
Behavioral Health HEDIS Measures · Behavioral Health HEDIS Measures Measurement/Age Criteria...
94
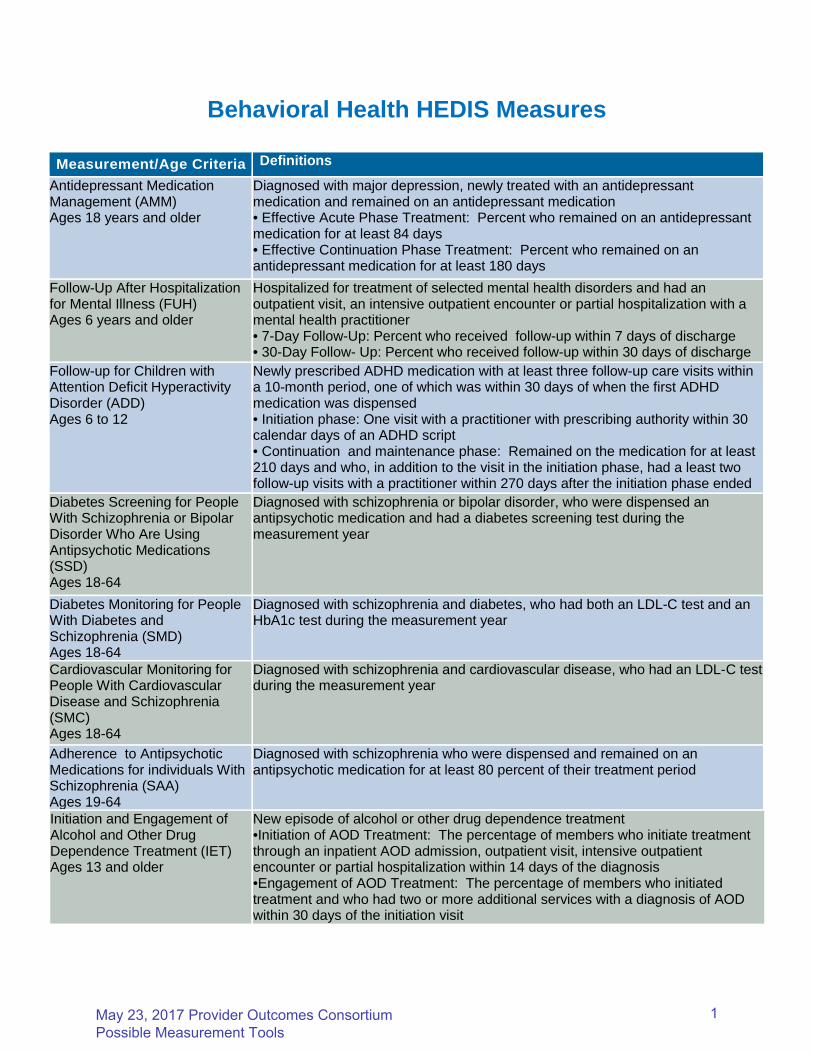
Behavioral Health HEDIS Measures Measurement/Age Criteria Definitions Antidepressant Medication Management (AMM) Ages 18 years and older Diagnosed with major depression, newly treated with an antidepressant medication and remained on an antidepressant medication • Effective Acute Phase Treatment: Percent who remained on an antidepressant medication for at least 84 days • Effective Continuation Phase Treatment: Percent who remained on an antidepressant medication for at least 180 days Follow-Up After Hospitalization for Mental Illness (FUH) Ages 6 years and older Hospitalized for treatment of selected mental health disorders and had an outpatient visit, an intensive outpatient encounter or partial hospitalization with a mental health practitioner • 7-Day Follow-Up: Percent who received follow-up within 7 days of discharge • 30-Day Follow- Up: Percent who received follow-up within 30 days of discharge Follow-up for Children with Attention Deficit Hyperactivity Disorder (ADD) Ages 6 to 12 Newly prescribed ADHD medication with at least three follow-up care visits within a 10-month period, one of which was within 30 days of when the first ADHD medication was dispensed • Initiation phase: One visit with a practitioner with prescribing authority within 30 calendar days of an ADHD script • Continuation and maintenance phase: Remained on the medication for at least 210 days and who, in addition to the visit in the initiation phase, had a least two follow-up visits with a practitioner within 270 days after the initiation phase ended Diabetes Screening for People With Schizophrenia or Bipolar Disorder Who Are Using Antipsychotic Medications (SSD) Ages 18-64 Diagnosed with schizophrenia or bipolar disorder, who were dispensed an antipsychotic medication and had a diabetes screening test during the measurement year Diabetes Monitoring for People With Diabetes and Schizophrenia (SMD) Ages 18-64 Diagnosed with schizophrenia and diabetes, who had both an LDL-C test and an HbA1c test during the measurement year Cardiovascular Monitoring for People With Cardiovascular Disease and Schizophrenia (SMC) Ages 18-64 Diagnosed with schizophrenia and cardiovascular disease, who had an LDL-C test during the measurement year Adherence to Antipsychotic Medications for individuals With Schizophrenia (SAA) Ages 19-64 Diagnosed with schizophrenia who were dispensed and remained on an antipsychotic medication for at least 80 percent of their treatment period Initiation and Engagement of Alcohol and Other Drug Dependence Treatment (IET) Ages 13 and older New episode of alcohol or other drug dependence treatment •Initiation of AOD Treatment: The percentage of members who initiate treatment through an inpatient AOD admission, outpatient visit, intensive outpatient encounter or partial hospitalization within 14 days of the diagnosis •Engagement of AOD Treatment: The percentage of members who initiated treatment and who had two or more additional services with a diagnosis of AOD within 30 days of the initiation visit May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools 1
Transcript of Behavioral Health HEDIS Measures · Behavioral Health HEDIS Measures Measurement/Age Criteria...
Behavioral Health HEDIS Measures
Measurement/Age Criteria Definitions
Antidepressant MedicationManagement (AMM)Ages 18 years and older
Diagnosed with major depression, newly treated with an antidepressantmedication and remained on an antidepressant medication• Effective Acute Phase Treatment: Percent who remained on an antidepressantmedication for at least 84 days• Effective Continuation Phase Treatment: Percent who remained on anantidepressant medication for at least 180 days
Follow-Up After Hospitalizationfor Mental Illness (FUH)Ages 6 years and older
Hospitalized for treatment of selected mental health disorders and had anoutpatient visit, an intensive outpatient encounter or partial hospitalization with amental health practitioner• 7-Day Follow-Up: Percent who received follow-up within 7 days of discharge• 30-Day Follow- Up: Percent who received follow-up within 30 days of discharge
Follow-up for Children withAttention Deficit HyperactivityDisorder (ADD)Ages 6 to 12
Newly prescribed ADHD medication with at least three follow-up care visits withina 10-month period, one of which was within 30 days of when the first ADHDmedication was dispensed• Initiation phase: One visit with a practitioner with prescribing authority within 30calendar days of an ADHD script• Continuation and maintenance phase: Remained on the medication for at least210 days and who, in addition to the visit in the initiation phase, had a least twofollow-up visits with a practitioner within 270 days after the initiation phase ended
Diabetes Screening for PeopleWith Schizophrenia or BipolarDisorder Who Are UsingAntipsychotic Medications(SSD)Ages 18-64
Diagnosed with schizophrenia or bipolar disorder, who were dispensed anantipsychotic medication and had a diabetes screening test during themeasurement year
Diabetes Monitoring for PeopleWith Diabetes andSchizophrenia (SMD)Ages 18-64
Diagnosed with schizophrenia and diabetes, who had both an LDL-C test and anHbA1c test during the measurement year
Cardiovascular Monitoring forPeople With CardiovascularDisease and Schizophrenia(SMC)Ages 18-64
Diagnosed with schizophrenia and cardiovascular disease, who had an LDL-C testduring the measurement year
Adherence to AntipsychoticMedications for individuals WithSchizophrenia (SAA)Ages 19-64
Diagnosed with schizophrenia who were dispensed and remained on anantipsychotic medication for at least 80 percent of their treatment period
Initiation and Engagement ofAlcohol and Other DrugDependence Treatment (IET)Ages 13 and older
New episode of alcohol or other drug dependence treatment•Initiation of AOD Treatment: The percentage of members who initiate treatmentthrough an inpatient AOD admission, outpatient visit, intensive outpatientencounter or partial hospitalization within 14 days of the diagnosis•Engagement of AOD Treatment: The percentage of members who initiatedtreatment and who had two or more additional services with a diagnosis of AODwithin 30 days of the initiation visit
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
1

