Metabolic Responses IGT, IAT, LM ...2003
9
ORIGINAL ARTICLE Blood glucose threshold and the metabolic responses to incremental exercise tests with and without prior lactic acidosis induction Accepted: 26 March 2003 / Published online: 21 May 2003 Ó Springer-Verlag 2003 Abstract This study compared the metabolic–ventila- tory responses and the glycemic threshold identified during lactate minimum (LM) and individual anaerobic threshold (IAT) tests. In addition, the ability to deter- mine the anaerobic power, aerobic–anaerobic transition (Trans) (e.g. ventilatory threshold; VT) and the maximal oxygen consumption ( _ V O 2max ) all within a single incre- mental treadmill test (IT) was investigated. Fifteen physically fit men [25.9 (5.5) years; 77.4 (6.5) kg] per- formed the following: test 1, IT for IAT; and test 2, LM: 30-s Wingate test followed by 8 min rest and then an IT that was the same as test 1. Blood lactate concentration [lac], glucose concentration [gluc], pH, PO 2 , PCO 2 , base excess (BE) and ventilatory variables were measured. At the beginning of the IT for LM, the ventilation, PO 2 and _ V O 2 were higher and the pH, BE and PCO 2 were lower in relation to IAT (P<0.05), while no differences were observed after reaching LM intensity during IT. More- over, the Trans could be identified by [lac] (IAT, LM), minute ventilation [ _ V E; VT identified during IAT pro- tocol (VT–IAT) and VT identified during LM protocol (VT–LM)], and [gluc] (IGT, GM) during the IT for IAT and LM. The velocities (kilometers per hour) corre- sponding to IAT (12.6±1.6), VT–IAT (12.5±1.7), IGT (12.6±1.6), LM (12.5±1.5), VT–LM (12.3±1.5), and GM (12.6±1.9) were not different from each other and the LM and IAT protocols resulted in the similar _ V O 2max . We concluded that: (1) after reaching the LM the metabolic responses during IT are similar to IAT; (2) performing a Wingate test prior to an IT does not interfere with the Trans and _ V O 2max attainment; (3) and the IGT and GM can predict the Trans. Keywords Anaerobic threshold Blood glucose Lactate minimum Wingate test pH Introduction The usefulness of incremental tests lies in their ability to identify parameters that have long been considered hallmarks of aerobic fitness. The aerobic–anaerobic transition (Trans) protocols [e.g. individual anaerobic threshold (IAT) and the ventilatory threshold (VT)] (Stegmann et al. 1981; Ribeiro et al. 1986), the maximal oxygen consumption ( _ V O 2max ) (Anderson and Rhodes 1989) and the running velocity related to _ V O 2max (V max ) (Hill and Howell 1996) are some examples of these parameters. Typically the protocols used to identify these parameters are initiated from the resting condition and do not allow for the evaluation of anaerobic power. Therefore, if the anaerobic power evaluation is desired in addition to aerobic measures, multiple visits to the laboratory are required and considerably increase the time and effort necessary. Tegtbur et al. (1993) have proposed the lactate minimum protocol (LM) for the identification of the maximal lactate steady state inten- sity (MSSLac). The incremental part of the LM is sim- ilar to an incremental testing protocol for IAT and VT identification. However, the LM is different from the IAT and VT protocols in that the incremental part of the LM test is preceded by an all-out supramaximal exercise for lactic acidosis induction (Tegtbur et al. 1993); these Eur J Appl Physiol (2003) 89: 603–611 DOI 10.1007/s00421-003-0851-1 Herbert Gustavo Simo˜es Carmen S. G. Campbell Michael R. Kushnick Akiko Nakamura Christos S. Katsanos Vilmar Baldissera Robert J. Moffatt H. G. Simo˜es (&) Catholic University of Brası´lia, A ´ guas Clams-DF, QS 07 Lote 1, Bloco G, sala 119, 72022-900, Brazil E-mail: [email protected] V. Baldissera Federal University of Sa˜o Carlos, UFSCar, Sa˜o Carlos, Sa˜o Paulo, Brazil M. R. Kushnick A. Nakamura C. S. Katsanos R. J. Moffatt Department of Nutrition, Food and Exercise Sciences at Florida State University, Tallahassee, Fla., USA C. S. G. Campbell Department of Physiology, Institute of Biosciences, University of Sa˜o Paulo, Sa˜o Paulo, Brazil
-
Upload
matheus-barbosa -
Category
Documents
-
view
11 -
download
0
Transcript of Metabolic Responses IGT, IAT, LM ...2003

ORIGINAL ARTICLE
Blood glucose threshold and the metabolic responses to incrementalexercise tests with and without prior lactic acidosis induction
Accepted: 26 March 2003 / Published online: 21 May 2003� Springer-Verlag 2003
Abstract This study compared the metabolic–ventila-tory responses and the glycemic threshold identifiedduring lactate minimum (LM) and individual anaerobicthreshold (IAT) tests. In addition, the ability to deter-mine the anaerobic power, aerobic–anaerobic transition(Trans) (e.g. ventilatory threshold; VT) and the maximaloxygen consumption ( _VV O2max) all within a single incre-mental treadmill test (IT) was investigated. Fifteenphysically fit men [25.9 (5.5) years; 77.4 (6.5) kg] per-formed the following: test 1, IT for IAT; and test 2, LM:30-s Wingate test followed by 8 min rest and then an ITthat was the same as test 1. Blood lactate concentration[lac], glucose concentration [gluc], pH, PO2, PCO2, baseexcess (BE) and ventilatory variables were measured. Atthe beginning of the IT for LM, the ventilation, PO2 and_VV O2 were higher and the pH, BE and PCO2 were lowerin relation to IAT (P<0.05), while no differences wereobserved after reaching LM intensity during IT. More-over, the Trans could be identified by [lac] (IAT, LM),minute ventilation [ _VV E; VT identified during IAT pro-tocol (VT–IAT) and VT identified during LM protocol(VT–LM)], and [gluc] (IGT, GM) during the IT for IATand LM. The velocities (kilometers per hour) corre-sponding to IAT (12.6±1.6), VT–IAT (12.5±1.7), IGT(12.6±1.6), LM (12.5±1.5), VT–LM (12.3±1.5), and
GM (12.6±1.9) were not different from each other andthe LM and IAT protocols resulted in the similar_VV O2max. We concluded that: (1) after reaching the LMthe metabolic responses during IT are similar to IAT; (2)performing a Wingate test prior to an IT does notinterfere with the Trans and _VV O2max attainment; (3) andthe IGT and GM can predict the Trans.
