Monitor MEDICINE PRICE - who.int · PNFP Private-not-for-profit (health facility) WHO World Health...
32
No. 11: July-September 2013 UGANDA COUNTRY WORKING GROUP Monitor MEDICINE PRICE MINISTRY OF HEALTH WORLD HEALTH ORGANISATION HEPS UGANDA HAI AFRICA HEALTH ACTION INTERNATIONAL WITH SUPPORT FROM Uganda No. 11 July-September 2013
Transcript of Monitor MEDICINE PRICE - who.int · PNFP Private-not-for-profit (health facility) WHO World Health...
No. 11: July-September 2013
Uganda CoUntry Working groUp
MonitorMEDICINE P R I C E
Ministry of HealtH
World HealtH organisation
HePs Uganda Hai afriCaHealtH action international
With sUpport from
Uganda No. 11 July-September 2013

2
UgandaMonitorMEDICINE P R I C E
aBBreViationS anD acronYMSCSO Civil Society OrganizationDANIDA Danish International Development AgencyDHO District Health OfficerDFID Department for International DevelopmentEMHS Essential Medicines and Health SuppliesHAI Health Action InternationalHEPS Coalition for Health Promotion and Social DevelopmentHSSIP Health Sector Strategic and Investment Plan MeTA Medicines Transparency AllianceMoH Ministry of HealthMPR Median Price RatioNGO Non-governmental organizationNPSSP National Pharmaceutical Sector Strategic PlanPFP Private-for-Profit (health facility)PNFP Private-not-for-profit (health facility)WHO World Health Organization

3
No. 11: July-September 2013
eXecUtiVe SUMMarYPrice is the most predominant barrier to access to essential medicines.1 Periodic monitoring of medicines is very important in determining if medicines are available and affordable to patients.
In September 2013, MeTA Council of Uganda implemented a Medicine Availability and Price (MAP) survey of 40 essential indicator medicines. The survey was a quantitative process that used the traditional WHO/HAI methodology in 4 geographical regions (Eastern, Central, Western, and Northern) of Uganda across 3 health sectors (Public, Private and Mission) on price and availability.
In total 120 facilities (taking into consideration urban and rural representation) were visited by a team of data collectors comprised of pharmacists/ pharmacy technicians and social scientists having bias in public health practice. The survey was managed by a Survey Manager who is a pharmacist.
Key findings from the survey included:
The overall availability of the surveyed medicines was 68% in the public facilities, •65% in private and 74% in mission facilities.
A relatively bigger proportion of urban-based facilities had medicines available than •rural-based facilities. At 30%, the difference was highest the private sector.
89% of the public and mission facilities had Artemether/Lumefantrine 20/120mg •tablets physically available on the day of the survey compared to 75% of the private facilities.
Medicines for the most common non-communicable diseases (diabetes and hypertension) •were found available in less than 70% of the facilities across the three sectors.
The public facilities had very low availability of paediatric formulations: amoxicillin •suspension (11%), cotrimoxazole syrup (16%) and metronidazole syrup (45%).
Medicine prices were comparable between urban and rural facilities in the private •sector (MPR 1:1).
1 Ellen fm & hoen t (2003): trips, pharmaceutical patents and access to Essential medicines: seattle, doha and Beyond

4
UgandaMonitorMEDICINE P R I C E
Medicines were 12% more expensive in urban than in rural mission facilities (MPR •1:1).
Comparing mission and private sectors, there was no difference in the price of 25 of •the 40 essential medicines surveyed.
In the private and mission sectors, medicines for chronic conditions like asthma, •depression, diabetes, hypertension and ulcers cost more than a day’s wage for the lowest paid government worker in Uganda. However, the following conditions are affordable in both sectors by the lowest paid government worker: RTI (both adult and paediatric), anxiety, arthritis and pain/inflammation.

5
No. 11: July-September 2013Table 3: Availability of 40 essential medicines across sectors Oct-Dec 2010
1. introDUction anD BacKGroUnD1.1 IntroductionThe Constitution of the World Health Organisation (1946) recognises access to medicines as a major component of the right to health. Therefore, periodic monitoring of medicine is very important in determining if medicines are available and affordable at the different levels in the distribution chain. One way of addressing the price barrier to access to essential medicines is by improving information flow through multi-stakeholder approaches that pool together diverse expertise. In Uganda, Ministry of Health (MOH), WHO and HAI Africa and its local partner HEPS Uganda through the Country Working Group (CWG) have since 2002 monitored medicine availability and prices. Medicines Transparency Alliance (MeTA) Uganda prioritised this activity in its work plan and funds were provided by the IMS.
1.2 Background
Uganda is among the least developed countries of the world. A big percentage of the population still lives under a dollar a day. Its health statistics are among the worst in the world. An estimated 7% of the population is living with HIV, which has put an extra burden on the country’s already weak public health system.
It is estimated that only one third of the population has access to essential medicines. Price is one of the most predominant barriers to access to medicines. In developing countries, at a national level, the cost of medicines may account for up to 80% of non-salaried health expenditure, and at community level, the majority of people pay out-of-pocket for the medicines they consume. It is clear, therefore, that price is often a determining factor in whether the government can offer treatment to its population for a particular disease, or whether an individual receives a full treatment, an incomplete course, or no medicine at all. Until recently, there has been little information on what government or people paid for medicine.
Data from the various surveys of the CWG have revealed that universal access to medicines has not been achieved and that medicines remain unaffordable for a significant section of the population. The results of these studies guide decisions on a strategy for improving affordability.

6
UgandaMonitorMEDICINE P R I C E
The monitoring system generates regular information on price changes over time, and comparisons between the three sectors (public, private and mission) and four regions of the country. By informing consumers and procurement agencies about current prices and patterns of price changes, these series of surveys are an important complement to efforts to improve access to medicines for Ugandans, especially the poor and vulnerable.
1.3 Objectives of the survey
By gathering and analysing comprehensive data on the prices of selected medicines in the four representative regions of Uganda and across three sectors (Public, Private for profit and private not for profit/NGO/mission), the survey aimed at achieving the following objectives:
To determine the availability of selected medicines in the public, private and mission •sectors;
To compare the prices of selected medicines between the private and mission sectors;•
To determine the affordability of treating key indicator conditions to ordinary Ugandans; •and
To inform policy interventions aimed at improving access to essential medicines in •Uganda

