Metabolism of Lipoproteins Hyperlipoproteinemia. Cardiovascular diseases caused by atherosclerosis...
70
Metabolism of Lipoproteins Hyperlipoproteinemia
Transcript of Metabolism of Lipoproteins Hyperlipoproteinemia. Cardiovascular diseases caused by atherosclerosis...

Metabolism of LipoproteinsHyperlipoproteinemia

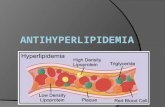
Cardiovascular diseases caused by atherosclerosis
• In Europe > 4 million CVD deaths/year
• 43% men and 55% women die of CVD
• 2002: 2557 CVD/100 000 hospitalized
• 2003: CVD treat. costs: 168 757 mil. €

Lipoproteins
• Micels transporting cholesterol esters and triglycerides in plasma Lipoprotein classes:
• CHYLOMICRONs (TG)
• VLDL (TG)
• IDL (TG+CHE)
• LDL (CHE)
• HDL (CHE)

Lipoprotein. class
Density (g/ml)
Diameter (nm)
Protein % Phospho-lipids %
Triglycerides %
HDL 1.063-1.21 5 – 15 33 29 8
LDL 1.019 – 1.063
18 – 28 25 21 4
IDL 1.006-1.019 25 - 50 18 22 31
VLDL 0.95 – 1.006 30 - 80 10 18 50
CHYLO-MIKRONS
< 0.95 100 - 500 1 - 2 7 84

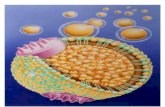
Lipoprotein structure

LDL molecule

Apoproteins
• Protein moiety of Lp
• Classification A,B,C,D,E,H,M
• Function:-hydrophilic properties
-receptor ligands
-enzyme cofactors

Classification of lipoproteins
Density EF
Chylomicrons Chylomicrons
VLDL pre-beta
IDL slow pre-beta
LDL beta
HDL alpha

Apoproteins
• A-I (28,300)- main apoprotein of HDL• activates LCAT
• A-II (8,700) – as a dimer namely in HDL• enhances activity of hepatic lipase
• B-48 (240,000) – only in chylomicrones– coded by apo-B-100 gene, edited mRNA stop-codone
at 48% length of the chain, binds to different receptors than B-100
• B-100 (500,000) – main apoprotein of VLDL, IDL, LDL
• ligand of apoB100:E receptor (LDL receptor)

• C-I (7,000) – present in CHM, VLDL, HDL• LCAT activation
• C-II (8,800) – present in CHM, VLDL, HDL • LPL activation
• C-III (8,800) – present in CHM, VLDL, IDL, HDL• LPL inhibition
• D (32,500) – present in HDL• equivalent - cholesterol ester transfer protein (CETP)
• E (34,100) – present in CHM, VLDL, IDL HDL• ligand of apo B100:E receptoru ( LDL receptoru)
• H (50,000) – present in CHM as -2-glycoprotein I (TAG metabolism)
• M – present in HDL (reverse cholesterol transport)
Apoproteins

Main lipoprotein classes
• Chylomicrones (intestine-dietary fat)– density < 1.006– diameter 80 - 500 nm– Dietary fat (esp. TAG)– apoB-48, apoA-I, apoA-II, apoA-IV, apoC-
II/C-III, apoE– ELFO- on the start line

Chylomicrones
• formed in enterocytes, resynthetised TG, less cholesterol-ester
• Transported in the lymph ductus thoracicus and v. subclavia (systemic circulation)
• TG hydrolized by lipoprotein lipase (LPL) present on capillary endothelium of peripheral tissues
• CHM remnants taken up by hepatocytes (CHM receptor binds apoE-III and apoE-IV isoforms)

Cholesterol and lipid transport by lipoproteins

Main lipoprotein classes
• VLDL– density >1.006– diameter 30 - 80nm– Formed in the liver, nascent VLDL contain
mainly TG, less CHE– apoB-100, apoE, apoC-II/C-III– EF - pre-beta fraction

