MRCS preparation emrcs questions Pathology
388
A 38 year old lady presents with a recent episode of renal colic. As part of her investigations the following results are obtained: Corrected Calcium 3.84 mmol/l PTH 88pg/ml (increased) Her serum urea and electrolytes are normal. What is the most likely diagnosis? A. Carcinoma of the bronchus B. Secondary hyperparathyroidism C. Primary hyperparathyroidism D. Tertiary hyperparathyroidism E. Carcinoma of the breast Theme from September 2012 exam Theme from September 2011 exam In this situation the most likely diagnosis is primary hyperparathyroidism. The question mentions that serum urea and electrolytes are normal, which makes tertiary hyperparathyroidism unlikely. Primary hyperparathyroidism In exams primary hyperparathyroidism is stereotypically seen in elderly females with an unquenchable thirst and an inappropriately normal or raised parathyroid hormone level. It is most commonly due to a solitary adenoma Causes of primary hyperparathyroidism 80%: solitary adenoma 15%: hyperplasia 4%: multiple adenoma 1%: carcinoma Features - 'bones, stones, abdominal groans and psychic moans' Polydipsia, polyuria Peptic ulceration/constipation/pancreatitis Bone pain/fracture Renal stones Depression Hypertension
-
Upload
faisol-kabir -
Category
Health & Medicine
-
view
528 -
download
64
Transcript of MRCS preparation emrcs questions Pathology

A 38 year old lady presents with a recent episode of renal colic. As part of her
investigations the following results are obtained:
Corrected Calcium 3.84 mmol/l
PTH 88pg/ml (increased)
Her serum urea and electrolytes are normal.
What is the most likely diagnosis?
A. Carcinoma of the bronchus
B. Secondary hyperparathyroidism
C. Primary hyperparathyroidism
D. Tertiary hyperparathyroidism
E. Carcinoma of the breast
Theme from September 2012 exam
Theme from September 2011 exam
In this situation the most likely diagnosis is primary hyperparathyroidism. The
question mentions that serum urea and electrolytes are normal, which makes tertiary
hyperparathyroidism unlikely.
Primary hyperparathyroidism
In exams primary hyperparathyroidism is stereotypically seen in elderly females with
an unquenchable thirst and an inappropriately normal or raised parathyroid hormone
level. It is most commonly due to a solitary adenoma
Causes of primary hyperparathyroidism
80%: solitary adenoma
15%: hyperplasia
4%: multiple adenoma
1%: carcinoma
Features - 'bones, stones, abdominal groans and psychic moans'
Polydipsia, polyuria
Peptic ulceration/constipation/pancreatitis
Bone pain/fracture
Renal stones
Depression
Hypertension

Associations
Hypertension
Multiple endocrine neoplasia: MEN I and II
Investigations
Raised calcium, low phosphate
PTH may be raised or normal
Technetium-MIBI subtraction scan
Treatment
Parathyroidectomy, if imaging suggests target gland then a focused approach
may be used
Theme: Head and neck lumps
A. Branchial cyst
B. Cystic hygroma
C. Carotid body tumour
D. Lymphadenopathy
E. Adenolymphoma of the parotid
F. Pleomorphic adenoma of the parotid
G. Submandibular tumour
H. Thyroglossal cyst
I. Thoracic outlet syndrome
J. Submandibular gland calculus
Please select the most likely lesion to account for the clinical scenario given.
Each option may be used once, more than once or not at all.
2. A 60 year old Tibetan immigrant is referred to the surgical clinic with a painless
neck swelling. On examination it is located on the left side immediately anterior
to the sternocleidomastoid muscle. There are no other abnormalities to find on
examination.
You answered Branchial cyst
The correct answer is Carotid body tumour
Carotid body tumours typically present as painless masses. They may compress
the vagus or hypoglossal nerves with symptoms attributable to these structures.
Over 90% occur spontaneously and are more common in people living at high

altitude. In familial cases up to 30% may be bilateral. Treatment is with
excision.
3. A 40 year old women presents as an emergency with a painful mass underneath
her right mandible. The mass has appeared over the previous week with the pain
worsening as the lump has increased in size. On examination there is a 4cm mass
underneath her mandible, there is no associated lymphadenopathy.
Submandibular gland calculus
The sub mandibular gland is the most common site for salivary calculi. Patients
will usually complain of pain, which is worse on eating. When the lesion is
located distally the duct may be laid open and the stone excised. Otherwise the
gland will require removal.
4. A 73 year old male smoker is referred to the clinic by his GP. On examination he
has a 3cm soft mass immediately anterior to his ear. It has been present for the
past five years and is otherwise associated with no symptoms.
You answered Pleomorphic adenoma of the parotid
The correct answer is Adenolymphoma of the parotid
Warthins tumours (a.k.a. adenolymphoma) are commoner in older men
(especially smokers). They are the second commonest benign tumour of the
parotid gland, they may be bilateral. They are soft and slow growing and
relatively easy to excise. Pleomorphic adenomas typically present in females
aged between 40 - 60 years.
Neck lumps
The table below gives characteristic exam question features for conditions
causing neck lumps:
Reactive
lymphadenopathy
By far the most common cause of neck swellings. There may
be a history of local infection or a generalised viral illness
Lymphoma Rubbery, painless lymphadenopathy
The phenomenon of pain whilst drinking alcohol is very
uncommon
There may be associated night sweats and splenomegaly
Thyroid swelling May be hypo-, eu- or hyperthyroid symptomatically
Moves upwards on swallowing
Thyroglossal cyst More common in patients < 20 years old
Usually midline, between the isthmus of the thyroid and the
hyoid bone

Moves upwards with protrusion of the tongue
May be painful if infected
Pharyngeal pouch More common in older men
Represents a posteromedial herniation between
thyropharyngeus and cricopharyngeus muscles
Usually not seen, but if large then a midline lump in the neck
that gurgles on palpation
Typical symptoms are dysphagia, regurgitation, aspiration
and chronic cough
Cystic hygroma A congenital lymphatic lesion (lymphangioma) typically
found in the neck, classically on the left side
Most are evident at birth, around 90% present before 2 years
of age
Branchial cyst An oval, mobile cystic mass that develops between the
sternocleidomastoid muscle and the pharynx
Develop due to failure of obliteration of the second branchial
cleft in embryonic development
Usually present in early adulthood
Cervical rib More common in adult females
Around 10% develop thoracic outlet syndrome
Carotid aneurysm Pulsatile lateral neck mass which doesn't move on swallowing
A 12 year old child is admitted with a 12 hour history of colicky right upper quadrant
pain. On examination the child is afebrile and is jaundiced. The abdomen is soft and
non tender at the time of examination. What is the most likely cause?
A. Infectious hepatitis
B. Acute cholecystitis
C. Cholangitis
D. Hereditary spherocytosis
E. Gilberts syndrome
Theme from September 2012 Exam
The child is most likely to have hereditary spherocytosis. In these individuals there
may be disease flares precipitated by acute illness. They form small pigment stones.
These may cause biliary colic and some may require cholecystectomy.
Hereditary Spherocytosis
Most common disorder of the red cell membrane, it has an incidence of 1 in 5000.
The abnormally shaped erythrocytes are prone to splenic sequestration and
destruction. This can result in hyperbilirubinaemia, jaundice and splenomegaly. In
older patients an intercurrent illness may increase the rate of red cell destruction
resulting in more acute symptoms.
Severe cases may benefit from splenectomy.

A 2 day old baby is noted to have voiding difficulties and on closer inspection is
noted to have hypospadias. Which of the following abnormalities is most commonly
associated with the condition?
A. Cryptorchidism
B. Diaphragmatic hernia
C. Ventricular - septal defect
D. Bronchogenic cyst
E. Atrial septal defect
Theme from January 2012 Exam
Hypospadias most commonly occurs as an isolated disorder. Associated urological
abnormalities may be seen in up to 40% of infants, of these cryptorchidism is the most
frequent (10%).
Hypospadias
The urethral meatus opens on the ventral surface of the penis. There is also a ventral
deficiency of the foreskin. The uretral meatus may open more proximally in the more
severe variants. However, 75% of the openings are distally located. The incidence is 1
in 300 male births.
Features include:
Absent frenular artery
Ventrally opened glans
Skin tethering to hypoplastic urethra
Splayed columns of spongiosum tissue distal to the meatus
Deficiency of the foreskin ventrally
Management:
No routine cultural circumcisions
Urethroplasty
Penile reconstruction
The foreskin is often utilised in the reconstructive process. In boys with very distal
disease no treatment may be needed.
Theme: Liver lesions
A. Cystadenoma

B. Hyatid cyst
C. Amoebic abscess
D. Mesenchymal hamartoma
E. Liver cell adenoma
F. Cavernous haemangioma
Please select the most likely lesion for the scenario given. Each option may be used
once, more than once or not at all.
7. A 38 year old lady presents with right upper quadrant pain and nausea. She is
otherwise well and her only medical therapy is the oral contraceptive pill which
she has taken for many years with no ill effects. Her liver function tests are
normal. An ultrasound examination demonstrates a hyperechoic well defined
lesion in the left lobe of the liver which measures 14 cm in diameter.
Cavernous haemangioma
Cavernous haemangioma often presents with vague symptoms and signs. They
may grow to considerable size. Liver function tests are usually normal. The
lesions are typically well defined and hyperechoic on ultrasound. A causative
link between OCP use and haemangiomata has yet to be established, but is
possible.
8. A 37 year old lady presents with right upper quadrant pain and nausea. She is
otherwise well and her only medical therapy is the oral contraceptive pill which
she has taken for many years with no ill effects. Her liver function tests and
serum alpha feto protein are normal. An ultrasound examination demonstrates a
4cm non encapsulated lesion in the right lobe of the liver which has a mixed
echoity and heterogeneous texture.
Liver cell adenoma
Liver cell adenomas are linked to OCP use and 90% of patients with liver cell
adenomas have used the OCP. Liver function tests are often normal. The lesions
will typically have a mixed echoity and heterogeneous texture.
9. A 38 year old shepherd presents to the clinic with a 3 month history of malaise
and right upper quadrant pain. On examination he is mildly jaundiced. His liver
function tests demonstrate a mild elevation in bilirubin and transaminases, his
full blood count shows an elevated eosinophil level. An abdominal x-ray is
performed by the senior house officer and demonstrates a calcified lesion in the
right upper quadrant of the abdomen.
Hyatid cyst

Similar theme in September 2011 Exam
Hyatid disease is more common in those who work with sheep or dogs. Liver
function tests may be abnormal and an eosinophilia is often present. Plain
radiographs may reveal a calcified cyst wall.
Benign liver lesions
Benign liver lesions
Haemangioma Most common benign tumours of mesenchymal origin
Incidence in autopsy series is 8%
Cavernous haemangiomas may be enormous
Clinically they are reddish purple hypervascular lesions
Lesions are normally separated from normal liver by ring of
fibrous tissue
On ultrasound they are typically hyperechoic
Liver cell
adenoma
90% develop in women in their third to fifth decade
Linked to use of oral contraceptive pill
Lesions are usually solitary
They are usually sharply demarcated from normal liver
although they usually lack a fibrous capsule
On ultrasound the appearances are of mixed echoity and
heterogeneous texture. On CT most lesions are hypodense
when imaged prior to administration of IV contrast agents
In patients with haemorrhage or symptoms removal of the
adenoma may be required
Mesenchymal
hamartomas
Congential and benign, usually present in infants. May compress
normal liver
Liver abscess Biliary sepsis is a major predisposing factor
Structures drained by the portal venous system form the
second largest source
Common symptoms include fever, right upper quadrant
pain. Jaundice may be seen in 50%
Ultrasound will usually show a fluid filled cavity,
hyperechoic walls may be seen in chronic abscesses
Amoebic abscess Liver abscess is the most common extra intestinal
manifestation of amoebiasis
Between 75 and 90% lesions occur in the right lobe
Presenting complaints typically include fever and right
upper quadrant pain
Ultrasonography will usually show a fluid filled structure
with poorly defined boundaries
Aspiration yield sterile odourless fluid which has an

anchovy paste consistency
Treatment is with metronidazole
Hyatid cysts Seen in cases of Echinococcus infection
Typically an intense fibrotic reaction occurs around sites of
infection
The cyst has no epithelial lining
Cysts are commonly unilocular and may grow to 20cm in
size. The cyst wall is thick and has an external laminated
hilar membrane and an internal enucleated germinal layer
Typically presents with malaise and right upper quadrant
pain. Secondary bacterial infection occurs in 10%.
Liver function tests are usually abnormal and eosinophilia is
present in 33% cases
Ultrasound may show septa and hyatid sand or daughter
cysts.
Percutaneous aspiration is contra indicated
Treatment is by sterilisation of the cyst with mebendazole
and may be followed by surgical resection. Hypertonic
swabs are packed around the cysts during surgery
Polycystic liver
disease
Usually occurs in association with polycystic kidney disease
Autosomal dominant disorder
Symptoms may occur as a result of capsular stretch
Cystadenoma Rare lesions with malignant potential
Usually solitary multiloculated lesions
Liver function tests usually normal
Ultrasonography typically shows a large anechoic, fluid
filled area with irregular margins. Internal echos may result
from septa
Surgical resection is indicated in all cases
A 72 year old man presents with symptoms and signs of benign prostatic hyperplasia.
Which of the following structures is most likely to be enlarged on digital rectal
examination?
A. Posterior lobe of the prostate
B. Median lobe of the prostate
C. Right lateral lobe of the prostate
D. Left lateral lobe of the prostate
E. Anterior lobe of the prostate
Carcinoma of the prostate typically occurs in the posterior lobe. The median lobe is

usually enlarged in BPH. The anterior lobe has little in the way of glandular tissue and
is seldom enlarged.
Benign Prostatic Hyperplasia
Prostatic enlargement occurs in many elderly men
>90% of men aged over 80 will have at least microscopic evidence of benign
prostatic hyperplasia
Pathology As part of the hyperplastic process increase in both stromal and glandular components
are seen. The changes are most notable in the central and periurethral region of the
gland.
Image showing enlarged prostate removed by transvesical prostatectomy with
massive enlargement of the median lobe

Image sourced from Wikipedia
Presentation The vast majority of men will present with lower urinary tract symptoms. These will
typically be:
Poor flow
Nocturia
Hesitancy
Incomplete and double voiding
Terminal dribbling
Urgency
Incontinence
Investigation

Digital rectal examination to assess prostatic size and morphology.
Urine dipstick for infections and haematuria.
Uroflowmetry (a flow rate of >15ml/second helps to exclude BOO)
Bladder pressure studies may help identify detrusor failure and whilst may not
form part of first line investigations should be included in those with atypical
symptoms and prior to redo surgery.
Bladder scanning to demonstrate residual volumes. USS if high pressure
chronic retention.
Management
Lifestyle changes such as stopping smoking and altering fluid intake may help
those with mild symptoms.
Medical therapy includes alpha blockers and 5 alpha reductase inhibitors. The
former work quickly on receptor zones located at the bladder neck.
Cardiovascular side effects are well documented. The latter work on
testosterone metabolising enzymes. Although they have a slower onset of
action, the 5 alpha reductase inhibitors may prevent acute urinary retention.
Surgical therapy includes transurethral resection of the prostate and is the
treatment of choice in those with severe symptoms and those who fail to
respond to medical therapy. More tailored bladder neck incision procedures
may be considered in those with small prostates. Retrograde ejaculation may
occur following surgery. The change in the type of irrigation solutions used
has helped to minimise the TURP syndrome of electrolyte disturbances.
A 58 year old man has been suffering from mechanical back pain for several years.
One morning he awakes from sleep and feels a sudden onset of pain in his back
radiating down his left leg. Which of the following events is most likely to account for
his symptoms?
A. Prolapse of inner annulus fibrosus
B. Prolapse of outer annulus fibrosus
C. Prolapse of nucleus pulposus
D. Rupture of the ligamentum flavum
E. None of the above
Theme from 2009 Exam
Theme from September 2012 Exam
The symptoms would be most likely the result of intervertebral disk prolapse. In disk
prolapse the nucleus pulposus is the structure which usually herniates.
Intervertebral discs

Consist of an outer annulus fibrosus and an inner nucleus pulposus.
The anulus fibrosus consists of several layers of fibrocartilage.
The nucleus pulposus contains loose fibres suspended in a mucoprotein gel
with the consistency of jelly. The nucleus of the disc acts as a shock absorber.
Pressure on the disc causes posterior protrusion of the nucleus pulposus. Most
commonly in the lumbrosacral and lower cervical areas.
The discs are separated by hyaline cartilage.
There is one disc between each pair of vertebrae, except for C1/2 and the
sacrococcygeal vertebrae.
heme: Paediatric neck masses
A. Cystic hygroma
B. Thyroglossal cyst
C. Rhabdomyosarcoma
D. Branchial cyst
E. Dermoid cyst
Please select the most likely underlying diagnosis for the situation that is described.
Each option may be used once, more than once, or not at all.
12. A 2 year old boy is brought to the clinic by his mother who has noticed that he
has developed a small mass. On examination a small smooth cyst is identified
which is located above the hyoid bone. On ultrasound the lesion appears to be a
heterogenous and multiloculated mass.
You answered Thyroglossal cyst
The correct answer is Dermoid cyst
Dermoid cysts are usually multiloculated and heterogeneous. Most are located
above the hyoid and their appearances on imaging differentiate them from
thyroglossal cysts.
13. A 22 month old baby is brought to the clinic by her mother who is concerned
that she has developed a swelling in her neck. On examination she has a soft,
lesion located in the posterior triangle that transilluminates.
Cystic hygroma
Cystic hygromas are soft and transilluminate. Most are located in the posterior
triangle.
14. A 3 year old boy is brought to the clinic by his mother who has noticed a mass
in his neck. On examination he has a smooth mass located on the lateral aspect

of his anterior triangle, near to the angle of the mandible. On ultrasound it has a
fluid filled, anechoic, appearance.
You answered Dermoid cyst
The correct answer is Branchial cyst
Branchial cysts are usually located laterally and derived from the second
branchial cleft. Unless infection has occurred they will usually have an
anechoic appearance on ultrasound.
Neck Masses in Children
Thyroglossal cyst Located in the anterior triangle, usually in the midline
and below the hyoid (65% cases)
Derived from remnants of the thyroglossal duct
Thin walled and anechoic on USS (echogenicity
suggests infection of cyst)
Branchial cyst Six branchial arches separated by branchial clefts
Incomplete obliteration of the branchial apparatus may
result in cysts, sinuses or fistulae
75% of branchial cysts originate from the second
branchial cleft
Usually located anterior to the sternocleidomastoid
near the angle of the mandible
Unless infected the fluid of the cyst has a similar
consistency to water and is anechoic on USS
Dermoids Derived from pleuripotent stem cells and are located
in the midline
Most commonly in a suprahyoid location
They have heterogeneous appearances on imaging and
contain variable amounts of calcium and fat
Thyroid gland True thyroid lesions are rare in children and usually
represent thyroglossal cysts or tumours like lymphoma
Lymphatic
malformations
Usually located posterior to the sternocleidomastoid
Cystic hygroma result from occlusion of lymphatic
channels
The painless, fluid filled, lesions usually present prior
to the age of 2
They are often closely linked to surrounding structures
and surgical removal is difficult

They are typically hypoechoic on USS
Infantile
haemangioma
May present in either triangle of the neck
Grow rapidly initially and then will often
spontaneously regress
Plain x-rays will show a mass lesion, usually
containing calcified phleboliths
As involution occurs the fat content of the lesions
increases
Lymphadenopathy Located in either triangle of the neck
May be reactive or neoplastic
Generalised lymphadenopathy usually secondary to
infection in children (very common)
An unusually tall 43 year old lady presents to the surgical clinic with bilateral inguinal
hernias. She develops chest pain and collapses. As part of her investigations a chest x-
ray shows evidence of mediastinal widening. What is the most likely underlying
diagnosis?
A. Pulmonary embolus
B. Aortic dissection
C. Tietze syndrome
D. Boerhaaves syndrome
E. Myocardial infarct
Marfans syndrome may present with a variety of connective tissue disorders such as
bilateral inguinal hernia. They are at high risk of aortic dissection, as in this case.
Aortic dissection
More common than rupture of the abdominal aorta
33% of patients die within the first 24 hours, and 50% die within 48 hours if
no treatment received
Associated with hypertension
Features of aortic dissection: tear in the intimal layer, followed by formation
and propagation of a subintimal hematoma. Cystic medial necrosis (Marfan's)
Most common site of dissection: 90% occurring within 10 centimetres of the
aortic valve
Stanford Classification

Type Location Treatment
A Ascending aorta/ aortic root Surgery- aortic root replacement
B Descending aorta Medical therapy with antihypertensives
DeBakey classification
Type Site affected
I Ascending aorta, aortic arch, descending aorta
II Ascending aorta only
III Descending aorta distal to left subclavian artery
Clinical features
Tearing, sudden onset chest pain (painless 10%)
Hypertension or Hypotension
A blood pressure difference greater than 20 mm Hg
Neurologic deficits (20%)
Investigations
CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation
trachea/oesophagus
CT (spiral)
MRI
Angiography (95% of patients diagnosed)
Management
Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg.
Urgent surgical intervention: type A dissections. This will usually involve
aortic root replacement.
An unusually tall 43 year old lady presents to the surgical clinic with bilateral inguinal
hernias. She develops chest pain and collapses. As part of her investigations a chest x-
ray shows evidence of mediastinal widening. What is the most likely underlying
diagnosis?
A. Pulmonary embolus
B. Aortic dissection
C. Tietze syndrome
D. Boerhaaves syndrome
E. Myocardial infarct

Marfans syndrome may present with a variety of connective tissue disorders such as
bilateral inguinal hernia. They are at high risk of aortic dissection, as in this case.
Aortic dissection
More common than rupture of the abdominal aorta
33% of patients die within the first 24 hours, and 50% die within 48 hours if
no treatment received
Associated with hypertension
Features of aortic dissection: tear in the intimal layer, followed by formation
and propagation of a subintimal hematoma. Cystic medial necrosis (Marfan's)
Most common site of dissection: 90% occurring within 10 centimetres of the
aortic valve
Stanford Classification
Type Location Treatment
A Ascending aorta/ aortic root Surgery- aortic root replacement
B Descending aorta Medical therapy with antihypertensives
DeBakey classification
Type Site affected
I Ascending aorta, aortic arch, descending aorta
II Ascending aorta only
III Descending aorta distal to left subclavian artery
Clinical features
Tearing, sudden onset chest pain (painless 10%)
Hypertension or Hypotension
A blood pressure difference greater than 20 mm Hg
Neurologic deficits (20%)
Investigations
CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation
trachea/oesophagus
CT (spiral)
MRI
Angiography (95% of patients diagnosed)
Management
Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg.

Urgent surgical intervention: type A dissections. This will usually involve
aortic root replacement.
A 72 year old man has just undergone an emergency repair for a ruptured
abdominal aortic aneurysm. Pre operatively he was taking aspirin, clopidogrel
and warfarin. Intra operatively he received 5000 units of unfractionated
heparin prior to application of the aortic cross clamp. His blood results on
admission to the critical care unit are as follows:
Full blood count
Hb 8 g/dl
Platelets 40 * 109/l
WBC 7.1 * 109/l
His fibrin degradation products are measured and found to be markedly
elevated. Which of the following accounts for these results?
A. Anastomotic leak
B. Disseminated intravascular coagulation
C. Heparin induced thrombocytopenia
D. Adverse effect of warfarin
E. Adverse effects of antiplatelet agents
Theme from April 2012 Exam
The combination of low platelet counts and raised FDP in this setting maked
DIC the most likely diagnosis.
Disseminated intravascular coagulation - Diagnosis
Under homeostatic conditions, coagulation and fibrinolysis are coupled. The
activation of the coagulation cascade yields thrombin that converts fibrinogen
to fibrin; the stable fibrin clot being the final product of hemostasis. The
fibrinolytic system breaks down fibrinogen and fibrin. Activation of the
fibrinolytic system generates plasmin (in the presence of thrombin), which is
responsible for the lysis of fibrin clots. The breakdown of fibrinogen and
fibrin results in polypeptides (fibrin degradation products). In a state of
homeostasis, the presence of plasmin is critical, as it is the central proteolytic
enzyme of coagulation and is also necessary for fibrinolysis.
In DIC, the processes of coagulation and fibrinolysis are dysregulated, and the
result is widespread clotting with resultant bleeding. Regardless of the
triggering event of DIC, once initiated, the pathophysiology of DIC is similar
in all conditions. One critical mediator of DIC is the release of a
transmembrane glycoprotein (tissue factor =TF). TF is present on the surface
of many cell types (including endothelial cells, macrophages, and monocytes)
and is not normally in contact with the general circulation, but is exposed to
the circulation after vascular damage. For example, TF is released in response

to exposure to cytokines (particularly interleukin 1), tumor necrosis factor, and
endotoxin. This plays a major role in the development of DIC in septic
conditions. TF is also abundant in tissues of the lungs, brain, and placenta.
This helps to explain why DIC readily develops in patients with extensive
trauma. Upon activation, TF binds with coagulation factors that then triggers
the extrinsic pathway (via Factor VII) which subsequently triggers the intrinsic
pathway (XII to XI to IX) of coagulation.
Diagnosis Fibrin degradation products are often raised.
Disorder Prothrombin time APTT Bleeding
time
Platelet
count
Warfarin
administration
Prolonged Normal Normal Normal
Aspirin
administration
Normal Normal Prolonged Normal
Heparin Often normal (may be
prolonged)
Prolonged Normal Normal
DIC Prolonged Prolonged Prolonged Low
A 53 year old man from Hong Kong presents with symptoms of fatigue, weight loss
and recurrent epistaxis. Clinical examination reveals left sided cervical
lymphadenopathy and oropharyngeal examination reveals an ulcerated mass in the
naso pharynx. Which of the following viral agents is most commonly implicated in
the development of this condition?
A. Cytomegalovirus
B. Epstein Barr virus
C. Coxsackie virus
D. Herpes simplex virus
E. None of the above
The clinical scenario is most typical for nasopharyngeal carcinoma. An association
with previous Epstein Barr Virus is well established. Infection with the other viruses
listed is not a recognised risk factor for the development of the condition.
Nasopharyngeal carcinoma
Squamous cell carcinoma of the nasopharynx
Rare in most parts of the world, apart from individuals from Southern China
Associated with Epstein Barr virus infection

Presenting features
Systemic Local
Cervical lymphadenopathy Otalgia
Unilateral serous otitis media
Nasal obstruction, discharge and/ or epistaxis
Cranial nerve palsies e.g. III-VI
Imaging Combined CT and MRI.
Treatment Radiotherapy is first line therapy.
An 18 year old male presents with lethargy, night sweats and on examination is found
to have left supraclavicular lymphadenopathy. A surgical registrar performs a left
supraclavicular lymph node biopsy. The pathologist identifies Reed- Sternberg cells
on the subsequent histology sections, what is the most likely diagnosis?
A. Metastatic gastric cancer
B. Hodgkins lymphoma
C. Non Hodgkins lymphoma
D. Tuberculosis
E. None of the above
Reed-Sternberg cells are characteristic histological cell type found in Hodgkins
disease.
Lymphadenopathy
Lymphadenopathy in the neck, axillae, groins and abdomen
Need to note: solitary/multiple, defined/indistinct, hard/rubbery/soft,
tender/painless
Causes of lymphadenopathy
Mnemonic: Hodgkins disease
H aematological: Hodgkins lymphoma, NHL, Leukaemia
O ncological: metastases
D ermatopathic lympadenitis
G aucher's disease
K awasaki disease

I nfections: TB, glandular fever, Syphilis
N iemann Pick disease
S erum sickness
D rug reaction (phenytoin)
I mmunological (SLE)
S arcoidosis
E ndocrinological (Hyperthyroidism)
A ngioimmunoplastic lymphadenopathy
S LE
E osinophilic granulomatosis
Which of the following lesions is least likely to occur in the presence of severe
atrophic gastritis?
A. Duodenal ulcer
B. Gastric cancer
C. Gastric polyp
D. Iron deficiency anaemia
E. Pernicious anaemia
Due the absence of acid a duodenal ulcer is unlikely to occur.
Gastric cancer
Overview There are 700,000 new cases of gastric cancer worldwide each year. It is most
common in Japan and less common in western countries. It is more common in men
and incidence rises with increasing age. The exact cause of many sporadic cancer is
not known, however, familial cases do occur in HNPCC families. In addition,
smoking and smoked or preserved foods increase the risk. Japanese migrants retain
their increased risk (decreased in subsequent generations). The distribution of the
disease in western countries is changing towards a more proximal location (perhaps
due to rising obesity).
Pathology There is some evidence of support a stepwise progression of the disease through
intestinal metaplasia progressing to atrophic gastritis and subsequent dysplasia,
through to cancer. The favoured staging system is TNM. The risk of lymph node
involvement is related to size and depth of invasion; early cancers confined to
submucosa have a 20% incidence of lymph node metastasis. Tumours of the gastro-
oesophageal junction are classified as below:
Type
1
True oesophageal cancers and may be associated with Barrett's oesophagus.
Type
2
Carcinoma of the cardia, arising from cardiac type epithelium
or short segments with intestinal metaplasia at the oesophagogastric junction.

Type
3
Sub cardial cancers that spread across the junction. Involve similar nodal
stations to gastric cancer.
Groups for close endoscopic monitoring
Intestinal metaplasia of columnar type
Atrophic gastritis
Low to medium grade dysplasia
Patients who have previously undergone resections for benign peptic ulcer
disease (except highly selective vagotomy).
Referral to endoscopy
Patients of any age with
dyspepsia and any of the
following
Patients without
dyspepsia
Worsening dyspepsia
Chronic gastrointestinal
bleeding
Dysphagia Barretts oesophagus
Dysphagia Unexplained
abdominal pain or
weight loss
Intestinal metaplasia
Weight loss Vomiting Dysplasia
Iron deficiency anaemia Upper abdominal mass Atrophic gastritis
Upper abdominal mass Jaundice Patient aged over 55 years
with unexplained or persistent
dyspepsia
Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as
shown in the bottom right) may facilitate identification of smaller tumours

Image sourced from Wikipedia
Staging
CT scanning of the chest abdomen and pelvis is the routine first line staging
investigation in most centres.
Laparoscopy to identify occult peritoneal disease
PET CT (particularly for junctional tumours)
Treatment
Proximally sited disease greater than 5-10cm from the OG junction may be
treated by sub total gastrectomy
Total gastrectomy if tumour is <5cm from OG junction
For type 2 junctional tumours (extending into oesophagus)
oesophagogastrectomy is usual
Endoscopic sub mucosal resection may play a role in early gastric cancer
confined to the mucosa and perhaps the sub mucosa (this is debated)
Lymphadenectomy should be performed. A D2 lymphadenectomy is widely
advocated by the Japanese, the survival advantages of extended
lymphadenectomy have been debated. However, the overall recommendation
is that a D2 nodal dissection be undertaken.
Most patients will receive chemotherapy either pre or post operatively.
Prognosis

UK Data
Disease extent Percentage 5 year survival
All RO resections 54%
Early gastric cancer 91%
Stage 1 87%
Stage 2 65%
Stage 3 18%
Operative procedure
Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis
General anaesthesia
Prophylactic intravenous antibiotics
Incision: Rooftop.
Perform a thorough laparotomy to identify any occult disease.
Mobilise the left lobe of the liver off the diaphragm and place a large pack over it.
Insert a large self retaining retractor e.g. omnitract or Balfour (take time with this, the
set up should be perfect). Pack the small bowel away.
Begin by mobilising the omentum off the transverse colon.
Proceed to detach the short gastric vessels.
Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling
device.
Continue the dissection into the lesser sac taking the lesser omentum and left gastric
artery flush at its origin.
The lymph nodes should be removed en bloc with the specimen where possible.
Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull
back on the nasogastric tube. Divide the distal oesophagus and remove the stomach.
The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and
bring a loop of jejunum up to the oesophagus (to check it will reach). Divide the
jejunum at this point. Bring the divided jejunum either retrocolic or antecolic to the
oesophagus. Anastamose the oesophagus to the jejunum, using either interrupted 3/0
vicryl or a stapling device. Then create the remainder of the Roux en Y reconstruction
distally.
Place a jejunostomy feeding tube.
Wash out the abdomen and insert drains (usually the anastomosis and duodenal
stump). Help the anaesthetist insert the nasogastric tube (carefully!)
Close the abdomen and skin.
Enteral feeding may commence on the first post-operative day. However, most
surgeons will leave patients on free NG drainage for several days and keep them nil
by mouth.
A 28 year old man develops an acute paronychia and subsequent spreading sepsis.
The tissue exudate has a higher protein content than normal tissue because?

A. Breakdown of tissue cells release protein
B. Capillary walls are more permeable
C. Increased blood flow transports more protein into the area
D. Intracapillary pressure is raised
E. Plasma cells release gamma globulin
The increased permeability allows the exudation of plasma proteins.
Acute inflammation
Inflammation is the reaction of the tissue elements to injury. Vascular changes occur,
resulting in the generation of a protein rich exudate. So long as the injury does not
totally destroy the existing tissue architecture, the episode may resolve with
restoration of original tissue architecture.
Vascular changes
Vasodilation occurs and persists throughout the inflammatory phase.
Inflammatory cells exit the circulation at the site of injury.
The equilibrium that balances Starlings forces within capillary beds is
disrupted and a protein rich exudate will form as the vessel walls also become
more permeable to proteins.
The high fibrinogen content of the fluid may form a fibrin clot. This has
several important immunomodulatory functions.
Sequelae
Resolution Typically occurs with minimal initial injury
Stimulus removed and normal tissue architecture
results
Organisation Delayed removed of exudate
Tissues undergo organisation and usually fibrosis
Suppuration Typically formation of an abscess or an empyema
Sequestration of large quantities of dead
neutrophils
Progression to chronic
inflammation
Coupled inflammatory and reparative activities
Usually occurs when initial infection or
suppuration has been inadequately managed
Causes

Microbacterial infections e.g. Viruses, exotoxins or endotoxins released by
bacteria
Chemical agents
Physical agents e.g. Trauma
Hypersensitivity reactions
Tissue necrosis
Presence of neutrophil polymorphs is a histological diagnostic feature of acute
inflammation As a busy surgical trainee on the colorectal unit you are given the unenviable task of
reviewing the unit's histopathology results for colonic polyps. Which of the polyp
types described below has the greatest risk of malignancy?
A. Hyperplastic polyp
B. Tubular adenoma
C. Villous adenoma
D. Hamartomatous polyp
E. Serrated polyp
Villous adenomas carry the highest risk of malignant transformation. Hyperplastic
polyps carry little in the way of increased risk. Although, patients with
hamartomatous polyp syndromes may have a high risk of malignancy, the polyps
themselves have little malignant potential.
Colonic polyps
Colonic Polyps May occur in isolation of greater numbers as part of the polyposis syndromes. In FAP
greater than 100 polyps are typically present. The risk of malignancy in association
with adenomas is related to size and is the order of 10% in a 1cm adenoma. Isolated
adenomas seldom give risk of symptoms (unless large and distal). Distally sited
villous lesions may produce mucous and if very large electrolyte disturbances may
occur.
Follow up of colonic polyps
Low risk
1 or 2 adenomas <1cm. No follow up or re-colonoscopy at 5 years.
Moderate risk
3 or 4 small adenomas or 1 adenoma >1cm. Re-scope at 3 years.

High risk
>5 small adenomas or >3 with 1 of them >1cm. Re scope at 1 year.
From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify
patients appropriately and ensure that a complete colonoscopy with good views was
performed.
Segmental resection or complete colectomy should be considered when:
1. Incomplete excision of malignant polyp
2. Malignant sessile polyp
3. Malignant pedunculated polyp with submucosal invasion
4. Polyps with poorly differentiated carcinoma
5. Familial polyposis coli
-Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy
-Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy.
Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery.
A 23 year old man presents to the surgical clinic with an inguinal hernia. On
examination he has a small direct hernia. However, you also notice that he has
pigmented spots around his mouth, on his palms and soles. In his history he
underwent a reduction of an intussusception aged 12 years. Which of the following
lesions is most likely to be identified if a colonoscopy were performed?
A. Hamartomas
B. Tubulovillous adenoma
C. Colorectal cancer
D. Crohns disease
E. Hyperplastic polyps
Theme from April 2012 Exam
He is most likely to have Peutz-Jeghers syndrome which is associated with
Hamartomas.
Peutz-Jeghers syndrome
Peutz-Jeghers syndrome is an autosomal dominant condition characterised by
numerous benign hamartomatous polyps in the gastrointestinal tract. It is also
associated with pigmented freckles on the lips, face, palms and soles. Around 50% of
patients will have died from a gastrointestinal tract cancer by the age of 60 years.
Genetics

Autosomal dominant
Responsible gene encodes serine threonine kinase LKB1 or STK11
Features
Hamartomatous polyps in GI tract (mainly small bowel)
Pigmented lesions on lips, oral mucosa, face, palms and soles
Intestinal obstruction e.g. intussusception (which may lead to diagnosis)
Gastrointestinal bleeding
Management
Conservative unless complications develop
A 56 year old surgeon has been successfully operating for many years. Over
the past few weeks she has begun to notice that her hands are becoming
blistering and weepy. A latex allergy is diagnosed. Which of the following
pathological processes accounts for this scenario?
A. Type 1 hypersensitivity reaction
B. Type 2 hypersensitivity reaction
C. Type 4 hypersensitivity reaction
D. Type 3 hypersensitivity reaction
E. None of the above
Hypersensitivity
reactions: ACID
type 1 --Anaphylactic
type 2 --Cytotoxic
type 3 --Immune complex
type 4 --Delayed
hypersensitivity
Theme from 2012 Exam
Contact dermatitis of a chronic nature is an example of a type 4
hypersensitivity reaction. Type 4 hypersensitivity reactions are cell mediated
rather than antibody mediated.
Hypersensitivity reactions
The Gell and Coombs classification divides hypersensitivity reactions into 4
types
Type I Type II Type III Type IV

Description Anaphylactic Cytotoxic Immune
complex
Delayed type
Mediator IgE IgG, IgM IgG, IgM T-cells
Antigen Exogenous Cell surface Soluble Tissues
Response
time
Minutes Hours Hours 2-3 days
Examples Asthma
Hay fever
Autoimmune
haemolytic anaemia
Pemphigus
Goodpasture's
Serum
sickness
SLE
Aspergillosis
Graft versus host
disease
Contact
dermatitis
A 56 year old motorcyclist is involved in a road traffic accident and sustains a
displaced femoral shaft fracture. Not other injuries are identified on the primary or
secondary surveys. The fracture is treated with closed, antegrade intramedullary
nailing. The following day the patient becomes increasingly agitated and confused.
On examination he is pyrexial, hypoxic SaO2 90% on 6 litres O2, tachycardic and
normotensive. Systemic examination demonstrates a non blanching petechial rash
present over the torso. What is the most likely explanation for this?
A. Pulmonary embolism with paradoxical embolus
B. Fat embolism
C. Meningococcal sepsis
D. Alcohol withdrawl
E. Chronic sub dural haematoma
This man has a recent injury and physical signs that would be concordant with fat
embolism syndrome. Meningococcal sepsis is not usually associated with hypoxia
initially. Pulmonary emboli are not typically associated with pyrexia.
Fat embolism
Diagnosis and clinical features
System Feature
Cardiothoracic Early persistent tachycardia
Tachypnoea, dyspnoea, hypoxia usually 72 hours following
injury
Pyrexia
Dermatological Red/ brown impalpable petechial rash (usually only in 25-
50%)
Subconjunctival and oral haemorrhage/ petechiae
CNS Confusion and agitation

Retinal haemorrhages and intra-arterial fat globules on
fundoscopy
Imaging
May be normal
Fat emboli tend to lodge distally and therefore CTPA may not show any
vascular occlusion, a ground glass appearance may be seen at the periphery
Treatment
Prompt fixation of long bone fractures
Some debate regarding benefit Vs. risk of medullary reaming in femoral shaft/
tibial fractures in terms of increasing risk (probably does not).
DVT prophylaxis
General supportive care
Which of these tumour markers is most helpful in identifying an individual with
hepatocellular carcinoma?
A. Serum AFP
B. Serum CA19-9
C. CEA
D. Beta HCG
E. CA125
Theme from September 2011 Exam
Hepatocellular carcinoma is commonly diagnosed with imaging and an elevated alpha
fetoprotein. Biopsy may seed the tumour and should be avoided. Up to 80% of
hepatocellular carcinoma arise in cirrhotic livers.
Liver tumours
Primary liver tumours The most common primary tumours are cholangiocarcinoma and hepatocellular
carcinoma. Overall metastatic disease accounts for 95% of all liver malignancies
making the primary liver tumours comparatively rare.
Primary liver tumours include:
Cholangiocarcinoma
Hepatocellular carcinoma
Hepatoblastoma

Sarcomas (Rare)
Lymphomas
Carcinoids (most often secondary although primary may occur)
Hepatocellular carcinoma These account for the bulk of primary liver tumours (75% cases). Its worldwide
incidence reflects its propensity to occur on a background of chronic inflammatory
activity. Most cases arise in cirrhotic livers or those with chronic hepatitis B infection,
especially where viral replication is actively occurring. In the UK it accounts for less
than 5% of all cancers, although in parts of Asia its incidence is 100 per 100,000.
The majority of patients (80%) present with existing liver cirrhosis, with a mass
discovered on screening ultrasound.
Diagnosis
CT/ MRI (usually both) are the imaging modalities of choice
a-fetoprotein is elevated in almost all cases
Biopsy should be avoided as it seeds tumours cells through a resection plane.
In cases of diagnostic doubt serial CT and aFP measurements are the preferred
strategy.
Treatment
Patients should be staged with liver MRI and chest, abdomen and pelvic CT
scan.
The testis should be examined in males (testicular tumours may cause raised
AFP). PET CT may be used to identify occult nodal disease.
Surgical resection is the mainstay of treatment in operable cases. In patients
with a small primary tumour in a cirrhotic liver whose primary disease process
is controlled, consideration may be given to primary whole liver resection and
transplantation.
Liver resections are an option but since most cases occur in an already
diseased liver the operative risks and post-operative hepatic dysfunction are
far greater than is seen following metastectomy.
These tumours are not particularly chemo or radiosensitive however, both may
be used in a palliative setting. Tumour ablation is a more popular strategy.
Survival Poor, overall survival is 15% at 5 years.
Cholangiocarcinoma This is the second most common type of primary liver malignancy. As its name
suggests these tumours arise in the bile ducts. Up to 80% of tumours arise in the extra
hepatic biliary tree. Most patients present with jaundice and by this stage the majority
will have disease that is not resectable.
Primary scelerosing cholangitis is the main risk factor. In deprived countries typhoid
and liver flukes are also major risk factors.

Diagnosis
Patients will typically have an obstructive picture on liver function tests.
CA 19-9, CEA and CA 125 are often elevated
CT/ MRI and MRCP are the imaging methods of choice.
Treatment
Surgical resection offers the best chance of cure. Local invasion of peri hilar
tumours is a particular problem and this coupled with lobar atrophy will often
contra indicate surgical resection.
Palliation of jaundice is important, although metallic stents should be avoided
in those considered for resection.
Survival Is poor, approximately 15% 5 year survival.
A 39 year old man has suffered from terminal ileal Crohns disease for the past 20
years. Which condition is he least likely to develop?
A. Gallstones
B. Malabsorption
C. Pyoderma gangrenosum
D. Amyloidosis
E. Feltys syndrome
Felteys syndrome:
Rheumatoid disease
Splenomegaly
Neutropenia
Feltys syndrome is associated with rheumatoid disease. Individuals with long standing
crohns disease are at risk of gallstones because of impairment of the enterohepatic
recycling of bile salts. Formation of entero-enteric fistulation may produce
malabsorption. Amyloidosis may complicate chronic inflammatory states.
Crohns disease
Crohns disease is a chronic transmural inflammation of a segment(s) of the
gastrointestinal tract and may be associated with extra intestinal manifestations.
Frequent disease patterns observed include ileal, ileocolic and colonic disease. Peri-

anal disease may occur in association with any of these. The disease is often
discontinuous in its distribution. Inflammation may cause ulceration, fissures, fistulas
and fibrosis with stricturing. Histology reveals a chronic inflammatory infiltrate that is
usually patchy and transmural.
Ulcerative colitis Vs Crohns
Crohn's disease Ulcerative colitis
Distribution Mouth to anus Rectum and colon
Macroscopic
changes
Cobblestone appearance, apthoid
ulceration
Contact bleeding
Depth of
disease
Transmural inflammation Superficial inflammation
Distribution
pattern
Patchy Continuous
Histological
features
Granulomas (non caseating epithelioid
cell aggregates with Langhans' giant
cells)
Crypt abscesses,
Inflammatory cells in the
lamina propria
Extraintestinal manifestations of Crohns
Related to disease extent Unrelated to disease extent
Aphthous ulcers (10%) Sacroiliiitis (10-15%)
Erythema nodosum (5-10%) Ankylosing spondylitis (1-2%)
Pyoderma gangrenosum (0.5%) Primary sclerosing cholangitis (Rare)
Acute arthropathy (6-12%) Gallstones (up to 30%)
Ocular complications (up to 10%) Renal calculi (up to 10%)
Theme: Renal stones
A. Calcium oxalate
B. Uric acid
C. Cystine
D. Struvite
E. Calcium phosphate
Please select the most likely stone type for each of the following urinary tract stone
scenarios. Each option may be used once, more than once or not at all.
28. A 73 year old lady is undergoing chemotherapy for treatment of acute
leukaemia. She develops symptoms of renal colic. Her urine tests positive for
blood. A KUB x-ray shows no evidence of stones.
Uric acid
Chemotherapy and cell death can increase uric acid levels. In this acute setting
the uric acid stones are unlikely to be coated with calcium and will therefore be

radiolucent.
29. A 16 year old boy presents with renal colic. His parents both have a similar
history of the condition. His urine tests positive for blood. A KUB style x-ray
shows a relatively radiodense stone in the region of the mid ureter.
Cystine
Cystine stones are associated with an inherited metabolic disorder.
30. A 43 year old lady with episodes of recurrent urinary tract sepsis presents with
a staghorn calculus of the left kidney. Her urinary pH is 7.3. A KUB x-ray
shows a faint outline of the calculus.
Struvite
Theme from April 2012 Exam
Chronic infection with urease producing enzymes can produce an alkaline urine
with formation of struvate stone.
Renal stones
Type of
stones
Features Percentage of
all calculi
Calcium
oxalate
Hypercalciuria is a major risk factor (various causes)
Hyperoxaluria may also increase risk
Hypocitraturia increases risk because citrate forms
complexes with calcium making it more soluble
Stones are radio-opaque (though less than calcium
phosphate stones)
Hyperuricosuria may cause uric acid stones to which
calcium oxalate binds
85%
Cystine Inherited recessive disorder of transmembrane cystine
transport leading to decreased absorption of cystine
from intestine and renal tubule
Multiple stones may form
Relatively radiodense because they contain sulphur
1%
Uric acid Uric acid is a product of purine metabolism
May precipitate when urinary pH low
May be caused by diseases with extensive tissue
breakdown e.g. malignancy
More common in children with inborn errors of
metabolism
Radiolucent
5-10%

Calcium
phosphate
May occur in renal tubular acidosis, high urinary pH
increases supersaturation of urine with calcium and
phosphate
Renal tubular acidosis types 1 and 3 increase risk of
stone formation (types 2 and 4 do not)
Radio-opaque stones (composition similar to bone)
10%
Struvite Stones formed from magnesium, ammonium and
phosphate
Occur as a result of urease producing bacteria (and are
thus associated with chronic infections)
Under the alkaline conditions produced, the crystals
can precipitate
Slightly radio-opaque
2-20%
Effect of urinary pH on stone formation Urine pH will show individual variation (from pH 5-7). Post prandially the pH falls as
purine metabolism will produce uric acid. Then the urine becomes more alkaline
(alkaline tide). When the stone is not available for analysis the pH of urine may help
to determine which stone was present.
Stone type Urine acidity Mean urine pH
Calcium phosphate Normal- alkaline >5.5
Calcium oxalate Variable 6
Uric acid Acid 5.5
Struvate Alkaline >7.2
Cystine Normal 6.5
A 64 year old man presents to the clinic with
right upper quadrant discomfort. He has never attended the hospital previously and is
usually well. He has just retired from full time employment as a machinist in a PVC

factory. CT scanning shows a large irregular tumour in the right lobe of his liver.
Which of the following lesions is the most likely?
A. Liposarcoma
B. Angiosarcoma
C. Hamartoma
D. Hyatid liver disease
E. Benign angioma
Angiosarcoma of the liver is a rare tumour. However, it is linked to working with
vinyl chloride, as in this case. Although modern factories minimise the exposure to
this agent, this has not always been the case.
Occupational cancers
Occupational cancers accounted for 5.3% cancer deaths in 2005.
In men the main cancers include:
Mesothelioma
Bladder cancer
Non melanoma skin cancer
Lung cancer
Sino nasal cancer
Occupations with high levels of occupational tumours include:
Construction industry
Working with coal tar and pitch
Mining
Metalworkers
Working with asbestos (accounts for 98% of all mesotheliomas)
Working in rubber industry
Shift work has been linked to breast cancer in women (Health and safety executive
report RR595).
The latency between exposure and disease is typically 15 years for solid tumours and
20 for leukaemia.
Many occupational cancers are otherwise rare. For example sino nasal cancer is an
uncommon tumour, 50% will be SCC. They are linked to conditions such as wood
dust exposure and unlike lung cancer is not strongly linked to cigarette smoking.
Another typical occupational tumour is angiosarcoma of the liver which is linked to

working with vinyl chloride. Again in the non occupational context this is an
extremely rare sporadic tumour.
A 64 year old man presents to the clinic with right upper quadrant discomfort. He has
never attended the hospital previously and is usually well. He has just retired from full
time employment as a machinist in a PVC factory. CT scanning shows a large
irregular tumour in the right lobe of his liver. Which of the following lesions is the
most likely?
A. Liposarcoma
B. Angiosarcoma
C. Hamartoma
D. Hyatid liver disease
E. Benign angioma
Angiosarcoma of the liver is a rare tumour. However, it is linked to working with
vinyl chloride, as in this case. Although modern factories minimise the exposure to
this agent, this has not always been the case.
Occupational cancers
Occupational cancers accounted for 5.3% cancer deaths in 2005.
In men the main cancers include:
Mesothelioma
Bladder cancer
Non melanoma skin cancer
Lung cancer
Sino nasal cancer
Occupations with high levels of occupational tumours include:
Construction industry
Working with coal tar and pitch
Mining
Metalworkers
Working with asbestos (accounts for 98% of all mesotheliomas)
Working in rubber industry
Shift work has been linked to breast cancer in women (Health and safety executive
report RR595).
The latency between exposure and disease is typically 15 years for solid tumours and
20 for leukaemia.

Many occupational cancers are otherwise rare. For example sino nasal cancer is an
uncommon tumour, 50% will be SCC. They are linked to conditions such as wood
dust exposure and unlike lung cancer is not strongly linked to cigarette smoking.
Another typical occupational tumour is angiosarcoma of the liver which is linked to
working with vinyl chloride. Again in the non occupational context this is an
extremely rare sporadic tumour.
A 32 year old man is involved in a house fire and sustains extensive partial thickness
burns to his torso and thigh. Two weeks post operatively he develops oedema of both
lower legs. The most likely cause of this is:
A. Iliofemoral deep vein thrombosis
B. Venous obstruction due to scarring
C. Hypoalbuminaemia
D. Excessive administration of intravenous fluids
E. None of the above
Theme from 2009 Exam
Loss of plasma proteins is the most common cause of oedema developing in this time
frame.
Burns pathology
Extensive burns
Haemolysis due to damage of erythrocytes by heat and microangiopathy
Loss of capillary membrane integrity causing plasma leakage into interstitial
space
Extravasation of fluids from the burn site causing hypovolaemic shock (up to
48h after injury)- decreased blood volume and increased haematocrit
Protein loss
Secondary infection e.g. Staphylococcus aureus
ARDS
Risk of Curlings ulcer (acute peptic stress ulcers)
Danger of full thickness circumferential burns in an extremity as these may
develop compartment syndrome
Healing
Superficial burns: keratinocytes migrate to form a new layer over the burn site
Full thickness burns: dermal scarring. Usually need keratinocytes from skin
grafts to provide optimal coverage.
What is the diagnostic marker for carcinoid syndrome?
A. B-HCG
B. Histamine
C. Chromogranin A
D. 5-Hydroxyindoleacetic acid
E. 5-Hydroxytryptamine
Urinary measurement of 5- HIAA is an important part of clinical follow up.
Carcinoid syndrome
Carcinoid tumours secrete serotonin
Originate in neuroendocrine cells mainly in the intestine (midgut-distal
ileum/appendix)
Can occur in the rectum, bronchi
Hormonal symptoms mainly occur when disease spreads outside the bowel
Clinical features - Onset: years
- Flushing face
- Palpitations
- Tricuspid stenosis causing dyspnoea
- Asthma
- Severe diarrhoea (secretory, persists despite fasting)
Investigation - 5-HIAA in a 24-hour urine collection
- Scintigraphy
- CT scan
Treatment
Octreotide
Surgical removal
A 42 year old man from Southern India presents with chronic swelling of both lower
legs, they are brawny and indurated with marked skin tophic changes. Which of the
following organisms is the most likely origin of this disease process?
A. Loa loa

B. Wuchereria bancrofti
C. Trypanosoma cruzi
D. Trypanosoma gambiense
E. None of the above
W. Bancrofti is the commonest cause of filariasis leading to lymphatic obstruction.
Infection with Loa loa typically occurs in the African sub continent and usually
results in generalised sub cutaneous infections without lymphatic obstruction.
Trypanosomal infections would not produce this clinical picture.
Wuchereria bancrofti
Parasitic filarial nematode
Accounts for 90% of cases of filariasis
Usually diagnosed by blood smears
Usually transmitted by mosquitos
Treatment is with diethylcarbamazine
A 45 year old lady has recently undergone a thyroidectomy for treatment of medullary
thyroid cancer. Which of the following tumour markers is used clinically to screen for
recurrence?
A. Free T3
B. Thyroglobulin
C. Calcitonin
D. Free T4
E. Thyroid stimulating hormone
Theme from 2011 Exam
Calcitonin is clinically utilised to screen for medullary thyroid cancer recurrence.
Thyroid function testing does not form part of either diagnosis or follow up from a
malignancy perspective. However, routine assessment of TSH may be needed in
patients on thyroxine.
Thyroid malignancy
Papillary carcinoma
Commonest sub-type
Accurately diagnosed on fine needle aspiration cytology

Histologically they may demonstrate psammoma bodies (areas of
calcification) and so called 'orphan Annie' nuclei
They typically metastasise via the lymphatics and thus laterally located
apparently ectopic thyroid tissue is usually a metastasis from a well
differentiated papillary carcinoma.
Follicular carcinoma
Are less common than papillary lesions
Like papillary tumours they may present as a discrete nodule. Although they
appear to be well encapsulated macroscopically there invasion on microscopic
evaluation.
Lymph node metastases are uncommon and these tumours tend to spread
haematogenously. This translates into a higher mortality rate.
Follicular lesions cannot be accurately diagnosed on fine needle aspiration
cytology and thus all follicular FNA's will require at least a hemi
thyroidectomy.
Anaplastic carcinoma
Less common and tend to occur in elderly females
Disease is usually advanced at presentation and often only palliative
decompression and radiotherapy can be offered.
Medullary carcinoma
These are tumours of the parafollicular cells ( C Cells) and are of neural crest
origin.
The serum calcitonin may be elevated which is of use when monitoring for
recurrence.
They may be familial and occur as part of the MEN -2A disease spectrum.
Spread may be either lymphatic or haematogenous and as these tumours are
not derived primarily from thyroid cells they are not responsive to radioiodine.
Lymphoma
These respond well to radiotherapy
Radical surgery is unnecessary once the disease has been diagnosed on biopsy
material. Such biopsy material is not generated by an FNA and thus a core
biopsy has to be obtained (with care!).
A 45 year old lady has recently undergone a thyroidectomy for treatment of medullary
thyroid cancer. Which of the following tumour markers is used clinically to screen for
recurrence?

A. Free T3
B. Thyroglobulin
C. Calcitonin
D. Free T4
E. Thyroid stimulating hormone
Theme from 2011 Exam
Calcitonin is clinically utilised to screen for medullary thyroid cancer recurrence.
Thyroid function testing does not form part of either diagnosis or follow up from a
malignancy perspective. However, routine assessment of TSH may be needed in
patients on thyroxine.
Thyroid malignancy
Papillary carcinoma
Commonest sub-type
Accurately diagnosed on fine needle aspiration cytology
Histologically they may demonstrate psammoma bodies (areas of
calcification) and so called 'orphan Annie' nuclei
They typically metastasise via the lymphatics and thus laterally located
apparently ectopic thyroid tissue is usually a metastasis from a well
differentiated papillary carcinoma.
Follicular carcinoma
Are less common than papillary lesions
Like papillary tumours they may present as a discrete nodule. Although they
appear to be well encapsulated macroscopically there invasion on microscopic
evaluation.
Lymph node metastases are uncommon and these tumours tend to spread
haematogenously. This translates into a higher mortality rate.
Follicular lesions cannot be accurately diagnosed on fine needle aspiration
cytology and thus all follicular FNA's will require at least a hemi
thyroidectomy.
Anaplastic carcinoma
Less common and tend to occur in elderly females
Disease is usually advanced at presentation and often only palliative
decompression and radiotherapy can be offered.

Medullary carcinoma
These are tumours of the parafollicular cells ( C Cells) and are of neural crest
origin.
The serum calcitonin may be elevated which is of use when monitoring for
recurrence.
They may be familial and occur as part of the MEN -2A disease spectrum.
Spread may be either lymphatic or haematogenous and as these tumours are
not derived primarily from thyroid cells they are not responsive to radioiodine.
Lymphoma
These respond well to radiotherapy
Radical surgery is unnecessary once the disease has been diagnosed on biopsy
material. Such biopsy material is not generated by an FNA and thus a core
biopsy has to be obtained (with care!).
A 22 year old man is kicked in the head during a rugby match. He is temporarily
concussed, but then regains consciousness. Half an hour later he develops slurred
speech, ataxia and loses consciousnesses. On arrival in hospital he is intubated and
ventilated. A CT Scan is performed which shows an extradural haematoma. What is
the most likely cause?
A. Basilar artery laceration
B. Middle meningeal artery laceration
C. Laceration of the sigmoid sinus
D. Laceration of the anterior cerebral artery
E. Laceration of the middle cerebral artery
Theme based on September 2011 Exam
The most likely vessel from those in the list to cause an acute extra dural haemorrhage
is the middle meningeal artery. The anterior and middle cerebral arteries may cause
acute sub dural haemorrhage. Acute sub dural haemorrhages usually take slightly
longer to evolve than acute extra dural haemorrhages.
Middle meningeal artery
Middle meningeal artery is typically the third branch of the first part of the
maxillary artery, one of the two terminal branches of the external carotid
artery. After branching off the maxillary artery in the infratemporal fossa, it

runs through the foramen spinosum to supply the dura mater (the outermost
meninges) .
The middle meningeal artery is the largest of the three (paired) arteries which
supply the meninges, the others being the anterior meningeal artery and the
posterior meningeal artery.
The middle meningeal artery runs beneath the pterion. It is vulnerable to
injury at this point, where the skull is thin. Rupture of the artery may give rise
to an extra dural hematoma.
In the dry cranium, the middle meningeal, which runs within the dura mater
surrounding the brain, makes a deep indention in the calvarium.
The middle meningeal artery is intimately associated with the
auriculotemporal nerve which wraps around the artery making the two easily
identifiable in the dissection of human cadavers and also easily damaged in
surgery.
A 22 year old man is kicked in the head during a rugby match. He is temporarily
concussed, but then regains consciousness. Half an hour later he develops slurred
speech, ataxia and loses consciousnesses. On arrival in hospital he is intubated and
ventilated. A CT Scan is performed which shows an extradural haematoma. What is
the most likely cause?
A. Basilar artery laceration
B. Middle meningeal artery laceration
C. Laceration of the sigmoid sinus
D. Laceration of the anterior cerebral artery
E. Laceration of the middle cerebral artery
Theme based on September 2011 Exam
The most likely vessel from those in the list to cause an acute extra dural haemorrhage
is the middle meningeal artery. The anterior and middle cerebral arteries may cause
acute sub dural haemorrhage. Acute sub dural haemorrhages usually take slightly
longer to evolve than acute extra dural haemorrhages.
Middle meningeal artery
Middle meningeal artery is typically the third branch of the first part of the
maxillary artery, one of the two terminal branches of the external carotid
artery. After branching off the maxillary artery in the infratemporal fossa, it
runs through the foramen spinosum to supply the dura mater (the outermost
meninges) .
The middle meningeal artery is the largest of the three (paired) arteries which
supply the meninges, the others being the anterior meningeal artery and the
posterior meningeal artery.