7
No. 11: July-September 2013
2. MetHoDoloGY2.1 Design
The survey was conducted using the standard methodology co-developed by WHO and HAI1. The survey used mainly quantitative methods to assess availability and prices of medicines in the public, private and mission sectors (See annex 2 for the survey tool).
2.2 Geographical areas
The survey was conducted in four regions of Uganda (Central, Eastern, Western, and Northern). The four regions were chosen as a realistic representation of the diversity in epidemiological and geographical characteristics of the country.
2.3 Sectors and facilities
The survey was conducted in three sectors: public, private (PFP) and mission (NGO/PNFP). All three contribute a significant proportion of health services in the country. The standard WHO/HAI methodology recommends 30 outlets per sector for a survey to achieve enough data points for analysis.2 The current survey targeted a total 120 facilities disaggregated as follows: 40 outlets per sector (20 rural and 20 urban) and in each region 10 per sector (5 rural and 5 urban).
2.4 Sampling strategy
One hundred and twenty (120) facilities - 40 facilities per sector - were selected for the survey (see annex 1). In each region, the main regional referral hospitals (purposively selected), district hospitals and health centre IVs were selected to represent the public health sector facilities. Five licensed community pharmacies, 3 drug shops and 2 clinics located within 5 km of each of the selected public facilities were purposively selected to represent the private sector.
1 www.haiweb.org/medicineprices2 it is noted that a number of validation studies (in addition to the 9 pilot studies) were done during the original
process of methodology development. the most important validation was on the sampling frame where it was found that sampling more regions, and those in areas greater than one days car travel from the capital, and in each area from more outlets a greater distance from the main hospital produced the same results as using the standard sampling frame. the adequacy of collecting data on just the originator brand and lowest priced generic equivalent was also studied – again it was found there was no significant difference in the results. The volatility of msh prices (used as an external bench-mark) have also been studied and little volatility has been found. a paper on validation has been published, and is cited as madden Jm, meza E, Ewen m, Laing ro, stephens p, ross-degnan d. measuring medicine prices in peru: validation of key aspects of Who/hai survey methodology. rev panamsaludpublica. 010;27 (4):291–9.

8
UgandaMonitorMEDICINE P R I C E
The NGO facilities with similar characteristics to public sector (e.g. mission hospitals of similar size and capacity to the regional, district and sub-district hospitals in the region) were purposively selected.
The list of sites surveyed is attached (Annex 1).
Urban and rural representation was taken into consideration when selecting. Urban areas were considered to be towns with a population of more than 50,000 and rural areas to at least 10 km away from the urban centres.
2.5 Medicines surveyed
The selection of a basket of 40 essential medicines was based on the methodology’s core and supplementary lists. The list was approved by the Pharmacy Division of Ministry of Health – Uganda.

9
No. 11: July-September 2013
Table 1: Medicines surveyedNO MeDIcINe STreNGTh DOSaGe fOrM caTeGOry
1 Aciclor 200mg Tablet Antiviral2 Albendazole 200mg Tablet Anthelmintic3 Amitriptyline 25mg Tablet Antidepressant4 Amoxicillin 250mg cap/tab Antibacterial5 Amoxicillin 250mg/5ml Suspension Antibacterial6 Artemether/Lumefantrine 20/120mg Tablet Antimalarial7 Bendrofluazide 5mg Tablet Diuretic8 Betamethasone 1% w/v cream/ointment Anti-inflammatory9 Carbamazepine 200mg Tablet Antiepileptic10 Ceftriaxone 1gm Powder for inj Antibacterial11 Cimetidine 400mg Tablet Anti-ulcer12 Ciprofloxacin 500mg Tablet Antibacterial13 Co-trimoxazole 8/40 mg/ml Suspension Antibacterial14 Co-trimoxazole 400+80 mg Tablet Antibacterial15 Dextrose 5% Injection Parenteral16 Diazepam 5mg Tablet Anxiolytic17 Diclofenac 50mg Tablet Analgesic18 Doxycycline 100mg Capsule Antibacterial19 Erythromycin 250mg Tablet Antibacterial20 Fluconazole 200mg tab /cap Antifungal21 Furosemide 40mg Tablet Diuretic22 Gentamycin 80mg/ml Injection Antibacterial23 Glibenclamide 5mg Tablet Antidiabetic24 Mebendazole 100mg Tablet Anthelmintic25 Metformin 500mg Tablet Antidiabetic26 Methyergometrine 200ug/ml Injection Oxyticic27 Metronidazole 200mg/5ml Suspension Antibacterial28 Metronidazole 200mg Tablet Antibacterial29 Nifedipine retard 20mg Tablet Antihypertensive30 Nystatin 100000iu Pessaries Antifungal31 Omeprazole 20mg Capsule Antiulcer32 Oral Rehydration Salt
(ORS)- Powder Antidiarrhoea
33 Paracetamol 500mg Tablet Analgesic34 Phenytoin 100mg Tablet Antiepileptic35 Prednisolone 500mg Tablet Antiinflammatory36 Pyrimethamine /sulfadoxide 25/500mg Tablet Antimalarial37 Propranolol 40mg Tablet Antihypertensive38 Quinine 300mg/5ml Injection Antimalarial39 Salbutamol 0.1mg(100mcg)/dose Inhaler Antiasthmatic40 Tetracycline 1% eye ointment Antibacterial

