Holistic Nursing Interventions: Stress Relief with Autogenic Training

Hindawi Publishing CorporationAutoimmune DiseasesVolume 2012, Article ID 567324, 12 pagesdoi:10.1155/2012/567324
Review Article
Mind-Body Medicine for Multiple Sclerosis:A Systematic Review
Angela Senders,1 Helane Wahbeh,1 Rebecca Spain,1, 2 and Lynne Shinto1
1 Department of Neurology, Oregon Health & Science University, Portland, OR 97239, USA2 Department of Neurology, Portland Veterans Affairs Medical Center, Portland, OR 97239, USA
Correspondence should be addressed to Angela Senders, [email protected]
Received 8 August 2012; Accepted 6 October 2012
Academic Editor: D. N. Bourdette
Copyright © 2012 Angela Senders et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background. Mind-body therapies are used to manage physical and psychological symptoms in many chronic health conditions.Objective. To assess the published evidence for using mind-body techniques for symptom management of multiple sclerosis.Methods. MEDLINE, PsycINFO, and Cochrane Clinical Trials Register were searched from inception to March 24, 2012. Elevenmind-body studies were reviewed (meditation, yoga, biofeedback, hypnosis, relaxation, and imagery). Results. Four high qualitytrials (yoga, mindfulness, relaxation, and biofeedback) were found helpful for a variety of MS symptoms. Conclusions. The evidencefor mind-body medicine in MS is limited, yet mind-body therapies are relatively safe and may provide a nonpharmacologicalbenefit for MS symptoms.
1. Introduction
Multiple sclerosis (MS) is a chronic neurological disor-der with emotional, cognitive, and physical consequences.Patients can experience a diverse array of symptoms includ-ing impaired mobility, sensory disturbance, chronic pain,fatigue, bladder and bowel dysfunction, depression, andcognitive impairment. Patients report high levels of stress,independent of physical disability [1–3], and the risk ofdeveloping stress-related disorders like anxiety and depres-sion is high (25% and 34–50% lifetime prevalence, resp.) [4–7]. There is no cure for MS, and both disease-modifying andsymptomatic therapies have limitations in compliance due toside effects and cost [8, 9].
Mind-body therapies are used by a growing numberof American adults and children [10]. In a survey of1,110 MS patients, 32% of respondents had used mind-body modalities and reported a high perceived benefit [11].The National Center for Complementary and AlternativeMedicine defines mind-body therapies as those that integratethe brain, mind, body, and behavior, with the intent touse the mind to affect physical functioning and promotehealth [12]. Examples of such modalities include meditation,yoga, relaxation techniques, breathwork, visual imagery,
hypnotherapy, and biofeedback. While these practices varyin technique and application, they share a common objectiveto enhance the capacity of the mind to improve physical andpsychological wellbeing.
Many mind-body therapies can be taught in a clinicalsetting and then subsequently used at home by the patientin a self-directed way, making them ideal tools to promoteincreased self-efficacy. Mind-body techniques often have acalming effect on the autonomic nervous system [13] andthus may be helpful for conditions where psychological stressis a factor. From this perspective, mind-body interventionshold strong potential for use in MS. Broad reviews haveaddressed the use of mind-body therapies in general practice[14] and neurology [15], yet no comprehensive review ofevidence for MS exists. The objective of this paper is tosystematically review the published evidence for mind-bodytherapies for symptom management in MS.
2. Methods
One reviewer performed the searches, assessed inclusioncriteria, and extracted data on trial design and outcomes.Two reviewers independently assessed methodology and risk

2 Autoimmune Diseases
of bias for each study included in this paper. Because weexpected the sample size of mind-body studies to be small,we intentionally kept inclusion criteria broad.
2.1. Types of Studies. We included only controlled trials inthis paper.
2.2. Types of Participants. We included studies of any kindof MS. Studies that did not verify diagnosis of MS or useaccepted diagnostic criteria for their time were included inthis paper; however, their risk of bias is included in ouranalysis. We added the category “MS diagnosis confirmationand criteria” to the Cochrane Risk of Bias Table for thispurpose.
2.3. Types of Interventions. Mind-body therapies includedmeditation and mindfulness, yoga, hypnosis, biofeedback,relaxation, imagery, tai chi, and qi gong.
2.4. Types of Outcome Measures. Included were studieswith any MS outcome related to physical or psychosocialwellbeing. Specific outcomes were not defined.
2.5. Search Strategy for Identification of Studies. One reviewer(A. Senders) searched the electronic databases MEDLINE,PsychInfo, and Cochrane Clinical Trials Register. Databaseswere searched in Ovid (http://www.ovid.com/) from incep-tion to March 24, 2012, using the exploded medical subjectheadings (MeSH): Mind-Body Therapies; Mind-Body Rela-tions, Metaphysical; Therapeutics; Hypnosis; Yoga; Imagery;Biofeedback; Tai Ji; Meditation; Relaxation; Muscle Relax-ation; Relaxation Therapy; Breathwork; Breathing Exercises.Tai chi, Qi Gong, Breathing Technique, and Mindfulnesswere searched as keywords. These MeSH terms and keywordswere then combined with MS terms Multiple Sclerosis;Multiple Sclerosis, Chronic Progressive; Multiple Sclerosis,Relapsing-Remitting. A medical librarian was consulted toreview the search protocol. Only studies reported in theEnglish language were considered in this review. A manualreview of references or related reviews was not completed.The specific search strategy can be found in the Appendix.
2.6. Selection of Studies. One author (A. Senders) conductedthe initial search. Potential publications were selected byscreening titles and abstracts for clinical trials that used amind-body intervention for any type of multiple sclerosis.Final selections were made by screening full articles for thefollowing inclusion criteria: any type of MS, any mind-body intervention, any kind of comparator group, and anyoutcome related to physical or mental wellbeing.
2.7. Data Extraction and Management. Data extraction fromeach study was performed by one author (A. Senders) usinga data collection form that included study design, participantcharacteristics, type and duration of intervention, compara-tor treatment, primary and secondary outcome measures,whether or not homework was prescribed, adherence to
homework, dropout rate/loss to follow up, and summary ofresults. Authors of reviewed studies were not contacted formissing information or clarification.
2.8. Assessment of Risk of Bias in Included Studies. Themethodological quality of clinical trials was assessed accord-ing to the Cochrane Risk of Bias Tool [36]. Assessmentsof bias were independently performed for each paper induplicate (AS, HW, or LS) and any disagreements wererecorded and resolved through discussion.
2.9. Issues of Heterogeneity. One objective of this paper wasto grade the body of evidence for mind-body medicine inMS using the Grading of Recommendations Assessment,Development and Evaluation tool (GRADE) [37]. However,a meta-analysis or reliable grading of the body of evidence isnot feasible due to a large amount of clinical and method-ological variability between studies. Instead we describe andreport on the state of the published evidence to date.
3. Results
Mind-body therapies are briefly described in Table 1. Whilethe therapies are described in discrete categories, consid-erable crossover exists between them. For example, guidedimagery is often included as a part of meditation andrelaxation protocols, yoga has a meditative component to it,and biofeedback for stress reduction often involves relaxationor autogenic training.