SUMMARY TABLE OF MEASURES, PRODUCT LINES AND CHANGES
HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
General Guidelines for Data Collection and Reporting
Updated deadlines in General Guideline 9.
Clarified in General Guidelines 17 and 18 that members with dual commercial and Medicaidcoverage should only be reported in the commercial HEDIS reports.
Added General Guideline 20; renumbered subsequent guidelines.
Clarified General Guideline 23 (combined former General Guidelines 22 and 23).
Updated the “plan-lock” deadline in General Guideline 30.
Added the Electronic Clinical Data Systems (ECDS) data collection method to GeneralGuideline 33.
Clarified in the Note in General Guideline 33 that if any data found in a supplemental datasource are considered a supplemental data hit.
Clarified requirements for General Guideline 34.
Replaced the Human Papillomavirus Vaccine for Female Adolescents measure with theImmunizations for Adolescents measures in General Guideline 39.
Added requirement for the Independent Laboratory Value Set in General Guideline 41.
Added General Guideline 43.
Added CVX—Vaccines Administered to General Guideline 44 (formerly General Guideline43).
Added General Guideline 46.
Guidelines for Calculations and Sampling
Deleted the Human Papillomavirus Vaccine for Female Adolescents measure from themembership-dependent denominators in the Guidelines for the Hybrid Method.
Deleted the Human Papillomavirus Vaccine for Female Adolescents measure from Table 1:Sample Size Information for Hybrid Measures.
Revised Table 1 to indicate that prior year rates may not be used to reduce the sample forthe Immunizations for Adolescents measure.
EFFECTIVENESS OF CARE
Guidelines for Effectiveness of Care
Adult BMI Assessment No changes to this measure.
Weight Assessment and Counseling for Nutrition and Physical Activity for Children/ Adolescents
Included examples of services specific to the assessment or treatment of an acute or chroniccondition that do not count toward the “Counseling for nutrition” and “Counseling for physicalactivity” indicators.
Replaced “Each of the 3 rates” with “” for the “Measurement year” row in Table WCC-1/2.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
2
HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
EFFECTIVENESS OF CARE
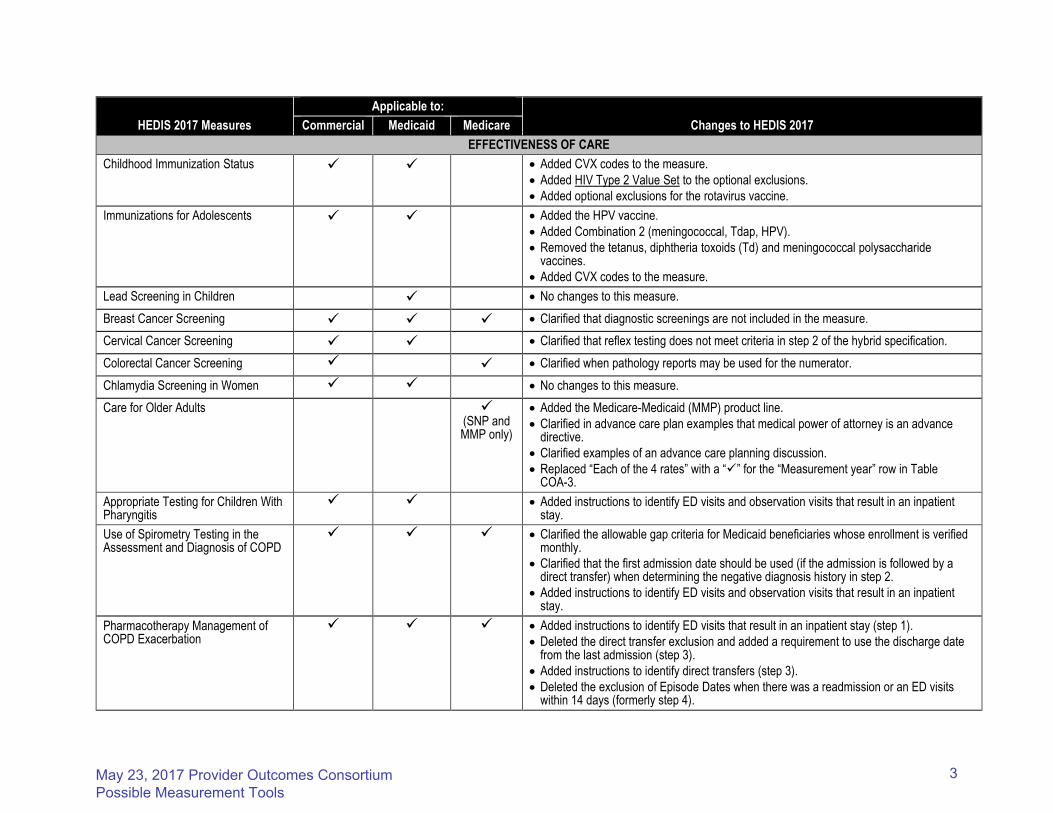
Childhood Immunization Status Added CVX codes to the measure.
Added HIV Type 2 Value Set to the optional exclusions.
Added optional exclusions for the rotavirus vaccine.
Immunizations for Adolescents Added the HPV vaccine.
Added Combination 2 (meningococcal, Tdap, HPV).
Removed the tetanus, diphtheria toxoids (Td) and meningococcal polysaccharidevaccines.
Added CVX codes to the measure.
Lead Screening in Children No changes to this measure.
Breast Cancer Screening Clarified that diagnostic screenings are not included in the measure.
Cervical Cancer Screening Clarified that reflex testing does not meet criteria in step 2 of the hybrid specification.
Colorectal Cancer Screening Clarified when pathology reports may be used for the numerator.
Chlamydia Screening in Women No changes to this measure.
Care for Older Adults
(SNP and MMP only)
Added the Medicare-Medicaid (MMP) product line.
Clarified in advance care plan examples that medical power of attorney is an advancedirective.
Clarified examples of an advance care planning discussion.
Replaced “Each of the 4 rates” with a “” for the “Measurement year” row in TableCOA-3.
Appropriate Testing for Children With Pharyngitis
Added instructions to identify ED visits and observation visits that result in an inpatientstay.
Use of Spirometry Testing in the Assessment and Diagnosis of COPD
Clarified the allowable gap criteria for Medicaid beneficiaries whose enrollment is verifiedmonthly.
Clarified that the first admission date should be used (if the admission is followed by adirect transfer) when determining the negative diagnosis history in step 2.
Added instructions to identify ED visits and observation visits that result in an inpatientstay.
Pharmacotherapy Management of COPD Exacerbation
Added instructions to identify ED visits that result in an inpatient stay (step 1).
Deleted the direct transfer exclusion and added a requirement to use the discharge datefrom the last admission (step 3).
Added instructions to identify direct transfers (step 3).
Deleted the exclusion of Episode Dates when there was a readmission or an ED visitswithin 14 days (formerly step 4).
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
3

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
EFFECTIVENESS OF CARE
Medication Management for People With Asthma
No changes to this measure.
Asthma Medication Ratio No changes to this measure.
Controlling High Blood Pressure
Added a Note clarifying the intent when confirming the diagnosis of hypertension.
Revised Table CBP-1/2/3 to include the medical record data elements only.
Persistence of Beta-Blocker Treatment After a Heart Attack
Removed language instructing organizations to use only facility claims to identify dischargesand diagnoses for denominator events. This is now addressed in General Guideline 46.
Added instructions to identify direct transfers.
Statin Therapy for Patients With Cardiovascular Disease
Added a Note section.
Comprehensive Diabetes Care
Added an administrative method and new value set to identify negative eye exams in the yearprior to the measurement year.
Added glycohemoglobin, glycated hemoglobin and glycosylated hemoglobin as acceptableHbA1c tests.
Clarified documentation requirements for a negative eye exam.
Replaced “Each of the 7 rates” with a “” for the “Measurement year” row in Table CDC-1/2/3.
Statin Therapy for Patients With Diabetes
Clarified that optional exclusions are excluded from the denominator for both rates.
Added a Note.
Disease-Modifying Anti-Rheumatic Drug Therapy for Rheumatoid Arthritis
Added the HIV Type 2 Value Set to the optional exclusions.
Osteoporosis Management in Women Who Had a Fracture
Added a requirement to not include ED visits and observation visits that result in an inpatientstay in steps 1 and 2 of the event/diagnosis.
Added instructions to identify direct transfers.
Clarified that for direct transfers, the first admission date should be used when determining thenumber of days prior to the IESD in step 4.
Antidepressant Medication Management
Revised the required exclusion instructions for inpatient stays to search for admissions ordischarges that occur during the 121-day period.
Clarified the number of gap days allowed for each numerator.
Follow-Up Care for Children Prescribed ADHD Medication
No changes to this measure.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
4

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
EFFECTIVENESS OF CARE
Follow-Up After Hospitalization for Mental Illness
Removed language instructing organizations to use only facility claims to identify discharges and diagnoses for denominator events. This is now addressed in General Guideline 46.
Added value sets to identify direct transfers.
Follow-Up After Emergency Department Visit for Mental Illness
First-year measure.
Follow-Up After Emergency Department Visit for Alcohol and Other Drug Dependence
First-year measure.
Diabetes Screening for People With Schizophrenia or Bipolar Disorder Who Are Using Antipsychotic Medications
Replaced all references to BH ED POS Value Set with ED POS Value Set (the codes in these value sets are the same).
Added cariprazine to the description of “Miscellaneous antipsychotic agents” in Table SSD-D.
Diabetes Monitoring for People With Diabetes and Schizophrenia
Replaced all references to BH ED POS Value Set with ED POS Value Set (the codes in these value sets are the same).
Clarified the criteria for optional exclusions.
Cardiovascular Monitoring for People With Cardiovascular Disease and Schizophrenia
Replaced all references to BH ED POS Value Set with ED POS Value Set (the codes in these value sets are the same).
Adherence to Antipsychotic Medications for Individuals With Schizophrenia
Clarified how to calculate number of days covered if both oral medications and long-acting injections are dispensed in the new Notes in the Definition section.
Replaced all references to BH ED POS Value Set with ED POS Value Set (the codes in these value sets are the same).
Added Cariprazine to the description of “Miscellaneous antipsychotic agents (oral)” in Table SAA-A.
Metabolic Monitoring for Children and Adolescents on Antipsychotics
Added Cariprazine to the description of “Second generation antipsychotic medications” in Table APM-A.
Annual Monitoring for Patients on Persistent Medications
No changes to this measure.
Medication Reconciliation Post-Discharge
Removed the anchor date requirement.
Added value sets to identify direct transfers.
Clarified medical record documentation requirements for medication reconciliation.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
5

