
Measurement Based Care: Behavioral Health Joint …
46
Measurement Based Care: Behavioral Health Joint Commission Accredited Organizations Share Their Experiences Scott Williams, PsyD Maeve O’Neill, MEd, LCDC, LPC-S, CHC Shawna Granato, LISW-S Antoinette Giedzinska, PhD January 30, 2020
Transcript of Measurement Based Care: Behavioral Health Joint …
Measurement Based Care: Behavioral Health Joint Commission Accredited Organizations Share Their Experiences
Scott Williams, PsyD
Maeve O’Neill, MEd, LCDC, LPC-S, CHC
Shawna Granato, LISW-S
Antoinette Giedzinska, PhD
January 30, 2020

2
© 2019 The Joint Commission. All Rights Reserved.
CTS.03.01.09(Effective January 1, 2018)
– Standard CTS.03.01.09 – The organization assesses the outcomes of care,
treatment, or services provided to the individual served
– EP 1 – The organization uses a standardized tool or instrument to monitors the individual’s
progress in achieving his or her care, treatment, or service goals
– EP 2 – The organization gathers and analyzes the data generated through standardized
monitoring, and the results are used to inform the goals and objectives of the
individual’s plan for care, treatment, or services as needed
– EP 3 – The organization evaluates the outcomes of care, treatment, or services provided to
the population(s) it serves by aggregating and analyzing the data gathered through the