Keywords Anaerobic threshold Æ Blood glucose ÆLactate minimum Æ Wingate test Æ pH
Introduction
The usefulness of incremental tests lies in their ability toidentify parameters that have long been consideredhallmarks of aerobic fitness. The aerobic–anaerobictransition (Trans) protocols [e.g. individual anaerobicthreshold (IAT) and the ventilatory threshold (VT)](Stegmann et al. 1981; Ribeiro et al. 1986), the maximaloxygen consumption ( _VV O2max) (Anderson and Rhodes1989) and the running velocity related to _VV O2max (Vmax)(Hill and Howell 1996) are some examples of theseparameters.
Typically the protocols used to identify theseparameters are initiated from the resting condition anddo not allow for the evaluation of anaerobic power.Therefore, if the anaerobic power evaluation is desiredin addition to aerobic measures, multiple visits to thelaboratory are required and considerably increase thetime and effort necessary. Tegtbur et al. (1993) haveproposed the lactate minimum protocol (LM) for theidentification of the maximal lactate steady state inten-sity (MSSLac). The incremental part of the LM is sim-ilar to an incremental testing protocol for IAT and VTidentification. However, the LM is different from theIAT and VT protocols in that the incremental part of theLM test is preceded by an all-out supramaximal exercisefor lactic acidosis induction (Tegtbur et al. 1993); these
Eur J Appl Physiol (2003) 89: 603–611DOI 10.1007/s00421-003-0851-1
Herbert Gustavo Simoes Æ Carmen S. G. Campbell
Michael R. Kushnick Æ Akiko Nakamura
Christos S. Katsanos Æ Vilmar Baldissera
Robert J. Moffatt
H. G. Simoes (&)Catholic University of Brasılia, Aguas Clams-DF,QS 07 Lote 1, Bloco G, sala 119, 72022-900, BrazilE-mail: [email protected]
V. BaldisseraFederal University of Sao Carlos, UFSCar,Sao Carlos, Sao Paulo, Brazil
M. R. Kushnick Æ A. Nakamura Æ C. S. Katsanos Æ R. J. MoffattDepartment of Nutrition, Food and Exercise Sciencesat Florida State University, Tallahassee, Fla., USA
C. S. G. CampbellDepartment of Physiology, Institute of Biosciences,University of Sao Paulo, Sao Paulo, Brazil

authors have shown that during the LM protocol, per-formed under a lactic acidosis state, there is a predom-inance of blood lactate removal during the beginning ofthe incremental test (IT) and that the lactate concen-tration ([lac]) diminishes until the Trans is reached.Following the attainment of Trans the [lac] stopsdecreasing and the production is outweighed by its re-moval, thus [lac] begins to increase again. This ‘‘turningpoint’’ identifies the LM and has been used as a pre-dictor of the Trans and the MSSLac (Simoes et al. 1999;MacIntosh et al. 2002).
Simoes et al. (1999) have proposed the identificationof the Trans by blood glucose responses [individualglucose threshold (IGT) and the glucose minimum(GM)] rather than blood lactate responses during theIAT and LM protocols. Although the LM test has beenrelated to VT, MSSLac and running performance (Jonesand Doust 1998), the validity of this protocol has beenquestioned. It has been suggested that the LM test isprotocol dependent (Carter et al. 1999b) and not sensi-tive to training adaptations (Carter et al. 1999a). On theother hand, in a more recent investigation of the lactate-to-pyruvate ratio during the LM test, Carter et al. (2000)suggested that the mechanisms responsible for the‘‘turning point’’ in the [lac] response during IT for LMare the same as IT without previous lactic acidosisinduction.
The validity of the IAT protocol in identifying theTrans and MSSLac has been documented (McLellanand Jacobs 1993; Coen et al. 2001). However the validityof the IGT, LM and GM methods and their relationshipto other parameters remains under investigation. Nostudies have compared ventilatory, perceptual and bloodvariable responses during incremental tests beginningfrom resting and after lactic acidosis induction. Wehypothesize that some physiological responses would beaccentuated during IT for LM and, even so, the indi-vidual’s anaerobic power, the Trans (e.g. VT, IGT andLM intensity), and the _VV O2max would be identified in asingle testing session with this protocol.
The purposes of this study were to investigate themetabolic and ventilatory responses during IT with andwithout previous lactic acidosis induction, and thepossibility of identifying the anaerobic power, theTrans and the _VV O2max intensities during a single testingsession. In addition, the relationships between the glu-cose thresholds (IGT and GM), VTs [VT identifiedduring IAT protocol (VT–IAT) and VT identifiedduring LM protocol (VT–LM)], LM and IAT wereexamined.
Methods
Subjects
The Ethics Committee for Human Research at Florida StateUniversity approved the methods used in this study. All experi-mental procedures complied with the current laws for humanstudies. Potential subjects were introduced to all testing equipmentand procedures. After completing the informed consent procedure,15 physically active men, who were students at Florida StateUniversity, volunteered to participate in this investigation. Themean characteristics of the subjects are shown in Table 1. Bodydensity was estimated by the skinfold technique, from which bodycomposition was determined using the Siri formula for estimationof percent body fat and fat-free mass (Guedes and Guedes 1991).The subjects had been involved in recreational training programs(e.g. endurance running, resistive training, sprint exercise) for theprevious 2 years, consisting of at least 20 min of exercise threetimes per week on a regular basis.
Procedures
All tests were performed in the Exercise Physiology Laboratory atFlorida State University. The subjects took part in two testingsessions in the laboratory in random order during a period of nomore than 1 week. Tests were performed on separate days at thesame time of day. The conditions were similar between tests with aroom temperature between 22�C and 23�C, barometric pressure of760 mmHg and room humidity of about 45%. The subjects wereinstructed to have their last meal at least 3 h before testing. Vol-unteers performed an incremental test for IAT determination(Stegmann et al. 1981, modified), and an incremental test precededby lactic acidosis induction through a 30 s all-out lower body cycleexercise (Wingate test) for LM identification (Simoes et al. 1999,modified). The incremental test was performed on a treadmill(Quinton XT) and the Wingate test (Dotan & Bar-Or 1983; Bar-Or1987) was performed on a mechanical braked, basket-loaded cycleergometer (Monark 824E). Before each test session the subjectsperformed a warm-up consisting of low intensity running for 5 minat about 5–6 mph (8–9.5 km h)1) followed by 10 min lower bodystretching. The tests proceeded as described in the followingsections.
