Matt Campbell MD, MS Assistant Professor · •Amado Zuria-Saavedra •Research GU Med Oncology...
63
Transcript of Matt Campbell MD, MS Assistant Professor · •Amado Zuria-Saavedra •Research GU Med Oncology...


Matt Campbell MD, MSAssistant Professor
Department GU Medical [email protected]
Systemic Treatment for bladder cancer 2018

Disclosures:
• Advisory Board: Eisai, AstraZeneca, EMD Sereno, Pfizer, Genentech
• Consulting: Eisai, AstraZeneca, EMD Sereno, Pfizer, Genentech

Objectives
• Quick Overview of Anatomy
• Catching up on era prior to Immuno-Oncology (IO) in Urothelial Cancer
• Immune Checkpoint therapy Overview
• Post cisplatin space and cisplatin ineligible space for unresectable and metastatic disease
• Discuss the challenges of using programmed death ligand staining in selecting patients for immune therapy
• Highlight future potential of molecular signatures to help select patients for immunotherapy
• Future Areas of Exploration

Understanding Urothelial Anatomy
National Cancer Institutehttps://www.cancer.gov/images/cdr/live/CDR765031.jpg
90%
10%

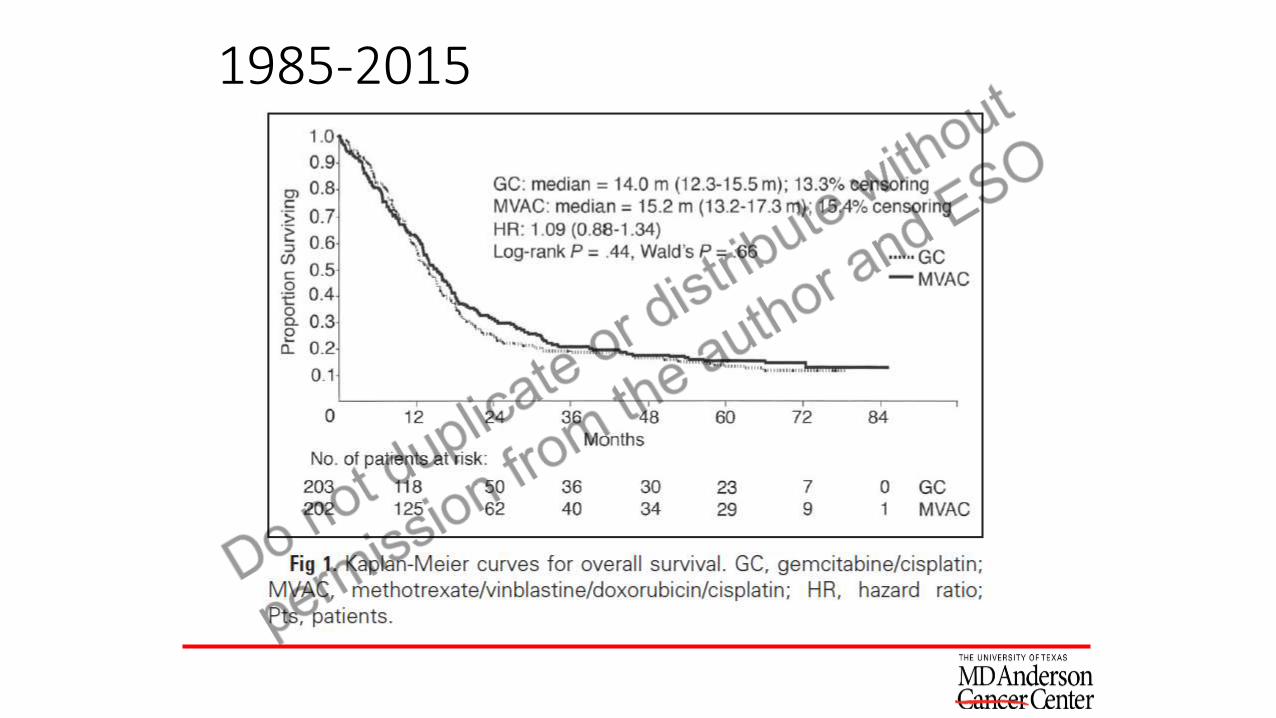
1985-2015

1985-2015

Complete responders do better
Grossman et al. NEJM 349;9: 859-866, 2003.
1985-2015


