
MINERAL AND BONE DISORDERS IN CHRONIC KIDNEY DISEASE PEDRAM.AHMADPOOR SHAHID BEHESHTI MEDICAL...
44
MINERAL AND BONE MINERAL AND BONE DISORDERS IN CHRONIC DISORDERS IN CHRONIC KIDNEY DISEASE KIDNEY DISEASE PEDRAM.AHMADPOOR PEDRAM.AHMADPOOR SHAHID BEHESHTI MEDICAL SHAHID BEHESHTI MEDICAL UNIVERSITY UNIVERSITY
-
Upload
cadence-hadwin -
Category
Documents
-
view
216 -
download
0
Transcript of MINERAL AND BONE DISORDERS IN CHRONIC KIDNEY DISEASE PEDRAM.AHMADPOOR SHAHID BEHESHTI MEDICAL...

MINERAL AND BONE MINERAL AND BONE DISORDERS IN CHRONIC DISORDERS IN CHRONIC
KIDNEY DISEASEKIDNEY DISEASE
PEDRAM.AHMADPOORPEDRAM.AHMADPOOR
SHAHID BEHESHTI MEDICAL SHAHID BEHESHTI MEDICAL UNIVERSITYUNIVERSITY

Normal Bone Metabolic UnitNormal Bone Metabolic Unit
Low turn over bone disease High turn over bone disease mixed
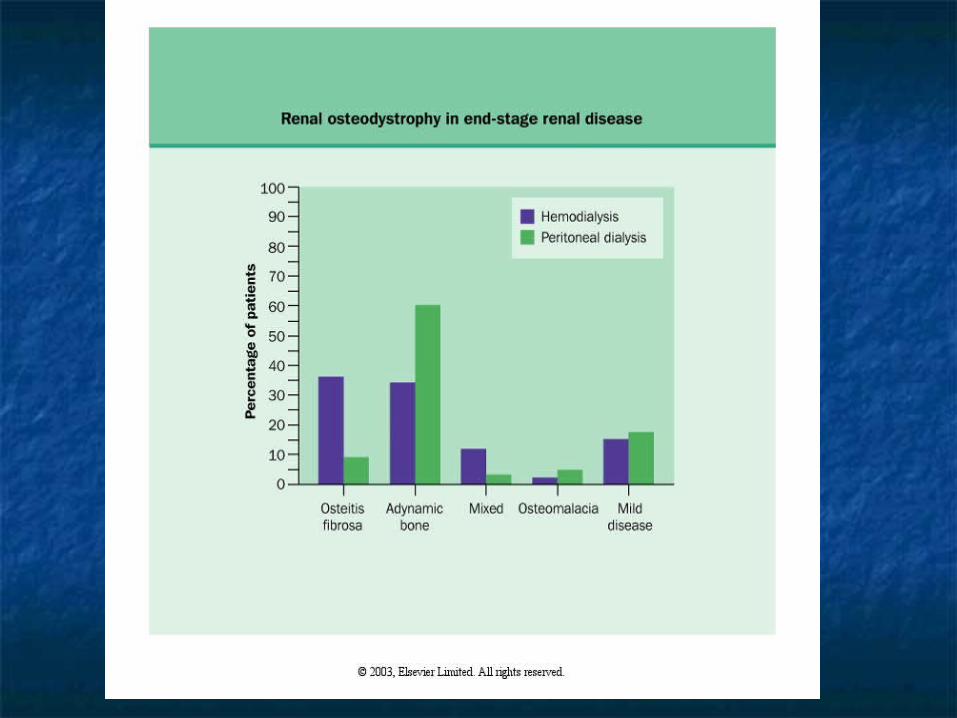
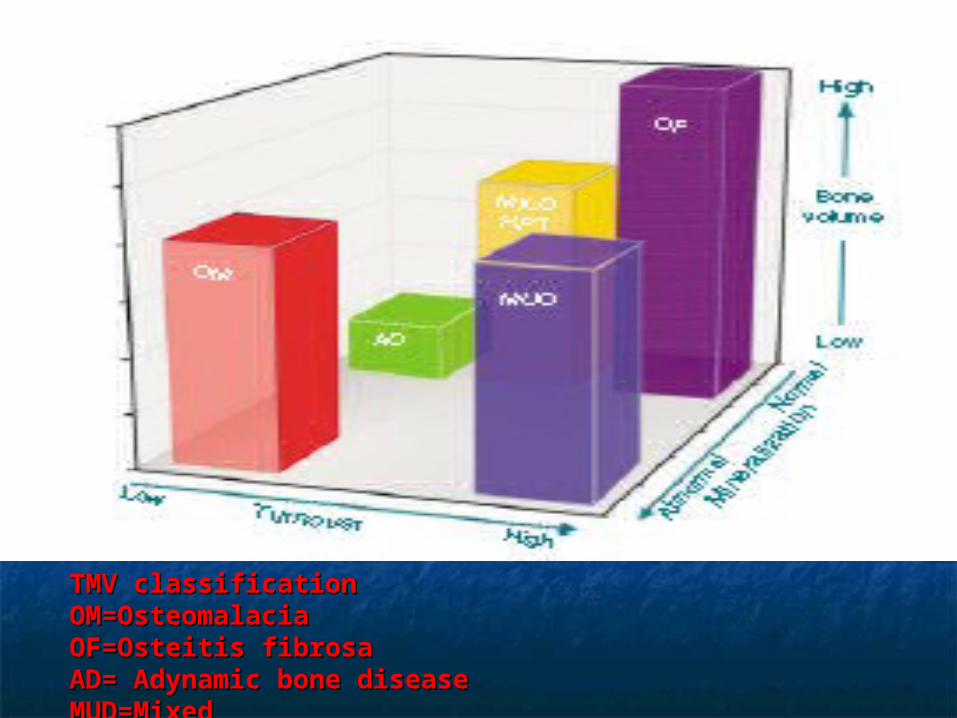
TMV classificationTMV classificationOM=OsteomalaciaOM=OsteomalaciaOF=Osteitis fibrosaOF=Osteitis fibrosaAD= Adynamic bone diseaseAD= Adynamic bone diseaseMUD=Mixed MUD=Mixed

