MedEd Histopathology Revision Lecture 2013 Part 1 · What is the differential diagnosis for acute...
130
Part 1 26 th March 2013 H ISTOPATHOLOGY ICSM M ED E D 5 TH Y EAR R EVISION S ERIES 2013 M R G UY M ARTIN MBBS BS C MRCS C ORE S URGICAL T RAINEE T HE R OYAL L ONDON & S T B ARTHOLOMEW ’ S H OSPITAL
Transcript of MedEd Histopathology Revision Lecture 2013 Part 1 · What is the differential diagnosis for acute...

Part 126 th March 2013
HISTOPATHOLOGYICSM MEDED 5TH YEAR REVISION SERIES 2013
MR GUY MARTIN MBBS BSC MRCSCORE SURGICAL TRAINEE
T HE R OYAL LONDON & S T B ARTHOLOMEW ’ S H OSPITAL

� Revision sessions organised and run by The Medical
Education Society
� We are not examiners / lecturers
� These lectures are not formal Imperial College lectures
� No promises about completeness
� General overview, key principles, example questions
� You will require more in depth specific knowledge
� Please fill in the feedback forms!
OVERVIEW

� Why is histopathology important, I want to be a GP?
� You have an exam to pass
� Why do people from Tanzania get squamous cell carcinoma and not
transitional cell carcinoma of the bladder?
� What is Bielschowsky’s stain used for?
� It is very important in day to day clinical practice – the essence of
clinical medicine and surgery
� What is the differential diagnosis for acute onset abdominal pain?
� Why is it important to recognise and treat a CVA as soon as possible?
� 2 sessions - Tuesday 26th and Thursday 28th March
� General principles of histopathology
� System specific histopathology
OVERVIEW
� General principles
� System specific pathology
� Cardiovascular
� Bone and joint
� Connective tissue
� Breast
� Neurological and cerebrovascular
� Respiratory
� GI Tract
� Hepatobiliary and pancreas
� Genitourinary tract
OVERVIEW

GENERAL PRINCIPLES OF
HISTOPATHOLOGY
“While there are several chronic diseases more destruct ive
to l i fe than cancer, none is more feared”
- Charles Mayo 1926

• Transitional cell carcinoma of the bladder
• Melanoma
• Basal cell carcinoma
• Breast cancer
• Colon polyp – tubular adenoma
A. Affects 1:12 women
B. Affects 1:250 women
C. Can be treated with local polyp resection
D. Can only occur in mucous membranes
E. Does not metastasise
F. If malignant, resection is the only treatment
G. Only occurs in the skin
H. Superficial tumour are high grade & associated with poor prognosis
I. Superficial tumours are low grade and associated with good prognosis
EMQ - TUMOURS
• Transitional cell carcinoma of the bladder - I
• Melanoma - D
• Basal cell carcinoma - E
• Breast cancer - A
• Colon polyp – tubular adenoma - C
A. Affects 1:12 women
B. Affects 1:250 women
C. Can be treated with local polyp resection
D. Can only occur in mucous membranes
E. Does not metastasise
F. If malignant, resection is the only treatment
G. Only occurs in the skin
H. Superficial tumour are high grade & associated with poor prognosis
I. Superficial tumours are low grade and associated with good prognosis
EMQ - TUMOURS
� “A specialty concerned with the nature and cause of
disease as expressed by changes in cellular or tissue
structure and function caused by the disease process”
� Histopathology – examination of tissues
� Cytopathology – examination of isolated cells
� “Disease is not something personal and special, but only a
manifestation of life under modified conditions, operating
according to the same laws as apply to the living body at
all times, from the first moment until death”
- Rudolph Virchow
GENERAL PRINCIPLES
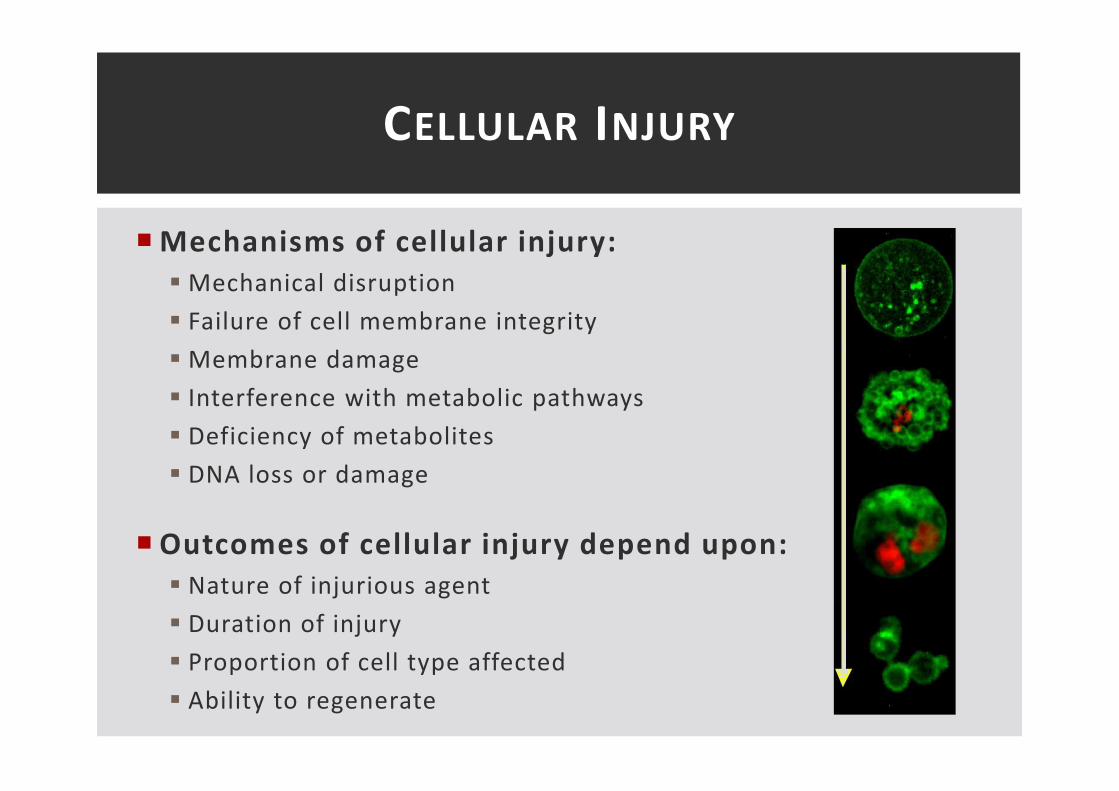
� Mechanisms of cellular injury:
� Mechanical disruption
� Failure of cell membrane integrity
� Membrane damage
� Interference with metabolic pathways
� Deficiency of metabolites
� DNA loss or damage
� Outcomes of cellular injury depend upon:
� Nature of injurious agent
� Duration of injury
� Proportion of cell type affected
� Ability to regenerate
CELLULAR INJURY

CELL DEATH - APOPTOSIS VS NECROSIS
� Cell death – “irreversible loss of the cell’s ability to
maintain independence from the environment”
Apoptosis Necrosis
Induction Physiological/pathological Pathological
Extent Single cells Groups of cells
Biochemical
Energy dependent fragmentation
of DNA
Lysosomes intact
Impairment/cessation of ion
homeostasis
Lysosome lytic enzyme release
Cell membrane integrity Preserved Lost
Morphology
Cell shrinkage and apoptosis with
dense chromatin filled apoptotic
bodies
Cell swelling and lysis
Inflammatory response None Usual
Fate of dead cellsPhagocytosed by neighbouring
cells
Phagocytosed by
neutrophils/macrophages
� Regeneration – total healing with restitution of
original tissue structure and function
� Labile cells – good capacity for regeneration
� Stable cells – divide at slow rate under physiological conditions
� Permanent cells – no capacity for regeneration
� Repair – repair via formation of mature connective
tissue; fibrous organisation and scarring
HEALING – REGENERATION VS REPAIR

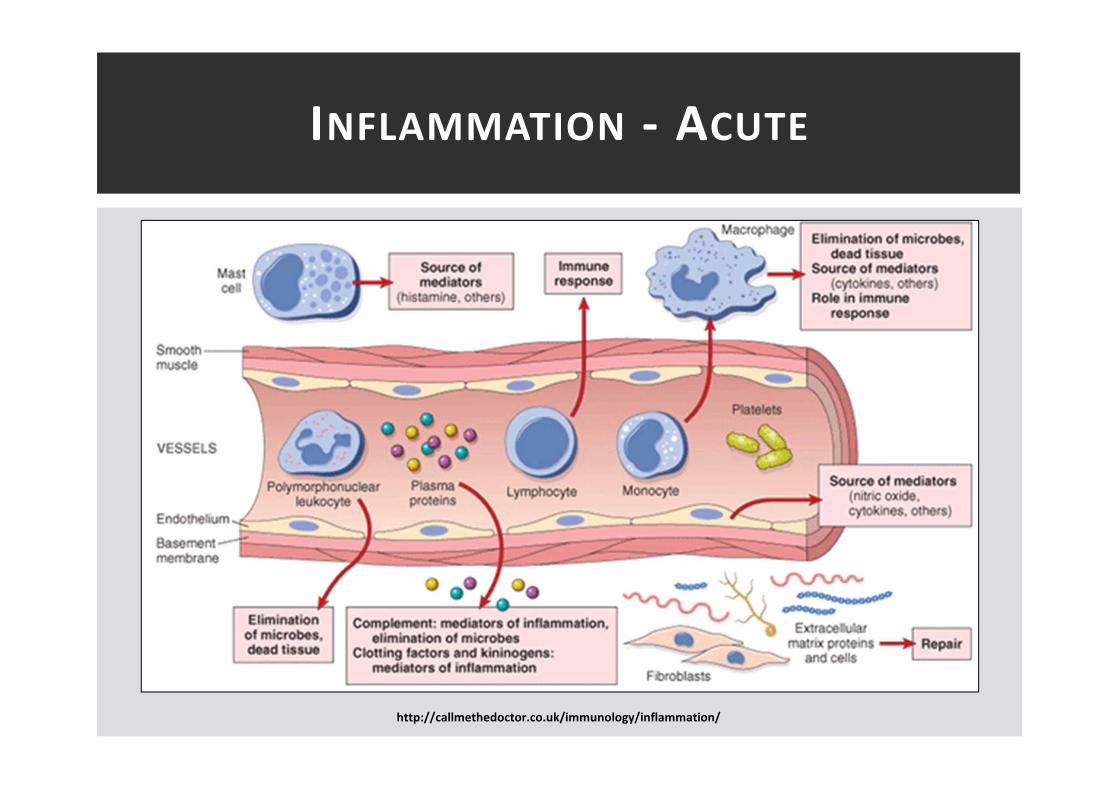
� Acute inflammation - initial transient reaction to
injury
� 3 principle phases
� Vascular phase: change in vascular caliber and permeability
� Exudative cellular phase: formation cellular exudate
� Outcome: resolution, suppuration, organisation, chronicity
� Macroscopic signs and symptoms
� Rubor (redness)
� Calor (heat)
� Tumour (swelling)
� Dolor (pain)
� Functio laesa (loss of function)
INFLAMMATION - ACUTE
INFLAMMATION - ACUTE
http://callmethedoctor.co.uk/immunology/inflammation/

� Chronic inflammation – prolonged tissue reaction to to
injury with formation of different cellular infiltrate
from acute inflammation
� Lymphocytes, plasma cells, macrophages predominant
� Usually primary, may follow acute inflammation
� Macroscopic appearances:
� Chronic ulceration
� Chronic abscess
� Granulomatous inflammation
� Fibrosis
� Thickening of hollow viscus
INFLAMMATION - CHRONIC

