Decompressive Abdominal Laparotomy for Abdominal Compartment ...

8/17/15
1
Missed Abdominal cases Sheila Sheth, MD, FACR, FSRU
Selected missed or difficult cases
Findings missed Interpreta:on incorrect
Teaching points
Case 1: A 59 year old woman with history of Primary Sclerosing
Cholangi=s
Case 1 § Gallbladder fundal mass being followed on MR and CT, mass had more solid appearance since prior
§ US requested § Addi:onal history of right breast cancer and radia:on
Interpreta:on, Outcome, Final Diagnosis
§ “Gallbladder mass with vascularity concerning for gallbladder carcinoma”
§ Pa:ent underwent open cholecystectomy § Path: Acute and chronic cholecys11s with intramural organizing abscess
Differen:al Diagnosis of Polypoid Gallbladder Mass
§ Tumefac:ve sludge (mobile) § Focal adenomyomatosis (fundus) § Cholesterol Polyps (small, mul:ple, not associated with stones
§ Inflammatory polyps § Abscess / focal perfora:on § Xanthogranulomatous cholecys::s § Gallbladder carcinoma § Metastasis to gallbladder
GB mass: size maWers § Benign lesions
§ More common (74%) § Cholesterol polyps § Small size <10mm and mul:ple § Younger pa:ents
§ Malignant lesions § Size >10mm § Age >60 y § Associated with gallstones

8/17/15
2
GB cancer: imaging § Focal mass arising from GB § Mass replacing the GB § Focal or diffuse thickening of GB wall § Invasion into adjacent liver § Periportal adenopathy causing BD obstruc:on
§ Carcinomatosis
Gallbladder metastases § Seen in pa:ents with widespread metastases
§ Melanoma most common primary cancer (>50%)
§ Other primary cancers: § Breast, RCC, lung § Invasion from HCC, cholangioca
§ Lymphoma very rare
Xanthogranulomatous cholecys::s
§ Rare form of chronic cholecys::s § Destruc:ve inflammatory process
§ Extension to adjacent structures § Occlusion of RA sinuses with extravasa:on of inspissated bile
§ Lipid laden macrophages within GB wall § Poten:ally difficult surgery
§ Conversion to open cholecystectomy § Adhesions, risk of fistuliza:on
Technical and Teaching points § Image in mul:ple posi:ons and wait to let tumefac:ve sludge move
§ Color and Power Doppler to detect flow and twinkling ar:fact
§ Use high frequency linear transducer when fundus is close to the anterior abdominal wall
§ Size and number maWers (5mm or less, mul:ple)
Case 2: A 52 year old man with back pain and history of substance
use
Case 2

8/17/15
3
Findings, Interpreta:on
§ “Hypoechoic enlarged pancreas sugges:ve of pancrea::s, correlate with Lipase”