standardized monitoring effort
3
© 2019 The Joint Commission. All Rights Reserved.
Complying with Standard CTS.03.01.09
Ultimately… to comply with the standard you need to:
−Select an instrument that is appropriate for measurement-
based care
−Administer it consistently throughout the care process
−Actually look at the data and do something in response to it
https://attendee.gotowebinar.com/register/7417914957620236547
Webinar Replay available at:
4
© 2019 The Joint Commission. All Rights Reserved.
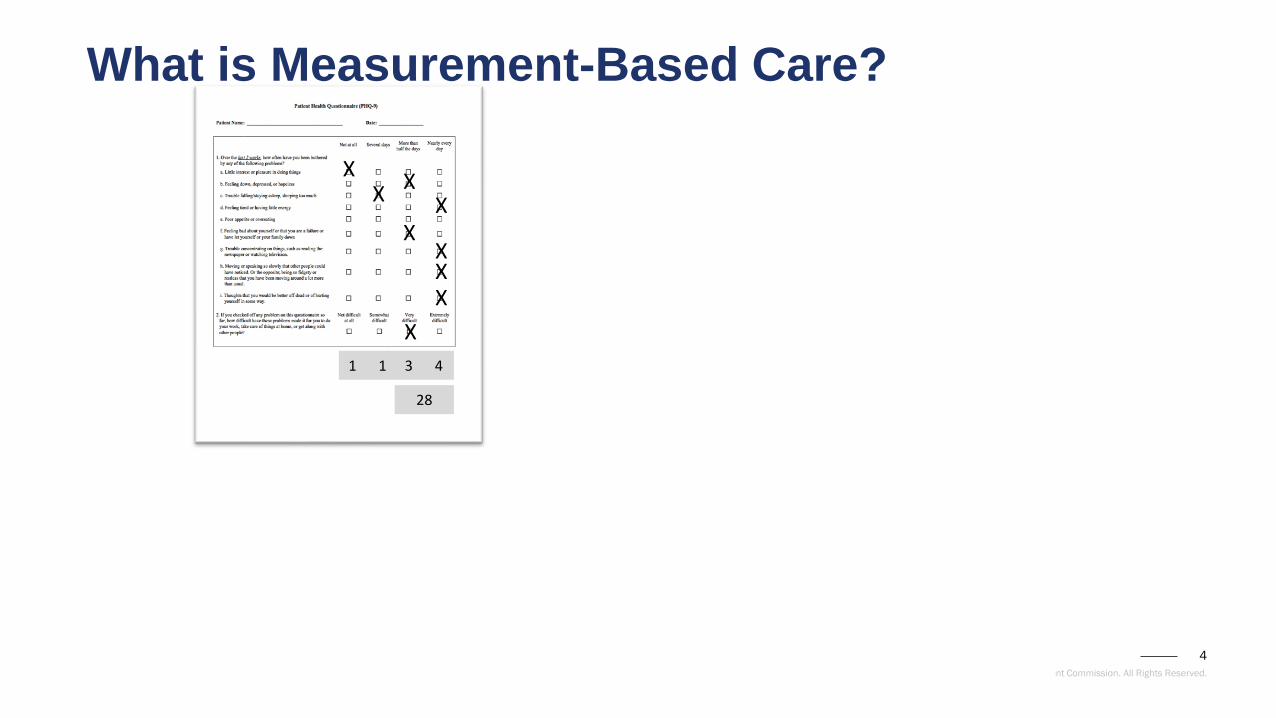
What is Measurement-Based Care?
XX
XX
XX
XX
X
1 1 3 4
28
5
© 2019 The Joint Commission. All Rights Reserved.
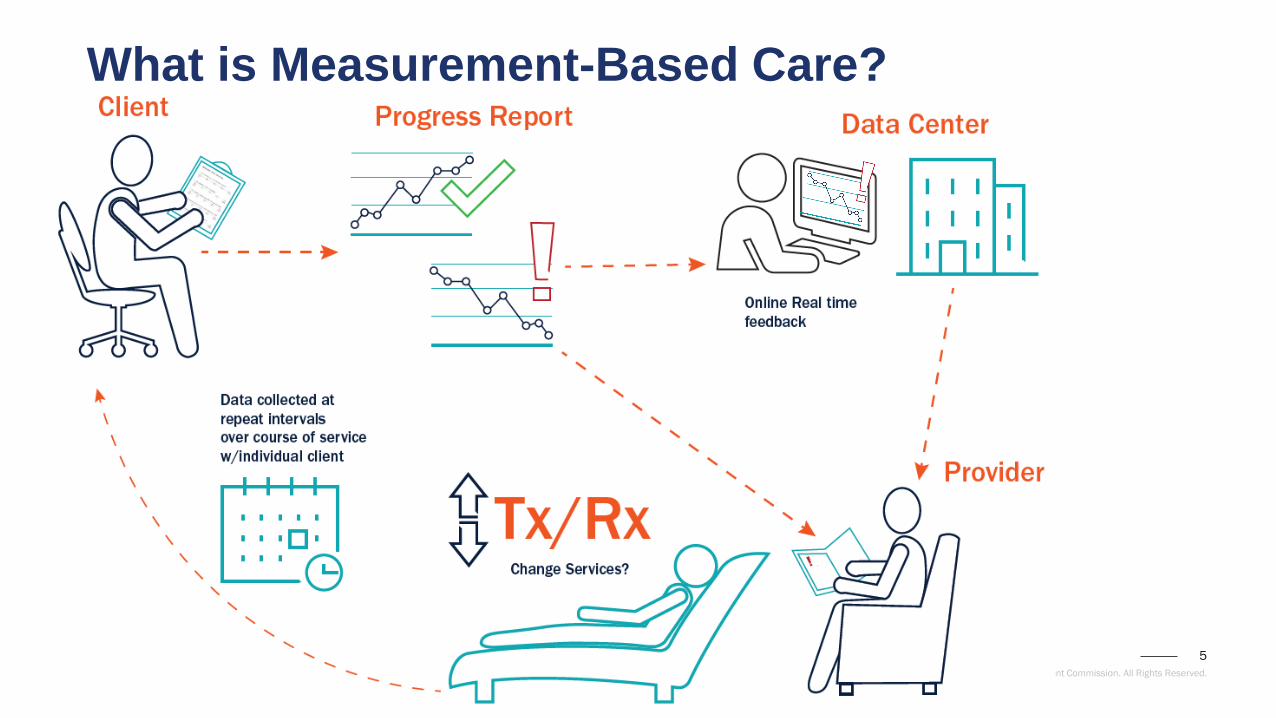
What is Measurement-Based Care?
6
© 2019 The Joint Commission. All Rights Reserved.
What is Measurement-Based Care?
− Implementation will vary
based upon:
− Type of population, service and
setting
− Frequency of repeated
administration
7
© 2019 The Joint Commission. All Rights Reserved.
What Kind of Instruments Meet the Requirement?
– The instrument should:
– Have well-established reliability and validity for use as a repeated
measure
– Be sensitive to change
– Be appropriate for use as a repeated measure
– Be capable of discriminating between populations that may or may
not benefit from services (if appropriate)