10
UgandaMonitorMEDICINE P R I C E
2.6 Personnel
One pharmacist or pharmacy technician and one social scientist with bias in public health, from each of the 4 regions were trained on how to collect data. A pharmacist with bias in public health was recruited as the survey manager, took the responsibility of setting up and conducting the survey, supervising data collectors, analysing the data, and writing the report.
An Expert Advisory Group guided the survey process through supporting the survey manager in setting up and conducting the survey; providing feedback on the survey findings and earlier drafts of this report; informing recommendations on policy options; and promoting the survey and its findings.
Table 2: advisory GroupNaMe TITLe, OrGaNIZaTION1. Mr. Nazeem Mohamed Chief Executive Officer, Kampala Pharmaceutical Industries2. JoanitaLwanyagaNamutebi Head Quality Assurance, Joint Medical Store3.Ms. Rosette Mutambi Executive Director, HEPS Uganda4. Ms. HellenByomire Head Drug Information, National Drug Authority5. Mr. MorriesSeru Principle Pharmacist, Ministry of Health6. Mr. SowediMuyingo CEO, Medical Access Uganda Limited7. Mr. Joseph Mwoga National Professional Officer, WHO Uganda Country Office8. Opio Sam Secretary, Pharmaceutical Society of Uganda9. Fred Kitutu Lecturer School of Pharmacy, Makerere University10. Denis Kibira Coordinator, MeTA Uganda
2.7 Data collection
Prior to data collection, all survey personnel participated in a training/briefing led by the survey manager. Data collectors were provided with introductory letters from Ministry of Health. At the district, data collectors introduced themselves and the purpose of the survey to the District Health Officer (DHO) before proceeding to collect data from the selected facilities.
At the facility, for each medicine, data on prices and availability of the lowest priced product that was physically available on the day of the visit were collected using a standard data collection form. The collected data was delivered to the survey manager at the coordinating office physically or by courier or post. Data collectors retained a copy of their data collection forms in case there was need for further verification. The HEPS Uganda Secretariat in Namirembe, Kampala acted as the central coordinating office to support the logistics for the survey.
11
No. 11: July-September 2013
2.8 Data validation, entry, analysis and management
The survey manager checked all the data collection forms for completeness and accuracy. Questionable entries were validated by contacting either the data collectors or the health facility or both. Validation of the data collection was conducted in 10% of the sampled outlets. This was done by calling the outlets using telephones contacts given on the data collection forms.
Data analysis was done using a customised WHO/HAI Excel workbook. Tables, graphs were generated for the report. Availability was determined as a percentage of facilities having a particular medicine on the day of the survey. Median price ratios (MPR) were calculated to compare prices between mission and private facilities. The following conditions were used to gauge affordability of medicines: Diabetes, hypertension, asthma, acute respiratory infection (ARI), peptic ulcers and malaria. The earning of the government’s lowest paid worker was used as a benchmark for affordability assessment.
12
UgandaMonitorMEDICINE P R I C E
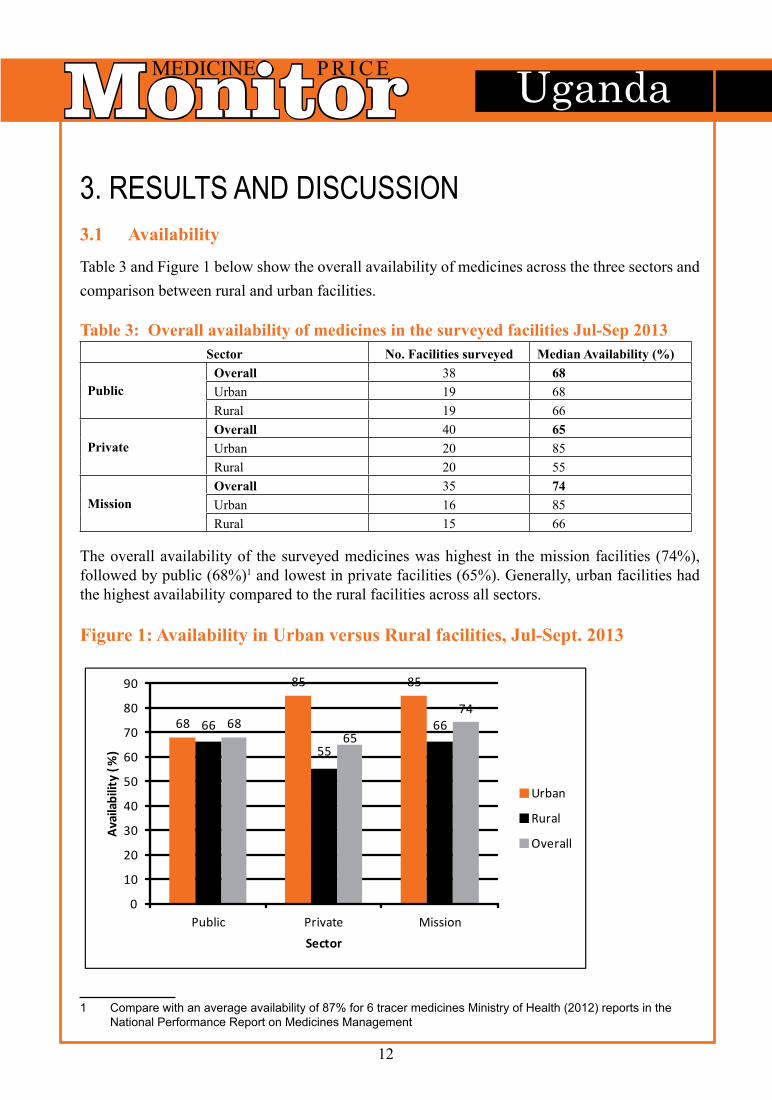
3. reSUltS anD DiScUSSion3.1 availability
Table 3 and Figure 1 below show the overall availability of medicines across the three sectors and comparison between rural and urban facilities.
Table 3: Overall availability of medicines in the surveyed facilities Jul-Sep 2013Sector No. facilities surveyed Median availability (%)
PublicOverall 38 68Urban 19 68Rural 19 66
PrivateOverall 40 65Urban 20 85Rural 20 55
MissionOverall 35 74Urban 16 85Rural 15 66
The overall availability of the surveyed medicines was highest in the mission facilities (74%), followed by public (68%)1 and lowest in private facilities (65%). Generally, urban facilities had the highest availability compared to the rural facilities across all sectors.
figure 1: availability in Urban versus rural facilities, Jul-Sept. 2013
1 Compare with an average availability of 87% for 6 tracer medicines ministry of health (2012) reports in the national performance report on medicines management
68
85 85
66
55
666865
74
0
10
20
30
40
50
60
70
80
90
Public Private Mission
Avai
labi
lity
(%)
Sector
Urban
Rural
Overall

13
No. 11: July-September 2013
There was a 2% difference in availability between urban and rural facilities in the public sector, 30% difference in the private sector and 19% in the mission sector. The big difference in availability between urban and rural facilities in the private sector can be attributed to the fact that drug shops and clinics are the most common drug outlets in the rural areas in Uganda and in urban areas pharmacies are the most predominant. According to NDA statute1, drug shops are licensed to stock only Class C drugs whereas pharmacies stock all classes of drugs, and this could have affected availability of some medicines.
a) Overall availability of the 40 essential medicines across the three sectors, Jul–Sep 2013
Table 4 below compares overall availability of the 40 essential medicines surveyed across the public, private, and mission sectors.
In the public sector, 45% (18/40) of the medicines were available in more than 75% •the facilities and 35% (14/40) were in less than 50% of the facilities
In the mission sector, 40% (16/40) of the medicines were found in more than 75% of •the facilities surveyed, whereas 12.5% (5/40) were in less than 50%.
In the private sector, 25% (10/40) of the medicines were in more than 75% of the •facilities, whereas 15% (6/40) were in less than 50% of facilities.
1 national drug policy and authority act 1993

14
UgandaMonitorMEDICINE P R I C E
Table 4: Overall availability of 40 essential medicines across sectorMedicine Overall availability (%)
Public sector Private sector Mission SectorAciclor tab 200mg 50 65 74Albendazole tab 200mg 37 30 46Amitriptyline tab 25mg 95 70 83Amoxicillin cap/tab 250mg 84 85 91Amoxicillin susp 250mg/5ml 11 75 74Artemether/Lumefantrine tab 20/120mg 89 75 89Bendrofluazide tab 5mg 71 53 69Betamethasone cream/ointment 1%w/v 32 60 43Carbamazepine tab 200mg 82 65 71Ceftriaxone 1g pwder for inj'n 76 68 83Cimetidine tab 400mg 8 38 34Ciprofloxacin tab 500mg 82 83 94Co-trimoxazolesusp 8/40 mg/ml 16 65 57Co-trimoxazole tab 400+80 mg 89 80 86Dextrose 5% inj 84 58 77Diazepam tab 5mg 95 80 74Diclofenac tab 50mg 58 95 83Doxycycline cap/tab 100mg 76 70 100Erythromycin tab 250mg 63 65 80Fluconazole tab /cap 200mg 32 38 49Furosemide tab 40mg 61 55 66Gentamycin inj 80mg/ml 45 63 80Glibenclamide tab 5mg 55 53 63Mebendazole tab 100mg 76 88 77Metformin tab 500mg 71 63 66Methyergometrineinj 200ug/ml 45 20 51Metronidazole susp 200mg/5ml 45 50 63Metronidazole tab 200mg 92 93 97Nifedipine retard tab 20mg 79 63 74Nystatinpessaries 100000iu 13 68 63Omeprazole cap 20mg 66 85 83Oral Rehydration Salt (ORS) 89 80 89Paracetamol tab 500mg 89 98 100Phenytoin tab 100mg 76 35 57Prednisolone tab 500mg 16 75 74Pyrimethamine /sulfadoxide (SP) tab 25/500mg 79 63 71Propranolol tab 40mg 39 65 69Quinimeinj 300mg/5ml 45 63 74Salbutamol inhaler 0.1mg(100mcg)/dose 11 43 37Tetracycline eye ointment 1% 89 60 69

15
No. 11: July-September 2013
b) a comparison of overall availability of selected anti-malarial medicines across the three sectors:
Figure 2 below compares the overall availability of artemether/lumefantrine 20/120mg and Sulfadoxine/Pyrimethamine used for treating uncomplicated malaria and prophylaxis of malaria during pregnancy respectively, across the three health sectors.
figure 2: comparison of overall availability of medicines for malaria across sectors
89
7975
63
89
71
0
10
20
30
40
50
60
70
80
90
100
Artemether/Lumefantrine • Sulphadoxine/Pyrimethamine
Avai
labi
lity
(%)
-malarial medicines
Public
Private
Mission
89% of the public and mission facilities had Artemether/Lumefantrine tablets 20/120mg in stock on the day of the visit compared to 75% of the private facilities.
Sulphadoxine/Pyrimethamine had the highest availability of 79% in the public facilities followed by mission (71%) and lowest in the private at 63%.

