
May 2008
36
VOL.81 NO.4 May 2008 $5.00 S AN F RANCISCO M EDICINE JOURNAL OF THE SAN FRANCISCO MEDICAL SOCIETY Back to the Future of Medicine Medicine as Told from the Year 2050
-
Upload
san-francisco-medical-society -
Category
Documents
-
view
212 -
download
0
description
San Francisco Medicine, May 2008. Back to the Future of Medicine: Medicine as Told From the Year 2050.
Transcript of May 2008

VOL.81 NO.4 May 2008 $5.00
SAN FRANCISCO MEDICINEJ O U R N A L O F T H E S A N F R A N C I S C O M E D I C A L S O C I E T Y
Back to the Future of MedicineMedicine as Told from the Year 2050
MIEC reduced its already low rates in the last 15 of 18 years (1991-2008) with dividend credits on premiums for $1M/3M limits - averaging a 24.4% savings a year to its policyholders.
Which insurance carrier has distributed dividends* 15 of the last 18 years?
Has your professional liability carrier done that for you? If not, it may be time to ask why not!
Other benefits include:n We have a ZERO profit motiven MIEC is 100% owned and governed by its
policyholdersn We have provided California policyholders
continuous service for over 30 years n We have resolved over 24,000 malpractice
claims and lawsuits reported by our policyholders. Nearly 90% were closed without payment.
n We are rated A- {excellent} by AM Best’s
For more information or to apply: Go to www.miec.com or call 1-800-227-4527 and ask for our San Francisco Underwriter or email us at [email protected].* Future dividends cannot be guaranteed.
Cumulative California Dividends
0
22,000,000
44,000,000
66,000,000
88,000,000
110,000,000
1 9 9 1 — 2 0 0 8
Medical Insurance Exchange of California6250 Claremont Avenue, Oakland, California 94618 800-227-4527 www.miec.comSFmedSoc_ad_01.28.08
MIECOwned by the policyholders we protect.
SFmedSoc_ad_01.28.08.indd 1 2/6/08 9:44:35 AM

www.sfms.org may 2008San FranciSco Medicine�
conTenTS
San FranciSco Medicine May 2008 Volume 81, number 4Back to the Future of Medicine
FEATURE ARTICLES
10 A Look Back from the Future: Twenty-first Century Biomedical Practice and Research MikeDenney,MD,PhD
12 Missing the Mumps: A Medical Anthropologist Reports from the Year 2050 MegJordan,PhD,RN
14 Learning from Our Past: Lessons for Our Financial Future ThomasH.Lee,MD
16 Sounds Simple, Wasn’t Easy: Finding Good Health for Physicians LindaHawesClever,MD,MACP
18 Looking Back and Beyond: Holistic Health in the Year 2050 WilliamB.Stewart,MD
20 A Fragile Balance: Humans and Microbes in the Year 2050 KristenJ.Razzeca,MD
22 Darwin Revised! Reflecting on Darwin’s Theories in the Year 2050 LeonardShlain,MD
24 Psychiatric Moments: Experiences from the Years 2008 and 2050 LynnPonton,MD
26 Biomedical Imaging: Computerized Radiology in the Year 2050 GretchenA.W.Gooding,MD
27 Bad Bugs Bite Back: A Cautionary Tale SteveHeilig,MPH
28 The Future of AI: A Look at Stanford’s Artificial Intelligence Program AshleySkabarandAmandaDenz
MONTHLY COLUMNS
4 On Your Behalf
6 Executive Memo MaryLouLicwinko,JD,MHSA
7 President’s Message StevenFugaro,MD
9 Editorial MikeDenney,MD,PhD
�5 Hospital News
�8 In Memoriam NancyThomson,MD
Editorial and advertising offices
1003 a o’reilly
san francisco, Ca 94129
Phone: 415.561.0850 ext.261
fax: 415.561.0833
Email: [email protected]
web: www.sfms.org
subscriptions:
$45 per year; $5 per issue
advertising information is available on our
website, www.sfms.org, or can be sent upon
request.
Printing:
sundance Press
P.o. Box 26605
Tuscon, aZ 85726-6605

4San FranciSco Medicinemay 2008 www.sfms.org
on YoUr BeHaLF
TherearemanyexcitingSFMSsocialeventsintheworksfortherestoftheyear.Watchupcoming issuesofSan Francisco Medicine,SFMS Action News,andfax/e-mailMembershipUpdatesformoreinformationabouttheseevents.ContactTheresePorterin theMembershipDepartmentat (415)561-0850extension268ortporter@sfms.orgwithyourquestionsandcomments.
Member Benefit UpdateThecontactpersonforSFMSmembers
atWellsFargohaschanged.Ifyouarein-terestedinexploringthefinancialservicesavailable tomembers,pleasecontact JonPolahaat(650)[email protected].
Marsh affinity Update: Workers’ compensation
SanFranciscoMedicalSocietymem-bersrenewingtheirworkers’compensationinsurancethisyeardon’thaveveryfartogotoseehowtheirmembershipcanhelpsavethemmoney.Notonlyareratesgoingdownagainthisyear,SFMSmemberswillenjoyaspecialmemberdiscountnotprevi-ouslyavailable.
ThespecialmemberdiscountisonlyavailablethroughMarsh,SFMS’ssponsoredinsurance program administrator. TheprogramisunderwrittenbyEmployersCom-pensation Insurance Company (ECIC),rated “A-”by theA.M.BestCompany.SFMSmembersinsuredthroughMarshwillreceivethenewdiscountonrenewal.
If you are not insured through theSFMS-sponsoredworkers’ compensationprogram,callMarshforinformationonhowyoucanaccessyourdiscount.Anddepend-inguponwhereyouhaveyourgrouphealthinsurance,youmaybeentitledtoevenlargerdiscounts.FindouttodaybycallingMarshat(800)842-3761.
A sampling of activities and actions of interest to SFMS members
cMa requests PhysicianParticipation in a Study
TheCaliforniaMedicalAssociation(CMA)needsyourassistance fora studyinwhichitiscurrentlyengaged.AtitslastHouseofDelegates,CMAwasmandatedtodevelopareportoncurrentpeerreviewinCalifornia.The studywill cover: (1)adequacyof fairhearing rightsunder thelaw;(2)shampeerreviewinallitsmani-festations;(3)whetherandtowhatdegreea peer review hearing panel member’sfinancialrelationshipwiththehospitalhasaneffectontheabilityofthatmembertorenderanimpartialdecisioninthematter;(4)thephysician’sright(orlackthereof)tochoosearbitrationinlieuofpeerreview;(5)thebenefitsandpossiblestructureofanexternalpeerreviewprogram;and(6)anyother mechanisms available to improvepeerreviewintheseandanyotherrelevantpeer review issues,whichwould include,butnotbelimitedto,legislativeandlegaladvocacy.
CMAstaffiscurrentlyintheprocessofpreparingthisstudyandrequeststhatifyou,oranyoneyouknow,wouldliketoprovideinputorknowofindividualswhohavebeencontactedbyLumetra—theentitythatcon-tractedwiththeMedicalBoardtoreviewpeerreview—thatyoudosoinwritingandsubmitcommentstoAstridMeghrigianatameghrigian@cmanet.org.
Medical Board changing cMe requirements
TheMedicalBoardofCalifornia ischanging its continuingmedical educa-tion(CME) requirements forphysicians.Thoughitisunclearexactlywhenthenewrequirementswilltakeeffect,themedicalboardhasannouncedthatphysicianswillberequiredtocomplete50CMEhoursduringeverytwo-yearlicensureperiod.Currently,physicians are required to complete100everyfouryears.
ThemedicalboardhasalsoclarifiedthatCMEhoursaretobecalculatedbasedonthephysician’spersonallicense-renewal
notes from the Membership department
May 2008Volume 81, number 4
Editor Mike DenneyManaging Editor Amanda DenzCopy Editor Mary VanClayCover Artist Ashley Skabar and Amanda Denz
Editorial Board
Chairman Mike DenneyObituarist Nancy Thomson
SFMS oFFicErS
President Steven H. FugaroPresident-Elect Charles J. Wibbelsman Secretary Gary L. ChanTreasurer Michael RokeachEditor Mike DenneyImmediate Past President Stephen E. Follansbee
SFMS Executive Staff
Executive Director Mary Lou LicwinkoDirector of Public Health & Education Steve HeiligDirector of Administration Posi LyonDirector of Membership Therese PorterDirector of Communications Amanda Denz
CMA Trustee Robert J. MargolinAMA Representatives
H. Hugh Vincent, DelegateRobert J. Margolin, Alternate Delegate
Stephen Askin Toni Brayer Linda Hawes-CleverGordon Fung Erica Goode Gretchen Gooding
Shieva Khayam-BashiArthur LyonsTerri Pickering Ricki Pollycove Kathleen Unger Stephen Walsh
Board of directors
Term: Jan 2008-Dec 2010George A. FourasKeith LoringWilliam MillerJeffrey NewmanThomas J. PeitzDaniel M. RaybinMichael H. SiuTerm: Jan 2007-Dec 2009Brian T. Andrews Lucy S. CrainJane M. HightowerDonald C. Kitt
Jordan ShlainLily M. TanShannon Udovic-ConstantTerm: Jan 2006-Dec 2008Mei-Ling E. FongThomas H. LeeCarolyn D. MarRodman S. RogersJohn B. SikorskiPeter W. SullivanJohn I. Umekubo

www.sfms.org may 2008San FranciSco Medicine54San FranciSco Medicinemay 2008 www.sfms.org
date (the last dayof themonthof yourbirthday),notthecalendaryear.
PhysiciansareremindedthatCMA’sInstituteforMedicalQuality(IMQ)certi-fiesphysicians’CMEactivity forcreden-tialingpurposes to theMedicalBoardofCalifornia,aswellas tohospitals,healthplans,specialtysocieties,andothers.CMEcertificationis$29ayearformembers,$49fornonmembers.
Formoreinformation,contactPauletteRichardsonat(415)[email protected].
SFMS Seminar ScheduleAdvanceregistrationisrequiredforall
[email protected](415)561-0850exten-sion260formoreinformation.AllseminarstakeplaceattheSFMSoffices,locatedinthePresidioinSanFrancisco.
October3,2008Customer Service/Front Office Telephone TechniquesThishalf-daypracticemanagementseminarwillprovidevaluablestafftrainingtohandlephonecallsand schedulingprofessionallyandefficiently.9:00a.m.to12:00p.m.(8:40a.m.registra-tion/continentalbreakfast)$99forSFMS/CMAmembersandtheirstaff($89eachforadditionalattendeesfromthesameoffice);$149eachfornonmembers.
November4,2008“MBA” for Physicians and Office Managers9:00a.m.to5:00p.m.(8:40a.m.registra-tion/continentalbreakfast)Thisone-dayseminarisdesignedtoprovidecriticalbusinessskillsintheareasoffinance,operations, andpersonnelmanagement.$250forSFMS/CMAmembersandtheirstaff ($225each foradditionalattendeesfromsameoffice);$325fornonmembers.
other eventsJune12–15,2008Living on the Fault Line: Advances in Occupational Medicine
TheClaremontResortandSpa,41TunnelRd.,Berkeley,California8:00a.m.to6:00p.m.TheCaliforniaSocietyofIndustrialMedi-cineandSurgery (CSIMS), inconjunc-tionwith faculty fromUCSF, isofferingacontinuingeducation seminar thatwilladdress cutting-edge concepts regardingpractice,research,andpolicyinthefieldofoccupationalmedicine.Visitwww.csims.netformoreinformation.
June15–18,2008ENDO 08: The Endocrine Society’s 90th Annual MeetingThe Moscone Center, San FranciscoThismeetingoffersanunprecedentedop-portunitytolearnaboutthelatestadvancesin endocrine research and clinical carewhilenetworkingandcollaboratingwithmore than7,000colleagues fromaroundtheworld.Discoverandevaluatethelatestadvancesinendocrinology.Hearfromlead-ersinthefield.Choosefromamongmorethan200educationalprograms,includingplenary symposia, updates, debates, andmore.Formore information,visitwww.endo-society.org.
August10–15,2008Essentials of Primary Care: A Core Cur-riculum for Ambulatory PracticeResortatSquawCreek,NorthLakeTahoeThiscourseisdesignedtoprovideacompre-hensive“corecurriculum”inadultprimarycare.Itwillserveasanexcellentupdateandreviewforcurrentprimarycarephysiciansandotherprimarycareprofessionals,andasanopportunityforspecialiststoexpandtheirprimarycareknowledgeandskills.Particularemphasiswillbeplacedonprinciplesofpri-marycare,office-basedpreventivemedicine,practicalmanagementofthemostcommonproblemsseeninprimarycarepractice,andexpanded skills in clinical examinationandcommonofficeprocedures.Emphasiswillalsobeplacedonskillsindermatology,psychiatry,gynecologyandwomen’shealth,andneurology.Formoreinformation,visitwww.cme.ucsf.edu.
What Have We done for YoU Lately?The San Francisco Medical Society/Cali-fornia Medical Association form a valuable resource for members. What follows is a sample of the benefits of membership:
•TheSFMSPhysicianReferralSer-vice,whichhelpsyouexpandyourpracticebyenablingpotentialpatientstofindyou.This service is available topatientsbothon theSFMSwebsiteandbycalling theSFMSoffices.Allmembersareeligibletoparticipate.
•Listing in theSFMSMembershipDirectory, a trustedhealth resource thatenableseasyaccesstomemberinformationformembers,patients,andotherhealthcareprofessionals.
•Access tomedical-legal resourcesthroughCMAandhelpfromCMA’sna-tionally-recognized reimbursementadvo-catestohelpyougetpaidwhatisrightfullyyours.
•Accesstoacomprehensivearrayofinsurance services (personal andprofes-sional)atcompetitiverates.
With CMA, the San Francisco Medical Society has fought for issues crucial to the practice of medicine, including:
•Stoppingthegovernor’stwo-percenttaxonphysicians.
•Fightinginsurancecompanyabusesagainstdoctorsandpatients.
•Stoppingnonphysiciansfromprac-ticingmedicine.
•OpposingMedi-Calcuts.
SFMS is constantly advocating on behalf of San Francisco physicians and their pa-tients. Recent examples include:
• Cosponsoring, with the SutterHealthInstitute,apalliativecareworkshoponstate-of-the-artend-of-lifecare.
•Cosponsoringaninternationalcon-ference,attendedbypractitionersfromallovertheworld,examiningtheeffectsoftheenvironmentonfertility.
•WorkingwiththeCityandCountyof San Francisco to advocate improvedhealthcareaccessfortheCity’suninsured.
6San FranciSco Medicinemay 2008 www.sfms.org
execUTiVe MeMo
E arlierthisyearIparticipatedinastudymissiontoIndiawiththeAmericanSocietyofAssociationExecutives.Thepurposeofthetripwastoeducate
ourselvesaboutIndiaasanemergingworldmarketandtolearnhowassociationsmightplayapartinthefutureofIndia.OurtravelstookustoMumbai,Delhi,Jaipur,andAgra,wherewemetwithcorporateexecutives,governmentleaders,diplomats,healthworkers,newspapereditors,uni-versityprofessors,andevenaproducerfromBollywood.
ThesheervolumeofpeoplelivinginIndiahasatre-mendouseffectoneverythingthatgoeson,fromtraffictobusinesstohealthcaredelivery.Indiaiscurrentlyhometo1.1billionpeople,makingitsecondonlytoChinainpopulation,butgeographicallyitisaboutathirdthesizeofChina.Thereare29statesand6unionterritoriesinIndia,22languageswith122dialects,and9differentreligions.TheIndianswespokewithoftenreferredtothe“two”Indias:oneiscomprisedofaburgeoningmiddleandupperclass,andtheotherlivesinpovertyintheslumsofthecitiesandintheshantytownsofthecountryside.Onlyabout10percentofthepopulationlivesincities.ThereisgreatawarenessthatpovertyneedstobedealtwithinIndia.Therewasneveranattempttohideorignorethepoverty,andthesentimentweoftenheardwasthatitwasbettertoseeitthantopretenditdoesnotexist.
TheIndianhealthcaresectorisvaluedat$34billionandisoneofthefasting-growingsegmentsoftheIndianeconomy.In2004,nationalhealthcarespendingwasabout5.2percentoftheGDP,orabout$34.9billion;by2009itisexpectedtototal5.5percentoftheGDP,orabout$60.9billion.Otherestimatesindicatethatby2012,healthcare spendingcouldcomprise8percentof theGDPandemploy9millionpeople.Thesefiguresarebasedontheexpectationthatdemandforhealthcarewilloutstripsupplyoverthenextdecade;itisestimatedthatabout80,000newhospitalbedswillbeneededeveryyearforthenextthreetofouryearsinordertomeetthisdemand.
Therearemorethan5millionphysiciansinIndia,and162highlycompetitivemedicalschools.Themedicaldeliverysystemissplitbetweenthepublicandprivatesectors.Thereisnouniversalhealthcarecoverageinthecountry,andlessthan10percentofthepopulationhashealthinsurance,sohealthcareisdelivered
throughapatchworkofpublicandprivatehospitals,communityhealthcenters,primaryhealthcenters,primaryhealthposts,urbanhealthposts,andnursinghomes. It isbelievedthat theprivatesectorprovides60percentofthealltheoutpatientcareinIndiaandasmuchas40percentofallinpatientcare.Itisestimatedthat70percentofallhospitalsand40percentofallhospitalbedsinthecountryareintheprivatesector.Anumberofthehospitalsareaccreditedbyinternationalagenciesandprovidehealthcarethatisofasgoodaqualityasanywhereintheworld.Becauseofitshigh-qualityhealthcarefacilities,whicharecheaperthanthoseinmanyothercountries,Indiahasbeguntocapitalizeon“medi-caltourism”bytryingtoattractforeignerstoreceivehealthcareservicesthere.
Indiahasbeenabletodealsomewhatsuccessfullywithinfec-tiousdiseasesandtherehasbeenashiftinthehealthcaresystemfromemphasisondiseasessuchastyphoidandcholeratoheartdisease,arthritis,anddiabetes.Asinotherdevelopinganddevel-opedcountries,chronicdiseasesandobesityareontheriseandarebecomingthedominanthealthcareconcernsfortheIndianpopulation.
Wewere impressedbytheoptimismof thepeoplewemetaboutthefutureofIndia.Theglassalwaysseemedtobehalffullinsteadofhalfempty,despitepovertyandinfrastructureproblems.Wealsolearnedthatthereisan“Indiancontext”thatneedstobeunderstood.OneofthespeakerswhodiscussedopportunitiesinIndialeftuswithalistof“realities”aboutdoingbusinessinthatcountry.Thefinalrealitywasthat“[f]oreveryquestion,thereareatleastthreerightanswers.”
Travels in India
Mary Lou Licwinko, JD, MHSA

