
Lumps and Bumps Anne Moore, MD Assistant Professor Radiology Children’s Mercy Hospital and...
52
Lumps and Bumps Anne Moore, MD Assistant Professor Radiology Children’s Mercy Hospital and University of Missouri, Kansas City
-
Upload
unique-spears -
Category
Documents
-
view
224 -
download
3
Transcript of Lumps and Bumps Anne Moore, MD Assistant Professor Radiology Children’s Mercy Hospital and...

Lumps and BumpsAnne Moore, MD
Assistant Professor Radiology
Children’s Mercy Hospital and
University of Missouri, Kansas City

Imaging Modalities
• Plain Xray imaging• ULTRASOUND• CT imaging• MR imaging

Lumps and Bumps
Congenital Lesions
Vascular Anomalies
Acquired Lesions
Infectious Lesions
Traumatic Lesions

Head, Shoulders, Knees and Toes
Eyes and ears and mouth and nose

Head and neck
»Start with Ultrasound!
Head and Neck
• Dermoid/Epidermoid• Branchial Cleft Cyst• Thyroglossal Duct Cyst• Accessory Parotid Tissue• Fibromatosis Coli• Vascular Anomalies
– Hemangioma– Lymphatic/Venous Malformation
Dermoid/Epidermoid
• Found in a variety of locations around the skull, midface and neck
• Commonly in midline and frontotemporal location, followed by parietal location
• Midline or near midline lesion in neck

Dermoid
• Cystic or solid• Hypovascular

Dermoid/Epidermoid
• Note Midline location
• Near sutures• Often contains fat
– Negative Hounsfield Units

Branchial Cleft Cyst:Second
• Most common Branchial anomaly
• Presents acutely with mass at the angle of the mandible
Accessory Parotid Tissue
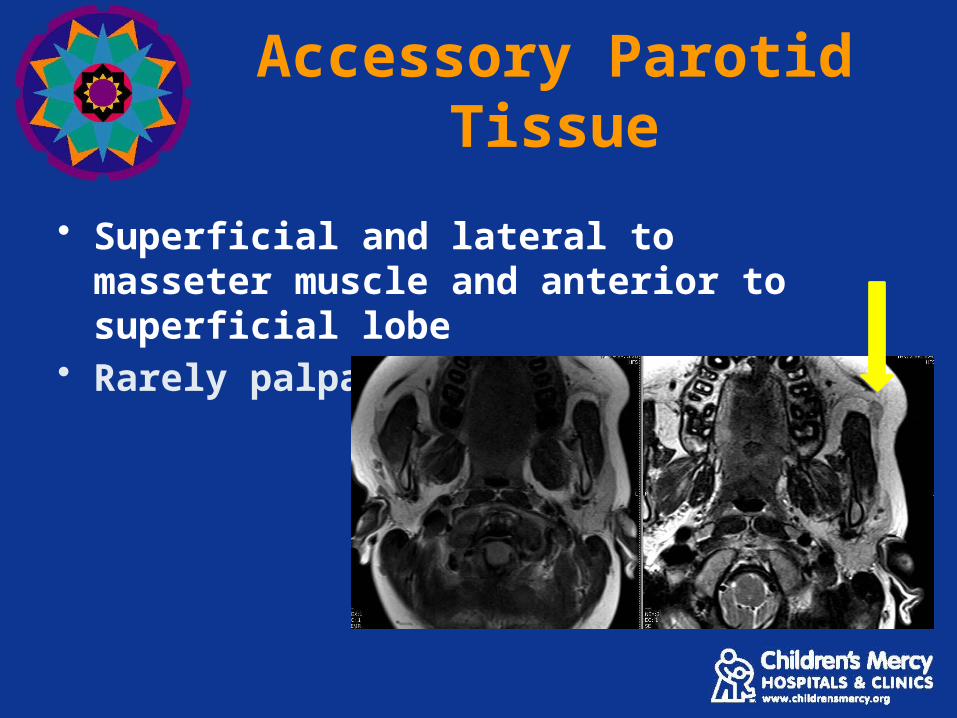
• Superficial and lateral to masseter muscle and anterior to superficial lobe
• Rarely palpable

