Michael J. Sileo, MD, FAAOS - St Charles › sites › default... · Loose bodies Benign...
52
Michael J. Sileo, MD, FAAOS Sports Medicine Injuries Arthroscopic Shoulder, Knee & Hip Surgery December 7, 2018
Transcript of Michael J. Sileo, MD, FAAOS - St Charles › sites › default... · Loose bodies Benign...

Michael J. Sileo, MD, FAAOSSports Medicine Injuries
Arthroscopic Shoulder, Knee & Hip SurgeryDecember 7, 2018

NONE

Groin and hip pain is common in athletes Especially hockey, soccer, and
football 5% of all soccer injuries
Renstrom et al: Br J Sports Med 1980.
Complex anatomy and wide differential diagnoses that span multiple medical specialties make diagnosis difficult

Snapping hip Trochanteric bursitis Abductor tears Compression neuropathies LFCN (meralgia
paresthetica) Sciatic nerve (Piriformis
syndrome) Ilioinguinal,
iliohypogastric, or genitofemoral nerve
Muscle strain Adductor Iliopsoas Gluteus medius Hamstrings Gracilis
Avulsion injuries Sports Hernia Osteitis Pubis
• Extra-articular causes:

Intra-articular causes: Labral pathology Femoroacetabular impingement Chondral pathology Ligamentum teres injury Loose bodies Benign Intra-articular tumors PVNS Synovial chondromatosis
Capsular laxity Stress fracture Septic arthritis Adhesive capsulitis Osteonecrosis SCFE Transient synovitis

Soft-tissue injuries such as muscle strains and contusions are the most common causes of hip pain in the athlete
It is important to be aware and suspicious of intra-articular causes of hip pain
Up to 60% of athletes undergoing arthroscopy are initially misdiagnosed
Delay to diagnosis is typically 7 months Labral pathology may not be diagnosed for up to 21
monthsByrd et al: Clin Sports Med 2001.
Burnett et al: JBJS 2006.

Nature of discomfort Mechanical symptoms Stiffness Weakness Instability
Location of discomfort Onset of symptoms History of any trauma or developmental
abnormality

Assess gait, posture, limb-length inequality, and scoliosis
Complete neurovascular examination Active and passive hip range of motion Palpation for focal tenderness
Rare with intra-articular pathology

Full Lumbar spine, neuro exam!
“C-sign”: Hand cupped above
greater trochanter with thumb over posterior aspect of trochanter and fingers gripping into groin
Suggests intra-articular pathology

Log rolling: Pain suggests intra-articular pathology

Resisted Straight Leg Raise test (Stinchfield) Pain suggests intra-articular pathology

Thomas test: Hip flexion contracture

Patrick’s Test (FABER): Posterior pain suggests SI joint pathology Anterior pain suggests anterior capsule, labrum, or psoas
pathology

Anterosuperior Impingement Test (FADIR/Ganz): Hip is flexed, adducted,
and internally rotated Pain with most intra-
articular pathology Associated click may be
present Not specific for labral
pathology
Ganz: CORR 2003.


Fibrocartilaginous rim that overlies the articular cartilage and surrounds the perimeter of the acetabulum
Triangular in cross section Widest anteriorly and
superiorly; thickest superiorly
Bharam: Clin Sports Med 2006.

Contains free nerve endings May explain pain and decreased
proprioception
McCarthy: J Arthroplasty 2001.Kelly et al: Arthroscopy 2005.

Deepens acetabulum by approximately 21% Creates a seal of the hip joint
Maintains hydrostatic pressure enhancing lubrication Maintains negative pressure enhancing stability
Reinforces acetabular rim Contributes to containment of femoral head at extremes of motion Contributes to joint stability
Does NOT significantly participate in load transmission
Ferguson et al: J Biomech 2001
Presenter
Presentation Notes
Reasons to preserve labrum

Trauma Injury or fall MVA Dislocation
Muscle weakness/imbalance FAI
Femoroacetabular impingement

Subtle osseous morphologic abnormalities result in abnormal contact between the femoral neck/head and the acetabular margin during terminal motion of the hip
Parvizi et al: JAAOS 2007.



Repetitive abnormal contact leads to labral and chondral damage
Continued progression leads to premature degenerative arthritis
Acetabular labral tears are frequently the manifestation of primary structural hip disease

Legg-Calve-Perthes disease Congenital hip dysplasia Slipped capital femoral ephiphysis Avascular necrosis Malunited fractures (acetabulum or femoral neck) Prior periacetabular or proximal femoral osteotomy Retroverted acetabulum Most patients lack a clear history for any predisposing
conditions
Parvizi et al: JAAOS 2007.

