
Medical Evacuation Network Project LT McMullen LT Dunham.
30
Medical Evacuation Network Project LT McMullen LT Dunham
-
Upload
herbert-powers -
Category
Documents
-
view
226 -
download
2
Transcript of Medical Evacuation Network Project LT McMullen LT Dunham.
Medical Evacuation Network Project
LT McMullenLT Dunham
Presentation: Medical Evacuation
• Background Information• Helmand Province Graph / Network
• Analysis• Questions
Medical Evaculation
• ~500AD Byzantine Empire’s Army was first to employ a organized medical evacuation.
• By 1800 most armies had some medical evacuation capability.
• Almost every conceivable mode of transportation has served to evacuate wounded from the battlefield.
Medical Evacuation
• Today US military doctrine employs a combination of ground, rotary and fixed wing transport.
• In southern Afghanistan, urgent patient transport relies almost entirely on a robust aeromedical evacuation network.
Update 7 June 2007 4
Golden Hour
• “Golden Hour” in emergency medicine refers to the span of time immediately after a traumatic injury of a soldier and the time medical intervention offers the greatest chance of survival.
Levels of Care
Intra Theater Medical Care•Level 1
– Care is administered at/close to POI and includes self or buddy aid, emergency lifesaving measures.
•Level 2– Care includes basic resuscitation, limited surgical capability, basic transfusion services, limited ancillary services.
•Level 3– The highest level of care in an operational theater and has all the capabilities of a medical treatment facility (MTF) in the States.
6
Purpose
Initial Intent (week 1 of the course)
– Model an aeromedical medevac network in Helmand Province.
– Assess the robustness of the network with two medical evacuation platforms transporting multiple patients.
– Assess design impact of providing critical care capabilities onboard current platform and extending “golden hour”
7
Purpose
Revised Intent (week 9 of the course)– Model a notional aero medical evacuation network in Helmand Province Afghanistan.
– Test the network’s ability capacities evacuate patients on demand.
– Optimize placement of Military Treatment Facilities (MTFs).
8
Purpose
Measures of Effectiveness•The ability to transport patients throughout the entire medevac network in under 60 minutes (binary).
9
Update 7 June 2007
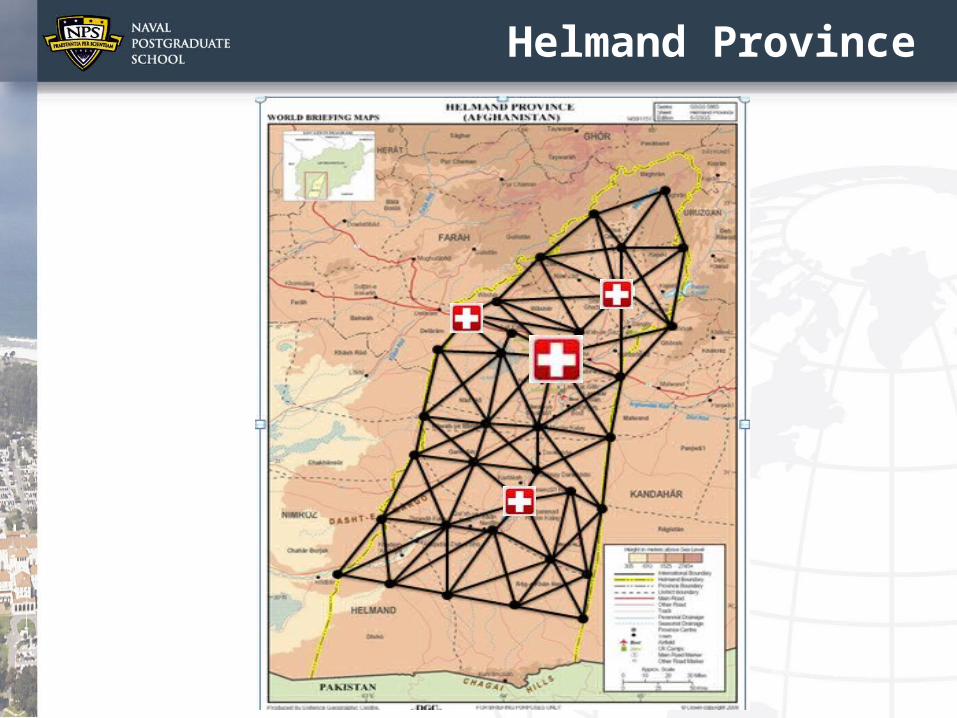
Helmand Province
Medical Evacuation Helicopters
• SH-60 – Max Speed ~145 knots– Capacity 4 litter patients
• MH-4E Chinook (British)– Max Speed 154 knots– Capacity 1-2 patients
• Helicopter Assumptions:– 115 miles per hours (patient load/unload time, threat, etc).