Fibromatosis Coli
• Idiopathic intramuscular hematoma
• Focal mass or fusiform enlargement of sternocleidomastoid
• Presents with torticollis < 8 weeks of age

Fibromatosis Coli
Fibromatosis Coli Normal for comparison

In a 6 week old with torticollis, which imaging study is
initially suggested?
A. B. C. D.
0% 0%0%0%
A. MRI
B. CT
C. Ultrasound
D. Plain Radiographs
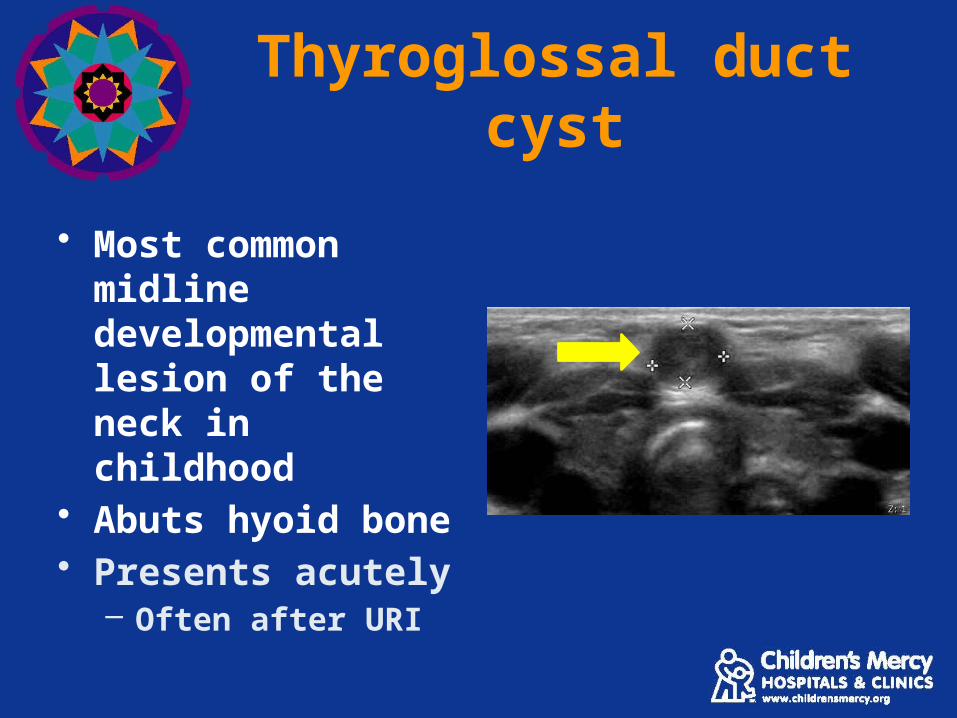
Thyroglossal duct cyst
• Most common midline developmental lesion of the neck in childhood
• Abuts hyoid bone• Presents acutely
– Often after URI