§ What mislead us: Age of the pa:ent, substance use, at risk for pancrea::s
§ Lipase: 52 § CT requested by ED (Rou:ne)
Case 2:
CT shows infiltra:ng unresectable pancrea:c mass: adenocarcinoma
Adenocarcinoma pancreas 54 yo Pancrea:c cancer § Adenocarcinoma, neuroendocrine tumor § US can be the 1st exam requested if suspected biliary obstruc:on (head of pancreas mass)
§ Hypoechoic mass, ductal dilata:on § NO calcifica:ons § Diffuse form of pancrea:c cancer can mimic pancrea::s on US
§ Recommend CT especially in older pa:ents if pancrea:c abnormality seen on US
§ Differen:al diagnosis: § Pancreas metastases (widespread cancer) § Peripancrea:c adenopathy
Case 3: 26 year old in 3d trimester of pregnancy with LUQ mass
Case 3:
8/17/15
4
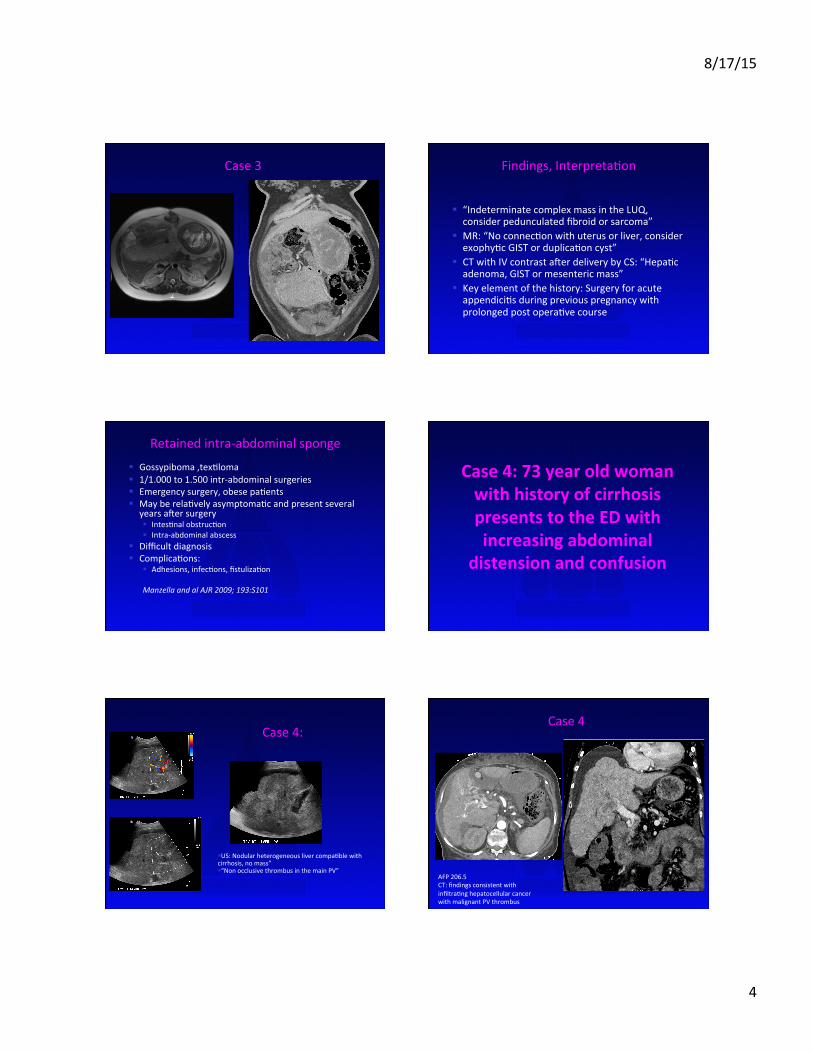
Case 3 Findings, Interpreta:on
§ “Indeterminate complex mass in the LUQ, consider pedunculated fibroid or sarcoma”
§ MR: “No connec:on with uterus or liver, consider exophy:c GIST or duplica:on cyst”
§ CT with IV contrast aler delivery by CS: “Hepa:c adenoma, GIST or mesenteric mass”
§ Key element of the history: Surgery for acute appendici:s during previous pregnancy with prolonged post opera:ve course
Retained intra-‐abdominal sponge § Gossypiboma ,tex:loma § 1/1.000 to 1.500 intr-‐abdominal surgeries § Emergency surgery, obese pa:ents § May be rela:vely asymptoma:c and present several
years aler surgery § Intes:nal obstruc:on § Intra-‐abdominal abscess
§ Difficult diagnosis § Complica:ons:
§ Adhesions, infec:ons, fistuliza:on Manzella and al AJR 2009; 193:S101
Case 4: 73 year old woman with history of cirrhosis presents to the ED with increasing abdominal
distension and confusion
Case 4:
§ US: Nodular heterogeneous liver compa:ble with cirrhosis, no mass” § “Non occlusive thrombus in the main PV”
Case 4
AFP 206.5 CT: findings consistent with infiltra:ng hepatocellular cancer with malignant PV thrombus
8/17/15
5
Portal vein thrombosis
• Cirrhosis • Portal hypertension • Venous stasis
• Hypercoagulable states • Pyelephlebi:s • Malignant thrombosis
• Tumor thrombus: HCC • Encasement occlusion: pancrea:c ca
• Pediatric age group • Umbilical cord infec:on • Dehydra:on
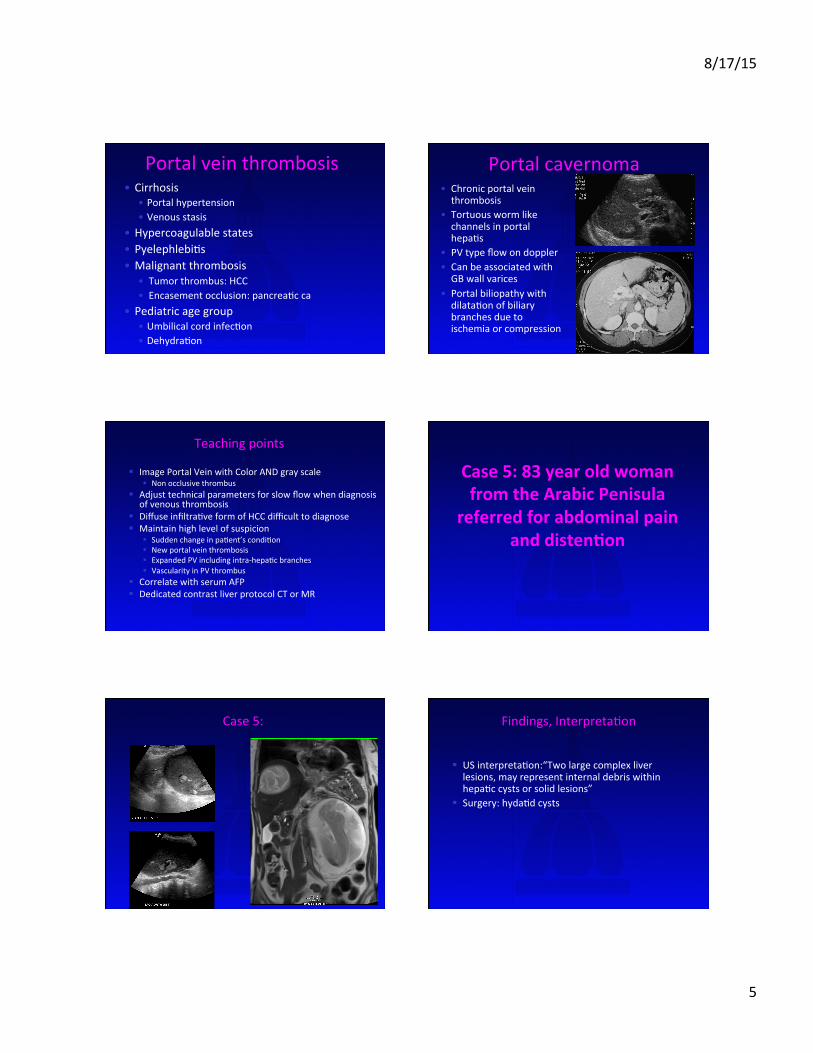
Portal cavernoma • Chronic portal vein thrombosis
• Tortuous worm like channels in portal hepa:s
• PV type flow on doppler • Can be associated with GB wall varices