� Positive effects
� Dilution of toxins
� Migration/infiltration of immucological cells + Ab’s
� Initiation of coagulation cascade (initiation of fibrin clots)
� Increased delivery of oxygen/nutrients for repair
� Harmful effects
� Damage to local healthy tissue
� Swelling and compression of local structures
� Fibrosis/scarring
� Systemic response - SIRS
� Hypersensitivity
INFLAMMATION
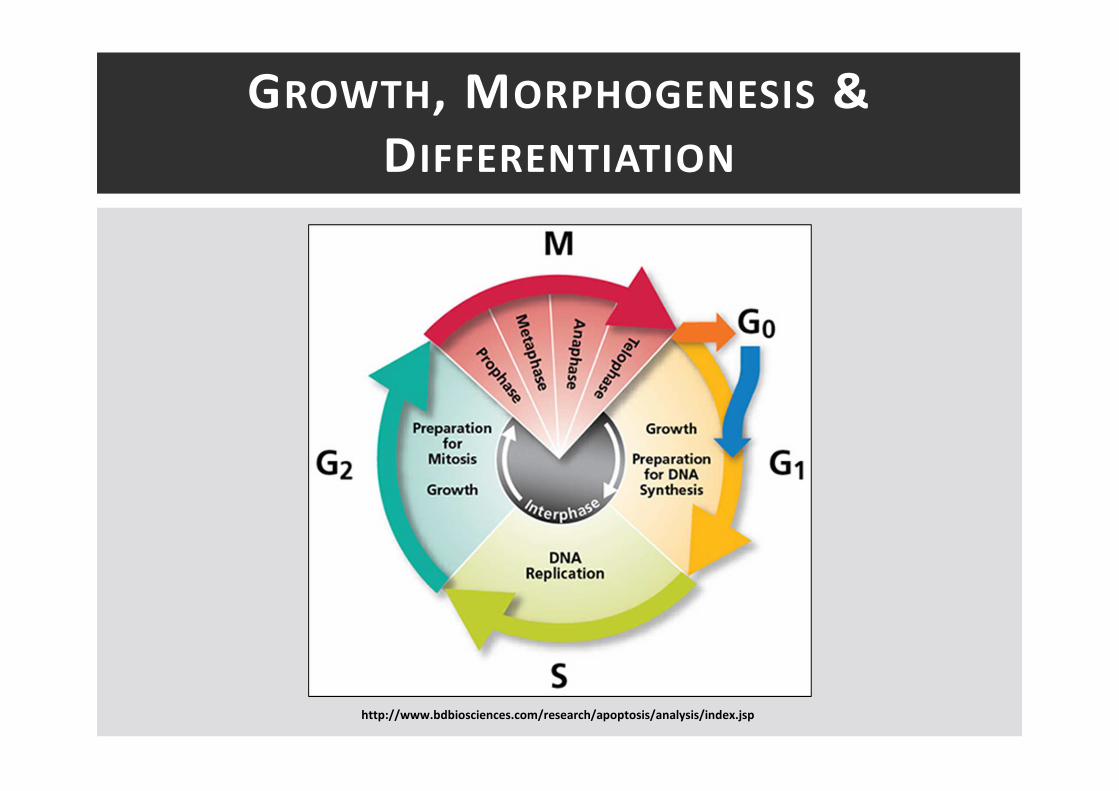
GROWTH, MORPHOGENESIS &
DIFFERENTIATION
http://www.bdbiosciences.com/research/apoptosis/analysis/index.jsp
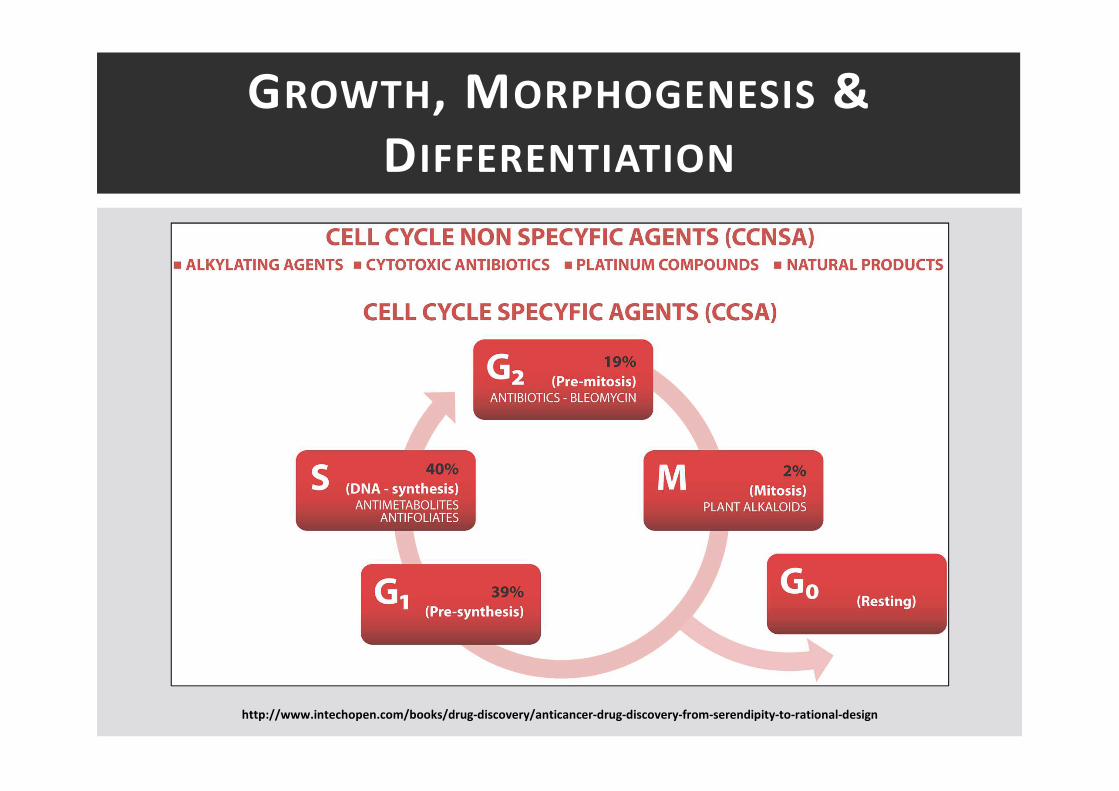
GROWTH, MORPHOGENESIS &
DIFFERENTIATION
http://www.intechopen.com/books/drug-discovery/anticancer-drug-discovery-from-serendipity-to-rational-design

� Hypertrophy – increase in cell size
� Hyperplasia – increase in cell number
� Atrophy – decrease in size due to loss of cells or
reduction in cell size
� Hypoplasia – failure of an organ to attain normal size
� Aplasia – failure of development of an organ
� Atresia – failure of development of a lumen in a
normally tubular structure
GROWTH – KEY PRINCIPLES
� Genetic factors
� Hormones
� Nutrition
� Blood supply
� Oxygen supply
� Nerve supply
� Growth factors
FACTORS AFFECTING GROWTH

� Process by which a cell develops a specialised function
and structure
� Control of differentiation
� Genes, hormones, growth factors
� Differentiation may be disturbed by environmental
teratogens
� Irradiation, drugs, infections
DIFFERENTIATION

� Metaplasia – reversible transformation of a terminally
differentiated cell into another cell type
� Dysplasia – premalignant condition characterised by
cell growth, cellular atypia and decreased
differentiation
� Neoplasia – abnormal and excessive un-cordinated cell
growth autonomous of normal growth controls
ACQUIRED DISORDERS OF
DIFFERENTIATION

DYSPLASIA
http://en.wikipedia.org/wiki/Dysplasia

� Carcinogenesis – conversion of normal cells to those
capable of forming neoplasms
� Carcinogen – agent known/suspected to participate in
the causation of tumours
� Carcinogenic: cancer causing (malignant)
� Oncogenic: tumour causing (benign + malignant)
� Host factors and carcinogenesis
� Race, diet, inherited pre-disposition, age, gender
CARCINOGENESIS

� Multi-step process
� Latency: causal event followed by latent period
� Initiation: development of irreversible neopalstic potential
� Promotion: event stimulating clonal proliferation
� Persistence: continued growth independent of initiators and
promoters
� Oncogenes – genes whose presence in certain forms
stimulates development of cancer
� Tumour suppressor genes – normal genes whose
absence can lead to development of cancer
CARCINOGENESIS
NEOPLASIA
� Neoplasia – abnormal and excessive un-cordinated cell
growth autonomous of normal growth controls
� Classification
� Behavioural: benign vs malignant
� Histogenetic: cell origin, differentiation
� Major categories
� Epithelial cells – adenoma/papilloma vs
adenocarcinoma/carcinoma
� Mesenchymal cells – -oma va sarcoma
� Lymphoid/haemopoietic cells
NEOPLASIA
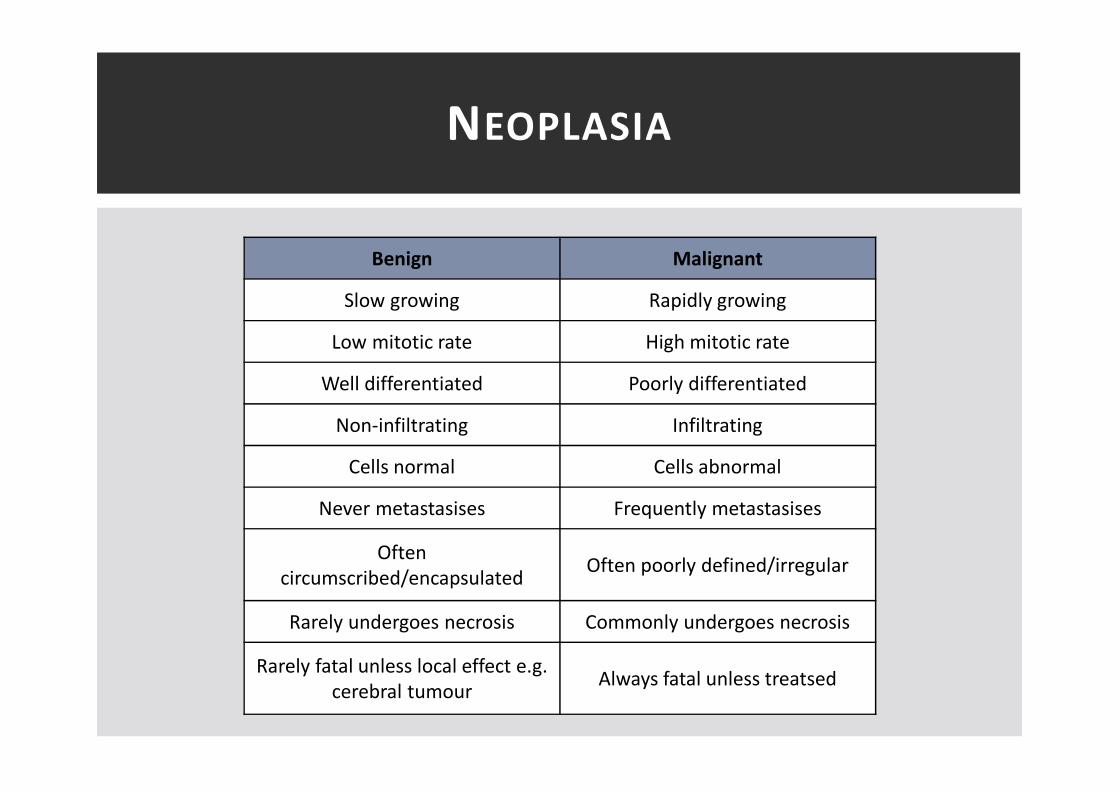
Benign Malignant
Slow growing Rapidly growing
Low mitotic rate High mitotic rate
Well differentiated Poorly differentiated
Non-infiltrating Infiltrating
Cells normal Cells abnormal
Never metastasises Frequently metastasises
Often
circumscribed/encapsulatedOften poorly defined/irregular
Rarely undergoes necrosis Commonly undergoes necrosis
Rarely fatal unless local effect e.g.
cerebral tumourAlways fatal unless treatsed

CARDIAC & VASCULAR
PATHOLOGY
“I think the worst t ime to have a heart attack is during a
game of charades”
- Demitri Mart in

� A 46 year old man presents with progressive heart
failure and AF. His previous discharge summaries show
multiple admissions in the last year – Upper GI bleed,
Boxer ’s Fracture, Head Injury. XR – enlarged heart
shadow
a) Restrictive cardiomyopathy
b) Hypertrophic cardiomyopathy
c) Dilated cardiomyopathy
EMQ - CARDIOMYOPATHY

� A 46 year old woman with progressive heart failure. No
cardiac risk factors, is a non smoker and doesn’t drink
alcohol. Arthritis of her MCP joints, and her renal
function has been deteriorating on her last 2 blood
tests. Histology – pale pink amorphous material
between myocardial fibres
a) Restrictive cardiomyopathy
b) Hypertrophic cardiomyopathy
c) Dilated cardiomyopathy
EMQ - CARDIOMYOPATHY

� Thrombosis, embolism & infarction
� Atherosclerosis
� Acute coronary syndrome
� Cardiac failure
� Cardiomyopathy
� Rheumatic fever and endocarditis
� Valvular heart disease
� Hypertension
CARDIAC & VASCULAR PATHOLOGY
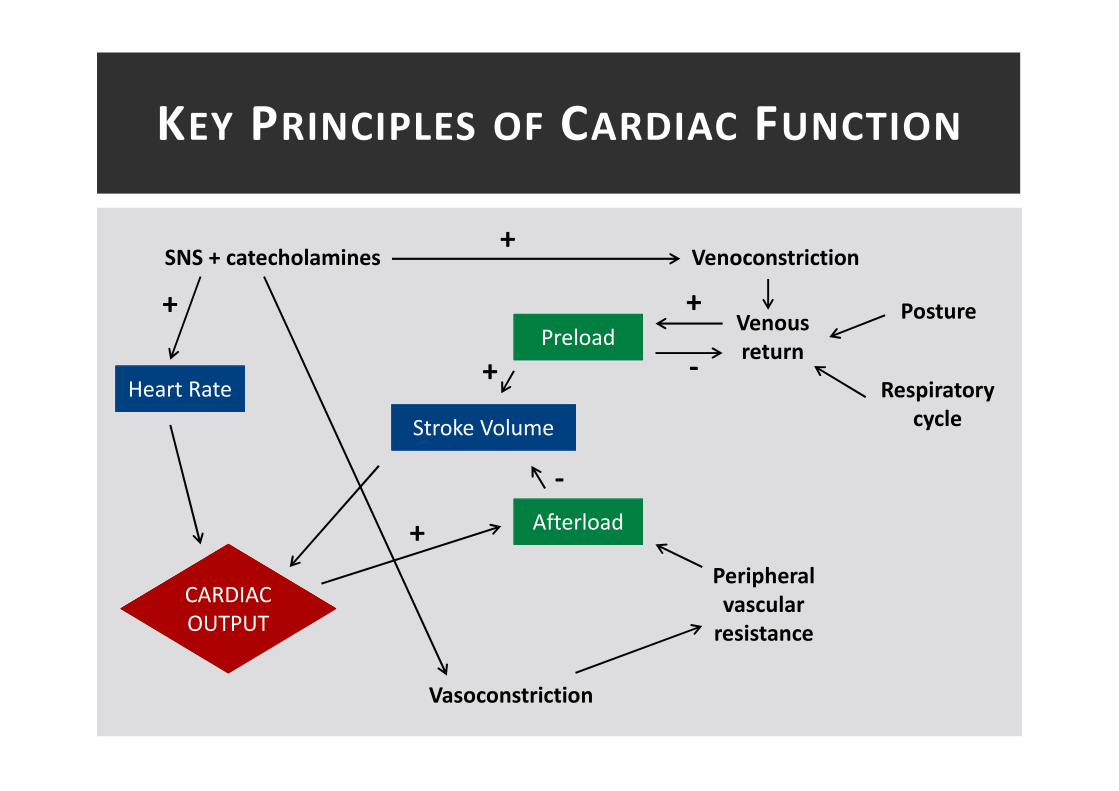
KEY PRINCIPLES OF CARDIAC FUNCTION
CARDIAC
OUTPUT
Heart Rate
Stroke Volume
Afterload
Preload
SNS + catecholamines
Vasoconstriction
Peripheral
vascular
resistance
Venous
return
Venoconstriction
Posture
Respiratory
cycle
+
+
+
+
-
+
-