The middle meningeal artery runs beneath the pterion. It is vulnerable to
injury at this point, where the skull is thin. Rupture of the artery may give rise
to an extra dural hematoma.
In the dry cranium, the middle meningeal, which runs within the dura mater
surrounding the brain, makes a deep indention in the calvarium.
The middle meningeal artery is intimately associated with the
auriculotemporal nerve which wraps around the artery making the two easily
identifiable in the dissection of human cadavers and also easily damaged in
surgery.
Which of the following is not characteristic of a granuloma?
A. Altered macrophages
B. Fused macrophages
C. Epithelioid cells
D. Mixture of chronic inflammatory cells
E. Polymorphnuclear leucocytes, cellular debris and fibrin
These are typical components of an abscess cavity. Polymorphonuclear leucocytes
may be found in a granuloma if there is a focus of suppuration.
Chronic inflammation
Overview Chronic inflammation may occur secondary to acute inflammation.In most cases
chronic inflammation occurs as a primary process. These may be broadly viewed as
being one of three main processes:
Persisting infection with certain organisms such as Mycobacterium
tuberculosis which results in delayed type hypersensitivity reactions and
inflammation.
Prolonged exposure to non-biodegradable substances such as silica or suture
materials which may induce an inflammatory response.
Autoimmune conditions involving antibodies formed against host antigens.
Acute vs. Chronic inflammation
Acute inflammation Chronic inflammation
Changes to existing vascular structure and
increased permeability of endothelial cells
Angiogenesis predominates
Infiltration of neutrophils Macrophages, plasma cells and
lymphocytes predominate
Process may resolve with: Healing by fibrosis is the main
result

Suppuration
Complete resolution
Abscess formation
Progression to chronic inflammation
Healing by fibrosis
Granulomatous inflammation A granuloma consists of a microscopic aggregation of macrophages (with epithelial
type arrangement =epitheliod). Large giant cells may be found at the periphery of
granulomas.
Mediators Growth factors released by activated macrophages include agents such as interferon
and fibroblast growth factor (plus many more). Some of these such as interferons may
have systemic features resulting in systemic symptoms and signs, which may be
present in individuals with long standing chronic inflammation.
The finding of granulomas is pathognomonic of chronic inflammation, as illustrated
in this biopsy from a patient with colonic Crohns disease
Image sourced from Wikipedia
A 42 year old man presents with a painless lump in the left testicle that he noticed on
self examination. Clinically there is a firm nodule in the left testicle, ultrasound
appearances show an irregular mass lesion. His serum AFP and HCG levels are both
within normal limits. What is the most likely diagnosis?
A. Yolk sack tumour
B. Seminoma
C. Testicular teratoma

D. Epididymo-orchitis
E. Adenomatoid tumour
Seminomas typically have normal AFP and HCG. These are usually raised in
teratomas and yolk sac tumours
This mans age, presenting symptoms and normal tumour markers make a seminoma
the most likely diagnosis. Epididymo-orchitis does not produce irregular mass lesions
which are painless.
Testicular disorders
Testicular cancer Testicular cancer is the most common malignancy in men aged 20-30 years. Around
95% of cases of testicular cancer are germ-cell tumours. Germ cell tumours may
essentially be divided into:
Tumour type Key features Tumour
markers
Pathology
Seminoma Commonest
subtype (50%)
Average age at
diagnosis = 40
Even advanced
disease
associated with
5 year survival
of 73%
AFP usually
normal
HCG
elevated in 10%
seminomas
Lactate
dehydrogenase;
elevated in 10-
20% seminomas
(but also in
many other
conditions)
Sheet like
lobular
patterns of
cells with
substantial
fibrous
component.
Fibrous septa
contain
lymphocytic
inclusions and
granulomas
may be seen.
Non seminomatous germ
cell tumours (42%)
Teratoma
Yolk sac tumour
Choriocarcinoma
Mixed germ cell
tumours (10%)
Younger age at
presentation =20-30
years
Advanced disease
carries worse prognosis
(48% at 5 years)
Retroperitoneal
lymph node dissection
may be needed for
residual disease after
chemotherapy
AFP elevated
in up to 70% of
cases
HCG
elevated in up
to 40% of cases
Other
markers rarely
helpful
Heterogenous
texture with
occasional
ectopic tissue
such as hair
Image demonstrating a classical seminoma, these tumours are typically more uniform
than teratomas

Image sourced from Wikipedia
Risk factors for testicular cancer
Cryptorchidism
Infertility
Family history
Klinefelter's syndrome
Mumps orchitis
Features
A painless lump is the most common presenting symptom
Pain may also be present in a minority of men
Other possible features include hydrocele, gynaecomastia

Diagnosis
Ultrasound is first-line
CT scanning of the chest/ abdomen and pelvis is used for staging
Tumour markers (see above) should be measured
Management
Orchidectomy (Inguinal approach)
Chemotherapy and radiotherapy may be given depending on staging
Abdominal lesions >1cm following chemotherapy may require retroperitoneal
lymph node dissection.
Prognosis is generally excellent
5 year survival for seminomas is around 95% if Stage I
5 year survival for teratomas is around 85% if Stage I
Benign disease
Epididymo-orchitis Acute epididymitis is an acute inflammation of the epididymis, often involving the
testis and usually caused by bacterial infection.
Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or
chlamydia are the usual infections.
Amiodarone is a recognised non infective cause of epididymitis, which
resolves on stopping the drug.
Tenderness is usually confined to the epididymis, which may facilitate
differentiating it from torsion where pain usually affects the entire testis.
Testicular torsion
Twist of the spermatic cord resulting in testicular ischaemia and necrosis.
Most common in males aged between 10 and 30 (peak incidence 13-15 years)
Pain is usually severe and of sudden onset.
Cremasteric reflex is lost and elevation of the testis does not ease the pain.
Treatment is with surgical exploration. If a torted testis is identified then both
testis should be fixed as the condition of bell clapper testis is often bilateral.
A baby is born by normal vaginal delivery at 39 weeks gestation. Initially all appears
well and then the clinical staff become concerned because the baby develops recurrent
episodes of cyanosis. These are worse during feeding and improve dramatically when
the baby cries. The most likely underlying diagnosis is:

A. Choanal atresia
B. Oesophageal reflux
C. Tetralogy of Fallot
D. Oesophageal atresia
E. Congenital diaphragmatic hernia
Question theme from 2011 exam
In Choanal atresia the episodes of cyanosis are usually worst during feeding.
Improvement may be seen when the baby cries as the oropharyngeal airway is used.
Choanal atresia
Congenital disorder with an incidence of 1 in 7000 births.
Posterior nasal airway occluded by soft tissue or bone.
Associated with other congenital malformations e.g. coloboma
Babies with unilateral disease may go unnoticed.
Babies with bilateral disease will present early in life as they are obligate nasal
breathers.
Treatment is with fenestration procedures designed to restore patency.
A 28 year old lady presents with a pigmented lesion on her calf. Excisional biopsy
confirms a diagnosis of melanoma measuring 1cm in diameter with a Breslow
thickness of 0.5mm. The lesion is close <1 mm to all resection margins. Which of the
following surgical resection margins is acceptable for this lesion?
A. 5 cm
B. 1 cm
C. 0.5 cm
D. 2 cm
E. 3 cm
Malignant melanoma
The main diagnostic features (major
criteria):
Secondary features (minor
criteria)

Change in size
Change in shape
Change in colour
Diameter >6mm
Inflammation
Oozing or bleeding
Altered sensation
Treatment
Suspicious lesions should undergo excision biopsy. The lesion should be
removed in completely as incision biopsy can make subsequent
histopathological assessment difficult.
Once the diagnosis is confirmed the pathology report should be reviewed to
determine whether further re-exicision of margins is required (see below):
Margins of excision-Related to Breslow thickness
Lesions 0-1mm thick 1cm
Lesions 1-2mm thick 1- 2cm (Depending upon site and pathological features)
Lesions 2-4mm thick 2-3 cm (Depending upon site and pathological features)
Lesions >4 mm thick 3cm
Marsden J et al Revised UK guidelines for management of Melanoma. Br J Dermatol
2010 163:238-256.
Further treatments such as sentinel lymph node mapping, isolated limb perfusion and
block dissection of regional lymph node groups should be selectively applied.
A 20 year old man is involved in a road traffic accident. Following the incident he is
unable to extend his wrist. However, this improves over the following weeks. Which
type of injury is he most likely to have sustained?
A. Radial nerve neurotmesis
B. Radial nerve neuropraxia
C. Axillary nerve axonotmesis
D. Ulnar nerve neuropraxia
E. Ulnar nerve axonotmesis
Theme from April 2011 Exam
Transient loss of function makes neuropraxia the most likely injury. The wrist
extensors are innervated by the radial nerve making this the most likely site of injury.
Neuropraxia

Nerve intact but electrical conduction is affected
Myelin sheath integrity is preserved
Full recovery
Autonomic function preserved
Wallerian degeneration does not occur
A 53 year old lady has undergone a bilateral breast augmentation procedure
many years previously. The implants are tense and uncomfortable and are
removed. During their removal the surgeon encounters a dense membrane
surrounding the implants, it has a coarse granular appearance. The tissue is
sent for histology and it demonstrates fibrosis with the presence of
calcification. The underlying process responsible for these changes is:
A. Hyperplasia
B. Dysplasia
C. Metastatic calcification
D. Dystrophic calcification
E. Necrosis
Breast implants often become surrounded by a pseudocapsule and this may
secondarily then be subjected to a process of dystrophic calcification.
Pathological calcification
Dystrophic
calcification
Deposition of calcium deposits in tissues that have undergone,
degeneration, damage or disease in the presence of normal serum
calcium levels
Metastatic
calcification
Deposition of calcium deposits in tissues that are otherwise normal
in the presence of increased serum calcium levels
A 4 year old girl presents with symptoms of right sided loin pain, lethargy and
haematuria. On examination she is pyrexial and has a large mass in the right upper
quadrant. The most likely underlying diagnosis is:
A. Perinephric abscess
B. Nephroblastoma
C. Renal cortical adenoma
D. Grawitz tumour
E. Squamous cell carcinoma of the kidney
In a child of this age, with the symptoms described a nephroblastoma is the most
likely diagnosis. A perinephric abscess is most unlikely. If an abscess were to occur it

would be confined to Gertotas fascia in the first instance, and hence anterior extension
would be unlikely.
Nephroblastoma
Nephroblastoma (Wilms tumours)
Usually present in first 4 years of life
May often present as a mass associated with haematuria (pyrexia may occur in
50%)
Often metastasise early (usually to lung)
Treated by nephrectomy
Younger children have better prognosis (<1 year of age =80% overall 5 year
survival)
Theme: Thyroid neoplasms
A. Follicular carcinoma
B. Anaplastic carcinoma
C. Medullary carcinoma
D. Papillary carcinoma
E. Lymphoma
F. Hashimotos thyroiditis
G. Graves disease
For the following histological descriptions please select the most likely underlying
thyroid neoplasm. Each option may be used once, more than once or not at all.
45. A 22 year old female undergoes a thyroidectomy. The resected specimen
shows a non encapsulated tumour with papillary projections and pale empty
nuclei.
Papillary carcinoma
Theme from April 2012
The presence of papillary structures together with the cytoplasmic features
described is strongly suggestive of papillary carcinoma. They are seldom
encapsulated.
46. A thyroidectomy specimen from a 43 year old lady shows a mass with
prominent oxyphil cells and scanty thyroid colloid.
You answered Medullary carcinoma

The correct answer is Follicular carcinoma
Hurthle cell tumours are a variant of follicular neoplasms in which oxyphil
cells predominate. They have a poorer prognosis than conventional follicular
neoplasms
47. A 32 year old lady undergoes a thyroidectomy for a mild goitre. The resected
specimen shows an intense lymphocytic infiltrate with acinar destruction and
fibrosis.
You answered Lymphoma
The correct answer is Hashimotos thyroiditis
Lymphocytic infiltrates and fibrosis are typically seen in Hashimotos
thyroiditis. In Lymphoma only dense lymphatic type tissue is usually present.
Thyroid neoplasms
Lesion Common features
Follicular
adenoma
Usually present as a solitary thyroid nodule
Malignancy can only be excluded on formal histological
assessment
Papillary
carcinoma
Usually contain a mixture of papillary and colloidal filled
follicles
Histologically tumour has papillary projections and pale empty
nuclei
Seldom encapsulated
Lymph node metastasis predominate
Haematogenous metastasis rare
Account for 60% of thyroid cancers
Follicular
carcinoma
May appear macroscopically encapsulated, microscopically
capsular invasion is seen. Without this finding the lesion is a
follicular adenoma.
Vascular invasion predominates
Multifocal disease rare
Account for 20% of all thyroid cancers
Anaplastic
carcinoma
Most common in elderly females
Local invasion is a common feature

Account for 10% of thyroid cancers
Treatment is by resection where possible, palliation may be
achieved through isthmusectomy and radiotherapy.
Chemotherapy is ineffective.
Medullary
carcinoma
Tumours of the parafollicular cells (C Cells)
C cells derived from neural crest and not thyroid tissue
Serum calcitonin levels often raised
Familial genetic disease accounts for up to 20% cases
Both lymphatic and haematogenous metastasis are recognised,
nodal disease is associated with a very poor prognosis.
Theme: Thyroid neoplasms
A. Follicular carcinoma
B. Anaplastic carcinoma
C. Medullary carcinoma
D. Papillary carcinoma
E. Lymphoma
F. Hashimotos thyroiditis
G. Graves disease
For the following histological descriptions please select the most likely underlying
thyroid neoplasm. Each option may be used once, more than once or not at all.
45. A 22 year old female undergoes a thyroidectomy. The resected specimen
shows a non encapsulated tumour with papillary projections and pale empty
nuclei.
Papillary carcinoma
Theme from April 2012
The presence of papillary structures together with the cytoplasmic features
described is strongly suggestive of papillary carcinoma. They are seldom
encapsulated.
46. A thyroidectomy specimen from a 43 year old lady shows a mass with
prominent oxyphil cells and scanty thyroid colloid.
You answered Medullary carcinoma
The correct answer is Follicular carcinoma

Hurthle cell tumours are a variant of follicular neoplasms in which oxyphil
cells predominate. They have a poorer prognosis than conventional follicular
neoplasms
47. A 32 year old lady undergoes a thyroidectomy for a mild goitre. The resected
specimen shows an intense lymphocytic infiltrate with acinar destruction and
fibrosis.
You answered Lymphoma
The correct answer is Hashimotos thyroiditis
Lymphocytic infiltrates and fibrosis are typically seen in Hashimotos
thyroiditis. In Lymphoma only dense lymphatic type tissue is usually present.
Thyroid neoplasms
Lesion Common features
Follicular
adenoma
Usually present as a solitary thyroid nodule
Malignancy can only be excluded on formal histological
assessment
Papillary
carcinoma
Usually contain a mixture of papillary and colloidal filled
follicles
Histologically tumour has papillary projections and pale empty
nuclei
Seldom encapsulated
Lymph node metastasis predominate
Haematogenous metastasis rare
Account for 60% of thyroid cancers
Follicular
carcinoma
May appear macroscopically encapsulated, microscopically
capsular invasion is seen. Without this finding the lesion is a
follicular adenoma.
Vascular invasion predominates
Multifocal disease rare
Account for 20% of all thyroid cancers
Anaplastic
carcinoma
Most common in elderly females
Local invasion is a common feature
Account for 10% of thyroid cancers
Treatment is by resection where possible, palliation may be

achieved through isthmusectomy and radiotherapy.
Chemotherapy is ineffective.
Medullary
carcinoma
Tumours of the parafollicular cells (C Cells)
C cells derived from neural crest and not thyroid tissue
Serum calcitonin levels often raised
Familial genetic disease accounts for up to 20% cases
Both lymphatic and haematogenous metastasis are recognised,
nodal disease is associated with a very poor prognosis.
A 43 year old lady with hypertension is suspected of having a phaeochromocytoma.
Which of the following investigations is most likely to be beneficial in this situation?
A. Dexamethasone suppression test
B. Urinary 5-Hydroxyindoleacetic Acid (5-HIAA)
C. Histamine provocation test
D. Tyramine provocation test
E. Urinary vanillymandelic acid measurements
Theme from September 2011 Exam
Theme from September 2012 Exam
Urinary VMA measurements are not completely specific but constitute first line
assessment. Stimulation tests of any sort are not justified in first line assessments.
Phaeochromocytoma and adrenal lesions
Phaeochromocytoma Neuroendocrine tumour of the chromaffin cells of the adrenal medulla. Hypertension
and hyperglycaemia are often found.
10% of cases are bilateral.
10% occur in children.
11% are malignant (higher when tumour is located outside the adrenal).
10% will not be hypertensive.
Familial cases are usually linked to the Multiple endocrine neoplasia syndromes
(considered under its own heading).
Most tumours are unilateral (often right sided) and smaller than 10cm.
Diagnosis

Urine analysis of vanillymandelic acid (VMA) is often used (false positives may
occur e.g. in patients eating vanilla ice cream!)
Blood testing for plasma metanephrine levels.
CT and MRI scanning are both used to localise the lesion.
Treatment Patients require medical therapy first. An irreversible alpha adrenoreceptor blocker
should be given, although minority may prefer reversible bockade(1). Labetolol may
be co-administered for cardiac chronotropic control. Isolated beta blockade should not
be considered as it will lead to unopposed alpha activity.
These patients are often volume depleted and will often require moderate volumes of
intra venous normal saline perioperatively.
Once medically optimised the phaeochromocytoma should be removed. Most
adrenalectomies can now be performed using a laparoscopic approach(2). The
adrenals are highly vascular structures and removal can be complicated by
catastrophic haemorrhage in the hands of the inexperienced. This is particularly true
of right sided resections where the IVC is perilously close. Should the IVC be
damaged a laparotomy will be necessary and the defect enclosed within a Satinsky
style vascular clamp and the defect closed with prolene sutures. Attempting to
interfere with the IVC using any instruments other than vascular clamps will result in
vessel trauma and make a bad situation much worse.
Incidental adrenal lesions Adrenal lesions may be identified on CT scanning performed for other reasons(3).
Factors suggesting benign disease on CT include(4):
Size less than 3cm
Homogeneous texture
Lipid rich tissue
Thin wall to lesion
All patients with incidental lesions should be managed jointly with an endocrinologist
and full work up as described above. Patients with functioning lesions or those with
adverse radiological features (Particularly size >3cm) should proceed to surgery.
References 1. Weingarten TN, Cata JP, O'Hara JF, Prybilla DJ, Pike TL, Thompson GB, et al.
Comparison of two preoperative medical management strategies for laparoscopic
resection of pheochromocytoma. Urology. 2010 Aug;76(2):508 e6-11.
2. Nguyen PH, Keller JE, Novitsky YW, Heniford BT, Kercher KW. Laparoscopic
approach to adrenalectomy: review of perioperative outcomes in a single center. Am
Surg. 2011 May;77(5):592-6.

3. Ng VW, Ma RC, So WY, Choi KC, Kong AP, Cockram CS, et al. Evaluation of
functional and malignant adrenal incidentalomas. Arch Intern Med. 2010 Dec
13;170(22):2017-20.
4. Muth A, Hammarstedt L, Hellstrom M, Sigurjonsdottir HA, Almqvist E, Wangberg
B. Cohort study of patients with adrenal lesions discovered incidentally. Br J Surg.
2011 May 27.
A 46 year old lady presents with symptoms of diarrhoea, weight loss of 10 Kg and a
skin rash of erythematous blisters involving the abdomen and buttocks. The blisters
have an irregular border and both intact and ruptured vesicles. What is the most likely
diagnosis?
A. Colonic adenocarcinoma
B. Pancreatic adenocarcinoma
C. Tropical sprue
D. Glucagonoma
E. Insulinoma
Theme from September 2011 Exam
Theme from September 2012 Exam
Glucagonoma is strongly associated with necrolytic migratory erythema.
Glucagonoma
Rare pancreatic tumours arising from the alpha cells of the pancreas.
Glucagon levels markedly elevated.
Symptoms include diarrhoea, weight loss and necrolytic migratory erythema.
A serum level of glucagon >1000pg/ml usually suggests the diagnosis,
imaging with CT scanning is also required.
Treatment is with surgical resection.
A 56 year old man presents with symptoms of neuropathic facial pain and some
weakness of the muscles of facial expression on the right side. On examination he has
a hard mass approximately 6cm anterior to the right external auditory meatus. What is
the most likely diagnosis?
A. Pleomorphic adenoma
B. Adenocarcinoma

C. Mucoepidermoid carcinoma
D. Adenoid cystic carcinoma
E. Lymphoma
Theme from September 2011 Exam
The patient is most likely to have a malignant lesion within the parotid. Of the
malignancies listed; adenoid cystic carcinoma has the greatest tendency to perineural
invasion.
Parotid gland malignancy
Most parotid neoplasms (80%) are benign lesions
Most commonly present with painless mass in cheek region
Up to 30% may present with pain, when this is associated with a discrete mass
lesion in the parotid it usually indicates perineural invasion.
Perineural invasion is very unlikely to occur in association with benign lesions
80% of patients with facial nerve weakness caused by parotid malignancies
will have nodal metastasis and a 5 year survival of 25%
Types of malignancy
Mucoepidermoid
carcinoma
30% of all parotid malignancies
Usually low potential for local invasiveness and metastasis
(depends mainly on grade)
Adenoid cystic
carcinoma
Unpredictable growth patter
Tendency for perineural spread
Nerve growth may display skip lesions resulting in incomplete
excision
Distant metastasis more common (visceral rather than nodal
spread)
5 year survival 35%
Mixed tumours Often a malignancy occurring in a previously benign parotid
lesion
Acinic cell carcinoma Intermediate grade malignancy
May show perineural invasion
Low potential for distant metastasis
5 year survival 80%
Adenocarcinoma Develops from secretory portion of gland
Risk of regional nodal and distant metastasis
5 year survival depends upon stage at presentation, may be up
to 75% with small lesions with no nodal involvement
Lymphoma Large rubbery lesion, may occur in association with Warthins
tumours

Diagnosis should be based on regional nodal biopsy rather
than parotid resection Treatment is with chemotherapy (and
radiotherapy)
A 20 year old African lady undergoes an open appendicectomy. She is reviewed for
an unrelated problem 8 months later. On abdominal inspection the wound site is
covered by shiny dark protuberant scar tissue that projects beyond the limits of the
skin incision. Which of the following is the most likely underlying process?
A. Hypertrophic scar
B. Keloid scar
C. Marjolins ulcer
D. Repeated episodes of wound sepsis
E. Mycosis fungoides
Keloid scars extend beyond the limits of the incision. Mycosis fungoides is a
cutaneous T cell lymphoma.
Wound healing
Surgical wounds are either incisional or excisional and either clean, clean
contaminated or dirty. Although the stages of wound healing are broadly similar their
contributions will vary according to the wound type.
The main stages of wound healing include:
Haemostasis
Vasospasm in adjacent vessels, platelet plug formation and generation of
fibrin rich clot.
Inflammation
Neutrophils migrate into wound (function impaired in diabetes).
Growth factors released, including basic fibroblast growth factor and vascular
endothelial growth factor.
Fibroblasts replicate within the adjacent matrix and migrate into wound.
Macrophages and fibroblasts couple matrix regeneration and clot substitution.
Regeneration

Platelet derived growth factor and transformation growth factors stimulate
fibroblasts and epithelial cells.
Fibroblasts produce a collagen network.
Angiogenesis occurs and wound resembles granulation tissue.
Remodeling
Longest phase of the healing process and may last up to one year (or longer).
During this phase fibroblasts become differentiated (myofibroblasts) and these
facilitate wound contraction.
Collagen fibres are remodeled.
Microvessels regress leaving a pale scar.
The above description represents an idealised scenario. A number of diseases may
distort this process. It is obvious that one of the key events is the establishing well
vascularised tissue. At a local level angiogenesis occurs, but if arterial inflow and
venous return are compromised then healing may be impaired, or simply nor occur at
all. The results of vascular compromise are all too evidence in those with peripheral
vascular disease or those poorly constructed bowel anastomoses.
Conditions such as jaundice will impair fibroblast synthetic function and overall
immunity with a detrimental effect in most parts of healing.
Problems with scars:
Hypertrophic scars Excessive amounts of collagen within a scar. Nodules may be present histologically
containing randomly arranged fibrils within and parallel fibres on the surface. The
tissue itself is confined to the extent of the wound itself and is usually the result of a
full thickness dermal injury. They may go on to develop contractures.
Image of hypertrophic scarring. Note that it remains confined to the boundaries of the
original wound:

Image sourced from Wikipedia
Keloid scars Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond
the boundaries of the original injury. They do not contain nodules and may occur
following even trivial injury. They do not regress over time and may recur following
removal.
Image of a keloid scar. Note the extension beyond the boundaries of the original
incision:
Image sourced from Wikipedia
Drugs which impair wound healing:
Non steroidal anti inflammatory drugs

Steroids
Immunosupressive agents
Anti neoplastic drugs
Closure Delayed primary closure is the anatomically precise closure that is delayed for a few
days but before granulation tissue becomes macroscopically evident.
Secondary closure refers to either spontaneous closure or to surgical closure after
granulation tissue has formed.
The pathogenicity of the tubercle bacillus is due to which of the following?
A. Necrosis caused by expanding granulomas
B. Ability to multiply within fibroblasts
C. Delayed hypersensitivity reaction against bacteria
D. Effect of antibody response
E. Direct toxic effect on host cells
Mycobacteria stimulate a specific T cell response of cell mediated immunity. This is
effective in reducing the infection, the delayed hypersensitivity also damages tissues.
Necrosis occurs in TB but is usually within the granuloma.
Tuberculosis pathology
Is a form of primary chronic inflammation, caused by the inability of
macrophages to kill the Mycobacterium tuberculosis.
The macrophages often migrate to regional lymph nodes, the lung lesion plus
affected lymph nodes is referred to as a Ghon complex.
This leads to the formation of a granuloma which is a collection of epithelioid
histiocytes.
There is the presence of caseous necrosis in the centre.
The inflammatory response is mediated by a type 4 hypersensitivity reaction.
In healthy individuals the disease may be contained, in the
immunocompromised disseminated (miliary TB) may occur.
Diagnosis
Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl -
Neelsen staining is typically used.
Culture based methods take far longer.

Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen
method
Image sourced from Wikipedia
A 45 year old women with a thyroid carcinoma undergoes a total thyroidectomy. The
post operative histology report shows a final diagnosis of medullary type thyroid
cancer. Which of the tests below is most likely to be of clinical use in screening for
disease recurrence?
A. Serum CA 19-9 Levels
B. Serum thyroglobulin levels
C. Serum PTH levels
D. Serum calcitonin levels
E. Serum TSH levels
Theme from September 2012 Exam
Medullary thyroid cancers often secrete calcitonin and monitoring the serum levels of
this hormone is useful in detecting sub clinical recurrence.
Thyroid neoplasms
Lesion Common features
Follicular
adenoma
Usually present as a solitary thyroid nodule
Malignancy can only be excluded on formal histological
assessment
Papillary
carcinoma
Usually contain a mixture of papillary and colloidal filled
follicles

Histologically tumour has papillary projections and pale empty
nuclei
Seldom encapsulated
Lymph node metastasis predominate
Haematogenous metastasis rare
Account for 60% of thyroid cancers
Follicular
carcinoma
May appear macroscopically encapsulated, microscopically
capsular invasion is seen. Without this finding the lesion is a
follicular adenoma.
Vascular invasion predominates
Multifocal disease rare
Account for 20% of all thyroid cancers
Anaplastic
carcinoma
Most common in elderly females
Local invasion is a common feature
Account for 10% of thyroid cancers
Treatment is by resection where possible, palliation may be
achieved through isthmusectomy and radiotherapy.
Chemotherapy is ineffective.
Medullary
carcinoma
Tumours of the parafollicular cells (C Cells)
C cells derived from neural crest and not thyroid tissue
Serum calcitonin levels often raised
Familial genetic disease accounts for up to 20% cases
Both lymphatic and haematogenous metastasis are recognised,
nodal disease is associated with a very poor prognosis.
A 15 year old boy undergoes an emergency splenectomy for trauma. He makes a full
recovery and is discharged home. Eight weeks post operatively the general
practitioner performs a full blood count with a blood film. Which of the following is
most likely to be present?
A. Myofibroblasts
B. Howell-Jolly bodies
C. Multinucleate giant cells
D. Reed Sternberg Cells
E. None of the above
Post splenectomy blood
film features:
Howell- Jolly bodies

Pappenheimer bodies
Target cells
Irregular contracted
erythrocytes
As the filtration function is the spleen is no longer present Howell-Jolly bodies are
found.
Post splenectomy blood film changes
The loss of splenic tissue results in the inability to readily remove immature or
abnormal red blood cells from the circulation. The red cell count does not alter
significantly. However, cytoplasmic inclusions may be seen e.g. Howell-Jolly bodies.
In the first few days after splenectomy target cells, siderocytes and reticulocytes will
appear in the circulation. Immediately following splenectomy a granulocytosis
(mainly composed of neutrophils) is seen, this is replaced by a lymphocytosis and
monocytosis over the following weeks.
The platelet count is usually increased and this may be persistent, oral antiplatelet
agents may be needed in some patients.
Image showing Howell Jolly bodies (arrowed)
Image sourced from Wikipedia
A 43 year old women is identified as being a carrier of a BRCA 1 mutation. Apart
from breast cancer, which of the following malignancies is she at greatest risk of
developing?
A. Colonic cancer
B. Ovarian cancer
C. Follicular carcinoma of the thyroid
D. Pituitary adenoma
E. Phaeochromocytoma
BRCA 1 mutation patients are 55% more likely to get ovarian cancer. Those with
BRCA 2 are 25% more likely. The risk of developing other malignancies is slightly
increased but not to the same extent, and not enough to justify screening.
Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.
Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:
*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2
Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age
80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one
of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.

Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5
Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli
A 53 year old man is due to undergo a splenectomy as a treatment for
refractory haemolytic anaemia. The underlying pathological basis for
haemolytic anaemia is thought to be a Type 2 hypersensitivity response.
Which of the following mechanisms best describes this process
A. Deposition of immune complexes
B. Cell mediated immune response
C. IgE mediated response
D. Formation of autoantibodies against cell surface
antigens
E. None of the above
Mnemonic for the reactions and
the mediators involved
ACID EGG-T
Type 1 Anaphylactic
Type 2 Cytotoxic
Type 3 Immune complex
Type 4 Delayed type
EGG T (mediators)
IgE
IgG
IgG
T cells
Type 2 hypersensitivity reactions (which includes haemolytic anaemia) are
associated with formation of antibody against cell surface antigens.
Hypersensitivity reactions
The Gell and Coombs classification divides hypersensitivity reactions into 4
types
Type I Type II Type III Type IV
Description Anaphylactic Cytotoxic Immune
complex
Delayed type
Mediator IgE IgG, IgM IgG, IgM T-cells
Antigen Exogenous Cell surface Soluble Tissues
Response
time
Minutes Hours Hours 2-3 days
Examples Asthma
Hay fever
Autoimmune
haemolytic anaemia
Pemphigus
Goodpasture's
Serum
sickness
SLE
Aspergillosis
Graft versus host
disease
Contact
dermatitis
A 25 year old man is injured in a road traffic accident. His right tibia is fractured and
is managed by fasciotomies and application of an external fixator. Over the next 48
hours his serum creatinine rises and urine is sent for microscopy, muddy brown casts
are identified. What is the most likely underlying diagnosis?
A. Acute interstitial nephritis
B. Acute tubular necrosis
C. Glomerulonephritis
D. IgA Nephropathy
E. Thin basement membrane disease
This patient is likely to have had compartment syndrome (tibial fracture +
fasciotomies) which may produce myoglobinuria. The presence of worsening renal
function, together with muddy brown casts is strongly suggestive of acute tubular
necrosis. Acute interstitial nephritis usually arises from drug toxicity and does not
usually produce urinary muddy brown casts. Thin basement membrane disease is an
autosomal dominant condition that causes persistent microscopic haematuria, but not
worsening renal function.
Acute Renal Failure
Final pathway is tubular cell death.
Renal medulla is a relatively hypoxic environment making it susceptible to
renal tubular hypoxia.
Renovascular autoregulation maintains renal blood flow across a range of
arterial pressures.

Estimates of GFR are best indices of level of renal function. Useful clinical
estimates can be obtained by considering serum creatinine, age, race, gender
and body size. eGFR calculations such as the Cockcroft and Gault equation
are less reliable in populations with high GFR's.
Nephrotoxic stimuli such as aminoglycosides and radiological contrast media
induce apoptosis. Myoglobinuria and haemolysis result in necrosis. Overlap
exists and proinflammatory cytokines play and important role in potentiating
ongoing damage.
Post-operative renal failure is more likely to occur in patients who are elderly,
have peripheral vascular disease, high BMI, have COPD, receive
vasopressors, are on nephrotoxic medication or undergo emergency surgery.
Avoiding hypotension will reduce risk of renal tubular damage.
There is no evidence that administration of ACE inhibitors or dopamine
reduces the incidence of post-operative renal failure.
A 56 year old man has undergone a radical nephrectomy. The pathologist bisects the
kidney and identifies a pink fleshy tumour in the renal pelvis. What is the most likely
disease?
A. Renal cell carcinoma
B. Transitional cell carcinoma
C. Angiomyolipoma
D. Phaeochromocytoma
E. Renal adenoma
Most renal tumours are yellow or brown in colour. TCC's are one of the few tumours
to appear pink.
Theme from April 2012
The finding of a TCC in the renal pelvis mandates a nephroureterectomy.
Renal lesions
Lesion Disease specific features Treatment
Renal cell
carcinoma
Most present with
haematuria (50%)
Common renal tumour (85%
cases)
Paraneoplastic features
include hypertension and
polycythaemia
Most commonly has
haematogenous mestastasis
Usually radical or partial
nephrectomy

Nephroblastoma Rare childhood tumour
It accounts for 80% of all
genitourinary malignancies
in those under the age of 15
years
Up to 90% will have a mass
50% will be hypertensive
Diagnostic work up includes
ultrasound and CT scanning
Surgical resection combined
with chemotherapy (usually
vincristine, actinomycin D
and doxorubicin
Neuroblastoma Most common extracranial
tumour of childhood
80% occur in those under 4
years of age
Tumour of neural crest
origin (up to 50% occur in
the adrenal gland)
The tumour is usually
calcified and may be
diagnosed using MIBG
scanning
Staging is with CT
Surgical resection,
radiotherapy and
chemotherapy
Transitional cell
carcinoma
Accounts for 90% of upper
urinary tract tumour, but
only 10% of renal tumours
Males affected 3x more than
females
Occupational exposure to
industrial dyes and rubber
chemicals may increase risk
Up to 80% present with
painless haematuria
Diagnosis and staging is with
CT IVU
Radical nephroureterectomy
Angiomyolipoma 80% of these hamartoma
type lesions occur
sporadically, the remainder
are seen in those with
tuberous sclerosis
Tumour is composed of
blood vessels, smooth
muscle and fat
Massive bleeding may occur
in 10% of cases
50% of patients with lesions
>4cm will have symptoms
and will require surgical
resection
A 65 year old lady presents with a lesion affecting her right breast. On examination
she has a weeping, crusting lesion overling the right nipple, the areolar region is not

involved. There is no palpable mass lesion in the breast, there is a palpable axillary
lymph node. The patients general practitioner has tried treating the lesion with 1%
hydrocortisone cream, with no success. What is the most likely diagnosis?
A. Infection with Staphylococcus aureus
B. Pagets disease of the nipple
C. Phyllodes tumour
D. Nipple eczema
E. Basal cell carcinoma
A weeping, crusty lesion such as this is most likely to represent Pagets disease of the
nipple (especially since the areolar region is spared). Although no mass lesion is
palpable, a proportion of patients will still have an underlying invasive malignancy
(hence the lymphadenopathy).
Pagets disease of the nipple
Pagets disease is an eczematoid change of the nipple associated with an underlying
breast malignancy and it is present in 1-2% of patients with breast cancer. In half of
these patients, it is associated with an underlying mass lesion and 90% of such
patients will have an invasive carcinoma. 30% of patients without a mass lesion will
still be found to have an underlying carcinoma. The remainder will have carcinoma in
situ.
Pagets disease differs from eczema of the nipple in that it involves the nipple
primarily and only latterly spreads to the areolar (the opposite occurs in eczema).
Diagnosis is made by punch biopsy, mammography and ultrasound of the breast.
Treatment will depend on the underlying lesion.
A 73 year old man presents with haemoptysis and is suspected of suffering from lung
cancer. On examination he has an enlarged supraclavicular lymph node. Which of the
following features is most likely to be present on histological examination?
A. Increased mitoses
B. Apoptosis
C. Barr Bodies
D. Multinucleate giant cells
E. Granuloma

Theme from 2011 Exam
Increased mitoses are commonly seen in association with malignant transformation of
cells. Apoptosis is not a common feature of metastatic cancer. Barr Bodies are formed
during X chromosome inactivation in female somatic cells.
Histopathology of malignancy
Abnormal tissue architecture
Coarse chromatin
Invasion of basement membrane*
Abnormal mitoses
Angiogenesis
De-differentiation
Areas of necrosis
Nuclear pleomorphism
*= Those features that distinguish invasive malignancy from in situ disease
Which of the following pathological explanations best describes the initial
pathological processes occurring in an abdominal aortic aneurysm in an otherwise
well 65 year old, hypertensive male?
A. Loss of elastic fibres from the adventitia
B. Loss of collagen from the adventitia
C. Loss of collagen from the media
D. Loss of elastic fibres from the media
E. Decreased matrix metalloproteinases in the adventitia
Theme from April 2012 Exam
In established aneurysmal disease there is dilation of all layers of the arterial wall and
loss of both elastin and collagen. The primary event is loss of elastic fibres with
subsequent degradation of collagen fibres.
Pathology of abdominal aortic aneurysm
Abdominal aortic aneurysms occur primarily as a result of the failure of elastic
proteins within the extracellular matrix. Anuerysms typically represent dilation of all
layers of the arterial wall. Most aneurysms are caused by degenerative disease. After
the age of 50 years the normal diameter of the infrarenal aorta is 1.5cm in females and
1.7cm in males. Diameters of 3cm and greater, are considered aneurysmal. The
pathophysiology involved in the development of aneurysms is complex and the

primary event is loss of the intima with loss of elastic fibres from the media. This
process is associated with, and potentiated by, increased proteolytic activity and
lymphocytic infiltration.
Major risk factors for the development of aneurysms include smoking and
hypertension. Rare but important causes include syphilis and connective tissues
diseases such as Ehlers Danlos type 1 and Marfans syndrome.
Layers of arterial wall
Image sourced from Wikipedia
A 28 year old lady has a malignant melanoma removed from her calf. Which of the
following pathological criteria carries the greatest prognostic weighting?
A. Vascular invasion
B. Abnormal mitoses
C. Breslow thickness
D. Perineural invasion
E. Lymphocytic infiltrates
Theme from April 2012 Exam
The Breslow thickness has considerable prognostic importance. Lymphocytic
infiltrates may be associated with an improved prognosis, but do not carry nearly the
same weight as increased thickness.
Malignant melanoma
The main diagnostic features (major
criteria):
Secondary features (minor
criteria)

Change in size
Change in shape
Change in colour
Diameter >6mm
Inflammation
Oozing or bleeding
Altered sensation
Treatment
Suspicious lesions should undergo excision biopsy. The lesion should be
removed in completely as incision biopsy can make subsequent
histopathological assessment difficult.
Once the diagnosis is confirmed the pathology report should be reviewed to
determine whether further re-exicision of margins is required (see below):
Margins of excision-Related to Breslow thickness
Lesions 0-1mm thick 1cm
Lesions 1-2mm thick 1- 2cm (Depending upon site and pathological features)
Lesions 2-4mm thick 2-3 cm (Depending upon site and pathological features)
Lesions >4 mm thick 3cm
Marsden J et al Revised UK guidelines for management of Melanoma. Br J Dermatol
2010 163:238-256.
Further treatments such as sentinel lymph node mapping, isolated limb perfusion and
block dissection of regional lymph node groups should be selectively applied.
A 34 year old lady undergoes an elective cholecystectomy for attacks of recurrent
cholecystitis due to gallstones. Microscopic assessment of the gallbladder is most
likely to show which of the following?
A. Dysplasia of the fundus
B. Widespread necrosis
C. Ashoff-Rokitansky sinuses
D. Metaplasia of the fundus
E. None of the above
Aschoff-Rokitansky sinuses are the result of hyperplasia and herniation of epithelial
cells through the fibromuscular layer of the gallbladder wall. They may be
macroscopic or microscopic. Ashoff-Rokitansky sinuses may be identified in cases of
chronic cholecystitis and gallstones. Although gallstones may predispose to the
development of gallbladder cancer the actual incidence of dysplasia and metaplastic
change is rare. In the elective setting described above necrosis would be rare.

Gallbladder
Fibromuscular sac with capacity of 50ml
Columnar epithelium
Relations of the gallbladder
Anterior Liver
Posterior Covered by peritoneum
Transverse colon
1st part of the duodenum
Laterally Right lobe of liver
Medially Quadrate lobe of liver
Arterial supply Cystic artery (branch of Right hepatic artery)
Venous drainage Cystic vein
Nerve supply Sympathetic- mid thoracic spinal cord, Parasympathetic- anterior vagal trunk
Common bile duct
Origin Confluence of cystic and common hepatic ducts
Relations at
origin
Medially - Hepatic artery
Posteriorly- Portal vein
Relations
distally
Duodenum - anteriorly
Pancreas - medially and laterally
Right renal vein - posteriorly
Arterial supply Branches of hepatic artery and retroduodenal branches of
gastroduodenal artery
Calot's triangle
Medially Common hepatic duct
Inferiorly Cystic duct
Superiorly Inferior edge of liver
Contents Cystic artery
Which of the following are not true of Li-Fraumeni syndrome?

A. It consists of mutations to the p53 tumour suppressor gene
B. Is likely to be present in a teenager presenting with a liposarcoma
C. It has an autosomal dominant inheritance pattern
D. Affected individuals are unlikely to develop acute myeloid leukaemia
E. Adrenal malignancies are more common than in normal population
They are at high risk of developing leukaemia.
Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.
Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:
*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2
Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age
80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one

of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.
Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5
Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli
A 35 year old type 1 diabetic presents with difficulty mobilising and back pain
radiating to the thigh. He has a temperature of 39 oC and has pain on extension of the
hip. He is diagnosed with an iliopsoas abscess. Which of the following statements is
false in relation to his diagnosis?
A. Staphylococcus aureus is the most likely primary cause
B. Recurrence occurs in 60% cases
C. More common in males
D. Crohn's is the most likely secondary cause
E. CT guided drainage is preferable first line management
Classical features include: a limp, back pain and fever. Recurrence rates are about 15-
20%. Staphylococcus is the commonest primary cause, others include Streptococcus
and E.coli. Management is ideally by CT guided drainage.
Iliopsoas abscess
Collection of pus in iliopsoas compartment (iliopsoas and iliacus)
Causes:
Primary
Haematogenous spread of bacteria

Staphylococcus aureus: most common
Secondary
Crohn's (commonest cause in this category)
Diverticulitis, Colorectal cancer
UTI, GU cancers
Vertebral osteomyelitis
Femoral catheter, lithotripsy
Endocarditis
Note the mortality rate can be up to 19-20% in secondary iliopsoas abscesses
compared with 2.4% in primary abscesses.
Clinical features
Fever
Back/flank pain
Limp
Weight loss
Clinical examination
Patient in the supine position with the knee flexed and the hip mildly
externally rotated
Specific tests to diagnose iliopsoas inflammation:
Place hand proximal to the patient's ipsilateral knee and ask patient to lift thigh
against your hand. This will cause pain due to contraction of the psoas muscle.
Lie the patient on the normal side and hyperextend the affected hip. In inflammation
this should elicit pain as the psoas muscle is stretched.
Investigation
CT is gold standard
Management
Antibiotics
Percutaneous drainage
Surgery is indicated if:

1. Failure of percutaneous drainage
2. Presence of an another intra-abdominal pathology which requires surgery
Surgical approach The authors technique for draining these collections is given here.
Review the CT scans and plan surgical approach. An extraperitoneal approach is
important.
The collection usually extends inferiorly and can be accessed from an incision at a
level of L4 on the affected side.
GA
Transverse laterally placed incision.
Incise external oblique.
Split the subsequent muscle layers.
As you approach the peritoneum use blunt dissection to pass laterally around it.
Remember the ureter and gonadal veins lie posterior at this level.
Eventually you will enter the abscess cavity, a large amount of pus is usually released
at this point. Drain the area with suction and washout with saline.
Place a corrugated drain well into the abscess cavity.
If you have made a small skin incision it is reasonable to bring the drain up through
the skin wound. Otherwise place a lateral exit site and close the skin and external
oblique. If you do this ensure that you use interrupted sutures.
Anchor the drain with strong securely tied silk sutures (it is extremely tiresome if it
falls out!)
Reference
Iliopsoas abscesses
I H Mallick, M H Thoufeeq, T P Rajendran
Postgrad Med J 2004;80:459-462
Which of the following statements relating to parathyroid neoplasms is incorrect?
A. 15% of cases are due to parathyroid carcinoma
B. 80% of cases are due to parathyroid adenomas
C. Parathyroid adenomas are often encapsulated
D. 10% of parathyroid adenomas develop in ectopically located glands
E. 85% of cases of primary hyperparathyroidism are due to solitary
adenomas
Parathyroid carcinomas account for up to 5% of tumours. Adenomas are often
encapsulated .Lesions that are fibrotic and densely adherent to the gland may be a

carcinoma. 85% cases of primary hyperparathyroidism are due to a single adenoma
and this is the reason some surgeons favour a focussed parathyroidectomy.
Parathyroid glands and disorders of calcium metabolism
Hyperparathyroidism
Disease type Hormone profile Clinical features Cause
Primary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Elevated)
Phosphate
(Low)
Serum Calcium
: Creatinine
clearance ratio
> 0.01
May be
asymptomatic if
mild
Recurrent
abdominal pain
(pancreatitis, renal
colic)
Changes to
emotional or
cognitive state
Most cases due to
solitary adenoma
(80%), multifocal
disease occurs in
10-15% and
parathyroid
carcinoma in 1% or
less
Secondary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Low or
normal)
Phosphate
(Elevated)
Vitamin D
levels (Low)
May have few
symptoms
Eventually may
develop bone
disease, osteitis
fibrosa cystica and
soft tissue
calcifications
Parathyroid gland
hyperplasia occurs
as a result of low
calcium, almost
always in a setting
of chronic renal
failure
Tertiary
hyperparathyroidism
Ca2+ (Normal
or high)
PTH (Elevated)
Phosphate
levels
(Decreased or
Normal)
Vitamin D
(Normal or
decreased)
Alkaline
phosphatase
(Elevated)
Metastatic
calcification
Bone pain and /
or fracture
Nephrolithiasis
Pancreatitis
Occurs as a result
of ongoing
hyperplasia of the
parathyroid glands
after correction of
underlying renal
disorder,
hyperplasia of all 4
glands is usually
the cause
Differential diagnoses It is important to consider the rare but relatively benign condition of benign familial
hypocalciuric hypercalcaemia, caused by an autosomal dominant genetic disorder.
Diagnosis is usually made by genetic testing and concordant biochemistry (Serum
Calcium : Creatinine clearance ratio <0.01-distinguished from primary
hyperparathyroidism).
Treatment

Primary hyperparathyroidism
Indications for surgery
Elevated serum Calcium > 1mg/dL above normal
Hypercalciuria > 400mg/day
Creatinine clearance < 30% compared with normal
Episode of life threatening hypercalcaemia
Nephrolithiasis
Age < 50 years
Neuromuscular symptoms
Reduction in bone mineral density of the femoral neck, lumbar spine, or distal
radius of more than 2.5 standard deviations below peak bone mass (T score
lower than -2.5)
Secondary hyperparathyroidism Usually managed with medical therapy.
Indications for surgery in secondary (renal) hyperparathyroidism:
Bone pain
Persistent pruritus
Soft tissue calcifications
Tertiary hyperparathyroidism Usually treatment is surgical
The presence of an autonomously functioning parathyroid gland may require surgery.
If the culprit gland can be identified then it should be excised. Otherwise total
parathyroidectomy and re-implantation of part of the gland may be required.
References 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical
Management. Surg Clin North Am 2009 Oct;89(5):1227-39.
2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J
Endocrinol 2011; 2011: 251410.
A 20 year old girl presents with a thyroid cancer, she is otherwise well with no
significant family history. On examination she has a nodule in the left lobe of the
thyroid with a small discrete mass separate from the gland itself. Which of the
following is the most likely cause?
A. Follicular carcinoma
B. Anaplastic carcinoma
C. Medullary carcinoma

D. Papillary carcinoma
E. B Cell Lymphoma
Theme from September 2011 Exam
Papillary carcinoma is the most common subtype and may cause lymph node
metastasis (mass separate from the gland itself) that is rare with follicular tumours.
Anaplastic carcinoma would cause more local symptoms and would be rare in this age
group.
Thyroid malignancy
Papillary carcinoma
Commonest sub-type
Accurately diagnosed on fine needle aspiration cytology
Histologically they may demonstrate psammoma bodies (areas of
calcification) and so called 'orphan Annie' nuclei
They typically metastasise via the lymphatics and thus laterally located
apparently ectopic thyroid tissue is usually a metastasis from a well
differentiated papillary carcinoma.
Follicular carcinoma
Are less common than papillary lesions
Like papillary tumours they may present as a discrete nodule. Although they
appear to be well encapsulated macroscopically there invasion on microscopic
evaluation.
Lymph node metastases are uncommon and these tumours tend to spread
haematogenously. This translates into a higher mortality rate.
Follicular lesions cannot be accurately diagnosed on fine needle aspiration
cytology and thus all follicular FNA's will require at least a hemi
thyroidectomy.
Anaplastic carcinoma
Less common and tend to occur in elderly females
Disease is usually advanced at presentation and often only palliative
decompression and radiotherapy can be offered.
Medullary carcinoma
These are tumours of the parafollicular cells ( C Cells) and are of neural crest
origin.

The serum calcitonin may be elevated which is of use when monitoring for
recurrence.
They may be familial and occur as part of the MEN -2A disease spectrum.
Spread may be either lymphatic or haematogenous and as these tumours are
not derived primarily from thyroid cells they are not responsive to radioiodine.
Lymphoma
These respond well to radiotherapy
Radical surgery is unnecessary once the disease has been diagnosed on biopsy
material. Such biopsy material is not generated by an FNA and thus a core
biopsy has to be obtained (with care!).
A 28 year old lady is breast feeding her first child. She presents with discomfort of the
right breast. Clinical examination demonstrates erythema and an area that is fluctuant.
Aspiration and culture of the fluid is most likely to demonstrate infection with which
of the following organisms?
A. Clostridium perfringens
B. Staphylococcus aureus
C. Streptococcus pyogenes
D. Staphylococcus epidermidis
E. Actinomycosis
Theme from 2010 and 2009 Exam
Staphylococcus aureus is the commonest cause. The infants mouth is usually the
source as it damages the nipple areolar complex allowing entry of bacteria.
Breast abscess
In lactational women Staphylococcus aureus is the most common cause
Typical presentation is with a tender mass in a lactating women
There is often tenderness and pain and a fluctuant mass
Diagnosis and treatment is performed using USS and associated drainage of
the abscess cavity. Antibiotics should also be administered
Where there is necrotic skin overlying the abscess, the patient should undergo
surgery

An 18 year old rock climber falls onto his left arm and sustains a large haematoma of
the left upper arm. Unfortunately the wound associated with the injury is neglected
and it becomes infected. Which of the following changes is least likely to occur?
A. Axillary lymphadenopathy
B. Leucopenia
C. Tenderness
D. Mild pyrexia
E. Local formation of yellow pus
Leucopenia would be unusual and should prompt a search for another cause.
Acute inflammation
Inflammation is the reaction of the tissue elements to injury. Vascular changes occur,
resulting in the generation of a protein rich exudate. So long as the injury does not
totally destroy the existing tissue architecture, the episode may resolve with
restoration of original tissue architecture.
Vascular changes
Vasodilation occurs and persists throughout the inflammatory phase.
Inflammatory cells exit the circulation at the site of injury.
The equilibrium that balances Starlings forces within capillary beds is
disrupted and a protein rich exudate will form as the vessel walls also become
more permeable to proteins.
The high fibrinogen content of the fluid may form a fibrin clot. This has
several important immunomodulatory functions.
Sequelae
Resolution Typically occurs with minimal initial injury
Stimulus removed and normal tissue architecture
results
Organisation Delayed removed of exudate
Tissues undergo organisation and usually fibrosis
Suppuration Typically formation of an abscess or an empyema
Sequestration of large quantities of dead
neutrophils

Progression to chronic
inflammation
Coupled inflammatory and reparative activities
Usually occurs when initial infection or
suppuration has been inadequately managed
Causes
Microbacterial infections e.g. Viruses, exotoxins or endotoxins released by
bacteria
Chemical agents
Physical agents e.g. Trauma
Hypersensitivity reactions
Tissue necrosis
Presence of neutrophil polymorphs is a histological diagnostic feature of acute
inflammation Theme: Tumour markers
A. Invasive ductal carcinoma of the breast
B. Prostate cancer
C. Gastric cancer
D. Ovarian cancer
E. Colorectal cancer
F. Pancreatic adenocarcinoma
G. Seminoma testicular cancer
H. Non-seminomatous testicular cancer
I. Hepatocellular carcinoma
For each tumour marker please select the most likely underlying malignancy. Each
option may be used once, more than once or not at all.
13. Raised beta-human chorionic gonadotropin with a raised alpha-feto protein
level
Non-seminomatous testicular cancer
Theme from April 2012 Exam
A raised alpha-feto protein level excludes a seminoma
14. Elevated CA 19-9
Pancreatic adenocarcinoma
15. Raised alpha-feto protein level in a 54-year-old woman
Hepatocellular carcinoma
Tumour markers
Tumour markers may be divided into:
monoclonal antibodies against carbohydrate or glycoprotein tumour antigens
tumour antigens
enzymes (alkaline phosphatase, neurone specific enolase)
hormones (e.g. calcitonin, ADH)
It should be noted that tumour markers usually have a low specificity
Monoclonal antibodies
Tumour marker Association
CA 125 Ovarian cancer
CA 19-9 Pancreatic cancer
CA 15-3 Breast cancer
NB: The breast cancer tumour marker is not specific or sensitive enough to be used
routinely.
Tumour antigens
Tumour marker Association
Prostate specific antigen (PSA) Prostatic carcinoma
Alpha-feto protein (AFP) Hepatocellular carcinoma, teratoma
Carcinoembryonic antigen (CEA) Colorectal cancer
Theme: Benign breast lesions
A. Fibroadenoma
B. Breast abscess
C. Cyst of Montgomery's gland
D. Galactocele
E. Lipoma
F. Duct ectasia

G. Intraductal papilloma
H. Fat necrosis
What is the most likely diagnosis for the scenario given? Each option may be used
once, more than once or not at all.
16. A 64 year old obese female presents with a breast lump. She was hit on the
breast by a cricket ball when playing with her grandson.
Fat necrosis
An obese, post menopausal woman, with a history of trauma points towards
fat necrosis. Trauma causes inflammation of fat cells, leading to formation of
a lump. Mammography will be needed to differentiate it from breast disease.
17. A 21 year old female notices a bloody discharge from the nipple. She is
otherwise well. On examination there are no discrete lesions to feel and
mammography shows dense breast tissue but no mass lesion.
Intraductal papilloma
Intraductal papillomata are the commonest cause of blood stained nipple
discharge in younger women. There is seldom any palpable mass. An
ultrasound is required and possibly a galactogram.
18. A 18 year old female notices a non tender mobile breast lump. Clinically
there is a smooth lump which is not tethered to the skin.
Fibroadenoma
Also called a breast 'mouse' due to its mobility. It is a benign condition
arising from the breast lobule. May enlarge in pregnancy.
Benign Breast lesions
Benign Breast Diseases
Lesion Features Treatment
Fibroadenoma Develop from a whole
lobule
Mobile, firm breast lumps
If >3cm surgical excision is
usual, Phyllodes tumours
should be widely excised

12% of all breast masses
Over a 2 year period up to
30% will get smaller
No increase in risk of
malignancy
(mastectomy if the lesion is
large)
Breast cyst 7% of all Western
females will present with
a breast cyst
Usually presents as a
smooth discrete lump
(may be fluctuant)
Small increased risk of
breast cancer (especially
if younger)
Cysts should be aspirated,
those which are blood stained
or persistantly refill should be
biopsied or excised
Sclerosing adenosis,
(radial scars and
complex sclerosing
lesions)
Usually presents as a
breast lump or breast pain
Causes mammographic
changes which may
mimic carcinoma
Cause distortion of the
distal lobular unit,
without hyperplasia
(complex lesions will
show hyperplasia)
Considered a disorder of
involution, no increase in
malignancy risk
Lesions should be biopsied,
excision is not mandatory
Epithelial
hyperplasia
Variable clinical
presentation ranging from
generalised lumpiness
through to discrete lump
Disorder consists of
increased cellularity of
terminal lobular unit,
atypical features may be
present
Atypical features and
family history of breast
cancer confers greatly
increased risk of
malignancy
If no atypical features then
conservative, those with
atypical features require either
close monitoring or surgical
resection
Fat necrosis Up to 40% cases usually
have a traumatic
aetiology
Physical features usually
Imaging and core biopsy

mimic carcinoma
Mass may increase in size
initially
Duct papilloma Usually present with
nipple discharge
Large papillomas may
present with a mass
The discharge usually
originates from a single
duct
No increase risk of
malignancy
Microdochectomy
A 17 year old man is identified as having a Meckels diverticulum. From which of the
following embryological structures is it derived?
A. Foregut
B. Hindgut
C. Uranchus
D. Cloaca
E. Vitello-intestinal duct
Rule of 2's
2% of population
2 inches (5cm) long
2 feet (60 cm) from the
ileocaecal valve
2 x's more common in men
2 tissue types involved
The Meckels diverticulum is a persistence of the vitello-intestinal duct.
Meckel's diverticulum
Congenital abnormality resulting in incomplete obliteration of the vitello-
intestinal duct
Normally, in the foetus, there is an attachment between the vitello-intestinal
duct and the yolk sac.This disappears at 6 weeks gestation.
The tip is free in majority of cases.
Associated with enterocystomas, umbilical sinuses, and omphaloileal fistulas.
Arterial supply: omphalomesenteric artery.

2% of population, 2 inches long, 2 feet from the ileocaecal valve.
Typically lined by ileal mucosa but ectopic gastric mucosa can occur, with the
risk of peptic ulceration. Pancreatic and jejunal mucosa can also occur.
Clinical
Normally asymptomatic and an incidental finding.
Complications are the result of obstruction, ectopic tissue, or inflammation.
Removal if narrow neck or symptomatic. Options are between wedge excision
or formal small bowel resection and anastomosis.
Theme: Rectal bleeding
A. Solitary rectal ulcer syndrome
B. Haemorroidal disease
C. Fissure in ano
D. Fistula in ano
E. Anal cancer
F. Ulcerative colitis
Please select the most likely diagnosis for the scenario given. Each option may be
used once, more than once or not at all.
20. A 22 year old man presents with a 6 day history of passage of bloody
diarrhoea with passage of mucous and slime. He is passing an average of 8 to
9 bowel movements per day. On digital rectal examination there is no discrete
abnormality to feel, but there is some blood stained mucous on the glove.
Ulcerative colitis
The passage of bloody diarrhoea together with mucous and a short history
makes this a likely first presentation of inflammatory bowel disease.
21. A 17 year old man presents with a 2 week history of significant pain on
defecation accompanied by the presence of a small amount of blood which is
noticed on toilet paper.
Fissure in ano
Young patients with painful rectal bleeding may have a fissure. Treatment is
with stool softeners and either GTN or Diltiazem initially.

22. A 24 year old women presents with a long history of obstructed defecation
and chronic constipation. She often strains to open her bowels for long
periods and occasionally notices that she has passed a small amount of blood.
On examination she has an indurated area located anteriorly approximately
3cm proximal to the anal verge.
Solitary rectal ulcer syndrome
Solitary rectal ulcers are associated with chronic constipation and straining. It
will need to be biopsied to exclude malignancy (the histological appearances
are characteristic). Diagnostic work up should include endoscopy and
probably defecating proctogram and ano-rectal manometry studies.
Rectal bleeding
Rectal bleeding is a common cause for patients to be referred to the surgical clinic. In
the clinical history it is useful to try and localise the anatomical source of the blood.
Bright red blood is usually of rectal anal canal origin, whilst dark red blood is more
suggestive of a proximally sited bleeding source. Blood which has entered the GI tract
from a gastro-duodenal source will typically resemble malaena due to the effects of
the digestive enzymes on the blood itself.
In the table below we give some typical bleeding scenarios together with physical
examination findings and causation.
Cause Type of
bleeding
Features in history Examination findings
Fissure in
ano
Bright red
rectal
bleeding
Painful bleeding that occurs
post defecation in small
volumes. Usually antecedent
features of constipation
Muco-epithelial defect
usually in the midline
posteriorly (anterior fissures
more likely to be due to
underlying disease)
Haemorroids Bright red
rectal
bleeding
Post defecation bleeding
noted both on toilet paper
and drips into pan. May be
alteration of bowel habit and
history of straining. No
blood mixed with stool. No
local pain.
Normal colon and rectum.
Proctoscopy may show
internal haemorrhoids.
Internal haemorrhoids are
usually impalpable.
Crohns
disease
Bright red
or mixed
blood
Bleeding that is
accompanied by other
symptoms such as altered
bowel habit, malaise, history
of fissures (especially
Perineal inspection may
show fissures or fistulae.
Proctoscopy may
demonstrate indurated
mucosa and possibly

anterior) and abscesses. strictures. Skip lesions may
be noted at colonoscopy.
Ulcerative
colitis
Bright red
bleeding
often mixed
with stool
Diarrhoea, weight loss,
nocturnal incontinence,
passage of mucous PR.
Proctitis is the most marked
finding. Peri anal disease is
usually absent. Colonoscopy
will show continuous
mucosal lesion.
Rectal
cancer
Bright red
blood
mixed
volumes
Alteration of bowel habit.
Tenesmus may be present.
Symptoms of metastatic
disease.
Usually obvious mucosal
abnormality. Lesion may be
fixed or mobile depending
upon disease extent.
Surrounding mucosa often
normal, although polyps may
be present.
Image showing a fissure in ano. Typically these are located posteriorly and in the
midline. Fissures at other sites may be associated with underlying disease.
Image sourced from Wikipedia
Colonoscopic image of internal haemorroids. Note these may often be impalpable.

Image sourced from Wikipedia
Investigation
All patients presenting with rectal bleeding require digital rectal examination
and procto-sigmoidoscopy as a minimal baseline.
Remember that haemorrhoids are typically impalpable and to attribute
bleeding to these in the absence of accurate internal inspection is
unsatisfactory.
In young patients with no other concerning features in the history a carefully
performed sigmoidoscopy that demonstrates clear haemorrhoidal disease may
be sufficient. If clear views cannot be obtained then patients require bowel
preparation with an enema and a flexible sigmoidscopy performed.
In those presenting with features of altered bowel habit or suspicion of
inflammatory bowel disease a colonoscopy is the best test.
Patients with excessive pain who are suspected of having a fissure may require
an examination under general or local anaesthesia.
In young patients with external stigmata of fissure and a compatible history it
is acceptable to treat medically and defer internal examination until the fissure
is healed. If the fissure fails to heal then internal examination becomes
necessary along the lines suggested above to exclude internal disease.
Special tests
In patients with a malignancy of the rectum the staging investigations
comprise an MRI of the rectum to identify circumferential resection margin
compromise and to identify mesorectal nodal disease. In addition to this CT
scanning of the chest abdomen and pelvis is necessary to stage for more

distant disease. Some centres will still stage the mesorectum with endo rectal
ultrasound but this is becoming far less common.
Patients with fissure in ano who are being considered for surgical
sphincterotomy and are females who have an obstetric history should probably
have ano rectal manometry testing performed together with endo anal
ultrasound. As this service is not universally available it is not mandatory but
in the absence of such information there are continence issues that may arise
following sphincterotomy.
Management
Disease Management
Fissure in ano GTN ointment 0.2% or diltiazem cream applied topically is the usual
first line treatment. Botulinum toxin for those who fail to respond.
Internal sphincterotomy for those who fail with botox, can be
considered at the botox stage in males.
Haemorroids Lifestyle advice, for small internal haemorrhoids can consider
injection sclerotherapy or rubber band ligation. For external
haemorrhoids consider haemorrhoidectomy. Modern options include
HALO procedure and stapled haemorrhoidectomy.
Inflammatory
bowel disease
Medical management- although surgery may be needed for
fistulating Crohns (setons).
Rectal cancer Anterior resection or abdomino-perineal excision of the colon and
rectum. Total mesorectal excision is now standard of care. Most
resections below the peritoneal reflection will require defunctioning
ileostomy. Most patients will require preoperative radiotherapy.
Which of the following is the most common childhood brain tumour?
A. Glioblastoma multiforme
B. Astrocytoma
C. Medulloblastoma
D. Ependymoma
E. Meningioma
Glioblastoma multiforme is rare in childhood. In contrast, medulloblastoma (more
correctly termed primitive neuroectodermal tumours) is the commonest brain tumour
in children, and the 2nd commonest malignant solid neoplasm in children.

