Molecular Biology of kidney cancers Dr. Roshani Gala DNB resident Rajiv Gandhi Cancer Institute and...
44
Molecular Biology of kidney cancers Dr. Roshani Gala DNB resident Rajiv Gandhi Cancer Institute and research centre, New Delhi
-
Upload
maria-willis -
Category
Documents
-
view
215 -
download
0
Transcript of Molecular Biology of kidney cancers Dr. Roshani Gala DNB resident Rajiv Gandhi Cancer Institute and...

Molecular Biology of kidney cancers
Dr. Roshani Gala
DNB resident
Rajiv Gandhi Cancer Institute and research centre, New Delhi

Why is molecular biology important?• Helps understand the cancer initiation, growth and
progress of disease• This understanding promotes development of
specific pathway targeted drugs• Hereditary/familial cancers can be picked up and
genetic counselling can be done to prevent cancer in family
• Future trials may require homogenous molecular groups of patients

WHO classification
• Renal cell tumours• Clear cell renal cell carcinoma • Multilocular clear cell renal cell carcinoma • Papillary renal cell carcinoma • Chromophobe renal cell carcinoma • Carcinoma of the collecting ducts of Bellini • Renal medullary carcinoma • Xp11 translocation carcinomas• Carcinoma associated with neuroblastoma• Mucinous tubular and spindle cell carcinoma• Renal cell carcinoma, unclassified • Papillary adenoma • Oncocytoma

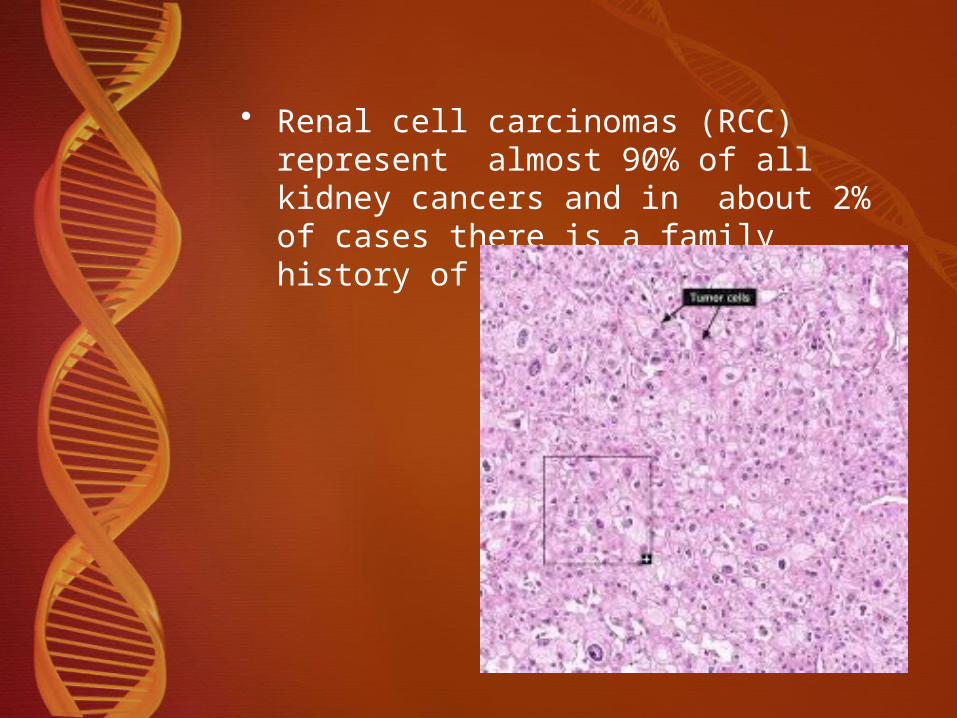
• Renal cell carcinomas (RCC) represent almost 90% of all kidney cancers and in about 2% of cases there is a family history of RCC

Clear cell renal carcinoma
• most common form of kidney cancer• Germ line VHL mutations are linked to an increased risk• VHL is a tumor suppressor gene, located at
chromosome 3p25• VHL gene is involved in both hereditary and sporadic
RCC.

