
Moore County Hospital District Education Department · Moore County Hospital District Education...
43
MCHD Critical Care Drips Meds and Procedures Moore County Hospital District Education Department
Transcript of Moore County Hospital District Education Department · Moore County Hospital District Education...

MCHD Critical Care Drips Meds and Procedures
Moore County Hospital District Education Department

Dopamine • Increases systolic and diastolic BP • 400 mg in 250 cc D5W 1600 mcg/ml (pre-mixed bag) • Initial Infusion 1-5 mcg/kg/min • Maintenance Infusion rate 5-20 mcg/kg/min • Maximum Infusion Rate rarely > 25mcg/kg/min • For renal perfusion, titrate infusion by 1-4 mcg/kg/min Q 10-30 min until desired response is achieved (physician usually orders rate for renal perfusion) maintenance dosage. • Ml/hr rate chart in drip book in ICU or ED 250ml ?mcg kg 1 mg 60 min ml 400 mg kg/min 1 1000 mcg 1 hr hr

Dobutamine • Positive inotrope to increase cardiac output3 • Dilution: 250mg in 250 ml o D5W = 1mg/ml • Initial dose 2.5-10 mcg/kg/minute • Titrate to desired response • Max 40 mcg/kg/minute • Monitor BP q 15 min • Maintain parameters ordered by physician • Do not mix with Sodium Bicarbonate injection , is incompatible with Dobutamine • Use with caution in patients allergic to sulfites • Administer in largest vein possible such as antecubital vein
Lidocaine • Prophylaxis and treatment for suppression of ventricular arrhythmias (PVC’s and Ventricular tachycardia). • 2 Grams in 500 ml of D5W for 4mg/ml (pre-mixed bag) • Bolus 1-1.5 mg/kg IV push over 2 minutes • May give 0.5-0.75 mg/kg q 5-10 minutes total dose not to exceed 3mg/kg. • Maintenance infusion 1mg/min= 15 cc/hr, 2 mg/min = 30 cc/hr, 3mg min = 45 cc/hr, 4 mg/min = 60 cc/hr • Note 60 cc/hr is not recommended. • Side Effects: Confusion, tremors, stupor, lightheadedness, seizures, hypotension, double vision, worsening arrhythmias.

Amiodarone • For stable VT, a Fib • Stocked as Nexterone in 150 mg premix for loading dose and 360 mg premix for infusion. • Administer loading bolus over 10 min • Begin infusion at 1mg per minute or 33.3 ml/hr for 6 hours, • After 6 hours reduce rate to 0.5 mg/min or 16ml/hr for 18 hours for maintenance. • Use an in-line filter for infusions • Monitor rhythm, vitals , and for edema in hands and feet • Monitor for pulmonary toxicity

Cardizem • Add 125 mg (25 ml) of Cardizem to 100 ml of NS or D5W to make a solution with a concentration of 1mg/ml. • Initial dosage: 0.25mg/kg over 2 minutes • If desired response is not achieved in 15 min, then administer 2nd dose at 0.35mg/kg over 2 minutes. • Maintenance Dosage: 5-10 mg/hr, increase in 5mg/hr increments up to a maximum of 15mg/hr • Piggyback into lowest port of main line of NS • Change solution every 24 hours • Infuse through separate line due to many incompatibilities • Patient will be monitored in ICU for arrhythmias & hypotension

Epinephrine • Vasopressor • Administer in a large vein • Dilution: 2mg in 250 ml NS or D5W • Concentration: 8mcg/ml • Initial Dose: 1 mcg/minute • Extravasation management: Use phentolamine as antidote. Mix 5 mg with 9 ml NS. Inject a small amount of this dilution into extravasated area. Blanching should reverse immediately. If blanching should occur, additional injections of phentolamine may be needed.

Norepinephrine, (levophed) • 4 mg in 250 ml D5W for 16 mcg/ml • Initial Dose: 8-12 mcg/min, dose can go up to 3 mcg/kg/min in
sepsis patients. • Maintenance Dose: 2-4 mcg/min , Titrate to maximum of 30 mcg/ min. • Should be administered in a large vein such as an AC • Requires infusion pump • Monitor vitals, especially BP • For extravasation, apply warm compress or use nitroglycerin 1 inch to site, may also inject 0.5 ml terbutaline Sub q to affected area.