Test 1: IT for IAT
An IT was used to identify the IAT, the VT–IAT, the IGT, the_VV O2max ( _VV O2max–IAT) and the running velocity associated with_VV O2max–IAT. Initial running velocity was about 75% of the indi-vidual’s best 2-mile (approximately 3.2 km) performance (reportedfrom questionnaire). The incline was set at 1%, with 0.3 mph(about 0.5 km h)1) increments at each 3-min stage (Coen et al.1991). A rating of perceived exertion (RPE) was assessed by directcommunication between the subject and the investigator bypointing to a number in the perceptual Borg Scale (Borg 1982)during stage intervals. The subject’s heart rate (HR) was recordedat the end of each stage (Polar Sport Tester, Finland). When 95%of the age-predicted maximal HR (220 ) age) was reached, orwhen an RPE of 17 was given, the velocity was kept constant and
Table 1 Physical profile data of all subjects (n=15). Peak power The highest peak power reached during the Wingate test; mean powermean power developed over the 30 s of the Wingate test
Age (years) Bodymass (kg)
Height (cm) Bodyfat (%)
Training (years) _VV O2max
(ml.kg.min)1)Peak power[W (kg body mass))1]
Mean power[W (kg body mass))1]
Mean 25.9 77.4 178.9 15.9 11.9 52.5 11.8 9.0SD 5.5 6.5 5.1 6.6 4.3 5.3 1.5 1.1
604

the inclination was increased by 1% min)1 until the volitional fa-tigue. Expired gases were collected and ventilatory variables weremeasured continuously (Parvomedics MMS-2400 system) forcomparison between tests and identification of the minute venti-lation ( _VV E), oxygen consumption ( _VV O2), carbon dioxide production( _VV CO2), respiratory exchange ratio (R) and VT–IAT. This kind ofmethodology has been applied to reach both the _VV O2max and Trans(e.g. ventilatory and lactate thresholds) during the same incre-mental test (Jones and Doust 1998; Weltman et al. 1990). Thehighest _VV O2 obtained during the last completed 30 s of the vol-untary exhaustion was considered to be _VV O2max–IAT. The VT–IATwas identified by two independent researchers, who followed thecriteria established prior to the investigation. The criteria consistedof an increase in the _VV E/ _VV O2 without a parallel increase in the _VV E/_VV CO2 curve (Koyal et al. 1976; Weltman 1995). If the VT–IATcould not be identified by _VV E/ _VV O2 and _VV E/ _VV CO2 curves, the VT–IAT was identified considering the breakpoint in the _VV CO2– _VV O2
relationship (Ahmaidi et al. 1998).A 45-s rest period was utilized between 3-min stages during
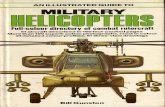
which a 25 ll sample of blood was collected from the ear lobe for[lac] and glucose concentration [gluc] measurements made with alactate/glucose analyzer (YSI 2300 S). In addition, blood samplingwas continued through a 12-min passive recovery period. The IATvelocity was identified by the kinetics of [lac] during the test andpost-exercise recovery period (Stegmann et al. 1981; Simoes et al.1999). The IGT was similarly determined by [gluc] kinetics con-sidering the exercise intensity corresponding to the lower [gluc]during the test (Simoes et al. 1999). The IAT, VT–IAT and IGTdeterminations for a single subject are presented in Fig. 1. Inaddition to capillary blood obtained for determination of [lac] and[gluc], 75 ll of capillary blood was collected at rest, at the middle ofthe incremental test (usually at stages 3–5/around the Trans) andimmediately at the conclusion of the test (exhaustion moment).These 75 ll samples were used for determination of pH, base excess(BE), partial pressure of oxygen (PO2) and partial pressure ofcarbon dioxide (PCO2).
The final velocity reached during the incremental test before theinclination increments, and the treadmill incline (percentage)reached by conclusion of the test were considered for comparison.Also, the running velocity (kilometers per hour) associated with_VV O2max–IAT ( _VV max–IAT) was identified indirectly by dividing the_VV O2max–IAT by the oxygen cost (C) at submaximal exercise( _VV O2max/C) (di Pamprero 1986). The running velocity and _VV O2
corresponding to the IAT were used to calculate the C at sub-maximal exercise.
Test 2: incremental test preceded by lactic acidosis induction
This test was performed in order to investigate the ventilatory andmetabolic responses during an incremental exercise test after lacticacidosis induction and to identify the LM, VT–LM, glucoseminimum (GM), _VV O2max ( _VV O2max–LM) and the running velocityassociated with _VV O2max–LM. The subjects first performed amaximal 30-s Wingate test on a cycle ergometer [0.0872 kilo-pondÆ(kg body mass))1] in order to optimize the power output(Dotan and Bar-Or 1983) and induce a high level of lactic aci-dosis. The Wingate test was chosen because it is a simple, familiarand extensively used method to assess anaerobic power. The [lac],pH, BE, PO2, PCO2 and [gluc] were measured in an uprightposition before exercise (rest), immediately after, and at 7 mininto recovery after the Wingate test. At the 8th min of recoveryafter the Wingate test, the subjects performed an incremental testwith ventilatory and metabolic measurements following the sameprocedures as test 1. The running velocity associated to the momentat which the [lac] curve showed a ‘‘U-shaped’’ feature duringthe incremental test was considered the LM. During the LM test theVT–LM, _VV O2max–LM and R were determined by considering thesame criterion as test 1. The GM was similarly determined by[gluc] kinetics (Simoes et al. 1999). The LM and VT–LM deter-minations for a single subject are shown in Fig. 2. Both the finalvelocity, percent of treadmill incline and the running velocity
(kilometers per hour) associated with the _VV O2max–LM ( _VV max–LM)were identified in the same fashion as in test 1. The runningvelocity and _VV O2 corresponding to the transition moment (LMvelocity) was used for _VV O2max–LM prediction.
