AUTOGENIC DENTAL TRANSPLANTS - Northway...
26
AUTOGENIC DENTAL TRANSPLANTS William M. Northway The movement of one or more teeth from one location in a person’s mouth to another location in that individual’s mouth is referred to as an autogenic dental transplant. It is thought that Ambrose Pare was the first author to describe replantation of teeth in 1562. He detailed the replacement of a tooth for a woman of nobility that was provided from the mouth of one of her ladies in waiting. This would have been an allogenic transplant; this kind of transplant has not been shown to be very successful. Conversely, autogenic transplants are well documented and have gained acceptance, especially in Europe and Japan. However, autogenic transplants have not attained much popularity in North America, in spite of their documented success. Slagsvold reported on 34 consecutively trans- planted premolars with 100% success (Slagsvold and Bjercke, 1978a,b). Ahlberg discussed the transplantation of 33 maxillary canines with 88% suc- cess (Ahlberg et al., 1983). Pogrel reported a 72% success rate on 416 trans- plants performed under less than ideal circumstances (Pogrel, 1987). Andreasen in his four-article series discussed 370 premolar transplants with a success rate of 95% for transplants with incomplete roots and 98% for transplants with completed roots (Andreasen et al., 1990a,b,c,d). Our own survey turned up a success rate of 80.2% among members of the Angle society who responded as having been involved with transplants and 73.9% among chairmen of oral surgery departments who had provided transplants. The indications for autogenic transplants historically have consti- tuted the need for a tooth in one region in the mouth while having an abun- dance of teeth in another part of the mouth. A comparison of the esthetic results that have been produced by transplantation in the maxillary incisor area with those found following osseointegrated implants might lead one to consider strongly transplants for anterior replacement (Czochrowska, 2002b,c). Further, the property of developing increased alveolar bone while the transplanted root develops in areas of diminished alveolus provides a powerful incentive for transplantation in such edentulous areas. With the advances in stem cell research and the progress being made in growing dentin, it is probable that tooth-like structures with the potential for im- plantation will begin replacing edentulous areas in the not too distant future (Batouli et al., 2003; Bianco and Robey, 2001; Gronthos et al., 2002; Krebs- bach and Robey, 2002; Miura et al., 2003). Multiple authors (Slagsvold and Bjercke, 1974; Andreasen, 1980a,b; Northway and Konisgberg, 1980; Andreasen and Kristerson, 1981a,b; Ahlberg et al., 1983; Monsour and Adkins, 1983; Pogrel, 1987; Andreasen 1990a; Czochrowska et al., 2000; Tsukiboshi, 2001) have reported on the
Transcript of AUTOGENIC DENTAL TRANSPLANTS - Northway...

AUT
The movemeto another lodental transpdescribe repltooth for a wher ladies in of transplant
Congained acceptransplants htheir documeplanted premAhlberg discucess (Ahlbergplants perfoAndreasen ina success rattransplants wsurvey turnesociety who ramong chairm
The tuted the needance of teetresults that harea with thoconsider str2002b,c). Furthe transplanpowerful incadvances in dentin, it is plantation wi(Batouli et al.bach and Rob
MultNorthway aAhlberg et al1990a; Czoch
OGENIC DENTAL TRANSPLANTS
William M. Northway nt of one or more teeth from one location in a person’s mouth cation in that individual’s mouth is referred to as an autogenic lant. It is thought that Ambrose Pare was the first author to antation of teeth in 1562. He detailed the replacement of a oman of nobility that was provided from the mouth of one of waiting. This would have been an allogenic transplant; this kind has not been shown to be very successful. versely, autogenic transplants are well documented and have tance, especially in Europe and Japan. However, autogenic ave not attained much popularity in North America, in spite of nted success. Slagsvold reported on 34 consecutively trans-olars with 100% success (Slagsvold and Bjercke, 1978a,b). ssed the transplantation of 33 maxillary canines with 88% suc- et al., 1983). Pogrel reported a 72% success rate on 416 trans-rmed under less than ideal circumstances (Pogrel, 1987). his four-article series discussed 370 premolar transplants with e of 95% for transplants with incomplete roots and 98% for ith completed roots (Andreasen et al., 1990a,b,c,d). Our own
d up a success rate of 80.2% among members of the Angle esponded as having been involved with transplants and 73.9% en of oral surgery departments who had provided transplants.
indications for autogenic transplants historically have consti-d for a tooth in one region in the mouth while having an abun-h in another part of the mouth. A comparison of the esthetic ave been produced by transplantation in the maxillary incisor se found following osseointegrated implants might lead one to ongly transplants for anterior replacement (Czochrowska, ther, the property of developing increased alveolar bone while ted root develops in areas of diminished alveolus provides a entive for transplantation in such edentulous areas. With the stem cell research and the progress being made in growing probable that tooth-like structures with the potential for im-ll begin replacing edentulous areas in the not too distant future , 2003; Bianco and Robey, 2001; Gronthos et al., 2002; Krebs-ey, 2002; Miura et al., 2003).
iple authors (Slagsvold and Bjercke, 1974; Andreasen, 1980a,b; nd Konisgberg, 1980; Andreasen and Kristerson, 1981a,b; ., 1983; Monsour and Adkins, 1983; Pogrel, 1987; Andreasen rowska et al., 2000; Tsukiboshi, 2001) have reported on the