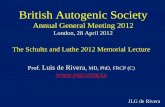
3.1. Search Results. Searching three electronic databasesrevealed a total of 106 articles. Titles and available abstractswere screened for clinical trials that used a mind-bodyintervention for MS; 87 articles were excluded because theywere nonintervention papers and 19 articles were identifiedfor further review (see Figure 1). From this, 10 studies wereselected based on the inclusion criteria above. Six mind-body modalities are included in this paper: two studies ofhypnosis, one of yoga, two of relaxation, two of mindfulness,two of biofeedback, and one study of guided imagery. Ofthe two mindfulness studies, one incorporated the principleof “mindfulness of movement” from tai chi/qi gong. Wecategorized this study as a mindfulness trial. No specificstudies of tai chi or qi gong were identified.
3.2. Description of Included Studies. A summary of thecharacteristics of the 10 studies is provided in Table 2.There were seven randomized controlled trials (RCTs)[25, 27, 30–34], one controlled trial in which the firsteight eligible subjects were enrolled in the experimentalgroup and the subsequent 14 subjects were randomized[28], one prospective cohort study with matched controls[26], and one prospective repeated measures design thatcompared within subject change between four differenthypnosis interventions [29]. Subjects were recruited fromlocal MS Society chapters, outpatient neurology clinics,community advertisements, rehabilitation centers, and localpractitioners. Sample sizes varied from 20 to 150; mean

Autoimmune Diseases 3
Table 1: Description of mind-body therapies and percent use by the general public.
Modality DescriptionUse by the
general public(%) [10]
Meditation
(i) A mental training that is a state of being more than a task. Practices incorporate self-observation andawareness, emotional and attentional regulatory strategies, and the cultivation of an attitude of acceptance.(ii) Many forms exist, share some distinctive features but vary in purpose and technique.(iii) Most widely researched forms include transcendental meditation and mindfulness meditation.
(a) Transcendental meditation: a silent word or phrase (a mantra) is repeated in order to reduce mentalactivity.(b) Mindfulness meditation: practitioners cultivate an open, nonjudgmental awareness of both internalexperiences (thoughts, emotions, and bodily sensations) and external experiences (sights, sounds) inthe present moment. Has been formalized for clinical intervention with mindfulness-based stressreduction, a program that is an amalgam of several mind-body techniques, including mindfulnessmeditation, breathing exercises, yoga postures, and relaxation techniques.
9.4
Yoga
(i) Incorporates physical postures, breathing, meditation into a multifaceted approach to physical/mentalwellbeing.(ii) Many different practices of yoga, each varying in focus.
(a) Hatha yoga is typically gentle with an emphasis on poses and breathwork.(b) Ashtanga and Vinyasa yoga are more physically demanding, moving from posture to posturewithout stopping.(c) Iyengar yoga is most concerned with precision of poses, encourages prop use to attain correctalignment.(d) Bikram Yoga is practiced in a heated room (typically 105◦F).(e) Kundalini yoga incorporates an added emphasis on the breath in conjunction with physical poses.
(iii) Like meditation, the practice of yoga cultivates a way of being rather than performing a task, although,Western practices that focus on exercise and physical health rather than awareness, insight, or spiritualityhave emerged.
6.1
Hypnosis
(i) Relaxed state of focused, inward attention in which peripheral awareness is reduced.(ii) Attaining alteration of consciousness involves absorption, dissociation, and suggestibility.
(a) Absorption: deep immersion in an internal experience.(b) Dissociation: disconnect from peripheral events that would normally be conscious (perceptions,thoughts, emotions, or sensory activity).(c) Suggestibility: suspension of conscious editing (not asking “why?”), respond to suggestion morereadily.
(iii) Therapist may use guided imagery or hypnotic suggestion to help the person to understand behavioralpatterns and envision making desired change.(iv) Self-hypnosis techniques can be used at home, reducing the cost of therapy and encouragingself-efficacy.
0.2
Biofeedback
(i) Electrodes placed on the body provide feedback to the patient about peripheral physiological markerslike heart rate, breathing rate, muscle tension, or electrodermal activity.(ii) Neurofeedback uses scalp electrodes to measure EEG activity.(iii) Information relayed with visual or auditory cues; patient can attempt to change thoughts, emotions, orbehaviors in order to control physiological reactions, such as slowing the heart rate or relaxing certainmuscles.(iv) Strategies are developed and refined with a practitioner, then utilized in real time outside thetherapeutic encounter.(v) Portable biofeedback devices available to enhance relaxation.(vi) Individualized treatment goals depend on the specific condition being addressed.
0.2
Relaxation
(i) Reduces reactivity to physical, psychosocial, and environmental stressors by reducing sympatheticnervous system arousal and enhancing parasympathetic response [16].(ii) The physiological counterpart of the fight-or-flight, response [17].(iii) Jacobson’s progressive muscular relaxation technique and autogenic training are formalized relaxationtechniques, all the mind-body therapies initiate some kind of relaxation response.(iv) Often incorporates breathing techniques that create awareness of breathing rate, rhythm, and volume.(v) Voluntary control of breathing patterns influences autonomic nervous system functions: heart ratevariability, cardiac vagal tone, and CNS excitation as indicated by EEG and MRI [18].(vi) Relaxation training enhances awareness of nervous system activation; patients can employ techniquesat any time to reduce reactivity.
15.6

4 Autoimmune Diseases
Table 1: Continued.
Modality DescriptionUse by the
general public(%) [10]
Imagery
(i) Most prominent forms are guided imagery and motor imagery.(a) Guided imagery: involves visualization and imagination, goal of evoking a state of relaxation ora specific outcome (visualizing the repair of myelin, or one’s white blood cells attacking a tumor).(b) Motor imagery: patient relives the sensations of undertaking a skilled movement without actuallydoing the movement [19]. Physiologic similarities between physically executed and imaginedmovements have been noted in motor evoked potentials, MRI, PET, and EMG studies [20–24].
(ii) Can engage visual, tactile, kinesthetic, olfactory, gustatory, or any combination of these senses.(iii) Imagery typically developed and refined with a therapist, then practiced regularly outside thetherapeutic encounter. Motor imagery is used in addition to physical therapy or exercise and not as anisolated treatment.(iv) Tailored to condition and abilities, it should be practiced in patient’s own context to be meaningful fortheir progress.