16
UgandaMonitorMEDICINE P R I C E
c) a comparison of overall availability of selected anti-diabetic medicines across the three sectors
Figure 3 below compares the overall availability of Glibenclamide 5mg and Metformin 500mg used in management of diabetes, across the three health sectors
figure 3: comparison of overall availability of medicines for diabetes across sectors
45
71
63 63
80
66
0
10
20
30
40
50
60
70
80
90
Glibenclamide 5mg
Avai
labi
lity
(%)
-
Public
Private
Mission
At least 60% of facilities in the public, private and mission sectors had Metformin 500mg in stock on the day of the survey. Glibenclamide 5mg was less available in the public sector (45%), but more available in the mission sector (80%).

17
No. 11: July-September 2013
d) a comparison of overall availability of selected anti-hypertensive medicines across the three sectors
Figure 4 below compares the overall availability of Nifedipine 20mg and propranolol used in management of hypertension, across the three health sectors.
fig. 4: comparison of overall availability of medicines for hypertension across sectors
79
39
63 65
7469
0
10
20
30
40
50
60
70
80
90
Nifedipine 20mg Propranolol
Avai
labi
lity
(%)
-hypertensive medicines
Public
Private
Mission
The public sector had the highest availability of Nifedipine 20mg (79%) and lowest availability of propranolol (39%) compared to other sectors.

18
UgandaMonitorMEDICINE P R I C E
e) a comparison of overall availability of selected paediatric formulations across the three sectors
Figure 4 below compares the overall availability of selected medicines formulated for paediatric use across the three health sectors
figure 5: comparison of overall availability of paediatric formulations across sectors
1116
45
75
65
50
74
5763
0
10
20
30
40
50
60
70
80
Amoxicillin susp Cotrimoxazole susp Metronidazole susp
Avai
labi
lity
(%)
Public
Private
Mission
The Public sector had the lowest availability of appropriate paediatric formulations: amoxicillin suspension 125mg/5ml in 11% of facilities, cotrimoxazole syrup 8/40mg in 16% and metronidazole syrup in 45% of public facilities.

19
No. 11: July-September 2013
3.2 Medicine prices
Table 5: Comparison of medicine median price ratios between and within private and mission sectors.
PrivUrb/Privrural MisUrb/Misrural PrivUrb/MisUrb Privrural/Misrural
No. of times more expensive 1.00 1.12 1.00 1.00No. of Pairs Compared 37 40 40 37
As shown in table 5 above, the prices charged to consumers for medicines in the private facilities were comparable across urban and rural facilities (ratio 1:1). However, in the mission facilities medicines were 12% more expensive in the urban than rural facilities (ratio 1:1.12).
Medicine prices were comparable between urban private and mission facilities and in rural private and mission facilities (ratio 1:1).
Table 6 below shows the median consumer prices per unit of selected medicines in the private and mission facilities. There was no difference in price of 25 of the medicines between mission and private facilities. A marked 50% and above price difference between prices in the private and mission sectors were noted for Mebendazole 100mg, Diclofenac 50mg , carbamazepine 200mg, Albendazole 200mg, Artmetther/Lumefantrine 20/120mg and Prednisolone tablets.
More information on prices is in annex 2.

20
UgandaMonitorMEDICINE P R I C E
Table 6: Median unit price of the 40 medicines in the private and mission facilities
MedicineMedian unit price (Ushs.)
% price differencePrIVaTe SecTOr
MISSION SecTOr
Aciclor tab 200mg 300.0 300.0 0.0Albendazole tab 200mg 1000.0 500.0 50.0Amitriptyline tab 25mg 100.0 100.0 0.0Amoxicillin cap/tab 250mg 100.0 100.0 0.0Amoxicillin susp 250mg/5ml 30.0 30.0 0.0Artemether/Lumefantrine tab 20/120mg 250.0 125.0 50.0Bendrofluazide tab 5mg 100.0 100.0 0.0Betamethasone cream/ointment 1%w/v 200.0 166.7 16.7Carbamazepine tab 200mg 100.0 150.0 50.0Ceftriaxone 1g pwder for inj'n 3000.0 3250.0 8.3Cimetidine tab 400mg 200.0 200.0 0.0Ciprofloxacin tab 500mg 250.0 250.0 0.0Co-trimoxazolesusp 8/40 mg/ml 30.0 30.0 0.0Co-trimoxazole tab 400+80 mg 100.0 100.0 0.0Dextrose 5% inj 2000.0 2000.0 0.0Diazepam tab 5mg 100.0 100.0 0.0Diclofenac tab 50mg 50.0 80.0 60.0Doxycycline cap/tab 100mg 100.0 100.0 0.0Erythromycin tab 250mg 200.0 200.0 0.0Fluconazole tab /cap 200mg 1000.0 1000.0 0.0Furosemide tab 40mg 100.0 100.0 0.0Gentamycin inj 80mg/ml 800.0 800.0 0.0Glibenclamide tab 5mg 100.0 100.0 0.0Mebendazole tab 100mg 50.0 100.0 100.0Metformin tab 500mg 200.0 150.0 25.0Methyergometrineinj 200ug/ml 2000.0 1100.0 45.0Metronidazole susp 200mg/5ml 27.5 25.0 9.1Metronidazole tab 200mg 50.0 66.7 33.3Nifedipine retard tab 20mg 200.0 200.0 0.0Nystatinpessaries 100000iu 285.7 300.0 5.0Omeprazole cap 20mg 200.0 250.0 25.0Oral Rehydration Salt (ORS) 500.0 500.0 0.0Paracetamol tab 500mg 50.0 50.0 0.0Phenytoin tab 100mg 100.0 100.0 0.0Prednisolone tab 500mg 100.0 50.0 50.0Pyrimethamine /sulfadoxide (SP) tab 25/500mg 500.0 500.0 0.0Propranolol tab 40mg 100.0 100.0 0.0Quinimeinj 300mg/5ml 1000.0 1100.0 10.0Salbutamol inhaler 0.1mg(100mcg)/dose 8000.0 8000.0 0.0Tetracycline eye ointment 1% 571.4 500.0 12.5