Mechanism for 2 HPT in CRFMechanism for 2 HPT in CRF
Increased intracellular P in remaining proximal Increased intracellular P in remaining proximal tubulestubules suppression of 1-alpha OHase suppression of 1-alpha OHase
Decreased level of 1,25 D3 starts with GFR<80Decreased level of 1,25 D3 starts with GFR<80
Increased intracellular P starts earlier than Increased intracellular P starts earlier than changes in serum P changes in serum P

Consequences of 1,25( OH )D3 deficiency Consequences of 1,25( OH )D3 deficiency
Increase in PTH level Increase in PTH level Parathyroid cell proliferation ( VDR)Parathyroid cell proliferation ( VDR) Decreased bone calcemic response Decreased bone calcemic response
to PTHto PTH Increased PTH set point ,Decreased Increased PTH set point ,Decreased
CaSRCaSR HypocalcemiaHypocalcemia

PTH - Calcium set pointPTH - Calcium set point
PTH
Ionised Calcium1.25 mmol/l
Normal Uraemia50%

Causes of decreased Causes of decreased 1,25(OH)D3 synthesis in 1,25(OH)D3 synthesis in
renal failurerenal failure Phosphate retention and Phosphate retention and
HyperphosphatemiaHyperphosphatemia Renal tissue lossRenal tissue loss Uremic toxins(GSA,Uric acid)Uremic toxins(GSA,Uric acid) FGF-23FGF-23


Clinical Manifestation of Clinical Manifestation of Renal OsteodystrophyRenal Osteodystrophy
Bone painBone pain Myopathy and muscle weaknessMyopathy and muscle weakness PruritisPruritis Metastatic and extraskeletal Metastatic and extraskeletal
calcification (vascular –soft tissue)calcification (vascular –soft tissue) Arthritis and PeriarthritisArthritis and Periarthritis Spontaneous tendon ruptureSpontaneous tendon rupture


rugger jersey spine

sub-periosteal resorption

AP view looser’s zone
frogleg view looser’s zone

Vascular Calcification in Vascular Calcification in ESRDESRD
Reprinted from: London, et al. Nephrol Transpl Dial. 2003;18:1731-1740. (London, 2003 p. 1733 fig.1)


Increased Death Risk in CKD Increased Death Risk in CKD Stage 5 with Elevated Serum Stage 5 with Elevated Serum
CalciumCalcium
0.6
0.8
1.0
1.2
1.4
1.6
< 8.0 8-8.5 8.5-9 9-9.5 9.5-10 10-10.5 10.5-11 >11
Measured Serum Calcium Concentration (mg/dL)
Re
lati
ve
Ris
k o
f D
ea
th Multivariable Adjusted
Adapted from Block GA et al. J Am Soc Nephrol. 2004;15:2208-2218