Autogenic Dental Implants
significance of the care taken during the procedure. It is, in fact, the most critical aspect in the determination of success. Consequently, the practi-tioner who delivers the transplant should be carefully selected and well pre-pared. Generally it is suggested that the donor tooth be measured carefully so that the recipient site can be developed precisely. It often is instructive to construct a mock tooth by matching long-cone x-rays of the donor tooth. This can be used for trial insertion prior to extracting the donor tooth. This protocol is especially helpful in minimizing the amount of time that the transplant remains outside of the extraction socket. It is best to use a direct delivery method; i.e., remove the transplant and place it directly into the recipient site. This requires preparing the recipient site before the donor tooth is harvested. This procedure will allow for minimal desiccation of the periodontal membrane or dental follicle. Damage and contamination of the peripheral cells also are concerns if the transplant is placed somewhere other than in the socket. If the transplant cannot be placed immediately into the recipient site, it can be returned to the donor site or it could be placed into a culture medium (there are commercial receptacles such as Sav-a-tooth or ToothSaver for this circumstance).
The extraction should be carried out in a very delicate manner, carefully dissecting the surrounding bone so that no damage is done to the root sheath or its components. Sometimes, a more aggressive removal of surrounding bone must be performed so as to allow a coronal delivery with an intact follicle. An excellent discussion of surgical techniques is provided by Andreasen and colleagues (1990a). With more periodontists performing implants, they have become very adept in providing such a service. There-fore, it is a good idea to consider having a periodontist perform this pro-cedure. They often are more accustomed to the kind of care and attention to soft tissue necessary for successful treatment. They also are more likely to have a recall system conducive to monitoring transplant patients.
CASE ONE
Case 1 is useful in demonstrating a number of the relevant issues discussed here. The patient was missing two premolars in the upper left quadrant and could spare one from the lower left. At initial observation, the root length of the donor tooth was about one-third complete, so we waited for almost a year to allow for increased development. The follow-up photos demonstrate continued root elongation and a successful replacement that has provided 26 years of service to-date.
The best age for transplantation is determined by the stage of tooth development. Because it is desirable that the tooth experience revasculariza-tion, the best results are obtained well before the apex of the root closes. Andreasen first set the ideal time as that at three-quarter root completion
2

Northway
(Andreasen et al., 1970). Slagsvold and Bjercke (1974) discussed the other aspects of development that need to be taken into consideration when de-termining the best stage of development for transplantation. They included the number of roots (depending on which tooth is being transplanted) and the depth of the recipient site. Stressing that the root responds best when it is about 4 to 7 mm in length, they pointed out that the proximity of the maxillary sinus or the mandibular nerve might dictate moving up the time-table for performing the transplantation. It is worth noting that, as the apices of transplantable teeth are approaching apexification (typically about 18 years-of-age for third molars) and the opportunity for vital revasculariza-tion is waning, the appropriate age for implantation is at the time when facial and alveolar growth is coming to a halt. Of course, teeth can be trans-planted later than this, but these patients will require endodontic treatment after the periodontium has healed.
Monsour and Adkins (1983, 1984) performed experiments with beagle pups transplanting teeth at various stages of development and plac-ing them at different depths. Half of the teeth had just completed crown formation and the other half had differing amounts of root formation. Some were placed completely submerged, some partially erupted, and some in partial occlusion. The transplants that responded the best were those that had partially completed roots and were completely submerged. Trans-plants that were placed in occlusion simply did not survive (Andreasen 1981c). There was a gradient of success between these two extremes.
If the transplant survives the procedure well, there is an excellent chance that the root will continue to grow in length (Paulsen and Andrea-sen, 1998). This is obviously desirable in terms of functional support for the tooth. Slagsvold and Bjercke reported in 1974 that radiographs demon-strated a 1.3 mm (6%) reduction in root length. Andreasen reported that 14% of transplants experienced a total arrest of root development at the time of transplantation, 65% experienced a partial arrest, and 21% achieved full root development (Andreasen et al., 1990c).
CASE TWO
Case 2 demonstrates the ability of transplanted teeth to continue to grow and even to provide a viable canal that will allow endodontic treat-ment. It is regrettable that the perceived urgency of the impaction did not allow a bit more formation of the root. Teeth transplanted at a develop-mental stage too close to crown completion can have greater difficulty forming than those transplanted when root formation is at least half com-pleted. Another complicating factor in this case was the questionable quality of dental care prior to receiving the bridge and lapses in oral hygiene shortly
3

Autogenic Dental Implants
thereafter. Nevertheless, the patient continues to do well with a highly func-tional prosthesis.
Case 1. Intra-oral photos and panarex reveal agenesis of the upper right 2nd pre-molar and upper left 1st and 2nd premolars (Sept., 1977).
Case 1. (cont.). Mock tooth for trial insertion developed from long-cone x-rays. Records taken seven months after the lower left 2nd premolar was transplanted into the upper left premolar region (Jan., 1979).
4

Northway
Case 1 (cont.). Final records taken 3appliance wear (May, 1981).
Case 1 (cont.). Left: Periapical view takopment of the lamina dura, periodon(Oct., 1978). Middle. Periapical view development is complete and apex htaken 20 years later shows no signs of
As suggested above, this becom
4 months after transplant and 16 months of
Case 1 (cont.). Follow-up photostaken 20.5 years after transplantation(Feb., 1998).
en 4 months after transplant; note the devel-
tal space and continued growth of root length taken 4 years, 5 months after transplant; root as closed (Nov., 1982). Right. Periapical view failure (Feb., 1998).
es important because of the trade off in
5

Autogenic Dental Implants
systems. On one hand, the practitioner can be more assured of an in-creased root length by delaying the timing of transplantation, but prolonged delay can reduce the chances for a vital pulp. Once the tooth is transplant-ed, the vital components within the pulp chamber have the potential to be totally replaced through a process of revascularization. Initially the neuro-vascular components necrotize, but an infiltration of new capillaries marks
cell layers along the dentinal wall. As new dentin is formed, a regeneration
a revitalization of the pulp chamber during the first four weeks after trans-plantation (Andreasen and Kristerson, 1981c; Byers et al., 1992). This pro-gresses to a proliferation of mesenchymal cells and the laying down of new
6