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
EFFECTIVENESS OF CARE
Non-Recommended Cervical Cancer Screening in Adolescent Females
Added HIV Type 2 Value Set to the required exclusions.
Non-Recommended PSA-Based Screening in Older Men
No changes to this measure.
Appropriate Treatment for Children With Upper Respiratory Infection
Added instructions to identify ED visits and observation visits that result in aninpatient stay.
Added a requirement to not include denied claims in the numerator.
Avoidance of Antibiotic Treatment in Adults With Acute Bronchitis
Revised the allowable gap and anchor date criteria.
Added instructions to identify ED visits and observation visits that result in aninpatient stay.
Added two value sets to step 3 of the event/diagnosis criteria (HIV Type 2 ValueSet; Disorders of the Immune System Value Set).
Added a requirement to not include denied claims in the numerator.
Use of Imaging Studies for Low Back Pain
Replaced the Low Back Pain Value Set with the Uncomplicated Low Back PainValue Set in step 1 of the event/diagnosis.
Added instructions to identify ED visits and observation visits that result in aninpatient stay.
Renamed the Osteopathic Manipulative Treatment Value Set to Osteopathic andChiropractic Manipulative Treatment Value Set in step 1 of the event/diagnosis.
Added the Physical Therapy Value Set to step 1 of the event/diagnosis.
Added the Telehealth Value Set to step 1 of the event/diagnosis.
Replaced the Low Back Pain Value Set with the Uncomplicated Low Back PainValue Set in step 3 of the event/diagnosis.
Revised the look back period to exclude members with recent trauma from 12-months to 3-months in step 4 of the event/diagnosis.
Added required exclusions and the following value sets: HIV Value Set, SpinalInfection Value Set, Organ Transplant Other Than Kidney Value Set, KidneyTransplant Value Set to step 4 of the event/diagnosis.
Added a required exclusion for prolonged use of corticosteroids to step 4 of theevent/diagnosis.
Replaced the Low Back Pain Value Set with the Uncomplicated Low Back PainValue Set in the numerator.
Added a requirement to not include denied claims in the numerator.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
6

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
EFFECTIVENESS OF CARE
Use of Multiple Concurrent Antipsychotics in Children and Adolescents
Added Cariprazine to the description of “Second generation antipsychotic medications” in Table APC-A.
Added a requirement to not include denied claims in the numerator.
Added a Note.
Removed “Numerator events by supplemental data” from Table APC-1/2.
Potentially Harmful Drug-Disease Interactions in the Elderly
Updated the medications included in the measure to align with the 2015 American Geriatrics Society Beers Criteria.
Removed delirium codes from the Psychosis Value Set.
Added a requirement to not include denied claims in the numerator for all rates.
Use of High-Risk Medications in the Elderly
Updated the medications included in the measure to align with the 2015 American Geriatrics Society Beers Criteria.
Revised numerators 1 and 2 for high-risk medications with days supply criteria (Table DAE-B) and with average daily dose criteria (Table DAE-C).
Revised numerator 2 to identify multiple dispensing events for the same high-risk medication.
Added a requirement to not include denied claims in numerators 1 and 2.
Medicare Health Outcomes Survey
This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 6: Specifications for the Medicare Health Outcomes Survey.
Fall Risk Management
This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 6: Specifications for the Medicare Health Outcomes Survey.
Management of Urinary Incontinence in Older Adults
This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 6: Specifications for the Medicare Health Outcomes Survey.
Osteoporosis Testing in Older Women This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 6: Specifications for the Medicare Health Outcomes Survey.
Physical Activity in Older Adults This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 6: Specifications for the Medicare Health Outcomes Survey.
Aspirin Use and Discussion This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 3: Specifications for Survey Measures.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
7

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
EFFECTIVENESS OF CARE
Flu Vaccinations for Adults Ages 18-64 This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 3: Specifications for Survey Measures.
Flu Vaccinations for Adults Ages 65 and Older
This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 3: Specifications for Survey Measures.
Medical Assistance With Smoking and Tobacco Use Cessation
This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 3: Specifications for Survey Measures.
Pneumococcal Vaccination Status for Older Adults
This measure is collected using survey methodology. Detailed specifications and summary of changes are contained in HEDIS 2017, Volume 3: Specifications for Survey Measures.
ACCESS/AVAILABILITY OF CARE
Adults’ Access to Preventive/ Ambulatory Health Services
No changes to this measure.
Children’s and Adolescents’ Access to Primary Care Practitioners
No changes to this measure.
Annual Dental Visit No changes to this measure.
Initiation and Engagement of Alcohol and Other Drug Dependence Treatment
Added instructions to identify direct transfers.
Added instructions to identify ED visits that result in an inpatient stay.
Clarified that an AOD diagnosis is not required for direct transfers when identifying the IESD.
Prenatal and Postpartum Care Clarified that the prenatal visit for the Timeliness of Prenatal Care numerator can occur on the date of enrollment.
Clarified in the Note that the EDD must be on or between November 6 of the year prior to the measurement year and November 5 of the measurement year.
Added a Note explaining that the organization may use EDD to identify the first trimester for the Timeliness of Prenatal Care rate and use the date of delivery for the Postpartum Care rate.
Replaced “Each of the 2 rates” with a “” for the “Measurement year” row in Table PPC-1/2.
Call Answer Timeliness No changes to this measure.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
8

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
EXPERIENCE OF CARE
Use of First-Line Psychosocial Care for Children and Adolescents on Antipsychotics
Added Cariprazine to the description of “Second generation antipsychoticmedications” in Table APP-A.
CAHPS Health Plan Survey 5.0H, Adult Version
This measure is collected using survey methodology. Detailed specifications andsummary of changes are contained in HEDIS 2017, Volume 3: Specifications forSurvey Measures.
CAHPS Health Plan Survey 5.0H, Child Version
This measure is collected using survey methodology. Detailed specifications andsummary of changes are contained in HEDIS 2017, Volume 3: Specifications forSurvey Measures.
Children With Chronic Conditions This measure is collected using survey methodology. Detailed specifications andsummary of changes for the measure are contained in HEDIS 2017, Volume 3:Specifications for Survey Measures.
UTILIZATION AND RISK ADJUSTED UTILIZATION
Guidelines for Utilization Measures “Guidelines for Utilization and Risk Adjusted Utilization Measures” have beenrenamed, “Guidelines for Utilization Measures.”
Clarified in General Guideline 6 that all inpatient stays must be considered,regardless of payment status, when identifying ED visits that do not result in aninpatient stay.
Frequency of Ongoing Prenatal Care Clarified the example calculation in step 2.
Well-Child Visits in the First 15 Months of Life
Clarified that services specific to the assessment or treatment of an acute orchronic condition do not count toward the measure.
Well-Child Visits in the Third, Fourth, Fifth and Sixth Years of Life
Clarified that services specific to the assessment or treatment of an acute orchronic condition do not count toward the measure.
Adolescent Well-Care Visits Clarified that services specific to the assessment or treatment of an acute orchronic condition do not count toward the measure.
Frequency of Selected Procedures No changes to this measure.
Ambulatory Care Added instructions to identify ED visits that result in an inpatient stay.
Inpatient Utilization—General Hospital/Acute Care
No changes to this measure.
Identification of Alcohol and Other Drug Services
Deleted instructions to use place of service or location of service codes to excludeservices known to be inpatient.
Added instructions to identify ED and observation visits that result in an inpatientstay.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
9