• Portal biliopathy with dilata:on of biliary branches due to ischemia or compression
Teaching points § Image Portal Vein with Color AND gray scale
§ Non occlusive thrombus § Adjust technical parameters for slow flow when diagnosis
of venous thrombosis § Diffuse infiltra:ve form of HCC difficult to diagnose § Maintain high level of suspicion
§ Sudden change in pa:ent’s condi:on § New portal vein thrombosis § Expanded PV including intra-‐hepa:c branches § Vascularity in PV thrombus
§ Correlate with serum AFP § Dedicated contrast liver protocol CT or MR
Case 5: 83 year old woman from the Arabic Penisula
referred for abdominal pain and disten=on
Case 5: Findings, Interpreta:on
§ US interpreta:on:“Two large complex liver lesions, may represent internal debris within hepa:c cysts or solid lesions”
§ Surgery: hyda:d cysts

8/17/15
6
Differen:al diagnosis hepa:c cys:c mass § Complex cyst (bleeding) § Infec:on
§ Pyogenic abscess § Hyda:d cyst § Amebic abscess
§ Cys:c metastases (squamous cell ca, GIST tumors) § Biliary cystadenoma/carcinoma § Mass with extensive bleeding (adenoma)
Hyda:d disease § Infesta:on by Echinoccocus Granulosus (cys:c form) § Endemic regions
§ Mediterranean basin § Middle East § Australia § Some part of USA and Canada
§ Affected organs § LIVER § Lungs, kidneys,spleen, CNS, bones
Case 6: 33 year old woman underwent CT for painful
palpable abdominal wall mass
CT findings: ‘Fluid collec:on with rim enhancementand surrounding inflamma:on and indura:on of the right rectus muscle” No specific diagnosis offered Clinic note: Abdominal pain and tenderness around menses, CT not contributory
Case 6: 33 yo woman with painful palpable mass
Axial
US: hypodense fluid collec:on in the anterior abdominal wall with small tract connec:ng to the anterior uterus. On US, the C-‐sec:on scar is seen, which was an important clue to the diagnosis. Ques:oning the pa:ent revealed cyclical abdominal pain and focal tenderness And history of CSec:on MR (sagiWal T2): blood fluid level within the collec:on, which confirmed the diagnosis ( not shown)
US 2 months later
Axial

8/17/15
7
Endometriosis § Endometrial glands implanted outside the endometrial cavity undergo cyclical bleeding
§ Found in 20 to 24% to women evaluated for infer:lity or chronic pelvic pain
§ Pathology: § Superficial implants (laparoscopy) § Chocolate cysts, easiest to diagnose on US § Deep infiltra:ng endometriosis with fibrosis and adhesions § Affect GYN organs, rectosigmoid, bladder, surgical scars