21
No. 11: July-September 2013
d) affordability
Affordability was calculated as the number of days the lowest paid government worker would have to pay for one treatment course of an acute condition or one month’s treatment of a chronic condition. Treatments less than or equal to one days’ wages are considered affordable. The monthly earning of the lowest paid government worker is UShs. 222,976 (U8L) before tax, and after tax it is Ushs. 156,083. This gives daily wage of about 5200 (2.00 US$) as take home. Table 7 below shows the number of days it would take the lowest paid government worker to pay for treatment of the most common diseases in the private and mission sectors.
Table 7: affordability (Daily wage of lowest paid government worker is Ushs. 5200)
condition Select MedicineTreatment duration (in days)
# of units per treatment
MTP (Ushs.) Days' wages
Private MissionPrivate(MTP/5200)
Mission(MTP/5200)
Adult Malaria
Artemether/Lumefantrine tab 20/120mg 3 24 6000 3000 1.2 0.6
Adult RTI
Amoxicillin cap/tab 250mg 7 42 4200 4200 0.8 0.8Ceftriaxone 1g pwder for inj'n 1 1 3000 3250 0.6 0.6Ciprofloxacin tab 500mg 7 14 3500 3500 0.7 0.7
Anxiety Diazepam tab 5mg 7 7 700 700 0.1 0.1
Arthritis Diclofenac tab 50mg 30 60 3000 4800 0.6 0.9
AsthmaSalbutamol inhaler 0.1mg/dose as need 200 8000 8000 1.5 1.5
Depression Amitriptyline tab 25mg 30 90 9000 9000 1.7 1.7
Diabetes Glibenclamide tab 5mg 30 60 6000 6000 1.2 1.2
HypertensionNifedipine retard tab 20mg 30 30 6000 6000 1.2 1.2
Paediatric RTICo-trimoxazolesusp 8/40 mg/ml 7 70 2100 2100 0.4 0.4
Pain/Inflammation Paracetamol tab 500mg 3 18 900 900 0.2 0.2
Ulcer Omeprazole cap 20mg 30 30 6000 7500 1.2 1.4
In both the private and mission sectors medicines for treatment of chronic conditions like asthma, depression, diabetes, hypertension and ulcers cost more than a day’s wage.
22
UgandaMonitorMEDICINE P R I C E
4. conclUSionThe overall availability of the surveyed medicines was 68% in the public facilities, •65% in private and 74% in mission facilities
More of urban based facilities had medicines available than rural, a big difference of •30% being in the private sector
89% of the public and mission facilities had Artemether/Lumefantrine 20/120mg •tablets physically available on the day of the survey compared to 75% of the private
Medicines for the most common non-communicable diseases (diabetes and hypertension) •were found available in less than 70% of the facilities across the 3 sectors
The public facilities had a very low availability of paediatric formulations: amoxicillin •suspension (11%), cotrimoxazole syrup (16%) and metronidazole syrup (45%)
Medicine prices were comparable between urban and rural facilities in the private •sector (median price ratio). However, medicines were 12% more expensive in urban than rural mission facilities
There was no difference in price of 25 out of the 40 essential medicines surveyed •between mission and private facilities
In the private and mission sector, medicines for chronic conditions like asthma, •depression, diabetes, hypertension and ulcers cost more than a day’s wage for the lowest paid government worker in Uganda. However, the following conditions are affordable in both sectors by the lowest paid government worker: RTI (both adult &paediatric), anxiety, arthritis and pain/inflammation

23
No. 11: July-September 2013
referenceSUganda: Health Sector Strategic Investment Plan 2010/11-2014/15•
Madden JM, Meza E, Ewen M, Laing RO, Stephens P, Ross-Degnan D. Measuring •medicine prices in Peru: validation of key aspects of WHO/HAI survey methodology. Rev PanamSaludPublica. 010;27 (4):291–9
MeTA Uganda Work Plan, 2012•
Ministry of Health 2008b.Access to and use of medicines by Households in Uganda, •Report. Kampala, Uganda.
Ministry of Health, 2002.Pharmaceutical Baseline Survey, Report. Kampala, •Uganda.
Ministry of Health, 2008a.Pharmaceutical Situation Assessment, Report. Kampala, •Uganda.
Ministry of Health, 2010. WHO, HAI (HEPS) Medicine Price Monitor Volume 1-8. •Kampala, Uganda.
Ministry of Health.MoH., 2008.Access to and use of medicines by households in •Uganda. Kampala: Ministry of Health.MoH.
World Health Organisation, 2006. Health Financing: A basic guide. WHO; Western •Pacific Region.
www.haiweb.org/medicineprice• s

24
UgandaMonitorMEDICINE P R I C Ea
nnex
1: M
onito
ring
ava
ilabi
lity
and
Pric
es o
f Med
icin
e in
Uga
nda:
Lis
t of f
acili
ties –
aug
ust,
2013
re
GIO
NM
ISSI
ON
(40)
PU
BL
Ic (4
0)Pr
IVaT
e (4
0)ur
ban
(20)
rura
l (20
)ur
ban
(20)
rura
l (20
)ur
ban
(20)
rura
l (20
)Ea
ster
n R
egio
n 1.
Kam
uli m
issi
on
Hos
pita
l 2.
Isla
mic
Uni
vers
ity
HC
Mba
le3.
Ahm
adiy
a H
C M
bale
4.St
- Aus
tin H
C M
bale
1.Ir
apa
chur
ch o
f God
HU
K
amul
i2.
St F
ranc
is B
ulub
a ho
spita
l May
uge
3. K
olon
yi h
ealth
ce
ntre
Mba
le
1.Ji
nja
Reg
iona
l Ref
ho
spita
l 2.
Mba
le re
gion
al R
ef
hosp
ital
3.Ig
anga
hos
pita
l4.
Kam
uli G
ovt
hosp
ital
5.Pa
llisa
ho
spita
l
1.W
aluk
uba
HC
2.
Buw
enge
HC
jin
ja
3. B
udad
iri H
C
Mba
le4.
Bub
ulo
HC
M
bale
5.
Bud
uda
hosp
ital
1.G
ilead
pha
rmac
y 2.
Ran
a m
edic
al c
ente
r 3.
Sky
phar
mac
y M
bale
2 cl
inic
s 3
Dru
g sh
ops
Nor
ther
n1.
St M
ary’
s Hos
pita
l La
corG
ulu
2.PA
G h
ealth
uni
t L
ira
3.A
muc
a di
spen
sary
Li
ra 4
.Nge
eta
hosp
ital
Lira
1.A
mai
hos
pita
l Lira
2.O
pit H
C
3.A
loi H
C L
ira
4. A
liwan
g H
C L
ira
5.A
lany
i HC
Lira
1.G
ulu
regi
onal
Ref
ho
spita
l2.
Lira
regi
onal
Ref
ho
spita
l3.
Am
aka
hosp
ital G
ulu
1.O
gur H
C2.
Am
uc H
C L
ira
3. D
okol
o H
C
4.
Lal
ogi H
C G
ulu
1.Fe
liest
a ph
arm
acy
Lira
2.G
ulu
inde
pend
ant
hosp
ital
3.
Opi
os c
linic
Gul
u
4.K
akan
yero
pha
rmac
y G
ulu
2 cl
inic
s
3
Dru
g sh
ops
Cen
tral
1.N
sam
bya
hosp
ital
2.R
ubag
a ho
spita
l
3.M
engo
hos
tal
4.K
isub
i hos
pita
l
1.N
koko
njer
u ho
spta
l 2.
Muk
ono
Hos
pita
l
3.N
agal
ama
hosp
ital
4.St
.Ste
phen
s dis
pens
ary
Mpe
rerw
e
5.M
akon
ge c
omm
unity
HC
M
ukon
o
1.M
ulag
o ho
spis
tal
2.B
utab
ika
hosp
ital 3
.Ent
ebbe
gr
ade
B h
ospi
tal
4.M
aker
ere
Uni
vers
ity
hosp
ital
1.K
ayun
ga h
ospi
tal
2.K
awol
o ho
spita
l 3
.Muk
ono
HC
4
4.
Gom
be h
ospi
tal
or a
ny H
C 4
1.Fr
osa
phar
mac
y N
akul
abye
2.G
enes
is p
harm
acy
Lu
zira
3.B
ugol
obi
mat
erni
ty
4.C
ase
clin
ic
4.K
adic
clin
ic
2 cl
inic
s
3
Dru
g sh
ops
Wes
tern
1.
Iban
da H
ospi
tal
2.Is
haka
Hos
pita
l3.
Ruh
aro
hosp
ital
4.K
isiz
i Hos
pita
l
1.N
yaki
bale
Hos
pita
l R
ukug
iri2.
Kya
muh
anga
Hos
pita
l B
ushe
nyi
3.R
ushe
re h
ospi
tal
Mba
rara
4.N
yaki
shen
yi H
C4
1.M
bara
ra R
eg H
osp
2.K
itaga
ta H
ospi
tal
Bus
heny
i3.
Itojo
Hos
pita
l4.
Kam
buga
Hos
pita
l R
ukun
giri
1.N
akiv
ule
HC
42.
Isho
ngor
era
HC
43.
Nsh
enge
zi H
C 4
4.B
wiz
ibw
era
1..M
ayan
ja m
emor
ial
2.M
bara
ra C
omm
unity
3.
Mul
tiple
pha
rmac
ist
4.M
uilti
care
pha
rcac
y
2 cl
inic
s 3
Dru
g sh
ops