www.sfms.org may 2008 San FranciSco Medicine7
PreSidenT’S MeSSage
o rgantransplants,MRI scans,kidneyhemodialysis,defi-brillators,HIV—thesearebutafewofthetremendousmedicaladvances,inventions,andchallengesthathave
transformedthefieldofmedicineinthelastfortyyears.Infact,theonlyabsoluteandimmutableaspectofmedicineisthatchangewillalwaysprevail.Aswebeginthetwenty-firstcentury,therateofchangecontinuestoaccelerate,andwearelefttowonderwheremedicinewillbeinthecomingyears.
InthisissueofSan Francisco Medicine,variousauthorsexploreatrulyfascinatingpremise:Wherewillmedicinebein2050?Inthenextfortyyears,whatwillhavehappenedinmedicaleconomics,psychiatry,imaging,HIV,etc.,andhowwillphysiciansthemselveschange?Willtherebenewillnessestochallengeus?Willourbattlewithresistantbacteriaultimatelyoverwhelmus?Theanswerstoallofthesequestionsare,ofcourse,extremelyspeculative.Yetponderingwhereweasphysiciansmayendupin2050isacompellingandulti-matelyusefulexerciseifwehaveanyhopeofshapingourfuture.
Howthentoapproachtheunknowable,theunchartedterritoryofourfuture,thehiddenfaceofmedicinein2050?Onewayofatleastappreciatingtheenormityofthistaskistoreflectbackonwhathastranspiredinmedicalscienceinthepastfortyyears,aperiodthatencompassesmuchofourlifetimes.
Since1968,infectiousdiseasesandadvancesinantimicrobialtherapyhaveimpactedalmosteveryoneontheplanet.Vaccinesweredevelopedagainstmumps,rubella,hepatitisA,hepatitisB,andmeningococcus.Multiplenewantibioticsandantiviralmedicationshavebeendeveloped.Itisnowthoughtthatvirusescause15percentofallcancers.Yetthebiggestchangeinthisareabyfarisourdiscov-eryof“new”diseases—HIVbeingclearlythemostprominent,butalsoincludingsuchinfectionsashepatitisC,SARS,Ebolavirus,andH5N1avianinfluenza,allaffectingpopulationsaroundtheglobe.
Medicaltechnologyhasengineeredsomeofthegreatesttrans-formationsofthelastfortyyears.Onlyafewactivephysiciansre-membertryingtomakediagnosesbeforeCATscans,MRImachines,ultrasound,andechocardiographymadetheinteriorofthehumanbodyinfinitelymoreaccessible.Endoscopyandlaparoscopyhaveutterlychangedourabilitytoenterthehumanbodylessinvasivelyandmoresuccessfully.Cardiacpacemakersanddefibrillatorsarenowroutinelyimplantedtopreventsuddendeath.
Someofthemostimportantandtransformativechangeshaveoccurredastheresultsofadvancesinbiotechnology.Themolecularrevolutionhasfinallybornefruit—thediscoveryofthesecretsofDNAbyWatson,Crick,andFranklininthe1950sdirectlyresultedin themiraclesof recombinantDNAresearch fromthe1970sonward.PioneeringbiochemistsatbothStanfordandUCSFdidmuchoftheoriginalworkinthisfield.Theconsequencesofthisresearcharetheplethoraofbiologicagentsavailabletousnow,particularlydrugsthatareemployedinhematology,oncology,andrheumatology.
Anevenmoreprofoundramificationofthisworkhasbeenourabilitytoidentifydefectivegenesinmultipleillnessesandtobecomeawareoftheprominentroleofoncogenesinthedevelopmentofcancerinourpatients.RecentlytheHumanGenomeProjecthasmadeusawareofthesequencesofeveryhumanchromosome,rais-ingtherealpossibilityofbeingabletounderstandallpathologicprocessesatthegeneticandmolecularlevels.
Cardiac transplantation is alsonew in the last fortyyears,andotherorgantransplantation(liver,kidney,etc.)hasbecomecommonplace.Thesuccessoftheseremarkableproceduresisalsoatestamenttothediscoveriesinthefieldofimmunologyandtheabilitytosafelypreventorganrejectionwithdrugstargetedatspecificcomponentsoftheimmunesystem.
Finally,aswehavebecomeevermoreproficientinadvanc-ing the scienceandtechnologyofmedicine, therehasbeenanincreasingawarenessoftheneedtofocusonthewell-beingofourpatients.Physiciansandpatientshavethusbegunembracingthevariousaspectsofintegrativemedicine—meditation,acupuncture,therapeuticmassage,andmindfulness.Thesetechniquesallsharethegoalofenhancingourabilitytohealourpatientsfrombothwithinandwithout.
Whenonereflectsonwhatthepastfortyyearshavewroughtinourfield, it isbothexcitingand intimidatingtocontemplatewhatthenextfourdecadesmaybring.Thevariedarticlesinthisissueattempttogiveussomehintatthisextraordinaryfuture.Allthatweknowforsureisthatphysiciansin2050reflectingbackonuswillmostlikelyfindthatwhatwenowthinkofassophisticatedandcutting-edge ishopelesslyprimitiveby the standardsof themid-twenty-firstcentury!
The Medical Future ... As Seen from Our Past
Steven Fugaro, MD
CardiologyDermatologyFamily PracticeGastroenterologyGeneral SurgeryHospitalistInternal MedicineOB-GYNOrthopedic SurgeryOtolaryngologyPsychiatryRadiologySurgical OncologyUrgent CareUrology
Other opportunities available; contact usfor more information.
Sutter Health offers a wide variety of practice styles, geographies, and lifestyles.
With facilities in Northern California from the Oregon Border to the Central Valley, and from the Pacific Coast to the Sierra Foothills, we have plenty of career options to help you meet your goals.
We have opportunities in a variety of specialties, including:
Sutter HealthPhysician Recruitment
866-448-7070916-643-6677 fax
Northern CaliforniaPhysician Opportunities
www.sfms.org may 2008 San FranciSco Medicine9
ediToriaL
C assandracouldpredictthefuture.Intheancienttale,theIliadbyHomer,CassandraprophesiedthedeathofherbrotherHector,thedireconsequencesofallowingtheTro-
janhorsetoenterthewallsofthecity,andtheultimatedestructionofTroy.SheevenforetoldthedevastationoftheGreekarmyasitreturnedhomefromthebattle.However,Cassandraalsowascursed.Despiteherpowertoforeseeevents,noonewouldeverbelieveheruntilitwastoolatetostopthedisasterfromoccurring.
Contemplatingthis issueof San Francisco Medicinewith itsthemeofpredictingthefutureofmedicine,wemightpausetoreflectuponthegiftandthecurseofCassandra.Inthenineteenthcentury,withoutsolidscientificevidence,doctorslikeIgnazSemmelweis,JosephLister,MarionSims,andWilliamHalstedpredictedthatcleanlinessonthepartofcaregiverswouldresultinpreventionofinfection.LikeCassandra,theywereridiculedbythosewhodidnotbelieve them,yet theirpredictionscame true.Conversely,otherdoctors,whoapparentlyhadneitherthegiftnorthecurseofCassandra,madepredictionsofcurebyothertechniques,likeinternalmammaryarteryligationforheartdisease,theroutineuseofmilkandbakingsodatotreatpepticulcers,andhypophysectomyforbreastcancer,tonameafew.Thesedoctorswerebelievedbymanyestablishedphysicians,buttheirpredictionsforfuturesuccessdidnotcometrue.
Ineverydaymedicalpracticethisuneasyartofprophecy iscalledprognosis:fromtheGreekpro,before,plusgnosis,toknow—toknowbeforehand,ortheknowledgetopredictthefuture.IntheHippocratic Corpus,thetreatiseonPrognosisstates:“Anyonewhoistomakeacorrectforecastofapatient’srecoveryordeath,orofthelengthofhisillness,mustbethoroughlyacquaintedwiththesignsandformhisjudgmentbyestimatingtheirinfluenceononeanother,ashasbeendescribedinspeakingofurine,sputaandothersubjects...thebadbeingalwaysbadandthegood,good.”Inmodernterms,wemightsaythatwhenpredictingthefutureofsickpatientsphysiciansmustweighallthescientificevidence.
InhisbookDeath Foretold (1999),NicholasA.Christakis,professorofsociologyandmedicineattheUniversityofChicago,notesthatprognosismayinvolvemerelythebiologicalandtechni-calpartsofmedicalcare,butthataddingthemorespiritualelementofprophecybringstranscendentcreativity,meaning,andpurpose
to the task.Headmonishesdoctors, saying, “Theavoidanceofprognosisrepresentstheshirkingnotonlyofaclinicalbutalsoofamoralresponsibility,aresponsibilitythatpertainsbothtoindividualphysiciansandtotheprofessionasawhole.”AlthoughChristakisadmitsthat“Thetrueprognosiscanneverbeknowndefinitelyinaspecificpatient,”hedeemsa“deliberateassessmentofprognosisasabsolutelynecessary.”
Thus,practicingphysiciansarecaughtinadilemma.Theyarecalledupontoengageinprognosis,yettheydonothaveCassandra’sgiftofprophecy—theycannotpredictthefuture.Medicalexperi-enceisrepletewithpeoplewhodiedunexpectedlywhileundergoingtreatmentandotherswhofaroutlivedtheprognosisfortheirdemise,somewhoevenexperiencedaspontaneousremissionofincurabledisease.Indeed,fromascientificpointofviewitisclearthatalltheclinicalstatisticsintheworldcannotforetellwhatwillhappentoanyindividualpatient.Infact,thescientificapproachtomedicalprognosismightbeaptlycharacterizedascarefullypredictingthefutureofpatientsafterthoroughlyevaluatinginsufficientdata.
Aswefacethisdilemmainmedicalpractice,wemightnoticethatCassandrawaswonttopredictonlytragedy,failure,andbadoutcomes.InTroilus and Cressida,Shakespeare’splayaboutthefallofTroy,Cassandrashrieks,“Cry,Trojans,cry!Lendmeathousandeyes/AndIwillfillthemwithprophetictears.”Sheevenpredictedherowndeath.WemightalsoobservethatthenameofChristakis’bookisnot“lifeforetold”—itis“deathforetold.”Clearly,itseemsfareasiertopredictdestructionthancure.
Andsoitisthatrecognizingthatthetrueprognosiscanneverbeknowndefinitelyinaspecificpatientandthatsometimesprogno-sisisnecessary,wecandoourbesttoofferthoughtful,empathetic,andhelpfulassessments.Moreover,perhapswecanaddtoprognosisthemore spiritualelementofprophecy, remembering that thefamousancientGreekprophet,theOracleatDelphi,alwaysgavepredictionsthatcouldbeinterpretedinmorethanoneway.WemighttranscendtheperspectiveofHippocratesof“thebadbeingalwaysbad,andthegood,good,”soastoincludeinourworktheinherentmysteryofthefuture.Thus,prognosiscanbringmeaningandpurposetobothlifeanddeath.
Prognosis and Prophecy
Mike Denney, MD, PhD

10San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
f orty-two years ago, back in theyear2008,intheMayissueofSan Francisco Medicine,arevolutionary
newbiomedicalresearchandclinicalmeth-odologywasproposedbyDr.MikeDenney.Theproposalcalledforanadvancedmeth-odology that surpassed and transcendedordinaryempirical science in its efficacyforthemedicaltreatmentofhumanbeings,andthatincludedinitsresearchnotonlytheobjectivebutalso the subjective,notonlyquantitiesbutalsoqualities,notonlyfragmentationbutalsowholeness,andnotonlymatterbutalsospirit.
Thepresentationofthisnewsciencewas somewhat obtuse because it made,curiously,aproposalforthefuturethatwaswritteninthepasttense.ThishadresultedfromthefactthatforthatMay2008issueofSan Francisco Medicine,theEditorialBoardhaddecidedtoofferarticlesabout“BacktotheFutureofMedicine,”withtheuniqueslantofhavingtheauthorswriteasthoughtheywerelivingintheyear2050,thusre-cordinginthepasttensetheirpredictionsforthefutureofmedicine.Itwasasubtle,mind-bendingliteraryexercisethatgaveanentertainingfeelbutthat,understandably,mighthaveledsomereaderstothinkthatDenney’sproposalwasjustfrivolousspecula-tion,atime-warpplayonwords,oranidlefantasy.Buttoday,nowthatit istheyear2050,weknow,ofcourse,thattheproposalforanewkindof sciencewasprofoundlyserious,andthatitspublicationeventuallyresultedinchangesinthewaymedicalcareinthismid-twenty-firstcenturyisresearchedandpracticed.
Therewereothersbackin2008whopurported to include anew science andspiritualityinhealing.Researchof“alterna-tive”healingpracticessuchasacupuncture,
energyhealing,biofeedback,meditation,taichi, yoga,andprayer,amongothers,wasfinancedbygrantsfromtheNationalInsti-tutesofHealthandprivatefoundations.Inhealinginstitutionsacrossthecountry,thisresearchclaimedtobringaboutanintegra-tionofalternative,“evidence-based”heal-ingwithconventional,scientificallyprovenmedicalpractice.OrganizationsintheSanFranciscoBayArea,suchastheInstituteofNoeticSciences,theOsherCenterattheUniversityofCaliforniaatSanFrancisco,andtheInstituteforHealthandHealingatCaliforniaPacificMedicalCenter,engagedinresearchthatpurportedtofosteraunionofscienceandspiritualityinhealing.
As laudable as these efforts were,however,itisnowclearlyevidentthatthisresearchdidnot engage in true integra-tion.The studiesofferedneitheraunionof theobjectiveandsubjectiveaspectsofhealingnoramarriageofquantitativesci-encewithqualitativeandpoeticwaysofknowing. Instead, the researchers simplytriedtosubjectandsubordinateintuitive,
transpersonal, andmind-bodyhealing toempiricalstatisticaldata,seeminglyunawarethattheirmethodology,ordinaryempiricalscience, was inadequate to measure themetaphoric,poetic,andspiritualqualitiesofthephenomenatheychosetostudy.
Thetheoreticalfoundationforanewmethodology actually originated duringthe transition from latenineteenth-cen-turyPositivismtoearlytwentieth-centurydiscontinuityandparadoxintheartsandsciences.Tostartwith, intheyear1900,BertrandRussell,whohadcompletedhisPrincipia Mathematica,realizedthattheen-tirework—intendedtobethefinalwordontheperfectionofmathematics—containedabasicerror,arecursiveparadoxthathadbeenponderedbyphilosophersthroughouthistory.Afterexplainingtheparadoxwithcomplicatedmathematics,heexpresseditinthevernacular:Whatmanshavesthebarberinatowninwhichthebarbershavesthemenwhodonotshavethemselves?
Russell’srealizationofafundamentalparadox inmathematicswasprobably aresultof ideasexpressedduring theParisWorld’s Fair of 1900 at theSecond In-ternationalCongressofMathematicsandtheInternationalCongressofPhilosophy.FamousmathematiciansoftheoldPositivistschool,suchasDavidHilbert,proposedthattherewerenoproblemsinmathematicsthatcouldnotbereadilysolved,andthatmath-ematicswould soonattainabsolute rigorand formalitywithnothing leftundefin-able.However,othermathematiciansandphilosophersarguedthatitwasimpossibletodefinewhatismathematicallydefinable,citing such paradoxical concepts as thenatureofnumbersand themathematicalnatureofinfinity.
By1931,KurtGödel, a twenty-five-
A Look Back from the FutureTwenty-first Century Biomedical Research and Practice
Mike Denney, MD, PhD

10San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine11
SendYourMessageto2,500HealthCare
Professionals
TheSanFranciscoMedicalSocietyof-fersmultipleadvertisingopportunitiesranging from full-page,4-colordisplayads to classified ads with discountedratesformembers.PleasecontactGalenFosterformoreinformation,(415)[email protected].
year-olddoctoralgraduateinlogicalmath-ematics at theUniversityofVienna, setouttoexplainawaytheillogicalrecursiveparadox, but to his surprise he provedinstead that the recursiveparadoxwouldnevergoaway.InhisIncompleteness Theo-rem,mathematicsprovedthatmathematicswouldforeverbeincomplete,lockedintherecursiveparadox.
Earlier,themathematician,physicist,andphilosopherofscienceHenriPoincaré,whohadattendedthemeetingsinParisin1900,hadcalculatedtherecursiveparadoxintohisowntheoryofchaoticdetermin-istic systems,whichproposed thathighlycomplexsystemsdonotfollowthelogicofmathematics.AfterGödel’sIncompleteness Theorem,Poincaré’sideasconcerningchaosgainedcredence.AlanTuringinvestigatedtherecursiveparadoxanddiscoveredthatnotonlyweretheremathematicalproblemsthatcouldnotbesolved,therewereaninfi-nitenumberofsuchproblems.Turingwasthefatherofthemoderncomputer,anditwaswithacomputerthattheideaofchaosandcomplexitytheorywasfinallyrealized.
In1961attheMassuchusettsInstituteofTechnology, themeteorologistEdwardLorenzprogrammedacomputertopredicttheweather.Heenteredsomenumbersthatwere slightly lessaccurate than thecom-puterwascapableof,andwhenhereturneda fewhours later, thewhirringcomputerhadinventedanentirelyneworganizationofmathematics.Thustheideaofcomplex-ityandchaostheorybecamereality.Smallchangesinthewholenessofcomplexsys-temscanresultintranscendentphenomenathatspontaneously emerge andthatthereforecannotbemeasuredorpredictedbyordinaryscience.Thetheoreticalincompletenessinmathematicshadbecomemanifestintherealworld,andthenew,enchantedqualityofemergence transcendedlinearlogic.
Intheyear1900,physicistMaxPlanckwroteaformulathatexplainedwhyblackmetalglowsredwhenheated.Indoingso,heusedforthefirsttimetheconceptofthequantum,thesmallestunitofmatterorener-gypossible.Thousandsofexperimentsdoneinlinearacceleratorsnowconfirmwhatisacceptedtobethemostaccuratedescrip-tionofrealityeverknown.AsexplainedbyphysicistAmitGoswami:quantumparticles
canbeintwoplacesatthesametime,canbehereandthenappearovertherewithouttraversingtheinterveningspace,cannotbesaidtoexistinspace/timerealityuntiltheyareobserved,andcanaffectoneanotheratadistanceandfasterthanthespeedoflight.Theverynatureofmatterandenergywasthereafterunderstoodtogofarbeyondthatwhichcanbeexplainedbyordinaryscience.
Summarizingallof this incomplete-nessofmathematicsanddiscontinuityofquantumphysics,theastrophysicistJohnD.Barrow,inhisbookImpossibility: The Limits of Science and the Science of Limits(OxfordUniversityPress,1998), concluded that,paradoxically,scienceprovesthatsciencecannotproveeverything, and thus, “Nononpoetic description of reality can becomplete.”
Inhis2008proposalforanewpoeticmethodology inbiomedical researchandpractice,Denneyobserved that suchbio-logicaleventsasthebeginningoflifefrominorganiccarbonmolecules,theevolutionandmutationsofDNA,and thebirthofmindandconsciousnessfromthematterofthebrainareexamplesofspontaneousemer-genceoutofcomplexsystems.Moreover,henoticedthathumanbeingsarethemostcomplexentitiesintheknownuniverseandthattheyexhibitquantumparticleexchang-esatthetensofbillionsofneuronsynapsesinthebrainandwithinthezillionsofcellsofthebody—affectingneurology,physiol-ogy,psychology,andbodily-feltqualitiesofimagination,intuition,andmetaphor.Thus,allhealingofthehumanbody,takeninitswholenessinsteadoffragmentedparts,mustincludeaspectsofspontaneousemergenceofeventsincomplexsystemsandthedis-continuityandparadoxofquantumphysics.That’swhyheproposedanewbiomedicalresearchmethodologythatwouldincludenotonlytheobjectivebutalsothesubjec-tive,notonlyquantitiesbutalsoqualities,notonlyfragmentationbutalsowholeness,and not only matter but also spirit. Hepleadedforresearcherstobeginexploringpathwaystonewtranscendentandpoeticmethodologies.
Formanyyears,Denney’s ideaswererejectedorunnoticedexceptbyafewen-lightenedindividualswhodiscussedthem
inesotericmetaphysicalmeetings;inthinktanks;andinthecoursesinSpiritualityandScience, IntegralHealing, andFrontiersofDepthPsychology thatDenneytaughtatadvancedgraduate schools suchas theCaliforniaInstituteofIntegralStudiesandPacificaGraduateInstitute.
Finally, in the year 2045, his workwasbroughtforward,notbyscientistsbutbyphilanthropistscontributingmoneyforbiomedicalresearch,someofwhominsistedthattheirdollarsgotoinquiryintothenewmethodology thatDenneyhadproposedbackin2008.Now,intheyear2050,thereareatleastthreeresearchprojectsinvesti-gatinghis ideas:1)anopen-ended studyinwhich scientists andpoets engage indialoguesoastofuselogicwithmetaphor,seekingpathwaystowardspecific,newinte-gratedmethodologies;2)astudyinwhichradiologists interpretbiomedical imagingstudiesobjectivelyasusual, thendescribetheirowndeepsubjectiveandmetaphori-calexperiencesastheyimaginativelyandartisticallyengagetheimagesontheX-raysandscans;3)acardiacsurgeryexperimentinwhichoutcomesarenotonlymeasuredquantitativelybutalsotakeintoaccountthedeeplyqualitativepoetic, subjective,andspiritualexperiencesofboth thepatientsandthecaregivers.
Unfortunately, thisnewresearchdidnot occur during Denney’s lifetime.Hediedprematurelyattheageof110,onhisbirthdayintheyear2040,andthusneverlearnedof the fruitionofhiswork.Still,duringhistwilightyearsheoftenspokeofadeepgratificationthathisproposalforanewbiomedical sciencewaspublished inthatMay2008“BacktotheFuture”issueofSan Francisco Medicine.
12San FranciSco Medicinemay 2008 www.sfms.org12San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
w henthelastvestigesofchronicdiseasewerewipedoutthroughbiogenetic engineering four
years ago, in theyear2046, celebrationsoccurredaroundthegalaxy.Wehadnoideathenhowillnesswouldbemissed,howitssoul-shapingministrationswouldleavethehumanracegrimlywell.Lookingbackfiftyyearstotheyear2000,itishardformostpeople tobelieve that therewas a timewhenwecouldnothealbrokennervesorreprogramepigeneticmatrices.
Atonetimemedicalanthropologiststheorizedthattheonwardmarchofobesityanddiabeteswitnessedintheearlytwenty-firstcenturywasa sociopoliticaldisorder,butoncetheSino-IndianStemCellDis-pensaryUnitswere securely inplace inthedesignatedHighDiseaseBurdenareas,thewarnings from international teamsofsocialscientistswereconsideredarchaicandroundlydismissed.
Still, the eradication of inheriteddisorders and so-called “diseases of life-style”—alongwitheveryknowninfection,contagion, and pandemic that plaguedhumanityfrom1400to2046—hascreatedadiscomfitingwell-beingatbest.Itseemsthat illness itselfprovidedbiological scaf-foldingthatallowedthehumanspiritanddetermination to flourish.This isnot aphilosophicalview,butratherasignificantfindingfromqualitativeinterviewsandeth-nographicinquirywithmorethan100,000humaninformantsfromeverysociopoliticalquadrant.
eerie researchFrom2046to2050,thirty-eightmedi-
cal anthropologists participated in thefour-year EERIE Research (EncounterswithEradicationof IllnessEthnographic
Research)study.Thegroupthendissemi-natedthosefindingstotheFirstIntergalac-ticConsortiumofHealthandLongevityinJanuary.Reportingthisfirsthologramcastevent, themedical anthropologistswere
preparedforsomeresistancetothefindingsamongtheprofessionalheterodoxmedicalestablishment,but therewas little ifany.Mostoftherebuttalcamefromthetransna-tionalcorporatesponsorsoftheconsortiumandphilanthropicspecial-interestgroups,aswellashealthpolicydecisionmakersandgoverningeliteactors.
Ourattemptstoorganizethefindingsaccording to traditionalcategories (socialoriginsofdisease,biosocialattributes,class,race,ethnicity,gender)brokedown.ThetermclasswasrefutedbytheEconomicEq-uityCouncil,whicharguedthatsignificantclustersoffinancialandsocialinequitywerenolongeridentifiableandcouldcertainlyhavenoimpactonmedicaldisparity.Thisargument,ofcourse,heldnomeritforthoseremainingoutpostscientistswhotrackwaterprivatizationconsequencesintheRestrictedZones,wheresqualid,inhumaneconditions,sporadicpowersources,poortreatmentofwomenandchildren,anddeplorablelivingconditionsstillabound.
Racewasdeclaredanoutmodedcon-
cept, since the fourth symposium onRethinkingRaceintheAmericasin2014mergedthecriticaldialogueingenealogicalidentitywithdevelopments inbiologicalanthropology.
As for gender, any attempts toun-derstandgender’s implication inmedicaldiagnosisandtreatmentweredrownedoutinaheateddiscourseinwhichtwenty-twodistinct genders were identified, three-fourthsofwhichweredependentonelectivetransgenic-meiosisfabrication.
Whatfollowsisasummaryofthefind-ingspresentedtotheConsortium.
Study ParametersSample:More than140,000people
wereenrolledinthestudy,while100,000(approximately52,000womenand48,000men)completedthefour-yearprotocol.In-depthqualitativeinterviewswereconductedthroughuseofteletransfertechnologyatthebeginning,twomidpoints,andattheendofforty-eightmonths.DatafromobservationandinterviewswereorganizedintospecificcategoriesbyIlliac72softwarewithanalysisundertheguidanceoftheInstituteofHo-listicHealthStudies.
Questions determined a stratum oftrustworthy representation. More than90percentof informantshad successfullybeendeclareddisease-freethroughscientificmeasurements.Morethan88percenthadreceivedstemcellreplacement,whiletheremaining12percenthad surgicalproce-durestoexertcontroloverdiseaseformationprocesses.Only2percenthad functionaltransplants.
FindingsThe Gift of Stigma
Thestigmaofcopingwithachronic
“Looking back fifty years to the year 2000, it is hard for most people to believe that there was a time when we could not heal broken nerves or reprogram epigenetic matrices.”
Missing the MumpsA Medical Anthropologist Reports from the Year 2050
Meg Jordan, PhD, RN

