
Metal Ions – A Scientifi c Review Introduction...
12
1 have experienced a resurgence of popularity in recent times. This is due mainly to a significant number of long-term clinical studies highlighting the remarkably low wear rates of metal-on-metal bearings implanted over the past 40 years. 1-4 Clinical complications with the early generation components usually were related to manufacturing issues such as, improper tolerances and poor design. 5 Recent advancements in manufacturing technology have enabled more precise tolerances, surface finish, and designs that provide an increased range of motion (Figure 1). Documented clinical success with modern devices has led to the FDA granting market approval to some orthopedic companies in the US. 6,7 Introduction M Metal Ions – A Scientific Review Metal-on-metal is particularly attractive in the total hip not only due to the ultra-low wear exhibited in numerous clinical and simulator studies 1–8 (Figure 2), but also due to the flexibility afforded by designs based on the properties of cobalt chromium alloy. This flexibility enables the use of large diameter heads in a variety of acetabular configurations. Larger metal-on-metal femoral heads can provide increased range-of-motion and stability, as well as increased resistance to dislocation. 9-12 The incorporation of larger diameter femoral heads into ceramic and polyethylene bearings presents design challenges due to impingement concerns with ceramics, and increased brittleness with thin polyethylene liners, all leading to an increased risk of mechanical fracture. 13,14 Metal-on-metal components do not pose a risk of mechanical fracture. Current metal-on-metal designs allow the use of the larger 38mm heads in acetabular component sizes as small as 46mm. Despite its lengthy and positive clinical history, there have been concerns expressed regarding the long-term biological consequences of metal-on- metal wear debris, particularly the release of cobalt and chromium ions into the body. Questions about metal ions and their biological effects are not new. Many studies have been conducted over past decades. All have failed to establish a causal link between ion release, and cancer or other negative systemic effects. 15–22 As with each bearing surface, certain unknowns still exist, and in recent times, fueled by rumors and misinformation about the metal ions, the debate lingers on. Following are five reasons why many leading researchers consider the metal ion debate to be inconsequential. Metal-on-metal has exhibited ultra-low wear rates not only in simulator studies, but also through published in-vivo wear studies as shown in the in-vivo wear comparison above. Radial Clearance µm Sphericity = 10 µm Surface Finish Ra = 1 µm 120 – 500 10 – 20 .1 – 1 25 – 75 <5 <.005 Early Modern Early MOM Head Recent MOM Head 140 120 100 80 60 40 20 0 Poly (Head 44 ) ArCom ® (Head 44 ) HXLP (Oonishi 45 ) COC (Hamadouche 46 ) MOM (Schmidt 1 ) In-vivo Wear Rates Device 130 79 73 25 4 Linear Wear (µm/y) Figure 1 Figure 2
Transcript of Metal Ions – A Scientifi c Review Introduction...

1
etal-on-metalbearingsintotalhipreplacementhaveexperiencedaresurgenceofpopularityinrecenttimes.Thisisduemainlytoasignificantnumberoflong-termclinicalstudieshighlightingtheremarkablylowwearratesofmetal-on-metalbearingsimplantedoverthepast40years.1-4Clinicalcomplicationswiththeearlygenerationcomponentsusuallywererelatedtomanufacturingissuessuchas,impropertolerancesandpoordesign.5Recentadvancementsinmanufacturingtechnologyhaveenabledmoreprecisetolerances,surfacefinish,anddesignsthatprovideanincreasedrangeofmotion(Figure1).DocumentedclinicalsuccesswithmoderndeviceshasledtotheFDAgrantingmarketapprovaltosomeorthopediccompaniesintheUS.6,7
etal-on-metalbearingsintotalhipreplacement
Introduction
M
MetalIons–AScientificReview
Metal-on-metalisparticularlyattractiveinthetotalhipnotonlyduetotheultra-lowwearexhibitedinnumerousclinicalandsimulatorstudies1–8(Figure2),butalsoduetotheflexibilityaffordedbydesignsbasedonthepropertiesofcobaltchromiumalloy.Thisflexibilityenablestheuseoflargediameterheadsinavarietyofacetabularconfigurations.Largermetal-on-metalfemoralheadscanprovideincreasedrange-of-motionandstability,aswellasincreasedresistancetodislocation.9-12Theincorporationoflargerdiameterfemoralheadsintoceramicandpolyethylenebearingspresentsdesignchallengesduetoimpingementconcernswithceramics,andincreasedbrittlenesswiththinpolyethyleneliners,allleadingtoanincreasedriskofmechanicalfracture.13,14Metal-on-metalcomponentsdonotposeariskofmechanicalfracture.Currentmetal-on-metaldesignsallowtheuseofthelarger38mmheadsinacetabularcomponentsizesassmallas46mm.
Despiteitslengthyandpositiveclinicalhistory,therehavebeenconcernsexpressedregardingthelong-termbiologicalconsequencesofmetal-on-metalweardebris,particularlythereleaseofcobaltandchromiumionsintothebody.Questionsaboutmetalionsandtheirbiologicaleffectsarenotnew.Manystudieshavebeenconductedoverpastdecades.Allhavefailedtoestablishacausallinkbetweenionrelease,andcancerorothernegativesystemiceffects.15–22Aswitheachbearingsurface,certainunknownsstillexist,andinrecenttimes,fueledbyrumorsandmisinformationaboutthemetalions,thedebatelingerson.Followingarefivereasonswhymanyleadingresearchersconsiderthemetaliondebatetobeinconsequential.