25
No. 11: July-September 2013a
nnex
2: M
onito
ring
Pri
ces a
nd a
vaila
bilit
y of
Med
icin
es in
Uga
nda:
Dat
a c
olle
ctio
n fo
rm –
aug
ust 2
013
faci
lity
Nam
e:a
ddre
ss o
f fac
ility
:
fac
ility
Tel
epho
ne:
faci
lity
fax:
faci
lity
em
ail:
faci
lity
cod
e:
Type
of h
ealth
faci
lity
(Tic
k):
Pub
lic
Mis
sion
Pri
vate
reg
ion:
Dis
tric
t:Se
ttin
g (T
ick)
:
U
rban
r
ural
Dat
a co
llect
orN
ame
:M
obile
:e
-mai
l:
Dat
e of
dat
a co
llect
ion:
(DD
/MM
/Y
YY
Y)
/
/
INST
rU
cT
ION
S
1.
Faci
lity
info
rmat
ion:
Mak
e su
re th
at y
ou fi
ll al
l cel
ls o
f the
abo
ve ta
ble.
•
If fa
x or
e-m
ail d
on’t
exis
t put
“N
/A”
to in
dica
te n
ot a
vaila
ble
2.
Iden
tifyi
ng p
rodu
cts f
or p
rice
mon
itorin
g:
Iden
tify
prod
ucts
with
•
thee
xact
stre
ngth
and
dos
age
form
for e
ach
med
icin
e lis
ted
that
are
phy
sica
lly a
vaila
ble
for s
ale
or d
ispe
nsin
g on
the
day
of th
e da
ta c
olle
ctio
n
Mak
e su
re th
at y
ou d
o no
t mis
take
nly
incl
ude
prod
ucts
that
are
of d
iffer
ent
•st
reng
ths o
r for
mul
atio
ns (e
.g. s
low
rele
ase
tabl
et in
stea
d of
regu
lar t
able
t; or
nas
al sp
ray
inst
ead
of in
hale
r; or
com
bina
tion
prod
ucts
whi
ch in
clud
e an
othe
r act
ive
ingr
edie
nt)
Do
not w
rite
dow
n pr
ice
info
rmat
ion
if th
e co
rrec
t pro
duct
is
•no
t ph
ysic
ally
ava
ilabl
e in
the
heal
th fa
cilit
y on
the
day
of d
ata
colle
ctio
n. P
ut
“N/A
” un
der p
rodu
ct n
ame
to in
dica
te n
ot a
vaila
ble
3.
Rec
ordi
ng d
ata
for p
rice
mon
itorin
g:Yo
u•
MU
ST w
rite
dow
n th
e pr
oduc
t nam
e (th
at is
trad
e na
me
or b
rand
na
me)
, the
nam
e an
d co
untry
of t
he m
anuf
actu
rer,
actu
al p
ack
size
and
pa
ck p
rice
foun
d fo
r the
pro
duct
with
the
low
est p
rice
Dis
coun
ts:
• R
ecor
d di
scou
nt a
s % a
nd th
e di
scou
nted
pric
e on
ly w
hen
sam
e di
scou
nt is
ava
ilabl
e fo
r al
l pat
ient
s
If m
edic
ines
are
free
to p
atie
nts l
ike
in th
e pu
blic
sect
or fa
cilit
ies,
•re
cord
all
prod
uct d
etai
ls a
nd w
rite
0 in
the
Pack
Pric
e ce
ll
4.
Cal
cula
ting
the
unit
or p
ack
pric
e:Fo
r pro
duct
s whe
re p
ack
pric
e is
giv
en; d
ivid
e th
e pa
ck p
rice
by th
e •
pack
size
foun
d (p
ack
pric
e/pa
ck si
ze) t
o ge
t uni
t pric
e an
d w
rite
it do
wn
up to
four
dec
imal
s (e.
g 0.
1234
) in
the
Uni
t Pric
e ce
ll.
For
pro
duct
s whe
re u
nit p
rice
is g
iven
; mul
tiply
the
unit
pric
e by
the
•pa
ck si
ze fo
und
(uni
t pric
e x
pack
size
) to
get p
ack
pric
e an
d w
rite
it in
the
pack
size
cel
l
If th
e di
scou
nt is
app
lied
for a
ll pa
tient
s, th
en c
alcu
late
the
unit
•pr
ice
from
the
disc
ount
ed p
ack
pric
e on
ly.
5.
fina
l ste
ps:
Plea
se c
heck
that
all
data
is c
orre
ctly
reco
rded
and
dou
ble
chec
k un
it •
pric
e ca
lcul
atio
ns b
efor
e se
ndin
g th
e da
ta c
olle
ctio
n fo
rms t
o th
e Su
rvey
Man
ager
Send
com
plet
ed d
ata
colle
ctio
n fo
rms b
y co
urie
r or h
and
deliv
er
•as
soon
as p
ossi
ble
to: H
EPS-
Uga
nda,
P.O
. Box
242
6, K
ampa
la,
Bal
intu
ma
Roa
d, M
engo
If y
ou h
ave
any
ques
tions
ple
ase
phon
e th
e su
rvey
man
ager
(Gild
oOku
re)
at +
2567
82-9
5933
6 or
e-m
ail t
o od
uffo
rd@
gmai
l.com