CNS tumours
60% = Glioma and metastatic disease
20% = Meningioma
10% = Pituitary lesions
In paediatric practice medulloblastomas (neuroectodermal tumours) are the
commonest lesion, they are very rare in adults.
Tumours arising in right temporal and frontal lobe may reach considerable size before
becoming symptomatic. Whereas tumours in the speech and visual areas will typically
produce early symptoms.
Diagnosis MRI Scanning provides the best resolution.
Treatment Usually surgery, even if tumour cannot be completely resected conditions such as
rising ICP can be addressed with tumour debulking and survival and quality of life
prolonged.
Curative surgery can usually be undertaken with lesions such as meningiomas.
Gliomas have a marked propensity to invade normal brain and resection of these
lesions is nearly always incomplete.
A keen surgical trainee is about to embark on her first hemi arthroplasty for a
fractured neck of femur. In the anaesthetic room the patient is given 1.2g intravenous
co-amoxiclav. There is a possible history of penicillin allergy but the patient is
demented and the history is not checked. The patient then develops severe respiratory
compromise and haemodynamic collapse. Which of the following pathological
processes accounts for this event?
A. Binding of the drug to circulating IgG class antibodies
B. Recognition of the drug by IgE receptors on mast cells
C. Drug initiated formation of hapten-protein complexes
D. Binding of the drug to circulating IgM class antibodies
E. None of the above
Anaphylactic shock:
Antigen recognised by IgE molecules on the surface of mast cells resulting in rapid
degranulation with release of histamine and other inflammatory cytokines.
This is a case of anaphylactic shock. In anaphylaxis the mast cells degranulate.
Anaphylactic shock

Suspect if there has been exposure to an allergen
Management
- Remove allergen
- ABCD
- Drugs:
Adrenaline 1:1000 0.5ml INTRAMUSCULARLY (not IV). Repeat after 5 mins if no
response.
Then Chlorpheniramine 10mg IV
Then Hydrocortisone 100-200mg IV
Reference Emergency treatment of anaphylactic reactions. Guidelines for healthcare providers.
Working Group of the Resuscitation Council (UK).2008
Which of the following hepatobiliary disorders are most classically associated with
ulcerative colitis?
A. Gallstones
B. Primary sclerosing cholangitis
C. Bile duct stones
D. Liver hamartomas
E. Hepatocellular carcinoma
Primary sclerosing cholangitis is an idiopathic inflammation of the bile ducts. It may
result in episodes of cholestasis and cholangitis and ultimately result in the need for
liver transplantation. It carries a 10% risk of malignant transformation. Crohns disease
is associated with gallstones due to impaired entero-hepatic circulation. Apart from
PSC, ulcerative colitis does not increase the risk of other liver lesions.
Ulcerative colitis
Ulcerative colitis is a form of inflammatory bowel disease. Inflammation always starts
at rectum, never spreads beyond ileocaecal valve and is continuous. The peak
incidence of ulcerative colitis is in people aged 15-25 years and in those aged 55-65
years. It is less common in smokers.
The initial presentation is usually following insidious and intermittent symptoms.
Features include:
bloody diarrhoea

urgency
tenesmus
abdominal pain, particularly in the left lower quadrant
extra-intestinal features (see below)
Questions regarding the 'extra-intestinal' features of inflammatory bowel disease are
common. Extra-intestinal features include sclerosing cholangitis, iritis and ankylosing
spondylitis.
{Common to both Crohn's
disease (CD) and Ulcerative
colitis (UC)}
{Notes}
{Related to
disease activity}
Arthritis: pauciarticular,
asymmetric
Erythema nodosum
Episcleritis
Osteoporosis
Arthritis is the most common
extra-intestinal feature in both
CD and UC
Episcleritis is more common in
CD
{Unrelated to
disease activity}
Arthritis: polyarticular,
symmetric
Uveitis
Pyoderma gangrenosum
Clubbing
Primary sclerosing cholangitis
Primary sclerosing cholangitis is
much more common in UC
Uveitis is more common in UC
Pathology
red, raw mucosa, bleeds easily
no inflammation beyond submucosa (unless fulminant disease)
widespread superficial ulceration with preservation of adjacent mucosa which
has the appearance of polyps ('pseudopolyps')
inflammatory cell infiltrate in lamina propria
neutrophils migrate through the walls of glands to form crypt abscesses
depletion of goblet cells and mucin from gland epithelium
granulomas are infrequent
Barium enema
loss of haustrations
superficial ulceration, 'pseudopolyps'
long standing disease: colon is narrow and short -'drainpipe colon'
Endoscopy
Superficial inflammation of the colonic and rectal mucosa
Continuous disease from rectum proximally
Superifical ulceration, mucosal islands, loss of vascular definition and
continuous ulceration pattern.
Management
Patients with long term disease are at increased risk of development of
malignancy
Acute exacerbations are generally managed with steroids, in chronic patients
agents such as azathioprine and infliximab may be used
Individuals with medically unresponsive disease usually require surgery- in
the acute phase a sub total colectomy and end ileostomy. In the longer term a
proctectomy will be required. An ileoanal pouch is an option for selected
patients
Which of the following hepatobiliary disorders are most classically associated with
ulcerative colitis?
A. Gallstones
B. Primary sclerosing cholangitis
C. Bile duct stones
D. Liver hamartomas
E. Hepatocellular carcinoma
Primary sclerosing cholangitis is an idiopathic inflammation of the bile ducts. It may
result in episodes of cholestasis and cholangitis and ultimately result in the need for
liver transplantation. It carries a 10% risk of malignant transformation. Crohns disease
is associated with gallstones due to impaired entero-hepatic circulation. Apart from
PSC, ulcerative colitis does not increase the risk of other liver lesions.
Ulcerative colitis
Ulcerative colitis is a form of inflammatory bowel disease. Inflammation always starts
at rectum, never spreads beyond ileocaecal valve and is continuous. The peak
incidence of ulcerative colitis is in people aged 15-25 years and in those aged 55-65
years. It is less common in smokers.
The initial presentation is usually following insidious and intermittent symptoms.
Features include:
bloody diarrhoea
urgency
tenesmus

abdominal pain, particularly in the left lower quadrant
extra-intestinal features (see below)
Questions regarding the 'extra-intestinal' features of inflammatory bowel disease are
common. Extra-intestinal features include sclerosing cholangitis, iritis and ankylosing
spondylitis.
{Common to both Crohn's
disease (CD) and Ulcerative
colitis (UC)}
{Notes}
{Related to
disease activity}
Arthritis: pauciarticular,
asymmetric
Erythema nodosum
Episcleritis
Osteoporosis
Arthritis is the most common
extra-intestinal feature in both
CD and UC
Episcleritis is more common in
CD
{Unrelated to
disease activity}
Arthritis: polyarticular,
symmetric
Uveitis
Pyoderma gangrenosum
Clubbing
Primary sclerosing cholangitis
Primary sclerosing cholangitis is
much more common in UC
Uveitis is more common in UC
Pathology
red, raw mucosa, bleeds easily
no inflammation beyond submucosa (unless fulminant disease)
widespread superficial ulceration with preservation of adjacent mucosa which
has the appearance of polyps ('pseudopolyps')
inflammatory cell infiltrate in lamina propria
neutrophils migrate through the walls of glands to form crypt abscesses
depletion of goblet cells and mucin from gland epithelium
granulomas are infrequent
Barium enema
loss of haustrations
superficial ulceration, 'pseudopolyps'
long standing disease: colon is narrow and short -'drainpipe colon'
Endoscopy
Superficial inflammation of the colonic and rectal mucosa
Continuous disease from rectum proximally
Superifical ulceration, mucosal islands, loss of vascular definition and
continuous ulceration pattern.

Management
Patients with long term disease are at increased risk of development of
malignancy
Acute exacerbations are generally managed with steroids, in chronic patients
agents such as azathioprine and infliximab may be used
Individuals with medically unresponsive disease usually require surgery- in
the acute phase a sub total colectomy and end ileostomy. In the longer term a
proctectomy will be required. An ileoanal pouch is an option for selected
patients
Which of the following is not associated with thrombosis?
A. Endothelial cell damage
B. Use of tourniquets in surgery
C. Formation of platelet aggregates
D. Thrombocytopenia
E. Carcinoma of the stomach
All the other options either act directly to promote thrombosis e.g. endothelial cell
damage or via changes in consistency or flow of blood.
Abnormal coagulation
Cause Factors affected
Heparin Prevents activation factors 2,9,10,11
Warfarin Affects synthesis of factors 2,7,9,10
DIC Factors 1,2,5,8,11
Liver disease Factors 1,2,5,7,9,10
Interpretation blood clotting test results
Disorder APTT PT Bleeding time
Haemophilia Increased Normal Normal
von Willebrand's disease Increased Normal Increased
Vitamin K deficiency Increased Increased Normal
Which of the following is not associated with thrombosis?

A. Endothelial cell damage
B. Use of tourniquets in surgery
C. Formation of platelet aggregates
D. Thrombocytopenia
E. Carcinoma of the stomach
All the other options either act directly to promote thrombosis e.g. endothelial cell
damage or via changes in consistency or flow of blood.
Abnormal coagulation
Cause Factors affected
Heparin Prevents activation factors 2,9,10,11
Warfarin Affects synthesis of factors 2,7,9,10
DIC Factors 1,2,5,8,11
Liver disease Factors 1,2,5,7,9,10
Interpretation blood clotting test results
Disorder APTT PT Bleeding time
Haemophilia Increased Normal Normal
von Willebrand's disease Increased Normal Increased
Vitamin K deficiency Increased Increased Normal
A 16 year old boy develops a painful swelling of his distal femur. An osteoblastic
sarcoma is diagnosed. To which of the following sites is this lesion most likely to
metastasise?
A. Inguinal lymph nodes
B. Common iliac lymph nodes
C. Liver
D. Brain
E. Lung
Sarcomas in which Lymphatic
Metastasis is seen:

'RACE For MS'
R: Rhabdomyosarcoma
A: Angiosarcoma
C: Clear cell sarcoma
E: Epithelial cell sarcoma
For: Fibrosarcoma
M: Malignant fibrous histiocytoma
S: Synovial cell sarcoma
Or
'SCARE'
Synovial sarcoma
Clear cell sarcoma
Angiosarcoma
Rhabdomyosarcoma
Epithelioid sarcoma
Sarcomas often metastasise via the haematogenous route and the lung is a common
site for sarcoma metastasis. The liver and brain are often spared (at least initially). A
smaller number may develop lymphatic metastasis (see above).
Sarcomas
Malignant tumours of mesenchymal origin
Types May be either bone or soft tissue in origin.
Bone sarcoma include:
Osteosarcoma
Ewings sarcoma (although non bony sites recognised)
Chrondrosarcoma - originate from Chondrocytes
Soft tissue sarcoma are a far more heterogeneous group and include:
Liposarcoma-adipocytes
Rhabdomyosarcoma-striated muscle
Leiomyosarcoma-smooth muscle
Synovial sarcomas- close to joints (cell of origin not known but not synovium)
Malignant fibrous histiocytoma is a sarcoma that may arise in both soft tissue and

bone.
Features Certain features of a mass or swelling should raise suspicion for a sarcoma these
include:
Large >5cm soft tissue mass
Deep tissue location or intra muscular location
Rapid growth
Painful lump
Assessment Imaging of suspicious masses should utilise a combination of MRI, CT and USS.
Blind biopsy should not be performed prior to imaging and where required should be
done in such a way that the biopsy tract can be subsequently included in any
resection.
Ewings sarcoma
Commoner in males
Incidence of 0.3 / 1, 000, 000
Onset typically between 10 and 20 years of age
Location by femoral diaphysis is commonest site
Histologically it is a small round tumour
Blood borne metastasis is common and chemotherapy is often combined with
surgery
Osteosarcoma
Mesenchymal cells with osteoblastic differentiation
20% of all primary bone tumours
Incidence of 5 per 1,000,000
Peak age 15-30, commoner in males
Limb preserving surgery may be possible and many patients will receive
chemotherapy
Liposarcoma
Malignancy of adipocytes
Rare approximately 2.5 per 1,000,000. They are the second most common soft
tissue sarcoma
Typically located in deep locations such as retroperitoneum
Affect older age group usually >40 years of age
May be well differentiated and thus slow growing although may undergo
dedifferentiation and disease progression
Many tumours will have a pseudocapsule that can misleadingly allow
surgeons to feel that they can 'shell out' these lesions. In reality tumour may

invade at the edge of the pseudocapsule and result in local recurrence if this
strategy is adopted
Usually resistant to radiotherapy although this is often used in a palliative
setting
Malignant Fibrous Histiocytoma
Tumour with large number of histiocytes
Most common sarcoma in adults
Also described as undifferentiated pleomorphic sarcoma NOS (i.e. Cell of
origin is not known)
Four major subtypes are recognised: storiform-pleomorphic (70% cases),
myxoid (less aggressive), giant cell and inflammatory
Treatment is usually with surgical resection and adjuvant radiotherapy as this
reduces the likelihood of local recurrence
A 16 year old boy develops a painful swelling of his distal femur. An osteoblastic
sarcoma is diagnosed. To which of the following sites is this lesion most likely to
metastasise?
A. Inguinal lymph nodes
B. Common iliac lymph nodes
C. Liver
D. Brain
E. Lung
Sarcomas in which Lymphatic
Metastasis is seen:
'RACE For MS'
R: Rhabdomyosarcoma
A: Angiosarcoma
C: Clear cell sarcoma
E: Epithelial cell sarcoma
For: Fibrosarcoma
M: Malignant fibrous histiocytoma
S: Synovial cell sarcoma
Or
'SCARE'
Synovial sarcoma
Clear cell sarcoma
Angiosarcoma
Rhabdomyosarcoma
Epithelioid sarcoma
Sarcomas often metastasise via the haematogenous route and the lung is a common
site for sarcoma metastasis. The liver and brain are often spared (at least initially). A
smaller number may develop lymphatic metastasis (see above).
Sarcomas
Malignant tumours of mesenchymal origin
Types May be either bone or soft tissue in origin.
Bone sarcoma include:
Osteosarcoma
Ewings sarcoma (although non bony sites recognised)
Chrondrosarcoma - originate from Chondrocytes
Soft tissue sarcoma are a far more heterogeneous group and include:
Liposarcoma-adipocytes
Rhabdomyosarcoma-striated muscle
Leiomyosarcoma-smooth muscle
Synovial sarcomas- close to joints (cell of origin not known but not synovium)
Malignant fibrous histiocytoma is a sarcoma that may arise in both soft tissue and
bone.
Features Certain features of a mass or swelling should raise suspicion for a sarcoma these
include:
Large >5cm soft tissue mass
Deep tissue location or intra muscular location
Rapid growth
Painful lump
Assessment

Imaging of suspicious masses should utilise a combination of MRI, CT and USS.
Blind biopsy should not be performed prior to imaging and where required should be
done in such a way that the biopsy tract can be subsequently included in any
resection.
Ewings sarcoma
Commoner in males
Incidence of 0.3 / 1, 000, 000
Onset typically between 10 and 20 years of age
Location by femoral diaphysis is commonest site
Histologically it is a small round tumour
Blood borne metastasis is common and chemotherapy is often combined with
surgery
Osteosarcoma
Mesenchymal cells with osteoblastic differentiation
20% of all primary bone tumours
Incidence of 5 per 1,000,000
Peak age 15-30, commoner in males
Limb preserving surgery may be possible and many patients will receive
chemotherapy
Liposarcoma
Malignancy of adipocytes
Rare approximately 2.5 per 1,000,000. They are the second most common soft
tissue sarcoma
Typically located in deep locations such as retroperitoneum
Affect older age group usually >40 years of age
May be well differentiated and thus slow growing although may undergo
dedifferentiation and disease progression
Many tumours will have a pseudocapsule that can misleadingly allow
surgeons to feel that they can 'shell out' these lesions. In reality tumour may
invade at the edge of the pseudocapsule and result in local recurrence if this
strategy is adopted
Usually resistant to radiotherapy although this is often used in a palliative
setting
Malignant Fibrous Histiocytoma
Tumour with large number of histiocytes
Most common sarcoma in adults
Also described as undifferentiated pleomorphic sarcoma NOS (i.e. Cell of
origin is not known)

Four major subtypes are recognised: storiform-pleomorphic (70% cases),
myxoid (less aggressive), giant cell and inflammatory
Treatment is usually with surgical resection and adjuvant radiotherapy as this
reduces the likelihood of local recurrence
Infection with which of the following micro-organisms may result in a clinical picture
resembling achalasia of the oesphagus?
A. Epstein Barr virus
B. Wuchereria Bancrofti
C. Candida Spp
D. Trypanosoma Cruzi
E. Helicobacter Pylori
Infection with Trypanosoma Cruzi may result in destruction of the ganglion cells of
the myenteric plexus, resulting in a clinical picture similar to achalasia.
Trypanosoma Cruzi
Protozoan
Causes Chagas disease
Carried by bugs which infect the skin whilst feeding
Penetrate through open wounds and mucous membranes
Intracellular proliferation
Major infective sites include CNS, intestinal myenteric plexus, spleen, lymph
nodes and cardiac muscle
Chronic disease is irreversible, nifurtimox is used to treat acute infection
A 45-year-old man presents to surgical outpatients with a long history of recurrent
abdominal pain and vomiting. He is noted to have a peripheral motor neuropathy on
examination. What is the most likely diagnosis?
A. Huntington's disease
B. Myeloma
C. Acute intermittent porphyria
D. Lawrence-Moon-Biedl syndrome

E. Friedreich's ataxia
Neurological signs combined with abdominal pain is acute intermittent porphyria or
lead poisoning until proven otherwise.
Acute intermittent porphyria
Acute intermittent porphyria (AIP) is a rare autosomal dominant condition caused by
a defect in porphobilinogen deaminase, an enzyme involved in the biosynthesis of
haem. The results in the toxic accumulation of delta aminolaevulinic acid and
porphobilinogen. It characteristically presents with abdominal and neuropsychiatric
symptoms in 20-40 year olds. AIP is more common in females (5:1)
Features
abdominal: abdominal pain, vomiting
neurological: motor neuropathy
psychiatric: e.g. depression
hypertension and tachycardia common
Diagnosis
classically urine turns deep red on standing
raised urinary porphobilinogen (elevated between attacks and to a greater
extent during acute attacks)
assay of red cells for porphobilinogen deaminase
raised serum levels of delta aminolaevulinic acid and porphobilinogen
A 56 year old man presents with episodic facial pain and discomfort whilst eating. He
has suffered from halitosis recently and he frequently complains of a dry mouth. He
has a smooth swelling underneath his right mandible. What is the most likely
underlying diagnosis?
A. Stone impacted in Whartons duct
B. Stone impacted in Stensens duct
C. Benign adenoma of the submandibular gland
D. Adenocarcinoma of the submandibular gland
E. Squamous cell carcinoma of the submandibular gland
The symptoms are typical for sialolithiasis. The stones most commonly form in the

submandibular gland and therefore may occlude Whartons duct. Stensens duct drains
the parotid gland.
Submandibular glands- disease
Physiology The submandibular glands secrete approximately 800- 1000ml saliva per day. They
typically produce mixed seromucinous secretions. When paraympathetic activity is
dominant the secretions will be more serous. The parasympathetic fibres are derived
from the chorda tympani nerves and the submandibular ganglion, they travel to the
glands via the lingual nerves.
Sialolithiasis
80% of all salivary gland calculi occur in the submandibular gland
70% of the these calculi are radio-opaque
Stones are usually composed of calcium phosphate or calcium carbonate
Patients typically develop colicky pain and post prandial swelling of the gland
Investigation involves sialography to demonstrate the site of obstruction and
associated other stones
Stones impacted in the distal aspect of Whartons duct may be removed orally,
other stones and chronic inflammation will usually require gland excision
Sialadenitis
Usually occurs as a result of Staphylococcus aureus infection
Pus may be seen leaking from the duct, erythema may also be noted
Development of a sub mandibular abscess is a serious complication as it may
spread through the other deep fascial spaces and occlude the airway
Submandibular tumours
Only 8% of salivary gland tumours affect the sub mandibular gland
Of these 50% are malignant (usually adenoid cystic carcinoma)
Diagnosis usually involves fine needle aspiration cytology
Imaging is with CT and MRI
In view of the high prevalence of malignancy, all masses of the submandibular
glands should generally be excised.
Which of the following cellular types or features is not seen in sarcoidosis?
A. Reed Sternberg Cells
B. T lymphocytes

C. Macrophages
D. Asteroid bodies
E. B lymphocytes
Reed Sternberg cells are seen in Hodgkins disease. All of the other cell types are seen
in sarcoid.
Chronic inflammation
Overview Chronic inflammation may occur secondary to acute inflammation.In most cases
chronic inflammation occurs as a primary process. These may be broadly viewed as
being one of three main processes:
Persisting infection with certain organisms such as Mycobacterium
tuberculosis which results in delayed type hypersensitivity reactions and
inflammation.
Prolonged exposure to non-biodegradable substances such as silica or suture
materials which may induce an inflammatory response.
Autoimmune conditions involving antibodies formed against host antigens.
Acute vs. Chronic inflammation
Acute inflammation Chronic inflammation
Changes to existing vascular structure and
increased permeability of endothelial cells
Angiogenesis predominates
Infiltration of neutrophils Macrophages, plasma cells and
lymphocytes predominate
Process may resolve with:
Suppuration
Complete resolution
Abscess formation
Progression to chronic inflammation
Healing by fibrosis
Healing by fibrosis is the main
result
Granulomatous inflammation A granuloma consists of a microscopic aggregation of macrophages (with epithelial
type arrangement =epitheliod). Large giant cells may be found at the periphery of
granulomas.
Mediators Growth factors released by activated macrophages include agents such as interferon
and fibroblast growth factor (plus many more). Some of these such as interferons may

have systemic features resulting in systemic symptoms and signs, which may be
present in individuals with long standing chronic inflammation.
The finding of granulomas is pathognomonic of chronic inflammation, as illustrated
in this biopsy from a patient with colonic Crohns disease
Image sourced from Wikipedia
Which of the following diseases is not considered a risk factor for gastric cancer?
A. Polya gastrectomy for antral ulcer
B. Atrophic gastritis
C. Intestinal metaplasia of columnar type at the gastric cardia
D. Patient with polyp showing medium grade dysplasia
E. Long term therapy with H2 blockers
Although some acid lowering procedures increase the risk of gastric cancer the use of
H2 blockers does not, at the present time, seem to increase the risk.
Gastric cancer
Overview There are 700,000 new cases of gastric cancer worldwide each year. It is most
common in Japan and less common in western countries. It is more common in men
and incidence rises with increasing age. The exact cause of many sporadic cancer is
not known, however, familial cases do occur in HNPCC families. In addition,
smoking and smoked or preserved foods increase the risk. Japanese migrants retain
their increased risk (decreased in subsequent generations). The distribution of the
disease in western countries is changing towards a more proximal location (perhaps
due to rising obesity).

Pathology There is some evidence of support a stepwise progression of the disease through
intestinal metaplasia progressing to atrophic gastritis and subsequent dysplasia,
through to cancer. The favoured staging system is TNM. The risk of lymph node
involvement is related to size and depth of invasion; early cancers confined to
submucosa have a 20% incidence of lymph node metastasis. Tumours of the gastro-
oesophageal junction are classified as below:
Type
1
True oesophageal cancers and may be associated with Barrett's oesophagus.
Type
2
Carcinoma of the cardia, arising from cardiac type epithelium
or short segments with intestinal metaplasia at the oesophagogastric junction.
Type
3
Sub cardial cancers that spread across the junction. Involve similar nodal
stations to gastric cancer.
Groups for close endoscopic monitoring
Intestinal metaplasia of columnar type
Atrophic gastritis
Low to medium grade dysplasia
Patients who have previously undergone resections for benign peptic ulcer
disease (except highly selective vagotomy).
Referral to endoscopy
Patients of any age with
dyspepsia and any of the
following
Patients without
dyspepsia
Worsening dyspepsia
Chronic gastrointestinal
bleeding
Dysphagia Barretts oesophagus
Dysphagia Unexplained
abdominal pain or
weight loss
Intestinal metaplasia
Weight loss Vomiting Dysplasia
Iron deficiency anaemia Upper abdominal mass Atrophic gastritis
Upper abdominal mass Jaundice Patient aged over 55 years
with unexplained or persistent
dyspepsia
Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as
shown in the bottom right) may facilitate identification of smaller tumours

Image sourced from Wikipedia
Staging
CT scanning of the chest abdomen and pelvis is the routine first line staging
investigation in most centres.
Laparoscopy to identify occult peritoneal disease
PET CT (particularly for junctional tumours)
Treatment
Proximally sited disease greater than 5-10cm from the OG junction may be
treated by sub total gastrectomy
Total gastrectomy if tumour is <5cm from OG junction
For type 2 junctional tumours (extending into oesophagus)
oesophagogastrectomy is usual
Endoscopic sub mucosal resection may play a role in early gastric cancer
confined to the mucosa and perhaps the sub mucosa (this is debated)
Lymphadenectomy should be performed. A D2 lymphadenectomy is widely
advocated by the Japanese, the survival advantages of extended
lymphadenectomy have been debated. However, the overall recommendation
is that a D2 nodal dissection be undertaken.
Most patients will receive chemotherapy either pre or post operatively.
Prognosis

UK Data
Disease extent Percentage 5 year survival
All RO resections 54%
Early gastric cancer 91%
Stage 1 87%
Stage 2 65%
Stage 3 18%
Operative procedure
Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis
General anaesthesia
Prophylactic intravenous antibiotics
Incision: Rooftop.
Perform a thorough laparotomy to identify any occult disease.
Mobilise the left lobe of the liver off the diaphragm and place a large pack over it.
Insert a large self retaining retractor e.g. omnitract or Balfour (take time with this, the
set up should be perfect). Pack the small bowel away.
Begin by mobilising the omentum off the transverse colon.
Proceed to detach the short gastric vessels.
Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling
device.
Continue the dissection into the lesser sac taking the lesser omentum and left gastric
artery flush at its origin.
The lymph nodes should be removed en bloc with the specimen where possible.
Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull
back on the nasogastric tube. Divide the distal oesophagus and remove the stomach.
The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and
bring a loop of jejunum up to the oesophagus (to check it will reach). Divide the
jejunum at this point. Bring the divided jejunum either retrocolic or antecolic to the
oesophagus. Anastamose the oesophagus to the jejunum, using either interrupted 3/0
vicryl or a stapling device. Then create the remainder of the Roux en Y reconstruction
distally.
Place a jejunostomy feeding tube.
Wash out the abdomen and insert drains (usually the anastomosis and duodenal
stump). Help the anaesthetist insert the nasogastric tube (carefully!)
Close the abdomen and skin.
Enteral feeding may commence on the first post-operative day. However, most
surgeons will leave patients on free NG drainage for several days and keep them nil
by mouth.
A 56 year old man is diagnosed as having a glioma. From which of the following cell
types do these tumours usually originate?
A. Astrocytes

B. Oligodendrocytes
C. Ependymal cells
D. Squamous cells
E. Neuroglial cells
Theme from January 2012 Exam
Gliomas originate from glial (otherwise known as neuroglial) cells. These serve a
structural function in the CNS. The tumours produced may resemble a number of
CNS cell types. Tumours are therefore named according to the cells they resemble
rather than the origin. Where this is not possible they are termed gliomas.
Glioma
Glioma is a tumour that is typically found in the CNS. These tumours arise from glial
cells. They are sub categorised according to the cell type they most closely resemble.
Glioma sub types
Ependymomas- Ependymal cells
Astocytomas- Astrocytes (including glioblastoma)
Oligodendrogliomas- Oligodendrocytes
Mixed- e.g. oligoastrocytomas
Gliomas are categorised as being either high or low grade lesions (the former has the
worse prognosis). They may be either supra or infra tentorial. Their symptoms will
typically reflect their site of origin. Glioblastoma multiforme has the worst prognosis
and few patients will survive beyond 12 months.
A 78 year old man presents with unilateral deafness which has been present for the
past 3 months. On examination Webers test localises to the contralateral side and a
CT scan of his head shows a thickened calvarium with areas of sclerosis and
radiolucency. His blood tests show an elevated alkaline phosphatase, normal serum
calcium and normal PTH levels. Which of the following is the most likely underlying
diagnosis?
A. Multiple myeloma with skull involvement
B. Osteoporosis
C. Pagets disease with skull involvement
D. Lung cancer with skull metastasis
E. Osteopetrosis with skull involvement
Of the conditions listed Pagets disease is the most likely diagnosis (skull vault
expansion and sensorineural hearing loss). Multiple myeloma would typically result
in multiple areas of radiolucency and usually raised calcium in this setting.
Osteopetrosis is a recognised cause of the features described. However, it is a rare
inherited disorder and usually presents in children in young adults. Presentation at this
stage with no prior symptoms would be extremely rare and therefore this is not the
most likely diagnosis.
Pagets disease
Paget's disease is a disease of increased but uncontrolled bone turnover and is
characterised by architecturally abnormal bones. It is thought to be primarily a
disorder of osteoclasts, with excessive osteoclastic resorption followed by increased
osteoblastic activity causing areas of sclerosis and deformity. Paget's disease is
common (UK prevalence 5%) but symptomatic in only 1 in 20 patients
Predisposing factors
increasing age
male sex
northern latitude
family history
Clinical features
bone pain (e.g. pelvis, lumbar spine, femur)
classical, untreated features: bowing of tibia, bossing of skull
raised alkaline phosphatase (ALP) - calcium* and phosphate are typically
normal
skull x-ray: thickened vault, osteoporosis circumscripta
Indications for treatment include bone pain, skull or long bone deformity, fracture,
periarticular Paget's
bisphosphonate (either oral risedronate or IV zoledronate)
calcitonin is less commonly used now
Complications
deafness (cranial nerve entrapment)
bone sarcoma (1% if affected for > 10 years)
fractures
skull thickening
high-output cardiac failure

*usually normal in this condition but hypercalcaemia may occur with prolonged
immobilisation
Theme: Genetic causes of cancer
A. Multiple endocrine neoplasia type I
B. Multiple endocrine neoplasia type II
C. Gardner's syndrome
D. Lynch Syndrome
E. Kartagener's syndrome
F. Von Recklinghausen's disease
Please select the most likely condition for the disease process described. Each option
may be used once, more than once or not at all
13. A 5 year old boy presents with recurrent episodes of sinusitis. The casualty
staff are surprised to find his liver lying in the left upper quadrant of the
abdomen
Kartagener's syndrome
This is a case of Kartagener's syndrome. The primary problem is of immotile
cilia syndrome. When associated with situs inversus Kartagener's syndrome is
diagnosed.
14. A 22 year old man presents with carcinoma of the caecum. His brother died
from colorectal cancer aged 25 and his father died from the disease aged 30.
Lynch Syndrome
This is a case of Lynch syndrome HNPCC. It is transmitted in an autosomal
dominant fashion.
15. A tall 32 year old lady presents with a diffuse neck swelling a carcinoma of
the thyroid medullary type is diagnosed.
Multiple endocrine neoplasia type II
This is a case MEN type IIb. It is associated with phaeochromocytomas and is
transmitted in an autosomal dominant pattern if inherited. All MEN II tend to
have medullary carcinoma of the thyroid as a presenting feature

Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.
Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:
*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2
Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age
80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one
of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.
Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5

Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli
A 45 year old man presents with symptoms of urinary colic. In the history he has
suffered from recurrent episodes of frank haematuria over the past week or so. On
examination he has a left loin mass and a varicocele. The most likely diagnosis is:
A. Renal adenocarcinoma
B. Renal cortical adenoma
C. Squamous cell carcinoma of the renal pelvis
D. Retroperitoneal fibrosis
E. Nephroblastoma
Renal adenocarcinoma are the most common renal malignancy and account
for 75% cases.
Patients may develop frank haematuria and have episodes of clot colic.
A Grawitz tumour is an eponymous name for Renal Adenocarcinoma.
May metastasise to bone.
Renal tumours
Renal cell carcinoma Renal cell carcinoma is an adenocarcinoma of the renal cortex and is believed to arise
from the proximal convoluted tubule. They are usually solid lesions, up to 20% may
be multifocal, 20% may be calcified and 20% may have either a cystic component or
be wholly cystic. They are often circumscribed by a pseudocapsule of compressed
normal renal tissue. Spread may occur either by direct extension into the adrenal
gland, renal vein or surrounding fascia. More distant disease usually occurs via the
haematogenous route to lung, bone or brain.
Renal cell carcinoma comprise up to 85% of all renal malignancies. Males are more
commonly affected than females and sporadic tumours typically affect patients in
their sixth decade.
Patients may present with a variety of symptoms including; haematuria (50%), loin
pain (40%), mass (30%) and up to 25% may have symptoms of metastasis.Less than
10% have the classic triad of haematuria, pain and mass.
Investigation Many cases will present as haematuria and be discovered during diagnostic work up.
Benign renal tumours are rare, so renal masses should be investigated with multislice

CT scanning. Some units will add and arterial and venous phase to the scan to
demonstrate vascularity and evidence of caval ingrowth.
CT scanning of the chest and abdomen to detect distant disease should also be
undertaken.
Routine bone scanning is not indicated in the absence of symptoms.
Biopsy should not be performed when a nephrectomy is planned but is mandatory
before any ablative therapies are undertaken.
Assessment of the functioning of the contra lateral kidney.
Management T1 lesions may be managed by partial nephrectomy and this gives equivalent
oncological results to total radical nephrectomy. Partial nephrectomy may also be
performed when there is inadequate reserve in the remaining kidney.
For T2 lesions and above a radical nephrectomy is standard practice and this may be
performed via a laparoscopic or open approach. Preoperative embolisation is not
indicated nor is resection of uninvolved adrenal glands. During surgery early venous
control is mandatory to avoid shedding of tumour cells into the circulation.
Patients with completely resected disease do not benefit from adjuvant therapy
with either chemotherapy or biological agents. These should not be administered
outside the setting of clinical trials.
Patients with transitional cell cancer will require a nephroureterectomy with
disconnection of the ureter at the bladder.
References Lungberg B et al. EAU guidelines on renal cell carcinoma: The 2010 update.
European Urology 2010 (58): 398-406.
A 63 year old man finds that he has to stop walking after 100 yards due to bilateral
calf pain. He finds that bending forwards and walking up hill helps. He is able to ride
a bike without any pain. What is the most likely underlying cause?
A. Lumbar canal stenosis
B. Diabetic neuropathy
C. Aorto-iliac occlusion
D. Occlusion of the superficial femoral artery
E. Pelvic rheumatoid arthritis

Theme from April 2012 Exam The positional nature of the pain and the fact that improves with walking uphill makes
an underlying vascular aetiology far less likely.
Lumbar spinal stenosis
Lumbar spinal stenosis is a condition in which the central canal is narrowed by
tumour, disk prolapse or other similar degenerative changes.
Patients may present with a combination of back pain, neuropathic pain and
symptoms mimicking claudication. One of the main features that may help to
differentiate it from true claudication in the history is the positional element to the
pain. Sitting is better than standing and patients may find it easier to walk uphill rather
than downhill. The neurogenic claudication type history makes lumbar spinal stenosis
a likely underlying diagnosis, the absence of such symptoms makes it far less likely.
Pathology Degenerative disease is the commonest underlying cause. Degeneration is believed to
begin in the intervertebral disk where biochemical changes such as cell death and loss
of proteoglycan and water content lead to progressive disk bulging and collapse. This
process leads to an increased stress transfer to the posterior facet joints, which
accelerates cartilaginous degeneration, hypertrophy, and osteophyte formation; this is
associated with thickening and distortion of the ligamentum flavum. The combination
of the ventral disk bulging, osteophyte formation at the dorsal facet, and ligamentum
flavum hyptertrophy combine to circumferentially narrow the spinal canal and the
space available for the neural elements. The compression of the nerve roots of the
cauda equina leads to the characteristic clinical signs and symptoms of lumbar spinal
stenosis.
Diagnosis MRI scanning is the best modality for demonstrating the canal narrowing. Historically
a bicycle test was used as true vascular claudicants could not complete the test.
Treatment Laminectomy
A 73 year old lady is admitted for a laparoscopic cholecystectomy. During her pre-
operative assessment it is noted that she is receiving furosemide for the treatment of
hypertension. Approximately what proportion of the sodium that is filtered at the
glomerulus will be subsequently excreted?
A. Up to 25%
B. Upt to 75%
C. Between 3 and 5%
D. <2%
E. Between 1 and 2%
Theme from 2010 Exam
The loop diuretics can lead to marked increases in the amount of sodium excreted.
They act in the medullary and cortical aspects of the thick ascending limb of the loop
of Henle. This results in a decreased medullary osmolal gradient and increases free
water excretion (as well as loss of sodium). Because loop diuretics result in the loss of
both sodium and water they are less frequently associated with hyponatraemia than
thiazide diuretics (these latter agents act in the cortex and do not affect urine
concentrating ability).
Diuretic agents
The diuretic drugs are divided into three major classes, which are distinguished
according to the site at which they impair sodium reabsorption: loop diuretics in the
thick ascending loop of Henle, thiazide type diuretics in the distal tubule and
connecting segment; and potassium sparing diuretics in the aldosterone - sensitive
principal cells in the cortical collecting tubule.
In the kidney, sodium is reabsorbed through Na+/ K+ ATPase pumps located on the
basolateral membrane. These pumps return reabsorbed sodium to the circulation and
maintain low intracellular sodium levels. This latter effect ensures a constant
concentration gradient.
Physiological effects of commonly used diuretics
Site of action Diuretic Carrier or
channel inhibited
Percentage of filtered
sodium excreted
Ascending limb of loop
of Henle
Frusemide Na+/K+ 2Cl -
carrier
Upt to 25%
Distal tubule and
connecting segment
Thiazides Na+Cl- carrier Between 3 and 5%
Cortical collecting
tubule
Spironolactone Na+ channel Between 1 and 2%
A 59 year old man presents with recurrent episodes of urinary sepsis. In his history he
mentions that he has suffered from recurrent attacks of left iliac fossa pain over the
past few months. He has also notices bubbles in his urine. He undergoes a CT scan
which shows a large inflammatory mass in the left iliac fossa. No other abnormality is
detected. The most likely diagnosis is:
A. Ulcerative colitis
B. Crohns disease
C. Mesenteric ischaemia

D. Diverticular disease
E. Rectal cancer
Theme from 2009 and 2011 Exam
Recurrent attacks of diverticulitis may cause the development of local abscesses
which may erode into the bladder resulting in urinary sepsis and pneumaturia. This
would be an unusual presentation from Crohns disease and rectal cancer would be
more distally sited and generally evidence of extra colonic disease would be present if
the case were malignant and this advanced.
Diverticular disease
Diverticular disease is a common surgical problem. It consists of herniation of colonic
mucosa through the muscular wall of the colon. The usual site is between the taenia
coli which vessels pierce the muscle to supply the mucosa.
Symptoms
Altered bowel habit
Bleeding
Abdominal pain
Complications
Diverticulitis
Haemorrhage
Development of fistula
Perforation and faecal peritonitis
Perforation and development of abscess
Development of diverticular phlegmon
Diagnosis Patients presenting in clinic will typically undergo either a colonoscopy or barium
enema as part of their diagnostic work up. Both tests will identify diverticular disease.
It can be far more difficult to confidently exclude cancer, particularly in diverticular
strictures.
Acutely unwell surgical patients should be investigated in a systematic way. Plain
abdominal films and an erect chest x-ray will identify perforation. An abdominal CT
scan with oral and intravenous contrast will help to identify whether acute
inflammation is present but also the presence of local complications such as abscess
formation.
Severity Classification- Hinchey

I Para-colonic abscess
II Pelvic abscess
III Purulent peritonitis
IV Faecal peritonitis
Treatment
Increase dietary fibre intake.
Mild attacks of diverticulitis may be managed conservatively with antibiotics.
Peri colonic abscesses should be drained either surgically or radiologically.
Recurrent episodes of acute diverticulitis requiring hospitalisation are a
relative indication for a segmental resection.
Hinchey IV perforations (generalised faecal peritonitis) will require a
resection and usually a stoma. This group have a very high risk of post
operative complications and usually require HDU admission. Less severe
perforations may be managed by laparoscopic washout and drain insertion.
A 78 year old man is referred to the clinic by his general practitioner. For many years
he noticed a smooth swelling approximately 5cm anterior to the tragus of his right ear.
Apart from being a heavy smoker he has no co-morbidities. What is the most likely
diagnosis?
A. Pleomorphic adenoma
B. Liposarcoma
C. Warthins tumour
D. Adenocarcinoma
E. None of the above
Warthins tumours are most common in elderly smokers. They have a relatively
benign and indolent course. They are usually well circumscribed as illustrated below:

Image sourced from Wikipedia
Parotid gland clinical
Causes of bilateral parotid enlargement
Mumps: Associated with meningoencephalitis, pancreatitis, orchitis, or
deafness
Parotitis
Sialectasis - especially if related to eating
Sjogren's syndrome: dry eyes or mouth, connective tissue disease
Sarcoidosis
Tuberculosis
Alcoholism
Myxoedema
Cushing's disease
Diabetes/insulin resistance
Liver cirrhosis
Gout
Bulimia nervosa
Drugs
Severe dehydration
Malnutrition
Causes of unilateral parotid enlargement

Salivary calculus
Tumour
Parotid gland tumours
Pleomorphic adenomas are the most common.
Incisional biopsy of parotid masses is not recommended, so superficial
parotidectomy is the usual procedure of choice.
Signs of facial nerve palsy and a parotid mass should raise suspicion of
malignancy.
Warthins tumours are relatively benign lesions that are slow growing and
occur most commonly in elderly male smokers.
Adenoid cystic carcinoma have a tendency for perineural invasion.
Theme: Lung cancer
A. Adenocarcinoma
B. Small cell lung cancer
C. Large cell lung cancer
D. Squamous cell carcinoma
Please select the most likely lung cancer variant for the scenario described. Each
option may be used once, more than once or not at all.
21. A 73 year old heavy smoker presents with haemoptysis. On examination he is
cachectic and shows evidence of clubbing. Imaging shows a main bronchial
tumour with massive mediastinal lymphadenopathy together with widespread
visceral metastases.
Small cell lung cancer
Theme from April 2012
Small cell carcinoma is associated with disseminated disease at presentation
in the majority of cases. Most cases occur in the main airways and
paraneoplastic features are common.
22. A 68 year old female who has never smoked presents with a mass at the
periphery of her right lung.
You answered Large cell lung cancer
The correct answer is Adenocarcinoma

Adenocarcinomas are the most common tumour type present in never
smokers. They are usually located at the periphery.
23. An 85 year old man presents with a cough and haemoptysis. He has a modest
smoking history of 15 pack years. He is found to have a tumour located in the
right main bronchus, with no evidence of metastatic disease. He decides no
undergo any treatment and he remains well for a further 12 months before
developing symptomatic metastasis.
You answered Large cell lung cancer
The correct answer is Squamous cell carcinoma
Squamous cell carcinomas are reported to be more slow growing and are
typically centrally located. Small cell carcinomas are usually centrally
located. However, small cell carcinomas would seldom be associated with a
survival of a year without treatment.
Lung cancer
Lung cancers may be classified according to histological subtypes. The main
distinction is between small cell and non small cell lung cancer. Non small cell lung
cancer is the most common variant and accounts for 80% of all lung cancers.
Non small cell lung cancer These share common features of prognosis and management. They comprise the
following tumours:
Squamous cell carcinoma (25% cases)
Adenocarcinoma (40% cases)
Large cell carcinoma (10% cases)
Paraneoplastic features and early disease dissemination are less likely than with small
cell lung carcinoma. Adenocarcinoma is the most common lung cancer type
encountered in never smokers.
Small cell lung carcinoma Small cell lung carcinomas are comprised of cells with a neuro endocrine
differentiation. The neuroendocrine hormones may be released from these cells with a
wide range of paraneoplastic associations. These tumours are strongly associated with
smoking and will typically arise in the larger airways. They disseminate early in the
course of the disease and although they are usually chemosensitive this seldom results
in long lasting remissions.
Which of the following cells is not found on a blood film post splenectomy?

A. Pappenheimer bodies
B. Stipple cells
C. Erythrocyte containing siderotic granules
D. Howell-Jolly bodies
E. Target cells
Stipple cells are found in lead poisoning/haemoglobinopathies.
Blood film in hyposplenism:
Howell-Jolly bodies
Pappenheimer bodies
Poikilocytes (Target cells)
Erythrocyte containing siderotic granules
Heinz bodies
Post splenectomy blood film changes
The loss of splenic tissue results in the inability to readily remove immature or
abnormal red blood cells from the circulation. The red cell count does not alter
significantly. However, cytoplasmic inclusions may be seen e.g. Howell-Jolly bodies.
In the first few days after splenectomy target cells, siderocytes and reticulocytes will
appear in the circulation. Immediately following splenectomy a granulocytosis
(mainly composed of neutrophils) is seen, this is replaced by a lymphocytosis and
monocytosis over the following weeks.
The platelet count is usually increased and this may be persistent, oral antiplatelet
agents may be needed in some patients.
Image showing Howell Jolly bodies (arrowed)

Image sourced from Wikipedia
A 45 year old man with long standing ulcerative colitis and rectal dysplasia presents
with a DALM lesion in the rectum. What is the most appropriate management option?
A. Snare polypectomy
B. Repeat endoscopy in 2 years
C. Discharge
D. Anterior resection
E. Panproctocolectomy
DALM lesions complicating ulcerative colitis should be managed with
panproctocolectomy. An anterior resection is inadequate since it will only remove the
rectum and ulcerative colitis affects the entire colon. Since many will be associated
with invasion a snare polypectomy is not sufficient either.
Colonic lesions - DALM
The term DALM lesion refers to a Dysplasia Associated Lesion or Mass.
They may complicate dysplasia occurring in patients with longstanding
ulcerative colitis.
They have a high incidence of invasive foci.
When they complicate longstanding ulcerative colitis, they should be treated
by panproctocolectomy.

Which of the metastatic bone tumours described below is at the greatest risk of
pathological fracture ?
A. Proximal humeral lesion from a prostate cancer
B. Vertebral body lesions from a prostate cancer
C. Peritrochanteric lesion from a carcinoma of the breast
D. Proximal humeral lesion from a carcinoma of the breast
E. Peritrochanteric lesion from a prostate cancer
Peritrochanteric lesions have the greatest risks of fracture (due to loading).
The lesions from breast cancer are usually lytic and therefore at higher risk
rather than the sclerotic lesions from prostate cancer.
Metastatic bone disease- risk of fracture
Metastatic bone tumours may be described as blastic, lytic or mixed.
Osteoblastic metastatic disease has the lowest risk of spontaneous fracture
when compared to osteolytic lesions of a similar size.
Lesions affecting the peritrochanteric region are most prone to spontaneous
fracture (because of loading forces at that site).
The factors are incorportated into the Mirel Scoring system to stratify the risk
of spontaneous fracture for bone metastasis of varying types.
Mirel Scoring system
Score
points
Site Radiographic
appearance
Width of bone
involved
Pain
1 Upper
extremity
Blastic Less than 1/3 Mild
2 Lower
extremity
Mixed 1/3 to 2/3 Moderate
3 Peritrochanteric Lytic More than 2/3 Aggravated by
function
Depending upon the score the treatment should be as follows:
Score Risk of fracture Treatment
9 or greater Impending (33%) Prophylactic fixation
8 Borderline Consider fixation
7 or less Not impending (4%) Non operative management
A 63 year old male presents with several episodes of haematuria. He suffers from
COPD secondary to long term smoking. Which is the most likely underlying cause?

A. Renal cortical adenoma
B. Renal adenocarcinoma
C. Nephroblastoma
D. Transitional cell carcinoma of the bladder
E. Adenocarcinoma of the bladder
Theme from 2009 Exam
TCC is the most common subtype and is strongly linked to smoking. The important
point to note in this question is the term most likely as renal adenocarcinoma may
produce similar symptoms but is less likely.
Bladder cancer
Bladder cancer is the second most common urological cancer. It most commonly
affects males aged between 50 and 80 years of age. Those who are current, or
previous (within 20 years), smokers have a 2-5 fold increased risk of the disease.
Occupational exposure to hydrocarbons such as alanine increases the risk. Although
rare in the UK, chronic bladder inflammation arising from Schistosomiasis infection
remains a common cause of squamous cell carcinomas, in those countries where the
disease is endemic.
Benign tumours Benign tumours of the bladder including inverted urothelial papilloma and
nephrogenic adenoma are uncommon.
Bladder malignancies
Transitional cell carcinoma (>90% of cases)
Squamous cell carcinoma ( 1-7% -except in regions affected by
schistosomiasis)
Adenocarcinoma (2%)
Transitional cell carcinomas may arise as solitary lesions, or may be multifocal,
owing to the effect of "field change" within the urothelium. Up to 70% of TCC's will
have a papillary growth pattern. These tumours are usually superficial in location and
accordingly have a better prognosis. The remaining tumours show either mixed
papillary and solid growth or pure solid growths. These tumours are typically more
prone to local invasion and may be of higher grade, the prognosis is therefore worse.
Those with T3 disease or worse have a 30% (or higher) risk of regional or distant
lymph node metastasis.
TNM Staging

Stage Description
T0 No evidence of tumour
Ta Non invasive papillary carcinoma
T1 Tumour invades sub epithelial connective tissue
T2a Inner half of detrusor invaded
T2b Outer half of detrusor invaded
T3 Tumour extends to perivesical fat
T4a Invasion of uterus, prostate or bowel
T4b Invasion of other abdominal organs
N0 No nodal disease
N1 Single lymph node metastasis (up to 2cm)
N2 Single node >2cm or multiple nodes up to 5cm
N3 Nodes over 5cm
M1 Distant disease
Presentation Most patients (85%) will present with painless, macroscopic haematuria. In those
patients with incidental microscopic haematuria, up to 10% of females aged over 50
will be found to have a malignancy (once infection excluded).
Staging Most will undergo a cystoscopy and biopsies or TURBT, this provides histological
diagnosis and information relating to depth of invasion. Locoregional spread is best
determined using pelvic MRI and distant disease CT scanning. Nodes of uncertain
significance may be investigated using PET CT.
Treatment Those with superficial lesions may be managed using TURBT in isolation. Those
with recurrences or higher grade/ risk on histology may be offered intravesical
chemotherapy. Those with T2 disease are usually offered either surgery (radical
cystectomy and ileal conduit) or radical radiotherapy.
Prognosis
T1 90%
T2 60%
T3 35%
T4a 10-25%
Any T, N1-N2 30%
Theme: Neck lumps
A. Cystic hygroma
B. Bartonella infection
C. Mycobacterium tuberculosis infection
D. Branchial cyst
E. Thyroglossal cyst

F. Pharyngeal pouch
G. Follicular thyroid cyst
H. Parathyroid adenoma
I. None of the above
Please select the most likely underlying disease process for the scenario given. Each
option may be used once, more than once or not at all.
28. A 25 year old cat lover presents with symptoms of abdominal pain, lethargy
and sweats. These have been present for the past two weeks. On examination
she has lymphadenopathy in the posterior triangle.
You answered Mycobacterium tuberculosis infection
The correct answer is Bartonella infection
Bartonella infection may occur following a cat scratch. The organism is
intracellular. Generalised systemic symptoms may occur for a week or so
prior to clinical presentation.
29. A 25 year old lady presents with an swelling located at the anterior border of
the sternocleidomastoid muscle. The swelling is intermittent and on
examination it is soft and fluctuant.
Branchial cyst
Branchial cysts are remnants of the branchial cleft. They may become
infected.
30. A 38 year old lady presents with a mass in the midline of the neck
immediately below the hyoid bone. It moves upwards on tongue protrusion.
Thyroglossal cyst
Thyroglossal cysts are usually located in the midline and are linked to the
foramen caecum and will thus move upwards on tongue protrusion.
Neck lumps

The table below gives characteristic exam question features for conditions causing
neck lumps:
Reactive
lymphadenopathy
By far the most common cause of neck swellings. There may
be a history of local infection or a generalised viral illness
Lymphoma Rubbery, painless lymphadenopathy
The phenomenon of pain whilst drinking alcohol is very
uncommon
There may be associated night sweats and splenomegaly
Thyroid swelling May be hypo-, eu- or hyperthyroid symptomatically
Moves upwards on swallowing
Thyroglossal cyst More common in patients < 20 years old
Usually midline, between the isthmus of the thyroid and the
hyoid bone
Moves upwards with protrusion of the tongue
May be painful if infected
Pharyngeal pouch More common in older men
Represents a posteromedial herniation between
thyropharyngeus and cricopharyngeus muscles
Usually not seen, but if large then a midline lump in the neck
that gurgles on palpation
Typical symptoms are dysphagia, regurgitation, aspiration
and chronic cough
Cystic hygroma A congenital lymphatic lesion (lymphangioma) typically
found in the neck, classically on the left side
Most are evident at birth, around 90% present before 2 years
of age
Branchial cyst An oval, mobile cystic mass that develops between the
sternocleidomastoid muscle and the pharynx
Develop due to failure of obliteration of the second branchial
cleft in embryonic development
Usually present in early adulthood
Cervical rib More common in adult females
Around 10% develop thoracic outlet syndrome
Carotid aneurysm Pulsatile lateral neck mass which doesn't move on swallowing
A 22 year old man presents with a discharging area on his lower back. On
examination there is an epithelial defect located 6cm proximal to the tip of his coccyx
and located in the midline. There are two further defects located about 2cm superiorly
in the same position. He is extremely hirsute. What is the most likely diagnosis?
A. Pre sacral tumour
B. Sacrococcygeal teratoma
C. Pilonidal sinus
D. Fistula in ano
E. Occult spina bifida
Pilonidal sinuses are extremely common in hirsute individuals and typically present as
midline sinuses in the natal cleft.
Pilonidal sinus
Occur as a result of hair debris creating sinuses in the skin (Bascom theory).
Usually in the natal cleft of male patients after puberty.
It is more common in Caucasians related to their hair type and growth
patterns.
The opening of the sinus is lined by squamous epithelium, but most of its wall
consists of granulation tissue. Up to 50 cases of squamous cell carcinoma has
been described in patients with chronic pilonidal sinus disease.
Hairs become trapped within the sinus.
Clinically the sinus presents when acute inflammation occurs, leading to an
abscess. Patients may describe cycles of being asymptomatic and periods of
pain and discharge from the sinus.
Treatment is difficult and opinions differ. Definitive treatment should never be
undertaken when acute infection or abscess is present as this will result in
failure.
Definitive treatments include the Bascom procedure with excision of the pits
and obliteration of the underlying cavity. The Karydakis procedure involves
wide excision of the natal cleft such that the surface is recontoured once the
wound is closed. This avoids the shearing forces that break off the hairs and
has reasonable results.
Pilonidal sinuses are most commonly located in the midline of the natal cleft, as
illustrated below

Image sourced from Wikipedia
A 43 year old man from Greece presents with colicky right upper quadrant pain,
jaundice and a pruritic, erythematous rash over his body. He is initially treated with
ciprofloxacin, but does not improve. What is the most likely diagnosis?
A. Infection with Wucheria bancrofti
B. Infection with Echinococcus granulosus
C. Type III hypersentivity reaction
D. Allergy to ciprofloxacin
E. Common bile duct stones
Infection with Echinococcus granulosus will typically produce a type I
hypersensitivity reaction which is characterised by a urticarial rash. With biliary
rupture a classical triad of biliary colic, jaundice and urticaria occurs. Whilst jaundice
and biliary colic may be a feature of CBD stones they do not produce an urticarial
rash. Antibiotic sensitivity with ciprofloxacin may produce jaundice and a rash,
however it was not present at the outset and does not cause biliary colic.
Hydatid cysts

Hydatid cysts are endemic in Mediterranean and Middle Eastern countries. They are
caused by the tapeworm parasite Echinococcus granulosus. An outer fibrous capsule
is formed containing multiple small daughter cysts. These cysts are allergens which
precipitate a type 1 hypersensitivity reaction.
Clinical features are as follows:
Up to 90% cysts occur in the liver and lungs
Can be asymtomatic, or symptomatic if cysts > 5cm in diameter
Morbidity caused by cyst bursting, infection and organ dysfunction (biliary,
bronchial, renal and cerebrospinal fluid outflow obstruction)
In biliary ruputure there may be the classical triad of; biliary colic, jaundice,
and urticaria
CT is the best investigation to differentiate hydatid cysts from amoebic and pyogenic
cysts.
Surgery is the mainstay of treatment (the cyst walls must not be ruptured during
removal and the contents sterilised first).
A 22 year old lady presents with an episode of renal colic and following investigation
is suspected of suffering from MEN IIa. Which of the following abnormalities of the
parathyroid glands are most often found in this condition?
A. Hypertrophy
B. Hyperplasia
C. Adenoma
D. Carcinoma
E. Metaplasia
MEN IIa
Medullary thyroid cancer
Hyperparathyroidism (usually
hyperplasia)
Phaeochromocytoma
In MEN IIa the commonest lesion is medullary thyroid cancer, with regards to the
parathyroid glands the most common lesion is hyperplasia. In MEN I a parathyroid
adenoma is the most common lesion.
Multiple Endocrine Neoplasia

Multiple endocrine neoplasia (MEN) is inherited as an autosomal dominant disorder.
The table below summarises the three main types of MEN:
MEN type I MEN type IIa MEN type IIb
Mnemonic 'three P's':
Parathyroid (95%): Parathyroid adenoma
Pituitary (70%):
Prolactinoma/ACTH/Growth Hormone
secreting adenoma
Pancreas (50%): Islet cell
tumours/Zollinger Ellison syndrome
also: Adrenal (adenoma) and thyroid
(adenoma)
Phaeochromocytoma
Medullary thyroid
cancer (70%)
Hyperparathyroidism
(60%)
Same as MEN IIa
with addition of:
Marfanoid body
habitus
Mucosal neuromas
MENIN gene (chromosome 11)
Most common presentation =
hypercalcaemia
RET oncogene
(chromosome 10)
RET oncogene
(chromosome 10)
A male infant is born prematurely at 34 weeks gestation by emergency cesarean
section. He initially appears to be stable. However, over the ensuing 24 hours he
develops worsening neurological function. Which of the following processes is most
likely to have occurred?
A. Extra dural haemorrhage
B. Sub dural haemorrhage
C. Sub arachnoid haemorrhage
D. Intraventricular haemorrhage
E. Arteriovenous malformation
Theme from April 2012 Exam
Intraventricular haemorrhage
Intraventricular haemorrhage is a haemorrhage that occurs into the ventricular system
of the brain. It is relatively rare in adult surgical practice and when it does occur, it is
typically associated with severe head injuries. In premature neonates it may occur
spontaneously. The blood may clot and occlude CSF flow, hydrocephalus may result.
In neonatal practice the vast majority of IVH occur in the first 72 hours after birth, the
aetiology is not well understood and it is suggested to occur as a result of birth trauma

combined with cellular hypoxia, together the with the delicate neonatal CNS.
Treatment Is largely supportive, therapies such as intraventricular thrombolysis and prophylactic
CSF drainage have been trialled and not demonstrated to show benefit.
Hydrocephalus and rising ICP is an indication for shunting.
A 22 year old man is admitted to hospital with a lower respiratory chest infection. He
had a splenectomy after being involved in a car accident. What is the most likely
infective organism?
A. Haemophilus influenzae
B. Staphylococcus aureus
C. Rhinovirus
D. Mycobacterium tuberculosis
E. Moraxella catarrhalis
Organisms causing post
splenectomy sepsis:
Streptococcus pneumoniae
Haemophilus influenzae
Meningococci
Encapsulated organisms carry the greatest pathogenic risk following splenectomy.
The effects of sepsis following splenectomy are variable. This may be the result of
small isolated fragments of splenic tissue that retain some function following
splenectomy. These may implant spontaneously following splenic rupture (in trauma)
or be surgically implanted at the time of splenectomy.
Post splenectomy sepsis
The loss of splenic function renders individuals at increased risk of fulminant sepsis.
Young children are at the highest risk, especially in the first 2 years following
surgery. Surgery for trauma is associated with a lower risk than when splenectomy is
performed as a treatment for haematological disorders.
Infection with encapsulated organisms poses the greatest risk, these organisms may be
opsonised, but this then goes undetected at an immunological level due to loss of the
spleen.
Prophylactic vaccinations are usually administered to reduce the risk of pneumococcal
septicaemia. Since the vaccine only covers up to 80% of pneumococcal infections,
patients will usually recieve long term, low dose penicillin prophylaxis in addition to
vaccination.
A 24 year old man presents with symptoms of malaise, weight loss and
lymphadenopathy. A lymph node biopsy is performed and the subsequent histology

report states that there is evidence of granuloma formation and central necrosis. What
is the most likely underlying cause?
A. Non Hodgkins lymphoma
B. Churg Strauss syndrome
C. Epstein Barr Virus infection
D. Rheumatoid nodule
E. Infection with Mycobacterium tuberculosis
These histological features are typically seen in TB. Necrosis occurring in granulomas
is usually indicative of an underlying infective cause. Churg Strauss syndrome is a
form of vasculitis, which is the usual histological finding. Granulomas are reported in
the condition, but it is rare for them to demonstrate necrosis.
Tuberculosis pathology
Is a form of primary chronic inflammation, caused by the inability of
macrophages to kill the Mycobacterium tuberculosis.
The macrophages often migrate to regional lymph nodes, the lung lesion plus
affected lymph nodes is referred to as a Ghon complex.
This leads to the formation of a granuloma which is a collection of epithelioid
histiocytes.
There is the presence of caseous necrosis in the centre.
The inflammatory response is mediated by a type 4 hypersensitivity reaction.
In healthy individuals the disease may be contained, in the
immunocompromised disseminated (miliary TB) may occur.
Diagnosis
Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl -
Neelsen staining is typically used.
Culture based methods take far longer.
Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen
method

Image sourced from Wikipedia
A 20 year old man develops acute appendicitis, his appendix is removed and he
makes a full recovery. Which of the following pathological processes is least likely to
be present in the acutely inflamed tissues?
A. Altered Starlings forces.
B. Seqestration of neurophils
C. Formation of fluid exudate
D. Formation of granulomas
E. None of the above
Neutrophil polymorphs=Acute
inflammation.
Granuloma = Chronic
inflammation.
Acute inflammation:
3 phases:
1. Changes in blood vessel and flow: flush, flare, wheal
2. Fluid exudates (rich in protein i.e. Ig, coagulation factors) produced via increased
vascular permeability
3. Cellular exudates mainly containing neutrophil polymorphs pass into extravascular
space.
Neutrophils are then transported to tissues via:

a. Margination of neutrophils to the peripheral plasmatic of the vessel rather than the
central axial stream
b. Pavementing: Adhesion of neutrophils to endothelial cells in venules at site of
acute inflammation
c. Emigration: neutrophils pass between endothelial cells into the tissue
Acute inflammation
Inflammation is the reaction of the tissue elements to injury. Vascular changes occur,
resulting in the generation of a protein rich exudate. So long as the injury does not
totally destroy the existing tissue architecture, the episode may resolve with
restoration of original tissue architecture.
Vascular changes
Vasodilation occurs and persists throughout the inflammatory phase.
Inflammatory cells exit the circulation at the site of injury.
The equilibrium that balances Starlings forces within capillary beds is
disrupted and a protein rich exudate will form as the vessel walls also become
more permeable to proteins.
The high fibrinogen content of the fluid may form a fibrin clot. This has
several important immunomodulatory functions.
Sequelae
Resolution Typically occurs with minimal initial injury
Stimulus removed and normal tissue architecture
results
Organisation Delayed removed of exudate
Tissues undergo organisation and usually fibrosis
Suppuration Typically formation of an abscess or an empyema
Sequestration of large quantities of dead
neutrophils
Progression to chronic
inflammation
Coupled inflammatory and reparative activities
Usually occurs when initial infection or
suppuration has been inadequately managed
Causes
Microbacterial infections e.g. Viruses, exotoxins or endotoxins released by
bacteria
Chemical agents
Physical agents e.g. Trauma
Hypersensitivity reactions

Tissue necrosis
Presence of neutrophil polymorphs is a histological diagnostic feature of acute
inflammation Theme: Liver lesions
A. Haemangioma
B. Hepatocellular carcinoma
C. Hepatic metastasis
D. Polycystic liver disease
E. Simple liver cyst
F. Hyatid cyst
G. Amoebic abscess
H. Mesenchymal hamartoma
Please select the most likely liver lesion for the scenario given. Each option may be
used once, more than once or not at all.
38. A 42 year old lady has suffered from hepatitis C for many years and has also
developed cirrhosis. On routine follow up, an ultrasound has demonstrated a
2.5cm lesion in the right lobe of the liver.
Hepatocellular carcinoma
In patients with cirrhosis the presence of a lesion >2cm is highly suggestive
of malignancy. The diagnosis is virtually confirmed if the AFP is
>400ng/mL.
39. A 25 year old man from the far east presents with a fever and right upper
quadrant pain. As part of his investigations a CT scan shows an ill defined
lesion in the right lobe of the liver.
You answered Mesenchymal hamartoma
The correct answer is Amoebic abscess
Amoebic abscesses will tend to present in a similar fashion to other pyogenic
liver abscesses. They should be considered in any individual presenting from
a region where Entamoeba histiolytica is endemic. Treatment with
metronidazole usually produces a marked clinical response.