– Only SH-60s where employed.– Each SH-60 had a chase bird– Capacity 2 litter patients
Inaccessible Air Spaces
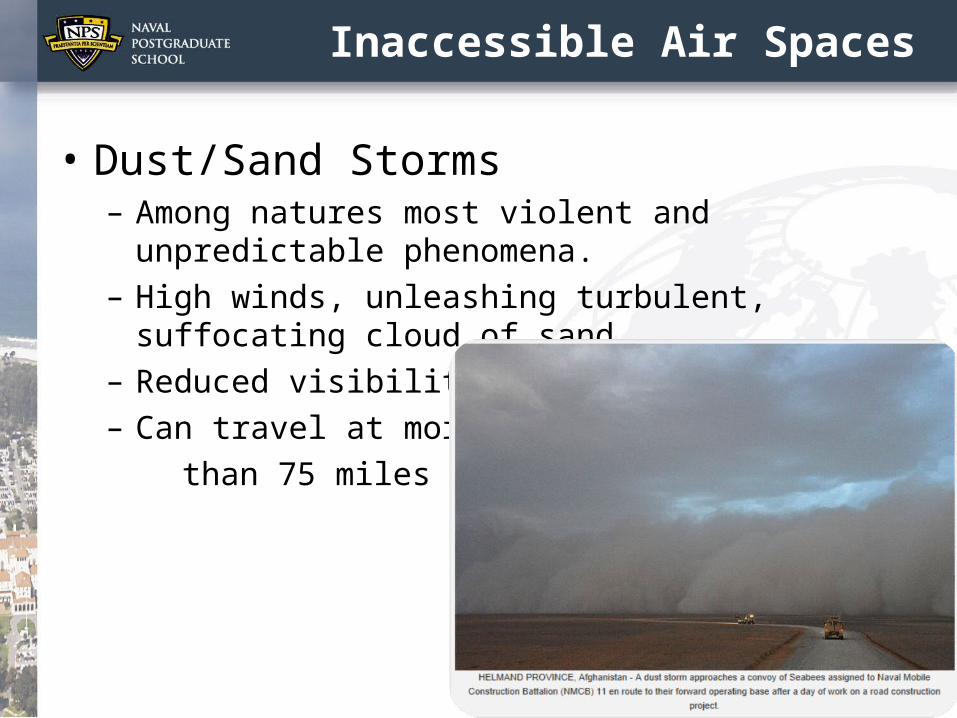
• Dust/Sand Storms– Among natures most violent and unpredictable phenomena.
– High winds, unleashing turbulent, suffocating cloud of sand
– Reduced visibility– Can travel at more than 75 miles per hour
12
Inaccessible Air Spaces
• Surface Air Missiles (SAMs) & Rocket Fire– "The US helicopter was shot down by the Taliban as it was taking off," … "It was hit by a rocket fired by the insurgents."
13
Assumptions