–e.g., clinical/non-clinical, healthy/non-healthy functioning,
typical/non-typical, etc.
8
© 2019 The Joint Commission. All Rights Reserved.
Measures NOT Complying with Standard CTS.03.01.09
– A measure that assesses the use of evidence-based care or clinical
practice guidelines
– A perception of care questionnaire or patient satisfaction survey
– A measure of medication/treatment compliance
– An assessment of outcome after the completion of service, even if it
compares a baseline score to a subsequent point of measurement
(e.g., intake/termination, admission/discharge)
9
© 2019 The Joint Commission. All Rights Reserved.
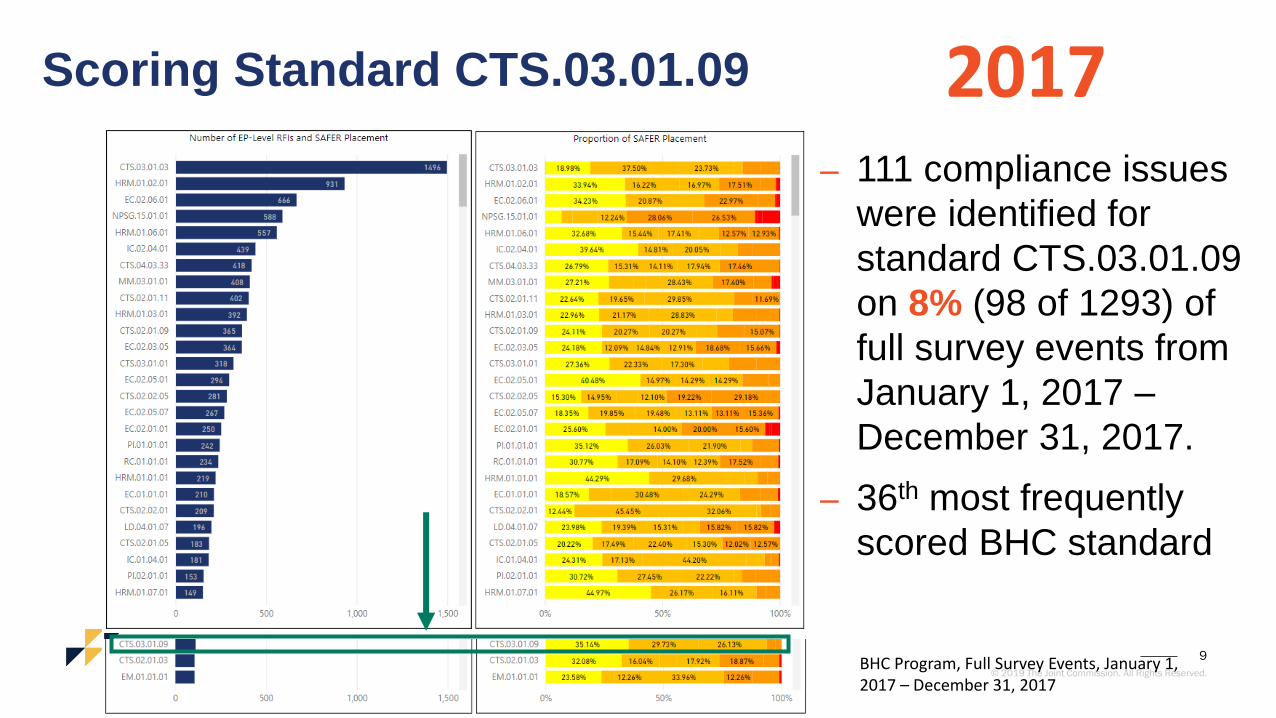
Scoring Standard CTS.03.01.09
– 111 compliance issues
were identified for
standard CTS.03.01.09
on 8% (98 of 1293) of
full survey events from
January 1, 2017 –
December 31, 2017.
– 36th most frequently
scored BHC standard
2017
BHC Program, Full Survey Events, January 1, 2017 – December 31, 2017
10
© 2019 The Joint Commission. All Rights Reserved.
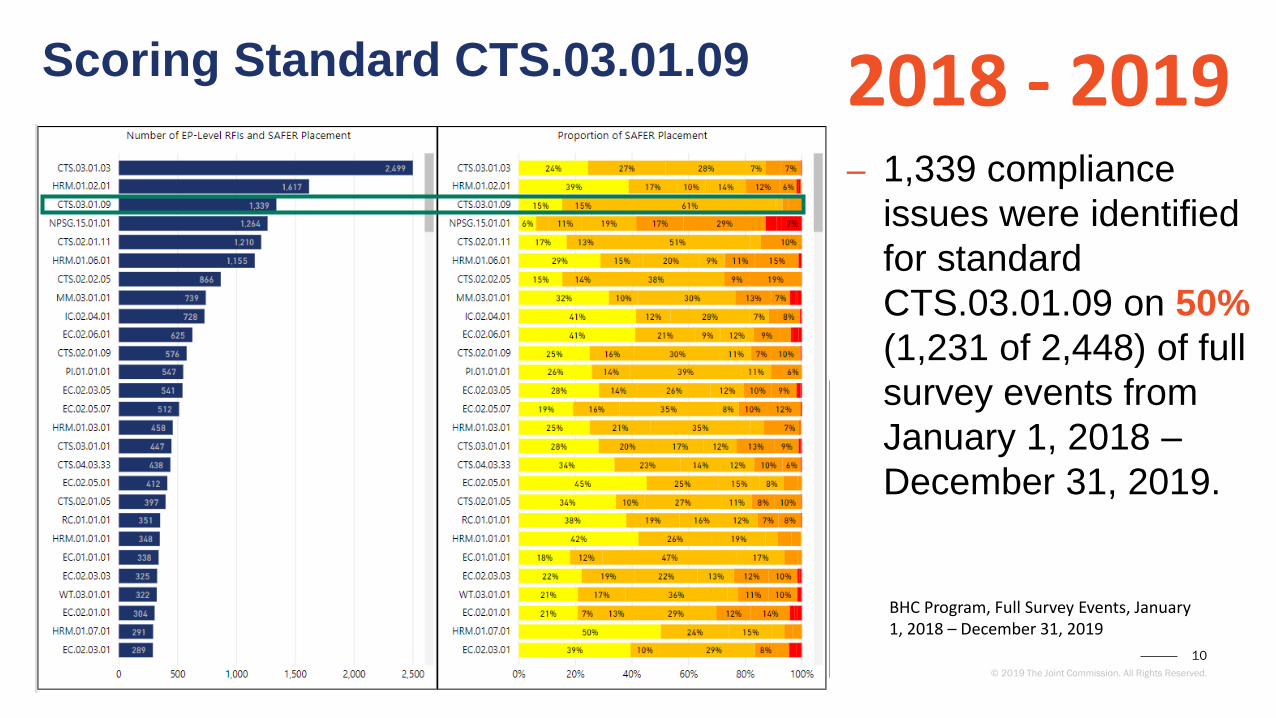
Scoring Standard CTS.03.01.09
– 1,339 compliance
issues were identified
for standard
CTS.03.01.09 on 50%
(1,231 of 2,448) of full
survey events from
January 1, 2018 –
December 31, 2019.
2018 - 2019
BHC Program, Full Survey Events, January 1, 2018 – December 31, 2019

