
An Atlas of Imaging Findings in Pulmonary and...
51
An Atlas of Imaging Findings in Pulmonary and Gastrointestinal Tuberculosis Stanley Kim University of Maryland School of Medicine, MS-IV Gillian Lieberman, MD Stanley Kim, MS-IV Gillian Lieberman, MD September 2015
Transcript of An Atlas of Imaging Findings in Pulmonary and...

An Atlas of Imaging Findings in Pulmonary and Gastrointestinal Tuberculosis Stanley Kim University of Maryland School of Medicine, MS-IV Gillian Lieberman, MD
Stanley Kim, MS-IV Gillian Lieberman, MD
September 2015

Agenda • Patient Presentation • Overview of Tuberculosis
• Epidemiology • Evaluation of Pulmonary and Gastrointestinal TB
• Radiographic Appearance • Pulmonary TB
• Primary • Post-Primary • Miliary
• Gastrointestinal TB • Management • Patient Clinical Course • Summary
2
Stanley Kim, MS-IV Gillian Lieberman, MD

HPI: • 56 year old male presenting with two months of loss of
appetite and weight loss and approximately three weeks of nausea, vomiting, and abdominal pain
• Found to have positive QuantiFERON-TB Gold and caseating granulomas on colonoscopy at an outside hospital
• Visiting from South America Social: • Former healthcare worker
Our Patient: History
3
Stanley Kim, MS-IV Gillian Lieberman, MD

Our Patient: Chest X-ray
AP portable chest x-ray: Distended loops of bowel.
PACS, UMMC
4
*
Stanley Kim, MS-IV Gillian Lieberman, MD

AP portable chest x-ray: Opacity in left lung near lingula. Bilateral pleural effusions.
Our Patient: Chest X-ray
PACS, UMMC
5
Stanley Kim, MS-IV Gillian Lieberman, MD

C- coronal chest CT: Multiple nodules in right upper lobe.
Our Patient: Chest CT
PACS, UMMC
6
Stanley Kim, MS-IV Gillian Lieberman, MD

C- axial chest CT: Tree-in-bud pattern in right upper lobe.
Our Patient: Chest CT
PACS, UMMC
7
Stanley Kim, MS-IV Gillian Lieberman, MD

C- axial chest CT: Patchy consolidation in lingula. Bilateral opacities in posterior lungs indicating atelectasis, abutting pleural effusions.
Our Patient: Chest CT
PACS, UMMC
8
Stanley Kim, MS-IV Gillian Lieberman, MD

C+ axial abdomen/pelvis CT: Bowel wall thickening in hepatic flexure of colon, consistent with colitis.
Our Patient: Abdomen CT
PACS, UMMC
9
Stanley Kim, MS-IV Gillian Lieberman, MD

C+ axial abdomen/pelvis CT: Inflammation in terminal ileum and cecum.
Our Patient: Abdomen CT
PACS, UMMC
10
Stanley Kim, MS-IV Gillian Lieberman, MD

Differential Diagnosis Tuberculosis Crohn’s disease Sarcoidosis Lymphoma
11
Stanley Kim, MS-IV Gillian Lieberman, MD

Differential Diagnosis
12
Tuberculosis Crohn’s disease Chest radiograph Positive chest film
(50%) Negative chest film
Barium Fleischner sign Cobblestone mucosa
CT No creeping fat Creeping fat Omental and peritoneal thickening
Normal omentum and peritoneum
Enlarged low density nodes
Enlarged soft tissue density nodes
Distinguishing Tuberculosis from Crohn’s on Imaging:
Source: http://www.isradiology.org/goed_tb_project/im-library/ECR2010_C-1658.pdf
Stanley Kim, MS-IV Gillian Lieberman, MD

Differential Diagnosis Tuberculosis, with both pulmonary and GI involvement • Positive QuantiFERON-TB Gold • Caseating granulomas on colonoscopy • Imaging consistent with infectious process • Inhabitance in endemic region Crohn’s disease • Rarely affects lungs • Tree-in-bud pattern more consistent with infectious than
inflammatory process • Presents with non-caseating, rather than caseating granulomas Sarcoidosis • Not consistent with +QuantiFERON-TB Gold or caseating
granulomas Lymphoma • Tree-in-bud pattern and bowel wall thickening less consistent with
lymphoma • Not consistent with +QuantiFERON-TB Gold 13
Stanley Kim, MS-IV Gillian Lieberman, MD