Standard NAC/Adjuvant/Front Line Metastatic Therapy

How do patients do that are unfit for cisplatin chemotherapy?
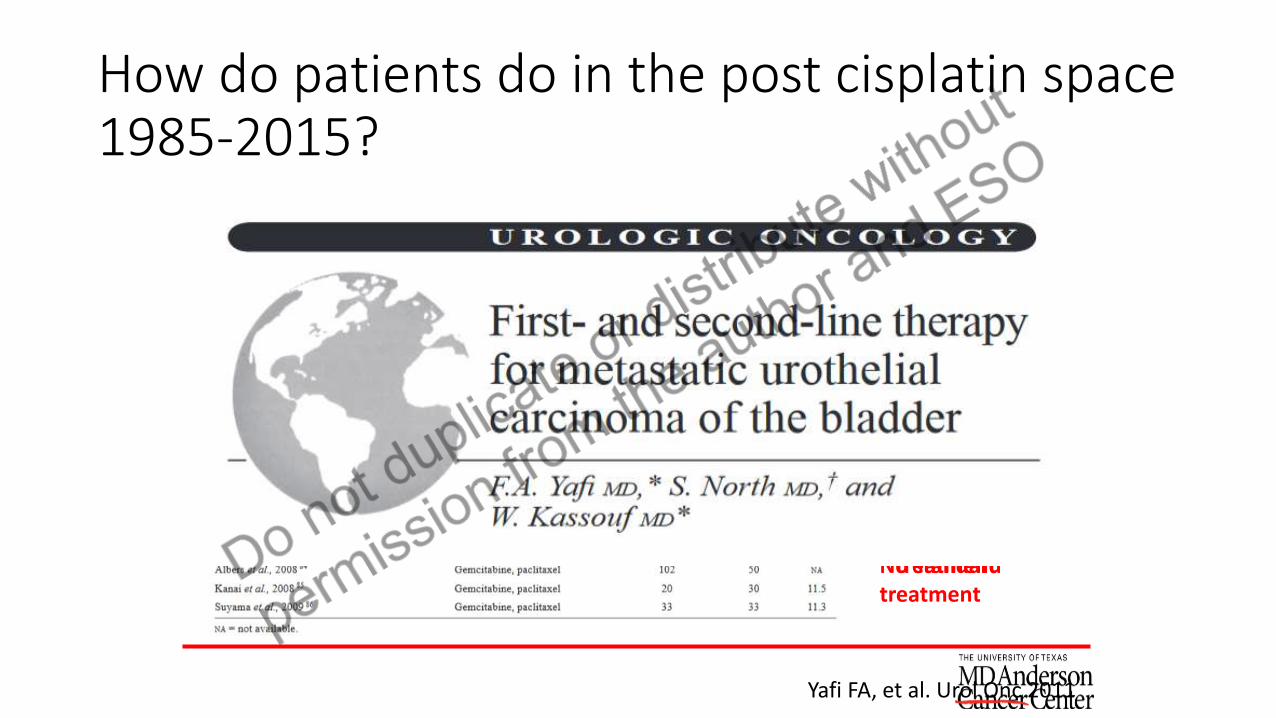
How do patients do in the post cisplatin space 1985-2015?
Single agent:
Response rate considered ~ 10%
Durable responses rare
No standard treatment
Combinations
More toxic
Fewer eligible patients
Small trials
No standard treatment
Yafi FA, et al. Urol Onc 2011

To understand immune checkpoint data it is important to understand the era of chemotherapy only