Blood collection and laboratory analysis
The 25 ll and 75 ll of capillary blood were collected from the earlobe using heparinized and calibrated microcapillaries. The 25 llwere deposited into Eppendorf tubes containing 50 ll of 1% so-dium fluoride (NaF). The [lac] and [gluc] were determined from thissample in duplicate by using a blood lactate and glucose analyzer(Yellow Springs 2300 S). The [lac] and [gluc] results were correctedby the volume of the blood sampled within the Eppendorf tubesand are presented in millimolar concentrations. The PO2 and PCO2
(mmHg), the BE (mM) and pH were measured in the AVL (bloodgas analyzer,OMNI 3 Modular Analyzer, AVL Scientific Corpo-ration, Roswell, Ga.) from the 75 ll capillary blood samples.
Fig. 1 Determination of thetransition intensities: individualanaerobic threshold (IAT ),ventilatory threshold identifiedduring IAT protocol (VT–IAT )and individual glucosethreshold (IGT ) in a singlesubject. The IAT and VT pointsare coincident
605

Ventilatory variables measurement
Gas exchange was measured continuously during both incrementaltests (Parvomedics MMS-2400 system), and the results obtainedfrom the last 30 s of each stage were considered for comparisons.The system was calibrated with known gases spanning the expectedrange of O2 and CO2 in the expirate immediately before every test.A 15-point flowmeter calibration took place before every test byusing a 3-L syringe (Hans Rudolph).
Statistical treatment and procedures for comparison
Data are presented as means and standard deviations (SD). Therewas variability among the subjects in the number of stages com-pleted during the incremental tests. Therefore, specific pointsduring both LM and IAT tests were plotted for analyses andcomparison of the ventilatory and blood variables. The results arepresented in both tests as ‘‘before’’ (rest for IAT and 7 minrecovery from Wingate for LM), ‘‘1st stage’’ (first stage of bothincremental tests), ‘‘M1’’ (midpoint between first stage and tran-sition point during both incremental tests), ‘‘transition’’ (eitherthe LM or IAT), ‘‘M2’’ (midpoint between the transition and thelast stage/exhaustion) and ‘‘end’’ (last stage/exhaustion moment).Differences between ventilatory and metabolic variables and be-tween running velocities determined during IAT, LM, [gluc] andVTs in both protocols were evaluated by using repeated measuresANOVA. When significant differences were observed, the Tukey–Kramer test for multiple comparisons was applied to indicate thedifferences. Also, Student’s t-test for paired samples was appliedto compare the metabolic responses at corresponding points be-tween both incremental tests. The level of significance was set atP<0.05 and the Graph Pad Instat (GraphPad software) wasused.
Results
It was possible to identify the Trans by ventilatory andmetabolic variables in both IAT and LM protocols forall subjects. Usually seven to ten stages were necessary toconclude the incremental portion of both protocols formost of the participants. Fig. 3(A–F) presents the mean(SD) results of [lac], [gluc], pH, BE, PO2 and PCO2 atrest, after the Wingate test (1 min and 7 min recovery)and during the incremental part of both LM and IATprotocols for comparison. The [gluc] and PO2 responseswere similar to [lac] responses, and the pH, BE and
PCO2 responded inversely to the [lac] during both LMand IAT protocols.
Before the initiation of the incremental test for LM(7th min of recovery after the Wingate test) a higher[lac], [gluc] and PO2 (Fig. 3A, B, E) and lower pH, BEand PCO2 (Fig. 3C, D, F) in relation to rest condition(before the initiation of the IAT test) (P<0.01) wereobserved. During the incremental part of the LM testthese variables moved towards baseline values until theTrans was achieved. Significant differences between LMand IAT protocols at Trans were observed only for BEand PCO2 (Fig. 3D, F) (P<0.01). However, no differ-ences were observed between the incremental tests forany variable after the Transition (P>0.05).
The mean responses of all subjects for _VV E, _VV O2,_VV CO2 and R during the incremental part of the IAT andLM tests are presented in Fig. 4A–D. Both the _VV E and_VV O2 (Fig. 4A–B) were higher at the first stage of the LMtest in relation to the IAT test (P<0.01). _VV CO2 wassignificantly higher at M1 and Trans points during LMtest in relation to IAT. Also, during the incremental testfor LM (first stage to Trans moments) the R were lowerin comparison to IAT (P<0.01).
The Trans could be identified for all participants by[lac] (IAT and LM), [gluc] (IGT and GM) and ventila-tory responses (VT–IAT and VT–LM) following theproposed methodology (Figs 1 and 2; Table 2).
No differences were observed for running velocity orthe _VV O2 corresponding to the Trans identified by thedifferent methods (Table 2), nor were they observed forthe [gluc], pH, PO2, HR, VE and RPE correspondingIAT and LM. In addition, no differences were observedfor the results related to the moment of exhaustionduring incremental tests with (LM) and without (IAT)previous lactic acidosis induction (Tables 3 and 4).
The HR and RPE responses during the IAT and LMtests are presented in Fig. 5. The HR during incrementaltests was significantly higher only at the 1st stage of theLM when compared to that of the IAT protocol(P<0.05). No differences were observed for the RPE atany time during the incremental tests for IAT and LM(P>0.05). Finally, the running velocities corresponding
Fig. 2 Determination of thetransition intensities: lactateminimum (LM ),ventilatorythreshold identified during LMprotocol (VT–LM ) and glucoseminimum (GM) for a singlesubject during an incrementaltest after lactic acidosisinduction. The LM and VTpoints are coincident
606

to transition parameters were highly correlated witheach other (Table 5).
Discussion
The metabolic responses and the determination of theTrans during IAT and LM tests were compared. Ourprotocols to identify the IAT and LM were adaptedfrom previous studies (Coen et al. 1991; Jones andDoust 1998; Simoes et al. 1999 ). It is known that specificincremental tests and/or protocol modifications may
affect the testing results. So, in order to minimize theseeffects we used the same incremental test for both IATand LM, and the initial running velocity was selected onindividual basis.