Northway
Case 2. Left: Impacted second molar (Aug., 1964). Middle: third molar was trans-planted into the site of the extracted second molar (Sept., 1964). Right: The root begins to form on the transplanted third molar (Feb., 1965).
Case 2 (cont.). Left: There is continued root progress, but idiopathic aberration be-gins to form (July, 1965). Middle: Root formation continues (Feb., 1966). Right: Questionable care has resulted in the loss of the first molar (Sept., 1975).
Case 2 (cont.). Left: A bridge has been placed between the transplant and the second premolar (April, 1976). Middle: Patient presents with periodontal involvement of distal abutment/transplant (April, 1980). Right: The bridge is removed and endo-dontics performed (Feb., 1983).
Case 2 (cont.). Left: The bridge is replaced even though problems persist in the fur-cation area (Nov., 1983). Right: Lesions on the mesial and distal areas are abated, but the furcation area remains as a persistent problem area for this transplanted tooth that has provided service for 40 years (March, 1998). Case presented cour-tesy of Drs. L. Prosterman, L. Slapcoff and M. Moskovich.
7
Autogenic Dental Implants
of new, functioning nerve fibers can be seen. The apex can close off, form-ing a normal root ending. Endodontics typically is not required for these teeth.
Once a root approaches apical closure (stage 5, or when there is about four-fifths root completion), the potential for complete revasculariza-tion is compromised (Öhman, 1965; Paulsen and Andreasen, 1995). Irrep-arable necrosis places the tooth at risk for infection and rejection. It is
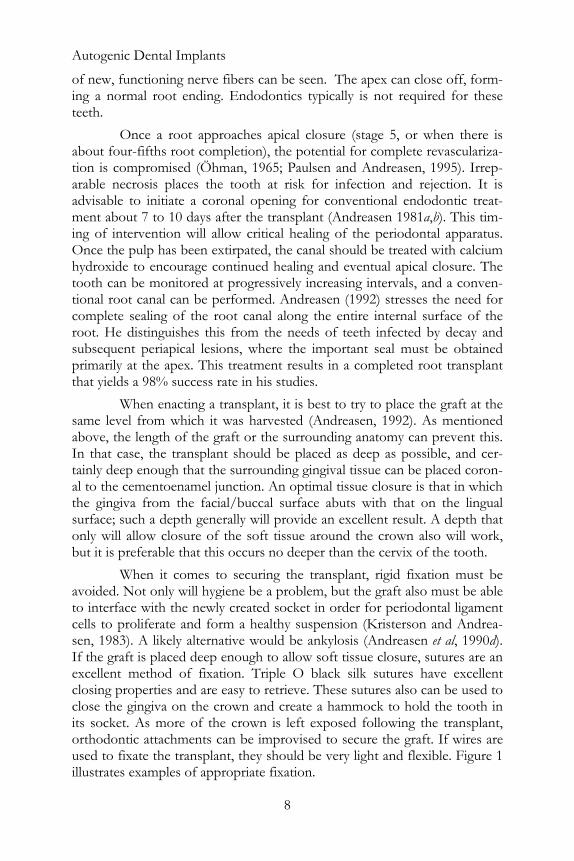
hydroxide to encourage continued healing and eventual apical closure. The tooth can be monitored at progressively increasing intervals, and a conven-tional root canal can be performed. Andreasen (1992) stresses the need for complete sealing of the root canal along the entire internal surface of the root. He distinguishes this from the needs of teeth infected by decay and subsequent periapical lesions, where the important seal must be obtained primarily at the apex. This treatment results in a completed root transplant that yields a 98% success rate in his studies.
as deep as possible, and cer-tainly de
erson and Andrea-sen, 198
advisable to initiate a coronal opening for conventional endodontic treat-ment about 7 to 10 days after the transplant (Andreasen 1981a,b). This tim-ing of intervention will allow critical healing of the periodontal apparatus. Once the pulp has been extirpated, the canal should be treated with calcium
When enacting a transplant, it is best to try to place the graft at the same level from which it was harvested (Andreasen, 1992). As mentioned above, the length of the graft or the surrounding anatomy can prevent this. In that case, the transplant should be placed
ep enough that the surrounding gingival tissue can be placed coron-al to the cementoenamel junction. An optimal tissue closure is that in which the gingiva from the facial/buccal surface abuts with that on the lingual surface; such a depth generally will provide an excellent result. A depth that only will allow closure of the soft tissue around the crown also will work, but it is preferable that this occurs no deeper than the cervix of the tooth.
When it comes to securing the transplant, rigid fixation must be avoided. Not only will hygiene be a problem, but the graft also must be able to interface with the newly created socket in order for periodontal ligament cells to proliferate and form a healthy suspension (Krist
3). A likely alternative would be ankylosis (Andreasen et al, 1990d). If the graft is placed deep enough to allow soft tissue closure, sutures are an excellent method of fixation. Triple O black silk sutures have excellent closing properties and are easy to retrieve. These sutures also can be used to close the gingiva on the crown and create a hammock to hold the tooth in its socket. As more of the crown is left exposed following the transplant, orthodontic attachments can be improvised to secure the graft. If wires are used to fixate the transplant, they should be very light and flexible. Figure 1 illustrates examples of appropriate fixation.
8

Northway
Figure 1. Recommended methods of fixation following transplantation. Left: Black silk suture material. Right: Wire bonded to adjacent teeth with bent frame to sup-port tooth (transplant has been bonded with Histocryl™).
Figure 1 (cont.). Left: Orthodontic attachments that will be stabilized with very re-silient wire. Right: Hammock soldered to a band on an adjacent tooth. If they are connected to the transplant as on the left, the connection should be made with very resilient wire and maintained for only 10-14 days.
The prognosis for a transplant is improved considerably if areas of infection are avoided during the placement of the transplant or if efforts are taken to heal the region prior to transplantation (Pogrel, 1987). Even so, the patient should be placed on a full regimen of antibiotics beginning about two days prior to the procedure (Andreasen, 1992). Andreasen suggests that there is a possibility of arrested revascularization if the graft becomes infected, and lists as possible sources of contamination extra-oral handling or exposure to bacteria from the saliva or the coagulum. Again, it bears re-peating that tportant factors relating to the success of the procedure.
he care exercised during transplantation is one of the most im-
Once a transplant has healed and sufficient time has been allowed for revascularization to take place (about 3 to 4 months), there is a brief period (approximately 6 to 9 months) during which the transplant will toler-ate orthodontic tooth movement (Paulsen and Andreasen, 1995). Heavy and prolonged forces should be avoided, as should eccentric tooth move-ments. The skills that have been developed for implantation should be im-plemented in planning cases that involve transplants. Effort should be made to place the transplant near its ultimately prescribed position so that mini-mal movement will be required to fine tune the placement of the tooth.
9