Quick Summary 1985-2015
• 3 decades of work by many dedicated oncologists, urologists, radiation oncologists…
• Cisplatin based chemotherapy followed by cystectomy SOC muscle invasive resectable patients
• Cystectomy SOC in muscle invasive disease in cisplatin ineligible population
• Cisplatin with ddMVAC or Gem+Cis based chemotherapy is standard in unresectable/metastatic setting
• No second line therapy existed

Immune Checkpoint Blockade Simplified
Pardoll D, Nature 2012


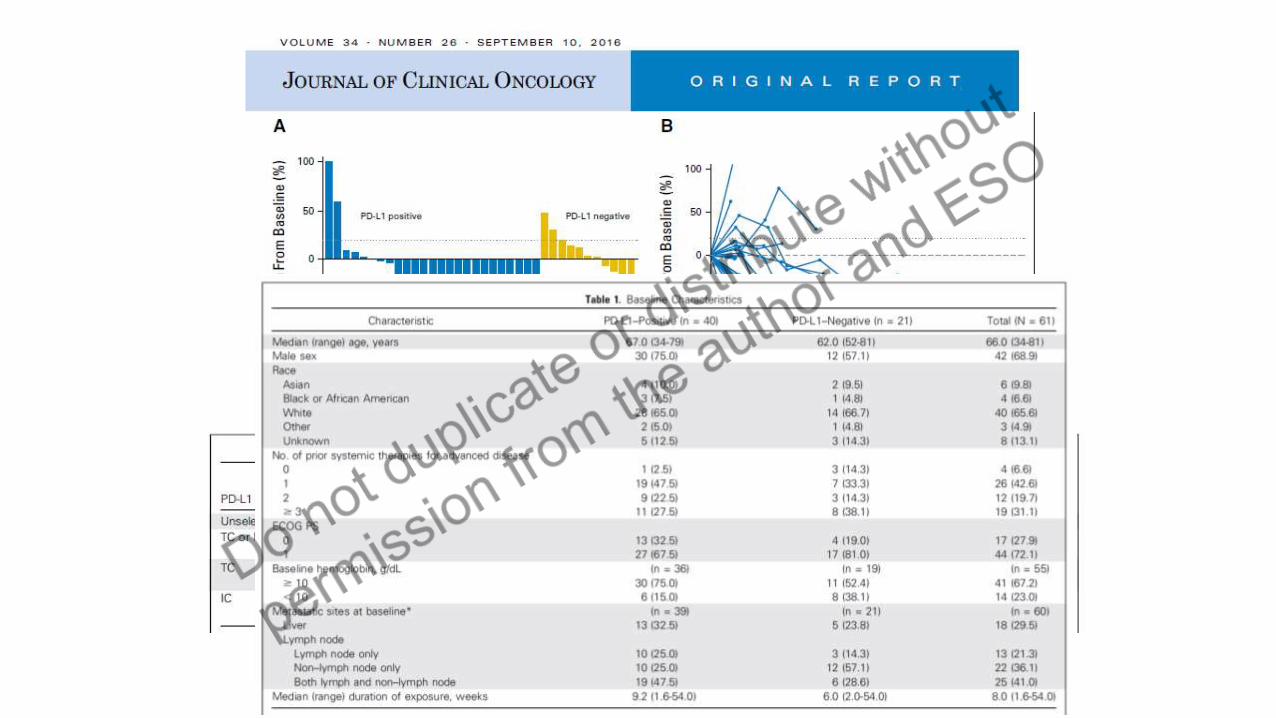
Another way to Look at PD-L1


Rosenberg J, et al. Lancet Oncol 2016

Adverse Events
Rosenberg J, et al. Lancet Oncol 2016

Rosenberg J, et al. Lancet Oncol 2016



Adverse Event Profile Slightly Different