� Thrombosis – “a pathological event when the
haemostatic system is abnormally active”
� Solid mass formed within the circulation
THROMBOSIS
� Embolism – “detached
mass within the
circulation”
� Thrombus
� Gas
� Fat
� Tumour
� Amniotic fluid
� Foreign body
� Therapeutic
EMBOLISM
� Ischaemia – “inadequate supply of oxygenated blood
to tissues or organs for its metabolic needs”
� General – shock
� Local – arterial, venous or small vessel obstruction
� Severity – speed of onset, extent of obstruction, presence of
collateral supply, metabolic requirements of tissues
� Infarction – “necrosis of tissue due to irreparable
ischaemic damage”
� White infarct: arterial
� Red infarct: venous
� Low-flow infarction: relative ischaemia
ISCHAEMIA & INFARCTION

� Atherosclerosis – “chronic
inflammation of the intima of
large arteries characterised by
plaque deposition, wall
thickening and loss of elasticity”
� Arterioloscelerosis: small/medium
vessels
� Calcific sclerosis: calcification of
small/medium vessels
� Responsible for more deaths
worldwide than all forms of
cancer
ATHEROSCLEROSIS
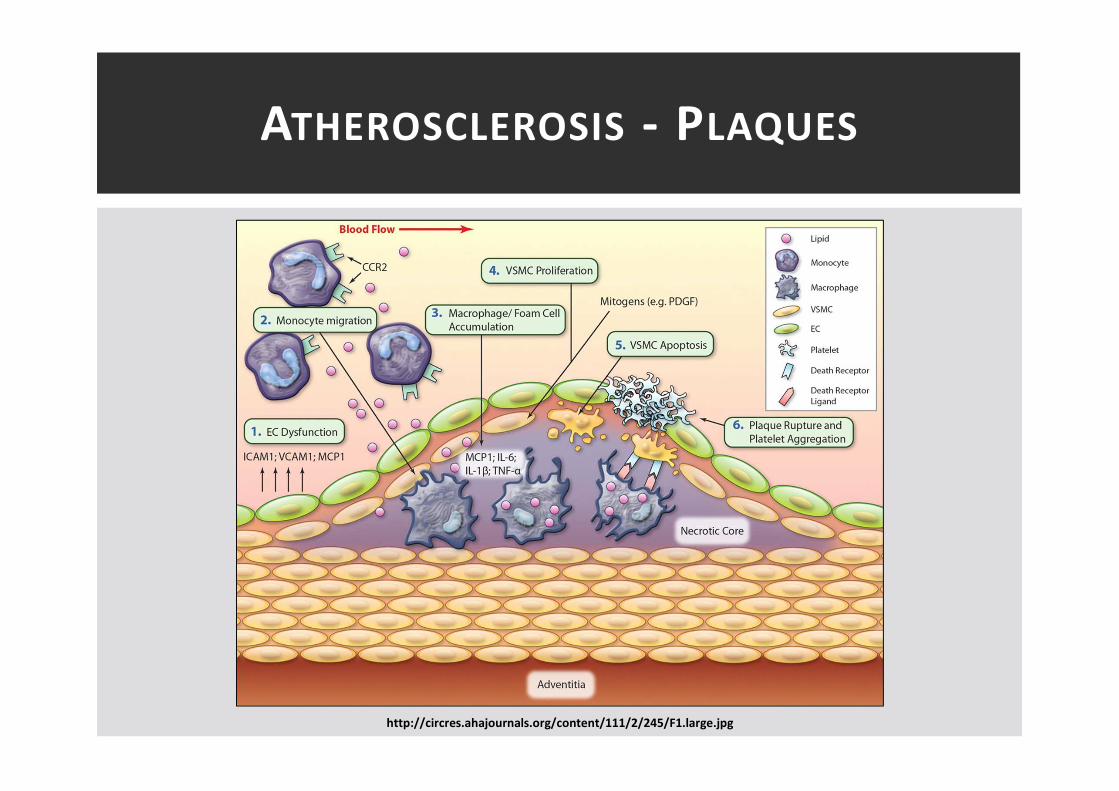
ATHEROSCLEROSIS - PLAQUES
http://circres.ahajournals.org/content/111/2/245/F1.large.jpg

http://en.wikipedia.org/wiki/File:Endo_dysfunction_Athero.PNG

ATHEROSCLEROSIS – RISK FACTORS
Key Risk Factors
Smoking
Hypertension
Diabetes
Hyperlipidaemia
Sedentary lifestyle
Age
Family history
� Key risk factors
� Modifiable vs non-modifiable
� Sheer stress
� Sideways force on endothelium
� Modulates endothelial function
� High laminar flow protective
� Low turbulent flow atherogenic

ATHEROSCLEROSIS - HYPERLIPIDAEMIA
� Low density lipoprotein (LDL)� “bad” – carries
cholesterol from liver to tissues
� Oxidised LDL principal agent in atherosclerosis
� High density lipoprotein (HDL)� “good” – carries
cholesterol from tissues to liver
� Converted to bile acids and catabolised in the liver
� Under negative feedback
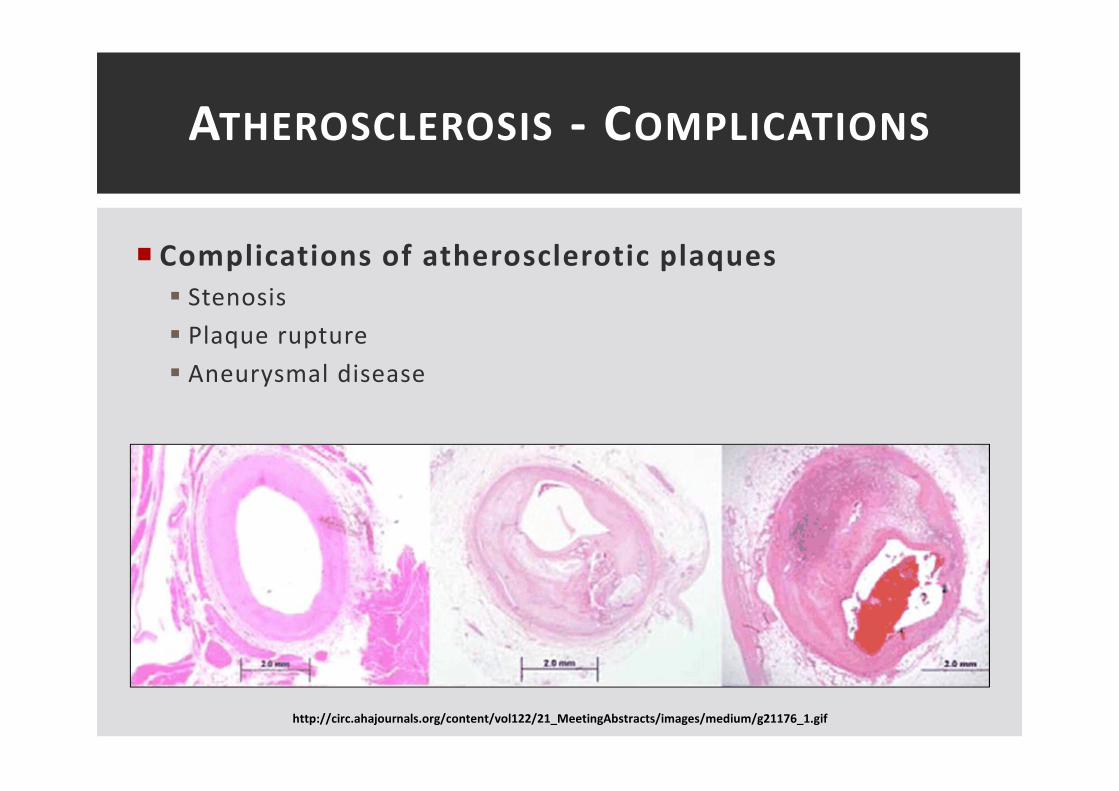
ATHEROSCLEROSIS - COMPLICATIONS
� Complications of atherosclerotic plaques
� Stenosis
� Plaque rupture
� Aneurysmal disease
http://circ.ahajournals.org/content/vol122/21_MeetingAbstracts/images/medium/g21176_1.gif

ACUTE CORONARY SYNDROME

ACUTE CORONARY SYNDROME
Clinical features suggestive of ACS
ECG
STEMI
Unstable Angina NSTEMI
Cardiac
Enzymes
ST-elevation / LBBB
/ Posterior MI
ECG changes
+ve-ve
Risk Stratification
- ST elevation >1mm in >2 limb leads
- ST elevation >2mm in >2 chest leads
- LBBB
- Posterior ST depression + R-waves V1-V3
Morphine + Oxygen
Nitrates
Aspirin 300mg
Clopidogrel 300/600mg
+/- LMWH – fondaparinux/enoxaparin

http://eurheartj.oxfordjournals.org/content/28/13/1598/F14.expansion

ACS- ENZYMES
http://www.bpac.org.nz/resources/bt/2009/december.asp
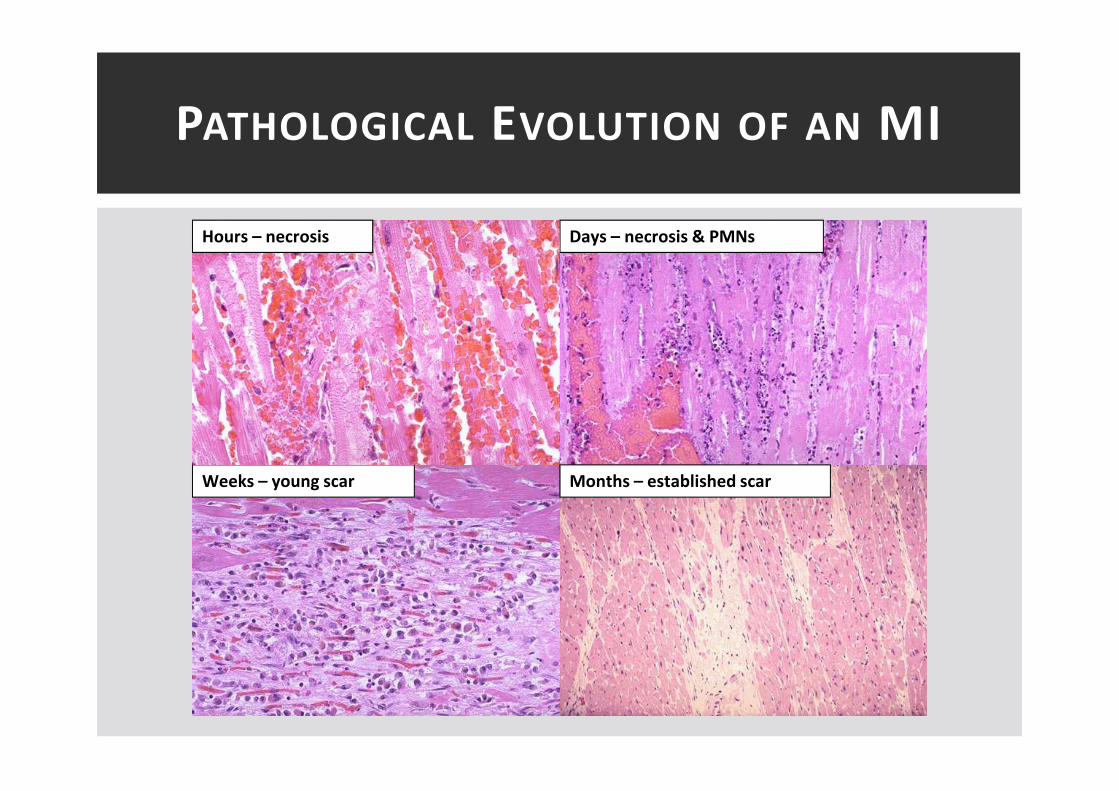
PATHOLOGICAL EVOLUTION OF AN MI
Weeks – young scar
Days – necrosis & PMNsHours – necrosis
Months – established scar
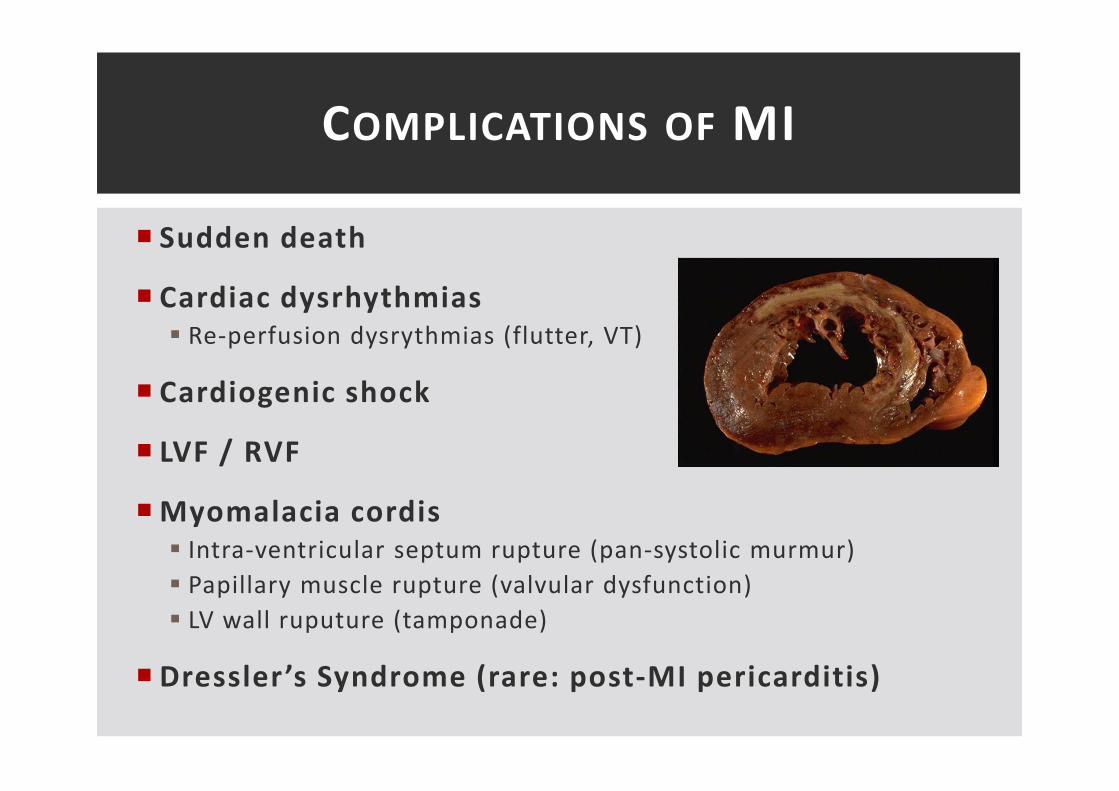
� Sudden death
� Cardiac dysrhythmias
� Re-perfusion dysrythmias (flutter, VT)
� Cardiogenic shock
� LVF / RVF
� Myomalacia cordis
� Intra-ventricular septum rupture (pan-systolic murmur)
� Papillary muscle rupture (valvular dysfunction)
� LV wall ruputure (tamponade)
� Dressler’s Syndrome (rare: post-MI pericarditis)
COMPLICATIONS OF MI