VLDL
• nascent VLDL – interaction with HDL, receive apoC-II and apoC-III, equimolar exchange of TG for CH-E with HDL)
• VLDL TG hydrolized by LPL in peripheral tissues resulting in formation ofVLDL remnants (IDL)
• IDL – cca. 50% taken up in the liver by apoB100:E receptor - cca. 50% degradation by HL resulting in LDL formation

Main lipoprotein classes
• IDL (intermediate density lipoproteins)– density: 1.006 - 1.019– diameter: 25 - 35nm– TG a CHE– apoB-100, apoE, apoC-II/C-III– EF slow pre-beta– highly atherogenic

Main lipoprotein classes
• LDL (low density lipoproteins)– density: 1.019 - 1.063– diameter: 18-25nm– cholesterol esters– apoB-100– EF beta fraction– highly atherogenic

Cholesterol and lipid transport by lipoproteins

Main lipoprotein classes
• HDL (high density lipoproteins)– density: 1.063-1.210– diameter: 5-12nm– cholesterol esters – apoA-I, apoA-II, apoC-II/C-III and apoE– EF alpha fraction

HDL
– formed in liver and enterocytes– nascent – discoid micels of PL monolayer,
with apoA-I, apoA-II, apoE – lecithin-cholesterol acyl transferase (LCAT)
in periph. tissues transfers CHE into the HDL-core which becomes spheric - HDL3
(smaller HDL)

HDL3
– HDL3
• Binds to the cell membranes of peripheral tissues and aquires free cholesterol from them
• LCAT – esterification of free cholesterol to CHE and its storage in the core of the particle
• More CHE aquisition HDL3 becomes bigger and transforms to HDL2a
• HDL2a and VLDL exchange in equimolar ratio 1:1 CHE za TG --- HDL2b


Function of HDL
• REVERSE CHOLESTEROL TRANSPORT
• donor of apoproteins to other LPs

Lp(a)
• independent Lp class (at least 19 polymorphisms described)
• structure similar to LDL• apoB-100 binds apo(a)• apo(a) – primary structure
asplasminogen• highly atherogenic

LDL receptor
• First described by Michael Brown a Joseph Goldstein (Nobelova cena v roce 1985)
• studies of familir hypercholesterolemia• also named as apo B-100:E receptor• present in the liver and all peripheral tissues

LDL receptor (839 aa)
Extracellular domain binds apo-B-100/apo-E
Intracellular domain –responsible for LDL recpetors clustering in coated pits of cellular membranes



Atherosclerosis
• Most common cause of death in developed industrial countries
• High socioeconomic impact• Multifactorial detrmination• Fibroproliferative inflammation• Hyperlipoproteinemia- important but
modifiable RF

Aterosklerotický plát

PRIMARY HYPERLIPOPROTEINEMIAS
• Primary genetic precondition
• Phenotype determined also by exogenic factors (diet, physical in-activity)






Primary HL-classification
• TG increased
• CHOL increased
• Both TG and CHOL increased

Primary hypertriglyceridemia
• Fredrickson: tFredrickson: typ Iyp IV V • TG 3-12 mmol/l• Frequency 1/500 ?• Primary incr. VLDL synthesis, low LPL activity
(identical phenotype in metabolic syndrom - IR)• Clinical signs: eruptive xanthomas• R: premature ATS, ac. pancreatitis (TG>18,0)• Th: diet, fibrates, nacin

Primary hyper-CHYLOMIKRON-emia
rare
• Fredrickson: tFredrickson: typ Iyp I • high chylomicrons, defect of LPL
or apo CII• autosomal recessive disorder,
frequ. 1/1000 000• TG 20-200 mmol/l• Clin.signs.: eruptive - tuberous xanthomas,
hypersplenism, acute pancreatitis• diet – fat max. 15 % of total calories

Primary monogenic hypercholesterolemia (FH, ABD)
• Fredrickson: tFredrickson: typ Iyp II aI a• Chol. >9,0 mmol/l, (homozyg. 14,5-23 mmol/l)• Gen. defect of LDL receptoru (FH)
or gen. defect of Apo B100 (ABD)• autosomal dominant hered., frequency heterozyg.
1/500-1/700, homozyg. 1/1000 000• Clinical signs: xanthelasmata, tendineous
xanthomas, arcus lipoides corneae• R: very high risk of premature ATS• Th: statin, ezetimibe, resins, (niacin),
in homozygous forms – LDL-apheresis