2.2
Titles and abstracts identified from electronic databases and screened for retrieval: 106
Potentially appropriate full publications retrieved for full evaluation: 19
Excluded: 87
Total number of controlled trials included in review: 10
Excluded: 9 4 studies were not controlled 1 study had a comparator group but did not make between group comparisons1 study had outcomes that did not meet inclusion criteria 1 study purported relaxation training but in actualityprovided more neuropsych training than relaxation
1 study was a dissertation thesis
1 study had only one MS subject in an n of 30
Figure 1: Flow diagram of literature search and study selection process.
sample size was 46.6 ± 40.1. In total, 466 people withMS were studied. Only three of the studies reported MStype [25, 26, 30]. Two studies used McDonald criteria [38]to confirm diagnosis [25, 27], three reported diagnosisconfirmation by a neurologist but did not discuss criteria[26, 31, 32], two studies reported confirmed diagnoses butdid not report by who or how [30, 33], and three studiesdid not report whether MS diagnosis was confirmed or not[28, 29, 34]. Five studies measured participants’ baselineExpanded Disability Status Scale (EDSS) scores [25, 27, 30–32]; three of these studies provided mean EDSS scores forintervention and comparator groups. The EDSS is a measureof neurological impairment from 0 (normal neurologicalexam) to 10.0 (dead). Patients with scores in the 1.0–3.5range have mild disability with no limitation of walking,4.0–6.5 have increasing difficulty walking, and those 7.0 orhigher require a wheelchair [39]. The average baseline EDSSfor these five studies ranged from 2.9 to 5.9. The duration of
interventions varied from four weeks (one training session aweek) to 6 months (one training session a week). Assessmenttools varied greatly and included a range of subjective andobjective measures consisting of physical (disability, painintensity, fatigue, incontinence, and symptom checklists),psychological (mood profiles, anxiety, pain catastrophizing,and sense of control over health), cognitive (attention, mem-ory, and executive function), and quality of life measures.Eight studies specifically acknowledged asking participantsto practice techniques on their own as homework [25, 27–30, 32–34], and six of these studies made some attemptto quantify homework adherence [25, 27, 28, 30, 32, 33].Dropout rates and loss to follow-up ranged from 0% to 33%.
3.3. Methodological Quality of Included Studies. Table 3 sum-marizes the risk of bias for each study. Review authors’judgments are categorized as High risk of bias (−), Unclearrisk of bias (?), or Low risk of bias (+). Assessments

Autoimmune Diseases 5
Ta
ble
2:Su
mm
ary
ofin
clu
ded
stu
dies
.
Stu
dyD
esig
nIn
terv
enti
onve
rsu
sco
mpa
riso
n
Part
icip
ant
char
acte
rist
ics
Du
rati
onof
inte
rven
tion
Dro
pou
t/lo
ssto
follo
wu
pO
utc
omes
Res
ult
sO
vera
llri
skof
bias
Gro
ssm
anet
al.,
2010
[25]
RC
T
Min
dfu
lnes
str
ain
ing
(n=
76)
vers
us
usu
alca
re(n=
74)
RR
MS
orSP
MS
1se
ssio
n/w
k×
8w
ks5%
Pri
mar
y:qu
alit
yof
life
(PQ
OLC
&H
AQ
UA
MS)
,dep
ress
ion
(CE
S-D
),fa
tigu
e(M
FIS)
.Se
cond
ary:
anxi
ety
(STA
I).
Min
dfu
lnes
str
ain
ing
impr
oved
QO
L(P
QO
LCP<.0
001,
HA
QU
AM
SP=.0
002)
,de
pres
sion
(P=.0
002)
,fat
igu
e(P=.0
005)
,an
dan
xiet
y(P=.0
02)
wh
enco
mpa
red
tou
sual
care
.
Low
Mill
san
dA
llen
,20
00[2
6]
Pro
spec
tive
coh
ort
wit
hm
atch
edco
ntr
ols
Min
dfu
lnes
str
ain
ing
(n=
12)
vers
us
usu
alca
re(n=
12)
SPM
S6
one-
to-o
ne
sess
ion
s33
%
Bal
ance
(sin
gle
leg
stan
d),
Sym
ptom
Rat
ing
Qu
esti
onn
aire
(SR
Q).
(No
prim
ary
outc
omes
stat
ed.)
Bal
ance
impr
oved
from
base
line
inm
indf
uln
ess
grou
p(P
<.0
5)bu
tn
otu
sual
care
(bet
wee
ngr
oup
com
pari
son
not
mad
efo
ra
bala
nce
).SR
Qim
prov
edaf
ter-
min
dfu
lnes
san
dat
3-m
onth
follo
wu
pco
mpa
red
toco
ntr
ols
(P<.0
01).
Hig
h
Oke
net
al.,
2004
[27]
RC
T
Iyen
gar
yoga
(n=
26)
vers
us
exer
cise
bike
(n=
21)
vers
us
wai
tLi
st(n=
22)
MS
type
not
spec
ified
Yoga
:90
min
/wk
for
6m
onth
sE
xerc
ise:
1cl
ass/
wk
for
6m
onth
s
17%
Pri
mar
y:at
ten
tion
(Str
oop
Col
oran
dW
ord
Test
),al
ertn
ess
(EE
G).
Seco
ndar
y:at
ten
tion
(mod
ified
Use
fulF
ield
ofV
iew
task
,ad
apte
dat
ten
tion
alsh
ift
task
,PA
SAT,
Wec
hsl
erM
emor
ySc
ales
III
Logi
calM
emor
y,W
ech
sler
Adu
ltIn
telli
gen
ceSc
ale
III
Sim
ilari
ties
),al
ertn
ess
(SSS
),m
ood
(PO
MS)
,dep
ress
ion
(CE
SD-1
0),a
nxi
ety
(STA
I),
fati
gue
(MFI
),qu
alit
yof
life
(SF-
36),
disa
bilit
y(T
imed
Wal
k,9-
hol
ePe
gTe
st,F
orw
ard
Ben
dFl
exib
ility
).
Th
ere
was
no
sign
ifica
nt
effec
tof
yoga
orex
erci
seon
atte
nti
on,
aler
tnes
s,co
gnit
ive
mea
sure
s,m
ood,
phys
ical
disa
bilit
y,or
gen
eral
qual
ity
oflif
e.B
oth
yoga
and
exer
cise
redu
ced
gen
eral
fati
gue
(P<.0
1)an
dim
prov
eden
ergy
(P<.0
01)
wh
enco
mpa
red
tow
ait
list
con
trol
s.
Low
Jen
sen
etal
.,20
09[2
8]
Con
trol
led
tria
l
Self
-hyp
nos
is(n=
15)
vers
us
PM
R(n=
7)
MS
wit
hch
ron
icda
ilypa
in,t
ype
not
spec
ified
10tr
ain
ing
sess
ion
sof
self
-hyp
nos
isor
PM
R
0%
Pri
mar
y:pa
inin
ten
sity
(0–1
0N
RS)
.Se
cond
ary:
pain
inte
rfer
ence
(mod
ified
BP
I).
Hyp
nos
isre
duce
dav
erag
eda
ilypa
inin
ten
sity
scor
esco
mpa
red
toP
MR
(P<.0
5).N
ogr
oup
diff
eren
cein
pain
inte
rfer
ence
(P<.1
0).
Un
clea
r

6 Autoimmune Diseases
Ta
ble
2:C
onti
nu
ed.
Stu
dyD
esig
nIn
terv
enti
onve
rsu
sco
mpa
riso
n
Part
icip
ant
char
acte
rist
ics
Du
rati
onof
inte
rven
tion
Dro
pou
t/lo
ssto
follo
wu
pO
utc
omes
Res
ult
sO
vera
llri
skof
bias
Jen
sen
etal
.,20
11[2
9]
Pro
spec
tive
,re
pea
ted
mea
sure
s,w
ith
insu
bjec
ttr
eatm
ent
com
pari
son
Edu
cati
onve
rsu
sse
lf-h
ypn
osis
trai
nin
g(H
T)
vers
us
cogn
itiv
ere
stru
ctu
rin
g(C
R)
vers
us
self
-hyp
nos
isan
dco
gnit
ive
rest
ruct
uri
ng
(Hyb
rid)
22p
eopl
ew
ith
MS
and
chro
nic
daily
pain
,typ
en
otsp
ecifi
ed
4se
ssio
ns
ofea
chof
the
4in
terv
enti
ons
32%
Pri
mar
y:pa
inin
ten
sity
(0–1
0N
RS)
,fre
quen
cyof
cata
stro
phiz
ing
cogn
itio
ns
(PC
S).