� CO inadequate for the body’s requirements
� Poor prognosis: 25-50% 5yr mortality
� 1-3% of population. 10% elderly population
� Systolic vs diastolic
� Right vs left
� Low output vs high output
� Acute vs chronic
� NYHA Classification
� I-IV
CARDIAC FAILURE

CARDIAC FAILURE
http://www.mc.uky.edu/pharmacology/instruction/pha824hf/pha824hf.html

LVF VS RVF
Right Ventricular Failure Left Ventricular Failure
Causes
LVF, pulmonary stenosis,
chronic lung disease (COPD,
PAH, fibrosis)
IHD, HTN, valvular disease, MI
Symptoms
Portal, systemic and
peripheral congestion
(pulmonary oedema, ascites,
facial engorgement), TR
Dyspnoea, reduced ET,
fatigue, PND, orthopnoea,
pulmonary oedema, cardiac
asthma, cool peripheries,
muscle wasting
� Key principles of management:
� Treat the cause + exacerbating factors
� Diuretics + ACE-i + β-blockers + spironolactove

� Intrinsic disease of heart
muscle
� Classification
� Physiological abnormality
� Underlying cause
� Clinical features:
� Sudden death / palpitations
� IHD symptoms
� Cardiac failure
CARDIOMYOPATHY

� Left ventricular hypertrophy (HOCM)
� Heavy muscular hypertrophy with poor compliance
� 0.2-0.5% population
� Enlargement of sarcomeres with disruption of alignment
� 50% familial (autosomal dominant, variable penetrance)
� Reduced LV outflow tract
� Presentation
� Arrhythmias
� LV outflow obstruction
� Cardiac failure
� Sudden death
HYPERTROPHIC CARDIOMYOPATHY
� 4 chamber dilatation and hypertrophy
� Progressive loss of myocytes
� Dilation + heart failure + arrhythmias
� 0.2% population
� 40% mortality at 2yrs
� Common causes
� Idiopathic – most common
� Genetic – autosomal dominant most common
� Infective – viral myocarditis
� Toxic – alcohol, chemotherapy (doxrubacin, herceptin), iron
DILATED CARDIOMYOPATHY
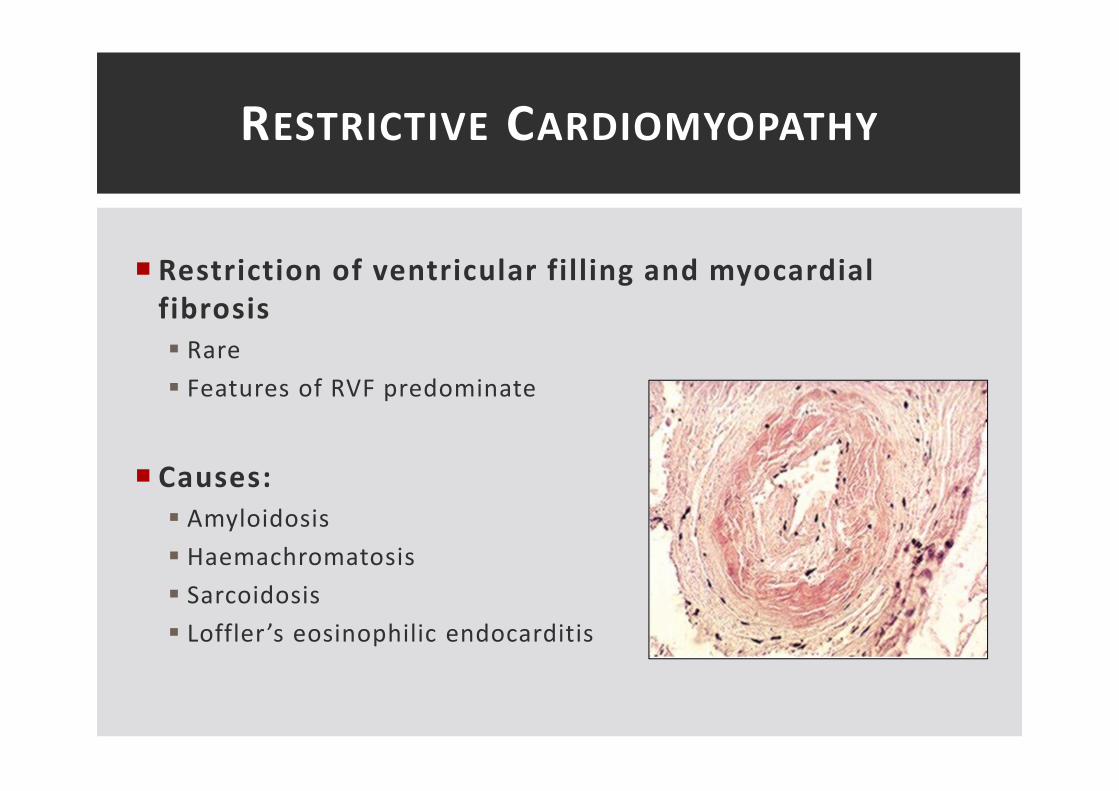
� Restriction of ventricular filling and myocardial
fibrosis
� Rare
� Features of RVF predominate
� Causes:
� Amyloidosis
� Haemachromatosis
� Sarcoidosis
� Loffler’s eosinophilic endocarditis
RESTRICTIVE CARDIOMYOPATHY

� A young Portuguese gentleman presents very unwell
with a high fever and fulminant TR. Blood cultures grow
Staph Aureus. Echo – large irregular vegetations
extending to the chordae
A. Acute Rheumatic Fever
B. Chronic Rheumatic fever
C. Acute Infective Endocarditis
D. Sub-acute Infective Endocarditis
E. Non-infective Endocarditis
F. Libman Sacks Endocarditis.
EMQ – VALVULAR PATHOLOGY

� A young woman presents with joint pains, a malar rash
and mitral regurgitation. ASOT negative. Blood cultures
negative. Echo shows small warty vegetations found
along the lines of closure.
A. Acute Rheumatic Fever
B. Chronic Rheumatic fever
C. Acute Infective Endocarditis
D. Sub-acute Infective Endocarditis
E. Non-infective Endocarditis
F. Libman Sacks Endocarditis
EMQ – VALVULAR PATHOLOGY

� A young woman presents with joint pains and a rash.
The rash is geographical, has raised red edges and a
clear centre. She also has mitral regurgitation. ASOT
positive. Blood cultures negative. Echo shows small
warty vegetations. Histology – Sterile vegetations.
A. Acute Rheumatic Fever
B. Chronic Rheumatic fever
C. Acute Infective Endocarditis
D. Sub-acute Infective Endocarditis
E. Non-infective Endocarditis
F. Libman Sacks Endocarditis
EMQ – VALVULAR PATHOLOGY

� Systemic infection
� Group-A β-haemolytic streptococci pharyngitis
� Ab cross-reactivity to valvular tissue (2-4/52 in 2% population)
� Modified Jones Criteria
� Evidence strep infection + 2 major / 1 major + 2 minor
RHEUMATIC FEVER
Evidence Group-A Strep
InfectionMajor Criteria Minor Criteria
Positive throat culture Carditis Fever
Rapid strep Ag test +ve Arthritis Raised CRP/ESR
Elevated strep Ab titre Subcutaneous nodules Arthralgia
Recent scarlet fever Erythema marginatum Prolonged PR interval
Sydenham’s chorea Previous rheumatic fever

� Aschoff bodies: acute foci of fibrinoid necrosis
� MacCalllum plaques - chronic subendocardial Aschoff collections
� 60% develop chronic rheumatic heart disease
� Thickening valve leaflet, thickening/shortening chordae tendinae
� MV (70%), AV (40%), TV (10%) PV (2%)
RHEUMATIC FEVER

� Fever + new murmur = endocarditis until proven
otherwise
� Infective
� Acute / sub-acute,
� Bacterial / fungal
� Non-infective – Libman-Sacks (SLE), Marantic (non-bacterial
thrombotic), verrucous (acute rheumatic fever)
ENDOCARDIDITIS
Acute Sub-acute
Staph aureus Strep viridans (>35% all cases)
Very virulent with acute course
5-50% mortality in weeks (age / embolic events)
Chronic, sub-acute course
Mortality in months
Previously normal valves Prosthetic valves / pre-existing valve damage
IV drug users / instrumentation Linked with dental infection

� Duke Criteria
� 2 major
� 1 major + 3 minor
� All 5 minor
ENDOCARDITIS
Major Criteria Minor Criteria
Positive blood culture
- Typical organism in >2 cultures
- 3x positive cultures >12hrs apart
Predisposition
Fever >38°c
Endocardium involvement
- Positive echo (vegetation, abscess,
dehiscence prosthetic valve)
- New valvular regurgitation
Vascular/immunological signs
+ve culture not major criteria
+ve echo not major criteria

� Cardiac complications
� Perforation of cusp/leaflet
� Rupture of chordae tendinae
� Abscess
� Fistula
� Outflow tract obstruction
� Most common cause of death is cardiac failure
� Abx prophylaxis is not recommended
� No proven association between intervention and endocarditis
� Risk of adverse reaction greater than endocarditis risk
ENDOCARDIDITS

� Aortic stenosis
� Aortic regurgitation
� Mitral stenosis
� Mitral regurgitation
� Common aetiologies
� Congenital
� Bicuspid valve
� Connective tissue disorders
� Acquired
� Infective - rheumatic fever / endocarditis
� Degenerative – calcification, MI
� Functional – HTN, PHTN
VALVULAR DISEASE

� Aortic stenosis
� Incomplete opening / narrowing of valve
� Valve area - mild (>1.5cm2), Critical (<0.5cm2)
� Pressure gradient (ventricular pressure > aortic pressure)
� Mild (<25mmHg), Critical (>80mmHg)
� Common causes
� Acquired – rheumatic fever
� Degenerative – calcification of valve cusps
� Congenital – bicuspid valve
� Classical triad – angina, syncope, heart failure
AORTIC VALVE DISEASE - STENOSIS

� Aortic regurgitation
� Valve incompetence
� Common causes:
� Acute – infective endocarditis, aortic dissection, trauma
� Chronic – congenital, connective tissue disorders, rheumatic fever,
vasculitis, rheumatoid arthritis, SLE, HTN
� Reduce systolic HTN
� Valve replacement prior to LV dysfuction
AORTIC VALVE DISEASE - REGURGITATION