Apolo AB, et al. JCO 2017

Lancet 2017; 398: 67-76
PD-L staining IC not important now???
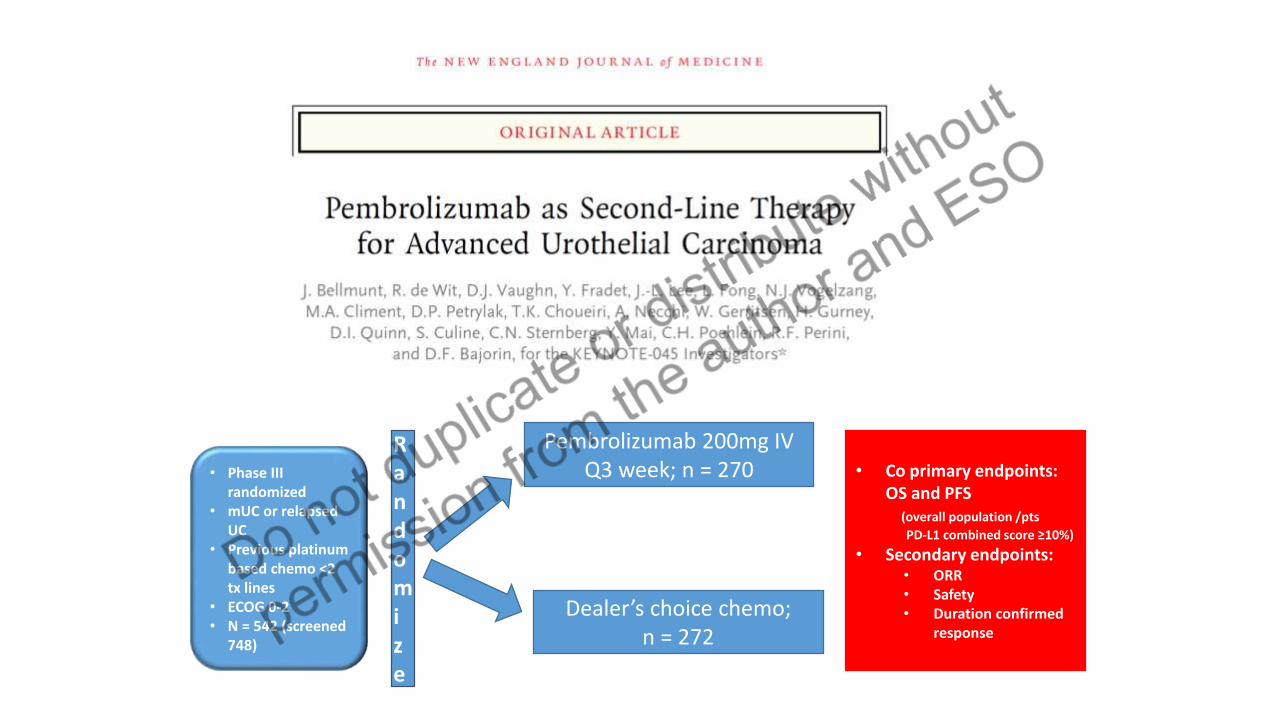
Randomize
• Phase III randomized
• mUC or relapsed UC
• Previous platinum based chemo <2 tx lines
• ECOG 0-2• N = 542 (screened
748)
Pembrolizumab 200mg IV Q3 week; n = 270
Dealer’s choice chemo; n = 272
• Co primary endpoints: OS and PFS
(overall population /pts
PD-L1 combined score ≥10%)
• Secondary endpoints:• ORR• Safety• Duration confirmed
response

Bellmunt J. et al. NEJM epub 2/17/17

Bellmunt J. et al. NEJM epub 2/17/17

Sub-group analysis were surprising
PD-L positive patients did worse in both groups (negative prognostic marker not predictive!)