Inherited defective allele of VHL
de novo VHL mutation
Somatic inactivation or loss of remaining VHL
gene
RCC

• -14q, +5q,• mutations tumor supressor genes such as CDK2A,
TP53, NF2 • or chromatin modifying genes such as PRBM1,
KDM6A, SETD2.

How does VHL work ?



Therapeutic perspective
• Most agents approved to treat clear cell renal cancer target downstream targets of HIF activity like VEGF (bevacizumab)
• Or inhibit mTor C1 which provides transitional control of HIF1-alpha. (mammalian target of Rapamycin like drugs)
• However these agents target only target only a small proportion of downstream genes regulated by HIFs
• An approach to target HIFs themselves will provide more effective therapy.

Bevacizumab• an anti-VEGF antibody• In a randSorafenibomized trial, patients treated with high
dose bevacizumab had a significantly increased progression free survival compared with those treated with placebo
Sorafenib• small molecule inhibitor which targets the tyrosine
kinase domain of a number of cell surface receptors, including VEGFR and PDGFR,
• as well as the intracellular signaling enzyme, raf kinase• used as a second line agent in patients who progress
while on sunitinib

Sunitinib
• another small molecule receptor tyrosine kinase inhibitor
• has activity against the vascular endothelial growth factor receptor (VEGFR), the platelet derived growth factor receptor (PDGFR) and the KIT receptor.
• In patients with metastatic clear cell kidney cancer sunitinib has been found to have a response rate of 31%, with a progression free survival of 11 months

Type I Papillary Renal cancer
• Papillae covered by small cells with scanty cytoplasm arranged in single layer on papillary basement membrane

Hereditary papillary renal carcinoma (HRPC)
• Autosomal dominant• Multifocal papillary RCC• Almost all cases are associated with
mutations in MET proto-oncogenes
Sporadic Type 1 PRCC• Only small subset are associated with
MET mutations• Mutation of KIT proto-oncogene is
described in 68%. Pathogenesis needs to be confirmed

The MET proto-oncogene encodes a receptor tyrosine kinase that is physiologically activated by hepatocyte growth factor (HGF)
Binding of HGF to the extracellular portion of the MET receptor
autophosphorylation of critical tyrosines in the intracellular tyrosine kinase domain,
activating a downstream signaling cascade
cell proliferation, cell motility, branching morphogenesis and epithelial-mesenchymal transition

Cross links with other energy, iron & oxygen sensing pathways

Therapeutic perspective
• Foretinib
• oral dual kinase small molecule agent • targets the tyrosine kinase domains of MET as well as
VEGFR2,• in patients with sporadic as well as hereditary papillary
kidney cancer
• Phase II clinical trial is currently underway evaluating the role
• .

Type 2 papillary kidney cancer
Higher nuclear grade, eosinophic cytoplasm, pseudo-stratified nuclei on papillary cores

• Associated with Hereditary Leiomyomatosis Renal Cell Carcinoma (HLRCC)
• affected individuals are at risk for the development of uterine and cutaneous leiomyomas and kidney cancer
RCC UterineLeiomyoma
CutaneousLeiomyoma

• Krebs cycle enzyme, fumarate hydratase (FH) , is the gene for HLRCC. Mutations of the fumarate hydratase gene are found in over 90% of HLRCC families.
Inactivation of FH
Increased levels of Fumarate and succinate , Hypoxic environment
HIF stabilization
Upreguration of VEGF, GLUT1
1.

2.
FH deficiency
Glycolytic environment
Reactive oxygen species
HIF stabilization

Familial pheochromocytoma/paraganglioma complex
• Renal carcinoma, • pheochromocytoma/paraganglioma• SDHB germline mutations • Succinate dehydrogenase another Krebs cycle enzyme• Act by accumulation of succinate leading to HIF
stabilization


Therapeutic perspectives
• Both enhanced tumor angiogenesis and glucose transport could be the best targets for the treatment of either FH-deficient or SDH-deficient renal tumors
• Targeting the vasculature has given better results than in VHL-deficient tumours.