� Mitral stenosis:
� Incomplete opening / narrowing of valve
� Valve area - <2cm2 (normal = 4-6cm2)
� Presentation: dyspnoea, fatigue, palpitations, chronic bronchitis
like picture
� Common causes:
� Rheumatic fever, congenital
� Complications
� PHTN, embolic disease, local mass effects
MITRAL VALVE DISEASE - STENOSIS
� Mitral regurgitation
� Valve incompetence
� Common causes:
� Functional - LV dilation
� Acquired - rheumatic fever, infective endocarditis, papillary
muscle/chordae tendinae rupture/damage
� Degenerative - annular calcification
� Congenital - connective tissue disorders, congenital defects
� Control AF, fluid offload, valve replacement
MITRAL VALVE DISEASE - REGURGITATION
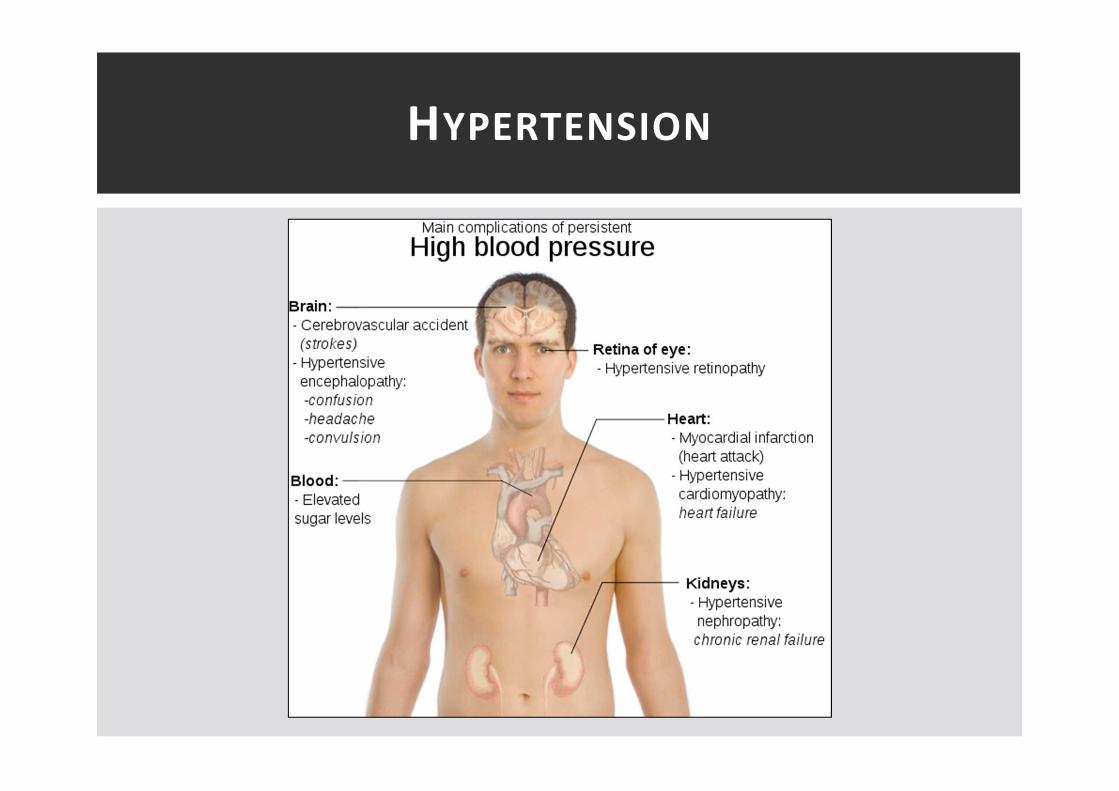
� “Blood pressure at which benefit of treatment
outweighs the risk”
� 140/90 (additional risk factors) OR 160/100 (absolute)
� Thickening of intima/elastic lamina due to arteriosclerosis –
chronic low grade ischaemia
� Primary
� Idiopathic / essential = 95%
� Secondary
� Renal disease, endocrine drisease (Conn’s, phaeochromocytoma,
hyperthyroidism, Cushing’s)
� Pregnancy
� Drugs
HYPERTENSION

HTN – DIAGNOSIS / MANGEMENT
CBPM ≥160/100 mmHg
& ABPM/HBPM
≥ 150/95 mmHg
Stage 2 hypertension
Consider specialist referral
Offer antihypertensive drug treatment
Offer lifestyle interventions
If younger than 40 years
If target organ damage present or 10-
year cardiovascular risk > 20%
Offer annual review of care to monitor blood pressure, provide support and discuss lifestyle, symptoms and medication
Offer patient education and interventions to support adherence to treatment
CBPM ≥140/90 mmHg &
ABPM/HBPM
≥ 135/85 mmHg
Stage 1 hypertension

HTN TREATMENT ALGORITHM
Aged over 55 years or
black person of
African or Caribbean
family origin of any
age
Aged under
55 years
C2A
A + C2
A + C + D
Resistant hypertension
A + C + D + consider further diuretic or
alpha- or beta-blocker
Consider specialist referral
Key
A – ACE inhibitor or low-cost
angiotensin II receptor blocker
(ARB)1
C – Calcium-channel blocker
(CCB)
D – Thiazide-like diuretic
HYPERTENSION

RESPIRATORY TRACT DISEASE
“Asthma is a disease that has pract ical ly the same symptoms
as passion except that with asthma it lasts longer ”
- Anonymous JAMA 1964

� 17yr presents with a cough that wakes her at night. CXR normal.
Peripheral eosinophilia. Histo – smooth muscle hyperplasia
� 35yr with CF. Cough with purulent sputum on most days. He also
c/o decreasing exercise tolerance. O/E he is clubbed and has
bilateral coarse crackles. HRCT gives you the diagnosis
� A 60 year old non-smoker with progressive SOB of several
months duration. O/E clubbed + BL fine end-inspiratory crackles.
HRCT – honeycomb fibrosis
EMQ – COUGH
a) Cryptogenic fibrosingalveolitis
b) Extrinsic allergic alveolitis
c) Pneumonia
d) Asthma
e) Bronchiectasis
f) Occupational Lung disease

� 17yr presents with a cough that wakes her at night. CXR normal.
Peripheral eosinophilia. Histo – smooth muscle hyperplasia - D
� 35yr with CF. Cough with purulent sputum on most days. He also
c/o decreasing exercise tolerance. O/E he is clubbed and has
bilateral coarse crackles. HRCT gives you the diagnosis - E
� A 60 year old non-smoker with progressive SOB of several
months duration. O/E clubbed + BL fine end-inspiratory crackles.
HRCT – honeycomb fibrosis - A
a) Cryptogenic fibrosingalveolitis
b) Extrinsic allergic alveolitis
c) Pneumonia
d) Asthma
e) Bronchiectasis
f) Occupational Lung disease
EMQ – COUGH

� The end point for all respiratory disease
� Type I respiratory failure
� PaO2 <8kPa
� V/Q mismatch
� Pneumonia, PE, asthma, fibrosis, LVF
� Type II respiratory failure
� PaO2 <8kPa + PCO2 >6kPa
� Alveolar hypoventilation +/- V/Q mismatch
� COPD, neuromuscular disease, reduced drive, severe acute
asthma
RESPIRATORY FAILURE

� 95% embolic from deep veins of the legs/pelvis
� Large – massive PE often fatal / right heart failure
� Medium – symptomatic + pulmonary haemorrhage + respiratory
failure
� Small – clinically silent
� Multiple small PE a common cause of pulmonary HTN
� Key signs and symptoms
� SOB, pleuritic chest pain, haemoptysis, syncope
� Pyrexia, tachycardia, tachypnoea, hypotension, raised JVP, pleural
effusion, respiratory failure
� D-dimer, ECG (SI, QIII, TIII or tachycardia/RBBB), CXR, CTPA, V/Q
scan
PULMONARY VASCULAR DISEASE –
PULMONARY EMBOLISM

PULMONARY VASCULAR DISEASE –
PULMONARY EMBOLISM

� Primary pulmonary hypertension
� Idiopathic
� PA pressure >25mmHg at rest
� Young women
� Secondary pulmonary hypertension
� Chronic lung disease, pulmonary vascular disease, thoracic cage
abnormalities, neuromuscular disease, hypoventilation
� Right heart failure – cor pulmonale
� 50% 5yr mortality
PULMONARY VASCULAR DISEASE –
PULMONARY HYPERTENSION

RESPIRATORY AIRWAYS DISEASE
http://www.frca.co.uk/article.aspx?articleid=100023
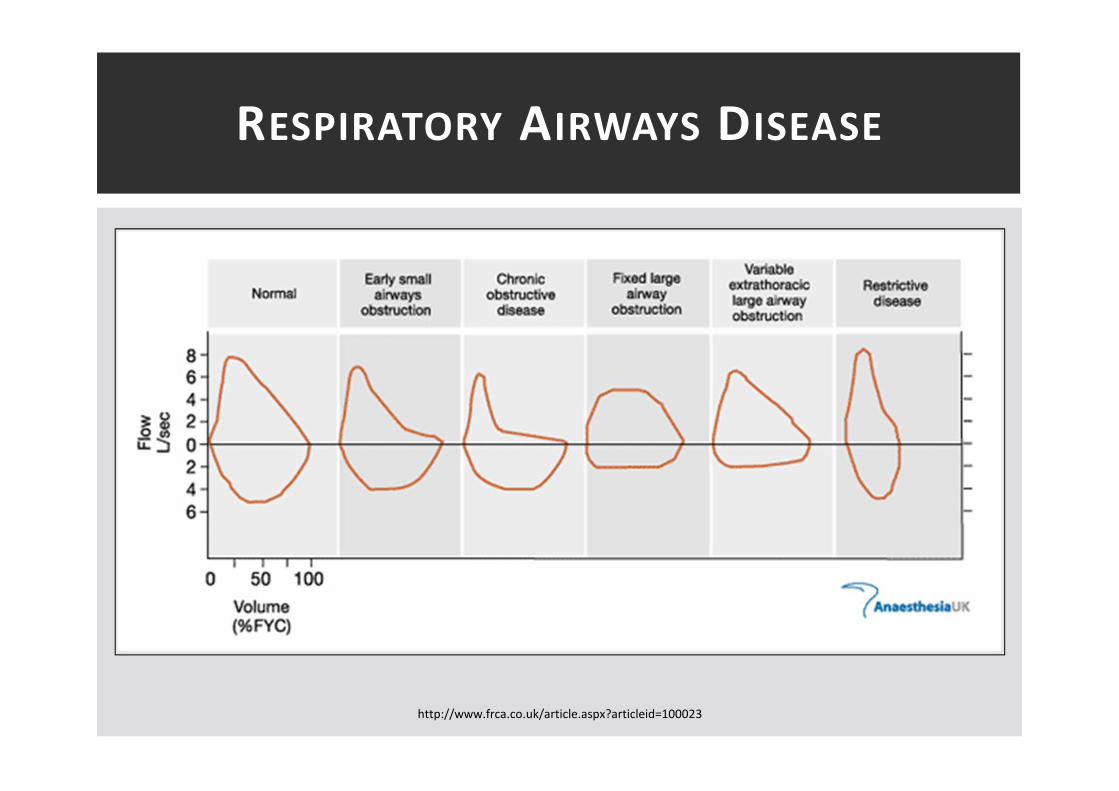
RESPIRATORY AIRWAYS DISEASE
http://www.frca.co.uk/article.aspx?articleid=100023

� Remember the key points
� Kids > adults
� Chronic airways inflammation that is usually reversible
� Part of atopic trait
� Can be severe and life threatening
� Pathology
� Macroscopic – overinflated, patchy atelectasis, mucus plugs
� Microscopic – oedema, inflammatory pulmonary infiltrates,
smooth muscle and mucosal gland hypertrophy
RESPIRATORY AIRWAYS DISEASE -
ASTHMA

� COPD – bronchitis + emphysema
� Bronchitis
� “chronic cough with production of sputum most days, for a least 3 months in 2 consecutive years.”
� Blue bloaters – chronic hypoxia
� Emphysema
� “destruction/dilatation of the lung parenchyma distal to the terminal bronchioles.”
� Pink puffer – increased respiratory effort
� Smokers / A1AT
RESPIRATORY AIRWAYS DISEASE - COPD

� Emphysema
� Panacinar – affects whole lobule
� A1AT deficiency
� Centrolobular– part of lobule
� Upper respiratory tree
� Smokers
� Complications
� Bullae formation
� Pneumothorax
� Cor-pulmonale
RESPIRATORY AIRWAYS DISEASE - COPD

RESPIRATORY AIRWAYS DISEASE - COPD

� Permanent abnormal dilation of bronchi associated
with inflammation and secondary weakening
� Congenital – CF, severe immune deficiency
� Post-infectious – viral, bacterial, fungal
� Bronchial obstruction – tumour, foreign body
� Ciliary dysfunction – smoking, Kartagener’s syndrome
� Traction bronchiectasis – contraction of fibrous scar tissue
� Complications
� Chronic infection – H.influenzae
� Secondary infection – s.aureus, pseudomonas, moraxela
� RVF
RESPIRATORY AIRWAYS DISEASE -
BRONCHIECTASIS

RESPIRATORY AIRWAYS DISEASE -
BRONCHIECTASIS

� Wide group of conditions affecting the lung
parenchyma diffusely
� Characterised by chronic inflammation +/- progressive fibrosis
� SOBOE, cyanosis, non-productive cough, abnormal CXR, restrictive
picture on spirometry, clubbing, fine end inspiratory crackles
� Classification:
� Known cause – occupational, drug, hypersensitivty, infectious
� Associated with systemic disorders – sarcoid, RA, SLE, UC
� Idiopathic – IPF, cryptogenic fibrosing alveolitis, cryptogenic
organising pneumonia, lymphocytic interstital pneumonia
INTERSTITIAL LUNG DISEASE
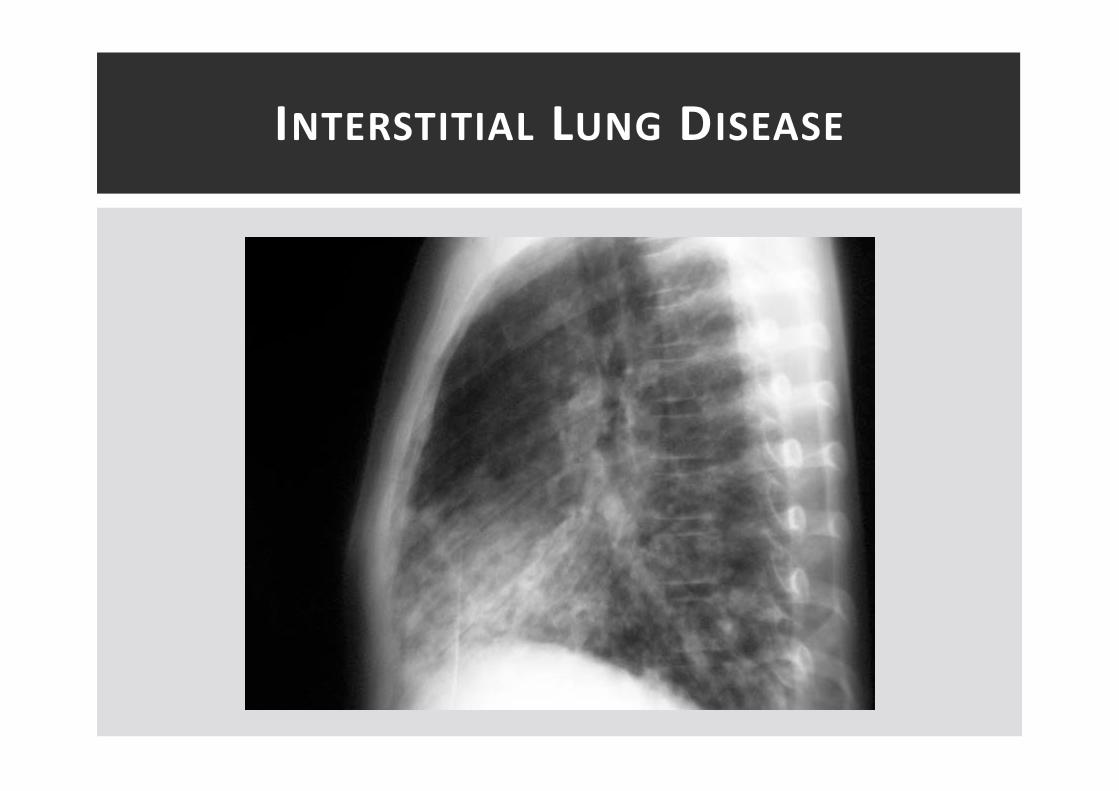
INTERSTITIAL LUNG DISEASE