Primary monogenic hyperchol. type ARH (rare)
• SYN. SYN. Autosomal recessive hyperchol.Autosomal recessive hyperchol.• Chol. 13,5-18 mmol/l• Gen. defect of ARH protein, which binds the
plasma-terminal of LDL receptor >>impaired LDL-R internalization
• Autosomal recesssive disorder• Clinical signs: xanthelasmata, tendineous
xanthomas, arcus lipoides corneae• R: very high risk of premature ATS• Th: LDL-apheresis

Primary polygenic hypercholesterolemia
• Fredrickson: tFredrickson: typypee I II aI a
• Chol. 5,5-9,0 mmol/l
• Down-regulation of LDL-R in liver (a/o periph. tissues) due to high dietary SFA and cholesterol (animal fat)
• Polygenic disease
• Clinical signs: xanthelasmata
• R: high risk of premature ATS
• Th: statin, ezetimibe, resins, (niacin),

Hyperlipidemia Lp(a)
• Lp(a) > 0,3 g/l
• Chol. 5-6 mmol/l,
• normal HDL-chol. and TAG
• Dg: direct estimation necessary !
• Et: increased Lp(a) synthesis in the liver
• R: premature ATS
• Th: lower cholesterol, (niacin)

Primary combined hyperlipidemia (common)
• Most frequent form of primary HLMost frequent form of primary HL
• Fredrickson: tFredrickson: typ yp II bII b
• Increased VLDL and LDL concentrations
• Chol. 5,5-10 mmol/l, TG 2-9 mmol/l
• Clnical signs: no xanthomas
• R: premature ATS
• Th: diet, statins, fibrates (combination)

Primary dysbetalipoproteinemia
• Fredrickson: tFredrickson: typ Iyp III II
• Increased VLDL remnants (IDL) and CHM remnants
• Chol. 7-20 mmol/l, TG 4,5-12 mmol/l
• Genotype E2/E2 + other gen.factor?
• Severe xanthomas (tuberoeruptive, tuberose, palmar)
• R: prematue ATS (CHD, PVD)
• Th: diet, fibrats, statin, (niacin)

SECONDARY HYPERLIPOPROTEINEMIAS
AlcoholHypothyroidismT2DM and decomp. T1DMHypercorticalism, corticosteroid therapyHormonal contraceptives Nephrotic syndromAcute nonfulminant hepatitisLymfomas, leukemias PlasmocytomaSLE Rheumatoid arthritisAnorexia neurosaGlycogenosis type I (Gierke)

THERAPY
• DIET
• HYPOLIPIDEMIC DRUGS

DIETARY PRINCIPLES
• Lower body weight (BMI < 25.0)• Increase physical activity-caloric balance !• Dietary cholesterol < 300 (200) mg/D• Dietary fat 25-30% of total calories• SFA:MUFA:PUFA=7:10:10 (%)• Fibres 20-30 g/D• Phytosterols cca. 2 g/D• Limit alcohol intake !• Quit smoking !

HYPOLIPIDEMIC DRUGS
• STATINS
• FIBRATES
• EZETIMIBE
• RESINS
• NIACIN

STATINS
• Cholesterol lowering
• HMG-CoA reductase inhibitors
• Very potent
• Mild decrease of TG
• atorvastatin, simvastatin, cerivastatin, fluvastatin, pravastatin, lovastatin

EZETIMIBE
• Cholesterol absorption inhibitor
• Block NPC1L1 channel
• Cholesterol lowering
• In combination with statin very effective

Ezetimibe (Zetia)
N
OH
O
F
OH
F
EZETIMIBE
This drug blocks the intestinal absorption of cholesterol. A dose of 10 mg qd leads toa 19% reduction of LDL; shows real promise in combo product with statins (Schering-Plough and Merck)

RESINS
• Cations binding bile acids in the gut
• Cholestyramine, colestipol, colesevelam