Thyroglossal Duct Cyst
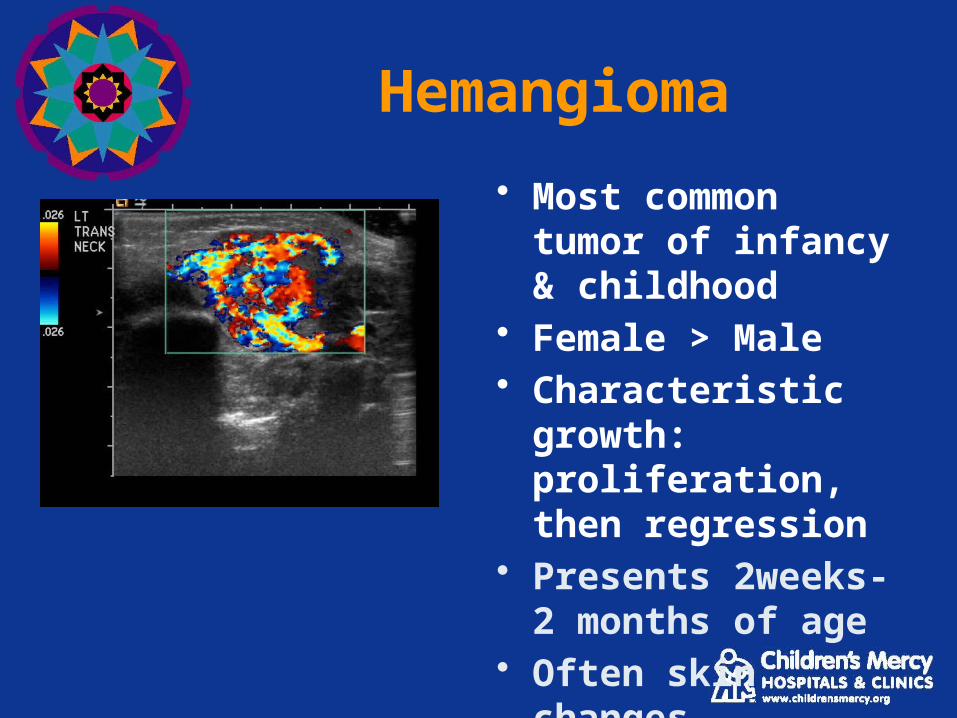
Hemangioma
• Most common tumor of infancy & childhood
• Female > Male • Characteristic growth:
proliferation, then regression
• Presents 2weeks-2 months of age
• Often skin changes
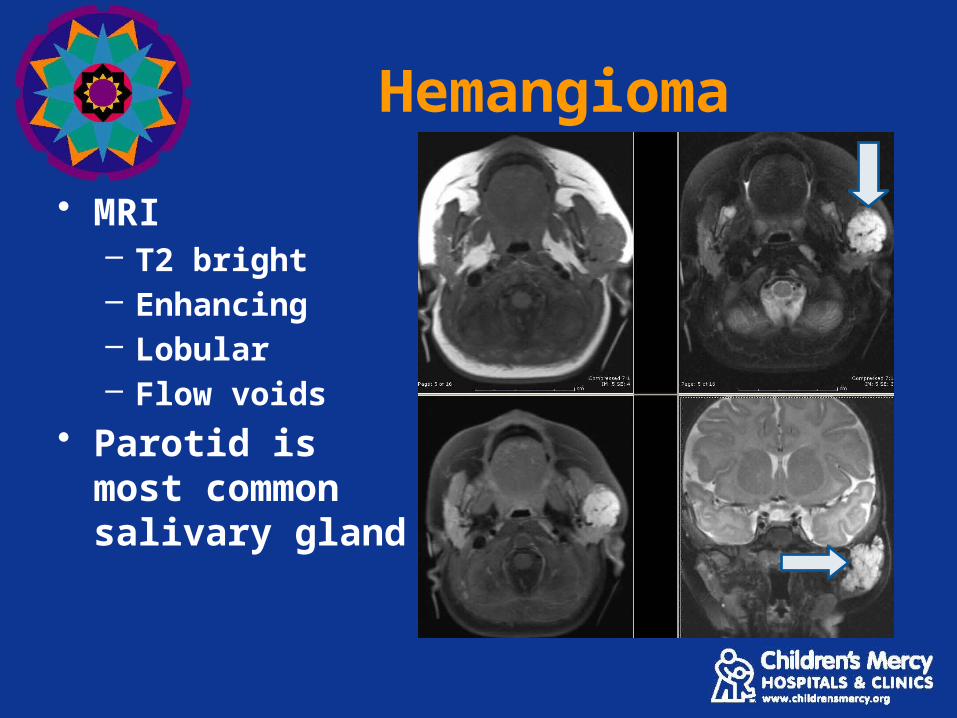
Hemangioma
• MRI– T2 bright– Enhancing– Lobular– Flow voids
• Parotid is most common salivary gland

HemangiomaProliferation Involution

Venous and Lymphatic Malformations
Present any age, but usually beyond infancy
• Venous Malformation: – Dysplastic venous channels; Solid with
phleboliths and venous Doppler wave forms
• Lymphatic Malformation: – Dysplastic lymphatic structures; Cystic with
fluid levels