12San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine1�12San FranciSco Medicinemay 2008 www.sfms.org
illness created lifelong adaptations thathadunexpected advantages. Informantswhowereoncedeaf (prior to transplantsurgery) did not deny that their formerconditionswereoftenpainfulordifficult;however,theidentitiesalsocreateddilem-masthatwereresolvedthroughnewsocialinteractions that normalized the harshrealities and brought forth an insider’slanguage,camaraderieoflivedexperiences,andcompassionateinteractionwiththosesharingidentityandunderstanding.Withthetransplantsuccess,theyweresuddenlynewactorsinahearingworld,strippedoftheirsocialnetworks.
Aformerdeafmansaid,“Idon’tknowhow to communicate anymore. I don’thavemyhumor,irony,sarcasm,jokes,signlanguage—there’snoreasontoconveywhatI’mupagainst.”Thefunctionsofself-helpgroups and nonprofit disease advocacygroupswere leftwithout a raisond’être,dismantlingextensivesocialnetworksthatprovideda senseofbelongingandcom-munity.
The Eclipsing of DifferenceSince genetic expression signatures
wereroutinelyannotatedforhopefulparentsapplyingforchildbirthlicenses,state-spon-soreddoctorshavebeenabletointegrategenomic information with clinical andpathologicalriskfactorassessment,therebyrefiningprognosisandtherapeuticoptions.Theend resultof thisearly interventionremovedthestratumof“identifiedother-ness”withinsociety:nomorebirthdefects,deformities, autism, impaired cognitiveabilities,ordevelopmentaldisabilitieswereevidentinsocialcirclesoronthestreetsofdeveloped societies.However,key infor-mantsrelatedabacklashtothiswhitewash-ingofthegenepool.Someillegalparentsanonymouslyreportedclandestinebirthingoperationsinruralareas,where“childrenofalessergod”weresafeguardedandeventu-allyrevered,someevenidolized,ashavingtheabilitytolisteninwardlyandthereforehaveaccesstospecializedknowledge.
Welcoming of Penultimate HealthTheevolutionofearlyattemptsatin-
tegrativemedicine(conventionalbiomedi-cinewithamenuofoptionsfromalternative
orcomplementaryhealthmodalities)inthe1990s into thenewPenultimateHealthCaremodelwasviewedasapositivechangebyinformants.Inshort,thevastnetworkofmedicalandalliedhealthprofessionals,pharmaceutical firms, hospitals, clinics,universityhealth systems,and related in-dustrieshadlittletodoaftertheeradicationofillness.Billionsofpeoplerequiredwork,purpose,andoccupation.
Prominent health researchers andmedicalpersonnelfromtheSanFranciscoBayAreacontributedtothenewsocialin-dicatorsforhealth,namely,CaliforniaInsti-tuteofIntegralStudies’IntegrativeHealth(IHL)program, the InstituteofHolisticHealthStudies(IHHS)fromSanFranciscoStateUniversity,andtheHealthMedicineInstituteandForum.IHLdevisedthewidelyacceptedsalutarymeasurementscaleofin-tegrativewell-being,whileIHHSoutlinedhow theevolutionof consciousness, theadaptationofbiomimicryprinciples fromnature,andthedeepintegrationofcreativelessonsonsustainabilitywerechiefcharac-teristicsfordevelopingandsustaininghealthandlongevity.ProgressingpeoplealongthisSalutaryScalehasbecomethemajoractiv-ityofthehealthcaresystemtoday.
Social IntelligenceWhen major medical research and
fundingorganizationselevatedsocialisola-tionasaleadingriskfactorforheartdiseaseandcertaincancersin2010,neurobiologiststracked the seatofbelongingwithin thehumanpsyche,genome,biochemistry,andneuralnetwork.The challengewas im-mediatelyposed:Ifsocietywasindeednow“bowlingalone,”what couldbedone toredirecthumanbehaviortohealthybond-ing?GenetictransplantsfromBonoboapesintohumanadolescentswereamong thefirstexperimentalproceduresperformedtoinstillmoresocialintelligenceandreverseisolationtrends.Theresultsreproducedtheearlier ancestral traitsofnesting, groom-ing,andeasyintimacyamongthehumansubjects.
OneinformantintheEERIEResearchstudywhowasarecipientoftheBonoboGene fragments reported, “I shriekwhenI’malonenowandcanonlybecomfortedby instantcopulation.”Again, theunin-
tendedconsequencesof this interventionareunthinkable toourgroupofmedicalanthropologists. As one Irish dramatisttoldtheresearchers,“Thisspellsdoomforself-reflection.Darknightsofthesoularerelegatedtohistory’swasteheap.Wheredoyouthinkcreativethinkingcomesfromifnotthetransformedfiresofloneliness?”
The Revival of Religious HealingAsignificantnumberofinformants(23
percent)believedtheeradicationofillnesswasthedirectresultofdivineintercession,andnot theconcertedeffortsofmillionsof international scientists and medicalresearchers.These informants identifiedthemselves asneoconservativemembersof religioushealing sects.Religiousheal-ingmethods(amoredogmaticversionoftraditional faithhealing)weredrivenbythe twodominant theocracies (Christianand Islamic) thatflourished in theearlytwenty-firstcentury.Thesereligious-culturalsocialforcesactivelyresistedinterventionfrommedicallypluralistic(biomedicalandnaturalistic) systems and practitioners.EERIEResearchethnographersconcludedthatdisaster-relatedtraumaandcertainty-oriented belief systems were foregroundissuesthatspawnedthisarchaicrevivalofreligioushealingfervor.Theseinformantsdidreceivetheirstemcells,transplants,andinoculations,however.Theysimplyattrib-utedtheirgoodhealthtodivinecauses.
Frozen Embryo GenerationInformantswhowerepartofthefrozen
embryogenerationscontinuetoprovidethegreatestchallengetomedicalethicists.Theyhavereframedthedebatesonidentity,kin-ship,lineage,andoriginsoflife.Informantsasked,“WhodoIbelongto?”“WhenwasIalive?”“WherewasIwhenIwasfrozen?”
Finally,thegreatestpointofconten-tionfromtheConsortiumwasovertheissueofMandatoryHealthoutlinedintheinter-national treaties.Anyemployer,whetherpublic, private, or government, whenfacedwith recalcitrant,uncooperative,oropenlydefiant resisters to theMandatoryHealthprogram,arefined,imprisoned,orpenallyrehabilitated.Lawsuitsbroughttoemployersbyoverweightpeople,smokers,
Continued on Page 17...

14San FranciSco Medicinemay 2008 www.sfms.org14San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
May 18, 2050To the Editors:
I n this year 2050, health care is incrisis.Costsarerisingfasterthanever,explosions inbiogenetic andmicro-
therapeutictechnologyareoverwhelmingtoday’sproviders, andworkdaysareonlygettinglonger.Meanwhile,theobliterationof food suppliesand theglobal spreadofpriondiseasesposerealthreatstothehumanrace.Itoccurstothishumblereaderthatweshouldhaltalldebateontheproposedincreaseinmembershipduesandbegintoconsider the realproblems that faceournobleprofession.
Thoughadistantmemoryalready, itwasonlyneartheturnofthecenturywhenwe facedchallenges that seemedequallyinsurmountable.Asrecentlyas2012,healthcarecoststotaledawhopping23percentofGDPandnotablebusinessessuchasFordandGMnearlywentbankruptbeforethefederalgovernmentintervened.Itmaybehardtobelieve,butbackthenmorethan80percentofphysiciansusedpaperforre-cordkeeping,50millionpatientsremaineduninsured,HIVwasconsideredaterminalillness, andnearly allvaccineswere stilldeliveredbyinjection.
Yes, we’ve made dramatic progresssincethenandwecandothesamegoingforward,butwemustrememberthatthesechangesdidn’thappenwithouthardwork,toughchangesinpolicy,andafirmdesiretodowhat’srightforthepatient.Lestweforget,ourlastfiftyyearsofaccomplishmentshavebeendrivenbykeymoments,move-ments,andmilestonesthatshouldserveasinspirationforournextfiftyyears.Giventoday’senvironmentofpoliticaldivideandturmoil,it’simportanttoremembersomeof
themorepivotaleventsinrecentmemoryandputourcurrentchallenges inproperperspective.
Financial crisis of 2010Perhapsthemostimportanteventin
thehistoryofU.S.medicinewasafinancialone.Therecessionandnearcollapseofthefederalbankingsystem,beginningin2008with themortgagemeltdownand furtherexacerbated by the near bankruptcy ofseveralfinancialinstitutionsandblue-chipcompanies, resulted ina radicalwake-upcall for policy makers in Washington.Despite thenation’swithdrawal fromtheMiddleEast,militaryconflictsworldwideandagrowingnumberofdomesticterror-istthreatsnecessitatedtheexpansionofamilitarybudget thatwas rivaledonlybythatofMedicare.
Facing the possible threat of fed-eralcollapse,thePresidentandlawmakerspassed theEmergencyMedicareReformBill, despitefierce anduniversalopposi-tion.Thoughthebillwaspositionedasatemporaryfive-yearcapontotalMedicareexpenditures, itwas renewed foranotherfiveyearsuntil itwasultimately replacedbythelandmarkHealthCareReformbillof2020.
Suddenly,thelifelineofthehealthcareeconomyhadbeencut.Andthecutswentdeep.Terminal illness:nonreimbursableaftersixmonths.Experimentalprocedures:uncovered.Lifestyle-relatedproceduresandhospitalizations:20percentcoinsuranceormandatedgapinsurance.Doomsdayprojec-tionsofplagueandpersonalbankruptcyabounded.Healthcarestocksplummetedwhileemigration toCanada skyrocketed.Themonumentalshifttoconsumer-basedfinancingofhealthcarehadbeenputinto
motion.
rise of innovative delivery Models (2010–2015)
Tothesurpriseofmostexperts,how-ever, thehealthcare systemdidnotcol-lapse.Mortalityratesremainedunchangedwhilehealthcareexpendituresleveledoff.Patientsstartedmakingfinancially-mindedhealthcaredecisionsandcommercialhealthplansseizedtheopportunitytocreateevenmoreconsumer-directedprograms.
Physician dissatisfaction, however,peakedduring thisperiod.Real incomescontinued to fall while cost-consciouspatients increasingly turned to theirphy-sicians forfinancial advice.Frustrated, agrowingnumberofprimarycarephysiciansandspecialistsstoppedacceptinginsurancealtogether.Overthenextseveralyears,theexodusfrominsurance-basedreimbursementcontinueddespitecallsforlegislation,andby2015,almost25percentofphysiciansdidnotacceptanyformofhealthinsurance,andalmost30percentofconsumersbelongedtoahigh-deductiblehealthplan.
Boutique and concierge practicesthrived in thisnewenvironment,whileradicalnewformsofdeliverymodelsbegantoappear.Web-basedmicroconsultation,packagedlifestyleservices,alacartehealthplans,andultra-boutiquemodelsallcameintoexistenceduring this time. Internet-enabled services and what were thencalled“electronichealthrecords”becamestandardamongphysicians,mostly fueledbytheneedtoinnovateanddifferentiateinan increasinglydigitalworld.Thoughtherewassomeconcernthattheseradicalnewdeliverymodels selectively targetedthemore affluent, it also appeared thatsomeofthesemodelsdemonstratedquality
Learning from Our PastLessons for Our Financial Future
Thomas H. Lee, MD

14San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine1514San FranciSco Medicinemay 2008 www.sfms.org
andcostoutcomes superior to traditionalinsurance-baseddeliverysystems.Withtheeconomy justcomingoutofaprolongedrecession,lawmakerswerereluctanttomakeanynewmovesandconsumersbythenhadgrownusedtoatwo-tiersystem.Congressdecided to focusonotherpriorities and,asaconsequence,almostone thirdofallnext-generationdeliverymodels(manyofwhichwestillseetoday)werebornduringthispivotalperiod.
Microtechnology for the Masses (2015–20�0)
Asnext-generationpracticeswerejustbecomingmainstream,newenvironmentalthreats began to pose large-scale publichealththreats,thelikesofwhichhadnotbeenseensincetheriseofMDR-TBandHIV.Global climate shift,microclimatevariation, population growth, and theemergenceofAsiaallcontributedtohorrificscenesofdrought,famine,andanewstrainofradicallytoxicretroviruses(laternamedRTRs).Within twoyears,millionsweredyingworldwide.
TheRTRsfirsthit theU.S. in2017and,by2020,deathtollswereestimatedinthehundredsof thousands.Despitewell-establishedprotocols, rapid immunizationprograms failed toeffectivelycontain thevirus,whichmutatedatalarminglyfastrates.First-linerespondersandprimarycareteamswereoverwhelmedasthenext-generationdeliverymodelsshowedtheirfirstsignsofweakness.Welldesigned tomanage thecareofindividualpatients,thepatchworkofpracticesfailedtorespondasacohesivepublichealthsystem.
Althoughbio-andmicrotechnologyfundinghadfallenduringthepriordecades,itwasnonethelesstwobreakthroughsfromtheprivateandpublicbiotechsectorsthatultimatelystemmedthetideagainstRTRs.ThefirstwastheabilityformicrofilamentsensorstodetectthefirstsignsofRTRinfec-tioninthebloodstream.Andthesecondwasmicroadaptivedenaturizationdeliveredvialong-actinginhaledtherapeuticvehicles.Bybeingabletoinstantaneouslydetectthefirstsignsofinfectionandthenoverwhelmtheviruswithhigh-exposureinhaledtherapeu-tics,theconceptofneedle-basedinjectionsandimmunizationsbecameinstantaneously
obsolete. IRMT (or Instant ResponseModulatedTherapy)waslateradaptedtotreat abroad rangeofvirus families andultimately led to theneareradicationofHIVjusttenyearslater.
In thewakeofRTRsand tobetteraddress the lingeringconcernsabout theresponsivenessofthepublichealthsystem,CongresspassedthelandmarkHealthCareReformbillof2020.Tothisdate,mostofthehealthcaresystemasweknowittodaytracesitsoriginsbacktothisimportantoverhaulofourfinanceanddeliverymechanisms.The legislationnotonly restructuredourpublichealthsystemwithfederallycoveredpreventiveanddisaster-responseprogramssupportedbyarichnetworkofpublichealthdatacentersandpracticeco-ops,italsoef-fectivelydismantledtheremainingelementsofMedicareandMedicaid.
ThesuccessofIRMTalsoresultedinahugeinfluxofcapitalsupportingbio-andmicrotechnologyinnovation.Overthenexttenyears,wesawthecommercializationofseveralblockbusterproducts,includingfirst-generationIDsensors,immunemodulators,andgenerepairkits.Anditwasduringthisperiodthatcompletelynewindustries,suchastransplantgenomicsandgenotherapeu-tics,cameintoexistence.
renaissance Period (20�0–2040)
Inthefaceofourcurrentchallenges,it’seasytotakeforgrantedwhatwehavetoday:thelowesthealthcarecostspercapitaanywhere;theneareradicationofinfectiousdiseaseasweknowit;andadynamic,flex-ibledeliverysystemabletoquicklyadapttochangesintheenvironment.
But itwas just twenty-fiveyearsagothatworldwidefamineandglobalextinctionwererealisticprobabilities.Andourpublichealthanddeliverysystemswerepushedtothefinancialandoperationalbrink.Howdidwearrivehere—fromthere?
I’msuremostofusrememberthethir-tiesasanidyllictimeinhealthcare.Anditwas.Economicgrowthfueledbyfallinghealthcarecostsresultedineconomicresur-genceintheU.S.andagreaterwillingnessby consumers to spendmoneyonnovelhealth care concepts.Home-based care,telemedicine,portablesensors,andmulti-
specialtyconsultationessentially replacedtheneedforofficevisitsaltogether.Alter-native and integrativepractices thrived.Mortality rates fell for a broad rangeofillnesses.Andobesityanddiabetesfinallytrendeddownward,giventheuniquefusionofsocialnetworkingandhomemonitoringtechnologies.Overall,consumers in2035spent30percent less in real terms thantheircounterpartsin2010,yetstillreceiveddramaticallyhigher levelsofpersonalizedandaccessiblecare.
Buttheprosperityofthethirtiesandfortieswasultimatelycreatedfromthechal-lengesoftheprevioustwodecades.Hadwenotfacedfinancialcrisesorenvironmentalthreats,wemightstillbeusingpaperchartsandneedles today.Outofhardshiparosenovel and revolutionary solutions thatbroughtaboutchangeandimprovementsinourhealthcaresystem.Anditisthosesortsofchallengesthatwefaceagaintoday.
new Threats (2040–present)Thehealthandenvironmentalchal-
lengeswefaceasasocietytodayareobvious.The storiespermeateournewsfeeds andmonitor-scopesalmosthourly.Overthelastdecade,wehavebecomecomplacentandoverconfidentinourabilitytofightillness,climatechange,andbioterrorism.Wehaveallowedpocketsofdiscontenttoproliferate,andtheynowemploythesameinnovativetechnologies,inaweaponizedform,againstus.Fraud,faultyproducts,andindifferencehaveerodedthegoodnamesofphysiciansandresearchers.Andthethreatofdispersiveprionsloomsinthenot-so-distantfuture.
Over the lastfiftyyears,criticalmo-mentsandcriseshavepushedoursocietytoimproveforthebetter.Aspolicymakers,entrepreneurs,andcaregivers,wehaveallbeeninvolvedinmakingthatchangehap-pen.Howwerise tomeet thechallengesofourdaywilldeterminewhatourworldbecomes.Letusnot forget that it isulti-matelyourresponsibilitytotakeownershipoftheseproblemstoday—tohelpshapeabetterfuture.
Respectfully,ThomasH.Lee,MD