K/DOQI™ Clinical Practice K/DOQI™ Clinical Practice GuidelinesGuidelines
on Bone Metabolism Target on Bone Metabolism Target LevelsLevelsCKD CKD
Stage 3Stage 3CKD CKD
Stage 4Stage 4CKD CKD
Stage 5Stage 5(on dialysis)(on dialysis)
PP(mg/dL)(mg/dL) 2.7 - 4.62.7 - 4.6 2.7 - 4.62.7 - 4.6 3.5 - 5.5*3.5 - 5.5*
CaCa(mg/dL)(mg/dL) ““Normal”Normal” ““Normal”Normal”
8.4 - 9.5; 8.4 - 9.5; Hypercalcemia Hypercalcemia
= >10.2= >10.2
Intact Intact PTHPTH
(pg/mL)(pg/mL)35 - 7035 - 70 70 - 11070 - 110 150 - 300*150 - 300*



Prevention and Treatment Prevention and Treatment of Renal Osteodystrophyof Renal Osteodystrophy
Prevention of Phosphate Prevention of Phosphate retention and retention and HyperphosphatemiaHyperphosphatemia
Treatment of HypocalcemiaTreatment of Hypocalcemia Vit. D analogsVit. D analogs CalcimimeticsCalcimimetics ParathyroidectomyParathyroidectomy

Phosphate bindersPhosphate binders
Calcium containing Calcium containing CaCO3CaCO3 Ca acetate (Phoslo)Ca acetate (Phoslo) non calcium containing non calcium containing Renagel ,Renvela Renagel ,Renvela lanthanum carbonate (Fosrenol)lanthanum carbonate (Fosrenol) Mg Mg AlAl

Al based phosphate Al based phosphate bindersbinders
Aluminium toxicities Aluminium toxicities
BoneBone
Neurologic Neurologic
hematologic hematologic Calcium based phosphate Calcium based phosphate
bindersbinders


P<5.5 Ca<9.5 P<5.5 Ca<9.5 Ca containing P binder Ca containing P binder
P<5.5 Ca >9.5 no P binderP<5.5 Ca >9.5 no P binder ( if vascular calc.( if vascular calc. non calcium containing P binder) non calcium containing P binder)
P>5.5 Ca <9.5 P>5.5 Ca <9.5 Ca containing P binder Ca containing P binder if Ca x P <55if Ca x P <55 P>5.5 Ca >9.5 P>5.5 Ca >9.5 non Ca containting P non Ca containting P
binderbinder
Ca containing P binders must not be used if:Ca containing P binders must not be used if: PTH <150PTH <150 corrected Ca >10.2corrected Ca >10.2 P binder elemental Ca >1500P binder elemental Ca >1500 total elemental Ca >2000total elemental Ca >2000
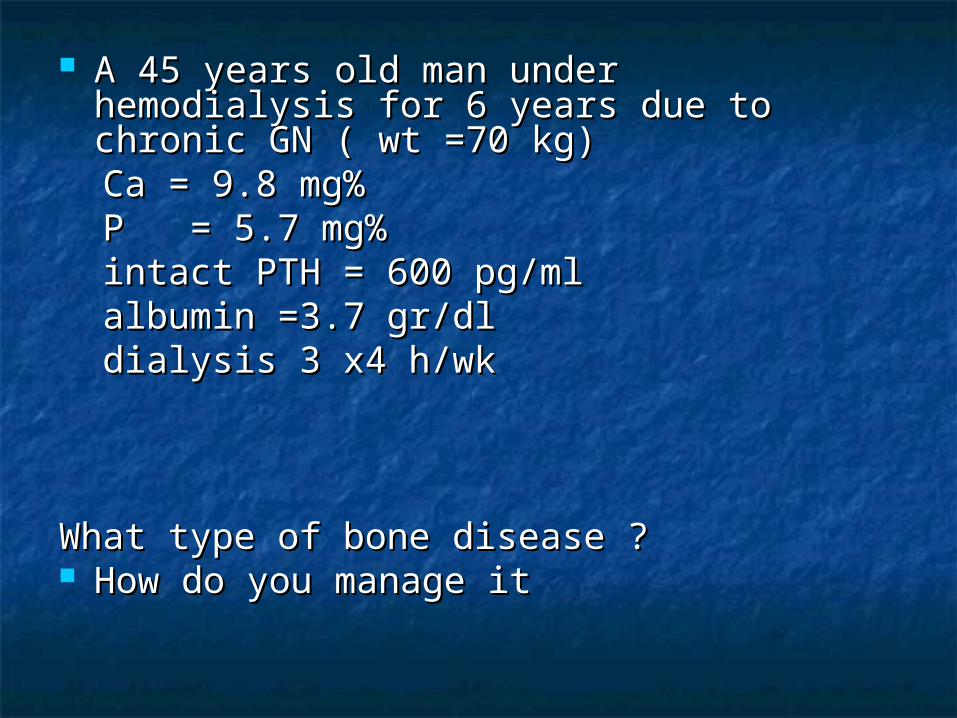
A 45 years old man under hemodialysis for A 45 years old man under hemodialysis for 6 years due to chronic GN ( wt =70 kg)6 years due to chronic GN ( wt =70 kg)
Ca = 9.8 mg%Ca = 9.8 mg% P = 5.7 mg%P = 5.7 mg% intact PTH = 600 pg/mlintact PTH = 600 pg/ml albumin =3.7 gr/dlalbumin =3.7 gr/dl dialysis 3 x4 h/wkdialysis 3 x4 h/wk
What type of bone disease ?What type of bone disease ? How do you manage itHow do you manage it