40. A 42 year old lady presents with right upper quadrant pain and a sensation of
abdominal fullness. An ultrasound scan demonstrates a 6.5 cm hyperechoic
lesion in the right lobe of the liver. Serum AFP is normal.
Haemangioma
A large hyperechoic lesion in the presence of normal AFP is likely to be a
haemangioma. An HCC of equivalent size will almost always result in rise in
AFP.
Benign liver lesions
Benign liver lesions
Haemangioma Most common benign tumours of mesenchymal origin
Incidence in autopsy series is 8%
Cavernous haemangiomas may be enormous
Clinically they are reddish purple hypervascular lesions
Lesions are normally separated from normal liver by ring of
fibrous tissue
On ultrasound they are typically hyperechoic
Liver cell
adenoma
90% develop in women in their third to fifth decade
Linked to use of oral contraceptive pill
Lesions are usually solitary
They are usually sharply demarcated from normal liver
although they usually lack a fibrous capsule
On ultrasound the appearances are of mixed echoity and
heterogeneous texture. On CT most lesions are hypodense
when imaged prior to administration of IV contrast agents
In patients with haemorrhage or symptoms removal of the
adenoma may be required
Mesenchymal
hamartomas
Congential and benign, usually present in infants. May compress
normal liver
Liver abscess Biliary sepsis is a major predisposing factor
Structures drained by the portal venous system form the
second largest source
Common symptoms include fever, right upper quadrant
pain. Jaundice may be seen in 50%
Ultrasound will usually show a fluid filled cavity,
hyperechoic walls may be seen in chronic abscesses
Amoebic abscess Liver abscess is the most common extra intestinal
manifestation of amoebiasis

Between 75 and 90% lesions occur in the right lobe
Presenting complaints typically include fever and right
upper quadrant pain
Ultrasonography will usually show a fluid filled structure
with poorly defined boundaries
Aspiration yield sterile odourless fluid which has an
anchovy paste consistency
Treatment is with metronidazole
Hyatid cysts Seen in cases of Echinococcus infection
Typically an intense fibrotic reaction occurs around sites of
infection
The cyst has no epithelial lining
Cysts are commonly unilocular and may grow to 20cm in
size. The cyst wall is thick and has an external laminated
hilar membrane and an internal enucleated germinal layer
Typically presents with malaise and right upper quadrant
pain. Secondary bacterial infection occurs in 10%.
Liver function tests are usually abnormal and eosinophilia is
present in 33% cases
Ultrasound may show septa and hyatid sand or daughter
cysts.
Percutaneous aspiration is contra indicated
Treatment is by sterilisation of the cyst with mebendazole
and may be followed by surgical resection. Hypertonic
swabs are packed around the cysts during surgery
Polycystic liver
disease
Usually occurs in association with polycystic kidney disease
Autosomal dominant disorder
Symptoms may occur as a result of capsular stretch
Cystadenoma Rare lesions with malignant potential
Usually solitary multiloculated lesions
Liver function tests usually normal
Ultrasonography typically shows a large anechoic, fluid
filled area with irregular margins. Internal echos may result
from septa
Surgical resection is indicated in all cases
Which of the following disorders is associated with massive splenomegaly?
A. Acute lymphoblastic leukaemia
B. Acute myeloblastic leukaemia
C. Acute myelomonocytic leukaemia

D. Acute monoblastic leukaemia
E. Chronic granulocytic leukaemia
Chronic leukaemia is more likely to be associated with splenomegaly than acute
leukaemia.
Spleen
Embryology: derived from mesenchymal tissue
Shape: orange segment
Position: below 9th-12th ribs
Weight: 75-150g
Relations
Superiorly- diaphragm
Anteriorly- gastric impression
Posteriorly- kidney
Inferiorly- colon
Hilum: tail of pancreas and splenic vessels (splenic artery divides here,
branches pass to the white pulp transporting plasma)
Forms apex of lesser sac (containing short gastric vessels)
Contents - White pulp: immune function. Contains central trabecular artery. The germinal
centres are supplied by arterioles called penicilliary radicles.
- Red pulp: filters abnormal red blood cells
Function
Filtration of abnormal blood cells and foreign bodies such as bacteria.
Immunity: IgM. Production of properdin, and tuftsin which help target fungi
and bacteria for phagocytosis.
Haematopoiesis: up to 5th month gestation or in haematological disorders.
Pooling: storage of 40% platelets.
Iron reutilisation
Storage red blood cells-animals, not humans.
Storage monocytes
Disorders of the spleen Massive splenomegaly
Myelofibrosis

Chronic myeloid leukaemia
Visceral leishmaniasis (kala-azar)
Malaria
Gaucher's syndrome
Other causes (as above plus)
Portal hypertension e.g. secondary to cirrhosis
Lymphoproliferative disease e.g. CLL, Hodgkin's
Haemolytic anaemia
Infection: hepatitis, glandular fever
Infective endocarditis
Sickle-cell*, thalassaemia
Rheumatoid arthritis (Felty's syndrome)
*the majority of adults patients with sickle-cell will have an atrophied spleen due to
repeated infarction
Causes of primary chronic inflammation do not include which of the following?
A. Sarcoidosis
B. Tuberculosis
C. Ulcerative colitis
D. Prostheses
E. Chronic cholecystitis
Chronic cholecystitis is caused by recurrent episodes of acute inflammation.
Prosthetic implants may be the site of primary chronic inflammation. A common
example clinically is breast implants which may become encapsulated. The
subsequent fibrosis then results in distortion and may be painful.
Chronic inflammation
Overview Chronic inflammation may occur secondary to acute inflammation.In most cases
chronic inflammation occurs as a primary process. These may be broadly viewed as
being one of three main processes:
Persisting infection with certain organisms such as Mycobacterium
tuberculosis which results in delayed type hypersensitivity reactions and
inflammation.

Prolonged exposure to non-biodegradable substances such as silica or suture
materials which may induce an inflammatory response.
Autoimmune conditions involving antibodies formed against host antigens.
Acute vs. Chronic inflammation
Acute inflammation Chronic inflammation
Changes to existing vascular structure and
increased permeability of endothelial cells
Angiogenesis predominates
Infiltration of neutrophils Macrophages, plasma cells and
lymphocytes predominate
Process may resolve with:
Suppuration
Complete resolution
Abscess formation
Progression to chronic inflammation
Healing by fibrosis
Healing by fibrosis is the main
result
Granulomatous inflammation A granuloma consists of a microscopic aggregation of macrophages (with epithelial
type arrangement =epitheliod). Large giant cells may be found at the periphery of
granulomas.
Mediators Growth factors released by activated macrophages include agents such as interferon
and fibroblast growth factor (plus many more). Some of these such as interferons may
have systemic features resulting in systemic symptoms and signs, which may be
present in individuals with long standing chronic inflammation.
The finding of granulomas is pathognomonic of chronic inflammation, as illustrated
in this biopsy from a patient with colonic Crohns disease
Image sourced from Wikipedia

A 30 year old man is trapped in a house fire and sustains 30% partial and full
thickness burns to his torso and limbs. Three days following admission he has a brisk
haematemesis. Which of the following is the most likely explanation for this event?
A. Dieulafoy lesion
B. Curlings ulcers
C. Mallory Weiss tear
D. Depletion of platelets
E. Depletion of clotting factors
Stress ulcers in burns patients are referred to as Curlings ulcers and may cause
haematemesis.
Burns
Types of burn
Type of burn Skin layers
affected
Skin
appearance
Blanching Management
Epidermal/Superficial Epidermis Red, moist Yes
Superficial partial
thickness
Epidermis and
part of papillary
dermis affected
Pale, dry Yes Normally heals
with no
intervention
Deep partial thickness Epidermis, whole
papillary dermis
affected
Mottled red
colour
No Needs surgical
intervention
(depending on
site)
Full thickness Whole skin layer
and subcutaneous
tissue affected
Dry, leathery
hard wound
No Burns centre
Depth of burn assessment
Bleeding on needle prick
Sensation
Appearance
Blanching to pressure
Percentage burn estimation Lund Browder chart: most accurate even in children

Wallace rule of nines
Palmar surface: surface area palm = 0.8% burn
>15% body surface area burns in adults needs urgent burn fluid resuscitation
Transfer to burn centre if:
Need burn shock resuscitation
Face/hands/genitals affected
Deep partial thickness or full thickness burns
Significant electrical/chemical burns
Escharotomies
Indicated in circumferential full thickness burns to the torso or limbs.
Careful division of the encasing band of burn tissue will potentially improve
ventilation (if the burn involves the torso), or relieve compartment syndrome
and oedema (where a limb is involved)
References www.euroburn.org/e107files/downloads/guidelinesburncare.pdf
Hettiaratchy S & Papini R. Initial management of a major burn: assessment and
resuscitation. BMJ 2004;329:101-103
Theme: Adrenal gland disorders
A. Nelsons syndrome
B. Conns syndrome
C. Cushings syndrome
D. Benign incidental adenoma
E. Malignant adrenal adenoma
F. Waterhouse- Friderichsen syndrome
G. Metastatic lesion
H. Walker - Warburg syndrome
I. Phaeochromocytoma
Please select the most appropriate adrenal disorder for the scenario given. Each
disorder may be selected once, more than once or not at all.
44. A 19 year old lady is admitted to ITU with severe meningococcal sepsis. She
is on maximal inotropic support and a CT scan of her chest and abdomen is
performed. The adrenal glands show evidence of diffuse haemorrhage.
Waterhouse- Friderichsen syndrome
This is often a pre-terminal event and is associated with profound sepsis and
coagulopathy.
45. A 34 year old lady is admitted with recurrent episodes of non-specific
abdominal pain. On each admission all blood investigations are normal, as are
her observations. On this admission a CT scan was performed. This
demonstrates a 1.5cm nodule in the right adrenal gland. This is associated
with a lipid rich core. Urinary VMA is within normal limits. Other hormonal
studies are normal.
You answered Nelsons syndrome
The correct answer is Benign incidental adenoma
This is typical for a benign adenoma.Benign adenomas often have a lipid rich
core that is readily identifiable on CT scanning. In addition the nodules are
often well circumscribed.
46. A 38 year old man is noted to have a blood pressure of 175/110 on routine
screening. On examination there are no physical abnormalities of note. CT
scanning shows a left sided adrenal mass. Plasma metanephrines are elevated.
Phaeochromocytoma
Hypertension in a young patient without any obvious cause should be
investigated. Urinary VMA and plasma metanephrines are typically elevated.
Phaeochromocytoma and adrenal lesions
Phaeochromocytoma Neuroendocrine tumour of the chromaffin cells of the adrenal medulla. Hypertension
and hyperglycaemia are often found.
10% of cases are bilateral.
10% occur in children.
11% are malignant (higher when tumour is located outside the adrenal).
10% will not be hypertensive.
Familial cases are usually linked to the Multiple endocrine neoplasia syndromes
(considered under its own heading).
Most tumours are unilateral (often right sided) and smaller than 10cm.
Diagnosis Urine analysis of vanillymandelic acid (VMA) is often used (false positives may
occur e.g. in patients eating vanilla ice cream!)
Blood testing for plasma metanephrine levels.
CT and MRI scanning are both used to localise the lesion.
Treatment Patients require medical therapy first. An irreversible alpha adrenoreceptor blocker
should be given, although minority may prefer reversible bockade(1). Labetolol may
be co-administered for cardiac chronotropic control. Isolated beta blockade should not
be considered as it will lead to unopposed alpha activity.
These patients are often volume depleted and will often require moderate volumes of
intra venous normal saline perioperatively.
Once medically optimised the phaeochromocytoma should be removed. Most
adrenalectomies can now be performed using a laparoscopic approach(2). The
adrenals are highly vascular structures and removal can be complicated by
catastrophic haemorrhage in the hands of the inexperienced. This is particularly true
of right sided resections where the IVC is perilously close. Should the IVC be
damaged a laparotomy will be necessary and the defect enclosed within a Satinsky
style vascular clamp and the defect closed with prolene sutures. Attempting to
interfere with the IVC using any instruments other than vascular clamps will result in
vessel trauma and make a bad situation much worse.
Incidental adrenal lesions Adrenal lesions may be identified on CT scanning performed for other reasons(3).
Factors suggesting benign disease on CT include(4):
Size less than 3cm
Homogeneous texture
Lipid rich tissue
Thin wall to lesion
All patients with incidental lesions should be managed jointly with an endocrinologist
and full work up as described above. Patients with functioning lesions or those with
adverse radiological features (Particularly size >3cm) should proceed to surgery.
References 1. Weingarten TN, Cata JP, O'Hara JF, Prybilla DJ, Pike TL, Thompson GB, et al.
Comparison of two preoperative medical management strategies for laparoscopic
resection of pheochromocytoma. Urology. 2010 Aug;76(2):508 e6-11.

2. Nguyen PH, Keller JE, Novitsky YW, Heniford BT, Kercher KW. Laparoscopic
approach to adrenalectomy: review of perioperative outcomes in a single center. Am
Surg. 2011 May;77(5):592-6.
3. Ng VW, Ma RC, So WY, Choi KC, Kong AP, Cockram CS, et al. Evaluation of
functional and malignant adrenal incidentalomas. Arch Intern Med. 2010 Dec
13;170(22):2017-20.
4. Muth A, Hammarstedt L, Hellstrom M, Sigurjonsdottir HA, Almqvist E, Wangberg
B. Cohort study of patients with adrenal lesions discovered incidentally. Br J Surg.
2011 May 27.
A 15 year old boy is admitted with colicky abdominal pain of 6 hours duration. On
examination he has a soft abdomen, on systemic examination he has brownish spots
around his mouth, feet and hands. His mother underwent surgery for intussusception,
aged 12, and has similar lesions. What is the most likely underlying diagnosis?
A. Li Fraumeni syndrome
B. Peutz-Jeghers syndrome
C. Addisons disease
D. McCune -Albright syndrome
E. Appendicitis
This is most likely to be Peutz-Jeghers syndrome. Addisons and McCune Albright
syndrome may produce similar skin changes but the intussusception resulting from
polyps combined with the autosomal inheritance pattern makes this the most likely
diagnosis.
Peutz-Jeghers syndrome
Peutz-Jeghers syndrome is an autosomal dominant condition characterised by
numerous benign hamartomatous polyps in the gastrointestinal tract. It is also
associated with pigmented freckles on the lips, face, palms and soles. Around 50% of
patients will have died from a gastrointestinal tract cancer by the age of 60 years.
Genetics
Autosomal dominant
Responsible gene encodes serine threonine kinase LKB1 or STK11
Features

Hamartomatous polyps in GI tract (mainly small bowel)
Pigmented lesions on lips, oral mucosa, face, palms and soles
Intestinal obstruction e.g. intussusception (which may lead to diagnosis)
Gastrointestinal bleeding
Management
Conservative unless complications develop
Which of the following is not included in Multiple Endocrine Neoplasia Type 2b?
A. Phaeochromocytoma
B. Visceral ganglioneuromas
C. Thyroid medullary carcinoma
D. Zollinger Ellison syndrome
E. Marfanoid features
MEN IIB
Medullary thyroid cancer
Phaeochromocytoma
Mucosal neuroma
Marfanoid appearance
Multiple Endocrine Neoplasia
Multiple endocrine neoplasia (MEN) is inherited as an autosomal dominant disorder.
The table below summarises the three main types of MEN:
MEN type I MEN type IIa MEN type IIb
Mnemonic 'three P's':
Parathyroid (95%): Parathyroid adenoma
Pituitary (70%):
Prolactinoma/ACTH/Growth Hormone
secreting adenoma
Pancreas (50%): Islet cell
tumours/Zollinger Ellison syndrome
Phaeochromocytoma
Medullary thyroid
cancer (70%)
Hyperparathyroidism
(60%)
Same as MEN IIa
with addition of:
Marfanoid body
habitus
Mucosal neuromas

also: Adrenal (adenoma) and thyroid
(adenoma)
MENIN gene (chromosome 11)
Most common presentation =
hypercalcaemia
RET oncogene
(chromosome 10)
RET oncogene
(chromosome 10)
Which virus is associated with Kaposi's sarcoma?
A. Human herpes virus 8
B. Human papillomavirus 16
C. Human T-lymphotropic virus 1
D. Epstein-Barr virus
E. Human papillomavirus 18
Oncoviruses
Viruses which cause cancer
These may be detected on blood test and prevented by vaccine
These are the main types of oncoviruses and their diseases:
Oncovirus Cancer
Epstein-Barr virus Burkitt's lymphoma
Hodgkin's lymphoma
Post transfusion lymphoma
Nasopharyngeal carcinoma
Human papillomavirus 16/18 Cervical cancer
Anal cancer
Penile cancer
Vulval cancer
Oropharyneal cancer
Human herpes virus 8 Kaposi's sarcoma
Hepatitis B virus Hepatocellular carcinoma
Hepatitis C virus Hepatocellular carcinoma
Human T-lymphotropic virus 1 Tropical spastic paraparesis
Adult T cell leukaemia

Which of the following is not a feature of Wallerian Degeneration?
A. May result from an axonotmesis
B. May occur in either the central or peripheral nervous systems
C. The axon remains excitable throughout the whole process
D. The distal neuronal stump is affected
E. Is a component of the healing process following neuronal injury
The axon loses its excitability once the process is established.
Wallerian degeneration
- Is the process that occurs when a nerve is cut or crushed.
- It occurs when the part of the axon separated from the neuron's cell nucleus
degenerates.
- It usually begins 24 hours following neuronal injury and the distal axon remains
excitable up until this time.
- The degeneration of the axon is following by breakdown of the myelin sheath, a
process that occurs by infiltration of the site with macrophages.
- Eventually regeneration of the nerve may occur although recovery will depend on
the extent and manner of injury
A 45 year old woman complains of painful tingling in her fingers. The pain is relieved
by hanging the arm over the side of the bed. She has a positive Tinel's sign. Which of
the following is most likely to contribute to her diagnosis?
A. Methotrexate use
B. Crohn's disease
C. Hyperthyroidism
D. Tuberculosis
E. Rheumatoid arthritis
This woman has a diagnosis of carpal tunnel syndrome. Rheumatological disorders
are a common cause. Clinical examination should focus on identifying stigmata of
rheumatoid arthritis, such as rheumatoid nodules, vasculitic lesions and
metacarpophalangeal joint arthritis.
Carpal tunnel syndome

Carpal tunnel syndrome is caused by compression of median nerve in the carpal
tunnel
History
pain/pins and needles in thumb, index, middle finger e.g. at night
patient flicks hand to obtain relief
Examination
weakness of thumb abduction
wasting of thenar eminence (NOT hypothenar)
Tinel's sign: tapping causes paraesthesia
Phalen's sign: flexion of wrist causes symptoms
Causes of carpal tunnel syndrome
MEDIAN TRAP Mnemonic
Myxoedema
Edema premenstrually
Diabetes
Idiopathic
Agromegaly
Neoplasm
Trauma
Rheumatoid arthritis
Amyloidosis
Pregnancy
Management
Non surgical
treatment
Surgery
May resolve
spontaneously
Avoid precipitants and
reassurance
Night-time splints
Local steroid
injections
Complete division of the flexor retinaculum and
decompression of the tunnel (successful in approximately
80% of patients)
Which of the following is not an oncogene?
A. ras

B. myc
C. sis
D. Ki 67
E. erb-B
Ki 67 is a nuclear proliferation marker (used in immunohistochemistry). Although,
Ki67 positivity is a marker of malignancy, it is not itself, an oncogene.
Oncogenes
Oncogenes are cancer promoting genes that are derived from normal genes (proto-
oncogenes). Proto-oncogenes play an important physiological role in cellular growth.
They are implicated in the development of up to 20% of human cancers.
Proto-oncogenes may become oncogenes via the following processes:
Mutation (point mutation)
Chromosomal translocation
Increased protein expression
Only one mutated copy of the gene is needed for cancer to occur - a dominant effect
Classification of oncogenes
Growth factors e.g. Sis
Transcription factors e.g. Myc
Receptor tyrosine kinase e.g. RET
Cytoplasmic tyrosine kinase e.g. Src
Regulatory GTPases e.g. Ras
Tumour supressor genes Tumour supressor genes restrict or repress cellular proliferation in normal cells. Their
inactivation through mutation or germ line incorporation is implicated in renal,
colonic, breast, bladder and many other cancers. One of the best known tumour
supressor genes is p53. p53 gene offers protection by causing apoptosis of damaged
cells. Other well known genes include BRCA 1 and 2.
A 30 year old male presents with a painless swelling of the testis. Histologically the
stroma has lymphocytic infiltrate. The most likely diagnosis is :
A. Differentiated teratoma
B. Malignant undifferentiated teratoma

C. Classical seminoma
D. Spermatocytic seminoma
E. Anaplastic seminoma
Seminoma is the commonest type of testicular tumour and is more common in males
aged between 30-40 years. Classical seminoma is the commonest subtype and
histology shows lymphocytic stromal infiltrate. Other subtypes include:
1. Spermatocytic: tumour cells resemble spermatocytes. Excellent prognosis.
2. Anaplastic
3. Syncytiotrophoblast giant cells: beta hCG present in cells
A teratoma is common in males aged 20-30 years.
Testicular disorders
Testicular cancer Testicular cancer is the most common malignancy in men aged 20-30 years. Around
95% of cases of testicular cancer are germ-cell tumours. Germ cell tumours may
essentially be divided into:
Tumour type Key features Tumour
markers
Pathology
Seminoma Commonest
subtype (50%)
Average age at
diagnosis = 40
Even advanced
disease
associated with
5 year survival
of 73%
AFP usually
normal
HCG
elevated in 10%
seminomas
Lactate
dehydrogenase;
elevated in 10-
20% seminomas
(but also in
many other
conditions)
Sheet like
lobular
patterns of
cells with
substantial
fibrous
component.
Fibrous septa
contain
lymphocytic
inclusions and
granulomas
may be seen.
Non seminomatous germ
cell tumours (42%)
Teratoma
Yolk sac tumour
Choriocarcinoma
Mixed germ cell
tumours (10%)
Younger age at
presentation =20-30
years
Advanced disease
carries worse prognosis
(48% at 5 years)
Retroperitoneal
lymph node dissection
may be needed for
residual disease after
chemotherapy
AFP elevated
in up to 70% of
cases
HCG
elevated in up
to 40% of cases
Other
markers rarely
helpful
Heterogenous
texture with
occasional
ectopic tissue
such as hair

Image demonstrating a classical seminoma, these tumours are typically more uniform
than teratomas
Image sourced from Wikipedia
Risk factors for testicular cancer
Cryptorchidism
Infertility
Family history
Klinefelter's syndrome
Mumps orchitis
Features
A painless lump is the most common presenting symptom

Pain may also be present in a minority of men
Other possible features include hydrocele, gynaecomastia
Diagnosis
Ultrasound is first-line
CT scanning of the chest/ abdomen and pelvis is used for staging
Tumour markers (see above) should be measured
Management
Orchidectomy (Inguinal approach)
Chemotherapy and radiotherapy may be given depending on staging
Abdominal lesions >1cm following chemotherapy may require retroperitoneal
lymph node dissection.
Prognosis is generally excellent
5 year survival for seminomas is around 95% if Stage I
5 year survival for teratomas is around 85% if Stage I
Benign disease
Epididymo-orchitis Acute epididymitis is an acute inflammation of the epididymis, often involving the
testis and usually caused by bacterial infection.
Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or
chlamydia are the usual infections.
Amiodarone is a recognised non infective cause of epididymitis, which
resolves on stopping the drug.
Tenderness is usually confined to the epididymis, which may facilitate
differentiating it from torsion where pain usually affects the entire testis.
Testicular torsion
Twist of the spermatic cord resulting in testicular ischaemia and necrosis.
Most common in males aged between 10 and 30 (peak incidence 13-15 years)
Pain is usually severe and of sudden onset.
Cremasteric reflex is lost and elevation of the testis does not ease the pain.
Treatment is with surgical exploration. If a torted testis is identified then both
testis should be fixed as the condition of bell clapper testis is often bilateral.

A 48 year old women presents with recurrent loin pain and fevers. Investigation
reveals a staghorn calculus of the left kidney. Infection with which of the following
organisms is most likely?
A. Staphylococcus saprophyticus
B. Proteus mirabilis
C. Klebsiella
D. E-Coli
E. Staphylococcus epidermidis
Theme from April 2012 Exam
Infection with Proteus mirabilis accounts for 90% of all proteus infections. It has a
urease producing enzyme. This will tend to favor urinary alkalinisation which is a
relative per-requisite for the formation of staghorn calculi.
Renal stones
Type of
stones
Features Percentage of
all calculi
Calcium
oxalate
Hypercalciuria is a major risk factor (various causes)
Hyperoxaluria may also increase risk
Hypocitraturia increases risk because citrate forms
complexes with calcium making it more soluble
Stones are radio-opaque (though less than calcium
phosphate stones)
Hyperuricosuria may cause uric acid stones to which
calcium oxalate binds
85%
Cystine Inherited recessive disorder of transmembrane cystine
transport leading to decreased absorption of cystine
from intestine and renal tubule
Multiple stones may form
Relatively radiodense because they contain sulphur
1%
Uric acid Uric acid is a product of purine metabolism
May precipitate when urinary pH low
May be caused by diseases with extensive tissue
breakdown e.g. malignancy
More common in children with inborn errors of
metabolism
Radiolucent
5-10%
Calcium
phosphate
May occur in renal tubular acidosis, high urinary pH
increases supersaturation of urine with calcium and
phosphate
10%

Renal tubular acidosis types 1 and 3 increase risk of
stone formation (types 2 and 4 do not)
Radio-opaque stones (composition similar to bone)
Struvite Stones formed from magnesium, ammonium and
phosphate
Occur as a result of urease producing bacteria (and are
thus associated with chronic infections)
Under the alkaline conditions produced, the crystals
can precipitate
Slightly radio-opaque
2-20%
Effect of urinary pH on stone formation Urine pH will show individual variation (from pH 5-7). Post prandially the pH falls as
purine metabolism will produce uric acid. Then the urine becomes more alkaline
(alkaline tide). When the stone is not available for analysis the pH of urine may help
to determine which stone was present.
Stone type Urine acidity Mean urine pH
Calcium phosphate Normal- alkaline >5.5
Calcium oxalate Variable 6
Uric acid Acid 5.5
Struvate Alkaline >7.2
Cystine Normal 6.5
Causes of granulomatous disease do not include:
A. Amiodarone
B. Allopurinol
C. Sulphonamides
D. Beryllium
E. Wegener's granulomatosis
Allopurinol and sulphonamides cause hepatic granulomas.
Chronic inflammation
Overview Chronic inflammation may occur secondary to acute inflammation.In most cases
chronic inflammation occurs as a primary process. These may be broadly viewed as
being one of three main processes:

Persisting infection with certain organisms such as Mycobacterium
tuberculosis which results in delayed type hypersensitivity reactions and
inflammation.
Prolonged exposure to non-biodegradable substances such as silica or suture
materials which may induce an inflammatory response.
Autoimmune conditions involving antibodies formed against host antigens.
Acute vs. Chronic inflammation
Acute inflammation Chronic inflammation
Changes to existing vascular structure and
increased permeability of endothelial cells
Angiogenesis predominates
Infiltration of neutrophils Macrophages, plasma cells and
lymphocytes predominate
Process may resolve with:
Suppuration
Complete resolution
Abscess formation
Progression to chronic inflammation
Healing by fibrosis
Healing by fibrosis is the main
result
Granulomatous inflammation A granuloma consists of a microscopic aggregation of macrophages (with epithelial
type arrangement =epitheliod). Large giant cells may be found at the periphery of
granulomas.
Mediators Growth factors released by activated macrophages include agents such as interferon
and fibroblast growth factor (plus many more). Some of these such as interferons may
have systemic features resulting in systemic symptoms and signs, which may be
present in individuals with long standing chronic inflammation.
The finding of granulomas is pathognomonic of chronic inflammation, as illustrated
in this biopsy from a patient with colonic Crohns disease

Image sourced from Wikipedia
Theme: Facial nerve palsy
A. Adenoid cystic carcinoma
B. Cerebrovascular accident
C. Petrous temporal fracture
D. Warthins tumour
E. Sarcoidosis
F. Pleomorphic adenoma
G. Cholesteatoma
Please select the most likely cause of facial nerve palsy for the scenario given. Each
option may be used once, more than once or not at all.
56. A 22 year old man presents with symptoms of lethargy and bilateral facial
nerve palsy. On examination he has bilateral parotid gland enlargement.
You answered Adenoid cystic carcinoma
The correct answer is Sarcoidosis
Theme from 2011 Exam
Facial nerve palsy is the commonest neurological manifestation of sarcoid. It
usually resolves. The absence of ear discharge or discrete lesion on palpation
is against the other causes.
57. A 21 year old man presents with a unilateral facial nerve palsy after being hit
in the head. On examination he has a right sided facial nerve palsy and a
watery discharge from his nose.
Petrous temporal fracture
Nasal discharge of clear fluid and recent head injury makes a basal skull
fracture the most likely underlying diagnosis.
58. A 43 year old lady presents with symptoms of chronic ear discharge and a
right sided facial nerve palsy. On examination she has foul smelling fluid
draining from her right ear and a complete right sided facial nerve palsy.
Cholesteatoma
Foul smelling ear discharge and facial nerve weakness is likely to be due to
cholesteatoma. The presence of a neurological deficit is a sinister feature.
Facial nerve palsy
Sarcoid Facial nerve palsy is the most frequent neurological manifestation
of sarcoid
Affects right and left side with equal frequency, may be bilateral
Typically resolves in up to 80% of cases
Cholesteatoma Destructive and expanding growth of keratinised squamous
epithelium
Patients often complain of chronic ear discharge
Infection with Pseudomonas may occur resulting in foul smell to
discharge
Aquired lesions usually arise from the Pars flaccida region of the
tympanic membrane
Surgical removal and mastoidectomy may be needed
Recurrence rates of 20% may be seen following surgery
Basal skull
fracture
History of head injury
Presence of features such as Battles sign on examination
Clinical presence of CSF leak strongly supports diagnosis
Assessment is by CT and MRI scan
Prophylactic antibiotics should be given in cases of CSF leak
A 59 year old lady is referred from the NHS breast screening program. A recent
mammogram is reported as showing linear, branching microcalcification with coarse
granules. Which disease process is the most likely underlying cause of these
appearances?

A. Invasive lobular cancer
B. Lobular carcinoma in situ
C. Cribriform type ductal carcinoma in situ
D. Comedo type ductal carcinoma in situ
E. Fibroadenosis
Comedo type DCIS is usually associated with microcalcifications. Cribriform lesions
are usually multifocal but less likely to form microcalcifications. Lobular cancers and
in situ lesions rarely form microcalcifications and are difficult to detect using
mammography.
Breast cancer - In situ disease
Breast cancer that has yet to invade the basement membrane is referred to as in situ
disease. Both ductal and lobular in situ variants are recognised.
Ductal carcinoma in situ
Sub types include; comedo, cribriform, micropapillary and solid
Comdeo DCIS is most likely to form microcalcifications
Cribriform and micropapillary are most likely to be multifocal
Most lesions are mixed (composed of multiple subtypes)
High nuclear grade DCIS is associated with more malignant characteristics
(loss of p53, increase erbB2 expression)
Local excision of low nuclear grade DCIS will usually produce satisfactory
outcomes.
Multifocal lesions, large and high nuclear grade lesions will usually require
mastectomy
Lobular carcinoma in situ
Much rarer than DCIS
Does not form microcalcifications
Usually single growth pattern
When an invasive component is found it is less likely to be associated with
axillary nodal metastasis than with DCIS
Low grade LCIS is usually treated by monitoring rather than excision
In patients with an annular pancreas where is the most likely site of obstruction?
A. The first part of the duodenum

B. The second part of the duodenum
C. The fourth part of the duodenum
D. The third part of the duodenum
E. The duodeno-jejunal flexure
Theme from 2011 Exam
Theme from September 2012 Exam
The pancreas develops from two foregut outgrowths (ventral and dorsal). During rotation
the ventral bud and adjacent gallbladder and bile duct lie together and fuse. When the
pancreas fails to rotate normally it can compress the duodenum with development of
obstruction. Usually occurring as a result of associated duodenal malformation. The second
part of the duodenum is the commonest site.
Pancreas
The pancreas is a retroperitoneal organ and lies posterior to the stomach. It may be
accessed surgically by dividing the peritoneal reflection that connects the greater omentum
to the transverse colon. The pancreatic head sits in the curvature of the duodenum. It's tail
lies close to the hilum of the spleen, a site of potential injury during splenectomy.
Relations
Posterior to the pancreas
Pancreatic head Inferior vena cava
Common bile duct
Right and left renal veins
Superior mesenteric vein and artery
Pancreatic neck Superior mesenteric vein, portal vein
Pancreatic body- Left renal vein
Crus of diaphragm
Psoas muscle
Adrenal gland
Kidney

Aorta
Pancreatic tail Left kidney
Anterior to the pancreas
Pancreatic head 1st part of the duodenum
Pylorus
Gastroduodenal artery
SMA and SMV(uncinate process)
Pancreatic body Stomach
Duodenojejunal flexure
Pancreatic tail Splenic hilum
Superior to the pancreas
Coeliac trunk and its branches common hepatic artery and splenic artery
Grooves of the head of the pancreas
2nd and 3rd part of the duodenum
Arterial supply
Head: pancreaticoduodenal artery Rest: splenic artery
Venous drainage
Head: superior mesenteric vein Body and tail: splenic vein
Ampulla of Vater
Merge of pancreatic duct and common bile duct Is an important landmark, halfway along the second part of the duodenum, that
marks the anatomical transition from foregut to midgut (also the site of transition between regions supplied by coeliac trunk and SMA).

Image sourced from Wikipedia
Rate question:
1
2
3
4
5
Theme: Chest pain
A. Achalasia
B. Pulmonary embolus
C. Dissection of thoracic aorta
D. Boerhaaves syndrome
E. Gastro-oesophageal reflux
F. Carcinoma of the oesophagus
G. Oesophageal candidiasis
Please select the most likely cause for chest pain for the scenario given. Each option
may be used once, more than once or not at all.

3. A 43 year old man who has a long term history of alcohol misuse is admitted
with a history of an attack of vomiting after an episode of binge drinking. After
vomiting he developed sudden onset left sided chest pain, which is pleuritic in
nature. On examination he is profoundly septic and drowsy with severe
epigastric tenderness and left sided chest pain.
Boerhaaves syndrome
In patients with Boerhaaves the rupture is often on the left side. The story here
is typical. All patients should have a contrast study to confirm the diagnosis
and the affected site prior to thoracotomy.
4. A 22 year old man is admitted with severe retrosternal chest pain and recurrent
episodes of dysphagia. These occur sporadically and often resolve
spontaneously. On examination there are no physical abnormalities and the
patient seems well.
You answered Dissection of thoracic aorta
The correct answer is Achalasia
Achalasia may produce severe chest pain and many older patients may undergo
cardiac investigations prior to endoscopy.
Endoscopic injection with botulinum toxin is a popular treatment (although the
benefit is not long lasting). Cardiomyotomy is a more durable alternative.
5. An obese 53 year old man presents with symptoms of recurrent retrosternal
discomfort and dyspepsia. This is typically worse at night after eating a large
meal. On examination there is no physical abnormality to find.
Gastro-oesophageal reflux
Patients with GORD often have symptoms that are worse at night. In this age
group an Upper GI endoscopy should probably be performed.
Surgical chest pain
Dissection of
thoracic aorta
Tearing interscapular pain
Discrepancy in arterial blood pressures taken in both arms
May show mediastinal widening on chest x-ray
Diffuse
oesophageal
spasm
Spectrum of oesophageal motility disorders
Caused by uncoordinated contractions of oesphageal muscles
May show "nutcracker oesophagus" on barium swallow
Symptoms include dysphagia, retrosternal discomfort and
dyspepsia
Gastro-
oesphageal
reflux
Common cause of retrosternal discomfort
Usually associated with symptoms of regurgitation,
odynophagia and dyspepsia
Symptoms usually well controlled with PPI therapy
Risk factors include obesity, smoking and excess alcohol
consumption
Boerhaaves
syndrome
Spontaneous rupture of the oesophagus
Caused by episodes of repeated vomiting often in association
with alcohol excess
Typically there is an episode of repetitive vomiting followed
by severe chest and epigastric pain
Diagnosis is by CT and contrast studies
Treatment is surgical; during first 12 hours primary repair,
beyond this usually creation of controlled fistula with a T
Tube, delay beyond 24 hours is associated with fulminent
mediastinitis and is usually fatal.
Achalasia Difficulty swallowing, dysphagia to both liquids and solids
and sometimes chest pain
Usually caused by failure of distal oesphageal inhibitory
neurones
Diagnosis is by pH and manometry studies together with
contrast swallow and endoscopy
Treatment is with either botulinum toxin, pneumatic
dilatation or cardiomyotomy
A 32 year old woman presents with an episode of haemoptysis and is found to have
metastatic tumour present within the parenchyma of the lungs. This is biopsied and
subsequent histology shows clear cells. What is the most likely primary site?
A. Kidney
B. Breast
C. Liver
D. Adrenal
E. Bone

Clear cell tumours are a sub type of renal cell cancer it is associated with specific
genetic changes localised to chromosome 3.
Renal lesions
Lesion Disease specific features Treatment
Renal cell
carcinoma
Most present with
haematuria (50%)
Common renal tumour (85%
cases)
Paraneoplastic features
include hypertension and
polycythaemia
Most commonly has
haematogenous mestastasis
Usually radical or partial
nephrectomy
Nephroblastoma Rare childhood tumour
It accounts for 80% of all
genitourinary malignancies
in those under the age of 15
years
Up to 90% will have a mass
50% will be hypertensive
Diagnostic work up includes
ultrasound and CT scanning
Surgical resection combined
with chemotherapy (usually
vincristine, actinomycin D
and doxorubicin
Neuroblastoma Most common extracranial
tumour of childhood
80% occur in those under 4
years of age
Tumour of neural crest
origin (up to 50% occur in
the adrenal gland)
The tumour is usually
calcified and may be
diagnosed using MIBG
scanning
Staging is with CT
Surgical resection,
radiotherapy and
chemotherapy
Transitional cell
carcinoma
Accounts for 90% of upper
urinary tract tumour, but
only 10% of renal tumours
Males affected 3x more than
females
Occupational exposure to
industrial dyes and rubber
chemicals may increase risk
Up to 80% present with
Radical nephroureterectomy

painless haematuria
Diagnosis and staging is with
CT IVU
Angiomyolipoma 80% of these hamartoma
type lesions occur
sporadically, the remainder
are seen in those with
tuberous sclerosis
Tumour is composed of
blood vessels, smooth
muscle and fat
Massive bleeding may occur
in 10% of cases
50% of patients with lesions
>4cm will have symptoms
and will require surgical
resection
A laceration of the wrist produces a median nerve transaction. The wound is clean and
seen immediately after injury. Collateral soft tissue damage is absent. The patient asks
what the prognosis is. You indicate that the nerve should regrow at approximately:
A. 0.1 mm per day
B. 1 mm per day
C. 5 mm per day
D. 1 cm per day
E. None of the above
Transaction of a peripheral nerve results in hemorrhage and in retraction of the
several nerve ends. Almost immediately, degeneration of the axon distal to the injury
begins. Degeneration also occurs in the proximal fragment back to the first node of
Ranvier. Phagocytosis of the degenerated axonal fragments leaves neurilemmal sheath
with empty cylindrical spaces where the axons were. Several days following the
injury, axons from the proximal fragment begin to regrow. If they make contact with
the distal neurilemmal sheath, regrowth occurs at about the rate of 1 mm/day.
However, if associated trauma, fracture, infection, or separation of neurilemmal
sheath ends precludes contact between axons, growth is haphazard and a traumatic
neuroma is formed. When neural transaction is associated with widespread soft tissue
damage and hemorrhage (with increased probability of infection), many surgeons
choose to delay reapproximation of the severed nerve end for 3 to 4 weeks.
Nerve injury
There are 3 types of nerve injury:
Neuropraxia Nerve intact but electrical conduction is affected
Full recovery

Autonomic function preserved
Wallerian degeneration does not occur
Axonotmesis Axon is damaged and the myelin sheath is preserved. The
connective tissue framework is not affected.
Wallerian degeneration occurs.
Neurotmesis Disruption of the axon, myelin sheath and surrounding
connective tissue.
Wallerian degeneration occurs.
Wallerian Degeneration
Axonal degeneration distal to the site of injury.
Typically begins 24-36 hours following injury.
Axons are excitable prior to degeneration occurring.
Myelin sheath degenerates and is phagocytosed by tissue macrophages.
Nerve repair
Neuronal repair may only occur physiologically where nerves are in direct
contact. Where a large defect is present the process of nerve regeneration is
hampered and may not occur at all or result in the formation of a neuroma.
Where nerve regrowth occurs it typically occurs at a rate of 1mm per day.
Which of the following statements relating to gastric cancer is untrue?
A. It is associated with chronic helicobacter pylori infection
B. 5% of gastric malignancies are due to lymphoma
C. In the Lauren classification the diffuse type of adenocarcinoma typically
presents as a large exophytic growth in the antrum
D. Smoking is a risk factor
E. It is associated with acanthosis nigricans
The Lauren classification describes a diffuse type of adenocarcinoma (Linitis plastica type

lesion) and an intestinal type. The diffuse type is often deeply infiltrative and may be difficult
to detect on endoscopy. Barium meal appearances can be characteristic.
Gastric cancer
Overview
There are 700,000 new cases of gastric cancer worldwide each year. It is most common in
Japan and less common in western countries. It is more common in men and incidence rises
with increasing age. The exact cause of many sporadic cancer is not known, however,
familial cases do occur in HNPCC families. In addition, smoking and smoked or preserved
foods increase the risk. Japanese migrants retain their increased risk (decreased in
subsequent generations). The distribution of the disease in western countries is changing
towards a more proximal location (perhaps due to rising obesity).
Pathology
There is some evidence of support a stepwise progression of the disease through intestinal
metaplasia progressing to atrophic gastritis and subsequent dysplasia, through to cancer.
The favoured staging system is TNM. The risk of lymph node involvement is related to size
and depth of invasion; early cancers confined to submucosa have a 20% incidence of lymph
node metastasis. Tumours of the gastro-oesophageal junction are classified as below:
Type
1
True oesophageal cancers and may be associated with Barrett's oesophagus.
Type
2
Carcinoma of the cardia, arising from cardiac type epithelium
or short segments with intestinal metaplasia at the oesophagogastric junction.
Type
3
Sub cardial cancers that spread across the junction. Involve similar nodal stations to
gastric cancer.
Groups for close endoscopic monitoring
Intestinal metaplasia of columnar type Atrophic gastritis Low to medium grade dysplasia Patients who have previously undergone resections for benign peptic ulcer disease
(except highly selective vagotomy).
Referral to endoscopy
Patients of any age with
dyspepsia and any of the
following
Patients without
dyspepsia
Worsening dyspepsia
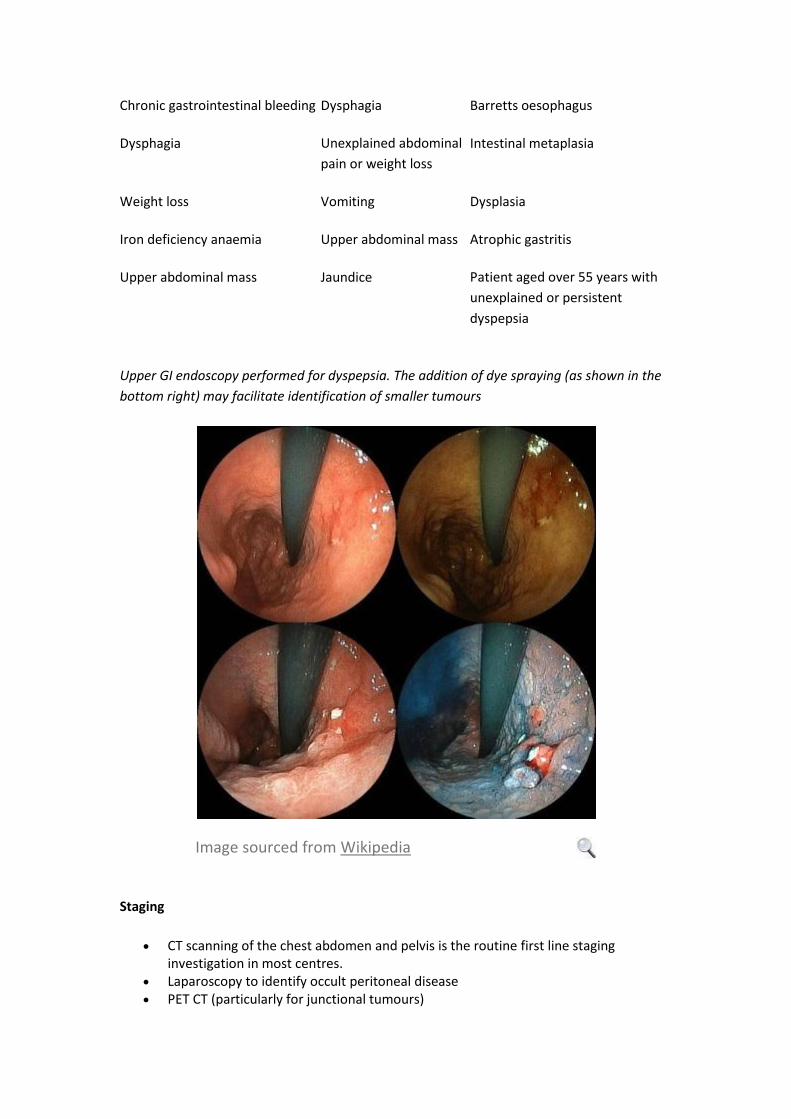
Chronic gastrointestinal bleeding Dysphagia Barretts oesophagus
Dysphagia Unexplained abdominal
pain or weight loss
Intestinal metaplasia
Weight loss Vomiting Dysplasia
Iron deficiency anaemia Upper abdominal mass Atrophic gastritis
Upper abdominal mass Jaundice Patient aged over 55 years with
unexplained or persistent
dyspepsia
Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as shown in the
bottom right) may facilitate identification of smaller tumours
Image sourced from Wikipedia
Staging
CT scanning of the chest abdomen and pelvis is the routine first line staging investigation in most centres.
Laparoscopy to identify occult peritoneal disease PET CT (particularly for junctional tumours)

Treatment
Proximally sited disease greater than 5-10cm from the OG junction may be treated by sub total gastrectomy
Total gastrectomy if tumour is <5cm from OG junction For type 2 junctional tumours (extending into oesophagus) oesophagogastrectomy is
usual Endoscopic sub mucosal resection may play a role in early gastric cancer confined to
the mucosa and perhaps the sub mucosa (this is debated) Lymphadenectomy should be performed. A D2 lymphadenectomy is widely
advocated by the Japanese, the survival advantages of extended lymphadenectomy have been debated. However, the overall recommendation is that a D2 nodal dissection be undertaken.
Most patients will receive chemotherapy either pre or post operatively.
Prognosis
UK Data
Disease extent Percentage 5 year survival
All RO resections 54%
Early gastric cancer 91%
Stage 1 87%
Stage 2 65%
Stage 3 18%
Operative procedure
Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis
General anaesthesia
Prophylactic intravenous antibiotics
Incision: Rooftop.
Perform a thorough laparotomy to identify any occult disease.
Mobilise the left lobe of the liver off the diaphragm and place a large pack over it. Insert a
large self retaining retractor e.g. omnitract or Balfour (take time with this, the set up should
be perfect). Pack the small bowel away.
Begin by mobilising the omentum off the transverse colon.
Proceed to detach the short gastric vessels.

Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling device.
Continue the dissection into the lesser sac taking the lesser omentum and left gastric artery
flush at its origin.
The lymph nodes should be removed en bloc with the specimen where possible.
Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull back on
the nasogastric tube. Divide the distal oesophagus and remove the stomach.
The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and bring a
loop of jejunum up to the oesophagus (to check it will reach). Divide the jejunum at this
point. Bring the divided jejunum either retrocolic or antecolic to the oesophagus.
Anastamose the oesophagus to the jejunum, using either interrupted 3/0 vicryl or a stapling
device. Then create the remainder of the Roux en Y reconstruction distally.
Place a jejunostomy feeding tube.
Wash out the abdomen and insert drains (usually the anastomosis and duodenal stump).
Help the anaesthetist insert the nasogastric tube (carefully!)
Close the abdomen and skin.
Enteral feeding may commence on the first post-operative day. However, most surgeons will
leave patients on free NG drainage for several days and keep them nil by mouth.
Which of the following statements relating to Gardners syndrome variant of familial
adenomatous polyposis coli is false?
A. It is an autosomal dominant condition
B. Patients may develop retroperitoneal desmoid tumours
C. The vast majority of the polyps are benign and thus the risk of
colorectal cancer is small
D. Patients are at increased risk of thyroid cancer
E. It is characterised by a mutation in the APC gene
The multiple polyps increase the risk of malignancy and most patients should undergo
a colectomy.
Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.
Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:

*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2
Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age
80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one
of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.
Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5
Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli
Which of the following statements relating to Gardners syndrome variant of familial
adenomatous polyposis coli is false?
A. It is an autosomal dominant condition
B. Patients may develop retroperitoneal desmoid tumours
C. The vast majority of the polyps are benign and thus the risk of

colorectal cancer is small
D. Patients are at increased risk of thyroid cancer
E. It is characterised by a mutation in the APC gene
The multiple polyps increase the risk of malignancy and most patients should undergo
a colectomy.
Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.
Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:
*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2
Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age
80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one
of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.

Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5
Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli
A 60-year-old man presents with lower urinary tract symptoms and is offered a PSA
test. Which one of the following could interfere with the PSA level?
A. Vigorous exercise in the past 48 hours
B. Poorly controlled diabetes mellitus
C. Drinking more than 4 units of alcohol in the past 48 hours
D. Smoking
E. Recent cholecystectomy
PSA testing
Prostate specific antigen (PSA) is a serine protease enzyme produced by normal and
malignant prostate epithelial cells. It has become an important tumour marker but
much controversy still exists regarding its usefulness as a screening tool.
The NHS Prostate Cancer Risk Management Programme (PCRMP) has published
updated guidelines in 2009 on how to handle requests for PSA testing in
asymptomatic men. A recent European trial (ERSPC) showed a statistically
significant reduction in the rate of death prostate cancer by 20% in men aged 55 to 69
years but this was associated with a high risk of over-diagnosis and over-treatment.
Having reviewed this and other data the National Screening Committee have decided
not to introduce a prostate cancer screening programme yet but rather allow men to
make an informed choice.
Age-adjusted upper limits for PSA were recommended by the PCRMP*:
{Age} {PSA level (ng/ml)}
50-59 years 3.0

60-69 years 4.0
> 70 years 5.0
PSA levels may also be raised by**:
benign prostatic hyperplasia (BPH)
prostatitis and urinary tract infection (NICE recommend to postpone the PSA
test for at least 1 month after treatment)
ejaculation (ideally not in the previous 48 hours)
vigorous exercise (ideally not in the previous 48 hours)
urinary retention
instrumentation of the urinary tract
Poor specificity and sensitivity
around 33% of men with a PSA of 4-10 ng/ml will be found to have prostate
cancer. With a PSA of 10-20 ng/ml this rises to 60% of men
around 20% with prostate cancer have a normal PSA
various methods are used to try and add greater meaning to a PSA level
including age-adjusted upper limits and monitoring change in PSA level with
time (PSA velocity or PSA doubling time)
*aide memoire for upper PSA limit: (age - 20) / 10
**whether digital rectal examination actually causes a rise in PSA levels is a matter of
debate
Which of the symptoms below is least typical of pancreatic cancer?
A. Painless jaundice
B. Hyperamylasaemia
C. Hyperglycaemia
D. Weight loss
E. Classical Courvoisier syndrome
Raised serum amylase is relatively uncommon. The typical Courvoisier syndrome
typically occurs in 20% and hyperglycaemia occurs in 15-20%.
Pancreatic cancer
Adenocarcinoma

Risk factors: Smoking, diabetes, Adenoma, Familial adenomatous polyposis
Mainly occur in the head of the pancreas (70%)
Spread locally and metastasizes to the liver
Carcinoma of the pancreas should be differentiated from other periampullary
tumours with better prognosis
Clinical features
Weight loss
Painless jaundice
Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a
late feature)
Pancreatitis
Trousseau's sign: migratory superficial thrombophlebitis
Investigations
USS: May miss small lesions
CT Scanning (pancreatic protocol). If unresectable on CT then no further
staging needed.
PET/CT for those with operable disease on CT alone
ERCP/ MRI for bile duct assessment.
Staging laparoscopy to exclude peritoneal disease.
Management
Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer
techniques include pylorus preservation and SMA/ SMV resection.
Carcinoma body and tail: poor prognosis, distal pancreatectomy if operable.
Usually adjuvent chemotherapy for resectable disease
ERCP and stent for jaundice and palliation.
Surgical bypass may be needed for duodenal obstruction.
A 53 year old man presents with dyspepsia. An upper GI endoscopy is performed and
Helicobacter pylori is identified. A duodenal ulcer is present in the first part of the
duodenum. Duodenal biopsies are taken and demonstrate epithelium that resembles
cells of the gastric antrum. Which of the following is the most likely explanation for
this process?
A. Hyperplasia of the crypts of Lieberkhun
B. Duodenal metaplasia
C. Duodenal dysplasia

D. Duodenal carcinoma
E. Hyptertrophy of Brunners glands
Metaplasia = cell type
conversion
Theme in January 2012 exam
The process involved is metaplasia. During metaplasia there is no direct
carcinogenesis, however the persistent presence of precipitants of metaplasia will lead
to malignant changes in cells.
Metaplastic changes in the duodenal cap are frequently seen in association with H-
Pylori induced ulcers. It typically resolves after ulcer healing and eradication therapy.
Metaplasia
Definition: reversible change of differentiated cells to another cell type.
May represent an adaptive substitution of cells that are sensitive to stress by
cell types better able to withstand the adverse environment.
Can be a normal physiological response (ossification of cartilage to form
bone)
Most common epithelial metaplasia occurs with transformation of columnar
cells to squamous cells (smoking causes ciliated columnar cells to be replaced
by squamous epithelial cells; Schistosomiasis).
Metaplasia from squamous to columnar cells occurs in Barrett oesophagus.
If the metaplastic stimulus is removed, the cells will return to their original
pattern of differentiation. However, if the stimulus is not removed then
progression to dysplasia may occur.
Not considered directly carcinogenic, however the factors which predispose to
metaplasia, if persistent may induce malignant transformation.
The pathogenesis involves a reprogramming of stem cells that are known to
exist in normal tissues, or of undifferentiated mesenchymal cells present in
connective tissue. In a metaplastic change, these precursor cells differentiate
along a new pathway.
A 22 year old lady presents with symptoms and signs of hyperthyroidism. Her
diagnostic work up results in a diagnosis of Graves disease. Which of the following
best describes the pathophysiology of the condition?
A. Formation of IgG antibodies to the TSH receptors on the thyroid

gland
B. Formation of IgG antibodies to the TRH receptors on the anterior
pituitary
C. Formation of IgM antibodies to the TSH receptors on the thyroid
gland
D. Formation of IgA antibodies to the TSH receptors on the thyroid
gland
E. Formation of IgM antibodies to the TRH receptors on the anterior
pituitary
Usually IgG antibodies are formed against the TSH receptors on the thyroid gland.
Which is why the TSH level is often very low in Graves disease.
Thyroid hormones
Hormones of the thyroid gland
Triiodothyronine T3 Major hormone active in target cells
Thyroxine T4 Most prevalent form in plasma, less biologically active than T3
Calcitonin Lowers plasma calcium
Synthesis and secretion of thyroid hormones
Thyroid actively concentrates iodide to twenty five times the plasma
concentration.
Iodide is oxidised by peroxidase in the follicular cells to atomic iodine which
then iodinates tyrosine residues contained in thyroglobulin.
Iodinated tyrosine residues in thyroglobulin undergo coupling to either T3 or
T4.
Process is stimulated by TSH, which stimulates secretion of thyroid hormones.
The normal thyroid has approximately 3 month reserves of thyroid hormones.
LATS and Graves disease In Graves disease patients develop IgG antibodies to the TSH receptors on the thyroid
gland. This results in chronic and long term stimulation of the gland with release of
thyroid hormones. The typically situation is raised thyroid hormones and low TSH.
Thyroid receptor autoantibodies should be checked in individuals presenting with
hyperthyroidism as they are present in up to 85% cases.
Theme: Breast disease
A. Tuberculosis
B. Actinomycosis
C. Duct ectasia
D. Fibroadenoma
E. Fat necrosis
F. Intraductal papilloma
G. Breast abscess
What is the most likely diagnosis for each scenario given? Each diagnosis may be
used once, more than once or not at all.
14. A 32 year old Indian woman presents with a tender breast lump. She has a 2
month old child. Clinically there is a tender, fluctuant mass of the breast.
Breast abscess
Similar theme in September 2011 Exam
This lady is likely to be breast feeding and is at risk of mastitis. This may lead
to an abscess if not treated. Staphylococcus aureus is usually the causative
organism.
15. A 53 year old lady presents with a green nipple discharge. On examination
she has discharge originating from multiple ducts and associated nipple
inversion.
Duct ectasia
Duct ectasia is common during the period of breast involution that occurs
during the menopausal period. As the ducts shorten they may contain
insipiated material. The discharge will often discharge from several ducts.
16. A 52 year old lady presents with an episode of nipple discharge. It is usually
clear in nature. On examination the discharge is seen to originate from a
single duct and although it appears clear, when the discharge is tested with a
labstix it is shown to contain blood. Imaging and examination shows no
obvious mass lesion,
Intraductal papilloma
Intraductal papilloma usually cause single duct discharge. The fluid is often
clear, although it may be blood stained. If the fluid is tested with a labstix
(little point in routiine practice) then it will usually contain small amounts of
blood. A microdocechtomy may be performed.
Non malignant breast disease

Duct ectasia
Mammary duct ectasia may be seen in up to 25% of normal female breasts
Patients usually present with nipple discharge, which may be from single or
multiple ducts (usually present age >50 years)
The discharge is often thick and green
Duct ectasia is a normal varient of breast involution and is not the same
condition as periductal mastitis
Periductal mastitis
Present at younger age than duct ectasia
May present with features of inflammation, abscess or mammary duct fistula
Stongly associated with smoking
Usually treated with antibiotics, abscess will require drainage
Intraductal papilloma
Growth of papilloma in a single duct
Usually presents with clear or blood stained discharge originating from a
single duct
No increase in risk of malignancy
Breast abscess
Lactational mastitis is common
Infection is usually with Staphylococcus aureus
On examination there is usually a tender fluctuant mass
Treatment is with antibiotics and ultrasound guided aspiration
Overlying skin necrosis is an indication for surgical debridement, which may
be complicated by the development of a subsequent mammary duct fistula.
Tuberculosis
Rare in western countries, usually secondary TB
Affects women later in child bearing period
Chronic breast or axillary sinus is present in up to 50% cases
Diagnosis is by biopsy culture and histology
A 45 year old man has widespread metastatic adenocarcinoma of the colon. Which of
the following tumour markers is most likely to be elevated?
A. CA19-9

B. Carcinoembryonic antigen
C. Alpha Feto Protein
D. CA 125
E. Beta BCG
Screening for colonic cancer
using CEA is not justified
Carcinoembryonic antigen is elevated in colonic cancer, typically in relation to
disease extent with highest serum levels noted in metastatic disease. It is falsely
elevated in a number of non-malignant disease states such as cirrhosis and colitis and
for this reason it has no role in monitoring colitics for colonic cancer[1].
Reference
1. Sturgeon, C.M., L.C. Lai, and M.J. Duffy, Serum tumour markers: how to order
and interpret them. BMJ, 2009. 339: p. b3527.
Colorectal cancer screening and diagnosis
Overview
Most cancers develop from adenomatous polyps. Screening for colorectal
cancer has been shown to reduce mortality by 16%
The NHS now has a national screening programme offering screening every 2
years to all men and women aged 60 to 69 years. Patients aged over 70 years
may request screening
Eligible patients are sent faecal occult blood (FOB) tests through the post
Patients with abnormal results are offered a colonoscopy
At colonoscopy, approximately:
5 out of 10 patients will have a normal exam
4 out of 10 patients will be found to have polyps which may be removed due
to their premalignant potential
1 out of 10 patients will be found to have cancer
Diagnosis
Essentially the following patients need referral:
- Altered bowel habit for more than six weeks

- New onset of rectal bleeding
- Symptoms of tenesmus
Colonoscopy is the gold standard, provided it is complete and good mucosal
visualisation is achieved. Other options include double contrast barium enema and CT
colonography.
Staging
Once a malignant diagnosis is made patients with colonic cancer will be staged using
chest / abdomen and pelvic CT. Patients with rectal cancer will also undergo
evaluation of the mesorectum with pelvic MRI scanning.
For examination purposes the Dukes and TNM systems are preferred.
Tumour markers Carcinoembryonic antigen (CEA) is the main tumour marker in colorectal cancer. Not
all tumours secrete this, and it may be raised in conditions such as IBD. However,
absolute levels do correlate (roughly) with disease burden and whilst this marker may
not be used extensively in follow up, it can be useful for investigation of patients with
cancer of unknown primary.
Which of the following does not cause hypercalcaemia?
A. Thiazides
B. DiGeorge syndrome
C. Vitamin A
D. Rhabdomylosis
E. Sarcoidosis
VITAMINS TRAP
V - Vitamins A & D
I - Immobilization
T - Thyrotoxicosis
A - Addison's disease
M - Milk-alkali syndrome
I - Inflammatory disorders
N - Neoplastic diseases
S - Sarcoidosis
T - Thiazides and other drugs
R - Rhabdomyolysis
A - AIDS
P - Paget's disease, Parenteral
nutrition, Parathyroid disease.