Venous Malformation
• Venous wave forms• Solid

Lymphatic Malformation
Note cystic and solid components

In a 1-month-old child with a hemangioma on the arm,
what is the suggested imaging study?
A. B. C. D.
0% 0%0%0%
A. No imaging needed
B. MRI
C. Bone scan
D. Plain radiographs
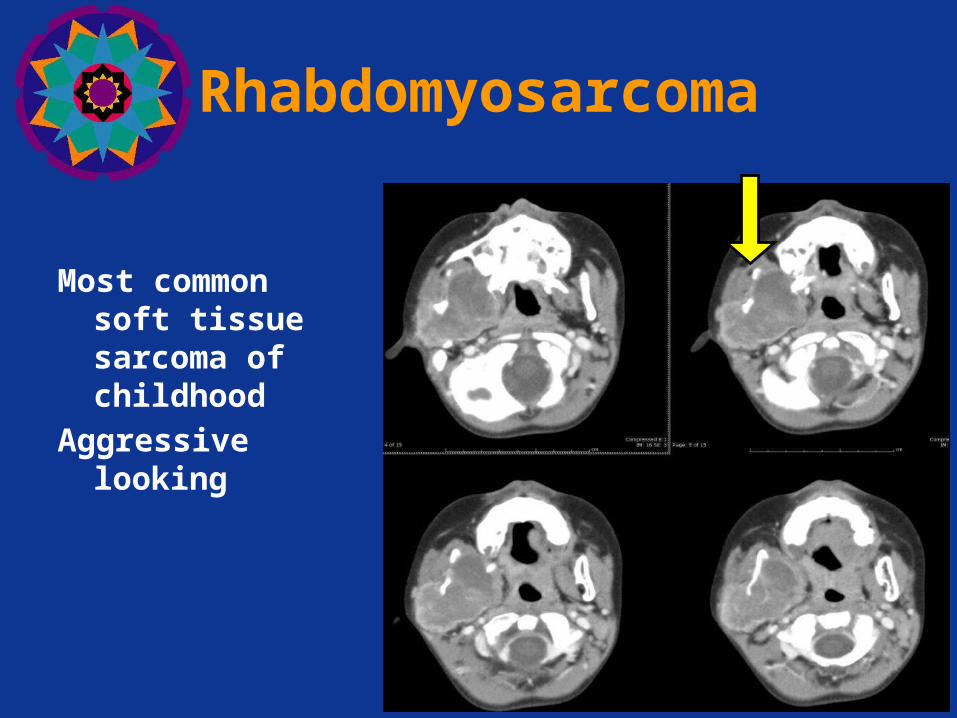
Rhabdomyosarcoma
Most common soft tissue sarcoma of childhood
Aggressive looking

Lymphoma
• Third most common childhood malignancy
• Asymptomatic lymphadenopathy

Cervical Lymphadenopathy
• Common in children• Imaging studies will show size, number and
location of enlarged lymph nodes
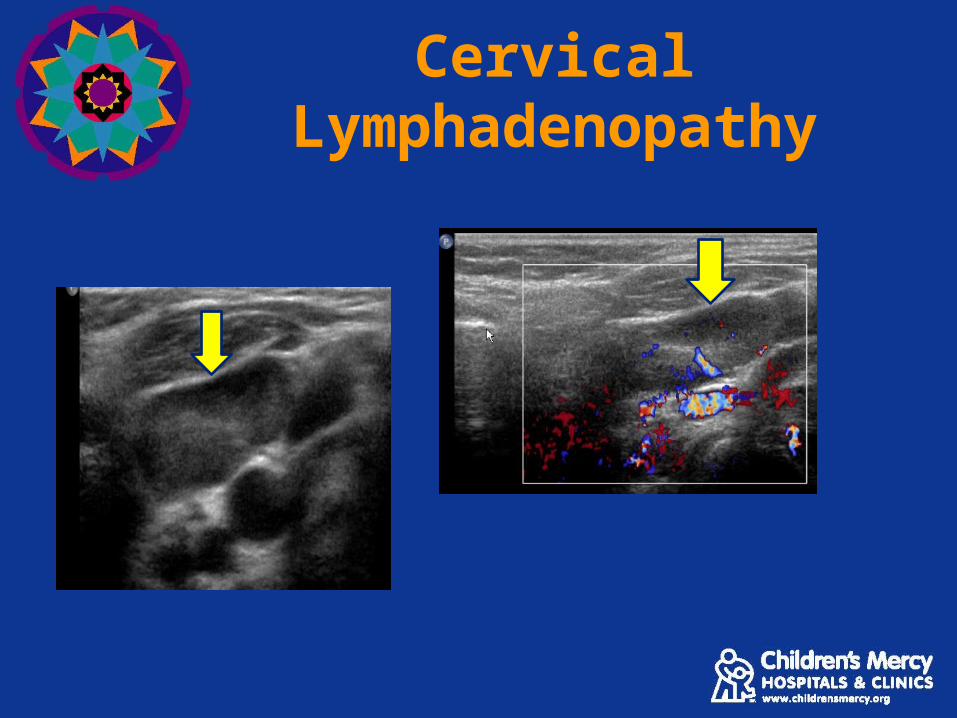
Cervical Lymphadenopathy