Differential Diagnosis Tuberculosis, with both pulmonary and GI involvement • Positive QuantiFERON-TB Gold • Caseating granulomas on colonoscopy • Imaging consistent with infectious process • Inhabitance in endemic region Crohn’s disease • Rarely affects lungs • Tree-in-bud pattern more consistent with infectious than
inflammatory process • Presents with non-caseating, rather than caseating granulomas Sarcoidosis • Not consistent with +QuantiFERON-TB Gold or caseating
granulomas Lymphoma • Tree-in-bud pattern and bowel wall thickening less consistent with
lymphoma • Not consistent with +QuantiFERON-TB Gold 14
Stanley Kim, MS-IV Gillian Lieberman, MD

Agenda • Patient Presentation • Overview of Tuberculosis
• Epidemiology • Evaluation of Pulmonary and Gastrointestinal TB
• Radiographic Appearance • Pulmonary TB
• Primary • Post-Primary • Miliary
• Gastrointestinal TB • Management • Patient Clinical Course • Summary
15
Stanley Kim, MS-IV Gillian Lieberman, MD

Epidemiology • Annually:
• 9 million new cases • 1.5 million deaths • 9,500 cases reported in
U.S. • Caused by M. tuberculosis • Transmitted through
respiratory fluids • Classic symptoms
• Fever • Night sweats • Cough • Weight loss
• Can impact nearly every organ system
Source: www.natureworldnews.com
16
Stanley Kim, MS-IV Gillian Lieberman, MD

Evaluation • Pulmonary:
• Acid-fast bacilli smear, sputum culture, CXR • PPD, IGRA (eg, QuantiFERON Gold, T-SPOT) • Chest CT is more sensitive than chest x-ray for
diagnosis, due to its ability to identify smaller nodules and abnormalities
• Gastrointestinal: • Biopsy
• Caseating granulomas • Imaging
• Non-specific findings • CT is the imaging modality of choice
17
Stanley Kim, MS-IV Gillian Lieberman, MD

Evaluation
Proposed algorithm for diagnosis of abdominal TB Source: Sood et al., 2007.
18
Stanley Kim, MS-IV Gillian Lieberman, MD

Agenda • Patient Presentation • Overview of Tuberculosis
• Epidemiology • Evaluation of Pulmonary and Gastrointestinal TB
• Radiographic Appearance • Pulmonary TB
• Primary • Post-Primary • Miliary
• Gastrointestinal TB • Management • Patient Clinical Course • Summary
19
Stanley Kim, MS-IV Gillian Lieberman, MD

Pulmonary TB • Primary vs. post-primary TB are often difficult to
distinguish with imaging due to overlapping characteristics
• Features seen in primary vs. post-primary TB: • Primary TB
• Often normal imaging • Hilar and/or mediastinal lymphadenopathy • Pleural effusions • Focal consolidation, affecting any lobe
• Post-primary TB • Usually abnormal imaging • Consolidation, nodular opacities in
apical/posterior segments of upper lobes, superior segment of lower lobes
• Cavitary lesions 20
Stanley Kim, MS-IV Gillian Lieberman, MD

Let’s view three companion patients with findings indicative of primary tuberculosis.
21
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #1: Primary TB
Often non-specific findings, like patchy opacities
Source: Frank Gaillard, MD. Radiopaedia.
22
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #2: Primary TB
23
Consolidation may mimic bacterial pneumonia
Source: Tara Catanzano, MD. Medscape.
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #3: Primary TB
May observe Ghon lesion (calcified granuloma), or Ranke complex (Ghon lesion with calcified hilar node)
Source: William Herring, MD. Learning Radiology.
24
Stanley Kim, MS-IV Gillian Lieberman, MD

Let’s view three companion patients with findings suggestive of post-primary tuberculosis.
25
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #4: Post-Primary TB
Cavitary lesions may occur (chest x-ray)
Source: Hani Al Salam, MD. Radiopaedia.
26
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #5: Post-Primary TB
Cavitary lesions may occur (chest CT)
27
Source: Natalie Yang, MD. Radiopaedia.
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #6: Chest X-ray • 70 year old male presenting
with weight loss and 2.5 wks of productive cough
• History of treated TB • Chest X-ray:
• Cavitary left apical lung mass
• Differential diagnosis • Post-primary TB • Mycetoma • Neoplasm
PACS, BIDMC
28
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #6: Chest CT • CT advised for further
evaluation • Sputum and
bronchoscopy: • Negative for TB • Positive for aspergillus
Demonstrates importance of both clinical and radiologic information in diagnosis
PACS, BIDMC
29
Stanley Kim, MS-IV Gillian Lieberman, MD