26
UgandaMonitorMEDICINE P R I C E
Med
icin
e nam
e,
dosa
ge fo
rm,
stre
ngth
Prod
uct
of
inte
rest
avai
labl
e?(“
yes”
or
“N/a
”)
Prod
uct n
ame
(bra
nd /
trad
e na
me)
Man
ufac
ture
r, co
untr
y of
m
anuf
actu
re
Pack
siz
e foun
d
Pack
pr
ice
Uni
t pri
ce (4
di
gits
)
Disc
ount
fo
r all?
Yes
%
Disc
ount
ed
pack
pri
cec
omm
ents
and
ob
serv
atio
ns
Aci
clov
ir ta
b 20
0mg
Low
est
pric
ed/ta
b
%
Alb
enda
zole
tab
200m
gLo
wes
t pr
ice
/tab
%
Am
itrip
tylin
e ta
b 25
mg
Low
est
pric
ed/ta
b
%
Am
oxic
illin
cap
25
0mg
Low
est
pric
ed/c
ap
%
Am
oxic
illin
Sus
p 12
5mg/
5ml
Low
est
pric
ed/m
l
%
Arte
met
her/
Lum
efan
trine
tab
20/1
20m
g
Low
est
pric
ed/ta
b
%
Ben
druo
fluaz
ide
tab
5mg
Low
est
pric
ed/ta
b
%
Bet
amet
haso
ne
crea
m/o
intm
ent
1% w
/v
Low
est
pric
ed/g
ram
%
Car
bam
azep
ine
tab
200m
gLo
wes
t pr
iced
/tab
%
Cef
triax
one
1g
pow
der f
or in
jLo
wes
t pr
ice
/via
l
%
Cim
etid
ine
tab
400m
gLo
wes
tpr
iced
/tab
%
Cip
roflo
xaci
n ta
b 50
0mg
Low
est
pric
ed/ta
b
%

27
No. 11: July-September 2013M
edic
ine n
ame,
do
sage
form
, st
reng
th
Prod
uct
of
inte
rest
avai
labl
e?(“
yes”
or
“N/a
”)
Prod
uct n
ame
(bra
nd /
trad
e na
me)
Man
ufac
ture
r, co
untr
y of
m
anuf
actu
re
Pack
siz
e foun
d
Pack
pr
ice
Uni
t pri
ce (4
di
gits
)
Disc
ount
fo
r all?
Yes
%
Disc
ount
ed
pack
pri
cec
omm
ents
and
ob
serv
atio
ns
Cot
rimox
azol
e Su
sp
40/2
00m
g/5m
l
Low
est
pric
ed/m
l
%
Cot
rimox
azol
e ta
b48
0mg
Low
est
pric
ed/ta
b
%
Dex
trose
5%
inj
Low
est
pric
e/b
ottle
%
Dia
zepa
m ta
b 5m
gLo
wes
t pr
iced
/tab
%
Dic
lofe
nac
tab
50m
gLo
wes
t pr
iced
/tab
%
Dox
ycly
clin
e ca
p 10
0mg
Low
est
pric
e/c
ap
%
Eryt
hrom
ycin
tab
250m
gLo
wes
t pr
iced
/tab
%
Fluc
onaz
ole
tab
/ ca
p 20
0mg
Low
est
pric
ed/ c
ap
%
Furo
sem
ide
tab
40m
gLo
wes
t pr
iced
/tab
%
Gen
tam
ycin
inj
80m
g/2m
lLo
wes
t pr
iced
/Am
p
%
Glib
encl
amid
e ta
b 5m
gLo
wes
t pr
iced
/tab
%
Meb
enda
zole
tab
100m
gLo
wes
t pr
iced
/tab
%

28
UgandaMonitorMEDICINE P R I C EM
edic
ine n
ame,
do
sage
form
, st
reng
th
Prod
uct
of
inte
rest
avai
labl
e?(“
yes”
or
“N/a
”)
Prod
uct n
ame
(bra
nd /
trad
e na
me)
Man
ufac
ture
r, co
untr
y of
m
anuf
actu
re
Pack
siz
e foun
d
Pack
pr
ice
Uni
t pri
ce (4
di
gits
)
Disc
ount
fo
r all?
Yes
%
Disc
ount
ed
pack
pri
cec
omm
ents
and
ob
serv
atio
ns
Met
form
in ta
b 50
0mg
Low
est
pric
ed/ta
b
%
Met
hyer
gom
et-
rinei
nj 2
00μg
/ml
/Am
p
%
Met
roni
dazo
le
Susp
200
mg/
5ml
Low
est
pric
ed/m
l
%
Met
roni
dazo
le ta
b 20
0mg
Low
est
pric
e/ta
b
%
Nife
dipi
ne re
tard
ta
b 20
mg
Low
est
pric
ed/ta
b
%
Nys
tatin
pess
arie
s 10
0,00
0 I.U
.Lo
wes
t pr
iced
/tab
%
Om
epra
zole
cap
20
mg
Low
est
pric
ed/c
ap
%
Ora
l Reh
ydra
tion
Salt
(OR
S)Lo
wes
t pr
ice
/sac
h
%
Para
ceta
mol
tab
500m
gLo
wes
t pr
iced
/tab
%
Phen
ytoi
n ta
b 10
0mg
Low
est
pric
ed/ta
b
%
Pred
niso
lone
tab
5m
gLo
wes
t pr
iced
/tab
%

29
No. 11: July-September 2013M
edic
ine n
ame,
do
sage
form
, st
reng
th
Prod
uct
of
inte
rest
avai
labl
e?(“
yes”
or
“N/a
”)
Prod
uct n
ame
(bra
nd /
trad
e na
me)
Man
ufac
ture
r, co
untr
y of
m
anuf
actu
re
Pack
siz
e foun
d
Pack
pr
ice
Uni
t pri
ce (4
di
gits
)
Disc
ount
fo
r all?
Yes
%
Disc
ount
ed
pack
pri
cec
omm
ents
and
ob
serv
atio
ns
Pyrim
etha
min
e/Su
lfado
xine
tab
25/5
00m
g
Low
est
pric
ed/ta
b
%
Prop
rano
lol t
ab
40m
gLo
wes
t pr
iced
/tab
%
Qui
nine
inj
300m
g/2m
lLo
wes
t pr
iced
/Am
p
%
Salb
utam
ol
inha
ler 0
.1m
g/do
se
Low
est
pric
ed/c
an
%
Tetra
cycl
ine
eye
oint
men
t 1%
Low
est
pric
ed/g
ram
%