Fosphenytoin (cerebyx) • Anti-epileptic • 1000 mg in 100 ml NS • Remove 20 ml from NS bag, add 20ml of Fosphenytoin • Usual Dose: Expressed in phenytoin equivalents (PE) 15-20 mg PE/kg at a rate not exceed 150 PE/min Given usually over 20-30 minutes Maintenance doses of 4-6 mg PE/kg/day IV may follow • Infuse in large vessel • Place patient on cardiac monitor during infusion • Ensure patency of IV cathater • Y site compatibility lorazepam, phenobarbital

Heparin • 25,000 units in 250cc D5W for 100u/cc • Administration: bolus followed by infusion • Contraindications: bleeding abnormalities, vitamin K deficiency, severe hepatic renal disease, severe HTN • Side effects: hemorrhage, nausea/vomiting, headaches • Determine baseline PTT prior to initiating therapy • Monitor for headache, abdominal or back pain use an electric razor, avoid IM injections. • Assess for hematuria and occult blood in stool 250 ml # units ml 25,000 u hr hr

Insulin • Dilution: Regular Human Insulin 100 units in 100 ml NS • Concentration: 1 unit/ml • Administration: Piggy back into lowest port of main line NS • Change solution every 24 hours • Initial Dose: 10-30 units IV per physicians orders. • Maintenance Dose: 2-12 units/hour for correction of hyperglycemia. Units/hr = ml/hr ( 5 units/hr = 5 ml/hr) • Must be verified by 2 nurses • Hourly accuchecks • Monitor for S/S of hypo and hyper glycemia.

Labetalol • Anti-hypertensive • 200 mg in 160 ml of D5W (200 ml total volume) for 1 mg/ml. • Remove 90 ml from D5W 250 ml bag , Add 40 ml (200 mg) of labetalol to make a total volume of 200 ml • Bolus :20 mg over 2 min q 10 minutes until desired BP achieved or to max of 300 mg administered. • Continuous drip: 2mg/min (120ml/hr) titrate rate per BP response or max of 300 mg administered. • Monitor vital signs especially BP and heart rate to avoid Hypotension and bradycardia.

Methylprednisolone Succinate • Solu-medrol only • Used in treatment of acute spinal cord injury • Must be administered within 8 hours of injury • Initial bolus: 30mg/kg in 50 cc D5W over 15 minutes • Wait 45 minutes then give maintenance infusion of 5.4mg/kg in 200 cc D5W at 10 cc/hr via pump over 23 hours. • Use with caution in pregnancy, and patients already on steroids. • If patient taken to surgery, continue dose. • Monitor for S/S of infection and GI bleed

Nitroprusside Sodium (Nipride)
• To lower BP quickly in hypertensive emergencies • 50 mg in 250 ml D5W for 200 mcg/ ml • Initial Dose: 0.3 to 0.5 mcg/kg/min, titrate by 0.5 mcg/kg/min every few minutes not to exceed 2 mcg kg/min. • Not compatible with protonix • Protect from light • Stable for 24 hours • Monitor BP, HR, Acid base status, o2 sat and for cyanide toxicity, (Metabolic acidosis, bradycardia, decreased O2 sat, confusion, and convulsions

Vasopressin • 20 units in 100 ml NS for 0.2 units/ml • Septic Shock: 0.03 units per minute with max dose of 0.7 units per minute. (doses greater than 0.03 units/min increase cardiac side effects). • Gastroesophageal Variceal Hemorrhage: 0.2 to 0.4 units/min max dose 0.8 units/min with max duration of 24 hours. • When used for hemorrhage at max dose, the use of nitroglycerin concurrently is recommended to prevent myocardial ischemic complications. • Compatible with Cardizem, Dobutamine, Dopamine, Levophed, Heparin, insulin, protonix, epi, and sodium bicarb.