Metal-on-metalhasexhibitedultra-lowwearratesnotonlyinsimulatorstudies,butalsothroughpublishedin-vivowearstudiesasshowninthein-vivowearcomparisonabove.
RadialClearanceµmSphericity=10µmSurfaceFinishRa=1µm
120–50010–20.1–1
25–75<5<.005
Early Modern
EarlyMOMHead RecentMOMHead
140120100806040200
Poly(Head44)
ArCom®
(Head44)HXLP(Oonishi45)
COC(Hamadouche46)
MOM(Schmidt1)
In-vivoWearRates
Device
130
7973
25
4
LinearW
ear(µm/y)
Figure1
Figure2

2 3
itallium™orcobaltchromiumalloyhasbeeninuseinorthopedicsformorethan80yearssinceitsfirstusebyDr.Smith-Petersenintotalhipreplacementsurgeryin1917.23Thestrengthanddurabilityofcobaltchromehasbeenappliedtoavarietyofbearingsurfacesovertheyearsincludingtotalknees,elbows,shouldersandhips.Cobaltchromewasfirstusedinmetal-on-metalapplicationsasearlyas1958indesignssuchastheRing,Muller,McKee/Farrar,andSivashprostheses.Sincethoseearlydaysoforthopedics,hundredsofthousandsofpatientshavereceivedmetal-on-metalimplants,withthemajoritybeingimplantedinEurope.Interestingly,40yearsandhundredsofthousandsofimplantslater,metal-on-metalionreleaseremainsanon-issueamongmostEuropeanorthopedicsurgeons.
Throughoutthehistoryofmetal-on-metalvariousauthorshaveexaminedtheionreleaseissue.Followingarebriefsummariesofsomeoftheirfindings.
TheRiskofCancerFollowingTotalHiporKneeArthroplasty,JBJS,May200115
Dr.Tharani,etal.,reportedontheriskofcancerfollowingtotalhiporkneearthroplasty.15Ninedifferentstudiesencompassing140,000totalhipandkneecaseswerecombinedandstatisticallyevaluatedinordertocomparetherelativeriskofcancertothatofthegeneralpopulationoracontrolgroup.Intheseninestudiesatotalof25casesofmalignantdiseasewerereported,and34%ofthecancersoccurredwithinthefirsttwoyearsofimplantation.Thesefindingsshowed,“theavailabledatadonotsupportacausallinkbetweentotalhiparthroplastyandthedevelopmentofcancer.”Inaddition,noincreasedriskofcancerwithametal-on-metalhipimplantversusapolyethyleneimplantwasfound.Long-termconcernsaboutmetal-on-metalinthehipshouldbeweighedagainstthestudydatashowingthat34%ofthecancersaftertotaljointreplacementoccurredwithinthefirsttwoyears,andwerenotassociatedwiththetotaljointimplant.
1 Cobaltchromealloyisaknownmaterial.
V Cobaltchromehasbeenusedinawidevarietyoforthopedicimplantsoverthepast80yearsincludingthishipimplantfromtheearly20thcentury.
Cobaltchromewasfirstusedinmetal-on-metalapplicationsasearlyas1958indesignssuchastheMuller,McKee/Farrar,SivashandRing(picturedontheleft)prostheses.

2 3
CancerRiskAfterMetal-on-MetalandPolyethylene-on-MetalTHA,CORR,August199616Dr.Visuri,etal.,alsostudiedthecancerriskaftermetal-on-metalandpolyethylene-on-metaltotalhiparthroplasty.16Thestudyinvolved579metal-on-metalpatientsand1,585metal-on-polyethylenepatientswithupto16yearfollow-up.Theirobjectivewastocomparetheincidenceofcancerafterbothmetal-on-metalandmetal-on-polyethylenetotalhipreplacementtothatofthegeneralpopulationinFinland.Therewasnostatisticallysignificantincreaseincancerofanytype,at16-yearfollow-up,witheitherametal-on-metalormetal-on-polyethylenecomparedtotheexpectedcancerrateofthegeneralpopulation.Theauthorsconcludedthat,“theobservedvariationintheincidenceofdifferentcancersamongpatientswhohadtotalhiparthroplastycomparedwiththegeneralpopulationsuggeststhatfactorsotherthantotalhiparthroplastyplayamajorroleintheoriginorcancer”(Figure3).
MOM
Expected
140
120
100
80
60
40
20
0
1 51015Years
CancerIncidence
Dr.Visurireportednostatisticallysignificantincreaseincancerofanytypewitheitherametal-on-metalormetal-on-polyethylenehipreplacementcomparedtotheexpectedcancerrateofthegeneralpopulationata16-yearfollow-up.
DistributionofCobaltChromiumWearandCorrosionProductsandBiologicReactions,CORR,August199617Dr.Merritt,etal.,examinedthedistributionofcobaltchromiumwearandcorrosionproductsandthesubsequentbiologicreactions.17Theissueofcobaltchromiumwearandcorrosionproductswasevaluatedinanefforttoseehowthismightrelatetothebiologicperformanceofimplantdevices.Thefindingswereextremelyfavorableasrelatedtoawellfunctioningmetal-on-metalhipimplant.Theauthorsconclude,“itisclearatthisstageintotaljointreplacement,thatmorereportedadversebiologicresponsesareoccurringtothepolyethylenethantothemetal.Itistemptingtoaddressthisissuebyeliminatingthepolyethylene.”