11
© 2019 The Joint Commission. All Rights Reserved.
The Good News…
−The other 50% of surveyed organizations
appear to be meeting the requirements of the
standard
− In late-2018 we interviewed a sample of these
organizations to get a better understanding of
what they were doing to comply

12
© 2019 The Joint Commission. All Rights Reserved.
Instruments Being Used:
− PHQ- 9 (Patient Health Assessment Questionnaire)
− The Clinical Opiate Withdrawal Scale (COWS)
− BAM (Brief Addiction Monitor)
− GAD-7 (Generalized Anxiety Disorder)
− CIWA (Clinical Institute Withdrawal Assessment for Alcohol)
13
© 2019 The Joint Commission. All Rights Reserved.
Instruments Being Used:
− Quality of Life Inventory (QOLI)
− OASAS forms PAS-26n, PAS-44, PAS-45
− Modified FAF
− Achenbach
− VISTA
− Severity of Dependence Scale (SDS)
− RSES-4
− SWLS
− Beck’s tool
− PTSD Checklist for DSM-5 (PCL-5)
− Outcome Rating Scale (ORS)
− Columbia Suicide Assessment
− Insight 20
− Physical Appearance Comparison Scale
− Child/Adolescent Behavioral Assessment
(CABA-Y and CABA-I)
− SF-36
− DAST-10
− AUDIT
− Alcohol Abstinence Self-Efficacy Scale
− Drug Avoidance Self Efficacy Scale
− AWARE
− Adult Global Health Scale
14
© 2019 The Joint Commission. All Rights Reserved.
Surveyor Examples of Data Use
– Using the tool and it's results to create discussions with
clients
– The system tracks the results and graphs them per client
as well as outcomes for the program.
– Tracking change using data, adjusting the treatment plan
as appropriate.
– Used a part of the high alert system.
– Data projected electronically and magnified for
consideration during treatment team meetings..

15
© 2019 The Joint Commission. All Rights Reserved.
What process did your organization utilize to selecta standardized instrument for measurement based care?

16
© 2019 The Joint Commission. All Rights Reserved.
What process did you use to implementmeasurement based care?
17
© 2019 The Joint Commission. All Rights Reserved.
How are you using your MBC data in care, treatment and services and to improve the overall services for the population you serve?
18
© 2019 The Joint Commission. All Rights Reserved.
Maeve O’Neill, MEd, LCDC, LPC-S, CHC
Shawna Granato, LISW-S
19
© 2019 The Joint Commission. All Rights Reserved.
Our story...
Maeve O’Neill, MEd, LCDC, LPC-S, CHC
Served as Chief Ethics & Compliance Officer at Addiction Campuses 2017-2019
Holly Steward, MEd, LPC
Clinical Director, The Treehouse
Mareikie Muszynski, MSW, LICSW
Clinical Director, Swift River
Shawna Granato, LISW-S
Clinical Director, The Bluffs
20
© 2019 The Joint Commission. All Rights Reserved.
Our experience implementing MBC...
TJC-”Using data as feedback toward achieving outcomes”
*Leadership/Culture enhanced and supportive of outcomes
*Teamwork empowered and challenges addressed
*Staff engaged and services improved care

21
© 2019 The Joint Commission. All Rights Reserved.
Leadership - Teamwork - Staff

22
© 2019 The Joint Commission. All Rights Reserved.
What process did your organization utilize to selecta standardized instrument for measurement based care?
23
© 2019 The Joint Commission. All Rights Reserved.
Leadership and Culture● Part of a robust and integrated Compliance program/plan
● Researched several standardized tools
● Reviewed numerous options and consulted with experts
● Discussed with all locations and teams
● Decision to utilize current tool-DASS weekly
● Education and Training of all providers
● Worked with IT/EMR for data
● Weekly calls to monitor
● Monthly data to audit
● Culture of Quality and Performance Improvement
24
© 2019 The Joint Commission. All Rights Reserved.
Payors saw the value and authorized more care!
UR used in appeals with insurance companies.
Insurance Companies asked about MBC and were
impressed with weekly scales and how integrated into
care.
Getting in-network with insurance panels was easier
based on MBC data.
25
© 2019 The Joint Commission. All Rights Reserved.
What process did you use to implementmeasurement based care?

26
© 2019 The Joint Commission. All Rights Reserved.
Teamwork and Challenges
● Building trust in purpose of the tool with staff/patients
● Integrating with existing workflow
● Onboarding new staff to process
● Evaluating staff performance in administering the tool
● Adjusting as needed-EMR
● Management investment in auditing and staff coaching
● Staff remembering to do it
● Staff turnover were challenges
● EMR functionality in data collection

27
© 2019 The Joint Commission. All Rights Reserved.
Patients noted value in surveys!
28
© 2019 The Joint Commission. All Rights Reserved.
How are you using your MBC data in care, treatment and services and to improve the overall services for the population you serve?
29
© 2019 The Joint Commission. All Rights Reserved.
Staff and Service Outcomes:
● Patients saw value in looking at scores during treatment
● Better documentation
● Improved treatment planning and discharge planning
● More individualized care based on DASS scores
● Added services such as yoga, meditation path, ropes
● Adjusted schedules and curricula to meet patient needs
30
© 2019 The Joint Commission. All Rights Reserved.
Staff saw value and impact!
Integrated DASS scores with tracking patient risk
assessments to manage safety needs.
Shared understanding and language about patient
status in regards to their coping with depressions,
anxiety and stress.
Daily emails and communicaiton aided proper
intervention and early detection of patient risk.