The parathyroid glands don't form as a result of this syndrome.
Hypercalcaemia
Main causes
Malignancy
Primary hyperparathyroidism
Less common
Sarcoidosis (extrarenal synthesis of calcitriol )
Thiazides, lithium
Immobilisation
Pagets disease
Vitamin A/D toxicity
Thyrotoxicosis
MEN
Milk alkali syndrome
Clinical features
“Stones, bones, abdominal moans, and psychic groans”
Theme: Diseases affecting the great vessels
A. Aortic coarctation
B. Cervical rib
C. Takayasu's arteritis
D. Subclavian steal syndrome
E. Patent ductus arteriosus
F. Aortic dissection
Please select the most likely underlying cause for the symptoms described. Each
option may be used once, more than once or not at all.
19. A 24 year old lady from Western India presents with symptoms of lethargy
and dizziness, worse on turning her head. On examination her systolic blood
pressure is 176/128. Her pulses are impalpable at all peripheral sites.
Auscultation of her chest reveals a systolic heart murmur.
You answered Aortic coarctation
The correct answer is Takayasu's arteritis

Takayasu's arteritis most commonly affects young Asian females. Pulseless
peripheries are a classical finding. The CNS symptoms may be variable.
20. A 48 year old man notices that he is becoming increasingly dizzy when he
plays squash, in addition he has also developed cramping pain in his left arm.
One day he is inflating his car tyre with a hand held pump, he collapses and is
brought to hospital.
Subclavian steal syndrome
Subclavian steal syndrome is associated with a stenosis or occlusion of the
subclavian artery, proximal to the origin of the vertebral artery. As a result the
increased metabolic needs of the arm then cause retrograde flow and
symptoms of CNS vascular insufficiency.
21. A 25 year old junior doctor has a chest x-ray performed as part of a routine
insurance medical examination. The x-ray shows evidence of rib notching.
Auscultation of his chest reveals a systolic murmur which is loudest at the
posterior aspect of the fourth intercostal space.
Aortic coarctation
Coarctation of the aorta may occur due to the remnant of the ductus arteriosus
acting as a fibrous constrictive band of the aorta. Weak arm pulses may be
seen, radiofemoral delay is the classical physical finding. Collateral flow
through the intercostal vessels may produce notching of the ribs, if the disease
is long standing.
Vascular disease
Aortic dissection Chest pain (anterior chest pain- ascending aorta, back pain
- descending aorta)
Widening of aorta on chest x-ray
Diagnosis made by CT scanning
Treatment is either medical (Type B disease) or surgical
(Type A disease)
Cervical rib Supernumery fibrous band arising from seventh cervical
vertebra
Incidence of 1 in 500
May cause thoracic outlet syndrome

Treatment involves surgical division of rib
Subclavian steal
syndrome
Due to proximal stenotic lesion of the subclavian artery
Results in retrograte flow through vertebral or internal
thoracic arteries
The result is that decrease in cerebral blood flow may
occur and produce syncopal symptoms
A duplex scan and/ or angiogram will delineate the lesion
and allow treatment to be planned
Takayasu's
arteritis
Large vessel granulomatous vasculitis
Results in intimal narrowing
Most commonly affects young asian females
Patients present with features of mild systemic illness,
followed by pulseless phase with symptoms of vascular
insufficiency
Treatment is with systemic steroids
Patent ductus
arteriosus
Ductus arteriosus is a normal foetal vessel that closes
spontaneously after birth
Results in high pressure, oxygenated blood entering the
pulmonary circuit
Untreated patients develop symptoms of congestive cardiac
failure
Coarctation of
the aorta
Aortic stenosis at the site of the ductus arteriosus insertion
Most common in boys and girls with Turners syndrome
Patients may present with symptoms of arterial
insufficiency, such as syncope and claudication
Blood pressure mismatch may be seen, as may mismatch
of pulse pressure in the upper and lower limbs
Treatment is either with angioplasty or surgical resection
(the former is the most common)
A 25 year old man is found to have carcinoid syndrome. Which of the following
hormones is released by carcinoids?
A. Serotonin
B. Dopamine
C. Nor adrenaline
D. Adrenaline
E. Aldosterone
Rule of thirds:
1/3 multiple
1/3 small bowel
1/3 metastasize
1/3 second
tumour
Carcinoids secrete serotonin. Carcinoid syndrome will only occur in the presence of
liver metastasis as the hormone released from primary lesions will typically be
metabolised by the liver.
Carcinoid syndrome
Carcinoid tumours secrete serotonin
Originate in neuroendocrine cells mainly in the intestine (midgut-distal
ileum/appendix)
Can occur in the rectum, bronchi
Hormonal symptoms mainly occur when disease spreads outside the bowel
Clinical features - Onset: years
- Flushing face
- Palpitations
- Tricuspid stenosis causing dyspnoea
- Asthma
- Severe diarrhoea (secretory, persists despite fasting)
Investigation - 5-HIAA in a 24-hour urine collection
- Scintigraphy
- CT scan
Treatment
Octreotide
Surgical removal
Which one of the following genes protects against neoplasms?
A. sis
B. p53
C. ras

D. myc
E. src
p53 is a tumour supressor gene and located on chromosome 17. It plays an important
role in causing cells that are undergoing neoplastic changes to enter an apoptotic
pathway.
Oncogenes
Oncogenes are cancer promoting genes that are derived from normal genes (proto-
oncogenes). Proto-oncogenes play an important physiological role in cellular growth.
They are implicated in the development of up to 20% of human cancers.
Proto-oncogenes may become oncogenes via the following processes:
Mutation (point mutation)
Chromosomal translocation
Increased protein expression
Only one mutated copy of the gene is needed for cancer to occur - a dominant effect
Classification of oncogenes
Growth factors e.g. Sis
Transcription factors e.g. Myc
Receptor tyrosine kinase e.g. RET
Cytoplasmic tyrosine kinase e.g. Src
Regulatory GTPases e.g. Ras
Tumour supressor genes Tumour supressor genes restrict or repress cellular proliferation in normal cells. Their
inactivation through mutation or germ line incorporation is implicated in renal,
colonic, breast, bladder and many other cancers. One of the best known tumour
supressor genes is p53. p53 gene offers protection by causing apoptosis of damaged
cells. Other well known genes include BRCA 1 and 2.
A 55 year old man with a long history of achalasia is successfully treated by a Hellers
Cardiomyotomy. Several years later he develops an oesophageal malignancy. Which
of the following lesions is most likely to be present?
A. Adenocarcinoma
B. Gastrointestinal stromal tumour
C. Leiomyosarcoma

D. Rhabdomyosarcoma
E. Squamous cell carcinoma
Achalasia is a rare condition. However, even once treated there is an increased risk of
malignancy. When it does occur it is most likely to be of squamous cell type.
Oesophageal cancer
Incidence is increasing
In most cases in the Western world this increase is accounted for by a rise in
the number of cases of adenocarcinoma. In the UK adenocarcinomas account
for 65% of cases.
Barretts oesophagus is a major risk factor for most cases of oesophageal
adenocarcinoma.
In other regions of the world squamous cancer is more common and is linked
to smoking, alcohol intake, diets rich in nitrosamines and achalasia.
Surveillance of Barretts is important as it imparts a 30 fold increase in cancer
risk and if invasive malignancy is diagnosed early then survival may approach
85% at 5 years.
Diagnosis
Upper GI endoscopy is the first line test
Contrast swallow may be of benefit in classifying benign motility disorders
but has no place in the assessment of tumours
Staging is initially undertaken with CT scanning of the chest, abdomen and
pelvis. If overt metastatic disease is identified using this modality then further
complex imaging is unnecessary
If CT does not show metastatic disease, then local stage may be more
accurately assessed by use of endoscopic ultrasound.
Staging laparoscopy is performed to detect occult peritoneal disease. PET CT
is performed in those with negative laparoscopy. Thoracoscopy is not
routinely performed.
Treatment Operable disease is best managed by surgical resection. The most standard procedure
is an Ivor- Lewis type oesophagectomy. This procedure involves the mobilisation of
the stomach and division of the oesophageal hiatus. The abdomen is closed and a right
sided thoracotomy performed. The stomach is brought into the chest and the
oesophagus mobilised further. An intrathoracic oesophagogastric anastomosis is
constructed. Alternative surgical strategies include a transhiatal resection (for distal
lesions), a left thoraco-abdominal resection (difficult access due to thoracic aorta) and
a total oesophagectomy (McKeown) with a cervical oesophagogastric anastomosis.
The biggest surgical challenge is that of anastomotic leak, with an intrathoracic

anastomosis this will result in mediastinitis. With high mortality. The McKeown
technique has an intrinsically lower systemic insult in the event of anastmotic leakage.
In addition to surgical resection many patients will be treated with adjuvent
chemotherapy.
Which of the following genes is not implicated in the adenoma-carcinoma sequence in
colorectal cancer?
A. src
B. c-myc
C. APC
D. p53
E. K-ras
Other genes involved are:
MCC
DCC
c-yes
bcl-2
Colorectal cancer
Annually about 150,000 new cases are diagnosed and 50,000 deaths from the
disease
About 75% will have sporadic disease and 25% will have a family history
Colorectal tumours comprise a spectrum of disease ranging from adenomas
through to polyp cancers and frank malignancy.
Polyps may be categorised into: neoplastic polyps, adenomatous polyps and
non neoplastic polyps.
The majority of adenomas are polypoidal lesions, although flat lesions do
occur and may prove to be dysplastic.
Non-neoplastic polyps include hyperplastic, juvenile, hamartomatous,
inflammatory, and lymphoid polyps, which have not generally been thought of
as precursors of cancer.
Three characteristics of adenomas that correlate with malignant potential have
been characterised. These include increased size, villous architecture and
dysplasia. For this reason most polyps identified at colonoscopy should be
removed.
The transformation from polyp to cancer is described by the adenoma -
carcinoma sequence and its principles should be appreciated. Essentially

genetic changes accompany the transition from adenoma to carcinoma; key
changes include APC, c-myc, K RAS mutations and p53 deletions.
A 63 year old lady is suspected as having sarcoidosis. She is sent to the general surgeons and
a lymph node biopsy is performed. Which of the following histological features is most likely
to be identified in a lymph node if sarcoid is present?
A. Psammoma bodies
B. Extensive necrosis
C. Dense eosinophillic infiltrates
D. Asteroid bodies
E. None of the above
Asteroid bodies are often found in the granulomas of individuals with sarcoid. Unlike the
granulomata associated with tuberculosis the granulomas of sarcoid are rarely associated
with extensive necrosis.
An Asteroid body in an individual with sarcoid

Image sourced from Wikipedia
Chronic inflammation
Overview
Chronic inflammation may occur secondary to acute inflammation.In most cases chronic
inflammation occurs as a primary process. These may be broadly viewed as being one of
three main processes:
Persisting infection with certain organisms such as Mycobacterium tuberculosis which results in delayed type hypersensitivity reactions and inflammation.
Prolonged exposure to non-biodegradable substances such as silica or suture materials which may induce an inflammatory response.
Autoimmune conditions involving antibodies formed against host antigens.
Acute vs. Chronic inflammation

Acute inflammation Chronic inflammation
Changes to existing vascular structure and increased
permeability of endothelial cells
Angiogenesis predominates
Infiltration of neutrophils Macrophages, plasma cells and
lymphocytes predominate
Process may resolve with:
Suppuration Complete resolution Abscess formation Progression to chronic inflammation Healing by fibrosis
Healing by fibrosis is the main result
Granulomatous inflammation
A granuloma consists of a microscopic aggregation of macrophages (with epithelial type
arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas.
Mediators
Growth factors released by activated macrophages include agents such as interferon and
fibroblast growth factor (plus many more). Some of these such as interferons may have
systemic features resulting in systemic symptoms and signs, which may be present in
individuals with long standing chronic inflammation.
The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this
biopsy from a patient with colonic Crohns disease
Image sourced from Wikipedia

Brown tumours of bone are associated with which of the following?
A. Hyperthyroidism
B. Hypothyroidism
C. Hyperparathyroidism
D. Hypoparathyroidism
E. Osteopetrosis
Brown tumors are tumors of bone that arise in settings of excess osteoclast activity,
such as hyperparathyroidism, and consist of fibrous tissue, woven bone and
supporting vasculature, but no matrix. They are radiolucent on x-ray. The osteoclasts
consume the trabecular bone that osteoblasts lay down and this front of reparative
bone deposition followed by additional resorption can expand beyond the usual shape
of the bone, involving the periosteum thus causing bone pain. They appear brown
because haemosiderin is deposited at the site.
Primary hyperparathyroidism
In exams primary hyperparathyroidism is stereotypically seen in elderly females with
an unquenchable thirst and an inappropriately normal or raised parathyroid hormone
level. It is most commonly due to a solitary adenoma
Causes of primary hyperparathyroidism
80%: solitary adenoma
15%: hyperplasia
4%: multiple adenoma
1%: carcinoma
Features - 'bones, stones, abdominal groans and psychic moans'
Polydipsia, polyuria
Peptic ulceration/constipation/pancreatitis
Bone pain/fracture
Renal stones
Depression
Hypertension
Associations

Hypertension
Multiple endocrine neoplasia: MEN I and II
Investigations
Raised calcium, low phosphate
PTH may be raised or normal
Technetium-MIBI subtraction scan
Treatment
Parathyroidectomy, if imaging suggests target gland then a focused approach
may be used
A 73 year old man is recovering following an emergency Hartmans procedure
performed for an obstructing sigmoid cancer. The pathology report shows a
moderately differentiated adenocarcinoma that invades the muscularis propria,
3 of 15 lymph nodes are involved with metastatic disease. What is the correct
stage for this?
A. Astler Coller Stage B2
B. Dukes stage A
C. Dukes stage B
D. Dukes stage C
E. Dukes stage D
Theme from September 2011 Exam
The involvement of lymph nodes makes this Dukes C. In the Astler Coller
system the B and C subsets are split to B1 and B2 and C1 and C2. Where C2
denotes involvement of the nodes in conjunction with penetration of the
muscularis propria.
Dukes classification
Gives the extent of spread of colorectal cancer
Dukes A Tumour confined to the mucosa (90%)
Dukes B Tumour invading bowel wall (70%)
Dukes C Lymph node metastases (45%)
Dukes D Distant metastases (6%)(20% if resectable)
5 year survival in brackets

A 55 year old man with dyspepsia undergoes an upper GI endoscopy. An irregular
erythematous area is seen to protrude proximally from the gastro-oesophageal
junction. Apart from specialised intestinal metaplasia, which of the following cell
types should also be present for a diagnosis of Barretts oesophagus to be made?
A. Goblet cell
B. Neutrophil
C. Lymphocytes
D. Epithelial cells
E. Macrophages
Goblet cells need to be present for a diagnosis of Barrett's oesophagus to be made.
Barrett's oesophagus
Intestinal metaplasia
Squamous epithelium replaced by columnar epithelium in the lower
oesophagus
3 types of columnar epithelium:
1. Junctional
2. Atrophic fundal
3. Specialised
Presence of goblet cells important in identification
Premalignant change (progress to dysplasia)
Risk of adenocarcinoma
Risk factors: middle age, men, smoker, Caucasian, gastro-oesophageal reflux,
obesity
Treatment
Long term proton pump inhibitor
Consider pH and manometry studies in younger patients who may prefer to
consider an anti reflux procedure
Regular endoscopic monitoring (more frequently if moderate dysplasia). With
quadrantic biopsies every 2-3 cm
If severe dysplasia be very wary of small foci of cancer
Which of the following amino acids is present in all types of collagen?

A. Alanine
B. Aspartime
C. Glycine
D. Tyrosine
E. Cysteine
Collagen has a generic structure of Glycine- X- Y, where X and Y are variable sub
units. The relatively small size of the glycine molecule enables collagen to form a
tight helical structure.
Collagen
One of the major connective tissue proteins
Composed of 3 polypeptide strands that are woven into a helix
Numerous hydrogen bonds exist within molecule to provide additional
strength
Many sub types but commonest sub type is I (90% of bodily collagen)
Vitamin c is important in establishing cross links
Collagen Diseases
Osteogenesis imperfecta
Ehlers Danlos
Osteogenesis imperfecta:
-8 Subtypes
-Defect of type I collagen
-In type I the collagen is normal quality but insufficient quantity
-Type II- poor quantity and quality
-Type III- Collagen poorly formed, normal quantity
-Type IV- Sufficient quantity but poor quality
Patients have bones which fracture easily, loose joint and multiple other defects
depending upon which sub type they suffer from
Ehlers Danlos:
-Multiple sub types
-Abnormality of types 1 and 3 collagen
-Patients have features of hypermobility.
-Individuals are prone to joint dislocations and pelvic organ prolapse. In addition to
many other diseases related to connective tissue defects

Which of the following amino acids is present in all types of collagen?
A. Alanine
B. Aspartime
C. Glycine
D. Tyrosine
E. Cysteine
Collagen has a generic structure of Glycine- X- Y, where X and Y are variable sub
units. The relatively small size of the glycine molecule enables collagen to form a
tight helical structure.
Collagen
One of the major connective tissue proteins
Composed of 3 polypeptide strands that are woven into a helix
Numerous hydrogen bonds exist within molecule to provide additional
strength
Many sub types but commonest sub type is I (90% of bodily collagen)
Vitamin c is important in establishing cross links
Collagen Diseases
Osteogenesis imperfecta
Ehlers Danlos
Osteogenesis imperfecta:
-8 Subtypes
-Defect of type I collagen
-In type I the collagen is normal quality but insufficient quantity
-Type II- poor quantity and quality
-Type III- Collagen poorly formed, normal quantity
-Type IV- Sufficient quantity but poor quality
Patients have bones which fracture easily, loose joint and multiple other defects
depending upon which sub type they suffer from
Ehlers Danlos:
-Multiple sub types
-Abnormality of types 1 and 3 collagen
-Patients have features of hypermobility.

-Individuals are prone to joint dislocations and pelvic organ prolapse. In addition to
many other diseases related to connective tissue defects
An 8 year old boy presented with a painless swelling on the superotemporal aspect of
his orbit. It was smooth on examination, produced no visual disturbances. Following
excision it was found to be lined by squamous epithelium and hair follicles. Which of
the following lesions most closely matches these findings?
A. Dermoid cyst
B. Desmoid tumour
C. Lipoma
D. Sebaceous cyst
E. Schwannoma
Dermoid cysts are embryological remnants and may be lined by hair and squamous
epithelium (like teratomas). They are often located in the midline and may be linked
to deeper structures resulting in a dumbbell shape to the lesion. Complete excision is
requires as they have a propensity to local recurrence if not excised.
Desmoid tumours are a different entity, they most commonly develop in ligaments
and tendons. They are also referred to as aggressive fibromatosis and consist of
fibroblast dense lesions (resembling scar tissue). They should be managed in a similar
manner to soft tissue sarcomas.
Skin Diseases
Skin lesions may be referred for surgical assessment, but more commonly will come
via a dermatologist for definitive surgical management.
Skin malignancies include basal cell carcinoma, squamous cell carcinoma and
malignant melanoma.
Basal Cell Carcinoma
Most common form of skin cancer.
Commonly occur on sun exposed sites apart from the ear.
Sub types include nodular, morphoeic, superficial and pigmented.
Typically slow growing with low metastatic potential.
Standard surgical excision, topical chemotherapy and radiotherapy are all
successful.
As a minimum a diagnostic punch biopsy should be taken if treatment other
than standard surgical excision is planned.
Squamous Cell Carcinoma

Again related to sun exposure.
May arise in pre - existing solar keratoses.
May metastasise if left.
Immunosupression (e.g. Following transplant), increases risk.
Wide local excision is the treatment of choice and where a diagnostic excision
biopsy has demonstrated SCC, repeat surgery to gain adequate margins may
be required.
Malignant Melanoma
The main diagnostic features (major
criteria):
Change in size
Change in shape
Change in colour
Secondary features (minor
criteria)
Diameter >6mm
Inflammation
Oozing or bleeding
Altered sensation
Treatment
Suspicious lesions should undergo excision biopsy. The lesion should be
removed in completely as incision biopsy can make subsequent
histopathological assessment difficult.
Once the diagnosis is confirmed the pathology report should be reviewed to
determine whether further re-exicision of margins is required (see below):
Margins of excision-Related to Breslow thickness
Lesions 0-1mm thick 1cm
Lesions 1-2mm thick 1- 2cm (Depending upon site and pathological features)
Lesions 2-4mm thick 2-3 cm (Depending upon site and pathological features)
Lesions >4 mm thick 3cm
Marsden J et al Revised UK guidelines for management of Melanoma. Br J Dermatol
2010 163:238-256.
Further treatments such as sentinel lymph node mapping, isolated limb perfusion and
block dissection of regional lymph node groups should be selectively applied.
Kaposi Sarcoma
Tumour of vascular and lymphatic endothelium.
Purple cutaneous nodules.
Associated with immunosupression.
Classical form affects elderly males and is slow growing.
Immunosupression form is much more aggressive and tends to affect those
with HIV related disease.

Non malignant skin disease
Dermatitis Herpetiformis
Chronic itchy clusters of blisters.
Linked to underlying gluten enteropathy (coeliac disease).
Dermatofibroma
Benign lesion.
Firm elevated nodules.
Usually history of trauma.
Lesion consists of histiocytes, blood vessels and fibrotic changes.
Pyogenic granuloma
Overgrowth of blood vessels.
Red nodules,
Usually follow trauma.
May mimic amelanotic melanoma.
Acanthosis nigricans
Brown to black, poorly defined, velvety hyperpigmentation of the skin.
Usually found in body folds such as the posterior and lateral folds of the neck,
the axilla, groin, umbilicus, forehead, and other areas.
The most common cause of acanthosis nigricans is insulin resistance, which
leads to increased circulating insulin levels. Insulin spillover into the skin
results in its abnormal increase in growth (hyperplasia of the skin).
In the context of a malignant disease, acanthosis nigricans is a paraneoplastic
syndrome and is then commonly referred to as acanthosis nigricans maligna.
Involvement of mucous membranes is rare and suggests a coexisting
malignant condition
A 55 year old man from Hong Kong presents with left sided otalgia and recurrent
episodes of epistaxis. On examination his pharynx appears normal. Examination of
his neck reveals left sided cervical lymphadenopathy. What is the most likely
underlying diagnosis?
A. Antrochoanal polyp
B. Nasopharyngeal carcinoma
C. Adenocarcinoma of the tonsil

D. Angiofibroma
E. Globus syndrome
Given this mans ethnic origin and presenting features a nasopharyngeal carcinoma is
the most likely underlying diagnosis.
Nasopharyngeal carcinoma
Squamous cell carcinoma of the nasopharynx
Rare in most parts of the world, apart from individuals from Southern China
Associated with Epstein Barr virus infection
Presenting features
Systemic Local
Cervical lymphadenopathy Otalgia
Unilateral serous otitis media
Nasal obstruction, discharge and/ or epistaxis
Cranial nerve palsies e.g. III-VI
Imaging Combined CT and MRI.
Treatment Radiotherapy is first line therapy.
Patients with suspected temporal arteritis are often sent for temporal artery biopsy.
Which statement is true?
A. Temporal artery biopsy is only diagnostic if there is visual loss
B. Biopsy is typically taken from the non-symptomatic side to avoid the
risk of blindness
C. Pre-operative localisation with duplex is mandatory
D. Biopsies may be non diagnostic in over 50% of cases
E. Biopsies are usually performed under general anaesthesia
Temporal artery biopsies are frequently non diagnostic. They should be taken from
the symptomatic side and though not mandatory a duplex ultrasound is a helpful
investigation, particularly if they mark the artery. It is usually performed under local
anaesthetic.

Temporal artery biopsy
Superficial temporal artery is a terminal branch of the external carotid artery
Main indication
Temporal arteritis
American College of Rheumatology guidelines recommend a temporal artery biopsy
if:
Age of onset older than 50 years
New-onset headache or localized head pain
Temporal artery tenderness to palpation or reduced pulsation
ESR > 50 mm/h
Histopathology
Vessel wall granulomatous arteritis with mononuclear cell infiltrates and giant
cell formation
Procedure
Position: supine, head 45 degrees
USS doppler to locate the superficial temporal artery or palpate
Local anaesthetic
Artery within temporoparietal fascia
Clamp and ligate the vessel
Cut 3-5cm
Ligate the remaining ends with absorbable suture
Close the skin
Contraindication Glucocorticoid therapy > 30 days
Risks Injury to facial or auriculotemporal nerve
Which of the following best describes the processes underpinning type IV
hypersensitivity reactions?
A. Deposition of immune complexes of IgG and antigen at
the site of inflammation

B. Deposition of IgA complexes at the site of inflammation
C. Deposition of IgM and IgG complexes at the site of
inflammation
D. Degranulation of mast cells at the site of inflammation
E. T cell mediated response at the site of inflammation
Hypersensitivity
reactions: ACID
type 1 --Anaphylactic
type 2 --Cytotoxic
type 3 --Immune complex
type 4 --Delayed
hypersensitivity
T Cells are the mediators of type 4 hypersensitivity reactions which are characterised
by the absence of immune complex deposition.
Hypersensitivity reactions
The Gell and Coombs classification divides hypersensitivity reactions into 4 types
Type I Type II Type III Type IV
Description Anaphylactic Cytotoxic Immune
complex
Delayed type
Mediator IgE IgG, IgM IgG, IgM T-cells
Antigen Exogenous Cell surface Soluble Tissues
Response
time
Minutes Hours Hours 2-3 days
Examples Asthma
Hay fever
Autoimmune
haemolytic anaemia
Pemphigus
Goodpasture's
Serum
sickness
SLE
Aspergillosis
Graft versus host
disease
Contact
dermatitis
Theme: Bone tumours
A. Osteosarcoma
B. Fibrosarcoma
C. Osteoclastoma
D. Ewings sarcoma
E. Leiomyosarcoma
F. Chondrosarcoma
G. Rhabdomyosarcoma
H. Osteoid osteoma
I. Malignant fibrous histiocytoma
Please select the most appropriate lesion for the clinical scenario given. Each option
may be used once, more than once or not at all.
7. A 16 year-old boy presents to his GP with loss of weight, pain and fever. On
examination, a soft tissue mass is palpable over the mid-thigh region
Ewings sarcoma
Ewing's sarcoma is a malignant round cell tumour occurring in the diaphysis of
the long bones in the children. These are not confined to the ends of long
bones. x Rays often show a large soft-tissue mass with concentric layers of
new bone formation ( 'onion-peel' sign). The ESR may be elevated, thus
suggesting an inflammatory or an infective cause such as osteomyelitis;
although osteomyelitis usually affects the metaphyseal region in children.
Treatment is with chemotherapy and surgical excision, an endoprothesis may
be used to conserve the limb.
8. A 75 year old lady presents with weight loss, pain and a swelling over her left
knee. She has been treated for Pagets disease of the bone for some time.
Osteosarcoma
Osteosarcoma may complicate Pagets disease of bone in up to 10% cases.
Radiological appearances include bone destruction coupled with new bone
formation, periosteal elevation may also occur. Surgical resection is the main
treatment.
9. A 17-year-old girl presents with weight loss, fever and a swelling over her
right knee. Movements of her knee are restricted. A plain x-ray of the affected
site shows multiple lytic and lucent lesions with clearly defined borders.
You answered Malignant fibrous histiocytoma
The correct answer is Osteoclastoma
Osteoclastoma has a characteristic appearance on x-ray with multple lytic and
lucent areas (Soap bubble) appearances. Pathological fractures may occur. The
disease is usually indolent.
Sarcomas

Malignant tumours of mesenchymal origin
Types May be either bone or soft tissue in origin.
Bone sarcoma include:
Osteosarcoma
Ewings sarcoma (although non bony sites recognised)
Chrondrosarcoma - originate from Chondrocytes
Soft tissue sarcoma are a far more heterogeneous group and include:
Liposarcoma-adipocytes
Rhabdomyosarcoma-striated muscle
Leiomyosarcoma-smooth muscle
Synovial sarcomas- close to joints (cell of origin not known but not synovium)
Malignant fibrous histiocytoma is a sarcoma that may arise in both soft tissue and
bone.
Features Certain features of a mass or swelling should raise suspicion for a sarcoma these
include:
Large >5cm soft tissue mass
Deep tissue location or intra muscular location
Rapid growth
Painful lump
Assessment Imaging of suspicious masses should utilise a combination of MRI, CT and USS.
Blind biopsy should not be performed prior to imaging and where required should be
done in such a way that the biopsy tract can be subsequently included in any
resection.
Ewings sarcoma
Commoner in males
Incidence of 0.3 / 1, 000, 000
Onset typically between 10 and 20 years of age
Location by femoral diaphysis is commonest site
Histologically it is a small round tumour
Blood borne metastasis is common and chemotherapy is often combined with
surgery

Osteosarcoma
Mesenchymal cells with osteoblastic differentiation
20% of all primary bone tumours
Incidence of 5 per 1,000,000
Peak age 15-30, commoner in males
Limb preserving surgery may be possible and many patients will receive
chemotherapy
Liposarcoma
Malignancy of adipocytes
Rare approximately 2.5 per 1,000,000. They are the second most common soft
tissue sarcoma
Typically located in deep locations such as retroperitoneum
Affect older age group usually >40 years of age
May be well differentiated and thus slow growing although may undergo
dedifferentiation and disease progression
Many tumours will have a pseudocapsule that can misleadingly allow
surgeons to feel that they can 'shell out' these lesions. In reality tumour may
invade at the edge of the pseudocapsule and result in local recurrence if this
strategy is adopted
Usually resistant to radiotherapy although this is often used in a palliative
setting
Malignant Fibrous Histiocytoma
Tumour with large number of histiocytes
Most common sarcoma in adults
Also described as undifferentiated pleomorphic sarcoma NOS (i.e. Cell of
origin is not known)
Four major subtypes are recognised: storiform-pleomorphic (70% cases),
myxoid (less aggressive), giant cell and inflammatory
Treatment is usually with surgical resection and adjuvant radiotherapy as this
reduces the likelihood of local recurrence
A 22 year old man is undergoing an abdominal ultrasound scan as part of a series of
investigations for abdominal pain. The radiologist notes that there is evidence of
splenic atrophy. What is the most likely cause?
A. Letterer-Siwe disease
B. Coeliac disease
C. Malaria

D. Niemann-Pick disease
E. Sarcoidosis
Splenic atrophy may occur in coeliac disease together with the appearance of Howell-
Jolly bodies in erythrocytes. Letterer - Siwe disease is a form of Histiocytosis X in
which macrophages proliferate.
Spleen
Embryology: derived from mesenchymal tissue
Shape: orange segment
Position: below 9th-12th ribs
Weight: 75-150g
Relations
Superiorly- diaphragm
Anteriorly- gastric impression
Posteriorly- kidney
Inferiorly- colon
Hilum: tail of pancreas and splenic vessels (splenic artery divides here,
branches pass to the white pulp transporting plasma)
Forms apex of lesser sac (containing short gastric vessels)
Contents - White pulp: immune function. Contains central trabecular artery. The germinal
centres are supplied by arterioles called penicilliary radicles.
- Red pulp: filters abnormal red blood cells
Function
Filtration of abnormal blood cells and foreign bodies such as bacteria.
Immunity: IgM. Production of properdin, and tuftsin which help target fungi
and bacteria for phagocytosis.
Haematopoiesis: up to 5th month gestation or in haematological disorders.
Pooling: storage of 40% platelets.
Iron reutilisation
Storage red blood cells-animals, not humans.
Storage monocytes
Disorders of the spleen Massive splenomegaly

Myelofibrosis
Chronic myeloid leukaemia
Visceral leishmaniasis (kala-azar)
Malaria
Gaucher's syndrome
Other causes (as above plus)
Portal hypertension e.g. secondary to cirrhosis
Lymphoproliferative disease e.g. CLL, Hodgkin's
Haemolytic anaemia
Infection: hepatitis, glandular fever
Infective endocarditis
Sickle-cell*, thalassaemia
Rheumatoid arthritis (Felty's syndrome)
*the majority of adults patients with sickle-cell will have an atrophied spleen due to
repeated infarction
Which statement relating to phaeochromocytoma is untrue?
A. They are tumours of chromaffin cells in the adrenal medulla.
B. They are bilateral in 10% of cases.
C. When located in an extra adrenal location have a higher incidence of
malignancy.
D. May be associated with an elevated urinary VMA.
E. Up to 40% may have a blood pressure within the normal range.
Normotension is seen in around 10% cases. The remainder show a degree of
hypertension.
Phaeochromocytoma and adrenal lesions
Phaeochromocytoma Neuroendocrine tumour of the chromaffin cells of the adrenal medulla. Hypertension
and hyperglycaemia are often found.
10% of cases are bilateral.
10% occur in children.
11% are malignant (higher when tumour is located outside the adrenal).
10% will not be hypertensive.

Familial cases are usually linked to the Multiple endocrine neoplasia syndromes
(considered under its own heading).
Most tumours are unilateral (often right sided) and smaller than 10cm.
Diagnosis Urine analysis of vanillymandelic acid (VMA) is often used (false positives may
occur e.g. in patients eating vanilla ice cream!)
Blood testing for plasma metanephrine levels.
CT and MRI scanning are both used to localise the lesion.
Treatment Patients require medical therapy first. An irreversible alpha adrenoreceptor blocker
should be given, although minority may prefer reversible bockade(1). Labetolol may
be co-administered for cardiac chronotropic control. Isolated beta blockade should not
be considered as it will lead to unopposed alpha activity.
These patients are often volume depleted and will often require moderate volumes of
intra venous normal saline perioperatively.
Once medically optimised the phaeochromocytoma should be removed. Most
adrenalectomies can now be performed using a laparoscopic approach(2). The
adrenals are highly vascular structures and removal can be complicated by
catastrophic haemorrhage in the hands of the inexperienced. This is particularly true
of right sided resections where the IVC is perilously close. Should the IVC be
damaged a laparotomy will be necessary and the defect enclosed within a Satinsky
style vascular clamp and the defect closed with prolene sutures. Attempting to
interfere with the IVC using any instruments other than vascular clamps will result in
vessel trauma and make a bad situation much worse.
Incidental adrenal lesions Adrenal lesions may be identified on CT scanning performed for other reasons(3).
Factors suggesting benign disease on CT include(4):
Size less than 3cm
Homogeneous texture
Lipid rich tissue
Thin wall to lesion
All patients with incidental lesions should be managed jointly with an endocrinologist
and full work up as described above. Patients with functioning lesions or those with
adverse radiological features (Particularly size >3cm) should proceed to surgery.
References 1. Weingarten TN, Cata JP, O'Hara JF, Prybilla DJ, Pike TL, Thompson GB, et al.

Comparison of two preoperative medical management strategies for laparoscopic
resection of pheochromocytoma. Urology. 2010 Aug;76(2):508 e6-11.
2. Nguyen PH, Keller JE, Novitsky YW, Heniford BT, Kercher KW. Laparoscopic
approach to adrenalectomy: review of perioperative outcomes in a single center. Am
Surg. 2011 May;77(5):592-6.
3. Ng VW, Ma RC, So WY, Choi KC, Kong AP, Cockram CS, et al. Evaluation of
functional and malignant adrenal incidentalomas. Arch Intern Med. 2010 Dec
13;170(22):2017-20.
4. Muth A, Hammarstedt L, Hellstrom M, Sigurjonsdottir HA, Almqvist E, Wangberg
B. Cohort study of patients with adrenal lesions discovered incidentally. Br J Surg.
2011 May 27. A 69 year old man presents with a purple lesion on his forearm. It is excised and an a 3 cm
Merkel cell tumour is diagnosed. Which of the following statements relating to this diagnosis
is false?
A. He should undergo a sentinel lymph node biopsy.
B. Lymphovascular invasion is typically seen histologically
C. They are more common in immunosupressed patients
D. Histologically they may resemble pyogenic granuloma
E. They are associated with visceral metastasis
Merkel cell tumours are rare cutaneous tumours. Histologically they consist of sheets and
nodules of hyperchromatic epithelial cells, with high rates of mitosis and apoptosis. As such
they are relatively easy to distinguish from pyogenic granuloma which has no features of
malignancy and would not show lymphovascular invasion.
Merkel cell tumours of the skin
Rare but aggressive tumour. Develops from intra epidermal Merkel cells. Usually presents on elderly, sun damaged skin. The periorbital area is the
commonest site.

Histologically these tumours appear within the dermis and subcutis. The lesions consist of sheets and nodules of small hyperchromatic epithelial cells with high rates of mitosis and apoptosis. Lymphovascular invasion is commonly seen.
Pre-existing infection with Merkel Cell Polyomavirus is seen in 80% cases.
Treatment
Surgical excision is first line. Margins of 1cm are required. Lesions >10mm in diameter
should undergo sentinel lymph node biopsy. Adjuvant radiotherapy is often given to reduce
the risk of local recurrence.
Prognosis
With lymph node metastasis 5 year survival is 50% or less. Small lesions without nodal spread are usually associated with a 5 year survival of
80%.
Skin biopsy demonstrating a Merkel Cell cancer. Note the hyperchromatic epithelial cells and
high mitotic rate

Image sourced from Wikipedia
A 58 year old lady undergoes a screening mammogram and appearances are
suspicious for ductal carcinoma in situ. A stereotactic core biopsy is performed. If
ductal carcinoma in situ is to be diagnosed, which of the following pathological
features must not be present?
A. Nuclear pleomorphism
B. Coarse chromatin
C. Abnormal mitoses
D. Angiogenesis

E. Dysplastic cells infiltrating the suspensory ligaments of the breast
The presence of invasion is a hallmark of invasive disease and thus would not be a
feature of DCIS. Angiogenesis may occur in association with high grade DCIS.
Histopathology of malignancy
Abnormal tissue architecture
Coarse chromatin
Invasion of basement membrane*
Abnormal mitoses
Angiogenesis
De-differentiation
Areas of necrosis
Nuclear pleomorphism
*= Those features that distinguish invasive malignancy from in situ disease
Which of the following does not occur as a pathological response to extensive burns?
A. Plasma leakage into interstitial space
B. Polycythaemia
C. Increased haematocrit
D. Keratinocyte migration during healing
E. Cardiac output reduction by 50% in first 30 minutes
Haemolysis is the main pathological response.
Burns pathology
Extensive burns
Haemolysis due to damage of erythrocytes by heat and microangiopathy
Loss of capillary membrane integrity causing plasma leakage into interstitial
space
Extravasation of fluids from the burn site causing hypovolaemic shock (up to
48h after injury)- decreased blood volume and increased haematocrit
Protein loss
Secondary infection e.g. Staphylococcus aureus
ARDS
Risk of Curlings ulcer (acute peptic stress ulcers)

Danger of full thickness circumferential burns in an extremity as these may
develop compartment syndrome
Healing
Superficial burns: keratinocytes migrate to form a new layer over the burn site
Full thickness burns: dermal scarring. Usually need keratinocytes from skin
grafts to provide optimal coverage.
Theme: Chest pain
A. Pulmonary embolism
B. Acute exacerbation asthma
C. Physiological
D. Mitral valve stenosis
E. Aortic dissection
F. Mitral regurgitation
G. Bronchopneumonia
H. Tuberculosis
I. None of the above
What is the most likely diagnosis for the scenario given? Each option may be used
once, more than once or not at all.
15. A 28 year old Indian woman, who is 18 weeks pregnant, presents with
increasing shortness of breath, chest pain and coughing clear sputum.
She is apyrexial, blood pressure is 140/80 mmHg, heart rate 130 bpm and
saturations 94% on 15L oxygen. On examination there is a mid diastolic
murmur, there are bibasal crepitations and mild pedal oedema. She
suddenly deteriorates and has a respiratory arrest. Her chest x-ray shows
a whiteout of both of her lungs.
Mitral valve stenosis
Mitral stenosis is the commonest cause of cardiac abnormality occurring
in pregnant women. Mitral stenosis is becoming less common in the UK
population, however should be considered in women from countries were
there is a higher incidence of rheumatic heart disease. Mitral stenosis
causes a mid diastolic murmur which may be difficult to auscultate
unless the patient is placed into the left lateral position. These patients
are at risk of atrial fibrillation (up tp 40%), which can also contribute to
rapid decompensation. Physiological changes in pregnancy may cause an
otherwise asymptomatic patient to suddenly deteriorate. Balloon
valvuloplasty is the treatment of choice.

16. A 28 year old woman, who is 30 weeks pregnant, presents with sudden
onset chest pain associated with loss of consciousness. Her blood
pressure is 170/90 mmHg, saturations on 15L oxygen 93%, heart rate
120 bpm and she is apyrexial. On examination there is an early diastolic
murmur, occasional bibasal creptitations and mild peal oedema. An ECG
shows ST elevation in leads II, III and aVF.
Aortic dissection
Aortic dissection is associated with the 3rd trimester of pregnancy,
connective tissue disorders (Marfan's, Ehlers- Danlos) and bicuspid
valve. Patients may complain of a tearing chest pain or syncope.
Clinically they may be hypertensive. The right coronary artery may
become involved in the dissection, causing myocardial infarct in up to
2% cases (hence ST elevation in the inferior leads). An aortic regurgitant
murmur may be auscultated.
17. A 28 year old woman, who is 18 weeks pregnant, presents with sudden
chest pain. Her blood pressure is 150/70 mmHg, saturations are 92% on
15L oxygen and her heart rate is 130 bpm. There are no murmurs and her
chest is clear. There is signs of thrombophlebitis in the left leg.
Pulmonary embolism
Chest pain, hypoxia and clear chest on auscultation in pregnancy should
lead to a high suspicion of pulmonary embolism.
Theme question in September 2011
exam Pregnant women can decompensate
rapidly from cardiac compromise.
Chest pain in pregnancy
Aortic dissection
Predisposing factors in pregnancy are hypertension, congenital heart disease
and Marfan's syndrome
Mainly Stanford type A dissections
Sudden tearing chest pain, transient syncope
Patient may be cold and clammy, hypertensive and have an aortic
regurgitation murmur
Involvement of the right coronary artery may cause inferior myocardial
infarction

Surgical management
Gestational
timeframe
Management
< 28/40 Aortic repair with the fetus kept in utero
28-32/40 Dependent on fetal condition
> 32/40 Primary Cesarean section followed by aortic repair at the same
operation
Mitral stenosis
Most cases associated with rheumatic heart disease
Becoming less common in British women; suspect in Immigrant women
Commonest cardiac condition in pregnancy
Commonly associated with mortality
Valve surgery; balloon valvuloplasty preferable
Pulmonary embolism
Leading cause of mortality in pregnancy
Half dose scintigraphy; CT chest if underlying lung disease should aid
diagnosis
Treatment with low molecular weight heparin throughout pregnancy and 4-6
weeks after childbirth
Warfarin is contra indicated in pregnancy
References 1. Bates S.M. and Ginsberg J.S. How we manage venous thromboembolism during
pregnancy. Blood 2002 (100): 3470-3478.
2. Scarsbrook A.Fand Gleeson V. Investigating suspected pulmonary embolism in
pregnancy. BMJ 2003 (326) : 1135 doi: 10.1136/bmj.7399.1135.
3. Morley C. A. and Lim B. A. Lesson of the Week: The risks of delay in diagnosis of
breathlessness in pregnancy. BMJ 1995 (311) : 1083. A 67 year old man is investigated for biliary colic and a 4.8 cm abdominal aortic aneurysm is
identified. Which of the following statements relating to this condition is untrue?
A. The wall will be composed of dense fibrous tissue only
B. The majority are located inferior to the renal arteries

C. They occur most often in current or former smokers
D. He should initially be managed by a process of active surveillance
E. Aortoduodenal fistula is a recognised complication following repair.
They are true aneurysms and have all 3 layers of arterial wall.
Abdominal aorta aneurysm
Abdominal aortic aneurysms are a common problem in vascular surgery. They may occur as either true or false aneurysm. With the former all 3 layers of the
arterial wall are involved, in the latter only a single layer of fibrous tissue forms the aneurysm wall.
True abdominal aortic aneurysms have an approximate incidence of 0.06 per 1000 people. They are commonest in elderly men and for this reason the UK is now introducing the aneurysm screening program with the aim of performing an abdominal aortic ultrasound measurement in all men aged 65 years.
Causes
Several different groups of patients suffer from aneurysmal disease. The commonest group is those who suffer from standard arterial disease, i.e. Those
who are hypertensive, have diabetes and have been or are smokers. Other patients such as those suffering from connective tissue diseases such as
Marfan's may also develop aneurysms. In patients with abdominal aortic aneurysms the extracellular matrix becomes disrupted with a change in the balance of collagen and elastic fibres.
Management
Most abdominal aortic aneurysms are an incidental finding. Symptoms most often relate to rupture or impending rupture. 20% rupture anteriorly into the peritoneal cavity. Very poor prognosis. 80% rupture posteriorly into the retroperitoneal space The risk of rupture is related to aneurysm size, only 2% of aneurysms measuring less
than 4cm in diameter will rupture over a 5 year period. This contrasts with 75% of aneurysms measuring over 7cm in diameter.
This is well explained by La Places' law which relates size to transmural pressure. For this reason most vascular surgeons will subject patients with an aneurysm size of
5cm or greater to CT scanning of the chest, abdomen and pelvis with the aim of

delineating anatomy and planning treatment. Depending upon co-morbidities, surgery is generally offered once the aneurysm is between 5.5cm and 6cm.
A CT reconstruction showing an infrarenal abdominal aortic aneurysm. The walls of the sac
are calcified which may facilitate identification on plain x-rays
Image sourced from Wikipedia
Indications for surgery

Symptomatic aneurysms (80% annual mortality if untreated) Increasing size above 5.5cm if asymptomatic Rupture (100% mortality without surgery)
Surgical procedures
Abdominal aortic aneurysm repair
Procedure:
GA
Invasive monitoring (A-line, CVP, catheter)
Incision: Midline or transverse
Bowel and distal duodenum mobilised to access aorta.
Aneurysm neck and base dissected out and prepared for cross clamp
Systemic heparinisation
Cross clamp (distal first)
Longitudinal aortotomy
Atherectomy
Deal with back bleeding from lumbar vessels and inferior mesenteric artery
Insert graft either tube or bifurcated depending upon anatomy
Suture using Prolene (3/0 for proximal , distal anastomosis suture varies according to site)
Clamps off: End tidal CO2 will rise owing to effects of reperfusion, at this point major risk of
myocardial events.
Haemostasis
Closure of aneurysm sac to minimise risk of aorto-enteric fistula
Closure: Loop 1 PDS or Prolene to abdominal wall
Skin- surgeons preference
Post operatively:
ITU (Almost all)
Greatest risk of complications following emergency repair
Complications: Embolic- gut and foot infarcts
Cardiac - owing to premorbid states, reperfusion injury and effects of cross clamp
Wound problems
Later risks related to graft- infection and aorto-enteric fistula
Special groups
Supra renal AAA
These patients will require a supra renal clamp and this carries a far higher risk of
complications and risk of renal failure.
Ruptured AAA

Preoperatively the management depends upon haemodynamic instability. In patients with
symptoms of rupture (typical pain, haemodynamic compromise and risk factors) then ideally
prompt laparotomy. In those with vague symptoms and haemodynamic stability the ideal
test is CT scan to determine whether rupture has occurred or not. Most common rupture
site is retroperitoneal 80%. These patients will tend to develop retroperitoneal haematoma.
This can be disrupted if Bp is allowed to rise too high so aim for Bp 100mmHg.
Operative details are similar to elective repair although surgery should be swift, blind
rushing often makes the situation worse. Plunging vascular clamps blindly into a pool of
blood at the aneurysm neck carries the risk of injury the vena cava that these patients do not
withstand. Occasionally a supracoeliac clamp is needed to effect temporary control,
although leaving this applied for more than 20 minutes tends to carry a dismal outcome.
EVAR
Increasingly patients are now being offered endovascular aortic aneurysm repair. This is
undertaken by surgeons and radiologists working jointly. The morphology of the aneurysm is
important and not all are suitable. Here is a typical list of those features favoring a suitable
aneurysm:
Long neck Straight iliac vessels Healthy groin vessels
Clearly few AAA patients possess the above and compromise has to be made. The use of
fenestrated grafts can allow supra renal AAA to be treated.
Procedure:
GA
Radiology or theatre
Bilateral groin incisions
Common femoral artery dissected out
Heparinisation
Arteriotomy and insertion of guide wire
Dilation of arteriotomy
Insertion of EVAR Device
Once in satisfactory position it is released
Arteriotomy closed once check angiogram shows good position and no endoleak
Complications:
Endoleaks depending upon site are either Type I or 2. These may necessitate re-intervention
and all EVAR patients require follow up . Details are not needed for MRCS.
References

A reasonable review is provided by:
Sakalihasan N, Limet R, Defawe O. Abdominal aortic aneurysm. Lancet 2005 (365):1577-
1589
Which of the following statements in relation to the p53 tumour suppressor protein is
false?
A. It may induce necrosis of cells with non repairable DNA damage
B. It is affected in Li Fraumeni syndrome
C. It can induce DNA repair
D. It can halt the cell cycle
E. It may inhibit angiogenesis
When DNA cannot be repaired it will induce cellular apoptosis (not necrosis)
Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.
Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:
*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2
Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age

80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one
of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.
Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5
Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli
Which of the following cell types is most likely to be identified in the wall of a fistula
in ano?
A. Squamous cells
B. Goblet cells
C. Columnar cells
D. Ciliated columnar cells
E. None of the above
A fistula is an abnormal connection between two epithelial lined surfaces, in the case
of a fistula in ano it will be lined by squamous cells.
Fistulas
A fistula is defined as an abnormal connection between two epithelial
surfaces.
There are many types ranging from Branchial fistulae in the neck to entero-
cutaneous fistulae abdominally.

In general surgical practice the abdominal cavity generates the majority and
most of these arise from diverticular disease and Crohn's.
As a general rule all fistulae will resolve spontaneously as long as there is no
distal obstruction. This is particularly true of intestinal fistulae.
The four types of fistulae are:
Enterocutaneous These link the intestine to the skin. They may be high (>1L) or low output (<1L)
depending upon source. Duodenal /jejunal fistulae will tend to produce high volume,
electrolyte rich secretions which can lead to severe excoriation of the skin. Colo-
cutaneous fistulae will tend to leak faeculent material. Both fistulae may result from
the spontaneous rupture of an abscess cavity onto the skin (such as following perianal
abscess drainage) or may occur as a result of iatrogenic input. In some cases it may
even be surgically desirable e.g. mucous fistula following sub total colectomy for
colitis.
Suspect if there is excess fluid in the drain.
Enteroenteric or Enterocolic This is a fistula that involves the large or small intestine. They may originate in a
similar manner to enterocutaneous fistulae. A particular problem with this fistula type
is that bacterial overgrowth may precipitate malabsorption syndromes. This may be
particularly serious in inflammatory bowel disease.
Enterovaginal Aetiology as above.
Enterovesicular This type of fistula goes to the bladder. These fistulas may result in frequent urinary
tract infections, or the passage of gas from the urethra during urination.
Management Some rules relating to fistula management:
They will heal provided there is no underlying inflammatory bowel disease
and no distal obstruction, so conservative measures may be the best option
Where there is skin involvement, protect the overlying skin, often using a well
fitted stoma bag- skin damage is difficult to treat
A high output fistula may be rendered more easily managed by the use of
octreotide, this will tend to reduce the volume of pancreatic secretions.
Nutritional complications are common especially with high fistula (e.g. high
jejunal or duodenal) these may necessitate the use of TPN to provide
nutritional support together with the concomitant use of octreotide to reduce
volume and protect skin.
When managing perianal fistulae surgeons should avoid probing the fistula
where acute inflammation is present, this almost always worsens outcomes.
When perianal fistulae occur secondary to Crohn's disease the best
management option is often to drain acute sepsis and maintain that drainage

through the judicious use of setons whilst medical management is
implemented.
Always attempt to delineate the fistula anatomy, for abscesses and fistulae that
have an intra abdominal source the use of barium and CT studies should show
a track. For perianal fistulae surgeons should recall Goodsall's rule in relation
to internal and external openings.
22 year old man is referred to the surgical clinic. He has been complaining of varicose
veins for many years. On examination he has extensive varicosities of the right leg,
there are areas of marked port wine staining. The saphenofemoral junction is
competent on doppler assessment. The most likely underlying diagnosis is:
A. Deep vein thrombosis
B. Klippel-Trenaunay syndrome
C. Varicose veins due to sapheno-popliteal junction incompetence
D. Sturge - Weber syndrome
E. Angiosarcoma
Sturge - Weber syndrome is a an arteriovenous malformation affecting the face and
CNS, the peripheral vessels are not affected. Simple varicose veins should not
typically be associated with port wine staining, not should a DVT or angiosarcoma.
Klippel-Trenaunay syndrome
Klippel-Trenaunay-Weber syndrome generally affects a single extremity, although
cases of multiple affected limbs have been reported. The leg is the most common site
followed by the arms, the trunk, and rarely the head and the neck
Signs and symptoms The birth defect is diagnosed by the presence of a combination of these symptoms:
One or more distinctive port-wine stains with sharp borders
Varicose veins
Hypertrophy of bony and soft tissues, that may lead to local gigantism or
shrinking.
An improperly developed lymphatic system
In some cases, port-wine stains (capillary port wine type) may be absent. Such cases
are very rare and may be classified as "atypical Klippel-Trenaunay syndrome".
KTS can either affect blood vessels, lymph vessels, or both. The condition most
commonly presents with a mixture of the two. Those with venous involvement
experience increased pain and complications.

A 68 year old man presents with an ulcerated lesion on his right cheek. It is excised and on
histological assessment a squamous cell carcinoma is diagnosed. It measures 25mm in
diameter and is 4mm deep. Which of the following statements relating to this condition is
false?
A. In this particular case margins of at least 6mm are
required
B. Use of cryosurgery to treat this patients lesion
would have been unsafe
C. Use of radiotherapy to treat this lesion would have
been unsafe
D. This patients local recurrence rate may approach
15%
E. The disese usually spreads via lymphatics
Poor prognostic factors in SCC:
Size >20mm (local recurrence rate of up to 15%)
Depth greater than 4mm (risk of metastasis up to 30%)
This man has an SCC with significant risk of metastasis. Although cryotherapy may be used to
treat SCC it would be most unsafe in this setting as the lesion extends deeply. However,
radiotherapy is a safe treatment modality for SCC and may be used in selected cases. It is
unwise to use radiotherapy in areas prone to radionecrosis e.g. the nose.
Squamous cell carcinoma of the skin
Second most common skin malignancy Derived from epidermal keratinocytes Commonest in fair skinned individuals in sun exposed sites May occur in perianal and genital skin especially in association with Human
Papilloma Virus 16 and 18 infections.
Groups at high risk

Renal transplant and on immunosuppression
Individuals with HIV
Those who have received psoralen UVA therapy
Chronic wounds (Marjolins ulcer)
Xeroderma pigmentosum
Oculocutaneous albinism
Prognosis
Good Prognosis Poor prognosis
Well differentiated tumours Poorly differentiated tumours
<20mm diameter >20mm in diameter
<2mm deep >4mm deep
No associated diseases Immunosupression for whatever reason
Treatment
Surgical excision with 4mm margins if lesion <20mm in diameter. If tumour >20mm then
margins should be 6mm.
Squamous cell carcinomas of the skin typically arise in areas of sun exposure as shown here

Image sourced from Wikipedia
References
The British Association of Dermatology provides guidelines for the diagnosis and treatment
of SCC.
http://www. bad.org.uk
A 23 year old man presents with weight loss fatigue and lymphadenopathy. He is
diagnosed with tuberculosis. Which of the following processes most closely matches
the underlying pathological process?
A. Type 1 hypersensitivity reaction
B. Type 2 hypersensitivity reaction
C. Type 3 hypersensitivity reaction
D. Type 4 hypersensitivity reaction
E. None of the above
Granulomas (which occur in tuberculosis) are a feature of Type 4 hypersensitivity
reactions.
Hypersensitivity reactions
The Gell and Coombs classification divides hypersensitivity reactions into 4 types
Type I Type II Type III Type IV
Description Anaphylactic Cytotoxic Immune
complex
Delayed type
Mediator IgE IgG, IgM IgG, IgM T-cells
Antigen Exogenous Cell surface Soluble Tissues
Response
time
Minutes Hours Hours 2-3 days
Examples Asthma
Hay fever
Autoimmune
haemolytic anaemia
Pemphigus
Goodpasture's
Serum
sickness
SLE
Aspergillosis
Graft versus host
disease
Contact
dermatitis
A 73 year old man undergoes an emergency amputation for severe lower limb sepsis
and gangrene. Post operatively he develops disseminated intravascular coagulation.
Which of the following clotting factors will be most rapidly consumed in this
process?

A. Factor V and VIII
B. Factor I
C. Factor I and III
D. Factor III and VII
E. Factor VI and VIII
D-I-S-S-E-M-I-N-A-T-E-D
D-Dx: D dimer
I-Immune complexes
S-Snakebite, shock, heatstroke
S-SLE
E-Eclampsia, HELLP syndrome
M-Massive tissue damage
I-Infections: viral and bacterial
N-Neoplasms
A-Acute promyelocytic leukemia
T-Tumor products: Tissue Factor (TF) and TF-like factors released by carcinomas of
pancreas, prostate, lung,
colon, stomach
E-Endotoxins (bacterial)
D-Dead fetus (retained)
DIC Will tend to consume factors five and eight intially (and platelets).
Disseminated intravascular coagulation
Simultaneous coagulation and haemorrhage caused by initially formation of thrombi
which consume clotting factors (factors 5,8) and platelets, ultimately leading to
bleeding
Causes include:
Infection
Malignancy
Trauma e.g. major surgery, burns, shock, dissecting aortic aneurysm
Liver disease
Obstetric complications
Key points
Clinically bleeding is usually a dominant feature, bruising, ischaemia and
organ failure

Blood tests: prolonged clotting times, thrombocytopenia, decreased
fibrinogen, increased fibrinogen degradation products
Treat the underlying cause and supportive management
A 63 year old Japanese man presents with epigastric discomfort and iron deficiency
anaemia. He undergoes an upper GI endoscopy, where the following appearances are found:
Image sourced from Wikipedia
The most likely diagnosis is:
A. Squamous cell carcinoma
B. Linitis plastica
C. Leiomyosarcoma
D. Gastric varices
E. None of the above

During upper GI endoscopy, a linitis plastica lesion may prevent gastric distension.
Linitis plastica produces a diffuse infiltrating lesion, the stomach is fibrotic and rigid and will
not typically distend. This may be described as a 'leather bottle stomach'. Diagnosis is made
with a combination of pathology examination with endoscopy, radiological or surgical
assessment. Pathologically signet-ring cell proliferation occurs.
At the present time clinical images do not form part of the MRCS Part A exam
Gastric cancer
Overview
There are 700,000 new cases of gastric cancer worldwide each year. It is most common in
Japan and less common in western countries. It is more common in men and incidence rises
with increasing age. The exact cause of many sporadic cancer is not known, however,
familial cases do occur in HNPCC families. In addition, smoking and smoked or preserved
foods increase the risk. Japanese migrants retain their increased risk (decreased in
subsequent generations). The distribution of the disease in western countries is changing
towards a more proximal location (perhaps due to rising obesity).
Pathology
There is some evidence of support a stepwise progression of the disease through intestinal
metaplasia progressing to atrophic gastritis and subsequent dysplasia, through to cancer.
The favoured staging system is TNM. The risk of lymph node involvement is related to size
and depth of invasion; early cancers confined to submucosa have a 20% incidence of lymph
node metastasis. Tumours of the gastro-oesophageal junction are classified as below:
Type
1
True oesophageal cancers and may be associated with Barrett's oesophagus.
Type
2
Carcinoma of the cardia, arising from cardiac type epithelium
or short segments with intestinal metaplasia at the oesophagogastric junction.
Type
3
Sub cardial cancers that spread across the junction. Involve similar nodal stations to
gastric cancer.
Groups for close endoscopic monitoring
Intestinal metaplasia of columnar type Atrophic gastritis Low to medium grade dysplasia Patients who have previously undergone resections for benign peptic ulcer disease
(except highly selective vagotomy).

Referral to endoscopy
Patients of any age with
dyspepsia and any of the
following
Patients without
dyspepsia
Worsening dyspepsia
Chronic gastrointestinal bleeding Dysphagia Barretts oesophagus
Dysphagia Unexplained abdominal
pain or weight loss
Intestinal metaplasia
Weight loss Vomiting Dysplasia
Iron deficiency anaemia Upper abdominal mass Atrophic gastritis
Upper abdominal mass Jaundice Patient aged over 55 years with
unexplained or persistent
dyspepsia
Upper GI endoscopy performed for dyspepsia. The addition of dye spraying (as shown in the
bottom right) may facilitate identification of smaller tumours
Image sourced from Wikipedia

Staging
CT scanning of the chest abdomen and pelvis is the routine first line staging investigation in most centres.
Laparoscopy to identify occult peritoneal disease PET CT (particularly for junctional tumours)
Treatment
Proximally sited disease greater than 5-10cm from the OG junction may be treated by sub total gastrectomy
Total gastrectomy if tumour is <5cm from OG junction For type 2 junctional tumours (extending into oesophagus) oesophagogastrectomy is
usual Endoscopic sub mucosal resection may play a role in early gastric cancer confined to
the mucosa and perhaps the sub mucosa (this is debated) Lymphadenectomy should be performed. A D2 lymphadenectomy is widely
advocated by the Japanese, the survival advantages of extended lymphadenectomy have been debated. However, the overall recommendation is that a D2 nodal dissection be undertaken.
Most patients will receive chemotherapy either pre or post operatively.
Prognosis
UK Data
Disease extent Percentage 5 year survival
All RO resections 54%
Early gastric cancer 91%
Stage 1 87%
Stage 2 65%
Stage 3 18%
Operative procedure
Total Gastrectomy , lymphadenectomy and Roux en Y anastomosis
General anaesthesia

Prophylactic intravenous antibiotics
Incision: Rooftop.
Perform a thorough laparotomy to identify any occult disease.
Mobilise the left lobe of the liver off the diaphragm and place a large pack over it. Insert a
large self retaining retractor e.g. omnitract or Balfour (take time with this, the set up should
be perfect). Pack the small bowel away.
Begin by mobilising the omentum off the transverse colon.
Proceed to detach the short gastric vessels.
Mobilise the pylorus and divide it at least 2cm distally using a linear cutter stapling device.
Continue the dissection into the lesser sac taking the lesser omentum and left gastric artery
flush at its origin.
The lymph nodes should be removed en bloc with the specimen where possible.
Place 2 stay sutures either side of the distal oesophagus. Ask the anaesthetist to pull back on
the nasogastric tube. Divide the distal oesophagus and remove the stomach.
The oesphago jejunal anastomosis should be constructed. Identify the DJ flexure and bring a
loop of jejunum up to the oesophagus (to check it will reach). Divide the jejunum at this
point. Bring the divided jejunum either retrocolic or antecolic to the oesophagus.
Anastamose the oesophagus to the jejunum, using either interrupted 3/0 vicryl or a stapling
device. Then create the remainder of the Roux en Y reconstruction distally.
Place a jejunostomy feeding tube.
Wash out the abdomen and insert drains (usually the anastomosis and duodenal stump).
Help the anaesthetist insert the nasogastric tube (carefully!)
Close the abdomen and skin.
Enteral feeding may commence on the first post-operative day. However, most surgeons will
leave patients on free NG drainage for several days and keep them nil by mouth.
Rate question:
1
2
3
4
5
Theme: Genetics and cancer
A. Multiple endocrine neoplasia type I
B. Multiple endocrine neoplasia type II
C. Gardner's syndrome
D. Lynch Syndrome
E. Kartagener's syndrome
F. Neurofibromatosis Type I
G. Neurofibromatosis Type II
Please select the most likely condition for the disease process described. Each option
may be used once, more than once or not at all.

