
Mondastri K Sudaryo , Besral , Ajeng T Endarti , Meidy F ... · Mount Kelud is an active volcano,...
18
Mondastri K Sudaryo 1 , Besral 1 , Ajeng T Endarti 1 , Meidy F Prameswari 1 , Barbara Chicon 2, Debarati Guha-Sapir 2 1. HRCCD, FPH, UI, Indonesia 2. CRED, UCL, Belgium
Transcript of Mondastri K Sudaryo , Besral , Ajeng T Endarti , Meidy F ... · Mount Kelud is an active volcano,...

Mondastri K Sudaryo1, Besral1, Ajeng T Endarti1, Meidy F Prameswari1, Barbara Chicon2, Debarati Guha-Sapir2
1. HRCCD, FPH, UI, Indonesia2. CRED, UCL, Belgium
Mount Kelud is an active volcano, located 120 km SW of Surabaya (capital city of East-Java Province), Indonesia and surrounded by districts Kediri, Blitar and Malang. Since 1919, Kelud had erupted several times and till mid of Oct. 2007 the alert status of Mt. Kelud had been raised to the highest level indicating serious continuing threatsOn Oct, 16 2007, local authorities in Kediri and Blitar had commenced a massive evacuation of 116,736 people, but about 25,000 people still remained in the dangerous zoneThe hazard of erupted material exposing human and the complexities of massive evacuation may direct or indirectly generate acute or chronic health impacts.

The study objective was:
to assess health problems related to eruption and evacuation, including the health status of children living in vulnerable villages in Kediri districts which were close to the crater of Kelud volcano.
Quantitative: -Population-based cross-sectional (survey):-Using multistage cluster sampling, randomly selecting:433 HH, including 89 under-five children living in HH in both “Circle-1” (within 10 km radius from crater) and in “Circle-2” (within 10-15 km)
Qualitative: (not fully presented here)

First Circle (radius 5-10 km): 216 HH Second Circle (radius 10-15 km): 217 HHNGANCAR_SEMPU1.NGANCAR_SUGIHWARAS2.PLOSOKLATEN_SEPAWON3.PUNCU_PUNCU4.KEPUNG_KEBONREJO5.KEPUNG_BESOWO6.KEPUNG_DAMARWULAN
NGANCAR_MANGGIS1.NGANCAR_NGANCAR2.PLOSOKLATEN_TRISULO3.PUNCU_SATAK4.PUNCU_ASMOROBANGUN5.KEPUNG_KAMPUNGBARU6.KEPUNG_SIMAN7.NGANCAR_BABADAN8.PUNCU_WONOREJO9.PUNCU_SIDOMULYO10.KEPUNG_BRUMBUNG11.KEPUNG_KEPUNG
F ig u r e . 1 . M a p o f K e lu d V o lc a n o A r e a
C r a t e r
E v a c u a t io n r o u t e
C ir c le - 1 C ir c le - 2
STUDY SITES
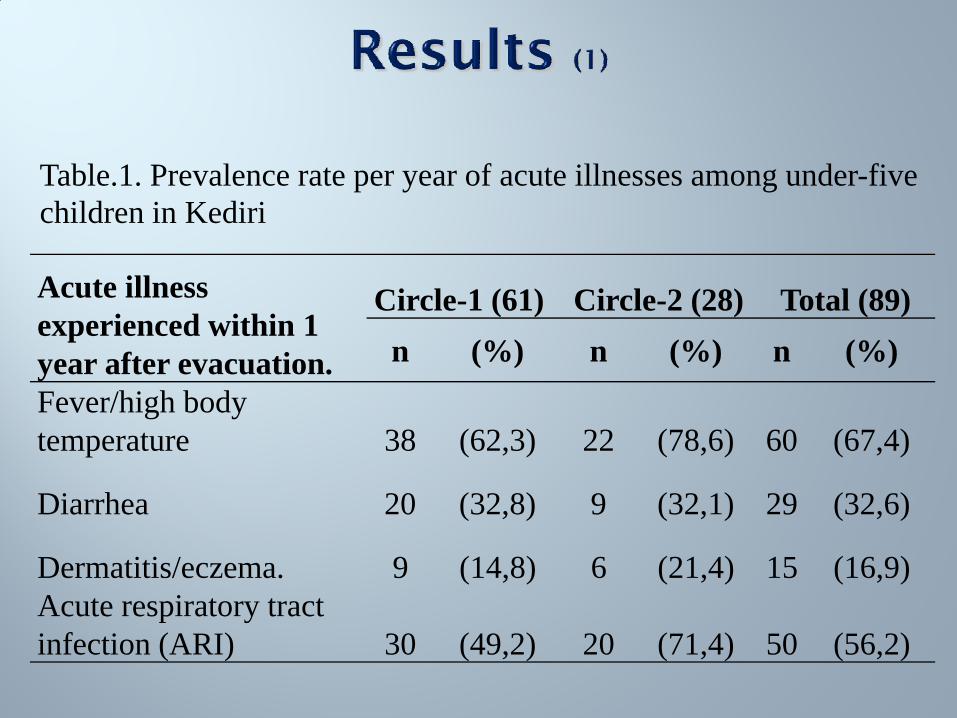
Acute illness experienced within 1 year after evacuation.
Circle-1 (61) Circle-2 (28) Total (89)n (%) n (%) n (%)
Fever/high body temperature 38 (62,3) 22 (78,6) 60 (67,4)
Diarrhea 20 (32,8) 9 (32,1) 29 (32,6)
Dermatitis/eczema. 9 (14,8) 6 (21,4) 15 (16,9)Acute respiratory tract infection (ARI) 30 (49,2) 20 (71,4) 50 (56,2)
Table.1. Prevalence rate per year of acute illnesses among under-five children in Kediri