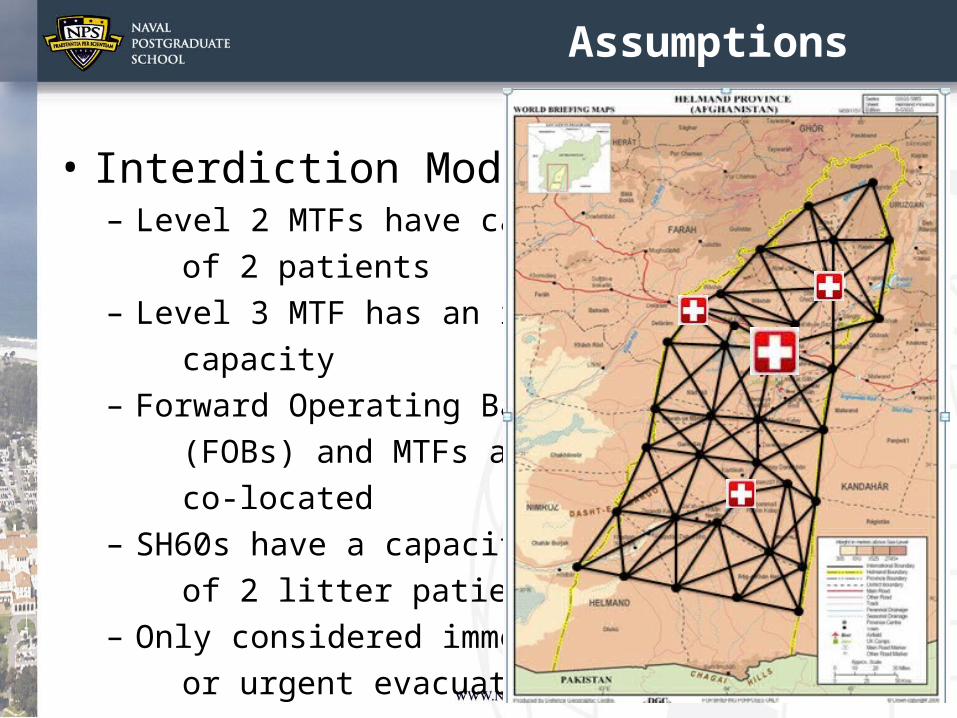
• Interdiction Model:– Level 2 MTFs have capacity of 2 patients – Level 3 MTF has an infinite capacity– Forward Operating Bases (FOBs) and MTFs are co-located – SH60s have a capacity of 2 litter patients– Only considered immediate or urgent evacuations
Assumptions
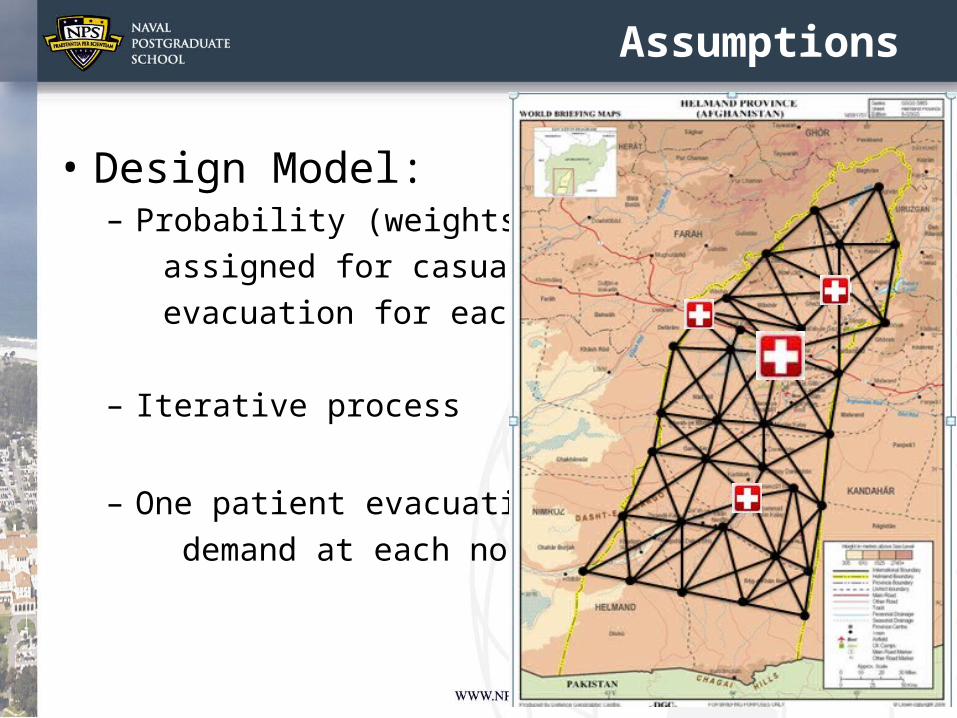
• Design Model:– Probability (weights) assigned for casualty evacuation for each POI
– Iterative process
– One patient evacuation demand at each node
Update 7 June 2007
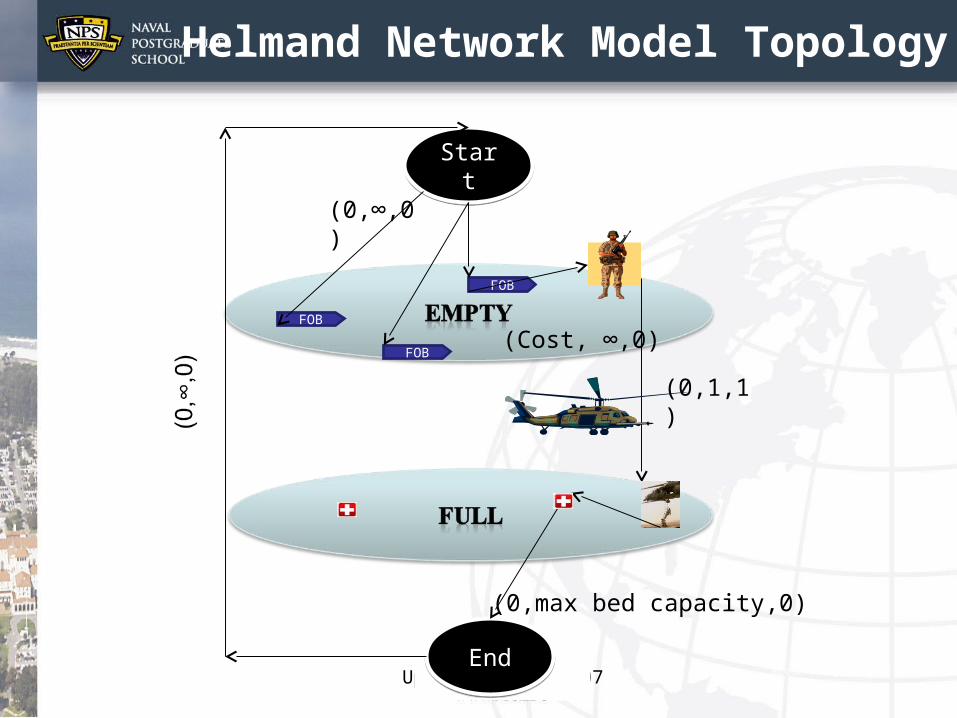
Helmand Network Model Topology