31
© 2019 The Joint Commission. All Rights Reserved.
Antoinette Giedzinska, PhD
32
© 2019 The Joint Commission. All Rights Reserved.
3 Levels Of Care• Acute Inpatient
• Residential• Mood• ADD/CO• Trauma Recovery• Chronic Pain
Recovery
• Outpatient• PHP• IOPJaime W. Vinck, MC, LPC, NCC
Group Chief Executive Officer

33
© 2019 The Joint Commission. All Rights Reserved.
What process did your organization utilize to selecta standardized instrument for measurement based care?
34
© 2019 The Joint Commission. All Rights Reserved.
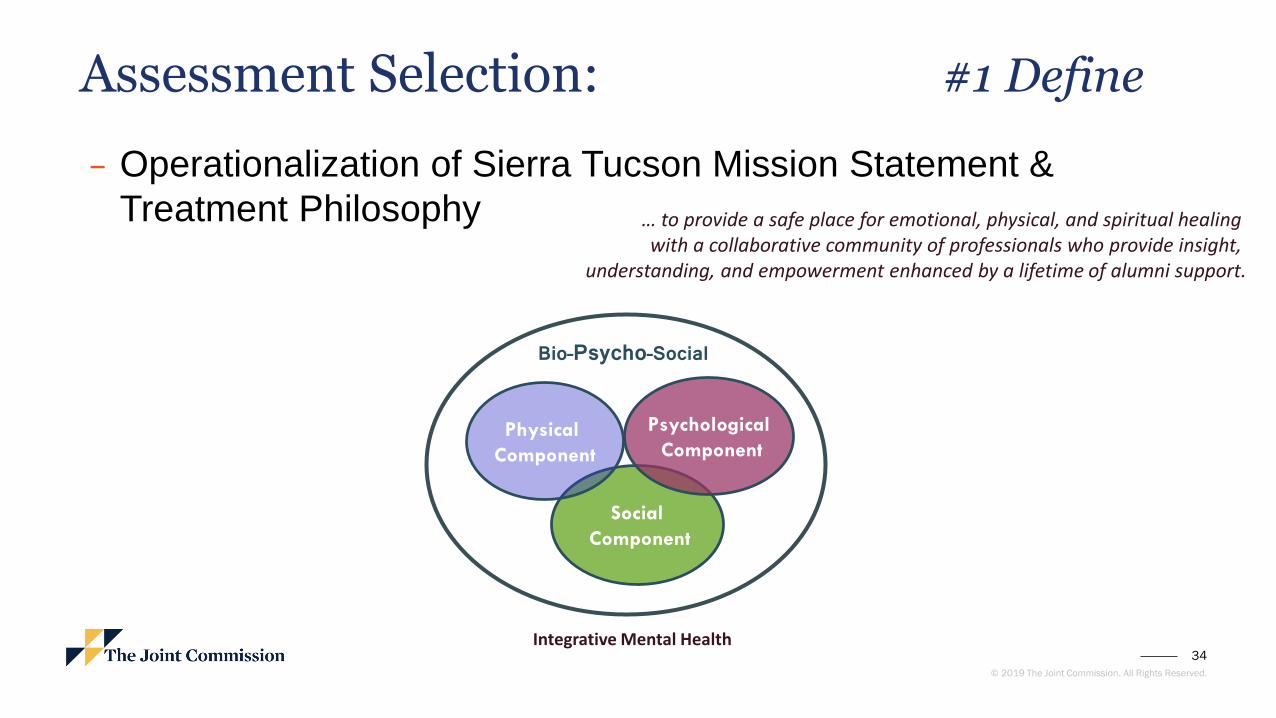
Assessment Selection: #1 Define
− Operationalization of Sierra Tucson Mission Statement &
Treatment Philosophy … to provide a safe place for emotional, physical, and spiritual healing with a collaborative community of professionals who provide insight,
understanding, and empowerment enhanced by a lifetime of alumni support.
Social
Component
Bio–Psycho–Social
Integrative Mental Health
Physical
Component
Psychological
Component
35
© 2019 The Joint Commission. All Rights Reserved.
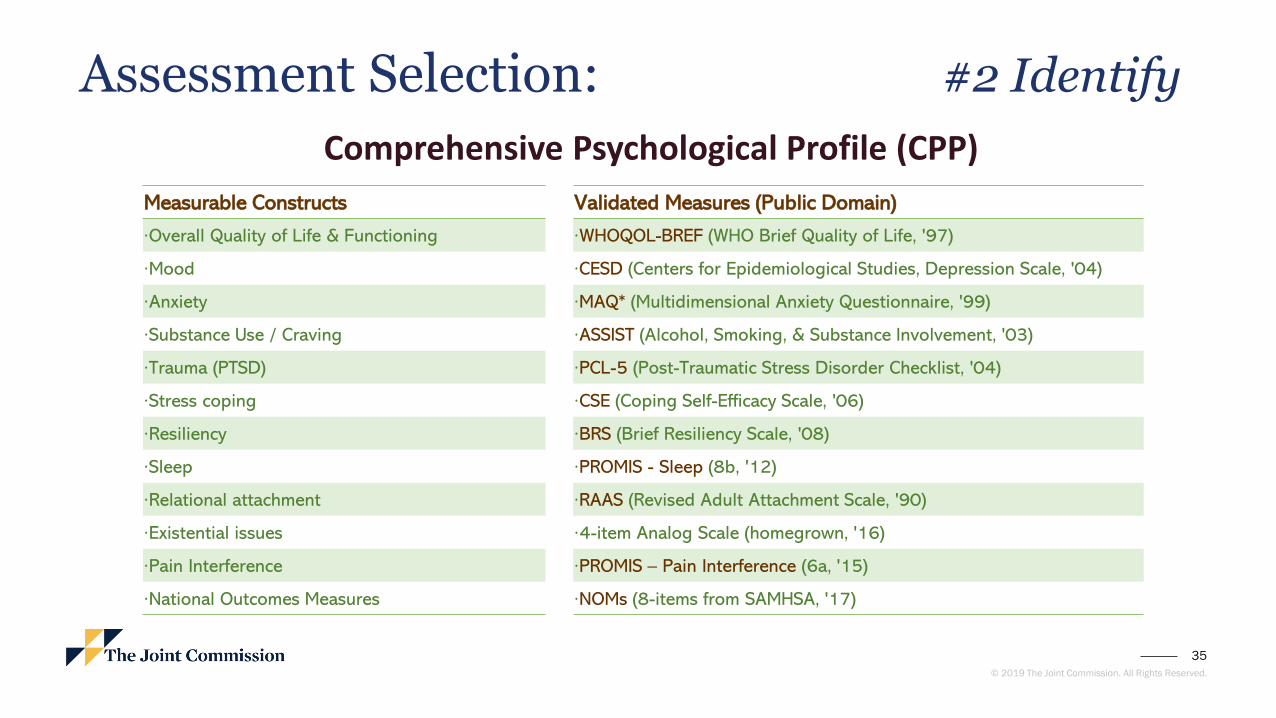
Assessment Selection: #2 Identify
Comprehensive Psychological Profile (CPP)
Measurable Constructs Validated Measures (Public Domain)
·Overall Quality of Life & Functioning ·WHOQOL-BREF (WHO Brief Quality of Life, '97)
·Mood ·CESD (Centers for Epidemiological Studies, Depression Scale, '04)
·Anxiety ·MAQ* (Multidimensional Anxiety Questionnaire, '99)
·Substance Use / Craving ·ASSIST (Alcohol, Smoking, & Substance Involvement, '03)
·Trauma (PTSD) ·PCL-5 (Post-Traumatic Stress Disorder Checklist, '04)
·Stress coping ·CSE (Coping Self-Efficacy Scale, '06)
·Resiliency ·BRS (Brief Resiliency Scale, '08)
·Sleep ·PROMIS - Sleep (8b, '12)
·Relational attachment ·RAAS (Revised Adult Attachment Scale, '90)
·Existential issues ·4-item Analog Scale (homegrown, '16)
·Pain Interference ·PROMIS – Pain Interference (6a, '15)
·National Outcomes Measures ·NOMs (8-items from SAMHSA, '17)
36
© 2019 The Joint Commission. All Rights Reserved.
What process did you use to implementmeasurement based care?