16San FranciSco Medicinemay 2008 www.sfms.org16San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
H ereisthegoodnewsinthisyear2050—andthereisnobadnews.Duringthelastfiftyyears,physi-
cianshave learnedoneconceptand twostrategiesthat,alongwithotherapproaches,havesavedlives,savedhealth,andsavedrelationships.Thesehavesavedphysicians’ lives,health, and relationships,notonlypatients’.
Now,atthismid-twenty-firstcenturymark,let’srecollectsomehistorytoputthisamazingprogressintoperspective.Backintheyear2000,whenPalmPilotswerenewandconfusingbecausetheyhadnothingtodowithcoconutsoraircraft,afairnumberofphysicianswereinsorryshape.Some,es-peciallyinprimarycare,weretenseandbit-ter,scrabblingtopayexpenses,nevermindfundingthechildren’stuitionandpersonalretirementplans.Proceduralistsseemedtobesittingpretty,buttheyhadtoagitateforequipment,space,andstaff.ResearchersfeltasiftheywerecaughtbetweenEdgarAl-lenPoe’spitandpendulumwithincreasedcompetition for decreased support fromNIHandelsewhere.Facultyhadtosnatchmomentsfrompatients,students,andtheirown families todo the research thatwasrequired for tenure—if achieving tenureweredesirableanymore.Allphysicianswerepressedfortimeandfeltunderthegunevenastheytriedveryhardtobecompetentandresponsive.Theywantedtodomorethanscrapethroughtheday.Theysearchedforexcellenceandmeaning—andtheywantedsomejoyintheirlives,too.
Itisnowonderthatfeelingsleakedintobehavior.Accordingtodatapublishedintheyear2000,physicians’ratesofdivorcewereabout10to20percenthigher thanthat of the general population, perhapsbecause they worked more at medicine
thanatmarriage.Somewherebetween3to5percentofphysiciansweredisruptiveeachyear,backthenwhentherewerescalpelstothrowacrossanoperatingroomandchartstoslamonthedeskatnursingstations(somereadersmayrecallscalpelsandnursingsta-tions).Itishardtoimagine,butphysicianscommitted suicidequiteoften,1.4 timesmoreoftenthanthegeneralpopulationformenandmorethan2.3timesmoreoftenthan thegeneralpopulation forwomen.Thoseprematuredeaths stole258to369colleagues fromus eachyear—wellovertwomedicalschoolclasses’worthoftalentandhardwork.
Whathappened to change that sadpicture to the goodnewsof 2050?Oneconceptandtwostrategiesappearedonthesceneandtookhold. The concept
Therevolutionaryconceptstartedtofloataround inSanFrancisco in the late1900s:It isn’t selfish to take care of ourselves. It’s self-preservation—so we can do what we want to do.Thisconceptwasdifficult toaccept,becausephysiciansweretrainedtoworkuntil theydropped.Theywere sup-posedtomeeteveryrelentlessdemand.Buttherewasneverenoughtime.Tobesure,theireffortswereoftenrewardedwithagrinorathank-youortheirownsenseofaccom-plishment,buttheheatwason,alwayson.Themiserytiterwashighenoughthatmorethana fewwanted relief andwondered,“OK,sohowdoItakecareofmyself?”
Ina realbreakthrough, forexample,somephysiciansweremovedtofindtheirownphysician,althoughaboutone thirdstillhadno“physician-in-chief”forthem-selves.These latterphysiciansweremorelikelythanphysicians-with-a-physicianto
missmammograms,colonoscopies,andvac-cinations,thusputtingthemselvesinharm’sway.Adoctoracquiringadoctormaybeanacknowledgmentthatphysicians—justlikepatients—arehuman,notsuperhuman.OurDNAspiralsjustlikeeveryoneelse’s.Havingsomeonehelptakecareofusispartoftakingcareofourselves.
Thetwostrategiesthatgrewfromthe“NotSelfishbutSelf-Preservation”con-cept—hence thenow-familiar “NSBSP”acronym—werelearningmoreabouthowphysicians’ personalities are wired, andlearninghowto say“no”—and“yes”—attherighttime.
The First StrategyOfthemanycharmsandchallengesof
physicians’personalities,weandourpatientsappropriatelytreasureourthoroughnessandcontentiousness.Wesimplymustthinkandrethink, checkand recheck, inorder todoourworkwell.(Raiseyourhandifyoumakelists.Raiseyourhandagainifyouaddanitemtothelistsoyoucancheckitoffifyoudoitafterthelistwasmade.Ahhh,thesatisfaction!)
Perpetually seeking perfection hasdisadvantages, however. We may havetroublewithcloserelationshipsbecausewewanteveryoneelsetobeperfectaswell,andweimply,“Mywayorthehighway.”Thismessageoftentransmitstocolleagues,kids,and spousesorpartners,notallofwhomwelcomehavingourdirectivesthrustuponthem.Also,becausewewanttocontrolandfixeverythinginordertomeetourownhighstandards,lossofcontrolisalmostintoler-able tous.Therefore,havingaperfectlyreasonablerequestsenselesslyturneddownbyaninsurancecompany(thiswasbeforeuniversalcoveragewasenacted)was like
Sounds Simple, Wasn’t EasyFinding Good Health for Physicians
Linda Hawes Clever, MD, MACP

16San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine1716San FranciSco Medicinemay 2008 www.sfms.org
someonerubbingsandonasecond-degreesunburn.
Going for perfection and havingobsessive-compulsivetraitsaremorethandouble trouble.They lead toexceptionalvulnerabilitytocriticism.Wemayflareifashadowofdoubtiscastoveroneofourdiagnosesordecisions.Furthermore,ourownintuitionsuggeststhatperfectionisnotpossibleandthatwearetryingtolivealie,leadingtochronicdiscomfort.Alloftheseelementscanresultinhighself-doubtandevenlowself-esteem.
Once physicians learned this, theycould,asamentoronceadvisedme,temperthewindto the shorn lamb.Theybegantreating eachotherwithmore empathybecausetheysawthatphysiciansthemselvesweresometimestheshornlambs,underslept,overwhelmed, and insecure. They sawothers’mistakesaspotentially theirownand sought touse themasopportunitiesfor learningandcompassion, rather thanviewing themwithdisgustor antipathy.Asphysicians learnedwhy theywere sodefensive,theywereabletostoprearingupandstrikingout.Theywereabletolistenandlearnfromresearchers,othercolleagues,nurses,andpatients,andtheyfoundcuresforthoselong-gonemaladies,irritablebowelsyndromeandthecommon(nowuncom-mon)cold.They listened toand learnedfrom their spouses, children, and friendsandfoundnewsourcesofmeaningandjoy.Theycutthemselvessomeslackandbegantoenjoytheirwhole,healthylives.
The Second Strategy
Discoveringthesecondofthetwostrat-egiesputthedoctorsoverthetopandintorobusthealthandfulfillment.Theyrecog-nizedthat,alongwiththeirotheradmirableyet sometimes sabotagingattributes, theylikedtopleaseothers.Mostofusstilldo,andthatisgood.Theproblemisthatwantingtopleasemayleadustosay“yes”fartoomuchand“no”notnearlyenough.
Evennow,in2050,itcanbehardtosay“no”whenweareaskedtobeonacom-mittee,takemoreholidaysoncall,chairthefunddrive,serveonaboard,clearourdeskorgarage,dodoubleshifts,volunteeragainandagain.Sometimesphysicianswere,andare, afraid—afraidof beingperceived as
weak,lagging,incapable,or,touseasportsterm,nota“teamplayer.”Besides,physi-cianslikedtothinkofthemselvesaslimitlessandalwayshavingtheonly/bestideas.Quitequickly,astheNSBSP—somecalledit“re-newing”—movementtookhold,physicianssawthat saying“no”gavethemstrength,energy, time to learnnewmedical skills,time toflourishwith family and friends,timeto takecareof themselves,exercise,andvote!Whenexhausted incumbentssaid“no”moreoften,newblood,vigor,andideascouldbeinfusedintothejobstheyhadvacated,allowingworthyprojectstoreachnewheights.
Saying “no” tooka script and somepractice, as youcan imagine. If youfindyourselfattractedtothesirencallofinap-propriate“yes”answers,chooseoneortwofavorite“no”responsesfromthefollowinglistandtattoothemintoyourfrontoparietallobe.Youcouldgiveyourselfarefresherinfrontofamirror.Somepeoplehavetousetheirfingersandactuallymovetheirlipsintotheshapeofthewords:
•“No”or“No,thankyou.”•“I’llhavetotakesomethingelseoff
myplate.”•“Notnowbutmaybelater.”•“Whoelsecanpitchin?”•“I’d love todo it, but youdeserve
andneedabetterjobthanIcandorightnow.”
•“Thisismyyearforsaying‘no.’”•“Youwantmetodowhat?”Ortrytheanatomicalapproach:Bite
yourtongueandsitonyourhands.Overall,this isanimportantstoryof
concepts,strategies,learning,andpersever-ance,allenroutetoassuringgreaterhealthfor physicians who, after all, need anddeserveit.Thestoryhasnoend,actually.Whatwillhappeninthesecondhalfofthetwenty-firstcentury?Itiseasytoslipbackintobrain-deadeningschedules,soul-searingmisunderstandings,desperation,ortorpor.Theringingcheerthathasresoundedforthefirsthalf of the twenty-first centuryneeds refreshing: Taking care of yourself is not selfish. It is self-preservation—so you can do what you want to do.
Linda Hawes Clever, MD MACP, is the founder of RENEW, a program that helps busy health care professionals regain and maintain
their vitality in the face of competing professional and personal demands. She also serves as Chief of Occupational Health at CPMC.
ReferencesMillerNM,McGowanRK.Thepain-
ful truth:Physicians arenot invincible.South Med J. 2000;93:966-973.
LeapeLL,FromsonJA.Problemdoc-tors:Isthereasystem-levelsolution?Ann Intern Med.2006;144:107-115.
SchernhammerES,ColditzGA.Sui-cideratesamongphysicians:Aquantitativeandgenderassessment(meta-analysis).Am J Psychiatry.2004;161:2295-2302.
AmericanMedicalAssociation:Wom-enPhysicians’ConferenceTable1.Ac-cessedat
http://mw.ama-assn.org/ama/pub/category/12912.htmlon23March2008.
GrossCP,MeadLA,FordDE.Arch Intern Med.2000;160:3209-3214.
andthosewitheradicableillnesswhohavenotreceivedMandatoryHealthbenefitsarefast-trackedinthecourts.
Questionsof self-responsiblebehav-ior versus legal-cultural impositions arediscussed in thecomplete listoffindingsfromtheEERIEResearchStudy,availableatWIFI/hhhdialin:Telestar200042.Theresearcherswelcomeyourcommentsandhaveestablishedaforum,inthehopethattheEERIEResearchdimensionswill bedebatedforyearstocome.
Meg Jordan, PhD, RN, is a medical anthropologist, health journalist, president of Global Health Media, and author and presenter on faculty at San Francisco State University and California Institute of Integral Studies.
ReferencesBeckerC.Copingwithstigma:Lifelong
adaptationofdeafpeople. InUnderstand-ing and Applying Medical Anthropology (P.Brown, ed.), 1998, London: Mayfield;311-315.
InhornM.Copingwithstigma:Life-longadaptationofdeafpeople.InUnder-standing and Applying Medical Anthropology(P.Brown,ed.),1998,London:Mayfield;315-321.
Missing the MumpsContinued from Page 12...

18San FranciSco Medicinemay 2008 www.sfms.org18San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
w hatacompellinginvitation,towritefromtheyear2050!Yes,in my reverie I contemplate
thehospital inwhich Iwork—the sun-light, streaming into theentryatriumofthemedicalcenter,warmsthedecorativestonefloor and the spacious,plant-filledspace.Thesoundofthebubblingfountainiscomplementedbythemusicofaharp.AsIinhalethesoothingfragranceoflavender...suddenlymyreverieisinterrupted,andIamstruckwiththerealizationthatIam107yearsold!Wasmygeneticandgeographicluck,andtheeffectivenessofmymedicalassistanceandself-care,suchthatIcannowconceiveofsuchlongevity?
Toenvisionwhatisnowcalledintegra-tivemedicineandholistichealthisafreshreminder thatwe live livesofpossibilityandprobability.Nomatterhowwellweresearch,plan,andprepare,theelementsofunpredictability,uncertainty,andimperma-nence,inthefinalanalysis,prevail.
Looking back from the year 2050remindsmeoftherealitythatithasbeenfortyyearssincemygraduationfrommedicalschool.Inthe1960s,heartsurgeonswerereconfiguringthecardiacanatomy.Organtransplantationwasanemerging frontierfor pioneers and visionaries. Imagingequipmentwasonthedrawingboardsthatwouldrevolutionizediagnosticcapabilities.Informationonnewdrugswas fatteningtheprinteditionoftheannualPhysicians’ Desk Reference,andgovernment-sponsoredhealthinsurancefortheelderly,Medicare,wasvotedintolaw.
In the1990s, theboundariesof thepracticeofmedicinecontinuedtoevolveand expand. The human genome wasmappedand theelucidationof complexcellular and subcellularphysiologicpro-
cesseswereoccurringatthesametimethatpracticessuchastraditionalChinesemedi-cine,Ayurveda (indigenousmedicineofIndia),homeopathy,naturopathy,yoga,andmeditationwerebecomingbetterknown,
understood,andmorewidelyapplied.Therewasanindividualandcollectivemovementtowardrelationship,collaboration,integra-tion, wholeness, and prevention in thepracticeofmedicine.
Thiswasallhappeningevenasbio-technical, pharmacologic, and geneticbreakthroughswerereportedalmostdaily.Backin2008,Cohenetal(NEJM2008)noted that “preventablecausesofdeath,suchastobaccosmoking,poordiet,physi-calinactivity,andmisuseofalcohol,havebeenestimatedtoberesponsiblefor900,000deathsannually—nearly40percentoftotalyearlymortalityintheUnitedStates.”Inlargepart, these “preventable” causesofdeathweretreatablewiththerapeuticlife-stylechanges.Furthermore, theestimatesofthenumberofpeoplewhosesymptomsand signs represented “psychosomatic,”“functional,” or “stress-mediated” illnesscontinuedtobesignificant.Withchronicillness in all age groupson the increaseandanagingpopulation, thechallengestohealth careproviderswere clear and
growing.Itwasunderstandablethatpeoplewereseekingguidanceandsolutionsfromsourcesrelatedtothepracticeofintegrativemedicine,anditseemedlikelytheywouldcontinuetodosointhefuture.
Eisenberg (JAMA 1998)haddocu-mentedthelargenumberofpeopledrawntocomplementaryandalternativemedicalpractices(CAM).AccordingtoJohnAstin,PhD,oftheCPMCResearchInstitute,animportantreasonthatpeoplesoughtalter-nativetherapieswasbecausetherepatientsfound“…anacknowledgmentoftheim-portanceoftreatingillnesswithinalargercontextofspiritualityandlifemeaning.Theuseof alternativecare graduallybecameapartofabroadervalueorientationandsetofculturalbeliefs,onethatembracedaholistic,spiritualorientationtolife”(JAMA1998).Bydefinition,medicineslowlycametomeantheartandscienceofhealingratherthanjustascientificmethodologyforcure.Medicinespecialtiesrangedfromaviationmedicine to environmental medicine;fromforensicandgeriatrictointernalandphysical;fromsocializedtotropicalandvet-erinary;and fromalternative, indigenous,unorthodox, traditional, and nontradi-tionaltocomplementary,comprehensive,mind-body,multidimensional,preventive,integrative, and simply “good”medicine.Theprofessionhadmanynuances,nooks,andcrannies, as it sought to reduceandrelievepainandsuffering,curedisease,andhealillness.
Priortothisfirsthalfofthetwenty-firstcentury,welivedwithmanymetaphorstohelpdefineandcharacterizeourmission.Oneofthesewasthe“battlefield”metaphor.Herediseasewastheenemy;doctors,nurses,andhealthcareprofessionalsweresoldiers;andourmindsandbodieswerethebattle-
“To envision what is now called integrative medicine and holistic health is a fresh reminder that we live lives of possibility and probability.”
Looking Back and BeyondHolistic Health in the Year 2050
William B. Stewart, MD