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
UTILIZATION AND RISK ADJUSTED UTILIZATION
Mental Health Utilization Added instructions to identify ED and observation visits that result in an inpatient stay.
Antibiotic Utilization No changes to this measure.
Standardized Healthcare-Associated Infection Ratio
First-year measure.
Guidelines for Risk Adjusted Utilization Measures
New section added for HEDIS 2017.
Plan All-Cause Readmissions Moved the Risk Adjustment Determination section to the Guidelines for Risk Adjusted Utilization Measures.
Clarified that organizations may not consolidate stays into a single stay if the discharge date from the first setting and the admission date of the second setting are two or more calendar days apart.
Added instructions to identify direct transfers.
Changed the reference of “discharges” to “admissions” in step 3 of the Numerator.
Inpatient Hospital Utilization Revised the instructions for calculating observed events.
Moved the Risk Adjustment Determination section to the Guidelines for Risk Adjusted Utilization Measures.
Clarified that the final Expected counts must be rounded to four decimal places using the .5 rule and no rounding should occur before this step.
Added Expected Discharges/1,000 Members as a data element to Table IHU-B-2/3, Table IHU-C-2/3 and Table IHU-D-2/3.
Emergency Department Utilization Added instructions to identify ED visits that result in an inpatient stay when identifying observed events.
Moved the Risk Adjustment Determination section to the Guidelines for Risk Adjusted Utilization Measures.
Clarified that the final Expected counts must be rounded to four decimal places using the .5 rule and no rounding should occur before this step.
Added Expected ED Visits/1,000 Members as a data element to Table EDU-B-2/3.
Hospitalization for Potentially Preventable Complications
Added instructions to identify direct transfers when identifying observed events.
Moved the Risk Adjustment Determination section to the Guidelines for Risk Adjusted Utilization Measures.
Clarified that the final Expected counts must be rounded to four decimal places using the .5 rule and no rounding should occur before this step.
Added Expected Chronic/Acute/Total ACSC Discharges/1,000 Members as a data element to Table HPC-B-3, Table HPC-C-3 and Table HPC-D-3.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
10
HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
RELATIVE RESOURCE USE
Guidelines for Relative Resource Use Measures
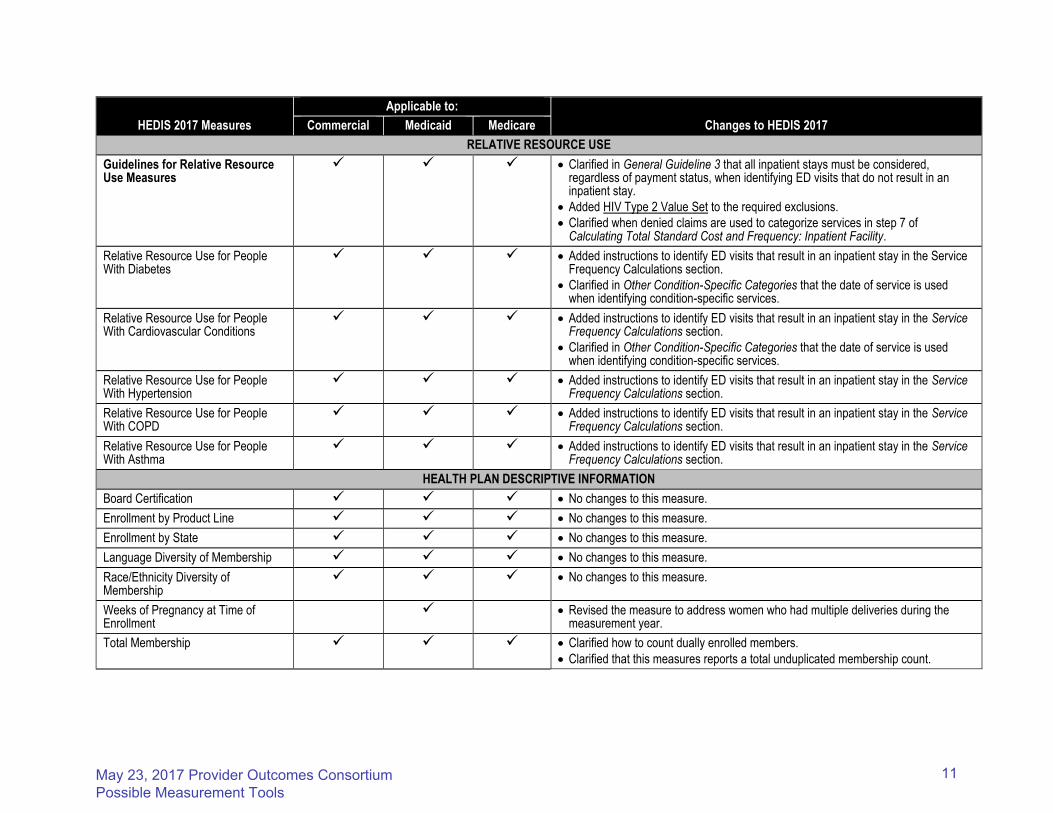
Clarified in General Guideline 3 that all inpatient stays must be considered, regardless of payment status, when identifying ED visits that do not result in an inpatient stay.
Added HIV Type 2 Value Set to the required exclusions.
Clarified when denied claims are used to categorize services in step 7 of Calculating Total Standard Cost and Frequency: Inpatient Facility.
Relative Resource Use for People With Diabetes
Added instructions to identify ED visits that result in an inpatient stay in the Service Frequency Calculations section.
Clarified in Other Condition-Specific Categories that the date of service is used when identifying condition-specific services.
Relative Resource Use for People With Cardiovascular Conditions
Added instructions to identify ED visits that result in an inpatient stay in the Service Frequency Calculations section.
Clarified in Other Condition-Specific Categories that the date of service is used when identifying condition-specific services.
Relative Resource Use for People With Hypertension
Added instructions to identify ED visits that result in an inpatient stay in the Service Frequency Calculations section.
Relative Resource Use for People With COPD
Added instructions to identify ED visits that result in an inpatient stay in the Service Frequency Calculations section.
Relative Resource Use for People With Asthma
Added instructions to identify ED visits that result in an inpatient stay in the Service Frequency Calculations section.
HEALTH PLAN DESCRIPTIVE INFORMATION
Board Certification No changes to this measure.
Enrollment by Product Line No changes to this measure.
Enrollment by State No changes to this measure.
Language Diversity of Membership No changes to this measure.
Race/Ethnicity Diversity of Membership
No changes to this measure.
Weeks of Pregnancy at Time of Enrollment
Revised the measure to address women who had multiple deliveries during the measurement year.
Total Membership Clarified how to count dually enrolled members.
Clarified that this measures reports a total unduplicated membership count.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
11

HEDIS 2017 Measures
Applicable to:
Changes to HEDIS 2017 Commercial Medicaid Medicare
MEASURES COLLECTED USING ELECTRONIC CLINICAL DATA SYSTEMS
Utilization of the PHQ-9 to Monitor Depression Symptoms for Adolescents and Adults
Revised specification layout to align with new ECDS measure layout.
Simplified steps to calculate the Initial Population.
Revised the data collection platform to require the use of XML.
Depression Remission or Response for Adolescents and Adults
First-year measure.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
12
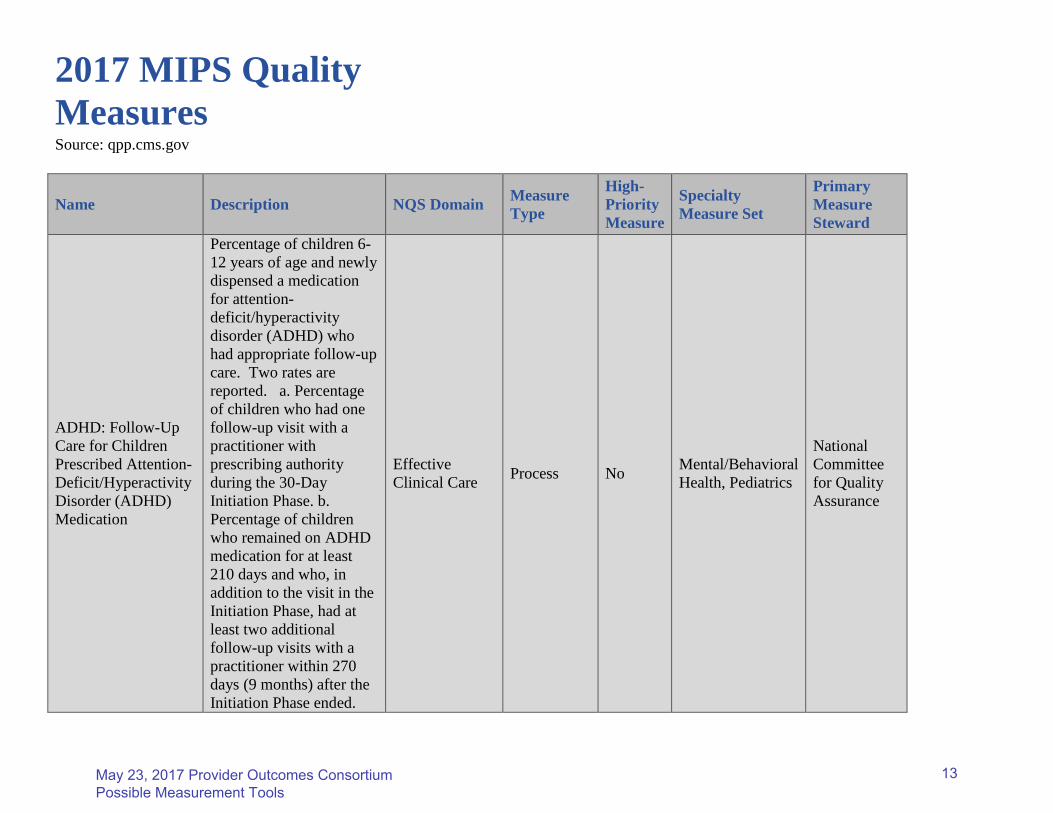
2017 MIPS Quality Measures Source: qpp.cms.gov
Name Description NQS Domain Measure Type
High-Priority Measure
Specialty Measure Set
Primary Measure Steward
ADHD: Follow-Up Care for Children Prescribed Attention-Deficit/Hyperactivity Disorder (ADHD) Medication
Percentage of children 6-12 years of age and newly dispensed a medication for attention-deficit/hyperactivity disorder (ADHD) who had appropriate follow-up care. Two rates are reported. a. Percentage of children who had one follow-up visit with a practitioner with prescribing authority during the 30-Day Initiation Phase. b. Percentage of children who remained on ADHD medication for at least 210 days and who, in addition to the visit in the Initiation Phase, had at least two additional follow-up visits with a practitioner within 270 days (9 months) after the Initiation Phase ended.
Effective Clinical Care Process No Mental/Behavioral
Health, Pediatrics
National Committee for Quality Assurance
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
13