Diet Diet 800-1000 mg P /d 800-1000 mg P /d Phosphate binder? Phosphate binder? Types of Phosphate binder? Types of Phosphate binder? Calcium containing Calcium containing CaCO3CaCO3 Ca acetate (Phoslo)Ca acetate (Phoslo) non calcium containing non calcium containing Renagel ,Renvela Renagel ,Renvela lanthanum carbonate (Fosrenol)lanthanum carbonate (Fosrenol) Mg Mg Al Al
P>5.5 Ca >9.5 P>5.5 Ca >9.5 non Ca containting P non Ca containting P binderbinder
Dose?Dose? Depends on P blood levelDepends on P blood level daily removaldaily removal daily intake /absorptiondaily intake /absorption binder potencybinder potency

39 mg P will bind to 1 gr CaCO339 mg P will bind to 1 gr CaCO3 45 mg P will bind to 1 gr Ca acetate45 mg P will bind to 1 gr Ca acetate 32 mg to each 400 mg renagel32 mg to each 400 mg renagel 64 mg to each 800 mg renagel tab64 mg to each 800 mg renagel tab 15.3 mg to each Al tab15.3 mg to each Al tab 22.3 mg to 5 ml AlOH322.3 mg to 5 ml AlOH3

For each gr protein intake consider 10-12mg P For each gr protein intake consider 10-12mg P intakeintake
Recommended protein intake in HD=1-1.2 g/kgRecommended protein intake in HD=1-1.2 g/kg 70 x 1.2 = 840 mg /d70 x 1.2 = 840 mg /d 840 x 60% = 504 mg /d 840 x 60% = 504 mg /d accumulation accumulation each dialysis P removal each dialysis P removal 700-800 mg 700-800 mg CAPDCAPD 300 mg/d 300 mg/d 800 x 3= 2400 mg800 x 3= 2400 mg 504 x 7 = 3528 504 x 7 = 3528 3528 – 2400 = 1128 /7= 160 mg /d ( amount of P 3528 – 2400 = 1128 /7= 160 mg /d ( amount of P
that must be bound)that must be bound)
64 mg to each 800 mg renagel tab64 mg to each 800 mg renagel tab about 3 renagel tab /dabout 3 renagel tab /dCa-P recheck within 1-4 wksCa-P recheck within 1-4 wksPTH q 1-3 monthsPTH q 1-3 months

How many Ca CO3 pills ?How many Ca CO3 pills ?
160 mg/39= 4 gr CaCO3 ( 8 tab /d)160 mg/39= 4 gr CaCO3 ( 8 tab /d)
elemental Ca = 4000 mg x40%=elemental Ca = 4000 mg x40%=1600 mg1600 mg
Ca containing P binders must not be used Ca containing P binders must not be used if:if:
PTH <150PTH <150
corrected Ca >10.2corrected Ca >10.2
P binder elemental Ca >1500P binder elemental Ca >1500
total elemental Ca >2000total elemental Ca >2000
COMBINATION POLICYCOMBINATION POLICY

