Mechanical and Chemotherapeutic Home Oral Hygiene-1

of 6
Transcript of Mechanical and Chemotherapeutic Home Oral Hygiene-1
-
7/29/2019 Mechanical and Chemotherapeutic Home Oral Hygiene-1
1/6
Mechanical and Chemotherapeutic Home Oral
Hygiene
Mechanical Methods of Plaque Control
- The most accepted techniques for plaque
removal
- These include:
o Tooth brushing
o Flossing
o Disclosing agents
o Oral irrigators
o Tongue scrapers
Manual toothbrush
- Most common method for removing plaque
- Variable
o Bristle materialo Length
o Diameter
o Number of fibers
o Length of brush head
o Number and arrangement of bristle
tufts
o Angulation of brush head to handle
o Handle design
Nowadays, brushes are made of synthetic (nylon)
bristles
Classification of brushes based on diameter of bristles
- Soft (0.16 0.22mm)
- Medium (0.23 0.29mm)
- Hard (0.30 mm and higher)
Types of Bristle Ends
- Coarse cut
- Enlarged bulbous
- Round (bristle type of choice. Why? Because its
associated with a lower incidence of gingival
tissue irritation)
What do you think is the most preferred brush to
be used in pediatric dentistry?
Answer: the soft brush with smaller head and thicker
handle.
o Decreased gingival tissue trauma.
o Increased interproximal cleaning
ability
o Aid in access to oral cavity
o Facilitates childs grip of hadle
When is the best time to replace your toothbrush?
Answer: when it appears well worn. Some children
chew their brushes.
Floss
Tooth brushing alone cannot remove plaque from all
tooth surfaces, especially the interproximal plaque.
Types of floss
- Flavoured and unflavored
- Waxed and unwaxed
-
7/29/2019 Mechanical and Chemotherapeutic Home Oral Hygiene-1
2/6
- Thin, tape and meshwork
Flosses can be made of:
- Nylon (floss of choice because of ease of
passing the floss in between teeth, lack of wax
residue, squeaking sound effect, fiber spread
increases the surface contact)
- Teflon
Powered Mechanical Plaque Removal
- Significantly proven more effective and
beneficial in reducing plaque index, gingival
index, percentage of sites that bled on probing,
pocket depth, total gram negative bacteria in
subgingval plaque than the manual tooth
brushes.
- It was designed because some people lackmanual dexterity in manipulation of brushes
- Uses acoustic energy
- Has an electromagnetic device that drives
bristles motion at 260 Hz or 31,320 brush
strokes per minute.
- Brushes with rotation-oscillation action removes
more plaque and reduces gingivitis
- Requires single handed usage
- Filament rotates to undergo an elliptical
movement, removes plaque attached to adjacent
Dentrifices
- Plaque and stain removing agents through the
use of abrasives and surfactants
- Composition
o Incorporated with pleasant flavors
and colors
o tartar control properties such as
pyrophosphate
o fluoride - anticaries and
desensitiation properties
- amount of dentrifices given to child patients
should be taken in consideration.
- Parents should be advised to delay the use of
fluoride dentrifice until the child is older than 36months and to use small pea-sized amount of
toothpaste
Disclosing Agents
- Allow visualization of plaque
- Compostion
o Iodine
o Gentian violet
o Erythrosine
o Basic fuchsin
o Fast green
o Food agents with antimicrobial
activity
Adjuncts for Plaque Control
- oral irrigators (uses pulsed water or
chemotherapeutic agents to dislodge plaque)
- tongue scrapers (flat, flexible plastic sticks that
are used to remove bacterial and food deposits
that accumulate within the rough dorsal surface
of the tongue. )
- gauze or special dental wash cloths (used in
infants to massage the gums and remove the
plaque in newly erupted teeth)
Techniques
- roll method- Charters method
- Horizontal scrubbing method
- Modified stillman method
- Roll method
o Brush is placed in vestibule
o Bristles ends directly apically
o Sides of bristles touching gingival
tissue
o Patient exerts lateral pressure with
the sides of the bristles and brush is
moved occlusally
o Brush is placed again in high
vestibule while rolling motion is
repeated
o Lingual surfaces are brush in the
same manner, with 2 teeth brushed
simultaneously
o Seldom used
- Charters Method
o Ends of the bristles are placed in
contact with the enamel and gingiva
o Bristles are pointed 45 degree
angle toward the plane of occlusion
o Lateral and downward pressure is
then placed on brush
o Brush is vibrated gently back and
forth a millimetre or so.