Figure3
4 5
2 Metalionreleaseisnotuniquetometal-on-metaldevices.
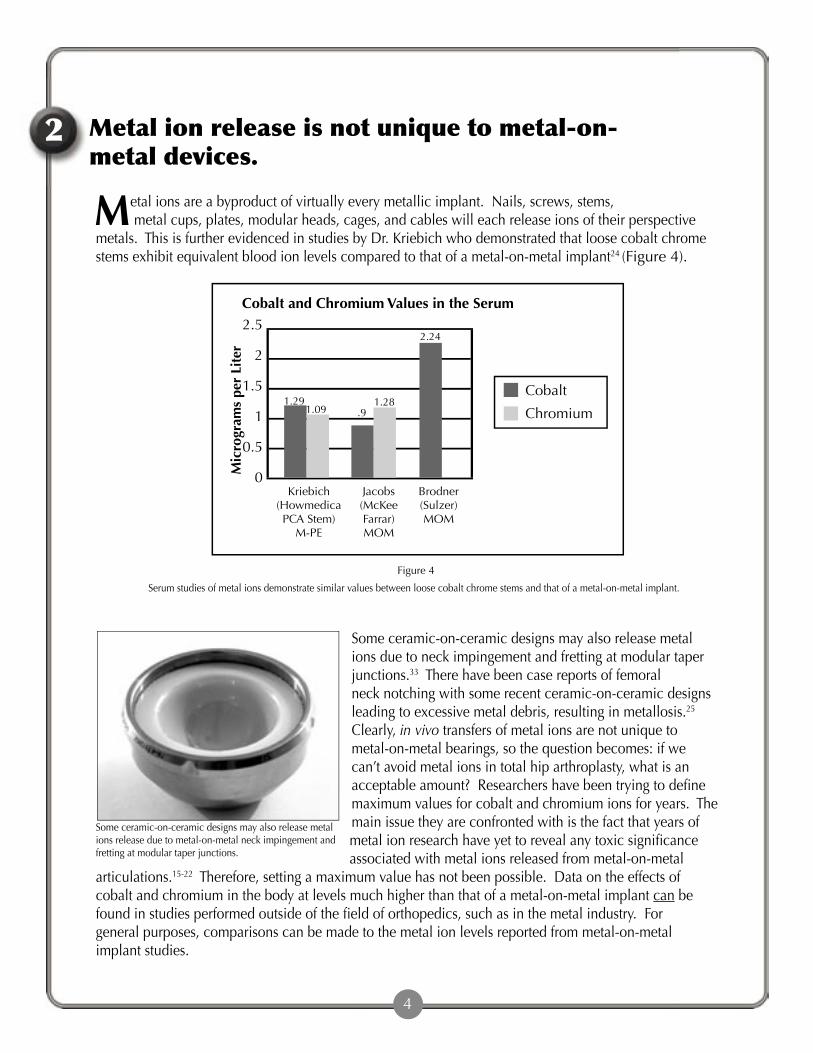
etalionsareabyproductofvirtuallyeverymetallicimplant.Nails,screws,stems,metalcups,plates,modularheads,cages,andcableswilleachreleaseionsoftheirperspectivemetals.ThisisfurtherevidencedinstudiesbyDr.Kriebichwhodemonstratedthatloosecobaltchromestemsexhibitequivalentbloodionlevelscomparedtothatofametal-on-metalimplant24(Figure4).
Someceramic-on-ceramicdesignsmayalsoreleasemetalionsreleaseduetometal-on-metalneckimpingementandfrettingatmodulartaperjunctions.
2.5
2
1.5
1
0.5
0Brodner(Sulzer)MOM
Jacobs(McKeeFarrar)MOM
Kriebich(HowmedicaPCAStem)
M-PE
CobaltandChromiumValuesintheSerum
Cobalt
Chromium
Serumstudiesofmetalionsdemonstratesimilarvaluesbetweenloosecobaltchromestemsandthatofametal-on-metalimplant.
Someceramic-on-ceramicdesignsmayalsoreleasemetalionsduetoneckimpingementandfrettingatmodulartaperjunctions.33Therehavebeencasereportsoffemoralnecknotchingwithsomerecentceramic-on-ceramicdesignsleadingtoexcessivemetaldebris,resultinginmetallosis.25Clearly,invivotransfersofmetalionsarenotuniquetometal-on-metalbearings,sothequestionbecomes:ifwecan’tavoidmetalionsintotalhiparthroplasty,whatisanacceptableamount?Researchershavebeentryingtodefinemaximumvaluesforcobaltandchromiumionsforyears.Themainissuetheyareconfrontedwithisthefactthatyearsofmetalionresearchhaveyettorevealanytoxicsignificanceassociatedwithmetalionsreleasedfrommetal-on-metal
articulations.15-22Therefore,settingamaximumvaluehasnotbeenpossible.Dataontheeffectsofcobaltandchromiuminthebodyatlevelsmuchhigherthanthatofametal-on-metalimplantcanbefoundinstudiesperformedoutsideofthefieldoforthopedics,suchasinthemetalindustry.Forgeneralpurposes,comparisonscanbemadetothemetalionlevelsreportedfrommetal-on-metalimplantstudies.