Let’s view two companion patients with findings of miliary tuberculosis.
30
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #7: Miliary TB
• Can occur with either primary or post-primary TB, although more common with primary
• Randomly distributed nodules
Source: Mark Holland, MD. Radiopaedia.
31
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #8: Chest X-ray • 31 year old male
presenting with fever, mild dyspnea, 3-4 weeks of non-productive cough
• Chest X-ray: • Superior mediastinal
mass • CT revealed bilateral
lymphadenopathy and tree-in-bud opacities
• Mediastinoscopy, lymph node biopsy, bronchoscopy: AFB+
• Started RIPE treatment 32
PACS, BIDMC
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #8: Chest CT
33
• Patient found to have isoniazid resistance • Follow-up CT: new, diffuse random small nodules
consistent with hematogenous spread (miliary TB)
PACS, BIDMC
Stanley Kim, MS-IV Gillian Lieberman, MD

Agenda • Patient Presentation • Overview of Tuberculosis
• Epidemiology • Evaluation of Pulmonary and Gastrointestinal TB
• Radiographic Appearance • Pulmonary TB
• Primary • Post-Primary • Miliary
• Gastrointestinal TB • Management • Patient Clinical Course • Summary
34
Stanley Kim, MS-IV Gillian Lieberman, MD

Gastrointestinal TB • Abdominal involvement may occur through:
• Ingestion • Hematogenous spread • Lymphatics • Nearby infected foci
• Gastrointestinal TB is rare • Increased frequency in high-risk individuals (eg,
immunosuppressed) • May impact any area of the GI tract
• Especially: • Ileocecal valve • Terminal ileum • Cecum
• Ileocecal area is involved in nearly 80-90% of cases 35
Stanley Kim, MS-IV Gillian Lieberman, MD

Gastrointestinal TB • Plain radiograph
• Dilated bowel loops caused by obstruction • Signs of perforation
• CT • Bowel wall thickening • Lymphadenopathy • Low attenuated areas suggesting caseous necrosis • Strictures
• Barium studies • Mucosal involvement (eg, ulcers) • Fleischner sign – thickening or widening of the
ileocecal valve with narrowed terminal ileum • Stierlin sign – narrowing of terminal ileum with rapid
emptying into a diminished cecum 36
Stanley Kim, MS-IV Gillian Lieberman, MD

Let’s view five companion patients with findings of gastrointestinal tuberculosis on different modalities.
37
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #9: Abdomen X-ray • Plain radiograph
• Dilated bowel loops caused by obstruction
• Signs of perforation
Source: Jeremy Jones, MD. Radiopaedia.
38
Stanley Kim, MS-IV Gillian Lieberman, MD
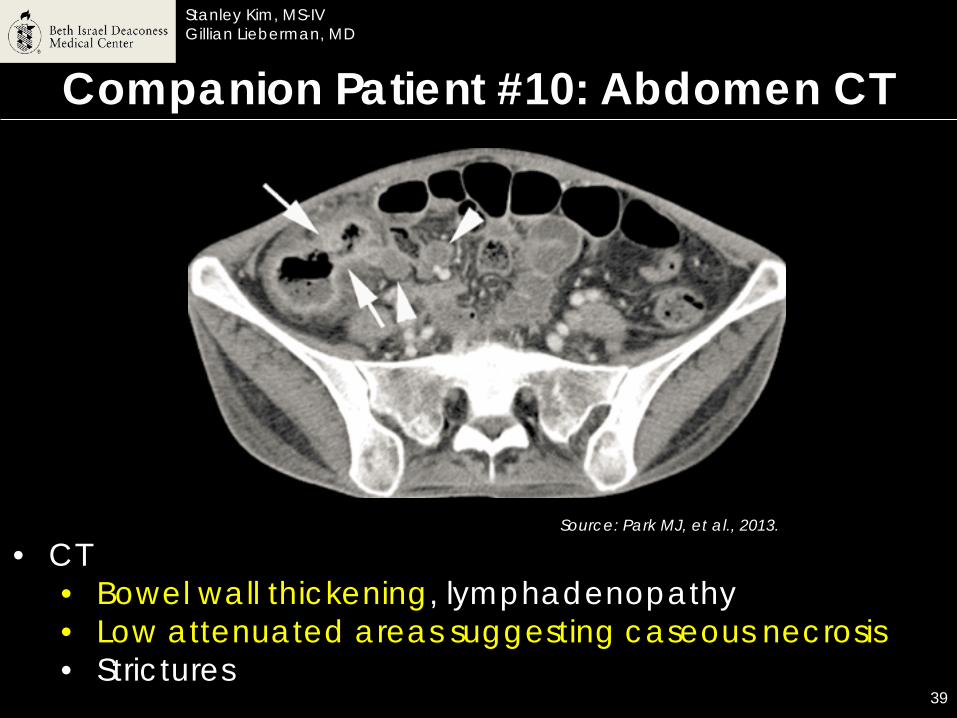
Companion Patient #10: Abdomen CT
• CT • Bowel wall thickening, lymphadenopathy • Low attenuated areas suggesting caseous necrosis • Strictures
Source: Park MJ, et al., 2013.
39
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #11: Barium Study
40
Source: Eisenberg, 1990.
• Barium studies • Stierlin sign
• Narrowing of terminal ileum with rapid emptying into a diminished cecum
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #12: Barium Study
Thickened, incompetent ileocecal valve 41
Source: Burrill J, et al., 2007.
Stanley Kim, MS-IV Gillian Lieberman, MD

