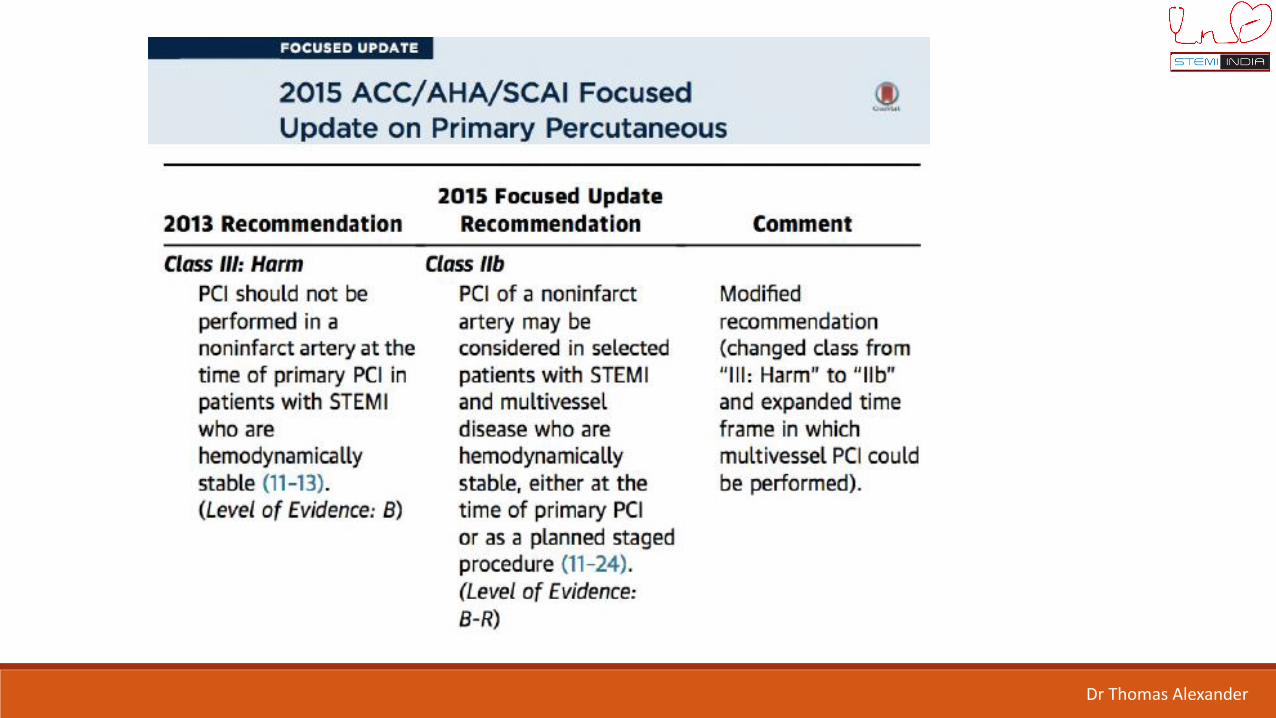
With the current evidence, non-culprit artery intervention, during the Index
procedure, in STEMI is no more deemed as “Harmful”.
At present, in patients with Cardiogenic Shock, complete
revascularization during STEMI should be considered only in the
presence of multiple, critical stenoses or highly unstable lesions
(angiographic signs of possible thrombus or lesion disruption), and if
there is persistent ischemia after PCI.
Dr Thomas Alexander
Dr Thomas Alexander

Dr Thomas Alexander

Thank You for Your Attention
Dr Thomas Alexander