Seco
ndar
y:pa
inin
terf
eren
ce(m
odifi
edB
PI)
,wor
stpa
inin
ten
sity
(0–1
0N
RS)
.
HT
and
Hyb
rid
decr
ease
dpa
inin
ten
sity
com
pare
dto
pret
reat
men
tle
vels
(P<.0
5).
HT,
CR
,an
dth
eH
ybri
dre
duce
dpa
inca
tast
roph
izin
gsc
ores
com
pare
dto
pret
reat
men
t(H
TP<.0
5,C
RP<.0
5,H
ybri
dP<.0
5)bu
tth
ere
wer
en
odi
ffer
ence
sbe
twee
nth
eth
ree
trai
nin
gs.O
nly
Hyb
rid
redu
ced
pain
inte
rfer
ence
com
pare
dto
pret
reat
men
t(P
<.0
5).
Hig
h
McC
lurg
etal
.,20
06[3
0]R
CT
PFT
(Gro
up
1,n=
10)
vers
us
PFT
&bi
ofee
dbac
k(G
rou
p2,
n=
10)
vers
us
PFT
,B
iofe
edba
ck,
and
ESt
im(G
rou
p3,
n=
10)
Wom
enw
ith
RR
MS,
SPM
S,or
PP
MS
1se
ssio
n/w
k×
9w
ks10
%
Pri
mar
y:le
akag
eep
isod
esp
er24
hrs
(3-d
aydi
ary)
.Se
cond
ary:
24h
rpa
dte
st,v
oidi
ng
freq
uen
cy,m
axim
um
flow
rate
,po
stvo
idre
sidu
alvo
lum
e,st
ren
gth
ofpe
lvic
floo
rm
usc
les,
qual
ity
oflif
e(K
HQ
,MSQ
OL)
,in
con
tin
ence
impa
ct(I
IQ),
uri
nar
ydi
stre
ss(U
DI)
.
Leak
age
epis
odes
decr
ease
d58
%(P=.0
28)
inG
rou
p2
and
76%
(P=.0
03)
inG
rou
p3
com
pare
dto
base
line;
littl
ech
ange
inG
rou
p1.
Th
isre
duct
ion
was
sign
ifica
nt
betw
een
Gro
ups
1an
d3
(P<.0
14).
Gro
ups
2an
d3
impr
oved
inK
HQ
sym
ptom
seve
rity
scal
e(P
<.0
34),
qual
ity
oflif
e(P
<.0
25),
and
uri
nar
ydi
stre
ss(P
<.0
01)
scal
es.N
osi
gnifi
can
tch
ange
sin
pad
test
,vo
idin
gfr
equ
ency
,max
imu
mfl
owra
te,p
ostv
oid
resi
dual
s,an
dpe
lvic
floo
rm
usc
lest
ren
gth
betw
een
grou
ps.
Low
Kla
rsko
vet
al.,
1994
[31]
RC
T
PFT
and
phar
-m
acot
her
apy
(n=
10)
vers
us
PFT
,ph
arm
a-co
ther
apy,
and
biof
eedb
ack
(n=
10)
Gen
eral
reh
abili
tati
onin
pati
ents
wit
hM
S,ty
pe
not
spec
ified
Bio
feed
back
:30
–60
min
less
onq2
wk,
med
ian
3ti
mes
.P
FT:4
0m
inse
ssio
ns
twic
ea
wee
k(m
edia
n6
tim
es).∗
10%
Subj
ecti
vevi
sual
anal
ogfo
rin
con
tin
ence
and
void
ing
sym
ptom
s,le
akag
eep
isod
esp
er24
hrs
(dia
ry),
pad
wei
ght,
cyst
omet
ric
capa
city
,mea
nvo
ided
volu
me,
max
imu
mfl
owra
te,r
esid
ual
uri
ne.
(No
prim
ary
outc
omes
stat
ed.)
No
sign
ifica
nt
diff
eren
ces
betw
een
trea
tmen
tgr
oup
and
con
trol
sfo
ral
lou
tcom
es.
Subj
ecti
vesy
mpt
oms
impr
oved
(P<.0
1),n
um
ber
ofin
con
tin
ence
epis
odes
decr
ease
d(P
<.0
5)an
dm
axim
alcy
stom
etri
cca
paci
tyin
crea
sed
(P<.0
1)fo
ral
lpar
tici
pan
ts.N
och
ange
sse
enin
pad
wei
ght,
mea
nvo
ided
volu
me,
max
imu
mfl
owra
te,a
nd
resi
dual
volu
me
for
allp
arti
cipa
nts
.
Hig
h

Autoimmune Diseases 7
Ta
ble
2:C
onti
nu
ed.
Stu
dyD
esig
nIn
terv
enti
onve
rsu
sco
mpa
riso
n
Part
icip
ant
char
acte
rist
ics
Du
rati
onof
inte
rven
tion
Dro
pou
t/lo
ssto
follo
wu
pO
utc
omes
Res
ult
sO
vera
llri
skof
bias
Gh
afar
iet
al.,
2009
[32]
Con
trol
led
tria
l
PM
RTr
ain
ing
(n=
35)
vers
us
usu
alca
re(n=
35)
MS
type
not
spec
ified
16da
ysof
trai
nin
gin
PM
Rfo
llow
edby
8w
eeks
ofh
ome
prac
tice
wit
hC
D
6%P
rim
ary:
qual
ity
oflif
e(S
F-8)
.
PM
Rtr
ain
ing
grou
psh
owed
sign
ifica
nt
impr
ovem
ents
inqu
alit
yof
life
com
pare
dto
usu
alca
reco
ntr
ols
(P<.0
04).
Low
Suth
erla
nd
etal
.,20
05[3
3]R
CT
Au
toge
nic
trai
nin
g(n=
14)
vers
us
usu
alca
re(n=
12)
MS
type
not
spec
ified
1se
ssio
n/w
k×
10w
ks15
%
Qu
alit
yof
life
(MSQ
OL
),m
ood
(PO
MS-
SF),
depr
essi
on(C
ES-
D).
(No
prim
ary
outc
omes
stat
ed.)
AT
grou
pre
por
ted
mor
een
ergy
than
con
trol
grou
p(P=.0
1)an
dw
ere
less
limit
edin
thei
rro
les
due
toph
ysic
alan
dem
otio
nal
prob
lem
s(P=.0
2,P=.0
5).N
osi
gnifi
can
tdi
ffer
ence
sbe
twee
ngr
oups
wer
ese
enfo
rm
ood
orde
pres
sion
.
Un
clea
r
Mag
uir
e,19
96[3
4]R
CT
Imag
ery
(n=
15)
vers
us
usu
alca
re(n=
18)
MS
type
not
spec
ified
Six
1-h
our
grou
pse
ssio
ns
0%
Moo
d(P
OM
S),a
nxi
ety
(STA
I),
hea
lth
attr
ibu
tion
(HA
T),
MS
sym
ptom
chec
klis
t(d
evel
oped
byP
I).(
No
prim
ary
outc
omes
stat
ed.)