Adherence to Antipsychotic Medications For Individuals with Schizophrenia
Percentage of individuals at least 18 years of age as of the beginning of the measurement period with schizophrenia or schizoaffective disorder who had at least two prescriptions filled for any antipsychotic medication and who had a Proportion of Days Covered (PDC) of at least 0.8 for antipsychotic medications during the measurement period (12 consecutive months)
Patient Safety Intermediate Outcome Yes Mental/Behavioral
Health
Health Services Advisory Group
Adult Major Depressive Disorder (MDD): Coordination of Care of Patients with Specific Comorbid Conditions
Percentage of medical records of patients aged 18 years and older with a diagnosis of major depressive disorder (MDD) and a specific diagnosed comorbid condition (diabetes, coronary artery disease, ischemic stroke, intracranial hemorrhage, chronic kidney disease [stages 4 or 5], End Stage Renal Disease [ESRD] or congestive heart failure) being treated by another clinician with communication to the clinician treating the comorbid condition
Communication and Care Coordination
Process Yes Mental/Behavioral Health
American Psychiatric Association
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
14
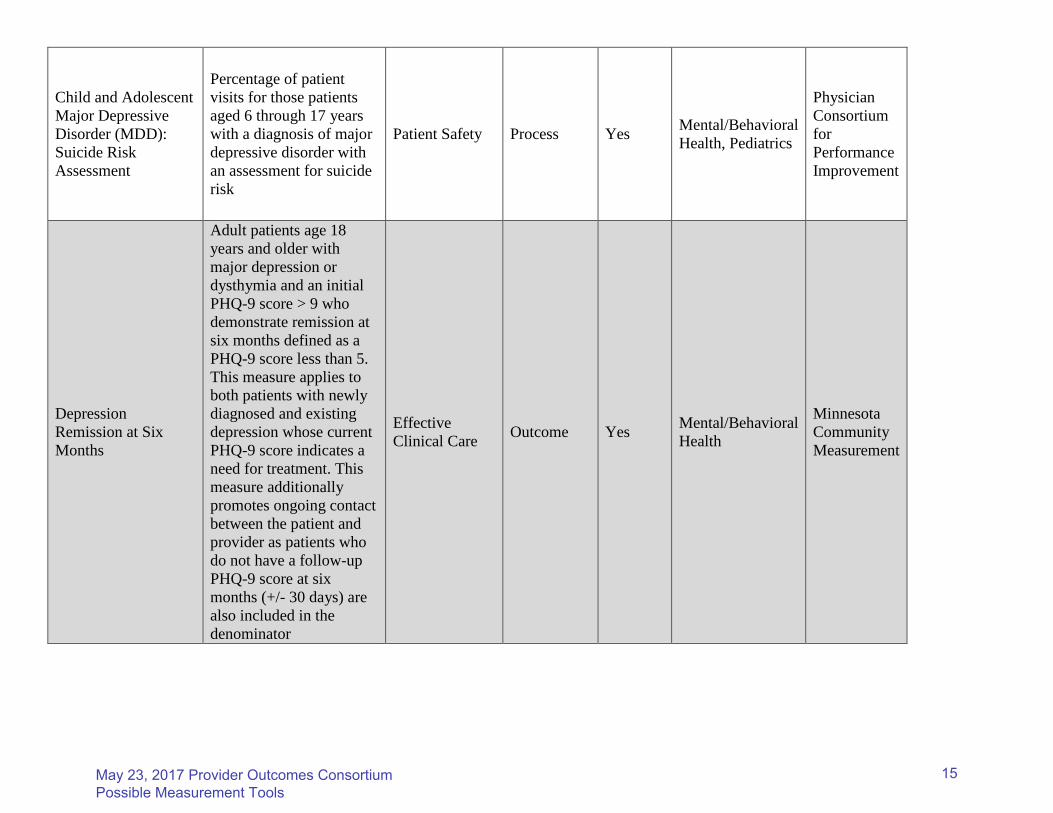
Child and Adolescent Major Depressive Disorder (MDD): Suicide Risk Assessment
Percentage of patient visits for those patients aged 6 through 17 years with a diagnosis of major depressive disorder with an assessment for suicide risk
Patient Safety Process Yes Mental/Behavioral Health, Pediatrics
Physician Consortium for Performance Improvement
Depression Remission at Six Months
Adult patients age 18 years and older with major depression or dysthymia and an initial PHQ-9 score > 9 who demonstrate remission at six months defined as a PHQ-9 score less than 5. This measure applies to both patients with newly diagnosed and existing depression whose current PHQ-9 score indicates a need for treatment. This measure additionally promotes ongoing contact between the patient and provider as patients who do not have a follow-up PHQ-9 score at six months (+/- 30 days) are also included in the denominator
Effective Clinical Care Outcome Yes Mental/Behavioral
Health
Minnesota Community Measurement
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
15

Depression Remission at Twelve Months
Patients age 18 and older with major depression or dysthymia and an initial Patient Health Questionnaire (PHQ-9) score greater than nine who demonstrate remission at twelve months (+/- 30 days after an index visit) defined as a PHQ-9 score less than five. This measure applies to both patients with newly diagnosed and existing depression whose current PHQ-9 score indicates a need for treatment.
Effective Clinical Care Outcome Yes
Mental/Behavioral Health, General Practice/Family Medicine
Minnesota Community Measurement
Depression Utilization of the PHQ-9 Tool
Patients age 18 and older with the diagnosis of major depression or dysthymia who have a Patient Health Questionnaire (PHQ-9) tool administered at least once during a 4-month period in which there was a qualifying visit
Effective Clinical Care Process No Mental/Behavioral
Health
Minnesota Community Measurement
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
16
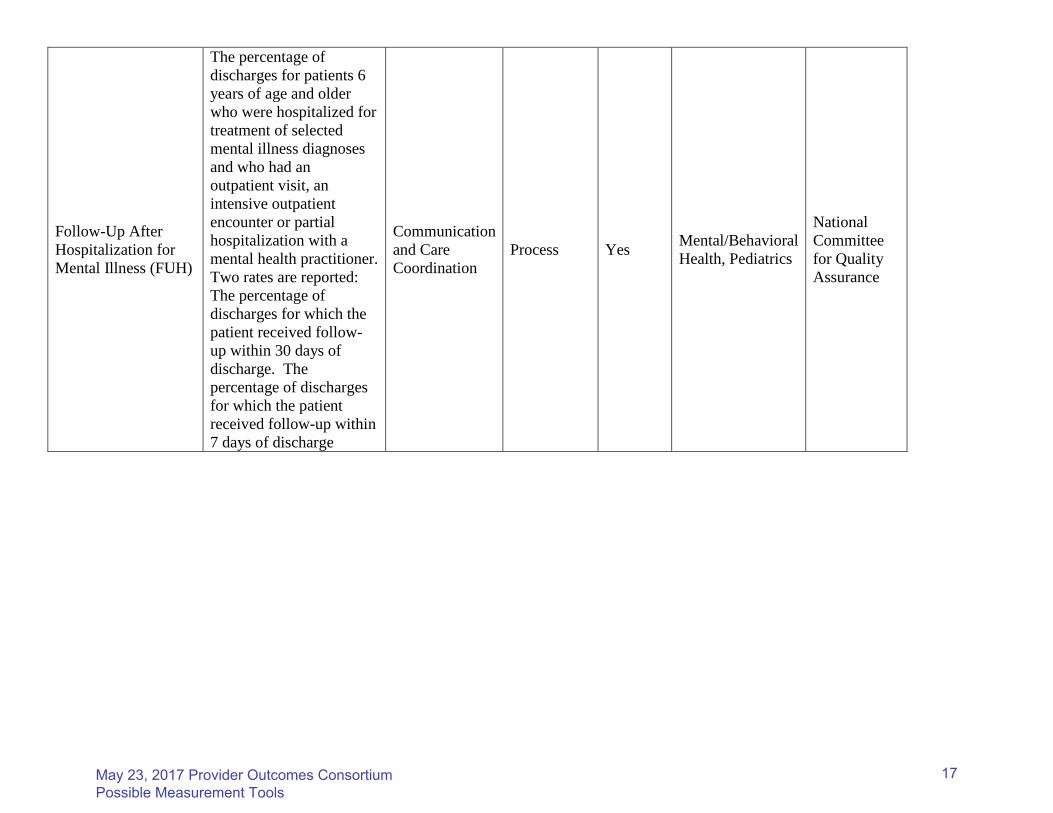
Follow-Up After Hospitalization for Mental Illness (FUH)
The percentage of discharges for patients 6 years of age and older who were hospitalized for treatment of selected mental illness diagnoses and who had an outpatient visit, an intensive outpatient encounter or partial hospitalization with a mental health practitioner. Two rates are reported: The percentage of discharges for which the patient received follow-up within 30 days of discharge. The percentage of discharges for which the patient received follow-up within 7 days of discharge
Communication and Care Coordination
Process Yes Mental/Behavioral Health, Pediatrics
National Committee for Quality Assurance
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
17

IDD Measure possibilities
Provider Suggestions: “quality of life” and “meaningful day” measures “Satisfaction with Services”
CQL: Council on Quality Leadership Survey
• Data is collected from consumers during 1:1 interviews with approved surveyors o Personal Outcome Measures (quality of life) (meaningful life) o Basic Assurances Measures (satisfaction with services)
Health Risk Screening Tool (HRST)
• For individuals with significant, ongoing health requirements and service coordination needs, routine screening for health risks will assist in focusing provision of health care. (quality of life)
• Identifies and tracks health risks in vulnerable populations, making it possible to design a plan tailored to meet the unique health and safety needs of each individual in the least restrictive setting. The instrument can objectively justify resources allocated both financially and in service intensity.
NC DHHS Specifications and Reporting Manual - October 2015
*30 day readmission rate for mental health
* 30 day readmission rate for substance use
* Annual wellness visit
* Follow up after hospitalization for mental illness within 7 days of discharge
* Follow up after hospitalization for substance use within 7 days of discharge
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
18

Hospital Measure possibilities
Provider Suggestions: “HBIPS” “Readmission rates” “Ambulatory Follow Up”
HEDIS Measures see packet
HBIPS Measures (Joint Commission Measures Effective 7/1/17)
HBIPS 1: Admission Screening for Violence Risk, Substance Use, Psychological Trauma History and Patient Strengths completed HBIPS 2: Hours of physical restraint use HBIPS 3: Hours of seclusion use HBIPS 5: Patients discharged on multiple antipsychotic medications with appropriate justification NC DHHS Specifications and Reporting Manual - October 2015
*30 day readmission rate for mental health
* 30 day readmission rate for substance use
* ED readmission rates
* Payment Denials
* Follow up after hospitalization for mental illness within 7 days of discharge
* Follow up after hospitalization (detox) for substance use within 7 days of discharge
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
19

Mental Health and Substance Use providers Measure possibilities
Provider feedback: “planned v/s unplanned discharges”, “symptom improvement”, “satisfaction with services” “engagement in services” “integrated care”
HEDIS measures: see packet (engagement and integrated care)
• DMA/H specs for LME-MCOs either match HEDIS or are similar • 7 day follow up after discharge for both MH & SU • IDD consumers receiving primary physician care at least once per year • Integrated care measures for diabetes screens, cardiac care, etc • NEW measure this year: 7 day follow up from Emergency Room visit
MIPS (formally PQRS) see packet (engagement and symptom improvement and integrated care)
ACORN: see packet (engagement in services, symptom improvement, satisfaction with services)
• Tool allows consumers to give real time feedback using tablets to respond to survey questions
o Rates symptom changes/improvement o Direct clinician feedback o Aggregate scores for outcomes and “clinician effectiveness”
NCTOPPS: (planned v/s unplanned discharges, symptom improvement, engagement, satisfaction with services)
• Data is gathered at various points in the treatment continuum for ages 6-11, 12-17 and adults. Required for many providers.
• Episode of Completion interviews gather feedback regarding symptom reduction, functioning levels and satisfaction with services.
o Final EOC questions are gathered in person only and measure outcomes of treatment
NC DHHS Specifications and Reporting Manual - October 2015
*30 day readmission rate for mental health
* 30 day readmission rate for substance use
* Follow up after hospitalization for mental illness within 7 days of discharge
* Follow up after hospitalization for substance use within 7 days of discharge
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
20