P<5.5 Ca<9.5 P<5.5 Ca<9.5 Ca containing P binder Ca containing P binder
P<5.5 Ca >9.5 no P binderP<5.5 Ca >9.5 no P binder
( if vascular calc.( if vascular calc. non calcium containing P non calcium containing P binder)binder)
P>5.5 Ca <9.5 P>5.5 Ca <9.5 Ca containing P binder Ca containing P binder
P>5.5 Ca >9.5 P>5.5 Ca >9.5 non Ca containting P binder non Ca containting P binder

Vit D derivativesVit D derivatives
if intact PTH >300 & Ca <9.5 & P<5.5 & if intact PTH >300 & Ca <9.5 & P<5.5 &
Ca x P <55Ca x P <55
Corrected Ca >10.2 Corrected Ca >10.2 stopstop
Corrected Ca 9.5-10.2 Corrected Ca 9.5-10.2 50% dose reduction50% dose reduction
corrected Ca rising corrected Ca rising dose reduction dose reduction
Role of low dose active vitamin D irrespective of parathyroid Role of low dose active vitamin D irrespective of parathyroid suppression on overall mortalitysuppression on overall mortality

Vitamin D analogs
25(OH) D3 ( calcifediol)1,25 (OH) D3 (calcitriol, rocaltrol)1 alpha (OH) D3 ( alphacalcidiol ,one alpha)1alpha (OH) D2 (doxercalciferol , hectoral)22 oxa 1,25 (OH) D3 (22 oxacalcitriol ,maxacalcitol)19 nor 1,25( OH) D2 (paricalcitol , zemplar)24,25(OH)D3

CinacalcetCinacalcet indicated in all pts with intact PTH >300 and Ca >8.4 indicated in all pts with intact PTH >300 and Ca >8.4
(decrease parathyroidectomy,cardivascular (decrease parathyroidectomy,cardivascular hospitalizations,Fx)hospitalizations,Fx)
Hyperphosphatemia is not containdicationHyperphosphatemia is not containdication starting dose 30 mg/d starting dose 30 mg/d 180 q4wks180 q4wks cinacalcet must not be started if Ca<8.4cinacalcet must not be started if Ca<8.4 during Tx during Tx Ca <7.4 Ca <7.4 stopstop 7.4-8.47.4-8.4 adding vit d and /calcium if P adding vit d and /calcium if P
<5.5<5.5
So if Ca <9.5 and P <5.5 and Ca x P <55 So if Ca <9.5 and P <5.5 and Ca x P <55 +PTH>300+PTH>300 start with vit.D derivative start with vit.D derivative

28 cinacalcet = 400,000 toman 28 cinacalcet = 400,000 toman Renagel 400 mg= 1980 tomanRenagel 400 mg= 1980 toman AlOH3AlOH3 Increasing dialysisIncreasing dialysis parathyroidectomyparathyroidectomy



How can we calculate daily protein intakeHow can we calculate daily protein intake
CRF= 6.25 ( urine urea nitrogen + nonurea CRF= 6.25 ( urine urea nitrogen + nonurea nitrogen) + proteinuria if > 5 gr/dnitrogen) + proteinuria if > 5 gr/d
nonurea nitrogen =30mg/kgnonurea nitrogen =30mg/kg

How can we calculate daily protein How can we calculate daily protein intakeintake
HD (anuric ) HD (anuric )
PCR = 0.22 + 0.86 x delta BUNPCR = 0.22 + 0.86 x delta BUN
Interval Interval BUN before dialysis = 70BUN before dialysis = 70
BUN after diaysis = 30BUN after diaysis = 30
interval =44 interval =44
0.86 x 40= 34/44= 0.86 x 40= 34/44= 0.78 0.78 gr/kg/dgr/kg/d


Urinary urea nitrogen (g) x 150 Urinary urea nitrogen (g) x 150 anuric PCR+ ——————————————— anuric PCR+ ——————————————— ID interval (hrs) x weight (kg) ID interval (hrs) x weight (kg)
PD: PCR = 6.25 x (Urea appearance + 1.81+[0.031x lean body weight, kg]) PD: PCR = 6.25 x (Urea appearance + 1.81+[0.031x lean body weight, kg])


