Imag
ery
grou
psh
owed
no
chan
gein
moo
dco
mpa
red
toco
ntr
ols.
Imag
ery
show
edde
crea
sein
stat
ean
xiet
yaf
ter
inte
rven
tion
(P<.0
5)bu
tn
ottr
ait
anxi
ety
com
pare
dto
con
trol
s.T
he
“in
tern
alco
ntr
olof
hea
lth”
scor
efo
rim
ager
ygr
oup
rem
ain
edst
able
but
decr
ease
dfo
rco
ntr
ols
(P<.0
5).
Un
clea
r
BP
I:B
rief
Pain
Inve
nto
ry;
CE
S-D
:C
ente
rfo
rE
pide
mio
logi
cSt
udi
es-D
epre
ssio
nSc
ale;
ESt
im:
Neu
rom
usc
ula
rel
ectr
ical
stim
ula
tion
;H
AQ
UA
MS:
Ham
burg
Qu
alit
yof
Life
Qu
esti
onn
aire
inM
ult
iple
Scle
rosi
s;H
AT
:H
ealt
hA
ttri
buti
onTe
st;
IIQ
:In
con
tin
ence
Impa
ctQ
ues
tion
nai
re;
KH
Q:
Kin
g’s
Hea
lth
Qu
esti
onn
aire
;M
FI:
Mu
ltid
imen
sion
alFa
tigu
eIn
ven
tory
;M
FIS:
Mod
ified
Fati
gue
Inve
nto
rySc
ale;
MSQ
OL
:M
SQ
ual
ity
ofLi
feIn
stru
men
t;N
RS:
Nu
mbe
rR
atin
gSc
ale;
PASA
T:P
aced
Au
dito
rySe
rial
Add
itio
nTe
st;P
CS:
Pain
Cat
astr
oph
izin
gSc
ale;
PFT
:pel
vic
floo
rtr
ain
ing;
PM
R:p
rogr
essi
vem
usc
lere
laxa
tion
;PO
MS-
SF:
Pro
file
ofM
ood
Stat
es-S
hor
tFo
rm;P
PM
S:pr
imar
ypr
ogre
ssiv
eM
S;P
QO
LC:P
rofi
leof
Hea
lth
-Rel
ated
Qu
alit
yof
Life
inC
hro
nic
Dis
orde
rs;
RC
T:r
ando
miz
edco
ntr
olle
dtr
ial;
RR
MS:
rela
psin
gre
mit
tin
gM
S;SP
MS:
seco
nda
rypr
ogre
ssiv
eM
S;SS
S:St
anfo
rdSl
eepi
nes
sSc
ale;
STA
I:St
ate
Trai
tA
nxi
ety
Inve
nto
ry;U
DI:
Uri
nar
yD
istr
ess
Inve
nto
ry.
∗ Tot
aln
um
ber
ofse
ssio
ns
over
wh
atle
ngt
hof
tim
eis
un
clea
r.

8 Autoimmune Diseases
Ta
ble
3:Su
mm
ary
ofri
skof
bias
asse
ssm
ent.
Stu
dyIn
terv
enti
onR
ando
mse
quen
cege
ner
atio
n
Allo
cati
onco
nce
alm
ent
Blin
din
gof
part
icip
ants
and
pers
onn
el
Blin
din
gof
outc
ome
asse
ssm
ent
Inco
mpl
ete
outc
ome
data
Sele
ctiv
ere
port
ing
MS
diag
nos
isan
dcr
iter
iaO
ther
bias∗
Ove
rall
risk
ofbi
asfo
rst
udy
Gro
ssm
anet
al.2
010,
[25]
Min
dfu
lnes
s+
+−
++
++
++
Mill
san
dA
llen
,200
0[2
6]M
indf
uln
ess
??
−−
−?
+−
−O
ken
etal
.,20
04[2
7]Yo
ga+
+−
++
++
?+
McC
lurg
etal
.,20
06[3
0]B
iofe
edba
ck+
?−
++
++
++
Kla
rsko
vet
al.,
1994
[31]
Bio
feed
back
??
−−
++
?−
−Je
nse
net
al.,
2011
[29]
Hyp
nos
is?
?−
+−
+?
−−
Jen
sen
etal
.,20
09[2
8]H
ypn
osis
??
−+
++
?−
?G
haf
arie
tal
.,20
09[3
2]R
elax
atio
n?
?−
?+
++
++
Suth
erla
nd
etal
.,20
05[3
3]R
elax
atio
n?
?−
?+
++
−?
Mag
uir
e,19
96[3
4]Im
ager
y?
?−
?+
+?
−?
(+)
Low
risk
ofbi
as.
( −)
Hig
hri
skof
bias
.(?
)U
ncl
ear
risk
ofbi
as.
∗ Oth
erbi
asca
tego
ryin
clu
des
smal
lsam
ple
size
(n<
30)
[35]
,stu
dies
wh
ich
repo
rted
bein
gu
nde
rpow
ered
and
min
imal
orn
ogr
oup
com
pari
son
atba
selin
e.

Autoimmune Diseases 9
Table 4: Of 10 studies reviewed, four high quality studies werefound helpful for symptoms of MS.
Study Intervention Helpful for
Ghafari et al.,2009 [32]
Relaxation Quality of Life
Grossman et al.,2010 [25]
Mindfulness-basedstress reduction
DepressionAnxietyFatigueQuality of Life
Oken et al.,2004 [27]
Yoga Fatigue
McClurg et al.,2006 [30]
Biofeedback Bladder incontinence
consider the risk of bias of sufficient magnitude to have anotable impact on the results or conclusions of the trial.Several of the studies failed to provide enough detail foradequate assessment. Details regarding random sequencegeneration and allocation concealment were particularlypoorly reported. Three studies did not provide sufficientdetails about baseline characteristics of comparison groups[28, 29, 31]. As it is impossible to blind participants tointerventions that require their active involvement, all 10studies received High risk of bias scores for this category.Sample sizes were generally small and seven of the studieshad ≤33 subjects. Only three studies provided intention totreat analysis [25, 27, 30]. Overall, we found four of the 10studies to be methodologically sound [25, 27, 30, 32], threeto have an Unclear risk of bias [28, 33, 34], and three to havehigh overall risk of bias (Table 3) [26, 29, 31].
4. Discussion
The objective of this paper was to assess the publishedevidence for using mind-body techniques for symptommanagement of multiple sclerosis. Four high quality studiesshowed that mindfulness, yoga, biofeedback, and relaxationhad a positive effect on depression, anxiety, fatigue, qualityof life, and bladder incontinence (Table 4) and no effect ondisability, executive function, or other cognitive measures.The remaining studies demonstrated benefit for balance anddaily pain intensity, but had no effect on executive function,mood, or disability—although many methodological inade-quacies were identified. This paper demonstrates that studiesof mind-body techniques for treating MS symptoms arefeasible, and that more stringently designed, well-executedresearch is needed in this population to determine efficacy.