Not All Responses Were Durable!
Bellmunt J. et al. NEJM epub 2/17/17

Excellent Side Effect Profile As Expected
Bellmunt J. et al. NEJM epub 2/17/17

Atezolizumab versus chemotherapy as a Second-line Therapy in Advanced UC IMvigor211 Study Design
Key Eligibility Criteria
• Urothelial carcinoma of the renal pelvis, ureter, bladder, or urethra
• Transitional cell predominant
• PD after 1-2 lines of platinum-based chemo or recurrence within 12 mo of perioperative platinum-based therapy
• ECOG PS 0-1
• Provision of tumor sample for biomarker assessment
Atezolizumab 1200 mg IV Q3W
for 2 years
SOCPaclitaxel 175 mg/m2 Q3W
ORDocetaxel 75 mg/m2 Q3W
ORVinflunine 320 mg/m2
Q3W
R (1:1)N = 931
Key EndpointsPrimary: OSSecondary: ORR, PFS and DOR in totalTwo sided alpha 0.05, 97% Power ITT HR 0.74, IC1/2/3
subgroup HR 0.68, IC 2/3 subgroup HR 0.57
RequirementsAt least 230 pts IC2/3, at least 537 pts IC1,2,3 status
N = 467
N = 464
Stratification Factors
• PD-L1 expression• Chemotherapy type (vinflunine vs
taxanes)• Liver metastases (yes vs no)• Number of prognostic factors
(none vs 1, 2 or 3)(time from chemo<3 vs ≥3 mo, PS≥1, Hgb<10g/dL)
IC score = Immune infiltrate IC0 = 0, IC1 =1% to <5%,
IC2/3 ≥ 5%.
Powles,T et al. Lancet. 2018;391:748-757.

IMvigor 211: Overall Survival
ITT populationPrimary: OSDid not achieve primary endpoint
IC2/3 populationDid not achieve significance
Powles,T et al. Lancet. 2018;391:748-757.

Lancet 2017; 398: 67-76
PD-L staining IC not important now???

• Definition of Cisplatin ineligible per trial• ECOG PS 2 (32%) as sole reason• GFR 30-60 (49%) as sole reason• Grade 2 hearing loss• Grade 2 peripheral neuropathy• Class III heart failure
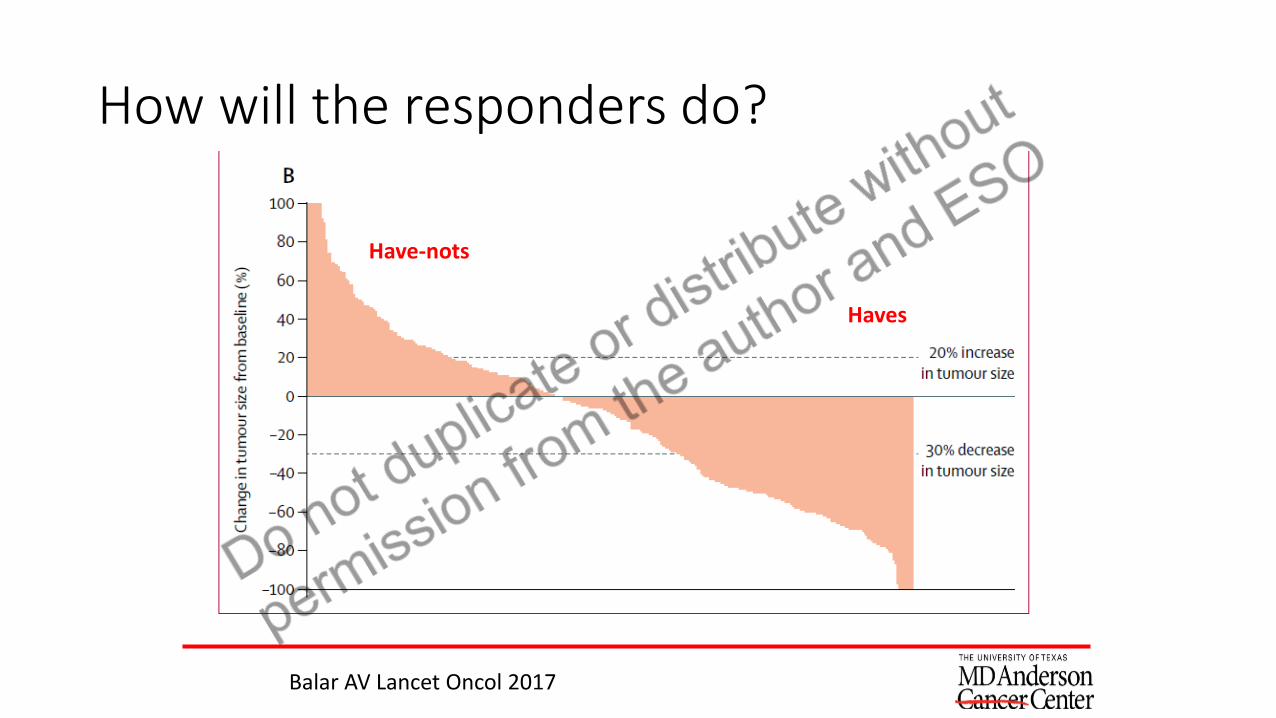
How will the responders do?
Have-nots
Haves
Balar AV Lancet Oncol 2017