Companion Patient #13: Barium Study
42
Source: Aditya Shetty, MD. Radiopaedia.
1
2
3
Small cecum (1), narrowed terminal ileum (2), and dilated proximal ileum (3)
Stanley Kim, MS-IV Gillian Lieberman, MD

Agenda • Patient Presentation • Overview of Tuberculosis
• Epidemiology • Evaluation of Pulmonary and Gastrointestinal TB
• Radiographic Appearance • Pulmonary TB
• Primary • Post-Primary • Miliary
• Gastrointestinal TB • Management • Patient Clinical Course • Summary
43
Stanley Kim, MS-IV Gillian Lieberman, MD
Management • Most patients: 6 month empiric treatment
• 2 months – Rifampin, Isoniazid, Pyrazinamide, Ethambutol (RIPE)
• 4 months – Rifampin, Isoniazid • Latent TB:
• Isoniazid daily for 9 months • Multi-drug resistant tuberculosis:
• Combination therapy • Surgical resection, if poor prognosis
44
Stanley Kim, MS-IV Gillian Lieberman, MD

Agenda • Patient Presentation • Overview of Tuberculosis
• Epidemiology • Evaluation of Pulmonary and Gastrointestinal TB
• Radiographic Appearance • Pulmonary TB
• Primary • Post-Primary • Miliary
• Gastrointestinal TB • Management • Patient Clinical Course • Summary
45
Stanley Kim, MS-IV Gillian Lieberman, MD

Our Patient: Clinical Course • After being diagnosed with gastrointestinal tuberculosis,
our patient was treated with rifampin, isoniazid, pyrazinamide, and ethambutol
• Although several AFB smears returned negative, the decision to forgo bronchoscopy was made because RIPE therapy had already been initiated and bronchoscopy findings would not change management
• Our patient was discharged from the hospital with follow-up arranged in his home country
46
Stanley Kim, MS-IV Gillian Lieberman, MD

Agenda • Patient Presentation • Overview of Tuberculosis
• Epidemiology • Evaluation of Pulmonary and Gastrointestinal TB
• Radiographic Appearance • Pulmonary TB
• Primary • Post-Primary • Miliary
• Gastrointestinal TB • Management • Patient Clinical Course • Summary
47
Stanley Kim, MS-IV Gillian Lieberman, MD