4.1. Implications for Research. More rigorous research isneeded utilizing mind-body techniques for MS. Of the fewstudies identified in this paper, most were not of highquality, often due to small numbers and a lack of assessorblinding. In trials where it is impossible to blind participantsto the study intervention, it is imperative to ensure thatthose assessing outcomes have no knowledge of the subjects’group assignment. Reporting on the blinding methodology
for outcome assessors including maintenance of blindingthroughout the study will improve the quality of future trials.
Placebo effects due to expectation are important to assessin trials where subjects are not blinded. Because subjectsknow which intervention group they will be participatingin, it is possible that anticipation of improvement mayinfluence outcomes. Only one study in this paper evaluatedexpectation effects. Jensen et al., 2009 found that expectancywas associated with a positive treatment outcome in responseto self-hypnosis training for chronic pain. It is importantto measure such relationships so that expectancy effectsare distinguished from true intervention effects, and theimpact of expectancy on outcome can be determined. Fur-thermore, such research may help identify ways to enhanceexpectancy in the clinical setting. In clinical practice whenpatients are given a known therapy, the effectiveness of thetherapy is a combination of nonspecific and biologicallyactive effects. Understanding the nonspecific effects thatcontribute to beneficial findings in trials (e.g., expectation,self-efficacy, motivation for improvement, locus of control,patient/provider relations, and attitudes toward one’s diseaseand healing) will further our knowledge of mind-bodytherapies and enhance the generalizability of research trialsto clinical practice.
The selection of appropriate comparison groups iscritical when designing nonblinded intervention trials usingmind-body techniques. Six studies in this paper used anonintervention control group (either usual care or waitlist)[25–27, 32–34]. A limitation of this design is that it doesnot control for nonspecific factors involved in the treatmentgroup like social effects of group work and attention frominstructors [40]. A well-chosen active comparison group cancontrol both treatment-specific and nonspecific effects ofthe study intervention, although this kind of comparisonhas disadvantages as well. A drawback to active controls isthat they can exert their own therapeutic benefit beyondnonspecific social effects, thus making comparisons betweengroups difficult to interpret [41]. For example, Oken etal. compared yoga with an active control (exercise) toevaluate yoga-specific effects and control time and attentionof the intervention and found few differences betweengroups. Exercise is known to have a therapeutic benefit inMS [42] and this could have been problematic had theauthors not also included a nonintervention (waitlist) groupfor comparison. Three-arm trials that include both activeand nonintervention controls are favorable if they can beafforded. Challenges regarding control group selection formind-body medicine are not new and have been describedby others [41, 43, 44].
Level of disability should be considered during the designof a study. One example is highlighted by the Klarskov study[31]. The biofeedback protocol in this trial was specificallydesigned to enhance the awareness of muscles in the pelvicfloor, yet 11 of the 20 subjects could not voluntarily contractpelvic floor muscles as measured by EMG, and 18 of the20 subjects were unable to contract muscles voluntarily asmeasured by digital exam. The goal of the intervention wasto use EMG feedback and yet a majority of the participantswere unable to produce an EMG signal. Thus, the high

10 Autoimmune Diseases
baseline disability scores may have accounted for the absenceof biofeedback effect between groups. Inclusion criteria fora baseline disability that allowed for an appropriate EMGfeedback would have strengthened the study design andhelped determine a therapeutic benefit.
While it may appear self-evident that mind-body ther-apies have a favorable risk-benefit ratio, only one studyspecifically discussed safety in terms of adverse events [27].Four papers reported why subjects dropped out of thestudy, but furnished no other safety information [25, 26, 30,33]. Based on limited data, no intervention-related safetyissues were identified in this paper. Even though mind-body interventions are typically gentle and serious adverseevents, unlikely, future trials should collect data necessary tocalculate appropriate risk assessments.
In order to advance mind-body research for MS, futurestudies must attempt to adequately power their trials for anappropriate sample size. Only three studies reported poweranalyses a priori and as a result had adequate sample sizes[25, 27, 32]. The remaining trials did not benefit from poweranalyses and thus risked type II error, or false negative results.
4.2. Implications for Practice. Mind-body therapies are valu-able because they can improve symptoms that affect qualityof life. For example, fatigue is one of the most common andtroubling symptoms in MS. MS-related fatigue is associatedwith decreased quality of life and depression and is describedas the worst symptom of MS by 69% of patients [45]. It isestimated that 75–95% of MS patients suffer from fatigue[45, 46] and pharmaceutical treatment provides limitedrelief. Our paper found that both yoga and mindfulnesstraining improved MS fatigue, offering support with fewerside effects than conventional treatment. Therapies that canimprove quality of life and the patient’s ongoing experienceof MS are essential to the successful management of thisdisease.
While there are not enough research studies to providestrong evidence for the use of mind-body therapies inMS, there is no evidence stating that they are harmfuleither. Patients who express interest in participating in suchtherapies do not necessarily need to be dissuaded because ofharmful effects. However, clinicians should be mindful of afew key points when discussing mind-body medicine withMS patients.
(i) Hypnosis can allow distressing, repressed psycholog-ical content to come into consciousness and maynot be appropriate for some patients with psychiatricdisorders [47].
(ii) Guided or motor imagery requires that individualsimagine themselves performing a task, including thesensations that may accompany that activity and maynot be suitable for patients with substantial cognitiveimpairment [48].
(iii) Yoga may not be appropriate for people withmusculoskeletal conditions unless postures can bemodified for individual circumstances. Props, suchas cushions, blocks, and straps, can aid patients in
holding poses, requiring less muscular effort. BikramYoga is practiced in a heated room (typically 105◦)and risks exacerbating MS symptoms [49]. Workingwith a teacher who has experience adapting yogapractice for those with disabilities is advised.
(iv) Practitioner training and licensing may be an issuefor some modalities. Health care providers can usebiofeedback devices within the scope of practicedefined by their license. Voluntary certification isavailable [50] for those who do not hold a health carelicense, but is not currently required by most states.Thus, training and experience may vary greatly fromone therapist to the next and should be investigated.Hypnosis is typically practiced as an adjunct to psy-chotherapy by mental health care providers; however,most states do not require a license to practice anda hypnotherapist’s credentials should be investigated.Patients should be advised to seek out appropriatelytrained providers for the modality they are interestedin.
4.3. Limitations of This Paper. The current study had limita-tions that should be considered in interpreting the results.A single author performed database searches, conductedinitial reviews, and extracted data; thus the initial studyselection and data extraction may have been subject to biasand error. To address this, a librarian formulated a secondsearch strategy that failed to retrieve any new articles (seethe Appendix). That both search strategies retrieved identicalresults suggests no bias at the initial searching level. OnlyEnglish language trials were included. Including foreignlanguage search results may have contributed additionalstudies. Other studies may have been inadvertently missedbecause a manual search of references and reviews wasnot done. Authors were also not contacted for missinginformation. Regardless of these limitations, this is thefirst paper to assess the published research for mind-bodymedicine in MS. This is a starting point upon which onecan build further assessment of the efficacy and feasibility ofmind-body therapies for MS.