Vasopressin

Neo-Synephrine • Indicated in hypotensive emergencies during spinal anesthesia, severe hypotension, shock, and psvt. • Mix 10 mg in 250 NS = 40 mcg/ml, may also be mixed in 500cc NS or D5W. • Initial infusion rate is at 100 to 180 mcg/min ; then decrease to maintenance infusion of 40-60 mcg/min when BP stable. • May also be given as a bolus: administer 0.2 mg IV, SC or IM. • Contraindicated in severe hypertension or V Tach. • Side Effects: May cause Headaches, bradycardia, arrhythmias, hypertension, asthmatic episodes, tissue with extravasations, possible tachyphylaxis with continued use.

Neo-Synephrine • Use with extreme caution in elderly patients and patients with heart disease, hyperthyroidism, bradycardia, partial heart block, and myocardial. disease. • Use large bore IV for administration. • Use IV pump • Continuous monitoring of EKG, BP, CO, CVP, PAWP, urine output, and color and temp of limbs. • Monitor administration site for extravasations.

Propofol • Indicated for: Sedation, Anesthesia, Rapid sequence intubation. • Requires a dedicated IV cathater • Use the 100ml premixed bottle 10 mg/ml • Disinfect rubber stopper with 70% isopropyl alcahol and allow drying before spiking. • Initial Infusion: 5mcg/kg/min for 5 minutes. • Increase rate at 5-10 minute intervals in increments of 5-10 mcg/kg/min until desired level of sedation is achieved.

Propofol • Maintenance Infusion: Rates of 5-50 mcg/kg/min or higher may be required. • The tubing and any unused portions of propofol should be discarded every 12 hours. • Propofol contains no preservative and is capable of supporting growth of microorganisms. • Nurses may monitor infusions post intubation, Physicians need to administer bolus. • Monitor vital signs every 5-10 min (HR BP)

Propofol • Do not administer with blood. • Discontinue /notify doctor if patient has severe hypotension, bradycardia, or if hypersensitivity occurs. • If Triglycerides level is > 500mg/dl, use is not recommended • Prolonged therapy leads to a decrease in Zinc levels • Daily awakening assessments • Reduce dose by 20 % in elderly patients • Smaller doses may be required when used with narcotics. • Rate chart in IV Drip book in ER and ICU

Nitroglycerin (Tridil) • 50 mg in 250 ml D5W = 200 mcg/100cc • Initial Infusion: 10 mcg/min (3cc/hr) • Maintenance Infusion rate; 10-400 mcg/min • 400 mcg/min is rarely necessary • 10 mcg/min = 3 ml/hr • 20 mcg/min = 6 ml/hr • 30 mcg/min = 9 ml/hr ect • Titration: Increase by increments of 10 mcg/min (3cc/hr) every 3-5 minutes until desired response is noted • Pain free for a patient with chest pain • Or lowered BP

Nitroglycerin (Tridil) • Use Nitroglycerin tubing found in bottom cabinet on crash cart or in pharmacy. • Monitor BP and EKG continuously (BP at q dose change and at least q 5-15 min while titrating. • Side Effects: Severe headaches, tachycardia, bradycardia, hypotension. • Record onset, duration, location of CP, obtain baseline BP, monitor for postural hypotension, keep BP within parameters ordered by (usually > 100 systolic) • MAP (Mean Arterial Pressure) = SBP + (DBPX2)
• 3

Pantoprazole (Protonix) • Usual Dose: 80mg bolus, followed by 8 mg/hr continuous infusion for active GI bleed. • Withdraw 20 ml from the NS 100 ml bag and add 10 ml of that volume to each vial of protonix. • Using one syringe, draw up both vials of Protonix and add back into the NS bag. For 0.8 mg/ml. • 8 mg/hr = 10 ml/hr (Limit use to 72 hours • May be administered IV through a dedicated line or through a Y-site. • The Y-site line should be flushed before and after administration of Protonix IV with 5% DD5W, NS or LR.

Midazolam (Versed) • 50 mg in 50 ml NS for 1 mg/ml • Start at 0.02 to 0.1 mg/kg/hr and titrate to effect using sedation scales SAS or RASS • Max drip rate 20 mg/hr • May produce apnea with rapid administration. • Respiratory monitoring is critical to avert potential problems • Hypotension in hypovolemic patients • Consider reducing dose 20 to 50% in elderly, chronically ill, and patients receiving opiods or other CNS depressants. • Use with caution in hepatic and renal impairment • Incompatible with LR

Procainamide (Pronestyl) • 2gm in 250ml of D5W for 8 mg/ml • Bolus: 100mg by slow IV push q 5 minutes. No faster than 25-50 mg/min. • Give until arrhythmias disappear, adverse reactions develop (ORS widens > 50% of original width), or total dose of 1 GM has been given. • Loading dose may also be given IVPB in 50ml D5W over 25-30 minutes.