37
© 2019 The Joint Commission. All Rights Reserved.
Methodology: Pre-Treatment Profile Assessment (PTE)
At Admission
All Admitted Patients
Admission Paperwork Outcomes Consent
ResidentialFirst 1-3 days
PTE - Admins Pre-Tx Evaluation
Proctor AdministrationData Entry & MergeStaff Tasks:
24-hourTurn-around
Staff Tasks:
PTE - Prep
PDFs uploaded to EMRHand-outs to Med Provider
ResidentialFirst 3-5 days
Medical Provider
PTE - Feedback Review PTE ProfileTx Plan Decision MakingUpdate EMR
38
© 2019 The Joint Commission. All Rights Reserved.
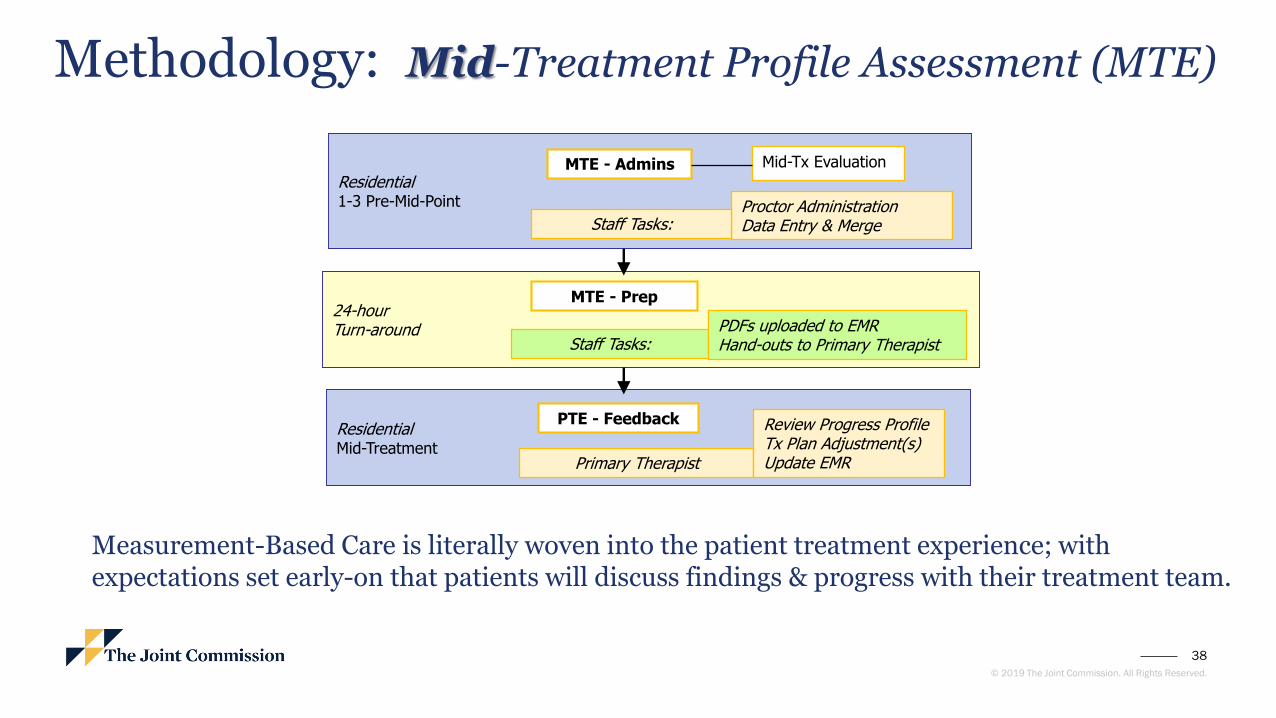
Residential1-3 Pre-Mid-Point
MTE - Admins Mid-Tx Evaluation
Proctor AdministrationData Entry & MergeStaff Tasks:
24-hourTurn-around
Staff Tasks:
MTE - Prep
PDFs uploaded to EMRHand-outs to Primary Therapist
ResidentialMid-Treatment
Primary Therapist
PTE - Feedback Review Progress ProfileTx Plan Adjustment(s)Update EMR
Methodology: Mid-Treatment Profile Assessment (MTE)
Measurement-Based Care is literally woven into the patient treatment experience; with expectations set early-on that patients will discuss findings & progress with their treatment team.