MMicrogram
sperLiter
1.291.09 .9
1.28
2.24
Figure4
4 5
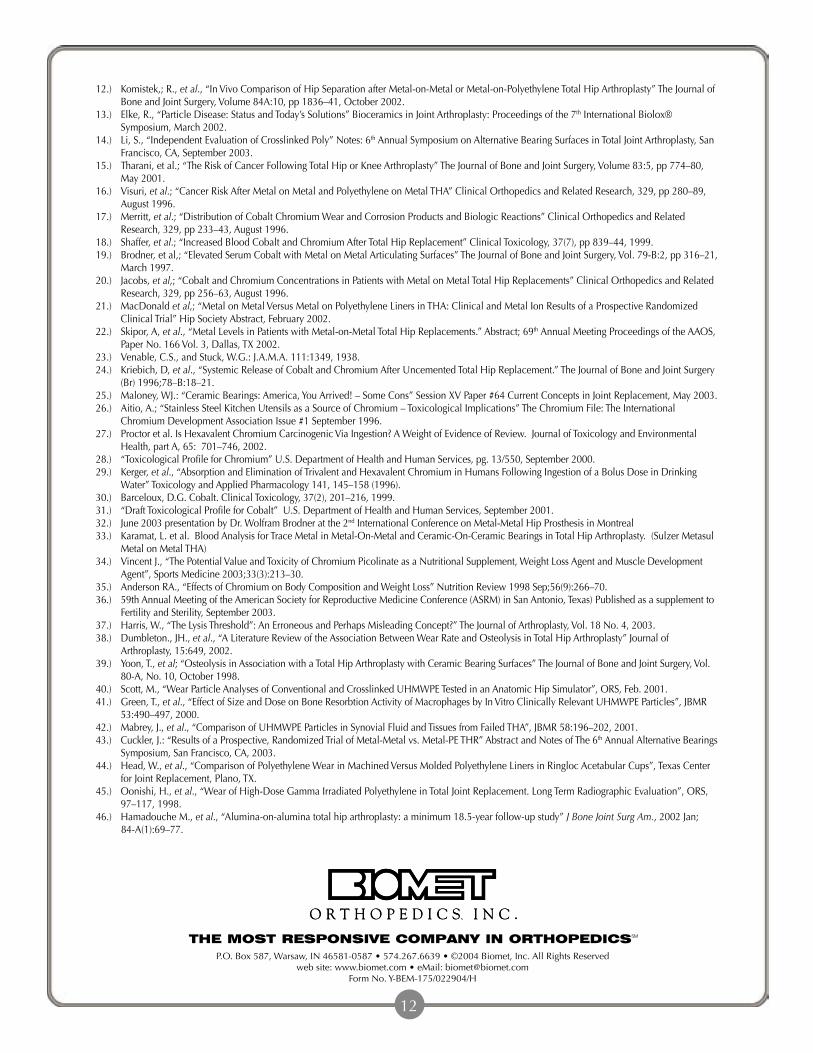
orkersinthemetalindustryaretypicallyexposedtohigherthannormallevelsofthemetalstheyareprocessing.Testshaveshownhigherthannormalbloodionvaluesinfactoryworkersexposedtochromiumandcobalt.
Thesemetalscanbeintroducedintotheirsystemthroughdermalexposure,inhalationandaccidentalingestion.27-31Itshouldbenotedthateventhoughtheseworkersdemonstratebloodionvalues15-20timeshigherthanthatofametal-on-metalimplant,nosystemictoxicityhasbeenestablished.Metal-on-metalionlevelsofchromiumcanalsobecomparedto“studiesonworkercohortswhohavehistoricallybeenexposedwellabovethecurrentpermissiblestandards(IARC,1990),andhavenotshownaconsistentpatternofelevatedcancerincidence”(Figure5)(Proctor,2002).27
3 Casereportsandstudiesofcobaltandchromiuminotherindustriessupporttheuseofmetal-on-metalbearingsinorthopedics.
ChromiumBloodLevels
100
80
60
40
20
0
Microgram
s/Liter
JacobsMetal-on-Metal
1.28
Proctor(FactoryWorkers)
75
3.03
MacDonaldMetal-on
Metal
3
SchafferMetal-on-Metal
Forexample,discussionsoftoxicityhavealsoextendedtothefemalepopulationandpregancy.Inthe1960scobaltwassometimesusedasaremedyforanemiainpregnantwomen.Barcelouxreportedononegroupofwomenreceivingover100,000Mcgofcobaltperday,allofwhomdeliveredhealthyfull-terminfants,andexperiencednoadversesideeffectsrelatedtothecobaltmedication30(Figure8).
W
Metal-on-metalionlevelsofchromiumcanalsobecomparedto“studiesonworkercohortswhohavehistoricallybeenexposedwellabovethecurrentpermissiblestandards,andhavenotshownaconsistentpatternofelevatedcancerincidence.”27
Figure5

6 7
Dr.BrodnerfromVienna,Austriarecentlyreported(Montreal,June2003)onthreepregnantwomenwhowererecipientsofmetal-on-metalhips.Metaliontestingwasperformedatthetimeofdelivery.Traceamountofionscouldbedetectedinthemothers,withnodetectableamountintheumbilicalcords.Dr.Brodnerconcludedthatmetal-on-metalwassafeforwomenofchildbearingageas“theplacentaactsasaneffectivebarrierforcobaltandchromiumdisseminatedfrommetal-on-metalarticulations.”31Notonlyhascobaltbeenusedasamedicineforrefractoryanemia,butchromiumalsohasbeneficialeffectsinthebody,suchasassistinginpropermetabolicfunction.