- Horizontal Scrubbing Method
o Brush is placed horizontally on
buccal and lingual surfaces and
moved back and forth with a
scrubbing motion.
-
7/29/2019 Mechanical and Chemotherapeutic Home Oral Hygiene-1
3/6
o Exhibited a more significant plaque
removing effect that the other
methods.
o Recommended for bushing
childrens teeth.
- Modified Stillman Method
o
Combines a vibratory action of thebristles with a stroke movement of
the brush in the long axis of the
teeth.
o Brush is placed at the mucogingival
line, with the bristles pointed away
from the crown, and moved with a
stroking motion along the gingival
and the tooth surface.
o The handle is rotated toward the
crown and vibrated as the brush is
moved.
Techniques in Flossing
o 46 to 61 cm is obtained and the
ends are wrapped in the middle
finger. Floss should be long enough
to allow the thumbs to touch each
other when the hands are laid flat.
o Thumbs and index fingers are used
to guide the floss as it gently sawed
between the two teeth to be
cleaned. Gingival trauma may occur
if the floss snaps down through the
interproximal area.
o
Floss is manipulated into C shapearound tooth individually and
moved in a cervical- occlusal
reciprocating motion until the
plaque is removed. In between
cleaning each pair of teeth the floss
is repositioned on the fingers so
that fresh, unsoiled floss is used at
each new location.
Time Consideration
How often should we brush and floss our teeth and for
how long?
Answer: 1 minute brushing period provides the
greatest plaque removal.
In Children, oral hygiene procedures must be done
once or twice daily with parental supervision.
Chemotherapeutic Plaque Control
- characteristics of an ideal Chemotherapeutic
plaque control agent
o specificity only for the pathogenic
bacteria
o substantivity, the ability to attach to
and be retained by oral surfaces
and then be released over time
without loss of potency
o chemical stability during storage
o absence of adverse reactions, such
as staining or mucosal interactions
o toxicology safety
o ecologic safety so as not to
adversely alter the microbiotic flora
o ease of use
- Different ways to administer antiplaque agents
o Mouthwashes
o
Dentrificeso Gels
o Irrigators (provide supragingival and
subgingival delivery)
o Floss
o Chewing gum
o Lozenges
o Capsules (systemic distribution)
o All of these are for local,
supragingival administration except
capsules and irrigators
Antiseptic Agents
- Chlorhexidine
o Positively Charged Organic
antiseptic agent
o Reduces plaque, gingivitis,
mucositis
o Binds with anionic glycoproteins
and phosphoproteins on the buccal,
palatal and labial mucosa and
tooth-borne pellicle
o Can be of great use in
immunocompromised patients esp.
mental retardation and patients
undergoing bone marrowtransplantation
o Antibacterial effects:
Binding well to bacterial
cell membrane
Increasing their
permeability
Initiating leakage
Precipitating intracellular
components
-
7/29/2019 Mechanical and Chemotherapeutic Home Oral Hygiene-1
4/6
Decrease levels of
streptococcus mutans
o Form
Rinse, spray, varnish, gel
in flossing
o Adverse reactions of positively
charged antiplaque agents Staining of teeth
Impaired taste sensation
Increased supragingival
calculus formation
Listerine
- Noncharged phenolic antiseptic agent
- Burning sensation
- Bitter taste
- Highest alcohol contents (25 %)
Enzymes, Plaque- Modifying Agents and Plaque
Attachment Interference Agents
- Enzyme System
o Alter plaque architecture
- Urea Peroxide
o Plaque modifying agent
o Increased stability over hydrogen
peroxide
o Protein denaturation effect of urea
- Delmopinol
o Binds to salivary protein and alters
cohesiveness and adhesiveness
properties of films formed
Sugar Substitutes
- Incorporated in chewing gums to:
o Decrease plaque accumulation and
pH
o Lower incidence of caries
- Examples of Sugar Substitutes
o Xylitol
o Mannitol
o Sucralose
o Aspartame
Age Specific Home Oral Hygiene Instructions
- Prenatal Counseling
o Before birth of child
o Discuss Pregnancy gingivitis
- Infants (0 1 year old)
o Plaque removal activity should
begin on eruption of primary teeth
o Cleaning and massaging of gums
using moistened gauze or
washcloth, soft bristled infant sized
toothbrush may be introduced
o Performed once daily
o Childs first visit to the dentist
approximately when the tootherupts or by the age of 12 months
- Toddlers (1 to 3 years old)
o Toothbrush must be introduced