Suppurative Lymphadenitis
• Bacterial infection may result in abscess formation

Suppurative Lymphadenitis
• Nodes with central necrosis/fluid
• May take weeks to resolve
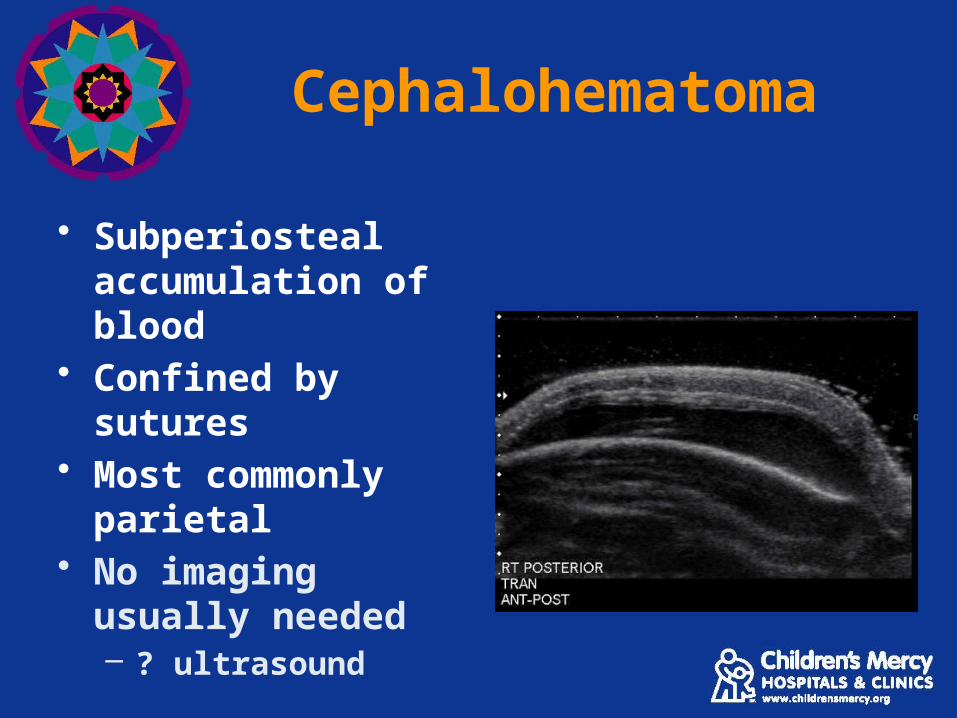
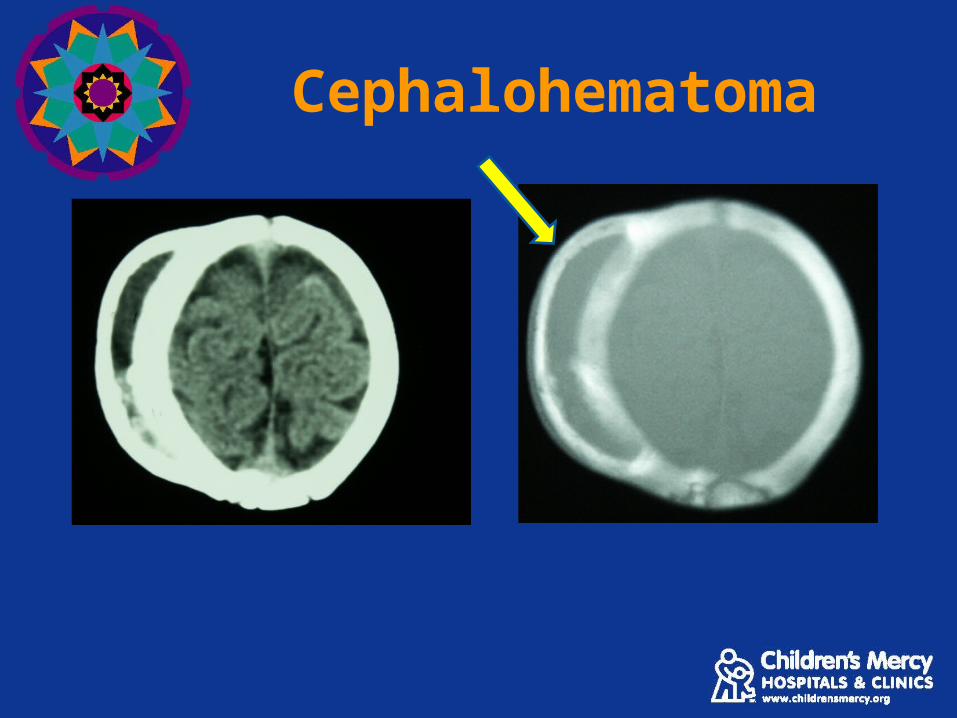
Cephalohematoma
• Subperiosteal accumulation of blood
• Confined by sutures• Most commonly
parietal• No imaging usually
needed– ? ultrasound
Cephalohematoma