May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
21
1
What it is, how it works, and how it can significantly benefit
you and your clients
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
22

2
What it is: A little Research (slide 3) How it Works: Day to Day Practicalities (slide 17) Using ACORN: Web-Based Panel Discussions
(slide 36) Using ACORN Data to Inform Service Conclusion
(slide 43) Using ACORN in Supervision: Web-Based Panel
Discussion (slide 53) Using ACORN Data in Program Evaluation (slide
62)
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
23

3
A little research
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
24

4
Outcomes Informed Care is the… … routine use of patient self report outcome
and therapeutic alliance questionnaires to inform the treatment process,
combined with feedback to clinicians, to achieve improved outcomes and greater
value for treatment $$
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
25

5
“The combination of measuring progress (i.e. monitoring) and providing feedback consistently yields clinically significant change…. Rates of deterioration are cut in half, as is drop out. Include feedback about the client’s formal assessment of the relationship, and the client is less likely to deteriorate, more likely to stay longer, and twice as likely to achieve a clinically significant change.”
- Duncan, Miller, Wampold & Hubble (2009); From Introduction in Heart & Soul of Change; page 39
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
26
6
“This review underscores the value of monitoring treatment response, applying statistical algorithms for identifying problematic cases, providing timely feedback to therapists (and clients), and providing therapists with problem-solving strategies. It is becoming clear that such procedures are well substantiated, not just matters for debate or equivocation. When implemented, these procedures enhance client outcome and improve quality of care.”
- Michael Lambert (2009); From Yes It Is Time for Clinicians to Routinely Monitor Treatment Outcomes; in Heart & Soul of Change; Duncan, Miller, Wampold & Hubble (Eds); page 259
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
27

7
“The variance of outcomes due to the therapists (8%-9%) is larger than the variability due to treatments (0%-1%), the alliance (5%) and the superiority of empirically supported treatment to placebo (0%-4%).”- Wampold (2005); From The psychotherapist in Evidence-Based Practices in
Mental Health, Norcross, Beutler & Levant (Eds), p. 204
“… when effects to treatments are noted, who provides the treatment, the quality of the alliance, and the clinician and recipients expectations for success provide a far better explanation of the results than any presumed specific effects due to the medications.”- Sparks et al. (2009) Psychiatric drugs and common factors: An evaluation of risks
and benefits for clinical practice in Heart & Soul of Change; Duncan, Miller, Wampold & Hubble (Eds); page 221
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
28

8
Items written to 4th grade reading level Simple to understand frequency anchors
Never, Hardly Ever, Sometimes, Often, Very Often Common sentence structure aids rapid
completion How often in the past two weeks did you
…feel unhappy or sad? …have little or no energy?
Item domains include : Symptoms, relationships, functioning & productivity,
substance abuse, self harm, therapeutic alliance
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
29

9
Review your agency’s chosen questionnaire(s) now https://www.cci-acorn.org/login.asp
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
30

10
Three Components: Goals: Objectives of therapy that both client
and therapist endorse Tasks: Behaviors and processes within the
therapy session that constitute the actual work of therapy
Bonds: The positive interpersonal attachment between therapist and client of mutual trust, confidence, and acceptance
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
31

11
“Practitioners are encouraged to routinely monitor patients’ responses to the therapy relationship and ongoing treatment. Such monitoring leads to increased opportunities to repair alliance ruptures, improve the relationship, modify technical strategies, and avoid premature termination.”
- Norcross & Lambert (2006) in Evidence-Based Practices in Mental Health, Norcross, Beutler & Levant (Eds), p. 218
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
32
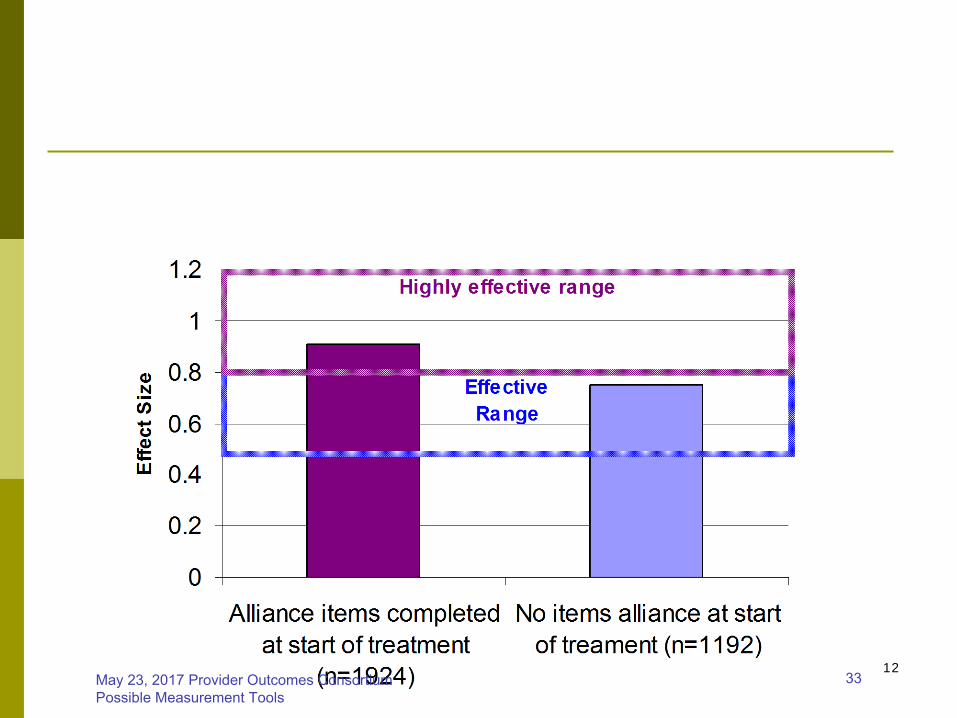
12May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
33
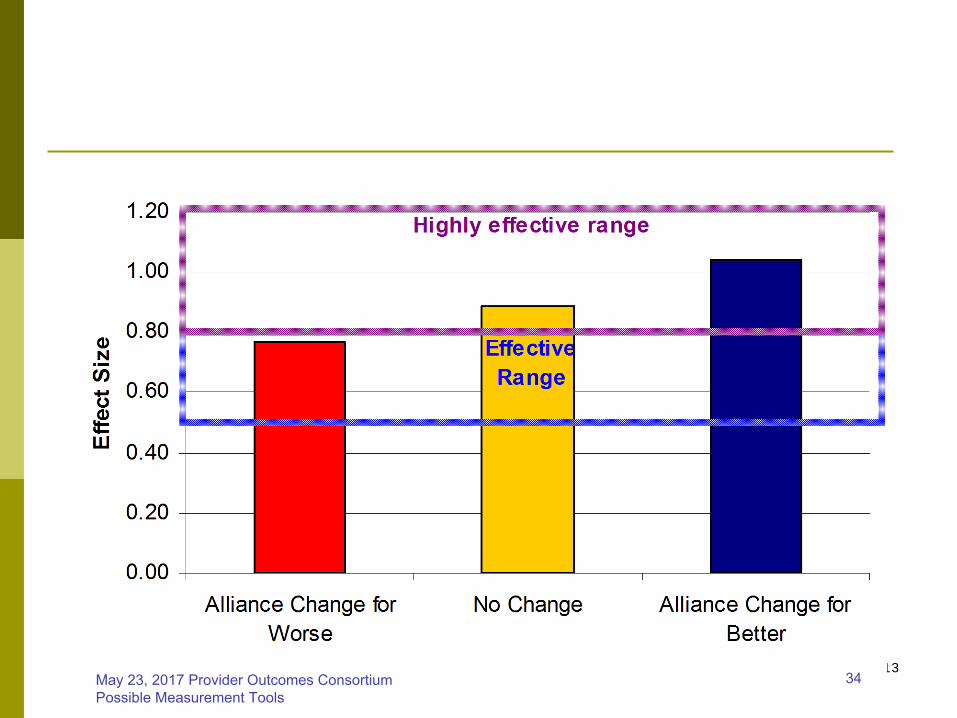
13May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
34

14
A consumer volunteer asked other consumers what they thought about completing the ACORN in a meta analysis
Feedback was overwhelmingly positive Clients liked that the form helped them focus
their thoughts Clients liked the increased focus of therapy Success felt more tangible Forms were short, easy to read, and quick to
complete
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
35

15
96%
13%
96%
55%
34%
83%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Found the questionnaires
helpful
Had concerns about
questionnaires
Were honest on
questionnaires
% o
f c
on
su
me
rs w
ho
ag
ree
Agree (74%)
Unsure/Disagree (26%)
I believe the clinician was interested in how I answered the questions…
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
36
16
Saves time at the beginning of session because ACORN allows me to see how things are going at a glance
Some clients are more honest on ACORN than with verbal responses. Alerts me to things I didn’t know where going on (thoughts of self-harm in particular)
Monitoring client outcomes helps me keep things on track, improves working relationship
ACORN helps my client set concrete treatment goals to work toward
Showing a client their graph can be a powerful reflection of progress, and can help identify times when things were going well and when things were not going as well.
ACORN can be helpful in having the discharge planning / step down conversation
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
37
17
Day to day practicalities
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
38

18
Your agency has a ‘gatekeeper’ – often a supervisor or other administrator – who will need to register you in the system.
The gatekeeper will create a username and password for you. You can change your password later.
Once you are registered, you will receive an email with the link to log-in to the web-based system and your username and password.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
39
19
Every Verity client needs to complete an ACORN form at least once per month (at least twice per month is best)
Actual frequency is dependent on how often you see the client. The general recommendation is: At every visit, but No more than once per week
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
40
20
Each ACORN is a check on how things are going. The more time that passes between ACORNs, the more opportunities are missed to monitor progress and address any ruptures in alliance. Example:
I have high blood pressure. My doctor tells me I can either change my diet and start exercising, or take a medicine. I choose the first option. The next time I come in for an appointment, my doctor takes my blood pressure to see if I’ve made any progress. If so, my doctor will probably keep things the same. If not, my doctor may change the intervention. But the doctor needs to take my blood pressure to know if we’re on the right track. The same is true of the ACORN.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
41