The main finding of the present study was that theanaerobic power (Table 1), Trans and _VV O2max wereidentified in a single LM test protocol (Fig. 2; Tables 2and 3). In addition, the [gluc] responses were similar to[lac] responses during IAT and LM protocols (Fig. 3)
Fig. 4 A Minute ventilation ( _VV E), B oxygen consumption ( _VV O2), Ccarbon dioxide production ( _VV CO2) and D rate of exchange ratio( _VV CO2/ _VV O2) during incremental test with (LM) and without (IAT)previous lactic acidosis induction. Data are means (SD) of allparticipants (n=15). 1st stage First stage of the incremental test;M1 midpoint between the 1st stage and the aerobic–anaerobictransition; Trans moment of the test corresponding to aerobic–anaerobic transition identified by the IAT or LM method; M2midpoint between the Trans and the End of the incremental test
Fig. 3 A Blood lactate concentration ([lac]), B glucose concentra-tion ([gluc]), C pH, D base excess (BE), E partial pressure of O2
(PO2) and F partial pressure of CO2 (PCO2) at rest, after lacticacidosis induction (Wingate test) and during incremental tests forIAT and LM identification. Results are means (SD) of allparticipants (n=15); [gluc] is expressed as mean (SEM). 1’recWing First minute of recovery after the Wingate test; Transaerobic–anaerobic transition identified by IAT or LM; Endexhaustion moment
607

Table 2 Running velocity andoxygen consumptioncorresponding to IAT, LM,IGT, GM, VT–IAT and VT–LM for all subjects (n=15).IAT Individual anaerobicthreshold; IGT individualglucose threshold, identifiedduring IAT protocol; LMlactate minimum; GM glucoseminimum (blood glucosethreshold) identified during LMprotocol; VT–IAT ventilatorythreshold identified during IATprotocol; VT–LM ventilatorythreshold identified during LMprotocol
Subject Running velocity (km.h)1) Oxygen consumption (ml.kg.min)1)
IAT IGT VT–IAT LM GM VT–LM IAT IGT VT–IAT LM GM VT–LM
PH 10.8 11.2 10.8 10.6 10.3 10.8 37.6 38.1 37.6 37.4 36.0 38.8PR 14.8 14.8 14.8 14.2 14.3 14.3 49.8 49.8 49.8 46.5 46.7 46.7BS 13.5 14.0 13.5 13.5 14.0 13.5 40.7 43.0 40.7 43.6 44.6 43.6HG 13.8 12.9 13.4 13.7 12.7 13.7 48.6 45.8 47.0 47.9 46.3 47.9TW 13.8 13.4 14.3 14.3 14.8 13.4 43.7 41.8 45.0 42.0 42.1 40.9SS 13.7 12.7 12.7 12.7 12.7 12.2 42.5 39.9 39.9 39.1 39.1 37.6DC 13.8 14.5 14.5 13.8 15.0 13.4 47.5 48.4 48.4 48.4 52.5 43.7CK 14.2 14.2 13.7 13.7 13.7 13.7 48.7 48.7 47.3 49.9 49.9 49.9TR 13.7 13.7 13.2 13.7 14.2 13.2 52.2 52.2 48.1 52.0 55.3 48.0BE 12.2 12.2 12.2 12.2 13.2 12.2 43.5 43.5 43.5 43.6 43.9 43.6KE 12.4 10.9 11.9 12.1 11.4 12.4 44.7 39.7 41.8 43.4 42.9 43.5JE 11.7 12.7 12.2 11.7 10.8 11.3 41.6 43.4 43.2 41.6 40.6 41.0PL 9.5 9.5 9.5 9.5 9.0 9.5 37.4 37.4 37.4 37.8 37.4 37.8MH 10.3 9.8 9.8 10.3 9.8 10.3 37.9 36.0 36.0 36.6 36.3 36.6JM 11.3 12.4 10.8 11.3 12.4 10.8 41.0 42.0 40.6 39.8 43.9 38.0Mean 12.6 12.6 12.5 12.5 12.6 12.3 43.8 43.3 43.1 43.3 43.8 42.5SD 1.6 1.6 1.7 1.5 1.9 1.5 4.7 4.8 4.4 4.8 5.7 4.3
Table 3 Results associated to maximal exercise intensity identifiedduring both IAT and LM incremental tests for all participants(n=15). Final velocity Final velocity reached during the incre-mental test, just before the inclination increments; Inclin (%)per-centage of treadmill incline reached at exhaustion moment; _VV O2max
oxygen consumption at exhaustion moment; Vmax running velocityassociated with _VV O2max, identified indirectly by considering theoxygen cost (C) at submaximal exercise intensity ( _VV O2max/C) (diPamprero 1986). In this case the velocity corresponding to thetransition (IAT or LM) was used
Subject Final velocity (km.h)1) Final incline (%) _VV O2max (ml.kg.min)1) Vmax(km.h)1)
IAT LM IAT LM IAT LM IAT LM
PH 12.2 12.2 4.0 4.0 43.1 46.5 12.4 13.2PR 15.8 15.8 5.0 5.0 58.5 59.9 17.4 18.3BS 14.5 14.5 5.0 5.0 54.6 55.7 18.1 17.2HG 14.8 14.8 6.0 4.0 57.3 57.3 16.3 16.4TW 14.8 14.8 7.0 5.0 55.9 53.1 17.6 18.1SS 15.1 13.7 1.0 4.0 50.6 49.2 16.3 16.0DC 15.0 15.4 3.0 1.0 50.6 54.5 14.7 15.5CK 15.1 15.1 4.0 5.0 58.6 57.2 17.1 15.7TR 14.2 14.2 4.0 4.0 61.3 60.0 16.1 15.8BE 13.7 13.7 4.0 6.0 54.3 54.3 15.2 15.2KE 12.9 12.9 6.0 6.0 51.9 51.9 14.4 14.5JE 12.7 12.2 3.0 1.0 48.6 43.6 13.7 12.3PL 10.9 10.9 6.0 5.0 50.9 52.1 12.9 13.1MH 11.3 11.3 4.0 5.0 44.5 44.5 12.1 12.5JM 12.4 12.4 4.0 3.0 47.3 47.3 13.0 13.4Mean 13.7 13.6 4.4 4.2 52.5 52.5 15.2 15.1SD 1.5 1.5 1.5 1.5 5.3 5.3 3.8 3.6
Table 4 General results corresponding to transition and exhaustionmoments during IAT and LM incremental tests (n=15). [Lac]Blood lactate concentration; [Gluc] blood glucose concentration;
BE base excess; HR heart rate; _VV E minute ventilation; _VV O2 oxygenconsumption; _VV CO2 carbon dioxide production; R respiratoryexchange ratio; RPE rate of perceived exertion
Transition moment Exhaustion moment Transition moment Exhaustion moment
[Lac] (mM) IAT 3.3 (1.1) 8.2 (2.3) HR (beats.min)1) IAT 174.5 (12.1) 191.9 (7.9)LM 4.2 (2.0)* 7.8 (1.9) LM 172.5 (10.1) 192.6 (9.9)
