Modified Early Warning Score Effect in the ICU Patient ...
30
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Modified Early Warning Score Effect in the ICU Patient Population Anne Rabert RN, DHA, CCRN, NE-BC Lehigh Valley Health Network, [email protected] Follow this and additional works at: hp://scholarlyworks.lvhn.org/patient-care-services-nursing Part of the Nursing Commons is Presentation is brought to you for free and open access by LVHN Scholarly Works. It has been accepted for inclusion in LVHN Scholarly Works by an authorized administrator. For more information, please contact [email protected]. Published In/Presented At Rabert, A. (2013, October 29) Modified Early Warning Score Effect in the ICU Patient Population. Presented at Research Day 2015, Lehigh Valley Health Network, Allentown, PA.
Transcript of Modified Early Warning Score Effect in the ICU Patient ...

Lehigh Valley Health NetworkLVHN Scholarly Works
Patient Care Services / Nursing
Modified Early Warning Score Effect in the ICUPatient PopulationAnne Rabert RN, DHA, CCRN, NE-BCLehigh Valley Health Network, [email protected]
Follow this and additional works at: http://scholarlyworks.lvhn.org/patient-care-services-nursing
Part of the Nursing Commons
This Presentation is brought to you for free and open access by LVHN Scholarly Works. It has been accepted for inclusion in LVHN Scholarly Works byan authorized administrator. For more information, please contact [email protected].
Published In/Presented AtRabert, A. (2013, October 29) Modified Early Warning Score Effect in the ICU Patient Population. Presented at Research Day 2015,Lehigh Valley Health Network, Allentown, PA.

Modified Early Warning
Score Effect in the ICU
Patient Population
Anne Rabert, RN, DHA, CCRN, NE-BC
LVHN

Rapid Response Teams (RRT)
Team of credentialed health care providers
who can treat patients wherever they are
located
Emergence occurred in the late 1990s based on
the successful outcomes reported in Australia
and the United Kingdom
Composition and function of the team aligns
with the organizational capabilities

RRT at LVHN
Teams operational at the two largest acute care
campuses
Team composed of a critical care RN,
respiratory therapist, and hospitalist
Program began in 2007
Average 55-60 calls per month at the larger
campus and 20-25 calls at the smaller campus

RRT Program Goal
Primary goal of the RRT program is to reduce
the number of cardiac arrest outside of the ICU
Program at LVHN has not met this goal
Why and how could it?

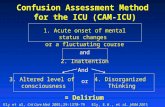
Modified Early Warning Score
(MEWS)
Scoring system rating physiologic parameters at
designated intervals
Adjunctive strategy to RRT programs
Proactive approach to care rather than reactive
approach of RRT
Study its effect since no prior use in the organization

MEWS Tool Score 3 2 1 0 1 2 3
Heart Rate per
Minute Less than 40 40-50 51-100 101-110 111-129 Greater
tha
n
13
0
Systolic Blood
Pressure Less than 70 71-80 81-100 101-159 160-199 200-220 More
tha
n
22
0
Respiratory Rate per
Minute Less than 8 9-17 18-20 21-29 Greater
tha
n
30
Level of
Consciousness Unresponsive Responds to
pain Responds to
voice Alert Agitation or
confusion New onset
agitation
or
confusion
Temperature Less than
95.0° 95.1-96.8° 96.9-
100.
4°
100.5-101.3° Greater than
101.4°

MEWS Score Score 3 2 1 0 1 2 3
Heart Rate per Minute Less than 40 40-50 51-100 101-110 111-129 Greater
tha
n
130
Systolic Blood
Pressure Less than 70 71-80 81-100 101-159 160-199 200-220 More
tha
n
220
Respiratory Rate per
Minute Less than 8 9-17 18-20 21-29 Greater
tha
n
30
Level of
Consciousness Unresponsive Responds to
pain Responds to
voice Alert Agitation or
confusion New onset
agitation
or
confusion
Temperature Less than
95.0° 95.1-96.8° 96.9-
100.4
°
100.5-101.3° Greater than
101.4°