Start
Start
EndEnd
FOB
FOB
FOB
(0,1,1)
(0,∞,0)
(0,max bed capacity,0)
(Cost, ∞,0)
Update 7 June 2007
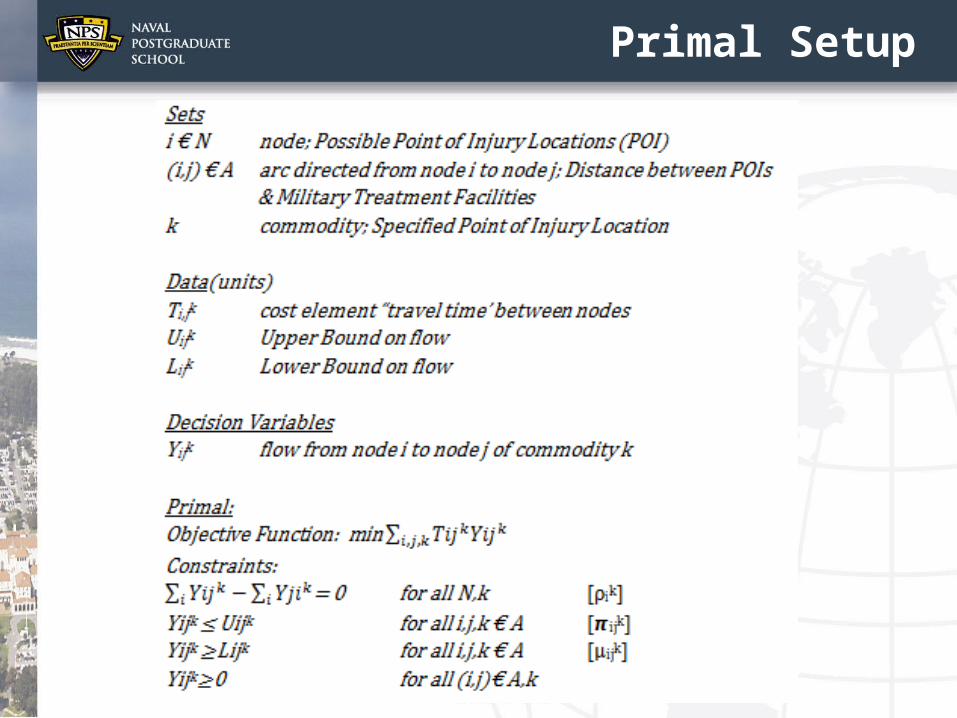
Primal Setup
Update 7 June 2007
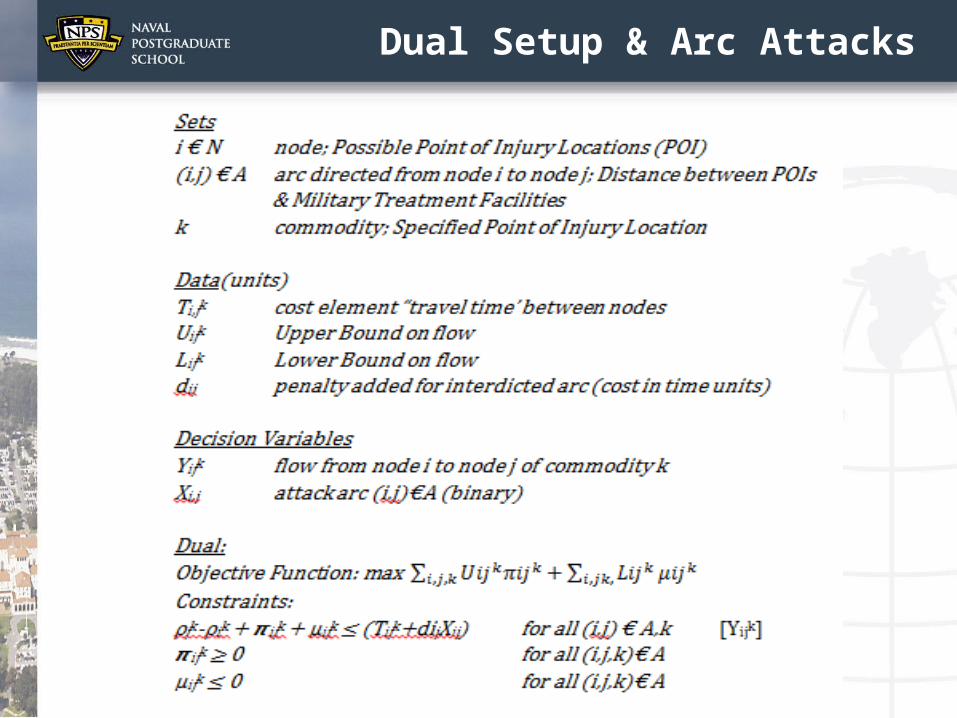
Dual Setup & Arc Attacks
Interdiction: 1-2 Patient @ each POC
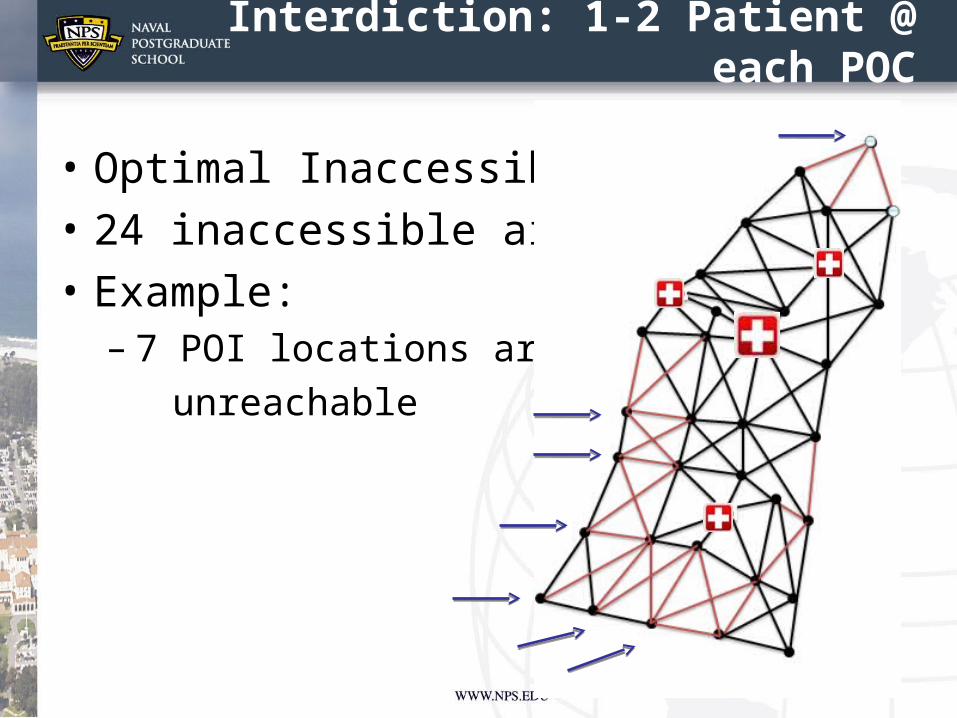
• Optimal Inaccessibility • 24 inaccessible air spaces• Example:
– 7 POI locations are unreachable
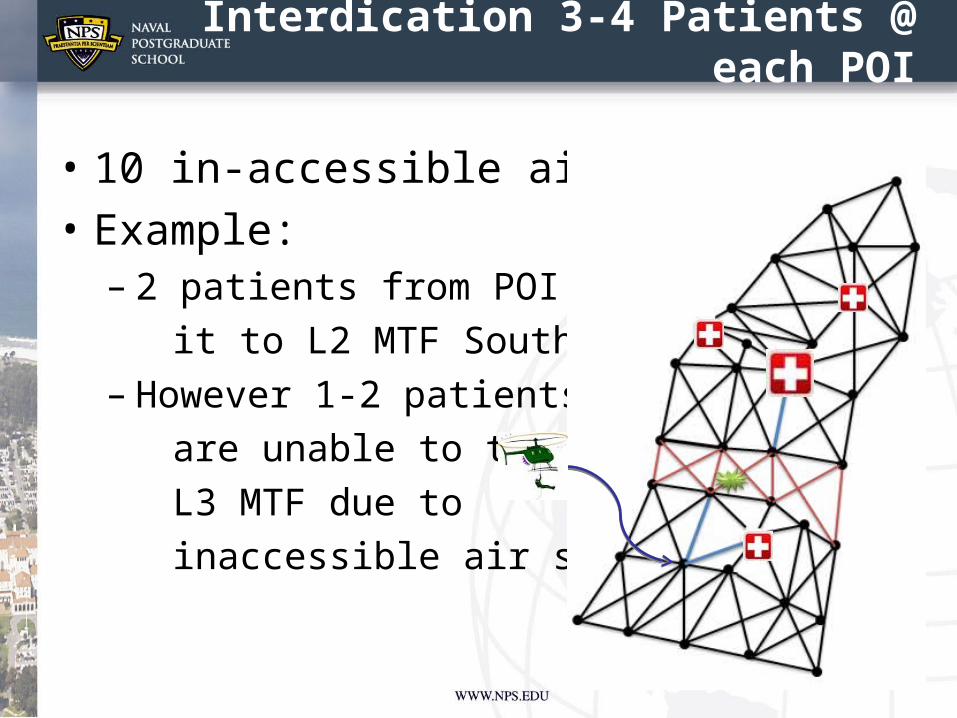
Interdication 3-4 Patients @ each POI
• 10 in-accessible air spaces• Example:
– 2 patients from POI make it to L2 MTF South, – However 1-2 patients are unable to travel to L3 MTF due to inaccessible air space
20
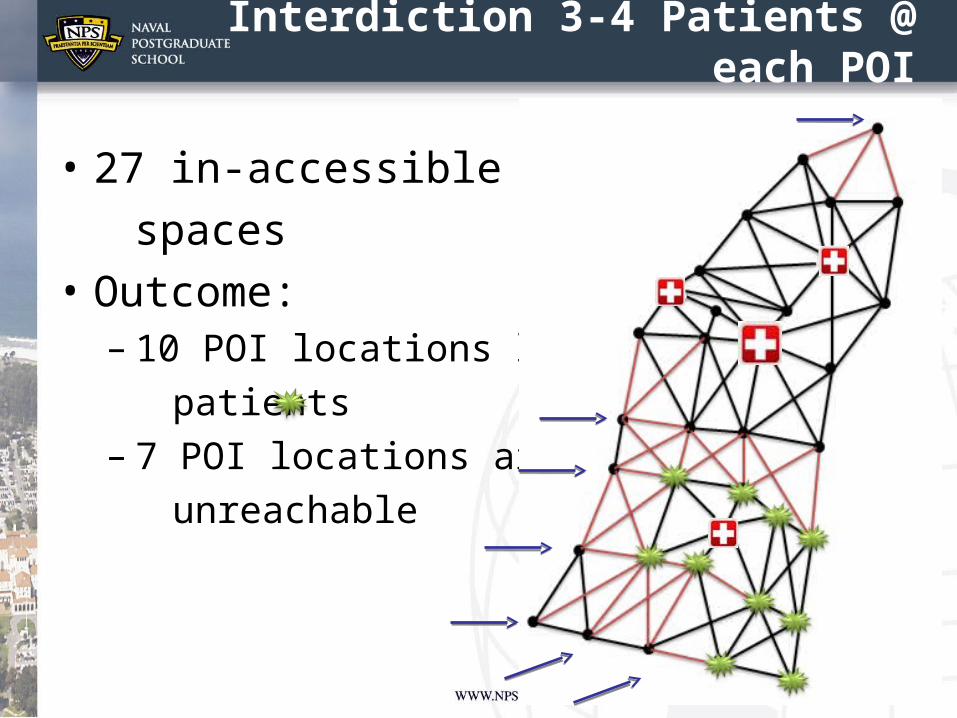
Interdiction 3-4 Patients @ each POI
• 27 in-accessible air spaces• Outcome:
– 10 POI locations lose 1-2 patients – 7 POI locations are unreachable
21
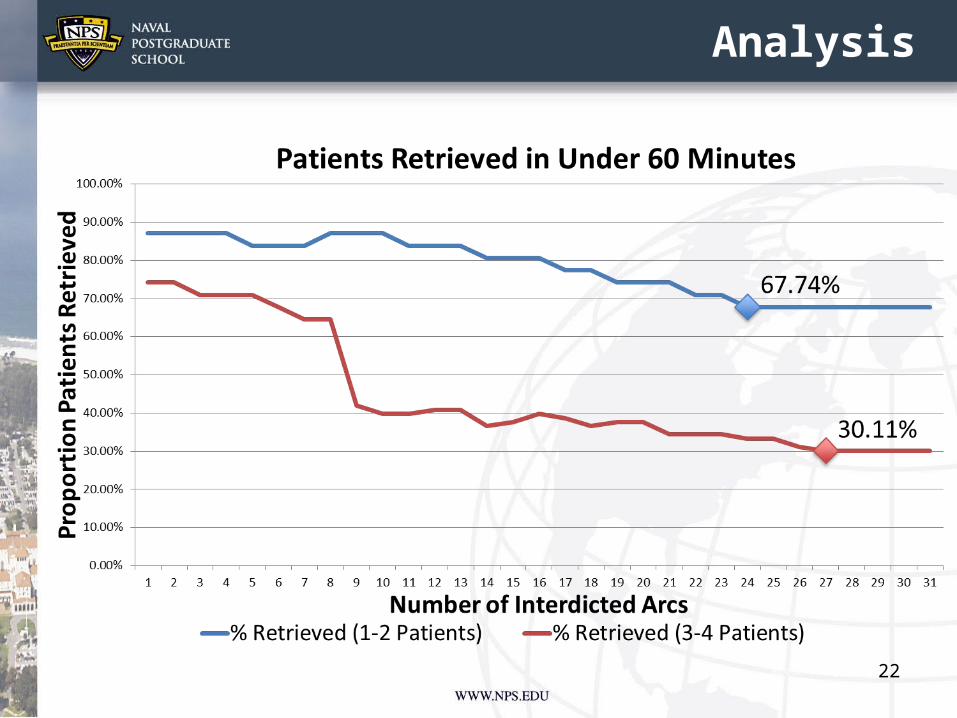
Analysis
22
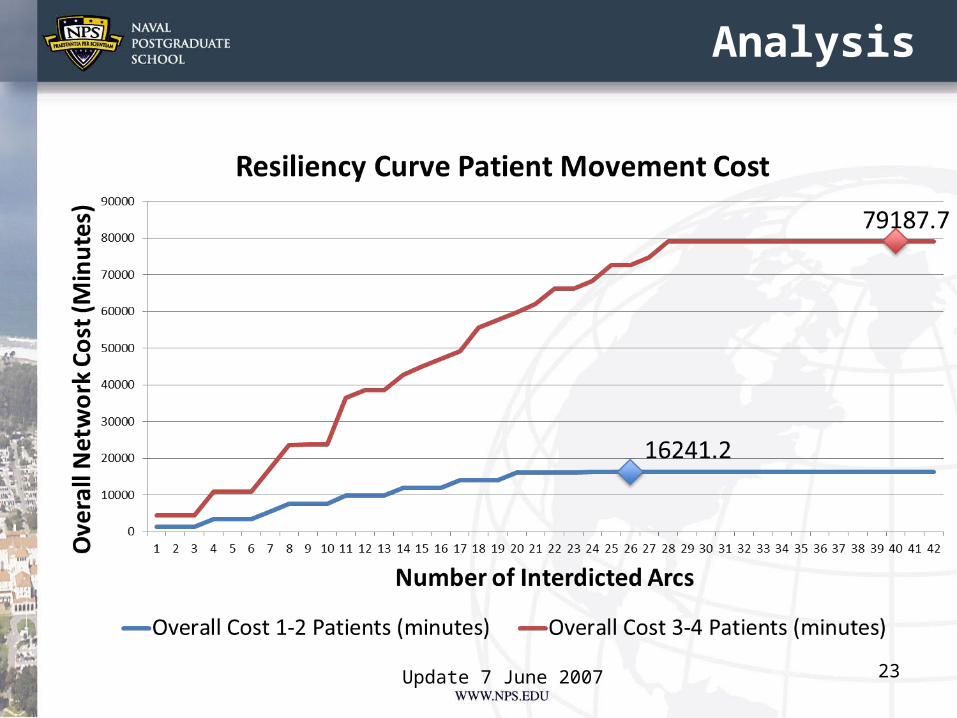
Analysis
Update 7 June 2007 23
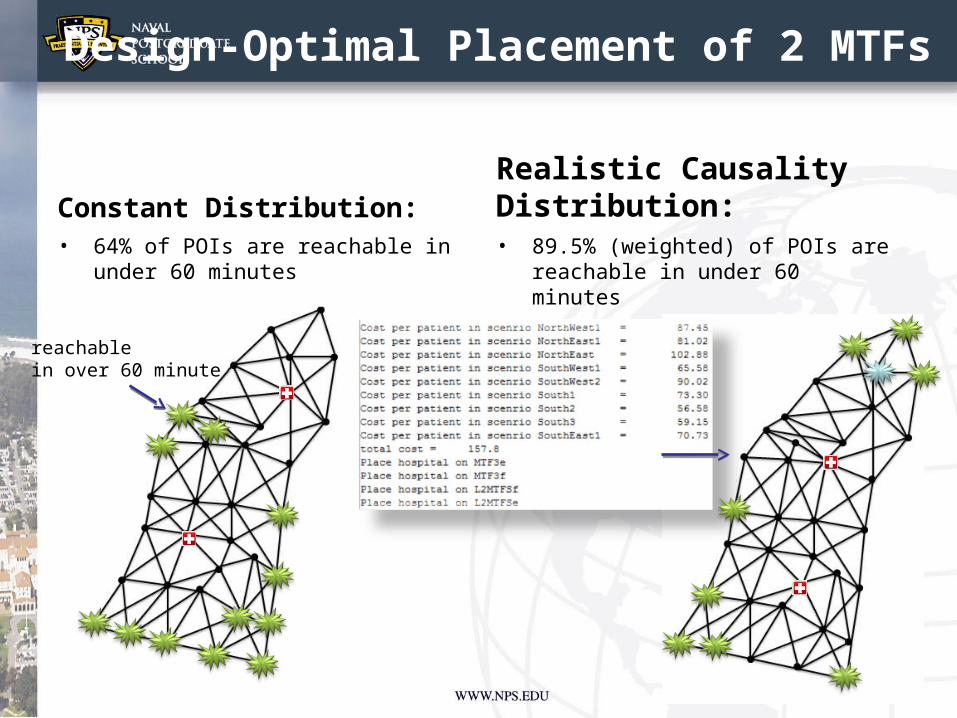
Design-Optimal Placement of 2 MTFs
Constant Distribution: • 64% of POIs are reachable in
under 60 minutes
