PULMONARY FUNCTION TESTING Pat Allan Pulmonary, CC, Sleep, NeuroCC, Int Pulmonary Medicine.

Payal Kohli, HMS IIIGillian Lieberman, MD
Mr. M: A Case Study of Pulmonary Pathology
Payal Kohli, Harvard Medical School Year IIIGillian Lieberman, MD
September 2004

2
Payal Kohli, HMS IIIGillian Lieberman, MD
LateralPACS, BIDMCPAPACS, BIDMC
Mr. M: 33 yo Kenyan M with cough and SOB
Lymphadenopathy
Lymphadenopathy

3
Payal Kohli, HMS IIIGillian Lieberman, MD
Mediastinal Lymph nodes
http://www.bartleby.com/107/illus621.html http://rad.usuhs.mil/medpix/medpix.html?mode=tsearch2#top
Patient 2: Lymphadenopathy

4
Payal Kohli, HMS IIIGillian Lieberman, MD
Differential Diagnosis for “Hilar Lymphadenopathy”
• Lymphadenitis, infectious
• Lymphoma, lymphosarcoma
• Mets (esp. undifferentiated or small cell ca of lung)
• Sarcoidosis
http://rad.usuhs.mil/medpix/medpix.html?mode=defaultPara-bronchial nodes
Sub-carinal nodes Pre-carinal
PACS, BIDMC
Mr. M: Chest CT with contrast

5
Payal Kohli, HMS IIIGillian Lieberman, MD
Sarcoidosis• Multi-system granulomatous
disease• Unknown etiology• Peaks in third decade; F>M• Can also get pleural effusions,
cor pulmonale, mycetoma, infection and pneumothorax
• Clinical, pathological and radiological diagnosis
Stage I: Stage I: LymphadenopathyLymphadenopathy
Stage II: Stage II: LymphadenopathyLymphadenopathy + + parenchymalparenchymal opacityopacity
Stage III: Stage III: ParenchymalParenchymal opacity opacity alonealone
Stage IV:Stage IV:Pulmonary fibrosisPulmonary fibrosis
http://rad.usuhs.mil/medpix/medpix.html?mode=default

6
Payal Kohli, HMS IIIGillian Lieberman, MD
Menu of tests for imaging lung in Sarcoidosis
• Plain Film and CT: Staging– hilar lymphadenopathy– parenchymal opacities/fibrotic changes
• MR: mediastinal fat and nodes• Gallium-67 scanning
– direct relationship between number of macrophages in lung during alveolitis and uptake of Gallium-67
– Non-specific, low neg. predictive value, difficult to interpret
7
Payal Kohli, HMS IIIGillian Lieberman, MD
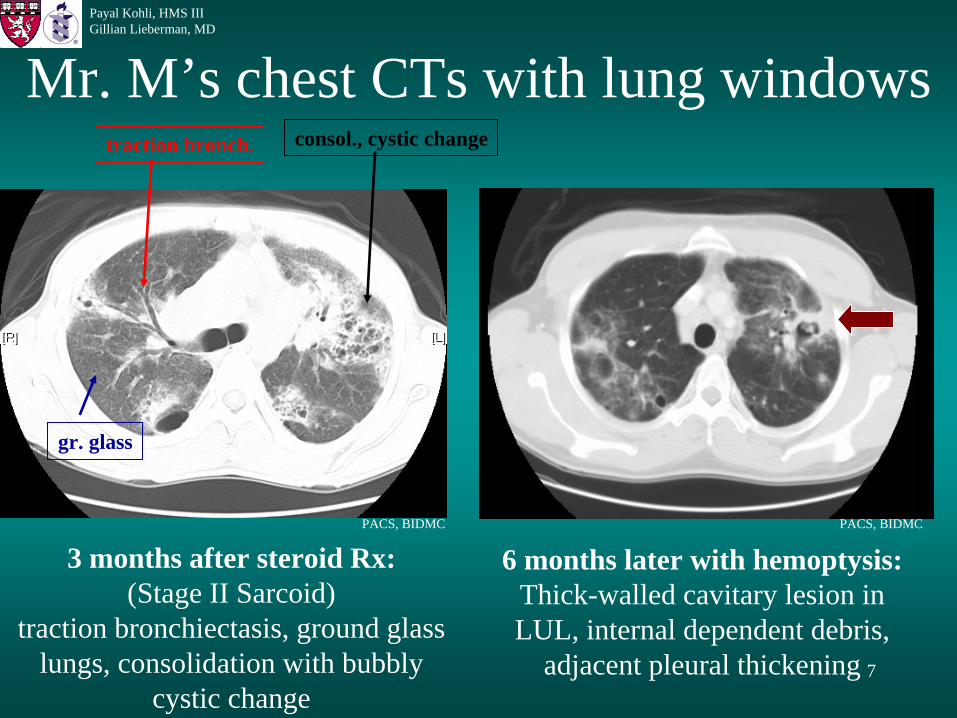
Mr. M’s chest CTs with lung windows
3 months after steroid Rx:(Stage II Sarcoid)
traction bronchiectasis, ground glass lungs, consolidation with bubbly
cystic change
traction bronch. consol., cystic change
gr. glass
PACS, BIDMC
6 months later with hemoptysis:Thick-walled cavitary lesion in LUL, internal dependent debris,
adjacent pleural thickening
PACS, BIDMC