INTERSTITIAL LUNG DISEASE
Upper ZoneTB
Extrinsic allergic alveolitis
Ankylosing spondylitis
Radiotherapy
Sarcoidosis / Histoplasmosis
Middle ZoneProgressive massive fibrosis
Lower ZoneIdiopathic pulmonary fibrosis
Asbestosis

� Idiopathic/Cryptogenic fibrosing alveolitis
� Idiopathic diffuse pulmonary fibrosis
� Persistent fibroblast proliferation and fibrosis
� Dry cough, exertional dyspnoea, malaise, weight loss
� Right heart failure and increased risk malignancy
� Extrinsic allergic alveolitis
� Hypersensitivity pneumonitis – inhalation antigens
� Farmer’s lung – thermophilic actinomycetes
� Bird fancier’s lung – avaian proteins
� Pathology – interstitial pneumonitis + non-caseating gramulomas
PULMONARY FIBROSIS – 5 IMPORTANT
CAUSES
� Pneumoconioses
� Inflammatory lung disease due to mineral dust inhalation
� Coal dust – lung nodules (coal macules) + massive fibrosis
� Silicosis – nodular fibrosis
� Asbestosis – diffuse fibrosis
� Auto-immune disease
� Sarcoidosis – non-caseating granulomas + multi-system disease
� RA / SLE / systemic sclerosis / ankylosing spondylitis
� Drugs
� Potentially reversible pneumonitis � fibrosis
� Bleomycin, amiodarone, nitrofurantoin
PULMONARY FIBROSIS – 5 IMPORTANT
CAUSES

� Asbestosis – family of silicates
� Chrysotile (serpentines) – white
� Crocidolite (straight) – blue
� Amosite – brown
� Asbestos related lung disease:
� Pleural plaques – marker of exposure
� Asbestosis – pulmonary fibrosis
� Adenocarcinoma
� Synergistic effect with smoking
� Mesothelioma
� Cancer of mesothelial lining (pleural, pericardial, peritoneal)
� Estimated peak of disease 2020
� Any exposure – no threshold
ASBESTOSIS

INTRA-ALVEOLAR DISEASE – PULMONARY
OEDEMA / EFFUSION
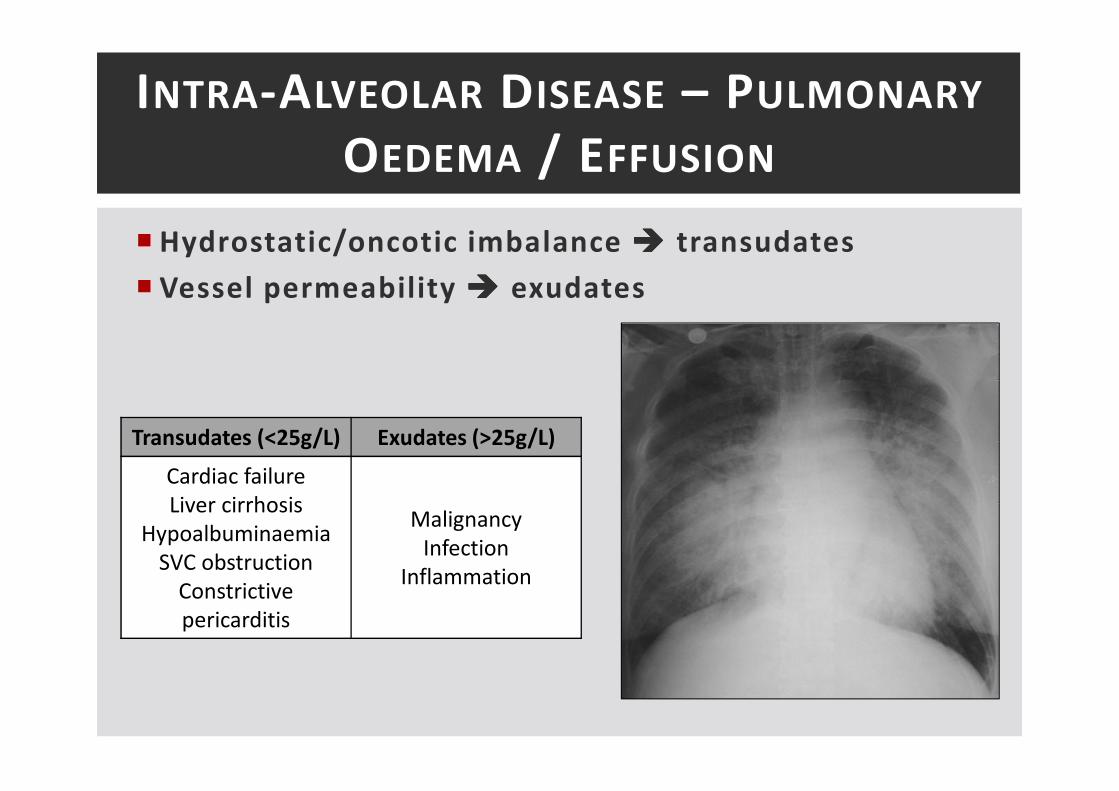
� Hydrostatic/oncotic imbalance ���� transudates
� Vessel permeability ���� exudates
INTRA-ALVEOLAR DISEASE – PULMONARY
OEDEMA / EFFUSION
Transudates (<25g/L) Exudates (>25g/L)
Cardiac failure
Liver cirrhosis
Hypoalbuminaemia
SVC obstruction
Constrictive
pericarditis
Malignancy
Infection
Inflammation
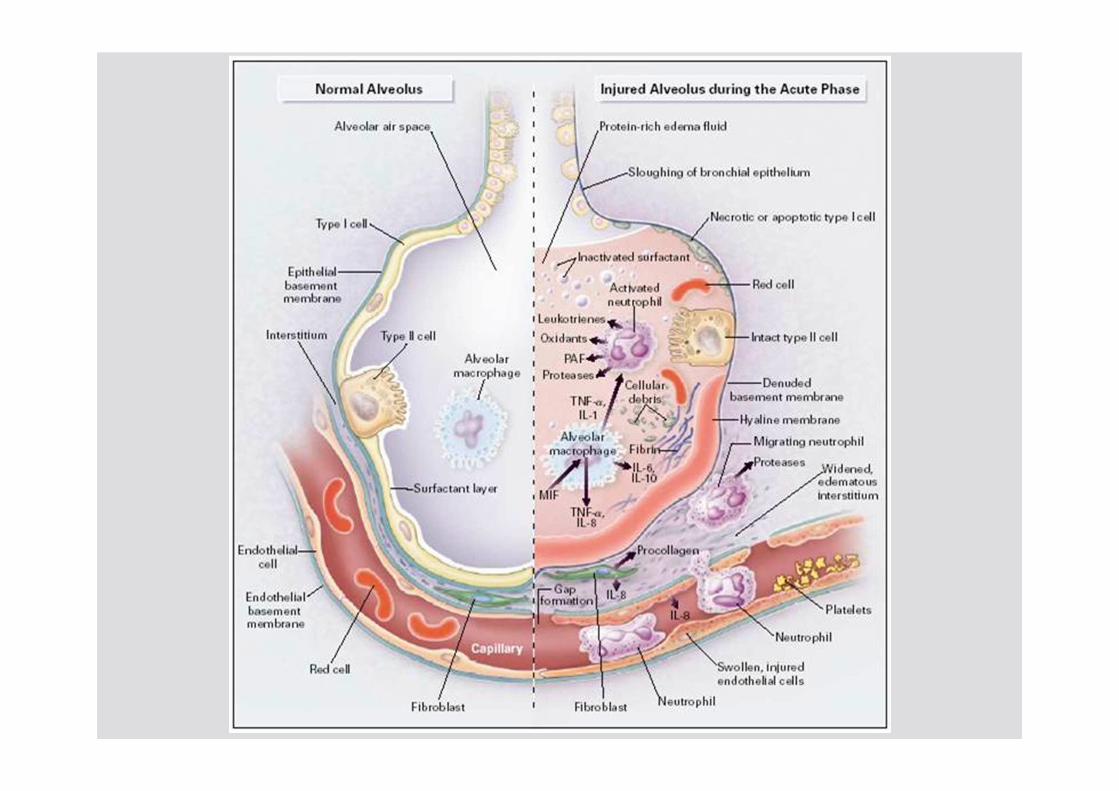
� Acute Respiratory Distress Syndrome (ARDS)
� Acute respiratory failure + non-cardiogenic pulmonary oedema �
reduced lung compliance + refractory hypoxaemia
� Respiratory component of SIRS / MOF
� Discrete histopathological stages
� Inflammatory/exudative phase – 24hrs
� Massive inflammatory response
� Formation of non-cardiogenic pulmonary oedema
� Type II pneumocyte dysfunction – reduced surfactant production
� Proliferative phase – 5-10 days
� Proliferation type II pneumocytes + fibroblasts
� Progressive interstitial fibrosis
ARDS

NEOPLASTIC LUNG DISEASE
� The most common primary malignancy in the world
� 7-10% 5yr survival - ¼ all male cancer deaths in UK
� Benign tumours
� Rare - <10%
� Hamartomas, clear cell tumours, papillomas, gland adenomas
� Commonly asymptomatic
� Malignant tumours
� Non-small cell (adenocarcinoma, large cell carcinoma, SCC) – 80%
� Small cell (neuroendocrine) – 20%
NEOPLASTIC LUNG DISEASE

� Clearly defined risk factors
� Smoking - >75% cases
� Progressive squamous metaplasia � dysplasia � neoplasia
� Abnormal cells proportional to exposure
� Asbestosis – 50x increased risk
� Synergistic with tobacco smoke exposure
� Environmental agents
� Ionising radiation
� Infection
� Cryptogenic fibrosing alveolitis
NEOPLASTIC LUNG DISEASE -
PATHOGENESIS

� Squamous cell carcinoma
� 25-40% all lung cancers
� Closely associated with smoking
� Commonly central tumour arising from bronchial epithelium
� Significant early hilar LN spread, metastasises late
� Squamous cell differentiation
� Frequently haemorrhagic with cavitating necrosis
NEOPLASTIC LUNG DISEASE –
SQUAMOUS CELL CARCINOMA

� Adenocarcinoma
� 25-40% of all lung cancers
� Arises from glandular cells – e.g. mucus goblet cells
� P53 – 30% of adenomatous hyperplasia
� More common in far east, females and non-smokers
� Commonly peripheral and multi-centric
� Associated with pulmonary fibrosis/asbestosis
� Metastasises late – 80% at diagnosis
NEOPLASTIC LUNG DISEASE –
ADENOCARCINOMA
� Large cell carcinoma
� Central and highly aggressive/destructiove
� Haemorrhage and necrosis common
� Un-differentiated
� Poor prognosis
� Small cell carcinoma (Oat cell)
� 20-25% of all lung cancers
� Often central and arising from near main brinchi
� 80% present with advanced disease
� Paraneoplastic syndrome common
� Metastasise early
� Histologically hyperchromatic nuclei and indistinct nucleoli
NEOPLASTIC LUNG DISEASE –
LARGE CELL / SMALL CELL CARCINOMA
� Local effects
� Bronchial obstruction
� Impaired mucus clearance
� Local invasion
� Distant effects
� Peptide production – ACTH, ADH, PTH (SCC)
� Paraneoplastic syndromes
� Lambert-Eaton myaesthenic syndrome, acanthosis nigrans
� Metasteses – bone, brain, liver
NEOPLASTIC LUNG DISEASE –
CLINICAL EFFECTS
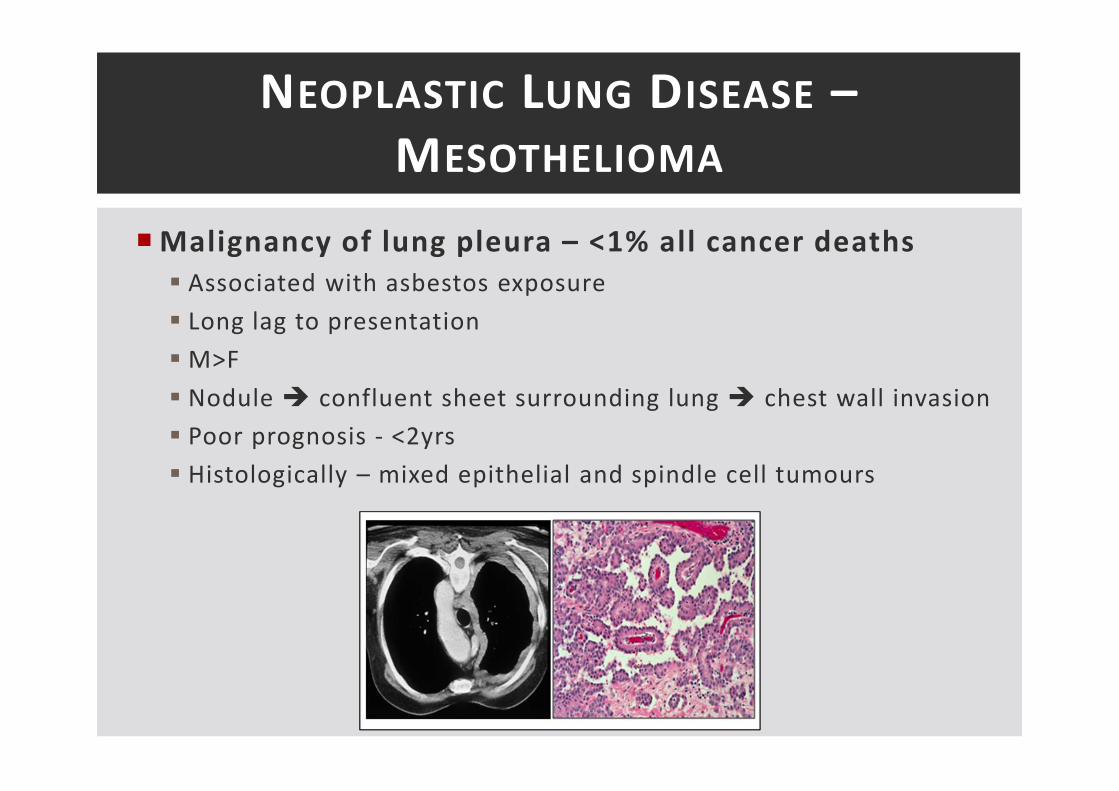
� Malignancy of lung pleura – <1% all cancer deaths
� Associated with asbestos exposure
� Long lag to presentation
� M>F
� Nodule � confluent sheet surrounding lung � chest wall invasion
� Poor prognosis - <2yrs
� Histologically – mixed epithelial and spindle cell tumours
NEOPLASTIC LUNG DISEASE –
MESOTHELIOMA