Chromophobe renal cell carcinomas-oncocytomas• Birt-Hogg-Dubè syndrome• rare autosomal dominant disorder • characterized by hair-follicle hamartomas
(fibrofolliculomas) of the face and neck

• spontaneous pneumotorax, lung cysts and RCCs, particularly chromophobe RCC (33%), hybrid oncocytic renal cell carcinoma (50%), clear-cell RCC (9%) and oncocytomas (5%)

Genetics of BHD syndrome
• The FLCN gene is impaired in Birt-Hogg-Dubè syndrome,
• encodes a protein called folliculin• folliculin (FLCN), forms a complex with two FLCN
interacting proteins, FNIP1 and FNIP2, which bind AMPK, a key molecule for energy sensing that negatively regulates mTOR activity

FLCN deficiency allows activation of proto-oncogenes

Therapeutic perspective
• a mouse model was prepared
• BHD gene was selectively knocked out in the kidneys• Affected mice developed enlarged, polycystic kidneys
and died from renal failure by 3 weeks of age
• Rapamycin treated mice had significantly smaller kidneys than control animals and their life-expectancy was nearly doubled

Tuberous Sclerosis Complex
• autosomal dominant genodermatosis• characterized by multiple hamartomatous lesions that
affect the skin, retina, brain, lungs and kidneys• Eighty percent of children with TSC have renal lesions
including benign angiomyolipomas (70%), cysts (20%), and oncocytoma (<1%)

Renal angiomyolipomas
• often multiple and bilateral• rarely transform to a malignant tumor (<1%)• cumulative renal cancer incidence is 2.2%–4.4%• the average age at diagnosis is 28 years

Associated Lesions/Tumors in AML
epithelial lesions, such as
• cysts, • oncocytomas• clear cell, papillary, or chromophobe carcinomas • mesenchymal lesions (angiomyolipomas),
suggesting that TSC genes regulate early differentiation and proliferation of renal precursor cells

Genetics of AML
• mutation of either the TSC1 or TSC2 gene
• TSC1-TSC2 complex interacts with a number of cellular pathways, including modulation of mTOR.
Therapeutic perspective• Role of sirolimus, an agent which targets the mTOR
pathway has been evaluated in a trial• In this trial, the renal angiomyolipomas regressed during
sirolimus therapy,• however, they tended to increase in size after the
treatment was stopped

Renal Carcinomas with Xp11.2 translocation
• Several different translocations involving chromosome Xp11.2.
• All resulting in gene fusions involving TFE3 gene.
• These include the t(X;1)(p11.2;q21) which results in fusion of the PRCC and TFE3 genes,
• the t(X;17)(p11.2;q25) which results in fusion of the ASPL and TFE3 genes

Histopathology
• papillary architecture comprised of clear cells
ASPL-TFE3 renal carcinomas are characterized by • cells with voluminous clear to eosinophilic cytoplasm, • discrete cell borders,• vesicular chromatin and prominent nucleoli. • Psammoma bodies are constant and sometimes
extensive, often arising within characteristic hyaline nodules