[Gluc] (mM) IAT 4.1 (0.7) 5.9 (1.1) _VV E (l.min)1) IAT 77.0 (9.9) 107.6 (13.6)LM 4.0 (0.9) 5.8 (0.9) LM 75.5 (10.4) 106.9 (11.7)
pH IAT 7.39 (0.02) 7.31 (0.04) _VV O2 (l.min)1) IAT 3.4 (0.3) 4.0 (0.3)LM 7.38 (0.04) 7.30 (0.04) LM 3.3 (0.3) 4.0 (0.4)
BE (mM) IAT )1.7 (1.4) )8.6 (2.3) _VV CO2 (l.min)1) IAT 3.4 (0.4) 4.3 (0.5)LM )4.0 (2.6)*** )8.7 (2.8) LM 3.1 (0.4)*** 4.3 (0.5)
PO2 (mmHg) IAT 75.2 (5.1) 80.8 (5.3) R IAT 1.0 (0.05) 1.07 (0.06)LM 74.7 (6.7) 78.6 (7.0) LM 0.94 (0.04)*** 1.06 (0.04)
PCO2 (mmHg) IAT 38.9 (2.3) 34.3 (2.3) RPE IAT 14.9 (1.2) 19.4 (0.7)LM 35.8 (2.9)*** 34.8 (1.9) LM 14.8 (1.2) 19.1 (1.0)
Significant difference between LM and IAT results *P<0.05, ***P<0.001
608

and allowed for identification of the Trans by IGT andGM respectively (Figs 1 and 2; Table 2).
The IGT and GM identification from the presentstudy did not differ between IAT and LM intensities andour results are in agreement with previous studies(Simoes et al. 1998, 1999). The new contribution of thepresent study was that the IGT and GM intensities wereobserved at the same moment after which the acid–basebalance was disrupted during incremental exercise(Fig. 3B–D). Also, besides being well correlated withIAT and LM as previously described by Simoes et al.(1999), the IGT and GM intensities did not differ fromeach other and were highly correlated with the ventila-tory thresholds (Tables 2 and 5). Thus, these findingssupport the use of the [gluc] response to identify theTrans.
Usually the identification of anaerobic power, Trans(VT, [lac] and/or [gluc] parameters) and aerobic power( _VV O2max and/or _VV max) is time consuming and requiresmany visits to the laboratory. For this reason, the pos-sibility of identifying these parameters in a single exer-cise test is attractive for both the subject and theexaminer. The metabolic (Fig. 3A–F) and ventilatoryresponses (Fig. 4A–D) were similar between thetests after reaching the transition (IAT and/or LM
intensities). While the IAT test began from rest, theincremental test for LM began with a disruption of thephysiological homeostasis state due to prior induction oflactic acidosis invoked by the 30-s Wingate test. While[lac] was increased (Fig. 3A), both pH and BE levelsdecreased progressively during recovery (1 min and7 min) from the Wingate test (Fig. 3C–D). During thisperiod of time, the PO2 increased, while the PCO2 de-creased (Fig. 3E–F). We suspect that the PO
2increase
was due to the decrease in pH. The result would be ashift to the right of the O2 dissociation curve and in-creased O2 unloading. The PCO2 decrease was probablydue the hyperventilation induced by high intensityexercise. Others (Oren et al. 1982; Prefaut et al. 2000)have documented similar behavior in relation to PO2
and PCO2 responses.The metabolic responses presented in this study
during the first part of the LM test (high [lac], high[gluc], low pH, low BE, high PO2 and low PCO2) de-scribe a disruption of the physiological homeostasis dueto lactic acidosis induction (Fig. 3A–F). However, fromthe initial stages of the incremental test and until the LMintensity was attained, both the [lac], [gluc], pH, BE,PO2 and PCO2 moved towards the resting levels in anattempt to re-establish homeostasis. After reaching theTrans no differences were verified between IAT and LMtests for [lac], pH, BE, PO2 and PCO2, and all variablesstudied demonstrated the same profile throughout theremainder of both tests. These findings suggest that themechanisms underlying the attainment of the Trans arethe same for both IAT and LM protocols.
The interaction between [lac], pH, BE, _VV E, _VV CO2 and_VV O2 during incremental exercise without previous lacticacidosis induction has been well documented (Wasser-man et al. 1967; Koyal et al. 1976; Beaver et al. 1986;Anderson and Rhodes 1989; Weltman 1995). However,no prior studies have shown the interaction of theseresponses during an incremental test after lactic acidosisinduction. Figure 4 presents the ventilatory responsesduring both incremental tests with and without previouslactic acidosis induction. Both _VV E and _VV O2 were higherat the first stage of the LM test in relation to the cor-responding IAT test (Fig. 4A–B). The higher ventilationwas probably due to the lactic acidosis and the bufferingduring the Wingate test and post-exercise recovery per-iod (8 min), which resulted in decreased alkaline storesin relation to resting (Fig. 3D) to prevent pH diminu-tion. Buffering and hyperventilation are the most effi-cient processes for acid–base balance during exercise(Wasserman et al. 1967; Medbo and Sejersted 1985;Beaver et al. 1986; Anderson and Rhodes 1989). TheWingate exercise in the present study increased both themechanical inputs and the levels of H+ and CO2.Therefore, we speculate that these factors stimulated therespiratory center of the medulla oblongata and as aresult of this compensatory response, the _VV E was higher(Fig. 4A) and both the alkaline store (BE) and PCO2
were decreased (Fig. 3D and F) in the LM as comparedwith IAT.