8
Payal Kohli, HMS IIIGillian Lieberman, MD
• Infection or abscess (bacteria, mycobacteria, fungi, parasites)
• Neoplasms (bronchogenic cancer, lymphoma, mets)
• Pulmonary infarct• Septic embolism• Vasculitidies (Wegener’s granulomatosis)
DDX of cavitary lung lesion
Ryu and Swenson. Mayo Clinic Proc. 2003;78:744-752
9
Payal Kohli, HMS IIIGillian Lieberman, MD
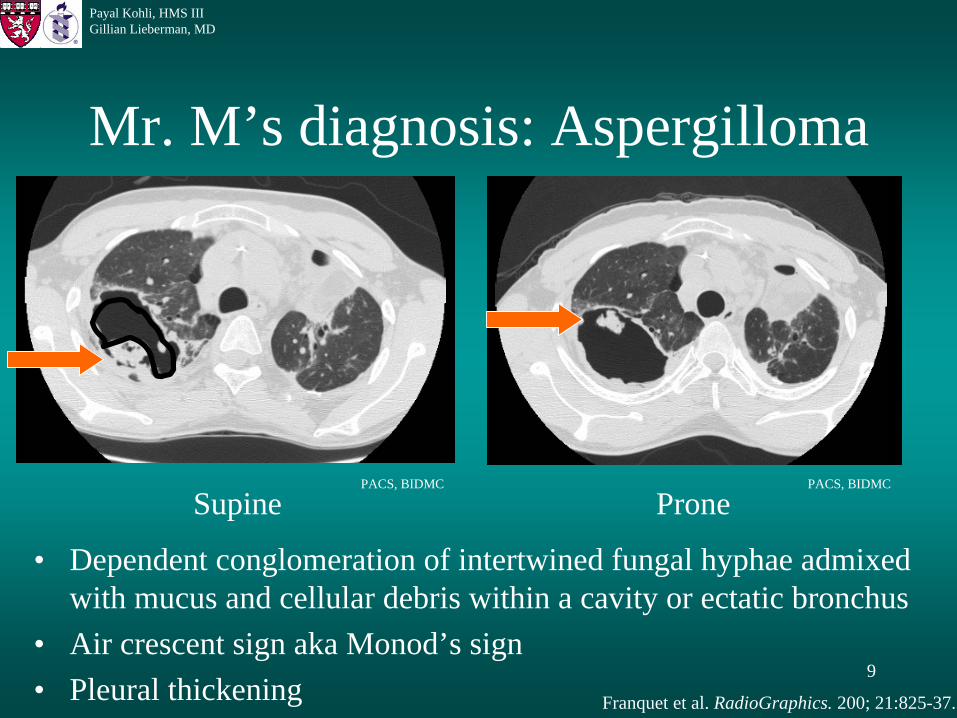
Mr. M’s diagnosis: Aspergilloma
• Dependent conglomeration of intertwined fungal hyphae admixed with mucus and cellular debris within a cavity or ectatic bronchus
• Air crescent sign aka Monod’s sign• Pleural thickening
Supine
Franquet et al. RadioGraphics. 200; 21:825-37.
PACS, BIDMC
PronePACS, BIDMC