Autogenic Dental Implants
Another area in which the science of implants bears similar insight into that of transplantation is the concept of space; i.e., having enough room to be able to accommodate a transplant. As with the creation of a socket for the delivery of an implant, care must be taken to avoid the adja-cent root structures by at least 1 to 2 mm when preparing the recipient site for a transplant. It also is helpful to have about 0.5 to 1 mm of bone both labial and lingual to the transplant graft. Andreasen (1992) reported on cases that demonstrate the removal and replantation of the labial plate of bone to accommodate the placement of the graft into a compromised alve-olus. Between the osteogenic potential of the transplanted root surface and the remarkable healing potential of autogenous bone, these grafts work with incredible success. Such transplant cases, as presented by Scandinavian sur-geons, profoundly challenge the esthetic potential of today’s finest implants. To this extent, proficiency with the procedure could well force a new para-digm in the realm of esthetic replacem nt of anterior teeth. The esthetic
ow will they look as our patients enter their geriatric years? One of the more recently perceived benefits of autogenic trans-
plants is the aforementioned osteogenic potential (Czochrowska et al., 2000). As the root develops its full potential length, alveolar bone can deve-lop in the vicinity. If the tooth is erupting, the alveolus is brought along. If the root is growing away from the plane of occlusion, e.g., growing into the maxillary sinus, the depth of the alveolar bone is increased. Considering this new potential, transplants might well be considered the treatment of choice in cases where grafting is a likelihood especially when the encroachment of the maxillary sinus yields a limited alveolar dimension. Even if the trans-plant fails, it might be considered useful in the development of the site for an eventual implant. Particularly when considering the appropriateness of age in planning either an implant or a transplant, a transplant might buy time for the eventual placement of an implant once alveolar growth is completed.
CASE 3
In case 3, the conditions of oligodontia, microdontia and severely
vertical augmentation of the alveolus, especially on the left side where ankylosis was causing an intrusion of the premolar region. With transplants, the final result was one that allowed easy restoration, but the
e s of a restored biological root―that which is left when a premolar is used to replace an incisor―has far more esthetic potential than most implants, and we only have knowledge of the esthetic quality of implants for their first 15 to 20 years. H
,
inadequate depth of alveolus were present. While the case was presented and treatment started in 1977 (before osseointegration was an accepted phenomenon in North America), it would be a challenge even today. Numerous grafts would have been required, lifting the maxillary sinus and attempting a
10

Northway
significance of this case lies in the vertical increase in alveolar bone in the region of the developing transplant.
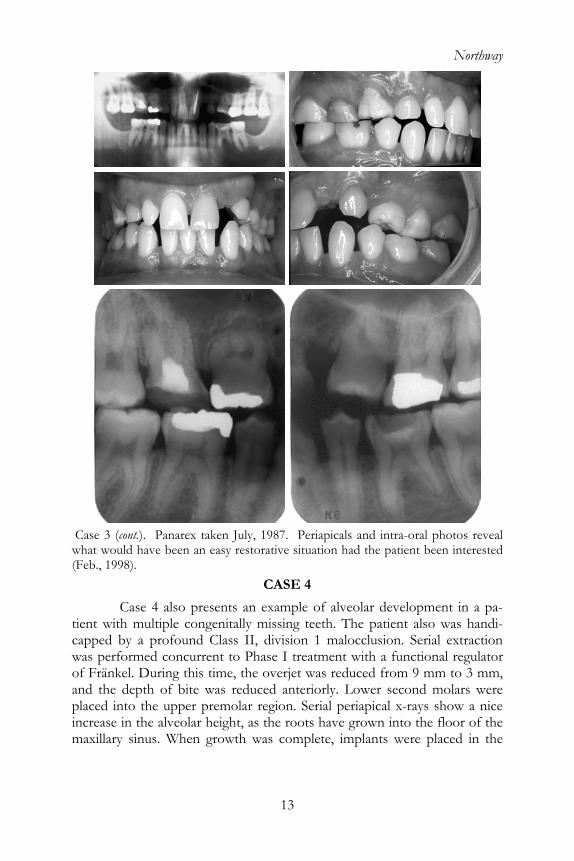
Case 3. Intra-oral photos and panarex showing Class II, division 1 malocclusion with spacing due to microdontia and oligodontia―congenital absence of 10 teeth (Feb., 1977). Complicating the case is the minimal alveolus in the maxillary pre-molar regions.
Case 3 (cont.). Photos and panarex following transplantation of the lower right 3rd molar into the upper right premolar region (June, 1978). Notice the relative intru-sion (worsening condition due to ankylosis) of the upper left primary molars. Lower Right: Photo shows the floor of the maxillary sinus during the second transplant (Aug., 1978).
11