In a newborn male with unilateral parietal swelling since birth, which imaging
study is indicated?
A. B. C. D.
0% 0%0%0%
A. MRI
B. CT
C. Plain radiographs
D. No imaging indicated

Shoulder, Knees and Toesaka Below the Neck
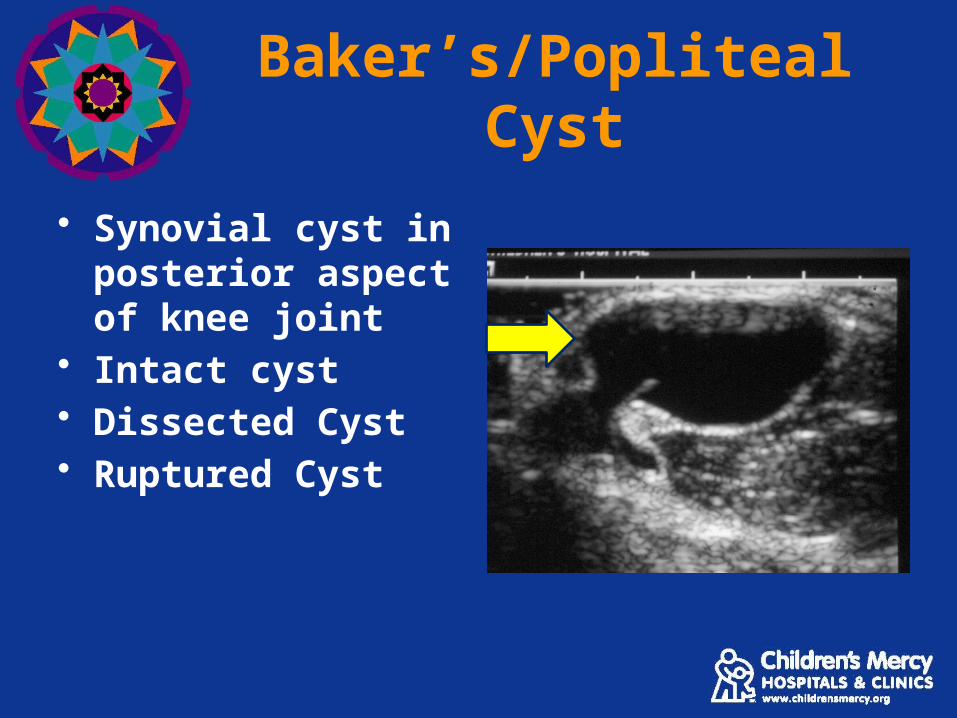
Baker’s/Popliteal Cyst
• Synovial cyst in posterior aspect of knee joint
• Intact cyst• Dissected Cyst• Ruptured Cyst