Bile sequestering resins
HC
H2C
HC
H2C
CHH2C
N(CH3)3
n
CHOLESTYRAMINE
H2NHN
HN
HN
(CH2)6N(CH3)3
HN
(CH2)9-CH3
OH
HN
(CH2)6N(CH3)3
HN
(CH2)9CH3
H2N. n HCl
. n HCl
. n HCl
. n HCl . n HCl . n HCl
. n HCl. n HCl
COLESEVELAM

FIBRATES
• PPARs alpha agonists
• Lower TG, increase HDL-chol.
• Mild decrease of chol. (TC, LDL-C)
• Fenofibrate, bezafibrate, ciprofibrate

NICOTINIC ACID (Niacin)
N
COOH
NICOTINIC ACID (NIACIN)
A water soluble vitamin of the B family;nicotinamide is not active
Cholesterol, TG and Lp(a) loweringHDL-chol. increasing
Severe side effects (flush, GI symptoms, hyperglycemia, gout)TREDAPTIVE (combination with laropiprant (PGD inhibitor)


DIAGNOSTIC
• Total. chol., HDL-chol., TAG, Lp(a)• LDL-chol. (Friedewald‘s equ.)-primární th. Cíl• nonHDL-chl. (Total chol. - HDL-chol.) –
secondary th. goal.• apo B event. , apo A1 (sec.th.goal)---------------------------------------------------------------Other specialised diagnostic methods• Calculation of atherogenic index of plasma (AIP)=logTAG/HDL-ch
• Genotype LDL-R, apo-B, apo-E
• Ultracentrifugation-accurate estimation of chol. and TG in v CHM, VLDL, IDL, LDL, HDL
• Electrophoresis (unusual)

nonHDL-cholesterol
Cholesterol within all atherogenic lipoproteins (not only LDL, but also VLDL, IDL, chylomikronech i Lp(a) !

FRIEDEWALD‘S FORMULAFOR LDL-chol.
LDLchol. = TCH – HDLchol – TAG/2,2
TCH-total cholesterolTAG-triglycerides

TREATMENT GOALS
• Depend on the risk level• 4 levels• SCORE tables: in primary prevention only
(w/o CVD, PVD or stroke) • Secondary prevention patients reperesent the
highest risk group
• New EAS guidelines 2011

VERY HIGH RISK• SEC. PREVENTION: CVD, PVD, STROKE
• SCORE ≥ 10 %• DM 2T• DM 1T with organ complications (MAU)
• CRF moderate or severe (GFR 60 ml/min/1,73m2)
• Asymptomatic atherosclerosis (carotids, aorta, peripheral arteries, coron.calcium score, ankle/brachial index)

HIGH RISK
• SCORE ≥ 5 - <10 %• Total.chol.> 8,0 mmol/l, LDL-chol.> 6,0 mmol/l
• BP ≥ 180/110, HT w.nephro-/retinopathy
• Positive family history ( M<55 y, W<65 y)

MODERATE RISK• SCORE ≥1 - < 5%
Risk value may be underestimated if: • Positive family history • Phisical inactivity• Dyslipidemia high TG / lowHDL-chol• Hyper Lp(a)• Hyperfibrinogenemia
• Hyperhomocysteinemia (?)

LOW RISK
• SCORE < 1%

TREATMENT GOALS IN BASIC LIPID PARAMETERS
Lowrisk
Moderarisk
Highrisk
VeryHighrisk
LDL cholestrol
< 3,0 mmol/l < 3,0 mmol/l < 2,5 mmol/l < 1,8 mmol/l
Non HDL chol. < 3,8 mmol/l < 3,8 mmol/l < 3,3 mmol/l < 2,6 mmol/l
HDL chol/apoA1
muži > 1,0 mmol/l / 1,2 g/lženy > 1,2 mmol/l / 1,4 g/l
Triglycerides < 1,7 mmol/l
*LDL-cholesterol is the primary therapeutical goal In very high risk patients is lowering of the LDL chol. by 50% an option

GOAL for APO B
Low risk Moderate risk High risk Very highrisk
Apo B < 1,0 g/l < 0,8 g/l
* Apo B – below 0,75 g/l may be of profitable