Autogenic Dental Implants
Case 3 (cont.). Left: Lower left third molar flush against the inferior membrane of the maxillary sinus. Right: Adequate surrounding gingiva allows for soft tissue closure.
Case 3 (cont.). Periapicals and intraoral photos show continued growth of the third molars, initial formation of the furcation,alveolus (Sept., 1979). Note that no ave been placed on the developing 3rd mola
and increased vertical development of the brackets h
rs.
Case 3 (cont.). Periapicals taken at the final appointment. Apices have closed and the elevation in the floor of the sinus is visible (Oct. 1981).
12
Northway
Case 3 (cont.). Panarex taken July, 1987. Pwhat would have been an easy restorative si(Feb., 1998).
CASE
Case 4 also presents an exampltient with multiple congenitally missingcapped by a profound Class II, divisiowas performed concurrent to Phase I trof Fränkel. During this time, the overjet
the depth of bite was reduced tand anplaced into the upper premolar region. increase in the alveolar height, as the roomaxillary sinus. When growth was com
13
eriapicals and intra-oral photos reveal
tuation had the patient been interested
4
e of alveolar development in a pa- teeth. The patient also was handi-n 1 malocclusion. Serial extraction eatment with a functional regulator was reduced from 9 mm to 3 mm, eriorly. Lower second molars were
Serial periapical x-rays show a nice ts have grown into the floor of the plete, implants were placed in the
Autogenic Dental Implants
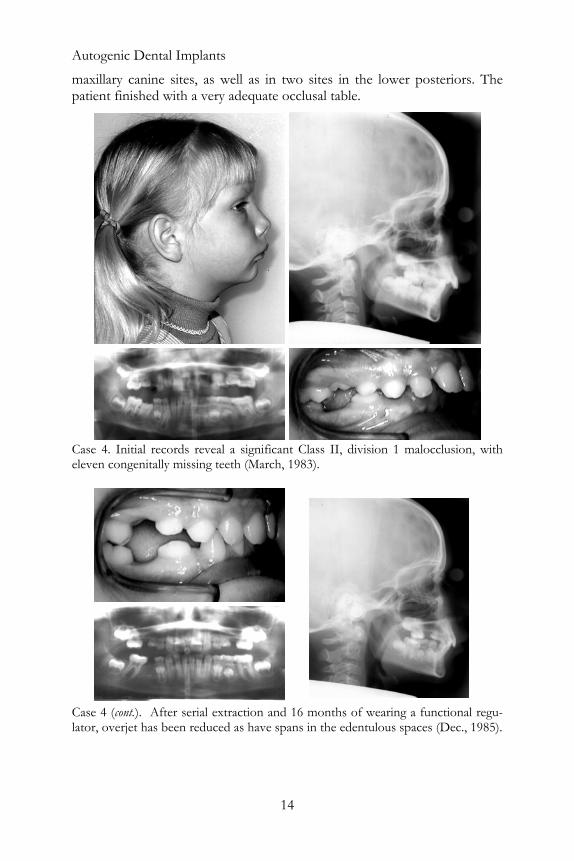
maxillary canine sites, as well as in two sites in the lower posteriors. The patient finished with a very adequate occlusal table.
Case 4. Initial records reveal a significant Class II, division 1 malocclusion, with eleven congenitally missing teeth (March, 1983).
Case 4 (cont.). After serial extraction and 16 months of wearing a functional regu-lator, overjet has been reduced as have spans in the edentulous spaces (Dec., 1985).
14