10
Payal Kohli, HMS IIIGillian Lieberman, MD
Saprophytic Aspergillosis
Patient 3: Plain Film Patient 4: Linear Tomogram
Surgical Specimen
Dependent debris
Franquet et al. RadioGraphics. 200; 21:825-37.
11
Payal Kohli, HMS IIIGillian Lieberman, MD
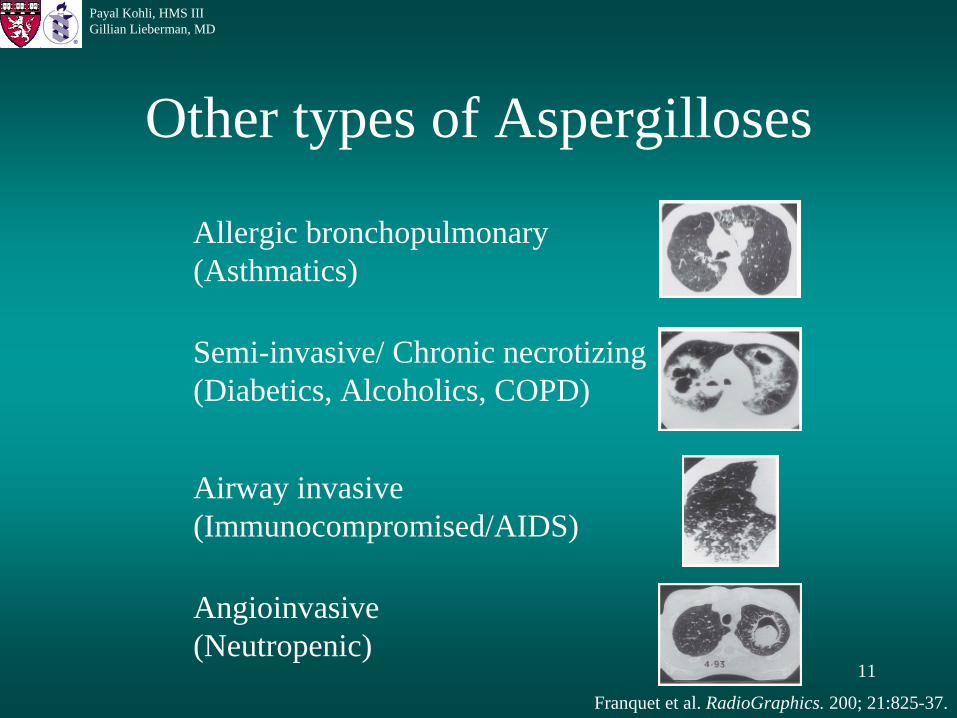
Other types of Aspergilloses
Allergic bronchopulmonary(Asthmatics)
Semi-invasive/ Chronic necrotizing(Diabetics, Alcoholics, COPD)
Airway invasive(Immunocompromised/AIDS)
Angioinvasive(Neutropenic)
Franquet et al. RadioGraphics. 200; 21:825-37.

12
Payal Kohli, HMS IIIGillian Lieberman, MD
Treatment of Aspergilloma
• Primary: Surgical intervention• Secondary:
– anti-fungal therapy• Systemic Itraconazole• Topical Amphoterecin B (CT-guided)• Limited efficacy
– Bronchial artery embolization for hemoptysis
Sugar, A. “Aspergilloma”. UptoDate. 2004.