MEWS Score Score 3 2 1 0 1 2 3
Heart Rate per Minute Less than 40 40-50 51-100 101-110 111-129 Greater
tha
n
130
Systolic Blood
Pressure Less than 70 71-80 81-100 101-159 160-199 200-220 More
tha
n
220
Respiratory Rate per
Minute Less than 8 9-17 18-20 21-29 Greater
tha
n
30
Level of
Consciousness Unresponsive Responds to
pain Responds to
voice Alert Agitation or
confusion New onset
agitation
or
confusion
Temperature Less than
95.0° 95.1-96.8° 96.9-
100.4
°
100.5-101.3° Greater than
101.4°

MEWS Score Score 3 2 1 0 1 2 3
Heart Rate per Minute Less than 40 40-50 51-100 101-110 111-129 Greater
tha
n
130
Systolic Blood
Pressure Less than 70 71-80 81-100 101-159 160-199 200-220 More
tha
n
220
Respiratory Rate per
Minute Less than 8 9-17 18-20 21-29 Greater
tha
n
30
Level of
Consciousness Unresponsive Responds to
pain Responds to
voice Alert Agitation or
confusion New onset
agitation
or
confusion
Temperature Less than
95.0° 95.1-96.8° 96.9-
100.4
°
100.5-101.3° Greater than
101.4°

MEWS Score Score 3 2 1 0 1 2 3
Heart Rate per Minute Less than 40 40-50 51-100 101-110 111-129 Greater
tha
n
130
Systolic Blood
Pressure Less than 70 71-80 81-100 101-159 160-199 200-220 More
tha
n
220
Respiratory Rate per
Minute Less than 8 9-17 18-20 21-29 Greater
tha
n
30
Level of
Consciousness Unresponsive Responds to
pain Responds to
voice Alert Agitation or
confusion New onset
agitation
or
confusion
Temperature Less than
95.0° 95.1-96.8° 96.9-
100.4
°
100.5-101.3° Greater than
101.4°

MEWS Score Score 3 2 1 0 1 2 3
Heart Rate per Minute Less than 40 40-50 51-100 101-110 111-129 Greater
tha
n
130
Systolic Blood
Pressure Less than 70 71-80 81-100 101-159 160-199 200-220 More
tha
n
220
Respiratory Rate per
Minute Less than 8 9-17 18-20 21-29 Greater
tha
n
30
Level of
Consciousness Unresponsive Responds to
pain Responds to
voice Alert Agitation or
confusion New onset
agitation
or
confusion
Temperature Less than
95.0° 95.1-96.8° 96.9-
100.4
°
100.5-101.3° Greater than
101.4°

Research Study Design
Quantitative Study—Retrospective medical
record review
Case-Control Design
Cases—possess the disease or event to be studied
Controls—do not
Hypothesis tested at the 0.05 level of
significance

Research Questions
Research Question 1:
What differences exist
between case and
control group subjects
exhibiting a MEWS
score of 5 or greater at
least once in the first 24
hours of an ICU stay?
Research Question 2:
What deleterious changes
in respiratory rate occur
within eight hours prior
to a cardiac arrest
event?

Target Population
Inclusion Criteria
Patients over 18 years of age
Patients admitted to the MICU/SICU between June 1, 2011 and December 31, 2012
Cardiac arrest event (case group only)
Exclusion Criteria
Patients under the age of 18
Patients transferred to the MICU/SICU from another level one ICU on the campus
Patients admitted to the MICU/SICU with comfort care orders

Target Population Formulation
Target population included 2,792 patients
4 patients excluded because they were under 18
Case group = 45 patients experiencing a cardiac
arrest event
Control group = purposive convenience sampling
of the remaining 2,743 patients resulted in
identification of 45 subjects matched by age and
gender to those in the case group.