Procainamide (Pronestyl) • Maintenance Infusion Rate • 1-6 mg/min • 1mg/min = 7.5ml/hr • 2mg/min = 15ml/hr • If arrhythmias recur, repeat bolus and increase infusion rate • Monitor EKG and BP, Run on IV pump only • Side Effects: Hallucinations, Seizures, abdominal Pain, anorexia, diarrhea, hypotension, AV block, ventricular asystole. • Use cautiously in patients with second or third degree heart block. Monitor QT interval closely in renal failure.

Verapamil (Calan, Isoptin) • 5 mg/2cc vial • Slow IV push only. Verapamil should be given over a minimum of 2 minutes. Administer over 3 minutes in the elderly. • Adults: Initially 5-10 mg may repeat in 30 minutes with 10mg dose if response is not adequate. • Use with caution in patients with sick sinus syndrome or 2nd or 3rd degree heart blocks, severe hypotension, impaired renal function, and impaired liver function. • Continuously monitor EKG and BP during IV administration. monitor for rapid ventricular rates, bradycardia, heart blocks. prolongation of PR interval Notify DR immediately if occurs

Corvert (Ibutilide Fumarate) • Indicated for the rapid conversion of atrial fibrillation or atrial flutter of recent onset to sinus rhythm. • 0.1mg/ml (available in 10cc vial) • May be diluted in 50cc NS or given IV push • Must be given over 10 minutes • Initial infusion: Patient weighing 60 kg (132 lbs) or more One vial: 1 mg of Corvert. • Patient weighing < 60 kg (< 132 lbs) 0.1 mg/kg Covert. • If arrhythmia does not terminate within 10 minutes after the end of the initial infusion, a second 10 minute infusion of equal strength may be administered 10 min after the end of the initial infusion.

Corvert (Ibutilide Fumarate) • Physician Must be Present during Administration • Contraindicated in patients with hypersensitivity to drug or its components. • Side Effects: Headache, nausea, nonsustained VT, hypotension, BBB, AV block, sustained polymorphic VT, prolonged QT, bradycardia, tachycardia. • Patient must have cardiac monitoring before during and after infusion ( for at least 4 hours after). Monitor defibrillator must be at patients bedside during administration. • Have recent Mag, Potassium, levels prior to administration.

MCHD Drip Protocol

MCHD Drip Protocol

Rapid Sequence Intubation • Equipment: • Intubation Equipment available in Drawer # 2 of any crash cart • Contents of Respiratory Tray • Laryngoscope Handle in middle • Oral and Nasal Airways in middle • End cap Co2 detector in middle • Laryngoscope blades with size L side • Flexible Suction catheter L side • ET Tubes with size on PKG R side

Rapid Sequence Intubation • Medications: • Physicians Intubation Box in Omnicel • Propofol • Vecuronium (Norcuron) • Etomidate • Omnicel Central and ER - Versed • Omnicel ER Only - Ketamine • Omnicel frige Central and ER • Succinylcholine (Succs) • Omnicel frige ER only • Rocuronium (Roc)