26. A 40 year old male is found to have multiple colonic polyps during a
colonoscopy. He mentions that he has extra teeth.
You answered Kartagener's syndrome
The correct answer is Gardner's syndrome
Gardner's syndrome is an AD disorder, characterised by: Colonic polyps,
supernumerary teeth, jaw osteomas, congenital hypertrophy of retinal
pigment. osteomas of the skull, thyroid cancer, epidermoid cysts, fibromas
and sebaceous cysts.
27. A 10 year old boy who has learning difficulties, reports a difference in size
between his two legs.
You answered Gardner's syndrome
The correct answer is Neurofibromatosis Type I
Neurofibromatosis type I. A hallmark finding is a plexiform neurofibroma,
which is a sheet of neurofibromatosis tissue which encases major nerves. In
children this attracts extra blood circulation, which can accelerate growth of
the affected limb.
Other features include:
Schwannoma, > 6
Cafe au lait spots, axillary freckling, Lisch nodules, Optic glioma.
Meningiomas, Glioma, or Schwannoma.
28. A 22 year old is found to have bilateral acoustic neuromas.
You answered Neurofibromatosis Type I
The correct answer is Neurofibromatosis Type II
In NF2 bilateral acoustic neuromas are characteristic with a FH of
Neurofibroma,
Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.

Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:
*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2
Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age
80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one
of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.
Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5
Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli

A 52 year old lady is referred to the breast clinic with symptoms of nipple discharge.
The discharge is usually thick and green. Which of the following statements relating
to the most likely underlying diagnosis is untrue?
A. The majority of patients will be smokers
B. Typically produces blood stained nipple
discharge
C. It is not associated with increased risk of breast
cancer
D. May result in development of mammary duct
fistula
E. May require total duct excision (Hadfields
operation) if it fails to resolve
Blood stained nipple discharge
should always be investigated.
Nipple fluid cytology is generally
unhelpful.
Discharge of this type of material is most likely to be due to duct ectasia. Green or
brown discharge is most common. Blood stained discharge should raise concern of
intraductal papilloma or cancer.
Nipple discharge
Causes of nipple discharge
Physiological During breast feeding
Galactorrhoea Commonest cause may be response to emotional events,
drugs such as histamine receptor anatagonists are also
implicated
Hyperprolactinaemia Commonest type of pituitary tumour
Microadenomas <1cm in diameter
Macroadenomas >1cm in diameter
Pressure on optic chiasm may cause bitemporal
hemianopia
Mammary duct
ectasia
Dilatation breast ducts.
Most common in enopausal women
Discharge typically thick and green in colour
Most common in smokers
Carcinoma Often blood stained
May be underlying mass or axillary lymphadenopathy

Intraductal
papilloma
Commoner in younger patients
May cause blood stained discharge
There is usually no palpable lump
Assessment of patients
Examine breast and determine whether there is mass lesion present
All mass lesions should undergo Triple assessment.
Reporting of investigations Where a mass lesion is suspected or investigations are requested these are prefixed
using a system that denotes the investigation type e.g. M for mammography, followed
by a numerical code as shown below:
1 No abnormality
2 Abnormality with benign features
3 Indeterminate probably benign
4 Indeterminate probably malignant
5 Malignant
Management of non malignant nipple discharge
Exclude endocrine disease
Nipple cytology unhelpful
Smoking cessation advice for duct ectasia
For duct ectasia with severe symptoms, total duct excision may be warrented.
Which of the following statements relating to gas gangrene is untrue?
A. There is necrosis with putrefaction
B. The causative pathogens may be detected on normal perineal skin
C. Treatment with low dose penicillin is indicated
D. Hyperbaric oxygen may be beneficial
E. Clostridium perfringens is a recognised cause

Rapid surgery and high dose antibiotics are indicated in the treatment of gas gangrene.
Meleney's Gangrene and Necrotising Fasciitis
Necrotising fasciitis
Advancing soft tissue infection associated with fascial necrosis Uncommon, but can be fatal In many cases there is underlying background immunosuppression e.g. Diabetes Caused by polymicrobial flora (aerobic and anaerobic) and MRSA is seen increasingly
in cases of necrotising fasciitis Streptococcus is the commonest organism in isolated pathogen infection (15%)
Meleneys gangrene
Meleneys is a similar principle but the infection is more superficially sited than necrotising fasciitis and often confined to the trunk
Fournier gangrene
Necrotising fasciitis affecting the perineum Polymicrobial with E.coli and Bacteroides acting in synergy
Clinical features
Fever
Pain
Cellulitis
Oedema
Induration
Numbness
Late findings
Purple/black skin discolouration
Blistering
Haemorrhagic bullae
Crepitus
Dirty Dishwater fluid discharge
Septic shock
A typical case of gas gangrene presenting late demonstrating some of the features described
above

Image sourced from gangrene" target="_blank" style =
"font-size:11px; color:#777;" >Wikipedia
Diagnosis is mainly clinical
Management
Radical surgical debridement forms the cornerstone of management Sterile dressing is used to dress the wound Reconstructive surgery is considered once the infection is completely treated
Reference
Necrotising fasciitis
Saiidy Hasham, Paolo Matteucci, Paul R W Stanley, Nick B Hart
BMJ 2005;330:830-833
A 30 year old man presents with abdominal distension, a laparotomy is performed, at
operation the abdomen is filled with a large amount of gelatinous fluid. What is the
most likely underlying diagnosis?
A. Infection with entamoeba histolytica
B. Pseudomxyoma peritonei
C. Metastatic colonic cancer

D. Chylous ascites
E. None of the above
Pseudomyxoma is associated with the deposition of large amounts of gelatinous
material. The appendix is the commonest organ or origin.
Pseudomyxoma Peritonei
Rare mucinous tumour
Most commonly arising from the appendix (other abdominal viscera are also
recognised as primary sites)
Incidence of 1-2/1,000,000 per year
The disease is characterised by the accumulation of large amounts of
mucinous material in the abdominal cavity
Treatment Is usually surgical and consists of cytoreductive surgery (and often peritonectomy c.f
Sugarbaker procedure) combined with intra peritoneal chemotherapy with mitomycin
C.
Survival is related to the quality of primary treatment and in Sugarbakers own centre
5 year survival rates of 75% have been quoted. Patients with disseminated
intraperitoneal malignancy from another source fare far worse.
In selected patients a second look laparotomy is advocated and some practice this
routinely.
A 30 year old man is suspected of having appendicitis. At operation an inflamed
Meckels diverticulum is found. Which of the following vessels is responsible for the
blood supply to a Meckels diverticulum?
A. Right colic artery
B. Vitelline artery
C. Appendicular artery
D. Internal iliac artery
E. External iliac artery
The vitelline arteries supply a Meckels these are usually derived from the ileal
arcades.
Meckel's diverticulum

Congenital abnormality resulting in incomplete obliteration of the vitello-
intestinal duct
Normally, in the foetus, there is an attachment between the vitello-intestinal
duct and the yolk sac.This disappears at 6 weeks gestation.
The tip is free in majority of cases.
Associated with enterocystomas, umbilical sinuses, and omphaloileal fistulas.
Arterial supply: omphalomesenteric artery.
2% of population, 2 inches long, 2 feet from the ileocaecal valve.
Typically lined by ileal mucosa but ectopic gastric mucosa can occur, with the
risk of peptic ulceration. Pancreatic and jejunal mucosa can also occur.
Clinical
Normally asymptomatic and an incidental finding.
Complications are the result of obstruction, ectopic tissue, or inflammation.
Removal if narrow neck or symptomatic. Options are between wedge excision
or formal small bowel resection and anastomosis.
A 23 year old man suffers a thermal injury to his left hand. It becomes red and
painful. Which of the following mediators are not involved in this process?
A. Histamine
B. Free radicals
C. Prostaglandins
D. Leukotrienes
E. Serotonin
Acute inflammation is not
mediated by free radicals
Chemical mediators facilitate the spread of inflammation into normal tissue
Chemical mediators include:
Lysosomal compounds
Chemokines such as serotinin and histamine (released by platelets and mast
cells)
Other enzyme cascades producing inflammatory mediators include:
Complement, kinin, coagulation system & fibrinolytic system

Acute inflammation
Inflammation is the reaction of the tissue elements to injury. Vascular changes occur,
resulting in the generation of a protein rich exudate. So long as the injury does not
totally destroy the existing tissue architecture, the episode may resolve with
restoration of original tissue architecture.
Vascular changes
Vasodilation occurs and persists throughout the inflammatory phase.
Inflammatory cells exit the circulation at the site of injury.
The equilibrium that balances Starlings forces within capillary beds is
disrupted and a protein rich exudate will form as the vessel walls also become
more permeable to proteins.
The high fibrinogen content of the fluid may form a fibrin clot. This has
several important immunomodulatory functions.
Sequelae
Resolution Typically occurs with minimal initial injury
Stimulus removed and normal tissue architecture
results
Organisation Delayed removed of exudate
Tissues undergo organisation and usually fibrosis
Suppuration Typically formation of an abscess or an empyema
Sequestration of large quantities of dead
neutrophils
Progression to chronic
inflammation
Coupled inflammatory and reparative activities
Usually occurs when initial infection or
suppuration has been inadequately managed
Causes
Microbacterial infections e.g. Viruses, exotoxins or endotoxins released by
bacteria
Chemical agents
Physical agents e.g. Trauma
Hypersensitivity reactions
Tissue necrosis
Presence of neutrophil polymorphs is a histological diagnostic feature of acute
inflammation

Which of the following associations are incorrect?
A. Afro-Caribbean skin and keloid scarring
B. Extensive third degree burns and wound contraction
C. Chemotherapy and dehisence of healed wounds
D. Poor healing at the site of previous radiotherapy
E. Zinc deficiency and delayed healing
Wound healing
Surgical wounds are either incisional or excisional and either clean, clean contaminated or
dirty. Although the stages of wound healing are broadly similar their contributions will vary
according to the wound type.
The main stages of wound healing include:
Haemostasis
Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot.
Inflammation
Neutrophils migrate into wound (function impaired in diabetes). Growth factors released, including basic fibroblast growth factor and vascular
endothelial growth factor. Fibroblasts replicate within the adjacent matrix and migrate into wound. Macrophages and fibroblasts couple matrix regeneration and clot substitution.
Regeneration
Platelet derived growth factor and transformation growth factors stimulate fibroblasts and epithelial cells.

Fibroblasts produce a collagen network. Angiogenesis occurs and wound resembles granulation tissue.
Remodeling
Longest phase of the healing process and may last up to one year (or longer). During this phase fibroblasts become differentiated (myofibroblasts) and these
facilitate wound contraction. Collagen fibres are remodeled. Microvessels regress leaving a pale scar.
The above description represents an idealised scenario. A number of diseases may distort
this process. It is obvious that one of the key events is the establishing well vascularised
tissue. At a local level angiogenesis occurs, but if arterial inflow and venous return are
compromised then healing may be impaired, or simply nor occur at all. The results of
vascular compromise are all too evidence in those with peripheral vascular disease or those
poorly constructed bowel anastomoses.
Conditions such as jaundice will impair fibroblast synthetic function and overall immunity
with a detrimental effect in most parts of healing.
Problems with scars:
Hypertrophic scars
Excessive amounts of collagen within a scar. Nodules may be present histologically
containing randomly arranged fibrils within and parallel fibres on the surface. The tissue
itself is confined to the extent of the wound itself and is usually the result of a full thickness
dermal injury. They may go on to develop contractures.
Image of hypertrophic scarring. Note that it remains confined to the boundaries of the
original wound:

Image sourced from Wikipedia
Keloid scars
Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the
boundaries of the original injury. They do not contain nodules and may occur following even
trivial injury. They do not regress over time and may recur following removal.
Image of a keloid scar. Note the extension beyond the boundaries of the original incision:
Image sourced from Wikipedia
Drugs which impair wound healing:

Non steroidal anti inflammatory drugs Steroids Immunosupressive agents Anti neoplastic drugs
Closure
Delayed primary closure is the anatomically precise closure that is delayed for a few days but
before granulation tissue becomes macroscopically evident.
Secondary closure refers to either spontaneous closure or to surgical closure after
granulation tissue has formed.
A 23 year old man fractures his right tibia in a sporting accident. At which point in the
healing process is fracture callus most likely to be visible radiologically?
A. 1 day
B. 7 days
C. 8 weeks
D. 6 weeks
E. 3 weeks
Fracture callus is composed of fibroblasts and chondroblasts and the synthesis of
fibrocartilage. It is typically visible on radiographs approximately 3 weeks following
injury. If delayed then there may be risk of non union.
Fracture healing
Bone fracture - Bleeding vessels in the bone and periosteum
- Clot and haematoma formation
- The clot organises over a week (improved structure and collagen)
- The periosteum contains osteoblasts which produce new bone
- Mesenchymal cells produce cartilage (fibrocartilage and hyaline cartilage) in the soft
tissue around the fracture
- Connective tissue + hyaline cartilage = callus
- As the new bone approaches the new cartilage, endochondral ossification occurs to
bridge the gap
- Trabecular bone forms
- Trabecular bone is resorbed by osteoclasts and replaced with compact bone
Factors Affecting Fracture Healing

Age
Malnutrition
Bone disorders: osteoporosis
Systemic disorders: diabetes, Marfan's syndrome and Ehlers-Danlos syndrome
cause abnormal musculoskeletal healing.
Drugs: steroids, non steroidal anti inflammatory agents.
Type of bone: Cancellous (spongy) bone fractures are usually more stable,
involve greater surface areas, and have a better blood supply than cortical
(compact) bone fractures.
Degree of Trauma: The more extensive the injury to bone and surrounding soft
tissue, the poorer the outcome.
Vascular Injury: Especially the femoral head, talus, and scaphoid bones.
Degree of Immobilization
Intra-articular Fractures: These fractures communicate with synovial fluid,
which contains collagenases that retard bone healing.
Separation of Bone Ends: Normal apposition of fracture fragments is needed
for union to occur. Inadequate reduction, excessive traction, or interposition of
soft tissue will prevent healing.
Infection
Of the options below, which does not cause lymphadenopathy?
A. Kawasaki disease
B. Systemic Lupus Erthematosus
C. Phenytoin
D. Hydrallazine
E. Amiodarone
Lymphadenopathy
Lymphadenopathy in the neck, axillae, groins and abdomen
Need to note: solitary/multiple, defined/indistinct, hard/rubbery/soft,
tender/painless
Causes of lymphadenopathy
Mnemonic: Hodgkins disease
H aematological: Hodgkins lymphoma, NHL, Leukaemia

O ncological: metastases
D ermatopathic lympadenitis
G aucher's disease
K awasaki disease
I nfections: TB, glandular fever, Syphilis
N iemann Pick disease
S erum sickness
D rug reaction (phenytoin)
I mmunological (SLE)
S arcoidosis
E ndocrinological (Hyperthyroidism)
A ngioimmunoplastic lymphadenopathy
S LE
E osinophilic granulomatosis A 23 year old man is reviewed on the ward 10 days following a laparotomy. The wound is
inspected and is healing well. Which of the following processes is least likely to be occurring
in the wound at this stage?
A. Angiogenesis
B. Synthesis of collagen
C. Necrosis of fibroblasts
D. Secretion of matrix metalloproteinases by
fibroblasts
E. Proliferation of fibroblasts
Vasculogenesis vs Angiogenesis
Vascu is new. Angi is pre
Vasculogenesis is new vessels developing
in situ from existing mesenchyme.
Angiogenesis is vessels develop from
sprouting off pre-existing arteries.
Fibroblasts are an important cell type in healing wounds. They typically proliferate in the
early phases of wound healing. They release matrix metalloproteinases and these facilitate

in the remodelling of the matrix within the healing wound. Necrosis in a healing wound
would be unusual as wounds will tend to show clinical evidence of angiognesis by this time.
Wound healing
Surgical wounds are either incisional or excisional and either clean, clean contaminated or
dirty. Although the stages of wound healing are broadly similar their contributions will vary
according to the wound type.
The main stages of wound healing include:
Haemostasis
Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot.
Inflammation
Neutrophils migrate into wound (function impaired in diabetes). Growth factors released, including basic fibroblast growth factor and vascular
endothelial growth factor. Fibroblasts replicate within the adjacent matrix and migrate into wound. Macrophages and fibroblasts couple matrix regeneration and clot substitution.
Regeneration
Platelet derived growth factor and transformation growth factors stimulate fibroblasts and epithelial cells.
Fibroblasts produce a collagen network. Angiogenesis occurs and wound resembles granulation tissue.
Remodeling
Longest phase of the healing process and may last up to one year (or longer). During this phase fibroblasts become differentiated (myofibroblasts) and these
facilitate wound contraction. Collagen fibres are remodeled. Microvessels regress leaving a pale scar.
The above description represents an idealised scenario. A number of diseases may distort
this process. It is obvious that one of the key events is the establishing well vascularised
tissue. At a local level angiogenesis occurs, but if arterial inflow and venous return are
compromised then healing may be impaired, or simply nor occur at all. The results of
vascular compromise are all too evidence in those with peripheral vascular disease or those

poorly constructed bowel anastomoses.
Conditions such as jaundice will impair fibroblast synthetic function and overall immunity
with a detrimental effect in most parts of healing.
Problems with scars:
Hypertrophic scars
Excessive amounts of collagen within a scar. Nodules may be present histologically
containing randomly arranged fibrils within and parallel fibres on the surface. The tissue
itself is confined to the extent of the wound itself and is usually the result of a full thickness
dermal injury. They may go on to develop contractures.
Image of hypertrophic scarring. Note that it remains confined to the boundaries of the
original wound:
Image sourced from Wikipedia
Keloid scars
Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the
boundaries of the original injury. They do not contain nodules and may occur following even
trivial injury. They do not regress over time and may recur following removal.
Image of a keloid scar. Note the extension beyond the boundaries of the original incision:

Image sourced from Wikipedia
Drugs which impair wound healing:
Non steroidal anti inflammatory drugs Steroids Immunosupressive agents Anti neoplastic drugs
Closure
Delayed primary closure is the anatomically precise closure that is delayed for a few days but
before granulation tissue becomes macroscopically evident.
Secondary closure refers to either spontaneous closure or to surgical closure after
granulation tissue has formed.
A 25 year old women presents with a slowly enlarging mass on the side of the face.
Clinical examination demonstrates that the mass is located in the tail of the parotid
gland. There is no evidence of facial nerve involvement. What is the most likely
cause?
A. Sialolithiasis
B. Adenocarcinoma
C. Warthins tumour
D. Oncocytoma

E. Pleomorphic adenoma
Pleomorphic adenomas are the commonest tumours of the parotid gland and are often
slow growing, smooth and mobile. Warthins tumours are typically found in elderly
males and are composed of multiple cysts and solid components consisting of
lymphoid tissue. Warthins tumours are most often found in the tail of the parotid
gland, but not in 25 year old females, where a pleomorphic adenoma remains the most
likely lesion.
Parotid gland clinical
Causes of bilateral parotid enlargement
Mumps: Associated with meningoencephalitis, pancreatitis, orchitis, or
deafness
Parotitis
Sialectasis - especially if related to eating
Sjogren's syndrome: dry eyes or mouth, connective tissue disease
Sarcoidosis
Tuberculosis
Alcoholism
Myxoedema
Cushing's disease
Diabetes/insulin resistance
Liver cirrhosis
Gout
Bulimia nervosa
Drugs
Severe dehydration
Malnutrition
Causes of unilateral parotid enlargement
Salivary calculus
Tumour
Parotid gland tumours
Pleomorphic adenomas are the most common.
Incisional biopsy of parotid masses is not recommended, so superficial
parotidectomy is the usual procedure of choice.
Signs of facial nerve palsy and a parotid mass should raise suspicion of
malignancy.
Warthins tumours are relatively benign lesions that are slow growing and
occur most commonly in elderly male smokers.
Adenoid cystic carcinoma have a tendency for perineural invasion.

Beta-naphthalamine is associated with which of the following malignancies?
A. Lung cancer
B. Bowel cancer
C. Bladder cancer
D. Liver cancer
E. Renal cancer
Beta-naphthalamine is used in the rubber industry.
The following factors are associated with the development of bladder cancer:
smoking
occupational: aniline dyes used in printing and textile industry, rubber
manufacture
schistosomiasis
drugs: cyclophosphamide
Occupational cancers
Occupational cancers accounted for 5.3% cancer deaths in 2005.
In men the main cancers include:
Mesothelioma
Bladder cancer
Non melanoma skin cancer
Lung cancer
Sino nasal cancer
Occupations with high levels of occupational tumours include:
Construction industry
Working with coal tar and pitch
Mining
Metalworkers
Working with asbestos (accounts for 98% of all mesotheliomas)
Working in rubber industry
Shift work has been linked to breast cancer in women (Health and safety executive

report RR595).
The latency between exposure and disease is typically 15 years for solid tumours and
20 for leukaemia.
Many occupational cancers are otherwise rare. For example sino nasal cancer is an
uncommon tumour, 50% will be SCC. They are linked to conditions such as wood
dust exposure and unlike lung cancer is not strongly linked to cigarette smoking.
Another typical occupational tumour is angiosarcoma of the liver which is linked to
working with vinyl chloride. Again in the non occupational context this is an
extremely rare sporadic tumour.
A 56 year old man with Wilsons disease presents with right upper quadrant
discomfort. An ultrasound scan is performed and this demonstrates a mass lesion in
the right lobe of the liver. What is the most appropriate method of establishing the
underlying diagnosis?
A. PET CT scan
B. Ultrasound guided biopsy
C. Measurement of serum alpha feto protein
D. MRI scan of the liver
E. CT scan of the liver
High AFP + chronic liver
inflammation = Hepatocellular
carcinoma.
This is likely to be a hepatocellulcar carcinoma. Diagnosis is usually made by AFP
measurement (with further imaging depending on the result). Biopsy should not be
performed as it may seed the tumour. Chronic liver diseases such as Wilsons disease
(Hepato-lenticular degeneration) increase the risk.
Liver tumours
Primary liver tumours The most common primary tumours are cholangiocarcinoma and hepatocellular
carcinoma. Overall metastatic disease accounts for 95% of all liver malignancies
making the primary liver tumours comparatively rare.
Primary liver tumours include:
Cholangiocarcinoma
Hepatocellular carcinoma
Hepatoblastoma
Sarcomas (Rare)

Lymphomas
Carcinoids (most often secondary although primary may occur)
Hepatocellular carcinoma These account for the bulk of primary liver tumours (75% cases). Its worldwide
incidence reflects its propensity to occur on a background of chronic inflammatory
activity. Most cases arise in cirrhotic livers or those with chronic hepatitis B infection,
especially where viral replication is actively occurring. In the UK it accounts for less
than 5% of all cancers, although in parts of Asia its incidence is 100 per 100,000.
The majority of patients (80%) present with existing liver cirrhosis, with a mass
discovered on screening ultrasound.
Diagnosis
CT/ MRI (usually both) are the imaging modalities of choice
a-fetoprotein is elevated in almost all cases
Biopsy should be avoided as it seeds tumours cells through a resection plane.
In cases of diagnostic doubt serial CT and aFP measurements are the preferred
strategy.
Treatment
Patients should be staged with liver MRI and chest, abdomen and pelvic CT
scan.
The testis should be examined in males (testicular tumours may cause raised
AFP). PET CT may be used to identify occult nodal disease.
Surgical resection is the mainstay of treatment in operable cases. In patients
with a small primary tumour in a cirrhotic liver whose primary disease process
is controlled, consideration may be given to primary whole liver resection and
transplantation.
Liver resections are an option but since most cases occur in an already
diseased liver the operative risks and post-operative hepatic dysfunction are
far greater than is seen following metastectomy.
These tumours are not particularly chemo or radiosensitive however, both may
be used in a palliative setting. Tumour ablation is a more popular strategy.
Survival Poor, overall survival is 15% at 5 years.
Cholangiocarcinoma This is the second most common type of primary liver malignancy. As its name
suggests these tumours arise in the bile ducts. Up to 80% of tumours arise in the extra
hepatic biliary tree. Most patients present with jaundice and by this stage the majority
will have disease that is not resectable.
Primary scelerosing cholangitis is the main risk factor. In deprived countries typhoid
and liver flukes are also major risk factors.

Diagnosis
Patients will typically have an obstructive picture on liver function tests.
CA 19-9, CEA and CA 125 are often elevated
CT/ MRI and MRCP are the imaging methods of choice.
Treatment
Surgical resection offers the best chance of cure. Local invasion of peri hilar
tumours is a particular problem and this coupled with lobar atrophy will often
contra indicate surgical resection.
Palliation of jaundice is important, although metallic stents should be avoided
in those considered for resection.
Survival Is poor, approximately 15% 5 year survival.
A 55 year old man has suffered from reflux oesophagitis for many years. During a
recent endoscopy a biopsy is taken from the distal oesophagus. The histopathology
report indicates that cells are identified with features of coarse chromatin and
abnormal mitoses. The cells are confined to the superficial epithelial layer only.
Which of the following accounts for this process?
A. Metaplasia
B. Apoptosis
C. Autoimmune oesophagitis
D. Dysplasia
E. Infection with Helicobacter pylori
Dysplasia = pre
cancerous
Dysplasia tends to develop as a result of prolonged stimulation by precipitants.
Removal of these precipitants may possibly reverse these changes. Replacement of
differentiated cells wth another cell type describes metaplasia rather than dysplasia.
The absence of invasion distinguishes this from malignancy.
Dysplasia
Premalignant condition
Disordered growth and differentiation of calls

Alteration in size, shape, and organization of cells
Features increased abnormal cell growth (increased number of
mitoses/abnormal mitoses and cellular differentiation)
Underlying connective tissue is not invaded
Causes include smoking, Helicobacter pylori, Human papilloma virus
Main differences to metaplasia is that dysplasia is considered to be part of
carcinogenesis (pre cancerous) and is associated with a delay in maturation of
cells rather than differentiated cells replacing one another.
The absence of invasion differentiates dysplasia from invasive malignancy.
Severe dysplasia with foci of invasion are well recognised.
A 63 year old man has a history of claudication that has been present for many years.
He is recently evaluated in the clinic and a duplex scan shows that he has an 85%
stenosis of the superficial femoral artery. Two weeks later he presents with a 1 hour
history of severe pain in his leg. On examination he has absent pulses in the affected
limb and it is much cooler than the contra-lateral limb. Which process best accounts
for this presentation?
A. Thrombosis
B. Embolus
C. Atheroma growth
D. Sub intimal dissection
E. Anaemia
Theme from April 2012 Exam
In an existing lesion a complication such as thrombosis is more likely than embolus.
These patients should receive heparin and imaging with duplex scanning. Whilst an
early surgical bypass or intra-arterial thrombolysis may be indicated, an embolectomy
should not generally be performed as the lesion is not an embolus and the operation
therefore ineffective.
Claudication
Claudication is a condition in which patients develop pain in a limb during periods of
exercise. The underlying disorder is usually that of arterial insufficiency. Atheroma
develops in the arterial wall and once this occludes >50-75% of the lumenal diameter
the supply to metabolising tissues distally may become compromised. The typical
claudicant complains of calf pain that is worse on exercise and relieved by rest. This
typical description assumes that the SFA is the site of disease, more proximal disease
may present with other symptoms such as buttock claudication and impotence.
The history is usually a progressive one, patients presenting as an emergency with

severe pain, diminished sensation, pallor and absent pulses have critical limb
ischaemia. This may complicate claudication and usually indicates a plaque related
complication, such as thrombosis.
Risk factors Risk factors for claudication include smoking, diabetes and hyperlipidaemia.
Diagnosis Diagnostic work -up includes measurement of ankle- brachial pressure indices, duplex
scanning and formal angiography.
Treatment Those with long claudication distances, no ulceration or gangrene may be managed
conservatively. Patients with rest pain, ulceration or gangrene will almost always
require intervention. All patients should receive an antiplatelet agent and a statin
unless there are compelling contra-indications.
The following are true of carcinoid tumours except:
A. When present in the appendix tip and measure less than 2 cm have
an excellent prognosis
B. Even when metastatic disease is present it tends to follow a
protracted course
C. When present in the appendix body tend to present with carcinoid
syndrome even when liver metastases are not present
D. May be imaged using 5 HIAA radionucleotide scanning
E. Advanced appendiceal carcinoids may require right hemicolectomy.
Rule of thirds:
1/3 multiple
1/3 small bowel
1/3 metastasize
1/3 second
tumour
Liver metastases are necessary for the presence of carcinoid syndrome.
Carcinoid syndrome
Carcinoid tumours secrete serotonin
Originate in neuroendocrine cells mainly in the intestine (midgut-distal
ileum/appendix)
Can occur in the rectum, bronchi
Hormonal symptoms mainly occur when disease spreads outside the bowel

Clinical features - Onset: years
- Flushing face
- Palpitations
- Tricuspid stenosis causing dyspnoea
- Asthma
- Severe diarrhoea (secretory, persists despite fasting)
Investigation - 5-HIAA in a 24-hour urine collection
- Scintigraphy
- CT scan
Treatment
Octreotide
Surgical removal
During a difficult femoro-popliteal bypass operation the surgeon inadvertently places
a clamp across the femoral nerve. It remains there for most of the procedure. At the
end of the operation the nerve is inspected, it is in continuity but has evidence of
being crushed. Which of the following is most likely to occur over the following
months?
A. Wallerian degeneration
B. Rapid restoration of neuronal function because the axon itself is
intact
C. Normal but delayed neuronal transmission due to disruption of the
myelin
D. Absence of neuroma formation
E. None of the above
A neuronal injury such as this will result in Wallerian degeneration even though the
nerve remains in continuity. Neuromas may well form.
Nerve injury
There are 3 types of nerve injury:
Neuropraxia Nerve intact but electrical conduction is affected
Full recovery
Autonomic function preserved

Wallerian degeneration does not occur
Axonotmesis Axon is damaged and the myelin sheath is preserved. The
connective tissue framework is not affected.
Wallerian degeneration occurs.
Neurotmesis Disruption of the axon, myelin sheath and surrounding
connective tissue.
Wallerian degeneration occurs.
Wallerian Degeneration
Axonal degeneration distal to the site of injury.
Typically begins 24-36 hours following injury.
Axons are excitable prior to degeneration occurring.
Myelin sheath degenerates and is phagocytosed by tissue macrophages.
Nerve repair
Neuronal repair may only occur physiologically where nerves are in direct
contact. Where a large defect is present the process of nerve regeneration is
hampered and may not occur at all or result in the formation of a neuroma.
Where nerve regrowth occurs it typically occurs at a rate of 1mm per day.
A 38 year old lady who smokes heavily presents with recurrent episodes of
infection in the right breast. On examination she has an indurated area at the
lateral aspect of the nipple areaolar complex. Imaging shows no mass lesions.
What is the most likely diagnosis?
A. Duct ectasia
B. Periductal mastitis
C. Pagets disease of the nipple
D. Mondors disease of the breast
E. Radial scar
Periductal mastitis is common in smokers and may present with recurrent
infections. Treatment is with co-amoxyclav. Mondors disease of the breast is a
localised thrombophlebitis of a breast vein.
Duct ectasia
Duct ectasia is a dilatation and shortening of the terminal breast ducts within

3cm of the nipple. It is common and the incidence increases with age. It
typically presents with nipple retraction and occaisionally creamy nipple
discharge. It may be confused with periductal mastitis, which presents in
younger women, the vast majority of which are smokers. Periductal mastitis
typically presents with periareolar or sub areolar infections and may be
recurrent.
Patients with troublesome nipple discharge may be treated by
microdochectomy (if young) or total duct excision (if older). Which of the following statements relating to chronic inflammation is true?
A. Chronic inflammation is mainly secondary to acute inflammation
B. Neutrophils are the predominant cells involved
C. Growth factors are not involved in the process
D. Appendicitis is mainly a form of chronic inflammation
E. Fibrosis is a macroscopic feature
Macroscopic features include:
Ulcers Fibrosis Granulomatous process
It most commonly occurs as a primary event rather than as a result of acute inflammation.
Chronic inflammation
Overview
Chronic inflammation may occur secondary to acute inflammation.In most cases chronic
inflammation occurs as a primary process. These may be broadly viewed as being one of
three main processes:
Persisting infection with certain organisms such as Mycobacterium tuberculosis which results in delayed type hypersensitivity reactions and inflammation.
Prolonged exposure to non-biodegradable substances such as silica or suture materials which may induce an inflammatory response.
Autoimmune conditions involving antibodies formed against host antigens.

Acute vs. Chronic inflammation
Acute inflammation Chronic inflammation
Changes to existing vascular structure and increased
permeability of endothelial cells
Angiogenesis predominates
Infiltration of neutrophils Macrophages, plasma cells and
lymphocytes predominate
Process may resolve with:
Suppuration Complete resolution Abscess formation Progression to chronic inflammation Healing by fibrosis
Healing by fibrosis is the main result
Granulomatous inflammation
A granuloma consists of a microscopic aggregation of macrophages (with epithelial type
arrangement =epitheliod). Large giant cells may be found at the periphery of granulomas.
Mediators
Growth factors released by activated macrophages include agents such as interferon and
fibroblast growth factor (plus many more). Some of these such as interferons may have
systemic features resulting in systemic symptoms and signs, which may be present in
individuals with long standing chronic inflammation.
The finding of granulomas is pathognomonic of chronic inflammation, as illustrated in this
biopsy from a patient with colonic Crohns disease

Image sourced from Wikipedia
Theme: Paediatric ano-rectal disorders
A. Ulcerative colitis
B. Juvenile polyps
C. Haemorroids
D. Intussceception
E. Rectal cancer
F. Anal fissure
G. Arteriovenous malformation
Please select the most likely cause for the condition described. Each option may be
used once, more than once or not at all.
6. A 4 year old boy is brought to the clinic. He gives a history of difficult, painful
defecation with bright red rectal bleeding.
Anal fissure
Theme from April 2012 Exam
Painful rectal bleeding in this age group is typically due to a fissure. Treatment
should include stool softeners and lifestyle advice.
7. A 2 year old has a history of rectal bleeding. The parents notice that post
defecation, a cherry red lesion is present at the anal verge.
Juvenile polyps
Theme from September 2012 Exam
These lesions are usually hamartomas and this accounts for the colour of the
lesions. Although the lesions are not themselves malignant they serve as a
marker of an underlying polyposis disorder.
8. A 12 year old is brought to the colorectal clinic with a history of rectal
bleeding, altered bowel habit, weight loss and malaise. Abdominal
examination is normal.
Ulcerative colitis

The systemic features in the history are strongly suggestive of inflammatory
bowel disease rather than the other causes.
Paediatric proctology
Children may present with altered bowel habit and/ or rectal bleeding. Classical
haemorroidal disease is relatively rare in children. Painful bright red rectal bleeding is
much more common since constipation is a relatively common childhood disorder.
The hard stool causes a tear of the ano-rectal mucosa with subsequent fissure. The
pain from the fissure must be addressed promptly or the child will delay defecation
and this fissure will worsen.
Inflammatory bowel disease may present in a similar pattern in paediatric practice
with altered bowel habit (usually diarrhoea) and bleeding. Systemic features may be
present and investigation with an endoscopy may be required.
Children with intussceception usually present at a relatively young age and the history
is usually one of colicky abdominal pain, together with a mass on clinical
examination.The often cited red current jelly type stool is a rare but classical feature.
Juvenile polyps may occur as part of the familial polyposis coli syndromes. The
lesions, which are hamartomas, are often cherry red if they protrude externally
You review a 42-year-old woman 8 months following a renal transplant for focal
segmental glomerulosclerosis. She is on a combination of tacrolimus, mycophenolate,
and prednisolone. She has now presented with a five day history of feeling generally
unwell with jaundice, fatigue and arthralgia. On examination she has jaundice,
widespread lymphadenopathy and hepatomegaly. What is the most likely diagnosis?
A. Hepatitis C
B. Epstein-Barr virus
C. HIV
D. Hepatitis B
E. Cytomegalovirus
Post transplant complications
CMV: 4 weeks to 6 months post
transplant

EBV: post transplant lymphoproliferative
disease. > 6 months post transplant
Post transplant lymphoproliferative disorder is most commonly associated with
Epstein-Barr virus. It typically occurs 6 months post transplant and is associated with
high dose immunosupressant therapy. Remember cytomegalovirus presents within the
first 4 weeks to 6 months post transplant.
Renal transplant:HLA typing and graft failure
The human leucocyte antigen (HLA) system is the name given to the major
histocompatibility complex (MHC) in humans. It is coded for on chromosome 6.
Some basic points on the HLA system
Class 1 antigens include A, B and C. Class 2 antigens include DP,DQ and DR
When HLA matching for a renal transplant the relative importance of the HLA
antigens are as follows DR > B > A
Graft survival
1 year = 90%, 10 years = 60% for cadaveric transplants
1 year = 95%, 10 years = 70% for living-donor transplants
Post-op problems
ATN of graft
Vascular thrombosis
Urine leakage
UTI
Hyperacute acute rejection
Due to antibodies against donor HLA type 1 antigens
Rarely seen due to HLA matching
Acute graft failure (< 6 months)
Usually due to mismatched HLA
Other causes include cytomegalovirus infection
Management: give steroids, if resistant use monoclonal antibodies
Causes of chronic graft failure (> 6 months)
Chronic allograft nephropathy

Ureteric obstruction
Recurrence of original renal disease (MCGN > IgA > FSGS)
Which of the following processes facilitates phagocytosis?
A. Apoptosis
B. Opsonisation
C. Proteolysis
D. Angiogenesis
E. Necrosis
Theme from 2008 Exam
Opsonisation will facilitate phagocytosis. The micro-organism becomes coated with
antibody, C3b and certain acute phase proteins. The macrophages and neutrophils
have up regulation of phagocytic cell surface receptors in these circumstances, a
process mediated by pro-inflammatory cytokines. These cells then engulf the micro
organism.
Phagocytosis
Ingestion of pathogens or foreign materials by cells
First step is opsonisation whereby the organism is coated by antibody
Second step is adhesion to cell surface
Third step is pseudopodial extension to form a phagocytic vacuole
Lysosomes fuse with vacuole and degrade contents
Features which are evaluated for the grading of breast cancer include all the
following, except:
A. Tubule formation
B. Mitoses
C. Nuclear pleomorphism
D. Tumour necrosis
E. Coarse chromatin
The necrosis of a tumour may be suggestive of a high grade tumour which has

out grown its blood supply. However, the grading of breast cancer which
classically follows the Bloom -Richardson grading model will tend to favor
nuclear appearances (which include mitoses, coarse chromatin and
pleomorphism). Tubule formation is an important marker of the degree of
differentiation with formation of tubular structures being associated with well
differentiated tumours.
Tumour grading
Tumours may be graded according to their degree of differentiation, mitotic
activity and other features. Grade 1 tumours are the most differentiated and
grade 4 the least. The assessment is subjective, in most cases high grade
equates to poor prognosis, or at least rapid growth.
Tumours of glandular epithelium will tend to arrange themselves into acinar
type structures containing a central lumen. Well differentiated tumours may
show excellent acinar formation and poorly differentiated tumours simply
clumps of cells around a desmoplastic stroma. Sometimes tumours
demonstrate mucous production without evidence of acinar formation. Since
mucous production is evidence of a glandular function such tumours are often
termed mucinous adenocarcinoma.
Squamous cell tumours will typically produce structures resembling epithelial
cell components. Well differentiated tumours may also produce keratin
(depending upon tissue of origin). Which of the following is associated with poor wound healing?
A. Jaundice
B. Patients taking carbamazepine
C. General anaesthesia using thiopentone
D. General anaesthesia using ketamine
E. Multiple sclerosis
Mnemonic to remember factors
affecting wound healing: DID NOT HEAL
D iabetes
I nfection, irradiation
D rugs eg steroids, chemotherapy
N utritional deficiencies (vitamin A, C &

zinc, manganese), Neoplasia
O bject (foreign material)
T issue necrosis
H ypoxia
E xcess tension on wound
A nother wound
L ow temperature, Liver jaundice
Multiple sclerosis is associated with pressure sores, however the cellular healing process is
not affected.
Wound healing
Surgical wounds are either incisional or excisional and either clean, clean contaminated or
dirty. Although the stages of wound healing are broadly similar their contributions will vary
according to the wound type.
The main stages of wound healing include:
Haemostasis
Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot.
Inflammation
Neutrophils migrate into wound (function impaired in diabetes). Growth factors released, including basic fibroblast growth factor and vascular
endothelial growth factor. Fibroblasts replicate within the adjacent matrix and migrate into wound. Macrophages and fibroblasts couple matrix regeneration and clot substitution.
Regeneration
Platelet derived growth factor and transformation growth factors stimulate fibroblasts and epithelial cells.
Fibroblasts produce a collagen network. Angiogenesis occurs and wound resembles granulation tissue.
Remodeling
Longest phase of the healing process and may last up to one year (or longer).

During this phase fibroblasts become differentiated (myofibroblasts) and these facilitate wound contraction.
Collagen fibres are remodeled. Microvessels regress leaving a pale scar.
The above description represents an idealised scenario. A number of diseases may distort
this process. It is obvious that one of the key events is the establishing well vascularised
tissue. At a local level angiogenesis occurs, but if arterial inflow and venous return are
compromised then healing may be impaired, or simply nor occur at all. The results of
vascular compromise are all too evidence in those with peripheral vascular disease or those
poorly constructed bowel anastomoses.
Conditions such as jaundice will impair fibroblast synthetic function and overall immunity
with a detrimental effect in most parts of healing.
Problems with scars:
Hypertrophic scars
Excessive amounts of collagen within a scar. Nodules may be present histologically
containing randomly arranged fibrils within and parallel fibres on the surface. The tissue
itself is confined to the extent of the wound itself and is usually the result of a full thickness
dermal injury. They may go on to develop contractures.
Image of hypertrophic scarring. Note that it remains confined to the boundaries of the
original wound:
Image sourced from Wikipedia

Keloid scars
Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the
boundaries of the original injury. They do not contain nodules and may occur following even
trivial injury. They do not regress over time and may recur following removal.
Image of a keloid scar. Note the extension beyond the boundaries of the original incision:
Image sourced from Wikipedia
Drugs which impair wound healing:
Non steroidal anti inflammatory drugs Steroids Immunosupressive agents Anti neoplastic drugs
Closure
Delayed primary closure is the anatomically precise closure that is delayed for a few days but
before granulation tissue becomes macroscopically evident.
Secondary closure refers to either spontaneous closure or to surgical closure after
granulation tissue has formed.
A 55 year old man undergoes a colonoscopy and a colonic polyp is identified. It has a
lobular appearance and is located on a stalk in the sigmoid colon. Which of the
processes below best accounts for this disease?

A. Apoptosis
B. Metaplasia
C. Dysplasia
D. Calcification
E. Degeneration
Theme from April 2012 Exam
Most colonic polyps described above are adenomas. These may have associated
dysplasia. The more high grade the dysplasia the greater the level of clinical concern.
Colonic polyps
Colonic Polyps May occur in isolation of greater numbers as part of the polyposis syndromes. In FAP
greater than 100 polyps are typically present. The risk of malignancy in association
with adenomas is related to size and is the order of 10% in a 1cm adenoma. Isolated
adenomas seldom give risk of symptoms (unless large and distal). Distally sited
villous lesions may produce mucous and if very large electrolyte disturbances may
occur.
Follow up of colonic polyps
Low risk
1 or 2 adenomas <1cm. No follow up or re-colonoscopy at 5 years.
Moderate risk
3 or 4 small adenomas or 1 adenoma >1cm. Re-scope at 3 years.
High risk
>5 small adenomas or >3 with 1 of them >1cm. Re scope at 1 year.
From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify
patients appropriately and ensure that a complete colonoscopy with good views was
performed.
Segmental resection or complete colectomy should be considered when:
1. Incomplete excision of malignant polyp
2. Malignant sessile polyp

3. Malignant pedunculated polyp with submucosal invasion
4. Polyps with poorly differentiated carcinoma
5. Familial polyposis coli
-Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy
-Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy.
Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery.
56 year old lady has just undergone a colonoscopy and a lesion was identified in the
caecum. The histology report states that biopsies have been taken from a sessile
serrated polyp with traditional features? What is the best management option?
A. Perform a right hemicolectomy
B. List the patient for colonoscopic polypectomy
C. Discharge the patient
D. Re scope the patient in 6 months
E. Re scope the patient at 3 years
These polyps represent an alternative pathway to progression to carcinoma and may
be diagnostically confused with hyperplastic polyps. Hyperplastic polyps are more
common in the left colon and confer no increased risk. SSA's are more common in the
right colon and are usually larger. Those with "traditional features" on histology have
dysplasia with increased risk of malignant transformation.
Colonic polyps
Colonic Polyps May occur in isolation of greater numbers as part of the polyposis syndromes. In FAP
greater than 100 polyps are typically present. The risk of malignancy in association
with adenomas is related to size and is the order of 10% in a 1cm adenoma. Isolated
adenomas seldom give risk of symptoms (unless large and distal). Distally sited
villous lesions may produce mucous and if very large electrolyte disturbances may
occur.
Follow up of colonic polyps
Low risk
1 or 2 adenomas <1cm. No follow up or re-colonoscopy at 5 years.
Moderate risk
3 or 4 small adenomas or 1 adenoma >1cm. Re-scope at 3 years.

High risk
>5 small adenomas or >3 with 1 of them >1cm. Re scope at 1 year.
From Atkins and Saunders Gut 2002 51 (suppl V:V6-V9). It is important to stratify
patients appropriately and ensure that a complete colonoscopy with good views was
performed.
Segmental resection or complete colectomy should be considered when:
1. Incomplete excision of malignant polyp
2. Malignant sessile polyp
3. Malignant pedunculated polyp with submucosal invasion
4. Polyps with poorly differentiated carcinoma
5. Familial polyposis coli
-Screening from teenager up to 40 years by 2 yearly sigmoidoscopy/colonoscopy
-Panproctocolectomy and Ileostomy or Restorative Panproctocolectomy.
Rectal polypoidal lesions may be amenable to trans anal endoscopic microsurgery. A 30 year old male presents with gynaecomastia. Clinically he is noted to have a nodule in
the left testis. The most likely diagnosis is:
A. Oestrogen abuse
B. Seminoma with syncytiotrophoblast giant cells
C. Teratoma
D. Choriocarcinoma
E. Leydig cell tumour
Leydig cell tumours are rare testicular sex cord stromal tumours (which also include sertoli
cell tumours) which are associated with hormonal activity.
Patients with Leydig cell tumours may present with gynaecomastia before they notice testicular enlargement.
Majority are benign Histology: eosinophilic cells in columns

Testicular disorders
Testicular cancer
Testicular cancer is the most common malignancy in men aged 20-30 years. Around 95% of
cases of testicular cancer are germ-cell tumours. Germ cell tumours may essentially be
divided into:
Tumour type Key features Tumour markers Pathology
Seminoma Commonest subtype (50%)
Average age at diagnosis = 40
Even advanced disease associated with 5 year survival of 73%
AFP usually
normal
HCG elevated
in 10%
seminomas
Lactate
dehydrogenase;
elevated in 10-
20% seminomas
(but also in many
other conditions)
Sheet like lobular
patterns of cells
with substantial
fibrous
component.
Fibrous septa
contain
lymphocytic
inclusions and
granulomas may
be seen.
Non seminomatous germ cell
tumours (42%)
Teratoma Yolk sac tumour Choriocarcinoma Mixed germ cell
tumours (10%)
Younger age at
presentation =20-30
years
Advanced disease
carries worse prognosis
(48% at 5 years)
Retroperitoneal lymph
node dissection may be
needed for residual
disease after
chemotherapy
AFP elevated in
up to 70% of
cases
HCG elevated
in up to 40% of
cases
Other markers
rarely helpful
Heterogenous
texture with
occasional
ectopic tissue
such as hair
Image demonstrating a classical seminoma, these tumours are typically more uniform than
teratomas

Image sourced from Wikipedia
Risk factors for testicular cancer
Cryptorchidism Infertility Family history Klinefelter's syndrome Mumps orchitis
Features
A painless lump is the most common presenting symptom Pain may also be present in a minority of men

Other possible features include hydrocele, gynaecomastia
Diagnosis
Ultrasound is first-line CT scanning of the chest/ abdomen and pelvis is used for staging Tumour markers (see above) should be measured
Management
Orchidectomy (Inguinal approach) Chemotherapy and radiotherapy may be given depending on staging Abdominal lesions >1cm following chemotherapy may require retroperitoneal lymph
node dissection.
Prognosis is generally excellent
5 year survival for seminomas is around 95% if Stage I 5 year survival for teratomas is around 85% if Stage I
Benign disease
Epididymo-orchitis
Acute epididymitis is an acute inflammation of the epididymis, often involving the testis and
usually caused by bacterial infection.
Infection spreads from the urethra or bladder. In men <35 years, gonorrhoea or chlamydia are the usual infections.
Amiodarone is a recognised non infective cause of epididymitis, which resolves on stopping the drug.
Tenderness is usually confined to the epididymis, which may facilitate differentiating it from torsion where pain usually affects the entire testis.
Testicular torsion
Twist of the spermatic cord resulting in testicular ischaemia and necrosis. Most common in males aged between 10 and 30 (peak incidence 13-15 years) Pain is usually severe and of sudden onset. Cremasteric reflex is lost and elevation of the testis does not ease the pain. Treatment is with surgical exploration. If a torted testis is identified then both testis
should be fixed as the condition of bell clapper testis is often bilateral.
Which of the following features are not typical of Crohns disease?

A. Complex fistula in ano
B. Small bowel strictures
C. Skip lesions
D. 'Rose thorn ulcers' on barium studies
E. Pseudopolyps on colonoscopy
Pseudopolyps are a feature of ulcerative colitis and occur when there is severe
mucosal ulceration. The remaining islands of mucosa may then appear to be
isolated and almost polypoidal.
Crohns disease
Crohns disease is a chronic transmural inflammation of a segment(s) of the
gastrointestinal tract and may be associated with extra intestinal
manifestations. Frequent disease patterns observed include ileal, ileocolic and
colonic disease. Peri-anal disease may occur in association with any of these.
The disease is often discontinuous in its distribution. Inflammation may cause
ulceration, fissures, fistulas and fibrosis with stricturing. Histology reveals a
chronic inflammatory infiltrate that is usually patchy and transmural.
Ulcerative colitis Vs Crohns
Crohn's disease Ulcerative colitis
Distribution Mouth to anus Rectum and colon
Macroscopic
changes
Cobblestone appearance, apthoid
ulceration
Contact bleeding
Depth of
disease
Transmural inflammation Superficial inflammation
Distribution
pattern
Patchy Continuous
Histological
features
Granulomas (non caseating epithelioid
cell aggregates with Langhans' giant
cells)
Crypt abscesses,
Inflammatory cells in the
lamina propria
Extraintestinal manifestations of Crohns
Related to disease extent Unrelated to disease extent
Aphthous ulcers (10%) Sacroiliiitis (10-15%)
Erythema nodosum (5-10%) Ankylosing spondylitis (1-2%)
Pyoderma gangrenosum (0.5%) Primary sclerosing cholangitis (Rare)
Acute arthropathy (6-12%) Gallstones (up to 30%)
Ocular complications (up to 10%) Renal calculi (up to 10%)

A 32 year old lady presents with a 1.5cm pigmented lesion on her back. The surgeon
is concerned that this may be a melanoma. What is the most appropriate course of
action?
A. 2mm punch biopsy from the centre of the lesion
B. 4mm punch biopsy from the centre of the lesion
C. Wide excision of the lesion with 3cm margins
D. Excisional biopsy of the lesion
E. Wide excision of the lesion with 1cm margins
Suspicious naevi should NOT be partially sampled as histological interpretation is
severely compromised. Complete excision is mandatory where lesions fulfil
diagnostic criteria. However, wide excision for margins may be deferred until
definitive histology is available.
Lesions that are suspicious for melanoma should be excised with complete margins.
Radical excision is not routinely undertaken for diagnostic purposes and therefore if
subsequent histopathological assessment determines that the lesion is a melanoma a
re-exicision of margins may be required. Incisional punch biopsies of potential
melanomas makes histological interpretation difficult and is best avoided.
Malignant melanoma
The main diagnostic features (major
criteria):
Change in size
Change in shape
Change in colour
Secondary features (minor
criteria)
Diameter >6mm
Inflammation
Oozing or bleeding
Altered sensation
Treatment
Suspicious lesions should undergo excision biopsy. The lesion should be
removed in completely as incision biopsy can make subsequent
histopathological assessment difficult.
Once the diagnosis is confirmed the pathology report should be reviewed to
determine whether further re-exicision of margins is required (see below):
Margins of excision-Related to Breslow thickness
Lesions 0-1mm thick 1cm

Lesions 1-2mm thick 1- 2cm (Depending upon site and pathological features)
Lesions 2-4mm thick 2-3 cm (Depending upon site and pathological features)
Lesions >4 mm thick 3cm
Marsden J et al Revised UK guidelines for management of Melanoma. Br J Dermatol
2010 163:238-256.
Further treatments such as sentinel lymph node mapping, isolated limb perfusion and
block dissection of regional lymph node groups should be selectively applied.
A 70 year old male presents with painless frank haematuria. Clinical examination is
unremarkable. Routine blood tests reveal a haemoglobin of 18g/dl but are otherwise
normal. What is the most likely underlying diagnosis?
A. Squamous cell carcinoma of the bladder
B. Adenocarcinoma of the prostate
C. Adenocarcinoma of the kidney
D. Wilms tumour
E. Transitional cell carcinoma of the renal pelvis
Theme from April 2012 Exam
Polycythaemia is a recognised feature of renal cell carcinoma. Wilms tumours most
commonly occur in children.
Haematuria
Causes of haematuria
Trauma Injury to renal tract
Renal trauma commonly due to blunt injury (others
penetrating injuries)
Ureter trauma rare: iatrogenic
Bladder trauma: due to RTA or pelvic fractures
Infection Remember TB
Malignancy Renal cell carcinoma (remember paraneoplastic
syndromes): painful or painless
Urothelial malignancies: 90% are transitional cell
carcinoma, can occur anywhere along the urinary tract.
Painless haematuria.
Squamous cell carcinoma and adenocarcinoma: rare
bladder tumours
Prostate cancer

Penile cancers: SCC
Renal disease Glomerulonephritis
Stones Microscopic haematuria common
Structural
abnormalities
Benign prostatic hyperplasia (BPH) causes haematuria
due to hypervascularity of the prostate gland
Cystic renal lesions e.g. polycystic kidney disease
Vascular malformations
Renal vein thrombosis due to renal cell carcinoma
Coagulopathy Causes bleeding of underlying lesions
Drugs Cause tubular necrosis or interstitial nephritis:
aminoglycosides, chemotherapy
Interstitial nephritis: penicillin, sulphonamides, and
NSAIDs
Anticoagulants
Benign Exercise
Gynaecological Endometriosis: flank pain, dysuria, and haematuria that
is cyclical
Iatrogenic Catheterisation
Radiotherapy; cystitis, severe haemorrhage, bladder
necrosis
Pseudohaematuria
References Http://bestpractice.bmj.com/best-practice/monograph/316/overview/aetiology.html
Theme: Thyroid neoplasms
A. Follicular carcinoma
B. Follicular adenoma
C. Papillary carcinoma
D. Papillary adenoma
E. Anaplastic carcinoma
F. Medullary carcinoma
Please select the most likely underlying diagnosis for the thyroid masses described.
Each option may be used once, more than once or not at all.
19. A 78 year old lady presents to the surgical clinic with symptoms of both
dysphagia and dyspnoea. On examination there is a large mass in the neck
that moves on swallowing. CT scanning of the neck shows a locally
infiltrative lesion arising from the thyroid and invading the strap muscles.
Anaplastic carcinoma
Marked local invasion is a feature of anaplastic carcinoma. These tumours are
more common in elderly females.
20. A 25 year old female presents with a lump in her neck. On examination she
has a discrete nodule in the right lobe of the thyroid. A fine needle aspirate
shows papillary cells. An adjacent nodule is also sampled which shows
similar well differentiated papillary cells.
Papillary carcinoma
Multifocal disease is a recognised feature of papillary lesions. Papillary
adenomas are not really recognised and most well differentiated lesions are
papillary carcinomas.
21. A 45 year old man presents with a fracture of his right humerus. On
examination there is a lytic lesion of the proximal humerus and a mass in the
neck, this moves on swallowing.
You answered Medullary carcinoma
The correct answer is Follicular carcinoma
Follicular carcinomas are a recognised source of bone metastasis. Up to 60%
will show vascular invasion histologically.
Thyroid neoplasms
Lesion Common features
Follicular
adenoma
Usually present as a solitary thyroid nodule
Malignancy can only be excluded on formal histological
assessment
Papillary
carcinoma
Usually contain a mixture of papillary and colloidal filled
follicles

Histologically tumour has papillary projections and pale empty
nuclei
Seldom encapsulated
Lymph node metastasis predominate
Haematogenous metastasis rare
Account for 60% of thyroid cancers
Follicular
carcinoma
May appear macroscopically encapsulated, microscopically
capsular invasion is seen. Without this finding the lesion is a
follicular adenoma.
Vascular invasion predominates
Multifocal disease rare
Account for 20% of all thyroid cancers
Anaplastic
carcinoma
Most common in elderly females
Local invasion is a common feature
Account for 10% of thyroid cancers
Treatment is by resection where possible, palliation may be
achieved through isthmusectomy and radiotherapy.
Chemotherapy is ineffective.
Medullary
carcinoma
Tumours of the parafollicular cells (C Cells)
C cells derived from neural crest and not thyroid tissue
Serum calcitonin levels often raised
Familial genetic disease accounts for up to 20% cases
Both lymphatic and haematogenous metastasis are recognised,
nodal disease is associated with a very poor prognosis.
Rate questi
Which of the following lesions is most closely associated with Barretts oesophagus?
A. Squamous cell carcinoma
B. Gastro intestinal stromal tumours
C. Carcinoid tumours
D. Leiomyosarcoma
E. Adenocarcinoma
Barretts oesphagus is most closely associated with adenocarcinoma, and it confers at
30 fold increased risk of developing the condition.

Oesophageal cancer
Incidence is increasing
In most cases in the Western world this increase is accounted for by a rise in
the number of cases of adenocarcinoma. In the UK adenocarcinomas account
for 65% of cases.
Barretts oesophagus is a major risk factor for most cases of oesophageal
adenocarcinoma.
In other regions of the world squamous cancer is more common and is linked
to smoking, alcohol intake, diets rich in nitrosamines and achalasia.
Surveillance of Barretts is important as it imparts a 30 fold increase in cancer
risk and if invasive malignancy is diagnosed early then survival may approach
85% at 5 years.
Diagnosis
Upper GI endoscopy is the first line test
Contrast swallow may be of benefit in classifying benign motility disorders
but has no place in the assessment of tumours
Staging is initially undertaken with CT scanning of the chest, abdomen and
pelvis. If overt metastatic disease is identified using this modality then further
complex imaging is unnecessary
If CT does not show metastatic disease, then local stage may be more
accurately assessed by use of endoscopic ultrasound.
Staging laparoscopy is performed to detect occult peritoneal disease. PET CT
is performed in those with negative laparoscopy. Thoracoscopy is not
routinely performed.
Treatment Operable disease is best managed by surgical resection. The most standard procedure
is an Ivor- Lewis type oesophagectomy. This procedure involves the mobilisation of
the stomach and division of the oesophageal hiatus. The abdomen is closed and a right
sided thoracotomy performed. The stomach is brought into the chest and the
oesophagus mobilised further. An intrathoracic oesophagogastric anastomosis is
constructed. Alternative surgical strategies include a transhiatal resection (for distal
lesions), a left thoraco-abdominal resection (difficult access due to thoracic aorta) and
a total oesophagectomy (McKeown) with a cervical oesophagogastric anastomosis.
The biggest surgical challenge is that of anastomotic leak, with an intrathoracic
anastomosis this will result in mediastinitis. With high mortality. The McKeown
technique has an intrinsically lower systemic insult in the event of anastmotic leakage.
In addition to surgical resection many patients will be treated with adjuvent
chemotherapy.
A 56 year old man presents with epigastric discomfort and episodes of migratory
thrombophlebitis. On examination he is mildly jaundiced. A CT scan shows peri hilar
lymphadenopathy and a mass in the pancreatic head. Which of the following is the
most likely underlying diagnosis?

A. Squamous cell carcinoma of the pancreas
B. Adenocarcinoma of the pancreas
C. Insulinoma
D. Glucagonoma
E. Gastrinoma
Adenocarcinoma of the pancreas is the most likely diagnosis and migratory
thrombophlebitis is associated with the condition. Squamous cells carcinoma is
extremely uncommon in the pancreas. Gastrinoma are extremely rare and thus not the
most likely diagnosis.
Pancreatic cancer
Adenocarcinoma
Risk factors: Smoking, diabetes, Adenoma, Familial adenomatous polyposis
Mainly occur in the head of the pancreas (70%)
Spread locally and metastasizes to the liver
Carcinoma of the pancreas should be differentiated from other periampullary
tumours with better prognosis
Clinical features
Weight loss
Painless jaundice
Epigastric discomfort (pain usually due to invasion of the coeliac plexus is a
late feature)
Pancreatitis
Trousseau's sign: migratory superficial thrombophlebitis
Investigations
USS: May miss small lesions
CT Scanning (pancreatic protocol). If unresectable on CT then no further
staging needed.
PET/CT for those with operable disease on CT alone
ERCP/ MRI for bile duct assessment.
Staging laparoscopy to exclude peritoneal disease.
Management

Head of pancreas: Whipple's resection (SE dumping and ulcers). Newer
techniques include pylorus preservation and SMA/ SMV resection.
Carcinoma body and tail: poor prognosis, distal pancreatectomy if operable.
Usually adjuvent chemotherapy for resectable disease
ERCP and stent for jaundice and palliation.
Surgical bypass may be needed for duodenal obstruction.
A 22 year old man presents with symptoms of headache, lethargy and confusion. On
examination he is febrile and has a right sided weakness. A CT scan shows a ring
enhancing lesion affecting the left motor cortex. Which of the following is the most
likely diagnosis?
A. Arteriovenous malformation
B. Cerebral abscess
C. Herpes simplex encephalitis
D. Metastatic renal adenocarcinoma
E. Glioblastoma multiforme
The combination of rapidly progressive neurology, fever and headache is highly
suggestive of cerebral abscess. CT scanning will show a ring enhancing lesion
because the intravenous contrast cannot penetrate the centre of the abscess cavity.
HSV encephalitis does not produce ring enhancing lesions.
Brain abscess
CNS abscesses may result from a number of causes including, extension of
sepsis from middle ear or sinuses, trauma or surgery to the scalp, penetrating
head injuries and embolic events from endocarditis.
The presenting symptoms will depend upon the site of the abscess (those in
critical areas e.g.motor cortex) will present earlier. Abscesses have a
considerable mass effect in the brain and raised intra cranial pressure is
common.
Although fever, headache and focal neurology are highly suggestive of a brain
abscess the absence of one or more of these does not exclude the diagnosis,
fever may be absent and even if present, is usually not the swinging pyrexia
seen with abscesses at other sites.
Assessment of the patient includes imaging with CT scanning.
Treatment is usually surgical, a craniotomy is performed and the abscess
cavity debrided. The abscess may reform because the head is closed following
abscess drainage.