Northway
Case 4 (cont.). Top: Periapical taken at transplantation of the lower left second molar into the upper left premolar site (March, 1987). Bottom: Bilateral periapicals taken at transplantation of lower right second molar into the upper right premolar region (May, 1987).
Case 4 (cont.). Upper: Roots begin to grow into maxillary sinus (Aug., 1987). Lower: Apexification is nearly complete; alveolar depth has increased as the roots have grown into the maxillary sinus (Oct., 1989).
15
Autogenic Dental Implants
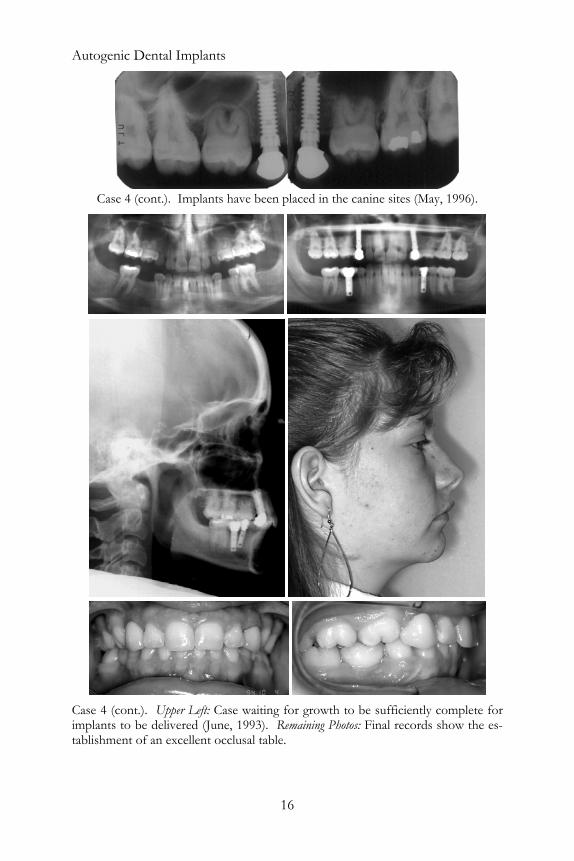
Case 4 (cont.). Implants have been placed in the canine sites (May, 1996).
Case 4 (cont.). Upper Left: Case waiting for growth to be sufficiently complete for implants to be delivered (June, 1993). Remaining Photos: Final records show the es-tablishment of an excellent occlusal table.
16
Northway
Cases presented by Andreasen and Zachrisson, and by Hans Paul-sen in his chapter in this monograph, in which transplanted premolars have been used to replace missing maxillary incisors, demonstrate a development of interproximal gingival papillae and gingival contours that is not currently predictably possible when using implants (Andreasen, 1992; Czochrowska et al., 2000; 2002a,b,c). The cases shown reveal tissues that were judged to be normal or slightly hyperplastic, making them a superior treatment alter-native to implants when replacing maxillary anteriors. When it is considered that we are not far from being able to culture stem cells that will allow the creation of dentin specific to an individual patient, and that we will be able to develop that tissue into a scaffolding that will take on the form of the root that we wish to replace, it becomes even more regrettable that we in North America are not actively developing the techniques and skill to pre-dictably deliver transplants.
One of the difficult aspects of transplants is case selection limita-tion due to inadequate donor teeth. The inadvertent use of a premolar may cause a drain on anchorage in terms of providing a full facial profile. When one considers the esthetic benefits of premolars used to replace maxillary incisors, especially in the aftermath of a traumatic episode and resultant compromised alveolar width, we gain a new appreciation for the concept of intentional loss of anchorage (protraction) to support facial profile.
CASE
Case 5 provides an excellent ex -plants to turn a potential loss into a re r second premolars. His significant Cla h deep bite, 6 mm overjet, and the roll and entrapment of his lower lip pro-
e a situation that would render a di lapse in facial fullness if we were to simply remove the four primary molars and close the spaces through conventional orthodontics.
Instead, a functional appliance was used to facilitate the eruption of the lower posterior teeth, while encouraging a shift in his dentition that re-sulted in an excellent overbite and overjet relationship. Use of this appliance simultaneously protected the third molars from the heavy occlusion that was transplanted into the lower second premolar sites and improved space closure potential. An excellent improvement in facial profile was attained in
5
ample of the beneficial use of transal gain. The patient is missing fouss II, division 2 malocclusion, wit
sastrous colvid
a case that otherwise was highly prone to labial inversion.
17
Autogenic Dental Implants
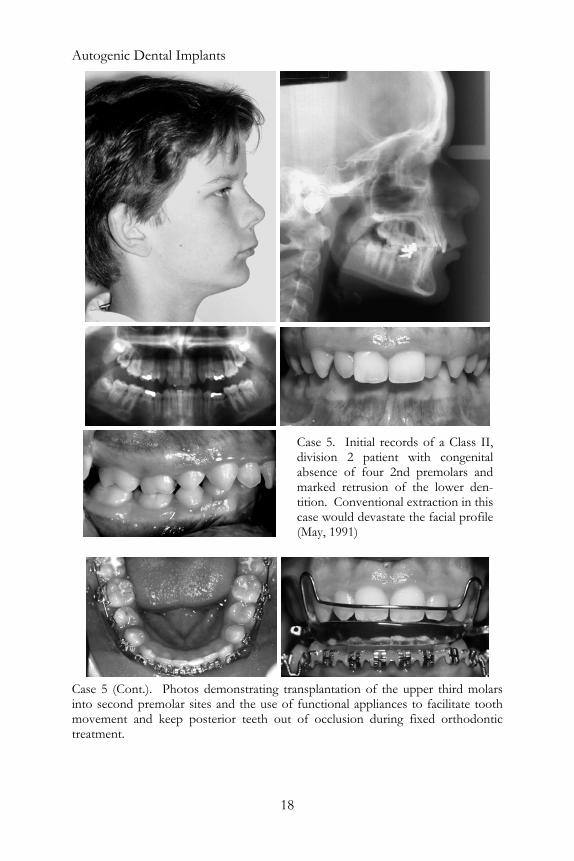
Case 5 (Cont.). Photos demonstrating transplantation of the upper third molars into second premolar sites and the use of functional appliances to facilitate tooth movement and keep posterior teeth out of occlusion during fixed orthodontic treatment.
Case 5. Initial records of a Class II,division 2 patient with congenitalabsence of four 2nd premolars andmarked retrusion of the lower den-tition. Conventional extraction in thiscase would devastate the facial profile(May, 1991)
18
Northway
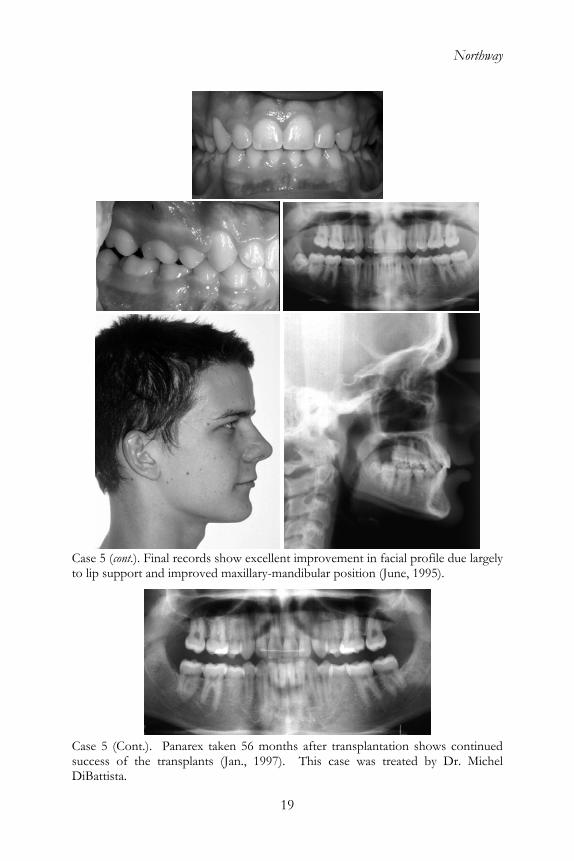
Case 5 (cont.). Final records show excellent improvement in facial profile due largely to lip support and improved maxillary-mandibular position (June, 1995).
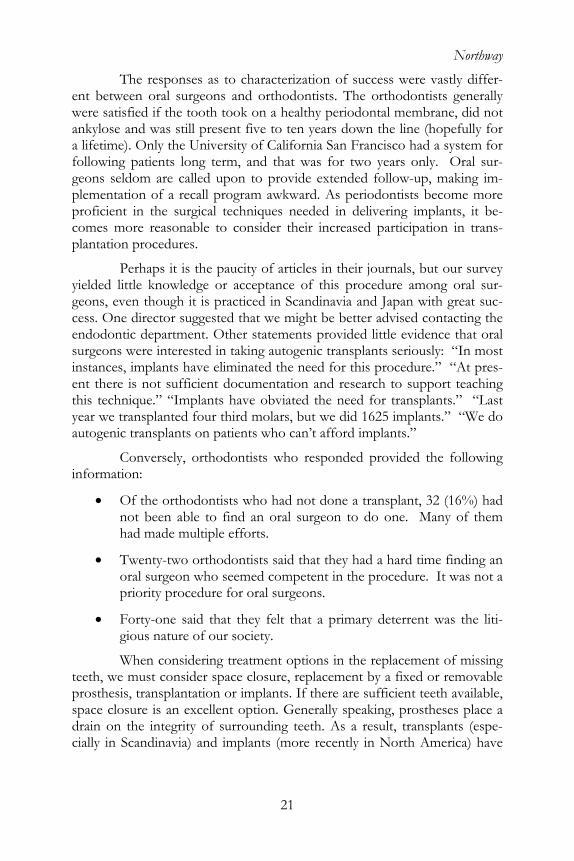
Case 5 (Cont.). Panarex taken 56 months after transplantation shows continued
Michel success of the transplants (Jan., 1997). This case was treated by Dr.DiBattista.
19