Summary • You learned how to distinguish tuberculosis from
Crohn’s disease on imaging • You learned about the most appropriate imaging
modalities for pulmonary and gastrointestinal TB • You were shown images demonstrating findings of
primary, post-primary, and miliary tuberculosis and learned distinguishing features of each
• You learned about gastrointestinal TB and its predilection for the ileocecal area
• You were shown findings of gastrointestinal TB on different imaging modalities and learned about its characteristic features
• You briefly learned about the management of tuberculosis
48
Stanley Kim, MS-IV Gillian Lieberman, MD
• Al Salam H. Pulmonary Tuberculosis. Radiopaedia website. http://radiopaedia.org/cases/pulmonary-tuberculosis-2. Accessed 9/10/15.
• Burrill J, Williams CJ, Bain G, et al. Tuberculosis: a radiologic review. Radiographics. 2007; 27(5):1255-73.
• Catanzano TM. Primary Tuberculosis Imaging. Medscape website. http://emedicine.medscape.com/article/358610-overview#a2. July 30, 2013. Accessed 9/9/15.
• da Rocha EL, Pedrassa BC, Bormann RL, et al. Abdominal tuberculosis: a radiological review with emphasis on computed tomography and magnetic resonance imaging findings. Radiol Bras. 2015; 48(3):181-91.
• Debi U, Ravisankar V, Prasad KK, et al. Abdominal tuberculosis of the gastrointestinal tract: revisited. World J Gastroenterol. 2014; 20(40):14831-40.
• Eisenberg RL. Gastrointestinal Radiology: A Pattern Approach. 2nd ed. Philadelphia, PA: J.B. Lippincott Company; 1990.
• Engin G, Acunaş B, Acunaş G, et al. Imaging of extrapulmonary tuberculosis. Radiographics. 2000; 20(2):471-88.
• Gaillard F. Pulmonary tuberculosis – on chest radiograph. Radiopaedia website. http://radiopaedia.org/cases/pulmonary-tuberculosis-on-chest-radiograph. Accessed 9/9/15.
• Herring W. Pulmonary Tuberculosis. Learning Radiology website. http://learningradiology.com/lectures/chestlectures/Pulmonary%20Tuberculosis-2012/Pulmonary%20Tuberculosis-2012.html. Accessed 9/11/15.
• Holland M. Miliary Tuberculosis. Radiopaedia website. http://radiopaedia.org/cases/miliary-tuberculosis-5. Accessed 9/10/15.
• Jones J. Tuberculosis with small bowel obstruction. Radiopaedia website. http://radiopaedia.org/cases/tuberculosis-with-small-bowel-obstruction. Accessed 9/7/15.
References
49
Stanley Kim, MS-IV Gillian Lieberman, MD

• Leder RA, Low VH. Tuberculosis of the abdomen. Radiol Clin North Am. 1995; 33(4):691-705. • Leung AN. Pulmonary tuberculosis: the essentials. Radiology. 1999; 210(2):307-22. • McAdams HP, Erasmus J, Winter JA. Radiologic manifestations of pulmonary tuberculosis. Radiol
Clin North Am. 1995; 33(4):655-78. • Park MJ, Lim JS. Computed tomography enterography for evaluation of inflammatory bowel
disease. Clin Endosc. 2013; 46(4):327-66. • Shetty A. Ileocaecal tuberculosis. Radiopaedia website.
http://radiopaedia.org/cases/ileocaecal-tuberculosis-1. Accessed 9/7/15. • Sood R, Sethu Madhavan M. Diagnostic approach to abdominal tuberculosis. In: Agarwal AK,
Jain DG, editors. Clinical Medicine: A Practical manual for students and practitioners. India: Jaypee Brothers Medical Publishers Ltd, 2007: 249.
• Stallard B. Researchers Barcode Tuberculosis. Nature World News website. http://www.natureworldnews.com/articles/8903/20140905/researchers-barcode-tuberculosis.htm. September 2014. Accessed 9/9/15.
• Vanhoenacker FM, De Backer AI, Op de BB, et al. Imaging of gastrointestinal and abdominal tuberculosis. Eur Radiol 2004; 14 Suppl 3: E103-E115.
• WHO. Global Tuberculosis Report 2014. World Health Organization, Geneva; 2014. http://apps.who.int/iris/bitstream/10665/137094/1/9789241564809_eng.pdf. Accessed 9/9/15.
• Williams AL, Stockley H, Filobbos R, et al. A pictorial review of the imaging findings in abdominal tuberculosis. The International Society of Radiology website: http://www.isradiology.org/goed_tb_project/im-library/ECR2010_C-1658.pdf. March 2010. Accessed 9/9/15.
• Yang N. Pulmonary Tuberculosis. Radiopaedia website. http://radiopaedia.org/cases/pulmonary-tuberculosis-6. Accessed 9/10/15.
References
50
Stanley Kim, MS-IV Gillian Lieberman, MD

Thank you to all the BIDMC faculty, residents, and staff who made this a wonderful rotation! A special thank you to: • Gillian Lieberman, MD and Katie Armstrong • Ronald Eisenberg, MD • Matt Miller, MD • Robert Pugatch, MD
Acknowledgements
51
Stanley Kim, MS-IV Gillian Lieberman, MD





![Intrapulmonary Lymph Nodes:Thin-Section CT … Lymph Nodes:Thin-Section CT Findings, Pathological Findings,and CT Differential Diagnosis from Pulmonary Metastatic ... shadows[3-10],and](https://static.fdocuments.in/doc/165x107/5acbaebf7f8b9a73128bf3e4/intrapulmonary-lymph-nodesthin-section-ct-lymph-nodesthin-section-ct-findings.jpg)