5. Conclusion
We found evidence to suggest that mind-body therapiesare effective for treating common MS symptoms, includingfatigue, anxiety, depression, incontinence, and quality of life.Mind-body modalities appear safe, can be prescribed as anadjunct to conventional care, and may be especially helpfulwhen psychosocial stress is a factor or non-pharmacologicaloptions are desired (e.g., polypharmacy, pregnancy, andpatient preference). More rigorously designed trials of mind-body interventions applied specifically to MS are neededin order to determine their efficacy and optimal selectionfor specific MS symptoms. Such research will enhance ourunderstanding of the clinical effects of mind-body medicineas well as increase awareness and availability to clinicians andpatients alike.

Autoimmune Diseases 11
Appendix
Two search strategies were applied to each electronic data-base: MEDLINE, PsycINFO, and Cochrane Clinical TrialsRegister.
(1) Hannon search strategy: (exp Mind-Body TherapiesOR exp Mind-Body Relations, Metaphysical) AND(exp therapeutics OR th.fs.) AND exp multiplesclerosis OR multiple sclerosis, chronic progressiveOR multiple sclerosis, relapsing-remitting).
(2) Senders search strategy: (exp multiple sclerosis ORmultiple sclerosis, chronic progressive OR multiplesclerosis, relapsing-remitting) AND (qi gong.mp.OR exp Meditation OR mindfulness.mp. OR expRelaxation OR exp Muscle Relaxation OR expRelaxation Therapy OR exp Breathing Exercises ORbreathing technique.mp. OR breathwork.mp. ORbreathwork.mp. OR exp Hypnosis OR exp “Imagery(Psychotherapy)” OR exp Yoga OR exp Biofeedback,Psychology OR exp Tai Ji OR tai chi.mp.).
Conflict of Interests
The authors have no conflict of interests.
Acknowledgments
The authors thank Marian McDonagh for valuable directionand Todd Hannon for help with the search strategies. Thiswork was supported by the Oregon Clinical and TranslationalResearch Institute Grant number UL1 RR024140 from theNational Center for Research Resources and the NationalCenter for Advancing Translational Sciences of the NationalInstitutes of Health, and the National Center for Comple-mentary and Alternative Medicine of the National Institutesof Health Grant numbers AT002688, K01AT004951. Thecontent of this paper is solely the responsibility of the authorsand does not necessarily represent the official views of theNational Institutes of Health.
References
[1] J. M. Buelow, “A correlational study of disabilities, stressorsand coping methods in victims of multiple sclerosis,” TheJournal of Neuroscience Nursing, vol. 23, no. 4, pp. 247–252,1991.
[2] M. A. Counte, L. A. Bieliauskas, and M. Pavlou, “Stressand personal attitudes in chronic illness,” Archives of PhysicalMedicine and Rehabilitation, vol. 64, no. 6, pp. 272–275, 1983.
[3] H. M. Chalk, “Mind over matter: cognitive-behavioral deter-minants of emotional distress in multiple sclerosis patients,”Psychology, Health and Medicine, vol. 12, no. 5, pp. 556–566,2007.
[4] M. Korostil and A. Feinstein, “Anxiety disorders and theirclinical correlates in multiple sclerosis patients,” MultipleSclerosis, vol. 13, no. 1, pp. 67–72, 2007.
[5] S. L. Minden, J. Orav, and P. Reich, “Depression in multiplesclerosis,” General Hospital Psychiatry, vol. 9, no. 6, pp. 426–434, 1987.
[6] D. S. P. Schubert and R. H. Foliart, “Increased depression inmultiple sclerosis patients: a meta-analysis,” Psychosomatics,vol. 34, no. 2, pp. 124–130, 1993.
[7] S. B. Patten, C. A. Beck, J. V. A. Williams, C. Barbui, and L. M.Metz, “Major depression in multiple sclerosis: a population-based perspective,” Neurology, vol. 61, no. 11, pp. 1524–1527,2003.
[8] H. L. Zwibel and J. Smrtka, “Improving quality of life in mul-tiple sclerosis: an unmet need,” American Journal of ManagedCare, vol. 17, supplement 5, pp. S139–S145, 2011.
[9] A. Rinon, M. Buch, D. Holley, and E. Verdun, “The MSChoices Survey: findings of a study assessing physician andpatient perspectives on living with and managing multiplesclerosis,” Patient Prefer Adherence, vol. 5, pp. 629–643, 2011.
[10] P. M. Barnes, B. Bloom, and R. L. Nahin, “Complementary andalternative medicine use among adults and children: UnitedStates, 2007,” National Health Statistics Reports, no. 12, pp. 1–23, 2009.
[11] V. Yadav, L. Shinto, C. Morris, A. Senders, S. Baldauf-Wagner,and D. Bourdette, “Use and self-reported benefit of comple-mentary and alternative medicine among multiple sclerosispatients,” International Journal of Multiple Sclerosis Care, vol.8, pp. 5–10, 2006.
[12] “What is complementary and alternative medicine?” 2012,http://nccam.nih.gov/health/whatiscam.
[13] A. G. Taylor, L. E. Goehler, D. I. Galper, K. E. Innes, and C.Bourguignon, “Top-down and bottom-up mechanisms inmind-body medicine: development of an integrative frame-work for psychophysiological research,” Explore, vol. 6, no. 1,pp. 29–41, 2010.
[14] J. A. Astin, S. L. Shapiro, D. M. Eisenberg, and K. L. Forys,“Mind-body medicine: state of the science, implications forpractice,” Journal of the American Board of Family Practice, vol.16, no. 2, pp. 131–147, 2003.
[15] H. Wahbeh, S. M. Elsas, and B. S. Oken, “Mind-body interven-tions: applications in neurology,” Neurology, vol. 70, no. 24,pp. 2321–2328, 2008.
[16] T. Esch, G. L. Fricchione, and G. B. Stefano, “The therapeuticuse of the relaxation response in stress-related diseases,”Medical Science Monitor, vol. 9, no. 2, pp. RA23–RA34, 2003.
[17] H. Benson, J. F. Beary, and M. P. Carol, “The relaxationresponse,” Psychiatry, vol. 37, no. 1, pp. 37–46, 1974.
[18] R. P. Brown and P. L. Gerbarg, “Sudarshan Kriya yogicbreathing in the treatment of stress, anxiety, and depression—part I—neurophysiologic model,” Journal of Alternative andComplementary Medicine, vol. 11, no. 1, pp. 189–201, 2005.
[19] S. Braun, M. Kleynen, J. Schols, T. Schack, A. Beurskens, andD. Wade, “Using mental practice in stroke rehabilitation: aframework,” Clinical Rehabilitation, vol. 22, no. 7, pp. 579–591, 2008.
[20] J. Decety and M. Jeannerod, “Mentally simulated movementsin virtual reality: does Fitt’s law hold in motor imagery?”Behavioural Brain Research, vol. 72, no. 1-2, pp. 127–134, 1996.
[21] B. Wuyam, S. H. Moosavi, J. Decety, L. Adams, R. W. Lansing,and A. Guz, “Imagination of dynamic exercise produced ven-tilatory responses which were more apparent in competitivesportsmen,” Journal of Physiology, vol. 482, no. 3, pp. 713–724,1995.
[22] S. Thobois, P. F. Dominey, J. Decety et al., “Motor imageryin normal subjects and in asymmetrical Parkinson’s disease:a PET study,” Neurology, vol. 55, no. 7, pp. 996–1002, 2000.