18San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine1918San FranciSco Medicinemay 2008 www.sfms.org
grounds.Thetherapeuticarmamentariumincludedthemedicationsandtechnologiesemployedaswewagedwaragainstcancer,foughtheartdisease,wipedout resistantinfections,andadvancedbattle linesandfrontiers.Inanothermetaphor,the“market-place,”healthwasacommodity,somethingof tradeandcommerce.Patientsbecameconsumers, clients, and“managed lives.”Hospitals and clinics becameproviders,whileinsurancecompaniesandHMOswerepayers.Inthisview,linesofrevenue,costcenters,booksofbusiness,andbottomlinescametodominate.
Lookingaheadtotoday’smedicineintheyear2050,wecanenjoyan“ecologic”metaphor.Inthismetaphorformedicine,disease is an imbalance, theworkof thephysicianandnurseisstewardship,healingbecomespartoftheprocessofchange,andthehospitalpartoftheecosystem.Withthewisdomofnatureasaguide,theecologicmetaphoroffersaworkableandsustainableapproachtohealththatacknowledgeskeyprinciplessuchasevolution(i.e.,weareina continuous,dynamic stateof change),interdependence(ourexistenceispartofalargerweboflife),limits(wehavelimitedresourcesanddefinedboundaries),diversity(everypartof thewhole isauniqueandessential contribution), and cycles (weareapartofnature’scyclicalpatternsandrhythms).
Now,intheyear2050,therearesev-eralnewfeaturesinthedesignofmedicine.Theseincludetechnologicalcurrencythatcan monitor “best practices” in clinicalmedicineandqualityandsafety.Thesefea-turesarepartneredwitheffortstohumanizethetechnologicalmedicalexperience.Thishasbroughtaboutagreateremphasisontheimportanceof“therapeuticpresence”andthevalueand impactof relationship forhealthcareprofessionals.Theappreciationofthepoweroflight,color,andbeautyhastransformedthedesignofourplacesofheal-ing,makingthemmorewelcoming,calm-ing,andtranquil.Themeaningfulandvitalpractices thatoccur inthesespaces, frommidwiferytobirthanddeathtoministeringtoallformsofdiseaseandillness,maketheexperiencebetweenhealerandpatientmoresacred.Thishas transformedthehospitalsetting into a templelike environment,
rather thanone that tends towardbeingantiseptically sterile andmechanisticallyprocedural.Compassion,hope,presence,and loveare seenashealingenergies aspowerfulasany.Theseandother“feminine”aspectsofhealthcare, suchas listening,service,andattendingskills,havechangedthefaceofmedicine.Further,asithasdonewithpolitics,economics,andissuesoftheenvironment,theglobal,multiculturalviewhascometodominatemedicineandhealthcare.AwarenessofsystemsofhealinghasspreadacrossinternationalbordersviatheWorldwideWebandthecollaborationandcooperationofpractitioners.Thepublichascometofavor,wheneverpossible,holistic,nontoxic,minimally invasive, “natural”care.Consequently,carethatispreventiveandoccursearlierinthepresenceorprogres-sionofadiseasestatehasnowbecomemorecommonplace, and thecareof end-stagediseaseislessconsumingofresources.
Patientsin2050continuetodemonstrateadesireforempowerment.Theytakemorepersonal responsibility for their self-careandlifestylechoices,evenastheycontinuetoseektheverybestinexpertadviceandcare.Understandingof the term“healthplan”has takenonanewmeaning andsignificancebeyondthenarrowimplicationsof insurance fordiseasecare.Morecost-effective solutionshelpbalance thehighcostsoftechnologicallybasedcare.Healthcareemphasizesprograms forwell-being,disease prevention and early detection,optimalaging,recoveryfrominterventions,and the replacementof badhabitswithgoodones. Integrativemedicine isnowawell-recognized,comprehensiveapproachinthepracticeofcontemporarymedicine,anapproachthatisrelationship-centered.Iteducatesandempowersindividualstobeactiveparticipantsintheirowncare,whilecomplementing biotechnical medicinewithabroadunderstandingofthenatureofhealth,illness,andhealing.Integrativemedicineacknowledgesaholisticapproachtothehealthandhealingofmind,body,andspiritinthecontextofthecollectiveandthecommunity.Itmakesuseofabroadspectrumofevidenced-basedtherapiesfrommultiplecultures tocreatepersonalwell-being,thepublichealth,andglobalhealing.Integrativemedicinehasa strong link to
ancientand timelessmedicalknowledgeandpractices.The“remembering”ofthisheritagehasthepotentialtostrengthenthepracticeofcontemporarymedicineasnewknowledgeandpracticesarediscoveredoverthecomingdecades.
Inthesecondhalfofthetwenty-firstcentury,peoplewillhaveagreateraware-nessandappreciationforthehealthimpactofthoughts,emotions,attitude,intention,optimism, gratitude,happiness, spiritualpractices, socialnetworks, and altruism.Evidencewillcontinuetogrowsupportingthebeneficialeffectsofahealthylifestyleonmorbidityandmortality.
Dr. Stewart is cofounder and Medical Director of the Institute for Health & Heal-ing at California Pacific Medical Center, San Francisco. He is a well-known ophthalmic plastic surgeon; editor of the three-volume classic text SurgeryoftheEyelid,Orbit,andLacrimalSystem, published by the American Academy of Ophthalmology; and past Chair of the Department of Ophthalmology at CPMC. He is presently a member of CPMC’s Senior Management Team and is the author of DeepMedicine, a book about unlocking the healing power of your inner wisdom.
ReferencesCohen JT,NeumannPJ,Weinstein
MC.Doespreventive care savemoney?Health economics and the presidentialcandidates.New England Journal of Medicine.2008;358,7:661-663.
EisenbergDMetal.Trends inalter-nativemedicineuseintheUnitedStates,1990–1997,Journal of the American Medical Association.1998;280,18:1569-75.
AstinJA.Whypatientsusealternativemedicine. Journal of the American Medical Association.1998;279,19:1548-53.
The Institute for Health & Healing began in 1990 at CPMC. Today it is a well-established hospital-based integrative medicine program. The Institute provides a wide range of inpatient and outpatient services across the spectrum of care and the life span. The Institute is located at CPMC, Marin General Hospital, and Mills-Peninsula Health Services. Learn more at www.myhealthandhealing.org or call (415) 600-HEAL (4325).
20San FranciSco Medicinemay 2008 www.sfms.org20San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
This article is not based on facts or even on predictions of inevitable future events. It is a projec-tion of possible infectious disease evolution and of the ramifications of some of our current treatments. It is a brief look into what we may be focusing on in the year 2050 in the world of microbes and their effects on humans.
I nthisyearof2050,wecontinuetofacepublic health challenges created byemergingorreemerginginfections.Zoo-
noseshavebeenthemajornewlyidentifiedinfections.Contributingfactorsunderlyingtheemergenceofinfectiousdiseasesincludemicrobialadaptationandmutation,changesin human demographics and behavior,increasedflowof internationalcommerceand travel, and failure of public healthmeasures.Rapidrecognitionandresponseonaglobal levelarenecessarytocontrolinfectiousdiseases.
Inthelatetwentiethandearlytwenty-firstcenturies,wewereimmersedinseveralviralepidemics—humanimmunodeficiencyvirus(HIV),hepatitisB(HBV),hepatitisC(HCV),andhumanpapillomavirus(HPV).Antiviral therapy was developed andrefined,providingeffectivecontrol,ifnoteradication,ofsomeoftheseviralinfections.By2008,HIVwasconsideredacontrollablebutnotcurableillness.ProjectedaveragelifeexpectancyofnewlyinfectedHIVpatientswasthirtyyears,withappropriateantiviraltreatment.Preventiveandtherapeuticvac-cinesagainstHIVwereaggressivelypursuedbut remained elusive. The retrovirus’sabilitytomutaterapidlyresultedinmanydiversecladesofHIV,precludingavaccineengineeredtorecognizeallthesesubtypes.Thefutileattemptatvaccinedevelopmentwasadifficultandexpensivelessonwewereforcedtolearn.
Asof2050,aneffectivevaccine forHIV has not been developed. In 2008,fundswere reallocated foraggressivepre-ventionprogramsand research shifted tomanipulationsoftheimmuneeffectorcells.Thesemanipulations involved the recep-tors (CCR5andCXCR4)on the surfaceoftheCD4TcellswhichweretargetedbyHIVtoallowentryoftheviralRNAintothecytoplasmoftheTcell.Later,in2022,anewchemokine,Interleukin18(Il-18),producedbytheCD8Tcellsthathadbeenactivatedagainsta similar retrovirus,wasidentified.Thischemokinecouldcomplete-lyblockexpressionofthereceptors(CCR5andCXCR4)ontheCD4cells.Asyntheticversionwasformulatedinpillform.Peoplecannowtakethispillonceeachmonthforsixmonths,andthereceptorsontheirCD4Tcellsbecomepermanentlyobsolete.HIVisnowapreventableinfection.InpatientsalreadyinfectedwithHIV,Il-18hasbeenusedasa therapeutictool inconjunctionwithantivirals.Because thecoreceptors’expression isblocked,HIV isnotable tocommandeertheCD4Tcelltouseinitsreplication,and so iteventuallydiesout.Themostdevastatingepidemic in recenthistoryhasfinallycometoanend.
Information learned from the HIVepidemicwas invaluable in treating thehepatitis epidemics. The recombinantHBVvaccinehasremainedaneffectiveandinexpensivepreventivetherapy.AvaccinedirectedagainstHCV,although initiallydifficulttorefine,wasfinallydevelopedin2040andhasprovedtobeefficacious.Ad-equatetreatmentofthosealreadyinfectedbyHBVand/orHCV followed thepathoutlinedforHIV.High-potencydrugsusedincombinationtosetahighgeneticbarrierwererequiredtoreducethedevelopmentof
resistancebytheviruses.ThedevelopmentofanHPVvaccine
hasprovedtobeanexampleofignoringoratleastnotfullyunderstandingtheinforma-tionwehadlearnedworkingwithHIV.Hu-manpapillomaviruswasalsoaviruscapableofrapidmutations,resultinginnumerousstrains.AswithHIVvaccineattempts,itwas impossible toproduceavaccineabletoidentifyallthevariousstrains.However,giventhatthemajorityofdiseases(analandgenitalwarts,analandcervicaldysplasia,andcancers)werecausedby fourof thestrains,avaccinewasdevelopedagainstonlythosefourstrains.Thesecondmajormistakewastherecommendationthatonlyaportionofthepopulationatrisk(girlsandyoungwomenagesthirteentotwenty-five)shouldreceivethevaccine,leavingalargegroupatriskforinfection.Thisproducedaselectivepressureon thevirus,allowingmutationstoarise.Nowin2050,forty-fiveyearsafterintroductionoftheHPVvaccine,weareagainimmersedinanepidemic.Severalofthepreviously“benign”strainshavetrans-formedintopathogenicand/oroncogenicstrainscausing significantmorbidity.Wearewitnessingmorerecalcitrantanalandgenitalwartsandmoreaggressivecervicalandanalcancers.
TheinfluenzaApandemicof2046wasanexampleofrapidrecognition,interna-tionalcollaboration,andeffectivecontrolmeasures. The pandemic was predictedandanticipatedbyanalyzingtheantigenicshifts of the virus and identifying twohighlypathogenic strains found inavianpopulationscocirculatingwithhumanin-fluenzaviruses.Rapidresponseteamswerequicklydeployedtocontrol the infectionintheavianpopulations,implementingaquarantineandisolationpolicyinaffected
A Fragile BalanceHumans and Microbes in the Year 2050
Kristin J. Razzeca, MD

20San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine2120San FranciSco Medicinemay 2008 www.sfms.org
communities and enforcing the closingof schools,churches, shoppingmalls,andgyms. The travel industry, includingairportsandbusand train terminals,wasquickly closeddown.Stockpilingof theantiviralsupratamivir(afourth-generationoseltamivir)andtheuseofprotocolsthatallowedrapiddisseminationofthemedica-tionto“hotspots”provedtobeefficaciousandprevented significantmorbidity andmortality.Despitetheseefforts,theinfluenzapandemicof2046stillclaimedthelivesofsixmillionpeople,mostlytheelderlyandtheveryyoung.
Many of the zoonoses, transmittedthroughvectors,thathadappearedinthefirsthalfof the twenty-firstcenturywereparticularlychallenging.Climatevariabil-ityhadfosteredincreasesinthemosquitopopulation,resultinginseveraloutbreaksofzoonosessuchasdengue,WestNilevirus,malaria,andothers.Aggressivemosquitocontrolprogramswereundertaken,incor-poratingaerial sprayingof infestedareasand reductionof larvalbreeding sources.DengueandWestNilevirusoutbreakswerelastidentifiedin2030.Casesofmalariahavedeclinedsignificantly.
Poor andunderdeveloped countriesgiverisetomanyofthezoonosescapableofcausinglife-threateningdisease.Emerginginfectiousdiseases require thatproactiveratherthanreactiveactionbetaken.Thebushmeattradeandwildlifeencroachmenthave been stopped. Conservation anddisease surveillanceprogramshavebeenimplementedandhaveplayedintegralrolesincurtailingoutbreaks.
Developedcountrieshavealsoexperi-encedchallengingproblems.ThousandsofpeopleworldwidehavebeeninfectedwithavariantofCreutzfeldt-Jakobvirus,caus-ingearlydementia.Itwasnotuntil2045thatmanygovernmentsinstitutedstricterinspection and control measures in thebeefindustry,sharplyreducingthenumberofnewcases.
Vaccinationsremainacornerstoneofinfectiousdiseaseprevention.Understand-ingtransmissionpathwaysandidentifyingnatural,definitivereservoirsfortheviruseshelpdeterminecandidatesforvaccination.Batswereidentifiedasdefinitivehostsfora number of lethal infections including
Marburg/Ebola,SARScoronavirus, andNipah/Hendraviruses.Humanswereac-cidentaltargets.AvaccinewasdevelopedagainstthelethalMarburg/EbolavirusandwasgiventotheAfricanminerswhoseworkbroughtthemintoclosecontactwithbats.AnoutbreakofMarburg/Ebolahasnotbeendocumentedsince2025.Attemptsatvac-cinedevelopmentagainsttheseandotherdeadlypathogenscontinue.
Mutatingbacteria developing resis-tancetoantibioticshavecontinuedtobeproblematic. Highly resistant strains oftuberculosiscontinuetoevolve.Newmedi-cationshavekeptthisreasonablycontrolled,butitbecameapparentthatadditionalmea-sureswereneeded.AttheUnitedNationsMilleniumSummitin2000,representativesfromseveralnationsauthoredtheMillen-niumDevelopmentGoals tohelppoorercountries.Proposalsaddressingseveralissuessuchaspoornutrition,availabilityofcleanwaterandhealthcare,educationaloppor-tunities,genderinequality,andpreservationoftheenvironmentwerefunded.Significantimprovementsweremade and the goalshavebeenreviewedandreestablished,oradditional ones formulated and funded,everyfifteenyears.Theachievementsresult-ingfromthiscollaborativeendeavorhavebeenextensiveandareexpressedinamajordeclineinTBcases.
Another rapidly mutating bacte-rium,Staphylococcusaureus (MRSA), isstillmakingheadlines in theyear2050.Methicillin-resistantStaphaureusbecameamajorproblem inhospitalswhere an-tibioticsusewasprevalent.Community-acquiredMRSA(CA-MRSA)appearedasadauntingprobleminthefirstdecadeof the twenty-first century.Outbreaks ingyms,prisons,schools,andinthegaycom-munityposeddifficult challenges as thebacteriadevelopedresistancetopreviouslyeffectiveantibiotics suchasvancomycin,linezolid,andtigecycline.Third-, fourth-,andfifth-generationantibiotics arenowusedincombinationtocontrolthisinfec-tion.Medicalstudentsareinstructedcare-fullyon judicioususeof antibiotics, androutineuseofantibioticsisprohibitedinthelivestockindustry.Basicpersonalhygiene,with frequenthand-washing, cleaningofgroupequipment,andwearingofmasksand
respiratorsinhigh-riskencounters,hasbeenshowntodecreasetransmissionofseveralinfectiousdiseases.
Themappingofthehumangenome,oneof themost innovative and collab-orativeenterprisesinthehistoryofscience,providedusauniquemeansofinterveningin human disease states. Coupled withtheability toharvest stemcells fromtheskin,gene therapy isnowwidelyused inthepreventionand treatmentof severalcommondiseases—cysticfibrosis, diabe-tes, schizophrenia,majordepression,andmultiplesclerosis—aswellaslesscommonillnessessuchasHuntington’s,Wilson’s,andMarfan’s.WenoworderagenogramfortheindividualpatienttoidentifyabnormalitiesdetectedintheirDNA,topredictthepos-sibilityofdiseaseoccurring,andtodecidewhetherinterventioniswarranted.
Oncology and immunology havebeen themost rapidly developing fieldsusingthesemethods.Todaytreatmentofamalignancyistailoredtospecificreceptorsexpressedonthetumor.Theappropriateim-munomodulatorstosuppressthesereceptors,allowinglesstoxicchemotherapytobemoreeffective,areused.Computerizedanalysisofsubmittedbiopsyspecimensgeneratesahistologicdiagnosis,identifieschromosomaltranslocations andgene rearrangements,anddescribesreceptorexpression.Thespe-cificimmunomodulatorsandchemotherapyrequiredfordestructionoftheneoplasmcanthenbeselected.Finally,in2050,wecansaywearewinningthewaroncancer.
Thisretrospectivelookatthefirstfiftyyearsofthetwenty-firstcenturyhasfocusedontheaccomplishmentsaswellasthemistakesmadeininfectiousdiseasecontrol.Newandold infectiousdiseasescontinuetoemergeandreemerge.Evennow,as inthehistoryofthelast200years,itremainsobviousthatold-fashionedpersonalhygieneisanessentialcomponentinlimitingdiseasetransmission.Sopleaseremembertowashyourhandsandcontinuetousecondoms.
Kristin J. Razzeca is an immunologist and HIV specialist at Stanford University School of Medicine, with a clinical practice at Camino Medical Group.

22San FranciSco Medicinemay 2008 www.sfms.org22San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
H ereweareintheyear2050,alreadymakingpreparationstocelebratethebicentennialofCharlesDar-
win’sculture-transformingopus On the Ori-gin of Species(1859).AsIreflectonthismo-mentousupcomingoccasion,IamamazedathowDarwin’soriginaltheoryhashadtoberevised.Theramificationsofthesemajorchangeshavehadtheirgreatestimpactonmedicineandcontinuetoreverberatewitheachnewstunninginnovation.
Darwin’s bookdid forbiologywhatNewton’s1687 Principiadidforthefieldofphysics:Itpresentedanentirelynewpara-digm.Duringthe200yearsafterNewton’spublication,physicistsbecameincreasinglyconvincedthathistheorieswerethefinalword.Whatashock,then,whenEinstein’srelativitytheoryandBohr’srefinementofthequantumforcedphysiciststoabrogateNewton’sseeminglyimmutablelawsfortheworldoftheveryfastandtheverysmall.So,too,hasthesameturnofeventscometopassforDarwin,whoseexplanationconcerninglifewas also thoughtbybiologists tobedefinitive.
LetusbrieflyreviewDarwin’scentralidea.Evidenceexiststhatlifeappearedonthis planet approximately200,000yearsafter the planet coalesced four billionyearsago.Fromthebeginning,thecarbonbenzeneringhasformedthebasicbuildingblockofeverylifeform.Theimprobabilitythatheavyatoms forged indistantsuper-heated supernova managed to combinewithcarbon,nitrogen,andoxygentoformaminoacidsinthevastwastelandoffrigidintergalacticdustcloudsstaggerstheimagi-nation.ThathereonEarth theseaminoacidswouldarrange themselves into theself-replicatingmoleculeDNAisanothercauseforsheerwonder.
According toDarwin, lifebotspro-gressedinfitsandstarts,seekingenviron-mentalnichesinwhichtheycouldsurvive.Adaptationstochangecameaboutthroughbeneficialmutationsof individual genes
(anearlierMendeliandiscoveryofwhichDarwinwasunaware). Initially, cloningwasthepreferredformofreproduction,butitsufferedonemajordrawback:Clonesareimmortal.Itwasslowgoinguntilanentirelyunexpectedeventturnedthewholeshowintoariotousprofusionoflifeforms.Outofnowhere,naturalselectionserveduptwostartlinginnovations—sexanddeath.
Sexshuffledandreshuffledthegenesoforganismsthatwereconstantlyfacedwithenvironmental challenges.Resemblingaplanetaryvaudevilleact,anongoingcongalineofpossibilitiessnakedacrossthestageunderthelimelight,auditioningforapartin theplay called life.Death sat in thedarkenedsecondrow,decidingwhichactswouldbe inthenextseason’sproductionandwhosecareerswouldbeextinguished.
Sexcombinedwithdeathprovedtobeanexceedinglysuccessfulprogram.Naturalselectionpopulatedtheentireplanetwithabewilderingvarietyof living creaturesthat swam,flew,crawled,plodded, leapt,andstalked—andallofwhomeventuallydied.Despitetheirprofusion,everyspecies’
chassishadasitsbasistheubiquitouscar-bonmolecule.Andanabsolutelyessentialrequirementofalllivingformswasthattheyneededaphysicalbodyinordertoexist.
Aftermorethanfourbillionyears,onespeciesemergedthatbrokethemold. Homo sapiens developedacomplexformofcom-municationthatwentbeyondanythingthathadprecededit.Noscientisthasacredibleexplanation forhoworwhyhuman lan-guageemergedinallitsrocococomplexity,butforthefirsttimeinthehistoryofearth-basedlife,somethingemergedthatdefiedthegeneralschemeofDarwin’sgrandthesis.Humanlanguagewasthefirstlivingentitythatdidnotpossessaphysicalbody.
Languageisasymbioticorganismthatneedsthecorporealbodiesofacriticalmassofhumansinordertoexist.Andhumansasaspecieswouldneverhaveattainedtheirexaltedpositionwithout their incessantabilitytoyakitty-yak.Languagespossessallthecharacteristicsofalivingform:Theyareborn,theymature,theycompetewithoneanother,theyadapt,theysplinterintonewspecies,andtheydie.
Humanlanguageshort-circuitednatu-ral selection.Forachild to learn to lookbothwaysbeforecrossingthestreetundertheold (speechless)methodwouldhaverequiredthatmanygenerationsofchildrendiedbeforeabeneficialmutationappearedinthegenomethatforcedthechildtolookbothways.Withtheadventofspeech,par-entscouldteachtheirchildrenthelessoninafewhoursinsteadoftheeonsitwouldhavetakentowaitforamutation.
Knowledgeaccumulated in thevastwebof culture.Languagemidwifed intoexistence an ancillary improvement insurvivalforhumanscalledmedicine.Thereisnothing in theobservablebehaviorof
Darwin Revised!Reflecting on Darwin’s Theories from the Year 2050
Leonard Shlain, MD
“The ramifications of these major changes have had their greatest impact on medicine and continue to reverberate with each new stunning innovation.”