Adebateaboutmetalionrelease,similartothatoccurringinorthopedics,iscurrentlybeingwagedinthefoodindustry.Someinvestigatorshaveexpressedconcernregardingtheleachingofmetals,suchaschromium,intofoodfrommetalliccookingutensils.Asintheorthopedicfield,somehaveremainedcautious,statingthatmoreresearchinthisareaisneeded.Dr.Aitio,ChiefPhysicianfortheDepartmentofIndustrialHygieneandToxicologyattheFinnishInstituteofOccupationalHealth,concludedthat:“Notoxicityistobeexpectedfromthechromiumleachedfromkitchenware,itmayinfactbebeneficialtohealth,sincetheamountsofchromiuminpresentWestern-typedietsaregenerallysmallincomparisontoamountsconsideredtobeoptimal.”26
Metal-on-Metalhasbeenusedinwomenofchildbearingage.
Debateaboutmetallicionreleasefromfoodutensils.

6 7
ttimesinthemidstofthedebatesregardingmetalions,itishelpfultorememberthatmetal-on-metaldevicesareFDAregulatedandclearedfororthopedicapplicationsbytheUSgovernment.Thegovernmenthasalsoestablishedarecommendeddailyallowanceforchromium.“ChromiumIII(trivalentchromium)isanessentialmicronutrientwitharecommendeddailyrequirementforhumansintherangeof50to200microgramsperday(µg/d).”27Asdemonstratedinthechartbelow,ametal-on-metalhipisassociatedwithbloodchromiumlevelsof3–5Mcg/l,themajorityofwhichisexcretedthoughtheurine.18
Aswithmanyelements,chromiumcanexistinseveralatomicvalencestates.ChromiumVI(hexavalent)andChromiumIII(trivalent)arethetwomostcommon.“ChromiumIIIdisplaysextremelylowornotoxicityviaallroutesofhumanexposureanddoesnotposeacarcinogenichazard(ATSDR,2000;U.S.EPA,1998a;IARC,1990;WHO,1988).”27ChromiumpicolinateisoneformofchromiumIIIthatwassoldinlargequantitiesduringthe“chromiumcraze”ofthemid1990s.Itwaspromotedasawaytoburnfatandregulatemetabolism,andisstillastandardingredientinmanyhealthfoodsupplementsbeingsoldtoday.34,35
“ChromiumVI(hexavalentchromium)isimportanttoavarietyofindustriesincludingpigmentmanufacturingandpainting,metalplating,woodtreating,andleathertanning…”27Hexavalentchromiumcanhaveatoxiceffectinphysiologicalenvironmentsespeciallyifintroducedtothebodyinlargeamounts.
CobaltandChromiummaybebeneficialtothebodyasestablishedbyresearchandlistedbytheUSgovernment.
4
Aswithmanyelementschromiumcanexistinseveralatomicvalencestates.
Chromiumisastandardingredientinmanyhealthsupplementsbeingsoldtoday.
A

8 9
Itiswidelyacceptedthatthevalencestateofchromiumreleasedfromametal-on-metalimplantisprimarilytrivalentwhichisthemorebiocompatibleformofchromium.Also,evenifchromiumionswerereleasedinthehexavalentstate,thelevelsappeartomuchlowerthantheamountsthatmightcausetoxicity,asillustratedinthefindingslistedbelow:
• “recentkineticsandinvivogenotoxicitydatademonstratethatCr(VI)isreducedtonontoxicCr(III)insaliva,intheacidicconditionsofthestomach,andintheblood.”27
• “AtconcentrationsatleastashighasthecurrentU.S.maximumcontaminantlevelof100microgramsperliter(µg/L),andprobablyatleastanorderofmagnitudehigher,Cr(VI)isreducedtoCr(III)priorto,oruponsystemicabsorption.”27
• “Redbloodcelllysateshaveasubstantialandregenerativecapacitytoreduce>100McgofCr(VI)(toCr(III)basedonthehematocritofanaverageadult(DeFloraandWetterhahn,1989;DeFlora,1996).”29
• “EssentiallyalltissuespossessasimilarhighcapacitytoreduceCr(VI)toCr(III),especiallytheliver,whichisresponsibleforthe“firstpasseffect”biotransformationsofmanychemicals(SipesandGandolfi,1991).”29
Currentmetal-on-metalionreleasestudieshaveshowntrivalentchromiumlevelsinserumtobemuchlowerthaneventhe100µg/lmaximumlistedforhexavalentchromium.18–22Also,mostresearchersagreethatchromiumionsreleasedintothebodyfrommetal-on-metalimplantsareinthetrivalentCr(III)state,andaccordingtothestatementsabove,evenifalloftheionsoccurredinthehexavalentCr(VI)state–theycouldstillbereducedtothetrivalentstatewithouttoxiceffects(Figure6).
Currentmetal-on-metalionreleasestudiesshowtrivalentchromiumlevelsintheserumtobemuchlowerthanthe100µg/dmaximumlistedforhexavalentchromium.18,21,27EvenifalloftheionsoccurredinthehexavalentCr(VI)state–theycouldstillbereducedtothetrivalentstatewithouttoxiceffects.