21
All users have access to a web-based ACORN Toolkit Forms can be downloaded and printed from
the website Electronic and fax submission formats available You have the option to pre-fill your Clinician ID
and Site ID numbers
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
42
22
Every client needs to be registered in ACORN. One page form, completed the first time the
client completes an ACORN Basic demographic information Check with your agency for their exact client registration
procedure Registration is important
Clients are matched with a national sample. The more demographic information available, the more accurate the match.
Payer must be identified to bill correctly (Verity vs. Non-Verity)
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
43
23
Review client registration form now https://www.cci-acorn.org/login.asp
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
44

24
The client should complete the ACORN before the appointment In the waiting room if services are clinic based At the start of session if services are community based
When ACORN is completed before the appointment, the clinician can tailor the session to what’s important to the client that day
Symptom items are a snapshot of the last 1-2 weeks
Alliance items are looking back at the last session If a client cannot read or has cognitive
difficulties, it is okay to read and/or explain the questions to them.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
45

25
The therapist should always be the first person to introduce the ACORN
Explain that the ACORN is an integral part of therapy. It will help them get the most out of your time together.
Completing the ACORN is an expectation of therapy, not an option.
Be clear about why you’re asking them to complete it, and address any concerns. A little investment in this education up front will
save a lot of time down the road!
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
46

26May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
47

27May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
48

28
The client hands their completed ACORN to the clinician at the start of the session.
Clinician reviews the client’s responses with the client, and uses this information as needed in session.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
49

29
Responses can inform treatment plan See Attachment #1 for sample treatment plan
Responses can inform progress note See Attachment #2 for sample progress note
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
50

30
Your agency will instruct you to submit data in one of two ways Fax: All forms are faxed to 1-800-961-1224.
Faxed forms are ‘read’ like a voting ballot or standardized test, where bubbled items are recorded as data.
Electronic: Client either completes ACORN on a computer, or client completes paper form and agency has a designated staff person do data entry, or clinicians enter data.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
51
31
At all future appointments, front desk staff will ask clients to complete the ACORN in the waiting room (in clinic-based settings).
Front desk staff need to be well-versed in the ACORN so they can explain it to clients if needed.
Emphasize how the form helps the clinician provide better service, and helps the client get more out of therapy.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
52

32
Video Vignette: front desk
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
53
33
Many clients appreciate seeing their progress in a graph (especially true of visual learners and youth)
Graph can act as an objective mirror on the client (reflection of client-reported distress)
Identify highs and lows, use to discuss what was working/not working for client at that time.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
54

34
Video Vignette #1: Adult Video Vignette #2: Child and Parent
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
55
35
After 3+ ACORN forms (not including the registration form) have been submitted, it is helpful to review progress to date. Log in to the web-based Toolkit (https://www.cci-
acorn.org/login.asp ) Review summary statistics, sort fields Review caseload summary table Review specific client graph with domains
Watch this 8-minute tutorial of how to use the Toolkit https://psychoutcomes.org/bin/view/DecisionSupportTo
olkit/ToolkitHelp
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
56

36
January 12th, 2012Panelists (youth providers): Suzanne McCann, Nathalie Matson, and Anne
Coussens
March 8th, 2012 Panelists (adult providers): Gabriel
Shannon, Lisa Stewart, Natalie Seibel
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
57

37
The ACORN is a helpful way to get clients to talk about things in a more concrete way.
Refusals are rare because of the approach when ACORN is first explained. Explain what it is, what it’s for, thank client for
completing the form every time, and look at their answers. Gives it value/worth.
If a client still refuses, don’t press them. If a client is too distracted, don’t push them to
complete ACORN. Do it next time. Look at client responses at the start of each
session. If a client is obviously in distress but reports everything is going well, will discuss.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
58

38
Acknowledge the form (alliance questions specifically) may be uncomfortable, but encourage clients to complete it each time. The forms provide an avenue for honesty. The alliance questions are very helpful in talking about the
relationship. Clients will talk about things in the ACORN even if they
can’t complete the form on their own. Some more concrete clients like to assign percentages to
the answer options (“Sometimes” = 50%, etc.) ACORN is incorporated into the treatment plan by asking
the client where they want to be. It provides a nice objective measure of mental health stability.
ACORN is incorporated into the progress note too, when commenting on the client’s progress to date.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
59

39
If you suspect or know that clients not telling the truth either on the ACORN or verbally in session, it’s easier to bring this discrepancy into session without direct confrontation by using the ACORN as a conduit.
Pay attention to blank items (e.g. suicidal ideation). The ACORN provides relevant clinical information, and it’s
important to look at Keep the questionnaires meaningful for long term clients,
especially those with chronic high levels of distress. Information from questions and a check on therapeutic alliance
are always important to monitor. Modify the way the questions are presented and used in
session with intensive case management and refugee populations.
Advice to other clinicians: explore the toolkit. The more you use it the easier it gets.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
60

40
With a client who is too distracted to complete the form all at once, clinician asked client to complete 2-3 questions at a time throughout the session. Physically moving to complete each set can be helpful.
With a client who felt rushed but liked homework, clinician sent ACORN home after session with instructions to bring it completed to the next appointment.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
61

41
Looking at the current and last form is helpful. What’s better? What’s worse?
Wait until the 3rd ACORN before bringing up the client’s graph to show them. Ask the client “Does this graph represent what you think is
going on?” This “outside observer” can help client recognize their own
success. ACORN is a self-awareness tool. Because it’s a self-report,
looking at answers and improvement over time is a reflection of self.
Use clinical messages to address specific areas of concern. With SMI clients with drug issues seen in community,
therapists don’t have a computer, so can’t pull up graph to show client.
ACORN results provide objective measure of improvement –incremental improvement is very good and sometimes surprising.May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
62

42
Seeing good client results helps clinician morale – it feels good to see clients improving.
Sometimes clients will go off their meds without permission. The results are reflected in their ACORN scores.
Unintended benefit: discovered a client needed glasses because they had trouble reading and completing the ACORN form.
One panelist was alerted by the client’s parole officer that they had had a positive urine analysis, but the client reported no drug or alcohol use on the ACORN. Clinician discussed this discrepancy with the client, built trust over time, and the client’s answers got more honest and accurate.
As a clinician, unhook yourself from the severity adjusted effect size in the toolkit, and recognize that clients have bad runs sometimes. Look at your caseload outcomes, but don’t hang your self-worth on the results.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
63
43
T. Bialozor, LCSWACORN User Group Meeting
4/23/2012
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
64
44
Termination / Service Conclusion is commonly a difficult process for clients, therapists, and agencies.
ACORN data has the potential to be used, in part, to identify: Clients’ readiness to conclude treatment Timelines related to service conclusion Relevant information for client / therapist
discussions related to closure
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
65

45
Therapist observation / clinical judgment related to client progress in treatment.
Patient self-report → improvement in symptoms.
Clients feel like they are “done” with therapy → call to cancel sessions or “no-show”.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
66

46
Evidence-based on length of treatment (i.e individual CBT has greatest benefit for client at 10-12 sessions).
Other clinical measures such as PHQ-9, Beck Depression Inventory, Compulsiveness Inventory, etc.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
67

47
For clients → planned termination results in more positive associations with therapy (making them more likely to return for new episode of care, if needed).
For therapists → planned termination results in a greater perception of success in work with clients.
For agencies → planned termination results in greater predictability for staffing levels and case assignments.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
68

48
ACORN provides clinicians with objective data which helps open the door to discussions on termination.
ACORN is a self-report for clients to have a “mirror on themselves” related to their progress in treatment.
Research shows that both children and visual learners benefit from seeing trends represented in ACORN data.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
69
49
Data on spikes related to client levels of distress can inform wellness/resiliency planning that is part of service conclusion required by the ISSR.
Clinicians can pull out specific successes from individual ACORN items to discuss in termination, even if global distress remains high.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
70

50
Early in treatment, clinicians ask clients “what does it look like to have completed treatment”? This information also informs ‘criteria for
service conclusion’ section in ISSP. Early in treatment, clinicians provide
clients with a preview that ACORN is one resource that can help inform when clients are ready to end treatment.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
71
51
Early in treatment, clinicians provide client with a brief explanation of the “clinical threshold” and how this represented in ACORN.
Encourage clinicians to look at the “clinical message” which gives therapist general ideas about what to expect for recovery trends based on all ACORN data.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
72
52
How could you see your agency using ACORN to facilitate effective service conclusion?
Are there other benefits that you can see related to using ACORN to inform treatment planning and discharge planning?
Are there circumstances where you would not want clinicians using ACORN in processes related to treatment planning and/or termination with clients?May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
73
53
Web-Based Panel TrainingApril 12, 2012
Panelists: Jessie Eagan, Christine Lau, and Pierre Morin
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
74

54
Internal staff experts hosted trainings with each program, used Sara Hallvik (Multnomah County) or Jeb Brown (Center for Clinical Informatics) for consultation or training when needed.
Agency developed internal policy directing staff use of ACORN. Used Multnomah County ACORN policy as a template.
SEE ATTACHMENT #3 Having a policy has been helpful because it is based on
the OARs, and puts the use of ACORN in context while making a clear agency expectation.
Supervisors can use policies as a guideline when talking with staff, and maintain a consistent message across the entire agency.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
75

55
New staff orientation includes ACORN. New staff are also linked with a mentor who
has been using ACORN effectively. Ongoing training is necessary, as memory
fades and new staff are hired Identified “super users” within each
program or site Use these internal champions to leverage the
importance of ACORN.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
76