Morphology of translocation RCC
• The PRCC-TFE3 renal carcinomas• less abundant cytoplasm, fewer psammoma bodies, • fewer hyaline nodules, • more nested, compact architecture
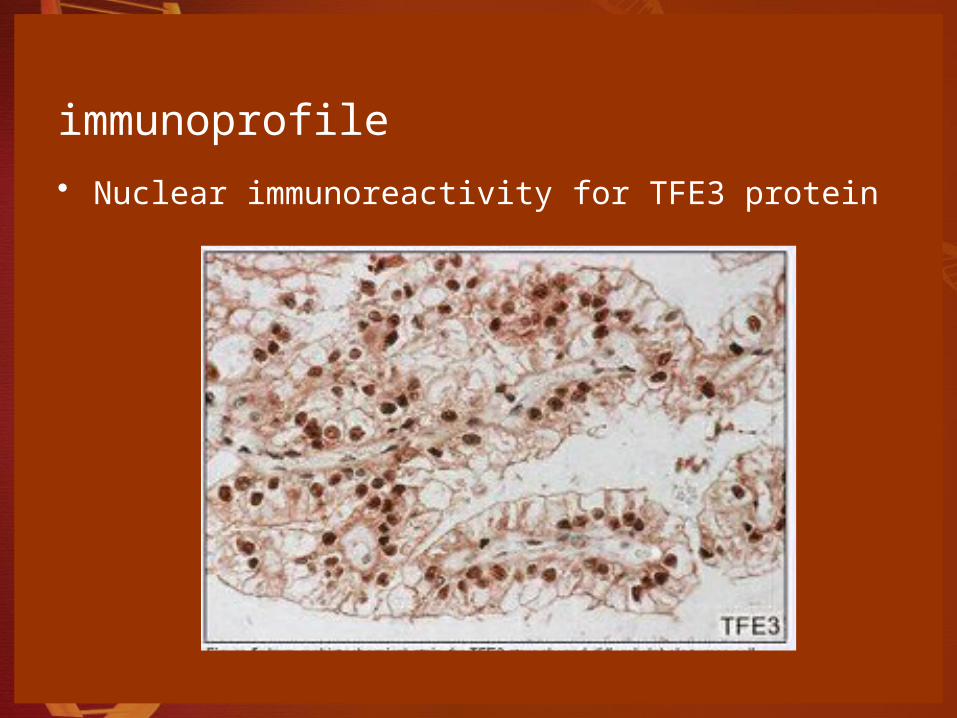
immunoprofile
• Nuclear immunoreactivity for TFE3 protein

Therapeutic perspective
• some tumors with PRCC-TFE3 fusion have been shown to lack a normal mitotic checkpoint control,
• which may turn them more sensitive to chemotherapeutic agents that target microtubules, such as vincristine and paclitaxel.

Table summarizing the genetic pathways

Summary Points
• 1. Clear cell kidney cancer and kidney cancer associated with von Hippel-Lindau are caused by mutation of the VHL gene, which results in a disorder of oxygen sensing.
• 2. Hereditary papillary renal cell carcinoma and a subset of sporadic type 1 papillary kidney cancers are caused by mutation of the MET gene.
• 3. The hereditary form of chromophobe kidney cancer associated with Birt-Hogg-Dubé is caused by mutation of the BHD gene, which is involved with the AMPK/mTOR pathway.

• 4. The hereditary form of kidney cancer associated with Hereditary Leiomyomatosis Renal Cell Carcinoma is caused by mutation of the gene for theKrebs cycle enzyme, fumarate hydratase.
• 5. The hereditary form of kidney cancer associated with familial pheochromocytoma/paraganglioma results from mutations of the gene for the Krebs cycle enzyme, succinate dehydrogenase B.
• 6. The hereditary form of angiomyolipoma results from mutations of the TSC1 and TSC2 genes, which are involved in the AMPK/mTOR pathway.
• 7. Understanding the pathways of the kidney cancer genes has provided the foundation for the development of targeted therapeutic approaches to the treatment of these diseases

References:
• 1. Molecular Diagnosis and Therapy of Kidney Cancer; W. Marston Linehan, M.D., Gennady Bratslavsky, Peter A. Pinto, Laura S. Schmidt, Len
Neckers, Donald Bottaro, and Ramaprasad Srinivasan; Annu Rev Med. 2010 ; 61: 329–343
• 2. Molecular Pathogenesis of Renal Cell Carcinoma: A Review ; Israel Gomy and Wilson Araújo Silva Jr.; Emerging Research and Treatments in Renal Cell Carcinoma.