NCCN updates every couple of months!!!!!

DrugAb type
PD-L ICH Ab
IC Cut Point
TC Cut Point
Phase/line# subjectsComparator
Tissue ORR total (%)
ORR Based onPD-L status
Atezolizumab(prior platinum)
VENTANA SP142
IC 0 -0%IC 1 <5%IC2/3 ≥5%
None Phase IIN = 310 ptsSingle arm
ARCHIVED Response 15% all comers
26% IC 2/3 (11% CR), 18% IC 1/2/3(6% CR), 10% IC 1 (2%), 8% IC0 (2%)
Atezolizumab(cis-ineligible)Front line
VENTANA SP142
IC 0 -0%IC 1 <5%IC2/3 ≥5%
None Phase IIN = 123 ptsSingle arm
ARCHIVED Response 23% all comers
28% IC 2/3 (13%)24% IC 1/2/3 (10% CR) 21% IC 1 (8.3% CR), 21% IC 0 (7.7% CR)
Nivolumab(prior platinum)
DAKO 28-8 None TC<1%TC≥1%
Phase IIN =78 ptsSingle arm
ARCHIVED Response24% all comers (6% CR)
26% ORR PD-L negative (11/42) (2.3% CR, 1CR), 25% ORR PD-L positive 6/25 (16% CR, 4/25)
Durvalumab(prior platinum)
VENTANA SP263
Combined score IC or TC IC<25% -IC ≥25%+
TC<25% -TC ≥25%+
Phase II61 pts
(after initial 20, only IC>5%allowed)
ARCHIVED OR FRESH
Response 31% 5% CR(only 42 evaluablepatients)
67% PD-L positive (28/42 with + in either domain) 46.4% PD-L positve (13/28) 46.6% TC positive (7/15) , TC negative 22% (6/27)55.5% IC positive (10/18), IC negative 12.5% (3/24)0% if negative both demains (0/14
Avelumab(prior platinum)
DAKO clone 73-10
None TC<5% negTC≥5%+
Phase IbN =44 ptssingle arm
ARCHIVEDOR FRESH
Response18% (11% CR)
64% TC ≥ 5% (7/13, 4 CR) 4.2% TC <5% (1/24 if TC PD-L1 <5%
PembrolizumabVsChemo(prior platinum)
DAKO 22C3 Combined score IC or TC
IC<10% -IC≥10%+
CombinedTC<10% -TC≥10%+
Phase IIIN = 542 pts270 pembro(74PD-L +)272 chemo(90 PD-L+)
ARCHIVED Response21% versus 11% chemo
PD-L+ pembro 22% (CR 7%)PD-L + chemo 7% (CR 2%)
PembrolizumabFront line
DAKO 22C3 Combined
IC<1% -IC ≥1%+
Combined
TC<1% -TC≥1%+
Phase IIN = 374Single arm
FRESH Response24% CR 5%
38% combined PD-L ≥ 10% (42 of 110)27% combined PD-L ≥ 1% (75 of 282)11% combined PD-L <1% (5 of 26)

Case 1
• 83yo retired veteran presents with acute renal failure found to be due to obstructive uropathy

Next Steps
• Patient had bilateral percutaneous nephrostomy tubes placed
• Cystoscopy + TURBT outside bulky tumor in bladder trigone, specimen high grade urothelial cancer invasion into lamina propria, no muscularis propria present

What to Do
• Repeat cystoscopy 5cm mass excised, EUA with fixed irregular mass fixed to anterior rectum
• What additional information would be helpful?