Autogenic Dental Implants
THE SURVEYS
All members of the Edward H. Angle Society of Orthodontists were sur-veyed, as were each of the departmental chairpersons of all of the American departments of oral surgery. The response rate among Angle orthodontists was 65.5% and 46.6% for surgical chairs. Of the respondents 20.9% of the orthodontists had been involved in a transplant case, while 47.9% of the oral surgeons had transplanted a tooth. As Figure 2 shows, those orthodon-tists who had been involved in more than four transplant cases experienced about a 90% success rate, while those who had been involved in fewer had a generally lower success rate. Figure 3 shows that the rate of success did not appear to be correlated to experience among oral surgeons. Nine of the responding 48 departments nation-wide teach autogenic transplantation of teeth, with about 45 being performed by oral surgery residents annually (15 to 20 of those are being carried out at the University of California San Francisco).
Figure 2. Success related to experience for orthodontists
Figure 3. Success related to experience for oral surgeons
20
Northway
The responses as to characterization of success were vastly differ-ent between oral surgeons and orthodontists. The orthodontists generally wer , did not ank fully for a liffollowing patients long term, and that was for two geons seldom are called upon to provide extended follow-up, making im-plemprofic ering implants, it be-complan
yielgeons n with great suc-cessendodontic department. Other statements provided little evidence that oral surgeons were interested in taking autogenic transplants seriously: “In most instent there is not sufficient documentation and research to support teaching thisyearautog implants.”
inform
• ad not done a transplant, 32 (16%) had
•
e satisfied if the tooth took on a healthy periodontal membraneylose and was still present five to ten years down the line (hopeetime). Only the University of California San Francisco had a system for
years only. Oral sur-
entation of a recall program awkward. As periodontists become more ient in the surgical techniques needed in deliv
es more reasonable to consider their increased participation in trans-tation procedures.
Perhaps it is the paucity of articles in their journals, but our survey ded little knowledge or acceptance of this procedure among oral sur-
, even though it is practiced in Scandinavia and Japa. One director suggested that we might be better advised contacting the
ances, implants have eliminated the need for this procedure.” “At pres-
technique.” “Implants have obviated the need for transplants.” “Last we transplanted four third molars, but we did 1625 implants.” “We do
enic transplants on patients who can’t afford
Conversely, orthodontists who responded provided the following ation:
Of the orthodontists who hnot been able to find an oral surgeon to do one. Many of them had made multiple efforts.
• Twenty-two orthodontists said that they had a hard time finding an oral surgeon who seemed competent in the procedure. It was not a priority procedure for oral surgeons.
Forty-one said that they felt that a primary deterrent was the liti-gious nature of our society.
When considering treatment options in the replacement of missing teeth, we must consider space closure, replacement by a fixed or removable prosthesis, transplantation or implants. If there are sufficient teeth available, space closure is an excellent option. Generally speaking, prostheses place a drain on the integrity of surrounding teeth. As a result, transplants (espe-cially in Scandinavia) and implants (more recently in North America) have
21

Autogenic Dental Implants
gained favor during the last two decades. A fair comparison of these two options must take into consideration the following:
• Transplants generally cost a fraction of the cost of implants.
• Transplants are a biological solution, whereas implants are an arti-ficial one.
• Transplants (for the time being) rely upon the availability of donor teeth, while implants can be purchased easily.
• Transplants can grow alveolar bone and even interdental papillae during eruption, while implants do not erupt and, therefore, cannot.
• The age for effecting a vital transplant is dissipating at the same time that one can provide, for the first time, an implant.
• Transplants can be moved, while implants cannot and make excellent anchor units.
• Transplants often do not require a prosthetic completion, while im-
ave excellent prognoses, but there are some patients (especially th
ioengineering, transplants will gain dominance, especially for the replacement of teeth with v ins. In the meantime, it is regrettable that the oral surgery community not better preparing them-
hopl transplants can provide a superior
lishcon at the future might hold, it is hard
If, tran nsider the dilemma present-
plants do.
• Transplants are susceptible to caries, but implants have been shown to be prone to new-tech hygiene problems.
• Both hose involving the replacement of maxillary anterior teeth) in whom
the potential for soft tissue improvement profoundly tips the advan-tage scale toward transplants.
When the time arrives that we can generate root-like structures through b
isible gingival margis
selves for proficiency in this technique-sensitive dental procedure. It is our e that this will change.
In summary, autogenic dentaform of tooth replacement. The longevity of this treatment is well estab-
ed, especially when the surgery is accomplished with care. When we sider the potential, not to mention wh
to comprehend why more transplants are not being done in North America. for example, your appreciation has not yet developed for the need of splantation as a treatment option, please co
ed in Case 6. The lower left second molar is impacted, probably ankylosed.
22

Northway
Case 6. Left: Panarex showing impaction of the lower right second molar. How do you treat this condition? Do you allow your oral surgeon to remove all four third
ars? Right: Panarex taken after two years of trying to elevate the tooth that ed out to be ankylosed. If a transplant might have worked, there are now
molturn no
moplaced? Do not let it happen that the potential donor teeth are absent when
03.
ncisors in monkeys. Int J Oral Surg 1981;10:54-61.
donor teeth.
Are you going to allow your oral surgeon to remove all four third lars at the time that the second molar is exposed and an attachment is
it is decided that the tooth is never going to erupt and behave in a healthy fashion.
REFERENCES
Ahlberg K, Bystedt H, Eliasson S, Odenrick L. Long-term evaluation of autotransplanted maxillary canines with completed root formation. Acta Odontol Scan 1983;1:23-31.
Andreasen JO. A time-related study of periodontal healing and root resorp-tion activity after replantation of mature permanent incisors in mon-keys. Swed Dent J 1980a;4:101-110.
Andreasen JO. Delayed replantation after submucosal storage in order to prevent root resorption after replantation: An experimental study in monkeys. Int J Oral Surg 1980b;9:394-4
Andreasen JO. Periodontal healing after replantation and autotransplan-tation of i
23