Baker’s/popliteal cyst

Ganglion Cyst
• Cystic lesion usually attached to a tendon sheath
• Location: hand, wrist, dorsum of foot

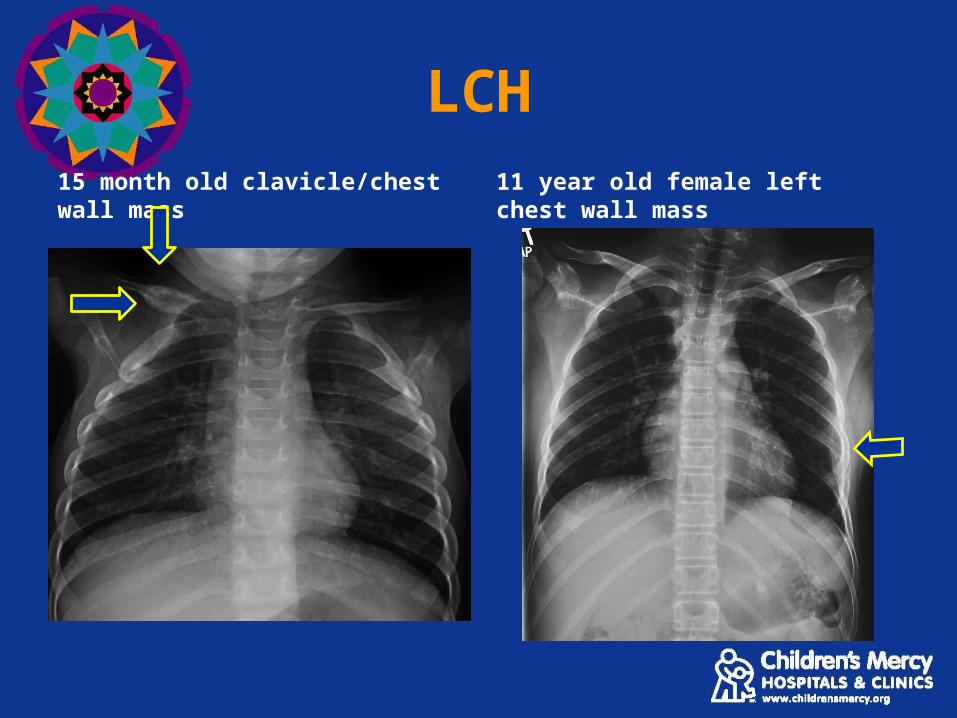
Langerhan Cell Histiocystosis
• Idiopathic disorder that can manifest as focal or systemic disease
• Initial lesion often identified with radiography
• Radiographic appearance is extremely variable
• May presents with palpable lumps– Especially on skull or ribs

LCH
15 month old

LCH
15 month old
LCH
15 month old clavicle/chest wall mass 11 year old female left chest wall mass

Inguinal Hernia
• Patent processus vaginalis
• Imaging not usually needed– Ultrasound if unsure about
etiology

Inguinal Hernia

Osteochondroma
• Most common benign growth of the skeleton
• Usually painless mass• Painful=possible
malignancy and need MRI

Sacral Dimple
• Classified as low or high risk• Low risk does not require imaging• High risk require imaging
– Ultrasound if < 6 months– MR imaging thereafter

Sacral dimple
• Low risk– Midline– Less than 5mm in
diameter– Located with the
gluteal crease– No cutaneous
abnormalities or drainage
– Can see bottom of dimple

Sacral dimple
• High risk– Greater than 5mm in diameter– Located above the gluteal crease– Cutaneous abnormalities– Draining cerebrospinal fluid– Bottom of dimple cannot be seen

Sacral Dimple
Tethered Cord Normal

Sacral Dimple
• Dermal sinus tract

Sacral Dimple

Lumps and bumps
• Ultrasound First• Use Ultrasound and Clinical Setting to
Determine Next Best Step in Evaluation and Treatment

In a 4-mo-old with skin lesion. Which imaging study
is indicated?
A. B. C. D.
0% 0%0%0%
A. MRI
B. Ultrasound
C. No imaging needed
D. Plain radiographs


