Trivalentchromiumisakeyelementofglucoseregulationandmetabolicfunction.Ithasbeenwidelyconsumedinpillformasameansofhelpingtoregulatediabetes,controlsugarcravings,andaidinweightloss.Ithasbeenthesubjectofmorethan35clinicalstudiesinvolvingover2,000participants36.Therecommendeddailydoseasrecommendedbythesestudiesisaround200Mcgperday(Figure7).ArecentstudyfundedbytheNationalInstitutesofHealthshowedthat:
“Dailysupplementationwith1,000Mcgofchromiumaschromiumpicolinatesignificantlyenhancedinsulinsensitivity.Theseinitialresultsofferapotentialnewnutritionaltherapyforapproximately2millionAmericanwomensufferingfromPolycysticOvarianSyndrome(PCOS).
100
80
60
40
20
0
ChromiumlevelsfromMetal-on-MetalImplants
ThemaximumamountofCRVIthebodyisabletosafelyconverttoCRIII.27
ChromiumValenceComparison
Microgram
sperDay
(Shafferetal21) (MacDonaldetal18)
15 15.15
100
Figure6

8 9
PCOSisalittle-understoodhormonalconditionthatisaleadingcauseofinfertility,andisassociatedwithinsulinresistance,gestationaldiabetesandtype2diabetes.”36(Figure7)
obaltalsohasaroleinthebody.CobaltisanessentialelementnecessaryfortheformationofvitaminB12,andthemetabolismofproteins.Consequently,consumingextraproteinandvitaminB12(ie:meatandmultivitamins),maysubstantiallyinfluencetheurinaryconcentrationsofcobalt.Theaveragepersonconsumesbetween5and45micrograms(mcg)ofcobaltperday.30Theamountofcobaltexcretedintheurinefromametal-on-metalimplantappearstobebetween3and350Mcgperday.19-21Inthe1960ssomeheavybeerdrinkersdevelopedcardiacproblemsacoupleofmonthsaftercobaltchloridewasaddedtotheirlocalbeersupply.Theestimateddailyintakeofcobaltbythesebeerdrinkerswas6000to8000Mcgperday.Reducedproteinintakeandapoordietwerealsocitedascontributingtothebeerdrinker’sheartconditions30(Figure8).Assumingacumulativeeffectofcobaltionreleasefromametal-on-metalimplant(inotherwordsnoreleasefromthebody)itwouldtakeapproximately438yearsofcumulativecobaltionreleasetocomparewithwhatthebeerdrinkerswereingestingintwomonths!Furthermore,“cancerinhumansasaresultofexposuretocobaltbyanyroutehasnotbeendemonstrated.”30TheUSNationalToxicologyProgramdoesnotlistcobaltasarecognizedanimalorhumancarcinogen.31
100000
90000
80000
70000
60000
50000
40000
30000
20000
10000
0DailyIngestion(Barceloux)
MOMUrinaryExcretion
(MacDonald)
BeerDrinkers(Barceloux)
PregnantWomen(Barceloux)
100000
800045 50.5
CobaltLevelsintheBody
Microgram
sperDay
ChromiumBloodLevels
1000
800
650
400
200
0
Microgram
sperDay
JacobsMetal-on-Metal
6.4
RecommendedDaily
Requirement(USRDA)
200
15.15
MacDonaldMetal-on
Metal
15
SchafferMetal-on-Metal
RecommendedChromiumforPCOS
1000
Studiesofelevatedcobaltlevelsinpregnantwomen,andbeerdrinkershavenotdemonstratedanelevatedriskofcancerdespitelevelsmuchhigherthanthosereportedfrommetal-on-metalimplants.
CConcernsregardingthetotalchromiumvaluesreportedinmetal-on-metalionsstudiesshouldbeweighedagainstthedailyvaluesrecommendinotherstudies.
Figure7
Figure8

verybearingsurfaceproducesanenvironmentalburdenofwearrelateddebris,nonebeingtotallyinertinthebody.Occurrenceofosteolysisduetohighermagnitudesofpolythyelenewearhasbeenreportedintheliterature.37,38Metallicparticlesmayalsobeassociatedwithosteolysis,althoughreportsofthisarelacking,andoccurrenceisrare.Ceramicparticleshavebeenassociatedwithosteolysis.Dr.Yoon,etal.,reportedon103ceramic-on-ceramichipsat7.6yearsfollow-up,finding22%femorallysisand49%acetabularlysis.39Somehavesuggestedthatthehighlycrosslinkedpolyethylenesmaynoteliminateosteolysis,inthatincreasedirradiationenergycanleadtosmaller,rounderparticulate40whichhasbeendirectlyassociatedwithanincreasedosteolyticresponse.41,42Areducedlocalresponsetometal-on-metalwearproductshasbeenwelldocumentedintwenty-yearstudiesbySchmidt,McKellop,andCuckler.1,2,43Dr.Cuckler,amongotherresearchers,hassuggestedthatreasonsforthereducedtissueresponseofmetal-on-metalweardebrisareduetoultra-lowmetal-on-metalwearrateswhichreducestheenvironmentalburdenandlocalinflammatoryresponses.43Themajorityofwearproductsexistatasubmicronlevelenablingtheweardebristobeexcretedfromthebodythroughthebody’snormalmetabolicprocesses.ThiswasreportedbyDr.Schaffer;“Weconcludethattheeliminationofcobaltandchromiumproceedsoverseveralyears,affectingabalancebetweenreleaseandexcretion”(Figure9).Thisreleasefromthebodyinanionicformmayavoidalocalresponseaswellanytoxicbuild-uponasystemiclevel.
Concernsregardingionreleasemustbeweighedagainstthewearby-productsofotherbearingsurfaces.