Scar Endometriosis § Most common aler CSec:on § Dissemina:on of endometrial cells at surgery § Olen infiltrates deeper into Rectus Abdominus muscle
§ May not be associated with pelvic endometriosis § Preopera:ve diagnosis made in 20 to 50% of women § US: solid hypoechoic heterogeneous mass, irregular or spiculated margins
§ May have internal vascularity
Scar Endometriosis Differen:al Diagnosis § Desmoid tumor § Suture granuloma § Hematoma § Metastases (ovarian cancer, pancrea:c cancer..)
Teaching points § Elicit specific history § Should always try to offer specific diagnosis or differen:al diagnosis
§ Advantages of US § Interac:on with pa:ent § Correla:on of findings with symptoms
Case 7: 75 year old man with elevated crea=nine
US report: “Mild right hydronephrosis” Pa:ent also had history of palpable mass in the jaw and scrotal enlargement CT showed hypodense mass in the right renal pelvis Biopsy of Jaw mass: B cell lymphoma
Case 7:

8/17/15
8
Differen:al diagnosis of mass in the renal sinus
• Cys:c/fluid filled • Dilated collec:ng system • Parapelvic cysts
• Normal variant simula:ng a solid mass • Hypoechoic renal sinus fat • Hypertrophied column of Ber:n
• Solid mass • Transi:onal cell carcinoma • Lymphoma • Renal cell carcinoma
Renal lymphoma US findings
• Usually B cell Lymphoma • Mul:ple hypoechoic renal masses • Solitary mass • Direct invasion of the kidney from retroperitoneal adenopathy
• Bilateral renal infiltra:on with large heterogeneous kidneys
• Perinephric hypoechoic mass • Hypoechoic mass in the renal sinus • Lymphoma can be quite hypoechoic (densely packed cells with few interfaces) and mimic fluid
Case 8: 50 year old woman with abdominal bloa=ng
Case 8: 50 yo woman with bloa:ng
US interpreta:on: “ Echogenic mass likely from right adrenal gland, less likely liver mass, recommend CT” CT showed faWy adrenal mass consistent with adrenal myelolipoma
Adrenal myelolipoma • Benign non func:oning tumors • Incidental finding • Contain variable amount of fat and bone marrow deriva:ves
• Echogenic supra renal mass • Speed propaga:on ar:fact allows diagnosis of fat containing mass – Velocity of sound in fat slower then velocity of sound in sol :ssue
– Apparent break in diaphragm – Mass >4cm
Determining origin of large RUQ mass
Anterior displacement of echogenic retroperitoneal fat stripe in large adrenal cor:cal carcinoma
Not seen in this case of hepatocellular carcinoma