A 56 year old man from Egypt has suffered from recurrent attacks of haematuria for
many years. He presents with suprapubic discomfort and at cystoscopy is found to
have a mass lesion within the bladder. What is the most likely diagnosis?
A. Squamous cell carcinoma
B. Transitional cell papilloma
C. Adenocarcinoma
D. Leiomyosarcoma
E. Rhabdomyosarcoma
In Egypt Schistosomiasis is more common than in the UK and may cause recurrent
episodes of haematuria. In those affected with the condition who develop a bladder
neoplasm, an SCC is the most common type.
Bladder cancer
Bladder cancer is the second most common urological cancer. It most commonly
affects males aged between 50 and 80 years of age. Those who are current, or
previous (within 20 years), smokers have a 2-5 fold increased risk of the disease.
Occupational exposure to hydrocarbons such as alanine increases the risk. Although
rare in the UK, chronic bladder inflammation arising from Schistosomiasis infection
remains a common cause of squamous cell carcinomas, in those countries where the
disease is endemic.
Benign tumours Benign tumours of the bladder including inverted urothelial papilloma and
nephrogenic adenoma are uncommon.
Bladder malignancies
Transitional cell carcinoma (>90% of cases)
Squamous cell carcinoma ( 1-7% -except in regions affected by
schistosomiasis)
Adenocarcinoma (2%)
Transitional cell carcinomas may arise as solitary lesions, or may be multifocal,
owing to the effect of "field change" within the urothelium. Up to 70% of TCC's will
have a papillary growth pattern. These tumours are usually superficial in location and
accordingly have a better prognosis. The remaining tumours show either mixed
papillary and solid growth or pure solid growths. These tumours are typically more
prone to local invasion and may be of higher grade, the prognosis is therefore worse.
Those with T3 disease or worse have a 30% (or higher) risk of regional or distant

lymph node metastasis.
TNM Staging
Stage Description
T0 No evidence of tumour
Ta Non invasive papillary carcinoma
T1 Tumour invades sub epithelial connective tissue
T2a Inner half of detrusor invaded
T2b Outer half of detrusor invaded
T3 Tumour extends to perivesical fat
T4a Invasion of uterus, prostate or bowel
T4b Invasion of other abdominal organs
N0 No nodal disease
N1 Single lymph node metastasis (up to 2cm)
N2 Single node >2cm or multiple nodes up to 5cm
N3 Nodes over 5cm
M1 Distant disease
Presentation Most patients (85%) will present with painless, macroscopic haematuria. In those
patients with incidental microscopic haematuria, up to 10% of females aged over 50
will be found to have a malignancy (once infection excluded).
Staging Most will undergo a cystoscopy and biopsies or TURBT, this provides histological
diagnosis and information relating to depth of invasion. Locoregional spread is best
determined using pelvic MRI and distant disease CT scanning. Nodes of uncertain
significance may be investigated using PET CT.
Treatment Those with superficial lesions may be managed using TURBT in isolation. Those
with recurrences or higher grade/ risk on histology may be offered intravesical
chemotherapy. Those with T2 disease are usually offered either surgery (radical
cystectomy and ileal conduit) or radical radiotherapy.
Prognosis
T1 90%
T2 60%
T3 35%
T4a 10-25%
Any T, N1-N2 30%
A newborn infant is noted to have a unilateral cleft lip only. What is the most likely
explanation for this process?

A. Incomplete fusion of the second branchial arch
B. Incomplete fusion of the nasolabial muscle rings
C. Incomplete fusion of the first branchial arch
D. Incomplete fusion of the third branchial arch
E. Incomplete fusion of the secondary palate
Theme from April 2012 Exam
Unilateral isolated cleft lip represents a failure of nasolabial ring fusion. It is not
related to branchial arch fusion. Arch disorders have a far more profound phenotype
and malformation sequences.
Cleft lip and palate
Cleft lip and palate are the most common congenital deformity affecting the orofacial
structures. Whilst they may be an isolated developmental malformation they are also a
recognised component of more than 200 birth defects. The incidence is as high as 1 in
600 live births. The commonest variants are:
Isolated cleft lip (15%)
Isolated cleft palate (40%)
Combined cleft lip and palate (45%)
The aetiology of the disorder is multifactorial; both genetic (affected first degree
relative increases risk) and environmental factors play a role.
Cleft lip Cleft lip occurs as a result of disruption of the muscles of the upper lip and nasolabial
region. These muscles comprise a chain of muscles viz; nasolabial, bilabial and
labiomental. Defects may be unilateral or bilateral.
Cleft palate The primary palate consists of all anatomical structures anterior to the incisive
foramen. The seconday palate lies more posteriorly and is sub divided into the hard
and soft palate. Cleft palate occurs as a result of non fusion of the two palatine
shelves. Both hard and soft palate may be involved. Complete cases are associated
with complete separation of the nasal septum and vomer from the palatine processes.
Treatment Surgical reconstruction is the mainstay of management. The procedures are planned
according to the extent of malformation and child age. Simple defects are managed as
a single procedure. Complex malformations are usually corrected in stages. Affected
individuals have a higher incidence of hearing and speech problems.

A 72 year old woman with back pain and chronic renal failure has the following
results:
Reference range
Ca2+ 2.03 2.15-2.55 mmol/l
Parathyroid hormone 10.4 1-6.5 pmol/l
Phosphate 0.80 0.6-1.25 mmol/l
What is the most likely diagnosis?
A. Hypoparathyroidism
B. Primary hyperparathyroidism
C. Secondary hyperparathyroidism
D. Tertiary hyperparathyroidism
E. Pseudohypoparathyroidism
In relation to secondary hyperparathyroidism; there is a HIGH PTH and the Ca2+ is
NORMAL or LOW. In secondary hyperparathyroidism there in hyperplasia of the
parathyroid glands in response to chronic hypocalcaemia (or hyperphosphataemia)
and is a normal physiological response. Calcium is restored from bone, kidneys and
the gastrointestinal system.
Parathyroid glands and disorders of calcium metabolism
Hyperparathyroidism
Disease type Hormone profile Clinical features Cause
Primary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Elevated)
Phosphate
(Low)
Serum Calcium
: Creatinine
clearance ratio
> 0.01
May be
asymptomatic if
mild
Recurrent
abdominal pain
(pancreatitis, renal
colic)
Changes to
emotional or
cognitive state
Most cases due to
solitary adenoma
(80%), multifocal
disease occurs in
10-15% and
parathyroid
carcinoma in 1% or
less
Secondary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Low or
normal)
Phosphate
(Elevated)
Vitamin D
May have few
symptoms
Eventually may
develop bone
disease, osteitis
fibrosa cystica and
Parathyroid gland
hyperplasia occurs
as a result of low
calcium, almost
always in a setting
of chronic renal

levels (Low) soft tissue
calcifications
failure
Tertiary
hyperparathyroidism
Ca2+ (Normal
or high)
PTH (Elevated)
Phosphate
levels
(Decreased or
Normal)
Vitamin D
(Normal or
decreased)
Alkaline
phosphatase
(Elevated)
Metastatic
calcification
Bone pain and /
or fracture
Nephrolithiasis
Pancreatitis
Occurs as a result
of ongoing
hyperplasia of the
parathyroid glands
after correction of
underlying renal
disorder,
hyperplasia of all 4
glands is usually
the cause
Differential diagnoses It is important to consider the rare but relatively benign condition of benign familial
hypocalciuric hypercalcaemia, caused by an autosomal dominant genetic disorder.
Diagnosis is usually made by genetic testing and concordant biochemistry (Serum
Calcium : Creatinine clearance ratio <0.01-distinguished from primary
hyperparathyroidism).
Treatment
Primary hyperparathyroidism
Indications for surgery
Elevated serum Calcium > 1mg/dL above normal
Hypercalciuria > 400mg/day
Creatinine clearance < 30% compared with normal
Episode of life threatening hypercalcaemia
Nephrolithiasis
Age < 50 years
Neuromuscular symptoms
Reduction in bone mineral density of the femoral neck, lumbar spine, or distal
radius of more than 2.5 standard deviations below peak bone mass (T score
lower than -2.5)
Secondary hyperparathyroidism Usually managed with medical therapy.
Indications for surgery in secondary (renal) hyperparathyroidism:
Bone pain
Persistent pruritus
Soft tissue calcifications

Tertiary hyperparathyroidism Usually treatment is surgical
The presence of an autonomously functioning parathyroid gland may require surgery.
If the culprit gland can be identified then it should be excised. Otherwise total
parathyroidectomy and re-implantation of part of the gland may be required.
References 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical
Management. Surg Clin North Am 2009 Oct;89(5):1227-39.
2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J
Endocrinol 2011; 2011: 251410.
A 72 year old woman with back pain and chronic renal failure has the following
results:
Reference range
Ca2+ 2.03 2.15-2.55 mmol/l
Parathyroid hormone 10.4 1-6.5 pmol/l
Phosphate 0.80 0.6-1.25 mmol/l
What is the most likely diagnosis?
A. Hypoparathyroidism
B. Primary hyperparathyroidism
C. Secondary hyperparathyroidism
D. Tertiary hyperparathyroidism
E. Pseudohypoparathyroidism
In relation to secondary hyperparathyroidism; there is a HIGH PTH and the Ca2+ is
NORMAL or LOW. In secondary hyperparathyroidism there in hyperplasia of the
parathyroid glands in response to chronic hypocalcaemia (or hyperphosphataemia)
and is a normal physiological response. Calcium is restored from bone, kidneys and
the gastrointestinal system.
Parathyroid glands and disorders of calcium metabolism
Hyperparathyroidism
Disease type Hormone profile Clinical features Cause
Primary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Elevated)
Phosphate
May be
asymptomatic if
mild
Most cases due to
solitary adenoma
(80%), multifocal

(Low)
Serum Calcium
: Creatinine
clearance ratio
> 0.01
Recurrent
abdominal pain
(pancreatitis, renal
colic)
Changes to
emotional or
cognitive state
disease occurs in
10-15% and
parathyroid
carcinoma in 1% or
less
Secondary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Low or
normal)
Phosphate
(Elevated)
Vitamin D
levels (Low)
May have few
symptoms
Eventually may
develop bone
disease, osteitis
fibrosa cystica and
soft tissue
calcifications
Parathyroid gland
hyperplasia occurs
as a result of low
calcium, almost
always in a setting
of chronic renal
failure
Tertiary
hyperparathyroidism
Ca2+ (Normal
or high)
PTH (Elevated)
Phosphate
levels
(Decreased or
Normal)
Vitamin D
(Normal or
decreased)
Alkaline
phosphatase
(Elevated)
Metastatic
calcification
Bone pain and /
or fracture
Nephrolithiasis
Pancreatitis
Occurs as a result
of ongoing
hyperplasia of the
parathyroid glands
after correction of
underlying renal
disorder,
hyperplasia of all 4
glands is usually
the cause
Differential diagnoses It is important to consider the rare but relatively benign condition of benign familial
hypocalciuric hypercalcaemia, caused by an autosomal dominant genetic disorder.
Diagnosis is usually made by genetic testing and concordant biochemistry (Serum
Calcium : Creatinine clearance ratio <0.01-distinguished from primary
hyperparathyroidism).
Treatment
Primary hyperparathyroidism
Indications for surgery
Elevated serum Calcium > 1mg/dL above normal
Hypercalciuria > 400mg/day
Creatinine clearance < 30% compared with normal
Episode of life threatening hypercalcaemia
Nephrolithiasis
Age < 50 years
Neuromuscular symptoms

Reduction in bone mineral density of the femoral neck, lumbar spine, or distal
radius of more than 2.5 standard deviations below peak bone mass (T score
lower than -2.5)
Secondary hyperparathyroidism Usually managed with medical therapy.
Indications for surgery in secondary (renal) hyperparathyroidism:
Bone pain
Persistent pruritus
Soft tissue calcifications
Tertiary hyperparathyroidism Usually treatment is surgical
The presence of an autonomously functioning parathyroid gland may require surgery.
If the culprit gland can be identified then it should be excised. Otherwise total
parathyroidectomy and re-implantation of part of the gland may be required.
References 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical
Management. Surg Clin North Am 2009 Oct;89(5):1227-39.
2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J
Endocrinol 2011; 2011: 251410. Theme: Pharyngitis
A. Infectious mononucleosis
B. Acute bacterial tonsillitis
C. Quinsy
D. Lymphoma
E. Diptheria
Please select the most likely underlying cause for the following patients presenting with
pharyngitis. Each option may be used once, more than once or not at all.
2. An 8 year old child presents with enlarged tonsils that meet in the midline and are
covered with a white film that bleeds when you attempt to remove it. He is pyrexial
but otherwise well.

Acute bacterial tonsillitis
Theme from April 2012 Exam
In acute tonsillitis the tonsils will often meet in the midline and may be covered with
a membrane. Individuals who are systemically well are unlikely to have diptheria.
3. A 10 year old child presents with enlarged tonsils that meet in the midline.
Oropharyngeal examination confirms this finding and you also notice peticheal
haemorrhages affecting the oropharynx. On systemic examination he is noted to
have splenomegaly.
Infectious mononucleosis
A combination of pharyngitis and tonsillitis is often seen in glandular fever.
Antibiotics containing penicillin may produce a rash when given in this situation,
leading to a mistaken label of allergy.
4. A 19 year old man has had a sore throat for the past 5 days. Over the past 24 hours
he has notices increasing and severe throbbing pain in the region of his right tonsil.
He is pyrexial and on examination he is noted to have a swelling of this area.
Quinsy
Unilateral swelling and fever is usually indicative of quinsy. Surgical drainage usually
produces prompt resolution of symptoms.
Acute tonsillitis
Characterised by pharyngitis, fever, malaise and lymphadenopathy. Over half of all cases are bacterial with Streptococcus pyogenes the most common
organism The tonsils are typically oedematous and yellow or white pustules may be present Infectious mononucleosis may mimic the condition. Treatment with penicillin type antibiotics is indicated for bacterial tonsillitis. Bacterial tonsillitis may result in local abscess formation (quinsy)

Acute streptococcal tonsillitis
Image sourced from Wikipedia
A 4 year old boy is brought to the clinic by his mother who has noticed a small lesion
at the external angle of his eye. On examination there is a small cystic structure which
has obviously been recently infected. On removal of the scab, there is hair visible
within the lesion. What is the most likely diagnosis?
A. Dermoid cyst
B. Desmoid cyst
C. Sebaceous cyst
D. Epidermoid cyst
E. Keratoacanthoma
Dermoid cysts occur at sites of embryonic fusion and may contain multiple cell types.
They occur most often in children.

The lesion is unlikely to be a desmoid cyst as these are seldom located either at this
site or in this age group. In addition they do not contain hair. Sebaceous cysts will
usually have a punctum and contain a cheesy material. Epidermoid cysts contain
keratin plugs.
Dermoid cysts
A cutaneous dermoid cyst may develop at sites of embryonic developmental fusion.
They are most common in the midline of the neck, external angle of the eye and
posterior to the pinna of the ear. They typically have multiple inclusions such as hair
follicles that bud out from its walls. They may develop at other sites such as the ovary
and in these sites are synonymous with teratomas.
A desmoid tumour is a completely different entity and may be classified either as low
grade fibrosarcomas or non aggressive fibrous tumours. They commonly present as
large infiltrative masses. They may be divided into abdominal, extra abdominal and
intra abdominal. All types share the same biological features. Extra abdominal
desmoids have an equal sex distribution and primarily arise in the musculature of the
shoulder, chest wall, back and thigh. Abdominal desmoids usually arise in the
musculoaponeurotic structures of the abdominal wall. Intra abdominal desmoids tend
to occur in the mesentery or pelvic side walls and occur most frequently in patients
with familial adenomatous polyposis coli syndrome.
Which of the following tumours are most likely to give rise to para-aortic nodal
metastasis early?
A. Ovarian
B. Bladder
C. Rectal
D. Caecal
E. Cervical
Theme from 2009 Exam
Ovarian tumours are supplied by the ovarian vessels, these branch directly from the
aorta. The cervix drains to the internal and external iliac nodes.
Para-aortic lymphadenopathy
Organ sites that may metastasise (early) to the para-aortic lymph nodes:
Testis
Ovary
Uterine fundus

Many other organs may result in para-aortic nodal disease. However, these deposits
will represent a much later stage of the disease, since other nodal stations are involved
earlier.
Which of the following statements relating to malignant mesothelioma is false?
A. It may be treated by extrapleural pneumonectomy.
B. It is linked to asbestos exposure.
C. It is linked to cigarette smoking independent of asbestos exposure.
D. It may occur intra abdominally.
E. It is relatively resistant to radiotherapy
It is not linked to cigarette smoking. When identified at an early stage a radical
resection is the favored option. Radiotherapy is often given perioperatively. However,
it is not a particularly radiosensitive tumour. Combination chemotherapy gives some
of the best results and most regimes are cisplatin based.
Occupational cancers
Occupational cancers accounted for 5.3% cancer deaths in 2005.
In men the main cancers include:
Mesothelioma
Bladder cancer
Non melanoma skin cancer
Lung cancer
Sino nasal cancer
Occupations with high levels of occupational tumours include:
Construction industry
Working with coal tar and pitch
Mining
Metalworkers
Working with asbestos (accounts for 98% of all mesotheliomas)
Working in rubber industry
Shift work has been linked to breast cancer in women (Health and safety executive
report RR595).
The latency between exposure and disease is typically 15 years for solid tumours and
20 for leukaemia.

Many occupational cancers are otherwise rare. For example sino nasal cancer is an
uncommon tumour, 50% will be SCC. They are linked to conditions such as wood
dust exposure and unlike lung cancer is not strongly linked to cigarette smoking.
Another typical occupational tumour is angiosarcoma of the liver which is linked to
working with vinyl chloride. Again in the non occupational context this is an
extremely rare sporadic tumour.
Theme: Thyroid disorders
A. Sick euthyroid
B. Hyperthyroidism
C. Hypothyroidism
D. Normal euthyroid
E. Anxiety state
F. Factitious hyperthyroidism
For each of the scenarios please match the scenario with the most likely underlying
diagnosis. Each answer may be used once, more than once or not at all.
8. A 33 year old man is recovering following a protracted stay on the intensive
care unit recovering from an anastomotic leak following a difficult Trans
hiatal oesophagectomy. His progress is slow, and the intensive care doctors
receive the following thyroid function test results:
TSH 1.0 u/L
Free T4 8
T3 1.0 (1.2-3.1 normal)
You answered Normal euthyroid
The correct answer is Sick euthyroid
Theme from April 2012 Exam
Sick euthyroid syndrome is caused by systemic illness. With this, the patient
may have an apparently low total and free T4 and T3, with a normal or low
TSH. Note that the levels are only mildly below normal.
9. A 28 year old female presents to the general practitioner with symptoms of
fever and diarrhoea. As part of her diagnostic evaluation the following
thyroid function tests are obtained:
TSH < 0.01
Free T4 30

T3 4.0
Hyperthyroidism
The symptoms are suggestive of hyperthyroidism. This is supported by the
abnormal blood results; suppressed TSH with an elevated T3 and T4.
10. A 19 year old lady presents with palpitations. The medical officer takes a
blood sample for thyroid function tests. The following results are obtained:
TSH > 6.0
Free T4 20
T3 2.0
Hypothyroidism
An elevated TSH with normal T4 indicates partial thyroid failure. This is
caused by Hashimotos, drugs (lithium, antithyroids) and dyshormogenesis.
Hyperthyroidism
Causes of hyperthyroidism include:
Diffuse toxic goitre (Graves Disease)
Toxic nodular goitre
Toxic nodule
Rare causes
Graves disease Graves disease is characterised by a diffuse vascular goitre that appears at the same
time as the clinical manifestations of hyperthyroidism. It is commonest in younger
females and may be associated with eye signs. Thyrotoxic symptoms will
predominate. Up to 50% of patients will have a familial history of autoimmune
disorders. The glandular hypertrophy and hyperplasia occur as a result of the thyroid
stimulating effects of the TSH receptor antibodies.
Toxic nodular goitre In this disorder the goitre is present for a long period of time prior to the development
of clinical symptoms. In most goitres the nodules are inactive and in some cases it is

the internodular tissue that is responsible for the goitre.
Toxic nodule Overactive, autonomously functioning nodule. It may occur as part of generalised
nodularity or be a true toxic adenoma. The TSH levels are usually low as the
autonomously functioning thyroid tissue will exert a negative feedback effect.
Signs and symptoms
Symptoms Signs
Lethargy Tachycardia
Emotionally labile Agitation
Heat intolerance Hot, moist palms
Weight loss Exopthalmos
Excessive appetite Thyroid goitre and bruit
Palpitations Lid lag/retraction
Diagnosis The most sensitive test for diagnosing hyperthyroidism is plasma T3 (which is raised).
Note in hypothyroidism the plasma T4 and TSH are the most sensitive tests. A TSH
level of <0.5U/L suggests hyperthyroidism. TSH receptor antibodies may be tested
for in the diagnosis of Graves.
Treatment First line treatment for Graves disease is usually medical and the block and replace
regime is the favored option. Carbimazole is administered at higher doses and
thyroxine is administered orally. Patient are maintained on this regime for between 6
and 12 months. Attempts are then made to wean off medication. Where relapse then
occurs the options are between ongoing medical therapy, radioiodine or surgery.
Which of the following conditions is least likely to exhibit the Koebner phenomenon?
A. Vitiligo
B. Molluscum contagiosum
C. Lichen planus
D. Psoriasis
E. Lupus vulgaris
Lupus vulgaris is not associated with the Koebner phenomenon.
Koebner phenomenon
The Koebner phenomenon describes skin lesions which appear at the site of injury. It
is seen in:

Psoriasis
Vitiligo
Warts
Lichen planus
Lichen sclerosus
Molluscum contagiosum
Which of the tumour types listed below is found most frequently in a person
with aggressive fibromatosis?
A. Medullary thyroid cancer
B. Basal cell carcinoma of the skin
C. Desmoid tumours
D. Dermoid tumours
E. Malignant melanoma
Aggressive fibromatosis
Aggressive fibromatosis is a disorder consisting of desmoid tumours, which
behave in a locally aggressive manner. Desmoid tumours may be identified in
both abdominal and extra-abdominal locations. Metastatic disease is rare. The
main risk factor (for abdominal desmoids) is having APC variant of familial
adenomatous polyposis coli. Most cases are sporadic.
Treatment is by surgical excision.
A 20 year old man is suspected of having an inflamed Meckels diverticulum. At
which of the following locations is it most likely to be found?
A. Approximately 60 cm distal to the ileo-caecal valve
B. Approximately 60 cm proximal to the ileocaecal valve
C. Approximately 200cm distal to the ileocaecal valve
D. Approximately 200cm proximal to the ileocaecal valve
E. 50cm distal to the DJ flexure
Rule of 2's
2% of population
2 inches (5cm) long

2 feet (60 cm) from the
ileocaecal valve
2 x's more common in men
2 tissue types involved
They are typically found 2 feet proximal to the ileocaecal valve (or approximately
60cm).
Meckel's diverticulum
Congenital abnormality resulting in incomplete obliteration of the vitello-
intestinal duct
Normally, in the foetus, there is an attachment between the vitello-intestinal
duct and the yolk sac.This disappears at 6 weeks gestation.
The tip is free in majority of cases.
Associated with enterocystomas, umbilical sinuses, and omphaloileal fistulas.
Arterial supply: omphalomesenteric artery.
2% of population, 2 inches long, 2 feet from the ileocaecal valve.
Typically lined by ileal mucosa but ectopic gastric mucosa can occur, with the
risk of peptic ulceration. Pancreatic and jejunal mucosa can also occur.
Clinical
Normally asymptomatic and an incidental finding.
Complications are the result of obstruction, ectopic tissue, or inflammation.
Removal if narrow neck or symptomatic. Options are between wedge excision
or formal small bowel resection and anastomosis.
A 43 year old lady presents with severe chest pain. Investigations demonstrate a
dissecting aneurysm of the ascending aorta which originates at the aortic valve. What
is the optimal long term treatment?
A. Endovascular stent
B. Medical therapy with beta blockers
C. Medical therapy with ACE inhibitors
D. Sutured aortic repair
E. Aortic root replacement
Proximal aortic dissections are generally managed with surgical aortic root
replacement. The proximal origin of the dissection together with chest pain (which
may occur in all types of aortic dissection) raises concerns about the possibility of

coronary ostial involvement (which precludes stenting). There is no role for attempted
suture repair in this situation.
Aortic dissection
More common than rupture of the abdominal aorta
33% of patients die within the first 24 hours, and 50% die within 48 hours if
no treatment received
Associated with hypertension
Features of aortic dissection: tear in the intimal layer, followed by formation
and propagation of a subintimal hematoma. Cystic medial necrosis (Marfan's)
Most common site of dissection: 90% occurring within 10 centimetres of the
aortic valve
Stanford Classification
Type Location Treatment
A Ascending aorta/ aortic root Surgery- aortic root replacement
B Descending aorta Medical therapy with antihypertensives
DeBakey classification
Type Site affected
I Ascending aorta, aortic arch, descending aorta
II Ascending aorta only
III Descending aorta distal to left subclavian artery
Clinical features
Tearing, sudden onset chest pain (painless 10%)
Hypertension or Hypotension
A blood pressure difference greater than 20 mm Hg
Neurologic deficits (20%)
Investigations
CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation
trachea/oesophagus
CT (spiral)
MRI
Angiography (95% of patients diagnosed)
Management
Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg.

Urgent surgical intervention: type A dissections. This will usually involve
aortic root replacement.
A 45 year old lady presents with a pathological fracture of her femoral shaft. She is a
poor historian, but it transpires that she underwent a thyroidectomy 1 year previously.
She has no other illness or co-morbidities. What is the most likely underlying
diagnosis?
A. Hyperparathyroidism
B. Metastatic papillary carcinoma of the thyroid
C. Metastatic medullary carcinoma of the thyroid
D. Metastatic follicular carcinoma of the thyroid
E. None of the above
Follicular carcinomas are a recognised cause of bone metastasis. Papillary lesions
typically spread via the lymphatics.
Thyroid malignancy
Papillary carcinoma
Commonest sub-type
Accurately diagnosed on fine needle aspiration cytology
Histologically they may demonstrate psammoma bodies (areas of
calcification) and so called 'orphan Annie' nuclei
They typically metastasise via the lymphatics and thus laterally located
apparently ectopic thyroid tissue is usually a metastasis from a well
differentiated papillary carcinoma.
Follicular carcinoma
Are less common than papillary lesions
Like papillary tumours they may present as a discrete nodule. Although they
appear to be well encapsulated macroscopically there invasion on microscopic
evaluation.
Lymph node metastases are uncommon and these tumours tend to spread
haematogenously. This translates into a higher mortality rate.
Follicular lesions cannot be accurately diagnosed on fine needle aspiration
cytology and thus all follicular FNA's will require at least a hemi
thyroidectomy.

Anaplastic carcinoma
Less common and tend to occur in elderly females
Disease is usually advanced at presentation and often only palliative
decompression and radiotherapy can be offered.
Medullary carcinoma
These are tumours of the parafollicular cells ( C Cells) and are of neural crest
origin.
The serum calcitonin may be elevated which is of use when monitoring for
recurrence.
They may be familial and occur as part of the MEN -2A disease spectrum.
Spread may be either lymphatic or haematogenous and as these tumours are
not derived primarily from thyroid cells they are not responsive to radioiodine.
Lymphoma
These respond well to radiotherapy
Radical surgery is unnecessary once the disease has been diagnosed on biopsy
material. Such biopsy material is not generated by an FNA and thus a core
biopsy has to be obtained (with care!).
Theme: Cardiac murmurs
A. Pulmonary stenosis
B. Mitral regurgitation
C. Tricuspid regurgitation
D. Aortic stenosis
E. Mitral stenosis
F. Aortic sclerosis
What is the most likely cause of the cardiac murmur in the following patients? Each
option may be used once, more than once or not at all.
16. A 35 year old Singaporean female attends a varicose vein pre operative clinic.
On auscultation a mid diastolic murmur is noted at the apex. The murmur is
enhanced when the patient lies in the left lateral position.
Mitral stenosis
Theme from September 2011 exam

A mid diastolic murmur at the apex is a classical description of a mitral
stenosis murmur. The most common cause is rheumatic heart disease.
Complications of mitral stenosis include atrial fibrillation, stroke, myocardial
infarction and infective endocarditis.
17. A 22 year old intravenous drug user is found to have a femoral abscess. The
nursing staff contact the on call doctor as the patient has a temperature of
39oC. He is found to have a pan systolic murmur loudest at the left sternal
edge at the 4th intercostal space.
You answered Mitral regurgitation
The correct answer is Tricuspid regurgitation
Intravenous drug users are at high risk of right sided cardiac valvular
endocarditis. The character of the murmur fits with a diagnosis of tricuspid
valve endocarditis.
18. An 83 year old woman is admitted with a left intertrochanteric neck of femur
fracture. On examination the patient is found to have an ejection systolic
murmur loudest in the aortic region. There is no radiation of the murmur to
the carotid arteries. Her ECG is normal.
You answered Aortic stenosis
The correct answer is Aortic sclerosis
The most likely diagnosis is aortic sclerosis. The main differential diagnosis
is of aortic stenosis, however as there is no radiation of the murmur to the
carotids and the ECG is normal, this is less likely.
Cardiac murmurs
Type of Murmur Conditions
Ejection systolic Aortic stenosis
Pulmonary stenosis, HOCM
ASD, Fallot's
Pan-systolic Mitral regurgitation
Tricuspid regurgitation
VSD
Late systolic Mitral valve prolapse

Coarctation of aorta
Early diastolic Aortic regurgitation
Graham-Steel murmur (pulmonary regurgitation)
Mid diastolic Mitral stenosis
Austin-Flint murmur (severe aortic regurgitation)
A 55 year old lady presents with discomfort in the right breast. On clinical
examination a small lesion is identified and clinical appearances suggest
fibroadenoma. Imaging confirms the presence of a fibroadenoma alone. A core biopsy
is taken, this confirms the presence of the fibroadenoma. However, the pathologist
notices that a small area of lobular carcinoma in situ is also present in the biopsy.
What is the best management?
A. Whole breast irradiation
B. Simple mastectomy
C. Mastectomy and sentinal lymph node biopsy
D. Wide local excision and sentinel lymph node biopsy
E. Breast MRI scan
Lobular carcinoma in situ has a low association with invasive malignancy. It is
seldom associated with microcalcification and therefore MRI is the best tool for
determining disease extent. Resection of in situ disease is not generally recommended
and most surgeons would simply pursue a policy of close clinical and radiological
follow up.
Lobular carcinoma of the breast
Lobular breast cancers are less common than their ductal counterparts. They typically
present differently, the mass is usually more diffuse and less obvious on the usual
imaging modalities of ultrasound and mammography. This is significant since the
disease may be understaged resulting in inadequate treatment when wide local
excision is undertaken.
In women with invasive lobular carcinoma it is usually safest to perform an MRI scan
of the breast, if breast conserving surgery is planned.
Lobular carcinomas are also more likely to be multifocal and metastasise to the
contralateral breast.
Lobular carcinoma in situ is occasionally diagnosed incidentally on core biopsies.
Unlike DCIS, lobular carcinoma in situ is far less strongly associated with foci of
invasion and is usually managed by close monitoring.
Which one of the following may be associated with an increased risk of venous
thromboembolism?

A. Diabetes
B. Cannula
C. Hyperthyroidism
D. Tamoxifen
E. Amiodarone
Consider thromboembolism in breast cancer patients on tamoxifen!
Venous thromboembolism: risk factors
ommon predisposing factors include malignancy, pregnancy and the period following
an operation. The comprehensive list below is partly based on the 2010 SIGN venous
thromboembolism (VTE) guidelines:
General
increased risk with advancing age
obesity
family history of VTE
pregnancy (especially puerperium)
immobility
hospitalisation
anaesthesia
central venous catheter: femoral >> subclavian
Underlying conditions
malignancy
thrombophilia: e.g. Activated protein C resistance, protein C and S deficiency
heart failure
antiphospholipid syndrome
Behcet's
polycythaemia
nephrotic syndrome
sickle cell disease
paroxysmal nocturnal haemoglobinuria
hyperviscosity syndrome
homocystinuria
Medication

combined oral contraceptive pill: 3rd generation more than 2nd generation
hormone replacement therapy
raloxifene and tamoxifen
antipsychotics (especially olanzapine) have recently been shown to be a risk
factor
SIGN also state that the following are risk factors for recurrent VTE:
previous unprovoked VTE
male sex
obesity
thrombophilias
A 42 year old lady is investigated for symptoms of irritability and altered bowel habit.
On examination she is noted to have a smooth enlargement of the thyroid gland. As
part of her investigations thyroid function tests are requested, these are as follows:
TSH 0.1 mug/l
Free T4 35 pmol/l
The most likely underlying diagnosis is:
A. Multinodular goitre
B. Follicular carcinoma of the thyroid gland
C. Graves disease
D. Pregnancy
E. None of the above
TSH receptor antibodies will cause stimulation of the thyroid to synthesise T4.
However, this will have a negative feedback effect on the pituitary causing decrease
in TSH levels.
Where hyperthyroidism occurs secondary to pregnancy the TSH is typically elevated.
Thyroid disease
Patients may present with a number of different manifestations of thyroid disease.
They can be broadly sub classified according to whether they are euthyroid or have
clinical signs of thyroid dysfunction. In addition it needs to be established whether
they have a mass or not.
Assessment
History
Examination including USS

If a nodule is identified then it should be sampled ideally via an image guided
fine needle aspiration
Radionucleotide scanning is of limited use
Thyroid Tumours
Papillary carcinoma
Follicular carcinoma
Anaplastic carcinoma
Medullary carcinoma
Lymphoma's
Multinodular goitre
One of the most common reasons for presentation
Provided the patient is euthyroid and asymptomatic and no discrete nodules
are seen, they can be reassured.
In those with compressive symptoms surgery is required and the best
operation is a total thyroidectomy.
Sub total resections were practised in the past and simply result in recurrent
disease that requires a difficult revisional resection.
Endocrine dysfunction
In general these patients are managed by physicians initially.
Surgery may be offered alongside radio iodine for patients with Graves
disease that fails with medical management or in patients who would prefer
not to be irradiated (e.g. pregnant women).
Patients with hypothyroidism do not generally get offered a thyroidectomy.
Sometimes people inadvertently get offered resections during the early phase
of Hashimotos thyroiditis, however, with time the toxic phase passes and
patients can simply be managed with thyroxine.
Complications following surgery
Anatomical such as recurrent laryngeal nerve damage.
Bleeding. Owing to the confined space haematoma's may rapidly lead to
respiratory compromise owing to laryngeal oedema.
Damage to the parathyroid glands resulting in hypocalcaemia.
Further sources of information 1. http://www.acb.org.uk/docs/TFTguidelinefinal.pdf- Association of Clinical
Biochemistry guidelines for thyroid function tests.

2. British association of endocrine surgeons website- http://www.baets.org.uk
Which of the following is not a risk factor for developing tuberculosis?
A. Gastrectomy
B. Solid organ transplantation with immunosupression
C. Intravenous drug use
D. Haematological malignancy
E. Amiodarone
Risk factors for developing active tuberculosis include:
silicosis
chronic renal failure
HIV positive
solid organ transplantation with immunosuppression
intravenous drug use
haematological malignancy
anti-TNF treatment
previous gastrectomy
Tuberculosis
Tuberculosis (TB) is an infection caused by Mycobacterium tuberculosis that most
commonly affects the lungs. Understanding the pathophysiology of TB can be
difficult - the key is to differentiate between primary and secondary disease.
Primary tuberculosis A non-immune host who is exposed to M. tuberculosis may develop primary infection
of the lungs. A small lung lesion known as a Ghon focus develops. The Ghon focus is
composed of tubercle-laden macrophages. The combination of a Ghon focus and hilar
lymph nodes is known as a Ghon complex
In immunocompotent people the intially lesion usually heals by fibrosis. Those who
are immunocompromised may develop disseminated disease (miliary tuberculosis).
Secondary (post-primary) tuberculosis If the host becomes immunocompromised the initial infection may become
reactivated. Reactivation generally occurs in the apex of the lungs and may spread
locally or to more distant sites. Possible causes of immunocomprise include:
immunosuppressive drugs including steroids
HIV
malnutrition
The lungs remain the most common site for secondary tuberculosis. Extra-pulmonary
infection may occur in the following areas:
central nervous system (tuberculous meningitis - the most serious
complication)
vertebral bodies (Pott's disease)
cervical lymph nodes (scrofuloderma)
renal
gastrointestinal tract
What is the most common presentation of a parotid gland tumour?
A. Parapharyngeal mass
B. Mass at anterior border of masseter
C. Mass inferior to the angle of the mandible
D. Mass behind the angle of the mandible
E. Mass anterior to the ear
Parotid tumours may present at any region in the gland. However, most lesions will be
located behind the angle of the mandible, inferior to the ear lobe. Tumours of the deep
lobe of the parotid may present as a parapharyngeal mass and large lesions may
displace the tonsil.
Parotid gland malignancy
Most parotid neoplasms (80%) are benign lesions
Most commonly present with painless mass in cheek region
Up to 30% may present with pain, when this is associated with a discrete mass
lesion in the parotid it usually indicates perineural invasion.
Perineural invasion is very unlikely to occur in association with benign lesions
80% of patients with facial nerve weakness caused by parotid malignancies
will have nodal metastasis and a 5 year survival of 25%
Types of malignancy
Mucoepidermoid
carcinoma
30% of all parotid malignancies
Usually low potential for local invasiveness and metastasis

(depends mainly on grade)
Adenoid cystic
carcinoma
Unpredictable growth patter
Tendency for perineural spread
Nerve growth may display skip lesions resulting in incomplete
excision
Distant metastasis more common (visceral rather than nodal
spread)
5 year survival 35%
Mixed tumours Often a malignancy occurring in a previously benign parotid
lesion
Acinic cell carcinoma Intermediate grade malignancy
May show perineural invasion
Low potential for distant metastasis
5 year survival 80%
Adenocarcinoma Develops from secretory portion of gland
Risk of regional nodal and distant metastasis
5 year survival depends upon stage at presentation, may be up
to 75% with small lesions with no nodal involvement
Lymphoma Large rubbery lesion, may occur in association with Warthins
tumours
Diagnosis should be based on regional nodal biopsy rather
than parotid resection Treatment is with chemotherapy (and
radiotherapy)
A 52 year old male is referred to urology clinic with impotence. He is known to have
hypertension. He does not have any morning erections. On further questioning the
patient reports pain in his buttocks, this worsens on mobilising. On examination there
is some muscle atrophy. The penis and scrotum are normal. What is the most likely
diagnosis?
A. Leriche syndrome
B. S4-S5 cord lesion
C. Pudendal nerve lesion
D. Psychological impotence
E. Beta blocker induced impotence
Leriche syndrome
Classically, it is described in male
patients as a triad of symptoms:
1. Claudication of the buttocks and
thighs
2. Atrophy of the musculature of the

legs
3. Impotence (due to paralysis of the
L1 nerve)
Leriche syndrome, is atherosclerotic occlusive disease involving the abdominal aorta
and/or both of the iliac arteries. Management involves correcting underlying risk
factors such as hypercholesterolaemia and stopping smoking. Investigation is usually
with angiography.
Leriche syndrome
Atheromatous disease involving the iliac vessels. Blood flow to the pelvic viscera is
compromised. Patients may present with buttock claudication and impotence (in this
particular syndrome). Diagnostic work up will include angiography, where feasible
iliac occlusions are usually treated with endovascular angioplasty and stent insertion.
A 23 year old man presents with diarrhoea and passage of mucous. He is suspected of
having ulcerative colitis. Which of the following is least likely to be associated with
this condition?
A. Superficial mucosal inflammation in the colon
B. Significant risk of dysplasia in long standing disease
C. Epsiodes of large bowel obstruction during acute attacks
D. Haemorrhage
E. Disease sparing the anal canal
Large bowel obstruction is not a feature of UC, patients may develop megacolon.
However, this is a different entity both diagnostically and clinically. Ulcerative colitis
does not affect the anal canal and the anal transitional zone. Inflammation is
superficial. Dysplasia can occur in 2% overall, but increases significantly if disease
has been present over 20 years duration. Granulomas are features of crohn's disease.
Other features:
Disease maximal in the rectum and may spread proximally
Contact bleeding
Longstanding UC crypt atrophy and metaplasia/dysplasia
Ulcerative colitis
Ulcerative colitis is a form of inflammatory bowel disease. Inflammation always starts

at rectum, never spreads beyond ileocaecal valve and is continuous. The peak
incidence of ulcerative colitis is in people aged 15-25 years and in those aged 55-65
years. It is less common in smokers.
The initial presentation is usually following insidious and intermittent symptoms.
Features include:
bloody diarrhoea
urgency
tenesmus
abdominal pain, particularly in the left lower quadrant
extra-intestinal features (see below)
Questions regarding the 'extra-intestinal' features of inflammatory bowel disease are
common. Extra-intestinal features include sclerosing cholangitis, iritis and ankylosing
spondylitis.
{Common to both Crohn's
disease (CD) and Ulcerative
colitis (UC)}
{Notes}
{Related to
disease activity}
Arthritis: pauciarticular,
asymmetric
Erythema nodosum
Episcleritis
Osteoporosis
Arthritis is the most common
extra-intestinal feature in both
CD and UC
Episcleritis is more common in
CD
{Unrelated to
disease activity}
Arthritis: polyarticular,
symmetric
Uveitis
Pyoderma gangrenosum
Clubbing
Primary sclerosing cholangitis
Primary sclerosing cholangitis is
much more common in UC
Uveitis is more common in UC
Pathology
red, raw mucosa, bleeds easily
no inflammation beyond submucosa (unless fulminant disease)
widespread superficial ulceration with preservation of adjacent mucosa which
has the appearance of polyps ('pseudopolyps')
inflammatory cell infiltrate in lamina propria
neutrophils migrate through the walls of glands to form crypt abscesses
depletion of goblet cells and mucin from gland epithelium
granulomas are infrequent
Barium enema
loss of haustrations
superficial ulceration, 'pseudopolyps'

long standing disease: colon is narrow and short -'drainpipe colon'
Endoscopy
Superficial inflammation of the colonic and rectal mucosa
Continuous disease from rectum proximally
Superifical ulceration, mucosal islands, loss of vascular definition and
continuous ulceration pattern.
Management
Patients with long term disease are at increased risk of development of
malignancy
Acute exacerbations are generally managed with steroids, in chronic patients
agents such as azathioprine and infliximab may be used
Individuals with medically unresponsive disease usually require surgery- in
the acute phase a sub total colectomy and end ileostomy. In the longer term a
proctectomy will be required. An ileoanal pouch is an option for selected
patients
A 52 year old woman attends clinic for investigation of abdominal pain and
constipation. On examination you note blue lines on the gum margin. She mentions
that her legs have become weak in the past few days. What is the most likely
diagnosis?
A. Acute intermittent porphyria
B. Lead poisoning
C. Constipation
D. Guillan Barre syndrome
E. Rectal carcinoma
This would be an impressive diagnosis to make in the surgical out patient department!
The combination of abdominal pain and a motor periperal neuropathy, should indicate
this diagnosis. The blue line along the gum margin can occur in up to 20% patients
with lead poisoning.
Lead poisoning
Along with acute intermittent porphyria, lead poisoning should be considered in
questions giving a combination of abdominal pain and neurological signs

Features
abdominal pain
peripheral neuropathy (mainly motor)
fatigue
constipation
blue lines on gum margin (only 20% of adult patients, very rare in children)
Investigations
The blood lead level is usually used for diagnosis. Levels greater than 10
mcg/dl are considered significant
Full blood count: microcytic anaemia. Blood film shows red cell abnormalities
including basophilic stippling and clover-leaf morphology
Raised serum and urine levels of delta aminolaevulinic acid may be seen
making it sometimes difficult to differentiate from acute intermittent porphyria
Urinary coproporphyrin is also increased (urinary porphobilinogen and
uroporphyrin levels are normal to slightly increased)
Management - various chelating agents are currently used:
Dimercaptosuccinic acid (DMSA)
D-penicillamine
EDTA
Dimercaprol
Theme: Vasculitis
A. Wegeners granulomatosis
B. Polyarteritis nodosa
C. Giant cell arteritis
D. Takayasu's arteritis
E. Buergers disease
For each of the scenarios provided please select the most likely underlying diagnosis
from the list below. Each option may be used once, more than once or not at all.
5. A 20 year old lady is referred to the vascular clinic. She has been feeling
generally unwell for the past six weeks. She works as a typist and has noticed
increasing pain in her forearms whilst working. On examination she has absent
upper limb pulses. Her ESR is measured and mildly elevated.
Takayasu's arteritis

Takayasus arteritis may be divided into acute systemic phases and the chronic
pulseless phase. In the latter part of the disease process the patient may
complain of symptoms such as upper limb claudication. In the later stages of
the condition the vessels will typically show changes of intimal proliferation,
together with band fibrosis of the intima and media.
6. A 32 year old man presents to the vascular clinic with symptoms of foot pain
during exertion. He is a heavy smoker and has recently tried to stop smoking.
On examination he has normal pulses to the level of the popliteal. However,
foot pulses are absent. A diagnostic angiogram is performed which shows an
abrupt cut off at the level of the anterior tibial artery, together with the
formation of corkscrew shaped collateral vessels distally.
Buergers disease
Buergers disease is most common in young male smokers. This demographic
is changing in those areas where young female smokers are more common. In
the acute lesion the internal elastic lamina of the vessels is usually intact. As
the disease progresses the changes progress to hypercellular occlusive
thrombus. Tortuous corkscrew collaterals may reconstitute patent segments of
the distal tibial or pedal vessels.
7. A 78 year old man presents with symptoms of headaches and deteriorating
vision. He notices that there is marked pain on the right hand side of his face
when he combs his hair.
Giant cell arteritis
Temporal arteritis may present acutely with symptoms of headache and visual
loss, or with a less acute clinical picture. Sight may be threatened and
treatment with immunosupressants should be started promptly. The often
requested temporal artery biopsy (which can be the bane of many surgeons) is
often non diagnostic and unhelpful.
Vasculitis
The vasculitides are a group of conditions characterised by inflammation of the blood
vessel walls. This may, in turn, compromise vessel integrity. Constitutional symptoms
may be present. Whilst certain disease subtypes are reported to affect specific vessels,
there is often a degree of overlap clinically.

Vessel diameter and vasculitis classification
Aorta and branches Takayasu's arteritis
Buergers disease
Giant cell arteritis
Large and medium sized arteries Buergers disease
Giant cell arteritis
Polyarteritis nodosa
Medium sized muscular arteries Polyarteritis nodosa
Wegeners granulomatosis
Small muscular arteries Wegeners granulomatosis
Rheumatoid vasculitis
Specific conditions
Takyasu's arteritis Inflammatory, obliterative arteritis affecting aorta and
branches
Females> Males
Symptoms may include upper limb claudication
Clinical findings include diminished or absent pulses
ESR often affected during the acute phase
Buergers disease Segmental thrombotic occlusions of the small and
medium sized lower limb vessels
Commonest in young male smokers
Proximal pulses usually present, but pedal pulses are
lost
An acuter hypercellular occlusive thrombus is often
present
Tortuous corkscrew shaped collateral vessels may be
seen on angiography
Giant cell arteritis Systemic granulomatous arteritis that usually affects
large and medium sized vessels
Females > Males
Temporal arteritis is commonest type
Granulomatous lesions may be seen on biopsy
(although up to 50% are normal)
Polyarteritis nodosa Systemic necrotising vasculitis affecting small and
medium sized muscular arteries
Most common in populations with high prevalence of
hepatitis B
Renal disease is seen in 70% cases
Angiography may show saccular or fusiform

aneurysms and arterial stenoses
Wegeners
granulomatosis
Predominantly affects small and medium sized arteries
Systemic necrotising granulomatous vasculitis
Cutaneous vascular lesions may be seen (ulceration,
nodules and purpura)
Sinus imaging may show mucosal thickening and air
fluid levels
Treatment Conditions such as Buergers disease are markedly helped by smoking cessation.
Immunosupression is the main treatment for vasculitides.
A 28 year old man presents with right upper quadrant pain and hydatid disease is
suspected. Which of the following statements relating to the disease is untrue?
A. First line treatment is with pentavalent antimony.
B. Peritoneal contamination with active daughter cysts may complicate
surgery.
C. CT scanning of the liver may show a floating membrane.
D. Biliary communication with the cysts may occur.
E. It is caused by Echinococcus granulosus.
Drug treatment is with albendazole or mebendazole. Praziquantzel may be used in the
pre operative stages.
Hydatid cysts
Hydatid cysts are endemic in Mediterranean and Middle Eastern countries. They are
caused by the tapeworm parasite Echinococcus granulosus. An outer fibrous capsule
is formed containing multiple small daughter cysts. These cysts are allergens which
precipitate a type 1 hypersensitivity reaction.
Clinical features are as follows:
Up to 90% cysts occur in the liver and lungs
Can be asymtomatic, or symptomatic if cysts > 5cm in diameter
Morbidity caused by cyst bursting, infection and organ dysfunction (biliary,
bronchial, renal and cerebrospinal fluid outflow obstruction)
In biliary ruputure there may be the classical triad of; biliary colic, jaundice,
and urticaria

CT is the best investigation to differentiate hydatid cysts from amoebic and pyogenic
cysts.
Surgery is the mainstay of treatment (the cyst walls must not be ruptured during
removal and the contents sterilised first).
Which of the following statements relating to neutrophil polymorphs is true?
A. Produce nitrogen peroxide as a microbicidal agent
B. Not involved in opsonisation
C. Deficiency leads to AIDS
D. Neutrophil disorders cause chronic granulomatous diseases
E. Have a lifespan of 9 hours
Neutrophils are the main cells of acute inflammation, important action against
gram -ve and +ve bacteria
Appearance of segmented nucleus and granulated cytoplasm
Have a lifespan of 1-3 days (shorter when consumed during septic process,
though 9 hours is unusual)
Actions include: movement, opsonise microorganisms, phagocytosis &
intracellular killing of microorganisms via aerobic (produce HYDROGEN
PEROXIDE) & anaerobic mechanisms.
Neutrophil disorders include chronic granulomatous diseases: rare
AIDS associated with T cell deficiency
Acute inflammation
Inflammation is the reaction of the tissue elements to injury. Vascular changes occur,
resulting in the generation of a protein rich exudate. So long as the injury does not
totally destroy the existing tissue architecture, the episode may resolve with
restoration of original tissue architecture.
Vascular changes
Vasodilation occurs and persists throughout the inflammatory phase.
Inflammatory cells exit the circulation at the site of injury.
The equilibrium that balances Starlings forces within capillary beds is
disrupted and a protein rich exudate will form as the vessel walls also become
more permeable to proteins.
The high fibrinogen content of the fluid may form a fibrin clot. This has
several important immunomodulatory functions.

Sequelae
Resolution Typically occurs with minimal initial injury
Stimulus removed and normal tissue architecture
results
Organisation Delayed removed of exudate
Tissues undergo organisation and usually fibrosis
Suppuration Typically formation of an abscess or an empyema
Sequestration of large quantities of dead
neutrophils
Progression to chronic
inflammation
Coupled inflammatory and reparative activities
Usually occurs when initial infection or
suppuration has been inadequately managed
Causes
Microbacterial infections e.g. Viruses, exotoxins or endotoxins released by
bacteria
Chemical agents
Physical agents e.g. Trauma
Hypersensitivity reactions
Tissue necrosis
Presence of neutrophil polymorphs is a histological diagnostic feature of acute
inflammation A 33 year old man is involved in a road traffic accident. He is initially stable and
transferred to the accident and emergency department. On arrival he is catheterised.
One minute later he becomes hypotensive, with evidence of angioedema surrounding
his penis. What is the most likely explanation for this event?
A. Type V latex hypersensitivity reaction
B. Type IV latex hypersensitivity reaction
C. Type III latex hypersensitivity reaction
D. Type I latex hypersensitivity reaction
E. Type II latex hypersensitivity reaction
Theme from April 2012 Exam

Sudden collapse and angioedema following exposure to latex (of which most urinary
catheters are manufactured) suggests a type I hypersensitivity reaction.
Hypersensitivity reactions
The Gell and Coombs classification divides hypersensitivity reactions into 4 types
Type I Type II Type III Type IV
Description Anaphylactic Cytotoxic Immune
complex
Delayed type
Mediator IgE IgG, IgM IgG, IgM T-cells
Antigen Exogenous Cell surface Soluble Tissues
Response
time
Minutes Hours Hours 2-3 days
Examples Asthma
Hay fever
Autoimmune
haemolytic anaemia
Pemphigus
Goodpasture's
Serum
sickness
SLE
Aspergillosis
Graft versus host
disease
Contact
dermatitis
A 43 year old female develops severe chest wall cellulitis following a mastectomy.
On examination the skin is markedly erythematous. Which of the acute inflammatory
mediators listed below is least likely to produce vasodilation?
A. Complement component C5a
B. Lysosomal compounds
C. Histamine
D. Serotonin
E. Prostaglandins
Erythema is a classical feature of acute inflammation. Potent mediators of vascular
dilatation include; histamine, prostaglandins, nitric oxide, platelet activating factor,
complement C5a (and C3a) and lysosomal compounds. Although serotonin is
associated with acute inflammation it is a vasoconstrictor. The effects of serotonin are
dependant upon the state of the vessels in the tissues. Intact and healthy tissues and
vessels will respond to a serotonin infusion with vasodilation (hence the flushing seen
in carcinoid syndrome). In contrast it worsens cardiac ischaemia in myocardial
infarcts when released from damaged platelets.
Acute inflammation
Inflammation is the reaction of the tissue elements to injury. Vascular changes occur,
resulting in the generation of a protein rich exudate. So long as the injury does not
totally destroy the existing tissue architecture, the episode may resolve with
restoration of original tissue architecture.
Vascular changes
Vasodilation occurs and persists throughout the inflammatory phase.
Inflammatory cells exit the circulation at the site of injury.
The equilibrium that balances Starlings forces within capillary beds is
disrupted and a protein rich exudate will form as the vessel walls also become
more permeable to proteins.
The high fibrinogen content of the fluid may form a fibrin clot. This has
several important immunomodulatory functions.
Sequelae
Resolution Typically occurs with minimal initial injury
Stimulus removed and normal tissue architecture
results
Organisation Delayed removed of exudate
Tissues undergo organisation and usually fibrosis
Suppuration Typically formation of an abscess or an empyema
Sequestration of large quantities of dead
neutrophils
Progression to chronic
inflammation
Coupled inflammatory and reparative activities
Usually occurs when initial infection or
suppuration has been inadequately managed
Causes
Microbacterial infections e.g. Viruses, exotoxins or endotoxins released by
bacteria
Chemical agents
Physical agents e.g. Trauma
Hypersensitivity reactions
Tissue necrosis
Presence of neutrophil polymorphs is a histological diagnostic feature of acute
inflammation A 43 year old man presents with a 3 week history of malaise, sore throat,
odynophagia and dysphagia. On examination he is found to have patchy white spots
in his oropharynx. An upper GI endoscopy is performed and similar lesions are
identified in the oesophagus. Which investigation is most likely to identify the
underlying pathology in this case?

A. Serum urea and electrolytes
B. Oesophageal biopsy for culture
C. Oesophageal biopsy for histology
D. Glucose tolerance testing
E. Viral serology
Oesophageal candidiasis is associated with immunosupression; mainly in patients on
chemotherapy, with haematological malignancy, HIV or inhaled steroids. In patients
with HIV, oesophageal candidiasis is part of the spectrum of AIDS defining illnesses
and usually occurs when the CD4 count is less than 200. Others include PCP
pneumonia and CMV infections.
Oesophageal candidiasis
Characterised by white spots in the oropharynx with extension into the oesophagus.
Associated with broad spectrum antibiotic usage, immunosupression and
immunological disorders.
Patients may present with oropharyngeal symptoms, odynophagia and dysphagia.
Treatment is directed both at the underlying cause (which should be investigated for)
and with oral antifungal agents.
Theme: Colonic obstruction
A. Malignant obstruction
B. Olgilvies syndrome
C. Volvulus
D. Diverticular stricture
E. Ischaemic stricture
Please select the most likely cause of obstruction for the situation described. Each
option may be used once, more than once or not at all.
13. A 78 year old man has undergone a hemi-arthroplasty for a intracapsular hip
fracture. Post operatively he develops electrolyte derangement and receives
intravenous fluids. Over the previous 24 hours he develops marked abdominal
distension. On examination he has a tense, tympanic abdomen which is not
painful. A contrast enema shows flow of contrast through to the caecum and
through the ileocaecal valve.
Olgilvies syndrome

Patients with electrolyte disturbance and previous surgery may develop
colonic pseudo-obstruction (olgilvies syndrome). The diagnosis is made using
a contrast enema and treatment is usually directed at the underlying cause
with colonic decompression if indicated.
14. A 67 year old man has had multiple episodes with fever and left iliac fossa
pain. These have usually resolved with courses of intravenous antibiotics. He
is admitted with a history of increasing constipation and abdominal
distension. A contrast x-ray is performed which shows flow of contrast to the
sigmoid colon, here the contrast flows through a long narrow segment of
colon into dilated proximal bowel.
Diverticular stricture
The long history of left iliac fossa pain and development of bowel obstruction
suggests a diverticular stricture. These may contain a malignancy and most
will require resection.
15. A 78 year old lady from a nursing home is admitted with a 24 hour history of
absolute constipation and abdominal pain. On examination she has a
distended soft mass in her left iliac fossa. An x-ray is performed which shows
a large dilated loop of bowel in the left iliac fossa which contains a fluid
level.
Volvulus
Sigmoid volvulus may present with an asymmetrical mass in an elderly
patient. It may contain a fluid level, visible on plain films.
Colonic obstruction
Cause Features Treatment
Cancer Usually insidious onset
History of progressive constipation
Systemic features (e.g. anaemia)
Abdominal distension
Absence of bowel gas distal to site
of obstruction
Establish diagnosis (e.g.
contrast enema/
endoscopy)
Laparotomy and
resection, stenting,
defunctioning colostomy
or bypass
Diverticular
stricture
Usually history of previous acute
diverticulitis
Once diagnosis
established, usually

Long history of altered bowel habit
Evidence of diverticulosis on
imaging or endoscopy
surgical resection
Colonic stenting should
not be performed for
benign disease
Volvulus Twisting of bowel around its
mesentery
Sigmoid colon affected in 76%
cases
Patients usually present with
abdominal pain, bloating and
constipation
Examination usually shows
asymmetrical distension
Plain X-rays usually show
massively dilated sigmoid colon,
loss of haustra and "U" shape are
typical, the loop may contain fluid
levels
Initial treatment is to
untwist the loop, a
flexible sigmoidoscopy
may be needed
Those with clinical
evidence of ischaemia
should undergo surgery
Patient with recurrent
volvulus should undergo
resection
Acute colonic
pseudo-
obstruction
Symptoms and signs of large bowel
obstruction with no lesion
Usually associated with metabolic
disorders
Usually a cut off in the left colon
(82% cases)
Although abdomen tense and
distended, it is usually not painful
All patients should undergo contrast
enema (may be therapeutic!)
Colonoscopic
decompression
Correct metabolic
disorders
IV neostigmine
Surgery
A 52 year old man with dyspepsia is found to have a duodenal ulcer. A CLO test is
taken and is positive. Which statement relating to the likely causative organism is
false?
A. It is a gram negative organism
B. It lives only on gastric type mucosa
C. It may occupy areas of ectopic gastric metaplasia
D. In patients who are colonised there is commonly evidence of fundal
gastritis on endoscopy
E. It produces a powerful urease that forms the basis of the Clo test
Helicobacter pylori accounts for >75% cases of duodenal ulceration. It may be
diagnosed with either serology, microbiology, histology or CLO testing.

Theme from January 2011 Exam
Helicobacter pylori rarely produces any typical features on endoscopy. Where
infection is suspected the easiest course of action is to take an antral biopsy for Clo
testing in the endoscopy suite.
Helicobacter Pylori
Infection with Helicobacter Pylori is implicated in many cases of duodenal ulceration
and up to 60% of patients with gastric ulceration.
Gram negative, helix shaped rod, microaerophillic
Produces hydrogenase that can derive energy from hydrogen released by
intestinal bacteria
Flagellated and mobile
Those carrying the cag A gene may cause ulcers
It secretes urease that breaks down gastric urea> Carbon dioxide and
ammonia> ammonium>bicarbonate (simplified!) The bicarbonate can
neutralise the gastric acid.
Usually colonises the gastric antrum and irritates resulting in increased gastrin
release and higher levels of gastric acid. These patients will develop duodenal
ulcers. In those with more diffuse H-Pylori infection gastric acid levels are
lower and ulcers develop by local tissue damage from H-Pylori- these patients
get gastric ulcers.
Diagnosis may be made by serology (approx. 75% sensitive). Biopsy urease
test during endoscopy probably the most sensitive.
In patients who are colonised 10-20% risk of peptic ulcer, 1-2% risk gastric
cancer, <1% risk MALT lymphoma.
A 34 year old male presents with painful rectal bleeding and a fissure in ano is
suspected. On examination he has an epithelial defect at the mucocutaenous defect
that is located anteriorly. Approximately what proportion of patients with fissure in
ano will present with this pattern of disease?
A. 90%
B. 10%
C. 50%
D. 25%
E. 100%
Only a minority of patients with fissure in ano will have an anteriorly sited fissure.
They are particularly rare in males and an anterior fissure in a man should prompt a
search for an underlying cause.

Anal fissure
Anal fissures are a common cause of painful, bright red, rectal bleeding.
Most fissures are idiopathic and present as a painful mucocutaneous defect in the
posterior midline (90% cases). Fissures are more likely to be anteriorly located in
females, particularly if they are multiparous. Multiple fissures and those which are
located at other sites are more likely to be due to an underlying cause.
Diseases associated with fissure in ano include:
Crohns disease
Tuberculosis
Internal rectal prolapse
Diagnosis In most cases the defect can be visualised as a posterior midline epithelial defect.
Where symptoms are highly suggestive of the condition and examination findings are
unclear an examination under anaesthesia may be helpful. Atypical disease
presentation should be investigated with colonoscopy and EUA with biopsies of the
area.
Treatment Stool softeners are important as the hard stools may tear the epithelium and result in
recurrent symptoms. The most effective first line agents are topically applied GTN
(0.2%) or Diltiazem (2%) paste. Side effects of diltiazem are better tolerated.
Resistant cases may benefit from injection of botulinum toxin or lateral internal
sphincterotomy (beware in females). Advancement flaps may be used to treat resistant
cases.
Sphincterotomy produces the best healing rates. It is associated with incontinence to
flatus in up to 10% of patients in the long term.
The pathogenesis of osteopetrosis is best explained by a defect in which of the
following?
A. Osteoclast function
B. PTH receptors
C. Osteoblast function
D. Calcium resorption in proximal tubule
E. Calcium absorption
Osteopetrosis

Overview
aka marble bone disease
rare disorder of defective osteoclast function resulting in failure of normal
bone resorption
stem cell transplant and interferon-gamma have been used for treatment
A 13 month old boy is brought to the surgical clinic by his mother because his left
testicle is not located in the scrotum. At which of the following sites would the testicle
be located if it were an ectopic testis?
A. Canalicular
B. Inguinal
C. External inguinal ring
D. Superficial inguinal pouch
E. High scrotal
Theme from September 2011 Exam
Theme from January 2012 Exam
Ectopic testes are those that come to lie outside the normal range of embryological
descent (i.e. in the superficial inguinal pouch). Other sites of ectopic testes include;
base of penis, femoral and perineal.
Testicular disorders-paediatric
Testicular disorders Testicular disorders are some of the commonest conditions present in paediatric
urological practice.
Cryptorchidism
The embryological descent of the testicle from within the abdominal cavity
may be subject to a number of variations. Distinctions need to be made
clinically from a non descended testis and a testis that is retractile.
Testis that lie outside the normal path of embryological descent are termed
ectopic testis. Undescended testis occurs in 1% of male infants. Where the
testis does not lie in an intra scrotal location, its location should be
ascertained. Where both testes are absent the infant may be intersex.
MRI scanning may reveal intra-abdominal testes; however a GA is often
needed to perform this investigation in this age group.