Realistic Causality Distribution:• 89.5% (weighted) of POIs are
reachable in under 60 minutes
24
reachablein over 60 minute
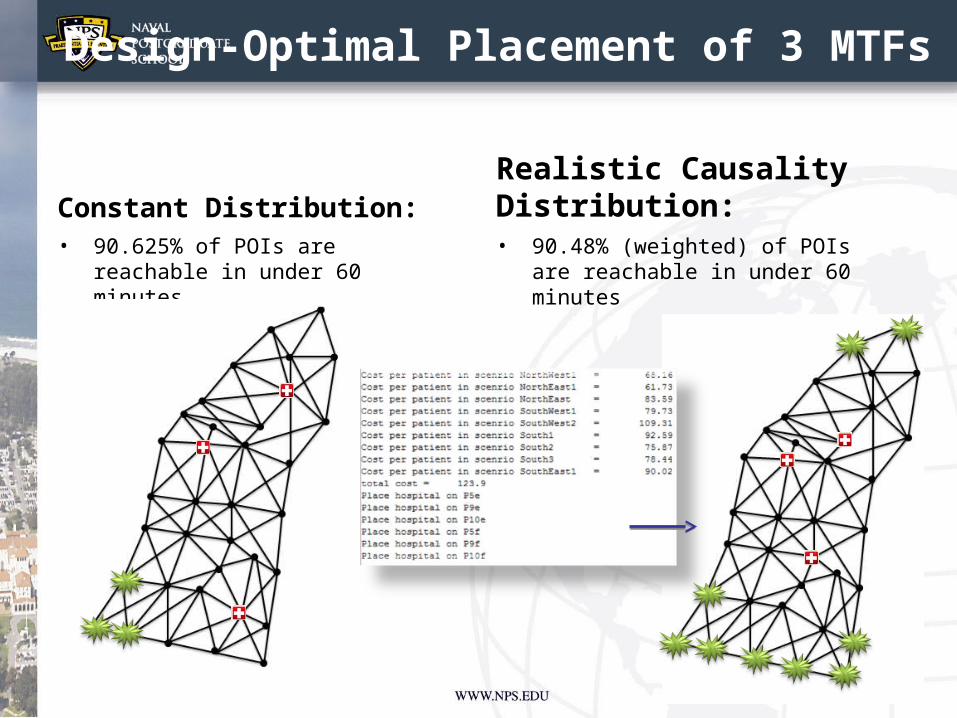
Design-Optimal Placement of 3 MTFs
Constant Distribution: • 90.625% of POIs are
reachable in under 60 minutes
Realistic Causality Distribution:• 90.48% (weighted) of POIs
are reachable in under 60 minutes
25
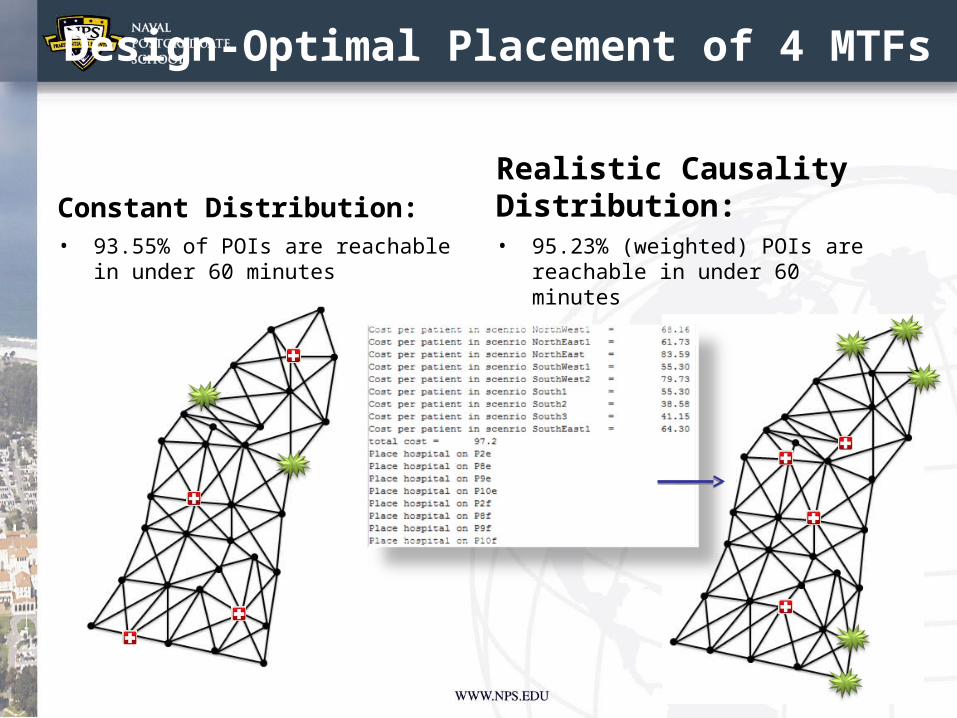
Design-Optimal Placement of 4 MTFs
Constant Distribution: • 93.55% of POIs are reachable
in under 60 minutes
Realistic Causality Distribution:• 95.23% (weighted) POIs are
reachable in under 60 minutes
26
Design Analysis
• Optimal placement of MTFs under constant distribution increases our ability to reach patients in under 60 minutes.– Original Placement of 4 MTFs: 87.1%– New Placement of 3 MTFs: 90.625% – New Placement of 4 MTFs: 93.55%
• Optimal placement of MTFs under realistic causality distribution increases our ability to reach patients in under 60 minutes.– New Placement of 3 MTFs: 90.48%– New Placement of 4 MTFs: 95.23% 27
Conclusions
• Current MTF placement is very close to the optimal position suggested by our model.
• Interdiction is probably not the best model for this network.
• If interdiction model was desired one that models weather would be more appropriate.
Update 7 June 2007 28
Conclusions
• Network should be reevaluated as the battle space evolves.
• Political and historical factors will be considered in facility placement by decision makers.
• Combined or Joint Operations adds more complexity (more medevac platforms types, country caveat constraints, medical rules of eligibility, etc.)
Update 7 June 2007 29
Questions
• Questions?


