22San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine2�22San FranciSco Medicinemay 2008 www.sfms.org
otheranimalsthatsuggeststhattheyhavemasteredtheartofinterferingwithnaturalselectionbyinventingmedicinesandpro-ceduresthatcancure,palliate,andprolongthelifespanoftheirspeciesbytamperingwiththenaturalorder.Someevidenceexiststhatchimpanzees,ourclosestcousins,plusbaboonsandafewotherspecies,intuitivelyknowtochoosecertainmedicinalplantstoalleviatethatwhichailsthem.Butwithoutlanguagetherecouldbenoscienceandob-viouslynoNew England Journal of Medicine,noralltheotheradvancesthathaveaccruedto the speciesdue tohumans’ constant,invisibledoppelgänger—language.
Medicinedidnotreallybegintoalterour species until the refinement of thescientific method, which began in theRenaissanceandfloweredintheEnlighten-ment.Inthenineteenthcenturyitgainedspeedandmomentum,andinthetwentiethcentury an astonishing arrayofmedicaladvancesaidedandprolonged life spans.Thushumans,inleaguewiththeirsymbioticectoplasmicpartner,mushroomedintothemostpopulouslargemammalontheplanetand intheprocessgaineddominionoverallthebeastsandfowl.Andthecrosstalkthatlanguageengenderedledtoaseriesofmodernmedicaladvancesthatfinallygavehumansdominionoverbacteria,parasites,andmostviruses.
Butitwasthefirsthalfofthetwenty-firstcenturythatwitnessedanothersharpriftwiththelawofnaturalselection.Theemergenceof an insubstantial symbioticlifeformallowedthisonespeciestobuildanewhybridthatbegantobreaklife’sutterdependenceonthecarbonring.
Carbonisoneofthemostcommonelementson theplanet.Another, found
inabundance,issilicon.Whencombinedwithoxygenintheformofsilicondioxide,itformssandanddirt.Thesiliconatom,oneofthetraceelementsnecessarytomaintainhomeostasis,playedaminorroleinkeepinglivingthingshealthy.Andthen,inthelatterhalfofthetwentiethcentury,cleverhumansdiscoveredthatsilicondioxidepossessedapropertythatwouldallowittoconductalow-resistanceelectriccurrent.Fromthatdiscovery, combinedwithanewbranchofphysicsknownasquantummechanics,themoderntransistorwasborn.Replacingbulkyvacuumtubes, transistorsbegan toappearinincreasingnumbersinallelectricalappliances.Everydevice—radios,TVs,cellphones—shrank.But siliconcompoundspossessedanotherpropertythatmadesomeofthemespeciallyfelicitousformedicine:Theyfailedtoarousetheever-vigilantim-munesystem.Encasingsilicondioxidetran-sistorsinasiliconesleeveallowedphysicianstoimplantsophisticatedminimachinesintothehumanbody.
Soonsurgeonswereimplantingallsortsofsilicon-baseddevicesthatincreasedlifespans,alleviateddisease,andevenincreasedsexualallure.Cardiacpacemakers,insulinandmorphinepumps,transistor-basedar-raystolettheblindseeandthedeafhearallbecameincreasinglyroutine.Monitorsto check for arrhythmias andoncomingepileptic fits competed for space in thephysicalbodyalongsideoldercarboncon-glomerations.
Asthetwenty-firstcenturyprogressed,thespeedwithwhichnewmedicaladvancesarose,especiallythosethatrelieduponsili-condioxide transistors, tookone’sbreathaway.Moreandmorehumanswerelivinghealthier, longer lives because of these
implants.As the amountof silicon increased
in relation to theamountofcarbon inaperson’sbody,itbecameincreasinglyclearthatDarwin’s theoryofnatural selectionwouldhave tobe revisedonce again ashumansmorphedintocyborgs(cybernetics+organic).Partiallyinorganicandpartiallyorganic,weconstitutedanentirelynewlifeform.Further,themassivecomputersthatallowedmedicalresearcherstomanipulatethegenomedependedontheinteractionofsiliconandcarbontounexpectedlyreviseDarwin’stheoryinanotherspecies-changingmanner.Whocouldhave imagined thatsuch a stunning series of events couldhappentoevolutionaryprocesseswhen On the Origin of Species appearedin1859!
Complexity theory, formerlyknownaschaos theory,proposes thatas systemsbecome more complex, the possibilityincreases thatanemergentpropertywillsuddenly appear thatnooneexaminingthesystemcouldhaveeverpredicted.(Hy-drogen,aflammablegas, combinedwithoxygen,acombustiblegas,canyieldaliquidthatextinguishesfire!Whowouldathunk!)Asweenterthelasthalfofthetwenty-firstcentury,deeply immersed in theanneal-ingoftechnologyandlifeforms,whocanpossiblyanticipatewhatmightcomenext?We humans are undergoing a profoundmetamorphosis aswe transition into anentirelynovelspecies.Forthosewhodoubtitishappening,remember:Whenyouarebuffetedinthecenterofaspinningwashingmachine,it isnearlyimpossibletonoticethattheclothesarebecomingcleaner.
Leonard Shlain can be reached at [email protected].
Welcome New Members!TheSanFranciscoMedicalSocietywouldliketowelcomethefollowingnewmembers:
ACTIVE REGULAR MEMBERSCary Canoun, MD—Referred by Gregory Buncke, MD
Ping Chow, MD—Referred by CMA Ofelia Maristela, MD—Online Application
Amir Ali Rafii, MD—The Permanente GroupMark J. Savant, MD—Referred by Robert Murray, MD

24San FranciSco Medicinemay 2008 www.sfms.org24San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
I nthefollowingtwosnapshots,twocaseswillbepresented—one fromtheyear2008, theother from2050.Thefirst
underscoresmissingaspectsof treatmentin2008,andthesecondcovershoped-fortreatmentin2050.
Psychiatric Moment 2008Twomonthsago,amotherandfather
calledmyofficeaskingformyadviceaboutthepsychiatriccareoftheireighteen-year-olddaughter,Eva,whohasanorexianervosa.TheytoldmethatEvabegandietingtwo-and-a-halfyearsagowhenshewasfifteenyearsold,buttheymention,sadly,thattheydidn’tnoticetheseriousnessofherbehavioruntilalmostayearlater.“Shelookedsomuchbetter,thinner,thatwedidn’trecognizeherdietingcouldbesuchaproblem.”
Oneyearlater,attherecommendationofEva’spediatrician,whowasconcernedaboutherweightdropatheryearlyphysi-cal,theysoughtpsychiatrictreatmenteventhoughtheydiscoveredthattheirdaughter’scondition—and,infact,mostmentalhealthproblems—wasnotcoveredbytheirhealthcareinsurance.Theirfirsttreatmentexperi-encewaswithafamilytherapistwhotreatedanorexianervosasolelyfromthisperspective.Aftersixmonths,theyunderstoodtheirfam-ilybetter,buttheirdaughterhadcontinuedtoloseweight.Frustratedandworried,theychangedtreatmentandthistimeworkedwithapsychopharmacologistwhodiagnosedEvawithdepressioninadditiontoanorexiaandbeganaselectiveserotoninreuptakeinhibi-tor,butnoothertherapy.Theirdaughter’sweightcontinuedtofallandshecomplainedthatshehadnoonetotalkwith.Herpar-entsswitchedtreatmentagain,thistimetoa therapistwhoworked individuallywithpatientswithanorexianervosa.Duringthis
treatment,thegirlstoppedhermedicationabruptlyandhernewtherapistrefusedtotalkwithEva’sparents,becauseofconfidential-ity.Theirdaughtersaidshewashappier,butherweightcontinuedtodropandhernowveryworriedpediatrician insistedthat theparentscallme.
Theydocalland,notsurprisingly,theyareangry. Inourfirst sessiontogetherweexploreseveralreasonswhytheyareangry.First,theyareangrywiththemselvesbecausetheymissedtheearlysymptomsofanorexianervosa; inaddition, theyareangrywithaculturethatovervalues thinness inado-lescentgirls.Theyarealsoangrywiththethree treaterswhoadheredexclusively totheirownperspectivesonhealthcarewhiletheirdaughter’shealthdeclined.Andlastly,theyareangrywiththeirinsurancecompany,whichdoesnotcovermostmentalhealthillness.Althoughtheycannotsayit,theyarealsoangrywiththeirdaughterforhavingthisillnessandnotgettingbetter.
Theyare frustratedwhen IdescribetheytypeofcarethatIbelieveisneededtohelptheirdaughter—regularvital-signandweightcheckswiththeirpediatricianand,ifnecessary,aspecialistinadolescentmedicine;andacombinationofindividual,family,andpsychopharmacologictherapieswithsome-onewhoworkswitheatingdisorders.Iaddthatgroupand inpatient treatmentmightalsobenecessary,dependinguponthesever-ityandchronicityofEva’sillness.Iexplainthatanorexianervosaisoftenatoughillnessthatrequiresthecombinedenergyandcareofseveraltreatersandperspectivestofight,andthatIamsorrythatthetreatmentthattheirdaughterhasreceivedsofarhasnothelpedhermoreandthattheirinsuranceplandoesnotcovermostmentalillness.
Tobesthelp,ItellthemthatIwillmeet
withthemandtheirdaughterandconsultwith all of their daughter’s treaters,herschool,andtheirinsurancecompany.Then,withtheirdaughterpresent,wewillstrategizetogether,lookingatwhatwillworkbesttohelpherandthem,andalsoexaminingwhattreatmentisabsolutelynecessary.Whatcantheyafford?Whattreatmentscantheyfindatnoorlowcost?
WhenImeetwithEvaIdiscoverthatshe,likeherparents,isdisheartenedbythetreatmentexperiencesofthelastyearandahalf.Sheregretsthetremendousexpensethatshehascausedherfamilyandisstrugglingtochangebothherthoughtsandherbehaviors,but sheadmits tomereluctantly that thenegativepatternshavebecomestrongeroverthepasttwo-and-a-halfyears,andthatshenowspendsmuchofherfreetimeonInternetanorexiasitesthatsupportherillness.
WhenIspeakwithherthreetreaters—eachrecognizedexpertsintheirrespectivespecialtiesoffamilytherapy,psychopharma-cology,andindividualtherapywithadoles-cents—Iamimpressedwiththeirknowledgeandconcernfortheiryoungpatient,butIamalsostruckbytheirinabilitytothinkoutsidetheirownboxandcreativelystrategizeaboutEva’streatment.
NextIspeakwiththehealthinsurancecompany,whichtellsmethatitwillpayforcare—thatis,ifEvaishospitalizedformalnu-tritiontheywillcoverhercostsbecausetheyviewthatasamedicalillness,buttheywillnotcoveranyoutpatientpsychiatrictreat-ment.Scoutingforlow-costorfreeservices,Idiscover that thereare severalprogramsavailable.Aresearchstudywillprovidefreeshort-termcare—fourmonthsforEvawhilesheisintheirprogram—butfollow-upisnotavailable.IconsultwithBeyondHunger,agrassrootsanorexiaorganization,whichoffers
Psychiatric MomentsExperiences from the Years 2008 and 2050
Lynn Ponton, MD

24San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008San FranciSco Medicine2524San FranciSco Medicinemay 2008 www.sfms.org
apositiveexperienceformanygirls,schools,andfamilies.
Although Ihaveworkedwith ado-lescentgirlswitheatingdisordersformorethanthirtyyears,Ialsoconsulttherecentliterature,looking,inthiscase,fortreatmentadvancesthatareapplicabletoEvaandherfamily.Whileonline, Ivisit thegrowingnumberofanorexiasitesthatEvaspendssomuchtimeonandnotetheir increasinglyseductiveoutreach.Thesitesofferanidentitywithothergirlswhohaveanorexia,providingexchangeof information,connection,andacertainpower to thegirlswho frequentthesites.
WhenImeetwithEvaandherparentstodiscussmyideas,Ioutlineseveralseriousproblemsalongwithpossible strategies. Irecommendandoffer tohelpthemfindasingletreater,experiencedinworkwitheat-ingdisorders,whocanprescribemedications,conductbothindividualandfamilytherapy,andworkcloselywiththeirpediatrician.AsecondchoicewouldbeatherapistwhocanconductbothindividualandfamilytherapyandcollaboratecloselywiththepsychiatristwhowillevaluateEvaformedications.
I also recommend thatEvaandherschoolcounselor (whohasbeenhelpful,lettingmeknowthatEvaand severalofher friendsarepartofamini-epidemicofgirlsstrugglingwitheatingdisorders)attendBeyondHunger,thegrassrootseducationalgroup—andthatthecounselordevelopthestress-reductionmeditationgroup shehasbeenplanningtostartatEva’sschool.IhelpEva’spediatrician,whohasbeenvaliantlystrugglingwithhercare,connectwithanadolescentmedicinephysicianwhospecial-izes in thisarea. Ihelp theparents limitcomputeraccesstotheanorexiasites.
At theendof this evaluation,Eva’sparentsarelessangryandEvaismorewill-ingtocooperatewithhertreatment.Buthertreatmentisstillexpensive—prohibitivelysoformanyfamilies—andhercasehighlightsmajor problems associated with mentalhealthcarein2008.
challenges in 2008Failure to Recognize Mental Health Illness as Disease
The treatmentofmental illnesshassufferedseriouslyduringthepasttwenty-five
years,victimtoafailuretoacknowledgetheproblem.Therearemanyreasons for this.Publicstigmaagainstmentalillness,presentforcenturies,continuesdespitevalianteffortsfromindividualandnationalorganizations.Inaddition,Eva’sillness,anorexianervosa,isoftenseenasapositivetraitbyapublicseducedbyunhealthy,air-brushedimagesofadolescentgirlswhosecollectivebodiesareusedtosellconsumergoodstoafemalepopu-lationwhosedissatisfactionwiththeirbodiesisincitedbythemedia.Lastly,mentalillnessisfrequentlynotacknowledgedbyinsurancecompanies,forfinancialreasons.
Failure to Pay for Mental Health CarePrivate insuranceand federalpayers
alikerefusetocoverevenaportionofthecostsofmentalhealthcare.Chronicmentalhealthcareisfinanciallydebilitatingforpa-tientsandtheirfamilies.Eva’sanorexiafallsintothiscategory.Recentlawshavemadeanimpact,requiringhealthcarecompaniestoprovideparityforsomementaldiseases;butoftennecessaryhealthservicesareso“carvedout”thatpaymentforthemleavesmorethananorecticsstarving.
Adherence to One Theory or One Treat-ment Approach
Psychiatricandpsychological treatersoftenlimitthemselvesbylearningandusingonetreatmentperspectiveoncare.Eva’scaseillustratesthisproblem.Anorexianervosaingirlsundereighteenisbesttreatedwithanintegrativeapproachthatcombines familyworkwith individual therapy,whichusescognitivebehavioraspectsatthebeginningoftreatmentwhenagirl’sweightisdanger-ously low,pairedwithdynamic relationalelementsasherweight increasesand shefurther engages.Medicationsareusedasneeded.Mostimportantistherecognitionoftheintegrationofmindandbodyinprac-ticalandeffective treatmentapproaches.Dogmaticadherencetoa single theoryortreatmentapproach is limiting topatientandclinicianalike.Insummary,deliveringpsychiatrictreatmentin2008leavesmuchtoworkonandtohopefor.
clinical Moment 2050In2050,Eva’sdaughterandherhusband
receiveacallaboutEva’sgranddaughter,Eri-
ca,fromthehighschoolclinic.ThecounselortherehasnoticedErica’sweightisdroppingandthatsheisnolongereatingherlunch.Ericaistheninvitedtojoina“healthylunch”groupwithseveralofherfriendswhoarealsodieting.Hermotherandherfatherareaskedtoparticipateinafour-partpreventionpro-gramforfamilies,whicheducatesthemaboutunhealthydieting,negativemediainfluences,adolescentdevelopment,andrisk-takinganddisease.Onemonthlater,whentheschool’snursepractitionernoticesErica’sweighthascontinuedtodrop,herpediatricianinitiatesregularvisits,comingtotheschoolcliniconeafternoonaweek.Inaddition,apsychiatristspecializinginadolescenteatingdisordersbe-ginstreatmentusinganintegrativeapproach,meetingwithEricaonehourperweek.Thecostsarepaidforbyabasichealthcarepack-agethatcoversallhealthconcerns—forbothmindandbody.Thesetwoaspectsofeachpersonarenolongertreatedseparatelybutareseenaspartsofanintegratedwhole.Aspartofthistreatmentpackage,familytherapyanddietarycounselingaredesignedforEricaandherparents.IndividualtherapyisavailableforErica’smotherandfatherforanadditionalfee.Supportedbythefamilytherapy,Erica’smotherelectstoparticipateinit.
AtthetimeofErica’streatmentin2050,anorexianervosa,anillnessthathasvariedepidemiologicallyoverthepast2,000yearsandisaffectedbyculturalcomponents,stillexists.Thereare,however,severalimportantchangesinitstreatment:
• Preventioneffortstargetingadolescentgirlsareongoing,andearlierdetectionleadstoearliertreatments.
• Researchisbuiltintoboththetreat-mentandpreventionefforts,whichbeginatErica’shighschoolanditsassociatedhealthclinic.Further researchstudieshavedem-onstratedandreinforcedtheimportanceofearlydetectionofanorexianervosa,diagnosisandtreatmentofcomorbiddisorders,andfamilyparticipationandtreatmentinaddi-tiontoindividualandpsychopharmacologictreatment.
• Newandmoreeffectivemedicationsaddressanxietyandabdominaldiscomfortassociatedwithrefeeding.
• Mostimportant,anorexianervosaisnowwidelyunderstoodasanillnessinvolv-
Continued on Page 31...