Labs
• Hgb 7.9
• BUN 18, Cr 2.52
• ECOG PS 2
• LVEF 52%
• Severe AS, AVA
0.5cm2/m2
So What Next
• On work up T4bN0M0 stage IV
• Ordered biomarkers, MSI status, molecular alterations panel, Her2neu status, PD-L1 testing (not for treatment decision we are tracking in our group)
• Valve replaced
• Started on pembrolizumab

• Definition of Cisplatin ineligible per trial• ECOG PS 2 (32%) as sole reason• GFR 30-60 (49%) as sole reason• Grade 2 hearing loss• Grade 2 peripheral neuropathy• Class III heart failure

Patient started on immunotherapyPre-treatment Post-treatment

Repeat Cystoscopy with TURBT

Unanswered Questions
• Does this patient need a cystectomy? Would this warrant a rectal resection if so?
• How long does the patient need to be continued on therapy?
• Why did this patient respond?
• When is the best time for a patient to receive immunotherapy?

Case 2
• 62yo male presents with gross hematuria
• On work up found to have a mass originating from his right renal pelvis with associated hydronephrosis
• GFR is 65, no major medical co-morbidities
• On staging no evidence of disease outside of renal pelvis, on ureteroscopy found to have high grade disease invasive into lamina propria no muscularis propria present
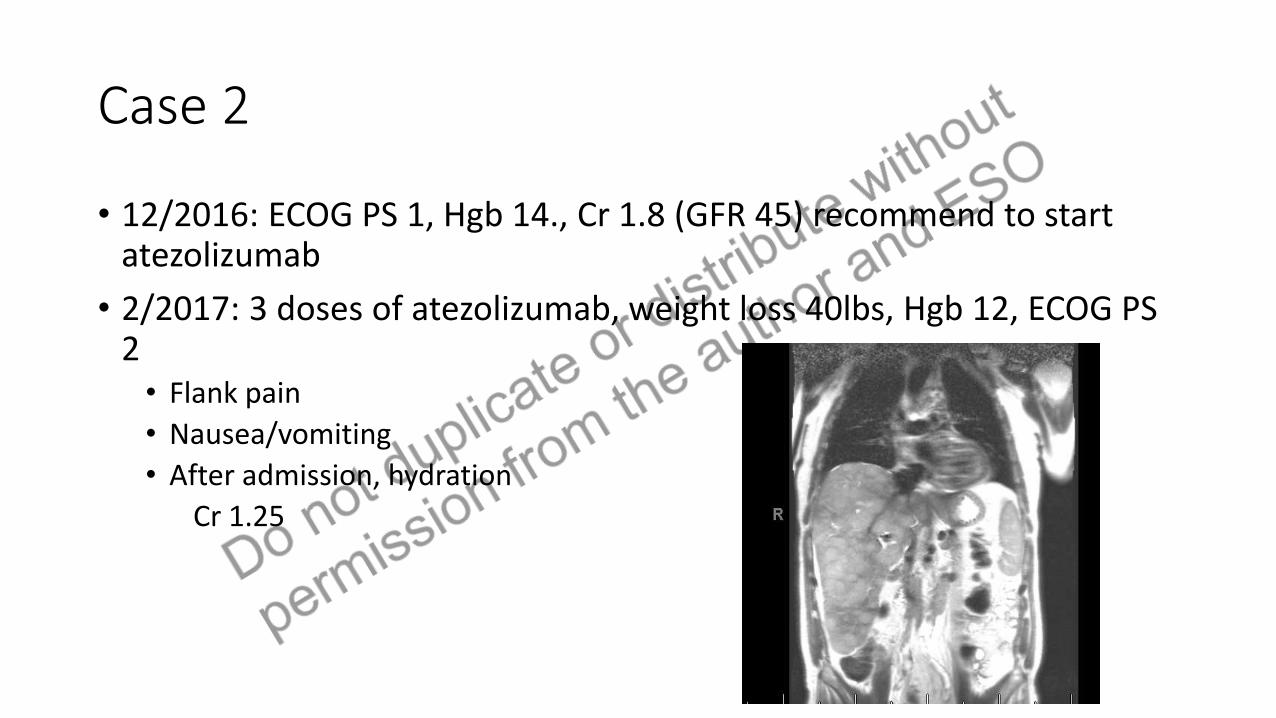
Case 2
• 12/2016: ECOG PS 1, Hgb 14., Cr 1.8 (GFR 45) recommend to start atezolizumab
• 2/2017: 3 doses of atezolizumab, weight loss 40lbs, Hgb 12, ECOG PS 2• Flank pain
• Nausea/vomiting
• After admission, hydration
Cr 1.25