Table 5 Relationships between running velocities corresponding toaerobic–anaerobic transition identified by different methods
IAT VT–LM VT–IAT GM IGT
LM 0.98 0.98 0.98 0.93 0.90IAT – 0.97 0.96 0.89 0.90VT–LM – – 0.96 0.88 0.87VT–IAT – – – 0.91 0.93GM – – – – 0.91
Fig. 5 Responses of A the heart rate (HR) and B the rate ofperceived exertion (RPE) after the Wingate test (Wing) and duringincremental tests for IAT and LM identification. Data are means(SD) of all participants (n=15)
609

In response to the incremental test the _VV O2 wasgreater during the first stage of the LM protocol incomparison with the IAT protocol (Fig. 4B). It is likelythat the higher _VV O2 was a result of an increased meta-bolic rate in an attempt to cover the aerobic deficitinduced previously through the Wingate test.
The _VV E during the recovery period after the lacticacidosis induction was not measured. However, thelower _VV CO2 observed at M1 (midpoint between 1ststage and Trans) and Trans moments of the LM testcompared with the same points at the IAT (Fig. 4C)may be explained by the hyperventilation induced ven-tilatory alkalosis after the Wingate. The lower PCO2 atthe 7th min of recovery from the Wingate test andduring the first part of the incremental test for LM(Fig. 3F), with a higher _VV E (Fig. 4A) may explain thelower _VV CO2 observed during the LM test.
The higher _VV O2 and lowered _VV CO2 during the initialstages of the incremental test for LM (Fig. 4B, C) re-sulted in a lower R in relation to the IAT test (Fig. 4D),and thus the R corresponding to LM intensity was lowerthan IAT (Table 4). This response may contribute tosome confusion in interpretation of the substrate utili-zation during exercise testing after lactic acidosis, andtherefore the R must be viewed with caution.
In spite of being different at the first stage of theincremental tests, no differences were observed for the_VV E and _VV O2 during the subsequent stages of IAT andLM tests (Fig. 4). We were able to identify the VT of theparticipants by considering an abrupt increase in the _VV E/_VV O2 without a proportional increase in the _VV E/ _VV CO2
curve in both tests. This method has been used/proposedby others during an incremental exercise test (Koyal et al.1976; Ribeiro et al. 1986; Weltman 1995). In the presentstudy, this method resulted in a visual identification ofthe VT, which was easier for the incremental exercise testafter lactic acidosis induction (Fig. 2) than for the IATthat began from rest (Fig. 1). The higher _VV E and _VV O2
during the beginning of the LM test contributed to thiseasier identification of the VT.
The blood lactate response to exercise has been sug-gested to be more reliable than ventilatory responses foraerobic assessment (Weltman 1995). Moreover, contro-versy exists over the cause and effect of the ventilatoryresponse during exercise (Neary et al. 1985; Berryet al. 1991). However, the ventilatory response to exer-cise has still been used extensively to identify the Trans,the aerobic power ( _VV O2max), _VV O2 kinetics and mechan-ical efficiency both for training and scientific purposes.In the present study the identification of the aerobic–anaerobic transition by LM, IAT, VT–LM, VT–IAT,GM and IGT methods did not differ and they correlatedwell with each other (Tables 2 and 5). Our results are inaccordance with Jones and Doust (1998) and Simoes etal. (1999). These authors have found no differences andhigh correlation between LM intensities and other aer-obic fitness parameters. In the present study, besidesbeing similar to blood lactate responses (Figs 1, 2, 3), theuse of blood [gluc] response to identify the transition
intensity yielded the same results as VT (Table 2). Wespeculate that the increase in blood [gluc] when exercisebecame more intense (e.g. above anaerobic threshold)was due to the catecholamines and glucagon responsesincreasing liver glucose output and decreasing the bloodglucose uptake (Wasserman et al. 1991). Therefore, theexercise intensity at which the [gluc] increases due to thehigher blood glucose output in relation to uptake definesthe blood glucose threshold.
With regard to _VV O2max results, no differences wereobserved for any variable attained at the end of theincremental tests with and without previous lactic aci-dosis induction (Fig. 4B; Tables 3, 4). These results re-veal that both submaximal exercise intensity (e.g. LMand VT) and the maximal aerobic power ( _VV O2max andVmax) can be identified during the same incremental testeven after previous lactic acidosis induction as in the LMprotocol.
The results of the RPE corresponding to the IAT andLM parameters in the present study were not differentfrom each other (Table 4). The mean RPE values relatedto IAT and LM (14.9 and 14.8) were higher than theRPE of 13.6 presented by Demello et al. (1987) fortrained individuals. However, our results are similar tothe RPE values between 14 and 15 corresponding toTrans determined in runners and physical active persons(Seip et al. 1991; Weltman 1995).
Interestingly our results reveal that RPE responses(Fig. 5) don’t seem to be directly dependent of the lacticacidosis responses or lower pH as previously proposedby others (Noble et al.1983; Seip et al. 1991). Immedi-ately after the Wingate test, the RPE responses weresimilar to [lac]. However, even after induced lactic aci-dosis (Fig. 3A, C) the RPE during incremental test forLM did not differ from IAT (Fig. 5B). In addition,during the LM protocol the RPE responses paralleledthose of the HR (Fig. 5A) and the _VV O2 (Fig. 4B). It isknown that these variables respond proportionally tochanges in exercise intensity. So, the results of thepresent study suggest that the RPE response may bemore related to the increasing workload than the acid–base disruption during incremental exercise. Finally, ourRPE results demonstrate the ability of RPE to identify/estimate the aerobic–anaerobic transition during anincremental test, even after lactic acidosis induction by aWingate test in an aerobically fit, male population.
In summary, the initial differences observed formetabolic and ventilatory responses during the LMprotocol in relation to the IAT protocol decreasedprogressively throughout the incremental tests and be-came non-significant around the LM intensity. TheTrans intensity was identified in both protocols by blood[lac], blood [glu] and ventilatory responses (e.g.LM, IAT, GM, IGT, VT–LM and VT–IAT) and bothprotocols yielded similar _VV O2max results. We concludedthat the homeostasis disruption evoked previously bythe lactic acidosis induction can be re-established duringthe subsequent incremental stages until the LM can beattained, and the anaerobic power, Trans and aerobic
610

power can be identified in a single LM protocol pro-posed in our methodology.