[23] M. Bonnet, J. Decety, M. Jeannerod, and J. Requin, “Mentalsimulation of an action modulates the excitability of spinal

12 Autoimmune Diseases
reflex pathways in man,” Cognitive Brain Research, vol. 5, no.3, pp. 221–228, 1997.
[24] L. Fadiga, G. Buccino, L. Craighero, L. Fogassi, V. Gallese, andG. Pavesi, “Corticospinal excitability is specifically modulatedby motor imagery: a magnetic stimulation study,” Neuropsy-chologia, vol. 37, no. 2, pp. 147–158, 1998.
[25] P. Grossman, L. Kappos, H. Gensicke et al., “MS quality of life,depression, and fatigue improve after mindfulness training: arandomized trial,” Neurology, vol. 75, no. 13, pp. 1141–1149,2010.
[26] N. Mills and J. Allen, “Mindfulness of movement as a copingstrategy in multiple sclerosis. A pilot study,” General HospitalPsychiatry, vol. 22, no. 6, pp. 425–431, 2000.
[27] B. S. Oken, S. Kishiyama, D. Zajdel et al., “Randomizedcontrolled trial of yoga and exercise in multiple sclerosis,”Neurology, vol. 62, no. 11, pp. 2058–2064, 2004.
[28] M. P. Jensen, J. Barber, J. M. Romano et al., “A comparison ofself-hypnosis versus progressive muscle relaxation in patientswith multiple sclerosis and chronic pain,” International Journalof Clinical and Experimental Hypnosis, vol. 57, no. 2, pp. 198–221, 2009.
[29] M. P. Jensen, D. M. Ehde, K. J. Gertz et al., “Effects of self-hypnosis training and cognitive restructuring on daily painintensity and catastrophizing in individuals with multiplesclerosis and chronic pain,” International Journal of Clinicaland Experimental Hypnosis, vol. 59, no. 1, pp. 45–63, 2011.
[30] D. McClurg, R. G. Ashe, K. Marshall, and A. S. Lowe-Strong,“Comparison of pelvic floor muscle training, electromyog-raphy biofeedback, and neuromuscular electrical stimulationfor bladder dysfunction in people with multiple sclerosis: arandomized pilot study,” Neurourology and Urodynamics, vol.25, no. 4, pp. 337–348, 2006.
[31] P. Klarskov, E. Heely, I. Nyholdt, K. Rottensten, and A.Nordenbo, “Biofeedback treatment of bladder dysfunction inmultiple sclerosis. A randomized trial,” Scandinavian Journalof Urology and Nephrology, no. 157, pp. 61–65, 1994.
[32] S. Ghafari, F. Ahmadi, M. Nabavi, K. Anoshirvan, R.Memarian, and M. Rafatbakhsh, “Effectiveness of applyingprogressive muscle relaxation technique on quality of life ofpatients with multiple sclerosis,” Journal of Clinical Nursing,vol. 18, no. 15, pp. 2171–2179, 2009.
[33] G. Sutherland, M. B. Andersen, and T. Morris, “Relaxation andhealth-related quality of life in multiple sclerosis: the exampleof autogenic training,” Journal of Behavioral Medicine, vol. 28,no. 3, pp. 249–256, 2005.
[34] B. L. Maguire, “The effects of imagery on attitudes and moodsin multiple sclerosis patients,” Alternative Therapies in Healthand Medicine, vol. 2, no. 5, pp. 75–79, 1996.
[35] R. A. Moore, D. Gavaghan, M. R. Tramer, S. L. Collins, and H.J. McQuay, “Size is everything—large amounts of informationare needed to overcome random effects in estimating directionand magnitude of treatment effects,” Pain, vol. 78, no. 3, pp.209–216, 1998.
[36] J. P. T. Higgins, D. G. Altman, P. C. Gøtzsche, P. Juni, D. Moher,and A. D. Oxman, “The Cochrane Collaboration’s tool forassessing risk of bias in randomised trials,” British MedicalJournal, vol. 343, Article ID d5928, 2011.
[37] J. L. Broek, E. A. Akl, P. Alonso-Coello et al., “Grading qualityof evidence and strength of recommendations in clinicalpractice guidelines—part 1 of 3. An overview of the GRADEapproach and grading quality of evidence about interven-tions,” Allergy, vol. 64, no. 5, pp. 669–677, 2009.
[38] W. I. McDonald, A. Compston, G. Edan et al., “Recommendeddiagnostic criteria for multiple sclerosis: guidelines from the
International panel on the diagnosis of multiple sclerosis,”Annals of Neurology, vol. 50, no. 1, pp. 121–127, 2001.
[39] J. F. Kurtzke, “Rating neurologic impairment in multiple scle-rosis: an expanded disability status scale (EDSS),” Neurology,vol. 33, no. 11, pp. 1444–1452, 1983.
[40] Z. Di Blasi, E. Harkness, E. Ernst, A. Georgiou, and J. Kleijnen,“Influence of context effects on health outcomes: a systematicreview,” Lancet, vol. 357, no. 9258, pp. 757–762, 2001.
[41] W. E. Whitehead, “Control groups appropriate for behavioralinterventions,” Gastroenterology, vol. 126, no. 1, supplement1,pp. S159–S163, 2004.
[42] U. Dalgas, E. Stenager, and T. Ingemann-Hansen, “Multiplesclerosis and physical exercise: recommendations for the appli-cation of resistance-, endurance- and combined training,”Multiple Sclerosis, vol. 14, no. 1, pp. 35–53, 2008.
[43] M. B. Ospina, K. Bond, M. Karkhaneh et al., “Clinical trialsof meditation practices in health care: characteristics andquality,” Journal of Alternative and Complementary Medicine,vol. 14, no. 10, pp. 1199–1213, 2008.
[44] P. Mansky, T. Sannes, D. Wallerstedt et al., “Tai chi chuan:mind-body practice or exercise intervention? Studying thebenefit for cancer survivors,” Integrative Cancer Therapies, vol.5, no. 3, pp. 192–201, 2006.
[45] H. L. Zwibel, “Contribution of impaired mobility and generalsymptoms to the burden of multiple sclerosis,” Advances inTherapy, vol. 26, no. 12, pp. 1043–1057, 2009.
[46] T. Ziemssen, “Multiple sclerosis beyond EDSS: depression andfatigue,” Journal of the Neurological Sciences, vol. 277, no. 1,supplement, pp. S37–S41, 2009.
[47] K. Barrows, Complementary & Alternative Medicine. CurrentMedical Diagnosis & Treatment, McGraw-Hill, 2012.
[48] C. L. Hovington and B. Brouwer, “Guided motor imagery inhealthy adults and stroke: does strategy matter?” Neuroreha-bilitation and Neural Repair, vol. 24, no. 9, pp. 851–857, 2010.
[49] T. C. Guthrie and D. A. Nelson, “Influence of temperaturechanges on multiple sclerosis: critical review of mechanismsand research potential,” Journal of the Neurological Sciences,vol. 129, no. 1, pp. 1–8, 1995.
[50] “Biofeedback Certification International Alliance,” 2012,http://www.bcia.org/i4a/pages/index.cfm?pageid=1.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com