o Parent remains primary caregiver of
hygienic procedures
o Flossing, if interproximal contacts
are closed
- Preschoolers (3 to 6 years)
o Fluoride dentrifice can be
introduced at 3 years
o Pea - sized amount of tooth paste
o Daily flossing
- School-Aged Children (6-12 years)o Parents may find they only need to
brush or floss their childs teeth in
difficult to reach areas of mouth
o Use of disclosing agent for parents
inspection
o Ingestion is the primary concern
o Fluoridated dentrifices is necessary
o Use of chemotherapeutic agents is
recommended
- Adolescents (12 19 years)
o Motivation
o Poor dietary habits and pubertal
hormonal changes increase the riskfor caries and gingivitis
- In- office Oral Hygiene Programs
o Dental education of parent and
child describing exactly the
importance of oral hygiene
o Delivered in simple terms with
enthusiasm and conviction
o Conveyed in a childs age-
appropriate language
o Positive reassurance, not critical
o let me show you how to improve
rather than saying youre doing it
all wrongo Recare intervals should be
personalized with patients needs
-
7/29/2019 Mechanical and Chemotherapeutic Home Oral Hygiene-1
5/6
Flossing
Flossing removes plaque and bacteria that you
cannot reach with your toothbrush. If you don't floss,
you are missing more than one-third of your tooth
surface. Plaque is the main cause of gum disease. It
is an invisible bacterial film that develops on your
teeth every day.
Within 24 to 36 hours, plaque hardens into tartar (also
called calculus), which can only be removed by
professional cleaning. Floss at least once a day, and
plaque never gets the chance to harden into tartar.
Getting into the habit of daily flossing is easier when
you floss while doing something else like watching TV
or listening to music, for example.
How to floss your teeth
Step 1
Take a length of floss equal to the distance from your
hand to your shoulder.
Wrap it around your index and middle fingers, leaving
about two inches between your hands.
Step 2
Slide the floss between your teeth and wrap it into a
"C" shape around the base of the tooth and gently
under the gumline. Wipe the tooth from base to tip
two or three times.
Step 3
Be sure to floss both sides of every tooth. Don't forget
the backs of your last molars. Go to a new section of
the floss as it wears and picks up particles.
Step 4
Brush your teeth after you floss - it is a more effective
method of preventing tooth decay and gum disease.
Flossing Problems and Solutions
Gums sometimes bleed when you first begin to floss.
Bleeding usually stops after a few days. If bleeding
does not stop, see your dentist. Floss can shred if you
snag it on an old filling or on the ragged edge of a
tooth.
-
7/29/2019 Mechanical and Chemotherapeutic Home Oral Hygiene-1
6/6
Try another type of floss or dental tape. Ask your
dentist or dental hygienist for advice. If your floss still
shreds, see your dentist.
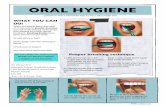
Brushing
Regular, thorough brushing is a very important step in
preventing tooth decay and gum disease. Brushing
removes the bacteria that promote tooth decay and
the plaque that can cause gum disease.
Ideally, you should brush after every meal, because
the bacterial attack on teeth begins minutes after
eating. At the very least, brush once a day and always
before you go to bed. Brushing your teeth isn't
complicated, but there is a right and a wrong way.
How to brush your teeth
Step 1
Brush at a 45 degree angle to your teeth. Direct the
bristles to where your gums and teeth meet. Use agentle, circular, massaging motion, up and down.
Don't scrub. Gums that recede visibly are often a
result of years of brushing too hard.
Step 2
Clean every surface of every tooth. The chewing
surface, the cheek side, and the tongue side.
Step 3
Don't rush your brush. A thorough brushing should
take at least two to three minutes. Try timing yourself.
Step 4
Change your usual brushing pattern. Most people
brush their teeth the same way all the time. Thatmeans they miss the same spots all the time. Try
reversing your usual pattern.
Step 5
Use a soft brush with rounded bristles. The right
toothbrush cleans better. Choose a size and shape
that allow you to reach all the way to your back teeth.
There are many different types of brushes, so ask
your dentist to suggest the best one for you. CDA
recommends you replace your toothbrush every three
months.