30
UgandaMonitorMEDICINE P R I C E
annex 3: availability of the 40 medicines in Urban versus rural facilities across the sectorsMedicine Urban rural
Public Private Mission Public Private Mission
Aciclor tab 200mg 53% 80% 81% 47% 50% 68%
Albendazole tab 200mg 26% 45% 38% 47% 15% 53%
Amitriptyline tab 25mg 100% 95% 94% 89% 45% 74%
Amoxicillin cap/tab 250mg 89% 100% 100% 79% 70% 84%
Amoxicillin susp 250mg/5ml 11% 85% 88% 11% 65% 63%
Artemether/Lumefantrine tab 20/120mg 89% 85% 81% 89% 65% 95%
Bendrofluazide tab 5mg 68% 80% 88% 74% 25% 53%
Betamethasone cream/ointment 1%w/v 16% 65% 44% 47% 55% 42%
Carbamazepine tab 200mg 79% 85% 94% 84% 45% 53%
Ceftriaxone 1g pwder for inj'n 84% 85% 94% 68% 50% 74%
Cimetidine tab 400mg 0% 50% 25% 16% 25% 42%
Ciprofloxacin tab 500mg 84% 95% 100% 79% 70% 89%
Co-trimoxazolesusp 8/40 mg/ml 11% 70% 75% 21% 60% 42%
Co-trimoxazole tab 400+80 mg 84% 80% 81% 95% 80% 89%
Dextrose 5% inj 95% 60% 75% 74% 55% 79%
Diazepam tab 5mg 95% 90% 81% 95% 70% 68%
Diclofenac tab 50mg 68% 90% 88% 47% 100% 79%
Doxycycline cap/tab 100mg 79% 80% 100% 74% 60% 100%
Erythromycin tab 250mg 63% 80% 94% 63% 50% 68%
Fluconazole tab /cap 200mg 26% 65% 56% 37% 10% 42%
Furosemide tab 40mg 47% 85% 75% 74% 25% 58%
Gentamycin inj 80mg/ml 58% 70% 88% 32% 55% 74%
Glibenclamide tab 5mg 58% 85% 75% 53% 20% 53%
Mebendazole tab 100mg 74% 90% 69% 79% 85% 84%
Metformin tab 500mg 79% 90% 88% 63% 35% 47%
Methyergometrineinj 200ug/ml 42% 30% 56% 47% 10% 47%
Metronidazole susp 200mg/5ml 42% 45% 69% 47% 55% 58%
Metronidazole tab 200mg 95% 95% 94% 89% 90% 100%
Nifedipine retard tab 20mg 79% 90% 88% 79% 35% 63%
Nystatinpessaries 100000iu 5% 75% 81% 21% 60% 47%
Omeprazole cap 20mg 74% 85% 94% 58% 85% 74%
Oral Rehydration Salt (ORS) 95% 90% 88% 84% 70% 89%
Paracetamol tab 500mg 100% 95% 100% 79% 100% 100%
Phenytoin tab 100mg 68% 50% 69% 84% 20% 47%
Prednisolone tab 500mg 16% 95% 94% 16% 55% 58%
Pyrimethamine /sulfadoxide (SP) tab 25/500mg 84% 65% 69% 74% 60% 74%
Propranolol tab 40mg 37% 85% 88% 42% 45% 53%
Quinimeinj 300mg/5ml 63% 60% 88% 26% 65% 63%
Salbutamol inhaler 0.1mg(100mcg)/dose 5% 60% 50% 16% 25% 26%
Tetracycline eye ointment 1% 84% 85% 63% 95% 35% 74%

31
No. 11: July-September 2013annex 4: Median unit price of the 40 medicines in the urban versus rural facilities
Medicine Urban rural
Private Mission % price diff. Private Mission % price diff.
Aciclor tab 200mg 300.0 350.0 -16.7 275.0 275.0 0.0
Albendazole tab 200mg 1000.0 700.0 30.0 400.0 #VALUE!
Amitriptyline tab 25mg 100.0 100.0 0.0 100.0 100.0 0.0
Amoxicillin cap/tab 250mg 100.0 100.0 0.0 100.0 100.0 0.0
Amoxicillin susp 250mg/5ml 30.0 27.5 8.3 25.0 30.0 -20.0
Artemether/Lumefantrine tab 20/120mg 250.0 166.7 33.3 208.3 125.0 40.0
Bendrofluazide tab 5mg 100.0 100.0 0.0 150.0 100.0 33.3
Betamethasone cream/ointment 1%w/v 200.0 183.3 8.3 200.0 133.3 33.3
Carbamazepine tab 200mg 100.0 150.0 -50.0 200.0 100.0 50.0
Ceftriaxone 1g pwder for inj'n 2500.0 5000.0 -100.0 3000.0 3000.0 0.0
Cimetidine tab 400mg 200.0 150.0 25.0 200.0 200.0 0.0
Ciprofloxacin tab 500mg 300.0 275.0 8.3 250.0 250.0 0.0
Co-trimoxazolesusp 8/40 mg/ml 30.0 30.0 0.0 30.0 30.0 0.0
Co-trimoxazole tab 400+80 mg 100.0 85.0 15.0 75.0 100.0 -33.3
Dextrose 5% inj 2000.0 2000.0 0.0 2000.0 2000.0 0.0
Diazepam tab 5mg 100.0 100.0 0.0 100.0 100.0 0.0
Diclofenac tab 50mg 50.0 50.0 0.0 50.0 100.0 -100.0
Doxycycline cap/tab 100mg 100.0 125.0 -25.0 100.0 100.0 0.0
Erythromycin tab 250mg 200.0 200.0 0.0 200.0 150.0 25.0
Fluconazole tab /cap 200mg 1000.0 1000.0 0.0 600.0 #VALUE!
Furosemide tab 40mg 100.0 100.0 0.0 50.0 87.5 -75.0
Gentamycin inj 80mg/ml 750.0 800.0 -6.7 800.0 700.0 12.5
Glibenclamide tab 5mg 100.0 100.0 0.0 100.0 100.0 0.0
Mebendazole tab 100mg 50.0 100.0 -100.0 50.0 75.0 -50.0
Metformin tab 500mg 200.0 200.0 0.0 200.0 100.0 50.0
Methyergometrineinj 200ug/ml 2000.0 1350.0 32.5 1000.0 #VALUE!
Metronidazole susp 200mg/5ml 30.0 25.0 16.7 25.0 25.0 0.0
Metronidazole tab 200mg 100.0 100.0 0.0 50.0 50.0 0.0
Nifedipine retard tab 20mg 200.0 200.0 0.0 150.0 150.0 0.0
Nystatinpessaries 100000iu 357.1 292.9 18.0 200.0 300.0 -50.0
Omeprazole cap 20mg 300.0 300.0 0.0 200.0 200.0 0.0
Oral Rehydration Salt (ORS) 500.0 500.0 0.0 500.0 500.0 0.0
Paracetamol tab 500mg 50.0 50.0 0.0 30.0 50.0 -66.7
Phenytoin tab 100mg 100.0 100.0 0.0 75.0 100.0 -33.3
Prednisolone tab 500mg 100.0 70.0 30.0 50.0 50.0 0.0
Pyrimethamine /sulfadoxide (SP) tab 25/500mg
500.0 500.0 0.0 500.0 500.0 0.0
Propranolol tab 40mg 100.0 100.0 0.0 100.0 50.0 50.0
Quinimeinj 300mg/5ml 1000.0 1100.0 -10.0 1200.0 1250.0 -4.2
Salbutamol inhaler 0.1mg(100mcg)/dose 8000.0 8000.0 0.0 8000.0 7500.0 6.3
Tetracycline eye ointment 1% 571.4 857.1 -50.0 428.6 428.6 0.0

32
For more information contact:
HePs-UgandaCoalition for Health Promotion & social development
Plot 351a, Balintuma road, namirembeP.o. Box 2426, Kampala, Uganda
tel: +256-414-270970email: [email protected]: www.heps.or.ug
this work is licensed underhttp://creativecommons.org/licenses/by/3.0/ug/