Chest Tube Placement • Equipment: • Sterile Chest tube Tray located in covered shelves in trauma 1 in the Emergency Department. • Thora-Seal Collection Chamber & Chest tubes located in covered shelves in trauma 1 in the Emergency Department or ICU supply room. • Betadine, Sterile gloves for physician • Lidocaine • 10 cc syringe
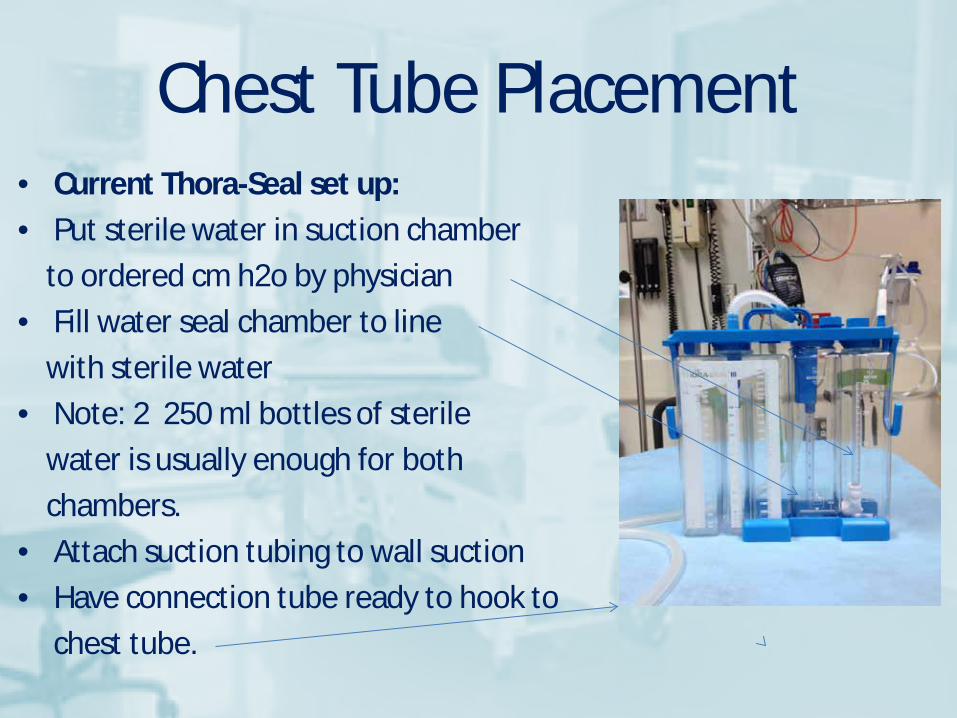
Chest Tube Placement • Current Thora-Seal set up: • Put sterile water in suction chamber to ordered cm h2o by physician • Fill water seal chamber to line with sterile water • Note: 2 250 ml bottles of sterile water is usually enough for both chambers. • Attach suction tubing to wall suction • Have connection tube ready to hook to chest tube.
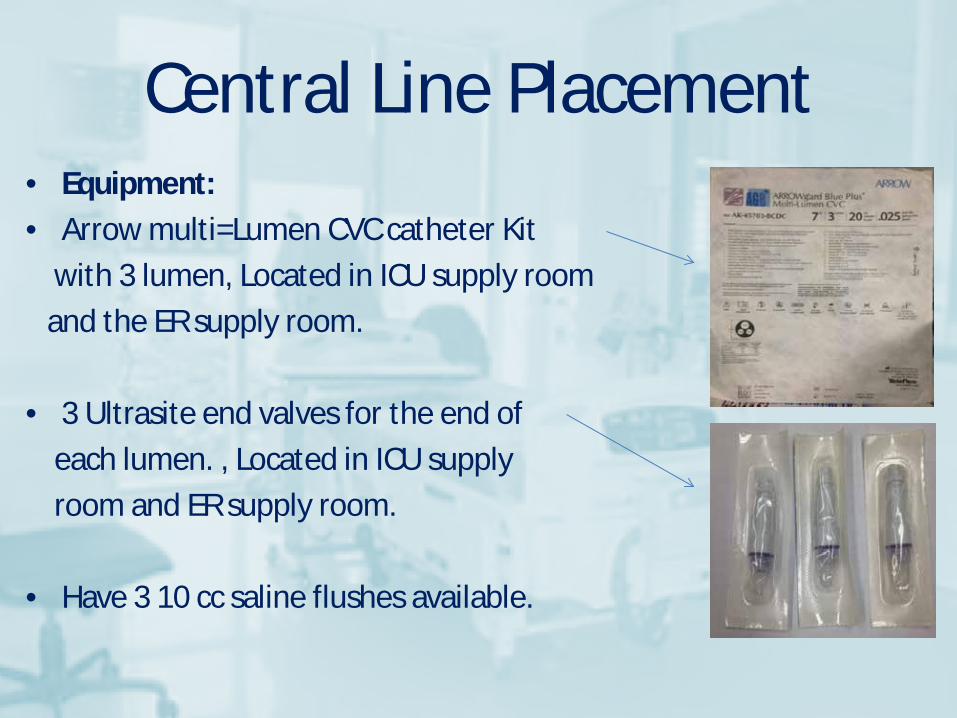
Central Line Placement • Equipment: • Arrow multi=Lumen CVC catheter Kit with 3 lumen, Located in ICU supply room and the ER supply room. • 3 Ultrasite end valves for the end of each lumen. , Located in ICU supply room and ER supply room. • Have 3 10 cc saline flushes available.