Data Collection
Data collection required verbatim data extraction
from 2 electronic health record systems used at the
study organization
MEWS score generation occurred after the
completion of all data collection
Small pilot sample of 10 subjects in case and control
groups occurred to verify accuracy of MEWS score
values
Continued data collection occurred with remaining group
members

Sample Demographics
Cases Controls
Length of Stay 5.6 days 3.26 days
Admission Source Emergency
Department
Emergency
Department
Admitting Service Medical ICU Medical ICU
Admitting Reason Respiratory Failure Post—operative
monitoring

RQ 1 Statistical Analysis
Conduction of McNemar’s test using bivariate
statistics
Assessed for presence of significant difference in
patients with at least one MEWS score of 5 or
greater between the case and control groups
Hypothesis testing required sample subject
categorization into two dichotomous groups of all
MEWS scores less than 5 or at least one score of 5
or greater

RQ 1 Statistical Analysis MEWS Score > 5 at least once
Group 1 = “Yes” Group 2 = “No”
Sample 49 41
Case Group 30 15
Highest Score
11 4
Average Number of times
score > 5
3 Not Applicable
Control Group 19 26
Highest Score
10 4
Average Number of times
score > 5
2 Not Applicable

RQ 1 Statistical Analysis
McNemar’s Test Results
30 cases had at least 1 MEWS score of > 5 in
the first 24 hours of an ICU stay
13 had matching controls with at least 1 score
17 had unmatched controls
15 cases did not have any MEWS score of >5
9 had matched controls without any score > 5
6 had unmatched controls

RQ 1 Conclusions
Statistically significant results (0.035) at the 0.05
level in a unique patient population
Null hypothesis rejection; support of the alternative
hypothesis indicating a difference existed between
cases an controls with at least 1 MEWS score of > 5
Research Implications include:
Create standard communication used with cognitive
continuum theory
MEWS score of 5 or greater at least one time in the first 24
hours of an ICU stay is a cardiac arrest event predictor

RQ 2 Statistical Analysis
Use of Wilcoxon signed-rank test to determine
difference between respiratory scores
Score 1 = immediately before cardiac arrest
Score 2 = four hours before cardiac arrest
Score 3 = eight hours before cardiac arrest
Each case subject required three Wilcoxon
signed rank tests
Score 2:1; Score 3:1; and Score 3:2

RQ 2 Statistical Analysis
MEWS Respiratory Scores—Case Group Only (n=45)
Score 1
(Immediately before
Cardiac Arrest)
Score 2 (4 hours
before Cardiac
Arrest)
Score 3 (8 hours
before Cardiac
Arrest)
Number of Cases
with Score 45 42 38
Score Range 0-3 0-3 0-3
Mean Score 1.38 1.60 1.13
Standard Deviation 1.248 1.127 0.991
Median Score 1.0 2.0 1.0
Mode Score 0 2 0

RQ 2 Statistical Analysis
Wilcoxon Signed-Rank Test Statistics
Score 2:Score 1 Score 3:Score 1 Score 3:Score 2
Z score -0.880 -1.314 -2.456
Significance 0.379 0.189 0.014

RQ 2 Conclusions
Null hypothesis rejection; support of the
alternative hypothesis
Contributed to the current literature in a
unique patient population
Research implications include:
Narrowing of eight hour pre-cardiac arrest
window for changes to those occurring
between four and eight hours prior to an event

Study Limitations
Single center study
Case-control design
MEWS tool
Selection and value selection
Sensitivity and specificity

Recommendations
Future Use
MEWS tool use across all inpatient units in the study organization Total Score
Respiratory parameter score
Electronic calculation
Treatment algorithms based on score values
Future Study
Non-ICU patients in the study organization
Varied MEWS score values for future study
Tool modification
Incorporation into new electronic medical record system
Adjunct treatment modality with current RRT practices

Summary
Study revealed significant outcomes of MEWS score benefit as a cardiac arrest predictor in a unique population.
Also revealed significant changes in respiratory status occurred between four and eight hours prior to a cardiac arrest event
Nursing research driving nursing practice changes

Questions