5
E
Everybearingsurfaceproducesanenvironmentalburdenofwearrelateddebris,noneofwhichareinerttothebody.Occurrenceofosteolysisduetoexcesspolythyelenewearisregularlyreportedintheliterature.37,38Reportsofosteolysiswithmetal-on-metalimplantsarerare.
Theexcretionofionsthroughtheurineisevidencedinclinicaltrialsofmetal-on-metalimplantsaslistedabove.
60
50
40
30
20
10
0Jacobs Jacobs MacDonald Schaffer
CobaltChromium
CobaltandChromiumValuesintheUrine
Microgram
sperDay
2.095.1
50.5
11.8
50
4
Figure9
10

References:
1.) Schmidt,etal,;“CobaltChromiumMolybdenumMetalCombinationforModularHipProstheses”ClinicalOrthopedicsandRelatedResearch,329,pp35–47,August1996.
2.) McKellop,etal,;“In-VivoWearof3TypesofMetalonMetalHipProsthesesDuringTwoDecadesofUse”ClinicalOrthopedicsandRelatedResearch,329,pp.128–40,August1996.
3.) Rieker,etal.;ClinicalTribologicalPerformanceof144Metal-on-MetalHipArticulations.MetasulaMetal-on-MetalBearing,HansHuberPress,Bern,Germany;pp.83–91,1999.
4.) Jacobsson,etal,;“20-YearResultsofMcKee-FarrarVersusCharnleyProsthesis”ClinicalOrthopedicsandRelatedResearch,329,ppS60–S68,1996.
5.) AmstutzandGrigoris,;“MetalonMetalBearingsinHipArthroplasty”ClinicalOrthopaedicsandRelatedResearch,Number329S,ppS11–S34,1996.
6.) Lombardi,etal:,“Short-TermResultsoftheM2a-TaperMetal-on-MetalArticulation”TheJournalofArthroplasty,Vol.16(8):122–28,December2001.
7.) Dorr,etal,;“ModernMetalonMetalArticulationforTotalHipReplacements”ClinicalOrthopedicsandRelatedResearch,333,pp108–117,1996.
8.) SimulatorDataonFileatBiometInc.9.) Burroughs,B.,Harris,W.,;“FemoralHeadSizeinTHR:RationaleforReassessment”Abstract32ndAnnualAdvancesinHipandKneeArthroplasty,
Cambridge,MAOctober2002.10.) AmstutzHC.,etal.,;“RangeofMotionStudiesforTotalHipReplacements:AComparativeStudywithExperimentalApparatus”,Clinical
OrthopedicsandRelatedResearch,111,pp124–130,1975.11.) Beaule,etal,;“JumboFemoralHeadfortheTreatmentofRecurrentDislocationFollowingTotalHipReplacement”TheJournalofBoneandJoint
Surgery,Vol.84–A:2,pp256–63,February2002.
Conclusion
hereareavarietyofbearingoptionsavailablefortotalhipreplacement.Metal-on-metalisthemostclinicallyprovenalternatebearingavailabletoday,withover40yearsofclinicaluse.Concernsassociatedwithmetalionreleasemustbeweighedagainsttherisksandbenefitsofotherbearingoptions.Metallicdebrisisanenvironmentalby-productofmetal-on-metalwearandispresentinthebodywithnon-metal-on-metalbearingsurfaces.24,33Extensiveresearchandyearsofclinicaltrialshavefailedtoproveanycauseforconcernassociatedwiththeionlevelsexhibitedfrommetal-on-metalimplants.Thelower-wearaspectsandwiderangeofdesignoptionsavailablewithametal-on-metalimplantmakeitparticularlyattractivefortheyounger,moreactivepatientpopulation.
Thelower-wearaspectsandwiderangeofdesignoptionsavailablewithametal-on-metalimplantmakeitparticularlyattractivefortheyounger,moreactivepatientpopulation.
T
11
12.) Komistek,;R.,etal.,“InVivoComparisonofHipSeparationafterMetal-on-MetalorMetal-on-PolyethyleneTotalHipArthroplasty”TheJournalofBoneandJointSurgery,Volume84A:10,pp1836–41,October2002.
13.) Elke,R.,“ParticleDisease:StatusandToday’sSolutions”BioceramicsinJointArthroplasty:Proceedingsofthe7thInternationalBiolox®Symposium,March2002.
14.) Li,S.,“IndependentEvaluationofCrosslinkedPoly”Notes:6thAnnualSymposiumonAlternativeBearingSurfacesinTotalJointArthroplasty,SanFrancisco,CA,September2003.
15.) Tharani,etal.;“TheRiskofCancerFollowingTotalHiporKneeArthroplasty”TheJournalofBoneandJointSurgery,Volume83:5,pp774–80,May2001.
16.) Visuri,etal.;“CancerRiskAfterMetalonMetalandPolyethyleneonMetalTHA”ClinicalOrthopedicsandRelatedResearch,329,pp280–89,August1996.
17.) Merritt,etal.;“DistributionofCobaltChromiumWearandCorrosionProductsandBiologicReactions”ClinicalOrthopedicsandRelatedResearch,329,pp233–43,August1996.