26San FranciSco Medicinemay 2008 www.sfms.org
Back To THe FUTUreoF Medicine
s ubject: AnnualBack-to-the-FutureReport on the status ofDepart-mentsofRadiologyandBiomedical
Imaging,2050
Patient ProceduresAdvances in systemsandprocedures
forbiomedicalimaginghaveprogressedinthepastfiftyyearssothatnow,intheyear2050,patientswhoneeddiagnosticorthera-peuticimagingmaketheirappointmentbycomputer,registerintothedepartmentviaa retinal scan, andhave theirprescribedstudies(X-ray,whole-bodyCTorMR,US,nuclearmedicine).When theprocedureis complete, thepatients leavewith thedictatedreportintheirhands,thereferringphysicianhavingbeenautomaticallysentthereportsimultaneouslywiththestudy.Ifavisuallyguidedbiopsywasneeded,thepro-cedurewasdoneduringthisinitialvisit.
Asanexampleof the increasedeffi-ciencyofbiomedicalimaging,adiagnosticworkupforjaundiceinthe1960smighthavetakenmanyweeks.Inthe1990s,withtheadventofCT,thediagnosisofobstructedbileducts couldbemadeat the timeoftheCTexamination,thenanERCPandbiopsywouldensueoverthenextfewdays,afterwhichatreatmentregimencouldbeinstituted.Nowadays,intheyear2050,thediagnosisofthemalignancycanbeidenti-fied inonevisitand treatment institutedimmediately.
Professional StaffingDepartmentsarelargelydevoidofpeo-
plewhooncewerethebackboneofradiology.Thereisnoneedforreceptionists,clericalpersons,or transcriptionists. It isalldonebycomputer.Theonlypersonnelon sitearetheradiologicalinterventionalists,their
technicians, and theirnurses.RadiologicultrasoundtechniciansandIT(informationtechnology)workersareonhandandareheld inhighregard fortheiruniqueskills,thelattermaintainingthepicturearchivingcommunicationsystems(PACS).
Inteachinginstitutions,acoreofcen-tralizedacademicians supervise residentsandfellowswhomaybeworkingindiffer-entinstitutions—videoconferencingallowsface-to-facecontacttodiscussproceduresorparticularteachingpoints.
radiologistsRadiologistscanpractice inreal time
anywhereintheworldforpatientsandrefer-ringphysiciansanywhereelseintheworld.Theradiologistsreviewthecasessentbycom-puter,usingadvancedelectronicenhancingtechniquesfordetails.Mostofthestudiesareinitiallyreadbyroboticneuralnetworksandthensentforconfirmationtotheradiologists.Forthereports,theradiologistssimplyspeakto the computer,which recognizes eachindividualvoice,printsoutthereports,andspeedsthemoffalmostinstantaneouslytothereferringfacilities.
If radiologistsneed to reviewcasesthathadpreviousbiomedical imagingatanotherhospitalinanotherstateorcountry,theradiologists,usinganaccesscode,cangetreadyaccesstotheseimagesandthedictatedreports.
Recognizingtheglobalimpactofimag-ing,radiologistsarenowcredentialedunderoneprocessinalloftheUnitedStatesandsomeforeigncountries,ratherthanbyanti-quatedstatelicensingboards.
UltrasoundStandardultrasoundisnowatoolthat
mostclinicianscarryintheirpockets:asmall
imagingcomputerforquickassessmentoffreefluidinthechest,abdomen,orsofttissues;forforeignbodydetection;forcalculiinthekidney;forgallstones;forearlypregnancyde-tection;andformasses,superficialordeep.Insomecases,familiesareprovidedwiththesecompactcomputersandtaughthowtousethemathometoscreenfamilymembersathomeforgrossabnormalitiesortomonitortheirfollow-upcare.Thesehomeunitscansendtheimagesinstantlytotheattendingphysiciansforfurtherevaluation.Addition-ally,mostmedicalschoolshaveanultrasoundunitintheirsciencesectionssothatstudentscanlearnanatomyandsomephysiologyinrealtimewithultrasound.
Ultrasoundindepartmentsofbiomedi-calimagingandradiologyisnowmechanized,similartoCT,toscanlargeareasofthebodyinrecordtimewithnoradiationdose.Trans-ducershavebeendeveloped topenetratethe skull andareused to localize lesionsquicklyin3-D,andthenfocusedultrasoundenergycanbedirectedtoaspecificlocationforlesionablation.Nanotechnologytargetstumorsproducingantigenswithantibodiesthatlightupintheorgantobetreatedwithfocusedultrasound.
Ultrasoundwithinbiomedicalimagingdepartmentsalsoisnow“volume”orientedforthecapabilityofablationproceduresoftumorssuchashepatoma,uterinefibroids,and thyroid lesions. It is combinedwithelastographytodetectfirmnessoflesions,anindicatorofmalignancy.Colorflowhasde-velopedtoshowmicrocirculationsinmassesandhaslargelyreplacedangiographyintheassessmentofvasculardisease. Imagesaregeneratedinamatterofsecondsandsignaltonoiseisgreatlyenhancedforimagesofincrediblefidelity.
Biomedical ImagingComputerized Radiology in the Year 2050
Gretchen A. W. Gooding, MD
Continued on Page 31...
www.sfms.org may 2008 San FranciSco Medicine27
Back To THe FUTUreoF Medicine
f irst, I should say, itwasneverpersonal.Butwe’retheinvisiblebugs,andwewon.
Wewereherefirst,youknow,beforeanyotherlivingthingandfortwobillionyearsbeforeyoustartedtoshowup.Butitwasnicehavingyouhumansaroundforarelativelyshortwhile,eventhoughfor a time there you seemeddeludedenough to thinkyoucouldget ridofus.Yourskinandinternalbodiesweresuchgoodhosts—infact,wesometimescolonized up to 90 percent of the cellsinyourbodies,withmaybeonehundredtrillionofusmicrobesthrivinginandonyou,fromtoothtotoe.Whilewetriedtoreachanicebalance—what you fancilycalleda“homeostatichost/parasiterelation-ship”—wheneverpossible,we’re sorry somanyofyouhadtodiewhenwereproducedabittooexuberantly.Wetendedtobetheleadingcauseofhumandeathworldwide,infact.Butthen,yourspeciesalsoseemedtoreproducetoomuchandtherewerealwaysenoughofyoutoreinfect.Well,upuntiltheend,anyway.
You did spookus with that “magicbullet”thing,atleastforacoupledecades.Thoseantibioticsyoudiscoveredworkedvery well when they were new, didn’tthey?Oneof your famousdoctors, soonafter youdiscovered thosedrugs,opinedthat“theageofinfectiousdiseasesisover.”ButthankstobiologicaldiversityandthatDarwinguy’sdynamics,afewofustendedtosurvivewhateveryouthrewatus.Thoseluckyfewgottoreproducelike,well,rabbits(althoughweinfectedthoseothermammalstoo,whichhelpedusgetaround).Andasyousoonlearned,wefoundwaystopasstheantibioticresistancearoundlikeabasket-ball,evenwhenyourdrugsweren’tdirectly
involved.In2008youevencaughtuseatingthoseveryantibioticsforfood.Prettytricky,no?Butthanksforlunch.
Youhelpedusinsomeotherwaystoo.Welikedthewaysomeofyouhandedoutthe antibiotics evenwhen theyweren’treallyneeded.Iimagineitcouldbetoughtoresistthepressurefromdrugcompaniesandpatients,andsomeofyoudidandsomeofyoudidn’t.Thosecountrieswhere thedrugswerejustsolddirectlytoanyonewithasniffleoranitch,well, thatwasconve-nient(forustoo).Itwasespeciallyhelpfulwhenyouused,oh,about70percentofalltheantibioticsyouhadonthosefarmsandfeedlots.Usingjustenoughtoallowourveryfittestbrethrentothrivewaskindofyou.Whensomeofyoustoppedvaccinatingyourkids,wehadabigcelebration.Andwhenitbecametougherandtougherforyoutofindnewantibioticstotossatus,well,thegigwasup,sorry.
Our tricky littlecousins, theviruses,havehadaquiteagoodtimewithyouaswell. IknowthatHIVbug reallycausedhavocandmiseryandspookedyou.Sorry.Butofcoursethatwasjustthebeginning;therewassoonMRSA,needIremindyou,andmeanwhile, someofouroldbench-warmersliketuberculosisandotherswere
gearingupagain,nowmultiply-resistant,waitingfortherightconditions,whichtheydideventuallyfind.Asmorepeopleand communities and entire nationsslippedfurtherintopoverty,withdirtywater, tainted food,badair, crampedandcrowdedconditions,allmannerofinsectsandothermobileparasitesbreed-ingaway,well,forusitwaspartytime.Especiallywithyourricherpeopleflyingaroundeverywhereontheglobe,sharingtheairandsoforth.
For those who could afford it, youcertainly did come up with some veryimpressive treatments and technologies.Weenjoyedallthepredictionsabouthowother,morechronicproblemswereallgoingtobetakencareofeventually,whenmanywarningspointedtheotherway.Butthatkindofoptimisminyourkindwasalwayssortofendearing.
Someof youused to speculate thatonly cockroaches and microbes wouldsurviveyourpossibleself-inflictednuclearholocaust.Andasmanyof youbelievedinspaceshipsasdidinevolution.Butyourextinctioncamemorewithawhimperthanabang.We’llfigureouthowtobestdealwiththeroacheslater.Asforapostmortemdiagnosis,well, inhindsightwe’dhavetocallyourconditionHumanHubris.What’s“hubris”?Oh,c’mon;yousaddledsomanyofuswitholdLatinnames,youshouldbeabletofigurethisGreekoneoutonyourown.Imean,ifyouhadsurvivedit.
For related information, see www.k e e p a n t i b i o t i c s w o r k i n g . c o m a n d www.aware.md.
ReferenceDantasetal.BacteriaSurviveonAnti-
biotics.Science.2008;320:100-103
Bad Bugs Bite Back: A Cautionary Tale A Bacteria Looks Back at the Medical “Age of Miracles”
As told to Steve Heilig, MPH

28San FranciSco Medicinemay 2008 www.sfms.org
w henoneimagineswhatlifeintheyear2050willre-allybelike,theideathatthatwemighteachhaveahomerobotsimilarto“Rosie”onThe Jetsonsisnotthat
far-fetched.AsMorganQuigley,aPhDcandidateattheStanfordArtificialIntelligenceLaboratory,says,“wealreadyhaverobotsinourhomes—ourdishwashers,ourwashersanddryers,ouransweringmachines.Oncearobotcomesoutthatcancombinemultiplehomefunctions,that’swhenwe’llseeconsumersbuyingthemandhavingrobotsaspersonalhomeassistants.”
AtStanford,Quigleyisworkingaspartofateamtodevelopthetypeofrobotthatwillsomedayfunctionasahomeassistant.Currently,theteamhasSTAIR(StanfordArtificialIntelligenceRobot)IandII,tworobotsthatappeartobenothingmorethanroboticarmsonacartwithcamerasmountedtothetop.
WhileSTAIRIandIImaynotappearasonewouldthinkarobotshouldinaleadingacademicinstitution,“theabilitytomake
aphysicalcasingfortherobotthatismoreappealingalreadyexists,”saysQuigley.“Herewe’refocusingondevelopingthesoftware.”
Theseaestheticallysimpleone-andtwo-armrobotsprovidetheteamwitheverythingitneedstotheconductexperimentsthatleadtoimprovedprogramming.Insteadofaesthetics,thefocusisonteachingtheserobotstolearnandthinkindependently.
InordertotrainSTAIRIandIItorecognizeitems,theteamshowseachrobotmorethan200imagesofthesameobject,ratherthanprogramminginthespecificationsof,say,oneapple.Thehopeindoingsoisthattherobotswillbeabletodecideontheirownwhatmakesanappleanappleandapearapear.Inreal-lifesituations,wherethingsarenotnecessarilyofperfectdimensionsorarrangedinaspecificorder,havingabroaderideaofwhatconstitutesanapple,gainedfromhundredsofexamples,willmaketherobotsmorelikelytosuccessfullyidentifytheapple.
“Rightnowtherearerobotsworkinginfactories,”saysQuigley,
Back To THe FUTUreoF Medicine
Photos by Ashley SkabarText by Amanda DenzThe Future of AI
A Look at The Stanford Artificial Intelligence Program
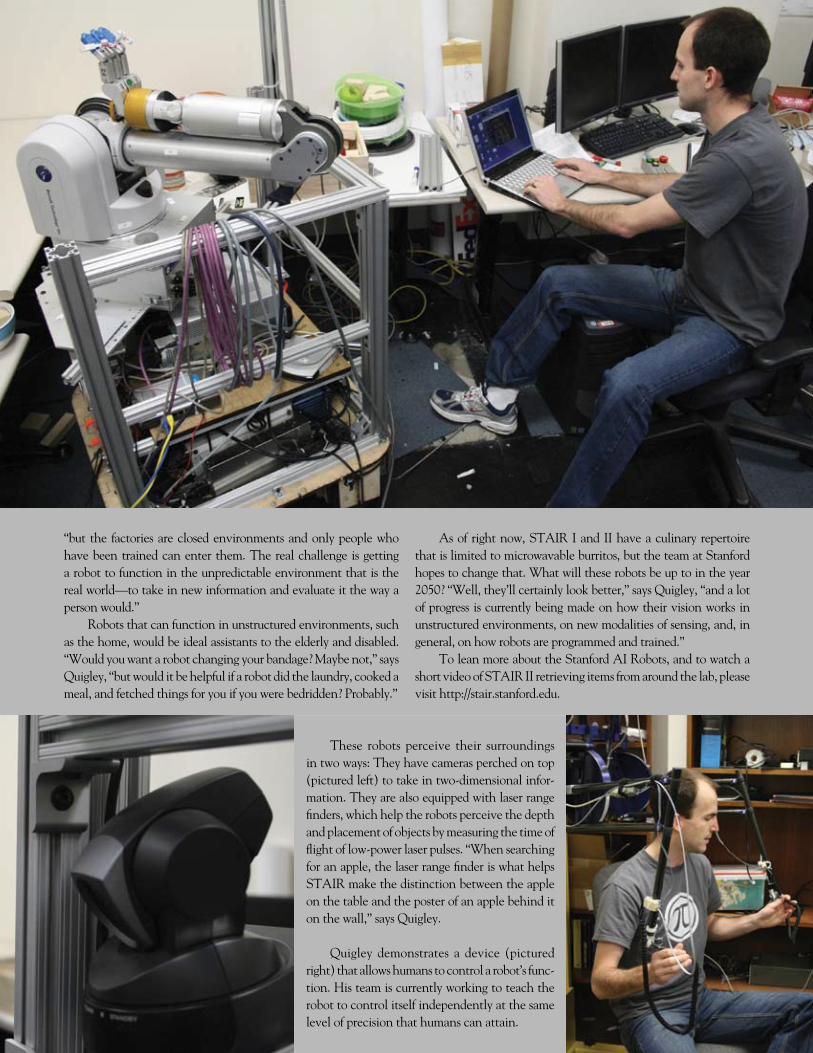
28San FranciSco Medicinemay 2008 www.sfms.org
“butthefactoriesareclosedenvironmentsandonlypeoplewhohavebeentrainedcanenterthem.Therealchallengeisgettingarobottofunctionintheunpredictableenvironmentthatistherealworld—totakeinnewinformationandevaluateitthewayapersonwould.”
Robotsthatcanfunctioninunstructuredenvironments,suchasthehome,wouldbeidealassistantstotheelderlyanddisabled.“Wouldyouwantarobotchangingyourbandage?Maybenot,”saysQuigley,“butwoulditbehelpfulifarobotdidthelaundry,cookedameal,andfetchedthingsforyouifyouwerebedridden?Probably.”
Asofrightnow,STAIRIandIIhaveaculinaryrepertoirethatislimitedtomicrowavableburritos,buttheteamatStanfordhopestochangethat.Whatwilltheserobotsbeuptointheyear2050?“Well,they’llcertainlylookbetter,”saysQuigley,“andalotofprogressiscurrentlybeingmadeonhowtheirvisionworksinunstructuredenvironments,onnewmodalitiesofsensing,and,ingeneral,onhowrobotsareprogrammedandtrained.”
ToleanmoreabouttheStanfordAIRobots,andtowatchashortvideoofSTAIRIIretrievingitemsfromaroundthelab,pleasevisithttp://stair.stanford.edu.
These robots perceive their surroundingsintwoways:Theyhavecamerasperchedontop(picturedleft)totakeintwo-dimensionalinfor-mation.Theyarealsoequippedwithlaserrangefinders,whichhelptherobotsperceivethedepthandplacementofobjectsbymeasuringthetimeofflightoflow-powerlaserpulses.“Whensearchingforanapple,thelaserrangefinderiswhathelpsSTAIRmakethedistinctionbetweentheappleonthetableandtheposterofanapplebehinditonthewall,”saysQuigley.
Quigley demonstrates a device (picturedright)thatallowshumanstocontrolarobot’sfunc-tion.Histeamiscurrentlyworkingtoteachtherobottocontrolitselfindependentlyatthesamelevelofprecisionthathumanscanattain.
Richard E. Anderson, MD, FACPChairman and CEO, The Doctors Company
We proudly announce our 2008 member dividend. We set a higher standard. We ensure that members benefit from our strength. We embrace opportunities to recognize and reward physicians. We exceed expectations. We offer tangible benefits to those who join us. We stand behind the promises we make. We are The Doctors Company.
We are on a mission to relentlessly defend, protect, and reward doctors who advance the practice of good medicine. We
act with single-minded determination to reward our members and to ensure that they share in the company’s financial
strength. In 2007, our members received a dividend of between 5 and 7.5 percent. For 2008, our members will receive
a dividend distribution at the same level. That’s $44 million returned to members in two years. To learn more about our
medical professional liability program, call The Doctors Insurance Agency at (415) 506-3030 or (800) 553-9293. You can
also visit us online at www.doctorsagency.com.
A2254_SFMedicine.indd 1 4/4/08 4:16:43 PM

www.sfms.org may 2008San FranciSco Medicine�1
computer-assisted and Positron emission Tomography
PET/CT,incombinationwithmolecularimaging, provides a method by whichabnormalities lightup indifferentcolorsto indicatevariouskindsofpathology—lymphomatous nodes are designated inpurple,neuroendocrine tumors inorange,metastaticdiseaseinred,andinflammationingreen. Degenerativebraindiseaseisreadilydifferentiatedbythis typeof imaging,andresponsetotherapyisindicatedbychanges
inthemolecularmakeupreadilyseenintheimagery.
For CT and MRI, sequences havebeenrefinedsothatcontrastagentsarenotrequiredtoget superb images, resulting inremarkablyreducedradiationforwhole-bodyscanning.
Oncologicradiologicreferralsarenowmore focused, since geneticprofiles andmolecularmarkersmakeinitialworkupmorespecificas tothe imagingneeded.Withadiagnosis,targeteddrugscanthenbedirectedtotreatment.
current Status of Biomedical im-aging diagnostic and Therapeutic Procedures
Currently,radiationtherapyisdeliveredwithroboticscombinedwithCTscanstopinpoint the radiationfieldprecisely,dif-ferentiatingthetissuetobetreatedfromthenormaltissuetobespared.
CardiacMRIandCTAhavereplacedcardiac catheterizations for imaging theheart.
RoutinegastrointestinalstudiesofupperGIandbariumenemashavebeencompletelysupplantedbycross-sectionalimaging.
Virtualcolonoscopyhasreplacedendos-copyforthediagnosisofcoloncancer,andinterventional radiol-ogyisusedtotreatthepolypoidcolonmassesbyembolization.
Vascular surgeryhas been largely sup-planted by interven-tional radiologic tech-niquesofstenting,laser-directedandradio-fre-quency(RF)ablationsof tumors and veins,embolizations, andatherectomies. Otherinterventional tech-niques such as verte-broplastieshavelargelyreplacedmanysurgicalproceduresofyore.
NanotechnologyhasvirtuallytransformedtheX-rayofold.Today’stechnology is capableofgeneratingelectrons
ing themind-bodyentity.Treatmentofmentalillnessisconsideredpartofstandardhealthcare,whichisunderstoodasaprior-ityforall.
Erica’streatment,aidedbytechnologicdevicesthatallowherteamtobeincloseconnection, is reviewedmonthlyby theentiretreatmentteam,includingEricaandherparents.Althoughtherearemanydiffer-encesin2050,thecoreofpsychotherapeutictreatmentremainsthesame: thedevelop-mentofa strongtherapeuticallianceandarelationshipthatsupportschangeforthepatientandherfamily.
Lynn Ponton, MD, grew up in Wisconsin and received her BA from the University of Wis-consin, Madison. After graduating, she worked at the Pasteur Institute in Paris before returning to the University of Wisconsin, Madison, to obtain her MD. She worked as an intern in pediatrics and completed two residencies in adult psychiatry. After finishing her work as a fellow in child and adolescent psychiatry in 1983, she began her training at the San Francisco Psycho-analytic Institute and joined the faculty at UCSF. Besides working as a professor of psychiatry, Dr. Ponton is also a practicing psychiatrist and psychoanalyst, as well as the author of TheRomanceofRisk:WhyTeenagersDotheThingsTheyDo and TheSexLivesofTeenagers:RevealingtheSecretWorldofAdolescentBoysandGirls. In her practice she works primarily with adolescents.The mother of two young-adult daughters, Dr. Ponton lives in San Francisco.
The width is 3.5 by 4” highCALL Kae with any questions or concerns 415-567-5888
Fusion Diagnostic Group’s advanced technology and software bring evaluation and measurementtools to the Physician to use in the clinical setting.we also have a full time physician on staff.
High Resolution PET/CT scans
Mon - Saturday 8-5 + (flexible hours with advance request)
Positron Emission Tomography (PET)Computed Tomography (CT)
Molecular / Functional ImagingAccurate & Precise Imaging
1700 California St. #260California at Van Ness in San Francisco, CA(415) 921-7226 • 1 (800) 334-0336 • (415) 921-7225 FAXwww.fdg-inc.net
atroomtemperaturethatareexcitedbyanelectricalfield,whichcanproduce imagesfromvariousanglesandperspectiveswithoutrotatingtheimagingdevice.
Serviceformalfunctionsisdoneon-sitebyoff-sitecomputersthatmakethediagnosisandprovidethesolution.
In past decades, radiologists wouldseehuge tumors,pseudocysts,andmassesthatwereexceedinglydifficultand time-consumingtodiagnoseandtreat.Asimagingbecamemoreprevalent,efficient,andprecise,wediscoveredthesespace-occupyinglesionsearlierandwhentheyweremuchsmaller,potentiallymoreamenabletotreatment.
With molecular imaging becomingmuchmoresophisticated,wearemorelikelytodealwithmicroscopicratherthanmac-roscopicdisease.Thuswecantreatdiseasemuchsoonerandwithgreatersuccess,andwecanprovideamuchwiderrangeofminimallyinvasiveprocedures.Whoknowswhatthefuturemaybring?
Gretchen A. W. Gooding, MD, is Profes-sor in Residence, Department of Radiology and Biomedical Imaging, University of California, San Francisco, and she serves on the Editorial Board of SanFranciscoMedicine.
Psychiatric MomentsContinued from Page 25...
Biomedical ImagingContinued from Page 23...