BONE & JOINT DISEASE

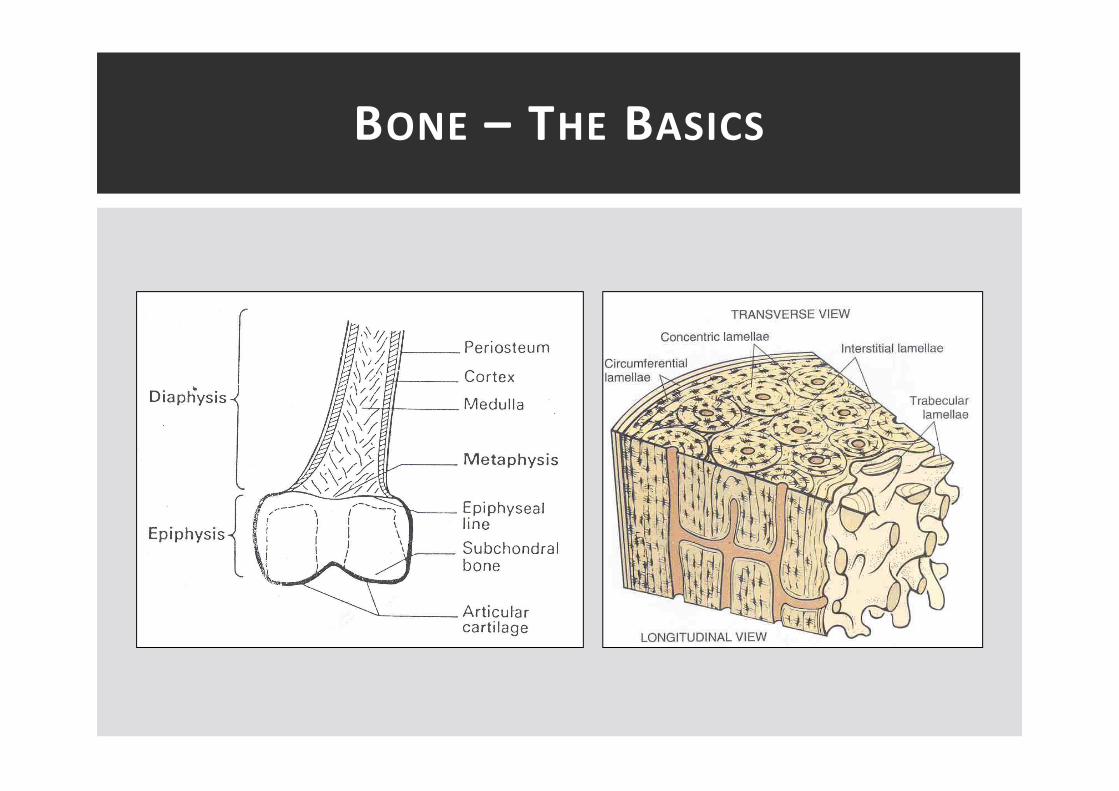
� Principle functions of bone
� Mechanical – support and site of muscle attachment
� Protective – vital organs and bone marrow
� Metabolic – calcium reserve and site of haematopoiesis
� Composition of bone
� Inorganic vs organic
� Bone subtypes
� Cortical bone – long bones, mechanical/protective
� Cancellous bone – axial skeleton, metabolic
BONE – THE BASCIS
BONE – THE BASICS
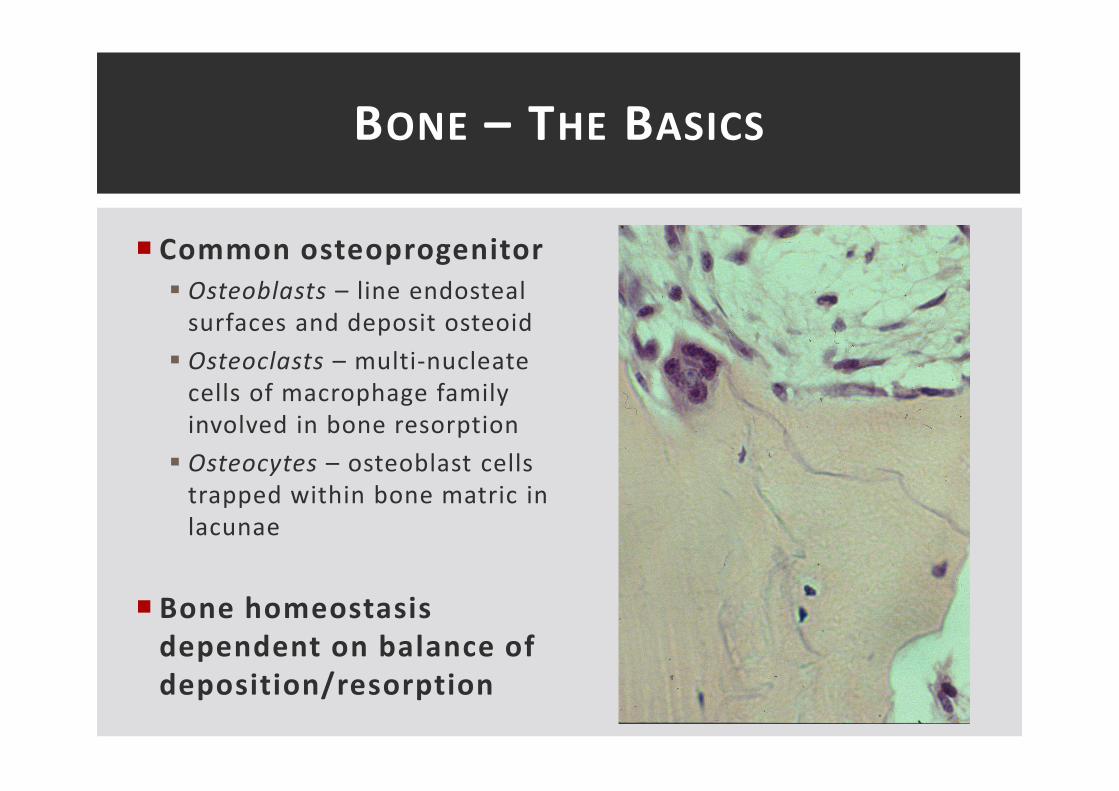
� Common osteoprogenitor
� Osteoblasts – line endosteal
surfaces and deposit osteoid
� Osteoclasts – multi-nucleate
cells of macrophage family
involved in bone resorption
� Osteocytes – osteoblast cells
trapped within bone matric in
lacunae
� Bone homeostasis
dependent on balance of
deposition/resorption
BONE – THE BASICS

• bone mass + normal mineralization
• Aggressive & malignant tumour of adolescents
• osteoclastic activity + PTH + Ca2+ + normal renal function
• bone mineralization + renal failure/malabsorption
• osteoblast activity + osteoclast activity bone pain with
normal Ca2+ & normal PTH
A. Bony metastasis
B. Chrondrosarcoma
C. Ewing’s sarcoma
D. Gout
E. Osteoarthritis
F. Osteomalacia
G. Osteomyelitis
H. Osteoporosis
I. Osteosarcoma
J. Paget ’s disease
K. 1° hyperparathyroidism
L. Rheumatoid arthritis
M. 2° hyperparathyroidism
N. 3° hyperparathyroidism
EMQ – DISORDERS OF BONE
• bone mass + normal mineralization - H
• Aggressive & malignant tumour of adolescents - C
• osteoclastic activity + PTH + Ca2+ + normal renal function - K
• bone mineralization + renal failure/malabsorption - F
• osteoblast activity + osteoclast activity bone pain with
normal Ca2+ & normal PTH - J
A. Bony metastasis
B. Chrondrosarcoma
C. Ewing’s sarcoma
D. Gout
E. Osteoarthritis
F. Osteomalacia
G. Osteomyelitis
H. Osteoporosis
I. Osteosarcoma
J. Paget ’s disease
K. 1° hyperparathyroidism
L. Rheumatoid arthritis
M. 2° hyperparathyroidism
N. 3° hyperparathyroidism
EMQ – DISORDERS OF BONE

METABOLIC BONE DISEASE
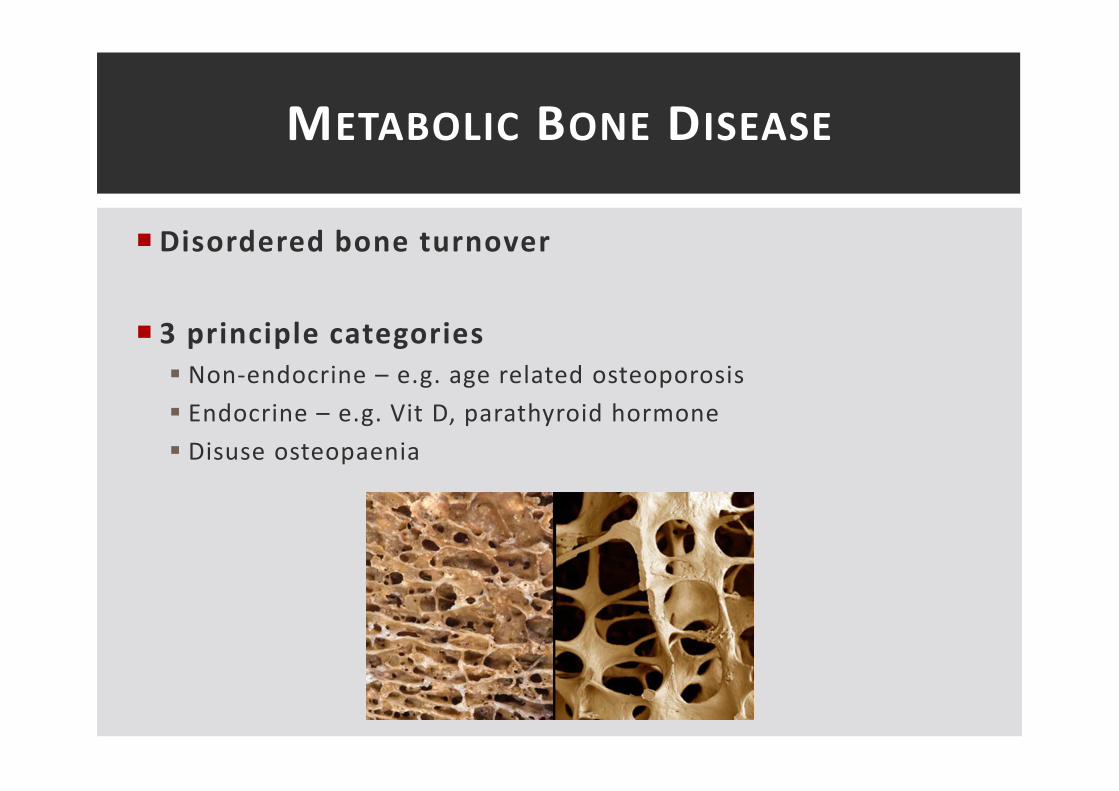
� Disordered bone turnover
� 3 principle categories
� Non-endocrine – e.g. age related osteoporosis
� Endocrine – e.g. Vit D, parathyroid hormone
� Disuse osteopaenia
METABOLIC BONE DISEASE

� Bone – normal quality, reduced density
� Primary – age, post-menopause
� Secondary – drugs, systemic disease
� Generalised vs local
� Key risk factors
� 1/3 women and 1/12 men >50yrs
� Fragility fractures � 50% lose independence, 20% mortality
OSTEOPOROSIS