Variables n Mean (SD) Range
Frequency of fever (times) 60 5(5) 1-17
Frequency of diarrhea (times) 29 3,4*(4,3) 1-17
Frequency of dermatitis (times) 15 3,4**(4) 1-17
Frequency of ARI (times) 50 6,7(6,2) 1-17
Table.2. Number of Suffering Diseases within Under-Five Children (0-59 months) in Kediri
*data is not normally distributed, median=2**data is not normally distributed, median=2

Potential risk factors ARI Fever
Yes No PR(95%CI) Yes No PR (95%CI)n (%) n (%) n (%) n (%)
1 Length of evacuation> 7 days 16 (62) 10 (38) 1.7 (0.8– 3.4) 18 (69) 8 (31) 1.2 (0.4 – 3.5)
0-7 days 3 (37) 5 (63) 1.0 5 (62) 3 (38) 1.02 Household members
evacuatedYes 9 (60) 6 (40) 1.1 (0.6 – 2.2) 12 (80) 3 (20) 1.8 (0.6 – 5.1)
No 41(55) 33 (45) 1.0 48 (65) 26 (35) 1.0
3 Exposed to ash rain/ gasYes 15 (58) 11 (42) 1.1 (0.6 – 1.8) 18 (69) 8 (31) 1.1 (0.6 – 2.1)
No 35 (56) 28 (44) 1.0 42 (67) 21 (33) 1.0
Table.3. factors associated with the occurrence of ARI and fever 1 year after evacuation

Figure.2. Prevalence rates/year of underweight and proportions of lack of breastfeeding and incomplete immunization among under-five children

Prevalence rates of all acute illnesses were much higher than official prevalence estimates in Kediri/East Java (by the National Report of BHR and Indonesian DHS, 2007, before evacuation
Proportions of children with underweight, incomplete immunization & lack of breastfeeding were all higher than official proportion estimates in Kediri (National Report of BHRand the Indonesian DHS in 2007, before evacuation).
Were both prevalent & proportion increases after evacuation and eruption due to direct exposure to volcanic ash/gas or indirectly due to displacement condition?
Proportion of whole subjects (adult & children) exposed to gas/fumes and ash rain were 27% and 15% of respectively.
After controlling the possible confounding of variables “household member evacuation” and “ash rain/gas exposure” through Cox regression model, the length of evacuation was still associated with ARI (adjusted PR =1.6; 95% CI: 0.5--5.4)
Assuming adjPR=1.6 is a valid estimate of (cumulative) risk ratio, we may predict that being evacuated for > 7days would give 60% increase of risk for under-five children to suffer from ARI, as compared to being evacuated not longer than a week.

After controlling possible confounding of variables “length of evacuation” and “ash rain/gas exposure” through Cox regressionmodel, the household member evacuation was still (weakly) associated with fever (adjusted PR=1.4; 95% CI: 0.6 – 3.2)
Assuming that this adjusted PR of 1.4 is a valid estimate of risk ratio, we may predict that being evacuated would give 40% increase of risk for under-five children to suffer from fever, as compared to not being evacuated.
Seems that it was not the ash and/or gas exposure increasing the risk to suffer from ARI or fever, but, rather the evacuation factors (i.e. experience of being evacuated and the length of evacuation > 7 days), increased the risk to get ARI or fever among under-five children.

"Flu, cough, sore throat or ARI were common, it was probably because too many people has increased the requirement for O2, while more CO2 was produced in the room because there was people suffered from diarrhea and rash skin" (FGD of NGOs activist)
The waiting line was quite long during food distribution (ofmainly noodles & bread), as was said:" We didn’t calculate, maybearound 30 (minutes), it was registered in the book. The longest linefound during bread distribution "(FGD of Polindes)
It was said about shellter’s facility:" it was not a comfortable place, there was only a thin mat for sleeping pad that less convenient to use ..". (FGD of mothers)

Fact: previously predicted big explosion (considerationto enforce massive evacuation) did not really happen. Experts found out that eruption intensity was slow, namely “effusive” type of eruption, which may not give serious direct impact for the health of the people.
On the other hand, the massive evacuation enforced by the authorities to move more than 116,000 people to farther villages might have created particular health problems, due to inadequate evacuation management.
Our findings have shown increasing occurrence of health problems among under-five children population living in vulnerable areas surrounding Mount Kelud, after evacuation.
Compared to exposure to volcanic materials, like ash rain and gases, after Kelud effusive eruption, the evacuation factors might have played more important role in increasing the risk of child health problems.

Potential increase of predominant/important health problems among under five children in vulnerable areas surrounding Kelud should always be anticipated and prioritized through strong health promotion and prevention program.Important to carefully plan and safeguard the proper and adequate mass evacuation management, since an improper and inadequate massive evacuation, management in itself, may also, generate, increase risk or complicate the potential health problems among most vulnerable population like under-five children.

This collaborative study (between UI, CRED-UCL and ULB) was supported by Kediri Health District Office and funded by the Government of Belgium and European Community



