Testes that are undescended should be placed in the scrotum after 1 year of
age as the testosterone surge that may facilitate descent occurs at 6 months of
age.
Where the testes lie distally e.g. Superficial inguinal pouch an open
orchidopexy is the procedure of choice.
With abdominal testes a laparoscopy should be performed. The risk of
seminoma is increased in individuals with a non descended testes and this risk
is not reduced by orchidopexy.
Testicular torsion
Typically the patient has severe sudden onset of scrotal pain. The difficulty in
paediatric practice is the lack of clear history.
On examination the testis is tender and enlarged.
Management is by surgical exploration.
Delay beyond 6 hours is associated with low salvage rates.
A torted hyatid produces pain that is far more localised and the testis itself
should feel normal. However, diagnostic doubt often exists and in such cases
surgical exploration is warranted.
A splenectomy increases the risk of infection from all the following organisms
except?
A. Pneumococcus
B. Klebsiella
C. Haemophilus influenzae
D. Staphylococcus aureus
E. Neisseria meningitidis
Theme from 2010 Exam
Staphylococcus aureus infection following splenectomy is no more common than in
non splenectomised individuals. The other organisms are encapsulated, which is why
they are more likely to cause overwhelming post splenectomy sepsis.
Post splenectomy sepsis
The loss of splenic function renders individuals at increased risk of fulminant sepsis.
Young children are at the highest risk, especially in the first 2 years following
surgery. Surgery for trauma is associated with a lower risk than when splenectomy is
performed as a treatment for haematological disorders.

Infection with encapsulated organisms poses the greatest risk, these organisms may be
opsonised, but this then goes undetected at an immunological level due to loss of the
spleen.
Prophylactic vaccinations are usually administered to reduce the risk of pneumococcal
septicaemia. Since the vaccine only covers up to 80% of pneumococcal infections,
patients will usually recieve long term, low dose penicillin prophylaxis in addition to
vaccination.
Which of the following is not an extraintestinal feature Crohns disease?
A. Iritis
B. Clubbing
C. Aphthous ulcers
D. Erythema multiforme
E. Pyoderma gangrenosum
Extraintestinal manifestation of
inflammatory bowel disease: A PIE
SAC
Aphthous ulcers
Pyoderma gangrenosum
Iritis
Erythema nodosum
Sclerosing cholangitis
Arthritis
Clubbing
Crohns disease
Crohns disease is a chronic transmural inflammation of a segment(s) of the
gastrointestinal tract and may be associated with extra intestinal manifestations.
Frequent disease patterns observed include ileal, ileocolic and colonic disease. Peri-
anal disease may occur in association with any of these. The disease is often
discontinuous in its distribution. Inflammation may cause ulceration, fissures, fistulas
and fibrosis with stricturing. Histology reveals a chronic inflammatory infiltrate that is
usually patchy and transmural.
Ulcerative colitis Vs Crohns
Crohn's disease Ulcerative colitis
Distribution Mouth to anus Rectum and colon
Macroscopic Cobblestone appearance, apthoid Contact bleeding

changes ulceration
Depth of
disease
Transmural inflammation Superficial inflammation
Distribution
pattern
Patchy Continuous
Histological
features
Granulomas (non caseating epithelioid
cell aggregates with Langhans' giant
cells)
Crypt abscesses,
Inflammatory cells in the
lamina propria
Extraintestinal manifestations of Crohns
Related to disease extent Unrelated to disease extent
Aphthous ulcers (10%) Sacroiliiitis (10-15%)
Erythema nodosum (5-10%) Ankylosing spondylitis (1-2%)
Pyoderma gangrenosum (0.5%) Primary sclerosing cholangitis (Rare)
Acute arthropathy (6-12%) Gallstones (up to 30%)
Ocular complications (up to 10%) Renal calculi (up to 10%)
Which of the following is not considered a risk factor for the development of
oesophageal malignancy?
A. Oesophageal metaplasia
B. Smoking
C. Excessive intake of alcoholic spirits
D. Achalasia
E. Blood group O
Blood group O is not a risk factor for oesophageal cancer. Achalasia is associated
with the risk of developing squamous cell carcinoma of the oesophagus.
Oesophageal cancer
Incidence is increasing
In most cases in the Western world this increase is accounted for by a rise in
the number of cases of adenocarcinoma. In the UK adenocarcinomas account
for 65% of cases.
Barretts oesophagus is a major risk factor for most cases of oesophageal
adenocarcinoma.
In other regions of the world squamous cancer is more common and is linked
to smoking, alcohol intake, diets rich in nitrosamines and achalasia.

Surveillance of Barretts is important as it imparts a 30 fold increase in cancer
risk and if invasive malignancy is diagnosed early then survival may approach
85% at 5 years.
Diagnosis
Upper GI endoscopy is the first line test
Contrast swallow may be of benefit in classifying benign motility disorders
but has no place in the assessment of tumours
Staging is initially undertaken with CT scanning of the chest, abdomen and
pelvis. If overt metastatic disease is identified using this modality then further
complex imaging is unnecessary
If CT does not show metastatic disease, then local stage may be more
accurately assessed by use of endoscopic ultrasound.
Staging laparoscopy is performed to detect occult peritoneal disease. PET CT
is performed in those with negative laparoscopy. Thoracoscopy is not
routinely performed.
Treatment Operable disease is best managed by surgical resection. The most standard procedure
is an Ivor- Lewis type oesophagectomy. This procedure involves the mobilisation of
the stomach and division of the oesophageal hiatus. The abdomen is closed and a right
sided thoracotomy performed. The stomach is brought into the chest and the
oesophagus mobilised further. An intrathoracic oesophagogastric anastomosis is
constructed. Alternative surgical strategies include a transhiatal resection (for distal
lesions), a left thoraco-abdominal resection (difficult access due to thoracic aorta) and
a total oesophagectomy (McKeown) with a cervical oesophagogastric anastomosis.
The biggest surgical challenge is that of anastomotic leak, with an intrathoracic
anastomosis this will result in mediastinitis. With high mortality. The McKeown
technique has an intrinsically lower systemic insult in the event of anastmotic leakage.
In addition to surgical resection many patients will be treated with adjuvent
chemotherapy.
Theme: Thyroid blood testing
A. Measurement of antibodies to TSH receptor
B. Thyroid peroxidase antibodies
C. Thyroglobulin antibodies
D. Serum calcitonin
Please select the blood test most commonly performed for the diagnosis or assessment
of the thyroid disorder described. Each answer may be used once, more than once or
not at all.
23. A 32 year old lady is diagnosed with Medullary carcinoma of the thyroid and

has undergone resection of the tumour.
Serum calcitonin
Measurement of basal or stimulated calcitonin concentrations is used to
assess the completeness of surgical resection, and is of use in detecting
diseases recurrences during follow up.
24. A 20 year old lady has undergone a total thyroidectomy for a well
differentiated papillary carcinoma. She attends clinic and is well and the
surgeon wishes to screen for disease recurrence.
Thyroglobulin antibodies
Antibodies to thyroglobulin, the major constituent of colloid and precursor of
thyroid hormones may be elevated in those with metastatic or recurrent
thyroid cancer. Results may be erronoeous in those with other thyroid
disorders.
25. A 33 year old lady presents with a recently diagnosed goitre and a diagnosis
of Hashimotos thyroiditis is suspected.
Thyroid peroxidase antibodies
Antibodies to thyroid peroxidase are found in most patients with Graves
disease or Hashimotos thyroiditis.
Blood testing in thyroid disease
Assay Usage
Thyroid peroxidase
(microsomal)
antibodies
Found in autoimmune disease affecting the thyroid
(Hashimotos 100%) and Graves (70%)
Antibodies to TSH
receptor
Individuals with Graves disease (95%)
Thyroglobulin
antibodies
Not useful for clinically distinguishing between
different types of thyroid disease, may be used as part
of thyroid cancer follow up
Calcitonin Released from the parafollicular cells
Usually found in patient with Medullary carcinoma

of the thyroid
Which one of the following complications is least associated with ventricular septal
defects?
A. Right heart failure
B. Aortic regurgitation
C. Eisenmenger's complex
D. Infective endocarditis
E. Atrial fibrillation
Atrial fibrillation is associated more with atrial septal defects
Ventricular septal defect
Ventricular septal defects are the most common cause of congenital heart disease.
They close spontaneously in around 50% of cases. Non-congenital causes include post
myocardial infarction
Features
classically a pan-systolic murmur which is louder in smaller defects
Complications
aortic regurgitation*
infective endocarditis
Eisenmenger's complex
right heart failure
*aortic regurgitation is due to a poorly supported right coronary cusp resulting in cusp
prolapse A 24 year old man from Sudan presents with a lymphadenopathy and weight loss. A
diagnosis of tuberculosis is suspected and a lymph node biopsy is performed. Staining with
which of the agents below is most likely to facilitate identification of the causative
organism?

A. Gram stain
B. Ziehl-Neelsen stain
C. Von Kossa stain
D. Van Gieson stain
E. Masson Trichrome stain
Ziehl-Neelsen stain is typically used to identify mycobacteria. They are not stained in the
Gram staining process. Van Gieson and Masson trichrome are histological staining methods
for identification of connective tissues. The Von Kossa technique is useful for identifying
tissue mineralisation.
Tuberculosis pathology
Is a form of primary chronic inflammation, caused by the inability of macrophages to kill the Mycobacterium tuberculosis.
The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph nodes is referred to as a Ghon complex.
This leads to the formation of a granuloma which is a collection of epithelioid histiocytes.
There is the presence of caseous necrosis in the centre. The inflammatory response is mediated by a type 4 hypersensitivity reaction. In healthy individuals the disease may be contained, in the immunocompromised
disseminated (miliary TB) may occur.
Diagnosis
Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen staining is typically used.
Culture based methods take far longer.
Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method

Image sourced from Wikipedia
A 24 year old man from Sudan presents with a lymphadenopathy and weight loss. A
diagnosis of tuberculosis is suspected and a lymph node biopsy is performed. Staining with
which of the agents below is most likely to facilitate identification of the causative
organism?
A. Gram stain
B. Ziehl-Neelsen stain
C. Von Kossa stain
D. Van Gieson stain
E. Masson Trichrome stain
Ziehl-Neelsen stain is typically used to identify mycobacteria. They are not stained in the
Gram staining process. Van Gieson and Masson trichrome are histological staining methods
for identification of connective tissues. The Von Kossa technique is useful for identifying
tissue mineralisation.
Tuberculosis pathology

Is a form of primary chronic inflammation, caused by the inability of macrophages to kill the Mycobacterium tuberculosis.
The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph nodes is referred to as a Ghon complex.
This leads to the formation of a granuloma which is a collection of epithelioid histiocytes.
There is the presence of caseous necrosis in the centre. The inflammatory response is mediated by a type 4 hypersensitivity reaction. In healthy individuals the disease may be contained, in the immunocompromised
disseminated (miliary TB) may occur.
Diagnosis
Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen staining is typically used.
Culture based methods take far longer.
Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method
Image sourced from Wikipedia
Which of the following is not a pathological feature of breast cancer?
A. Resemblance to ductal epithelial cells
B. Angiogenesis
C. Nuclear pleomorphism
D. Metastatic calcification

E. Vascular invasion
Dystrophic calcification may be present in breast malignancy and is the basis for the
breast screening programme. Metastatic calcification is calcification which occurs in
otherwise normal tissues, usually as a result of hypercalcaemia. Invasive ductal
carcinoma is the most common type of breast cancer, unless the tumour is very poorly
differentiated there is usually some resemblance to ductal epithelial cells.
Breast cancer pathology
The histological features of breast cancer depend upon the underlying diagnosis. The
invasive component is usually comprised of ductal cells (unless it is an invasive
lobular cancer). In situ lesions may co-exist (such as DCIS).
Typical changes seen in conjunction with invasive breast cancer include:
1. Nuclear pleomorphism
2. Coarse chromatin
3. Angiogenesis
4. Invasion of the basement membrane
5. Dystrophic calcification (may be seen on mammography)
6. Abnormal mitoses
7. Vascular invasion
8. Lymph node metastasis
The primary tumour is graded on a scale of 1-3 where 1 is the most benign lesion and
3 the most poorly differentiated.
Immunohistochemistry for oestrogen receptor and herceptin status is routinely
performed.
The grade, lymph node stage and size are combined to provide the Nottingham
prognostic index.
Theme: Renal lesions
A. Renal cell carcinoma
B. Renal transitional cell carcinoma
C. Nephroblastoma
D. Neuroblastoma
E. Angiomyolipoma
F. Renal squamous cell carcinoma
G. Retroperitoneal fibrosis
For each scenario please select the most likely underlying diagnosis. Each option may
be used once, more than once or not at all.

29. A 69 year old male presents with haematuria. He worked in the textile
industry. He has a left flank mass. A CT IVU shows a lesion of the left renal
pelvis.
You answered Renal squamous cell carcinoma
The correct answer is Renal transitional cell carcinoma
TCC is a rare form of renal cancer, accounting for approximately 7% of all
renal tumours. Risk factors include exposure to chemicals in the textile,
plastic and rubber industry.
30. A 2 year old boy presents with a right renal mass. On examination he has an
irregular mass arisong from the right flank and is hypertensive. A CT scan
shows a non calcified irregular lesion affecting the apex of the right kidney
and the right adrenal gland.
Nephroblastoma
Wilm's tumour of the kidney is the most common renal tumour in children.
Both nephroblastoma and neuroblastoma may occupy the adrenal and apex of
the kidney. In the case of neuroblastoma the lesion will have arisen from the
adrenal, in the case of nephroblastoma the lesion will have arisen from the
kidney. Hypertension is more commonly associated with nephroblastoma.
Neuroblastomas are usually calcified, whereas nephroblastomas are not and
this may be of diagnostic usefulness pre operatively.
31. A 35 year old male presents with haematuria. He is found to have bilateral
masses in the flanks. He has a history of epilepsy and learning disability.
You answered Neuroblastoma
The correct answer is Angiomyolipoma
This patient has tuberous sclerosus. This is associated with angiomyolipoma,
which is present in 60-80% patients. It is a benign lesion.
Renal lesions
Lesion Disease specific features Treatment
Renal cell Most present with Usually radical or partial

carcinoma haematuria (50%)
Common renal tumour (85%
cases)
Paraneoplastic features
include hypertension and
polycythaemia
Most commonly has
haematogenous mestastasis
nephrectomy
Nephroblastoma Rare childhood tumour
It accounts for 80% of all
genitourinary malignancies
in those under the age of 15
years
Up to 90% will have a mass
50% will be hypertensive
Diagnostic work up includes
ultrasound and CT scanning
Surgical resection combined
with chemotherapy (usually
vincristine, actinomycin D
and doxorubicin
Neuroblastoma Most common extracranial
tumour of childhood
80% occur in those under 4
years of age
Tumour of neural crest
origin (up to 50% occur in
the adrenal gland)
The tumour is usually
calcified and may be
diagnosed using MIBG
scanning
Staging is with CT
Surgical resection,
radiotherapy and
chemotherapy
Transitional cell
carcinoma
Accounts for 90% of upper
urinary tract tumour, but
only 10% of renal tumours
Males affected 3x more than
females
Occupational exposure to
industrial dyes and rubber
chemicals may increase risk
Up to 80% present with
painless haematuria
Diagnosis and staging is with
CT IVU
Radical nephroureterectomy
Angiomyolipoma 80% of these hamartoma
type lesions occur
sporadically, the remainder
are seen in those with
50% of patients with lesions
>4cm will have symptoms
and will require surgical
resection

tuberous sclerosis
Tumour is composed of
blood vessels, smooth
muscle and fat
Massive bleeding may occur
in 10% of cases
An 18 month old boy presents with recurrent urinary tract infections. As part of the
diagnostic work-up he is noted to have abnormal renal function. An ultrasound scan is
performed and shows bilateral hydronephrosis. What is the most likely underlying
diagnosis?
A. Urethral valves
B. Meatal stenosis
C. Hydronephrosis
D. Pelvico-ureteric junction obstruction
E. Benign prostatic hyperplasia
Theme from April 2012 Exam
A posterior urethral valve is an obstructive, developmental uropathy that usually
affects male infants (incidence 1 in 8000). Diagnostic features include bladder wall
hypertrophy, hydronephrosis and bladder diverticula.
Urethral valves
Posterior urethral valves are the commonest cause of infravesical outflow obstruction
in males. They may be diagnosed on ante natal ultrasonography. Because the bladder
has to develop high emptying pressures in utero the child may develop renal
parenchymal damage. This translates to renal impairment noted in 70% of boys at
presentation. Treatment is with bladder catheterisation. Endoscopic valvotomy is the
definitive treatment of choice with cystoscopic and renal follow up. At which of the following anatomical sites does dormant tuberculosis most frequently
reactivate?
A. Apex of the lung
B. Base of the lung

C. Brain
D. Terminal ileum
E. Lumbar spine
TB reactivation most commonly occurs at the lung apex. This site is better oxygenated than
elsewhere allowing the mycobacteria to multiply more rapidly and then spread both locally
and distantly.
Tuberculosis pathology
Is a form of primary chronic inflammation, caused by the inability of macrophages to kill the Mycobacterium tuberculosis.
The macrophages often migrate to regional lymph nodes, the lung lesion plus affected lymph nodes is referred to as a Ghon complex.
This leads to the formation of a granuloma which is a collection of epithelioid histiocytes.
There is the presence of caseous necrosis in the centre. The inflammatory response is mediated by a type 4 hypersensitivity reaction. In healthy individuals the disease may be contained, in the immunocompromised
disseminated (miliary TB) may occur.
Diagnosis
Waxy membrane of mycobacteria prevents binding with normal stains. Ziehl - Neelsen staining is typically used.
Culture based methods take far longer.
Image showing acid- alcohol fast mycobacteria stained using the Ziehl- Neelsen method

Image sourced from Wikipedia
What is the commonest tumour type encountered in the colon?
A. Squamous cell carcinoma
B. Adenocarcinoma
C. Lymphoma
D. Anaplastic carcinoma
E. Sarcoma
Adenocarcinoma are the most common and typically arise as a result of the adenoma -
carcinoma sequence.
Colorectal cancer
Annually about 150,000 new cases are diagnosed and 50,000 deaths from the
disease
About 75% will have sporadic disease and 25% will have a family history
Colorectal tumours comprise a spectrum of disease ranging from adenomas
through to polyp cancers and frank malignancy.
Polyps may be categorised into: neoplastic polyps, adenomatous polyps and
non neoplastic polyps.
The majority of adenomas are polypoidal lesions, although flat lesions do
occur and may prove to be dysplastic.

Non-neoplastic polyps include hyperplastic, juvenile, hamartomatous,
inflammatory, and lymphoid polyps, which have not generally been thought of
as precursors of cancer.
Three characteristics of adenomas that correlate with malignant potential have
been characterised. These include increased size, villous architecture and
dysplasia. For this reason most polyps identified at colonoscopy should be
removed.
The transformation from polyp to cancer is described by the adenoma -
carcinoma sequence and its principles should be appreciated. Essentially
genetic changes accompany the transition from adenoma to carcinoma; key
changes include APC, c-myc, K RAS mutations and p53 deletions.
Which of the following changes are most likely to be identified in the aortic wall of a
38 year old lady with a Marfans syndrome and a dissecting aortic aneurysm?
A. Transmural aortitis
B. Cystic medial necrosis
C. Foamy macrophages
D. Dense dystrophic calcification
E. None of the above
Cystic medial necrosis ( or cystic medial degeneration) occurs when basophils and
mucoid material lie in between the intimal elastic fibres of the aorta. It is typically
found in the aortic degeneration of Marfans syndrome, but may also be seen in aortic
degeneration in older adults.
Aortic dissection
More common than rupture of the abdominal aorta
33% of patients die within the first 24 hours, and 50% die within 48 hours if
no treatment received
Associated with hypertension
Features of aortic dissection: tear in the intimal layer, followed by formation
and propagation of a subintimal hematoma. Cystic medial necrosis (Marfan's)
Most common site of dissection: 90% occurring within 10 centimetres of the
aortic valve
Stanford Classification
Type Location Treatment
A Ascending aorta/ aortic root Surgery- aortic root replacement
B Descending aorta Medical therapy with antihypertensives

DeBakey classification
Type Site affected
I Ascending aorta, aortic arch, descending aorta
II Ascending aorta only
III Descending aorta distal to left subclavian artery
Clinical features
Tearing, sudden onset chest pain (painless 10%)
Hypertension or Hypotension
A blood pressure difference greater than 20 mm Hg
Neurologic deficits (20%)
Investigations
CXR: widened mediastinum, abnormal aortic knob, ring sign, deviation
trachea/oesophagus
CT (spiral)
MRI
Angiography (95% of patients diagnosed)
Management
Beta-blockers: aim HR 60-80 bpm and systolic BP 100-120 mm Hg.
Urgent surgical intervention: type A dissections. This will usually involve
aortic root replacement.
A 58 year old man undergoes an upper GI endoscopy for the investigation of
odynophagia. At endoscopy a reddish area is seen to protrude up into the oesophagus
from the gastrooesophageal junction. Which of the following pathological processes
is most likely to explain this process?
A. Metaplasia
B. Anaplasia
C. Dysplasia
D. Hypoplasia
E. Hyperplasia

This is most likely to represent Barretts oesphagus and is thus metaplasia. Dysplasia is
less likely in this setting although biopsies are mandatory.
Barrett's oesophagus
Intestinal metaplasia
Squamous epithelium replaced by columnar epithelium in the lower
oesophagus
3 types of columnar epithelium:
1. Junctional
2. Atrophic fundal
3. Specialised
Presence of goblet cells important in identification
Premalignant change (progress to dysplasia)
Risk of adenocarcinoma
Risk factors: middle age, men, smoker, Caucasian, gastro-oesophageal reflux,
obesity
Treatment
Long term proton pump inhibitor
Consider pH and manometry studies in younger patients who may prefer to
consider an anti reflux procedure
Regular endoscopic monitoring (more frequently if moderate dysplasia). With
quadrantic biopsies every 2-3 cm
If severe dysplasia be very wary of small foci of cancer
A male infant is born by emergency cesarean section at 39 weeks gestation for foetal
distress. Soon after the birth the baby becomes progressively hypoxic and on
examination is found to have a scaphoid abdomen. What is the most likely underlying
diagnosis?
A. Intestinal malrotation
B. Hiatus hernia
C. Foramen of Bochdalek hernia
D. Foramen of Morgagni hernia

E. Tracheooesphageal fistula
The finding of a scaphoid abdomen and respiratory distress suggests extensive intra
thoracic herniation of the abdominal contents. This is seen most frequently with
Bochdalek hernias. Morgagni hernias seldom present in such a dramatic fashion. The
other options do not typically present with the symptoms and signs described.
Embryology of the diaphragm and diaphragmatic hernia
Embryology The diaphragm is formed between the 5th and 7th weeks of gestation through the
progressive fusion of the septum transversum, pleuroperitoneal folds and via lateral
muscular ingrowth. The pleuroperitoneal membranes from which the diaphragm
originates originate at somites located in cervical segments 3 to 5, which accounts for
the long path taken by the phrenic nerve. The components contribute to the following
diaphragmatic segments:
Septum transversum - Central tendon
Pleuroperitoneal membranes - Parietal membranes surrounding viscera
Cervical somites C5 to C7 - Muscular component of the diaphragm
Diaphragmatic hernia
Type of hernia Features
Morgagni Anteriorly located
Minimal compromise on lung development
Minimal signs on antenatal ultrasound
Usually present later
Usually good prognosis
Bochdalek hernia Posteriorly located
Larger defect
Often diagnosed antenatally
Associated with pulmonary hypoplasia
Poor prognosis
The posterior hernias of Bochdalek are the most common type and if not diagnosed
antenatally will typically present soon after birth with respiratory distress. The
classical finding is that of a scaphoid abdomen on clinical examination because of
herniation of the abdominal contents into the chest. Bochdalek hernias are associated
with a number of chromosomal abnormalities such as Trisomy 21 and 18. Infants
have considerable respiratory distress due to hypoplasia of the developing lung.
Historically this was considered to be due to direct compression of the lung by
herniated viscera. This view over simplifies the situation and the pulmonary
hypoplasia occurs concomitantly with the hernial development, rather than as a direct
result of it. The pulmonary hypoplasia is associated with pulmonary hypertension and
abnormalities of pulmonary vasculature. The pulmonary hypertension renders infants
at risk of right to left shunting (resulting in progressive and worsening hypoxia).
Diagnostic work up of these infants includes chest x-rays/ abdominal ultrasound scans
and cardiac echo.
Surgery forms the mainstay of treatment and both thoracic and abdominal approaches
may be utilised. Following reduction of the hernial contents a careful search needs to
be made for a hernial sac as failure to recognise and correct this will result in a high
recurrence rate. Smaller defects may be primarily closed, larger defects may require a
patch to close the defect. Malrotation of the viscera is a recognised association and
may require surgical correct at the same procedure (favoring an abdominal approach).
The mortality rate is 50-75% and is related to the degree of lung compromise and age
at presentation (considerably better in infants >24 hours old).
A 72 year old lady falls and lands on her left hip. She attends the emergency
department and is given some paracetamol by the junior doctor and discharged.
Several months later she presents with ongoing pain and discomfort of the hip.
Avascular necrosis of the femoral head is suspected. Which of the following features
is least likely to be present?
A. Non union of the fracture
B. Angiogenesis at the fracture site
C. Increased numbers of fibroblasts at the fracture site
D. Osteochondritis dissecans
E. Apoptosis of osteoblasts
Apoptosis is not a feature of necrotic cell death. By this stage there would usually be
attempted repair so angiogenesis and proliferation of fibroblasts would be expected.
These cells may differentiate further to become osteoblasts which in turn will lay
down new matrix.
Avascular necrosis
Cellular death of bone components due to interruption of the blood supply,
causing bone destruction
Main joints affected are hip, scaphoid, lunate and the talus.
It is not the same as non union. The fracture has usually united.
Radiological evidence is slow to appear.
Vascular ingrowth into the affected bone may occur. However, many joints
will develop secondary osteoarthritis.
Causes P ancreatitis
L upus
A lcohol
S teroids

T rauma
I diopathic, infection
C aisson disease, collagen vascular disease
R adiation, rheumatoid arthritis
A myloid
G aucher disease
S ickle cell disease
Presentation Usually pain. Often despite apparent fracture union.
Investigation MRI scanning will show changes earlier than plain films.
Treatment In fractures at high risk sites anticipation is key. Early prompt and accurate reduction
is essential.
Non weight bearing may help to facilitate vascular regeneration.
Joint replacement may be necessary, or even the preferred option (e.g. Hip in the
elderly).
Which one of the following is least associated with the development of colorectal
cancer in patients with ulcerative colitis?
A. Unremitting disease
B. Disease duration > 10 years
C. Onset before 15 years old
D. Poor compliance to treatment
E. Disease confined to the rectum
Ulcerative colitis and colorectal cancer
Overview
risk of colorectal cancer is 10-20 times that of general population
the increased risk is mainly related to chronic inflammation
worse prognosis than patients without ulcerative colitis (partly due to delayed
diagnosis)
lesions may be multifocal

Factors increasing risk of cancer
disease duration > 10 years
patients with pancolitis
onset before 15 years old
unremitting disease
poor compliance to treatment
Which of the following statements about wound healing is false?
A. During the course of the first 2 weeks the fibrin plug is replaced by a
collagen rich mesh.
B. Scar contraction is a late feature and is mediated by myofibroblasts.
C. May be impaired when an infected foreign body is present.
D. Is more cosmetically acceptable when incisions are made parallel to
Langer's lines.
E. Has features of chronic inflammation from the beginning.
Although wounds often contain cell types (macrophages) and processes (angiogenesis) these
typically take time to occur. They are not present in the immature wound.
Wound healing
Surgical wounds are either incisional or excisional and either clean, clean contaminated or
dirty. Although the stages of wound healing are broadly similar their contributions will vary
according to the wound type.
The main stages of wound healing include:
Haemostasis
Vasospasm in adjacent vessels, platelet plug formation and generation of fibrin rich clot.
Inflammation

Neutrophils migrate into wound (function impaired in diabetes). Growth factors released, including basic fibroblast growth factor and vascular
endothelial growth factor. Fibroblasts replicate within the adjacent matrix and migrate into wound. Macrophages and fibroblasts couple matrix regeneration and clot substitution.
Regeneration
Platelet derived growth factor and transformation growth factors stimulate fibroblasts and epithelial cells.
Fibroblasts produce a collagen network. Angiogenesis occurs and wound resembles granulation tissue.
Remodeling
Longest phase of the healing process and may last up to one year (or longer). During this phase fibroblasts become differentiated (myofibroblasts) and these
facilitate wound contraction. Collagen fibres are remodeled. Microvessels regress leaving a pale scar.
The above description represents an idealised scenario. A number of diseases may distort
this process. It is obvious that one of the key events is the establishing well vascularised
tissue. At a local level angiogenesis occurs, but if arterial inflow and venous return are
compromised then healing may be impaired, or simply nor occur at all. The results of
vascular compromise are all too evidence in those with peripheral vascular disease or those
poorly constructed bowel anastomoses.
Conditions such as jaundice will impair fibroblast synthetic function and overall immunity
with a detrimental effect in most parts of healing.
Problems with scars:
Hypertrophic scars
Excessive amounts of collagen within a scar. Nodules may be present histologically
containing randomly arranged fibrils within and parallel fibres on the surface. The tissue
itself is confined to the extent of the wound itself and is usually the result of a full thickness
dermal injury. They may go on to develop contractures.
Image of hypertrophic scarring. Note that it remains confined to the boundaries of the
original wound:

Image sourced from Wikipedia
Keloid scars
Excessive amounts of collagen within a scar. Typically a keloid scar will pass beyond the
boundaries of the original injury. They do not contain nodules and may occur following even
trivial injury. They do not regress over time and may recur following removal.
Image of a keloid scar. Note the extension beyond the boundaries of the original incision:
Image sourced from Wikipedia
Drugs which impair wound healing:

Non steroidal anti inflammatory drugs Steroids Immunosupressive agents Anti neoplastic drugs
Closure
Delayed primary closure is the anatomically precise closure that is delayed for a few days but
before granulation tissue becomes macroscopically evident.
Secondary closure refers to either spontaneous closure or to surgical closure after
granulation tissue has formed.
heme: Causes of chest pain
A. Pulmonary embolism
B. Anterior myocardial infarction
C. Inferior myocardial infarction
D. Proximal aortic dissection
E. Distal aortic dissection
F. Boerhaave Syndrome
G. Mallory weiss tear
H. Perforated gastric ulcer
Please select the most likely cause of chest pain for the scenario given. Each option
may be used once, more than once or not at all.
8. A 52 year old male presents with tearing central chest pain. On examination
he has an aortic regurgitation murmur. An ECG shows ST elevation in leads
II, III and aVF.
You answered Inferior myocardial infarction
The correct answer is Proximal aortic dissection
An inferior myocardial infarction and AR murmur should raise suspicions of
an ascending aorta dissection rather than an inferior myocardial infarction
alone. Also the history is more suggestive of a dissection. Other features may
include pericardial effusion, carotid dissection and absent subclavian pulse.
9. A 52 year old male presents with central chest pain and vomiting. He has
drunk a bottle of vodka. On examination there is some mild crepitus in the
epigastric region.

Boerhaave Syndrome
The Mackler triad for Boerhaave syndrome: vomiting, thoracic pain,
subcutaneous emphysema. It commonly presents in middle aged men with a
background of alcohol abuse.
10. A 52 year old male presents with central chest pain. On examination he has
an mitral regurgitation murmur. An ECG shows ST elevation in leads V1 to
V6. There is no ST elevation in leads II, III and aVF.
Anterior myocardial infarction
The most likely diagnosis is an anterior MI. As there are no ST changes in the
inferior leads, aortic dissection is less likely.
Chest pain
Aortic dissection
This occurs when there is a flap or filling defect within the aortic intima.
Blood tracks into the medial layer and splits the tissues with the subsequent
creation of a false lumen. It most commonly occurs in the ascending aorta or
just distal to the left subclavian artery (less common). It is most common in
Afro-carribean males aged 50-70 years.
Patients usually present with a tearing intrascapular pain, which may be
similar to the pain of a myocardial infarct.
The dissection may spread either proximally or distally with subsequent
disruption to the arterial branches that are encountered.
In the Stanford classification system the disease is classified into lesions with
a proximal origin (Type A) and those that commence distal to the left
subclavian (Type B).
Diagnosis may be suggested by a chest x-ray showing a widened mediastinum.
Confirmation of the diagnosis is usually made by use of CT angiography
Proximal (Type A) lesions are usually treated surgically, type B lesions are
usually managed non operatively.
Pulmonary embolism
Typically sudden onset of chest pain, haemoptysis, hypoxia and small pleural
effusions may be present.
Most patients will have an underlying deep vein thrombosis

Diagnosis may be suggested by various ECG findings including S waves in
lead I, Q waves in lead III and inverted T waves in lead III. Confirmation of
the diagnosis is usually made through use of CT pulmonary angiography.
Treatment is with anticoagulation, in those patients who develop a cardiac
arrest or severe compromise from their PE, consideration may be given to
thrombolysis.
Myocardial infarction
Traditionally described as sudden onset of central, crushing chest pain. It may
radiate into the neck and down the left arm. Signs of autonomic dysfunction
may be present. The presenting features may be atypical in the elderly and
those with diabetes.
Diangosis is made through identification of new and usually dynamic ECG
changes (and cardiac enzyme changes). Inferior and anterior infarcts may be
distinguished by the presence of specific ECG changes (usually II, III and aVF
for inferior, leads V1-V5 for anterior).
Treatment is with oral antiplatelet agents, primary coronary angioplasty and/
or thrombolysis.
Perforated peptic ulcer
Patients usually develop sudden onset of epigastric abdominal pain, it may be
soon followed by generalised abdominal pain.
There may be features of antecendant abdominal discomfort, the pain of
gastric ulcer is typically worse immediately after eating.
Diagnosis may be made by erect chest x-ray which may show a small amount
of free intra-abdominal air (very large amounts of air are more typically
associated with colonic perforation).
Treatment is usually with a laparotomy, small defects may be excised and
overlaid with an omental patch, larger defects are best managed with a partial
gastrectomy.
Boerhaaves syndrome
Spontaneous rupture of the oesophagus that occurs as a result of repeated
episodes of vomiting.
The rupture is usually distally sited and on the left side.
Patients usually give a history of sudden onset of severe chest pain that may
complicate severe vomiting.
Severe sepsis occurs secondary to mediastinitis.
Diagnosis is CT contrast swallow.
Treatment is with thoracotomy and lavage, if less than 12 hours after onset
then primary repair is usually feasible, surgery delayed beyond 12 hours is
best managed by insertion of a T tube to create a controlled fistula between
oesophagus and skin.
Delays beyond 24 hours are associated with a very high mortality rate.

A 78 year old lady presents with a tender swelling in her right groin. On examination there is
a tender swelling that lies lateral to the pubic tubercle. It has a cough impulse. What is the
most likely underlying diagnosis?
A. Thrombophlebitis of the great saphenous vein
B. Femoral hernia
C. Thrombophlebitis of saphena varix
D. Inguinal hernia
E. Obturator hernia
Theme from April 2012 Exam
Whilst a thrombophlebitis of a saphena varix may cause a tender swelling at this site, it
would not usually be associated with a cough impulse.
Femoral canal
The femoral canal lies at the medial aspect of the femoral sheath. The femoral sheath is a
fascial tunnel containing both the femoral artery laterally and femoral vein medially. The
canal lies medial to the vein.
Borders of the femoral canal
Laterally Femoral vein
Medially Lacunar ligament
Anteriorly Inguinal ligament
Posteriorly Pectineal ligament
Image showing dissection of femoral canal

Image sourced from Wikipedia
Contents
Lymphatic vessels Cloquet's lymph node
Physiological significance
Allows the femoral vein to expand to allow for increased venous return to the lower limbs.
Pathological significance
As a potential space, it is the site of femoral hernias. The relatively tight neck places these at
high risk of strangulation.
A 3 month old boy is suspected of having hypospadias. At which of the following
locations is the urethral opening most frequently located in boys suffering from the
condition?

A. On the distal ventral surface of the penis
B. On the proximal ventral surface of the penis
C. On the distal dorsal surface of the penis
D. On the proximal dorsal surface of the penis
E. At the base of the scrotum
The defect is located ventrally and most often distally. Proximally located urethral
openings are well recognised. Circumcision may compromise reconstruction.
Hypospadias
The urethral meatus opens on the ventral surface of the penis. There is also a ventral
deficiency of the foreskin. The uretral meatus may open more proximally in the more
severe variants. However, 75% of the openings are distally located. The incidence is 1
in 300 male births.
Features include:
Absent frenular artery
Ventrally opened glans
Skin tethering to hypoplastic urethra
Splayed columns of spongiosum tissue distal to the meatus
Deficiency of the foreskin ventrally
Management:
No routine cultural circumcisions
Urethroplasty
Penile reconstruction
The foreskin is often utilised in the reconstructive process. In boys with very distal
disease no treatment may be needed.
A 52 year old male attends for a preoperative assessment for an inguinal hernia repair.
You notice that the chest x-ray shows a loculated left pleural effusion. On further
questioning the patient reports that he worked as a builder 30 years ago. What is the
most likely cause for the effusion?
A. Asbestosis
B. Pneumonia

C. Mesothelioma
D. Silicosis
E. Left ventricular failure
This patient has a risk of asbestos exposure through his occupation as a builder. As
there a is latent period of 30 years and a complicated effusion, the most likely cause is
mesothelioma.
Mesothelioma
Features
Dyspnoea, weight loss, chest wall pain
Clubbing
30% present as painless pleural effusion
Only 20% have pre-existing asbestosis
History of asbestos exposure in 85-90%, latent period of 30-40 years
Basics
Malignancy of mesothelial cells of pleura
Metastases to contralateral lung and peritoneum
Right lung affected more often than left
Management
Investigation: pleural biopsy, CT Scanning, (PET Scanning if surgery
considered)
Symptomatic
Industrial compensation
Chemotherapy, Surgery if operable
Prognosis poor, median survival 12 months
A 64-year-old woman who is reviewed due to multiple non-healing leg ulcers. She
reports feeling generally unwell for many months. Examination findings include a
blood pressure of 138/72 mmHg, pulse 90 bpm, pale conjunctivae and poor dentition
associated with bleeding gums. What is the most likely underlying diagnosis?
A. Thyrotoxicosis
B. Vitamin B12 deficiency

C. Vitamin C deficiency
D. Diabetes mellitus
E. Sarcoidosis
Bleeding gums and poor healing are suggestive of vitamin C deficiency.
Vitamin C deficiency
Vitamin C deficiency (scurvy) leads to defective synthesis of collagen resulting in
capillary fragility (bleeding tendency) and poor wound healing
Features
gingivitis, loose teeth
poor wound healing
bleeding from gums, haematuria, epistaxis
general malaise
Which of the following is not a typical feature of neuropraxia?
A. Transient delay in neuronal transmission
B. Axonal degeneration distal to the site of injury
C. Absence of neuroma formation
D. Preservation of autonomic function
E. Absence of axonal degeneration proximal to the site of injury
Full recovery may occur 6-8 weeks after nerve injury in neuropraxia.
Wallerian degeneration does not usually occur in simple neuropraxia.
Autonomic function is usually preserved.
Nerve injury
There are 3 types of nerve injury:
Neuropraxia Nerve intact but electrical conduction is affected
Full recovery
Autonomic function preserved
Wallerian degeneration does not occur
Axonotmesis Axon is damaged and the myelin sheath is preserved. The

connective tissue framework is not affected.
Wallerian degeneration occurs.
Neurotmesis Disruption of the axon, myelin sheath and surrounding
connective tissue.
Wallerian degeneration occurs.
Wallerian Degeneration
Axonal degeneration distal to the site of injury.
Typically begins 24-36 hours following injury.
Axons are excitable prior to degeneration occurring.
Myelin sheath degenerates and is phagocytosed by tissue macrophages.
Nerve repair
Neuronal repair may only occur physiologically where nerves are in direct
contact. Where a large defect is present the process of nerve regeneration is
hampered and may not occur at all or result in the formation of a neuroma.
Where nerve regrowth occurs it typically occurs at a rate of 1mm per day.
A 44 year old lady presents with a pathological fracture of the left femur. She has
previously undergone a renal transplant for end stage renal failure. Her blood test
results are as follows:
Serum Ca2+ 2.80
PTH 88pg/ml
Phosphate 0.30
A surgeon decides to perform a parathyroidectomy on the basis of these results. When
the glands are assessed histologically, which of the appearances is most likely to be
identified?
A. Metaplasia the gland
B. Hypertrophy of the gland
C. Hyperplasia of the gland
D. Parathyroid carcinoma
E. Necrosis of the parathyroid gland
This is likely to be a case of tertiary hyperparathyroidism (high Calcium, high PTH,

low phosphate). Therefore the glands will be hyperplastic. Hypertrophy is not correct
as this implies an increase in size without an increase in cellularity. This mistake has
cost many candidates marks in the MRCS exams over the years!
Parathyroid glands and disorders of calcium metabolism
Hyperparathyroidism
Disease type Hormone profile Clinical features Cause
Primary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Elevated)
Phosphate
(Low)
Serum Calcium
: Creatinine
clearance ratio
> 0.01
May be
asymptomatic if
mild
Recurrent
abdominal pain
(pancreatitis, renal
colic)
Changes to
emotional or
cognitive state
Most cases due to
solitary adenoma
(80%), multifocal
disease occurs in
10-15% and
parathyroid
carcinoma in 1% or
less
Secondary
hyperparathyroidism
PTH (Elevated)
Ca2+ (Low or
normal)
Phosphate
(Elevated)
Vitamin D
levels (Low)
May have few
symptoms
Eventually may
develop bone
disease, osteitis
fibrosa cystica and
soft tissue
calcifications
Parathyroid gland
hyperplasia occurs
as a result of low
calcium, almost
always in a setting
of chronic renal
failure
Tertiary
hyperparathyroidism
Ca2+ (Normal
or high)
PTH (Elevated)
Phosphate
levels
(Decreased or
Normal)
Vitamin D
(Normal or
decreased)
Alkaline
phosphatase
(Elevated)
Metastatic
calcification
Bone pain and /
or fracture
Nephrolithiasis
Pancreatitis
Occurs as a result
of ongoing
hyperplasia of the
parathyroid glands
after correction of
underlying renal
disorder,
hyperplasia of all 4
glands is usually
the cause
Differential diagnoses It is important to consider the rare but relatively benign condition of benign familial
hypocalciuric hypercalcaemia, caused by an autosomal dominant genetic disorder.
Diagnosis is usually made by genetic testing and concordant biochemistry (Serum
Calcium : Creatinine clearance ratio <0.01-distinguished from primary
hyperparathyroidism).
Treatment

Primary hyperparathyroidism
Indications for surgery
Elevated serum Calcium > 1mg/dL above normal
Hypercalciuria > 400mg/day
Creatinine clearance < 30% compared with normal
Episode of life threatening hypercalcaemia
Nephrolithiasis
Age < 50 years
Neuromuscular symptoms
Reduction in bone mineral density of the femoral neck, lumbar spine, or distal
radius of more than 2.5 standard deviations below peak bone mass (T score
lower than -2.5)
Secondary hyperparathyroidism Usually managed with medical therapy.
Indications for surgery in secondary (renal) hyperparathyroidism:
Bone pain
Persistent pruritus
Soft tissue calcifications
Tertiary hyperparathyroidism Usually treatment is surgical
The presence of an autonomously functioning parathyroid gland may require surgery.
If the culprit gland can be identified then it should be excised. Otherwise total
parathyroidectomy and re-implantation of part of the gland may be required.
References 1. Pitt S et al. Secondary and Tertiary Hyperparathyroidism, State of the Art Surgical
Management. Surg Clin North Am 2009 Oct;89(5):1227-39.
2. MacKenzie-Feder J et al. Primary Hyperparathyroidism: An Overview. Int J
Endocrinol 2011; 2011: 251410.
A 56 year old man presents with lethargy, haematuria and haemoptysis. On
examination he is hypertensive and has a left loin mass. A CT scan shows a lesion
affecting the upper pole of the right kidney, it has a small cystic centre. Which of the
options below is the most likely diagnosis?
A. Squamous cell carcinoma of the kidney
B. Nephroblastoma
C. Renal adenocarcinoma

D. Transitional cell carcinoma of the kidney
E. Polycystic kidney disease
Renal adenocarcinoma are the most common renal tumours. These will typically
affect the renal parenchyma. Transitional cell carcinoma will usually affect urothelial
surfaces. Nephroblastoma would be very rare in this age group. Renal
adenocarcinoma may produce cannon ball metastasis in the lung which cause
haemoptysis, this is not a feature of PKD.
Renal tumours
Renal cell carcinoma Renal cell carcinoma is an adenocarcinoma of the renal cortex and is believed to arise
from the proximal convoluted tubule. They are usually solid lesions, up to 20% may
be multifocal, 20% may be calcified and 20% may have either a cystic component or
be wholly cystic. They are often circumscribed by a pseudocapsule of compressed
normal renal tissue. Spread may occur either by direct extension into the adrenal
gland, renal vein or surrounding fascia. More distant disease usually occurs via the
haematogenous route to lung, bone or brain.
Renal cell carcinoma comprise up to 85% of all renal malignancies. Males are more
commonly affected than females and sporadic tumours typically affect patients in
their sixth decade.
Patients may present with a variety of symptoms including; haematuria (50%), loin
pain (40%), mass (30%) and up to 25% may have symptoms of metastasis.Less than
10% have the classic triad of haematuria, pain and mass.
Investigation Many cases will present as haematuria and be discovered during diagnostic work up.
Benign renal tumours are rare, so renal masses should be investigated with multislice
CT scanning. Some units will add and arterial and venous phase to the scan to
demonstrate vascularity and evidence of caval ingrowth.
CT scanning of the chest and abdomen to detect distant disease should also be
undertaken.
Routine bone scanning is not indicated in the absence of symptoms.
Biopsy should not be performed when a nephrectomy is planned but is mandatory
before any ablative therapies are undertaken.
Assessment of the functioning of the contra lateral kidney.
Management T1 lesions may be managed by partial nephrectomy and this gives equivalent
oncological results to total radical nephrectomy. Partial nephrectomy may also be
performed when there is inadequate reserve in the remaining kidney.

For T2 lesions and above a radical nephrectomy is standard practice and this may be
performed via a laparoscopic or open approach. Preoperative embolisation is not
indicated nor is resection of uninvolved adrenal glands. During surgery early venous
control is mandatory to avoid shedding of tumour cells into the circulation.
Patients with completely resected disease do not benefit from adjuvant therapy
with either chemotherapy or biological agents. These should not be administered
outside the setting of clinical trials.
Patients with transitional cell cancer will require a nephroureterectomy with
disconnection of the ureter at the bladder.
References Lungberg B et al. EAU guidelines on renal cell carcinoma: The 2010 update.
European Urology 2010 (58): 398-406.
A 34-year-old man is taken immediately to theatre with aortic dissection. You note he
is tall with pectus excavatum and arachnodactyly. His condition is primarily due to a
defect in which one of the following proteins?
A. Polycystin-1
B. Fibrillin
C. Type IV collagen
D. Type I collagen
E. Elastin
Although fibrillin is the primary protein affected (due to a defect in the fibrillin-1
gene) it should be noted that fibrillin is used as a substrate of elastin.
Marfan's syndrome
Marfan's syndrome is an autosomal dominant connective tissue disorder. It is caused
by a defect in the fibrillin-1 gene on chromosome 15 and affects around 1 in 3,000
people.
Features
tall stature with arm span to height ratio > 1.05
high-arched palate
arachnodactyly
pectus excavatum
pes planus
scoliosis of > 20 degrees

heart: dilation of the aortic sinuses (seen in 90%) which may lead to aortic
aneurysm, aortic dissection, aortic regurgitation, mitral valve prolapse (75%),
lungs: repeated pneumothoraces
eyes: upwards lens dislocation (superotemporal ectopia lentis), blue sclera,
myopia
dural ectasia (ballooning of the dural sac at the lumbosacral level)
The life expectancy of patients used to be around 40-50 years. With the advent of
regular echocardiography monitoring and beta-blocker/ACE-inhibitor therapy this has
improved significantly over recent years. Aortic dissection and other cardiovascular
problems remain the leading cause of death however.
Which of the following are not typical of Lynch syndrome?
A. It is inherited in an autosomal recessive manner
B. Affected patients are more likely to develop right colon mucinous
tumours than the general population
C. Affected individuals have an 80% lifetime risk of colon cancer
D. Endometrial cancer is seen in 80%.
E. Gastric cancers are more common
Lynch syndrome is inherited in an autosomal dominant fashion. It is characterised by
microsatellite instability in the DNA mismatch repair genes. Colonic tumours in
patients with Lynch syndrome are more likely to be right sided tumours and to be
poorly differentiated.
Genetics and surgical disease
Some of the more commonly occurring genetic conditions occurring in surgical
patients are presented here.
Li-Fraumeni Syndrome
Autosomal dominant
Consists of germline mutations to p53 tumour suppressor gene
High incidence of malignancies particularly sarcomas and leukaemias
Diagnosed when:
*Individual develops sarcoma under 45 years
*First degree relative diagnosed with any cancer below age 45 years and another
family member develops malignancy under 45 years or sarcoma at any age
BRCA 1 and 2

Carried on chromosome 17
Linked to developing breast cancer (60%) risk.
Associated risk of developing ovarian cancer (55% with BRCA 1 and 25%
with BRCA2).
Lynch Syndrome
Autosomal dominant
Develop colonic cancer and endometrial cancer at young age
80% of affected individuals with get colonic and or endometrial cancer
High risk individuals may be identified using the Amsterdam criteria
Amsterdam criteria Three or more family members with a confirmed diagnosis of colorectal cancer, one
of whom is a first degree (parent, child, sibling) relative of the other two.
Two successive affected generations.
One or more colon cancers diagnosed under age 50 years.
Familial adenomatous polyposis (FAP) has been excluded.
Gardners syndrome
Autosomal dominant familial colorectal polyposis
Multiple colonic polyps
Extra colonic diseases include: skull osteoma, thyroid cancer and epidermoid
cysts
Desmoid tumours are seen in 15%
Mutation of APC gene located on chromosome 5
Due to colonic polyps most patients will undergo colectomy to reduce risk of
colorectal cancer
Now considered a variant of familial adenomatous polyposis coli
An enthusiastic medical student approaches you with a list of questions about blood
transfusion reactions. Which of her following points is incorrect?
A. Graft versus host disease involves neutrophil
proliferation
B. Thrombocytopaenia may occur in women with a prior
pregnancy
C. IgA antibodies may cause blood pressure compromise
during transfusion
D. Hypocalcaemia can occur

E. Iron overload can be avoided by chelation therapy
Mnemonic for transfusion
reactions:
Got a bad unit
G raft vs. Host disease
O verload
T hrombocytopaenia
A lloimmunization
B lood pressure unstable
A cute haemolytic reaction
D elayed haemolytic
reaction
U rticaria
N eutrophilia
I nfection
T ransfusion associated
lung injury
GVHD results from lymphocytic proliferation. The patient's own lymphocytes are
similar to the donor's lymphocytes, therefore don't perceive them as being foreign.
The donor lymphocytes, however, sees the recipient lymphocytes as being foreign.
Therefore they proliferate causing severe complications.
Thrombocytopaenia occurs a few days after transfusion and may resolve
spontaneously.
Patients with IGA antibodies need IgA deficient blood transfusions.
Blood transfusion reactions
Immune mediated Non immune mediated
Pyrexia Hypocalcaemia
Alloimmunization CCF
Thrombocytopaenia Infections
Transfusion associated lung injury Hyperkalaemia
Graft vs Host disease
Urticaria
Acute or delayed haemolysis
ABO incompatibility
Rhesus incompatibility

Notes:
GVHD: lymphocyte proliferation causing organ failure
Transfusion associated lung injury: neutrophil mediated allergic pulmonary oedema
ABO and Rhesus incompatibility: causes acute haemolytic transfusion reaction
leading to agglutination and haemolysis
An 82 year old lady presents with a carcinoma of the caecum. Approximately what
proportion of patients presenting with this diagnosis will have synchronous lesions?
A. <1%
B. 60%
C. 50%
D. 20%
E. 5%
Synchronous colonic tumours are seen in 5% cases and all patients having a flexible
sigmoidoscopy should have completion colonoscopy if tumours or polyps are found
Synchronous lesions may occur in up to 5% of patients with colorectal cancer. A full
and complete lumenal study with either colonoscopy, CT cologram or barium enema
is mandatory in all patients being considered for surgery.
Colorectal cancer
Annually about 150,000 new cases are diagnosed and 50,000 deaths from the
disease
About 75% will have sporadic disease and 25% will have a family history
Colorectal tumours comprise a spectrum of disease ranging from adenomas
through to polyp cancers and frank malignancy.
Polyps may be categorised into: neoplastic polyps, adenomatous polyps and
non neoplastic polyps.
The majority of adenomas are polypoidal lesions, although flat lesions do
occur and may prove to be dysplastic.
Non-neoplastic polyps include hyperplastic, juvenile, hamartomatous,
inflammatory, and lymphoid polyps, which have not generally been thought of
as precursors of cancer.
Three characteristics of adenomas that correlate with malignant potential have
been characterised. These include increased size, villous architecture and
dysplasia. For this reason most polyps identified at colonoscopy should be
removed.
The transformation from polyp to cancer is described by the adenoma -
carcinoma sequence and its principles should be appreciated. Essentially

genetic changes accompany the transition from adenoma to carcinoma; key
changes include APC, c-myc, K RAS mutations and p53 deletions. A 22 year old man undergoes a splenectomy for an iatrogenic splenic injury. On the
second post operative day a full blood count is performed. Which of the following
components of the full blood count is the first to be affected ?
A. Erythrocyte count
B. Reticulocyte count
C. Eosinophil count
D. Monocyte count
E. Lymphocyte count
Theme from January 2012 Exam
The granulocyte and platelet count are the first to be affected following
splenectomy. Then reticulocytes increase. Although a lymphocytosis and
monocytosis are reported, these take several weeks to develop.
Post splenectomy blood film changes
The loss of splenic tissue results in the inability to readily remove immature or
abnormal red blood cells from the circulation. The red cell count does not alter
significantly. However, cytoplasmic inclusions may be seen e.g. Howell-Jolly bodies.
In the first few days after splenectomy target cells, siderocytes and reticulocytes will
appear in the circulation. Immediately following splenectomy a granulocytosis
(mainly composed of neutrophils) is seen, this is replaced by a lymphocytosis and
monocytosis over the following weeks.
The platelet count is usually increased and this may be persistent, oral antiplatelet
agents may be needed in some patients.
Image showing Howell Jolly bodies (arrowed)

Image sourced from Wikipedia
A 28 year old lady presents with benign cyclical mastalgia. Which of the following is
not a recognised treatment for the condition?
A. Evening primrose oil
B. Bromocriptine
C. Methotrexate
D. Danazol
E. Tamoxifen
Surgical excision of tender breast
tissue is inappropriate
Methotrexate is used for the treatment of breast cancer. Whilst the use of tamoxifen is
of benefit other agents such as flaxseed oil or evening primrose oil should be tried
first. Danazol is effective, but many women dislike the side effects.
Benign cyclical mastalgia
Benign cyclical mastalgia is a common cause of breast pain in younger females. It
varies in intensity according to the phase of the menstrual cycle. It is not associated
with point tenderness of the chest wall (more likely to be Tietze's syndrome).
The underlying cause is difficult to pinpoint, examination should focus on identifying
focal lesions (such as cysts) that may be treated to provide symptomatic benefit.
Women should be advised to wear a supportive bra. Conservative treatments include

flax seed oil and evening primrose oil. There is slightly more evidence in favor of flax
seed oil, though neither has performed much better than placebo in RCT's.
Hormonal agents such as bromocriptine and danazol may be more effective.
However, many women discontinue these therapies due to adverse effects.
A 39 year old lady has undergone surgery for breast cancer. As part of the
histopathology report the pathologist provides the surgeon with a Nottingham
Prognostic Index score of 6.4. He also states that the tumour size is 2cm. Which of the
following inferences can be made in relation to this statement?
A. The tumour is likely to be grade 1
B. Vascular invasion is present
C. Lymph node metastasis are definitely present
D. The tumour is oestrogen receptor positive
E. None of the above
A score of this value is unlikely to be reached with a grade 1 tumour and a size of
2cm. Therefore lymph node metastasis are definitely present. In addition since the
maximal score for lymph node metastasis is 3 the tumour is likely be of a higher grade
(see below). The Nottingham Prognostic Index provides no information about
oestrogen receptor status or the presence or absence of vascular invasion.
Nottingham prognostic index
The Nottingham Prognostic Index can be used to give an indication of survival. In this
system the tumour size is weighted less heavily than other major prognostic
parameters.
Calculation of NPI
Tumour Size x 0.2 + Lymph node score(From table below)+Grade score(From
table below).
Score
Lymph nodes involved Grade
1 0 1
2 1-3 2
3 >3 3
Prognosis
Score Percentage 5 year survival
2.0 to 2.4 93%

2.5 to 3.4 85%
3.5 to 5.4 70%
>5.4 50%
This data was originally published in 1992. It should be emphasised that other factors
such as vascular invasion and receptor status also impact on survival and are not
included in this data and account for varying prognoses often cited in the literature.
Reference Galea, M.H., et al., The Nottingham Prognostic Index in primary breast cancer. Breast
Cancer Res Treat, 1992. 22(3): p. 207-19.
n patients with multiple endocrine neoplasia type IIb which of the following clinical
appearances is the patient most likely to display?
A. Acromegalic facies
B. Turners type features
C. Profound kyphoscoliosis
D. Multiple bony exostoses
E. Marfanoid features
Patients with MEN IIb may display Marfanoid features. It is unclear at the present
time whether they have discrete changes in the microfibrils of elastic fibres that are
present in Marfans.
Multiple Endocrine Neoplasia
Multiple endocrine neoplasia (MEN) is inherited as an autosomal dominant disorder.
The table below summarises the three main types of MEN:
MEN type I MEN type IIa MEN type IIb
Mnemonic 'three P's':
Parathyroid (95%): Parathyroid adenoma
Pituitary (70%):
Prolactinoma/ACTH/Growth Hormone
secreting adenoma
Pancreas (50%): Islet cell
tumours/Zollinger Ellison syndrome
also: Adrenal (adenoma) and thyroid
(adenoma)
Phaeochromocytoma
Medullary thyroid
cancer (70%)
Hyperparathyroidism
(60%)
Same as MEN IIa
with addition of:
Marfanoid body
habitus
Mucosal neuromas

MENIN gene (chromosome 11)
Most common presentation =
hypercalcaemia
RET oncogene
(chromosome 10)
RET oncogene
(chromosome 10)
32 year old man undergoes an appendicectomy. A large carcinoid tumour is identified
and a completion right hemicolectomy is performed. He is well for several months
and then develops symptoms of palpitations and facial flushing. Which of the
following diagnostic markers should be requested?
A. Alpha feto protein
B. 5-Hydroxyindoleacetic acid
C. Urinary catecholamines
D. Urinary VMA measurements
E. None of the above
5 HIAA is the most commonly used diagnostic marker for carcinoid syndrome.
Carcinoid syndrome
Carcinoid tumours secrete serotonin
Originate in neuroendocrine cells mainly in the intestine (midgut-distal
ileum/appendix)
Can occur in the rectum, bronchi
Hormonal symptoms mainly occur when disease spreads outside the bowel
Clinical features - Onset: years
- Flushing face
- Palpitations
- Tricuspid stenosis causing dyspnoea
- Asthma
- Severe diarrhoea (secretory, persists despite fasting)
Investigation - 5-HIAA in a 24-hour urine collection
- Scintigraphy
- CT scan
Treatment

Octreotide
Surgical removal
Which of the following breast tumours is most commonly associated with a
risk of metastasis to the contralateral breast?
A. Invasive ductal carcinoma
B. Invasive lobular carcinoma
C. Phyllodes tumour
D. Pagets disease of the breast
E. Atypical ductal hyperplasia
Risk of metastasis to the contralateral breast is a classical feature of invasive
lobular carcinoma.
Lobular carcinoma of the breast
Lobular breast cancers are less common than their ductal counterparts. They
typically present differently, the mass is usually more diffuse and less obvious
on the usual imaging modalities of ultrasound and mammography. This is
significant since the disease may be understaged resulting in inadequate
treatment when wide local excision is undertaken.
In women with invasive lobular carcinoma it is usually safest to perform an
MRI scan of the breast, if breast conserving surgery is planned.
Lobular carcinomas are also more likely to be multifocal and metastasise to
the contralateral breast.
Lobular carcinoma in situ is occasionally diagnosed incidentally on core
biopsies. Unlike DCIS, lobular carcinoma in situ is far less strongly associated
with foci of invasion and is usually managed by close monitoring.
With respect to oncogenes which statement is false?
A. Mutations in oncogenes lead to cell survival
B. Cells with oncogene mutations are resistant to cell necrosis
C. Oncogene mutations must typically involve two allelic mutations for
biological effects to become manifest
D. May prevent cellular apoptosis
E. Include MYC mutations in the development of Burkitts Lymphoma
Tumour suppressor gene mutations tend to be recessive and thus twin allelic

mutations are required as exemplified in the Knudson two hit hypothesis in the
development of retinoblastoma. Necrosis will occur at the centre of tumours that
outgrow their blood supply and induction of angiogenesis is a key feature of tumour
progression.
Oncogenes
Oncogenes are cancer promoting genes that are derived from normal genes (proto-
oncogenes). Proto-oncogenes play an important physiological role in cellular growth.
They are implicated in the development of up to 20% of human cancers.
Proto-oncogenes may become oncogenes via the following processes:
Mutation (point mutation)
Chromosomal translocation
Increased protein expression
Only one mutated copy of the gene is needed for cancer to occur - a dominant effect
Classification of oncogenes
Growth factors e.g. Sis
Transcription factors e.g. Myc
Receptor tyrosine kinase e.g. RET
Cytoplasmic tyrosine kinase e.g. Src
Regulatory GTPases e.g. Ras
Tumour supressor genes Tumour supressor genes restrict or repress cellular proliferation in normal cells. Their
inactivation through mutation or germ line incorporation is implicated in renal,
colonic, breast, bladder and many other cancers. One of the best known tumour
supressor genes is p53. p53 gene offers protection by causing apoptosis of damaged
cells. Other well known genes include BRCA 1 and 2.
Which is the characteristic finding on a blood film post splenectomy?
A. Stipple cell
B. Tear drop cell
C. Reticulocytes
D. Howell-Jolly bodies
E. Schistocyte
Blood film in hyposplenism:

Howell-Jolly bodies
Pappenheimer bodies
Poikilocytes (Target cells)
Erythrocyte containing siderotic granules
Heinz bodies
Splenectomy
Indications
Trauma: 1/4 are iatrogenic
Spontaneous rupture: EBV
Hypersplenism: hereditary spherocytosis or elliptocytosis etc
Malignancy: lymphoma or leukaemia
Splenic cysts, hydatid cysts, splenic abscesses
Post splenectomy changes
Platelets will rise first (therefore in ITP should be given after splenic artery
clamped)
Blood film will change over following weeks, Howell Jolly bodies will appear
Other blood film changes include target cells and Pappenheimer bodies
Increased risk of post splenectomy sepsis, therefore prophylactic antibiotics
and pneumococcal vaccine should be given.
Post splenectomy sepsis
Typically occurs with encapsulated organisms
Opsonisation occurs but then not recognised


