Acknowledgement We acknowledge the Fundacao de Amparo aPesquisa do Estado de Sao Paulo (Proc 97/04753–9) for thefinancial support of this study.
References
Ahmaidi S, Masse-Biron J, Choquet BAD, Freville M, Libert JP,Perfaut C (1998) Effects of interval training at the ventilatorythreshold on clinical and cardiorespiratory responses in elderlyhumans. Eur J Appl Physiol 78:170–176
Anderson GS, Rhodes EC (1989) A review of blood lactate andventilatory methods of detecting transition thresholds. SportsMed 8:43–45
Bar-Or O (1987) The Wingate anaerobic test. An update onmethodology, reliability and validity. Sports Med 4:381–394
Beaver WL, Wasserman K, Whipp BJ (1986) Bicarbonate bufferingof lactic acid generated during exercise. J Appl Physiol 60:472–478
Berry MJ, Stoneman JV, Weyrich AS, Burney B (1991) Dissocia-tion of the ventilatory and lactate thresholds following caffeineingestion. Med Sci Sports Exerc 23:463–469
Borg GAV (1982) Psycophysical bases of perceived exertion MedSci Sports Exerc 14:377–381
Carter H, Jones AM, Doust JH (1999a) Effects of endurancetraining on the lactate minimum speed. J Sports Sci 17:957–967
Carter H, Jones AM, Doust JH (1999b). Effect of incremental testprotocol on the lactate minimum speed. Med Sci Sports Exerc31:837–845
Carter H, Jones AM, Doust JH (2000) Changes in blood lactateto pyruvate concentrations and the lactate-to-pyruvate ratioduring the lactate minimum speed test. J Sports Sci 18:213–225
Coen B, Schwarz L, Urhausen A, Kinderman W (1991) Control oftraining in middle- and long-distance running by means of theindividual anaerobic threshold. Int J Sports Med 12:519–524
Coen B, Urhausen A, Kindermann W (2001) Individual anaerobicthreshold: methodological aspects of its assessment in running.Int J Sports Med 22: 8–16
Demello JJ, Cureton KJ, Boineau RE, Singh MM (1987) Ratingsof perceived exertion at the lactate threshold in trained anduntrained men and women. Med Sci Sports Exerc 19:354–362
Di Pamprero PE (1986) The energy cost of human locomotion onland and water. Int J Sports Med 7:55–72
Dotan R, Bar-Or O (1983) Load optimization for the wingateanaerobic test. Eur J Appl Physiol 51:409–417
Guedes DP, Guedes JE (1991) Proposed equations for predictingthe amount of body fat in young adults. Semina 12:61–70
Hill DW, Howell AL (1996) Running velocity at _VV O2max. Med SciSports Exerc 114–119
Jones AM, Doust JH (1998) The validity of the lactate minimumtest for determination of the maximal lactate steady state. MedSci Sports Exerc 30:1304–1313
Koyal SN, Whipp BJ, Huntsman D, Bray GA, Wasserman K(1976) Ventilatory responses to the metabolic acidosis oftreadmill and cycle ergometry. J Appl Physiol 40:864–867
MacIntosh BR, Esau S, Svedahl K (2002) The lactate minimum testfor cycling: estimation of the maximal lactate steady state. CanJ Appl Physiol 27:232–249
McLellan T, Jacobs I (1993) Reliability, reproducibility andvalidity of the Individual Anaerobic Threshold. Eur J ApplPhysiol 67:125–131
Medbo JI, Sejersted OM (1985) Acid-base and electrolyte balanceafter exhausting exercise in endurance-trained and sprint-trained subjects. Acta Physiol Scand 125:97–109
Neary PJ, MacDougall, Bachus R, Wenger HA (1985) The rela-tionship between lactate and ventilatory thresholds: coinciden-tal or cause and effect Eur J Appl Physiol 54:104–108
Noble BJ, Borg GAV, Jacobs I, Ceci R, Kaiser P (1983) A cate-gory–ratio perceived exertion scale: relationship to blood andmuscle lactates and heart rate. Med Sci Sports Exerc 15:523–528
Oren A, Whipp BJ, Wasserman K (1982) Effect of acid-base statuson the kinetics of the ventilatory response to moderate exercise.J Appl Physiol 52:1013–1017
Prefaut C, Durand F, Mucci P, Caillaud C (2000) Exercise-inducedarterial hypoxaemia in athletes: a review. Sports Med 30:47–61
Ribeiro JP, Yang J, Adams RP, Kuca B, Knutten HG (1986) Effectof different incremental exercise protocols on the determinationof lactate and ventilatory thresholds. Braz J Med Biol Res19:109–117
Seip RL, Snead D, Pierce EF, Stein P, Weltman A (1991) Per-ceptual responses and blood lactate concentration: effect oftraining state. Med Sci Sports Exerc 23:80–87
Simoes HG, Campbell CSG, Baldissera V, Denadai V, Kokubun E(1998) Determination of the anaerobic threshold by blood lac-tate and glucose measurements in track tests for runners. RevPaul Educ Fıs 12:17–30
Simoes HG, Campbell CSG, Kokubun E, Denadai BS, BaldisseraV (1999) Blood glucose responses in humans mirror lactateresponses for individual anaerobic threshold and for lactateminimum in track tests. Eur J Appl Physiol 80:34–40
Stegmann H, Kinderman W, Schnabel A (1981) Lactate kineticsand individual anaerobic threshold. Int J Sports Med 2:160–165
Tegtbur U, Busse MW, Braumann KM (1993) Estimation of anindividual equilibrium between lactate production and removalduring exercise. Med Sci Sports Exerc 25:620–627
Wasserman DH, Connolly CC, Pagliassotti MJ (1991) Regulationof hepatic lactate balance during exercise. Med Sci Sports Exerc23:912–919
Wasserman K, Van Kessel AL, Burton GG (1967) Interaction ofphysiological mechanisms during exercise. J Appl Physiol22:71–85
Weltman A (1995) The blood lactate response to exercise—currentissues in exercise science. Monograph no. 4. Human Kinetics,Champaign, Ill.
Weltman A, Snead D, Stein P, Seip R, Schurrer R, Rutt R,Weltman J (1990) Reliability and validity of a continuousincremental treadmill protocol for the determination of lactatethreshold, fixed blood lactate concentrations, and _VV O2max. Int JSports Med 11:26–32
611