39
© 2019 The Joint Commission. All Rights Reserved.
How are you using your MBC data in care, treatment and services and to improve the overall services for the population you serve?

40
© 2019 The Joint Commission. All Rights Reserved.
Implementation: Pre-Treatment Profile Results
-
10
20
30
40
50
60
70
80
Physical Emotional Social Environment
Sum
mar
y Sc
ore
s:
X <
20
= V
ery
Po
or;
X <
40
= P
oo
r;
40
< X
< 6
0, =
Fai
rX
> 6
0 =
Go
od
;
X >
80
= V
ery
Go
od
Domains of Life Quality
Quality of Life FunctioningHigher Scores are Better
General
You
Your MAQ T-score is: 84 99 (your percentile)
Which indicates that you may be experiencing a severe degree of Generalized Anxiety at this time.
Panicky Symptoms: T-Scores Percentile
Likely to be present or may be a problem for you. 80 98%
Social Anxiety:
Likely to be present or may be a problem for you. 80 99%
Worrying:
Likely to be present or may be a problem for you. 79 98%
Negative chatter:
Likely to be present or may be a problem for you. 76 99%
MAQ Summary
Anxiety
Data graphs are given to Patients & are discussed with Medical Providers, engendering:
• Treatment Decision Making• Therapeutic Alliance
• Insight / Understanding• Substantiation of Clinical Diagnosis
• Validation
41
© 2019 The Joint Commission. All Rights Reserved.
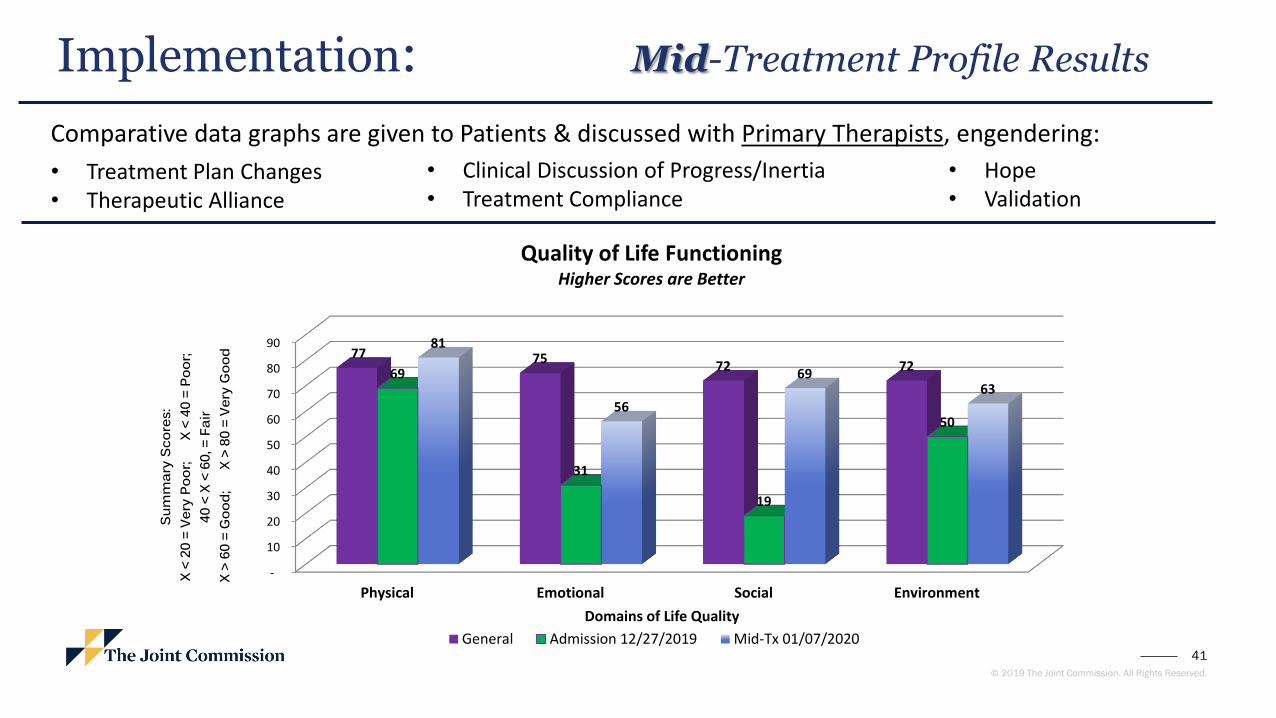
Implementation: Mid-Treatment Profile Results
-
10
20
30
40
50
60
70
80
90
Physical Emotional Social Environment
77 7572 72
69
31
19
50
81
56
6963
Sum
mar
y Sc
ores
: X
< 20
= V
ery
Poor
;
X <
40
= Po
or;
40 <
X <
60,
= F
air
X >
60 =
Goo
d;
X
> 80
= V
ery
Goo
d
Domains of Life Quality
Quality of Life FunctioningHigher Scores are Better
General Admission 12/27/2019 Mid-Tx 01/07/2020
Comparative data graphs are given to Patients & discussed with Primary Therapists, engendering:
• Treatment Plan Changes• Therapeutic Alliance
• Clinical Discussion of Progress/Inertia• Treatment Compliance
• Hope• Validation
42
© 2019 The Joint Commission. All Rights Reserved.
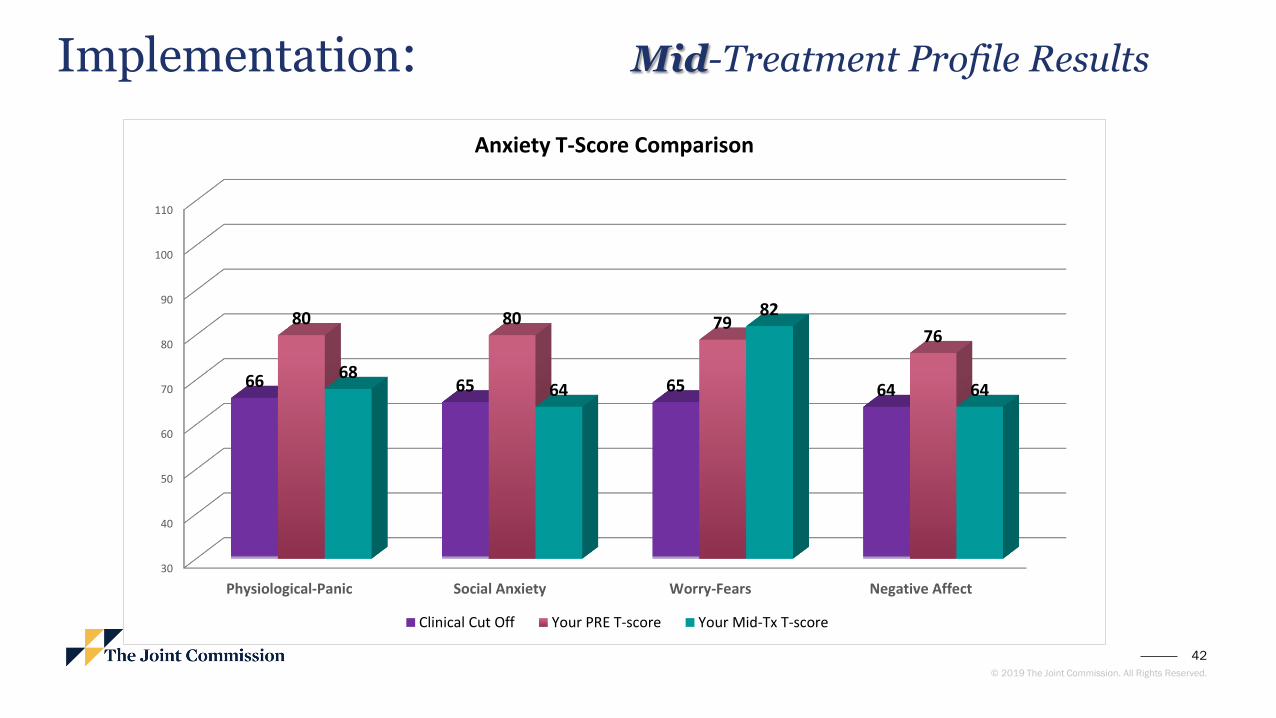
Implementation: Mid-Treatment Profile Results
30
40
50
60
70
80
90
100
110
Physiological-Panic Social Anxiety Worry-Fears Negative Affect
66 65 65 64
80 80 7976
6864
82
64
Anxiety T-Score Comparison
Clinical Cut Off Your PRE T-score Your Mid-Tx T-score
43
© 2019 The Joint Commission. All Rights Reserved.
Measure to Improve: Aggregating & Analysis
− Minimum Sample size: N= 500
− Multivariate analyses (hierarchical multiple regression, path analyses, etc).
− Identifying predictor & contributing variables associated with recovery success and relapse.
− What’s working? What’s not?
− Repeated measures analyses
− Are “changes” due to chance?
− Clinical v Statistical significance
− Program Fidelity
− Correlations to investigate interactions & associations of programmatic effectiveness.
− Understanding AMA behaviors
− Patient Satisfaction (e.g., Net-Promoter Score)

44
© 2019 The Joint Commission. All Rights Reserved.
Questions

45
© 2019 The Joint Commission. All Rights Reserved.
To register for a webinar or watch a replay, visit:https://www.jointcommission.org/webinarsBHC
46
© 2019 The Joint Commission. All Rights Reserved.
Behavioral Health Care Accreditation
Business Development Team
40
Julia Finken, BSN, MBA, CPHQ, CSSBB
Executive Director
630-792-5790
Darrell Anderson
Manager- BHC
630-792-5866
Yvonne Rockwood, MBA,MHA,CPHQ
Associate Director – BHC
630-792-5792
Eastern Region Western Region
Tiffany Holloway
Manager - BHC
630-792-5810
Colette Bukowski, LPCC-S
Associate Director -BHC
630-792-5812

