13
Payal Kohli, HMS IIIGillian Lieberman, MD
Back to Mr. M…
• Presented with cough, SOB sarcoidosis• Developed left upper lobe aspergilloma
left upper lobectomy• Developed right upper lobe aspergilloma
right main bronchial artery embolization• Right upper lobectomy

14
Payal Kohli, HMS IIIGillian Lieberman, MD
Mr. M: Another complication…
Pneumothorax with pleural effusion
PA Plain Film
tracheal deviation
blunted costophrenic
angle
Pleural outline
PACS, BIDMC CT w/o contrast PACS, BIDMCpleural efffusion
pneumothorax
15
Payal Kohli, HMS IIIGillian Lieberman, MD
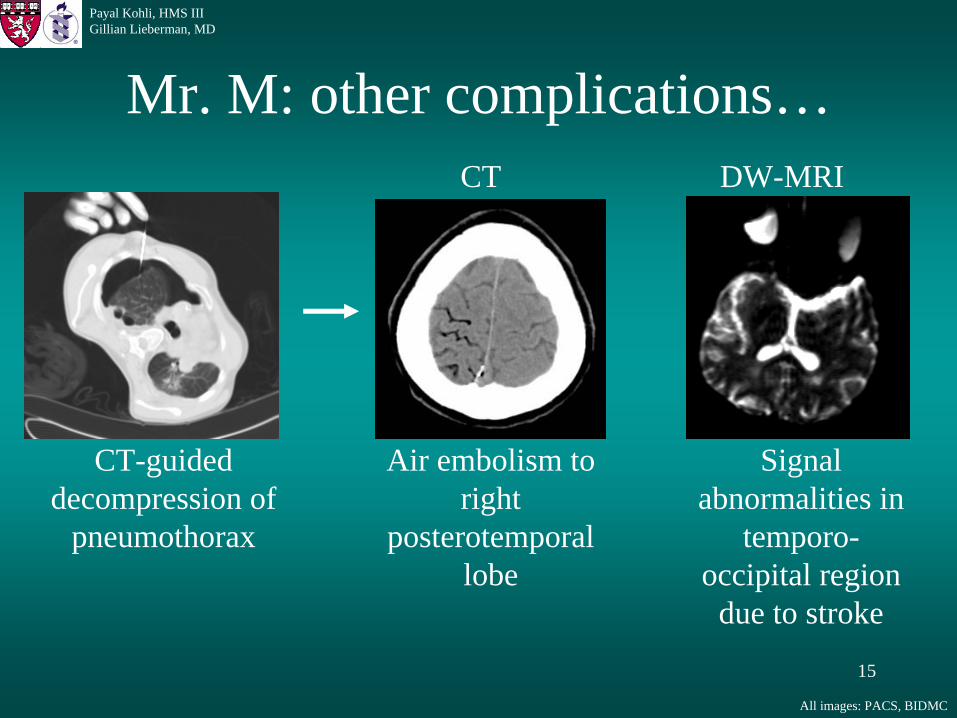
Mr. M: other complications…
CT-guided decompression of
pneumothorax
Air embolism to right
posterotemporal lobe
CT DW-MRI
Signal abnormalities in
temporo- occipital region
due to stroke
All images: PACS, BIDMC

16
Payal Kohli, HMS IIIGillian Lieberman, MD
Radiological care of Mr. M, a patient with sarcoidosis
Screened and followed with …– Doppler U/S of carotids and femorals to detect for
thrombus formation– MRA of Circle of Willis to detect embolic events– CT of maxillofacial sinuses to evaluate for infection– Routine (monthly) chest CTs and plain films for
staging of sarcoidosis and screening for infections

17
Payal Kohli, HMS IIIGillian Lieberman, MD
References
• Franquet T, Muller N, Gimenez A, Guembe P, de la Torre J, Bague S. Spectrum of Pulmonary
Aspergillosis: Histologic, Clinical, and Radiologic Findings. RadioGarphics. 2001; 21: 825-837.
• http://www.bartleby.com/107/illus621.html
• http://rad.usuhs.mil/medpix/medpix.html?mode=tsearch2#top
• Reeder, M. Reader’s & Felson’s Gamuts in Radiology, 4th ed. New York: Springer-Verlag,
2003.
• Ryu and Swenson. Mayo Clinic Proc. 2003;78:744-752.
• Sugar, A. “Aspergilloma”. UptoDate. 2004.

18
Payal Kohli, HMS IIIGillian Lieberman, MD
Acknowledgements
Many thanks to…• Damon Soeiro, MD• Erik Stien, MD• Mizuki Nishino, MD• Gillian Lieberman, MD• Pamela Lepkowski• Larry Barbaras, our Webmaster