What to do?• Went back to chemo (used CGI: cisplatin 50mg/m2,
gem 900mg/m2 over 90, ifos 1g) (very rocky first month) patient then begins to gain weight, no pain, back to working out PS 0
• CT scan 6/5/17: Major response

Who do we think does extremely well?

A patient with MSI12/2015 Dyspnea severe and sudden, EC found to have PE, large IVC thrombus, R right renal mass12/9/15 Bx Right renal mass Upper tract TCC12/17/15 Flank pain, gross hematuria, RP bleed, psoas hematomaInitiated on GTA 9 cycles last dose 4/28/16
5/26/16: Restaging with disease progression6/2016 Initiated Tecentriq (atezolizumab)2/9/2017: Worsening kidney function and chronic cough Stopped therapyMolecular profiling EGFR mutation, SMAD4 mutation, PTEN mutation
Variants MET and MLH1

Due to have primetime clinical parameters to help us predict?
Hopkins AM. BJC 2017
No
However, there are certainly signs to guide you:
PainWorsening anemiaWorsening albuminWorsening performance status
When these are occuringlikely not pseudoprogression

Ok So Now Where do we go?
• Superficial bladder disease – largest patient population, patients desire to keep bladder at all cost… BCG naïve, BCG refractory
• Muscle invasive bladder cancer – proven lethal disease… single agent IO or combination (what combination?)
• Variant histology bladder cancer – a tough nut to crack
• Lymph node positive bladder cancer – considered stage IV – currently cure 25-30% through chemotherapy+surgery
• What do we do post immunotherapy, does timing matter chemo then IO or IO then chemo or combining as in lung CA…

Chemotherapy + IO

• What will the molecular story add?



Conclusions
• Immunotherapy has added an important new treatment option for patients with mUC
• Understanding patients who will benefit and those who won’t from single agent therapy with anti PD-1/PD-L1 agents is of considerable importance
• A huge number of studies are ongoing that will shape the field for the next decade with the exploration of using these drugs earlier in the disease setting

Acknowledgements
• Clinical GU Med Oncology• Chris Logothetis• Nizar Tannir• Shi-Ming Tu• Pam Sharma• Eric Jonasch• Sumit Subudhi• Paul Corn• John Araujo• Arlene Siefker-Radtke• Jianjun Gao• Jennifer Wang• Eleni Efstathiou• Ana Aparacio• Jeri Kim• Amado Zuria-Saavedra
• Research GU Med Oncology
• Colleagues in Urology
• Colleagues in Radiation Oncology
• Colleagues in Pathology, Radiology, Nursing, Internal Medicine, Surgical Oncology, support staff
• Our institutional collaborators
• My wonderful team: Simi Varghese APN, Mei Wallace RN, Tiffany Razzo AA
• OUR PATIENTS AND THEIR FAMILIES

Questions
• Thank you for the honor of presenting urothelial cancer to you today
http://technorepublica.com/2016/01/18/beautiful-sunset-wallpaper/