56
Helps supervisors communicate in a concrete way about client outcomes. It introduces an objective element into supervision, especially
when clients are doing better. Supervisors regularly review data in the Toolkit
Overall data (effect size, distribution of patient change) is helpful, but better with filters (diagnosis, age, etc.)
Supervisor chooses some of the clients to review in supervision. Talk about what’s going well or what’s not working based on client’s current status.
Pull individual client graph, look for trends over time. Talk about discharge planning based on the client’s graph Therapists are not objective in evaluating their clients, so it’s
important to look at the client’s graph to monitor progress
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
77

57
Supervisors monitor how often clinicians log into the Toolkit, bring this up in team meetings and supervision
Talk about barriers to using data, like technical problems, in supervision
Time requirement of using ACORN in supervision Mention ACORN every time, and spend as much time as
feasible with outcomes depending how many other issues need to be covered that day.
Once a month, go to Toolkit with clinician and look at the caseload together. Pick “off track” clients to discuss.
Discuss usage in quarterly quality meetings. Build in a little to every session.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
78

58May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
79

59
Supervisors encourage clinicians to use ACORN with success stories.
Poor ACORN scores should never be used as punishment. Never use ACORN scores in evaluations or as discipline. Don’t use as element of performance evaluations. It can be a
great discussion opener if a clinician has low scores, but should never be used as punishment.
Use positive reinforcement – clinicians got into this career because they wanted to help clients, and the ACORN is a good way to show them evidence that they’re doing a good job.
Don’t rank clinicians, as this will just create fear and apprehension (instead, use ACE recognition).
Consider caseload size when looking at clinician results, because small caseload size can cause highly variable results.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
80
60
Over time, ACORN becomes routine and can lose meaning if you don’t remind clinicians in supervision to monitor their clients. Remind clinicians to look at the form in front of the
client every time the client completes it. Clients put information on the form that may not
otherwise be addressed in session. Educate clinicians about the variability in
outcomes scores with a small caseload. It’s normal to see large variations with a small number
of clients.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
81

61
Similar to concept of “Certified Organic” Process
Data analyzed by independent party (Center for Clinical Informatics)
Applies agreed upon criteria, including minimum effect size
Purpose Increase customer confidence of “value” Enable clinicians to demonstrate effectiveness to referral
sources such as employers, health plans and managed care companies
Empower clinicians to compete for business and negotiate contract based on demonstrated “value”
Great way to recognize clinicians, boost morale
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
82

62May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
83

63
Technical assistance, grant writing, program evaluation,
and other reports
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
84

64
If faxing, ensure the following steps always occur: ACORN forms are printed, not photocopied Bubbles are completely filled in Date, client ID, and clinician ID are written
clearly with pen inside the boxes Confirm that faxed batches are received
by checking the “fax report” under “HOME” in your toolkit.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
85

65
Email [email protected] Include in your email the date the data was sent, the
client ID, the clinician ID, and your organization ID, and what needs to be changed.
If you can include the record number (found in the “fax report” under “HOME” in your toolkit) that helps too.
The data center will reply to your email confirming the change.
You can also email your account representative directly. For most agencies, Jonny Maloney is the account representative ([email protected]).
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
86

66
Effect Size is a standardized method for reporting the magnitude of pre-post change.
The Severity Adjusted Effect Size provides an estimate of effect size after adjusting for differences in case mix and severity of symptoms.
An effect size of 1 means the patient improved one standard deviation on the outcome questionnaire.
Simple comparisons of effect sizes may be misleading due to differences in case mix. Use of the general linear model to calculate residualized
gain scores permits comparisons of outcomes after adjusting for differences in case mix.
However, while residual gain scores convey information about the difference between actual change compared to predicted change, they convey no information about the total magnitude of change.
The severity adjusted effect size conveys information about the magnitude of change while adjusting for differences in case mix.
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
87
67
The severity adjusted effect size is calculated only for patients with intake scores in the clinical range. The method involves calculating the average change score for all
cases in the clinical range from the entire population of patients as a reference sample, adding the residualized gain score for each patient to this constant, and then dividing this sum by the standard deviation of the reference sample.
Limiting the calculation of effect size to cases with intake scores in the clinical range has the effect of measuring pre-post change for only those patients with symptoms of sufficient severity that improvement with treatment is expected. This also has the benefit of enabling benchmarking against
published research studies, which likewise are conducted using patients with clinical levels of distress.
Effect sizes of 0.8 or larger are considered large, while effect sizes of 0.5 to 0.8 can be considered moderately large. Effect sizes of less than 0.3 are small and might well have occurred without any treatment at all. The ACORN Criteria for Effectiveness (ACE) uses 0.5 effect size as the threshold for "effective".
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
88

68
By clicking the radio button titled “View ALL Data (Summary and Episode Records)” you will see a row for every client. Hovering over the “Clinical Message” will give you more
detailed information on the client’s progress to date and a prediction of how they’ll do in the future.
These messages are based on a study of actual recovery trends on a national sample matched by specific client demographics.
Hovering over the “Admin” tab and clicking on “Compare Results” will allow agency administrators to compare their clients’ outcomes to the outcomes of a comparison group. Adjust any of the drop-down options to specify the populations
you want to compare. Log in to your toolkit and play around. It’s the best
way to learn. https://www.cci-acorn.org/login.asp
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
89

69
Clinicians and agencies that consistently collect ACORN data and who look at their data tend to have better client outcomes than those who collect data inconsistently and do not look at their data. This can be seen in the “ACE Statistics” under the “ACE” tab. If you change the minimum number of times a clinician has
logged in, you’ll see the SAES of individual clinicians grow. Clinical supervisors are important in ensuring clinicians
collect data regularly and look at their results. If the supervisor uses ACORN and talks about it frequently,
clinicians will use it and talk about it, improving client outcomes.
Regular feedback from customers has a strong positive effect on individual performance.
Raw data can be downloaded and analyzed by hovering over “Admin” and clicking on “View/Download Files”
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
90

70
Watch a 10 minute video about data in the Toolkit here https://psychoutcomes.org/pub/OutcomesMeasurement/WebHome/OutcomesMe
asurementWeb.swf
Take a minute to review the information about outcomes measurement included here https://psychoutcomes.org/bin/view/OutcomesMeasurement/WebHome
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
91
71
Jonny Maloney (Center for Clinical Informatics) [email protected] Questions about data, log-in or access trouble, or other
website/technical questions Sara Hallvik (Multnomah County MHASD)
[email protected], 503-988-5464 x26575 Clinic process questions, Verity requirements, all other
general questions Jeb Brown (Center for Clinical Informatics)
[email protected], 801-541-9720 Special data analysis requests, assistance
interpreting/using data
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
92
FaxComplete Forms to:
…feel unhappy or sad?......................…have little or no energy?.................
In the past two weeks, how oftendid you
This brief questionnaire asks about some of the most commonly reportedthoughts, feelings and behaviors among adults seeking behavioral healthtreatment. Please think about the past two weeks and indicate how often eachof the following occurred. This will help you and your therapist/doctor toplan your treatment and monitor your improvement.
…have a hard time getting along withfamily, friends or coworkers?..............
…have someone express concerns about youralcohol or drug use?.......................
S
Date completed
/ /
Session #
For more information on this and other questionnaires visitwww.psychoutcomes.org
Brief Adult Screening &Outcome Questionnaire
Version 10.0
Please print clearly
Hardlyever
Some-times
Often Veryoften
Never
…have a problem at work, school, or homebecause of alcohol or drug use?...........
…feel lonely?..............................
…feel tense or nervous?....................
…feel hopeless about the future?...........…have a hard time paying attention.........
…have problems with sleep (too much or toolittle)?...................................
…think about harming yourself?.............
…have more than five drinks of alcohol atone time?..................................
…feel unproductive at work or other dailyactivities?................................
I felt that the therapist liked andunderstood me.
I felt that we talked about thethings that were important to me.
I felt confident that the therapistand I worked well together.
Agree Somewhatagree
Notsure
Somewhatdisagree
Do notagree
If this is not your first session,please take a moment to give feedbackon your most recent session.
I felt that the session was helpful.
Clinician ID:
Please estimate the percent of your productivity at work, school orother important daily activities that is lost due to symptoms ofstress, anxiety or depression.
%
Org ID: Site ID:
Client ID:
Numerals only please
32365
32365
Fax completed forms to: 800 961-1224May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
93

…feel no interest in things?.
…feel unhappy or sad?
…have little or no energy?
In the past week how often did you
This brief questionnaire asks about some of the most commonly reportedthoughts, feelings and behaviors among adults involved in recovery fromsubstance abuse and and addictions. Please think about the week andindicate how often each of the following occurred. This will help you andyour therapist to plan your treatment and monitor your improvement.
…feel worthless?
…have problems with sleep (too much or too little)?
S
Adult Recovery QuestionnaireVersion 5
Hardlyever
Some-times
Often Veryoften
Never
…feel hopeless about the future?
…feel lonely?
…feel tense or nervous?
…feel the need to use alcohol or drugs?
…have a hard time controlling your temper?
…feel irritated?
…participate in activities that support a clean and sober life style?
…feel sad or angry that you can't use alcohol or drugs like other people?
…feel accepted by your recovery support group?
I felt that the therapist liked andunderstood me.
I felt that we talked about thethings that were important to me.
I felt confident that the therapistand I worked well together.
Agree Somewhatagree
Notsure
Somewhatdisagree
Do notagree
If this is not your first session,please take a moment to give feedbackon your most recent session.
I felt that the session was helpful.
Date Completed:
/ /
Session #:
Client ID:
Numerals Only Please
Org ID:
For more information on this and other questionnaires visitwww.psychoutcomes.org
Fax completed forms to: 800 961-1224
…have thoughts of ending your life?
Site ID: Clinician ID:
11483
May 23, 2017 Provider Outcomes Consortium Possible Measurement Tools
94


