Arterial Line Placement • Equipment: • Radial Artery catheterization Kit • Pressure Transducer • Pressure transducer Cable • 500 cc bag NS • Pressure infuser • Transducer Holder and Clamp • All Equipment in ICU Supply Room
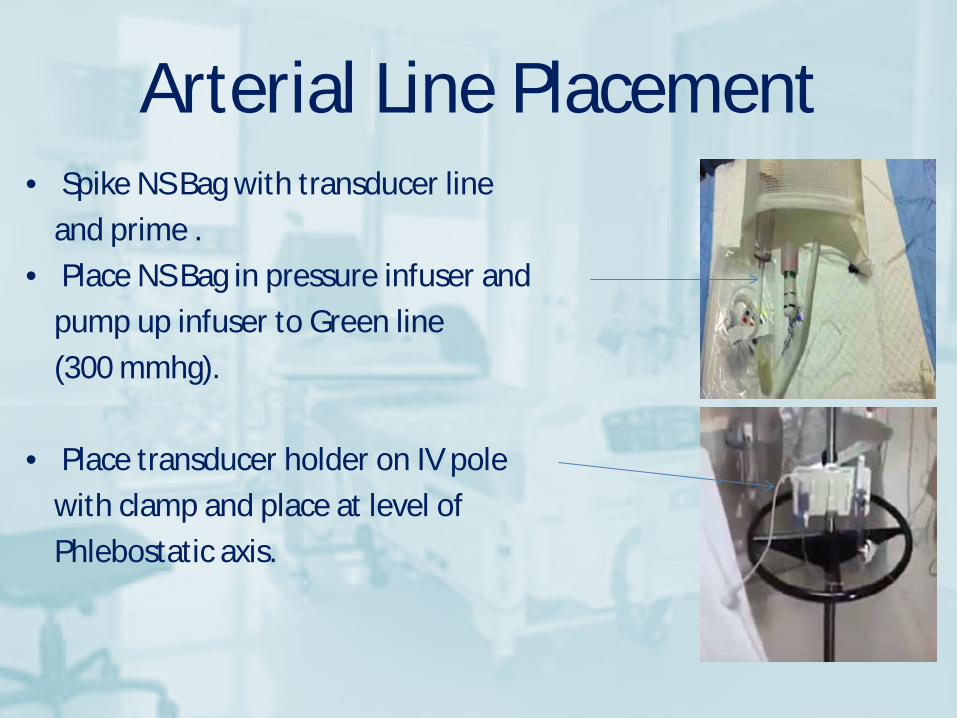
Arterial Line Placement • Spike NS Bag with transducer line and prime . • Place NS Bag in pressure infuser and pump up infuser to Green line (300 mmhg). • Place transducer holder on IV pole with clamp and place at level of Phlebostatic axis.

Arterial Line Placement • Plug Transducer cable into transducer on A line • Plug other end of transducer cable into top port on cardiac monitor.

Arterial Line Placement • Upon plugging transducer cable into monitor the red ABP wave form will appear. • Open transducer chamber to atmosphere and press zero button on monitor. then open valve to patient • Hook Transducer line to A line after placed by physician.

ML/HR Dose Calculations • Amount of Fluid over a period of time: # ml 60 min
# min 1 hr ____ ml/hr
• IV Solution with medication ml/hr: # ml ordered med Amount of med hr ____ ml/hr
• mcg/kg/min calculation:
250ml ?mcg kg 1 mg 60 min 400 mg kg/min 1 1000 mcg 1 hr _____ ml/hr

Conclusion Thank You And keep up the good work Our Patients are Counting On Us


