�2San FranciSco Medicinemay 2008 www.sfms.org�2San FranciSco Medicinemay 2008 www.sfms.org
KPSFRobert Mithun, MD
SaintFrancisWade Aubry, MD
St.Luke’sJerome Franz, MD
Fast-forwardingforty-twoyears,thefieldofmedicinewillseerevolutionarygenetic,biomedi-cal,andtechnologicaladvances.
Newbornswillhavegeneticprofiles en-ablingus toanticipateanynecessarymedicalinterventions.Inlightofthisinformation,wewillcreateindividualizedhealth-maintenanceroadmaps;anysubsequenthealthconcernsrequiringpharmaceuticalsortreatmentswillbetailoredtoanindividual’sgeneticblueprintimplications.
Themedicalsystemwillsupportlife’sstagesofbirth,growing,aging,anddeathasnaturalevents,notbillable codesordiagnoses. Indi-vidualswillbemembersoftheirownhealthcareteams,whichwillprovidedignity,compassion,andempowerment throughout life’s journey.Maintaininghealthwillbeapartofdaily lifeashealthcarewillpartnerwithschools,com-munities,andemployers.Virtualaccesstoafullyintegratedinterdisciplinaryhealthcareteamwillbethenormforeverymemberofsociety.
Asneeded,patientswillaccesslocaltele-medicinediagnosticsuites,whichuseminimallyintrusivetestingmethods,andthedatawillbetransmittedtohealthcareteamstoreview.Oncediagnosed,patientswill go to specializedcarecenters,suchascardiovascularorsportsmedicinecenters, with radically less invasive medicalinterventions.Theywillreceivefollow-upcarethroughouttheirrehabilitationprocesses.
Mammothleapsintechnology,withreq-uisiteprivacyandsecurity,willallowpeopletokeeptheirrelationshipswithhealthteamsovertimeandlocation.Withadvancedcommunica-tionsystemsandinstantaccesstopeople’sfullmedicalstories,healthcareteamswillfocusonhealingandcompassionatetreatment.
KaiserPermanente’scurrentcommitmentto the future vision of universal preventivehealth,virtualaccess,integration,andtechnol-ogyisguidingusbacktoourcoremission:helpingpeoplethrive.
AtSaintFrancisMemorialHospital,werecently had the chance to experience thefutureofrehabilitationinourSportsMedicineCenter,whichconductedamonthlongtrialoftheG-TrainerAnti-GravityTreadmill.ThemachineallowspatientstoexerciseatafractionoftheirbodyweightandwasrecentlyclearedbytheFDAforuse inmedicalapplications.Thetreadmillmaybeausefultoolforpatientsreha-bilitatingafterinjuryorsurgery,allowingthemtobuildstrengthandrangeofmotionataverylowimpacttothebody.Themachine’sgravitydifferentialtechnologywasoriginallydevelopedatNASA.Itusesanadvancedair-pressuresystemthatcreatesaliftingforcewithan“unweighting”effect.Theresultissimilartotheweightlessnessachieved in a pool, butwithout the limitedrangeofmotion.Hospitalsthathaveusedthemachinereportfasterrecoverytimesandlowertreatmentcosts.
We’realsoproudtoannouncethatSaintFrancis recentlyearned theGoldSealofAp-provalfromtheJointCommissionforPrimaryStrokeafteranextensiveon-siteJCAHOreview.Thesealrecognizescentersthatcanquicklydiag-nosestrokes,tailortreatmentplans,andanalyzedatatoimprovecareforfuturecases.I’mthankfultoeveryonewhoworkedsohardtomakethishappen,includingphysicianleadersCarlosQuin-tana,MD;MarcusZachary,MD;KeithLoring,MD;andFernandoMiranda,MD;aswellasstaffmembersAlyHemphill,CeliaRyan,GloriaLau,CherieVolk,LauraGutierrez,TheresaEdison,TomPanaccione,andJudithBolker.
Kudos toorthopaedic surgeonsThomasSampson, MD, and Elly LaRoque, MD, fortheirparticipationaspresentersat the recentAmericanAcademyofOrthopaedicSurgeonsinMarch.
2050 isbeyondanyexpectations Ihaveformyself,butIhaveexperiencedthechangesinthedeliveryofmedicalareoverjustsuchascopeofyears.
WhethertherewillbeaSt.Luke’sHospitalin2050hasbeenindoubtforyears,startingwiththeincreasingdeficitsofthe1990s.Theaffilia-tionwithSutterin2001broughtnewhopethattheinstitutionwouldbecomemorefinanciallysound throughbettermanagement.However,the losses only increased over the next fiveyears,andSutter,despairing, turned the reinsovertoCPMC.
CPMCwasinthemiddleofplanninghowtomeeta2013deadlinefortheseismicretrofit-tingof its threecampuses.Fromtheir side, itseemed reasonable tomoveacutecareatSt.Luke’s to theplannednewmedical centeratCathedralHill.TheydidnotexpecttheoutcrythisproposalbroughtfromtheSouthofMarketcommunitiesthatdependedonSt.Luke’sastheonlyprivatehospitalinthearea.NordidCPMCanticipatethattheDepartmentofPublicHealthwouldopposetheeffectiveclosingofSt.Luke’semergencyroom,whichhasbeenimportantasareliefvalveforSanFranciscoGeneralHospital.EnterSupervisorAlioto-Pier,who listened tooursupporters.AlongwithMitchKatz,andwiththewholeheartedcooperationofCPMC, sheestablishedaBlueRibbonPaneltoevaluatetheroleCPMCistoplayinthecitywidedeliveryofhealthcareservices—whatisneededandwhere.Thegroup iscomposedofdistinguished lead-ers fromcommunityorganizations, thehealthcarefield,and theunions.Theircharter is todeterminetheformofacutecareservicesatSt.Luke’sbeyond2013,notwhethersuchserviceswillexist.
By the time this column isprinted, thepanelwillhavemet three times. Its report totheCPMCBoardisdueJune30.Iwillsavemyspeculationsabout2050untilthen.
HoSPiTaL neWS

�2San FranciSco Medicinemay 2008 www.sfms.org www.sfms.org may 2008 San FranciSco Medicine���2San FranciSco Medicinemay 2008 www.sfms.org
St.Mary’sRichard Podolin, MD
VeteransDiana Nicoll, MD,
PhD, MPA
UCSFRonald Miller, MD
Patients at St. Mary’s Medical Center(SMMC)AcuteRehabilitationUnitarebuild-ingendurance, strength,andcoordinationbyusingthepopularvideogamesystemNintendoWii.KnownasWii-habilitation,thisnewformofphysical therapy ishelping inpatientsmeetrehabilitation goals using a fun, interactivetechnique.
“Wii-habilitation is a freshapproach tophysicalandcognitiverehabtherapy,”saysDr.MarcWakasa,medicaldirectorof theAcuteRehabilitationUnitatSMMC.
Wii-habilitationisusedtomovethebodyinwayssimilartotraditionaltherapyexercises.TheNintendoWiiusesawirelesscontrollertodirecttheactionsofanimatedathletesonscreen.TheWii’s interactive formathelps inpatientsrecoveringfromstrokes,spinalinjuries,brokenbones, and surgery.Patientsuse the skill setsassociatedwithsportstorebuildlostskillsandimproveconcentrationandphysicalfunctions.Currently,SMMCoffersWii-habilitationvideogamesfortennis,ping-pong,andbowling.
TheprogramwaspioneeredanddevelopedbyDr.JustinLiu,chairofbackandtraumareha-bilitationatSMMC.AccordingtoDr.Liu,“Intoday’sworldofconstantinnovation,itisonlynaturalthatweusecutting-edgetechnologytopush the envelopeof physical rehabilitationwhilemakingtheoverallprocessmoreexcitingandfun.”
Wii-habilitationisacost-effectiveprogram,totaling $1,300 for equipment and setup.Comparedtotraditionalhospitalgymequipment,this is significantly more economical andspace-efficient.This innovationcontinuesthehospital’straditionofadvancedmedicalcare.
TheAcuteRehabilitationUnitspecializesinstrokerehabilitation,spinalcordinjury,headinjury, and general rehabilitation. For moreinformationonWii-habilitationatSMMC,call(415)750-5933.
UCSFMedicalCenterhasdramaticplansfor the futureofmedicineandhealthcare intheBayArea.Acampaignisalreadyunderwaytobuildanewcomplexof specialtyhospitalsforchildren,women,andcancerpatientsona14.5-acreparcelof landattheUCSFMissionBayCampus.
ThecomplexwillnearlydoubletheMedi-calCenter’scurrentcapacity,whilecreatingaworld-classand family-centeredhealingenvi-ronment.ItslocationatMissionBaywillfoster“translationalresearch,”usingknowledgegainedinthelaboratorytodirectlybenefitpatients.ItalsooffersanopportunitytoexpandtheclinicalprogramsthatwillbebasedinthecurrentMedi-calCenteratParnassusHeights,byfreeingupandrevitalizingmuch-neededspaceforexpan-sionofworld-classprogramssuchasneurosurgery,cardiology,andtransplantsurgery.
TheplannedcomplexiscriticaltoUCSF’sabilitytoprovidethequaternaryandtertiarycareonwhich itspatientsdepend.UCSFMedicalCenter is the smallestof thenation’s top tenmedicalcenters,andithasbeenoperatingatfullcapacityforyears.Inthepastsixyearsalone,theaveragedailyhospitalcensushasrisen25percenttomorethan500patientsperday,withoutspacetoexpand.
Oncompletionofthefirstphasein2014,thenewcomplexwill includea183-bedchil-dren’shospitalwithurgent/emergencycareandpediatricprimaryandspecialtyfacilities;a36-bedwomen’shospitalwithabirthcenter,cancercare,specialty surgery,and selectwomen’s services;anda70-bedadultcancerhospital.
Planscall for the facility tomeetLEEDenvironmental standards, includinga reducedenergyfootprint,naturallightthroughout,androoftopgardensforpatientsandtheirfamilies.Italsowilluseevidence-baseddesigntosupportabuiltenvironment thatcanpositivelyaffecthealing,health,safety,andwell-being.
V.A.healthcareofthefuturewillbemoreinnovative, designed tomeet theneeds andexpectationsofanewgenerationofveterans,whilealso focusingonprevention, treatment,andmanagementofdiseases sufferedbyolderveterans.
Tomeetthesechallenges, theSanFran-ciscoV.A.MedicalCenterhasplanstoexpanditscommunity-basedoutpatientclinicslocatedinSantaRosaandUkiah,aswellastodevelopanewclinicinLakeCounty.
WehavehadgreatsuccesswithourOEF/OIFIntegratedCareClinic,whichexemplifiesanewmodelofhealthcareforreturningcombatveterans that integratesprimarycare,mentalhealthcare,andsocialworkwithinoneclinicalsetting.Wearenowexpandingthisinnovativeconcept and integratingprimary andmentalhealthcarethroughoutallofourprimarycareclinics.
WearewellintotheprojecttoexpandourEmergencyDepartment.Oncecompleted,thisnewstate-of-the-artdepartmentwillhavetwelveacute-carebedsaswellasimprovedpatientpri-vacy,nursingworkandwaitingareas,andbuilt-inoutdoordecontaminationshowers.
Ourtelehealthprogramcontinuestogrow,particularlyinourcommunity-basedoutpatientclinics.Telehealth involves theuseofvideo,digitalpictures,andmessagingdevicestotreatpatientswhomaybehundredsofmiles fromthemedical center.Wehave also expandedintotheareaoftelementalhealth,whichallowsus to increaseaccess ingeographically remoteareaswherenomentalhealthservicescurrentlyexist.
TheHome-BasedPrimaryCareprogramwillplaya significant role in the future.Thisoffersprimaryhealthcareinthehome,withthegoalofhelpingveteransavoidhospitalizationsandassistingthemandtheircaregiversinpre-ventingprematurenursing-homeplacement.
HoSPiTaL neWS

And the state’s first health benefits company suddenly became its youngest one with a fresh attitude and renewed commitment. A renewed commitment to improving the health of all Californians. This is a formative time in American health care. Expect Anthem Blue Cross, an old friend with a new name, to lead the way.
Welcome to Anthem Blue Cross, California’s oldest and newest health benefits company.
On April 1, 2008, Blue Cross of California became Anthem Blue Cross.
Anthem Blue Cross is the trade name of Blue Cross of California. Independent Licensee of the Blue Cross Association. ® ANTHEM is a registered trademark. ® The Blue Cross name and symbol are registered marks of the Blue Cross Association.
6148_PCAAD2601C_3_08_name_change_announcement ver1.indd 1 3/21/08 1:50:32 PM
in MeMoriaMNancy Thomson, MD
aubrey W. Metcalf, MdAubreyW.Metcalf,MD,diedofcancer,December7,2007,
age76.HewasborninLosAngelesonSeptember3,1931.Heat-tendedUCLAandthenbeganmedicalschoolinAustria,thoughistimetherewasinterruptedwhileheservedintheKoreanWar.Hegraduated fromU.C.Berkeleyandfinishedmedical schoolatUCSFin1958.Heandhisbride,Beverly,livedinFranceandAustria,wheretheyhadtheirfirstchild,Franz,beforereturningtoUCSFforhisresidencyinpsychiatry.
Dr.MetcalfusedtosayheusedhisprivateofficeinWestPortaltofinancehis“teachinghabit.”AsaprofessorofpsychiatryatUCSF,hisvisionexpandedasthosehesupervisedandmentoredcarrieditforward.Oneofthefirstpsychiatriststoembraceattachmenttheory,heencourageditsnewthinkers.Hesincerelycaredforhispatientsandhiscolleagues.Heeverchampionedthepsychotherapeuticrelationship,despitethefield’sincreasingrelianceondrugs.HewasawardedalifetimeachievementawardfromtheRegionalOrganiza-tionofChildandAdolescentPsychiatry(ROCAP),citinghis“outstandingservicetohisprofession, students,andpatients.”ROCAPisnowcreatinganannualawardinhisnametobegiventodeservingmedicalstudents.Hiscross-disciplinaryworkalsoenrichedhisandBeverly’ssupportoftheMultidisciplinaryAssociationofClinicalEducators(MACE)andtheAssociationofEducationalTherapists(AET).HebecameamemberoftheSanFranciscoMedicalSocietyandtheAMAin1965.
Heenjoyedlifeasdofewothers,andhesharedhispassion forfishing, camping,poetrywriting, andbookannotatingwithfriendsandfamily.Heissurvivedbyhiswife,Beverly;his son,Franz (NinaRuscio);daughter,Heidi (MichaelCooperman);andgranddaughter,PearlMetcalf.
Sanford e. Feldman, MdDr.SanfordE.Feldman,apastpresidentoftheSan
FranciscoMedicalSociety(1969),diedathishome inSantaFe,NewMexico,February4,2008,fromamelanomaoriginatingonhisscalp.Hewas93.HewasbornApril20,1914,andwasalongtimeresidentofSanFranciscoandMillValleybeforemovingtoSantaFe.
HewenttoStanfordUniversityasanundergraduateandreceivedhisMDfromStanfordin1938.Althoughhewasinprivatepracticeasasurgeon,hehadalifelonginterest in scienceand for yearsdidbasic researchonfoodandwaterintakewithDr.SamuelLepkovskyattheUniversityofCaliforniaatBerkeley.AfterservinginthemilitaryduringWorldWarII,hejoinedtheSanFranciscoMedicalSocietyin1948.HewasalsoactiveintheCalifor-niaMedicalAssociationandapioneerintheareaofpeer
review.HewasfounderandfirstdirectoroftheSanFranciscoPeerReviewOrganizationandbecamedirectoroftheCaliforniaPeerReviewOrganization.Afterretirementfromsurgery,Dr.Feldmancontinuedtoworkfortheimprovementofpatientcare.Hewasanexpertinqualitycareathospitalsandwroteaboutphysicianandhospitalerrorforvariousmedicaljournals.
Heissurvivedbyhiswife,Dr.LouiseTaichert,achild/familypsychiatrist;twosons,David(Linda)ofCoronado,California,andJohn(Carol)ofAlbuquerque;twodaughters,WendyFeldmanofAlbuquerqueandLaurieFeldman(SaverioSantoliquido)ofTorino,Italy;andtwogranddaughters.

New Discount Announcedfor Workers’ CompensationInsurance! For SFMS Members!
E X T R A !
Sponsored by: Administered by:Underwritten by:
© 2008 Seabury & Smith Insurance Program Management • CA License #0633005 • 4/08777 South Figueroa Street, Los Angeles, CA 90017 • 800-842-3761 • [email protected]
Marsh is part of the family of MMC companies, including Kroll, Guy Carpenter, Mercer, and the Oliver Wyman Group (including Lippincott and NERA Economic Consulting).
We are pleased to announce a new enhancement tothe sponsored San Francisco Medical Society /CMAWorkers’ Compensation program, underwritten byEmployers Compensation Insurance Company (rated“A -” by A.M. Best Company). Members are now eligibleto receive a rate of $1.13 per $100 of annual payroll.
Following are some highlights of the Employersprogram:
• Employers will provide a member credit on newand renewal policies of SFMS members.
• Employers will provide members insured with BlueCross on a group (2 – 250 employees) basis anadditional discount on their workers’ compensationpremium.
• This program is available to members only throughSeabury & Smith Insurance Program Management(Marsh).
Workers’ Compensation insurance is required by lawand covers your employees in the event of a job-relatedinjury. Coverage is standardized by statelaw and includes hospital and medicalexpenses, work-related disabilityincome and a death benefit.
For more information and a premiumindication, please call a Marsh ClientService Representative at 800-842-3761,or go to www.MarshAffinity.com/pages/cmadownload.html todownload a premium indicationrequest form.
See how much you could be saving onWorkers’ CompensationInsurance!
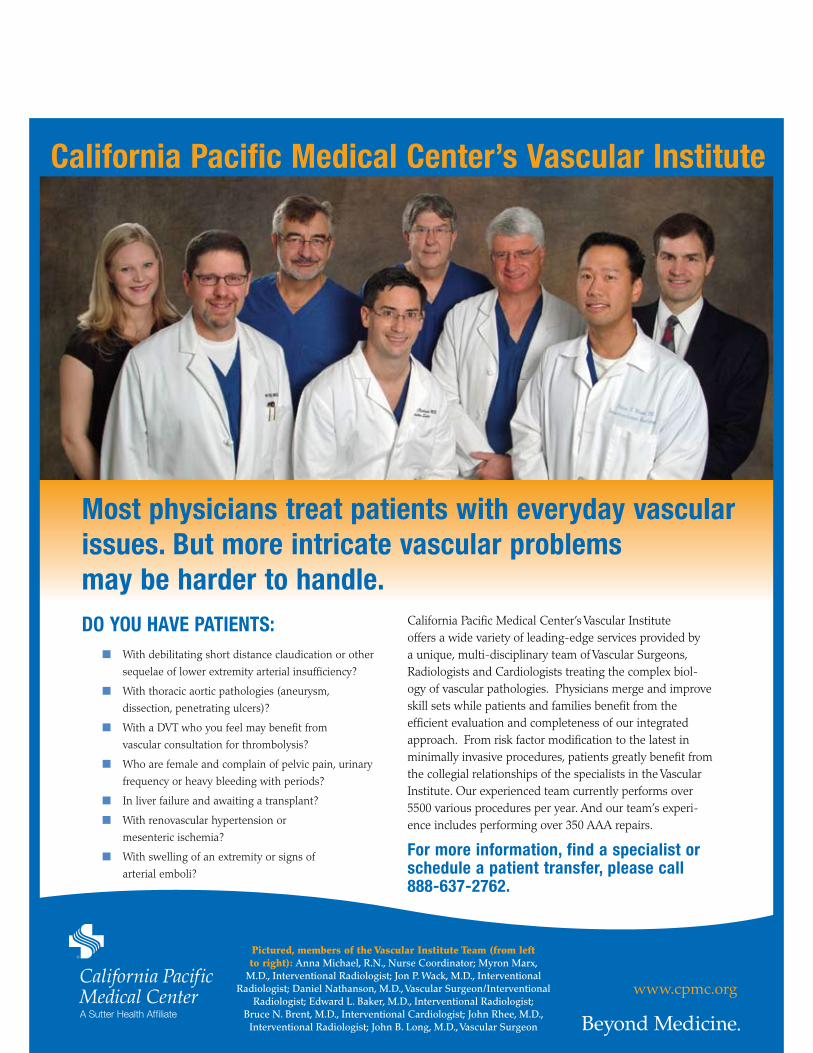
www.cpmc.org
Do you have patients:With debilitating short distance claudication or other
sequelae of lower extremity arterial insufficiency?
With thoracic aortic pathologies (aneurysm,
dissection, penetrating ulcers)?
With a DVT who you feel may benefit from
vascular consultation for thrombolysis?
Who are female and complain of pelvic pain, urinary
frequency or heavy bleeding with periods?
In liver failure and awaiting a transplant?
With renovascular hypertension or
mesenteric ischemia?
With swelling of an extremity or signs of
arterial emboli?
California Pacific Medical Center’s Vascular Institute offers a wide variety of leading-edge services provided by a unique, multi-disciplinary team of Vascular Surgeons, Radiologists and Cardiologists treating the complex biol-ogy of vascular pathologies. Physicians merge and improve skill sets while patients and families benefit from the efficient evaluation and completeness of our integrated approach. From risk factor modification to the latest in minimally invasive procedures, patients greatly benefit from the collegial relationships of the specialists in the Vascular Institute. Our experienced team currently performs over 5500 various procedures per year. And our team’s experi-ence includes performing over 350 AAA repairs.
For more information, find a specialist or schedule a patient transfer, please call 888-637-2762.
Most physicians treat patients with everyday vascular issues. But more intricate vascular problems may be harder to handle.
California pacific Medical Center’s vascular institute
Pictured, members of the Vascular Institute Team (from left to right): Anna Michael, R.N., Nurse Coordinator; Myron Marx,
M.D., Interventional Radiologist; Jon P. Wack, M.D., Interventional Radiologist; Daniel Nathanson, M.D., Vascular Surgeon/Interventional
Radiologist; Edward L. Baker, M.D., Interventional Radiologist; Bruce N. Brent, M.D., Interventional Cardiologist; John Rhee, M.D.,
Interventional Radiologist; John B. Long, M.D., Vascular Surgeon
SF 8 x 10.indd 1 2/29/08 9:59:46 AM

