Autogenic Dental Implants
Andreasen JO. Relationship between cell damage in the periodontal liga-ment after replantation and subsequent development of root resorption in monkeys. Acta Odont Scand 1981e;39:15-25.
Andreasen JO. The effect of excessive occlusal trauma upon periodontal
Andreasen JO. Atlas of Replantation and Transplantation of Teeth. W.B.
And;78:
Andntation of perma-
AndPeriodontal healing after replantation of mature
Andtial PDL substitutes during experi-
Andterm study of 370 autotransplanted premolars. Part I. Surgical
And g-term study
Andreasen JO, Paulsen HU, Yu Z, Bayer T. A long-term study of 370 auto-
o
Batouli S, Miura M, Brahim J, Tsutsui TW, Fisher LW, Gronthos S, Robey
Bian Robey PG. Stem cells in tissue engineering, Nature 2001;1:414: 118-121.
healing after replantation of mature permanent incisors in monkeys. Swedish Dent J 1981f;5:115-122.
Saunders Co., Harcourt Brace Jovanovich Inc. Philadelphia, 1992. reasen JO, Hjorting-Hansen E, Jolst O. A clinical and radiographic study of 76 autotransplanted third molars. Scand J Dent Res 1970512-523. reasen JO, Kristerson L. Effect of extra-alveolar period and storage media on periodontal and pulpal healing after replanent incisors in monkeys. Int J Oral Surg 1981a;10:43-53. reasen JO, Kristerson L. Effect of limited drying or removal of the periodontal ligament. incisors in monkeys. Acta Odont Scand 1981b;39:1-13. reasen JO, Kristerson L. Evaluation of different types of autotrans-planted connective tissues as potenmental replantations in monkeys. Int J Oral Surg 1981c;10:189-201. reasen JO, Paulsen HU, Yu Z, Ahlquist R, Bayer T, Schwartz O. A long-procedures and standardized techniques for monitoring healing. Eur J Orthod 1990a;12:3-13. reasen JO, Paulsen HU, Yu Z, Bayer T, Schwartz O. A lonof 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur J Orthod 1990b;12:14-24.
transplanted premolars. Part III. Root development subsequent to transplantation. Eur J Orthod 1990c;12:25-37.
Andreasen JO, Paulsen HU, Yu Z, Schwartz O. A long-term study of 370 autotransplanted premolars. Part IV. Periodontal healing subsequent ttransplantation. Eur J Orthod 1990d;12:38-50.
PG, Shi S. Comparison of stem-cell-mediated osteogenesis and dentin-ogenesis. J Dent Res 2003;82:976-981. co P,
24

Northway
Byers M, Kvinnsland I, Bothwell M. Analysis of low affinity nerve growth factor receptor during pulpal healing and regeneration of myelinated and unmyelinated axons in replanted teeth. J Comp Neurol 1992; 326:470-484.
Czochrowska EM, Semb G, Stenvik A. Nonprosthodontic management of alveolar clefts with 2 incisors missing on the cleft side: A report of 5 patients. Am J Orthod Dentofac Orthop 2002a;122:587-592.
ace maxillary incisors: a comparison with
Czoation: Survival and success rates 17-41 years post-treatment,
Czo come of
Krebsbach PH, Robey P. Dental and skeletal stem cells: Potential cellular therapeutics for craniofacial regeneration. J Dent Educ 2002;66:766-773.
Kristerson L, Andreasen JO. The effect of splinting upon periodontal pul-pal healing after autotransplantation of mature and immature perma-nent incisors in monkeys. Int J Oral Surg 983;12:239-249.
Miura M, Gronthos S, Zhao M, Lu B, Fisher LW, Robey PG, Shi S. SHED: Stem cells from human exfoliated deciduous teeth. Proc Nat’l Acad Sci USA 2003;100:5807-5812.
Monsour F, Adkins K.. A Radiographic Assessment of Autologous Tooth Transplants in Dogs. J Oral Max Surg 1983;41:377-384.
Monsour F, Adkins K.. Responses of periodontal tissues and cementum following transplantation of teeth. J Oral Max. Surg 1984;42:441-446.
Northway W, Konisgberg S. Autogenic tooth transplants: The state of the art. Am J Orthod 1980;77:146-62.
Öhman A. Healing and sensitivity to pain in young replanted human teeth. An experimental and histological study. Odontol Tlidskr 1965;73:168-227.
Czochrowska EM, Stenvik A, Album B, Zachrisson BU. Autotransplan-tation of premolars to replnatural incisors. Am J Orthod Dentofac Orthop 2000;118:592-600.chrowska EM, Stenvik A, Bjercke B, Zachrisson BU. Outcome of tooth transplantAm J Orthod Dentofac Orthop 2002b;121:110-119. chrowska EM, Stenvik A, Zachrisson BU. The esthetic outautotransplanted premolars replacing maxillary incisors. Dent Trauma-tol 2002c;18:237-245.
Gronthos S, Brahim J, Li W, Fisher LW, Cherman N, Boyde A, DenBesten P, Robey PG, Shi S. Stem cell properties of human dental pulp stem cells. J Dent Res 2002;81:531-535.
25

Autogenic Dental Implants
26
Paulsen H, Andreasen J. Pulp and periodontal healing, root development and root resorption subsequent to transpalatal and orthodontic rota-tion: A long-term study of autotransplanted premolars. Am J Orthod Dentofac Orthop 1995;108; 630-640.
Paulsen H, Andreasen J. Eruption of premolars subsequent to autotrans-plantation. A longitudinal radiographic study. Eur J Orthod 1998;20:45-55.
Pogrel M. Evaluation of over 400 autogenous tooth transplants. J. Oral Max Surg 1987;45:205-211.
Slagsvold O, Bjercke B. Autotransplantation of premolars with partly form-ed roots: A radiographic study of root growth. Am J Orthod 1974;66: 355-366.
Slagsvold O, Bjercke B. Applicability of autotransplantation in cases of missing upper anterior teeth. Am J Orthod 1978a;74:410-421.
Slagsvold O, Bjercke B. Indications for autotransplantation in cases of missing premolars. Am J Orthod 1978b;74:241-257.
Tsukiboshi M. Autotransplantation of Teeth, Quintessence Pub. Co., Chi-cago,2001