OSTEOPOROSIS
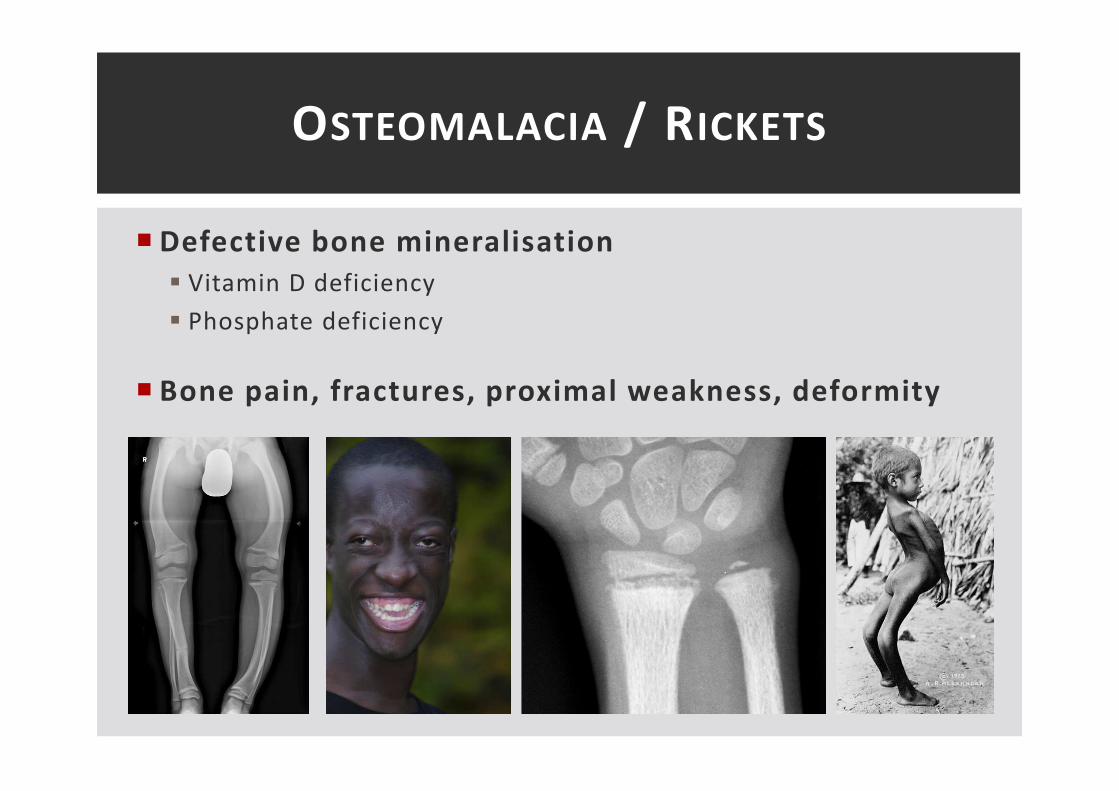
� Defective bone mineralisation
� Vitamin D deficiency
� Phosphate deficiency
� Bone pain, fractures, proximal weakness, deformity
OSTEOMALACIA / RICKETS

PARATHYROID DISEASE

� Hyperparathyroidism
� Primary - >80% single adenoma
� Secondary – prolonged hypocalcaemia
� Tertiary – autonomous PTH
PARATHYROID DISEASE
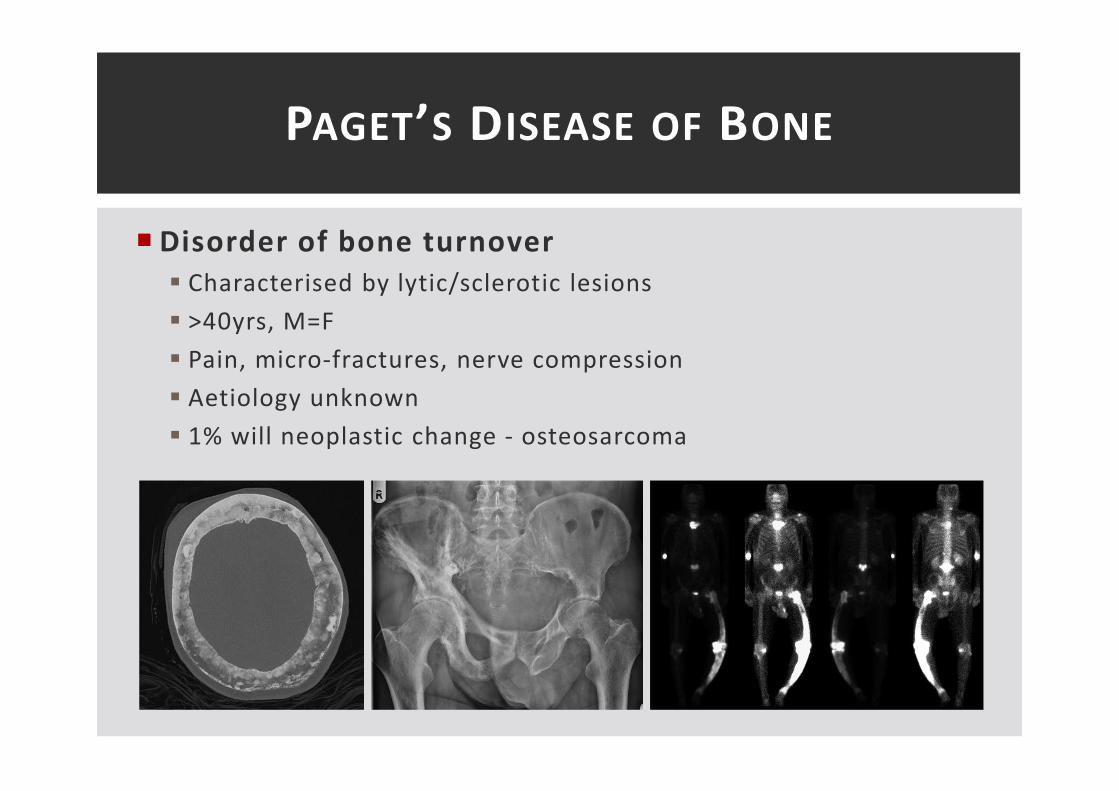
� Disorder of bone turnover
� Characterised by lytic/sclerotic lesions
� >40yrs, M=F
� Pain, micro-fractures, nerve compression
� Aetiology unknown
� 1% will neoplastic change - osteosarcoma
PAGET’S DISEASE OF BONE

NEOPLASTIC BONE DISEASE

� Benign tumours
� Primary bone tumours are uncommon
� <30yrs
� Site and age predilication
� Classification based upon cytological appearance and matrix
product
� Diagnosis – symptoms, XR appearance, biopsy
� Secondary bone tumours
� Common
� >50yrs
NEOPLASTIC BONE DISEASE
� Osteochrondroma
� Cartilage capped bony protrubence of metapysis/diaphysis
� Growth plate derived - 10-20yrs, M>F
� Osteochondromatosis may lead to malignant transformation
� Enchondroma
� Sub-periosteal chrondroma
� Radiological appearance of lytic cotton wool calcifcation
� Multiple enchrondromas = Maffucci’s Syndrome
� Significant risk of malignant transformation
BENIGN BONE TUMOURS

� Osteoma (“ivory osteoma”)
� Smooth non tender mound rarely
causing symptoms
� Common on surface of skull vaukt
� Osteoid Osteoma
� Long bones of young males, small <1cm
� Continuous pain worse at night
� Lytic lesion with a central nidus and
sclerotic rim
� Highly vascular and histologically well
defined
BENIGN BONE TUMOURS

PRIMARY BONE TUMOURS
Bone Tumour Age Site Radiology Histology Prognosis
Osteosarcoma<20yr
sLong bones
Lytic changes with
elevated periosteum
(Codman’s triangle)
Mesenchymal
cells
(osteoblastic/cho
ndroblastic)
60% 5yr
Chondrosarcoma>40yr
s
Pelvis, axial
skeleton or
long bones
Lytic destruction with
fluffy calcification
Myxoid/hyaline
cartilage70% 5yr
Ewing’s Sarcoma<20yr
sAny bone
Onion skinning of
periosteum + lytic
changes and sclerosis
Small round cell
tumour75%
� Osteosarcoma > chrondrosarcoma > Ewing’s sarcoma
� Rare – osteosarcoma ≈150/annum in UK

PRIMARY BONE TUMOURS
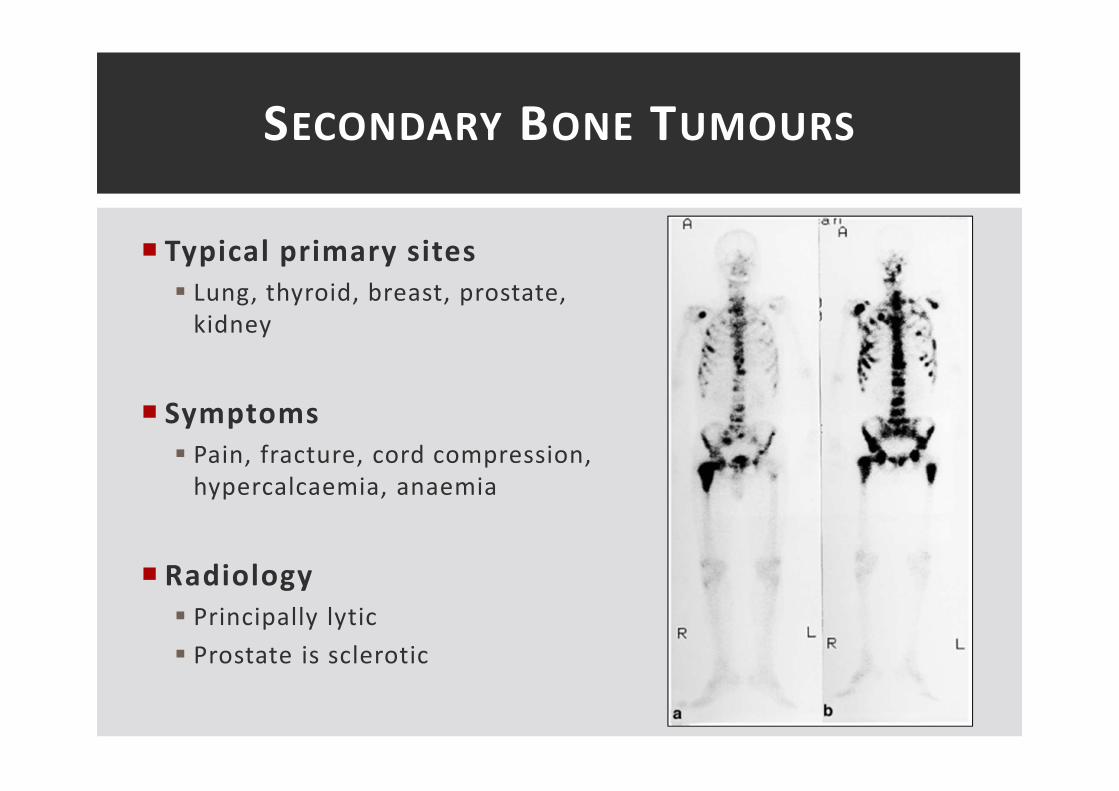
� Typical primary sites
� Lung, thyroid, breast, prostate,
kidney
� Symptoms
� Pain, fracture, cord compression,
hypercalcaemia, anaemia
� Radiology
� Principally lytic
� Prostate is sclerotic
SECONDARY BONE TUMOURS
• Epigastric pain which is worse lying f lat . An endoscopy and biopsy reveals
squamous inf lammation and basal cel l prol iferation
• 38yr with RA presents with melaena. Endoscopy & biopsy reveals gastric
erosions and a neutrophil inf i ltrate
• 30yr diarrhoea and weight. Duodenal biopsy - cytotoxic T-cel ls
• 60yr with epigastric pain rel ieved by meals and antacids. +ve CLO test
• Biopsy 2cm change to columnar epithel ium in the lower oesophagus
A. Active chronic gastritis
B. Acute gastritis
C. Barrett ’s oesophagus
D. Coeliac disease
E. Duodenal ulcer
F. Gastric ulcer
G. GORD
H. Intestinal metaplasia
I. Streptococcus pneumoniae
J. Normal oesophagus
K. Oesophageal varicies
L. Pernicious anaemia
M. Squamous carcinoma
EMQ – GI DISORDERS

• Epigastric pain which is worse lying f lat . An endoscopy and biopsy reveals
squamous inf lammation and basal cel l prol iferation - G
• 38yr with RA presents with melaena. Endoscopy & biopsy reveals gastric
erosions and a neutrophil inf i ltrate - B
• 30yr diarrhoea and weight. Duodenal biopsy - cytotoxic T-cel ls - D
• 60yr with epigastric pain rel ieved by meals and antacids. +ve CLO test - E
• Biopsy 2cm change to columnar epithel ium in the lower oesophagus - C
EMQ – GI DISORDERS
A. Active chronic gastritis
B. Acute gastritis
C. Barrett ’s oesophagus
D. Coeliac disease
E. Duodenal ulcer
F. Gastric ulcer
G. GORD
H. Intestinal metaplasia
I. Streptococcus pneumoniae
J. Normal oesophagus
K. Oesophageal varicies
L. Pernicious anaemia
M. Squamous carcinoma

� 25yr with weight loss, abdominal pain and PR bleeding.
Endoscopy – transmural inflammation, non-caseating
granulomas, skip lesions
� 24yr with known IBD presents with an itchy perineum. He has
noticed discharge which soils his underwear. Examination shows
a “Pepper pot anus”
a) Crohn’s Disease
b) Ulcerative colitis
c) Both
d) Neither
EMQ – INFLAMMATORY BOWEL DISEASE

� 25yr with weight loss, abdominal pain and PR bleeding.
Endoscopy – transmural inflammation, non-caseating
granulomas, skip lesions - A
� 24yr with known IBD presents with an itchy perineum. He has
noticed discharge which soils his underwear. Examination shows
a “Pepper pot anus” - A
a) Crohn’s Disease
b) Ulcerative colitis
c) Both
d) Neither
EMQ – INFLAMMATORY BOWEL DISEASE

END OF PART 1 – ANY QUESTIONS?