Patients typically 25-40 years of age Mean delay in diagnosis: 7-21 months Groin pain is most common complaint
Anterior groin: 92% Lateral hip: 59% Deep within the buttocks: 38%
Worse with activity, especially repetitive twisting and pivoting motions Pain with prolonged hip flexion (sitting) Pain with rising from a seated position
McCarthy et al: CORR 2003.Burnett et al: JBJS 2006.
Byrd: ICL 2007.

AP Pelvis Acetabular
Characteristics: Center edge angle Acetabular inclination Acetabular version Crossover sign
Presence of Osteoarthritis
Femoral Characteristics: Head sphericity Head-neck offset Neck-shaft angle Trochanteric height

Dunn lateral Obtained in 90° flexion
and 20° abduction Useful for evaluating: Femoral head-neck
junction Femoral head sphericity Alpha angle Congruency

Normal acetabular labrum has uniformly low signal intensity and a sharp triangular morphology
Sofka et al: Op Tech Sport Med 2007.

Sensitivity increased compared to MRI, but false-positive rate also increases Sensitivity: 57-95% Specificity: 75% False-Positive rate: 20%
Byrd et al: AJSM 2004.
Burnett et al: JBJS 2006.

Radiologically-guided intra-articular local anesthetic injections (easily performed in conjunction with MR arthrography) are useful to assess whether pain is intra-articular
**Transient pain relief is a 90% reliable indication of intra-articular pathology
Byrd et al: AJSM 2004.

Initial trial of non-surgical treatment Activity modification including restriction of athletic
activities NSAIDs Usually fails to control the symptoms
In an attempt to prevent progression of arthritis, surgery is recommended if non-surgical treatment fails
Fitzgerald: CORR 1995.Byrd: Arthroscopy 1996.
Kelly et al: Arthroscopy 2005



Post





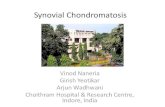
LABRAL TEAR LABRAL REPAIR



52 patients underwent arthroscopic labral repair Mean follow-up: 9 months – overall improvement in HHS Long term follow up needed
Hines et al: Arthroscopy 2007.

158 patients underwent arthroscopic surgery for FAI 50% pain resolution by 3 months 95% pain resolution by 1 year
Sampson: Tech Orthop 2005.

45 professional athletes with FAI 49% Cam lesions 7% Pincer lesions 44% Combined Cam and Pincer
42 athletes (93%) returned to professional competition 3 athletes who did not return to play all had diffuse
osteoarthritis 35 athletes (78%) remain active in professional
sport at an average follow-up of 1.6 years
Philippon et al: KSSTA 2007.

100 hips (mean age 34.7 years) with FAI treated with arthroscopic management
Follow-up at mean 9.9 months 75% good/excellent results 3 patients required total hip arthroplasty
All had grade 4 chondral injuries > 2 cm on acetabulum
Larson et al: Arthroscopy 2008.

Long term studies are needed to see if alteration in the natural progression to osteoarthritis and sustained pain relief can be achieved with arthroscopic management of FAI

CPM immediately post op 30-70 deg hip flexion (debateable)
Immediate PWB with crutches x 2-4 weeks Start PT immediately for AA/PROM, Strengthening

Indocin 75 mg PO daily 10-14 days Decreased incidence of HO
Baby ASA, chemical DVT prophylaxis Patients with previous history of DVT OCPs
Minimization of hip flexor inflammation

Labral repair/Osteoplasty/Chondroplasty Flexion 0-90, abd 0-25, ER 0-25 x 2 weeks (avoid labral stress) CPM x 4 weeks (4 hours/day) Isometrics/Core Advanced strengthening once FWB 3-6weeks Single leg stance Advanced bridging Single knee bends Sidestepping w/ resistance
Stalzer et al., Operative Tech Orthopaedics, 2005

Acetabular labral tears are a common cause of hip pain.
Acetabular labral tears rarely occur as isolated pathology.
FAI is a common cause of acetabular labral tears in the athlete.

To optimize results, surgical treatment should address not only the acetabular labral tear, but also the associated pathology Chonral injury Underlying impingement
Long-term studies are needed to see if these results are durable and delay or prevent the onset of osteoarthritis.