18.) Shaffer,etal.;“IncreasedBloodCobaltandChromiumAfterTotalHipReplacement”ClinicalToxicology,37(7),pp839–44,1999.19.) Brodner,etal,;“ElevatedSerumCobaltwithMetalonMetalArticulatingSurfaces”TheJournalofBoneandJointSurgery,Vol.79-B:2,pp316–21,
March1997.20.) Jacobs,etal,;“CobaltandChromiumConcentrationsinPatientswithMetalonMetalTotalHipReplacements”ClinicalOrthopedicsandRelated
Research,329,pp256–63,August1996.21.) MacDonaldetal,;“MetalonMetalVersusMetalonPolyethyleneLinersinTHA:ClinicalandMetalIonResultsofaProspectiveRandomized
ClinicalTrial”HipSocietyAbstract,February2002.22.) Skipor,A,etal.,“MetalLevelsinPatientswithMetal-on-MetalTotalHipReplacements.”Abstract;69thAnnualMeetingProceedingsoftheAAOS,
PaperNo.166Vol.3,Dallas,TX2002.23.) Venable,C.S.,andStuck,W.G.:J.A.M.A.111:1349,1938.24.) Kriebich,D,etal.,“SystemicReleaseofCobaltandChromiumAfterUncementedTotalHipReplacement.”TheJournalofBoneandJointSurgery
(Br)1996;78–B:18–21.25.) Maloney,WJ.:“CeramicBearings:America,YouArrived!–SomeCons”SessionXVPaper#64CurrentConceptsinJointReplacement,May2003.26.) Aitio,A.;“StainlessSteelKitchenUtensilsasaSourceofChromium–ToxicologicalImplications”TheChromiumFile:TheInternational
ChromiumDevelopmentAssociationIssue#1September1996.27.) Proctoretal.IsHexavalentChromiumCarcinogenicViaIngestion?AWeightofEvidenceofReview.JournalofToxicologyandEnvironmental
Health,partA,65:701–746,2002.28.) “ToxicologicalProfileforChromium”U.S.DepartmentofHealthandHumanServices,pg.13/550,September2000.29.) Kerger,etal.,“AbsorptionandEliminationofTrivalentandHexavalentChromiuminHumansFollowingIngestionofaBolusDoseinDrinking
Water”ToxicologyandAppliedPharmacology141,145–158(1996).30.) Barceloux,D.G.Cobalt.ClinicalToxicology,37(2),201–216,1999.31.) “DraftToxicologicalProfileforCobalt”U.S.DepartmentofHealthandHumanServices,September2001.32.) June2003presentationbyDr.WolframBrodneratthe2ndInternationalConferenceonMetal-MetalHipProsthesisinMontreal33.) Karamat,L.etal.BloodAnalysisforTraceMetalinMetal-On-MetalandCeramic-On-CeramicBearingsinTotalHipArthroplasty.(SulzerMetasul
MetalonMetalTHA)34.) VincentJ.,“ThePotentialValueandToxicityofChromiumPicolinateasaNutritionalSupplement,WeightLossAgentandMuscleDevelopment
Agent”,SportsMedicine2003;33(3):213–30.35.) AndersonRA.,“EffectsofChromiumonBodyCompositionandWeightLoss”NutritionReview1998Sep;56(9):266–70.36.) 59thAnnualMeetingoftheAmericanSocietyforReproductiveMedicineConference(ASRM)inSanAntonio,Texas)Publishedasasupplementto
FertilityandSterility,September2003.37.) Harris,W.,“TheLysisThreshold”:AnErroneousandPerhapsMisleadingConcept?”TheJournalofArthroplasty,Vol.18No.4,2003.38.) Dumbleton.,JH.,etal.,“ALiteratureReviewoftheAssociationBetweenWearRateandOsteolysisinTotalHipArthroplasty”Journalof
Arthroplasty,15:649,2002.39.) Yoon,T.,etal;“OsteolysisinAssociationwithaTotalHipArthroplastywithCeramicBearingSurfaces”TheJournalofBoneandJointSurgery,Vol.
80-A,No.10,October1998.40.) Scott,M.,“WearParticleAnalysesofConventionalandCrosslinkedUHMWPETestedinanAnatomicHipSimulator”,ORS,Feb.2001.41.) Green,T.,etal.,“EffectofSizeandDoseonBoneResorbtionActivityofMacrophagesbyInVitroClinicallyRelevantUHMWPEParticles”,JBMR
53:490–497,2000.42.) Mabrey,J.,etal.,“ComparisonofUHMWPEParticlesinSynovialFluidandTissuesfromFailedTHA”,JBMR58:196–202,2001.43.) Cuckler,J.:“ResultsofaProspective,RandomizedTrialofMetal-Metalvs.Metal-PETHR”AbstractandNotesofThe6thAnnualAlternativeBearings
Symposium,SanFrancisco,CA,2003.44.) Head,W.,etal.,“ComparisonofPolyethyleneWearinMachinedVersusMoldedPolyethyleneLinersinRinglocAcetabularCups”,TexasCenter
forJointReplacement,Plano,TX.45.) Oonishi,H.,etal.,“WearofHigh-DoseGammaIrradiatedPolyethyleneinTotalJointReplacement.LongTermRadiographicEvaluation”,ORS,
97–117,1998.46.) HamadoucheM.,etal.,“Alumina-on-aluminatotalhiparthroplasty:aminimum18.5-yearfollow-upstudy”JBoneJointSurgAm.,2002Jan;
84-A(1):69–77.
P.O.Box587,Warsaw,IN46581-0587•574.267.6639•©2004Biomet,Inc.AllRightsReservedwebsite:www.biomet.com•eMail:[email protected]
FormNo.Y-BEM-175/022904/H
THE MOST RESPONSIVE COMPANY IN ORTHOPEDICSSM
12


















